

Abstract
Aims, Settings, and Design:
The COVID-19 pandemic has forced upon sudden lifestyle changes because of nationwide lockdowns mandating isolation at home, affecting daily habits and lifestyle changes. The present study was conducted with an aim to assess these changes brought about because of COVID-19 lockdown restrictions.
Methods:
The web-survey aimed to understand the immediate impact of the COVID-19 lockdown on people by using a structured questionnaire collecting demographic, lifestyle, and dietary information. The survey was disseminated online among the literate, urban, adult population with internet access.
Results:
Of the 1,200 people who received the survey, a total of 1,008 respondents participated in the study, aged between 18 and 81 years (Median- 24). An increase in daily screen time has been observed in 56.7% of the population. A decrease in work-related stress was observed in 43% of the population, sleep pattern improved in 36.7% people, and 27.1% of the inactive population showed increased physical activity. A significant decrease in the proportion of people consuming junk food (73.8%), alcohol (27.6%), and smoking (8.1%) was observed.
Conclusions:
The present web-based survey study suggests a significant change in the lifestyle and dietary patterns of people brought about because of the COVID-19 lockdown most highly seen as a major increase in screen usage and a decrease in junk food consumption.
Keywords: Coronavirus, COVID-19, dietary habits, India, lifestyle
Introduction
On 30th January 2020, the WHO Emergency Committee declared COVID-19 as a global health emergency.[1] On 24 March 2020, the total confirmed positive cases in India were 500. A nationwide lockdown was ordered by the Government of India for 21 days, imposing restrictions on the movement of 1.3 billion citizens of India as a preventative measure to combat the spread of COVID-19 in India. All transport services as well as educational institutions, industrial establishments, and hospitality services were suspended. Due to this stringent lockdown, a sudden, significant change in the habits and lifestyles of the population is expected. Physical distancing and self-isolation strongly impacted citizens' lives, affecting everyday behavior.
There are two major influences of the lockdown: self-quarantine and inaccessibility of consumer goods. Remote working/suspension of professional work may have a direct impact on work-related stress. Moreover, working from home might translate into an increased screen use which has been linked with a sedentary lifestyle, weight gain, as well as decreased and poor quality sleep. Sleep deprivation has extremely detrimental effects on the human body.[2] Owing to social disengagement and decreased professional commitments, the sleep pattern is expected to improve in the population. Regular physical activity undertaken by people has both physical and mental health benefits which might also have been affected by territorial restrictions. Further, restrictions on transport of consumer goods is expected to affect the availability, and in turn, the consumption of products such as cigarettes, alcohol, fast food.
There have been many instances in the past wherein enforced restrictions on the public because of natural disasters (like tornados, hurricanes, earthquakes) or man-made disasters (war like situations) have had major implications like scarcity of resources and lifestyle modifications, which has consequently affected the overall health of the populations.[3,4,5]
Therefore, we sought to explore and analyze the changes in diet and lifestyle during COVID-19 lockdown among the Indian population. It is pertinent to know the extent and impact of this change. Secondly, this data can be correlated with the associated risk of developing chronic lifestyle diseases in the urban Indian population.[6] With the ongoing pandemic, the data needs to be investigated further in larger scale and extensive population studies.
Subjects and Methods
Survey methodology
We used a web-survey to obtain data from urban adults having access to the internet about eating habits and lifestyle during the COVID-19 lockdown. Territorial coverage of our web-survey extended to the states of Punjab, Himachal Pradesh, Haryana, Delhi, and Chandigarh, The survey was conducted from 11th to the 20th of May 2020. The survey was disseminated through WhatsApp. This administrative method provided a statistical collective in which the population parameters were uncontrolled. However, it successfully fulfilled the research objectives by facilitating the wide dissemination of the survey questionnaire during a time period of many territorial restrictions because of the lockdown.
The questionnaire
The questionnaire was built using Google Forms. The questionnaire consists of a set of 20 questions which included personal and demographic data (four questions: age, gender, current employment); dietary habits information: (six questions: alcohol, smoking, junk food); physical activity (two questions); other lifestyle changes (seven questions: stress levels, sleeping pattern, screen usage, weight changes). A feedback question was included at the end to enquire the overall perception in the population regarding their new lifestyle. The full version of the questionnaire is available as Appendix A. The study was conducted according to regulations outlined by national authorities and the Declaration of Helsinki (2000). Participants completed the questionnaire directly connected to the Google platform. Participants' personal information, including names, email, and residential addresses were not asked for to maintain anonymity and protect confidentiality. The anonymous nature of the web-survey does not allow any sensitive information to be traced in any way. Hence, the present web-survey study does not require approval from the Ethics Committee. Once completed, the final database was downloaded as a Microsoft Excel sheet for further analyses.
