

Highlights
-
•
Policies that support physical activity (PA) in the school-setting have promise but their impact is poorly understood.
-
•
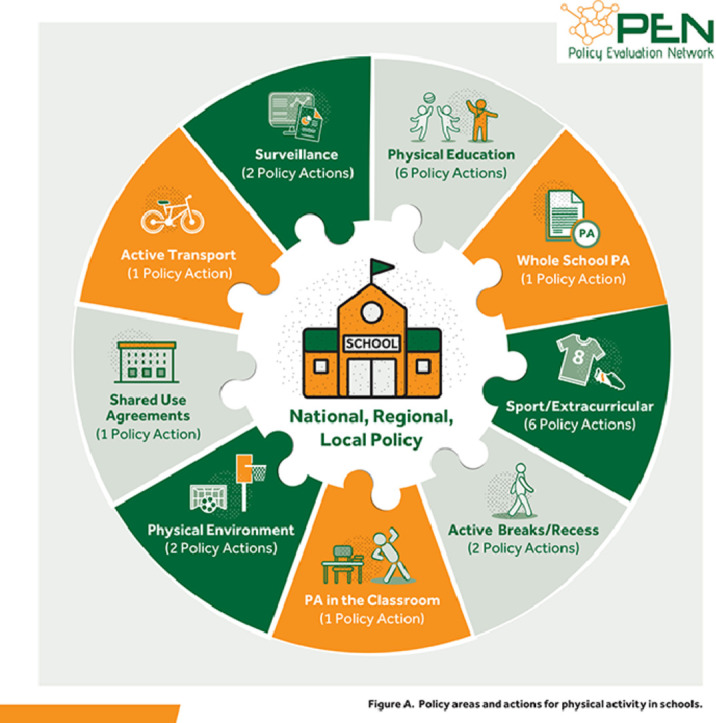
Nine policy action areas for which there was evidence of impact were identified. These were whole-school PA policy, physical education, sport/extracurricular PA, classroom-based PA, active breaks, physical environment, shared use agreements, active school transport and surveillance.
-
•
Evidence supports the effectiveness of PA policy actions within the school-setting but cautions a “one-size fits all” approach.
-
•
Further evaluation of policy implementation to maximize translation into practice is required.
-
•
Greater clarity regarding terminology, measurement, and methods for evaluation of policy interventions is needed, and suggestions provided.
Keywords: Evaluation, Physical activity, Policy, School, Systematic review
Abstract
Background
Despite the well-established health benefits of physical activity (PA) for young people (aged 4–19 years), most do not meet PA guidelines. Policies that support PA in schools may be promising, but their impact on PA behavior is poorly understood. The aim of this systematic review was to ascertain the level and type of evidence reported in the international scientific literature for policies within the school setting that contribute directly or indirectly to increasing PA.
Methods
This systematic review is compliant with Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. Six databases were searched using key concepts of policy, school, evaluation, and PA. Following title and abstract screening of 2323 studies, 25 progressed to data synthesis. Methodological quality was assessed using standardized tools, and the strength of the evidence of policy impact was described based on pre-determined codes: positive, negative, inconclusive, or untested statistically.
Results
Evidence emerged for 9 policy areas that had a direct or indirect effect on PA within the school setting. These were whole school PA policy, physical education, sport/extracurricular PA, classroom-based PA, active breaks/recess, physical environment, shared use agreements, active school transport, and surveillance. The bulk of the evidence was significantly positive (54%), 27% was inconclusive, 9% was significantly negative, and 11% was untested (due to rounding, some numbers add to 99% or 101%). Frequency of evidence was highest in the primary setting (41%), 34% in the secondary setting, and 24% in primary/secondary combined school settings. By policy area, frequency of evidence was highest for sport/extracurricular PA (35%), 17% for physical education, and 12% for whole school PA policy, with evidence for shared use agreements between schools and local communities rarely reported (2%). Comparing relative strength of evidence, the evidence for shared use agreements, though sparse, was 100% positive, while 60% of the evidence for whole school PA policy, 59% of the evidence for sport/extracurricular PA, 57% of the evidence for physical education, 50% of the evidence for PA in classroom, and 50% of the evidence for active breaks/recess were positive.
Conclusion
The current evidence base supports the effectiveness of PA policy actions within the school setting but cautions against a “one-size-fits-all” approach and emphasizes the need to examine policy implementation to maximize translation into practice. Greater clarity regarding terminology, measurement, and methods for evaluation of policy interventions is needed.
Graphic abstract
1. Introduction
Physical inactivity is the 4th leading risk factor for premature mortality worldwide.1 To improve public health and to prevent non-communicable diseases, the World Health Organization (WHO) physical activity (PA) guidelines recommend at least 150 min of moderate-to-vigorous PA (MVPA) per week for adults and at least 60 min of daily MVPA for children.2 Despite all the evidence of benefits, epidemiological data indicate that 28% of adults and 81% of children and adolescents globally do not meet PA recommendations.3,4 Research consistently shows that PA levels decline during adolescence,5, 6, 7, 8 that boys are more physically active than girls9,10 and that PA habits developed in childhood track into adulthood.11, 12, 13, 14, 15 Therefore, methods to effectively address such high levels of inactivity in children are urgently needed.
A substantial body of literature exists on solutions that can address the inactivity challenge. Guided by an ecological approach, this literature points to a multi-level response that addresses personal, environmental, and policy factors.16 Approaches that address all these levels have been used previously to successfully reduce the use of tobacco products.17 There has been an exponential growth in policies targeting the upstream determinants of health behaviors to reduce the burden of lifestyle-related diseases like physical inactivity.18 Examples include WHO's global action plan for the prevention and control of non-communicable diseases,19 which included a global target of reducing population prevalence of inactivity by 10% by 2020. More recently, WHO's global action plan on PA recommended a systems-based approach and identified 20 policy actions for enhancing population levels of PA, including whole-of-school approaches.20 Thus, understanding the systemic drivers of inactivity is paramount because in doing so we can hope to help promote PA not only to improve health but also to address the global syndemic, or the combined pandemics of obesity, undernutrition and climate change and their threats to human health and survival.21
Schools are an important setting because they reach the majority of children and adolescents, who spend a substantial amount of time in this setting. Whole-of-school approaches for the promotion of PA are recommended,20,22 yet there is a lack of studies focusing explicitly on the evidence for PA policies within this setting. Under whole-of-school approaches, the policy level is an important component. An article by Lounsbery23 explains how the presence or absence of policies related to PA, their nature (mandatory vs. recommended) and their level of implementation success can have substantial and direct implications for children's PA. They also articulate the different levels and key policy makers within each level, for example at national level—the minister or governor, at regional level—the school board, and at school level—the principal, and at classroom level—the teacher. However, PA policy implementation is not straightforward. PA policies vary widely and generally lack specificity, implementation, accountability, and funding.24 There is a need to investigate the status of the evidence for policies that increase PA within the school setting.
For the purpose of this paper, policies are defined as “decisions, plans, and actions that are enforced by national or regional governments or their agencies (including at the local level) which may directly or indirectly achieve specific health goals within a society”.18 The role of policy is to change systems instead of individuals, and in doing so, create supportive contexts in which programs and environments collectively can reduce non-communicable diseases, including obesity. Importantly, policy interventions are not to be confused with other types of program or environmental interventions; policy interventions provide the framework in which the programs or environmental changes are tendered, developed, financed, or implemented.25
Several frameworks exist that advocate for the use of policy as an instrument to promote health within the school setting. These frameworks mainly focus on a broad definition of health; however, they provide a useful conceptual starting point for reviewing the potential direct and indirect effects of policy on PA. The WHO published the diet and physical activity strategy school policy framework to guide policymakers at national and sub-national levels in the development and implementation of school policies.26 This framework highlighted that children are not immune to the negative consequences of physical inactivity, and it called for urgent action to effect change. This action included the development and implementation of policies that promote PA. More recently, the Creating Active Schools Framework was designed using a “systems” approach to identify all components of a whole school PA approach.27 This framework presents the school as a complex adaptive system, one that places an “active school” as central to the school's beliefs, customs, and practices that drive school policy. Through engaging with key stakeholders—children, teachers, management, parents, and the wider community, an “active school” creates the necessary physical and social environments within which schools can facilitate different types of PA opportunities.
Although these frameworks provide a useful theoretical background on PA policy within the school, the evidence presented in them is mainly descriptive; it explores policy content, presence, and level of implementation. No evidence on the effectiveness of policy, nor any reference to the policy evidence-base, is evident within these framework documents. This represents a gap in our knowledge. Thus, the rationale for this systematic review is aligned to the work of the Policy Evaluation Network (PEN; https://www.jpi-pen.eu/), which aims to develop a consolidated approach to policy evaluation across Europe by developing and prioritizing an agreed-upon set of indicators, measured using harmonized instruments that ideally can be used by existing monitoring and surveillance systems.18 Although research in PA is still mainly focused on its health effects (Type 1) or on the effectiveness of specific PA interventions (Type 2), there has been limited growth in research on policy and PA (Type 3).28,29 Although we are developing a better knowledge of PA policy, there are gaps in our understanding and evidence for the effectiveness of PA policies.30 Therefore, the purpose of this paper was to evaluate the status of the evidence base for the impact of policy on PA outcomes within the school setting.
