

Abstract
Individuals seeking to achieve weight loss are encouraged to achieve a negative energy balance, essentially eat less and move more. The complex relationship between energy expenditure and intake is often overlooked, leaving individuals and practitioners underwhelmed by the results of weight loss efforts. Independently, physical activity and diet interventions can yield modest weight loss and when combined have synergistic effects that promote sustained weight loss. Although physical activity benefits appetite suppression, reduces food rewards, and can be considered a gateway to healthy eating, high levels of daily activity are needed to induce weight loss. Diet is an important component to achieving weight loss, and high-protein diets have the potential for supporting weight loss as well. This column will be focused on the benefits of physical activity in reducing body weight, more specifically, the interdependent relationship between dietary intake and physical activity in achieving weight reduction.
Keywords: exercise, diet, appetite, weight loss
‘Individuals seeking to achieve weight loss are encouraged to achieve a negative energy balance, where energy consumed is lowered and/or energy expended, often through exercise, is increased.’
Physical activity has many immediate and long-term health benefits. In the short-term, just one, single bout of moderate to vigorous physical activity can improve sleep, reduce feelings of anxiety, and lower blood pressure. Over the long-term, regular physical activity is protective against depression, dementia, heart disease, stroke, diabetes, some forms of cancer, weight gain, osteoporosis, and falls. This column will be focused on the benefits of physical activity in reducing body weight, more specifically, the interdependent relationship between dietary intake and physical activity in achieving weight reduction.
Overweight or obesity is often described as the result of prolonged energy imbalance, where energy consumed from foods and beverages exceeds energy expended through resting energy expenditure (REE), thermal effect of food (TEF), spontaneous physical activity (SPA), and exercise (Figure 1). Individuals seeking to achieve weight loss are encouraged to achieve a negative energy balance, where energy consumed is lowered and/or energy expended, often through exercise, is increased. Often oversimplified though is the complex relationship between energy expenditure and intake, leaving individuals and practitioners underwhelmed by the results of weight loss efforts. Figure 2 depicts this relationship, where when exercise is increased, there have been observed compensatory mechanisms in both behavior and biology, whereby levels of energy intake, REE, TEF, and SPA are altered to offset the anticipated negative energy balance created by increasing exercise.1 Understanding this dynamic relationship can allow health care providers and patients to set more realistic and attainable weight loss goals. For example, REE, which makes up approximately 75% of energy utilized each day, is driven by body size, age, and sex, where fat-free mass contributes to a higher energy expenditure than fat mass. Weight loss interventions that include diet alone often yield a greater proportion of weight loss from fat-free mass, leading to a greater reduction in REE, and thus, dieters must further reduce energy intake to continue weight loss. Exercise interventions have demonstrated a protective effect against this loss in fat-free mass and declines in REE, which supports long-term weight loss and weight maintenance.2 Creating an energy imbalance, in favor of weight loss, via increases in exercise alone should, in theory, yield greater weight loss potential. In fact, the Institute of Medicine recommends levels of 60 minutes per day of moderate to vigorous physical activity for weight control.3 This recommendation is supported by 1 randomized clinical trial, where a 12-week exercise program yielded significant weight loss for men and women, when controlling for energy intake, where exercise equated to a 500- to 700-calorie energy deficit per day, and men achieved an 8-kg loss and women, 6 kg.4,5 However, the interindividual differences in weight change in response to exercise interventions have been noted, with questions raised regarding the compensatory behaviors in response to exercise that contribute to this variability.6 Below, the relationships between exercise and food rewards, appetite, diet, and weight management are further explored to underscore the need for both exercise- and diet-induced energy deficits to yield weight reduction.
Figure 1.
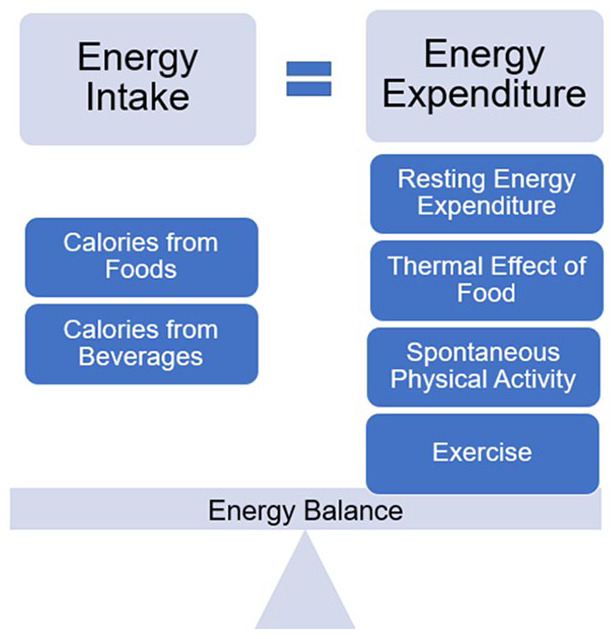
Energy balance equation, described as equivalent energy intake and energy expenditure.
