

Abstract
Oral health is a pivotal sign of overall health, well-being, and quality of life. With the emergence of COVID-19 pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), insights into the relationship between SARS-CoV-2 and oral diseases are urgently needed to elucidate the oral manifestations of SARS-CoV-2. The current review aims at analyzing various reports available on oral symptoms along with possible causation, their relationship to the time of occurrence of clinical symptoms, and to shape guidelines for dental practices that could help in combating this global pandemic. The common symptoms that patients report to the dental office even at the presymptomatic stage are ageusia (loss of taste), non-specific anosmia (loss of smell—not associated with rhinitis), and hyposalivation. Few studies also report unexplained ulcers in the oral cavity, desquamative gingivitis, herpetiform ulcers on attached gingiva, blisters/irregular ulcers on the tongue's dorsal surface enlargement of submandibular glands, and cervical lymph node enlargement. Dental surgeons should abide by the prevalent precautionary guidelines. They are at very high risk due to their close contact with patients and exposure to saliva and blood during treatment.
Keywords: Ageusia, anosmia, COVID-19, dental practice, oral manifestations, oral ulcers, SARS-CoV-2
Introduction
The World Health Organization (WHO) situation report on Corona Virus Disease-19 (COVID-19) published on Oct 12, 2020, states that the total number of cases of COVID-19 globally are 37,109,851, including 10,70,355 deaths.[1]
WHO classified the disease as Public Health Emergency of International Concern on Jan 30 and used the nomenclature COVID-19 for the disease caused by novel coronavirus Severe Acute Respiratory Syndrome Corona Virus – 2 (SARS-CoV-2) on Feb 11, 2020.
The disease started as pneumonia of unknown origin in Wuhan city of China in Nov 2019. It soon affected millions of individuals worldwide, causing life-threatening complications in medically compromised and healthy individuals with a propensity towards the diseased and elderly with decreased immune response.
The current pandemic is the third only reported incidence of human infection in which a coronavirus crossed the species barrier and caused severe mortality and morbidity. The first incidence was SARS in 2003, and the second was MERS in 2012. Before these incidences, coronaviruses were only associated with the infections in animals.
The Virus
The term “coronavirus” is derived from the Latin word CORONA meaning “Crown” as its structure resembles Crown with Multiple Spikes[2,3] under an electron microscope. They were first discovered in the early 1930s in poultry,[4] and later the first human coronaviruses were discovered in the 1960s.[5]
Structure and Classification
The new Corona Virus, SARS-CoV-2, is an enveloped, positive-sense single-stranded RNA virus with multiple spikes on the surface having a genome size of approximately 26-32 kilobases and belongs to genera beta coronaviruses. Similar to coronaviruses SARS-CoV that causes SARS and MERS-CoV that causes MERS, SARS-CoV-2 is considered zoonotic, with Chinese horseshoe bats (Rhinolophus sinicus) being the most probable natural reservoir,[6] and its genome is very much similar to coronavirus of bat origin RaTG13.[7] The SARS-CoV (SARS-S) enters the host target cells primarily through the endosomal membrane fusion, or CoV utilizes plasma membrane fusion.[8] The S protein (a glycoprotein) of SARS-CoV plays a trivial role in receptor binding, membrane fusion, and virus entry.[8] The SARS-CoV entry is initiated by binding of the S protein to the cellular receptor angiotensin-converting enzyme 2 (ACE2),[9] and also utilize the cellular serine protease-2 TMPRSS2 for S protein priming[10] [Figure 1]. In the recent outbreak, another isoform of CoV, i.e., CoV-2, is identified as primary virulent form. A recent study suggests that SARS-CoV-2 (SARS-S-2) cell entry also depends on ACE2 and TMPRSS2.[9,11] In summary, SARS-CoV-2 employs the SARS-CoV receptor ACE2 for entry in the host cell and TMPRSS2 primes the spike protein of SARS-CoV-2.
Figure 1.