2. Methods
The review is structured according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA).31 It has been registered with the International Prospective Register of Systematic Reviews (PROSPERO, CRD42020156630) and the study protocol has been published.32
2.1. Search strategy
A systematic search of the following electronic databases (limited to titles and abstracts) was conducted during November 2019 through January 2020: MEDLINE (EBSCO), SportDiscus, CINAHL, Cochrane, Web of Science, and Scopus. Search terms are presented in Table 1. Search results were limited to articles that were identified through a systematic stepwise identification approach, starting with screening of titles and abstracts. Duplicate studies and studies not in the English language were removed. This search was supplemented by manual reference checks of original reviews that were found in the systematic search.
Table 1.
Search terms.
| Keyword | Synonyms |
|---|---|
| Policy | (MH “Policy”) OR (MH “Public Policy”) OR (MH “Policy Making”) OR “policy” OR “policies” OR “national policy” OR “national framework” OR “policy framework” OR “policy action” OR “legislation” OR “strategy” OR “policy making” |
| Physical activity | (MH “Exercise”) OR (MH “Sedentary Behavior”) OR “physical activit*” OR “physical inactivity” OR “play” OR “physical education” OR “sedentar*” OR “sitting” OR “healthy lifestyle” OR “health initiative” |
| Impact | “evaluat*” OR “impact” OR “appraisal” OR “effect*” OR “assessment” |
| Whole of school approach | “Whole-of-school” OR “Whole School” OR “Whole of School” OR “WSCC” OR “school intervention” OR “school based intervention” OR “school initiative” OR “school based initiative” OR “school program*” OR “School health” OR “Wellness” OR “well-being” |
Abbreviations: MH = medical subject heading major topic; WSCC = whole school, whole community, whole child.
2.2. Eligibility criteria
Studies were included based on criteria for (a) study type, (b) participants/population, (c) policy exposure, and (d) outcomes.
-
(a)
The following study types were eligible for inclusion: (1) reviews and (2) empirical studies. Reviews (used to inform the Introduction and Discussion sections of this paper) could include systematic, scoping, and realist methods, all of which must have used a comprehensive search strategy. In addition, reviews must have reported an analysis of original research. Empirical studies could include randomized control studies, non-randomized studies, cohort studies, qualitative studies, and mixed-method designs.
-
(b)
Included review studies must have targeted children and/or adolescents, albeit not exclusively within the school setting or with this population. For empirical studies, the study must have targeted children, adolescents, and teachers in the school setting only.
-
(c)
The authors are not aware of any reviews to date that have exclusively assessed the impact of PA policy in the school setting. Therefore, included reviews did not need to meet this aim, but they did need to address some policy-related component that promoted PA within the school setting. Empirical studies must have referenced the impact of policy in the school setting. “Direct” policy refers to policies where the primary aim is improving the PA environment and increasing PA participation. “Indirect” policy refers to policies where the primary aim is not to increase PA levels, but this may occur as a co-benefit of successful implementation (e.g., car-free school streets).
-
(d)
All study designs (reviews, empirical evidence) had to include the one or both of the following outcome(s): (1) a change in PA (or proxy, i.e., fitness), assessed by means of self-report, wearable devices (e.g., accelerometer) or observational measure (e.g., System for Observing Fitness Instruction Time33) and (2) a change in features of the physical and social environment (e.g., facilities, equipment, action plans, programs) hypothesized to lead to changes in PA outcomes as a result of a policy intervention. Empirical studies were excluded if a direct or indirect form of policy intervention was not identifiable or if there was no information provided regarding the effects of the policy under consideration on the desired outcomes.
Our systematic review was supplemented by a targeted search of the grey literature, although this was not exhaustive. Book chapters and policy documents issued by major national and international stakeholder organizations (e.g., WHO) referred to in the reference lists of included papers were consulted in order to inform the Introduction and Discussion sections of the paper.
2.3. Screening of studies
Two of the authors (KV and LK) screened all retrieved titles and abstracts using the systematic review software Rayyan.34 After initial title and abstract screening, full texts were retrieved and crosschecked against the inclusion criteria by two of the authors (KV and LK). When necessary, eligible studies were also crosschecked by a third author (EGB). Discussion was held where the authors disagreed on inclusion of studies until agreement was reached.
2.4. Data extraction
Data were extracted using pre-defined criteria from all study designs (reviews, empirical studies, and grey literature/other). Data included type of study design, country of origin, demographics related to the school setting and policy description and content. To allow for the interpretation of the impact of the policy identified, information on changes in the outcomes of interest (PA and/or physical/social environment) was also collected. All data extraction was conducted by 2 authors (KV and LK) and checked and expanded by a third reviewer (EGB).
2.5. Quality assessment process
Risk of bias was assessed by 1 reviewer (EGB) and checked by another (BC). Discrepancies were resolved by consensus, where necessary, in consultation with a third researcher (CBW). Similar to the methods used by Messing et al.,35 we calculated the percentages of criteria met per study based on the criteria applicable to the type of study design. Studies were not ranked by methodological quality. The quality of the included quantitative studies was assessed by means of an adapted Downs and Black checklist tool.36 The Assessment of Multiple Systematic Reviews scale was used for the assessment of systematic reviews and comprehensive reviews, including reviews of reviews.37 The Critical Appraisal Skills Programme qualitative checklist was used to assess the quality of included qualitative studies.38 All tools were slightly modified to meet the aims and context of our review.
2.6. Data analysis
A narrative synthesis of the included empirical studies was used to interpret and analyze the data. Extracted PA outcome data were tabulated to determine the impact of policy on PA behavior and/or environment. This data were also used to outline how policy areas were defined, delineated, and identified (e.g., if a single study dealt with multiple policy areas). Evidence on the effectiveness of policy was described using the method described in Panter et al.,39 where the observed effects of policy actions were coded as “significantly-positive” (+), “significantly-negative” (–), “no significance test” (?), or “inconclusive” (0). The number of codes per policy area is presented to show differences in frequency with which each area was studied. To allow for relative comparison, the strength of evidence is presented as a percentage of positive, negative, untested, or inconclusive codes found within each policy area or policy action, where relevant. For the purpose of clarity, Table 2 describes the terms used in the presentation of the results, and Fig. 1 shows the relationship between concepts.
Table 2.
Inter-relations among policy-related concepts used in this review.
| Name | Description |
|---|---|
| Intervention | The policy, program, or environmental change used to promote PA. |
| PA program | Specific opportunities for the purpose of increasing PA behavior, attitudes, or knowledge in a target population for a specific period of time. |
| PA environment | Relevant physical and social features of the school environment that are hypothesized to support changes in PA behavior. |
| PA policy | Purposeful decisions, plans, and actions made by voluntary or authoritative actors in a system designed to create system-level change that may directly or indirectly impact on PA, and that are enforced by national or regional governments or their agencies (including at the local school level). |
| Policy domain | Settings in which policies are implemented (e.g., primary schools, secondary schools, or combined primary and secondary schools). |
| Policy level (relevant to schools) | These are the level in the system where policies can be targeted. This includes laws, state-, district-, and school-level codes or regulations, or class-level rules. |
| Policy area | Specific content areas for policy actions within the school setting (e.g., physical education). |
| Policy action | Actual options selected by policymakers. Policy actions are specific actions put into place by any level of government and associated agencies in order to achieve the PA objective directly or indirectly. They may be written into broad strategies, action plans, official guidelines and notifications, calls to action, legislation, or rules and regulations. An action may have its own exclusive policy document or may be part of a larger document. |
Abbreviation: PA = physical activity.
Fig. 1.

Diagram of inter-relations among policy-related concepts used in this review. PE = physical education.
After data extraction on review papers and multi-component empirical studies that met the inclusion criteria was completed, 17 papers (8 reviews and 9 multi-component empirical studies) were not included in data synthesis. The rationale for this was the lack of clarity in attributing evidence of impact on PA to policy. Details on these 8 reviews are listed in Supplementary Table 1,40, 41, 42, 43, 44, 45, 46, 47 with a further 9 multi-component studies detailed in Supplementary Table 2.48, 49, 50, 51, 52, 53, 54, 55, 56 Reference lists from these papers were used to identify additional studies that may have been missed in the initial database search. Furthermore, recurring headings in narrative reviews and book chapters were used to develop the policy areas used in the data synthesis and to frame the Discussion section of this manuscript.
