

Abstract
Background
The prevalence of substance use, both prescribed and non‐prescribed, is increasing in many areas of the world. Substance use by women of childbearing age contributes to increasing rates of neonatal abstinence syndrome (NAS). Neonatal opioid withdrawal syndrome (NOWS) is a newer term describing the subset of NAS related to opioid exposure. Non‐pharmacological care is the first‐line treatment for substance withdrawal in newborns. Despite the widespread use of non‐pharmacological care to mitigate symptoms of NAS, there is not an established definition of, and standard for, non‐pharmacological care practices in this population. Evaluation of safety and efficacy of non‐pharmacological practices could provide clear guidance for clinical practice.
Objectives
To evaluate the safety and efficacy of non‐pharmacological treatment of infants at risk for, or having symptoms consistent with, opioid withdrawal on the length of hospitalization and use of pharmacological treatment for symptom management.
Comparison 1: in infants at risk for, or having early symptoms consistent with, opioid withdrawal, does non‐pharmacological treatment reduce the length of hospitalization and use of pharmacological treatment?
Comparison 2: in infants receiving pharmacological treatment for symptoms consistent with opioid withdrawal, does concurrent non‐pharmacological treatment reduce duration of pharmacological treatment, maximum and cumulative doses of opioid medication, and length of hospitalization?
Search methods
We used the standard search strategy of Cochrane Neonatal to search CENTRAL (2019, Issue 10); Ovid MEDLINE; and CINAHL on 11 October 2019. We also searched clinical trials databases and the reference lists of retrieved articles for randomized controlled trials (RCTs), quasi‐RCTs, and cluster trials.
Selection criteria
We included trials comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions. We assessed non‐pharmacological interventions independently and in combination based on sufficient similarity in population, intervention, and comparison groups studied. We categorized non‐pharmacological interventions as: modifying environmental stimulation, feeding practices, and support of the mother‐infant dyad. We presented non‐randomized studies identified in the search process narratively.
Data collection and analysis
We used standard methodological procedures expected by Cochrane. We used the GRADE approach to assess the certainty of evidence. Primary outcomes in infants at risk for, or having early symptoms consistent with, opioid withdrawal included length of hospitalization and pharmacological treatment with one or more doses of opioid or sedative medication. Primary outcomes in infants receiving opioid treatment for symptoms consistent with opioid withdrawal included length of hospitalization, length of pharmacological treatment with opioid or sedative medication, and maximum and cumulative doses of opioid medication.
Main results
We identified six RCTs (353 infants) in which infants at risk for, or having symptoms consistent with, opioid withdrawal participated between 1975 and 2018. We identified no RCTs in which infants receiving opioid treatment for symptoms consistent with opioid withdrawal participated. The certainty of evidence for all outcomes was very low to low. We also identified and excluded 34 non‐randomized studies published between 2005 and 2018, including 29 in which infants at risk for, or having symptoms consistent with, opioid withdrawal participated and five in which infants receiving opioid treatment for symptoms consistent with opioid withdrawal participated. We identified seven preregistered interventional clinical trials that may qualify for inclusion at review update when complete.
Of the six RCTs, four studies assessed modifying environmental stimulation in the form of a mechanical rocking bed, prone positioning, non‐oscillating waterbed, or a low‐stimulation nursery; one study assessed feeding practices (comparing 24 kcal/oz to 20 kcal/oz formula); and one study assessed support of the maternal‐infant dyad (tailored breastfeeding support).
There was no evidence of a difference in length of hospitalization in the one study that assessed modifying environmental stimulation (mean difference [MD) –1 day, 95% confidence interval [CI) –2.82 to 0.82; 30 infants; very low‐certainty evidence) and the one study of support of the maternal‐infant dyad (MD –8.9 days, 95% CI –19.84 to 2.04; 14 infants; very low‐certainty evidence). No studies of feeding practices evaluated the length of hospitalization.
There was no evidence of a difference in use of pharmacological treatment in three studies of modifying environmental stimulation (typical risk ratio [RR) 1.00, 95% CI 0.86 to 1.16; 92 infants; low‐certainty evidence), one study of feeding practices (RR 0.92, 95% CI 0.63 to 1.33; 49 infants; very low‐certainty evidence), and one study of support of the maternal‐infant dyad (RR 0.50, 95% CI 0.13 to 1.90; 14 infants; very low‐certainty evidence).
Reported secondary outcomes included neonatal intensive care unit (NICU) admission, days to regain birth weight, and weight nadir. One study of support of the maternal‐infant dyad reported NICU admission (RR 0.50, 95% CI 0.13 to 1.90; 14 infants; very low‐certainty evidence). One study of feeding practices reported days to regain birth weight (MD 1.10 days, 95% CI 2.76 to 0.56; 46 infants; very low‐certainty evidence). One study that assessed modifying environmental stimulation reported weight nadir (MD –0.28, 95% CI –1.15 to 0.59; 194 infants; very low‐certainty evidence) and one study of feeding practices reported weight nadir (MD –0.8, 95% CI –2.24 to 0.64; 46 infants; very low‐certainty evidence).
Authors' conclusions
We are uncertain whether non‐pharmacological care for opioid withdrawal in newborns affects important clinical outcomes including length of hospitalization and use of pharmacological treatment based on the six included studies. The outcomes identified for this review were of very low‐ to low‐certainty evidence. Combined analysis was limited by heterogeneity in study design and intervention definitions as well as the number of studies. Many prespecified outcomes were not reported. Although caregivers are encouraged by experts to optimize non‐pharmacological care for opioid withdrawal in newborns prior to initiating pharmacological care, we do not have sufficient evidence to inform specific clinical practices. Larger well‐designed studies are needed to determine the effect of non‐pharmacological care for opioid withdrawal in newborns.
Plain language summary
Non‐pharmacological care for opioid withdrawal in newborns
Review question
Do one or more specific non‐pharmacological (treatments other than medicines) care practices benefit newborns with opioid withdrawal after birth?
Background
Newborns of mothers who take opioids during pregnancy often experience symptoms of withdrawal after delivery, such as high‐pitched cry, tremors, and high tone. Non‐pharmacological care is the first treatment for symptoms of withdrawal. If symptoms worsen despite non‐pharmacological care, a medication such as morphine, methadone, or buprenorphine is the second treatment to reduce symptoms. Though non‐pharmacological care is the first approach to symptom management, it is not the same at every hospital. We wanted to discover whether one or more non‐pharmacological care practices benefit newborns with opioid withdrawal after birth.
Study characteristics
We looked at randomized controlled trials (RCTs; clinical studies where people are randomly put into one of two or more treatment groups) of opioid‐exposed newborns treated with one or more non‐pharmacological care practice. Non‐pharmacological care practices include changes to the environment to reduce stimulation or provide soothing, changes to feeding frequency or type, changes that increase maternal care of the newborn or maternal wellness, and multiple changes such as occur in a new site or system of care. Search is up to date as of October 2019.
Key results
This review included six RCTs that enrolled 353 opioid‐exposed newborns. The studies were published between 1975 and 2018. We also identified seven ongoing studies that may qualify for inclusion at review update when complete.
Of the six RCTs, four assessed changes to the environment to reduce stimulation or provide soothing. These studies examined the effect of a mechanical rocking bed, prone positioning (lying on tummy), non‐oscillating waterbed, and a low‐stimulation nursery. We are uncertain whether modifying environmental stimulation is associated with length of hospitalization based on one study with 30 infants. Modifying environmental stimulation may be associated with little or no difference in use of pharmacological treatment based on three studies with 92 infants. We are uncertain whether modifying environmental stimulation is associated with weight nadir (lowest weight recorded during birth hospitalization) based on one study with 194 infants.
One study assessed a change to the feeding type comparing higher‐calorie formula to standard‐calorie formula. We are uncertain whether feeding practices are associated with use of medicines, days to regain birth weight, or weight nadir based on one study with 46 infants.
One study assessed changes to support the mother with tailored breastfeeding support. We are uncertain whether support of the mother‐infant dyad is associated with length of hospitalization, use of medicines, or neonatal intensive care unit admission based on one study with 14 infants.
Many potential important effects were not reported, and others were not reported in all studies.
Quality of evidence
We are uncertain whether one or more specific non‐pharmacological care practices benefit newborns with opioid withdrawal after birth. The quality of evidence for all outcomes is very low to low and provides limited information to inform individual non‐pharmacological care practices or combinations of non‐pharmacological care practices.
Summary of findings
Summary of findings 1. Non‐pharmacological treatment compared to placebo for infants at risk for, or having early symptoms consistent with, opioid withdrawal.
| Non‐pharmacological treatment compared to placebo for infants at risk for, or having early symptoms consistent with, opioid withdrawal | |||||
|
Patient or population: infants at risk for, or having early symptoms consistent with, opioid withdrawal Setting: newborn or neonatal unit, USA and UK Intervention: non‐pharmacological treatment Comparison: placebo | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | |
| Risk with placebo | Risk with non‐pharmacological treatment | ||||
| Primary outcome measures | |||||
| Length of hospitalization (days) | |||||
| – Modifying environmental stimulation | Mean was 11.5 days (SD 3.4) | MD 1 lower (2.82 lower to 0.82 higher) | — | 30 (1 RCT) | ⊕⊝⊝⊝ Very lowa |
| – Feeding practices | — | — | — | — | — |
| – Support of the mother‐infant dyad | Mean was 19.4 days (SD 13) | MD 8.9 lower (19.84 lower to 2.04 higher) | — | 14 (1 RCT) | ⊕⊝⊝⊝ Very lowb |
| Pharmacological treatment with ≥ 1doses of opioid or sedative medication | |||||
| – Modifying environmental stimulation | Study population | RR 1.00 (0.86 to 1.16) | 92 (3 RCTs) | ⊕⊕⊝⊝ Lowc | |
| 844 per 1000 (533 to 1000) |
851 per 1000 (533 to 1000) | ||||
| – Feeding practices | Study population | RR 0.92 (0.63 to 1.33) | 49 (1 RCT) | ⊕⊝⊝⊝ Very lowd | |
| 727 per 1000 | 667 per 1000 | ||||
| – Support of the mother‐infant dyad | Study population | RR 0.50 (0.13 to 1.90) | 14 (1 RCT) | ⊕⊝⊝⊝ Very lowb | |
| 571 per 1000 | 286 per 1000 | ||||
| Secondary outcome measures** | |||||
| NICU admission | |||||
| – Support of the mother‐infant dyad | Study population | RR 0.50 (0.13 to 1.90) | 14 (1 RCT) | ⊕⊝⊝⊝ Very lowb | |
| 571 per 1000 | 286 per 1000 | ||||
| Days to regain birthweight | |||||
| – Feeding practices | Mean was 14.7 days (SD 2.84) | MD 1.1 lower (2.76 lower to 0.56 higher) | — | 46 (1 RCT) | ⊕⊝⊝⊝ Very lowe |
| Weight nadir (% weight loss) | |||||
| – Modifying environmental stimulation | Mean was 5.5% weight loss | MD 0.28 lower (1.15 lower to 0.59 higher) | — | 194 (1 RCT) | ⊕⊝⊝⊝ Very lowf |
| – Feeding practices | Mean was 9.4% weight loss | MD 0.8 lower (2.24 lower to 0.64 higher) | — | 46 (1 RCT) | ⊕⊝⊝⊝ Very lowd |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). **Only interventions that reported on secondary outcomes are included in the 'Summary of findings' table. CI: confidence interval; MD: mean difference; NICU: neonatal intensive care unit; RCT: randomized controlled trial; SD: standard deviation. | |||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aDowngraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and serious concern for imprecision (due to wide CIs). bDowngraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and very serious concern for imprecision (due to very wide CIs). cDowngraded two levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias). dDowngraded three levels for very serious concerns about risk of bias (due to concern for attrition and reporting bias), serious concern about imprecision (due to wide CIs), and plausible confounding that would reduce demonstrated effect. eDowngraded three levels for very serious concerns about risk of bias (due to concern for attrition and reporting bias), very serious concern about imprecision (due to very wide CIs), and plausible confounding that would reduce demonstrated effect. fDowngraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance and detection bias) and serious concern for imprecision (due to wide CIs).
Background
Substance use, both prescribed and non‐prescribed, is an international public health concern. Prevalence is increasing in many areas of the world. Substance use by women of childbearing age contributes to increasing neonatal abstinence syndrome (NAS). Although mothers may have multiple substance exposures, opioid exposure constitutes the majority of cases described historically as NAS (Hudak 2012). Neonatal opioid withdrawal syndrome (NOWS) is a newer term describing the subset of NAS related to opioid exposure (Kelly 2020). For the purposes of this review, we will use the broader term of NAS to include the broader definition used in much of the literature.
Incidence of NAS varies by location, and rising rates are not universal. The incidence of NAS in Australia and England is 2.7 per 1000 hospital births and stable (Davies 2016). The incidence of NAS in the USA and Canada is rising. Incidence increased four‐fold in the USA between 2003 and 2012 to 5.8 per 1000 hospital births, then rose further to 7.0 per 1000 hospital births in 2016 (Corr 2017; HCUP 2019; Patrick 2015a). Incidence of NAS in Canada rose 21% between 2013 and 2017 to 5.2 per 1000 hospital births (CIHI 2018). There is also regional variability within countries. In New South Wales, Australia, incidence of NAS was 3.18 per 1000 hospital births in 2011 (Uebel 2016). Within the USA, there is a wide range in incidence of NAS, ranging from 0.7 to 33.4 per 1000 hospital births (Ko 2016). In 23 USA hospitals, NAS affected a range from less than 1% to 18% of neonatal encounters (Milliren 2018). Genetic, socioeconomic, racial, and local factors including legislation, culture, and medical practices contribute to the variability (Li 2009). Substance use affects all socioeconomic and racial groups, but is disproportionately reported in women of color and low socioeconomic status (Paltrow 2013). Incidence of NAS is 14.4 per 1000 hospital births in the subgroup of low‐income USA infants with public insurance (Winkelman 2018). Punitive state legislation policies are also associated with higher incidence of NAS (Faherty 2019). Under‐recognition and variable use of diagnostic codes may also affect the measured incidence of NAS (Burns 2007; Goyal 2020).
Care for infants with NAS in the neonatal period, and later in childhood, place demands on the medical system, social welfare system, educational system, and society at large. In 2013, infants with NAS occupied 4% of neonatal intensive care unit (NICU) beds in the USA, an increase from 0.6% in only nine years (Tolia 2015). Over 95% of these patients are withdrawing from prenatal exposure (Patrick 2012). Infants with NAS are at increased risk of morbidity or mortality in the neonatal period (Lisonkova 2019; Patrick 2012). Parental substance use is associated with increased child welfare involvement (O'Donnell 2009; Patrick 2019). Later in childhood, children with a history of NAS have an increased risk of rehospitalization (Uebel 2015). Non‐randomized studies demonstrate poorer cognitive and behavioral outcomes through childhood and into high school (Lee 2020; Yeoh 2019). Importantly, many of these associations are based on non‐randomized studies with both recognized and unrecognized complex confounding factors (Larson 2019). Further study is needed to distinguish causation related to opioid exposure versus other social, environmental, or biological factors.
Description of the condition
The contemporary definition of NAS is broad, and includes symptoms associated with prenatal exposure to many substances, both prescribed and non‐prescribed. Symptoms related to withdrawal from opioids, such as methadone, buprenorphine, heroin, oxycodone, and other prescribed and non‐prescribed opioids, may also be described as NOWS. Opioid withdrawal is a unique subset of NAS characterized by common symptomatology and is more likely to respond to postnatal treatment with opioids (Hudak 2012). Polysubstance use is common among opioid users and is associated with more severe NAS (Wachman 2018a). Non‐opioid substance exposures may be associated with NAS due to ongoing toxic effects of exposure (e.g. cocaine) or due to withdrawal following birth (e.g. benzodiazepines). Substances associated with NAS include benzodiazepines, selective serotonin reuptake inhibitors (SSRIs), and tobacco, among other substances. While exposure may occur in isolation or in combination with other substances, most documented NAS is at least partly due to opioids (Hudak 2012).
Infants express varied signs of withdrawal from opioids and other substances following birth. Symptoms are those of dysregulated autonomic, gastrointestinal, and central nervous systems. The most severe manifestations of withdrawal may include seizures, which are likely rare, and severe weight loss. Symptoms of opioid withdrawal peak in the first week of life due to cessation of opioid transfer through the placenta. Infants need medical monitoring and treatment during this period. Symptoms are more severe with maternal methadone maintenance, smoking, and polysubstance exposure (Brogly 2014; Patrick 2015b; Wachman 2018a). Symptoms are less severe in preterm infants; this may be related to a different physiologic response to opioids or a different manifestation of withdrawal in the preterm population (Lemon 2018).
The American Academy of Pediatrics recommends standardized assessment of symptom severity (Hudak 2012). Published standardized withdrawal assessment tools include the Finnegan Neonatal Abstinence Scoring Tool (score range 0 to 62) (Finnegan 1975), Lipsitz Neonatal Drug Withdrawal Scoring System (score range 0 to 20) (Lipsitz 1975), Neonatal Narcotic Withdrawal Index (score range 0 to 14) (Green 1981), Neonatal Withdrawal Inventory (score range 0 to 19) (Zahorodny 1998), and Maternal Opioid Treatment: Human Experimental Research (MOTHER) NAS scale (score range 0 to 42) (Jones 2010). Several recent efforts have been made to simplify scoring. Examples include Finnegan Neonatal Abstinence Syndrome Scale – Short Form (score range 0 to 16) (Maguire 2013), MOTHER NAS Short Form (score range not reported) (Jones 2016a), simplified Finnegan Neonatal Abstinence Scoring System (score range 0 to 23) (Gomez Pomar 2017), a new scoring system for NAS (score range 0 to 27) (Kocherlakota 2020), and the eight‐item simplified Finnegan Neonatal Abstinence Scoring System (score range 0 to 8) (Devlin 2020). Each tool assesses a combination of symptoms of opioid or non‐opioid withdrawal; however, most tools were designed in a time when single drug use was common, primarily heroin. Most hospitals use a version of the Finnegan Neonatal Abstinence Scoring Tool (Mehta 2013; Sarkar 2006; Snowden 2019); however, the pharmacological treatment threshold is not validated and the tool has poor psychometric properties and poor internal consistency (Jones 2016b). Newer approaches in the USA shift from reliance on a threshold score to initiate pharmacological treatment to an approach based on a care pathway. One example focuses on early modulation of symptoms with a standard non‐pharmacological care bundle including family involvement and a more nuanced evaluation of critical functional symptoms including the infant's ability to eat, sleep, and be consoled (Grossman 2018; Wachman 2018b).
The first‐line treatment for NAS is non‐pharmacological care (Hudak 2012; Mangat 2019). Severe symptoms despite maximal non‐pharmacological treatment mark a threshold for pharmacological treatment. Though norms exist, scores are often subjective, and treatment thresholds established based on historical norms are not validated. Pharmacological treatments that reduce withdrawal symptoms include opioid or sedative medications, or both. Morphine is the most common opioid treatment; methadone and buprenorphine are also used (Patrick 2016; Snowden 2019). Adjunctive therapies may include phenobarbital and clonidine to address polysubstance exposure. Long‐term developmental impact of pharmacological treatment is unclear. Immediate adverse effects of pharmacological treatment include respiratory depression and sedation. Most hospitals care for infants receiving sedating medications on a cardiac monitor in the intensive care unit (ICU) (Milliren 2018). Unfortunately, ICU care separates infants from caregivers and often is a high stimulus environment. This interferes with bonding, caregiver self‐efficacy, and full non‐pharmacological treatment, potentially affecting severity of NAS symptoms.
The approach to care for infants with NAS has wide variation (Bogen 2017; Mehta 2013; O'Grady 2009; Patrick 2016; Sarkar 2006; Snowden 2019). Surveys show differences in prenatal counseling, written policies, staff training, threshold for pharmacological treatment, weaning protocols, breastfeeding support, and location of care, among other aspects of care (Bogen 2017; Mehta 2013; Patrick 2016; Snowden 2019). Most hospitals use a standardized withdrawal assessment tool; however, hospitals have differing treatment protocols. Almost half lack a written policy for management of opioid‐exposed newborns (Patrick 2016; Sarkar 2006). There is no clear standard for non‐pharmacological care or pharmacological treatment thresholds (Mehta 2013). Non‐pharmacological treatment and pharmacological treatment thresholds are not well studied and likely vary between centers. Most importantly, efforts to standardize hospital policies are associated with improved outcomes (Patrick 2016).
Outcomes such as pharmacological treatment rate and length of hospital stay also vary widely. The percent of infants who receive pharmacological therapy ranges from 13% to 90% (Milliren 2018). The mean length of stay at some centers in the USA is as low as 5.9 days, while the national mean is 16.9 days (Grossman 2017; Patrick 2015a).
Variations in diagnosis and management of NAS represent an important opportunity to improve care. Multicenter quality improvement collaboratives in the USA show that increased standardization of care can reduce length of hospital stay (Hall 2015; Patrick 2016). Emerging evidence suggests that standardization of non‐pharmacological care also reduces length of hospital stay and use of pharmacological treatment (Grossman 2017; Holmes 2016; Wachman 2018b).
Description of the intervention
Non‐pharmacological treatments focus on minimizing dysregulation and maximizing infant functioning. Treatments are heterogeneous interventions within three main categories of care:
modifying environmental stimulation;
feeding practices; and
support of the mother‐infant dyad.
Interventions may occur alone, or in combination with other non‐pharmacological and pharmacological treatments. The 'dose' of non‐pharmacological intervention is difficult to assess, and may be related to timing, intensity, quality, consistency, and adequacy of interventions among other features.
Modifying environmental stimulation
Treatments addressing environmental stimulation reduce negative stimuli and promote positive experiences. Gentle handling and maintaining a low‐light, quiet environment reduce negative stimulation. Infant containment or swaddling, bedding choice including vibrating beds, and infant positioning may also soothe infants. Positive experiences may include non‐nutritive sucking and bathing. Aromatherapy, music therapy, massage, and acupuncture/acupressure are therapies that may also calm infants through stimulation.
Feeding practices
Disorganized feeding and weight loss are common in infants withdrawing from opioids. In general, breast milk and breastfeeding reduce withdrawal symptoms (Jansson 2009). Small, frequent feedings and infant‐led feeding are often helpful in improving the transfer of food. Higher‐calorie feedings or tube feedings may reduce weight loss and improve satiety in these infants. Non‐maternal or maternal breast milk or low‐lactose formula may reduce gas and feeding discomfort.
Support of the mother‐infant dyad
Treatments also address the health and support of the mother‐infant dyad as a unit (Krans 2019; Velez 2009). Parental presence alone is an important aspect of non‐pharmacological care (Howard 2017). Rooming in (where the baby's crib is kept by the side of the mother's bed) and skin‐to‐skin care promote mother‐infant bonding and infant regulation. Direct parental support promotes parental well‐being. Well caregivers are better able to recognize and respond to infant cues. Parental supports enhance comfort and plan for respite. Examples include 'cuddler' programs (where cuddling the baby is maximized) and designated spaces in the hospital to promote parent comfort. Staff contribute to parental well‐being by using trauma‐informed care principles. A comprehensive biopsychosocial needs assessment may also improve parental well‐being and prompt referral for comprehensive integrated care (Krans 2019). Needs may include addiction, social, mental health, legal, and custody supports.
How the intervention might work
Many non‐pharmacological practices improve autonomic regulation for infants and could mitigate the autonomic dysregulation noted in infants with NAS.
Environmental changes and feeding practices, individually and in combination, can affect physiologic parameters in infants. Facilitated tucking by holding the infant in a gently flexed position lowers stress‐related behaviors and vital sign changes in infants (Liaw 2012). Human touch through massage improves weight gain, growth, and sleep in infants (Juneau 2015). Non‐nutritive sucking and acupressure are associated with reduced infant pain response (Chen 2017; Pinelli 2002). Breastfeeding and breast milk odor are each associated with reduced infant pain response (Carbajal 2003; Gray 2002; Zhang 2018). Breastfeeding, especially combined with maternal holding, is associated with widespread cortical activity distinct from that of glucose exposure alone (Bembich 2018).
Maternal interaction and presence have many unique benefits for the infant, likely related to complex and multifactorial sensory stimuli involved in interactions within the mother‐infant dyad. Skin‐to‐skin contact between caregiver and infant (also termed 'kangaroo care') is associated with a reduced infant pain response (Gray 2000; Johnston 2017; Pandita 2018; Shah 2012). Mother's presence and tactile contact improve visual attention in term infants (Arditi 2006). Maternal well‐being and functioning appear to affect infant regulation. Sensitive maternal caregiving as measured by the Emotional Availability Scales is associated with lower infant cortisol and improved infant regulation (Kaplan 2008). Relationships between parents, specifically the levels of avoidance and dyadic adjustment, are associated with infant vagal tone (Graham 2010).
This literature suggests that non‐pharmacological measures affect autonomic functioning and are likely to attenuate withdrawal symptoms due to dysregulation in NAS.
Why it is important to do this review
Other Cochrane Reviews address the evidence for, and comparative effectiveness of, pharmacological treatments including opiates, sedatives, and naloxone treatments for opioid‐exposed newborns (Moe‐Byrne 2018; Osborn 2010a; Osborn 2010b). The reviews conclude that initial pharmacological treatment of neonatal opioid withdrawal should be an opiate. Opiates reduce the time to regain birth weight but increase the length of hospital stay. Adding a sedative may further reduce symptoms. Given the methodologic limitations of the included studies, further firm recommendations are not made.
Non‐pharmacological interventions are not assessed or controlled in most studies focused on pharmacological treatments for NAS. The use and 'dose' of non‐pharmacological care may be an important confounder in these studies. Standardized non‐pharmacological care may improve care outcomes (Grossman 2017; Holmes 2016; Wachman 2018b). Evidence for non‐pharmacological interventions will guide future efforts to improve care. This review evaluated the current literature and gaps in research regarding non‐pharmacological care. Acupuncture and acupressure will be addressed in a separate Cochrane Review, and was not included in this review.
Objectives
To evaluate the safety and efficacy of non‐pharmacological treatment of infants at risk for, or having symptoms consistent with, opioid withdrawal on the length of hospitalization and use of pharmacological treatment for symptom management.
Comparison 1: in infants at risk for, or having early symptoms consistent with, opioid withdrawal, does non‐pharmacological treatment reduce the length of hospitalization and use of pharmacological treatment?
Comparison 2: in infants receiving pharmacological treatment for symptoms consistent with opioid withdrawal, does concurrent non‐pharmacological treatment reduce duration of pharmacological treatment, maximum and cumulative doses of opioid medication, and length of hospitalization?
Methods
Criteria for considering studies for this review
Types of studies
We included randomized controlled trials (RCTs), quasi‐RCTs, and cluster trials in our formal analysis (see Selection of studies). We excluded cross‐over trials.
Types of participants
Inclusion criteria
Comparison 1
Term (37 weeks' gestation or greater) and late preterm infants (34 weeks' gestation to 37 weeks' gestation) with known or suspected prenatal opioid exposure or having opioid withdrawal in the first seven days of life.
Comparison 2
Term (37 weeks' gestation or greater) and late preterm infants (34 weeks' gestation to 37 weeks' gestation) on opioid treatment for opioid withdrawal in the first 28 days of life.
Opioid withdrawal may have been defined by the presence of symptoms consistent with opioid withdrawal or an elevated score on a standardized withdrawal assessment tool.
Symptoms consistent with opioid withdrawal are those of dysregulated autonomic, gastrointestinal, and central nervous systems. Symptoms included, but were not limited to: increased crying, irritability, inability to sleep, tremors, increased tone, myoclonic jerks, fever, sweating, rapid breathing, labored breathing, sneezing, yawning, unco‐ordinated feeding, excessive sucking, vomiting, loose stools, and excessive weight loss.
Scores are often used to quantify the symptoms and provide information to guide pharmacological treatment. Elevated scores on standardized withdrawal assessment tools include Finnegan Neonatal Abstinence Scoring Tool score above 8 (Finnegan 1975), Lipsitz Neonatal Drug Withdrawal Scoring System score above 4 (Lipsitz 1975), Neonatal Narcotic Withdrawal Index score above 5 (Green 1981), Neonatal Withdrawal Inventory score above 8 (Zahorodny 1998), MOTHER NAS score above 9 (Jones 2010), Finnegan Neonatal Abstinence Syndrome Scale – Short Form score above 8 (Maguire 2013), or a score exceeding the stated threshold on any novel validated assessment tool.
Exclusion criteria
Preterm infants less than 34 weeks' gestation.
Critically ill term and late preterm infants (greater than 34 weeks' gestation) with medical comorbidities unrelated to opioid withdrawal. Medical comorbidities included but were not limited to the need for mechanical ventilation (positive pressure ventilation), culture‐confirmed infection, necrotizing enterocolitis, major congenital anomaly, and status postmajor surgical intervention.
Types of interventions
Comparison 1
Trials comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions in infants at risk for, or having early symptoms consistent with, opioid withdrawal as defined above.
Comparison 2
Trials comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions in infants receiving opioid treatment for symptoms consistent with opioid withdrawal as defined above.
Non‐pharmacological care is a heterogeneous group of interventions addressing three aspects of care, as follows.
Modifying environmental stimulation: adjustments of environmental stimulation include low light, low noise, clustered care, containment or swaddling, bedding type, positioning, non‐nutritive sucking, bathing, aromatherapy, music therapy, and massage.
Feeding practices: feeding modifications include infant‐led feeding, high caloric feedings, tube feedings, maternal breast milk feedings, non‐maternal breast milk feedings, low‐lactose formula, and breastfeeding.
Support of the mother‐infant dyad: treatments focused on the mother‐infant dyad include parental presence, rooming in, skin‐to‐skin or 'kangaroo care,' parental respite or 'cuddler' programs, trauma‐informed care, social work support, mental health support, treatment program support, and legal support.
Bundled non‐pharmacological interventions: multiple non‐pharmacological interventions delivered in combination.
We assessed non‐pharmacological interventions independently and in combination based on sufficient similarity in population, intervention, and comparison groups studied.
Types of outcome measures
Primary outcomes
Comparison 1
Length of hospitalization (days).
Pharmacological treatment with one or more doses of opioid or sedative medication.
Comparison 2
Length of hospitalization (days).
Length of pharmacological treatment with opioid or sedative medication (days).
Maximum and cumulative dose of opioid medication (milligrams/kilogram and morphine milligram equivalents).
Secondary outcomes
Peak NAS score in first 72 hours of life as measured by a standardized withdrawal assessment tool. Tools included the Finnegan Neonatal Abstinence Scoring Tool (score range 0 to 62) (Finnegan 1975), Lipsitz Neonatal Drug Withdrawal Scoring System (score range 0 to 20) (Lipsitz 1975), Neonatal Narcotic Withdrawal Index (score range 0 to 14) (Green 1981), Neonatal Withdrawal Inventory (score range 0 to 19) (Zahorodny 1998), MOTHER NAS scale (score range 0 to 42) (Jones 2010), or Finnegan Neonatal Abstinence Syndrome Scale – Short Form (score range 0 to 16) (Maguire 2013). Separate assessments were made for each score (Comparison 1 only).
NICU admission (Comparison 1 only).
Length of NICU stay (days).
-
Physical growth: weight:
days to regain birth weight;
growth during study period and hospital stay (grams/day); growth velocity (grams/kg/day or change in z‐score);
weight nadir (percent weight loss) (Fenton 2017).
Neonatal seizures (any seizures, clinical seizures, electroencephalogram [EEG]‐confirmed seizures; seizure treated with anticonvulsant therapy).
Neonatal and infant all‐cause mortality.