Detail structure of coronavirus (a). Transmission of SARS-CoV-2 through respiratory droplets / aerosols (b). The entry of SARS-CoV-2 into the host target cells is initiated by binding Spike glycoproteins with angiotensin-converting enzyme-2 (ACE2) and also utilize serine protease for spike protein priming (c and d). Interaction of RBD with ACE2 (d). Oral Manifestations of SARS-CoV-2 (all or none can occur separately or concurrently) (e). The illustration is made Biorender.com
Transmission of SARS CoV-2
It is speculated that the initial transmission of SARS-CoV-2 occurs from bats to humans somewhere near Wuhan in China, followed by a human to human transfer. Direct person to person spread occurs through the accidental inhalation of respiratory droplets created during the sneezing and coughing by an infected individual. This type of transfer occurs between the closed contacts within a distance of 6 feet. Another mode of transmission is by touching the contaminated surfaces by hand and later transferring the viral particle to an individual's mouth, nose, or eyes.[12] The surface contamination occurs by the settling of viral particles formed during sneezing or coughing. Kampf et al. have observed that the human coronavirus can persist on inanimate surfaces such as metal, glass, or plastic at room temperature for up to 9 days. Further transmission by self inoculation to mouth, eye, and nose from contaminated dry surfaces also occurs.[13,14] Recent studies find the presence of the virus in the fecal samples and suggest that the transmission through the fecal-oral route as well[15,16]; few authors suggest that the SARS-CoV-2 can also spread through the air.[17]
The typical route of transmission is by contact with the symptomatic patient, but the disease can be transmitted by the asymptomatic individuals also.
Clinical Manifestations of COVID-19
WHO classified COVID-19 symptoms into three broad classes. The most common symptoms are fever, dry cough, and tiredness. Less common symptoms are body aches and pain, sore throat, diarrhea, conjunctivitis, headache, loss of taste or smell, a rash on the skin, or discoloration of fingers and toes. The severe symptoms are difficulty in breathing or shortness of breath, chest pain or pressure, and loss of speech or movement.[1,18] Clinical symptoms vary from totally asymptomatic to having mild flu-like symptoms to severe respiratory illness. The symptoms are more profound in individuals with comorbidities like diabetes, hypertension, and ischemic heart disease. ACE2 plays a very crucial role in the pathogenesis and pathophysiology of COVID-19 infection. Some antihypertensive drugs act as ACE inhibitors, and this further increases the amount of ACE2 in tissues and causes an increased risk of infection by SARS-CoV-2.[19]
Oral Manifestations
The common symptoms that patients report to the dental office even at the presymptomatic stage are ageusia (loss of taste), non-specific anosmia (loss of smell—not associated with rhinitis), and hyposalivation.[20,21] Few reports state that along with unexplained ulcers in the oral cavity, desquamative gingivitis, herpetiform ulcers on attached gingiva, blisters/irregular ulcers on the tongue's dorsal surface,[22] enlargement of submandibular glands, and cervical lymph node enlargement.[23] These oral manifestations may be associated with an erythematous rash on the face or viral enanthema.[24] Dysgeusia or ageusis and anosmia is found to be common in COVID-19 patients, and the range varies from 5.6%[25]– 88.8%[26] of patients [Table 1]. These symptoms are more common in young individuals and females, and these symptoms usually get resolved in 03 weeks.[20]
Table 1.
Comparative study chart of the percentage of patients with olfactory and gustatory symptoms and their time of onset in COVID patients
| Number of subjects | Percentage (number) of patients with olfactory and gustatory Symptoms | Onset of symptoms | Reference |
|---|---|---|---|
| 72 | 12.5% (09) Taste disorder only 14.4% (14) Smell Disorder 30 (41.41) both disorders |
Early symptoms within 05 days of admission | [21] |
| 3191 | 15.3% (488) have Anosmia and ageusia | Early symptoms | [20] |
| 214 | 5.1% (11) Anosmia 5.6% (12) ageusia |
Not Reported | [25] |
| 41 | 68% (28) anosmia/ageusia | Approx 12 days after infection | [27] |
| 320 | 19.4% (62) chemosensory dysfunction | Not Mentioned | [28] |
| 59 | 10.6% (06) taste disorder 5% (03) olfactory disorder 18.6% (11) mixed disorder |
Early as well as delayed onset | [29] |
| 417 | 85.6% (357) olfactory disorder 88.8% (342) gustatory disorder |
Not Mentioned | [26] |
Literature reveals that ACE2 is the receptor on target cells for the SARS-CoV-2 virus. It helps in the binding of the SARS-CoV-2 virus spike protein to the cells and subsequent infection [Figure 1].[30] Ageusia or loss of taste is attributed to the presence of ACE2 expressing cells in higher numbers in the epithelial cells of the oral tissues and nasal mucosa.[31,32] ACE2 expression is more profound in gustatory receptors of the tongue than the buccal or gingival tissues leading to certain chemosensory changes that led to ageusia.[30] These changes can occur due to the direct damage to the gustatory and olfactory receptors by the SAR-CoV-2 virus. The exact cause of ulcers/blisters is still unknown, and there is a wide difference in opinion of various authors. Some investigators suggest these as the direct result of the SARS-CoV-2 infection, but most of the authors regarded them as aphthous ulcers secondary to mental stress or reactivation or new infection by various pathogen including herpes simplex virus or other opportunistic infections due to change in the immunity status of the individual related to SARS-CoV-2 virus [Table 2].
