

Abstract
Severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection causes coronavirus disease-19 (COVID-19), which is characterized by clinical manifestations such as pneumonia, lymphopenia, severe acute respiratory distress, and cytokine storm. S glycoprotein of SARS-CoV-2 binds to angiotensin-converting enzyme II (ACE-II) to enter into the lungs through membrane proteases consequently inflicting the extensive viral load through rapid replication mechanisms. Despite several research efforts, challenges in COVID-19 management still persist at various levels that include (a) availability of a low cost and rapid self-screening test, (b) lack of an effective vaccine which works against multiple variants of SARS-CoV-2, and (c) lack of a potent drug that can reduce the complications of COVID-19. The development of vaccines against SARS-CoV-2 is a complicated process due to the emergence of mutant variants with greater virulence and their ability to invoke intricate lung pathophysiology. Moreover, the lack of a thorough understanding about the virus transmission mechanisms and complete pathogenesis of SARS-CoV-2 is making it hard for medical scientists to develop a better strategy to prevent the spread of the virus and design a clinically viable vaccine to protect individuals from being infected. A recent report has tested the hypothesis of T cell immunity and found effective when compared to the antibody response in agammaglobulinemic patients. Understanding SARS-CoV-2-induced changes such as “Th-2 immunopathological variations, mononuclear cell & eosinophil infiltration of the lung and antibody-dependent enhancement (ADE)” in COVID-19 patients provides key insights to develop potential therapeutic interventions for immediate clinical management. Therefore, in this review, we have described the details of rapid detection methods of SARS-CoV-2 using molecular and serological tests and addressed different therapeutic modalities used for the treatment of COVID-19 patients. In addition, the current challenges against the development of vaccines for SARS-CoV-2 are also briefly described in this article.
1. Introduction
SARS-CoV-2 infection spreads through the respiratory droplets when an infected person is in close contact with other individuals [1]. To date, there are wide ranges of therapies developed and evaluated for the effective management of COVID-19. For instance, the existing treatment methods such as antiviral drugs (remdesivir), antibodies (intravenous hyperimmunoglobulin therapy), anti-inflammatory drugs (statins, dexamethasone), immunomodulatory therapies, anticoagulants, and antifibrotics are reported to exhibit different therapeutic efficacies during COVID-19 treatment [2, 3]. However, currently, there is no single therapeutic modality proven effective apparently to mitigate this disease progression in hospitalized COVID-19 patients [1].
1.1. Structure and Pathophysiology of SARS-CoV-2
Coronavirus exhibits a crown-like appearance due to surface spike (S) glycoproteins when observed under the electron microscope [4]. Coronavirus is composed of a cis-acting RNA genome to foster the viral replication in host cells through RNA-dependent RNA polymerase [5, 6]. Besides, both cis- and trans-acting viral elements participate in spike (S) protein synthesis, coronaviral encapsidation, and packaging into host cells [7]. The spike glycoproteins consist of S1 and S2 heterotrimer subunits, in which S2 subunit significantly conserved with fusion peptide, a transmembrane domain, and a cytoplasmic domain [5] (Figure 1). Mutations in the genes coding for S protein induced the replacement of glycine (G) at 723 positions with serine (S) and isoleucine with proline (P) at 1010 amino acid position. These mutations in S proteins reported were to enhance the invading potential of SARS-CoV-2 [8]. CoV 229E and OC43 strains are detrimental to humans by causing common cold and lower respiratory infections in several immunocompromised patients [9–11]. The coronavirus-induced pathophysiology varies significantly in terms of its impact on alveolar inflammation, neutrophil infiltration, and immune responses during interstitial pneumonia [10, 12–14]. Recent studies have also shown that SARS-CoV-2 infection leads to multiple organ damage, which is due to severe cytokine storm.
Figure 1.
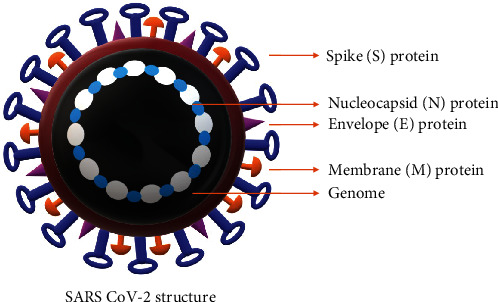
Schematic representation of the structure of SARS-CoV-2: SARS-CoV-2 is an enveloped virus containing RNA genome. The envelope contains spike (S) protein, nucleocapsid (N) protein, envelope protein (E), and membrane protein (M).
2. Modes of Transmission of SARS-CoV-2
Current studies have demonstrated that the infected individual can transmit SARS-CoV-2 virus to an average of 2.2 individuals, which is causing a significant increase in the number of individuals suffering from this disease [15]. Even though the virus is reported to be originated in animals and transmitted to humans, the subsequent transmission is primarily through respiratory mode [15]. Respiratory transmission is either by large droplets with virions of a size larger than 5 μm or aerosols smaller than 5 μm expelled out directly from the respiratory tract by the patient. These infectious droplets are reported to remain suspended in the air for an extended period of time and can travel up to 2 to 3 meters distance before they become inactive [16, 17].
Studies have reported a significant reduction in the risk of respiratory transmission of SARS-CoV-2 if a suitable mask is used [18–23]. Studies have shown a fomite or direct contact-mediated transmission of SARS-CoV-2 [24] when patients share common facilities (restrooms, elevators) and follow a poor hand hygiene [25–28]. Furthermore, the vertical transmission of SARS-CoV-2 has been reported in neonates, where three neonates tested positive for IgM on day 2 after birth while the other tested positive within 16 hours after delivery [28, 29]. Although a case report described transplacental transmission of SARS-CoV-2 [30–33], the transmission from breast milk to infants has not been reported yet. Likewise, the transmission of SARS-CoV-2 through the sexual, fecal, oral, and blood also has not been reported.
S proteins are responsible for the viral particle adherence and docking to the human cell surface receptors such as ACE-II [34]. The binding efficacy of S proteins in SARS-CoV-2 to the ACE-II is “10 to 20 times” stronger compared to the binding efficacy of SARS virus reported in 2002; hence, the spread of SARS-CoV-2 from one person to another is much higher and induces the viral-mediated pathophysiology [35]. Despite several structural similarities between SARS-CoV-2 and SARS virus, the antibodies that were effective against SARS failed to neutralize SARS-CoV-2; hence, targeting SARS-CoV-2 using these antibodies is not feasible, which poses a challenging task to medical scientists to develop a potent and specific approach for mitigating SARS-CoV-2 infection [4].
3. Need for the Improvement of Existing SARS-CoV-2 Detection Methods
Detection of SARS-CoV-2 is the preliminary step in testing, tracing, treating, and the management COVID-19. Therefore, a sensitive and low-cost screening test is highly essential. The existing SARS-CoV-2 detection tests are broadly divided into (a) molecular methods and (b) serological methods. The molecular methods detect “viral RNA” in the biopsy of nasal tissue (collected using a swab) of the infected individual by using reverse transcription polymerase chain reaction (RT-PCR) (Table 1) [36, 37]. Since the collection of nasal swabs can cause irritation to the soft tissues, studies are currently in progress to check whether saliva could be used to detect SARS-CoV-2 [38]. Andrew Brooks, the Chief Operating Officer (COO) and Director of Technology Development, Rutgers University Cell and DNA Repository (RUCDR) Infinite Biologics, has developed a saliva test, which requires the COVID-19 suspect to spit the saliva in a cup (Table 1). This test has received emergency use authorization approval from the United States Food and Drug Administration (USFDA). Recent studies are encouraging the collection of saliva as diagnostic fluid sample rather than the nasopharyngeal swab for detecting SARS-CoV-2 [38]. USFDA has authorized 22 companies to distribute these testing kits [39]. However, to date, the Indian Council of Medical Research (ICMR), Government of India, has not approved any saliva-based rapid antigen tests for screening and identification of SARS-CoV-2-infected individuals. World Health Organization (WHO) and the Center for Disease Control (CDC) are currently using more advanced RT-PCR-based tests for detecting SARS-CoV-2 accurately. The testing kits developed by Abbott can take about 5 minutes, whereas the rapid testing kits designed by other companies usually require more than 30 minutes to produce reliable detection results [39].