Cerebral palsy (clinical cerebral palsy diagnosed if the child had a non‐progressive motor impairment characterized by abnormal muscle tone and decreased range or control of movements). If data were available, we determined the level of gross motor function using the Gross Motor Function Classification System (Palisano 1997).
Neurodevelopmental outcome at approximately two years' corrected age (acceptable range 18 months to 28 months) including: cerebral palsy, significant mental developmental delay (Bayley Scales of Infant Development Mental Developmental Index less than 70 or Griffith 2 standard deviations [SD] below mean) (Bayley 1993; Chaudhary 2013), legal blindness (less than 20/200 visual acuity), and hearing deficit (aided or less than 60 dB on audiometric testing). The composite outcome 'neurodevelopmental impairment' was defined as having any one of the aforementioned deficits (modified from definitions of moderate‐to‐severe developmental delay) (Schmidt 2007).
Complications of therapy: apnea, need for positive pressure ventilation, need for oxygen, somnolence.
Measures of maternal mood and bonding including Edinburgh Postpartum Depression Scale (Cox 1987), Patient Health Questionnaire (2 or 9) (Kroenke 2001; Whooley 1997), Maternal Attachment Inventory (Muller 1994), Maternal Postpartum Attachment Scale (Condon 1998), Mother‐Infant Bonding Scale (Taylor 2005), or Postpartum Bonding Questionnaire (Brockington 2006). Separate comparisons were made for each score.
Custody status at discharge.
Cost of care: including economic analyses of the impact of care practices including total hospitalization cost or charges per patient.
Post hoc
Peak NAS score in first 72 hours of life definition expanded to include either a 'peak' score at any time or a score in the first 72 hours as measured by a standardized withdrawal assessment tool as described above (Comparison 1 only).
We added a secondary outcome, cost of care, to include economic analyses of the impact of care practices including total hospitalization cost or charges per patient.
Search methods for identification of studies
We used the criteria and standard methods of Cochrane and Cochrane Neonatal (see the Cochrane Neonatal search strategy for specialized register [neonatal.cochrane.org/resources-review-authors]). We searched for errata or retractions from included studies published in full text on PubMed (www.ncbi.nlm.nih.gov/pubmed), and reported the date this was done in the review.
Electronic searches
We conducted a comprehensive search including: Cochrane Central Register of Controlled Trials (CENTRAL 2019, Issue 10) in the Cochrane Library; Ovid MEDLINE(R) and Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Daily and Versions(R) (1946 to 11 October 2019); and CINAHL (1981 to 11 October 2019). We included the search strategies for each database in Appendix 1. We applied no language restrictions.
We searched clinical trial registries for ongoing or recently completed trials. We searched the World Health Organization's International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en/), and the US National Library of Medicine's ClinicalTrials.gov (clinicaltrials.gov), via Cochrane CENTRAL. Additionally, we searched the ISRCTN Registry for any unique trials not found through the Cochrane CENTRAL search.
The search strategies for the protocol are in Appendix 2 (Pahl 2018).
Searching other resources
We also searched the reference lists of all identified articles for relevant articles not located in the primary search.
Data collection and analysis
We collected information regarding the method of randomization, blinding, intervention, stratification, and whether the trial was single or multicenter for each included study. We noted information regarding trial participants including gestational age criteria, birth weight criteria, and other inclusion or exclusion criteria. We analyzed the clinical outcomes listed above in Types of outcome measures.
Selection of studies
We included all RCTs, quasi‐RCTs, and cluster trials fulfilling our inclusion criteria. Both superiority trials and non‐inferiority trials were eligible for inclusion. All review authors reviewed the results of the search and separately selected studies for inclusion. We resolved any disagreements by discussion.
We recorded the selection process in sufficient detail to complete a PRISMA flow diagram (Figure 1), and Characteristics of excluded studies table (Moher 2009).
1.
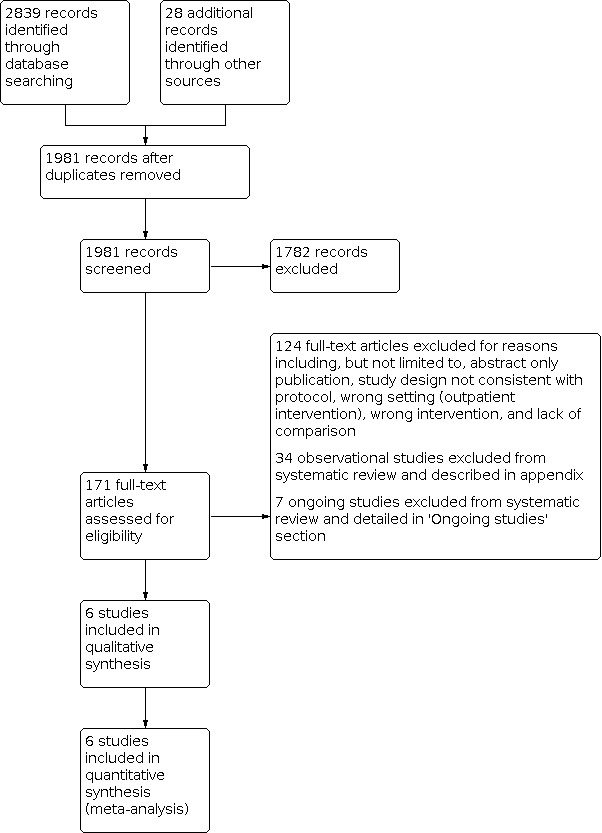
Study flow diagram.
We excluded non‐randomized studies and presented these studies narratively in Appendix 3.
Data extraction and management
Two review authors (AP and RS) extracted, assessed, and coded all data for each study, using a form designed specifically for this review. We replaced any standard error of the mean by the corresponding SD. We resolved any disagreements by discussion. For each study, one review author (AP) entered final data into Review Manager 5 (Review Manager 2020), which a second review author (RS) checked. All review authors reviewed the protocol, analysis, and draft manuscript.
Assessment of risk of bias in included studies
Two review authors (AP and RS) independently assessed the risk of bias (low, high, or unclear) of all included RCTs using the Cochrane 'Risk of bias' tool for the following domains (Higgins 2011).
Sequence generation (selection bias).
Allocation concealment (selection bias).
Blinding of participants and personnel (performance bias).
Blinding of outcome assessment (detection bias).
Incomplete outcome data (attrition bias).
Selective reporting (reporting bias).
Any other bias.
We resolved any disagreements by discussion or by consulting a third review author. See Appendix 4 for a more detailed description of risk of bias for each domain.
Measures of treatment effect
We performed the statistical analyses using Review Manager 5 (Review Manager 2020). We analyzed categorical data using risk ratio (RR) and risk difference (RD). We reported 95% confidence intervals (CIs) for all outcomes. For statistically significant outcomes, we calculated the number needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH). We calculated mean differences (MDs) between treatment groups where outcomes were measured in the same way and standardized mean differences (SMDs) where outcomes were measured using different scales for continuous data.
Unit of analysis issues
The unit of analysis was the participating infant in individually randomized trials, and an infant was considered only once in the analysis. The participating neonatal unit or section of a neonatal unit or hospital was the unit of analysis in cluster‐RCTs. While we identified no cluster RCTs, we planned to analyze them using an estimate of the intracluster correlation coefficient (ICC) derived from the trial (if possible), or from a similar trial or from a study with a similar population as described in Section 23.1.4 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2019). If we had used ICCs from a similar trial, or from a study with a similar population, we planned to report this and conduct a sensitivity analysis to investigate the effect of variation in the ICC. We identified no cluster trials and performed no sensitivity analysis.
If we identified both cluster‐RCTs and individually randomized trials, we would only combine the results from both if there was little heterogeneity between the study designs, and the interaction between the effect of the intervention and the choice of randomization unit was considered unlikely.
We acknowledged any possible heterogeneity in the randomization unit and performed a sensitivity analysis to investigate possible effects of the randomization unit.
Dealing with missing data
Where feasible, we carried out analysis on an intention‐to‐treat basis for all outcomes. Whenever possible, we analyzed all participants in the treatment group to which they were randomized, regardless of the actual treatment received. If we identified important missing data (in the outcomes) or unclear data, we requested the missing data by contacting the original investigators. We made explicit the assumptions of any methods used to deal with missing data. The search identified few studies for each intervention; therefore, sensitivity analyses were not performed. We addressed the potential impact of missing data on the findings of the review in the Discussion section of the review.
Assessment of heterogeneity
We estimated the treatment effects of individual trials and examined heterogeneity among trials by inspecting the forest plots and quantifying the impact of heterogeneity using the I² statistic. We graded the degree of heterogeneity as: less than 25%, no heterogeneity; 25% to 49%, low heterogeneity; 50% to 75%, moderate heterogeneity; more than 75%, substantial heterogeneity. If we noted statistical heterogeneity (I² greater than 50%), we explored the possible causes (e.g. differences in study quality, participants, intervention regimens, or outcome assessments).
Assessment of reporting biases
We conducted a comprehensive search for eligible studies and were alert for duplication of data. If we had identified 10 or more trials for meta‐analysis, we planned to assess possible publication bias by inspection of a funnel plot. If we uncovered reporting bias that could, in the opinion of the review authors, introduce serious bias, we planned to conduct a sensitivity analysis to determine the effect of including and excluding these studies in the analysis.
Data synthesis
If we identified multiple studies that we considered to be sufficiently similar, we performed meta‐analysis using Review Manager 5 (Review Manager 2020). We determined study similarity based on concordance of population, intervention or combination of interventions, and comparison group. For categorical outcomes, we calculated the typical estimates of RR and RD, each with its 95% CI; for continuous outcomes, we calculated the MD or SMD, each with its 95% CI. We used a fixed‐effect model to combine data where it was reasonable to assume that studies were estimating the same underlying treatment effect. If we judged meta‐analysis to be inappropriate, we analyzed and interpreted individual trials separately. If there was evidence of clinical heterogeneity, we tried to explain this based on the different study characteristics and subgroup analyses.
Subgroup analysis and investigation of heterogeneity
Planned subgroup analyses
Gestational age (late preterm [34 weeks' gestation to 37 weeks' gestation], term (37 weeks' gestation or greater]).
Birth weight (less than 2500 g or 2500 g or greater).
-
Type of non‐pharmacological intervention:
environmental stimulation: adjustments of environmental stimulation include low light, low noise, clustered care, containment or swaddling, bedding type, positioning, non‐nutritive sucking, bathing, aromatherapy, music therapy, and massage;
feeding practices: feeding modifications include infant‐led feeding, high‐caloric feedings, tube feedings, maternal breast milk feedings, non‐maternal breast milk feedings, low‐lactose formula, and breastfeeding;
support of the mother‐infant dyad: treatments focused on the mother‐infant dyad included parental presence, rooming in, skin‐to‐skin or 'kangaroo care,' parental respite or 'cuddler' programs, trauma‐informed care, social work support, mental health support, treatment program support, and legal support.
Prenatal opioid exposure: polysubstance use, single substance (opioid) use, prescribed opioid, non‐prescribed opioid, not known.
-
Other prenatal substance exposures:
nicotine exposure: nicotine use, no nicotine use;
alcohol exposure (based on maternal history or evidence of fetal alcohol spectrum disorder);
SSRI exposure.
Maternal social situation (custody status, homelessness, employment status, public insurance, ethnicity, involvement of birth father, marital status, family support).
We did not attempt to perform the subgroup analyses proposed due to insufficient similarity in population, intervention, and comparison groups studied. Few studies were identified for each non‐pharmacological intervention with significant differences between studies.
Sensitivity analysis
We identified few studies for each intervention and did not conduct sensitivity analysis.
Summary of findings and assessment of the certainty of the evidence
We used the GRADE approach, as outlined in the GRADE Handbook (Schünemann 2013), to assess the certainty of evidence for the following (clinically relevant) outcomes for comparison one.
Comparison 1
Length of hospitalization (days).
Pharmacological treatment with opioid or sedative medication.
Peak NAS score in first 72 hours of life.
NICU admission.
Neonatal seizures requiring anticonvulsant therapy.
Neurodevelopmental outcome at approximately two years' corrected age (cerebral palsy, developmental delay [Bayley or Griffith assessment more than two SD below mean] or intellectual impairment (intelligence quotient [IQ] more than two SD below mean), blindness (vision less than 6/60 in both eyes), sensorineural deafness requiring amplification.
Measures of maternal mood and bonding including Edinburgh Postpartum Depression Scale, Patient Health Questionnaire (2 or 9), Maternal Attachment Inventory, Maternal Postpartum Attachment Scale, Mother‐Infant Bonding Scale, or Postpartum Bonding Questionnaire (Brockington 2006; Condon 1998; Cox 1987; Kroenke 2001; Muller 1994; Taylor 2005; Whooley 1997)
We planned to assess the certainty of evidence for the following (clinically relevant) outcomes for comparison two.
Comparison 2
Length of hospitalization (days).
Length of pharmacological treatment with opioid or sedative medication (days).
Maximum and cumulative dose of opioid medication (morphine milligram equivalents).
Length of NICU stay.
Neonatal seizures requiring anticonvulsant therapy.
Neurodevelopmental outcome at approximately two years' corrected age (cerebral palsy, developmental delay [Bayley or Griffith assessment more than two SD below mean] or intellectual impairment [IQ] more than two SD below mean), blindness (vision less than 6/60 in both eyes), sensorineural deafness requiring amplification.
Measures of maternal mood and bonding including Edinburgh Postpartum Depression Scale, Patient Health Questionnaire (2 or 9), Maternal Attachment Inventory, Maternal Postpartum Attachment Scale, Mother‐Infant Bonding Scale, or Postpartum Bonding Questionnaire (Brockington 2006; Condon 1998; Cox 1987; Kroenke 2001; Muller 1994; Taylor 2005; Whooley 1997).
Two review authors (AP and RS) independently assessed the certainty of the evidence for each of the outcomes listed above. We considered evidence from RCTs as high certainty, downgrading the evidence one level for serious (or two levels for very serious) limitations based upon the following: design (risk of bias), consistency across studies, directness of the evidence, precision of estimates, and presence of publication bias.
We used GRADEpro GDT to create Table 1 to report the certainty of the evidence for comparison one.
The GRADE approach results in an assessment of the certainty of a body of evidence as one of four grades.
High certainty: further research is very unlikely to change our confidence in the estimate of effect.
Moderate certainty: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low certainty: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low certainty: we are very uncertain about the estimate.
Results
Description of studies
Included studies
The search identified six RCTs evaluating non‐pharmacological care for opioid withdrawal published between 1975 and 2018 (Characteristics of included studies table). Four studies compared modifications of environmental stimulation (D'Apolito 1999; Maichuk 1999; Oro 1988; Ostrea 1975), one study compared feeding practices (Bogen 2018), and one study compared interventions targeting support of the mother‐infant dyad (MacVicar 2018). Two studies were RCTs due to use of computer‐generated randomization (Bogen 2018; MacVicar 2018), one was classified as a quasi‐RCT due to randomization by hospital record number (Oro 1988), and three reported randomization of study participants without further details about the methods and may represent RCTs or quasi‐RCTs (D'Apolito 1999; Maichuk 1999; Ostrea 1975). The search identified no cluster trials.
Excluded studies
The search identified 34 non‐randomized studies published between 2005 and 2018 comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions for opioid withdrawal in newborns (see Characteristics of excluded studies table; Table 2; Table 3; Table 4; Table 5; and Appendix 3).
1. Excluded studies of modifying environmental stimulation.
| Study | Details | |
| Radziewicz 2018 | Methods | Prospective cohort |
| Participants | 30 newborns at risk for withdrawal in a newborn nursery | |
| Time period | Not reported | |
| Site of care | Newborn nursery (Ohio, USA) | |
| Interventions | Quote: "Each subject received one thirty‐minute treatment of Reiki in a private room." | |
| Outcomes |
|
|
| Notes | — | |
| Zuzarte 2017 | Methods | Prospective cohort (within‐subjects) |
| Participants | 26 opioid‐exposed newborns (> 37 weeks' gestation) treated pharmacologically for NAS | |
| Time period | Not reported | |
| Site of care | Neonatal intensive care unit and newborn nursery (Massachusetts, USA) | |
| Interventions | Quote: "A specially‐constructed mattress delivered low‐level SVS (30–60Hz, 10–12μm RMS [root‐mean‐square]), alternated in 30‐min intervals between continuous vibration (ON) and no vibration (OFF) over a 6–8 hr session." | |
| Outcomes |
|
|
| Notes | — | |
NAS: neonatal abstinence syndrome; SVS: stochastic vibrotactile stimulation.
2. Excluded studies of feeding practices.
| Study | Details | |
| Abdel‐Latif 2006 | Methods | Retrospective cohort |
| Participants | 190 consecutive drug‐dependent mother‐infant pairs | |
| Time period | 1998–2004 | |
| Site of care | Postnatal ward with mother unless medical or social contraindications (New South Wales, Australia) | |
| Interventions | Predominant feed on day 5 of life: ≤ 2 feeds daily of formula (85 infants) or > 2 feeds daily of formula (105 infants) | |
| Outcomes | ≤ 2 feeds daily of formula vs > 2 feeds daily of formula
|
|
| Notes | More heroin, non‐opioid, and polydrug use in formula group Emailed authors to clarify data |
|
| Arlettaz 2005 | Methods | Retrospective cohort |
| Participants | 86 infants of women enrolled in a methadone maintenance program | |
| Time period | 1996–2001 | |
| Site of care | Unit not specified, 77% transferred to the neonatal unit for medical reasons or pharmacological treatment (Switzerland) | |
| Interventions | Infants who received more than half of total amount of milk during hospital stay as human milk (27 infants) vs infants who received less than half (59 infants) | |
| Outcomes | Quote: "Twenty‐six percent of breast‐fed babies (7/27) and 78% of formula‐fed babies (42/54) developed NAS (P < 0.01)." Pharmacological treatment rate and custody not reported by feeding status |
|
| Notes | — | |
| Dryden 2009 | Methods | Retrospective cohort |
| Participants | 450 singleton pregnancies of drug misusing women prescribed substitute methadone for pregnancy 354 term substitute methadone‐exposed infants included in subgroup published in 2012 |
|
| Time period | January 2004 to December 2006 | |
| Site of care | Postnatal ward with mother unless any specific indication for admission to the neonatal unit (UK) | |
| Interventions | Received maternal breast milk ≥ 72 hours (99 infants) vs formula fed or received maternal breast milk < 72 hours (351 infants) | |
| Outcomes | Received maternal breast milk ≥ 72 hours vs formula fed or received maternal breast milk < 72 hours
|
|
| Notes | Emailed authors to clarify the relationship between the 2 publications, 2009 study is the primary study as fewer infants were included in 2012 study due to missing data. | |
| Hodgson 2012 | Methods | Retrospective cohort |
| Participants | 295 singleton mother‐infant dyads who received care in combined care for maternal substance use in a rooming in program | |
| Time period | October 2003 to December 2006 | |
| Site of care | Postnatal; quote: "combined care nursery" with mother including those receiving pharmacotherapy (British Columbia, Canada) | |
| Interventions | Breastfed (196 infants) vs not breastfed (99 infants) | |
| Outcomes |
|
|
| Notes | — | |
| Isemann 2011 | Methods | Retrospective cohort |
| Participants | 128 infants that received pharmacotherapy for opiate withdrawal in the newborn intensive care unit (92 infants > 37 weeks, 36 infants < 37 weeks) | |
| Time period | January 2002 to December 2007 | |
| Site of care | NICU (Ohio, USA) | |
| Interventions | Mother's breast milk ingested vs formula fed | |
| Outcomes |
|
|
| Notes | — | |
| Jansson 2008 | Methods | Prospective case control |
| Participants | 8 breastfed methadone‐exposed infants and 8 matched formula‐feeding infants | |
| Time period | January 2001 to September 2005 | |
| Site of care | Unit not specified (Maryland, USA) | |
| Interventions | Breastfed (8 infants) vs formula fed (8 infants) | |
| Outcomes | Breastfed vs formula fed
|
|
| Notes | More medical comorbidities in breastfed group 3 breastfeeding infants not included due to failure to provide complete study specimens 1 breastfeeding infants not included due to inability to find match |
|
| Liu 2015 | Methods | Retrospective cohort |
| Participants | 194 methadone‐maintained mother‐infant dyads > 30 weeks' gestation | |
| Time period | 2000–2006 | |
| Site of care | Unit not specified; quote: "two birthing units" (New South Wales, Australia) | |
| Interventions | Categorized in the 1st 2 days of life as predominantly breastfed (≥ 50% of feeds, 32 infants), fed expressed breast milk (≥ 15 mL expressed breast milk and breastfed < 3 times daily, 12 infants), or formula fed (≥ 50% of feeds and < 15 ml/day breast milk ingestion, 150 infants) | |
| Outcomes | Breastfed vs fed expressed breast milk vs formula fed
|
|
| Notes | — | |
| McQueen 2011 | Methods | Retrospective cohort |
| Participants | 28 term infants exposed to methadone with symptoms of NAS | |
| Time period | March 2007 to March 2008 | |
| Site of care | Unit not specified (Ontario, Canada) | |
| Interventions | Breastfeeding (> 75% breast milk, 8 infants) vs combination feeds (25% to 75% breast milk, 11 infants) vs formula fed (< 25% breast milk, 9 infants) | |
| Outcomes | Breastfed vs combination feed vs formula fed
|
|
| Notes | More regular prenatal care in the breastfed group Emailed with authors to clarify data |
|
| Metz 2015 | Methods | Retrospective cohort |
| Participants | 390 infants born to opioid‐dependent women undergoing comprehensive treatment during pregnancy (184 methadone, 77 buprenorphine, 129 slow‐release oral morphine) 50 infants excluded due to incomplete data |
|
| Time period | 1994 to January 2009 | |
| Site of care | Unit not specified (Austria) | |
| Interventions | Breastfed infants (100 infants; methadone group 48 infants, slow‐release oral morphine group 21 infants, buprenorphine group 31 infants) vs non‐breastfed infants (250 infants; methadone group 118 infants, slow‐release oral morphine group 91 infants, buprenorphine group 41 infants) | |
| Outcomes | Breastfed vs non‐breastfed
|
|
| Notes | Outcomes reported as subgroups only | |
| O'Connor 2013 | Methods | Retrospective cohort |
| Participants | 85 mother‐infant dyads in buprenorphine treatment program, infants > 35 weeks | |
| Time period | December 2007 to August 2012 | |
| Site of care | Unit not specified (Maine, USA) | |
| Interventions | Breastfeeding (65 infants) vs non‐breastfed infants (20 infants) | |
| Outcomes | Breastfed vs non‐breastfed
|
|
| Notes | Breastfed infants were significantly less likely to have exposure to illicit substances in the 3rd trimester (41.4% vs 80.0%; P = 0.004) | |
| Pritham 2012 | Methods | Retrospective cohort |
| Participants | 152 opioid‐dependent pregnant women in treatment (136 methadone, 16 buprenorphine) and their infants | |
| Time period | January 2005 to December 2007 | |
| Site of Care | NICU (Maine, USA) | |
| Interventions | Breastfed (17 infants, methadone group 14, buprenorphine group 3) vs both formula and breast (26 infants, methadone group 22, buprenorphine group 4) vs formula fed (105 infants, methadone group 96, buprenorphine group 9) | |
| Outcomes |
|
|
| Notes | — | |
| Radmacher 2017 | Methods | Prospective cohort (historically controlled feasibility study) |
| Participants | 12 term formula‐fed infants receiving oral morphine for opioid withdrawal matched to historical controls | |
| Time period | 2014–2017 | |
| Site of care | NICU (Kentucky, USA) | |
| Interventions | Exclusive donor milk for up to 2 weeks (12 infants) vs formula‐fed historical controls (12 infants) | |
| Outcomes | Donor milk vs formula fed
|
|
| Notes | Benzodiazepine exposure in the donor milk group but not the control group Significant deviation from intended intervention noted |
|
| Short 2016 | Methods | Retrospective cohort |
| Participants | 3725 singleton in‐hospital births > 35 weeks' gestation diagnosed with NAS based on discharge diagnosis codes | |
| Time period | 2012–2014 | |
| Site of care | Unit not specified, though mentions benefits of rooming in and 40% admission to NICU (Pennsylvania, USA) | |
| Interventions | Breastfeeding at discharge (1576 infants) vs not breastfeeding (1968 infants) as reported on birth certificate | |
| Outcomes |
|
|
| Notes | No information about in‐utero exposure or postnatal treatment for NAS Breastfed infants were more likely to have a higher birthweight and gestational age; less likely to be insured by Medicaid; and more likely to be born to mothers who completed high school, were married, had adequate prenatal care, and who did not smoke |
|
| Wachman 2013 | Methods | Prospective cohort |
| Participants | 86 infants > 36 weeks' gestation exposed to methadone or buprenorphine in utero | |
| Time period | July 2011 to July 2012 | |
| Site of care | Unit not specified, 5 tertiary care centers and community hospitals (Massachusetts and Maine, USA) | |
| Interventions | Assessed breastfeeding as a potential covariate related to NAS severity; breastfeeding (38 infants) vs no breastfeeding (48 infants) | |
| Outcomes | Breastfed vs non‐breastfed
|
|
| Notes | Objective: to determine whether single nucleotide polymorphisms in the μ‐opioid receptor (OPRM1), multiple‐drug resistance (ABCB1), and catechol‐O‐methyltransferase (COMT) genes are associated with length of hospital stay and the need for treatment of NAS | |
| Welle‐Strand 2013 | Methods | Retrospective and prospective cohort |
| Participants | 124 infants of women on opioid maintenance therapy (78 methadone, 46 muprenorphine) | |
| Time period | 1999–2003 (36 infants, retrospective), 2005–2007 (36 infants, prospective), 2007–2009 (52 infants, retrospective) | |
| Site of care | Unit not specified, national cohort (Norway) | |
| Interventions | Breastfed (95 infants; methadone exposed 58, buprenorphine exposed 37) vs not breastfed (29 infants; methadone exposed 20, buprenorphine exposed 9) | |
| Outcomes | Breastfed vs not breastfed
|
|
| Notes | More preterm birth and delivery by cesarean in non‐breastfed group | |
CI: confidence interval; NAS: neonatal abstinence syndrome; IQR: interquartile range; NICU: neonatal intensive care unit; OR: odds ratio; SD: standard deviation.
3. Excluded studies of support of the mother‐infant dyad.
| Study | Details | |
| Abrahams 2007 | Methods | Retrospective cohort |
| Participants | 106 infants of mothers with known heroin or methadone use during pregnancy | |
| Time period | October 2001 to December 2002 | |
| Site of care | Postnatal ward and intensive care nursery (BC, Canada) | |
| Interventions | Rooming in infants in study hospital (32 infants) compared to historical comparisons in study hospital (38 infants) and comparisons at a neighboring hospital without rooming in (36 infants) | |
| Outcomes | Rooming in vs historical comparisons in study hospital vs neighboring hospital without rooming in
|
|
| Notes | Several baseline differences between groups and hospitals with significant difference in feeding practices between groups (62.5% of the rooming in group breastfeeding compared to 7.9% of the historical cohort and 11.1% of the concurrent cohort) | |
| Abrahams 2010 | Methods | Retrospective cohort |
| Participants | 952 singleton infants of mothers with documented substance use | |
| Time period | October 2003 to December 2006 | |
| Site of care | Postnatal; quote: "combined care nursery" and intensive care nursery (British Columbia, Canada) | |
| Interventions | Rooming in with comprehensive education in study hospital (355 infants, term 255 infants) vs standard nursery care at all other hospitals (597 infants, term 434 infants) | |
| Outcomes | Rooming in vs standard nursery care
|
|
| Notes | Baseline differences between groups and hospitals. Newborns in rooming in group had increased odds of receiving breast milk during hospital stay. | |
| Crook 2017 | Methods | Retrospective and prospective cohort (quality improvement methodology) |
| Participants | 200 infants evaluated for NAS | |
| Time period | February 2014 to July 2015 | |
| Site of care | NICU, small percentage on pediatric unit if high NICU census (North Carolina, USA) | |
| Interventions | Baby friendly status Breastfeeding initiative (3 class curriculum) |
|
| Outcomes |
|
|
| Notes | Quote: "Infants who received more than 50% human milk had a predicted [length of stay] 2.78 days shorter than infants who received more than 50% formula during hospitalization (P = .08)." | |
| Howard 2017 | Methods | Retrospective cohort |
| Participants | 86 mother‐infant dyads in a single center rooming in cohort of infants treated pharmacologically for NAS | |
| Time period | March 2015 to April 2016 | |
| Site of care | Pediatric inpatient unit for pharmacological treatment (Massachusetts, USA) | |
| Interventions | Parental presence (percent of time) | |
| Outcomes |
|
|
| Notes | Quote: "In unadjusted analyses, any amount of breastfeeding was associated with a decreased [length of stay] (16.5 vs 21.2 days; P < .01) as was clinical trial participation (15.8 vs 20.0 days; P < .01). Similarly, breastfeeding and clinical trial participation were also significantly associated with decreased duration of opioid therapy and decreased total morphine equivalent dose." | |
| Hünseler 2013 | Methods | Retrospective cohort |
| Participants | 77 infants with NAS transferred from the maternity ward to the neonatal ward for potential pharmacological treatment | |
| Time period | 2004–2011 | |
| Site of care | Neonatal ward (Germany) | |
| Interventions | Rooming in within the neonatal ward (24 infants) vs not rooming in within the neonatal ward (53 infants) | |
| Outcomes | Rooming in vs no rooming in
|
|
| Notes | Only 2 infants were breastfed | |
| McKnight 2016 | Methods | Retrospective cohort (historical controls) |
| Participants | 44 singleton infants > 36 weeks' gestation of women taking chronic opioid therapy | |
| Time period | May 2012 to September 2014 (excluding June to August 2013) | |
| Site of care | Pediatrics unit with transfer to NICU for pharmacological treatment (Ontario, Canada) | |
| Interventions | Baseline (24 infants) and postimplementation (20 infants) of initial observation while rooming in with mother in a private room in the pediatrics unit. Infants transferred to the NICU if pharmacological treatment was required | |
| Outcomes |
|
|
| Notes | Quote: "While not significant, a higher proportion of infants in the rooming‐in group were breastfed exclusively or in combination with formula." Emailed authors to clarify data and the relationship between the 2 publications, 1 additional participant included in earlier publication (Newman 2015) who was different from the usual population |
|
| Metz 2011 | Methods | Retrospective cohort |
| Participants | 114 opioid‐exposed newborns of mothers maintained on methadone (70 infants) or buprenorphine (44 infants) | |
| Time period | June 2005 to December 2009 | |
| Site of care | Unit not specified (Austria) | |
| Interventions | Participation in a randomized double‐blind double‐dummy clinical trial ("MOTHER study", 37 infants) vs standard care (77 infants) Clinical trial included daily maternal contact with study staff and mandatory rooming in with mother for ≥ 10 days after delivery Standard care neonates were treated in a separate ward and mothers were discharged when medically cleared |
|
| Outcomes | Clinical trial vs standard protocol
|
|
| Notes | Modified Finnegan used for clinical trial vs traditional Finnegan for standard care Likely fundamentally different group self‐selected for clinical trial |
|
| Ordean 2015 | Methods | Retrospective cohort |
| Participants | 94 pregnant methadone‐maintained women attending integrated care programs and their children | |
| Time period | 1997–2009 | |
| Site of care | Unit not specified for rooming in cohort, NICU (Ontario, British Columbia, and Quebec, Canada) | |
| Interventions | Rooming in approach (36 infants) vs 2 neighboring hospitals that admit infants to the neonatal intensive care unit for NAS scoring (36 and 22 infants) | |
| Outcomes | Rooming in vs hospital 1 (no rooming in) vs hospital 2 (no rooming in)
|
|
| Notes | Minimal difference in breastfeeding between groups. Significant intersite differences were found in ethnicity and marital status. Emailed authors to clarify data. |
|
| Saiki 2010 | Methods | Retrospective cohort (historical controls) |
| Participants | 60 infants with NAS | |
| Time Period | 2002–2007 | |
| Site of Care | Postnatal ward for monitoring and pharmacological treatment and neonatal unit (UK) | |
| Interventions | Baseline (42 infants) and postimplementation (18 infants) of a system of pharmacological treatment of the infant in the postnatal ward instead of transferring from the postnatal ward to the neonatal unit if escalating symptoms | |
| Outcomes | Baseline vs postimplementation
|
|
| Notes | — | |
| Summey 2018 | Methods | Retrospective cohort |
| Participants | 466 infants receiving care for NAS | |
| Time period | 2006–2014 | |
| Site of care | Postnatal ward for monitoring and pharmacological treatment and Neonatal unit (South Carolina, USA) | |
| Interventions | Infants enrolled in the Managing Abstinence in Newborns (MAiN) intervention (110 infants) vs infants who were potentially eligible but did not receive the intervention (356 infants) MAiN; quote: "provides multidisciplinary, coordinated, community‐based care for infants at risk for opioid withdrawal and their families within a mother/baby unit. MAiN's three essential elements are early treatment (methadone administered within 48 hours of birth), the option to room in with the mother for the entire hospitalization, and a combined inpatient/outpatient wean." |
|
| Outcomes | MAiN vs no MAiN
|
|
| Notes | No significant difference in breastfeeding between groups (43.6% vs 48.9%; P = 0.57) | |
CI: confidence interval; DCF: Department of Children and Families; IQR: interquartile range; MAiN: Managing Abstinence in Newborns; MOTHER: Maternal Opioid Treatment: Human Experimental Research; NAS: neonatal abstinence syndrome; NICU: neonatal intensive care unit; OR: odds ratio; r: Pearson's correlation coefficient; RR: risk ratio; SD: standard deviation.