Table 2.
Comparative study chart of extraoral and intraoral symptoms and laboratory confirmation in various sub groups
| Number of Subjects | Age | Extraoral symptoms/Comorbidities | Intraoral symptoms | Laboratory confirmation of SARS CoV-2 | Reference |
|---|---|---|---|---|---|
| 03 | 56/M | Asthenia and fever, hyposmia,/ enlargement of cervical lymph nodes | Dysgeusia, lesion resembling herpetic stomatitis | Suspected case | [23] |
| 58/M | None declared/Diabetes Mellitus and Hypertension | Unilateral Multiple small ulcers on palate | Suspected case | ||
| 65/F | High fever, diarrhea/ Hypertension and obesity | Desquamative gingivitis, blisters on internal lip mucosa | Confirmed case | ||
| 01 | 45/F | Mild asthenia/Erythematous lesion on big toe | Irregular ulcer on the dorsal surface of the tongue | Confirmed case | [22] |
| 01 | 67/M | NA/Multiple systemic diseases | Hypogeusia, Multiple yellowish pinpoint ulcers on the dorsum of the tongue | Confirmed case | [33] |
| 02 | 56/F | Fever and shortness of breath/ Diabetes Mellitus | Multiple painful ulcers of varying sizes with Irregular margins on the entire hard palate | Confirmed case | [34] |
| 75/M | Hypertension with hypoxia | several painful small ulcers, with irregular margins, in red and non-hemorrhagic background on the anterior of the tongue. | Confirmed Case | ||
| 01 | 19/F | Hyposmia, Erythematous, macules, papules and petechiae on lower extremities, fever, sore throat | Erosion, ulceration and blood crusts on the inner surface of the lower lip, Palatal and gingival petechiae | Confirmed Case | [35] |
| 01 | 52/F | No Extraoral symptoms/ comorbidities reported | Erythematous lesions and erosions on lips and buccal mucosa | Confirmed Case | [36] |
| 01 | 35/F | Fever | Necrotic interdental papilla | Suspected case | [37] |
The treatment of COVID-19 includes a combination of therapies and experimental drugs. Because of these intensive drug therapies, patients may develop various side effects and suffer from several oral problems, including pathologies of the oral mucosa, changes in salivary gland function as well as neurological side effects.
Out of the various new therapies, antiviral drugs may cause certain side-effects affecting the oral cavity, such as, stomatitis, oral ulcers, and dry mouth. It has been reported that Interferon (IFN) α/β, used for their antiviral activities, reduces the severity of COVID-19 disease, potentially improving survival rate,[38] by decreasing the symptoms of severe respiratory illness such as COVID-19 related pneumonia and support improvements in lung function. Common oral side effects related to the use of IFN-α/β may comprise dry mouth, resulting in frequent oral thrush cases. SARS-CoV-2 can also cause a cytokine storm, which can aggravate existing autoimmune conditions in the oropharyngeal area, leading to oral symptoms.
These oral symptoms can be linked to the lack of proper oral care and oral examination in a hospital set up as the priority is to save lives during this pandemic. Besides all the causes discussed above, the oral ulcers can also be attributed due to the vasculitis caused by the excess accumulation of angiotensin II in the vascular cells. Excess accumulation of angiotensin II may cause vasoconstriction, vascular abnormalities, and increased vascular permeability leading to ulcer formation.
Dental Practice during COVID-19 Pandemic
COVID-19 pandemic leads to the complete closure of almost all dental practices throughout the world except for managing dental emergencies, which are potentially life-threatening due to airway obstruction, continuous tissue bleeding, trauma, facial bone fractures, and severe pain not manageable by medications alone. With the ease in lockdown, dental practices across the countries are opening up but with many changes in the way the treatment proceeds.