Statistical analyses
The collected data were represented as ordinal variables, and re-coded as numeric scalar values to undertake frequency distribution analyses. Descriptive statistical tests were performed to obtain mean, 95% confidence intervals, standard deviation, and skewness for each variable. The Shapiro–Wilk test was undertaken to investigate the distribution of the variables. All the variables had skewed distribution and failed the tests of normality, hence, medians and interquartile ranges were obtained and non-parametric statistical tests were used for further analyses. Related-samples marginal homogeneity test was employed to test the difference between frequency distribution pre- and during COVID-19 lockdown. Related-samples Wilcoxon signed rank test was employed to test the median of differences between the variables pre- and during the lockdown. Results were significant for P value < 0.05. Statistical analysis was performed using SPSS ver. 26.0 (IBM, Chicago, IL, USA).
Results
The survey was concluded on the 20th of May, 2020 and the collected data were analyzed. The survey was sent to 1,200 people, of which a total of 1,008 participants completed the questionnaire aged between 18 and 81 years (median - 24). The male respondents represent 571 (56.6%) of the population.
The overall changes (decrease/increase) reported by the total population for the lifestyle and dietary variables have been reported in Figure 1.
Figure 1.
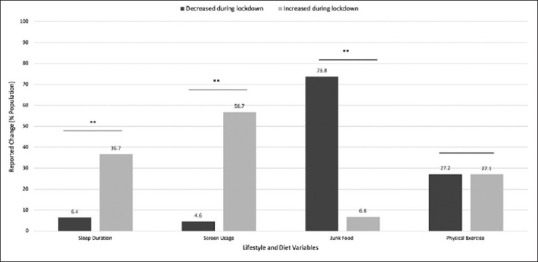
Bar graph showing percentage of total population reporting a change in lifestyle and dietary habits before and during lockdown. Values are expressed as percentage population reporting either a decrease or increase during the lockdown (** implies statistical significance, P < 0.001) All variables were statistically verified using the Wilcoxon Signed Rank test (p < 0.001) and Related-samples Marginal Homogeneity test (p < 0.001)
In particular, sleep hours and screen usage have significantly increased while junk food intake has significantly decreased. With physical activity, no significant difference was observed in the percentage of population that increased (27.1%) or decreased (27.2%) their physical exercise during the COVID-19 lockdown (P = 0.554). Due to an interchange of physical exercise habits between previously active and inactive subpopulations, it was found that the P values obtained from statistical analyses performed on the results were not significant.
Changes reported in the subpopulation experiencing work related stress because of the lockdown is summarized in Figure 2.
Figure 2.
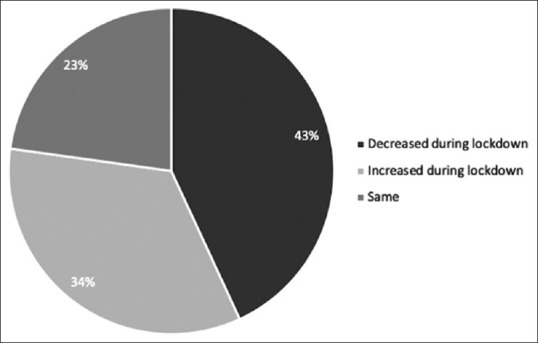
Pie-chart summarising reported change in work related stress due to the COVID-19 lockdown. Values are expressed as the percentage of subpopulation. The change was statistically verified using the Wilcoxon Signed Rank test (p < 0.001) and the Friedman's Two Way Analysis of Variance by Ranks test (Test statistic = -16.40, P < 0.001)
A total of 622 participants reported experiencing work-related stress before lockdown. More than three quarters of this subpopulation feel a change in their work-related stress during the lockdown: 268 (43.1%) reported a decrease, 212 (34.1%) report an increase in work-related stress levels during the lockdown period as shown in Figure 2.
Changes reported by the smoking and alcohol-consuming subpopulations because of the lockdown are summarized in the table below [Table 1]
Table 1.