3. Results
3.1. Characteristics of included studies
In total, 3035 publications were identified, of which 712 were removed as duplicates. The remaining 2323 titles and abstracts were screened; with 2195 removed, leaving 128 full texts for review. The main reasons for exclusion based on title or abstract were that the studies were not PA related (60%, n = 1317) or the studies did not describe a policy intervention (12%, n = 264). An additional 91 studies were excluded based on a full-text reading. A total of 5 more papers were included following reference checks, leaving a total of 25 papers included for data synthesis (Fig. 2). The most common reasons for excluding studies after full screening were that there was no evidence of a policy or that the policy impact on PA was not clear. Papers based on research in a childcare setting were excluded on population grounds, in accordance with our definition of what constitutes a school. Additional details on these papers, as well their quality ratings, are described in Supplementary Table 3.
Fig. 2.

Study inclusion flowchart.
3.2. Study design and location
Of the 25 studies included, 44% were pre–post studies, 24% were quasi-experimental, 24% were cross-sectional, 4% were qualitative, and 4% were randomized experiments. Most studies were conducted in the USA (60%), followed by Canada (16%), the UK (8%), Australia (8%), Slovenia (4%), and Belgium (4%). Quality ratings ranged from 42% to 92%, with most studies obtaining a rating of 60% or more, suggesting at least moderate methodological quality according to current standards and conventions.
3.2.1. Population
Included studies were based in either primary (n = 12), secondary (n = 8), or combined primary and secondary (n = 5) school settings and represented a sample of more than 370,000 students (an approximation from 24 studies reporting sample size), with a range of 120 to 220,000 students across studies. The reported age of included students ranged from 4.0 to 19.0 years. The number of schools sampled in each study ranged from 4 to 450, with a combined total of 1984 schools across all included studies (25 studies reporting the number of schools).
3.2.2. Exposure
Studies typically reported on state, district, or local public policies (e.g., related to the implementation of physical education (PE) standards). Others reported on organizational policies (e.g., shared use agreements (SUAs) between schools and local communities) or on school-level regulations relating to PA provision during curricular time. In the area of extracurricular provision, school sport policy was paramount. Two models for the provision of school sports were frequently mentioned or compared: interscholastic/intervarsity (IS) and intramural (IM).57, 58, 59, 60, 61 IS sports refer to sports played between schools and are generally more competitive.60 For this reason, places on the team are typically limited. By contrast, IM sports refer to sports played within the school institution, and participation is typically inclusive of all skill levels.
3.2.3. Outcome measures
The included studies used a range of PA outcome measures, including device-measured (n = 10), self-report methods (n = 11), observational methods (n = 6), and qualitative methods (n = 3). Device-measured methods included accelerometers (n = 6), pedometers (n = 2), fitness test batteries (n = 1) and, other, including Geographical Information Systems, the Measuring Wheel method and the Healthy Afterschool Program Index-PA (n = 1). In studies using accelerometers, MVPA, moderate PA, and vigorous PA (VPA) were the most commonly reported outcomes. Observational methods were used in 6 studies, with 2 outcome measures being used across these studies. These were the System for Observing Play and Leisure in Youth (n = 4) and the System for Observing Play and Recreation in Communities (n = 2). A range of self-report methods was used (n = 20 surveys/questionnaires), including the school PA policy assessment instrument (S-PAPA). Qualitative methods consisted of structured or semi-structured interviews (n = 3). Details on the outcome measures for each study are provided in Supplementary Table 3.
3.3. Policy areas and policy actions
3.3.1. Summary findings
The primary search identified a total of 9 policy areas, with 22 specific policy actions for which there were 82 evidence codes (Table 3). The bulk of the evidence, 54% (n = 44 codes) was “significantly positive”. A total of 27% (n = 22 codes) of evidence was “inconclusive”, 9% (n = 7 codes) of evidence was “significantly negative”, and 11% (n = 9 codes) indicated that there was “no significance test”. When analyzed by education sector, frequency of evidence, 41% (n = 34 codes) was highest in primary school settings. A total of 34% (n = 28 codes) of the evidence occurred in secondary school settings, and 24% (n = 20 codes) occurred in combined school settings (due to rounding, some numbers add to 99% or 101%). Fig. 3 and Supplementary Table 4 show that primary schools had the highest percentage, 68% (n = 23 codes), of positive policy actions; and, although infrequent, negative evidence (18%, n = 5 codes) was highest in secondary schools. Inconclusive evidence was highest in combined schools (50%, n = 10 codes). Fig. 3 also shows that when analyzed by policy area, frequency of evidence was highest for school sport/extracurricular PA (35%, n = 29 codes), followed by physical education (17%, n = 14 codes), and whole school PA policy (12%, n =10 codes). The evidence for policy impact on SUAs (2%, n = 2 codes) and active school transport (AST; 2%, n = 2 codes) was rarely reported. Comparing relative strength of evidence across policy areas, the evidence for SUAs, though sparse (n = 2 codes), was 100% positive. For other policy areas, evidence of policy impact was mixed. A total of 60% (n = 6 codes) of the evidence for whole school PA policy was positive. The percentage of positive evidence for sport/extracurricular PA was 59% (n = 17 codes), for physical education it was 57% (n = 8 codes), for classroom PA it was 50% (n = 3 codes), for active breaks/recess it was 50% (n = 4 codes), for physical environment it was 38% (n = 3 codes), and for surveillance it was 33% (n = 1 code). The evidence for AST was inconclusive. A more detailed analysis is given in each section below.
Table 3.
Frequency of publications investigating each policy action.
| Primary | Secondary | Combined primary and secondary | |
|---|---|---|---|
|
1. School PA/PE policy School has a PA policy |
+ 63, 64, 65,68,69 ? 24 0 67 |
? 70 | + 66 0 62 |
|
2. PE 2.1. Require minimum time in PE |
+ 24,72,73, 0 24(recess time) |
+ 61(interscholastic) 0 61(PA clubs) |
0 62 |
| 2.2. Require adherence to PE curriculum | – 24 |
||
| 2.3. Require PE/specialist teacher training | + 24 | + 61 – 71 |
|
| 2.4. Require PE evaluated annually | + 24 | ||
| 2.5. Measures to reduce PE class size | 0 24 | ||
| 2.6. Require adherence to PE standards | + 24 |
||
|
3. Sport/extracurricular PA 3.1. Provide IM |
– 67 |
+ 57, 58, 59,61 + (boys only)57,58 0 (girls only)58 |
+ 60,62 0 66 |
| 3.2. Provide IS | + 58,59 0 57 – (boys only)57 ? 61 |
+ 60 | |
| 3.3. Provide PA opportunities before/after school | + 65,68,69 | – 71 0 (before school only) 71 |
0 66 |
| 3.4. Provide unrestricted access to sport | + (boys)60 0 (girls)60 |
||
| 3.5. Provide a variety of sport options (choice) | + (girls)60 0 (boys)60 |
||
| 3.6. Provide teacher supervision/training |
+65 | 0 57 | |
|
4. Active breaks/recess 4.1. Require minimum PA time in breaks |
+ 64 |
+ 62 0 66 |
|
| 4.2. Provide structured and free play PA/sport during break | + 64,65 (free play) 0 74 |
– 71 ? 70 |
|
|
5. PA in the classroom Provide PA breaks in non-PE curriculum |
+ 75,76 0 74 |
– 71 ? 70 |
+ 62 |
|
6. Physical environment 6.1. Provide non-fixed PA equipment |
?63 |
||
| 6.2. Maximize access to physical space for PA | +64,65 067 |
+ 78 ? 77 |
0 62,66 |
|
7. Shared use agreements Provide PA programs in shared space |
+ 77 |
+ 79 |
|
|
8. AST Provide AST infrastructure/program |
067 |
0 66 |
|
|
9. Surveillance 9.1. Establish a national school PA surveillance system |
? 80 | ||
| 9.2. Implement school PA performance reporting/award | + 65 | ? 70 |
Notes: Evidence for a policy action providing “significantly positive” outcomes is coded as +, evidence for a policy action providing “significantly negative” outcomes is coded as –, evidence for a policy action providing “inconclusive” outcomes is coded as 0, and evidence that has not been subjected to a significant test is coded as ?.
Abbreviations: AST = active school transport; IM = intramural; IS = interscholastic/intervarsity; PA = physical activity; PE = physical education.
Fig. 3.

Evidence code frequency and strength by education sector and by policy area. EC = extracurricular; PA = physical activity.