These changes are especially necessary as the infection usually spreads through respiratory droplets or fomites,[2,7] and a very high viral load is found in the oral and nasal cavity of the infected patients. The virus has been found in saliva in the early stages of COVID-19 patients.[39] The dental surgeons/health care workers must be aware of this as they are at an increased risk of getting infected. Besides the very high viral load in respiratory droplets and saliva, the closed working environment and use of various instruments like high and low-speed turbines, ultrasonic scalers/piezoelectric instruments, 3-way syringes, dental intraoral X-rays, etc., also put the dental surgeons and health care workers at high risk of getting infected. Not only the saliva, various oral secretions, and blood may aerosolize because of inadvertent coughing by the patient or during the treatment procedure leading to cross-contamination. Thus, the aerosols may persist in the clinic environment for approximately 03 hrs, imposes an additional infection source.
It should be kept in mind that the incubation time for COVID-19 after the exposure to SARS-CoV-2 is 14 days, with patients developing COVID-19 disease 4–5 days (range between 2 and 7 days)[40] after being infected. This information is crucial as even the asymptomatic and paucisymptomatic patients can act as carriers of SARS-CoV-2 and can cause transmission of infection.[41] As per a report published by Rothe et al., 2020,[42] patients in the recovery phase also can be the potential sources of virus transmission. Till the time the report is negative, every patient must be considered infective, and proper measures are to be taken to avoid cross-infection.
Steps to be taken
Prevention of transmission
First and foremost, efforts should be made to reduce the risk of contamination to the patients and dental health care workers. This can be achieved by teaching the staff about the latest infection prevention protocols (WHO and CDC recommendations), careful handling of materials, equipments and by making appropriate changes in the infrastructure of dental operatory and reception. Patients are requested to wear the mask while entering the clinic and during all the time till they are not called to meet the dentist. They are advised to enter the dental clinic at the time of their appointment and advised to wait in the car or a designated area outside the dental clinic, if early. Patients attendants should only be allowed if necessary (old age and pediatric patient coming with parent), and they are preferably a family member to reduce exposure risk. Patients are advised to re-wear the masks immediately after the treatment.
Pre-visit evaluation of the patient
It is recommended to perform telephonic triage for all the patients. For triage, a pre-decided set of questions can be asked or sent electronically to the patients. For the patients, not requiring urgent management, telephonic consultation should be provided by audio or video calls after proper assessment and history taking [Figure 2].
Figure 2.
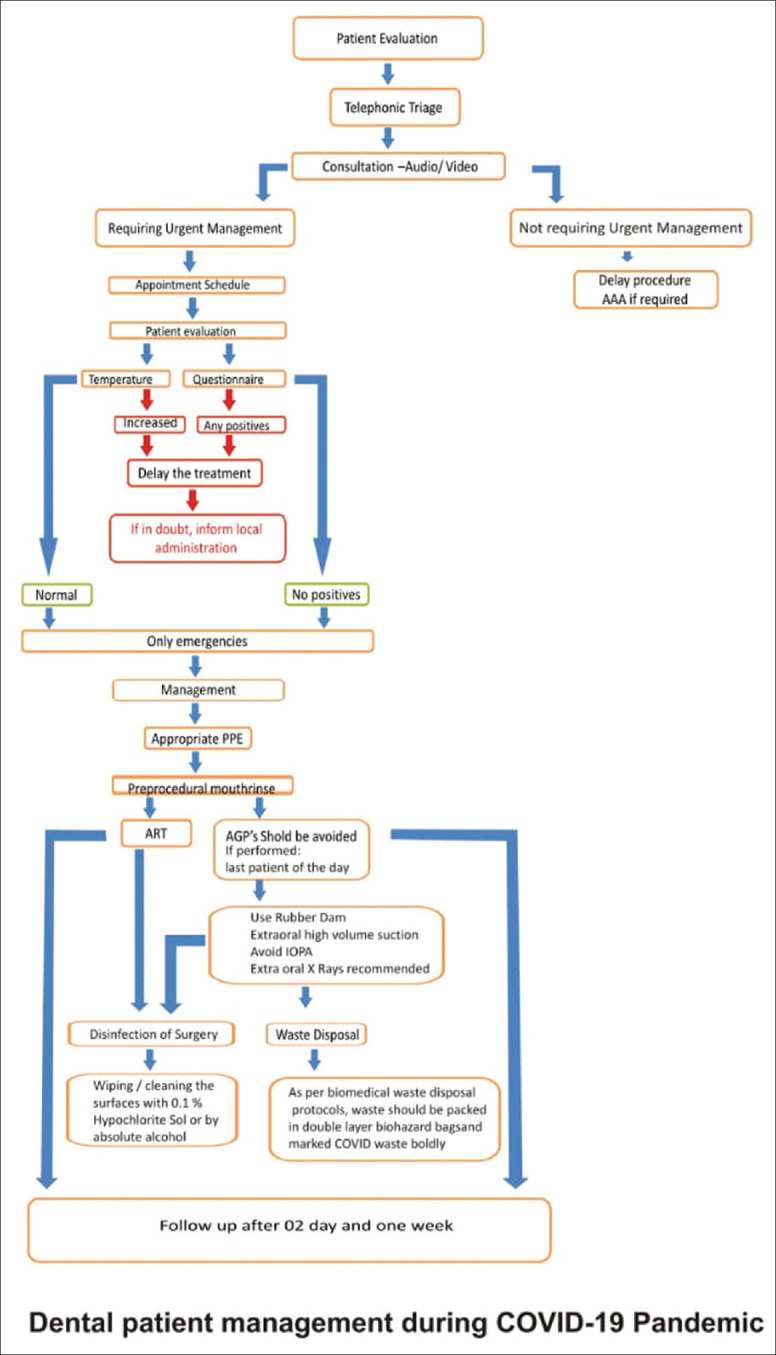
Algorithm for dental patient management during COVID-19 pandemic
Pharmacological Management
In cases where medicines can be prescribed to alleviate the pain of the patient, analgesics and antibiotics should be prescribed telephonically as per the requirement. Three A's should be followed -Advise, Analgesia, and Antimicrobials (AAA).
Schedule of appointments