4. Excluded studies of multiple non‐pharmacological care practices.
| Study | Details | |
| Grossman 2017 | Methods | Retrospective and prospective cohort (quality improvement methodology) |
| Participants | 287 infants diagnosed with NAS. Excluded infants not exposed to methadone and with serious comorbid conditions | |
| Time period | January 2008 to June 2016 | |
| Site of care | Pediatrics unit, postnatal ward, and NICU (Connecticut, USA) | |
| Interventions | Quote: "Standardization of nonpharmacologic care coupled with an empowering message to parents, development of a novel approach to assessment, administration of morphine on an as‐needed basis, and transfer of infants directly to the inpatient unit." Baseline period from January 2008 to February 2010 (55 infants), intervention period (188 infants), and postimplementation period from May 2015 to June 2016 (44 infants) |
|
| Outcomes |
|
|
| Notes | — | |
| Holmes 2016 | Methods | Retrospective and prospective cohort (quality improvement methodology) |
| Participants | 163 opioid‐exposed newborns Excluded infants with gestational age < 35 weeks, another reason for NICU admission, or who completed treatment at another facility |
|
| Time period | March 2012 to February 2015 | |
| Site of care | Pediatrics unit, postnatal ward, and NICU (New Hampshire, USA) | |
| Interventions | Staff training, family education (involvement in symptom monitoring and non‐pharmacological treatment), and care in inpatient pediatric unit Baseline period from March 2012 to February 2013 (54 infants), intervention year 1 from March 2013 to February 2014 (61 infants), and intervention year 2 from March 2014 to February 2015 (48 infants) |
|
| Outcomes |
|
|
| Notes | — | |
| Kirchner 2014 | Methods | Retrospective cohort |
| Participants | 131 infants who completed an international multicenter clinical trial ("MOTHER study") | |
| Time period | 2005–2008 | |
| Site of care | Unit not specified (international) | |
| Interventions | Comparison by site of enrollment; quote: "the 7 contributing sites were divided into 3 clusters: the European cluster (Vienna site, n=37), the rural US cluster (N=39): Burlington (University of Vermont, n=26), Nashville (Vanderbilt University, n=13), and the urban US cluster (n=55): Detroit (Wayne State University, n=12), Providence (Brown University, n=3), Philadelphia (Thomas Jefferson University, n=23), Baltimore (Johns Hopkins University, n=17)" Quote: "A standardized NAS rating and treatment protocol was applied, while non‐pharmacologic care of NAS symptoms differed across sites" Quote: "In Europe, all neonates (also those without treatment requirement) stayed in the hospital accommodated in a room with their mothers for at least 10 days" Quote: "The breastfeeding rate was much higher in Europe and was highest in rural US" |
|
| Outcomes |
|
|
| Notes | Quote: "No differences between sites could be found in behavioural symptoms, but interestingly a significant positive influence on these symptoms could be demonstrated by breastfeeding (β = –0.261; P = 0.034), with explaining 6.8% of variance" | |
| Loudin 2017 | Methods | Retrospective cohort (historical controls) |
| Participants | 1023; quote: "inborn neonates >35 weeks' gestational age with the diagnosis of NAS (ICD9‐CM 779.5), requiring pharmacologic treatment" | |
| Time period | 2010–2015 | |
| Site of care | Neonatal abstinence center, NTU, and NICU (West Virginia, USA) | |
| Interventions | Baseline (number of infants not reported); quote: "managed in the NICU, a 36 bed level III unit with an average of 550 admissions per year" and post‐implementation (number of infants not reported) of a neonatal therapeutic unit (NTU), (quote) "a 15‐bed low‐light, low‐noise unit with a dedicated nursing staff and nursing aids along with community volunteers called 'rockers' who were specially trained to hold and rock the neonates when appropriate and when family members were unavailable. The staff utilized therapeutic handling techniques that further enhanced calming effects on the neonates." Also compared to post‐implementation (78 infants) of an offsite; quote: "neonatal abstinence center with 12 beds and a dedicated staff of nurses, patient care assistants, and volunteers trained in the care of neonates with NAS. In addition, on‐site social service personnel served to transition caretakers (birth parents, foster parents or adopting families) … to a safe home environment. Limited number of patient rooms were available to accommodate rooming in, thus that space was utilized to help prepare caretakers prior to discharge." | |
| Outcomes |
|
|
| Notes | — | |
| Miles 2007 | Methods | Retrospective cohort (historical controls) |
| Participants | 176 infants of women in a methadone maintenance program | |
| Time period | 1991–1994, 1997–2001 | |
| Site of care | Postnatal ward and neonatal medicine unit (UK) | |
| Interventions | Baseline (78 infants) and postimplementation (98 infants) of a shared care approach in clinical management with a drug liaison midwife service for mothers and infants. Also changed from primary admission to the neonatal medicine unit to primary admission to the maternity ward with transfer to the neonatal medicine unit if pharmacological treatment was required. Additionally, scoring was modified, the threshold for pharmacological treatment adjusted, and treatment choice changed from chlorpromazine to phenobarbitone. Quote: "The [drug liaison midwife] provided specialist advice regarding methadone treatment, care of the newborn, and the advantages of breastfeeding." | |
| Outcomes |
|
|
| Notes | — | |
| Patrick 2016 | Methods | Retrospective and prospective cohort (quality improvement methodology) |
| Participants | 3458 infants pharmacologically treated for NAS. Data were collected through serial cross‐sectional audits of 199 participating centers | |
| Time period | 2012–2014 | |
| Site of care | Unit not specified (International) | |
| Interventions | Quote: "Participating NICUs shared common interests, worked collaboratively, shared information and ideas, and developed standardized practices." The goal was to facilitate guideline update "for the following: (1) screening for maternal substance use; (2) nonpharmacologic treatment of infants with NAS; (3) scoring signs of NAS; (4) breastfeeding; (5) pharmacologic management; and (6) duration of observation of exposed infants." | |
| Outcomes |
|
|
| Notes | — | |
| Wachman 2018 | Methods | Retrospective and prospective cohort (pre‐/postquality improvement methodology) |
| Participants | 240 opioid‐exposed infants > 36 weeks' gestation | |
| Time period | April 2015 to December 2017 | |
| Site of care | Pediatrics unit and postnatal ward (Massachusetts, USA) | |
| Interventions | Baseline (101 infants), intervention (54 infants), and postintervention (85 infants). Interventions included (quote): "a non‐pharmacologic care bundle, function‐based assessments consisting of symptom prioritization and then the "Eat, Sleep, Console" (ESC) Tool; and a switch to methadone for pharmacologic treatment." | |
| Outcomes |
|
|
| Notes | Quote: "Breastfeeding initiation rate did not differ during the two time periods." | |
CI: confidence interval; DCF: Department of Children and Families; ESC: Eat, Sleep, Console Tool; IQR: interquartile range; MOTHER: Maternal Opioid Treatment: Human Experimental Research; NAS: neonatal abstinence syndrome; NICU: neonatal intensive care unit; NTU: neonatal therapeutic unit.
Ongoing studies
We identified seven ongoing studies in the search that may qualify for inclusion at review update when complete (Characteristics of ongoing studies table; NCT02768844; NCT02801331; NCT03097484; NCT03113656; NCT03533985; NCT03549936; NCT03987165).
See Figure 1 for the selection process.
Results of the search
Comparison 1
We identified six RCTs comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions in infants at risk for, or having early symptoms consistent with, opioid withdrawal as defined above (see Characteristics of included studies table).
Comparison 2
We identified no RCTs comparing single or bundled non‐pharmacological interventions to no non‐pharmacological treatment or different single or bundled non‐pharmacological interventions in infants receiving opioid treatment for symptoms consistent with opioid withdrawal as defined above.
Included studies
Modifying environmental stimulation
Ostrea 1975 compared 198 infants randomized to either a study nursery or the regular nursery at a children's hospital in the USA. This study included infants at risk for opioid withdrawal due to maternal opioid exposure (131 clinic infants, 57 non‐clinic infants). Non‐opioid exposure and feeding type were not specified. Infants in the study nursery were placed in incubators; fed every three hours; and maintained in a secluded, quiet, dim room. In comparison, infants in the regular nursery were placed in open bassinets, fed every four hours, and exposed to normal nursery noise and light. As measured by a center‐specific withdrawal rating, there were no significant differences in severity or pattern of withdrawal symptoms or in degree of weight loss. Eleven infants received pharmacological treatment and there was no difference between groups.
Oro 1988 compared 49 infants randomized to either non‐oscillating waterbeds or conventional bassinets in a nursery at a hospital in the USA. This study included infants at risk for opioid withdrawal due to prenatal narcotic exposure and heroin or methadone, or both, on urine toxicology results. Twelve narcotic‐exposed and three with coexposure to cocaine or methamphetamine, or both, were chosen from the intervention group and matched to comparable control neonates. Outcomes were not reported for 19 randomized infants. All infants were formula fed. Infants in the intervention group showed less severe central nervous system withdrawal symptoms, improved weight gain, required a lower maximum dose of phenobarbital, and more infants were weaned off from medication prior to discharge. There was no significant difference in overall use of pharmacological treatment.
D'Apolito 1999 compared 14 infants randomized to either a rocking bed or a standard bed from 24 hours of life to seven days of life in a nursery at a university hospital in the USA. This study included infants at risk for opioid withdrawal due to prenatal methadone exposure. Non‐opioid exposures included ethanol, heroin, marijuana, and cigarettes, but excluded cocaine. Feeding type was not reported. The rocking bed intervention consisted of a motor‐driven rocking bed set at 75% rocking that started and stopped at randomly determined intervals and was used in combination with maternal intrauterine sounds. Infants in the intervention group showed increased withdrawal symptoms by the seventh day of life and increased sleep disruption. All infants received pharmacotherapy for withdrawal symptoms.
Maichuk 1999 compared 48 infants randomized to either prone sleep positioning or supine sleep positioning in an intensive care nursery at a university hospital in the USA. This study included infants at risk for opioid withdrawal with urine toxicology positive for heroin or methadone, or both. Approximately 60% of infants in each group also had urine toxicology positive for cocaine. All infants were formula fed. All infants were swaddled for sleep. Infants in the intervention group were then placed prone. Infants in the intervention group had lower peak and mean withdrawal scores as well as lower caloric intake. All infants received pharmacotherapy for withdrawal symptoms.
Feeding practices
Bogen 2018 compared 49 infants randomized to either 24 kcal/oz formula or 20 kcal/oz formula from day three to 21 of life at a large, urban hospital in the USA. Site of care was not specified. This study included infants at risk for opioid withdrawal due to maternal methadone treatment. Maternal and infant drug screens at delivery were positive for illicit drugs more often in the control group. Both breastfed and formula‐fed infants were included in the study and breast milk feedings were prioritized over study formula feedings. The main outcome was evaluation of weight parameters. Infants in the high‐calorie intervention group trended toward improved weight parameters as measured by weight nadir, days to return to birth weight, and mean daily weight gain. A similar proportion of infants in each group received pharmacological treatment and there was no significant difference in treatment duration for those who used pharmacological treatment. There was significant crossover between groups.
Support of the mother‐infant dyad
MacVicar 2018 compared 14 mother‐infant dyads randomized to either tailored breastfeeding support or standard Baby‐Friendly Initiative care in a tertiary maternity hospital in Scotland. Infants were admitted to a room with their mothers and transferred to the neonatal unit for pharmacological treatment. This study included infants at risk for opioid withdrawal due to maternal opioid substitution therapy during pregnancy. Mothers with ongoing illicit psychoactive drug or alcohol use were excluded. All mothers intended to breastfeed. Tailored support included a one‐hour session daily for five days with a dedicated support worker. Sessions focused on breastfeeding support, promotion of self‐efficacy, neonatal self‐consolation techniques, and low‐stimuli environment. Infants in the intervention group were less likely to receive pharmacological treatment, and had a shorter length of stay compared to the control group. This effect may have been related to feeding practice since all infants in the intervention group were breastfed on day five compared to four of seven in the control group or to the ability to continue to room in with their mothers. In post hoc analysis of feeding practice, breastfed infants were less likely to be treated with pharmacological therapy and had a shorter length of stay.
Excluded studies
We excluded 34 non‐randomized studies in the search. These studies are described in a narrative presentation here. Further details about studies are included in and supplementary tables and the appendix (see Characteristics of excluded studies table; Table 2; Table 3; Table 4; Table 5; and Appendix 3).
We described cohort studies, case‐controlled studies, and cross‐sectional studies with a clear comparison of non‐pharmacological care practices. We did not describe studies without a clear comparison of non‐pharmacological care practices such as case series or case reports. We classified studies as prospective, retrospective, or both prospective and retrospective. We described studies using quality improvement methodology as prospective and retrospective cohorts. We classified studies as either historically or concurrently controlled.
Modifying environmental stimulation
(Adjustments of environmental stimulation include low light, low noise, clustered care, containment or swaddling, bedding type, positioning, non‐nutritive sucking, bathing, aromatherapy, music therapy, and massage.)
Two prospective feasibility studies explored the effect of modifying environmental stimulation on individual opioid‐exposed newborns. Radziewicz 2018 evaluated the effect of a 30‐minute Reiki treatment in a newborn nursery. Zuzarte 2017 evaluated the effect of stochastic vibrotactile stimulation delivered by a specially constructed mattress in 30‐minute intervals in the NICU and a newborn nursery. Both studies were conducted in the USA. Neither study recorded outcomes prespecified for this review.
Feeding practices
(Feeding modifications include infant‐led feeding, high caloric feedings, tube feedings, maternal breast milk feedings, non‐maternal breast milk feedings, low‐lactose formula, and breastfeeding.)
Fifteen studies assessed the effect of feeding practices on outcomes in opioid‐exposed newborns. Thirteen studies were cohort studies including 11 retrospective (Abdel‐Latif 2006; Arlettaz 2005; Dryden 2009; Hodgson 2012; Isemann 2011; Liu 2015; McQueen 2011; Metz 2015; O'Connor 2013; Pritham 2012; Short 2016), one retrospective and prospective (Welle‐Strand 2013), and one prospective study (Wachman 2013). Two additional studies used case‐control methodology, one with concurrent controls (Jansson 2008), and one with historical controls (Radmacher 2017). Twelve studies assessed infants at risk for, or having, early symptoms consistent with opioid withdrawal (Abdel‐Latif 2006; Arlettaz 2005; Dryden 2009; Hodgson 2012; Jansson 2008; Liu 2015; McQueen 2011; Metz 2015; O'Connor 2013; Pritham 2012; Wachman 2013; Welle‐Strand 2013); two studies assessed infants receiving opioid treatment for symptoms consistent with opioid withdrawal (Isemann 2011; Radmacher 2017); and one study did not collect information about postnatal treatment (Short 2016). Seven studies were conducted in the USA (Isemann 2011; Jansson 2008; O'Connor 2013; Pritham 2012; Radmacher 2017; Short 2016; Wachman 2013); two in Australia (Abdel‐Latif 2006; Liu 2015); two in Canada (Hodgson 2012; McQueen 2011); and one each in the UK (Dryden 2009), Switzerland (Arlettaz 2005), Austria (Metz 2015), and Norway (Welle‐Strand 2013). One study evaluated infants cared for in the postnatal ward for monitoring and pharmacological treatment (Hodgson 2012), two studies evaluated infants cared for in the postnatal ward with transfer to the NICU for pharmacological treatment (Abdel‐Latif 2006; Dryden 2009), three studies evaluated infants cared for in the NICU (Isemann 2011; Pritham 2012; Radmacher 2017), and nine studies did not report the site of care (Arlettaz 2005; Jansson 2008; Liu 2015; McQueen 2011; Metz 2015; O'Connor 2013; Short 2016; Wachman 2013; Welle‐Strand 2013). All studies assessed the impact of breast milk feedings compared to non‐breast milk feedings on outcomes. Intervention definitions varied between studies in terms of timing and 'dose' of breast milk. Only one study assessed the impact of non‐maternal donor breast milk feedings (Radmacher 2017). Measured primary outcomes included length of hospitalization (Abdel‐Latif 2006; Dryden 2009; Isemann 2011; Metz 2015; O'Connor 2013; Pritham 2012; Radmacher 2017; Short 2016; Wachman 2013), use of pharmacological treatment (Abdel‐Latif 2006; Dryden 2009; Hodgson 2012; Jansson 2008; Liu 2015; O'Connor 2013; Wachman 2013; Welle‐Strand 2013), length of pharmacological treatment (Abdel‐Latif 2006; Jansson 2008; Metz 2015; Radmacher 2017; Welle‐Strand 2013), maximum dose of opioid medication (Abdel‐Latif 2006; Liu 2015), and cumulative dose of opioid medication (Metz 2015). One study evaluated the secondary outcomes of growth rate and days to regain birth weight (Radmacher 2017), another evaluated weight nadir (Dryden 2009), and one evaluated custody at discharge (Abdel‐Latif 2006). Though no studies assessed the predefined secondary outcome of peak NAS score in the first 72 hours of life, eight studies assessed the severity of NAS using other measures (Abdel‐Latif 2006; Arlettaz 2005; Jansson 2008; Liu 2015; McQueen 2011; Metz 2015; O'Connor 2013; Radmacher 2017).
Support of the mother‐infant dyad
(Treatments focused on the mother‐infant dyad include parental presence, rooming in, skin‐to‐skin or 'kangaroo care,' parental respite or 'cuddler' programs, trauma‐informed care, social work support, mental health support, treatment program support, and legal support.)
Ten studies evaluated methods of support for the mother‐infant dyad on outcomes in opioid‐exposed newborns. Nine were retrospective cohort studies, seven with concurrent controls (Abrahams 2007; Abrahams 2010; Howard 2017; Hünseler 2013; Metz 2011; Ordean 2015; Summey 2018), and two with historical controls (McKnight 2016; Saiki 2010). One study was a retrospective and prospective cohort utilizing quality improvement methodology (Crook 2017). Nine studies assessed infants at risk for, or having, early symptoms consistent with opioid withdrawal (Abrahams 2007; Abrahams 2010; Crook 2017; Hünseler 2013; McKnight 2016; Metz 2011; Ordean 2015; Saiki 2010; Summey 2018), and one study assessed infants receiving opioid treatment for symptoms consistent with opioid withdrawal (Howard 2017). Four studies were conducted in Canada (Abrahams 2007; Abrahams 2010; McKnight 2016; Ordean 2015); three in the USA (Howard 2017; Ordean 2015; Summey 2018); and one each in the UK (Saiki 2010), Austria (Metz 2011), and Germany (Hünseler 2013). Four studies evaluated infants cared for in the postnatal ward compared to a NICU setting (Abrahams 2007; Abrahams 2010; Saiki 2010; Summey 2018), two studies evaluated infants cared for in a pediatrics ward (Howard 2017; McKnight 2016), two studies evaluated infants cared for in the NICU (Crook 2017; Hünseler 2013), and two studies did not report the site of care (Metz 2011; Ordean 2015). Eight studies assessed the impact of rooming in, five as the primary intervention (Abrahams 2007; Hünseler 2013; McKnight 2016; Ordean 2015; Saiki 2010), and three in combination with additional support and education (Abrahams 2010; Metz 2011; Summey 2018). One study examined a breastfeeding education program (Crook 2017), and another examined the impact of parental presence (Howard 2017). Measured primary outcomes included length of hospitalization (Abrahams 2007; Abrahams 2010; Crook 2017; Howard 2017; Hünseler 2013; McKnight 2016; Metz 2011; Ordean 2015; Saiki 2010; Summey 2018), use of pharmacological treatment (Abrahams 2007; Crook 2017, Hünseler 2013, McKnight 2016; Metz 2011; Ordean 2015; Saiki 2010), length of pharmacological treatment (Abrahams 2007; Howard 2017; Hünseler 2013; McKnight 2016; Metz 2011; Ordean 2015; Saiki 2010), maximum dose of opioid medication (Hünseler 2013; McKnight 2016), and cumulative dose of opioid medication (Howard 2017; Metz 2011). Secondary outcomes assessed included NICU admission (Abrahams 2007; Abrahams 2010; Ordean 2015; Summey 2018), length of NICU stay (Abrahams 2010), weight nadir (Abrahams 2007; Ordean 2015; Summey 2018), seizure (Summey 2018), custody at discharge (Abrahams 2007; Abrahams 2010; Howard 2017; Hünseler 2013; Ordean 2015; Saiki 2010; Summey 2018), and cost of care (Hünseler 2013; Summey 2018). Though no studies assessed the predefined secondary outcome of peak NAS score in first 72 hours of life, two studies assessed the severity of NAS using other measures (Howard 2017; Hünseler 2013).
Multiple non‐pharmacological care practices
(Any combination of the above non‐pharmacological interventions.)
Seven studies examined multiple non‐pharmacological care practices in combination with other non‐pharmacological and pharmacological treatments. Four studies were retrospective and prospective cohorts utilizing quality improvement methodology (Grossman 2017; Holmes 2016; Patrick 2016; Wachman 2018). Three studies were retrospective cohort studies, one with concurrent controls (Kirchner 2014), and two with historical controls (Loudin 2017; Miles 2007). Five studies assessed infants at risk for, or having, early symptoms consistent with opioid withdrawal (Grossman 2017; Holmes 2016; Kirchner 2014; Miles 2007; Wachman 2018), and two studies assessed infants receiving opioid treatment for symptoms consistent with opioid withdrawal (Loudin 2017; Patrick 2016). Four studies were conducted in the USA (Grossman 2017; Holmes 2016; Loudin 2017; Wachman 2018), two at multiple international sites (Kirchner 2014; Patrick 2016), and one in the UK (Miles 2007). Two studies evaluated infants cared for in the postnatal ward, pediatrics unit, and NICU settings (Grossman 2017; Holmes 2016); one study evaluated infants cared for in the postnatal ward and the pediatrics unit (Wachman 2018); one study evaluated infants cared for in the postnatal ward and the NICU (Miles 2007); and two studies did not report the site of care (Kirchner 2014; Patrick 2016). Three studies assessed a combination of standardized non‐pharmacological care, education, and rooming in among other interventions (Grossman 2017; Holmes 2016; Wachman 2018). Two studies compared different care environments (Kirchner 2014; Loudin 2017). One study examined the combination of rooming in, maternal support, and changes in pharmacological care practices in combination (Miles 2007). One study evaluated the impact of a multicenter effort to standardize care and guidelines affecting both non‐pharmacological and pharmacological care practices (Patrick 2016). Measured primary outcomes included length of hospitalization (Grossman 2017; Holmes 2016; Loudin 2017; Miles 2007; Patrick 2016; Wachman 2018), use of pharmacological treatment (Grossman 2017; Holmes 2016; Kirchner 2014; Miles 2007; Wachman 2018), length of pharmacological treatment (Kirchner 2014; Patrick 2016; Wachman 2018), and cumulative dose of opioid medication (Holmes 2016; Kirchner 2014). Secondary outcomes evaluated include NICU admission (Grossman 2017; Loudin 2017; Miles 2007; Wachman 2018), seizures (Miles 2007; Wachman 2018), custody at discharge (Holmes 2016; Miles 2007), and cost of care (Grossman 2017; Holmes 2016; Loudin 2017). Though no studies assessed the predefined secondary outcome of peak NAS score in first 72 hours of life, two studies assessed the severity of NAS using other measures (Holmes 2016; Kirchner 2014). No studies assessed neurodevelopmental outcome as prespecified in the protocol at two years; however, one study assessed neurodevelopmental outcome in the first year of life (Miles 2007).
Risk of bias in included studies
Six RCTs are included in a risk of bias assessment (Figure 2).
2.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
Modifying environmental stimulation (D'Apolito 1999; Maichuk 1999; Oro 1988; Ostrea 1975).
Feeding practices (Bogen 2018).
Support of the mother‐infant dyad (MacVicar 2018).
The six studies demonstrated a generally high risk of bias. Bogen 2018 exhibited low risk of bias in several categories; however, sensitivity analysis was not performed because it was the only study in the category.
Allocation
Modifying environmental stimulation: we judged Oro 1988 to have high risk of sequence generation bias due to randomization of infants based on hospital record numbers. Three studies did not describe the randomization process and we judged risk of bias due to sequence generation as unclear (D'Apolito 1999; Maichuk 1999; Ostrea 1975). None of the four studies report blinded allocation and we judged risk of selection bias as unclear.
Feeding practices: we judged Bogen 2018 to have low risk of sequence generation and selection bias due to randomization of infants with blinded computer‐based sequence generation.
Support of the mother‐infant dyad: we judged MacVicar 2018 to have low risk sequence generation bias due to randomization of infants with computer‐based sequence generation. Blinded allocation was not reported, and we judged risk of selection bias as unclear.
Blinding
Modifying environmental stimulation: four studies did not blind caregivers or evaluators to the intervention due to inability to conceal the interventions during routine care. We judged the risk of performance and detection bias as high (D'Apolito 1999; Maichuk 1999; Oro 1988; Ostrea 1975).
Feeding practices:Bogen 2018 blinded all caregivers and evaluators to the intervention. We judged the risk of performance and detection bias as low.
Support of the mother‐infant dyad:MacVicar 2018 did not blind caregivers or evaluators to the intervention due to inability to conceal the interventions during routine care. We judged the risk of performance and detection bias as high.
Incomplete outcome data
Modifying environmental stimulation: we judged Oro 1988 to have a high risk of attrition bias due to the exclusion of randomized infants who were unable to be matched to controls (approximately 39% of randomized infants). Three studies reported outcomes for all enrolled infants, and we judged the risk of attrition bias as low (D'Apolito 1999; Maichuk 1999; Ostrea 1975).
Feeding practices: we judged Bogen 2018 to have a high risk of attrition bias due to the proportion of infants lost to follow‐up before reaching birth weight or the end of the study intervention on day 21 (18%).
Support of the mother‐infant dyad: we judged MacVicar 2018 to have a high risk of attrition bias due to the proportion of infants stopping the intervention early (approximately 43%), and the loss to follow‐up posthospitalization (approximately 21%).
Selective reporting
Modifying environmental stimulation: all four studies were not preregistered (study predated the mandatory requirement for preregistration) and there was no clear evidence of selective reporting (D'Apolito 1999; Maichuk 1999; Oro 1988; Ostrea 1975). We judged the risk of reporting bias as unclear.
Feeding practices:Bogen 2018 was preregistered; however, several prespecified outcomes were not reported in the publication raising the possibility of selective reporting. We judged the risk of reporting bias as high.
Support of the mother‐infant dyad:MacVicar 2018 was not preregistered (expected for the publication year) and there was no clear evidence of selective reporting. We judged the risk of reporting bias as unclear.
Other potential sources of bias
Modifying environmental stimulation:D'Apolito 1999 and Oro 1988 noted differences in the number of infants with fetal distress. Maichuk 1999 and Ostrea 1975 did not report differences between treatment groups. None of the studies reported the number of eligible infants not enrolled and we could not assess the risk for differential enrollment affecting generalizability of study results. We judged the risk of other potential sources of bias in these studies as unclear.
Feeding practices:Bogen 2018 noted crossover and protocol deviation between groups that could have biased the results toward the null. Six infants assigned to standard‐calorie formula and one assigned to high‐calorie formula changed to open‐label high‐calorie formula due to slow weight gain. The change was made per protocol for two infants, and determined by non‐study physicians for four infants. Three infants assigned to high‐calorie formula switched to soy formula based on physician or family preference. Primary analysis was performed based on original intention‐to‐treat analysis. Post hoc analysis was performed based on feeding type. Bogen 2018 also noted baseline differences between the intervention and control groups. Six infants had positive screens at delivery for drugs other than methadone in the intervention group with no exposure in the control group. Bogen 2018 did not enroll 35% of infants whose mothers enrolled during pregnancy, largely due to need for prolonged NICU care not related to NAS and low birth weight. This may affect generalizability of study results. We judged the risk of other potential sources of bias as high.
Support of the mother‐infant dyad:MacVicar 2018 noted baseline differences between the intervention and control groups. There were more multiparous women and women with experience breastfeeding in the intervention group compared to the control group, and this difference could have a significant effect on a mother's initial comfort with newborn care. MacVicar 2018 did not enroll 74% of mothers approached, suggesting the study group may be a non‐representative population and likely a self‐selected population with intent to breastfeed. This may affect generalizability of study results. We judged the risk of other potential sources of bias as high.
Effects of interventions
See: Table 1
Comparison 1. Infants at risk for, or having early symptoms consistent with, opioid withdrawal
See Table 1.
Modifying environmental stimulation
Four studies reported modifying environmental stimulation (D'Apolito 1999; Maichuk 1999; Oro 1988; Ostrea 1975).
The studies compared a study nursery to a regular nursery (Ostrea 1975), non‐oscillating waterbeds to conventional bassinets (Oro 1988), rocking beds to standard beds (D'Apolito 1999), and prone sleep positioning to supine sleep positioning (Maichuk 1999).
Primary outcomes
Length of hospitalization (days) (outcome 1.1.1)
Oro 1988 reported a mean reduction in length of hospitalization by 1 day with a wide 95% CI ranging from a reduction of 2.82 days to an increase of 0.82 days (30 infants) (Analysis 1.1). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and serious concern for imprecision (due to wide 95% CI).
1.1. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 1: Length of hospitalization (days)
Pharmacological treatment with one or more doses of opioid or sedative medication (outcome 1.2.1)
Three studies of modifying environmental stimulation reported no difference in the use of pharmacological treatment with one or more doses of opioid or sedative medication (D'Apolito 1999; Maichuk 1999; Oro 1988). Meta‐analysis of the three studies found no evidence of a difference in the use of pharmacological treatment (typical RR 1.00, 95% CI 0.86 to 1.16; I2 = 0; 92 infants; Analysis 1.2). We judged the certainty of evidence as low and downgraded two levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias).