Tables summarising change in smoking habits [Table 1.1] and alcohol consumption [Table 1.2] during the COVID-19 lockdown. Values are expressed as number of participants and percentage population reporting either a decrease or increase during the lockdown. The change was statistically verified using the Wilcoxon Signed Rank test (P < 0.001) and Related-samples Marginal Homogeneity test (P < 0.001)
| Table 1.1 | ||
|---|---|---|
| Smoking pre- lockdown | Smoking during lockdown | |
| I don’t smoke | 877 (87%) | 951 (94.3%) |
| Party smoker | 66 (6.5%) | 24 (2.4%) |
| At least 1 cigarette per day | 65 (6.4%) | 33 (3.3%) |
| Table 1.2 | ||
| Alcohol pre- lockdown | Alcohol during lockdown | |
| I don’t drink | 534 (53%) | 797 (79.1%) |
| Occasional/social drinker | 433 (43%%) | 178 (17.7%) |
| Regular drinker, <60 ml per day | 18 (1.8%) | 19 (1.9%%) |
| Regular drinker, >60 ml per day | 23 (2.3%) | 14 (1.4%) |
Smoking habits have been significantly reduced during lockdown as shown in Table 1.1. Of the 131 smoking subpopulation, 99 participants (75.5%) reported a reduced or no smoking at all during the lockdown. There was a reported significant decrease in the alcohol consumption during the COVID-19 lockdown as shown in the Table 1.2. 41 people reported drinking regularly before lockdown. Of these, 19 (46.3%) people indicated a decrease in their regular alcohol consumption during the lockdown.
Discussion
In this web-based survey to understand the impact of lockdown on lifestyle and dietary changes in the Indian population, we found a significant increase in screen usage and sleep duration and a significant decrease in junk food consumption among the participants. Risks associated with increased screen usage manifested as low levels of physical activity and sedentary behavior, represented by screen time of just >2 h/day have been well documented.[7,8,9] The significant increase in the screen usage during lockdown is theorized to be because of an abundance of leisure time, lack of outdoor activity, and social disengagement. Seeing this change in the degree of screen usage, an intervention is recommended to prevent subsequent long-term effects. The recommended sleeping time period per day has been found to be more than 6 h.[10] The increase in sleeping times can be attributed to an overall decrease in work-related stress, as well as decreased social and professional commitments. Raising awareness regarding the detrimental effects of sleep loss among the population could lead to the long-term maintenance of these improved sleeping patterns and in turn, improve overall health. During the lockdown, to enforce social distancing and prevent stage III transmission, all restaurants, cafes, and fast food joints for dining and take away were closed. The consequent unavailability of junk food as well as health and safety concerns led to a steep decrease in its consumption during lockdown. Henceforth, if this decrease in fast food consumption is maintained, and instead a healthy diet is adopted, it would be highly beneficial in preventing chronic health concerns associated with calorifically high and nutritionally low junk food.[11,12,13,14,15] We have observed a decrease in work-related stress in the participants. The possible reasons for this could be the partial/full transition to working remotely, and/or shift based work schedules during the lockdown. If such a mode of work is adapted by employers for a longer period of time, this could consequently lead to an overall decrease in work-related stress levels experienced by urban populations, and in turn put them at a lower risk for associated comorbidities.[16,17,18] An overall decrease in the frequency of smoking was found in the participants during the lockdown. We hypothesize a number of factors that can explain this decrease. These are: 1) Inaccessibility to local shops due to public lockdown and non-availability of cigarettes because of shutdown of all businesses; 2) Discouragement from smoking in the company of immediate family during extended time period of home isolation; 3) Fear induced in smokers of the increased risk of respiratory distress and mortality from COVID-19.[19] A change in smoking habits in regular smokers, if sustained long term, would lead to a decreased risk of developing chronic illnesses in the subpopulation. There is robust evidence that quitting smoking is beneficial and that the excess risk declines rapidly and significantly, with the risk approaching the level of never-smokers within about 10 years of quitting.[20] Cessation of smoking is associated with a reduced risk of many chronic health diseases and is associated with an increased life expectancy.[21] An overall decrease in alcohol consumption was observed during the lockdown. The nationwide lockdown led to the shutdown of all businesses including liquor shops. Additionally, online sale of liquor is currently prohibited in India (As of 1st June, 2020). Informing people who drink alcohol, especially regular consumers, of the risks associated with excessive alcohol consumption both in clinical contacts and through public health policy, might help to prevent infections in general and in particular such diffusive and invasive respiratory viruses as COVID-19.[22,23] The decrease observed in alcohol consumption, if sustained long term is expected to be beneficial by reducing the risk of developing chronic illnesses that have been correlated with excessive alcohol abuse. An increase in regular physical activity was observed in the sub-population that did not engage in regular exercise before lockdown, possibly because of ample free time or a less busy lifestyle during the lockdown. On the other hand, the participants engaging in regular physical exercise before lockdown presumably at gyms or fitness suites, were less likely to continue their active lifestyle during lockdown likely due to closure of these facilities and unavailability of the fitness equipment in the home environment. Sufficient health benefits have been seen in previously sedentary people who adopted regular physical exercise as their new lifestyle.[24] Furthermore, taking into account the many benefits of regular physical exercise on the immune system, it is suggested that people be made aware of the importance of consistent physical activity so that such a lifestyle can be maintained for long-term positive effects.[25] Another aspect that need attention is to understand the psychological aspect of the pandemic and enforced alteration of lockdown among individuals.[26]
The main limitation of the study is represented by the possibility of misrepresentation of the data because of the self-reporting based questionnaire format, although similar methodologies have been employed in various studies. Moreover, the limited number of participants might not be able to accurately represent the changes in the overall North Indian population. Additionally, since these lifestyle and dietary modifications were enforced upon the participants because of the lockdown, and not undertaken voluntarily, their long-term sustenance cannot be correctly estimated. The options provided for the participants in the questionnaire, were composed in such a manner as to be easily understood by the respondents. Consequently, the data collected in the survey was subjective and semi-quantitative. The reach of the survey was limited to working class, urban, North-Indian individuals with access to the internet, hence the study runs a risk of bias and should not be seen as representative of the overall Indian population. A strength of our study was represented by the fact that the survey was conducted during the most critical period of the COVID-19 pandemic in India, 3 weeks after the nationwide lockdown.