Scheduling should be done so as to minimize the number of patients at a given time in the waiting room to decrease the contact between two patients to avoid the chances of viral transmission. Enough time between the two appointments should be planned that will be sufficient to sanitize the surgery to prevent cross-infection.
Evaluation of the patients on arrival at the clinic
Visits to the dental operatory should be reduced to a minimum. If at all, the patient has to visit dental clinic/dental surgery for an emergency procedure, only those with prior appointment and triage should only be entertained in the clinic.
Upon arrival, the patient's risk assessment should be performed by measuring their body temperature before entering the clinic and through a questionnaire. The questionnaire should be pertaining to their recent travel status and any relevant past medical history specifically pertaining to respiratory distress, cold, cough, running nose, sore throat etc., Further management should be planned according to the responses received. Any positive responses to any of the questions should raise concern, the patient should be asked to stay separate from other patients, and the treatment should be postponed for at least 3 weeks except in dental emergencies.
Management of the patient
Before any procedure, the use of personal protective equipments (PPE), including face masks, gloves, gowns, shoe cover and goggles/face shield, is recommended to protect the skin and mucosa from infected saliva or blood.
It is recommended that every patient should be considered potentially infectious, and proper personnel protection measures should be taken.
For appointments that do not result in aerosols and need examination only, a dentist should wear a triple layer surgical mask and protective eyewear/face shield, and gloves.
For high-risk and very high-risk procedures, wear N95 face masks, protective eyewear/face shields, and double gloving along with coverall.
When examining patients with moderate risk, the treating doctor will require all PPE's as high risk except that the coveralls can be substituted with surgical gowns.
Minimally invasive procedures, atraumatic restorative techniques (ART) should be used for restorations.
Aerosol-generating procedures should be avoided/reduced to a minimum. It should always be kept in mind that SARS-CoV-2 may spread through aerosols produced during various dental procedures.[43] If the aerosol-generating procedure is required to be performed, rubber dam use is recommended along with high volume extra oral suction to reduce aerosols or splatter produced during the procedure. That patient should be the last patient for the day to prevent cross-contamination and further infection. After the completion of the procedure, proper disinfection of the surgery setup is to be done. Use of face shields and protective goggles are essential in aerosol-generating procedures because saliva is considered as a route of transmission. It should be noted that if a surgical mask and a face shield is not available, do not perform any aerosol-generating procedures in any case.
To decrease the viral load in the oral cavity, pre-examination mouth rinse with 0.2% povidone-iodine mouthwash or 1% hydrogen peroxide[33] is recommended. Procedures that may cause gagging, coughing should be avoided or if necessary, performed cautiously. Intraoral periapical X-rays may cause coughing and increase in salivation, thus increasing the chances of infection, extraoral X- rays like orthopantomogram (OPG) or cone-beam computed tomography (CBCT) should be used.