Figure 2.

Complex relationship between increasing exercise and other components of the energy balance equation that contribute to less-than-desired weight loss.
Food Rewards
Food reward is defined as either a “liking” or “wanting” for energy-dense foods, and broadly, food rewards are viewed as an important factor in weight management. The notion that individuals are unsuccessful in attaining weight loss is often blamed on food rewards, where it is hypothesized that high-fat and sugary foods are sought out after exercise. However, a recent review found that increasing levels of habitual physical activity and body fat demonstrated reductions in food rewards, where individuals who accumulated higher levels of moderate to vigorous physical activity showed preference for low-fat foods.7 Another systematic review found a propensity for food reward to decrease after weight loss, in response to weight management interventions; however, the relationship differed across weight management intervention type. Although 4 of the 5 diet interventions did have an impact on food rewards, none of the exercise interventions detected significant impact on food rewards.8 Together, this evidence suggests that, in general, weight management programs can positively influence food rewards when diet and exercise components are included.
Appetite Regulation
Appetite is regulated by a complex system of hormones, peptide YY, glucagon-like peptide 1, ghrelin, insulin, and glucagon. In overweight and obese individuals, appetite dysregulation is hypothesized to contribute to difficulty in weight regulation. There is evidence that suggests that energy deficits created from diet restriction alone, create greater increases in appetite and subsequent diet intake when compared with similar energy deficits created from exercise alone.9-11 In general, evidence suggests that exercise is an important mechanism for regulating appetite when weight loss is desired in lean adults and adults with obesity, with little variation between sexes.11,12 However, the appetite-suppressing effects of exercise appear to diminish in individuals with higher levels of habitual exercise.
Exercise as a Gateway to Improved Health
It is clear that exercise and diet are key factors to health, wellness, and reduction in chronic disease risk. As mentioned, exercise promotes weight loss by preserving fat-free mass, potentially reducing food rewards, and regulating appetite. Exercise behavior is hypothesized to be a gateway behavior for healthy eating across the life span. One study found that, among the elderly, those who were physically active reported improved diet quality, and another study found that in young adults, a high-intensity interval training intervention led to shifts toward a healthier diet.13,14
Diet
Macronutrients—carbohydrates, fat, and protein—all contribute to daily energy intake. Physiologically, each macronutrient has a different TEF, where protein, fat, and carbohydrates all require a different amount of energy to be digested, absorbed, and metabolized, and the components of these macronutrients are differentially preferred for providing energy during fasting. For example, in a fasted state when stored carbohydrate is not available, the body will preferentially utilize stored protein for energy, not fat. With regard to weight loss, energy consumed from each of these macronutrients is not all created equal. As such, much research has been dedicated to studying the macronutrient profile of diet as an important factor for weight loss. High-protein diets are hypothesized to yield greater weight loss because of their ability to preserve fat-free mass and subsequently maintain REE. In fact, energy-restricted diets, high in protein (25%-35% of energy), have been found to yield significant benefits for weight reduction, fat mass loss, and preserving fat-free mass and REE when compared with energy-restricted standard protein (12%-18% of energy) diets.15 Favorable changes in weight and body composition were also achieved in an energy-deficit, high-protein diet (2.4 g of protein per kilogram body weight), where men participated in resistance training and high-intensity interval training 6 days per week. The study showed greater increases in fat-free mass and losses in fat-free mass after the 4-week intervention in the high-protein compared with the lower-protein diet (1.2 g of protein per kilogram body weight).16 Another review of combined diet and exercise interventions for weight loss found that achieving a negative energy balance through diet and exercise is preferred over diet-only interventions, where there is evidence that protein is a limiting factor for maintaining fat-free mass.17
Practice Recommendations
Exercise and diet together are the optimal intervention for weight management and chronic disease prevention, and recommendations from health care providers should address both. Exercise recommendations for weight management include a minimum of 60 min/d of moderate to vigorous exercise. Evidence suggests that energy-restricted, high-protein diets can protect against losses in lean body mass, promote maintenance of REE, and have favorable weight loss outcomes. If available, health care providers should solicit the input of a registered dietitian nutritionist (RDN) and, if available, one with the Certified Specialist in Sports Dietetics (CSSD) credential, who will have specialized experience and expertise in sports and wellness. The RDN can aid in assessing current diet intake, activity levels, and health status to provide a nutrition prescription for energy and protein intake, provide education on foods that can support the patient in meeting those recommendations, and provide counseling to identify strategies to aid patients in implementing behavior change and self-monitoring. Subsequently, the RDN can follow up to monitor the patient’s progress, adjusting energy and protein intake recommendations over time. Health care providers without access to an RDN can encourage patients to consume a diet rich in nutrient-dense foods that are good sources of protein, limit sugary and high-fat foods, and incrementally increase exercise to meet the Institute of Medicine recommendations. Patients can be encouraged to keep food and activity diaries and record diet, physical activity, and changes in weight or fit of clothing to monitor progress.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval: Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent: Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration: Not applicable, because this article does not contain any clinical trials.