Table 1.
List of rapid methods used for detecting SARS-CoV-2.
| Diagnostic tests | Mechanism | Sample | Advantages | Limitations |
|---|---|---|---|---|
| Direct tests | ||||
| RT-PCR | SARS-CoV-2-specific hybridization probes are used to target envelope (E), RNA-dependent RNA polymerase (RdRp), and ORF1b and N regions of the virus. This test can detect the virus at least after two days after infection | Upper respiratory tract (URT) and lower respiratory tract (LRT) specimens | This test is a gold standard method for the diagnosis in symptomatic and asymptomatic patients. This test has a high sensitivity (~89%) and specificity (99%) | Needs infrastructure, very expensive, and requires qualified personnel |
| Reverse transcription loop-mediated isothermal amplification | Exponential amplification of virus-specific genes at a constant temperature | URT and LRT specimens | High sensitivity and specificity | Needs infrastructure, very expensive, and requires trained personnel |
| Nucleoprotein (NP) antigen detection test | Enzyme-linked immunoassay has a microplate precoated with specific antibodies against SARS-CoV-2 NP and the use of horseradish peroxidase- (HRP-) labeled secondary antibody | URT and LRT specimens and saliva | Simple and rapid technique. No trained personnel and expensive laboratory instruments are required | Less sensitivity (70-86%) and specificity (95-97%) when compared to RT-PCR |
| Indirect tests | ||||
| ELISA | Detects anti-SARS-CoV-2 IgG and IgM by identifying antibodies against the NP and spike proteins | Serum, plasma, whole blood | Widely used technique, inexpensive, easy sample collection, and high sensitivity (~82%) and high specificity (97%) | Needs infrastructure and trained personnel |
| Chemiluminescent immunoassay | Light-producing chemical reactions estimate the titers of IgG and IgM by the amount of the emitted luminous signal | Serum, plasma, whole blood | High-throughput and sensitive (77.9%) technique | Needs infrastructure and trained personnel |
| Rapid detection kits | Device with colloidal gold-labeled SARS-CoV-2 recombinant protein and murine anti-human IgG antibodies | Fingerpick blood samples | No need of infrastructure, easy sample collection results in 10-15 min | Low sensitivity (~88.6%) and specificity (~90.63%) |
Even though several detection methods have been developed, RT-PCR is considered as the gold standard for detection of SARS-CoV-2. The details presented in the table show various diagnostic approaches that have been developed in the detection of SARS-CoV-2.
Now, Wyllie and colleagues have examined the possibility of using saliva for diagnosis (salivaomics) and concluded that saliva could be used as an alternative for nasopharyngeal swab [40]. PCR data not only provides an absolute quantification of the number of copies of mRNA but also yields key information about the total viral load for efficient assessment of disease severity [40, 41]. Since appropriate standards are simultaneously subjected to amplification in parallel with saliva, the qPCR is considered as a more precise method to decipher the exact viral load [40]. However, the qPCR test is time-consuming and requires expertise to interpret the results [42].
3.1. Serological Tests for the Diagnosis of SARS-CoV-2
Unlike molecular tests, the serological tests can detect the antibodies produced against SARS-CoV-2 in the infected or recovered individuals using enzyme-linked immunosorbent assay (ELISA) [43]. The turnaround time (TAT) for serological tests is only 15 minutes; therefore, these diagnostic kits are the preferred choice for the rapid analysis of samples [36]. According to these tests, the presence of IgM indicates “recent exposure”, whereas the presence of IgG indicates “infection in late-stage” [43]. Although serological tests are much easier to execute, they are associated with certain limitations, viz., (a) lack of efficacy to detect the infection at a very early stage due to time gap required to generate antibodies in the body, (b) yielding many false-negative results, and (c) generation of false-positive results if the individual is infected with other related coronaviruses such as HKU1, NL63, OC43, and 229E. Currently, FDA has approved a unique serological test developed by Cellex, USA (Cellex qSARS-CoV-2 IgG/IgM rapid test). Few other companies such as Bodysphere have also announced 2-minute rapid detection methods; however, these tests still require clearance/approval from FDA, USA. The serological test results alone cannot be considered as a confirmatory test, as it requires further validation using molecular tests [39]. Furthermore, the utility of serological tests alone for detecting SARS-CoV-2 is still in debate among medical communities due to their poor accuracy and false positive/negative results [44].
In addition to the above strategies for viral detection, Zhang et al. reported the “CRISPR-Cas13-based SHERLOCK” (specific high sensitivity enzymatic reporter unLOCKing) technique for SARS-CoV-2 diagnosis. The protocol incorporated the Cas13, which targets the S gene, Cas13 enzyme, and ORF1ab gene [45], but this procedure requires further validation using COVID-19 patient samples. Procedurally, the technique involves isothermal amplification of RNA samples using recombinase and polymerase, followed by the incubation of amplified viral RNA with Cas13 enzyme, guide RNA, and reporter. Using a paper dipstick, the distinct band produced by the cleaved reporter is visualized [46].
Council of Scientific and Industrial Research-Institute of Genomics and Integrative Biology (CSIR-IGIB), New Delhi, Government of India, has developed a low-cost “paper-strip based laboratory test” to detect SARS-CoV-2 using CRISPR-Cas9 technology. The test is simple and low-cost (about Rs.500 (five hundred rupees only)) and does not require high-end equipment such as a real-time PCR machine [47]. In addition, this test does not involve the isolation of RNA and conversion of isolated RNA into cDNA and the requirement of PCR reagents etc., which are essential for other molecular testing kits. However, this test requires further validation to establish accuracy and sensitivity and is currently waiting for approval from regulatory authorities in India. At present, a total of 158 RT-PCR kits were validated and approved by the Indian Council of Medical Research (ICMR), Government of India, for screening and testing of SARS-CoV-2-induced COVID-19.
Although the above testing methods could detect the SARS-CoV-2 in infected individuals, the lack of specificity and sensitivity is a major problem and may generate false positive and negative results. Therefore, the prospective research should focus immediately to improve the specificity and sensitivity of SARS-CoV-2 detection methods in clinical samples [36]. One specific approach, which has been gaining medical importance, is the combined detection of SARS-CoV-2 RNA and its viral protein(s) using a signal amplification strategy rather than a “target amplification” procedure. This signal amplification strategy was successfully implemented and demonstrated to be effective in yielding many reliable results in the detection of HPV [48].
3.2. Methods of Sampling for Testing and Tracing COVID-19 Patients
Sampling methods do play a crucial role in detecting SARS-CoV-2. Studies have reported the identification of SARS-CoV-2 in respiratory secretions [49–56], feces or rectal swabs [57–61], blood [43, 60, 62–64], oral fluid [40, 65–67], ocular fluids [68–72], urine [73, 74], semen [75], brain tissue [76], and cerebrospinal fluid [77]. Therefore, the choice of sampling method depends on the clinical presentation and the time since the onset of symptoms. Respiratory tissues are the preferred samples to diagnose COVID-19. Table 2 summarizes various sampling methods used in the detection of SARS-CoV-2.
Table 2.