Disinfection and waste disposal
SARS-CoV-2 can survive for a few hours to days in the operatories, and the potential areas that may be contaminated with the virus need to be disinfected before further use. Fomites need to be reduced by removing any unnecessary material (toys, remotes, magazines, etc.) and instruments from the surgery. Frequent wiping/cleaning of all the surfaces that may come in contact with the patient should be done with the recommended cleaner (0.1% sodium hypochlorite sol).
The waste generated in the clinic should be considered as highly infectious, should be segregated as per protocols, and packed in the double-layered biohazard polythene bags. The surface of the bag should be marked COVID waste as per the biomedical waste guidelines.
Follow up
After a visit to the dental clinic, the patient should be contacted after 24 hrs and again after 01 weeks to ascertain the patient's health status and warn the dental staff to take necessary steps if in doubt. Patients should be advised to call the dental clinic if at all, there are any symptoms present.
Clinic setup
Reception area
Wearing of facemasks and hand hygiene procedures to be followed strictly. Signs and posters are to be placed at the entrance and reception area to provide information about hand and respiratory hygiene and coughing etiquettes. Sufficient supply of 3 ply masks and hand sanitizer (preferably with 70% - 80% of alcohol) to be made available at all times. Waiting chairs should be placed at least 06 feet apart to maintain social distancing norms. Objects that cannot be sterilized or disinfected regularly like Magazines, TV remotes, toys should be removed; they may act as fomites. The reception area should be kept well ventilated by opening windows, and cash handling should be minimized, and online payments are preferred.
Inside the operatory
New armamentarium
It is recommended that every dental surgery be equipped with a fumigator, high volume extra oral suction to reduce the dispersal of aerosols, dental handpieces, and dental water lines with anti-retraction valves prevent the spread of infection. Ultraviolet germicidal irradiation units can also be considered.
It should always be kept in mind that proper handwashing between patients and after touching any non-sterile surface is the most effective way to reduce transmission of COVID-19. Hand sanitization after the removal of PPE is of particular importance to remove any viral particle that may contaminate hands during removal. Handwashing with soap for 20 seconds or use of hand sanitizer with 70%-80% alcohol is recommended.
Conclusion
General Physicians and Dental Surgeons must be aware of the various oral signs and symptoms of COVID-19, as approximately 80% of the COVID-19 patients are asymptomatic,[34] and these may be the initial and the only symptoms present in a patient when they visit a Dental Clinic. Awareness regarding these initial symptoms is vital, and if in suspicion, the patient should be referred to a dedicated COVID-19 facility where the diagnosis and further management can be properly done.
Physicians and, most importantly, the Dental surgeons should abide by the prevalent precautionary guidelines. They are at very high risk due to their close contact with patients and exposure to saliva and blood during treatment. Telephonic consultation should be preferred, and elective treatment should be deferred until the COVID-19 situation improves.
After the pandemic's peak has passed, the proper guidelines for the elective procedures should be released to facilitate the normal situation in which all the dental procedures can be performed. SARS-CoV-2 infection may stay for a longer period; protocols should be devised so that patient management is not hampered and containment of cross-infection at dental clinics.
Key Points
Approximately 80% of the COVID-19 patients are asymptomatic, and oral symptoms may be the initial and only symptoms present in a patient when they visit a Dental Clinic or a Family Physician.
Telephonic consultation should be preferred,
All kinds of elective treatment should be deferred until the COVID-19 situation improves.
Proper triage using audio/video calls before the clinic/hospital visit.
Treatment if required, should be done only after wearing recommended PPE's.