1.2. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 2: Pharmacological treatment with ≥ 1 doses of opioid or sedative medication
Secondary outcomes
Peak neonatal abstinence syndrome score in first 72 hours of life (outcome 1.3.1)
None of the studies of modifying environmental stimulation reported the peak NAS score in the first 72 hours of life as prespecified in the protocol. Post hoc we decided to evaluate 'peak' score at any time or any score reported in the first 72 hours as measured by a standardized withdrawal assessment tool (Analysis 1.3).
1.3. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 3: Peak neonatal abstinence syndrome (NAS) score in first 72 hours of life
Maichuk 1999 studied infant positioning during sleep and reported a mean reduction of peak neonatal abstinence score at any time of 2.65 (95% CI –3.81 to –1.49; 48 infants). D'Apolito 1999 and Oro 1988 studied bed type. D'Apolito 1999 reported the mean score in the first 72 hours of life (MD 1.60, 95% CI –1.11 to 4.31; 14 infants) and Oro 1988 reported peak neonatal abstinence score at any time (MD –0.20, 95% CI –0.82 to 0.42; 30 infants). Neither demonstrated a reduction of score. Meta‐analysis of the three studies of peak NAS score demonstrated extremely high heterogeneity and are not reported.
Neonatal intensive care unit admission (outcome 1.4.1)
None of the studies reported the effect of modifying environmental stimulation on NICU admission.
Days to regain birth weight (outcome 1.5.1)
None of the studies reported the effect of modifying environmental stimulation on days to regain birth weight.
Weight nadir (outcome 1.6.1)
Ostrea 1975 reported a mean reduction in weight nadir by 0.28% with a wide 95% CI ranging from a reduction of 1.15% to an increase of 0.59% (194 infants) (Analysis 1.6). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance and detection bias) and serious concern for imprecision (due to wide 95% CI).
1.6. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 6: Weight nadir (% weight loss)
Feeding practices
One study reported feeding practices (Bogen 2018).
The study compared 24 kcal/oz formula to 20 kcal/oz formula.
Primary outcomes
Length of hospitalization (days) (outcome 1.1.2)
The study did not report the effect of feeding practices on length of hospitalization.
Pharmacological treatment with one or more doses of opioid or sedative medication (outcome 1.2.2)
Bogen 2018 reported a reduced use of pharmacological treatment with an RR of 0.92 and a wide 95% CI ranging from 0.63 to 1.33 (49 infants) (Analysis 1.2). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to concern for attrition and reporting bias), serious concern about imprecision (due to wide 95% CI), and plausible confounding that would reduce demonstrated effect.
Secondary outcomes
Peak neonatal abstinence syndrome (NAS) score in first 72 hours of life (outcome 1.3.2)
The study did not report the effect of feeding practices on peak NAS.
Neonatal intensive care unit admission (outcome 1.4.2)
The study did not report the effect of feeding practices on NICU admission.
Days to regain birth weight (outcome 1.5.2)
Bogen 2018 reported a reduction in the mean number of days to regain birth weight by 1.1 days with a wide 95% CI ranging from a reduction of 2.76 days to an increase of 0.56 days (46 infants) (Analysis 1.5). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to concern for attrition and reporting bias), very serious concern about imprecision (due to very wide 95% CI), and plausible confounding that would reduce demonstrated effect.
1.5. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 5: Days to regain birth weight
Weight nadir (outcome 1.6.2)
Bogen 2018 reported a mean reduction in weight nadir by 0.80% with a wide 95% CI ranging from a reduction of 2.24% to an increase of 0.64% (46 infants) (Analysis 1.6). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to concern for attrition and reporting bias), serious concern about imprecision (due to wide 95% CI), and plausible confounding that would reduce demonstrated effect.
Support of the mother‐infant dyad
One study reported support of the mother‐infant dyad (MacVicar 2018).
The study compared tailored breastfeeding support to standard Baby‐Friendly Initiative care.
Primary outcomes
Length of hospitalization (days) (outcome 1.1.3)
MacVicar 2018 reported a mean reduction in length of hospitalization by 8.9 days with a wide 95% CI ranging from a reduction of 19.84 days to an increase of 2.04 days (14 infants) (Analysis 1.1). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and very serious concern for imprecision (due to very wide 95% CI).
Pharmacological treatment with one or more doses of opioid or sedative medication (outcome 1.2.3)
MacVicar 2018 reported a reduced use of pharmacological treatment with an RR of 0.50 and a wide 95% CI ranging from 0.13 to 1.90 (14 infants) (Analysis 1.2). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and very serious concern for imprecision (due to very wide 95% CI).
Secondary outcomes
Peak neonatal abstinence syndrome (NAS) score in first 72 hours of life (outcome 1.3.3)
The study did not report the effect of support of the mother‐infant dyad on peak NAS.
Neonatal intensive care unit admission (outcome 1.4.3)
MacVicar 2018 reported a reduced need for NICU admission with an RR of 0.50 and a wide 95% CI ranging from 0.13 to 1.90 (14 infants) (Analysis 1.4). We judged the certainty of evidence as very low and downgraded three levels for very serious concerns about risk of bias (due to unblinded study, concern for performance, detection, and attrition bias) and very serious concern for imprecision (due to very wide 95% CI).
1.4. Analysis.

Comparison 1: Infants at risk for, or having early symptoms consistent with, opioid withdrawal, Outcome 4: Neonatal intensive care unit admission
Days to regain birth weight (outcome 1.5.3)
The study did not report the effect of support of the mother‐infant dyad on days to regain birth weight.
Weight nadir (outcome 1.6.3)
The study did not report the effect of support of the mother‐infant dyad on weight nadir.
Other secondary outcomes for studies of infants at risk for, or having early symptoms consistent with, opioid withdrawal
None of the studies reported on length of NICU stay, neonatal seizure requiring anticonvulsant therapy, neonatal and infant all‐cause mortality, cerebral palsy, neurodevelopmental outcome at approximately two years' corrected age (cerebral palsy, developmental delay [Bayley or Griffith assessment more than two SD below mean] or intellectual impairment [IQ more than two SD below mean], blindness [vision less than 6/60 in both eyes], sensorineural deafness requiring amplification), complications of therapy, measures of maternal mood and bonding including Edinburgh Postpartum Depression Scale, Patient Health Questionnaire (2 or 9), Maternal Attachment Inventory, Maternal Postpartum Attachment Scale, Mother‐Infant Bonding Scale, or Postpartum Bonding Questionnaire (Brockington 2006; Condon 1998; Cox 1987; Kroenke 2001; Muller 1994; Taylor 2005; Whooley 1997), custody status at discharge, or cost of care.
Comparison 2. infants receiving opioid treatment for symptoms consistent with opioid withdrawal
We identified no studies.
Discussion
Summary of main results
We identified six RCTs evaluating 353 infants for inclusion in the analysis. The RCTs were published between 1975 and 2018 (six for comparison one, and none for comparison two). We identified and excluded 34 non‐randomized studies published between 2005 and 2018. We identified and excluded seven preregistered interventional clinical trials. These studies may qualify for inclusion at review update when complete. The certainty of evidence for the outcomes in the RCTs was very low to low. This was due to risk of bias inherent in the intervention, imprecision related to study size, and heterogeneity in study design.
Four studies evaluated modifying environmental stimulation by comparing a study nursery to a regular nursery (Ostrea 1975), non‐oscillating waterbeds to conventional bassinets (Oro 1988), rocking beds to standard beds (D'Apolito 1999), and prone sleep positioning to supine sleep positioning (Maichuk 1999). We are uncertain whether modifying environmental stimulation is associated with length of hospitalization based on one study with 30 infants (Oro 1988). Modifying environmental stimulation may be associated with little or no difference in use of pharmacological treatment based on three studies with 92 infants (D'Apolito 1999; Maichuk 1999; Ostrea 1975). We are uncertain whether modifying environmental stimulation is associated with peak NAS score at any time based on three studies with 92 infants (D'Apolito 1999; Maichuk 1999; Ostrea 1975). We are uncertain whether modifying environmental stimulation is associated with weight nadir based on one study with 194 infants (Ostrea 1975).
One study evaluated feeding practices by comparing 24 kcal/oz formula to 20 kcal/oz formula (Bogen 2018). We are uncertain whether feeding practices are associated with use of pharmacological treatment, days to regain birth weight, or weight nadir based on one study with 46 infants (Bogen 2018).
One study evaluated support of the mother‐infant dyad by comparing tailored breastfeeding support to standard Baby‐Friendly Initiative care (MacVicar 2018). We are uncertain whether support of the mother‐infant dyad is associated with length of hospitalization, use of pharmacological treatment, or NICU admission based on one study with 14 infants (MacVicar 2018).
Many prespecified outcomes were not reported. None of the studies reported length of NICU stay, neonatal seizures requiring anticonvulsant therapy, neonatal and infant all‐cause mortality, cerebral palsy, neurodevelopmental outcome at approximately two years' corrected age (cerebral palsy, developmental delay [Bayley or Griffith assessment more than two SD below mean] or intellectual impairment [IQ more than two SD below mean], blindness [vision less than 6/60 in both eyes], sensorineural deafness requiring amplification), complications of therapy, measures of maternal mood and bonding including Edinburgh Postpartum Depression Scale, Patient Health Questionnaire (2 or 9), Maternal Attachment Inventory, Maternal Postpartum Attachment Scale, Mother‐Infant Bonding Scale, or Postpartum Bonding Questionnaire (Brockington 2006; Condon 1998; Cox 1987; Kroenke 2001; Muller 1994; Taylor 2005; Whooley 1997), custody status at discharge, or cost of care. No studies evaluating modifying environmental stimulation looked at NICU admission or days to regain birth weight. No studies evaluating feeding practices looked at length of hospitalization, peak NAS score at any time, or NICU admission. No studies evaluating support of the mother‐infant dyad looked at peak NAS score at any time, days to regain birth weight, or weight nadir.
In summary, we identified few small studies of low quality and many prespecified outcomes were not reported. We are uncertain whether non‐pharmacological care for opioid withdrawal in newborns affects the prespecified outcomes. Given the low‐ or very low‐certainty evidence for all outcomes, the included studies do not support a specific non‐pharmacological intervention or combination of interventions over others.
Overall completeness and applicability of evidence
We identified six RCTs with heterogeneous study population, interventions, and outcome measures. The heterogeneity limits our ability to address the initial research question as well as generalizability of the results to other sites of care. Baseline outcome measures varied between studies suggesting that there are significant undefined differences between study sites. There is also lack of standardization in outcome measures and important measures are not measured in all studies (Kelly 2020).
The population studied is heterogeneous due to the presence of variable non‐opioid exposures. There is also high risk for differential enrollment not representative of the general population in this vulnerable population (Stine 2009). Study publications ranged from 1975 to 2018, and both substance exposures and treatments have changed over time. Many of the older studies were conducted when single drug exposure was common (e.g. heroin), and the model of care was more restrictive with fewer opportunities for parent contact, breastfeeding, or other aspects of non‐pharmacological care (Kocherlakota 2020). All but one of the RCTs was conducted in the USA, potentially limiting generalizability to other countries. Important demographic information such as, exact substance exposures, coexposures, and maternal medical and psychiatric history was not consistently collected.
We identified few studies in each category of non‐pharmacological intervention and heterogeneity of interventions within categories. In many of the included studies, there is lack of clarity in the 'dose', both in quality and quantity, of the intended intervention. The small number of studies and heterogeneity limited our ability to combine and compare studies directly. The identified studies lacked sufficient similarity for meta‐analysis for all outcomes except for the effect of modifying environmental stimulation on the use of pharmacotherapy. Though combined, these meta‐analyses include different interventions categorized as modifying environmental stimulation, including a waterbed, a rocking bed, and prone positioning.
The included studies showed differences in baseline outcome values between studies with no clear pattern. Due to lack of detail, we were unable to explore this source of heterogeneity between studies fully. The differences may be due to undefined cointerventions, which could include pharmacological treatment thresholds, non‐pharmacological interventions, and other multifactorial differences between study sites. Baseline and co‐occurring non‐pharmacological interventions were poorly defined in the studies. Clinically, cointerventions are common and some non‐pharmacological care practices are typically accompanied by other non‐pharmacological care practices. For example, breastfeeding is often accompanied by increases in clustered care, holding, skin‐to‐skin or 'kangaroo care', rocking, parental presence, and potentially additional support from staff (Bogen 2019). The practice of rooming in is often associated with increased rates of breastfeeding and may be associated with differences in environmental stimulation (Whalen 2019). These cointerventions, or bundles of non‐pharmacological interventions, are not always clearly defined or measured. Within the hospital, nursing ratios and site of care are likely significant unmeasured confounders that affect the ability to deliver non‐pharmacological interventions (Smith 2018). A specific site of care may be the most effective and efficient way to deliver certain non‐pharmacological interventions or combinations of non‐pharmacological interventions because site of care is highly interrelated with the ability to deliver non‐pharmacological care (Whalen 2019). For example, one intensive care unit may be unable to offer rooming in and have limited ability to decrease environmental stimulation. However, these limitations are not universal, and another intensive care unit may offer private rooms, intensive lactation and social support, and specific non‐pharmacological therapies. For this review, we chose to incorporate these differences between sites by assessing and comparing the specific interventions offered in each site studied. Limited data on cointerventions, site of care, and baseline confounding affect the generalizability of the study results.
While these studies assessed many predefined short‐term outcomes, they were not addressed consistently and important outcomes, such as NICU admission, were often missing. Heterogeneity of outcome measures in studies of neonates experiencing opioid withdrawal is common (Shan 2020). The largest and oldest study only contributed one prespecified secondary outcome of limited clinical importance. No studies addressed neonatal seizures requiring anticonvulsant therapy, all‐cause mortality, neurodevelopmental outcome, complications of therapy, measures of maternal mood and bonding, and custody at discharge.
Overall, based on six small RCTs, the completeness of evidence and applicability to the study question were limited by study heterogeneity, unmeasured baseline confounders and cointerventions, and unmeasured outcomes.
We also identified and excluded 34 non‐randomized studies published between 2005 and 2018 (29 for comparison 1, and five for comparison 2). The evidence is at baseline very low‐certainty based on the non‐randomized study design. The non‐randomized studies were identified using the standardized search strategies for randomized trials with additional studies identified when cross‐referencing for additional randomized studies. The search strategies and criteria for description of non‐randomized studies are less rigorous than those of RCTs. For this reason, we consider there is high likelihood that all eligible non‐randomized studies were not identified in the search process.
While the non‐randomized evidence is not methodologically strong, the 34 studies variably suggest improved outcomes with non‐pharmacological care practices when implemented singly or in combination. The majority of the non‐randomized studies showed either a decrease or no change in length of hospitalization, use of pharmacological treatment, and length of treatment when non‐pharmacological interventions were systematically implemented. The most widely studied non‐pharmacological care practices included breastfeeding, rooming in, and multiple non‐pharmacological practices implemented as part of a quality improvement initiative. Similar to the identified RCTs, the baseline outcome values and differences between groups varied significantly between sites for all interventions. This suggests that there are many unmeasured variables that impact care. The differences are likely partially related to unmeasured baseline differences in non‐pharmacological cointerventions and other multifactorial differences at each study site. There is also variability in quality and quantity of non‐pharmacological interventions. Heterogeneity in study design and size contribute to further variability.
Similar to the identified RCTs, the completeness of evidence and applicability to the study question based on non‐randomized studies are limited by study heterogeneity, unmeasured baseline confounders and cointerventions, and unmeasured outcomes.
Quality of the evidence
We judged the certainty of evidence for all outcomes in the six included RCTs as very low to low. Risk of bias was very serious for all studies secondary to the high risk of performance and detection bias related to lack of blinding (D'Apolito 1999; MacVicar 2018; Maichuk 1999; Oro 1988; Ostrea 1975), concern for attrition bias (Bogen 2018; MacVicar 2018; Oro 1988), concern for reporting bias (Bogen 2018), concern for other bias related to differential enrollment (Bogen 2018; MacVicar 2018), as well as many areas of unclear bias. Many outcomes were also downgraded for imprecision due to small study sizes with wide CIs. Though three studies reported the outcome of peak NAS score or NAS score in first 72 hours of life, meta‐analysis was not performed, and the outcome was downgraded due to serious inconsistency with marked heterogeneity and serious indirectness of the outcome measure. All outcomes for feeding measures were further downgraded for plausible confounding that would bias the results toward the null due to the significant number of participants who switched intervention groups in Bogen 2018.
Potential biases in the review process
Non‐pharmacological care for opioid withdrawal in newborns encompasses a group of interventions that are not well defined in the literature. The lack of standard terminology or definitions is a significant source of bias in the review process. For this review, we utilized a categorization of non‐pharmacological interventions based on common interventions reported in treatment of opioid withdrawal in newborns (Mangat 2019). There is no established standard research classification of non‐pharmacological care for opioid withdrawal in newborns and we established search terms based on our knowledge of the literature. Studies may categorize similar interventions in different ways such that the search terms did not identify all eligible studies. Additionally, some interventions such as breastfeeding or breast milk feedings are often examined as a subanalysis of a larger study that may not have been captured in the initial search. We included studies in categories of individual or combined non‐pharmacological interventions based on the study description and may have categorized studies incorrectly if the study description lacked detail. Within a category, we assumed the class and intensity of intervention was similar in the studies. When not described, we assumed a constant dose of each non‐pharmacological intervention.
The literature search using this categorization may not have captured all studies of the heterogeneous and historically not well‐defined group of non‐pharmacological interventions. Despite our best efforts, incomplete identification of studies for this review is possible. We reviewed 171 full‐text studies, many abstracts were advanced to full‐text review due to lack of clarity in study abstract about intervention and study design. We identified 28 of the full‐text studies outside of the search, largely in the references of other studies. The number of studies that were not captured by the search terms supports our suspicion for incomplete identification of studies. The majority of the full‐text studies reviewed were excluded due to study design, and it is likely that missed studies were a non‐randomized study design and would not qualify for inclusion. Importantly, the last search was performed in October 2019 and there may be more recent studies that qualify for inclusion.
Agreements and disagreements with other studies or reviews
While a number of reviews have assessed the impact of non‐pharmacological care practices together or as subgroups, we found no combined systematic review and meta‐analysis that evaluate non‐pharmacological care practices. Unlike many reviews of non‐pharmacological care practices, we chose to exclude studies of acupuncture and acupressure. A separate Cochrane Review is currently planned to address acupuncture and acupressure for opioid withdrawal in newborns, the protocol is not yet published. Similar to other recent reviews, we identified few RCTs and a larger literature of non‐randomized studies (MacMillan 2018; MacVicar 2019; Mangat 2019; McQueen 2019; Oostlander 2019; Ryan 2019). Unlike these reviews, we excluded non‐randomized studies. Our conclusion based on six RCTs was that we are uncertain whether non‐pharmacological care for opioid withdrawal in newborns affects the prespecified outcomes.
Other reviews that included non‐randomized studies discussed a trend toward improved outcomes when non‐pharmacological care practices were purposefully implemented. MacMillan 2018 noted reduced use of pharmacotherapy, length of stay, and cost of care in a systematic review and meta‐analysis of six non‐randomized studies evaluating rooming in. McQueen 2019 noted reduced incidence and duration of pharmacological treatment, shorter hospital length of stay, and decreased severity of NAS in methadone‐exposed infants in one randomized study (MacVicar 2018), and seven non‐randomized studies evaluating newborn feeding methods, the effect in buprenorphine‐exposed infants was unclear. MacVicar 2019 noted reduced use of pharmacotherapy in 10 studies and reduced length of stay in nine studies in a narrative review of non‐pharmacological care including 14 studies of heterogeneous non‐pharmacological interventions (13 non‐randomized, 1 RCT evaluating acupuncture; 2 studies included changes to pharmacotherapy protocols). Other studies, such as Oostlander 2019, Mangat 2019, and Ryan 2019 described randomized studies of environmental changes (D'Apolito 1999; Maichuk 1999; Oro 1988), and acupuncture (Raith 2015), in combination with a larger body of non‐randomized evidence. Based on this combination of evidence, Mangat 2019 concluded "most non‐pharmacological treatments (exception of rocking and outpatient therapy) are safe, effective and easy to be implemented as adjunct therapies to pharmacological treatments."
In summary, recent reviews of non‐pharmacological care for opioid withdrawal in newborns described the potential benefits based largely on non‐randomized evidence. In the current review of RCTs, we concluded that the evidence was uncertain. There is a need for further high‐quality studies to identify the most efficacious interventions and guide clinical care teams to choose safe, cost‐effective, and impactful non‐pharmacological care practices.
Authors' conclusions
Implications for practice.
Although non‐pharmacological care for opioid withdrawal in newborns has biologic plausibility, is low cost, and has potentially low risk of harm, limited evidence informs specific practices. We found six randomized controlled trials (RCTs) that provide very low‐ to low‐certainty evidence for all reported outcomes. Based on this evidence, it is difficult to definitively state an association of specific interventions with outcomes. Given the limited evidence to guide practice, other factors, such as the risk associated with the interventions or the cost to implement the intervention, may guide practitioners to determine optimal non‐pharmacological care practices for their setting while awaiting further evidence. For example, prone positioning is associated with measurable risk of infant death and is not a recommended position for safe sleep in infants (Moon 2016). It is notable that there is often a greater difference in outcomes between sites than there is between comparison groups within a study, suggesting that there are many unmeasured variables that impact care. These may include variability in quality and quantity of non‐pharmacological interventions. We do not have sufficient evidence to guide clinical practice about the use of non‐pharmacological care for opioid withdrawal in newborns.
Implications for research.
Well‐designed appropriately powered studies are needed to determine the effect of non‐pharmacological care for opioid withdrawal in newborns. Studies should use clear and consistent definitions to reduce heterogeneity across sites and studies. To assess heterogeneity in population, it is important to record details about perinatal exposures and maternal medical history, particularly psychiatric history. Strategies to ensure representative enrollment of this vulnerable population are also important to ensure generalizability of studies. Clear definition and categorization of non‐pharmacological care practices is important in the framework of future studies. Better definition of timing and duration or 'dose' of non‐pharmacological interventions, cointerventions, and research outcomes will allow meaningful interpretation of interventions in a systematic review and meta‐analysis. Cointerventions may include other non‐pharmacological interventions, pharmacological interventions, and site of care among other interventions. Use of a core outcome set such as that proposed by Kelly 2020 could facilitate study of meaningful outcomes. Standardized definitions of outcome measures will facilitate meaningful combination of studies in systematic review and meta‐analysis. Future studies should consistently assess both important short‐term outcomes and longer‐term outcomes such as maternal mood and bonding, long‐term neurodevelopment, and social outcomes such as custody status.
The body of literature identified for this systematic review consists of few RCTs and a larger body of non‐randomized study. This is likely partially due to the practical challenges in designing randomized or blinded studies of point‐of‐care practices. Many practices, such as breastfeeding and rooming in, are difficult to randomize and impossible to blind. Others, such as systematic support of the maternal‐infant dyad, consist of cultural changes that will affect care of all patients in a care setting and may require broader community wide interventions. These cultural changes range from hospital practices such as staff ratios and site of care to deeper social issues such as stigma, racism, and poverty. Well‐designed larger studies to determine the most efficacious non‐pharmacological care practices will likely require creative design, such as a stepped wedge cluster randomized trial. To accomplish these important research goals, resources are needed to study point‐of‐care non‐pharmacological interventions and the effects of hospital practices such as site of care, staff ratios, and casualization of the workforce.
History
Protocol first published: Issue 12, 2018 Review first published: Issue 12, 2020
Acknowledgements
The Methods section of this review was based on a standard template used by Cochrane Neonatal.
We acknowledge the work of Ms Kath Wright in developing the search strategies. We would like to thank Cochrane Neonatal: Colleen Ovelman, Managing Editor, Jane Cracknell, Assistant Managing Editor, and Bill McGuire, Coco‐ordinating Editor, who provided editorial and administrative support. Carol Friesen, Information Specialist, in running the literature searches for this review, and Colleen Ovelman in peer reviewing the Ovid MEDLINE.
As a Cochrane Neonatal Associate Editor, XX has peer reviewed and offered feedback for this review.
We appreciate email correspondence to clarify information from the authors of the following studies: Abdel‐Latif 2006; Bogen 2018; Dryden 2009; McKnight 2016; McQueen 2011; Ordean 2015.
Appendices
Appendix 1. Search methods for the review
The RCT filters have been created using Cochrane's highly sensitive search strategies for identifying randomized trials (Higgins 2019). The Cochrane Neonatal Information Specialist created and tested the neonatal filters.