3.3.2. Whole school PA policy
In the area of whole school PA policy, 1 policy action was identified; 10 publications24,62, 63, 64, 65, 66, 67, 68, 69, 70 addressed overall or multi-component policies for PA established by individual schools. This represented 12% (n = 10 codes) of the total evidence and comprised positive (60%, n = 6 codes),63, 64, 65, 66,68,69 inconclusive (20%, n = 2 codes)24,70 and untested (20%, n = 2 codes).62,67 This action was more prevalent in primary schools than in secondary schools. In primary schools, 71% (n = 5)63, 64, 65,68,69 of codes were significantly positive, while 1 code was both inconclusive24 and untested.67 For secondary schools, there was a single untested code,70 while studies on combined primary and secondary schools had 2 codes (one significantly positive66 and one inconclusive62).
3.3.3. PE
Six policy actions were identified in 6 studies24,61,62,71, 72, 73 for the “Physical Education” policy area, which represented 17% (n = 14 codes) of the total evidence. The policy action “Require a minimum time in PE” was found to be effective in promoting PE and PA.24,61,72,73 Lounsbery and colleagues24 found that “Require a minimum time in PE” was positive at the district level but not at that school level; Kahan and McKenzie61 found this policy action to be positively related to IS but inconclusive for PA clubs. Both discrepancies were related to implementation. The policy actions “Require PE teacher training”,24,61 “Require adherence to PE standards”,24 and “Evaluate PE outcomes regularly”24 were associated with mainly favorable PA outcomes. Negative evidence was found for “Require adherence to PE curriculum”, and inconclusive evidence was found for “Measures to reduce PE class size”24 at the primary school level. More positive evidence for this policy area was found in primary (67%, n = 6 codes) than in secondary (50%, n = 2 codes) schools. Therefore, evidence suggests that studies on policy actions in PE are more prevalent and are more likely to be effective in primary schools than in secondary schools.
3.3.4. Sport/extracurricular PA
Six policy actions were identified in 11 studies57, 58, 59, 60, 61, 62,66, 67, 68, 69,71 for the policy area “Sport/extracurricular PA” from 11 publications,57, 58, 59, 60, 61, 62,66, 67, 68, 69,71 which represented 35% (n = 29 codes) of the total evidence (Table 3). The effects of 2 sport delivery policies, IM and IS, were described in detail in the reviewed studies. Evidence was more prevalent and more positive for IM (73%, n = 8 codes )57, 58, 59, 60, 61, 62 in comparison to IS (50%, n = 3 codes),58, 59, 60 with participation being greater under the IM model (35.9% vs. 27.3%, respectively).58 Few studies reported on policy in this area within primary schools (5 codes), with 3 studies showing positive effects for policies supporting afterschool PA programs,65,68,69 1 code for supporting teacher training in this area65 and a single negative code for IM sport.67 Research in secondary schools (n = 15 codes) was more prevalent, with positive effects most frequently being reported for IM sport policies.57, 58, 59,61 Some positive support was found for the IS model, with 2 positive codes,57,58 but a single code each for inconclusive,58 negative,57 or untested61 was also found for this model. Gender differences were found in relation to sport participation policy, with girls being more likely to participate when a broad range of sports were offered, thus encouraging choice, but girls were less likely to participate if the number of individuals allowed to access sport was unrestricted.60
3.3.5. Active breaks/recess
Two policy actions were identified in 7 studies62,64, 65, 66,70,71,74 for the policy area “Active breaks/recess”, representing 10% (n = 8 codes) of the total evidence. The policy action “Require minimum PA time in breaks” was coded as significantly positive in primary schools64 and as both significantly positive62 and inconclusive66 in primary and secondary combined schools. The policy action “Provide structured and free play PA/sport during break” was coded as significantly positive64,65 or inconclusive74 in primary schools and as significantly negative71 or no test70 in secondary school settings. Evidence64 suggests that policies promoting free play during break can be effective in increasing PA in primary schools. An example can be provided from the Australian context, in which a “no hat, no play policy” was replaced with a “no hat, play in the shade” policy.64
3.3.6. PA in the classroom
A single policy action was identified in 6 studies62,70,71,74, 75, 76 for the policy area “PA in the classroom”, representing 7% (n = 6 codes) of the total evidence. Broadly positive results were found for primary schools, with 66% (n = 2 codes) of the total evidence being significantly positive75,76 and 33% (n = 1 code) being coded as inconclusive.74 The evidence for secondary schools was mixed, with 1 code being negative71 (50%) and 1 code being inconclusive70 (50%). A single code indicating positive evidence was reported for combined primary and secondary schools.62
3.3.7. Physical environment
Two policy actions were identified in 8 studies62, 63, 64, 65, 66, 67,77,78 for the policy area “Physical environment”, representing 10% (n = 8 codes) of the total evidence. These included the 2 following areas: (a) “Provide non-fixed PA equipment”, which received a single untested code for primary schools,63 and (b) “Maximize access to physical spaces for PA”, which had 3 codes for primary schools (66% positive64,65, 33% inconclusive67), two for secondary schools (50% positive (boys only)78, 50% untested77) and two for combined settings (100% inconclusive).62,66
3.3.8. SUAs
A single policy action was identified in 2 studies77,79 for the policy area for SUAs—“Provide PA programs in shared space”—representing 2% (n = 2 codes) of the total evidence. This action is in contrast to simply opening the facility's space without running a structured program. Both studies reported an increase in use of the space and more MVPA within school grounds when a PA program was combined with an SUA.
3.3.9. AST
A single policy action was identified in 2 studies66,67 for the policy area “AST”, representing 2% (n = 2 codes) of the total evidence. This action encourages schools to “Provide AST infrastructure/program”. However, no studies provided conclusive evidence linking AST policy with PA outcomes, nor did they report on the impact of school policies to promote AST in secondary schools. A study combining data from both primary and secondary schools reported that AST policies are prevalent in secondary schools, yet the evidence for their impact was inconclusive.66
3.3.10. Surveillance
Two policy actions were identified in 3 studies65,70,80 for the policy area “Surveillance”, representing 4% (n = 3 codes) of the total evidence. The 2 actions are: (a) “Establish a national school PA surveillance system”, for which there was a single untested code in the combined primary and secondary school setting80 and (b) “Implement school PA performance reporting/award”, which had a significantly positive code for primary schools65 and an untested code for secondary schools.70
4. Discussion
This review builds on existing knowledge25 and is the first review to examine systematically the status of published scientific evidence, using empirical studies complemented with additional sources of evidence, on the impact of school policies on PA-related outcomes. The overall intent of policy is to provide the framework in which programs or environmental changes are implemented, thus eventually leading to higher levels of PA. The process of studying the school setting revealed 9 policy areas, several of which have been described in previous reviews, book chapters, and other types of documents, such as scientific statements and position papers (Supplementary Tables 1 and 2). However, our review presents, for the first time, the status of the scientific evidence on 22 policy actions under these policy areas. For some areas there is good support (e.g., PE), while evidence of effectiveness is lacking or inconclusive for other areas (e.g., surveillance). This makes it difficult at this stage to identify precisely the indicators and best practice benchmarks for evidence-based policy actions.
Strong support was found for a mandated minimum PE time.61,72 This policy approach is welcome due to its potential to reduce disparities across schools.43,41 Indeed, targets of 225 min per week (secondary) and 150 min per week (primary; Society for Health and Physical Educators),81 or 6%–8% of all taught time,82 have been recommended. Enforcing regulations requiring professional licensure of PE teachers is supported by our review and other research81 adding weight to the role of the PE specialist as a PA ambassador for schools. Similarly, we found evidence of effectiveness for policies requiring adherence to PE standards and regular evaluation of PE outcomes, which provides support to current guidelines advocated by national and international organizations regarding the delivery of quality PE.24
Pertinent to prescribing any school-based PA policy is the relative complexity of promoting participation for all.40,45 Youth sport programs have been advocated as a strategy to promote PA and prevent obesity.42 In school sport, 2 delivery models (IM and IS, which exist primarily in the United States) were found to have benefits and drawbacks. While participation in sport was found to be roughly equal between genders under the IS model, it was higher amongst boys under the IM model.58 This may be due to the unrestricted nature of participation in IM sports, which may be more favorable to participation by boys.60 Our findings also suggest that an IM model may exacerbate sex-based sport participation disparities due to the element of self-segregation, since girls may be less willing to participate when boys are present.58 This does not limit the importance of other sociological issues pertinent to the persistent sex and gender inequities in sport, such as the social construction of girls as less capable or somehow inferior to boys.83 However, the same studies note that the IM model may be superior to the IS model for increasing sport participation for all students, and specifically for ethnic minority or students of low-socioeconomic status. Also, the IM model was associated with more positive PA-related outcomes than the IS model. The reasons underlying these differences need to be further investigated, and they caution against a one-size-fits-all approach to policy. To develop a more realistic view on the potential of the sports/extracurricular policy area, the range of policy options evaluated needs to be expanded. Negative evidence for IM67 policy in primary schools was found, but positive evidence for before- or after-school PA opportunities65,68,69 and free-play activities64,65 was reported. These findings support the existing research emphasizing the multiple benefits of unstructured, child-directed free-play activities in school settings.84
Additional policy areas for opportunities to promote PA in both primary and secondary schools include minimum duration of break times and using policy to provide youth with access to PA physical spaces that maximize the impact of the school's physical environment.77, 78, 79 Cross-curricular integration of PA into non-PE classroom time was supported in primary schools, for example, through the use of math and language classes.82 Evidence suggests that school sport and PA facilities are under-utilized during after-school hours and on weekends, which limits the potential of these existing assets to encourage and facilitate PA participation among children and the wider community.77 Fittingly, our review found that opening school facilities to local communities through SUAs resulted in more adults and children using these facilities outside of school hours and was positively associated with PA in primary and secondary schools in under-resourced communities when supported with good-quality PA programs.79 Policy actions identified under the related areas of physical environment and SUAs provide evidence that the school environment offers considerable potential for increasing PA for everyone.