Certain modifications are required in the clinic to reduce the spread of aerosols and prevent cross-contamination.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organization. Coronavirus Disease (covid-19) Pandemic. 2020 [Google Scholar]
- 2.Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in china, 2019. N Engl J Med. 2020;382:727–33. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lan J, Ge J, Yu J, Shan S, Zhou H, Fan S, et al. Structure of the sars-cov-2 spike receptor-binding domain bound to the ace2 receptor. Nature. 2020;581:215–20. doi: 10.1038/s41586-020-2180-5. [DOI] [PubMed] [Google Scholar]
- 4.Beach J, Schalm O. A filterable virus, distinct from that of laryngotracheitis, the cause of a respiratory disease of chicks. Poul Sci. 1936;15:199–206. [Google Scholar]
- 5.Tyrrell D, Bynoe M. Cultivation of a novel type of common-cold virus in organ cultures. Br Med J. 1965;1:1467. doi: 10.1136/bmj.1.5448.1467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mackenzie JS, Smith DW. Covid-19: A novel zoonotic disease caused by a coronavirus from China: What we know and what we don't. Microbiol Aust. 2020;41:45–50. doi: 10.1071/MA20013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579:270–73. doi: 10.1038/s41586-020-2012-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Choudhary S, Malik YS, Tomar S, Tomar S. Identification of sars-cov-2 cell entry inhibitors by drug repurposing using in silico structure-based virtual screening approach? Front Immunol. 2020;11:1664. doi: 10.3389/fimmu.2020.01664. doi: 10.3389/fimmu. 2020.01664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Patel AB, Verma A. Covid-19 and angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: What is the evidence? JAMA. 2020;323:1769–70. doi: 10.1001/jama.2020.4812. [DOI] [PubMed] [Google Scholar]
- 10.Ou X, Liu Y, Lei X, Li P, Mi D, Ren L, et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat Commun. 2020;11:1620. doi: 10.1038/s41467-020-15562-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–80.e8. doi: 10.1016/j.cell.2020.02.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z, et al. Epidemiology and transmission of covid-19 in 391 cases and 1286 of their close contacts in shenzhen, china: A retrospective cohort study. Lancet Infect Dis. 2020;2020;20:911–9. doi: 10.1016/S1473-3099(20)30287-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020;104:246–51. doi: 10.1016/j.jhin.2020.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of sars-cov-2 as compared with sars-cov-1. N Engl J Med. 2020;382:1564–67. doi: 10.1056/NEJMc2004973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gu J, Han B, Wang J. Covid-19: Gastrointestinal manifestations and potential fecal–oral transmission. Gastroenterology. 2020;158:1518–19. doi: 10.1053/j.gastro.2020.02.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lee I-C, Huo T-I, Huang Y-H. Gastrointestinal and liver manifestations in patients with covid-19. J Chin Med Assoc. 2020;83:521–23. doi: 10.1097/JCMA.0000000000000319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morawska L, Cao J. Airborne transmission of sars-cov-2: The world should face the reality. Environ Int. 2020;139:105730. doi: 10.1016/j.envint.2020.105730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kar S. Covid-19: A brief clinical overview. J Geriatr Care Res. 2020;7:74–8. [Google Scholar]
- 19.Tignanelli CJ, Ingraham NE, Sparks MA, Reilkoff R, Bezdicek T, Benson B, et al. Antihypertensive drugs and risk of covid-19? Lancet Respir Med. 2020;8:e30–1. doi: 10.1016/S2213-2600(20)30153-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lee Y, Min P, Lee S, Kim S-W. Prevalence and duration of acute loss of smell or taste in covid-19 patients. J Korean Med Sci. 2020;35:e174. doi: 10.3346/jkms.2020.35.e174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vaira LA, Deiana G, Fois AG, Pirina P, Madeddu G, De Vito A, et al. Objective evaluation of anosmia and ageusia in covid-19 patients: Single-center experience on 72 cases. Head Neck. 2020;42:1252–8. doi: 10.1002/hed.26204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chaux-Bodard A-G, Deneuve S, Desoutter A. Oral manifestation of covid-19 as an inaugural symptom? J Oral Med Oral Surg. 2020;26:18. [Google Scholar]