List of various sampling methods currently in the usage for SARS-CoV-2 detection.
| Type of specimen used for COVID-19 testing | Stage of sample collection | Description |
|---|---|---|
| Upper respiratory specimens: nasopharyngeal and oropharyngeal swabs | Early-stage infections (asymptomatic or mild cases) | Individual nasopharyngeal swabs are reported to be more reliable [49, 60, 78, 79]. Combining nasopharyngeal and oropharyngeal swabs increases sensitivity and reliability for detecting COVID-19 [79–82] |
| Lower respiratory specimens: sputum, endotracheal aspirate, bronchoalveolar lavage | Later in the course of the disease, the individuals with strong clinical suspicion of COVID-19 test negative with URT sampling [56, 60, 80, 83] | Sputum is not recommended because of an increase in aerosol transmission [84]. Requires consultation by a physician. Invasive sampling method |
| Oral fluid collection methods (i) Posterior oropharyngeal fluid/saliva (spitting/drooling) (ii) Collection of oral fluid using pipette or sponges (iii) Gargling with saline solutions |
Individuals with clinical symptoms tested negative for URT | Less invasive and lower risk of exposure to other upon collection, when compared with the collection of URT specimens, therefore suitable for mass screening But not recommended by WHO as the sole specimen type for routine clinical diagnosis [85–88] |
| Serum specimens | One collected in the acute phase and the other in the convalescent phase (2-4weeks) | Considered when nucleic acid amplification tests negative |
| Fecal specimens | Second week after the onset of symptoms | Considered when there is clinical suspicion of COVID-19, but URT and LRT are negative [89] |
| Postmortem specimens (postmortem swabs, needle biopsy, or tissue specimen) | Collected during autopsy | For pathological and microbiological testing [89–95] |
URT: upper respiratory tract; LRT: lower respiratory tract; WHO: World Health Organization.
4. Strategies Targeting SARS-CoV-2: Development of Pharmacological Agents to Mitigate and Treat SARS-CoV-2 Infection
According to WHO, the fatality rate of COVID-19 patients has been increasing across the globe due to lack of selective therapeutic interventions and potent vaccines [96]. Existing vaccines and drug combinations are either selective to a particular variant of the virus or exhibit systemic toxicity. Therefore, it is crucial to develop potent, pan-specific, and long-lasting vaccines and better pharmacological agents for the prevention and treatment of SARS-CoV-2 infections (Table 3). The combination of alpha-interferon and anti-HIV drugs lopinavir/ritonavir has shown minimal success and proven to be toxic in recent studies [97] (Figure 2). Currently, a broad-spectrum antiviral drug remdesivir (developed by Gilead Sciences, Inc.) is being used for the treatment [97]. A recent study demonstrated the efficacy of two lead compounds 11a and 11b in vitro, which were synthesized using a structure-based drug design approach to target viral main protease (Mpro), and reported good pharmacokinetic and safety profile in animals [98]. However, further studies are warranted to consider these drugs for clinical use. Similarly, many other studies have also reported the development of drugs targeting various viral proteins and postinfection events [97, 99].
Table 3.
Key molecular targets of pharmacological agents tested against SARS-CoV-2.
| Drugs | Target | Description |
|---|---|---|
| Remdesivir | RNA-dependent RNA polymerase enzyme | Used in the treatment of individuals with mild-to-moderate COVID-19 [128, 129] Inhibit viral RNA synthesis It did not reduce mortality, the need for mechanical ventilation, or the duration of hospital stay |
| Tocilizumab | Interleukin-6 (IL-6) | Used in the treatment of severe cytokine release syndrome In COVID-19 patients, it reduces the use of mechanical ventilation and improves lung function [130, 131] More clinical validations are required [131] |
| Hydroxychloroquine | Target the binding of S protein to ACE2 receptor [132] | HCQ did not effectively prevent COVID-19 infections as it could not slow down the disease progression, pneumonia, acute respiratory distress, and death |
| Lopinavir/ritonavir | 3CLpro-CoV protease cleaves polyproteins during viral replication and assembly | The combination is used in the treatment of mild, moderate, and severe COVID-19 infection by suppressing the viral load [128] More clinical validations are required |
| Favipiravir | RNA-dependent RNA polymerase enzyme | Inhibits viral RNA synthesis; more clinical validations are required |
| Triazavirin | RNA-dependent RNA polymerase enzyme | Inhibits viral RNA synthesis; more clinical validations are required |
| Umifenovir | Blocks the viral entry to the host | Showed no effect in reducing viral load in COVID-19 patients |
| Corticosteroids—dexamethasone | Proinflammatory genes coding cytokines, chemokines, cell adhesion molecules, inflammatory enzymes, and receptors [129, 133] | Recommended for patients with severe COVID-19; reduces lung inflammation, duration of mechanical ventilation, and mortality [134], but not recommended to the patients comorbid with diabetes due to the chances of mucormycosis (black fungus) growth |
Figure 2.
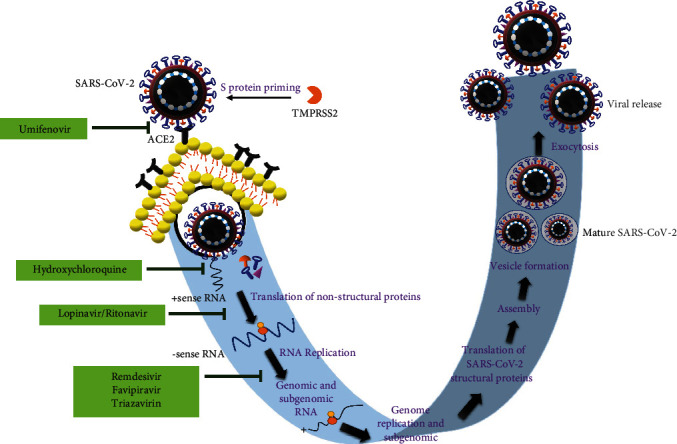
The mechanism of action of umifenovir, lopinavir/ritonavir, remdesivir, favipiravir, triazavirin, and hydroxychloroquine in the treatment of SARS-CoV-2-mediated pathophysiology.
Decreasing the viral load in infected individuals is one of the main strategies and considered by many investigators to reduce the COVID-19 complications. Supporting this idea, interestingly, the fatality rate was reported to be significantly low in pediatric patients as they have relatively low seroprevalence compared to adults [97, 99, 100]. Favipiravir is a derivative of pyrazinecarboxamide, which acts by inhibiting RNA-dependent RNA polymerase [97]. Favipiravir is available for the treatment of COVID-19 patients at mild-to-moderate phase. Therefore, a preventive strategy using a potent vaccine is urgently required. However, efforts in developing a potent vaccine are still in progress.
The development of a vaccine requires a thorough knowledge about viral surface glycoproteins (in the case of enveloped viruses such as SARS-CoV-2) and capsid proteins (in the case of nonenveloped proteins) [97]. The genome of SARS-CoV-2 encodes both structural (spike—S; membrane—M, envelope—E, and nucleocapsid—N) and nonstructural proteins that play crucial roles in the assembly and rapid spread of virus among the population [101]. SARS-CoV-2, similar to CoV-NL63, can use ACE-II receptors, which is a characteristic antigenic commonality of several coronaviruses with zoonotic potential [100]. ACE-II is extensively expressed in the gastrointestinal tract where viral shedding is marginally prolonged in the stools due to ACE-II binding. Despite extensive similarities between SARS-CoV and SARS-CoV-2 (>90% similarity between SARS-CoV and SARS-CoV-2 N, E, and M proteins and 76% similarity in S proteins), the available knowledge about key immunological epitopes, which are responsible for antibody and T cell responses, is very minimal [101]. Therefore, developing an effective vaccine against SARS-CoV-2 is still a major challenge.