Active transport, which has been the focus of a separate PEN systematic literature review, is an area where PA policies can have a promising impact.40, 41, 42, 43,81 Indeed, other reviews85, 86, 87, 88 have attempted to address the issue of effectiveness of active transport policies as part of the Active Living by Design Community Action 5P (preparation, promotions, programs, policy influences, and physical projects) Model. Documented positive effects supporting the use of policy action as a necessary condition for active transport effectiveness were found in urban design, transport and community settings89,90 rather than in school settings, where preparation, promotion and programs were prioritized.85,91 This is consistent with our review, which found limited, inconclusive evidence for AST policy actions within the school setting.67 Over the last 40 years in the United States, schools have increasingly been built in sparsely populated areas, away from residential areas.92 Distance to school has been identified as a strong factor influencing levels of active transport.93,94 Thus while state-level policymakers may influence active transport policy, the ability of individual schools to impact levels of active commuting by students is limited if the physical environment, external to the school, is unsupportive.94,95 In addition to policy, pursuing inter-sectoral partnerships with stakeholders in areas such as transport, planning and urban design is an important option for supporting changes in active transport to school.95
Our review revealed methodological issues within the literature and this should be taken into account when interpreting the results. Previous reviews have noted the importance of distinguishing policies from interventions.28,30 However, our review demonstrates that work in this area may be hampered by a number of conceptual issues and ambiguity surrounding the definition of policy or policies. This was evident in studies that assessed policies that were in some cases not clearly identified or were only vaguely defined.61,78 For example, Hunter and colleagues78 declared that “none of the schools made any policy-related changes”, but some of the strategies described by Hunter et al. met the definition of policy we used in our review.
Multi-level, multi-component approaches to the promotion of PA have been recommended.35,96 Several multi-component interventions that had a “policy” component progressed to full-text review (Supplementary Tables 1 and 2) but were ultimately excluded from our data synthesis due to a lack of clarity in attributing evidence of impact on PA to policy.48, 49, 50, 51, 52, 53, 54, 55, 56 For example, the Power Up for 30 (PU30) study included a “voluntary commitment to 30 min of PA outside of PE” and a “needs assessment of baseline PA opportunities”.49 The former is an action that is interesting to policymakers (school administrators), but the latter is an example of an individualized approach. This makes it difficult to declare with certainty whether a particular component of the intervention is effective.97 Multi-component interventions rarely included robust process evaluation, rendering it impossible to determine the actual effect of the policy component. To further compound matters, it was common practice in some studies and reviews to pool and examine together the effect of environmental and policy actions or strategies (e.g., Khan and colleagues46), when, in fact, these actions did not necessarily share the same characteristics and modus operandi.
Underlying these conceptual difficulties is the fact that schools are complicated autonomous systems and that while national or regional efforts may catalyze supportive policy environments, the translation of such policies into practice is far from simple, which supports the complexity of the policy process. A clear example of this perspective is the COMPASS study, which aims “to examine how naturally occurring changes to school PA policy, recreational programming, public health resources, and the physical environment impact adolescent MVPA”.78
Only a handful of studies included in our review used measures to assess the extent to which policies were implemented as originally intended.24,46,71,72 Although the results regarding the effects of accounting for this circumstance in the analyses were mixed, a greater emphasis on using appropriate tools to assess systematic fidelity to policy implementation is warranted in order to advance knowledge in this area.98 Hence, while the research into how policies can increase PA through the school setting may be useful, evidence of effective strategies for increasing implementation and compliance with established mandates is needed. Our understanding of how a degree of flexibility can be accommodated to allow for local interpretation and adaptation without compromising impact needs further investigation. Policy cycle models that differentiate between policy content and policy implementation could provide a useful theoretical framework for future analyses.99
Similarly, strong process evaluation protocols are necessary to allow researchers to gain an enhanced understanding of the barriers and facilitators to successful implementation of PA policies in the school setting. In particular, process evaluations including a robust qualitative component are needed to provide a more holistic understanding of interventions.100 Coupled with providing richer information on the context in which policies take place, collecting qualitative data on the participants’ and stakeholders’ responses to the policies can also help researchers address the question of how policies work, which is complementary to, and equally important as, the more commonly asked question of which policies work.39
There is considerable debate in the literature concerning the nature of the evidence required to understand what works to encourage people to increase their level of PA. For example, Broekhuizen and colleagues98 strongly advise researchers to conduct larger randomized controlled trials that investigate environmental interventions (e.g., modifications to school playgrounds) in order to draw conclusions that are more valid. On the other hand, Tones101 caution against the inappropriate use of a randomized controlled trial study design in health promotion, as adopting a public health perspective. Messing and colleagues35 advocate for the use of different study designs, such as pragmatic or hybrid trials, that allow for the simultaneous testing of both efficacy and effectiveness. These designs, researchers argue, could allow accelerating scale-up processes of PA interventions with children and adolescents.102 Similarly, Abu-Omar and colleagues85 called for increasing efforts to conduct natural experiments that investigate the effectiveness of policy and environmental approaches to PA promotion. This position is consistent with the view that in order to investigate the effects of policy changes, non-randomized studies103 and studies using difference-in-differences approaches might be useful. Likewise, it might be appropriate to use propensity scores, synthetic control approaches, or regression discontinuity, instrumental variables or near-far matching approaches that address unobserved confounders by utilizing quasi-random variations.104
Strengths of this review include the specific focus on school-based policies that have a direct or indirect impact on PA-related outcomes rather than a traditional broader focus on school-based strategies that promote PA. Reliance on empirical studies that analyze primary data, complemented with additional sources of evidence (e.g., different types of reviews, scientific statements, position papers), is another clear strength of our review because we are able to provide a holistic and more nuanced view of the existing evidence for the impact of school-based policies on PA outcomes. Policies made at the national, regional, local, and school level are all included in our review, thus providing a more comprehensive view on the topic.
Our review has some limitations as well. Only literature published in the English language was included. Thus, much of the evidence we reviewed came from studies conducted in only a few countries, the US in particular, and therefore it may not be applicable in other geographical, cultural, and political settings without appropriate translation to local realities. We focused on policies that promoted PA within the school setting because other settings, such as transport and sport, are covered in separate PEN reviews. One paper61 we used for data synthesis included a review of sport policy in private schools. Whilst we acknowledge that differences exist between private and public schools, we felt that this paper merited inclusion because information comparing different sport policies is limited and this study contributed knowledge to this area. There are also limitations stemming from liberal and ambiguous use of the term “policy” in the literature. Likewise, there was considerable heterogeneity regarding methodological aspects of the studies, such as research designs, assessment procedures, and types of outcomes reported, which created challenges when attempting to make coherent sense of the existing evidence. Similarly, “statistical significance”, as reported in the studies and coded in our review for synthesis purposes, is not necessarily synonymous with “practical significance” in terms of potential for impact in the real world.
5. Conclusion
There is a consensus that schools represent an ideal setting for the promotion of PA and that policy changes are needed to address the current issues of inactivity that affect children and adolescents around the world. Although work in this area is incipient and the evidence remains largely scattered, our review has identified 9 policy areas, with specific policy actions within each area, that add to the emerging body of knowledge regarding the impact of school-based policies on PA-related outcomes. The policy areas and specific policy actions provide a template to guide upstream PA promotion practice in the school setting. Policy areas with stronger evidence of PA impact were PE, school sport, classroom-based PA, active school breaks, and SUAs. However, the range of policy options implemented and evaluated in the school setting remains limited, and more attention needs to be paid to how policies are implemented and the consequent impact on the PA outcomes investigated. We recommend that there be greater clarity surrounding policy terminology, that the range of policy actions implemented within each of the identified areas be expanded and that robust and flexible evaluation methods appropriate to the real-world nature of policies be used. Finally, the impact of the context in which policies are implemented, exemplified by differences in the observed effects of some policies at the primary vs. secondary school levels, needs to be more clearly understood. Encouraging children and adolescents to participate in PA by means of policies implemented in the school setting is an area ripe for applied and conceptual or theoretical work, especially because it concerns the effects of public policies at the regional or national level over policies implemented at local level.