With this study, we sought to identify individual and cumulative risk factors for lifestyle disorders and analyze the effect of COVID-19 lockdown induced alterations on them. Preliminary data from the present study as well as similar studies suggest that the new remote work environments and movement restrictions have brought about changes in day-to-day habits leading to a more sedentary and confined lifestyle among the surveyed population. There is a need for primary care physicians to engage people for appropriate lifestyle counselling and adaptive skills to cope with the COVID-19 pandemic and subsequent restrictions. The changes were significant even in the limited time frame of the study. More comprehensive studies with larger population cohorts analysing similar risk factor patterns over a long duration may form a relevant knowledge base for primary care physicians in their practice going forward.
Conclusion
This survey brought out the impact of COVID-19 lockdown on lifestyle and dietary changes in the Indian population. A significant increase was observed in screen usage and sleep duration while a significant decrease was evident in junk food consumption among the participants. An overwhelming majority of participants report feeling positive about the changes made in their lifestyle because of the lockdown and would like to continue adhering to these changes for an extended period of time. Such positive lifestyle changes, if sustained over a longer period of time will be reflected in a significantly decreased risk of developing chronic illnesses. The data needs to be studied further in more extensive studies for more a more robust understanding.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Key Messages
Massive impact of territorial restriction imposed during the COVID-19 lockdown in India
Significant effect on various lifestyle and dietary consumption habits.
Significant decrease in work-related stress, junk food, alcohol, and cigarette consumption
Most pronounced increase in screen usage.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Velavan TP, Meyer CG. The COVID-19 epidemic. Trop Med Int Health. 2020;25:278–80. doi: 10.1111/tmi.13383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia. 2012;55:2895–905. doi: 10.1007/s00125-012-2677-z. [DOI] [PubMed] [Google Scholar]
- 3.Giorgadze T, Maisuradze I, Japaridze A, Utiashvili Z, Abesadze G. Disasters and their consequences for public health. Georgian Med News. 2011;194:59–63. [PubMed] [Google Scholar]
- 4.Trevisan M, Celentano E, Meucci C, Farinaro E, Jossa F, Krogh V, et al. Short-term effect of natural disasters on coronary heart disease risk factors. Arteriosclerosis. 1986;6:491–4. doi: 10.1161/01.atv.6.5.491. [DOI] [PubMed] [Google Scholar]
- 5.Ghosal S, Sinha B, Majumder M, Misra A. Estimation of effects of nationwide lockdown for containing coronavirus infection on worsening of glycosylated haemoglobin and increase in diabetes-related complications: A simulation model using multivariate regression analysis. Diabetes Metab Syndr. 2020;14:319–23. doi: 10.1016/j.dsx.2020.03.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Willett WC, Koplan JP, Nugent R, Dusenbury C, Puska P, Gaziano TA. 2nd ed. The International Bank for Reconstruction and Development/The World Bank; 2006. Prevention of chronic disease by means of diet and lifestyle changes. Disease Control Priorities in Developing Countries. [PubMed] [Google Scholar]
- 7.Costigan SA, Barnett L, Plotnikoff RC, Lubans DR. The health indicators associated with screen-based sedentary behavior among adolescent girls: A systematic review. J Adolesc Health. 2013;52:382–92. doi: 10.1016/j.jadohealth.2012.07.018. [DOI] [PubMed] [Google Scholar]