4.1. Monoclonal Antibodies (MABs) against SARS-CoV-2
COVID-19 patients are characterized by the presence of a dysregulated immune system, hyperinflammation, and very high IL-6 levels. IL-6 is one of the key cytokines implicated in COVID-19 severity and patient mortality [102–104]. Genomic analysis revealed that critically ill patients with COVID-19 exhibit genetic variations in IL-6-mediated inflammatory pathway proteins, which cause life-threatening disease [105]. The accumulation of lymphocytes, inflammatory monocytes, and other mediators such as apoptotic proteins and thrombotic factors results in pulmonary damage in these patients [106–109]. In addition to vascular permeability, the IL-6 can foster endothelial dysfunction; hence, IL-6 is an attractive drug target for mitigating the complications of COVID-19 [110, 111] (Figure 2). For instance, the administration of tocilizumab to COVID-19 patients resulted in the impaired activity of IL-6α receptors, which consequently fostered good clinical outcomes in these patients [112–114]. This was confirmed by several case reports, retrospective observational cohort studies, and randomized clinical trials. According to COVACTA phase 3 clinical trial, tocilizumab efficiently mitigated COVID-19-induced clinical manifestations such as fever and pneumonia [102–105, 115–117].
Sarilumab is another monoclonal antibody reported to be effective against SARS-CoV-2 by inactivating IL-6-mediated acute inflammatory responses [116–118]. It has proven efficacy in mitigating cytokine storm. Clinical usage of sarilumab was further confirmed by enhancement in patient survival and mitigation of multiple organ damage in critically ill patients with COVID-19[119–123].
4.2. Baricitinib and COVID-19
Adaptive COVID-19 treatment trial-2 (ACCT-2) has tested the benefit of combining baricitinib (a specific inhibitor of Janus kinase-1 and Janus kinase-2) with remdesivir in critically ill patients of COVID-19. Both primary and secondary clinical outcomes are reported to be satisfactory [124]. In addition, two reports of Cantini et al. (2020) also concluded the efficacy of baricitinib in inducing the impairment of JAK1 and JAK2, which consequently blocked the immune cascades and viral replication [125–127]. However, the supplemental oxygen through mechanical ventilation is an intriguing subject of research in COVID-19 patients who are receiving baricitinib and dexamethasone.
5. Challenges in the Development of Vaccines against SARS-CoV-2
Recent studies have shown that T cell responses against viral structural proteins are more immunogenic and long-lasting (up to 11 years of postinfection) when compared to nonstructural proteins and antibodies [101]. In a recent report, Walls et al. (2020) have identified a set of epitopes in S and N structural proteins that can launch an effective response against SARS-CoV-2 [101]. Furthermore, the authors of this study have incorporated significant details about the epitope associated with MHC alleles so that a wide population range can be covered globally [101]. Virus-specific effector memory T cells can encounter coronaviral strains thereby mitigate the complications of infections [135]. In the case of SARS-CoV and MERS-CoV, these viruses can use non- or subneutralizing antibodies and induce immune responses via the antibody-dependent enhancement (ADE), a kind of Trojan horse mechanism [136, 137]. ADE is involved in several viral infections such as Zika virus, Ebola, SARS-CoV, SARS-CoV-2, and HIV [136, 137]. In the case of SARS-CoV-2, the significant immune mechanism occurs via CD32a-mediated ADE, which limits the efficacy of current vaccination [96]. CD32 is an extensively expressed protein on the surface of monocytes and macrophages (ex. alveolar macrophages), which gets aggregated by IgG.
T cell responses are crucial when compared to the humoral responses as these T cell responses have a significant influence on the recovery from primary infection and avoid reinfection [97]. These immune responses can influence vaccine development against COVID-19. The vaccination should enhance both humoral immunity and cellular responses in order to prevent COVID-19-induced complications [138, 139]. In the first phase, the virus infection can be mitigated to reduce initial viral load and control the spread of SARS-CoV-2 to other respiratory organs. In the next phase, the cellular immune responses become significant and help in mitigating the inflammatory phase of COVID-19 disease. In the case of convalescent plasma therapy, the humoral response could be triggered by the vaccine to confer protection against SARS-CoV-2 [97].
5.1. Current Status and Challenges for COVID-19 Vaccination
The development of safe and efficacious vaccines against SARS-CoV-2 is a challenging task [4]. Previously, vaccines against coronaviruses were developed using passive/active immunization and used the animal models for SARS-CoV replication. This is due to the nonavailability of authentic animal models for the development of coronavirus vaccines [140–142]. The passive transfer of immune serum can mitigate the SARS-CoV load in naive BALB/c mice [143]. Earlier, Cheng et al. (2005) have reported the efficacy of “SARS-CoV neutralizing antibodies in SARS hyperimmune globulin” isolated from human convalescent-phase plasma for neutralizing the SARS-CoV infection [144]. Human SARS-CoV administration to animal models has been reported to mitigate the outbreaks of coronavirus infection suggesting that future studies should uncover these mechanisms for SARS-CoV-2 infection [4, 145–147]. However, many experimental studies must be conducted to ascertain the activity of MABs for their neutralizing efficacy by analyzing the immune memory repertoire of COVID-19 patients. Even though the usage of antiviral drugs, viz., proteinase inhibitors, calpain inhibitors, nucleoside analogues, interferons, and siRNAs against SARS-CoV-2 infection, is reported in recent times, several conflicting results with wide variations in clinical outcomes have been generated, which necessitate a global approach for the development of effective vaccines [148–153]. Therefore, a concerted effort is urgently warranted to develop a potent and clinically viable vaccine against SARS-CoV-2 [154].
Reverse genetics technology may be another important strategy to develop vaccines against coronavirus infections [153]. Recent reports have described the efficacy of both mutant and chimeric recombinant viruses to uncover the function of S protein in coronavirus [155, 156]. Reverse genetics has been widely used to elucidate the “structure/function relationship of viral UTRs at 5′ → 3′ of the genome” and the “function of replicase gene for enzymatic activity” in mediating coronaviral replication and pathogenesis [155, 157]. In addition, this strategy is significantly essential to express foreign gene sequences in place of noncoding genes which can help in the development of attenuated vaccines against coronaviruses [158–161].
5.2. Antibody-Dependent Enhancement (ADE) and SARS-CoV-2 Vaccines
The extensive immune backfiring induced through ADE is one of the critical reactions associated with SARS-CoV-2 infection. ADE is progressively produced from this viral infection followed by the induction of Th2 immunopathology, which further blocks the attempts to develop a safe and effective vaccine against SARS-CoV-2. ADE can modulate the immune reactions and induce sustained inflammation, lymphopenia, and cytokine storm, which further lead to the severe disease and death. ADE also requires prior exposure to similar antigenic epitopes most likely from the circulating viruses [162]. For instance, the neutralizing antibodies exhibit a greater ability to block viral entry, fusion without additional immune mediators, although the Fc region is mandatory for neutralizing the influenza virus [163]. In the case of SARS-CoV, the viral docking on ACE-2 was potentially impaired by the administration of neutralizing antibodies since they can recognize and block receptor-binding domain (RBD) and heptad repeat 2 (HR2) domain on the spike (S) protein [164]. Neutralizing antibodies could foster the immune activities of phagocytes, complement, and NK cells [162]. SARS-CoV-2-specific antibodies significantly can induce lung pathology through ADE engagement with Fc receptors that are expressed on several immune cells such as monocytes, macrophages, and B cells [165]. This process is predominantly independent of ACE-2 expression, pH, and host membrane proteases. Thus, the internalization of ADE-induced immune cascades can foster inflammation and tissue damage by mitigating the anti-inflammatory cytokines IL-10 and TGF-β and enhance the levels of the proinflammatory chemokines CCL2 and CCL3 (Figure 3) [166, 167]. However, the underlying mechanisms associated with ADE-mediated immune reaction in SARS-CoV-2 infection are yet to be investigated for effective vaccine development [136, 165].
Figure 3.