Acknowledgments
Acknowledgments
The PEN project is funded by the Joint Programming Initiative (JPI) “A Healthy Diet for a Healthy Life”, a research and innovation initiative of EU member states and associated countries. The funding agencies supporting this work are (in alphabetical order) Germany: Federal Ministry of Education and Research (BMBF); Ireland: Health Research Board (HRB); Italy: Ministry of Education, University and Research (MIUR); New Zealand: University of Auckland, School of Population Health; Norway: Research Council of Norway (RCN); Poland: National Centre for Research and Development (NCBR), and the Netherlands: the Netherlands Organization for Health Research and Development (ZonMw). Additionally, the French partners acknowledge support through the Institute National de la Recherche Agronomique (INRA).
Authors’ contributions
CBW was responsible for project administration, conceptualization, methodology, writing original draft, review, and editing; KV, JL, JZ, PG, SF, SM, and EGB were involved in conceptualization, and carried out methodology, writing original draft, review, and editing; LK carried out methodology, writing original draft, review, and editing; BC carried out writing, review, and editing. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Peer review under responsibility of Shanghai University of Sport.
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.01.006.
Appendix. Supplementary materials
References
- 1.World Health Organization . World Health Organization; Geneva: 2009. Global health risks: Mortality and burden of disease attributable to selected major risks. [Google Scholar]
- 2.World Health Organization (WHO) WHO Press; Geneva: 2010. Global recommendations on physical activity for health. [PubMed] [Google Scholar]
- 3.Hardy L.L., Mihrshahi S., Bellew W., Bauman A., Ding D. Children's adherence to health behavior recommendations associated with reducing risk of non-communicable disease. Prev Med Rep. 2017;8:279–285. doi: 10.1016/j.pmedr.2017.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Guthold R., Stevens G.A., Riley L.M., Bull F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. 2018;6:e1077–e1086. doi: 10.1016/S2214-109X(18)30357-7. [DOI] [PubMed] [Google Scholar]
- 5.Dumith S.C., Gigante D.P., Domingues M.R., Kohl H.W., III Physical activity change during adolescence: A systematic review and a pooled analysis. Int J Epidemiol. 2011;40:685–698. doi: 10.1093/ije/dyq272. [DOI] [PubMed] [Google Scholar]
- 6.Hallal P.C., Andersen L.B., Bull F.C., Guthold R., Haskell W., Ekelund U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. The Lancet. 2012;380:247–257. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- 7.Ortega F.B., Konstabel K., Pasquali E. Objectively measured physical activity and sedentary time during childhood, adolescence and young adulthood: A cohort study. PLoS One. 2013;8:e60871. doi: 10.1371/journal.pone.0060871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim Y., Beets M.W., Welk G.J. Everything you wanted to know about selecting the “right” Actigraph accelerometer cut-points for youth, but…: A systematic review. J Sci Med Sport. 2012;15:311–321. doi: 10.1016/j.jsams.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 9.Currie C., Zanotti C., Morgan A. WHO Regional Office for Europe; Copenhagen: 2012. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: International report from the 2009/2010 survey. [Google Scholar]
- 10.Woods C.B., Tannehill D., Walsh J. School of Health and Human Performance Dublin City University and the Irish Sports Council; Dublin: 2010. The children's sport participation and physical activity study (CSPPA) [Google Scholar]
- 11.Telama R. Tracking of physical activity from childhood to adulthood: A review. Obes Facts. 2009;2:187–195. doi: 10.1159/000222244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Telama R., Yang X., Viikari J., Valimaki I., Wanne O., Raitakari O. Physical activity from childhood to adulthood: A 21-year tracking study. Am J Prev Med. 2005;28:267–273. doi: 10.1016/j.amepre.2004.12.003. [DOI] [PubMed] [Google Scholar]
- 13.Malina R. President's Council on Physical Fitness and Sports Research Digest; Washington, DC: 2001. Tracking of physical activity across the lifespan. [Google Scholar]
- 14.Hardie Murphy M., Rowe D.A., Woods C.B. Impact of physical activity domains on subsequent physical activity in youth: A 5-year longitudinal study. J Sports Sci. 2017;35:262–268. doi: 10.1080/02640414.2016.1161219. [DOI] [PubMed] [Google Scholar]
- 15.Hardie Murphy M., Rowe D.A., Woods C.B. Sports participation in youth as a predictor of physical activity: A 5-year longitudinal study. J Phys Act Health. 2016;13:704–711. doi: 10.1123/jpah.2015-0526. [DOI] [PubMed] [Google Scholar]
- 16.Sallis J.F., Cervero R.B., Ascher W., Henderson K.A., Kraft M.K., Kerr J. An ecological approach to creating active living communities. Annu Rev Public Health. 2006;27:297–322. doi: 10.1146/annurev.publhealth.27.021405.102100. [DOI] [PubMed] [Google Scholar]
- 17.Institute of Medicine . National Academy Press; Washington, DC: 2001. Health and behavior: The interplay of biological, behavioral, and societal influences. [PubMed] [Google Scholar]
- 18.Lakerveld J., Woods C., Hebestreit A. Advancing the evidence base for public policies impacting on dietary behaviour, physical activity and sedentary behaviour in Europe: the Policy Evaluation Network promoting a multidisciplinary approach. Food Policy. 2020;96 doi: 10.1016/j.foodpol.2020.101873. [DOI] [Google Scholar]
- 19.World Health Organization . World Health Organization; Geneva: 2013. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. [Google Scholar]
- 20.World Health Organization . World Health Organization; Geneva: 2018. Global action plan on physical activity 2018–2030: More active people for a healthier world. [Google Scholar]
- 21.Swinburn B.A., Kraak V.I., Allender S. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. The Lancet. 2019;393:791–846. doi: 10.1016/S0140-6736(18)32822-8. [DOI] [PubMed] [Google Scholar]
- 22.International Society for Physical Activity and Health. Investments that work for physical activity. Br J Sports Med. 2012;46:709–712. doi: 10.1136/bjsm.2012.091485. [DOI] [PubMed] [Google Scholar]
- 23.Lounsbery M.A. School physical activity: Policy matters. Kinesiol Rev. 2017;6:51–59. [Google Scholar]
- 24.Lounsbery M.A.F., McKenzie T.L., Morrow Jr J.R., Monnat S.M., Holt K.A. District and school physical education policies: Implications for physical education and recess time. Ann Behav Med. 2013;45(Suppl. 1):S131–S141. doi: 10.1007/s12160-012-9427-9. [DOI] [PubMed] [Google Scholar]
- 25.Gelius P., Messing S., Goodwin L., Schow D., Abu-Omar K. What are effective policies for promoting physical activity? A systematic review of reviews. Prev Med Rep. 2020;18 doi: 10.1016/j.pmedr.2020.101095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.World Health Organization . World Health Organization; Geneva: 2004. Global strategy on diet, physical activity, and health. [Google Scholar]
- 27.Daly-Smith A., Quarmby T., Archbold V.S.J. Using a multi-stakeholder experience-based design process to co-develop the Creating Active Schools Framework. Int J Behav Nutr Phys Act. 2020;17:13. doi: 10.1186/s12966-020-0917-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rutten A., Schow D., Breda J. Three types of scientific evidence to inform physical activity policy: Results from a comparative scoping review. Int J Public Health. 2016;61:553–563. doi: 10.1007/s00038-016-0807-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Klepac Pogrmilovic B., O'Sullivan G., Milton K. A global systematic scoping review of studies analysing indicators, development, and content of national-level physical activity and sedentary behaviour policies. Int J Behav Nutr Phys Act. 2018;15:123. doi: 10.1186/s12966-018-0742-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gelius P., Tcymbal A., Abu-Omar K. Status and contents of physical activity recommendations in European Union countries: A systematic comparative analysis. BMJ Open. 2020;10 doi: 10.1136/bmjopen-2019-034045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Moher D., Liberati A., Tetzlaff J., Altman D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151:264–269. doi: 10.7326/0003-4819-151-4-200908180-00135. [DOI] [PubMed] [Google Scholar]
- 32.Volf K., Kelly L., García Bengoechea E. Policy Evaluation Network (PEN): Protocol for systematic literature review examining the evidence for impact of policies across seven different policy domains. HRB Open Research. 2020;3:62. doi: 10.12688/hrbopenres.13089.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McKenzie T.L., Sallis J.F., Nader P.R. SOFIT: System for Observing Fitness Instruction Time. J Teach Phys Educ. 1992;11:195–205. [Google Scholar]