CENTRAL via CRS web
Date searched: 11 October 2019 Terms: 1MESH DESCRIPTOR Neonatal Abstinence Syndrome EXPLODE ALL AND CENTRAL:TARGET 2neonatal abstinence AND CENTRAL:TARGET 3neonatal drug abstinence AND CENTRAL:TARGET 4neonatal drug withdrawal AND CENTRAL:TARGET 5neonatal substance withdrawal AND CENTRAL:TARGET 6neonatal withdrawal syndrome AND CENTRAL:TARGET 7newborn abstinence syndrome AND CENTRAL:TARGET 8newborn drug withdrawal syndrome AND CENTRAL:TARGET 9newborn withdrawal syndrome AND CENTRAL:TARGET 10neonatal withdrawal symptom* AND CENTRAL:TARGET 11#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 AND CENTRAL:TARGET 12MESH DESCRIPTOR Opioid‐Related Disorders EXPLODE ALL AND CENTRAL:TARGET 13MESH DESCRIPTOR Opiate Substitution Treatment EXPLODE ALL AND CENTRAL:TARGET 14opiate substitution treatment AND CENTRAL:TARGET 15opiate substitution therapy AND CENTRAL:TARGET 16opiate replacement therapy AND CENTRAL:TARGET 17opiate replacement treatment AND CENTRAL:TARGET 18opioid replacement therapy AND CENTRAL:TARGET 19opioid replacement treatment AND CENTRAL:TARGET 20NAS AND CENTRAL:TARGET 21#12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 AND CENTRAL:TARGET 22MESH DESCRIPTOR Infant EXPLODE ALL AND CENTRAL:TARGET 23MESH DESCRIPTOR Infant, Newborn EXPLODE ALL AND CENTRAL:TARGET 24neonat* or "neo nat*" AND CENTRAL:TARGET 25newborn* or "new born*" or "newly born*" AND CENTRAL:TARGET 26infant* or infancy AND CENTRAL:TARGET 27baby or babies AND CENTRAL:TARGET 28#22 OR #23 OR #24 OR #25 OR #26 OR #27 AND CENTRAL:TARGET 29#21 AND #28 AND CENTRAL:TARGET 30(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opioid dependen*" AND CENTRAL:TARGET 31(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opiate dependen*" AND CENTRAL:TARGET 32(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "narcotic dependen*" AND CENTRAL:TARGET 33(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "heroin dependen*" AND CENTRAL:TARGET 34(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "cocaine dependen*" AND CENTRAL:TARGET 35(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opioid toleran*" AND CENTRAL:TARGET 36(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opiate toleran*" AND CENTRAL:TARGET 37(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "narcotic toleran*" AND CENTRAL:TARGET 38(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "heroin toleran*" AND CENTRAL:TARGET 39(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "cocaine toleran*" AND CENTRAL:TARGET 40(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opioid withdraw*" AND CENTRAL:TARGET 41(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opiate withdraw*" AND CENTRAL:TARGET 42(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "narcotic withdraw*" AND CENTRAL:TARGET 43(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "heroin withdraw*" AND CENTRAL:TARGET 44(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "cocaine withdraw*" AND CENTRAL:TARGET 45(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opioid expos*" AND CENTRAL:TARGET 46(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opiate expos*" AND CENTRAL:TARGET 47(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "narcotic expos*" AND CENTRAL:TARGET 48(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "heroin expos*" AND CENTRAL:TARGET 49(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "cocaine expos*" AND CENTRAL:TARGET 50(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opioid addiction" AND CENTRAL:TARGET 51(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "opiate addiction" AND CENTRAL:TARGET 52(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "narcotic addiction" AND CENTRAL:TARGET 53(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "heroin addiction" AND CENTRAL:TARGET 54(neonatal* or newborn* or baby* or babies* or infant* or child*) ADJ5 "cocaine addiction" AND CENTRAL:TARGET 55#30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 OR #49 OR #50 OR #51 OR #52 OR #53 OR #54 AND CENTRAL:TARGET 56#29 OR #55 AND CENTRAL:TARGET 57MESH DESCRIPTOR Prenatal Exposure Delayed Effects EXPLODE ALL AND CENTRAL:TARGET 58MESH DESCRIPTOR Amphetamine‐Related Disorders EXPLODE ALL AND CENTRAL:TARGET 59MESH DESCRIPTOR Cocaine‐Related Disorders EXPLODE ALL AND CENTRAL:TARGET 60MESH DESCRIPTOR Heroin Dependence EXPLODE ALL AND CENTRAL:TARGET 61MESH DESCRIPTOR Inhalant Abuse EXPLODE ALL AND CENTRAL:TARGET 62MESH DESCRIPTOR Marijuana Abuse EXPLODE ALL AND CENTRAL:TARGET 63MESH DESCRIPTOR Opioid‐Related Disorders EXPLODE ALL AND CENTRAL:TARGET 64MESH DESCRIPTOR Phencyclidine Abuse EXPLODE ALL AND CENTRAL:TARGET 65MESH DESCRIPTOR Substance Abuse, Intravenous EXPLODE ALL AND CENTRAL:TARGET 66MESH DESCRIPTOR Substance Abuse, Oral EXPLODE ALL AND CENTRAL:TARGET 67MESH DESCRIPTOR Substance Withdrawal Syndrome EXPLODE ALL AND CENTRAL:TARGET 68(opioid* or opiate* or narcotic* or heroin or cocaine) ADJ5 (addiction or depend* or toleran* or withdraw* or expos*) AND CENTRAL:TARGET 69#58 OR #59 OR #60 OR #61 OR #62 OR #63 OR #64 OR #65 OR #66 OR #67 OR #68 AND CENTRAL:TARGET 70#57 AND #69 AND CENTRAL:TARGET 71#11 OR #56 OR #70 AND CENTRAL:TARGET
MEDLINE via Ovid
Date ranges: 1946 to 11 October 2019 Terms: 1. Neonatal Abstinence Syndrome/ 2. neonatal abstinence.ti,ab,kw. 3. neonatal drug abstinence.ti,ab,kw. 4. neonatal drug withdrawal.ti,ab,kw. 5. neonatal substance withdrawal.ti,ab,kw. 6. neonatal withdrawal symptom$.ti,ab,kw. 7. neonatal withdrawal syndrome.ti,ab,kw. 8. newborn abstinence syndrome.ti,ab,kw. 9. newborn drug withdrawal syndrome.ti,ab,kw. 10. newborn withdrawal syndrome.ti,ab,kw. 11. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 12. randomized controlled trial.pt. 13. controlled clinical trial.pt. 14. randomized.ab. 15. placebo.ab. 16. drug therapy.fs. 17. randomly.ab. 18. trial.ab. 19. groups.ab. 20. 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 21. exp animals/ not humans.sh. 22. 20 not 21 23. 11 and 22 24. exp Opioid‐Related Disorders/ 25. Opiate Substitution Treatment/ 26. (opiate substitution treatment or opioid substitution treatment).ti,ab,kw. 27. (opiate substitution therapy or opioid substitution therapy).ti,ab,kw. 28. (opiate replacement therapy or opioid replacement therapy).ti,ab,kw. 29. (opiate replacement treatment or opioid replacement treatment).ti,ab,kw. 30. NAS.ti,ab. 31. 24 or 25 or 26 or 27 or 28 or 29 or 30 32. exp Infant/ or Infant, Newborn/ 33. (neonat$ or neo nat$).ti,ab. 34. (newborn$ or new born$ or newly born$).ti,ab. 35. infan$.ti,ab. 36. (baby or babies).ti,ab. 37. 32 or 33 or 34 or 35 or 36 38. 31 and 37 39. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid dependen$).ti,ab,kw. 40. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate dependen$).ti,ab,kw. 41. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic dependen$).ti,ab,kw. 42. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin dependen$).ti,ab,kw. 43. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine dependen$).ti,ab,kw. 44. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid toleran$).ti,ab,kw. 45. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate toleran$).ti,ab,kw. 46. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic toleran$).ti,ab,kw. 47. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin toleran$).ti,ab,kw. 48. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine toleran$).ti,ab,kw. 49. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid withdraw$).ti,ab,kw. 50. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate withdraw$).ti,ab,kw. 51. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic withdraw$).ti,ab,kw. 52. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin withdraw$).ti,ab,kw. 53. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine withdraw$).ti,ab,kw. 54. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid expos$).ti,ab,kw. 55. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate expos$).ti,ab,kw. 56. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic expos$).ti,ab,kw. 57. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin expos$).ti,ab,kw. 58. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine expos$).ti,ab,kw. 59. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid addiction).ti,ab,kw. 60. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate addiction).ti,ab,kw. 61. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic addiction).ti,ab,kw. 62. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin addiction).ti,ab,kw. 63. ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine addiction).ti,ab,kw. 64. 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 65. randomized controlled trial.pt. 66. controlled clinical trial.pt. 67. randomized.ab. 68. placebo.ab. 69. drug therapy.fs. 70. randomly.ab. 71. trial.ab. 72. groups.ab. 73. 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 74. exp animals/ not humans.sh. 75. 73 not 74 76. 64 and 75 77. Prenatal Exposure Delayed Effects/ 78. amphetamine‐related disorders/ or cocaine‐related disorders/ or heroin dependence/ or inhalant abuse/ or marijuana abuse/ or opioid‐related disorders/ or phencyclidine abuse/ or substance abuse, intravenous/ or substance abuse, oral/ or substance withdrawal syndrome/ 79. ((opioid$ or opiate$ or narcotic$ or heroin or cocaine) adj5 (addiction or depend$ or toleran$ or withdraw$ or expos$)).ti,ab,kw. 80. 78 or 79 81. 77 and 80 82. randomized controlled trial.pt. 83. controlled clinical trial.pt. 84. randomized.ab. 85. placebo.ab. 86. drug therapy.fs. 87. randomly.ab. 88. trial.ab. 89. groups.ab. 90. 82 or 83 or 84 or 85 or 86 or 87 or 88 or 89 91. exp animals/ not humans.sh. 92. 90 not 91 93. 81 and 92 94. 23 or 76 or 93
CINAHL via EBSCOhost
Date ranges: 1981 to 11 October 2019 Terms: S1MH Neonatal abstinence syndrome OR TX ( "neonatal abstinence" OR "neonatal drug abstinence" OR "neonatal drug withdrawal" OR "neonatal substance withdrawal" OR "neonatal withdrawal syndrome" OR "newborn abstinence syndrome" OR "newborn drug withdrawal syndrome" OR "newborn withdrawal syndrome" OR "neonatal withdrawal symptom*" ) S2MH randomized controlled trials OR MH clinical trials S3S1 AND S2 S4TX opiate substitution treatment OR opioid substitution treatment OR opiate substitution therapy OR opioid substitution therapy OR opiate replacement therapy OR opioid replacement therapy OR opiate replacement treatment OR opioid replacement treatment S5TX NAS S6S4 OR S5 S7MH infant OR MH infant, newborn S8S6 AND S7 S9S2 AND S8 S10MH infant, drug‐exposed S11(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opioid dependen*" S12(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opiate dependen*" S13(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "narcotic dependen*" S14(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "heroin dependen*" S15(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "cocaine dependen*" S16S11 OR S12 OR S13 OR S14 OR S15 S17(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opioid toleran*" S18(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opiate toleran*" S19(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "narcotic toleran*" S20(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "heroin toleran*" S21(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "cocaine toleran*" S22S17 OR S18 OR S19 OR S20 OR S21 S23(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opioid withdraw*" S24(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opiate withdraw*" S25(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "narcotic withdraw*" S26(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "heroin withdraw*" S27(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "cocaine withdraw*" S28S23 OR S24 OR S25 OR S26 OR S27 S29(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opioid expos*" S30(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opiate expos*" S31(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "narcotic expos*" S32(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "heroin expos*" S33(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "cocaine expos*" S34S29 OR S30 OR S31 OR S32 OR S33 S35(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opioid addiction" S36(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "opiate addiction" S37(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "narcotic addiction" S38(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "heroin addiction" S39(neonatal* or newborn* or baby* or babies* or infant* or child*) N5 "cocaine addiction" S40S35 OR S36 OR S37 OR S38 OR S39 S41S10 OR S16 OR S22 OR S28 OR S34 OR S40 S42S2 AND S41 S43S3 OR S9 OR S42
ISRCTN
Date searched: 11 October 2019 Terms: "neonatal abstinence syndrome AND ( Participant age range: Neonate )"
Appendix 2. Search methods for the protocol
The Cochrane Central Register of Controlled Trials (CENTRAL) via John Wiley's the Cochrane Library
| ID | Search |
| #1 | MeSH descriptor: [Neonatal Abstinence Syndrome] explode all trees |
| #2 | neonatal abstinence:ti,ab,kw (Word variations have been searched) |
| #3 | neonatal drug abstinence:ti,ab,kw (Word variations have been searched) |
| #4 | neonatal drug withdrawal:ti,ab,kw (Word variations have been searched) |
| #5 | neonatal substance withdrawal:ti,ab,kw (Word variations have been searched) |
| #6 | neonatal withdrawal syndrome:ti,ab,kw (Word variations have been searched) |
| #7 | newborn abstinence syndrome:ti,ab,kw (Word variations have been searched) |
| #8 | newborn drug withdrawal syndrome:ti,ab,kw (Word variations have been searched) |
| #9 | newborn withdrawal syndrome:ti,ab,kw (Word variations have been searched) |
| #10 | neonatal withdrawal symptom*:ti,ab,kw (Word variations have been searched) |
| #11 | #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 |
| #12 | MeSH descriptor: [Opioid‐Related Disorders] explode all trees |
| #13 | MeSH descriptor: [Opiate Substitution Treatment] explode all trees |
| #14 | opiate substitution treatment:ti,ab,kw (Word variations have been searched) |
| #15 | opiate substitution therapy:ti,ab,kw (Word variations have been searched) |
| #16 | opiate replacement therapy:ti,ab,kw (Word variations have been searched) |
| #17 | opiate replacement treatment:ti,ab,kw (Word variations have been searched) |
| #18 | opioid replacement therapy:ti,ab,kw (Word variations have been searched) |
| #19 | opioid replacement treatment:ti,ab,kw (Word variations have been searched) |
| #20 | NAS:ti,ab,kw (Word variations have been searched) |
| #21 | #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 |
| #22 | MeSH descriptor: [Infant] explode all trees |
| #23 | MeSH descriptor: [Infant, Newborn] explode all trees |
| #24 | neonat* or "neo nat*":ti,ab,kw (Word variations have been searched) |
| #25 | newborn* or "new born*" or "newly born*":ti,ab,kw (Word variations have been searched) |
| #26 | infant* or infancy:ti,ab,kw (Word variations have been searched) |
| #27 | baby or babies:ti,ab,kw (Word variations have been searched) |
| #28 | #22 or #23 or #24 or #25 or #26 or #27 |
| #29 | #21 and #28 |
| #30 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opioid dependen*":ti,ab,kw (Word variations have been searched) |
| #31 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opiate dependen*":ti,ab,kw (Word variations have been searched) |
| #32 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "narcotic dependen*":ti,ab,kw (Word variations have been searched) |
| #33 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "heroin dependen*":ti,ab,kw (Word variations have been searched) |
| #34 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "cocaine dependen*":ti,ab,kw (Word variations have been searched) |
| #35 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opioid toleran*":ti,ab,kw (Word variations have been searched) |
| #36 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opiate toleran*":ti,ab,kw (Word variations have been searched) |
| #37 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "narcotic toleran*":ti,ab,kw (Word variations have been searched) |
| #38 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "heroin toleran*":ti,ab,kw (Word variations have been searched) |
| #39 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "cocaine toleran*":ti,ab,kw (Word variations have been searched) |
| #40 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opioid withdraw*":ti,ab,kw (Word variations have been searched) |
| #41 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opiate withdraw*":ti,ab,kw (Word variations have been searched) |
| #42 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "narcotic withdraw*":ti,ab,kw (Word variations have been searched) |
| #43 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "heroin withdraw*":ti,ab,kw (Word variations have been searched) |
| #44 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "cocaine withdraw*":ti,ab,kw (Word variations have been searched) |
| #45 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opioid expos*":ti,ab,kw (Word variations have been searched) |
| #46 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opiate expos*":ti,ab,kw (Word variations have been searched) |
| #47 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "narcotic expos*":ti,ab,kw (Word variations have been searched) |
| #48 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "heroin expos*":ti,ab,kw (Word variations have been searched) |
| #49 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "cocaine expos*":ti,ab,kw (Word variations have been searched) |
| #50 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opioid addiction":ti,ab,kw (Word variations have been searched) |
| #51 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "opiate addiction":ti,ab,kw (Word variations have been searched) |
| #52 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "narcotic addiction":ti,ab,kw (Word variations have been searched) |
| #53 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "heroin addiction":ti,ab,kw (Word variations have been searched) |
| #54 | (neonatal* or newborn* or baby* or babies* or infant* or child*) near/5 "cocaine addiction":ti,ab,kw (Word variations have been searched) |
| #55 | #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 or #40 or #41 or #42 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or #50 or #51 or #52 or #53 or #54 |
| #56 | #29 or #55 |
| #57 | MeSH descriptor: [Prenatal Exposure Delayed Effects] explode all trees |
| #58 | MeSH descriptor: [Amphetamine‐Related Disorders] explode all trees |
| #59 | MeSH descriptor: [Cocaine‐Related Disorders] explode all trees |
| #60 | MeSH descriptor: [Heroin Dependence] explode all trees |
| #61 | MeSH descriptor: [Inhalant Abuse] explode all trees |
| #62 | MeSH descriptor: [Marijuana Abuse] explode all trees |
| #63 | MeSH descriptor: [Opioid‐Related Disorders] explode all trees |
| #64 | MeSH descriptor: [Phencyclidine Abuse] explode all trees |
| #65 | MeSH descriptor: [Substance Abuse, Intravenous] explode all trees |
| #66 | MeSH descriptor: [Substance Abuse, Oral] explode all trees |
| #67 | MeSH descriptor: [Substance Withdrawal Syndrome] explode all trees |
| #68 | (opioid* or opiate* or narcotic* or heroin or cocaine) near/5 (addiction or depend* or toleran* or withdraw* or expos*):ti,ab,kw (Word variations have been searched) |
| #69 | #58 or #59 or #60 or #61 or #62 or #63 or #64 or #65 or #66 or #67 or #68 |
| #70 | #57 and #69 |
| #71 | #11 or #56 or #70 |
via OvidSP Database: Embase <1974 to current>
| 1 | Neonatal Abstinence Syndrome/ |
| 2 | Congenital Drug Dependence/ |
| 3 | neonatal abstinence.ti,ab,kw. |
| 4 | neonatal drug abstinence.ti,ab,kw. |
| 5 | neonatal drug withdrawal.ti,ab,kw. |
| 6 | neonatal substance withdrawal.ti,ab,kw. |
| 7 | neonatal withdrawal symptom$.ti,ab,kw. |
| 8 | neonatal withdrawal syndrome.ti,ab,kw. |
| 9 | newborn abstinence syndrome.ti,ab,kw. |
| 10 | newborn drug withdrawal syndrome.ti,ab,kw. |
| 11 | newborn withdrawal syndrome.ti,ab,kw. |
| 12 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 |
| 13 | (random* or factorial* or placebo* or assign* or allocat* or crossover*).tw. |
| 14 | (cross adj over*).tw. |
| 15 | (trial* and (control* or comparative)).tw. |
| 16 | ((blind* or mask*) and (single or double or triple or treble)).tw. |
| 17 | (treatment adj arm*).tw. |
| 18 | (control* adj group*).tw. |
| 19 | (phase adj (III or three)).tw. |
| 20 | (versus or vs).tw. |
| 21 | rct.tw. |
| 22 | Crossover Procedure/ |
| 23 | Double Blind Procedure/ |
| 24 | Single Blind Procedure/ |
| 25 | Randomization/ |
| 26 | Placebo/ |
| 27 | exp Clinical Trial/ |
| 28 | Parallel Design/ |
| 29 | Latin Square Design/ |
| 30 | 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 |
| 31 | exp animal/ or exp nonhuman/ or exp animal experiment/ or exp animal model/ |
| 32 | exp human/ |
| 33 | 31 not 32 |
| 34 | 30 not 33 |
| 35 | 12 and 34 |
| 36 | Opioid Addiction/ |
| 37 | exp Opioid‐Related Disorders/ |
| 38 | Opiate Substitution Treatment/ |
| 39 | (opiate substitution treatment or opioid substitution treatment).ti,ab,kw. |
| 40 | (opiate substitution therapy or opioid substitution therapy).ti,ab,kw. |
| 41 | (opiate replacement therapy or opioid replacement therapy).ti,ab,kw. |
| 42 | (opiate replacement treatment or opioid replacement treatment).ti,ab,kw. |
| 43 | NAS.ti,ab. |
| 44 | 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 |
| 45 | Infant/ or Newborn/ |
| 46 | (neonat$ or neo nat$).ti,ab. |
| 47 | (newborn$ or new born$ or newly born$).ti,ab. |
| 48 | infan$.ti,ab. |
| 49 | (baby or babies).ti,ab. |
| 50 | 45 or 46 or 47 or 48 or 49 |
| 51 | 44 and 50 |
| 52 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid dependen$).ti,ab,kw. |
| 53 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate dependen$).ti,ab,kw. |
| 54 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic dependen$).ti,ab,kw. |
| 55 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin dependen$).ti,ab,kw. |
| 56 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine dependen$).ti,ab,kw. |
| 57 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid toleran$).ti,ab,kw. |
| 58 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate toleran$).ti,ab,kw. |
| 59 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic toleran$).ti,ab,kw. |
| 60 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin toleran$).ti,ab,kw. |
| 61 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine toleran$).ti,ab,kw. |
| 62 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid withdraw$).ti,ab,kw. |
| 63 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate withdraw$).ti,ab,kw. |
| 64 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic withdraw$).ti,ab,kw. |
| 65 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin withdraw$).ti,ab,kw. |
| 66 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine withdraw$).ti,ab,kw. |
| 67 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid expos$).ti,ab,kw. (80) |
| 68 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate expos$).ti,ab,kw. |
| 69 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic expos$).ti,ab,kw. |
| 70 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin expos$).ti,ab,kw. |
| 71 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine expos$).ti,ab,kw. |
| 72 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid addiction).ti,ab,kw. |
| 73 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate addiction).ti,ab,kw. |
| 74 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic addiction).ti,ab,kw. |
| 75 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin addiction).ti,ab,kw. |
| 76 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine addiction).ti,ab,kw. |
| 77 | 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 or 73 or 74 or 75 or 76 |
| 78 | (random* or factorial* or placebo* or assign* or allocat* or crossover*).tw. |
| 79 | (cross adj over*).tw. |
| 80 | (trial* and (control* or comparative)).tw. |
| 81 | ((blind* or mask*) and (single or double or triple or treble)).tw. |
| 82 | (treatment adj arm*).tw. |
| 83 | (control* adj group*).tw. |
| 84 | (phase adj (III or three)).tw. |
| 85 | (versus or vs).tw. |
| 86 | rct.tw. |
| 87 | Crossover Procedure/ |
| 88 | Double Blind Procedure/ |
| 89 | Single Blind Procedure/ |
| 90 | Randomization/ |
| 91 | Placebo/ |
| 92 | exp Clinical Trial/ |
| 93 | Parallel Design/ |
| 94 | Latin Square Design/ |
| 95 | 78 or 79 or 80 or 81 or 82 or 83 or 84 or 85 or 86 or 87 or 88 or 89 or 90 or 91 or 92 or 93 or 94 |
| 96 | exp animal/ or exp nonhuman/ or exp animal experiment/ or exp animal model/ |
| 97 | exp human/ |
| 98 | 96 not 97 |
| 99 | 95 not 98 |
| 100 | 77 and 99 |
| 101 | prenatal exposure/ |
| 102 | drug dependence/ or amphetamine dependence/ or benzodiazepine dependence/ or cannabis addiction/ or cocaine dependence/ or drug misuse/ or glue sniffing/ or methamphetamine dependence/ or multiple drug abuse/ or exp narcotic dependence/ or phencyclidine dependence/ |
| 103 | ((opioid$ or opiate$ or narcotic$ or heroin or cocaine) adj5 (addiction or depend$ or toleran$ or withdraw$ or expos$)).ti,ab,kw. |
| 104 | 102 or 103 |
| 105 | 101 and 104 |
| 106 | (random* or factorial* or placebo* or assign* or allocat* or crossover*).tw. |
| 107 | (cross adj over*).tw. |
| 108 | (trial* and (control* or comparative)).tw. |
| 109 | ((blind* or mask*) and (single or double or triple or treble)).tw. |
| 110 | (treatment adj arm*).tw. |
| 111 | (control* adj group*).tw. |
| 112 | (phase adj (III or three)).tw. |
| 113 | (versus or vs).tw. |
| 114 | rct.tw. |
| 115 | Crossover Procedure/ |
| 116 | Double Blind Procedure/ |
| 117 | Single Blind Procedure/ |
| 118 | Randomization/ |
| 119 | Placebo/ |
| 120 | exp Clinical Trial/ |
| 121 | Parallel Design/ |
| 122 | Latin Square Design/ |
| 123 | 106 or 107 or 108 or 109 or 110 or 111 or 112 or 113 or 114 or 115 or 116 or 117 or 118 or 119 or 120 or 121 or 122 |
| 124 | exp animal/ or exp nonhuman/ or exp animal experiment/ or exp animal model/ |
| 125 | exp human/ |
| 126 | 124 not 125 |
| 127 | 123 not 126 |
| 128 | 105 and 127 |
| 129 | 35 or 100 or 128 |
Database: Maternity and Infant Care Database (MIDIRS) <1971 to current>
| 1 | Neonatal abstinence syndrome.de. |
| 2 | neonatal abstinence.ti,ab,kw. |
| 3 | neonatal drug abstinence.ti,ab,kw. |
| 4 | neonatal drug withdrawal.ti,ab,kw. |
| 5 | neonatal substance withdrawal.ti,ab,kw. |
| 6 | neonatal withdrawal symptom$.ti,ab,kw. |
| 7 | neonatal withdrawal syndrome.ti,ab,kw. |
| 8 | newborn abstinence syndrome.ti,ab,kw. |
| 9 | newborn drug withdrawal syndrome.ti,ab,kw. |
| 10 | newborn withdrawal syndrome.ti,ab,kw. |
| 11 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 |
| 12 | Opioid‐related disorders.de. |
| 13 | (opiate substitution treatment or opioid substitution treatment).ti,ab,kw. |
| 14 | (opiate substitution therapy or opioid substitution therapy).ti,ab,kw. |
| 15 | (opiate replacement therapy or opioid replacement therapy).ti,ab,kw. |
| 16 | (opiate replacement treatment or opioid replacement treatment).ti,ab,kw. |
| 17 | NAS.ti,ab. |
| 18 | 12 or 13 or 14 or 15 or 16 or 17 |
| 19 | (Infant or Infant ‐ newborn).de. |
| 20 | (neonat$ or neo nat$).ti,ab. |
| 21 | (newborn$ or new born$ or newly born$).ti,ab. |
| 22 | infan$.ti,ab. |
| 23 | (baby or babies).ti,ab. |
| 24 | 19 or 20 or 21 or 22 or 23 |
| 25 | 18 and 24 |
| 26 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid dependen$).ti,ab,kw. |
| 27 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate dependen$).ti,ab,kw. |
| 28 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic dependen$).ti,ab,kw. |
| 29 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin dependen$).ti,ab,kw. |
| 30 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine dependen$).ti,ab,kw. |
| 31 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid toleran$).ti,ab,kw. |
| 32 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate toleran$).ti,ab,kw. |
| 33 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic toleran$).ti,ab,kw. |
| 34 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin toleran$).ti,ab,kw. |
| 35 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine toleran$).ti,ab,kw. |
| 36 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid withdraw$).ti,ab,kw. |
| 37 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate withdraw$).ti,ab,kw. |
| 38 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic withdraw$).ti,ab,kw. |
| 39 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin withdraw$).ti,ab,kw. |
| 40 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine withdraw$).ti,ab,kw. |
| 41 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid expos$).ti,ab,kw. |
| 42 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate expos$).ti,ab,kw. |
| 43 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic expos$).ti,ab,kw. |
| 44 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin expos$).ti,ab,kw. |
| 45 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine expos$).ti,ab,kw. |
| 46 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid addiction).ti,ab,kw. |
| 47 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate addiction).ti,ab,kw. |
| 48 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic addiction).ti,ab,kw. |
| 49 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin addiction).ti,ab,kw. |
| 50 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine addiction).ti,ab,kw. |
| 51 | 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 |
| 52 | 11 or 25 or 51 |
| 53 | limit 52 to randomised controlled trial |
Database: Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) <1946 to Present>
| 1 | Neonatal Abstinence Syndrome/ |
| 2 | neonatal abstinence.ti,ab,kw. |
| 3 | neonatal drug abstinence.ti,ab,kw. |
| 4 | neonatal drug withdrawal.ti,ab,kw. |
| 5 | neonatal substance withdrawal.ti,ab,kw. |
| 6 | neonatal withdrawal symptom$.ti,ab,kw. |
| 7 | neonatal withdrawal syndrome.ti,ab,kw. |
| 8 | newborn abstinence syndrome.ti,ab,kw. |
| 9 | newborn drug withdrawal syndrome.ti,ab,kw. |
| 10 | newborn withdrawal syndrome.ti,ab,kw. |
| 11 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 |
| 12 | randomized controlled trial.pt. |
| 13 | controlled clinical trial.pt. |
| 14 | randomized.ab. |
| 15 | placebo.ab. |
| 16 | drug therapy.fs. |
| 17 | randomly.ab. |
| 18 | trial.ab. |
| 19 | groups.ab. |
| 20 | 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 |
| 21 | exp animals/ not humans.sh. |
| 22 | 20 not 21 |
| 23 | 11 and 22 |
| 24 | exp Opioid‐Related Disorders/ |
| 25 | Opiate Substitution Treatment/ |
| 26 | (opiate substitution treatment or opioid substitution treatment).ti,ab,kw. |
| 27 | (opiate substitution therapy or opioid substitution therapy).ti,ab,kw. |
| 28 | (opiate replacement therapy or opioid replacement therapy).ti,ab,kw. |
| 29 | (opiate replacement treatment or opioid replacement treatment).ti,ab,kw. |
| 30 | NAS.ti,ab. |
| 31 | 24 or 25 or 26 or 27 or 28 or 29 or 30 |
| 32 | exp Infant/ or Infant, Newborn/ |
| 33 | (neonat$ or neo nat$).ti,ab. |
| 34 | (newborn$ or new born$ or newly born$).ti,ab. |
| 35 | infan$.ti,ab. |
| 36 | (baby or babies).ti,ab. |
| 37 | 32 or 33 or 34 or 35 or 36 |
| 38 | 31 and 37 |
| 39 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid dependen$).ti,ab,kw. |
| 40 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate dependen$).ti,ab,kw. |
| 41 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic dependen$).ti,ab,kw. |
| 42 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin dependen$).ti,ab,kw. |
| 43 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine dependen$).ti,ab,kw. |
| 44 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid toleran$).ti,ab,kw. |
| 45 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate toleran$).ti,ab,kw. |
| 46 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic toleran$).ti,ab,kw. |
| 47 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin toleran$).ti,ab,kw. |
| 48 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine toleran$).ti,ab,kw. (0) |
| 49 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid withdraw$).ti,ab,kw. |
| 50 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate withdraw$).ti,ab,kw. |
| 51 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic withdraw$).ti,ab,kw. |
| 52 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin withdraw$).ti,ab,kw. |
| 53 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine withdraw$).ti,ab,kw. |
| 54 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid expos$).ti,ab,kw. |
| 55 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate expos$).ti,ab,kw. |
| 56 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic expos$).ti,ab,kw. |
| 57 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin expos$).ti,ab,kw. |
| 58 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine expos$).ti,ab,kw. |
| 59 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opioid addiction).ti,ab,kw. |
| 60 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 opiate addiction).ti,ab,kw. |
| 61 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 narcotic addiction).ti,ab,kw. |
| 62 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 heroin addiction).ti,ab,kw. |
| 63 | ((neonatal$ or newborn$ or baby$ or babies$ or infant$ or child$) adj5 cocaine addiction).ti,ab,kw. |
| 64 | 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 |
| 65 | randomized controlled trial.pt. |
| 66 | controlled clinical trial.pt. |
| 67 | randomized.ab. |
| 68 | placebo.ab. |
| 69 | drug therapy.fs. |
| 70 | randomly.ab. |
| 71 | trial.ab. |
| 72 | groups.ab. |
| 73 | 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 |
| 74 | exp animals/ not humans.sh. |
| 75 | 73 not 74 |
| 76 | 64 and 75 |
| 77 | Prenatal Exposure Delayed Effects/ |
| 78 | amphetamine‐related disorders/ or cocaine‐related disorders/ or heroin dependence/ or inhalant abuse/ or marijuana abuse/ or opioid‐related disorders/ or phencyclidine abuse/ or substance abuse, intravenous/ or substance abuse, oral/ or substance withdrawal syndrome/ |
| 79 | ((opioid$ or opiate$ or narcotic$ or heroin or cocaine) adj5 (addiction or depend$ or toleran$ or withdraw$ or expos$)).ti,ab,kw. |
| 80 | 78 or 79 |
| 81 | 77 and 80 |
| 82 | randomized controlled trial.pt. |
| 83 | controlled clinical trial.pt. |
| 84 | randomized.ab. |
| 85 | placebo.ab. |
| 86 | drug therapy.fs. |
| 87 | randomly.ab. |
| 88 | trial.ab. |
| 89 | groups.ab. |
| 90 | 82 or 83 or 84 or 85 or 86 or 87 or 88 or 89 |
| 91 | exp animals/ not humans.sh. |
| 92 | 90 not 91 |
| 93 | 81 and 92 |
| 94 | 23 or 76 or 93 |
Appendix 3. Details of non‐randomized studies
We identified 34 comparative non‐randomized studies published between 2005 and 2018 that evaluated non‐pharmacological care for opioid withdrawal (29 for comparison 1 and 5 for comparison 2). We described these non‐randomized studies in the narrative to provide additional context about existing comparative studies evaluating the effect of one or more non‐pharmacological care practice (see Excluded studies). The 34 non‐randomized studies included two studies of environmental interventions, 15 studies of feeding practices, 10 studies of support of the mother‐infant dyad, and seven studies of multiple non‐pharmacological care practices. The effects of interventions for the excluded non‐randomized studies are described in this appendix. Further detail, including information about statistical analysis, is described in the supplementary tables (Table 2; Table 3; Table 4; Table 5).
Assessment of risk of bias
We did not formally assess the certainty of evidence with a 'Risk of bias' assessment for the 34 non‐randomized studies or perform a GRADE analysis of outcomes. The certainty of evidence for non‐randomized studies is at baseline very low as there is high risk of bias inherent to the study design. We assumed a high risk of bias for all non‐randomized studies and very low‐certainty evidence for all reported outcomes. Common areas of bias as categorized by the ROBINS‐I tool include confounding, selection of participants, classification of interventions, deviations from interventions, missing data, measurement of outcomes, and selection of reported results (Sterne 2016). Broadly, the non‐randomized studies included in the narrative were often at high risk for bias related to lack of randomization, parental selection of intervention, lack of blinding, and simple study designs that are often either retrospective or pre–post comparisons.
Effects of interventions
We identified 34 non‐randomized trials that were excluded from formal analysis. Study outcomes are reported below without further statistical analysis. Study details are available in the supplementary tables (Table 2; Table 3; Table 4; Table 5).
Modifying environmental stimulation
Two non‐randomized studies assessed the effect of modifying environmental stimulation on outcomes in opioid‐exposed newborns (Radziewicz 2018; Zuzarte 2017). The modifying environmental stimulation studies assessed Reiki and stochastic vibrotactile stimulation. Neither study recorded outcomes prespecified for this review.
Feeding practices
Fifteen non‐randomized studies assessed the effect of feeding practices on outcomes in opioid‐exposed newborns (Abdel‐Latif 2006; Arlettaz 2005; Dryden 2009; Hodgson 2012; Isemann 2011; Jansson 2008; Liu 2015; McQueen 2011; Metz 2015; O'Connor 2013; Pritham 2012; Radmacher 2017; Short 2016; Wachman 2013; Welle‐Strand 2013). The feeding practice studies assessed the impact of breast milk feedings compared to non‐breast milk feedings.
Measured primary outcomes
Infants at risk for, or having early symptoms consistent with, opioid withdrawal
Length of hospitalization for infants at risk for, or having early symptoms consistent with, opioid withdrawal: seven studies compared length of hospitalization in populations fed breast milk to populations not fed breast milk (Abdel‐Latif 2006; Dryden 2009; Metz 2015; O'Connor 2013; Pritham 2012; Short 2016; Wachman 2013). The outcome values and differences between groups varied by site including a mean of 14.7 days versus 19.1 days in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life (Abdel‐Latif 2006); a median of seven days for both groups in a subgroup of infants not admitted to the neonatal intensive care unit (NICU) in a comparison of infants not admitted to the NICU who received maternal breast milk for 72 hours or more versus less than 72 hours or not at all (Dryden 2009); a mean of 7.08 days versus 6.60 days in a comparison of infants who initiated breastfeeding to those who did not (O'Connor 2013); and a mean of 15.8 days versus 27.4 days in a comparison of breastfed to non‐breastfed infants (Wachman 2013). Metz 2015 reported a differential effect based on exposure type in a comparison of breastfed to non‐breastfed infants (methadone‐exposed mean: 17.17 days versus 29.36 days; slow‐release oral morphine‐exposed mean: 19.71 days versus 31.03 days; buprenorphine‐exposed mean: 12.26 days versus 14.71 days). Pritham 2012 reported shorter length of stay in breastfed neonates than formula‐fed neonates or neonates that fed both formula and breast milk in a regression model of methadone‐exposed infants (β = –0.176, P = 0.05). Short 2016 reported 9.4% shorter length of stay in infants reported to be breastfed at discharge on the birth certificate, than infants not breastfed in regression model (β = –0.060, P = 0.05).