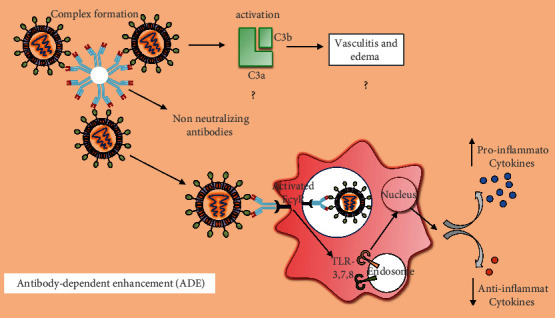
The process of antibody-dependent enhancement (ADE) in lung cells. Entry of SARS-CoV-2, which is mediated by ACE-2 receptors on lung cells, further actuates inflammatory cascades through the production of pathogen-specific antibodies followed by ADE. ADE consequently induces lung pathology through the engagement with Fc receptors expressed on several immune cells, viz., monocytes and macrophages. Internalization of ADE-induced immune cascades can foster inflammation and tissue damage by modulating the inflammatory factors in lung cells.
5.3. Th2 Immunopathology and SARS-CoV-2 Vaccines
The significant roles of host Th2 immunopathology and Th17 inflammatory responses are responsible for pneumonia and edema in the COVID-19 pathogenesis [168] (Figure 4). Release of IL-17 and granulocyte-macrophage colony-stimulating factor (GM-CSF) exacerbates viral immunopathological events by mitigating Treg cells and enhancing the neutrophil migration with concomitant induction of Th2 responses in the lungs [168, 169]. IL-6-mediated Th17 differentiation can foster lung pathology during SARS infection [170]. Th2-type immunopathology along with eosinophil infiltration has been observed with SARS vaccination against SARS-CoV in mouse models [171]. However, confirmatory studies are yet to be performed for IL-6-mediated Th17 responses during SARS-CoV-2 infection to develop anti-IL-6 monoclonal antibodies as new therapeutic interventions [114, 172]. RBD-based subunit vaccine is expected to be safer compared to other vaccines, which may induce Th2 immunopathology [173].
Figure 4.
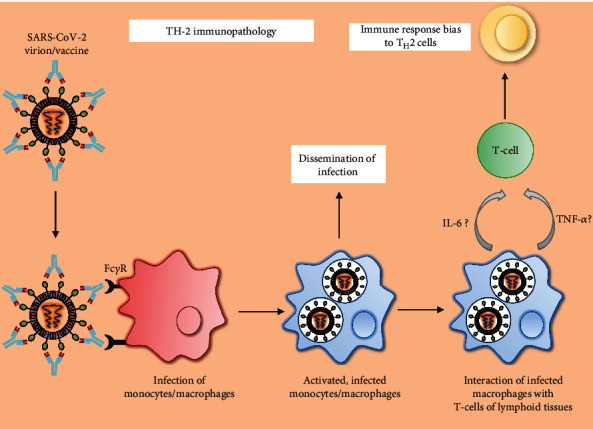
Sequence of events involved in SARS-CoV-2-induced Th2 immunopathology: antibody-bound SARS-CoV-2 virion interacts with the FcγR of host monocytes/macrophages. Virus-infected macrophages are not only responsible for various complications of the disease but also interact with T cells of lymphoid tissues in the host, which leads to the aggravated inflammatory responses which were reported in COVID-19.
The attenuated whole virus vaccine may elicit a significant immune response against SARS-CoV-2 because this virus uses ACE-2 receptors to enter into human cells [174]. Another method is to develop a subunit vaccine, which may induce sensitization of the immune system to foster immune response against S protein subunits of SARS-CoV-2 [153, 175]. In addition, recent studies are currently evaluating the efficacy of nucleic acid vaccines against SARS-CoV-2 to combat COVID-19 [176–178].
6. Recent Trends in the Development of Vaccines
As of 13th April 2021, a total of 166 vaccines have been registered; among which, 89 are under clinical trials in humans. A list of vaccines developed against SARS-CoV-2 is given in Table 4 and Figure 5. On 16th January 2021, the COVID-19 vaccines Covishield (Oxford-AstraZeneca and Serum Institute of India) and Covaxin (Bharat Biotech) were launched in India. Initially, these vaccines were made available for healthcare and frontline workers. As of 1st March 2021, these vaccines are also made available for individuals aged above 60 years of age and the ones aged between 45 and 59 years with comorbid conditions like cancer, diabetes, and hypertension. To date, worldwide, approximately 825 million vaccine doses have been administered. However, there is an immediate requirement for safe and effective vaccines as the number of SARS-CoV-2 infected cases is increasing at alarming rates with a current global estimate of 138,027,200 confirmed cases.
Table 4.
Current stage of vaccines and their manufacturer.
| Types of vaccine | Vaccine name | Phase | Manufacturer | Country of origin |
|---|---|---|---|---|
| mRNA vaccine | mRNA1273 | Phase 3 | Moderna | US |
| Comirnaty | Phase 2/3 | Pfizer-BioNtech | Multinational | |
| Protein subunits | EpiVacCorona | Phase 3 | Vector Institute | Russia |
| NUX-CoV2373 | Phase 3 | Novavax | Australia | |
| Inactivated virus | BBIBP-CorV | Phase 3 | Sinopharm | China |
| CoronaVac | Phase 3 | Sinovac | China | |
| Name not announced | Phase 3 | Sinopharm-Wuhan | China | |
| Covaxin | Phase 3 | Bharat Biotech | India | |
| DNA-based vaccine | Convidecia | Phase 3 | CanSino | China |
| JNJ-78436735 | Phase 3 | Johnson & Johnson | The Netherlands, US | |
| Sputnik V | Phase 3 | Gamaleya | Russia | |
| Covishield (AZD1222) | Phase 2/3 | Oxford-AstraZeneca | UK |
Figure 5.
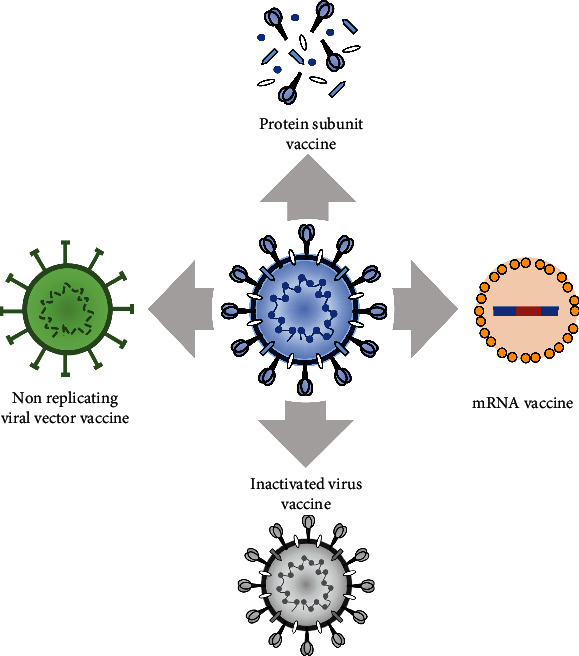
Schematic depiction of the four different kinds of vaccines, viz., nonreplicating viral vector vaccine, mRNA-based vaccine, inactivated virus vaccine, and protein subunit-based vaccine.