- 34.Ouzzani M., Hammady H., Fedorowicz Z., Elmagarmid A. Rayyan—A web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Messing S., Rütten A., Abu-Omar K. How can physical activity be promoted among children and adolescents? A systematic review of reviews across settings. Frontiers in Public Health. 2019;7:55. doi: 10.3389/fpubh.2019.00055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Downs S.H., Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–384. doi: 10.1136/jech.52.6.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Shea B.J., Grimshaw J.M., Wells G.A. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. doi: 10.1186/1471-2288-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Critical Appraisal Skills Programme . 2018. CASP Checklists.https://casp-uk.net/casp-tools-checklists/ Available at: [accessed 14.01.2020] [Google Scholar]
- 39.Panter J., Guell C., Humphreys D., Ogilvie D. Can changing the physical environment promote walking and cycling? A systematic review of what works and how. Health Place. 2019;58 doi: 10.1016/j.healthplace.2019.102161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lagarde F., LeBlanc C.M. Policy options to support physical activity in schools. Can J Public Health. 2010;101(Suppl. 2):S9–13. doi: 10.1007/BF03405618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sallis J.F., Carlson J.A., Mignano A.M. Promoting youth physical activity through physical education and after-school programs. Adolesc Med State Art Rev. 2012;23:493–510. [PubMed] [Google Scholar]
- 42.Pate R.R., Flynn J.I., Dowda M. Policies for promotion of physical activity and prevention of obesity in adolescence. J Exerc Sci Fit. 2016;14:47–53. doi: 10.1016/j.jesf.2016.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kohl H.W., III, Cook H.D. National Academies Press; Washington, DC: 2013. Educating the student body: Taking physical activity and physical education to school. [PubMed] [Google Scholar]
- 44.Lee A. Health-promoting schools: Evidence for a holistic approach to promoting health and improving health literacy. Appl Health Econ Health Policy. 2009;7:11–17. doi: 10.2165/00148365-200907010-00002. [DOI] [PubMed] [Google Scholar]
- 45.Umstattd Meyer M.R., Perry C.K., Sumrall J.C. Physical activity-related policy and environmental strategies to prevent obesity in rural communities: A systematic review of the literature, 2002–2013. Prev Chronic Dis. 2016;13:E03. doi: 10.5888/pcd13.150406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Khan L.K., Sobush K., Keener D. Recommended community strategies and measurements to prevent obesity in the United States. MMWR Recomm Rep. 2009;58:1–26. [PubMed] [Google Scholar]
- 47.Pate R.R., Davis M.G., Robinson T.N. Promoting physical activity in children and youth: a leadership role for schools: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism (Physical Activity Committee) in collaboration with the Councils on Cardiovascular Disease in the Young and Cardiovascular Nursing. Circulation. 2006;114:1214–1224. doi: 10.1161/CIRCULATIONAHA.106.177052. [DOI] [PubMed] [Google Scholar]
- 48.Benjamins M.R., Whitman S. A culturally appropriate school wellness initiative: Results of a 2-year pilot intervention in 2 Jewish schools. J Sch Health. 2010;80:378–386. doi: 10.1111/j.1746-1561.2010.00517.x. [DOI] [PubMed] [Google Scholar]
- 49.Cheung P., Franks P., Kramer M. Impact of a Georgia elementary school-based intervention on physical activity opportunities: A quasi-experimental study. J Sci Med Sport. 2019;22:191–195. doi: 10.1016/j.jsams.2018.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hollis J.L., Sutherland R., Campbell L. Effects of a “school-based” physical activity intervention on adiposity in adolescents from economically disadvantaged communities: Secondary outcomes of the ‘Physical Activity 4 Everyone' RCT. Int J Obes (Lond) 2016;40:1486–1493. doi: 10.1038/ijo.2016.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sutherland R., Reeves P., Campbell E. Cost effectiveness of a multi-component school-based physical activity intervention targeting adolescents: The “Physical Activity 4 Everyone” cluster randomized trial. Int J Behav Nutr Phys Act. 2016;13:94. doi: 10.1186/s12966-016-0418-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sutherland R.L., Campbell E.M., Lubans D.R. The physical activity 4 everyone cluster randomized trial: 2-year outcomes of a school physicalactivity intervention among adolescents. Am J Prev Med. 2016;51:195–205. doi: 10.1016/j.amepre.2016.02.020. [DOI] [PubMed] [Google Scholar]
- 53.Waters E., Gibbs L., Tadic M. Cluster randomised trial of a school-community child health promotion and obesity prevention intervention: Findings from the evaluation of fun'n healthy in Moreland! BMC Public Health. 2017;18:92. doi: 10.1186/s12889-017-4625-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Peterson K.E., Spadano-Gasbarro J.L., Greaney M.L. Three-year improvements in weight status and weight-related behaviors in middle school students: The healthy choices study. PLoS One. 2015;10 doi: 10.1371/journal.pone.0134470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Ling J., King K.M., Speck B., Kim S., Wu D. Preliminary assessment of a school-based healthy lifestyle intervention among rural elementary school children. J Schl Health. 2014;84:247–255. doi: 10.1111/josh.12143. [DOI] [PubMed] [Google Scholar]
- 56.Saraf D.S., Gupta S.K., Pandav C.S. Effectiveness of a school based intervention for prevention of non-communicable diseases in middle school children of rural North India: A randomized controlled trial. Indian Pediatr. 2015;82:354–362. doi: 10.1007/s12098-014-1562-9. [DOI] [PubMed] [Google Scholar]
- 57.Bocarro J.N., Kanters M.A., Cerin E. School sport policy and school-based physical activity environments and their association with observed physical activity in middle school children. Health Place. 2012;18:31–38. doi: 10.1016/j.healthplace.2011.08.007. [DOI] [PubMed] [Google Scholar]
- 58.Kanters M.A., Bocarro J.N., Edwards M.B., Casper J.M., Floyd M.F. School sport participation under two school sport policies: Comparisons by race/ethnicity, gender, and socioeconomic status. Ann Behav Med. 2013;45(Suppl. 1):S113–S121. doi: 10.1007/s12160-012-9413-2. [DOI] [PubMed] [Google Scholar]
- 59.Edwards M.B., Kanters M.A., Bocarro J.N. Policy changes to implement intramural sports in North Carolina middle schools: Simulated effects on sports participation rates and physical activity intensity, 2008–2009. Prev Chronic Dis. 2014;11 doi: 10.5888/pcd11.130195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Drake K.M., Longacre M.R., MacKenzie T. High school sports programs differentially impact participation by sex. J Sport Health Sci. 2015;4:282–288. [Google Scholar]
- 61.Kahan D., McKenzie T.L. Extracurricular physical activity programs in California private secondary schools. Res Q Exerc Sport. 2017;88:524–529. doi: 10.1080/02701367.2017.1370073. [DOI] [PubMed] [Google Scholar]
- 62.Morton K.L., Corder K., Suhrcke M. School polices, programmes and facilities, and objectively measured sedentary time, LPA and MVPA: Associations in secondary school and over the transition from primary to secondary school. Int J Behav Nutr Phys Act. 2016;13:54. doi: 10.1186/s12966-016-0378-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Parrish A.M., Yeatman H., Iverson D., Russell K. Using interviews and peer pairs to better understand how school environments affect young children's playground physical activity levels: A qualitative study. Health Educ Res. 2012;27:269–280. doi: 10.1093/her/cyr049. [DOI] [PubMed] [Google Scholar]
- 64.Parrish A.M., Okely A.D., Batterham M., Cliff D., Magee C. PACE: A group randomised controlled trial to increase children's break-time playground physical activity. J Sci Med Sport. 2016;19:413–418. doi: 10.1016/j.jsams.2015.04.017. [DOI] [PubMed] [Google Scholar]
- 65.Ajja R., Clennin M.N., Weaver R.G. Association of environment and policy characteristics on children's moderate-to-vigorous physical activity and time spent sedentary in afterschool programs. Prev Med. 2014;69(Suppl. 1):S49–S54. doi: 10.1016/j.ypmed.2014.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.De Meester F., Van Dyck D., De Bourdeaudhuij I., Deforche B., Cardon G. Changes in physical activity during the transition from primary to secondary school in Belgian children: What is the role of the school environment? BMC Public Health. 2014;14:261. doi: 10.1186/1471-2458-14-261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Naiman D.I., Leatherdale S.T., Gotay C., Masse L.C. School factors associated with the provision of physical education and levels of physical activity among elementary school students in Ontario. Can J Public Health. 2015;106:e290–e296. doi: 10.17269/cjph.106.4899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Huberty J., Beets M., Beighle A. Effects of a policy-level intervention on children's pedometer-determined physical activity: Preliminary findings from Movin' Afterschool. J Public Health Manag Pract. 2013;19:525–528. doi: 10.1097/PHH.0b013e31829465fa. [DOI] [PubMed] [Google Scholar]