- 8.Oliveira RGd, Guedes DP. Physical activity, sedentary behavior, cardiorespiratory fitness and metabolic syndrome in adolescents: Systematic review and meta-analysis of observational evidence. PLoS One. 2016;11:e0168503. doi: 10.1371/journal.pone.0168503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Loh K, Redd S. Understanding and preventing computer vision syndrome. Malays Fam Phys. 2008;3:128–30. [PMC free article] [PubMed] [Google Scholar]
- 10.Chaput JP, Dutil C, Sampasa-Kanyinga H. Sleeping hours: What is the ideal number and how does age impact this? Nat Sci Sleep. 2018;10:421–30. doi: 10.2147/NSS.S163071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fister K. Junk food advertising contributes to young Americans' obesity. BMJ. 2005;331:1426. doi: 10.1136/bmj.331.7530.1426-c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bandini LG, Vu D, Must A, Cyr H, Goldberg A, Dietz WH. Comparison of high-calorie, low-nutrient-dense food consumption among obese and non-obese adolescents. Obes Res. 1999;7:438–43. doi: 10.1002/j.1550-8528.1999.tb00431.x. [DOI] [PubMed] [Google Scholar]
- 13.Khatib O. Noncommunicable diseases: Risk factors and regional strategies for prevention and care. East Mediterr Health J. 2004;1:778–88. [PubMed] [Google Scholar]
- 14.Zhang Y, Vittinghoff E, Pletcher MJ, Allen NB, Al Hazzouri AZ, Yaffe K, et al. Associations of blood pressure and cholesterol levels during young adulthood with later cardiovascular events. J Am Coll Cardiol. 2019;74:330–41. doi: 10.1016/j.jacc.2019.03.529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Grillo A, Salvi L, Coruzzi P, Salvi P, Parati G. Sodium intake and hypertension. Nutrients. 2019;11:1970. doi: 10.3390/nu11091970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Spieker L, Noll G. Pathophysiologische Herz-Kreislauf-Ver¨anderungen bei Stress und De- pression. Therapeutische Umschau. 2003;60:667–72. doi: 10.1024/0040-5930.60.11.667. [DOI] [PubMed] [Google Scholar]
- 17.Kulkarni S, O’Farrell I, Erasi M, Kochar M. Stress and hypertension. WMJ. 1998;97:34–8. [PubMed] [Google Scholar]
- 18.Vlastelica M. Emotional stress as a trigger in sudden cardiac death. Psychiatr Danub. 2008;20:411–4. [PubMed] [Google Scholar]
- 19.Brake SJ, Barnsley K, Lu W, McAlinden KD, Eapen MS, Sohal SS. Smoking upregulates angiotensin-converting enzyme-2 receptor: A potential adhesion site for novel coronavirus SARS-CoV-2 (Covid-19) J Clin Med. 2020;9:841. doi: 10.3390/jcm9030841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chen Z, Boreham J. Seminars in Vascular Medicine. Vol. 2. Thieme Medical Publishers; 2002. Smoking and cardiovascular disease; pp. 243–52. [DOI] [PubMed] [Google Scholar]
- 21.Taylor DH, Jr, Hasselblad V, Henley SJ, Thun MJ, Sloan FA. Benefits of smoking cessation for longevity. Am J Public Health. 2002;92:990–6. doi: 10.2105/ajph.92.6.990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bosch AA, Biesbroek G, Trzcinski K, Sanders EA, Bogaert D. Viral and bacterial interac-tions in the upper respiratory tract. PLoS Pathog. 2013;9:e1003057. doi: 10.1371/journal.ppat.1003057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Testino G, Pellicano R. Alcohol consumption in the Covid-19 era. Minerva Gastroenterol Dietol. 2020;66:90–2. doi: 10.23736/S1121-421X.20.02698-7. [DOI] [PubMed] [Google Scholar]
- 24.Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: The evidence. CMAJ. 2006;174:801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gupta SK, Lakshmi PV, Kaur M, Rastogi A. Role of self-care in COVID-19 pandemic for people living with co-morbidities of diabetes and hypertension. J Family Med Prim Care. 2020;9:549–01. doi: 10.4103/jfmpc.jfmpc_1684_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Singhai K, Swami MK, Nebhinani N, Rastogi A, Jude E. Psychological adaptive difficulties and their management during COVID-19 pandemic in people with diabetes mellitus [published online ahead of print, 2020 Aug 23] Diabetes Metab Syndr. 2020;14:1603–5. doi: 10.1016/j.dsx.2020.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]