6.1. mRNA-Based Vaccines
6.1.1. mRNA-1273
The mRNA-1273, an mRNA vaccine, was developed by Boston-based Moderna therapeutics and the National Institute of Allergy and Infectious Diseases (NIAID), USA. The vaccine encodes the prefusion form of the SARS-CoV-2 spike protein in a lipid nanoparticle vector. Upon administration, mRNA undergoes transcription and translation to produce viral antigens. The immune system recognizes these viral antigens and initiates an adaptive immune response against the S protein of SARS-CoV-2. The preclinical studies on BALB/cJ, C57BL/6J, and B6C3F1/J mice showed induction of virus-specific antibodies upon administering intramuscular doses of 1 μg mRNA-1273, 3 weeks apart [179]. The phase 1 trial began on March 16th, 2020, with 45 healthy volunteers of age between 18 and 55 years. They were administered with three different doses (25 μg, 100 μg, and 250 μg), and the second dose was after four weeks. The trial reported a strong CD4+ T cell response and produced neutralizing antibodies, while CD8+ T cell responses were recorded by the medium-level dose (100 μg)[180, 181]. Myalgia, fatigue, headache, chills, and pain at the injection site were side effects recorded only after the second dose of vaccination and were prominent only in the group who had received the highest dose (250 μg). In a study of 40 older adults (56-70 years or ≥71 years), the immunogenic response was similar to 18-55 years, indicating its efficacy and less immunocompetency in all age groups. In the phase 2 trial, 300 young and 300 older adults were recruited to determine the ability of 25 μg and 100 μg doses. The data reported significant immunogenic responses at 100 μg dose. Phase 3 trials began on July 27th, 2020, with 30,420 participants in the USA, where half of the participants (15,210) received two doses of 100 μg of mRNA-1273 and other half received the placebo [182]. A total of 196 participants have shown symptomatic COVID-19 illness; among which, only 11 participants were vaccinated with mRNA-1273 indicating 94.1% [183] efficacy without any long-term adverse effects. Pain and redness at the injection site, myalgia, arthralgia, headache, and fatigue were the short-term adverse effects reported after the second dose. The vaccine remains stable at 2°C to 8 °C for 30 days, -20°C for 6 months, and room temperature up to 12 hours [184].
6.1.2. BNT162b2
BNT162b2 (Comirnaty®; BioNTech and Pfizer) was developed and manufactured by Pfizer, Biopharmaceutical New Technologies, and Shanghai-based Fosun Pharma. This vaccine has been approved for usage in several countries, viz., Bahrain, Brazil, New Zealand, Saudi Arabia, and Switzerland [185]. In the preliminary trials of this vaccine in BALB/c mice, the effective humoral anti-SARS-CoV-2 immune response was reported without any clinical signs of disease. The immunized mice showed CD8+ and CD4+ T lymphocytes activation and neutralizing antibodies, which was determined by a GFP-encoded vector on the envelope of SARS-CoV-2 [185]. In phase 1 trials, participants of age groups 18-55 years and 65-85 years showed minimum side effects when administered with BNT162b1 and BNT162b2[185]. Even though high-dose-dependent neutralizing antibodies were produced by both the candidates, BNT162b2 reported to produce less reactivity in older adults with a 30 μg dose range; therefore, this vaccine candidate is considered for large-scale phase 2/3 studies [185, 186]. The phase2/3 trial began on July 27th, 2020, with 43,488 volunteers. The study participants included individuals with comorbid conditions. The two-dose immunization with 30 μg of BNT162b vaccine induced neutralizing anti-SARS-CoV-2 antibodies and rendered 95% protection against the disease [187]. The most frequent side effects of this vaccine were fatigue and headache [187].
6.2. Nonreplicating Viral Vector Vaccine
6.2.1. Ad5-nCoV
The replication-defective vector vaccines, which are under phase 3 trial, are Ad5-nCoV, AZD1222, Sputnik V, and JNJ-78436735 [187]. Ad5-nCoV is a vaccine candidate that encodes the S protein of SARS-CoV-2 into host cells. It was developed by CanSino Biologics and the Institute of Biology of the Academy of Military Medical Sciences (AMMS), China [188]. The preclinical studies on BALB/c mice with a dose of intramuscularly or intranasally injected Ad5-nCoV induced humoral response, which subsequently enhanced the levels of neutralizing antibodies against SARS-CoV-2[188]. Results of phase 1 trial on 108 participants of age group between 18 and 60 showed that doses of 5 × 1010 and 1 × 1011 viral particles/dose were safe and produced good immunogenicity in study participants [189]. In phase 2 trial with 508 participants of age group 18-83, both the doses showed an equal immune response; however, mild adverse effects were reported in 74% and 72% of participants in the lower and higher dose groups, respectively [190]. The phase 3 trial was initiated in September 2020 with a dose of 5 × 1010 viral particles/dose in 40,000 volunteers in Saudi Arabia, Russia, and Pakistan. However, Central Military Commission of China has restricted the use of this vaccine in the military [187].
6.2.2. AZD1222
AZD1222 was developed by Oxford University and AstraZeneca, using a chimpanzee adenovirus (ChAdOx1) vector, which encodes the spike protein of wild-type SARS-CoV-2. In preclinical studies, the intramuscular administration of two doses of AZD1222 to BALB/c and CD1 mice had generated a high immunogenic profile [191]. Subsequent studies have evaluated the efficacy of this vaccine even in pigs. Further analysis using “lentiviral-based SARS-CoV-2 pseudovirus neutralization assay” reported significantly enhanced neutralizing antibodies in the study groups. In the phase 1 study of 1090 healthy volunteers of age group 18-55 years, single or double dose (5 × 1010 viral particles/dose) of AZD1222 exhibited no side effects but produced a strong neutralizing responses against the virus [191, 192]. During August 2020, phase 3 trials were initiated with 30,000 participants in the USA, India, Brazil, Russia, and South Africa [193]. However, due to severe neurological symptoms, the phase 3 studies were temporarily halted in September 2020 [193]. In-depth investigations should be performed to delineate prominent causes for such severe neurological symptoms; however, preliminary phase 3 trial concluded that these effects were due to undiagnosed multiple sclerosis at the time of vaccination, but not related to the vaccine [193]. The phase 3 study was resumed in other countries, except the USA. Results of phase 3 reported 70.4% efficiency without any severe effects. The vaccine has been approved for use in the UK on November 27th, 2020, in Argentina on December 20th, 2020, and in India on January 3rd, 2021 [194].
6.2.3. Sputnik V
Gamaleya, a Russian Research Institute, developed an adenoviral vector vaccine named Sputnik V [195]. Results of the phase 1/2 trial, which involved 38 participants, have shown an excellent immunogenic profile with mild side effects, myalgia, arthralgia, fever, headache, and minimal pain at the site of injection [187, 195]. Concerns regarding the vaccine's safety and efficacy were raised, as the Health Ministry approved the Russian Federation's vaccine before phase 3 trials. On September 7th, 2020, the phase 3 trial was initiated by recruiting 40,000 individuals across Russia and the Republic of Belarus. After a detailed analysis of 18,794 individuals, 91.4% efficacy was reported from the phase 3 study [195]. However, eight participants were tested COVID-19 positive among the vaccinated group. The vaccine trial has not reported any adverse effects except that some of the individuals experienced mild side effects such as fatigue and headache [187, 195].
6.2.4. JNJ-78436735
It is a replication-defective adenovirus vector (JNJ-78436735) developed by Janssen Pharmaceuticals (Johnson & Johnson) [187]. The vector is engineered for expressing the stabilized prefusion S protein of SARS-CoV-2 in the host. This vaccine was tested in Syrian golden hamsters with a single injection of the vaccine candidate, which resulted in the production of neutralizing antibodies against SARS-CoV-2 and reduced the severity of the disease and mortality. Studies on rhesus macaques reported a significant induction of antibody and T cell-mediated responses. The phase 1/2 trials were initiated in July 2020. Two different doses (0.5 × 1011/dose or 1 × 1011/dose) were administered to the participants of two different groups. Whereas the first group is composed of 402 individuals aged 18-55 years, the second group consisted of 394 individuals aged 65 years or above. According to this trial report, only mild symptoms such as fever, pain at the injection site, and headache were reported upon administration of this vaccine. Approximately, 80% of vaccinated individuals showed CD4+ T cell responses [187, 196, 197]. Phase 3 studies for this vaccine were initiated in the month of September 2020 with 60,000 individuals. The trial was paused because of the development of severe adverse effects in one of the vaccinated individuals; however, the exact clinical manifestations are not reported. The manufacturer announced the second phase 3 study, which involved recruiting 30,000 adults from Belgium, Colombia, France, Germany, Philippines, South Africa, Spain, United Kingdom, and USA [198].