References
- 1. Donnelly JE, Smith BK. Is exercise effective for weight loss with ad libitum diet? Energy balance, compensation, and gender differences. Exerc Sport Sci Rev. 2005;33:169-174. [DOI] [PubMed] [Google Scholar]
- 2. Wilmore JH, Stanforth PR, Hudspeth LA, et al. Alterations in resting metabolic rate as a consequence of 20 wk of endurance training: the HERITAGE Family Study. Am J Clin Nutr. 1998;68:66-71. doi: 10.1093/ajcn/68.1.66 [DOI] [PubMed] [Google Scholar]
- 3. Brooks GA, Butte NF, Rand WM, Flatt J-P, Caballero B. Chronicle of the Institute of Medicine physical activity recommendation: how a physical activity recommendation came to be among dietary recommendations. Am J Clin Nutr. 2004;79:921S-930S. doi: 10.1093/ajcn/79.5.921S [DOI] [PubMed] [Google Scholar]
- 4. Ross R, Janssen I, Dawson J, et al. Exercise-induced reduction in obesity and insulin resistance in women: a randomized controlled trial. Obes Res. 2004;12:789-798. doi: 10.1038/oby.2004.95 [DOI] [PubMed] [Google Scholar]
- 5. Ross R, Dagnone D, Jones PJ, et al. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men: a randomized, controlled trial. Ann Intern Med. 2000;133:92-103. doi: 10.7326/0003-4819-133-2-200007180-00008 [DOI] [PubMed] [Google Scholar]
- 6. Foright RM, Presby DM, Sherk VD, et al. Is regular exercise an effective strategy for weight loss maintenance? Physiol Behav. 2018;188:86-93. doi: 10.1016/j.physbeh.2018.01.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Beaulieu K, Oustric P, Finlayson G. The impact of physical activity on food reward: review and conceptual synthesis of evidence from observational, acute, and chronic exercise training studies. Curr Obes Rep. 2020;9:63-80. doi: 10.1007/s13679-020-00372-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Oustric P, Gibbons C, Beaulieu K, Blundell J, Finlayson G. Changes in food reward during weight management interventions—a systematic review. Obes Rev. 2018;19:1642-1658. doi: 10.1111/obr.12754 [DOI] [PubMed] [Google Scholar]
- 9. Cameron JD, Goldfield GS, Riou MÈ, Finlayson GS, Blundell JE, Doucet É. Energy depletion by diet or aerobic exercise alone: impact of energy deficit modality on appetite parameters. Am J Clin Nutr. 2016;103:1008-1016. doi: 10.3945/ajcn.115.115584 [DOI] [PubMed] [Google Scholar]
- 10. Deighton K, Batterham RL, Stensel DJ. Appetite and gut peptide responses to exercise and calorie restriction: the effect of modest energy deficits. Appetite. 2014;81:52-59. doi: 10.1016/j.appet.2014.06.003 [DOI] [PubMed] [Google Scholar]
- 11. Dorling J, Broom DR, Burns SF, et al. Acute and chronic effects of exercise on appetite, energy intake, and appetite-related hormones: the modulating effect of adiposity, sex, and habitual physical activity. Nutrients. 2018;10:1140. doi: 10.3390/nu10091140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Stensel D. Exercise, appetite and appetite-regulating hormones: implications for food intake and weight control. Ann Nutr Metab. 2010;57(suppl 2):36-42. doi: 10.1159/000322702 [DOI] [PubMed] [Google Scholar]
- 13. Stensel D. Exercise as a gateway behavior for healthful eating among older adults: an exploratory study. J Nutr Educ Behav. 2002;34:S14-S19. doi: 10.1016/S1499-4046(06)60306-0 [DOI] [PubMed] [Google Scholar]
- 14. Donati Zeppa S, Sisti D, Amatori S, et al. High-intensity interval training promotes the shift to a health-supporting dietary pattern in young adults. Nutrients. 2020;12:843. doi: 10.3390/nu12030843 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Wycherley TP, Moran LJ, Clifton PM, Noakes M, Brinkworth GD. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2012;96:1281-1298. doi: 10.3945/ajcn.112.044321 [DOI] [PubMed] [Google Scholar]
- 16. Longland TM, Oikawa SY, Mitchell CJ, Devries MC, Phillips SM. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. Am J Clin Nutr. 2016;103:738-746. doi: 10.3945/ajcn.115.119339 [DOI] [PubMed] [Google Scholar]
- 17. Stiegler P, Cunliffe A. The role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss. Sports Med. 2006;36:239-262. doi: 10.2165/00007256-200636030-00005 [DOI] [PubMed] [Google Scholar]