Pharmacological treatment: eight studies compared the use of pharmacological treatment in populations fed breast milk to populations not fed breast milk (Abdel‐Latif 2006; Dryden 2009; Hodgson 2012; Jansson 2008; Liu 2015; O'Connor 2013; Wachman 2013; Welle‐Strand 2013). The outcome values and differences between groups varied by site including 52.9% versus 79.0% in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life (Abdel‐Latif 2006); 12% versus 37% in a comparison of infants who were breastfed to infants who were not breastfed (Hodgson 2012); 12.5% versus 50% in a comparison of breastfed to formula‐fed infants (Jansson 2008); 72% versus 81% in a comparison of infants receiving 50% or greater of feedings as breast milk to 50% or greater of feedings as formula (Liu 2015); 23.1% versus 30.0% in a comparison of infants who initiated breastfeeding to those who did not (O'Connor 2013); 50% versus 77% in a comparison of breastfed to non‐breastfed infants (Wachman 2013); and 57% versus 69% in a comparison of breastfed to not breastfed infants with a differential effect based on exposure type (methadone exposed: 53% versus 80%; buprenorphine exposed: 64% versus 44%) (Welle‐Strand 2013). Dryden 2009 reported reduced odds of pharmacological treatment in infants who received maternal breast milk for 72 hours or more compared to those who received breast milk for less than 72 hours or not at all (odds ratio [OR] 0.55, 95% CI 0.34 to 0.88; 99 infants).
Infants receiving opioid treatment for symptoms consistent with opioid withdrawal
Length of hospitalization for infants receiving opioid treatment for symptoms consistent with opioid withdrawal: Isemann 2011 and Radmacher 2017 compared length of hospitalization for infants receiving pharmacological treatment in populations fed breast milk to populations not fed breast milk. The outcome values and differences between groups varied by site including a median of 12.5 days versus 18.5 days in a comparison of infants who ingested maternal breast milk to formula‐fed infants with an inverse correlation between the percentage of mother's breast milk ingested and length of stay (β = –0.03, P = 0.02) (Isemann 2011); and a mean of 37 days versus 29 days in a comparison of a population fed donor breast milk for up to two weeks compared to a historical comparison population fed formula (Radmacher 2017).
Length of pharmacological treatment: five studies compared length of pharmacological treatment in populations fed breast milk to populations not fed breast milk (Abdel‐Latif 2006; Jansson 2008; Metz 2015; Radmacher 2017; Welle‐Strand 2013). The outcome values and differences between groups varied by site including a mean of 85.4 days versus 108.2 days in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life (Abdel‐Latif 2006); a median of 6 days versus 13.5 days in a comparison of breastfed to formula‐fed infants (Jansson 2008); a mean of 37 days versus 29 days in a comparison of a population fed donor breast milk for up to two weeks compared to a historical comparison population fed formula (Radmacher 2017); and a mean of 28.6 days versus 46.7 days in a comparison of breastfed to not breastfed infants (Welle‐Strand 2013). Metz 2015 reported a differential effect based on exposure type in a comparison of breastfed to non‐breastfed infants (methadone‐exposed mean: 8.10 days versus 16.94 days; slow‐release oral morphine‐exposed mean: 10.20 days vs 18.07 days; buprenorphine‐exposed mean: 4.74 days versus 5.76 days). Welle‐Strand 2013 reported a differential effect based on exposure type in a comparison of breastfed to not breastfed infants (methadone‐exposed mean: 31.0 days versus 48.9 days; buprenorphine‐exposed mean: 25.7 days versus 38.8 days).
Maximum dose of opioid medication: Abdel‐Latif 2006 and Liu 2015 compared maximum dose of opioid medication in populations fed breast milk to populations not fed breast milk. Minimal difference was noted in either study including a mean 0.57 mg/kg/day versus 0.59 mg/kg/day in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life(Abdel‐Latif 2006), and a median of 0.5 mg/kg/day morphine versus 0.5 mg/kg/day in a comparison of infants receiving 50% or greater of feedings as breast milk to 50% or greater of feedings as formula (Liu 2015).
Cumulative dose of opioid medication: Metz 2015 reported a differential effect based on exposure type in a comparison of breastfed to non‐breastfed infants (methadone‐exposed mean: 4.35 mg versus 12.65 mg; slow‐release oral morphine‐exposed mean: 5.23 mg versus 8.75 mg; buprenorphine‐exposed mean: 1.90 mg versus 2.77 mg).
Measured secondary outcomes
Peak neonatal abstinence syndrome (NAS) score in first 72 hours of life: no studies assessed peak NAS score in the first 72 hours of life as predefined in our protocol. Abdel‐Latif 2006 reported lower mean Finnegan scores in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life (depicted graphically, 190 infants). Radmacher 2017 reported no significant difference in median Finnegan scores (values not reported, 24 infants), but a significant decrease in gastrointestinal subscore greater than 2 in a population fed donor breast milk for up to two weeks compared to a historical comparison population fed formula (39% versus 61%). Arlettaz 2005 reported less "NAS" in a comparison of infants who received more than half versus less than half of feedings during hospitalization as human milk (26% versus 78%). Jansson 2008 reported lower median day 3 NAS score (4.5 versus 6.8) and peak NAS score (6.5 versus 11.0) in a comparison of breastfed versus formula‐fed infants. Liu 2015 reported no difference in mean NAS score (5.1 versus 5.4) in a comparison of infants receiving 50% or greater of feedings as breast milk to 50% or greater of feedings as formula. McQueen 2011 reported lower mean modified Finnegan scores in a comparison of infants receiving more than 75% breast milk to less than 25% breast milk (4.9 versus 6.9) as well as fewer infants with a score greater than 8 (17% versus 40.2%). Metz 2015 reported a differential effect based on exposure type in a comparison of breastfed to non‐breastfed infants for the outcomes of mean modified Finnegan score (methadone‐exposed mean: 6.52 versus 7.94; slow‐release oral morphine‐exposed mean: 6.97 versus 9.07; buprenorphine‐exposed mean: 4.89 versus 5.77) and peak modified Finnegan score (methadone‐exposed mean: 12.60 versus 17.00; slow‐release oral morphine‐exposed mean: 15.24 versus 18.93; buprenorphine‐exposed mean: 11.19 versus 12.29). O'Connor 2013 reported lower mean peak modified Finnegan NAS score (8.83 versus 9.65), decreased likelihood of higher scores (8 or greater: 65% versus 75%; 12 or greater: 17% versus 30%) as well as a decrease mean time to first and last peak score (first: 66.5 hours versus 73.5 hours; last: 76.1 hours versus 78.3 hours) in a comparison of infants who initiated breastfeeding to those who did not.
NICU admission: Dryden 2009 reported fewer NICU admissions in infants who received maternal breast milk for 72 hours or more versus less than 72 hours or not at all (28% versus 45%).
Growth rate: Radmacher 2017 reported no significant difference in mean weight gain during study period in a population fed donor breast milk for up to two weeks compared to a historical comparison population fed formula (19.1 g/day versus 10.5 g/day).
Days to regain birth weight: Radmacher 2017 reported no significant difference in mean time to return to birth weight in a population fed donor breast milk for up to two weeks compared to a historical comparison population fed formula (17 days versus 16 days).
Weight nadir: Dryden 2009 reported a lower median weight nadir in infants who received maternal breast milk for 72 hours or more versus less than 72 hours or not at all (10.2% versus 8.5%).
Custody at discharge: Abdel‐Latif 2006 reported fewer predominantly breastfed infants in state custody in a comparison of infants fed two or fewer versus more than two formula feedings on day five of life (foster care: 9.4% versus 29.5%; "child at risk": 31.8% versus 68.6%).
Support of the mother‐infant dyad
Ten non‐randomized studies evaluated methods of support for the mother‐infant dyad on outcomes in opioid‐exposed newborns (Abrahams 2007; Abrahams 2010; Crook 2017; Howard 2017; Hünseler 2013; Metz 2011; McKnight 2016; Ordean 2015; Saiki 2010; Summey 2018). The support of the mother‐infant dyad studies assessed the impact of rooming in (eight studies), a breastfeeding education program (one study), and parental presence (one study).
Measured primary outcomes
Infants at risk for, or having early symptoms consistent with, opioid withdrawal
Length of hospitalization for infants at risk for, or having early symptoms consistent with, opioid withdrawal: six studies compared length of hospitalization in rooming in populations to non‐rooming in populations (Abrahams 2007; Abrahams 2010; Hünseler 2013; McKnight 2016; Ordean 2015; Saiki 2010). The outcome values and differences between groups varied by site including a mean of 11.8 days versus 23.5 days in a comparison of a rooming in cohort to a non‐rooming in historical control group and 25.9 days in a separate facility with a non‐rooming in group (Abrahams 2007); a mean of 17.6 days versus 8.1 days in a comparison of a rooming in cohort to non‐rooming in cohorts at separate facilities (Abrahams 2010); a mean of 36.6 days versus 42.8 days in a comparison of a rooming in cohort to a non‐rooming in group (Hünseler 2013), a median of 5.0 days versus 24.0 days in a comparison of a rooming in cohort to a non‐rooming in historical control group (McKnight 2016); a mean of 26 days versus 14 days and 16 days in a comparison of a rooming in cohort to a non‐rooming in cohorts at separate facilities (Ordean 2015); and 15.9 days versus 19.8 days in a comparison of a rooming in cohort to a non‐rooming in historical control group (Saiki 2010). Crook 2017 reported reduced mean length of stay over time with implementation of new interventions to support breastfeeding (18.80 days to 10.41 days). Metz 2011 reported shorter mean length of stay in a clinical trial group with daily contact with study staff and rooming in compared to a non‐rooming in standard care group (methadone exposed: 16.74 days versus 29.36 days; buprenorphine exposed: 13.67 days versus 13.92 days). Summey 2018 reported decreased median length of stay over time in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in compared to a group not receiving this care (eight days versus nine days).
Pharmacological treatment: five studies compared use of pharmacological treatment in rooming in populations to non‐rooming in populations (Abrahams 2007; Hünseler 2013; McKnight 2016; Ordean 2015; Saiki 2010). The outcome values and differences between groups varied by site including 25.0% in a rooming in cohort versus 55.3% in a non‐rooming in historical control group and 52.8% in a separate facility with a non‐rooming in group (Abrahams 2007); 79% versus 88.7% in a comparison of a rooming in cohort to a non‐rooming in comparison group (Hünseler 2013); 15% versus 83.3% in a comparison of a rooming in cohort to a non‐rooming in historical control group (McKnight 2016); 29% versus 31% and 18% in a comparison of a rooming in cohort to separate facilities with non‐rooming in sites (Ordean 2015); and 11% versus 45% in a comparison of a rooming in cohort to a non‐rooming in historical control group (Saiki 2010). Crook 2017 reported reduced pharmacological treatment over time with implementation of new interventions to support breastfeeding (67.3% to 34.8%). Metz 2011 reported more pharmacological treatment in a clinical trial group with daily contact with study staff and rooming in compared to a non‐rooming in standard care group (76% versus 60%).
Infants receiving opioid treatment for symptoms consistent with opioid withdrawal
Length of hospitalization for infants receiving opioid treatment for symptoms consistent with opioid withdrawal: Howard 2017 reported an association between 100% parental presence and a nine‐day shorter length of hospitalization for infants receiving pharmacological treatment.
Length of pharmacological treatment: five studies compared length of pharmacological treatment in rooming in populations to non‐rooming in populations (Abrahams 2007; Hünseler 2013; McKnight 2016; Ordean 2015; Saiki 2010). The outcome values and differences between groups varied by site including a mean of 5.9 days in a rooming in cohort versus 18.6 days in a non‐rooming in historical control group and 18.6 days in a separate facility with a non‐rooming in group (Abrahams 2007); a mean of 29.5 days versus 35.8 days in a comparison of a rooming in cohort to a non‐rooming in comparison group (Hünseler 2013); a median of 24.0 days versus 29.5 days in a comparison of a rooming in cohort to a non‐rooming in historical control group (McKnight 2016); a mean of 13 days versus 25 days and 30 days in a comparison of a rooming in cohort to groups at separate facilities with non‐rooming in sites (Ordean 2015); and a mean of 7.3 days versus 12.7 days in a comparison of a rooming in cohort to a non‐rooming in historical control group (Saiki 2010). Metz 2011 reported shorter mean length of pharmacological treatment in a clinical trial group with daily contact with study staff and rooming in compared to a non‐rooming in standard care group (methadone exposed: 9.53 days versus 21.25 days; buprenorphine exposed: 7.33 days versus 6.62 days). Howard 2017 reported an association between 100% parental presence and eight fewer days of infant opioid therapy.
Maximum dose of opioid medication: Hünseler 2013 and McKnight 2016 reported maximum doses of opioid medication in a rooming in population compared to a non‐rooming in population. The effect varied by site including a lower mean of 132 μg/kg/day versus 145 μg/kg/day diluted tincture of opium in a comparison of a rooming in cohort to a non‐rooming in comparison group (Hünseler 2013); and no change in a median of 0.48 mg/kg/day versus 0.48 mg/kg/day morphine in a comparison of a rooming in cohort to a non‐rooming in historical control group (McKnight 2016).
Cumulative dose of opioid medication: Metz 2011 reported a lower mean cumulative opioid dose in a clinical trial group with daily contact with study staff and rooming in compared to a non‐rooming in standard care group (methadone exposed: 5.18 mg versus 21.61 mg; buprenorphine exposed: 2.02 mg versus 4.30 mg). Howard 2017 reported an association between parental presence and a 5.3 mg decrease in total morphine equivalent dose.
Measured secondary outcomes
Peak NAS score in first 72 hours of life: no studies assessed peak NAS score in the first 72 hours of life as predefined in our protocol. Hünseler 2013 noted no difference in the frequency of Finnegan Scores of 12 or greater (6.4% in a rooming in cohort versus 6.3% in a non‐rooming in comparison group), and the same maximum Finnegan score in both groups (19 points). Howard 2017 reported an association between 100% parental presence and a 1‐point lower mean Finnegan score as well as a significantly lower mean NAS score when a parent was present compared to when a parent was not present.
NICU admission: three studies compared NICU admission in rooming in populations to non‐rooming in populations (Abrahams 2007; Abrahams 2010; Ordean 2015). The outcome values and differences between groups varied by site including 37.5% in a rooming in cohort versus 89.5% in a non‐rooming in historical control group and 83.3% in a separate facility with a non‐rooming in group (Abrahams 2007); 23.5% versus 38.5% in a comparison of a rooming in cohort to a non‐rooming in group at separate facilities (Abrahams 2010); and 42% versus 94% and 91% in a comparison of a rooming in cohort to non‐rooming in groups at separate facilities (Ordean 2015). Summey 2018 reported decreased NICU admission in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in compared to a group not receiving this care (0% versus 68.8%).
Length of NICU stay: Abrahams 2010 reported decreased mean length of NICU stay in a rooming in population compared to a non‐rooming in population (1.1 days versus 3.1 days in separate facilities with non‐rooming in groups).
Weight nadir: Ordean 2015 noted a mean weight loss of 7.4% in a rooming in cohort versus 7.0% and 8.7% at separate facilities with non‐rooming in sites and a mean weight nadir of 4.3 in a rooming in cohort versus 4.2 and 5.6 at separate facilities with non‐rooming in sites. Abrahams 2007 assessed the proportion of infants with weight loss greater than 10% during the first week and found more infants met this criterion in the rooming in group (16.6% versus 5.2% in a non‐rooming in historical control group and 5.3% in a separate facility with a non‐rooming in group). Summey 2018 noted more infants were diagnosed with "abnormal loss of weight" in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in compared to a group not receiving this care (3.6% versus 0.8%).
Seizures: Summey 2018 reported "convulsions" in one infant in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in and no infants in a group not receiving this care (electroencephalogram [EEG] confirmation not reported).
Custody at discharge: five studies compared custody at discharge in rooming in populations to non‐rooming in populations (Abrahams 2007; Abrahams 2010; Hünseler 2013; Ordean 2015; Saiki 2010). The outcome values and differences between groups varied by site including 71.9% discharged in the custody of the mother in a rooming in cohort versus 31.6% in a non‐rooming in historical control group and 42.5% in a separate facility with a non‐rooming in group (Abrahams 2007); 69.9% discharged home with the mother versus 58.7% in a comparison of a rooming in cohort to non‐rooming in groups in separate facilities (Abrahams 2010); 79.2% discharged home with the family versus 69.8% in a comparison of a rooming in cohort to a non‐rooming in comparison group (Hünseler 2013); 41% discharged in custody of mother versus 69% and 68% in a comparison of a rooming in cohort to non‐rooming in groups at separate facilities (Ordean 2015); and 67% discharged home with the mother versus 60% in a comparison of a rooming in cohort to a non‐rooming in historical control group (Saiki 2010). Howard 2017 reported an association between parental presence and custody status (36.6% parental presence at bedside noted for babies in state custody versus 59.7% parental presence at bedside noted for babies in parental custody). Summey 2018 reported increased child protective services involvement in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in compared to a group not receiving this care (32.7% versus 23.3%).
Cost of care: Hünseler 2013 reported lower mean costs in a comparison of a rooming in cohort to a non‐rooming in comparison group (EUR 10,620 versus EUR 14,331). Summey 2018 reported a lower median total charge in dollars in a group receiving multidisciplinary, co‐ordinated, community‐based care for NAS with an option to room in compared to a group not receiving this care (USD 10,058 versus USD 18,262).
Multiple non‐pharmacological care practices
Seven non‐randomized studies examined multiple non‐pharmacological care practices in combination with other non‐pharmacological and pharmacological treatments (Grossman 2017; Holmes 2016; Kirchner 2014; Loudin 2017; Miles 2007; Patrick 2016; Wachman 2018). The multiple non‐pharmacological care practice studies assessed the impact of quality improvement efforts including non‐pharmacological care practices (five studies) and different care environments (two studies).
Measured primary outcomes
Infants at risk for, or having early symptoms consistent with, opioid withdrawal
Length of hospitalization for infants at risk for, or having early symptoms consistent with, opioid withdrawal: four studies reported length of hospitalization over time with implementation of new interventions including multiple non‐pharmacological care practices (Grossman 2017; Holmes 2016; Miles 2007; Wachman 2018). The effect varied by site including decrease from a mean of 22.4 days to 5.9 days (Grossman 2017), a median of 28 days to 5 days (Miles 2007), a mean of 17.4 days to 11.3 days (Wachman 2018), and no change (Holmes 2016).
Pharmacological treatment: four studies reported reduced use of pharmacological treatment over time with implementation of new interventions including multiple non‐pharmacological care practices (Grossman 2017; Holmes 2016; Miles 2007; Wachman 2018). The outcome values and differences between groups varied by site including decreases from 98% to 14% (Grossman 2017), 87% to 40% (Wachman 2018), 79% to 14% (Miles 2007), and 46% to 27% (Holmes 2016). Kirchner 2014 noted differing treatment rates at different enrollment sites in the MOTHER NAS study (18.5% in Europe rooming in model versus 29.5% in urban USA versus 18.5% in rural USA).
Infants receiving opioid treatment for symptoms consistent with opioid withdrawal
Length of hospitalization for infants receiving opioid treatment for symptoms consistent with opioid withdrawal: Holmes 2016 and Wachman 2018 reported reduced length of hospitalization for infants receiving pharmacological treatment over time with implementation of new interventions including multiple non‐pharmacological care practices. The outcome values and differences between groups varied by site with a decrease from a mean of 16.9 days to 12.3 days (Holmes 2016), and a mean of 19.1 days to 17.6 days (Wachman 2018). Loudin 2017 noted differing treatment rates in different sites of care (median: 24 days in the NICU versus 26 days in the Neonatal Transition Unit versus 33 days in off‐site neonatal abstinence center). Patrick 2016 reported reduced median length of hospitalization over time with implementation of a multisite quality improvement collaborative including non‐pharmacological care and breastfeeding policy development (21 days to 19 days).
Length of pharmacological treatment: Wachman 2018 reported reduced mean length of pharmacological treatment over time with implementation of new interventions including multiple non‐pharmacological care practices (16.2 days to 12.7 days). Kirchner 2014 noted differing length of pharmacological treatment at different enrollment sites in the MOTHER NAS study with the longest treatment duration in urban USA. Patrick 2016 reported reduced median length of pharmacological treatment over time with implementation of a multisite quality improvement collaborative including non‐pharmacological care and breastfeeding policy development (16 days to 15 days).
Cumulative dose of opioid medication: Holmes 2016 reported lower mean cumulative dose of opioid over time with implementation of new interventions including multiple non‐pharmacological care practices (13.7 mg to 6.6 mg). Kirchner 2014 noted differing mean cumulative opioid doses at different enrollment sites in the MOTHER NAS study (total dose of morphine within the first 28 postpartum days 5.38 mg in Europe rooming in model versus 35.05 mg in urban USA versus 8.66 mg in rural US).
Measured secondary outcomes
Peak NAS score in first 72 hours of life: no studies assessed peak NAS score in the first 72 hours of life as predefined in our protocol. Holmes 2016 noted "no significant difference in median score, maximum score, or first score by year" over time with implementation of new interventions including multiple non‐pharmacological care practices. Kirchner 2014 noted differing mean daily MOTHER neonatal abstinence scoring tool scores at different enrollment sites in the MOTHER NAS study (3.63 in Europe rooming in model versus 4.67 in urban USA versus 3.06 in rural USA).
NICU admission: three studies reported reduced NICU admission over time with implementation of new interventions including multiple non‐pharmacological care practices (Grossman 2017; Miles 2007; Wachman 2018). The outcome values and differences between groups varied by site including decreases from 100% to 20% (Grossman 2017), 100% to 40% (Miles 2007), and 23.7% to 21.2% (Wachman 2018). Loudin 2017 noted decreased NICU admission following the introduction of a Neonatal Transition Unit (100% to 20%).
Seizures: Miles 2007 reported reduced clinical convulsions without routine EEG confirmation over time with implementation of new interventions including multiple non‐pharmacological care practices (27% to 6%). Wachman 2018 noted no seizures were reported over time with implementation of new interventions including multiple non‐pharmacological care practices.
Neurodevelopmental outcome at approximately two years' corrected age: no studies reported neurodevelopmental outcome as predefined in the protocol. Miles 2007 reported that no infants were noted to have "impairments of vision, hearing, growth, or development" in the first year of life in either group before or after implementation of new interventions including multiple non‐pharmacological care practices.
Custody at discharge: three studies reported custody status at discharge over time with implementation of new interventions including multiple non‐pharmacological care practices (Holmes 2016; Miles 2007; Wachman 2018). The outcome values and differences between groups and measurement approach varied by site including 93% to 90% in parent custody (Holmes 2016), 10% discharged to foster family in both time periods (Miles 2007), and 19.8% to 28.2% in Department of Children and Families (DCF) custody (Wachman 2018).
Cost of care: Grossman 2017 and Holmes 2016 reported cost of hospitalization per patient over time with implementation of new interventions including multiple non‐pharmacological care practices. The outcome values and differences between groups and measurement approach varied by site including a decrease from a mean of USD 44,824 to USD 10,289 (Grossman 2017), a mean of USD 19,737 to USD 8755 per treated infant and USD 11,000 to USD 5300 per at risk infant (Holmes 2016). Loudin 2017 noted decreased median cost per patient in different sites of care (NICU USD 90,601 versus neonatal therapeutic unit USD 68,750 versus offsite neonatal abstinence center USD 17,688)
Appendix 4. 'Risk of bias' tool
We used the standard methods of Cochrane and Cochrane Neonatal to assess the methodological quality of the trials. For each trial, we sought information regarding the method of randomization, blinding, and reporting of all outcomes of all the infants enrolled in the trial. We assessed each criterion as being at a low, high, or unclear risk of bias. Two review authors separately assessed each study. We resolved any disagreements by discussion. We added this information to the 'Characteristics of included studies' table. We evaluated the following issues and entered the findings into the 'Risk of bias' table.
1. Sequence generation (checking for possible selection bias). Was the allocation sequence adequately generated?
For each included study, we categorized the method used to generate the allocation sequence as:
low risk (any truly random process, e.g. random number table; computer random number generator);
high risk (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number); or
unclear risk.
2. Allocation concealment (checking for possible selection bias). Was allocation adequately concealed?
For each included study, we categorized the method used to conceal the allocation sequence as:
low risk (e.g. telephone or central randomization; consecutively numbered, sealed, opaque envelopes);
high risk (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth); or
unclear risk.
3. Blinding of participants and personnel (checking for possible performance bias). Was knowledge of the allocated intervention adequately prevented during the study?
For each included study, we categorized the methods used to blind study participants and personnel from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or class of outcomes. We categorized the methods as:
low risk, high risk, or unclear risk for participants; and
low risk, high risk, or unclear risk for personnel.
4. Blinding of outcome assessment (checking for possible detection bias). Was knowledge of the allocated intervention adequately prevented at the time of outcome assessment?
For each included study, we categorized the methods used to blind outcome assessment. We assessed blinding separately for different outcomes or class of outcomes. We categorized the methods as:
low risk for outcome assessors;
high risk for outcome assessors; or
unclear risk for outcome assessors.
5. Incomplete outcome data (checking for possible attrition bias through withdrawals, dropouts, protocol deviations). Were incomplete outcome data adequately addressed?
For each included study and for each outcome, we described the completeness of data including attrition and exclusions from the analysis. We noted whether attrition and exclusions were reported, the numbers included in the analysis at each stage (compared with the total randomized participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported or supplied by the trial authors, we reincluded missing data in the analyses. We categorized the methods as:
low risk (less than 20% missing data);
high risk (20% or greater missing data); or
unclear risk.
6. Selective reporting bias. Are reports of the study free of the suggestion of selective outcome reporting?
For each included study, we described how we investigated the possibility of selective outcome reporting bias and what we found. For studies in which study protocols were published in advance, we compared prespecified outcomes versus outcomes eventually reported in the published results. If the study protocol was not published in advance, we contacted the study authors to gain access to the study protocol. We assessed the methods as:
low risk (where it was clear that all the study's prespecified outcomes and all expected outcomes of interest to the review had been reported);
high risk (where not all the study's prespecified outcomes had been reported; one or more reported primary outcomes were not prespecified outcomes of interest and were reported incompletely and so could not be used; the study failed to include results of a key outcome that would have been expected to have been reported); or
unclear risk.
7. Other sources of bias. Was the study apparently free of other problems that could put it at high risk of bias?
For each included study, we described any important concerns we had about other possible sources of bias (e.g. whether there was a potential source of bias related to the specific study design or whether the trial was stopped early due to some data‐dependent process). We assessed whether each study was free of other problems that could put it at risk of bias as:
low risk;
high risk; or
unclear risk.
If needed, we explored the impact of the level of bias by undertaking sensitivity analyses.