6.3. Inactivated Virus Vaccine
6.3.1. CoronaVac
CoronaVac is an inactivated virus vaccine candidate with alum adjuvant. CoronaVac was developed by Sinovac Research and Development Co. A recent study reported high immunogenic profile of CoronaVac in BALB/c mice and Wistar rats. This vaccine reported to induce the activation of SARS-CoV-2-specific neutralizing antibodies. A study was performed on rhesus macaques to determine the efficacy of this vaccine, and the outcome of this study has concluded complete protection against SARS-CoV-2. The phase 2 study was conducted in 600 healthy participants aged between 18 and 59 years, who had received two different vaccine doses (3 and 6 μg/0.5 ml) [199, 200]. As per this study, subjects in both dosage groups exhibited mild adverse reactions and induced more than 90% seroconversion. In the phase 3 trial, a total of 8870 participants from Brazil, Indonesia, and Turkey were recruited and administered with two vaccine doses (2 weeks interval). Finally, this vaccine has been approved in China [187].
6.3.2. Wuhan Institute of Biological Products and Sinopharm Vaccines
An inactivated virus was isolated from WIV04 SARS-CoV-2 strain from a Jinyintan Hospital patient, Wuhan [201]. This vaccine candidate was developed by the Wuhan Institute of Biological Products and Sinopharm by inactivating the virus with β-propiolactone and alum adjuvant adsorption procedure [201]. In the phase 1 trial, three different doses (2.5 μg, 5.0 μg, and 10 μg) were administered to 96 participants of aged 18 to 59 years. In the phase 2 trial, 224 participants were recruited and administered two doses of 5.0 μg each [187]. Administration of the vaccine triggered mild adverse effects but induced the activation of neutralizing antibodies against SARS-CoV-2. This vaccine was approved only in China and in the United Arab Emirates [187, 201].
6.3.3. BBIBP-CorV
BBIBP-CorV is an inactivated virus isolated from 19nCoV-CDC-Tan-HB02 strain of SARS-CoV-2. The vaccine is developed by Sinopharm and the Beijing Institute of Biological Products [202]. Studies on animal models demonstrated the production of neutralizing antibodies against SARS-CoV-2 and rendered protection against SARS-CoV-2 [202, 203]. In the phase 1 study, a total of 192 participants were recruited and administered with one of the three different doses of the vaccine (2.0 μg, 4.0 μg, or 8.0 μg). Fever in 10% of participants was observed as an adverse effect. In the phase 2 trials, a total of 448 participants were recruited and administered either one dosage of 8.0 μg or two doses of 4.0 μg of vaccine at 2, 3, or 4 weeks apart [202]. Results of this trial showed a high immunogenicity and excellent safety profile with 4.0 μg/dose with an interval of 3 weeks. Furthermore, the vaccine has been examined for its efficacy in a phase 3 trial in Argentina, Bahrain, Jordan, Egypt, and UAE., among 63,000 participants. Two doses of vaccine (4.0 μg) in 3 weeks were administered. The vaccine was approved for public administration in UAE, Bahrain, China, and Egypt [202].
6.3.4. Covaxin
Covaxin is developed by India-based Bharat Biotech. and the Indian Council of Medical Research, Government of India. It is an inactivated virus developed in Vero CCL-81 cells [204]. The vaccine is isolated from an Indian strain inactivated by β-propiolactone along with the alum and imidazoquinoline adjuvant adsorption procedure. The inactivated whole SARS-CoV-2 virion was absorbed into the alum and Algel. This vaccine exhibited a significant reduction in the viral loads and bronchoalveolar infection in animal models [204]. Later, the phase 1 trial was conducted on 375 participants with three different formulations and two different dosages (3.0 μg or 6.0 μg). The vaccine showed a high safety and immunogenicity profile with mild-to-moderate adverse effects with a seroconversion rate of 93.4% in the 3.0 μg dosage group [205]. The phase 3 trials were launched on October 23rd, 2020, in India, with a total of 26,000 study participants of different age groups. The participants have received a vaccine dosage of 3.0 μg in the adjuvant formulation and compared with control groups in the study (2 doses/4 weeks apart). The use of this vaccine has been approved in India and currently in usage for the vaccination of the general public [205].
6.4. Protein Subunit Vaccine
6.4.1. NUX-CoV2373
NUX-CoV2373 is a protein subunit vaccine developed by Novavax. It is a recombinant SARS-CoV-2 S glycoprotein nanoparticle in a baculovirus-Sf9 vector with an adjuvant Matrix M1 [206, 207]. The adjuvant vaccine formulation was investigated in animal models (BALB/c mice), and it has shown a significant increase in the antibody production and strong T cell response [207]. In the phase 1/2 trial, 131 healthy participants received a total of two doses of the vaccine with and without adjuvant. The results of this trial reported a significant increase in the “immune response with vaccine”. Furthermore, anti-S IgG and neutralizing antibody levels were comparatively higher in the vaccinated subjects than those in the convalescent sera of COVID-19 patients [208]. First phase 3 trial was launched on September 23rd, 2020, with 9000 participants in the United Kingdom. Second phase 3 trial of this vaccine was initiated in the US with 30,000 participants in collaboration with Serum Institute of India. The study participants have been receiving a vaccine dosage of 5.0 μg dose with 50 μg of Matrix M1 adjuvant. Results of this study are yet to be announced [208].
7. COVID-19 Vaccines: Choices in a Crisis
Despite having a viable vaccine, the search for a more potent and pan-SARS-CoV-2-specific vaccine continues as the virus is capable of acquiring mutations and exhibits significantly variable pathophysiological effects. For instance, in a recent report, a total of 771 variants of SARS-CoV-2 were identified in India. Moreover, several hurdles, concerns, and queries regarding the safety and quality of the vaccines still persist, for example, (a) the demand for a vaccine against the COVID-19 pandemic far exceeds the supply. Hence, there is a shortage of vaccines to meet the increasing demand; (b) confusion about the safety and efficacy of existing vaccines. In this regard, the efforts have to be made to increase the percolation of information to the public [209, 210]; (c) the feasibility of producing and transporting the vaccine as per the requirement in several countries; (d) whether the vaccine is safer to administer to the “pregnant women and the individuals suffering from chronic health complications such as heart diseases”; and (e) the feasibility of supplying the vaccine at free of cost or at affordable price for the general public. Therefore, further studies are warranted to address all these queries, which will help to understand more about the vaccine and encourage individuals to attend vaccination camps for timely vaccination.
8. Safety Concerns Pertaining to COVID-19 Vaccines
In general, vaccination is known to induce minimal and transient side effects such as antigen-antibody-mediated reactions, urticaria, fever, and rare skin reactions, which may subside without any major interventions. However, questions about the safety of vaccines arise when the adverse events become a major health concern. Clinical trials of the BNT162b2 mRNA COVID-19 vaccine have been reported to cause minimal local and systemic side effects, viz., pain, redness, fatigue, joint pain, and muscle pain within 1 to 2 days of vaccination [211]. The excipients such as polyethylene glycol (PEG) derivatives may trigger mild anaphylactic adverse reactions upon administration [212]. Anaphylaxis is a serious adverse reaction that can foster asphyxiation, cardiovascular collapse, and multiorgan dysfunction, and sometimes may lead to death [212]. Therefore, it is crucial to delineate prompt recognition of these adverse effects. In general, the anaphylactic reactions are mediated by the mast cell activation via antigen binding and IgE cross-linking. Consequently, these events could trigger the tissue generation of inflammatory mediators such as histamines, prostaglandins, and leukotrienes and foster the development of hives, tachycardia, hypotension, and cardiovascular collapse. Tryptase is higher in blood at the time of both IgE-mediated anaphylaxis and non-IgE-mediated anaphylaxis. The characteristic release of tryptase from mast cells is indicative of the release of inflammatory mediators through mast cells [213]. These effects have raised concerns about the potential adverse risks after vaccine administration in a public community [214]. Therefore, appropriate measures should be taken to minimize these side effects. Further, proper education and awareness about vaccines should be provided to address these concerns and queries associated with vaccine safety and efficacy.