- 23.Martín Carreras-Presas C, Amaro Sánchez J, López-Sánchez AF, Jané-Salas E, Somacarrera Pérez ML. Oral vesiculobullous lesions associated with SARS-CoV-2 infection. Oral Dis. 2020 doi: 10.1111/odi.13382. doi: 10.1111/odi. 13382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rocha BA, Souto GR, de Mattos Camargo Grossmann S, de Aguiar MCF, de Andrade BAB, Romañach MJ, et al. Viral enanthema in oral mucosa: A possible diagnostic challenge in the covid-19 pandemic. Oral Dis. 2020 doi: 10.1111/odi.13473. doi: 10.1111/odi.13473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mao L, Wang M, Chen S, He Q, Chang J, Hong C, et al. Neurological manifestations of hospitalized patients with covid-19 in Wuhan, China: A retrospective case series study. JAMA Neurol. 2020;77:683–690. doi: 10.1001/jamaneurol.2020.1127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (covid-19): A multicenter european study. Eur Arch Otorhinolaryngol. 2020;277:2251–61. doi: 10.1007/s00405-020-05965-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schmithausen RM, Döhla M, Schößler H, Diegmann C, Schulte B, Richter E, et al. Characteristic temporary loss of taste and olfactory senses in sars-cov-2-positive-individuals with mild symptoms. Pathogens and Immunity. 2020;5:117–20. doi: 10.20411/pai.v5i1.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Vaira LA, Salzano G, Deiana G, De Riu G. Anosmia and ageusia: Common findings in covid-19 patients. Laryngoscope. 2020;130:1787. doi: 10.1002/lary.28692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Giacomelli A, Pezzati L, Conti F, Bernacchia D, Siano M, Oreni L, et al. Self-reported olfactory and taste disorders in patients with severe acute respiratory coronavirus 2 infection: A cross-sectional study. Clin Infect Dis. 2020 doi: 10.1093/cid/ciaa330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X, et al. High expression of ACE2 receptor of 2019-ncov on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12:8. doi: 10.1038/s41368-020-0074-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med. 2020;14:185–92. doi: 10.1007/s11684-020-0754-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ren X, Glende J, Al-Falah M, de Vries V, Schwegmann-Wessels C, Qu X, et al. Analysis of ACE2 in polarized epithelial cells: Surface expression and function as receptor for severe acute respiratory syndrome-associated coronavirus. J Gen Virol. 2006;87:1691–95. doi: 10.1099/vir.0.81749-0. [DOI] [PubMed] [Google Scholar]
- 33.dos Santos JA, Normando AGC, da Silva RLC, De Paula RM, Cembranel AC, Santos-Silva AR, et al. Oral mucosal lesions in a covid-19 patient: New signs or secondary manifestations. Int J Infect Dis. 2020 doi: 10.1016/j.ijid.2020.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ansari R, Gheitani M, Heidari F, Heidari F. Oral cavity lesions as a manifestation of the novel virus (covid-19): A letter-to-editor. Oral Dis. 2020 doi: 10.1111/odi.13465. doi: 10.1111/odi. 13465. [DOI] [PubMed] [Google Scholar]
- 35.Ciccarese G, Drago F, Boatti M, Porro A, Muzic SI, Parodi A. Oral erosions and petechiae during SARS-CoV-2 infection. J Med Virol. 2020 doi: 10.1002/jmv.26221. doi: 10.1002/jmv. 26221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sakaida T, Isao T, Matsubara A, Nakamura M, Morita A. Unique skin manifestations of covid-19: Is drug eruption specific to covid-19? J Dermatol Sci. 2020;99:62–4. doi: 10.1016/j.jdermsci.2020.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Patel J, Woolley J. Necrotizing periodontal disease: Oral manifestation of covid-19. Oral Dis. 2020 doi: 10.1111/odi.13462. doi: 10.1111/odi.13462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mahase E. Covid-19: What treatments are being investigated? Br Med J. 2020;368:m1252. doi: 10.1136/bmj.m1252. [DOI] [PubMed] [Google Scholar]
- 39.Chen L, Zhao J, Peng J, Li X, Deng X, Geng Z, et al. Detection of 2019-ncov in saliva and characterization of oral symptoms in covid-19 patients. 2020. Available from: https://ssrn.com/abstract=3556665 . [DOI] [PMC free article] [PubMed]
- 40.Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR, et al. The incubation period of coronavirus disease 2019 (covid-19) from publicly reported confirmed cases: Estimation and application. Ann Intern Med. 2020;172:577–82. doi: 10.7326/M20-0504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Jiang X-L, Zhang X-L, Zhao X-N, Li C-B, Lei J, Kou Z-Q, et al. Transmission potential of asymptomatic and paucisymptomatic sars-cov-2 infections: A three-family cluster study in China. J Infect Dis. 2020;221:1948–52. doi: 10.1093/infdis/jiaa206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-ncov infection from an asymptomatic contact in germany. N Engl J Med. 2020;382:970–71. doi: 10.1056/NEJMc2001468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Harrel SK, Molinari J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J Am Dent Assoc. 2004;135:429–37. doi: 10.14219/jada.archive.2004.0207. [DOI] [PMC free article] [PubMed] [Google Scholar]