Data and analyses
Comparison 1. Infants at risk for, or having early symptoms consistent with, opioid withdrawal.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Length of hospitalization (days) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1.1 Modifying environmental stimulation | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | ‐1.00 [‐2.82, 0.82] |
| 1.1.2 Feeding practices | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | Not estimable |
| 1.1.3 Support of the mother‐infant dyad | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | ‐8.90 [‐19.84, 2.04] |
| 1.2 Pharmacological treatment with ≥ 1 doses of opioid or sedative medication | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.2.1 Modifying environmental stimulation | 3 | 92 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.86, 1.16] |
| 1.2.2 Feeding practices | 1 | 49 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.63, 1.33] |
| 1.2.3 Support of the mother‐infant dyad | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.13, 1.90] |
| 1.3 Peak neonatal abstinence syndrome (NAS) score in first 72 hours of life | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.1 Modifying environmental stimulation | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.2 Feeding practices | 0 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.3 Support of the mother‐infant dyad | 0 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.4 Neonatal intensive care unit admission | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.13, 1.90] |
| 1.4.1 Modifying environmental stimulation | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.4.2 Feeding practices | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.4.3 Support of the mother‐infant dyad | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.13, 1.90] |
| 1.5 Days to regain birth weight | 1 | 46 | Mean Difference (IV, Fixed, 95% CI) | ‐1.10 [‐2.76, 0.56] |
| 1.5.1 Modifying environmental stimulation | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | Not estimable |
| 1.5.2 Feeding practices | 1 | 46 | Mean Difference (IV, Fixed, 95% CI) | ‐1.10 [‐2.76, 0.56] |
| 1.5.3 Support of the mother‐infant dyad | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | Not estimable |
| 1.6 Weight nadir (% weight loss) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.6.1 Modifying environmental stimulation | 1 | 194 | Mean Difference (IV, Fixed, 95% CI) | ‐0.28 [‐1.15, 0.59] |
| 1.6.2 Feeding practices | 1 | 46 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐2.24, 0.64] |
| 1.6.3 Support of the mother‐infant dyad | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | Not estimable |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bogen 2018.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: yes Blinding of intervention: yes Complete follow‐up: yes Blinding of outcome: yes |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal as defined above (comparison 1) 49 infants with fetal methadone exposure, ≥ 35 weeks' gestation and 2200 g 26 infants (35%) did not meet enrollment criteria (15 to NICU > 24 hours other than NAS, 9 birth weight < 2200 g, 2 withdrawn by mother) Site of care: not specified (NICU > 24 hours for reasons other than NAS excluded) Location: Pennsylvania, USA Enrollment period: July 2010 to August 2012 |
|
| Interventions |
Category: feeding practices Intervention: 24 kcal/oz formula from 3 to 21 days of life (27 infants) Comparison: 20 kcal/oz formula from 3 to 21 days of life (22 infants) |
|
| Outcomes |
|
|
| Notes | Protocol deviation noted in both groups. Quote: "Ten infants stopped taking the study formula before day 21" [intervention 4 infants, comparison 6 infants] 18% of infants were lost to follow‐up before reaching birth weight or day 21 (intervention 6 infants, comparison 3 infants." Reported on treatment duration among treated infants (intervention 16 infants, comparison 18 infants) Emailed with authors to clarify data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Eligible infants were randomly assigned within strata defined by gestational age groups (35–36, 37–38, and ≥ 39 weeks), sex (male or female), and feeding method (any breast milk or all formula). Assignment sequences, generated in blocks of 6 for each stratum by using SPSS (IBM SPSS Statistics, IBM Corporation, Armonk, NY), were provided by the statistician directly to the pharmacist." |
| Allocation concealment (selection bias) | Low risk | Quote: "Eligible infants were randomly assigned within strata defined by gestational age groups (35–36, 37–38, and ≥ 39 weeks), sex (male or female), and feeding method (any breast milk or all formula). Assignment sequences, generated in blocks of 6 for each stratum by using SPSS (IBM SPSS Statistics, IBM Corporation, Armonk, NY), were provided by the statistician directly to the pharmacist." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Parents, nurses, pediatric providers, and study staff were blinded to formula assignment. Only the hospital pharmacist who prepared labels covering the original labels, the statistician, and the medical monitor had access to randomization lists before the study's completion." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Parents, nurses, pediatric providers, and study staff were blinded to formula assignment. Only the hospital pharmacist who prepared labels covering the original labels, the statistician, and the medical monitor had access to randomization lists before the study's completion." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 18% of infants were lost to follow‐up before reaching birth weight or day 21 (intervention 6 infants, comparison 3 infants). |
| Selective reporting (reporting bias) | High risk | Preregistration not reported in publication. Trial registered on ClinicalTrials.gov. Several prespecified outcomes not reported in publication (total length of hospital stay, mean Finnegan scores on days 2–10, maximum concentration of morphine used to treat NAS, and the suck quality at 4–6 days of age). |
| Other bias | High risk | Quote: "Ten infants stopped taking the study formula before day 21." This change would bias the intention‐to‐treat analysis to the null. 6 infants in high‐calorie group screened positive for a drug other than methadone at delivery compared to 0 in standard‐calorie group. Quote: "Of infants, ~35% (26 of 75; mostly infants enrolled during pregnancy) did not meet randomization criteria largely because of admission to the NICU for issues other than NAS and low birth weight." |
D'Apolito 1999.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: unclear Blinding of intervention: no Complete follow‐up: yes Blinding of outcome: no |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal (comparison 1) 14 full‐term infants who were prenatally exposed to methadone plus other illicit drugs (including ethanol, heroin, marijuana, and cigarettes; excluding cocaine in late pregnancy) No report of number of infants who did not meet enrollment criteria Site of care: "Nursery." Quote: "All infants in the study received routine nursery care that included: placement in a quiet room; use of a pacifier on demand; swaddling; monitoring routine vital signs; and feedings on a 3‐hour schedule. Parents were allowed to care for their infant when visiting." Location: USA Enrollment period: not specified |
|
| Interventions |
Category: modifying environmental stimulation Intervention: mechanical rocking bed with maternal intrauterine sounds from 24 hours of life to day 7 of life (7 infants) Comparison: standard bed from 24 hours of life to day 7 of life (7 infants) |
|
| Outcomes |
|
|
| Notes | More infants in the intervention group experienced complications at delivery than in the control group (intervention mean 1.1, SD 1.2 vs control mean 0, SD 0). Alcohol and nicotine coexposures not described. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not able to perform with intervention. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not able to perform with intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No exclusion or attrition reported. |
| Selective reporting (reporting bias) | Unclear risk | Not reported in publication, trial registration unlikely given year of publication and no trial registration identified. |
| Other bias | Unclear risk | No report of number of infants who did not meet enrollment criteria. |
MacVicar 2018.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: unclear Blinding of intervention: no Complete follow‐up: no Blinding of outcome: no |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal (comparison 1) 14 mother‐infant dyads. Quote: "Inclusion criteria included opioid substitution medication therapy during pregnancy, intention to breastfeed, > 36 weeks' gestation, and over 16 years of age. Exclusion criteria: HIV positive, ongoing illicit psychoactive drug or alcohol use, and a child removal order in force 39 (74%) infants did not meet enrollment criteria (34 did not meet inclusion criteria, 1 declined to participate, 4 other) Site of care: multioccupancy room with mother and baby for standard postnatal care, admitted to the neonatal unit for pharmacotherapy Location: single site at tertiary maternity hospital, Scotland, UK Enrollment period: April 2014 to May 2015 |
|
| Interventions |
Category: support of the mother‐infant dyad Intervention: in hospital, tailored breastfeeding support (dedicated breastfeeding support worker, personalized capacity‐building approach, and a low‐stimuli environment for 5 days) (7 infants) Comparison: Baby‐Friendly Initiative care only (7 infants) |
|
| Outcomes |
Feasibility outcome measures including:
|
|
| Notes | Post hoc analysis of feeding practices performed. Quote: "Collectively breastfed infants were less likely to require pharmacotherapy (3 of 11 breastfeeding vs 3 of 3 formula feeding). Breastfeeding infants were discharged from the hospital sooner than formula‐fed infants (10.8 and 30.0 days respectively)." |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants were randomly allocated to the intervention or control group using a computer‐generated randomization process." |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Allocation to group was not concealed after the randomization process as intervention participants were located in a specifically designated area." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Allocation to group was not concealed after the randomization process as intervention participants were located in a specifically designated area." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Infants transferred to a different unit for treatment with pharmacotherapy (intervention 2, control 4) did not receive full allocated intervention. Loss to follow‐up (intervention 2 infant, control intervention 1 infant) with limited completion of maternal questionnaire. |
| Selective reporting (reporting bias) | Unclear risk | Not reported in publication and no trial registration identified in this feasibility trial. |
| Other bias | High risk | Quote: "Intervention group contained more multiparous women with greater parity than the control group." More mothers in the intervention group had prior breastfeeding experience. Frequency of nicotine exposure not reported. 39 infants did not meet enrollment criteria, suggesting the study group may be a non‐representative population. |
Maichuk 1999.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: unclear Blinding of intervention: no Complete follow‐up: yes Blinding of outcome: no |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal (comparison 1) Quotes: "48 newborns of narcotic‐dependent women, successive admissions." "All subjects had urine toxicology findings that were positive for heroin and/or methadone." Comment: infants were eligible after 2 successive NASS scores ≥ 5. Quotes: "Neonates with sepsis, congenital anomalies, respiratory disease, metabolic disorder, gastroesophageal reflux, and intraventricular hemorrhage were excluded. Also excluded were infants who were small for gestational age and infants of breastfeeding mothers." "All 48 subjects' withdrawal symptoms reach treatment threshold levels (two successive Neonatal Abstinence Scoring System scores of ≥ 8), causing them to receive pharmacotherapy for symptom management." No report of number of infants who did not meet enrollment criteria Site of care: intermediate care nursery Location: New Jersey, USA Enrollment period: not specified |
|
| Interventions |
Category: modifying environmental stimulation Intervention: prone positioning (25 infants) Comparison: supine positioning (23 infants) |
|
| Outcomes |
|
|
| Notes | Frequency of coexposure to alcohol and tobacco was not discussed. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not discussed. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not able to perform with intervention. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessors aware of interventions implemented, but blind to study hypothesis. Quote. "Nurses carrying out withdrawal severity scoring and recording caloric intake and daily weight were blind to the study hypothesis." Quote: "In stipulating that withdrawal scoring be conducted by the nurses involved in an affected infant's care, the NASS introduces the possibility of observer bias." Quote: "Although nurse‐raters did not know the study hypothesis and measures were taken to reduce the likelihood of their discerning our outcome measures, the manifest novelty of the experimental manipulation may have influenced them in their assessments of subjects' withdrawal severity." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Breastfed infants were excluded. No attrition. |
| Selective reporting (reporting bias) | Unclear risk | Not reported in publication, trial registration unlikely given year of publication and no trial registration identified. |
| Other bias | Unclear risk | No report of number of infants who did not meet enrollment criteria. |
Oro 1988.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: unknown Blinding of intervention: no Complete follow‐up: no Blinding of outcome: no |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal (comparison 1) 49 narcotic‐exposed newborns, defined by a history of prenatal narcotic exposure and heroin or methadone (or both) on urine toxicology results Excluded infants with unconfirmed exposure; additional exposure to phencyclidine, barbiturate, or glutethimide; or conditions that could potentially confound the symptoms of withdrawal 49 randomized, but study selected 15 intervention neonates and matched 15 comparable control neonates for analysis based on type of drug exposure, methadone dose, ethnicity, gestational age, birth weight, medication, and initial abstinence score No report of number of infants who did not meet enrollment criteria Site of care: "nursery" Location: USA Enrollment period: not specified |
|
| Interventions |
Category: modifying environmental stimulation Intervention: non‐oscillating waterbeds (15 infants) Comparison: conventional bassinets (15 infants) |
|
| Outcomes |
|
|
| Notes | Infants included only if matched with a similar infant for comparison. Details and outcomes not reported for 19 non‐matched infants. 10 infants in the control group exhibited fetal distress compared to 4 in the intervention group. 4 infants in the control group exposed to alcohol compared to 2 in the intervention group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "Randomly assigned on the basis of hospital record numbers." |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "All newborns were cared for by a small group of attending physicians who were uninvolved with this study (with one exception) and followed standard care and medication protocols that remained constant throughout the study period." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Although not blinded to bed placement, the physicians were not involved in determining the nursing practice." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 49 randomized, 19 excluded due to inadequate matching. No attrition. |
| Selective reporting (reporting bias) | Unclear risk | Not reported in publication, trial registration unlikely given year of publication and no trial registration is identified. |
| Other bias | Unclear risk | No report of number of infants who did not meet enrollment criteria. |
Ostrea 1975.
| Study characteristics | ||
| Methods | Randomized clinical trial: yes Blinding of randomization: unclear Blinding of intervention: no Complete follow‐up: yes Blinding of outcome: no |
|
| Participants | Assessed infants at risk for, or having early symptoms consistent with, opioid withdrawal (comparison 1) 198 mother‐infant dyads delivered at a single hospital (131 mothers enrolled in methadone clinic, 57 mothers not in a clinic) Excluded any baby; quote: "likely to develop neonatal problems other than those clearly due to narcotic withdrawal;" "this group consisted primarily of the premature infants and those with complications during delivery." Quote: "in either nursery they would be treated if they had severe withdrawal, or one of the criteria, and in these 198 babies which we had, we only treated 11." No report of number of infants who did not meet enrollment criteria Site of care: "nursery" Location: MI, USA Enrollment period: December 1972 to December 1973 |
|
| Interventions |
Category: modifying environmental stimulation Intervention: study nursery; quote: "The study nursery was a secluded, quiet (maximum of 60–70 decibels) and dimly lighted room. The infants in the study nursery were bundled and placed in non‐motorized Armstrong incubators and fed every three hours. The infants (control) in the regular nursery were bundled in open bassinets and exposed to the usual nursery noise and illumination and were fed every four hours." (101 infants) Comparison: regular nursery (97 infants) |
|
| Outcomes | Quote: "The frequency of central nervous system, vasomotor and gastrointestinal manifestations were essentially the same in both groups. The incidence of mild, moderate, or severe withdrawal was not significantly different in the control vs study group (chi squared = 0.99; p < 0.50). The withdrawal rating, obtained by assigning a score of 1 to mild, 2 to moderate, and 3 to severe, and then getting their mean were the same in both groups. Despite more frequent feedings in the experimental group, the weight loss was essentially identical in both groups. The bilirubin values were also identical, despite the curtailment of light in the experimental group." | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not able to perform with intervention. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not able to perform with intervention. Severity of NAS assessed by a study specific score with a single assessor for all infants. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition or exclusions. |
| Selective reporting (reporting bias) | Unclear risk | Not reported in publication, trial registration unlikely given year of publication and no trial registration is identified. |
| Other bias | Unclear risk | No report of number of infants who did not meet enrollment criteria. |
NAS: neonatal abstinence syndrome; NASS: Neonatal Abstinence Scoring System; NICU: neonatal intensive care unit; SD: standard deviation.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abdel‐Latif 2006 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Abrahams 2007 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Abrahams 2010 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Arlettaz 2005 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Crook 2017 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Dryden 2009 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Grossman 2017 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| Hodgson 2012 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Holmes 2016 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| Howard 2017 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Hünseler 2013 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Isemann 2011 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Jansson 2008 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Kirchner 2014 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| Liu 2015 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Loudin 2017 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| McKnight 2016 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| McQueen 2011 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Metz 2011 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Metz 2015 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Miles 2007 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| O'Connor 2013 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Ordean 2015 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Patrick 2016 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| Pritham 2012 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Radmacher 2017 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Radziewicz 2018 | Study design. Details in 'Excluded studies of modifying environmental stimulation' (Table 2). |
| Saiki 2010 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Short 2016 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Summey 2018 | Study design. Details in 'Excluded studies of support of the mother‐infant dyad' (Table 4). |
| Wachman 2013 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Wachman 2018 | Study design. Details in 'Excluded studies of multiple non‐pharmacological care practices' (Table 5). |
| Welle‐Strand 2013 | Study design. Details in 'Excluded studies of feeding practices' (Table 3). |
| Zuzarte 2017 | Study design. Details in 'Excluded studies of modifying environmental stimulation' (Table 2). |
Characteristics of ongoing studies [ordered by study ID]
NCT02768844.
| Study name | Physiology and therapeutic management of neonatal abstinence syndrome |
| Methods | Interventional (clinical trial), single group assignment, prospective within‐subject design, no masking |
| Participants | Estimated enrollment: 40 participants Inclusion criteria: full‐term infants, at risk for NAS due to fetal drug exposure, confirmed meconium or urine toxicology report for opioids (or both) (may also have exposure to benzodiazepines, barbiturates, amphetamines, cannabinoids, alcohol, nicotine, caffeine, or a combination of these) |
| Interventions | SVS |
| Outcomes | Change in:
|
| Starting date | April 2011 |
| Contact information | Principal investigator: Elisabeth B Salisbury, PhD, University of Massachusetts, Worcester |
| Notes |
NCT02801331.
| Study name | A randomized controlled study of stochastic vibrotactile stimulation for neonatal abstinence syndrome: therapeutic efficacy and neurobehavioral outcomes |
| Methods | Interventional (clinical trial), randomized, parallel assignment, single masking (outcomes assessor) |
| Participants | Estimated enrollment: 230 participants Inclusion criteria: full‐term infants, at risk for NAS due to opioid exposure in utero, confirmed meconium or urine toxicology report or documented medical record for opioids (or a combination of these) (may also have exposure to benzodiazepines, barbiturates, amphetamines, cannabinoids, alcohol, nicotine, caffeine, or a combination of these) |
| Interventions | SVS |
| Outcomes |
|
| Starting date | 9 March 2017 |
| Contact information | Principal investigator: Elisabeth B Salisbury, PhD, University of Massachusetts, Worcester |
| Notes |
NCT03097484.
| Study name | The effect of aromatherapy on neonatal abstinence syndrome and salivary cortisol levels |
| Methods | Interventional (clinical trial), randomized, parallel assignment, no masking |
| Participants | Actual enrollment: 38 participants Inclusion criteria: ≥ 36 weeks' estimated gestational age, intrauterine opioid exposure, primary diagnosis of NAS, parental permission to participate |
| Interventions | Lavender and chamomile essential oils |
| Outcomes |
|
| Starting date | 25 July 2015 |
| Contact information | John M Daniel, Fellow, Department of Pediatrics, Division of Neonatology, University of Kentucky |
| Notes |
NCT03113656.
| Study name | The use of weighted blankets in the care of infants with neonatal abstinence syndrome (NAS) |
| Methods | Interventional (clinical trial), randomized, crossover assignment, no masking |
| Participants | Actual enrollment: 16 participants Inclusion criteria: admitted to the NICU, gestational age > 37 weeks, positive maternal drug screen at delivery |
| Interventions | Weighted blanket first compared to non‐weighted blanket first |
| Outcomes |
|
| Starting date | 14 July 2017 |
| Contact information | Rachel Baker, Nurse Researcher, TriHealth Inc., Cincinnati |
| Notes |
NCT03533985.
| Study name | Effect of music therapy on neonates diagnosed with neonatal abstinence syndrome: a pilot study |
| Methods | Interventional (clinical trial), randomized, crossover assignment, double masking (participant, outcomes assessor) |
| Participants | Estimated enrollment: 200 participants Inclusion criteria: admitted to the NICU immediately postpartum, gestational age ≥ 28 weeks, no identified hearing disorder, no diagnosed developmental disability, no fetal alcohol syndrome, medically cleared to participate in the study, and parent or legal guardian able/willing to give consent and complete survey |
| Interventions | 6 different music therapy interventions |
| Outcomes |
|
| Starting date | 1 November 2017 |
| Contact information | Principal investigators: Joanne Loewy, PhD, Icahn School of Medicine at Mount Sinai, New York and Kathy Murphy, PhD, Loyola University, Chicago |
| Notes |
NCT03549936.
| Study name | Role of low lactose infant formula in the management of neonatal abstinence syndrome |
| Methods | Interventional (clinical trial), randomized, parallel assignment, quadruple masking (participant, care provider, investigator, outcomes assessor) |
| Participants | Actual enrollment: 74 participants Inclusion criteria: intrauterine exposure to opiate and related drugs, late preterm or full term (36–42 weeks' gestation) |
| Interventions | Low‐lactose formula |
| Outcomes |
|
| Starting date | 9 July 2014 |
| Contact information | Dr Deepak Kumar, Neonatologist, MetroHealth Medical Center, Cleveland |
| Notes |
NCT03987165.
| Study name | The effect of music therapy on newborns |
| Methods | Interventional (clinical trial), randomized, crossover assignment, no masking |
| Participants | Estimated enrollment: 300 participants. Summary states target population is infants with neonatal opioid withdrawal syndrome Inclusion criteria: admitted to NICU or newborn nursery, gestational age ≥ 28 weeks, no identified hearing disorder, no developmental disability, no fetal alcohol syndrome, medically cleared to participate in the study, and parent or legal guardian able/willing to give consent and complete surveys |
| Interventions | Experimental music therapy by a certified music therapist |
| Outcomes |
|
| Starting date | 10 December 2018 |
| Contact information | Meghan Howell, Assistant Professor, Tulane Hospital, New Orleans |
| Notes |
NAS: neonatal abstinence syndrome; NICU: neonatal intensive care unit; SVS: stochastic vibrotactile stimulation.
Differences between protocol and review
We made the following changes to the protocol (Pahl 2018).
As of July 2019, Cochrane Neonatal no longer searches Embase for its reviews. Randomized controlled trials (RCTs) and controlled clinical trials (CCTs) from Embase are added to the Cochrane Central Register of Controlled Trials (CENTRAL) via a robust process (see 'How CENTRAL is created'; www.cochranelibrary.com/central/central-creation). Cochrane Neonatal has validated their searches to ensure that relevant Embase records are found while searching CENTRAL.
As of July 2019, Cochrane Neonatal no longer searches for RCTs and CCTs on the following platforms: ClinicalTrials.gov or from The World Health Organization's International Clinical Trials Registry Platform (ICTRP; apps.who.int/trialsearch/), as records from both platforms are added to CENTRAL on a monthly basis (see 'How CENTRAL is created'; /www.cochranelibrary.com/central/central-creation). Comprehensive search strategies are executed in CENTRAL to retrieve relevant records. The ISRCTN (www.isrctn.com/, formerly Controlled‐trials.com), is searched separately.
In 2019, we developed a new search strategy, which we ran without date limits (Appendix 1).
We changed the order of the primary outcomes for ease of reading and comparison throughout the text. We did not alter the primary outcomes. We changed the population description from symptoms 'of' opioid withdrawal to symptoms 'consistent with' opioid withdrawal. We changed a primary outcome term from 'need for' pharmacological treatment to 'use of' pharmacological treatment.
We added a post hoc secondary outcome to include 'Cost of care' and adjusted the secondary outcome, 'Peak NAS score in the first 72 hours of life' to more broadly include the 'Peak NAS score at any time or in the first 72 hours of life.'
Few studies were identified for each intervention and sensitivity analysis was not performed.
We did not attempt to perform the subgroup analyses proposed above due to insufficient similarity in population, intervention, and comparison groups studied.
We chose to exclude all non‐randomized studies. We presented comparative non‐randomized studies such as cohort studies, case‐controlled studies, and cross‐sectional studies in narrative fashion and excluded without presenting non‐comparative non‐randomized studies such as case series or case reports. We elected not to apply a formal ROBINS‐I or GRADE analysis to non‐randomized studies since a formal meta‐analysis was not planned. The biases discussed in the ROBINS‐I tool informed the discussion of non‐randomized studies in the text (sites.google.com/site/riskofbiastool//welcome/home) (Sterne 2016).
Contributions of authors
AP and RS drafted the protocol, reviewed abstracts and full‐text articles, selected studies for inclusion, assessed risk of bias and GRADE, and drafted the manuscript.
LY, LM, and MEBF provided expert review and comment.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Vermont Oxford Network, USA
Cochrane Neonatal Reviews are produced with support from the Vermont Oxford Network, a worldwide collaboration of health professionals dedicated to providing evidence‐based care of the highest quality for newborn infants and their families.
-
National Institute for Health Research, UK
Editorial support for Cochrane Neonatal has been funded by a UK National Institute of Health Research (NIHR) Cochrane Programme Grant (16/114/03). The views expressed in this publication are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR, or the UK Department of Health.
Declarations of interest
AP: none.
LY: none.
MEBF: none.
LM has worked with Vermont Oxford Network since 2012 and received payments for lectures.
RS is the Co‐ordinating Editor of Cochrane Neonatal, President and Director of Clinical Trials of the Vermont Oxford Network, and a professor at the University of Vermont. Previously he has acted as a consultant and invited speaker for several of the pharmaceutical companies that manufacture surfactant preparations (Abbott Laboratories, Ross Laboratories, Chiesi Pharmaceuticals, Dey Laboratories, Burroughs Wellcome). He has done no paid consulting work since 2010.
New
References
References to studies included in this review
Bogen 2018 {published data only}
- Bogen DL, Hanusa BH, Baker R, Medoff-Cooper B, Cohlan B. Randomized clinical trial of standard- versus high-calorie formula for methadone-exposed infants: a feasibility study. Hospital Pediatrics 2018;8(1):7-14. [DOI: 10.1542/hpeds.2017-0114] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
D'Apolito 1999 {published data only}
- D'Apolito K. Comparison of a rocking bed and standard bed for decreasing withdrawal symptoms in drug-exposed infants. MCN. The American Journal of Maternal Child Nursing 1999;24(3):138-44. [DOI: 10.1097/00005721-199905000-00007] [PMID: ] [DOI] [PubMed] [Google Scholar]
MacVicar 2018 {published data only}
- MacVicar S, Humphrey T, Forbes-McKay KE. Breastfeeding and the substance-exposed mother and baby. Birth 2018;45(4):450-8. [DOI: 10.1111/birt.12338] [PMID: ] [DOI] [PubMed] [Google Scholar]
Maichuk 1999 {published data only}
- Maichuk GT, Zahorodny W, Marshall R. Use of positioning to reduce the severity of neonatal narcotic withdrawal syndrome. Journal of Perinatology 1999;19(7):510-3. [DOI: 10.1038/sj.jp.7200260] [PMID: ] [DOI] [PubMed] [Google Scholar]
Oro 1988 {published data only}
- Oro AS, Dixon SD. Waterbed care of narcotic-exposed neonates. A useful adjunct to supportive care. American Journal of Diseases of Children 1988;142(2):186-8. [DOI: 10.1001/archpedi.1988.02150020088036] [PMID: ] [DOI] [PubMed] [Google Scholar]
Ostrea 1975 {published data only}
- Ostrea EM, Chavez CJ, Strauss ME. A study of factors that influence the severity of neonatal narcotic withdrawal. Addictive Diseases 1975;2(1-2):187-99. [PMID: ] [PubMed] [Google Scholar]
References to studies excluded from this review
Abdel‐Latif 2006 {published data only}
- Abdel-Latif ME, Pinner J, Clews S, Cooke F, Lui K, Oei J. Effects of breast milk on the severity and outcome of neonatal abstinence syndrome among infants of drug-dependent mothers. Pediatrics 2006;117(6):e1163-9. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Abrahams 2007 {published data only}
- Abrahams RR, Kelly SA, Payne S, Thiessen PN, Mackintosh J, Janssen PA. Rooming-in compared with standard care for newborns of mothers using methadone or heroin. Canadian Family Physician Médecin de Famille Canadien 2007;53(10):1722-30. [DOI: 53/10/1722 [pii]] [PMID: ] [PMC free article] [PubMed] [Google Scholar]
Abrahams 2010 {published data only}
- Abrahams RR, Mackay-Dunn MH, Nevmerjitskaia V, Macrae GS, Payne SP, Hodgson ZG. An evaluation of rooming-in among substance-exposed newborns in British Columbia. Journal d'Obstetrique et Gynecologie du Canada : JOGC [Journal of Obstetrics and Gynaecology Canada : JOGC] 2010;32(9):866-71. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Arlettaz 2005 {published data only}
- Arlettaz R, Kashiwagi M, Das-Kundu S, Fauchère JC, Lang A, Bucher HU. Methadone maintenance program in pregnancy in a Swiss perinatal center (II): neonatal outcome and social resources. Acta Obstetricia et Gynecologica Scandinavica 2005;84(2):145-50. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Crook 2017 {published data only}
- Crook K, Brandon D. Prenatal breastfeeding education: impact on infants with neonatal abstinence syndrome. Advances in Neonatal Care 2017;17(4):299-305. [DOI: 10.1097/ANC.0000000000000392] [PMID: ] [DOI] [PubMed] [Google Scholar]
Dryden 2009 {published data only}
- Dryden C, Young D, Campbell N, Mactier H. Postnatal weight loss in substitute methadone-exposed infants: implications for the management of breast feeding. Archives of Disease in Childhood. Fetal and Neonatal Edition 2012;97(3):F214-6. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Dryden C, Young D, Hepburn M, Mactier H. Maternal methadone use in pregnancy: factors associated with the development of neonatal abstinence syndrome and implications for healthcare resources. BJOG 2009;116(5):665-71. [DOI: 10.1111/j.1471-0528.2008.02073.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
Grossman 2017 {published data only}
- Grossman MR, Berkwitt AK, Osborn RR, Xu Y, Esserman D, Shapiro E, et al. An initiative to improve the quality of care of infants with neonatal abstinence syndrome. Pediatrics 2017;139(6):e20163360. [DOI: 10.1542/peds.2016-3360] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hodgson 2012 {published data only}
- Hodgson ZG, Abrahams RR. A rooming-in program to mitigate the need to treat for opiate withdrawal in the newborn. Journal d'Obstetrique et Gynecologie du Canada : JOGC [Journal of Obstetrics and Gynaecology Canada : JOGC] 2012;34(5):475-81. [DOI: 10.1016/s1701-2163(16)35245-8] [PMID: ] [DOI] [PubMed] [Google Scholar]
Holmes 2016 {published data only}
- Holmes AV, Atwood EC, Whalen B, Beliveau J, Jarvis JD, Matulis JC, et al. Rooming-in to treat neonatal abstinence syndrome: improved family-centered care at lower cost. Pediatrics 2016;137(6):e1-e9. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Howard 2017 {published data only}
- Howard MB, Schiff DM, Penwill N, Si W, Rai A, Wolfgang T, et al. Impact of parental presence at infants' bedside on neonatal abstinence syndrome. Hospital Pediatrics 2017;7(2):62-9. [DOI: 10.1542/hpeds.2016-0147] [PMID: ] [DOI] [PubMed] [Google Scholar]
Hünseler 2013 {published data only}
- Hünseler C, Brückle M, Roth B, Kribs A. Neonatal opiate withdrawal and rooming-in: a retrospective analysis of a single center experience [Neonataler opiatentzug und rooming-in: retrospektive analyse der erfahrungen eines zentrums]. Klinische Pädiatrie 2013;225(5):247-51. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Isemann 2011 {published data only}
- Isemann B, Meinzen-Derr J, Akinbi H. Maternal and neonatal factors impacting response to methadone therapy in infants treated for neonatal abstinence syndrome. Journal of Perinatology 2011;31(1):25-9. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Jansson 2008 {published data only}
- Jansson LM, Choo R, Velez ML, Harrow C, Schroeder JR, Shakleya DM, et al. Methadone maintenance and breastfeeding in the neonatal period. Pediatrics 2008;121(1):106-14. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Kirchner 2014 {published data only}
- Kirchner L, Graf-Rohrmeister K, Klebermass-Schrehof K, Weninger M, Jagsch R, Metz V, et al. Neonatal abstinence syndrome in European and North American neonates: differences in clinical characteristics derived from a prospective randomized trial [Neonatales Abstinenzsyndrom bei europäischen und nordamerikani-schen Neugeborenen: Unterschiede im klinischen Verlauf an Hand vonDaten einer prospektiven randomisierten Studie]. Klinische Padiatrie 2014;226(5):274-80. [DOI: 10.1055/s-0034-1372586] [PMID: ] [DOI] [PubMed] [Google Scholar]
Liu 2015 {published data only}
- Liu A, Juarez J, Nair A, Nanan R. Feeding modalities and the onset of the neonatal abstinence syndrome. Frontiers in Pediatrics 2015;3:14. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Loudin 2017 {published data only}
- Loudin S, Werthammer J, Prunty L, Murray S, Shapiro JI, Davies TH. A management strategy that reduces NICU admissions and decreases charges from the front line of the neonatal abstinence syndrome epidemic. Journal of Perinatology 2017;37(10):1108-11. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
McKnight 2016 {published data only}
- McKnight S, Coo H, Davies G, Holmes B, Newman A, Newton L, et al. Rooming-in for infants at risk of neonatal abstinence syndrome. American Journal of Perinatology 2016;33(5):495-501. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Newman A, Davies GA, Dow K, Holmes B, Macdonald J, McKnight S, et al. Rooming-in care for infants of opioid-dependent mothers: Implementation and evaluation at a tertiary care hospital. Canadian Family Physician Medecin de Famille Canadien 2015;61(12):e555-61. [PMID: ] [PMC free article] [PubMed] [Google Scholar]
McQueen 2011 {published data only}
- McQueen KA, Murphy-Oikonen J, Gerlach K, Montelpare W. The impact of infant feeding method on neonatal abstinence scores of methadone-exposed infants. Advances in Neonatal Care 2011;11(4):282-90. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Metz 2011 {published data only}
- Metz V, Jagsch R, Ebner N, Wurzl J, Pribasnig A, Aschauer C, et al. Impact of treatment approach on maternal and neonatal outcome in pregnant opioid-maintained women. Human Psychopharmacology 2011;26(6):412-21. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Metz 2015 {published data only}
- Metz VE, Comer SD, Pribasnig A, Wuerzl J, Fischer G. Observational study in an outpatient clinic specializing in treating opioid dependent pregnant women: neonatal abstinence syndrome in infants exposed to methadone-, buprenorphine- and slow-release oral morphine. Heroin Addiction and Related Clinical Problems 2015;17(1):5-16. [Google Scholar]
Miles 2007 {published data only}
- Miles J, Sugumar K, Macrory F, Sims DG, D'Souza SW. Methadone-exposed newborn infants: outcome after alterations to a service for mothers and infants. Child Care Health and Development 2007;33(2):206-12. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
O'Connor 2013 {published data only}
- O'Connor AB, Collett A, Alto WA, O'Brien LM. Breastfeeding rates and the relationship between breastfeeding and neonatal abstinence syndrome in women maintained on buprenorphine during pregnancy. Journal of Midwifery and Women's Health 2013;58(4):383-8. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Ordean 2015 {published data only}
- Ordean A, Kahan M, Graves L, Abrahams R, Kim T. Obstetrical and neonatal outcomes of methadone-maintained pregnant women: a Canadian multisite cohort study. Journal d'Obstetrique et Gynecologie du Canada : JOGC [Journal of Obstetrics and Gynaecology Canada : JOGC] 2015;37(3):252-7. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Patrick 2016 {published data only}
- Patrick SW, Schumacher RE, Horbar JD, Buus-Frank M, Edwards E, Morrow K, et al. Improving care for neonatal abstinence syndrome. Pediatrics 2016;137(5):e20153835. [DOI: 10.1542/peds.2015-3835] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pritham 2012 {published data only}
- Pritham UA, Paul JA, Hayes MJ. Opioid dependency in pregnancy and length of stay for neonatal abstinence syndrome. Journal of Obstetric, Gynecologic, and Neonatal Nursing 2012;41(2):180-90. [DOI: 10.1111/j.1552-6909.2011.01330.x] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Radmacher 2017 {published data only}
- Radmacher P, Alexander C, Devlin L. Donor human milk may decrease severe gastrointestinal distress in infants with neonatal abstinence syndrome. Journal of Pregnancy and Neonatal Medicine 2017;1(1):11-5. [DOI: 10.35841/neonatal-medicine.1.1.11-15] [DOI] [Google Scholar]
Radziewicz 2018 {published data only}
- Radziewicz RM, Wright-Esber S, Zupancic J, Gargiulo D, Woodall P. Safety of reiki therapy for newborns at risk for neonatal abstinence syndrome. Holistic Nursing Practice 2018;32(2):63-70. [DOI: 10.1097/HNP.0000000000000251] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Saiki 2010 {published data only}
- Saiki T, Lee S, Hannam S, Greenough A. Neonatal abstinence syndrome-postnatal ward versus neonatal unit management. European Journal of Pediatrics 2010;169(1):95-8. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Short 2016 {published data only}
- Short VL, Gannon M, Abatemarco DJ. The association between breastfeeding and length of hospital stay among infants diagnosed with neonatal abstinence syndrome: a population-based study of in-hospital births. Breastfeeding Medicine 2016;11(7):343-9. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Summey 2018 {published data only}
- Summey J, Chen L, Mayo R, Charron E, Hudson JA, Sherrill WW, et al. Early treatment innovation for opioid-dependent newborns: a retrospective comparison of outcomes, utilization, quality, and safety, 2006–2014. Joint Commission Journal on Quality and Patient Safety / Joint Commission Resources 2018;44(6):312-20. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Wachman 2013 {published data only}
- Wachman EM, Hayes MJ, Brown MS, Paul J, Harvey-Wilkes K, Terrin N, et al. Association of OPRM1 and COMT single-nucleotide polymorphisms with hospital length of stay and treatment of neonatal abstinence syndrome. JAMA 2013;309(17):1821-7. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wachman 2018 {published data only}
- Wachman EM, Grossman M, Schiff DM, Philipp B, Minear S, Hutton E, et al. Quality improvement initiative to improve inpatient outcomes for neonatal abstinence syndrome. Journal of Perinatology 2018;38(8):1114-22. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Welle‐Strand 2013 {published data only}
- Welle-Strand GK, Skurtveit S, Jansson LM, Bakstad B, Bjarko L, Ravndal E. Breastfeeding reduces the need for withdrawal treatment in opioid-exposed infants. Acta Paediatrica 2013;102(11):1060-6. [DOI: ] [PMID: 23909865] [DOI] [PubMed] [Google Scholar]
Zuzarte 2017 {published data only}
- Zuzarte I, Indic P, Barton B, Paydarfar D, Bednarek F, Bloch-Salisbury E. Vibrotactile stimulation: a nonpharmacological intervention for opioid exposed newborns. PloS One 2017;12(4):e0175981. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to ongoing studies
NCT02768844 {published data only}
- NCT02768844. Physiology and therapeutic management of neonatal abstinence syndrome. clinicaltrials.gov/show/NCT02768844 (first received 11 May 2016).