- 69.Beets M.W., Huberty J., Beighle A. Systematic observation of physical activity in afterschool programs: Preliminary findings from Movin' Afterschool intervention. J Phys Act Health. 2013;10:945–981. doi: 10.1123/jpah.10.7.974. [DOI] [PubMed] [Google Scholar]
- 70.Moon A.M., Mullee M.A., Rogers L., Thompson R.L., Speller V., Roderick P. Helping schools to become health-promoting environments—An evaluation of the Wessex Healthy Schools Award. Health Promot Intern. 1999;14:111. doi: 10.1093/heapro/14.2.111. [DOI] [Google Scholar]
- 71.Seibert T.S., Allen D.B., Eickhoff J., Carrel A.L. CDC childhood physical activity strategies fail to show sustained fitness impact in middle school children. Prev Med Rep. 2018;12:60–65. doi: 10.1016/j.pmedr.2018.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Calvert H.G., Turner L., Leider J., Piekarz-Porter E., Chriqui J.F. Comprehensive policies to support comprehensive practices: Physical activity in elementary schools. J Phys Act Health. 2020;17:313–322. doi: 10.1123/jpah.2019-0402. [DOI] [PubMed] [Google Scholar]
- 73.Kelder S.H., Springer A.S., Barroso C.S. Implementation of Texas Senate Bill 19 to increase physical activity in elementary schools. J Public Health Policy. 2009;30(Suppl. 1):S221–S247. doi: 10.1057/jphp.2008.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Holt E., Bartee T., Heelan K. Evaluation of a policy to integrate physical activity into the school day. J Phys Act Health. 2013;10:480–487. doi: 10.1123/jpah.10.4.480. [DOI] [PubMed] [Google Scholar]
- 75.Stone M.R., Faulkner G.E.J., Zeglen-Hunt L., Cowie Bonne J.C. The Daily Physical Activity (DPA) policy in Ontario: Is it working? An examination using accelerometry-measured physical activity data. Can J Public Health. 2012;103:170–174. doi: 10.1007/BF03403807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Weatherson K.A., Locke S.R., Jung M.E. Exploring the effectiveness of a school-based physical activity policy in British Columbia, Canada: A mixed-methods observational study. Transl Behav Med. 2019;9:246–255. doi: 10.1093/tbm/iby053. [DOI] [PubMed] [Google Scholar]
- 77.Carlton T.A., Kanters M.A., Bocarro J.N., Floyd M.F., Edwards M.B., Suau L.J. Shared use agreements and leisure time physical activity in North Carolina public schools. Prev Med. 2017;95(Suppl. 1):S10–S16. doi: 10.1016/j.ypmed.2016.08.037. [DOI] [PubMed] [Google Scholar]
- 78.Hunter S., Leatherdale S.T., Storey K., Carson V. A quasi-experimental examination of how school-based physical activity changes impact secondary school student moderate- to vigorous-intensity physical activity over time in the COMPASS study. Int J Behav Nutr Phys Act. 2016;13:86. doi: 10.1186/s12966-016-0411-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Lafleur M., Gonzalez E., Schwarte L. Increasing physical activity in under-resourced communities through school-based, joint-use agreements, Los Angeles County, 2010–2012. Prev Chronic Dis. 2013;10:E89. doi: 10.5888/pcd10.120270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Jurak G., Kovac M., Sember V., Starc G. 30 years of SLOfit: Its legacy and perspective. Turk J Sports Med. 2019;54:23–27. [Google Scholar]
- 81.Hatfield D.P., Chomitz V.R. Increasing children's physical activity during the school day. Curr Obes Rep. 2015;4:147–156. doi: 10.1007/s13679-015-0159-6. [DOI] [PubMed] [Google Scholar]
- 82.European Commission/EACEA/Eurydice . Publications Office of the European Union; Luxembourg: 2013. Physical education and sport at school in Europe. [Google Scholar]
- 83.Mandic S., Bengoechea E.G., Stevens E., de la Barra S.L., Skidmore P. Getting kids active by participating in sport and doing it more often: Focusing on what matters. Int J Behav Nutr Phys Act. 2012;9:86. doi: 10.1186/1479-5868-9-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Gray P. Basic Books; New York, NY: 2013. Free to learn: Why unleashing the instinct to play will make our children happier, more self-reliant, and better students for life. [Google Scholar]
- 85.Abu-Omar K., Rutten A., Burlacu I., Schatzlein V., Messing S., Suhrcke M. The cost-effectiveness of physical activity interventions: A systematic review of reviews. Prev Med Rep. 2017;8:72–78. doi: 10.1016/j.pmedr.2017.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Jones R.A., Blackburn N.E., Woods C.B., Byrne M., van Nassau F., Tully M.A. Interventions promoting active transport to school in children: A systematic review and meta-analysis. Prev Med. 2019;123:232–241. doi: 10.1016/j.ypmed.2019.03.030. [DOI] [PubMed] [Google Scholar]
- 87.Pang B., Kubacki K., Rundle-Thiele S. Promoting active travel to school: A systematic review (2010–2016) BMC Public Health. 2017;17:638. doi: 10.1186/s12889-017-4648-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Villa-González E., Barranco-Ruiz Y., Evenson K.R., Chillón P. Systematic review of interventions for promoting active school transport. Prev Med. 2018;111:115–134. doi: 10.1016/j.ypmed.2018.02.010. [DOI] [PubMed] [Google Scholar]
- 89.Boarnet M.G., Anderson C.L., Day K., McMillan T., Alfonzo M. Evaluation of the California Safe Routes to School legislation: Urban form changes and children's active transportation to school. Am J Prev Med. 2005;28:134–140. doi: 10.1016/j.amepre.2004.10.026. [DOI] [PubMed] [Google Scholar]
- 90.Hoelscher D., Ory M., Dowdy D. Effects of funding allocation for safe routes to school programs on active commuting to school and related behavioral, knowledge, and psychosocial outcomes: Results from the Texas childhood obesity prevention policy evaluation (T-COPPE) study. Environ Behav. 2016;48:210–229. [Google Scholar]
- 91.Jones R.A., Hinkley T., Okely A.D., Salmon J. Tracking physical activity and sedentary behavior in childhood: A systematic review. Am J Prev Med. 2013;44:651–658. doi: 10.1016/j.amepre.2013.03.001. [DOI] [PubMed] [Google Scholar]
- 92.Kohl III H.W., Cook H.D. The National Academies Press; Washington, DC: 2013. Preliminary assessment of a school-based healthy lifestyle intervention among rural elementary school children. [Google Scholar]
- 93.Woods C.B., Nelson N.M. An evaluation of distance estimation accuracy and its relationship to transport mode for the home-to-school journey by adolescents. J Transport Health. 2014;1:274–278. [Google Scholar]
- 94.Nelson N.M., Foley E., O'Gorman D.J., Moyna N.M., Woods C.B. Active commuting to school: How far is too far? Int J Behav Nutr Phys Act. 2008;5:1. doi: 10.1186/1479-5868-5-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Ikeda E., Mavoa S., Cavadino A. Keeping kids safe for active travel to school: A mixed method examination of school policies and practices and children's school travel behaviour. Travel Behav Soc. 2020;21:57–68. doi: 10.1016/j.tbs.2020.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.van Sluijs E.M., McMinn A.M., Griffin S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ. 2007;335:703. doi: 10.1136/bmj.39320.843947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Craike M., Wiesner G., Hilland T.A., Bengoechea E.G. Interventions to improve physical activity among socioeconomically disadvantaged groups: an umbrella review. Int J Behav Nutr Phys Act. 2018;15:43. doi: 10.1186/s12966-018-0676-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Broekhuizen K., Scholten A.M., de Vries S.I. The value of (pre)school playgrounds for children's physical activity level: A systematic review. Int J Behav Nutr Phys Act. 2014;11:59. doi: 10.1186/1479-5868-11-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Howlett M., Ramesh M., Perl A. 3rd ed. Oxford University Press; Oxford: 2009. Studying public policy: Policy cycles and policy subsystems. [Google Scholar]
- 100.Camacho-Minano M.J., LaVoi N.M., Barr-Anderson D.J. Interventions to promote physical activity among young and adolescent girls: A systematic review. Health Educ Res. 2011;26:1025–1049. doi: 10.1093/her/cyr040. [DOI] [PubMed] [Google Scholar]
- 101.Tones K. Evaluating health promotion: A tale of three errors. Patient Educ Couns. 2000;39:227–236. doi: 10.1016/s0738-3991(99)00035-x. [DOI] [PubMed] [Google Scholar]
- 102.Curran G.M., Bauer M., Mittman B., Pyne J.M., Stetler C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50:217–226. doi: 10.1097/MLR.0b013e3182408812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Shea B.J., Reeves B.C., Wells G. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi: 10.1136/bmj.j4008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Basu S., Meghani A., Siddiqi A. Evaluating the health impact of large-scale public policy changes: Classical and novel approaches. Annu Rev Public Health. 2017;38:351–370. doi: 10.1146/annurev-publhealth-031816-044208. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.