NCT02801331 {published data only}
- NCT02801331. Efficacy and outcomes of a non-pharmacological intervention for neonatal abstinence syndrome. clinicaltrials.gov/show/NCT02801331 (first received 15 June 2016).
NCT03097484 {published data only}
- NCT03097484. The effect of aromatherapy on neonatal abstinence syndrome and salivary cortisol levels. clinicaltrials.gov/show/NCT03097484 (first received 31 March 2017).
NCT03113656 {published data only}
- NCT03113656. Weighted blankets with infants with NAS. clinicaltrials.gov/show/NCT03113656 (first received 13 April 2017).
NCT03533985 {published data only}
- NCT03533985. Effect of music therapy on Infants with Neonatal Abstinence Syndrome. clinicaltrials.gov/show/NCT03533985 (first received 23 May 2018).
NCT03549936 {published data only}
- NCT03549936. Role of low lactose infant formula in the management of neonatal abstinence syndrome. clinicaltrials.gov/show/NCT03549936 (first received 8 June 2018).
NCT03987165 {published data only}
- NCT03987165. The effect of music therapy on newborns. clinicaltrials.gov/show/NCT03987165 (first received 14 June 2019).
Additional references
Arditi 2006
- Arditi H, Feldman R, Eidelman A. Effects of human contact and vagal regulation on pain reactivity and visual attention in newborns. Developmental Psychobiology 2006;48(7):561-73. [DOI: 10.1002/dev.20150] [PMID: ] [DOI] [PubMed] [Google Scholar]
Bayley 1993
- Bayley N. Bayley Scales of Infant Development-II. San Antonio (TX): Psychological Corporation, 1993. [Google Scholar]
Bembich 2018
- Bembich S, Cont G, Causin E, Paviotti G, Marzari P, Demarini S. Infant analgesia with a combination of breast milk, glucose, or maternal holding. Pediatrics 2018;142(3):e20173416. [DOI: 10.1542/peds.2017-3416] [PMID: ] [DOI] [PubMed] [Google Scholar]
Bogen 2017
- Bogen D, Whalen B, Kair L, Vining M, King B. Wide variation found in care of opioid-exposed newborns. Academic Pediatrics 2017;17(4):374-80. [DOI: 10.1016/j.acap.2016.10.003] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bogen 2019
- Bogen DL, Whalen BL. Breastmilk feeding for mothers and infants with opioid exposure: What is best? Seminars in Fetal & Neonatal Medicine 2019;24(2):95-104. [DOI: 10.1016/j.siny.2019.01.001] [DOI] [PubMed] [Google Scholar]
Brockington 2006
- Brockington I, Fraser C, Wilson D. The Postpartum Bonding Questionnaire: a validation. Archives of Women's Mental Health 2006;9(5):233-42. [DOI: 10.1007/s00737-006-0132-1] [PMID: ] [DOI] [PubMed] [Google Scholar]
Brogly 2014
- Brogly S, Saia K, Walley A, Du H, Sebastiani P. Prenatal buprenorphine versus methadone exposure and neonatal outcomes: systematic review and meta-analysis. American Journal of Epidemiology 2014;180(7):673-86. [DOI: 10.1093/aje/kwu190] [PMID: ] [DOI] [PubMed] [Google Scholar]
Burns 2007
- Burns L, Mattick RP. Using population data to examine the prevalence and correlates of neonatal abstinence syndrome. Drug and Alcohol Review 2007;26(5):487-92. [DOI: 10.1080/09595230701494416] [PMID: ] [DOI] [PubMed] [Google Scholar]
Carbajal 2003
- Carbajal R, Veerapen S, Couderc S, Jugie M, Ville Y. Analgesic effect of breast feeding in term neonates: randomised controlled trial. BMJ (Clinical Research Ed.) 2003;326(7379):13. [DOI: 10.1136/bmj.326.7379.13] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chaudhary 2013
- Chaudhary T, Walch E, Herold B, Metze B, Lejeune A, Burkhardt F, et al. Predictive and concurrent validity of standardized neurodevelopmental examinations by the Griffiths scales and Bayley Scales of Infant Development II. Klinische Padiatrie 2013;225(1):8-12. [DOI: 10.1055/s-0032-1331169] [PMID: ] [DOI] [PubMed] [Google Scholar]
Chen 2017
- Chen K, Lindrea K, Quah-Smith I, Daly M, Schindler T, Oei J. Magnetic noninvasive acupuncture for infant comfort (MAGNIFIC) – a single-blinded randomised controlled pilot trial. Acta Paediatrica 2017;106(11):1780-6. [DOI: 10.1111/apa.14002] [PMID: ] [DOI] [PubMed] [Google Scholar]
CIHI 2018
- Canadian Institute for Health Information. Opioid-related harms in Canada, 2018. cihi.ca/sites/default/files/document/opioid-related-harms-report-2018-en-web.pdf (assessed prior to 1 December 2020).
Condon 1998
- Condon J, Corkindale CJ. The assessment of parent-to-infant attachment: development of a self-report questionnaire instrument. Journal of Reproductive and Infant Psychology 1998;16(1):57-76. [DOI: 10.1080/02646839808404558] [DOI] [Google Scholar]
Corr 2017
- Corr T, Hollenbeak C. The economic burden of neonatal abstinence syndrome in the United States. Addiction 2017;112(9):1590-9. [DOI: 10.1111/add.13842] [PMID: ] [DOI] [PubMed] [Google Scholar]
Cox 1987
- Cox J, Holden J, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry 1987;150(6):782-6. [DOI: 10.1192/bjp.150.6.782] [PMID: ] [DOI] [PubMed] [Google Scholar]
Davies 2016
- Davies H, Gilbert R, Johnson K, Petersen I, Nazareth I, O'Donnell M, et al. Neonatal drug withdrawal syndrome: cross-country comparison using hospital administrative data in England, the USA, Western Australia, and Ontario, Canada. Archives of Disease in Childhood. Fetal and Neonatal Edition 2016;101(1):F26-30. [DOI: 10.1136/archdischild-2015-308948] [PMID: ] [DOI] [PubMed] [Google Scholar]
Devlin 2020
- Devlin L, Breeze J, Terrin N, Gomez Pomar E, Bada H, Finnegan LP, et al. Association of a simplified Finnegan Neonatal Abstinence Scoring Tool with the need for pharmacologic treatment for neonatal abstinence syndrome. JAMA Network Open 2020;3(4):e202275. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Faherty 2019
- Faherty L, Kranz A, Russell-Fritch J, Patrick S, Cantor J, Stein B. Association of punitive and reporting state policies related to substance use in pregnancy with rates of neonatal abstinence syndrome. JAMA Network Open 2019;2(11):e1914078. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fenton 2017
- Fenton TR, Chan HT, Madhu A, Griffin IJ, Hoyos A, Ziegler EE, et al. Preterm infant growth velocity calculations: a systematic review. Pediatrics 2017;139(3):e20162045. [DOI: 10.1542/peds.2016-2045] [PMID: ] [DOI] [PubMed] [Google Scholar]
Finnegan 1975
- Finnegan LP, Connaughton JF Jr, Kron RE, Emich JP. Neonatal abstinence syndrome: assessment and management. Addictive Diseases 1975;2(1-2):141-58. [PMID: ] [PubMed] [Google Scholar]
Gomez Pomar 2017
- Gomez Pomar E, Finnegan LP, Devlin L, Bada H, Concina VA, Ibonia KT, et al. Simplification of the Finnegan Neonatal Abstinence Scoring System: retrospective study of two institutions in the USA. BMJ Open 2017;7(9):e016176. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Goyal 2020
- Goyal S, Saunders KC, Moore CS, Fillo K, Ko J, Manning S, et al. Identification of substance-exposed newborns and neonatal abstinence syndrome using ICD-10-CM – 15 Hospitals, Massachusetts, 2017. Morbidity and Mortality Weekly Report 2020;69(29):951-5. [DOI: 10.15585/mmwr.mm6929a2] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Version accessed 2 February 2018. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015. Available at gradepro.org.
Graham 2010
- Graham A, Ablow J, Measelle J. Interparental relationship dynamics and cardiac vagal functioning in infancy. Infant Behavior & Development 2010;33(4):530-44. [DOI: 10.1016/j.infbeh.2010.07.005] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gray 2000
- Gray L, Watt L Blass E. Skin-to-skin contact is analgesic in healthy newborns. Pediatrics 2000;105(1):e14. [DOI: 10.1542/peds.105.1.e14] [PMID: ] [DOI] [PubMed] [Google Scholar]
Gray 2002
- Gray L, Miller L, Philipp B, Blass E. Breastfeeding is analgesic in healthy newborns. Pediatrics 2002;109(4):590-3. [DOI: 10.1542/peds.109.4.590] [PMID: ] [DOI] [PubMed] [Google Scholar]
Green 1981
- Green M, Suffet F. The Neonatal Narcotic Withdrawal Index: a device for the improvement of care in the abstinence syndrome. American Journal of Drug and Alcohol Abuse 1981;8(2):203-13. [DOI: 10.3109/00952998108999125] [PMID: ] [DOI] [PubMed] [Google Scholar]
Grossman 2018
- Grossman M, Lipshaw M, Osborn R, Berkwitt A. A novel approach to assessing infants with neonatal abstinence syndrome. Hospital Pediatrics 2018;8(1):1-6. [DOI: 10.1542/hpeds.2017-0128] [PMID: ] [DOI] [PubMed] [Google Scholar]
Hall 2015
- Hall E, Wexelblatt S, Crowley M, Grow J, Jasin L, Klebanoff M, et al, OCHNAS Consortium. Implementation of a neonatal abstinence syndrome weaning protocol: a multicenter cohort study. Pediatrics 2015;136(4):e803. [DOI: 10.1542/peds.2015-1141] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
HCUP 2019
- Healthcare Cost and Utilization Project. HCUP Fast Stats, 2019. hcup-us.ahrq.gov/news/announcements/faststats092019update.jsp (accessed prior to 1 December 2020).
Higgins 2011
- Higgins JP, Altman DG, Sterne JA: on behalf of the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group. Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2019
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from www.training.cochrane.org/handbook. [DOI] [PMC free article] [PubMed]
Hudak 2012
- Hudak M, Tan R, Committee on Drugs, Committee on Fetus and Newborn, American Academy of Pediatrics. Neonatal drug withdrawal. Pediatrics 2012;129(2):e540-60. [DOI: 10.1542/peds.2011-3212] [PMID: ] [DOI] [PubMed] [Google Scholar]
Jansson 2009
- Academy of Breastfeeding Medicine Protocol Committee, Jansson LM. ABM clinical protocol #21: guidelines for breastfeeding and the drug-dependent woman. Breastfeeding Medicine 2009;4(4):225-8. [DOI: 10.1089/bfm.2009.9987] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Johnston 2017
- Johnston C, Campbell-Yeo M, Disher T, Benoit B, Fernandes A, Streiner D, et al. Skin-to-skin care for procedural pain in neonates. Cochrane Database of Systematic Reviews 2017, Issue 2. Art. No: CD008435. [DOI: 10.1002/14651858.CD008435.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jones 2010
- Jones HE, Kaltenback K, Heil SH, Stine S, Coyle M, Arria A, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. New England Journal of Medicine 2010;363(24):2320-31. [DOI: 10.1056/NEJMoa1005359] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jones 2016a
- Jones HE, Seashore C, Johnson E, Horton E, O'Grady KE, Andringa K. Measurement of neonatal abstinence syndrome: evaluation of short forms. Journal of Opioid Management 2016;12(1):19-23. [DOI: 10.5055/jom.2016.0308] [PMID: ] [DOI] [PubMed] [Google Scholar]
Jones 2016b
- Jones H, Seashore C, Johnson E, Horton E, O'Grady K, Andringa K, et al. Psychometric assessment of the Neonatal Abstinence Scoring System and the MOTHER NAS Scale. American Journal on Addictions 2016;25(5):370-3. [DOI: 10.1111/ajad.12388] [PMID: ] [DOI] [PubMed] [Google Scholar]
Juneau 2015
- Juneau A, Aita M, Heon M. Review and critical analysis of massage studies for term and preterm infants. Neonatal Network 2015;34(3):165-77. [DOI: 10.1891/0730-0832.34.3.165] [PMID: ] [DOI] [PubMed] [Google Scholar]
Kaplan 2008
- Kaplan L, Evans L, Monk C. Effects of mothers' prenatal psychiatric status and postnatal caregiving on infant biobehavioral regulation: can prenatal programming be modified? Early Human Development 2008;84(4):249-56. [DOI: 10.1016/j.earlhumdev.2007.06.004] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelly 2020
- Kelly L, Shan F, MacVicar S, Czaplinkski E, Moulsdale W, Simpson S, et al. A core outcome set for neonatal opioid withdrawal syndrome. Pediatrics 2020;146(1):e20200018. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Ko 2016
- Ko JY, Patrick SW, Tong VT, Patel R, Lind JN, Barfield WD. Incidence of neonatal abstinence syndrome – 28 states, 1999–2013. Morbidity and Mortality Weekly Report 2016;65(31):799-802. [DOI: 10.15585/mmwr.mm6531a2] [PMID: ] [DOI] [PubMed] [Google Scholar]
Kocherlakota 2020
- Kocherlakota P, Qian E, Patel VC, Mandru C, Vilar RE, Alpan G, et al. A new scoring system for the assessment of neonatal abstinence syndrome. American Journal of Perinatology 2020;37(3):333-40. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Krans 2019
- Krans EE, Campopiano M, Cleveland LM, Goodman D, Kilday D, Kendig S, et al. National partnership for maternal safety: consensus bundle on obstetric care for women with opioid use disorder. Obstetrics and Gynecology 2019;134(2):365-75. [DOI: 10.1097/AOG.0000000000003381] [PMID: ] [DOI] [PubMed] [Google Scholar]
Kroenke 2001
- Kroenke K, Spitzer R, Williams J. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine 2001;16(9):606-13. [DOI: 10.1046/j.1525-1497.2001.016009606.x] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Larson 2019
- Larson J, Graham D, Singer L, Beckwith A, Terplan M, Davis J, et al. Cognitive and behavioral impact on children exposed to opioids during pregnancy. Pediatrics 2019;144(2):e20190514. [DOI: ] [PMID: 31320466 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lee 2020
- Lee S, Bora S, Austin N, Westerman A, Hernderson J. Neurodevelopmental outcomes of children born to opioid-dependent mothers: a systematic review and meta-analysis. Academic Pediatrics 2020;20(3):308-18. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Lemon 2018
- Lemon L, Naimi A, Caritis S, Platt R, Venkataramanan R, Bodnar L. The role of preterm birth in the association between opioid maintenance therapy and neonatal abstinence syndrome. Paediatric and Perinatal Epidemiology 2018;32(2):213-22. [DOI: 10.1111/ppe.12443] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2009
- Li MD, Burmeister M. New insights into the genetics of addiction. Nature Reviews. Genetics 2009;10(4):225-31. [DOI: 10.1038/nrg2536] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Liaw 2012
- Liaw J, Yang L, Wang K, Chen C, Chang Y, Yin T. Non-nutritive sucking and facilitated tucking relieve preterm infant pain during heel-stick procedures: a prospective, randomised controlled crossover trial. International Journal of Nursing Studies 2012;49(3):300-9. [DOI: 10.1016/j.ijnurstu.2011.09.017] [PMID: ] [DOI] [PubMed] [Google Scholar]
Lipsitz 1975
- Lipsitz PJ. A proposed narcotic withdrawal score for use with newborn infants: a pragmatic evaluation of its efficacy. Clinical Pediatrics 1975;14(6):592-4. [DOI: 10.1177/000992287501400613] [PMID: ] [DOI] [PubMed] [Google Scholar]
Lisonkova 2019
- Lisonkova S, Richter L, Ting J, Muraca G, Mehrabadi A, Mitchell-Foster S, et al. Neonatal abstinence syndrome and associated neonatal and maternal mortality and morbidity. Pediatrics 2019;144(2):e20183664. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
MacMillan 2018
- MacMillan KD, Rendon CP, Verma K, Riblet N, Washer DB, Volpe Holmes A. Association of rooming-in with outcomes for neonatal abstinence syndrome: a systematic review and meta-analysis. JAMA Pediatrics 2018;172(4):345-51. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
MacVicar 2019
- MacVicar S, Kelly LE. Systematic mixed-study review of nonpharmacological management of neonatal abstinence syndrome. Birth 2019;46(3):428-38. [DOI: 10.1111/birt.12427] [DOI] [PubMed] [Google Scholar]
Maguire 2013
- Maguire D, Cline GJ, Parnell L, Tai C-Y. Validation of the Finnegan neonatal abstinence syndrome tool – short form. Advances in Neonatal Care 2013;13(6):430-7. [DOI: 10.1097/ANC.0000000000000033] [PMID: ] [DOI] [PubMed] [Google Scholar]
Mangat 2019
- Mangat AK, Schmolzer GM, Kraft WK. Pharmacological and non-pharmacological treatments for the neonatal abstinence syndrome (NAS). Seminars in Fetal and Neonatal Medicine 2019;24(2):133-41. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
McQueen 2019
- McQueen K, Taylor C, Murphy-Oikonen J. Systematic review of newborn feeding method and outcomes related to neonatal abstinence syndrome. Journal of Obstetric, Gynecologic, and Neonatal Nursing 2019;48(4):398-407. [DOI: 10.1016/j.jogn.2019.03.004] [DOI] [PubMed] [Google Scholar]
Mehta 2013
- Mehta A, Forbes K, Kuppala V. Neonatal abstinence syndrome management from prenatal counseling to postdischarge follow-up care: results of a national survey. Hospital Pediatrics 2013;3(4):317-23. [DOI: 10.1542/hpeds.2012-0079] [PMID: ] [DOI] [PubMed] [Google Scholar]
Milliren 2018
- Milliren CE, Gupta M, Graham DA, Melvin P, Jorina M, Ozonoff A. Hospital variation in neonatal abstinence syndrome incidence, treatment modalities, resource use, and costs across pediatric hospitals in the United States, 2013 to 2016. Hospital Pediatrics 2018;8(1):15-20. [DOI: 10.1542/hpeds.2017-0077] [PMID: ] [DOI] [PubMed] [Google Scholar]
Moe‐Byrne 2018
- Moe-Byrne T, Brown J, McGuire W. Naloxone for opioid-exposed newborn infants. Cochrane Database of Systematic Reviews 2018, Issue 10. Art. No: CD003483. [DOI: 10.1002/14651858.CD003483.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Journal of Clinical Epidemiology 2009;62(10):1006-12. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Moon 2016
- Moon RY, Task Force on Sudden Infant Death Syndrome. SIDS and other sleep-related infant deaths: evidence base for 2016 updated recommendations for a safe infant sleeping environment. Pediatrics 2016;138(5):e20162940. [DOI: 10.1542/peds.2016-2940] [DOI] [PubMed] [Google Scholar]
Muller 1994
- Muller ME. A questionnaire to measure mother-to-infant attachment. Journal of Nursing Measurement 1994;2(2):129-41. [PMID: ] [PubMed] [Google Scholar]
Newman 2015
- Newman A, Davies GA, Dow K, Holmes B, Macdonald J, McKnight S, et al. Rooming-in care for infants of opioid-dependent mothers: implementation and evaluation at a tertiary care hospital. Canadian Family Physician Medecin de Famille Canadien 2015;61(12):555-61. [PMID: ] [PMC free article] [PubMed] [Google Scholar]
O'Donnell 2009
- O'Donnell M, Nassar N, Leonard H, Hagan R, Mathews R, Patterson Y, et al. Increasing prevalence of neonatal withdrawal syndrome: population study of maternal factors and child protection involvement. Pediatrics 2009;123(4):e614-21. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
O'Grady 2009
- O'Grady MJ, Hopewell J, White MJ. Management of neonatal abstinence syndrome: a national survey and review of practice. Archives of Disease in Childhood. Fetal and Neonatal Edition 2009;94(4):F249-52. [DOI: 10.1136/adc.2008.152769] [PMID: ] [DOI] [PubMed] [Google Scholar]
Oostlander 2019
- Oostlander SA, Falla JA, Dow K, Fucile S. Occupational therapy management strategies for infants with neonatal abstinence syndrome: scoping review. Occupational Therapy in Health Care 2019;33(2):197-226. [DOI: 10.1080/07380577.2019.1594485] [DOI] [PubMed] [Google Scholar]
Osborn 2010a
- Osborn D, Jeffery H, Cole M. Opiate treatment for opiate withdrawal in newborn infants. Cochrane Database of Systematic Reviews 2010, Issue 10. Art. No: CD002059. [DOI: 10.1002/14651858.CD002059.pub3] [DOI] [PubMed] [Google Scholar]
Osborn 2010b
- Osborn D, Jeffery H, Cole M. Sedatives for opiate withdrawal in newborn infants. Cochrane Database of Systematic Reviews 2010, Issue 10. Art. No: CD002053. [DOI: 10.1002/14651858.CD002053.pub3] [DOI] [PubMed] [Google Scholar]
Palisano 1997
- Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Developmental Medicine and Child Neurology 1997;39(4):214-23. [DOI: 10.1111/j.1469-8749.1997.tb07414.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
Paltrow 2013
- Paltrow LM, Flavin J. Arrests of and forced interventions on pregnant women in the United States, 1973–2005: implications for women's legal status and public health. Journal of Health Politics, Policy and Law 2013;38(2):299-343. [DOI: 10.1215/03616878-1966324] [PMID: ] [DOI] [PubMed] [Google Scholar]
Pandita 2018
- Pandita A, Panghal A, Gupta G, Verma A, Pillai A, Singh A, et al. Is kangaroo mother care effective in alleviating vaccination associated pain in early infantile period? A RCT. Early Human Development 2018;127:69-73. [DOI: 10.1016/j.earlhumdev.2018.10.001] [PMID: ] [DOI] [PubMed] [Google Scholar]
Patrick 2012
- Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000–2009. JAMA 2012;307(18):1934-40. [DOI: 10.1001/jama.2012.3951] [PMID: ] [DOI] [PubMed] [Google Scholar]
Patrick 2015a
- Patrick SW, Davis MM, Lehman CU, Cooper WO. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009–2012. Journal of Perinatology 2015;35(8):650-5. [DOI: 10.1038/jp.2015.36] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Patrick 2015b
- Patrick SW, Dudley J, Martin PR, Harrell FE, Warren MD, Hartmann KE, et al. Prescription opioid epidemic and infant outcomes. Pediatrics 2015;135(5):842-50. [DOI: 10.1542/peds.2014-3299] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Patrick 2019
- Patrick SW, Frank RG, McNeer E, Stein BD. Improving the child welfare system to respond to the needs of substance-exposed infants. Hospital Pediatrics 2019;9(8):651-4. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pinelli 2002
- Pinelli J, Symington A, Ciliska D. Nonnutritive sucking in high-risk infants: benign intervention or legitimate therapy? Journal of Obstetric, Gynecologic, and Neonatal Nursing 2002;31(5):582-91. [DOI: 10.1111/j.1552-6909.2002.tb00084.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
Raith 2015
- Raith W, Schmölzer GM, Resch B, Reiterer F, Avian A, Koestenberger M, et al. Laser acupuncture for neonatal abstinence syndrome: a randomized controlled trial. Pediatrics 2015;136(5):876-84. [DOI: 10.1542/peds.2015-0676] [DOI] [PubMed] [Google Scholar]
Review Manager 2020 [Computer program]
- Review Manager 5 (RevMan 5). Version 5.4. Copenhagen: Nordic Cochrane Centre, Cochrane, 2020.
Ryan 2019
- Ryan G, Dooley J, Gerber Finn L, Kelly L. Nonpharmacological management of neonatal abstinence syndrome: a review of the literature. Journal of Maternal-fetal & Neonatal Medicine 2019;32(10):1735-40. [DOI: 10.1080/14767058.2017.1414180] [DOI] [PubMed] [Google Scholar]
Sarkar 2006
- Sarkar S, Donn SM. Management of neonatal abstinence syndrome in neonatal intensive care units: a national survey. Journal of Perinatology 2006;26(1):15-7. [DOI: 10.1038/sj.jp.7211427] [PMID: ] [DOI] [PubMed] [Google Scholar]
Schmidt 2007
- Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, et al, Caffeine for Apnea of Prematurity Trial Group. Long-term effects of caffeine therapy for apnea of prematurity. New England Journal of Medicine 2007;357(19):1893-902. [DOI: 10.1056/NEJMoa073679] [PMID: ] [DOI] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Shah 2012
- Shah PS, Herbozo C, Aliwalas LL, Shah VS. Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database of Systematic Reviews 2012, Issue 12. Art. No: CD004950. [DOI: 10.1002/14651858.CD004950.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Shan 2020
- Shan F, MacVicar S, Allegaert K, Offringa M, Jansson LM, Simpson S, et al. Outcome reporting in neonates experiencing withdrawal following opioid exposure in pregnancy: a systematic review. Trials 2020;21:262. [DOI: 10.1186/s13063-020-4183-9] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2018
- Smith JG, Rogowski JA, Schoenauer KM, Lake ET. Infants in drug withdrawal: a national description of nurse workload, infant acuity, and parental needs. Journal of Perinatal & Neonatal Nursing 2018;32(1):72-9. [DOI: 10.1097/JPN.0000000000000309] [ 29373422] [DOI] [PMC free article] [PubMed] [Google Scholar]
Snowden 2019
- Snowden JN, Akshatha A, Annett RD, Crawford MM, Das A, Devlin LA, et al. The ACT NOW clinical practice survey: gaps in the care of infants with neonatal opioid withdrawal syndrome. Hospital Pediatrics 2019;9(8):585-92. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sterne 2016
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016;12(355):i4919. [DOI: 10.1136/bmj.i4919] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stine 2009
- Stine SM, Heil SH, Kaltenbach K, Martin PR, Coyle MG, Fischer G, et al. Characteristics of opioid-using pregnant women who accept or refuse participation in a clinical trial: screening results from the MOTHER study. American Journal of Drug and Alcohol Abuse 2009;35(6):429-33. [DOI: 10.3109/00952990903374080] [DOI] [PMC free article] [PubMed] [Google Scholar]
Taylor 2005
- Taylor A, Atkins R, Kumar R, Adams D, Glover V. A new mother-to-infant bonding scale: links with early maternal mood. Archives of Women's Mental Health 2005;8(1):45-51. [DOI: 10.1007/s00737-005-0074-z] [PMID: ] [DOI] [PubMed] [Google Scholar]
Tolia 2015
- Tolia VN, Patrick SW, Bennett MM, Murthy K, Sousa J, Smith PB, et al. Increasing incidence of the neonatal abstinence syndrome in U.S. neonatal ICUs. New England Journal of Medicine 2015;372(22):2118-26. [DOI: 10.1056/NEJMsa1500439] [PMID: ] [DOI] [PubMed] [Google Scholar]
Uebel 2015
- Uebel H, Wright IM, Burns L, Hilder L, Bajuk B, Breen C, et al. Reasons for rehospitalization in children who had neonatal abstinence syndrome. Pediatrics 2015;136(4):e811-20. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Uebel 2016
- Uebel H, Wright IM, Burns L, Hilder L, Bajuk B, Breen C, et al. Epidemiological evidence for a decreasing incidence of neonatal abstinence syndrome, 2000–11. Paediatric and Perinatal Epidemiology 2016;30(3):267-73. [DOI: 10.1111/ppe.12282] [PMID: ] [DOI] [PubMed] [Google Scholar]
Velez 2009
- Velez M, Jansson LM. The opioid dependent mother and newborn dyad: non-pharmacologic care. Journal of Addiction Medicine 2008;2(3):113-20. [DOI: 10.1097/ADM.0b013e31817e6105] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wachman 2018a
- Wachman EM, Warden AH, Thomas Z, Thomas-Lewis JA, Shrestha H, Nikita FN, et al. Impact of psychiatric medication co-exposure on neonatal abstinence syndrome severity. Drug and Alcohol Dependence 2018;192:45-50. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Wachman 2018b
Whalen 2019
- Whalen BL, Holmes AV, Blythe S. Models of care for neonatal abstinence syndrome: what works? Seminars in Fetal & Neonatal Medicine 2019;24(2):121-32. [DOI: 10.1016/j.siny.2019.01.004] [DOI] [PubMed] [Google Scholar]
Whooley 1997
- Whooley MA, Avins AL, Miranda J, Browner WS. Case-finding instruments for depression. Two questions are as good as many. Journal of General Internal Medicine 1997;12(7):439-45. [DOI: 10.1046/j.1525-1497.1997.00076.x] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Winkelman 2018
- Winkelman T, Villapiano N, Kozhimannil K, Davis M, Patrick S. Incidence and costs of neonatal abstinence syndrome among infants with Medicaid: 2004–2014. Pediatrics 2018;141(4):e20173520. [DOI: 10.1542/peds.2017-3520] [PMID: ] [DOI] [PMC free article] [PubMed]
Yeoh 2019
- Yeoh SL, Eastwood J, Wright IM, Morton R, Melhuish E, Ward M, et al. Cognitive and motor outcomes of children with prenatal opioid exposure: a systematic review and meta-analysis. JAMA Network Open 2019;2(7):e197025. [DOI: ] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zahorodny 1998
- Zahorodny W, Rom C, Whitney W, Giddens S, Samuel M, Maichuk G, et al. The neonatal withdrawal inventory: a simplified score of newborn withdrawal. Journal of Developmental and Behavioral Pediatrics 1998;19(2):89-93. [DOI: ] [PMID: ] [DOI] [PubMed] [Google Scholar]
Zhang 2018
- Zhang S, Su F, Li J, Chen W. The analgesic effects of maternal milk odor on newborns: a meta-analysis. Breastfeeding Medicine 2018;13(5):327-34. [DOI: 10.1089/bfm.2017.0226] [PMID: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Pahl 2018
- Pahl A, Young L, Buus‐Frank ME, Marcellus L, Soll R. Non-pharmacological care for opioid withdrawal in newborns. Cochrane Database of Systematic Reviews 2018, Issue 12. Art. No: CD013217. [DOI: 10.1002/14651858.CD013217] [DOI] [PMC free article] [PubMed] [Google Scholar]