9. Conclusions and Future Directions
SARS-CoV-2 can actuate both innate and adaptive immunities in humans. The uncontrolled inflammatory cascades and blockade of adaptive immune function could induce lung tissue damage at local and systemic levels. Moreover, a drastic decline in the levels of CD4+ T cells, CD8+ T cells, B cells, monocytes, eosinophils, and natural killer (NK) cells was observed in COVID-19 patients. Significant improvement has been observed in the early detection of SARS-CoV-2 in the infected patients due to the development of new serological testing and diagnostic methods. Furthermore, the vaccine development using immunological approaches to block viral entry and replication is associated with a significant limitation of SARS-CoV-2-induced immunopathology. Although the mRNA-based and DNA-based vaccines and protein subunit-based vaccines have been developed, the COVID-19-induced immunopathological changes such as antibody-dependent enhancement (ADE) and Th2 immunopathology have significant implications in developing suitable antiviral agents. Hence, these aspects should be considered while designing a potent vaccine. Furthermore, studies should also focus on developing a drug-antibody conjugate, which can bind to the viral proteins while mitigating the exacerbations in already infected individuals.
Acknowledgments
SVT would like to thank the Indian Council of Medical Research (CMR, Govt. of India) for the award of a senior research fellowship (SRF) as a part of an extramural research grant (No. 54/06/2019-HUM/BMS dated 22nd November 2019) sanctioned to Dr. M.N. Suma, Professor and Head, Department of Biochemistry, JSS Medical College, JSS Academy of Higher Education & Research, Mysore, Karnataka, India. SVM would like to thank the Special Interest Group in Cancer Biology and Cancer Stem Cells (SIG-CBCSC), JSS Medical College, JSS Academy of Higher Education & Research, Mysore, Karnataka, India. Professor Aliev would like to acknowledge GALLY International Research Institute, San Antonio, TX, USA.
Additional Points
Human and Animal Rights. No animal or human was used in this study. All data were collected from open scientific and public sources.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
Narasimha M. Beeraka (NMB), SubbaRao V. Tulimilli (SVT), Medha Karnik (MK), Surya P. Sadhu (SPS), Rajeswara Rao Pragada (RRP), SubbaRao V. Madhunapantula (SVM), and Gjumrakch Aliev (GA) collected the literature. NMB, MK, SPS, and SVT collected and prepared tables and figures. NMB, RRP, SVM, and GA conceptualized and developed the sections and proofread the manuscript. All authors reviewed and approved the manuscript before submission. Prof. Gjumrakch Aliev passed away in the month of December 2020. This article is dedicated to late Prof. Gjumrakch Aliev.
References
- 1.Wiersinga W. J., Rhodes A., Cheng A. C., Peacock S. J., Prescott H. C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324(8):782–793. doi: 10.1001/jama.2020.12839. [DOI] [PubMed] [Google Scholar]
- 2.Sanders J. M., Monogue M. L., Jodlowski T. Z., Cutrell J. B. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;323(18):1824–1836. doi: 10.1001/jama.2020.6019. [DOI] [PubMed] [Google Scholar]
- 3.Wang M., Cao R., Zhang L., et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Research. 2020;30(3):269–271. doi: 10.1038/s41422-020-0282-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cascella M., Rajnik M., Cuomo A., Dulebohn S. C., Di Napoli R. StatPearls [Internet] StatPearls Publishing; 2020. Features, evaluation and treatment coronavirus (COVID-19) [PubMed] [Google Scholar]
- 5.Nichol S., Beaty B., Elliot R., et al. Virus Taxonomy: VIIIth Report of the International Committee on Taxonomy of Viruses. Elsevier Academic Press; 2005. VIIIth report of the International Committee on Taxonomy of Viruses. [Google Scholar]
- 6.Wei X., She G., Wu T., Xue C., Cao Y. PEDV enters cells through clathrin-, caveolae-, and lipid raft-mediated endocytosis and traffics via the endo-/lysosome pathway. Veterinary Research. 2020;51(1):1–18. doi: 10.1186/s13567-020-0739-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chan J. F.-W., Kok K.-H., Zhu Z., et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerging Microbes & Infections. 2020;9(1):221–236. doi: 10.1080/22221751.2020.1719902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Angeletti S., Benvenuto D., Bianchi M., Giovanetti M., Pascarella S., Ciccozzi M. COVID-2019: the role of the nsp2 and nsp3 in its pathogenesis. Journal of Medical Virology. 2020;92(6):584–588. doi: 10.1002/jmv.25719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Birch C., Clothier H., Seccull A., et al. Human coronavirus OC43 causes influenza-like illness in residents and staff of aged-care facilities in Melbourne, Australia. Epidemiology and Infection. 2005;133(2):273–277. doi: 10.1017/S0950268804003346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miura T. A., Wang J., Holmes K. V., Mason R. J. Rat coronaviruses infect rat alveolar type I epithelial cells and induce expression of CXC chemokines. Virology. 2007;369(2):288–298. doi: 10.1016/j.virol.2007.07.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pene F., Merlat A., Vabret A., et al. Coronavirus 229E-related pneumonia in immunocompromised patients. Clinical Infectious Diseases. 2003;37(7):929–932. doi: 10.1086/377612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wojcinski Z., Percy D. Sialodacryoadenitis virus-associated lesions in the lower respiratory tract of rats. Veterinary Pathology. 1986;23(3):278–286. doi: 10.1177/030098588602300308. [DOI] [PubMed] [Google Scholar]
- 13.Jacoby R., Bhatt P., Jonas A. Pathogenesis of sialodacryoadenitis in gnotobiotic rats. Veterinary Pathology. 1975;12(3):196–209. doi: 10.1177/030098587501200305. [DOI] [PubMed] [Google Scholar]
- 14.Bhatt P., Jacoby R. Experimental infection of adult axenic rats with Parker’s rat coronavirus. Archives of Virology. 1977;54(4):345–352. doi: 10.1007/BF01314779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Guo Z.-D., Wang Z.-Y., Zhang S.-F., et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerging Infectious Diseases. 2020;26(7):p. 1586. doi: 10.3201/eid2607.200885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wei J., Li Y. Airborne spread of infectious agents in the indoor environment. American Journal of Infection Control. 2016;44(9):S102–S108. doi: 10.1016/j.ajic.2016.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fennelly K. P. Particle sizes of infectious aerosols: implications for infection control. The Lancet Respiratory Medicine. 2020;8(9):914–924. doi: 10.1016/S2213-2600(20)30323-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chu D. K., Akl E. A., Duda S., et al. Physical distancing, face masks, and eye protection to prevent person-to- person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta- analysis. The Lancet. 2020;395(10242):1973–1987. doi: 10.1016/S0140-6736(20)31142-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee J. K., Jeong H. W. Wearing face masks regardless of symptoms is crucial for preventing the spread of COVID-19 in hospitals. Infection Control and Hospital Epidemiology. 2021;42(1):115–116. doi: 10.1017/ice.2020.202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mitze T., Kosfeld R., Rode J. Face masks considerably reduce Covid-19 cases in Germany. Proceedings of the National Academy of Sciences. 2020;117(51):32293–32301. doi: 10.1073/pnas.2015954117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lyu W., Wehby G. L. Community use of face masks and COVID-19: evidence from a natural experiment of state mandates in the US. Health Affairs. 2020;39(8):1419–1425. doi: 10.1377/hlthaff.2020.00818. [DOI] [PubMed] [Google Scholar]
- 22.Chou R., Dana T., Jungbauer R., Weeks C., McDonagh M. S. Masks for prevention of respiratory virus infections, including SARS-CoV-2, in health care and community settings: a living rapid review. Annals of Internal Medicine. 2020;173(7):542–555. doi: 10.7326/M20-3213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Courtemanche C., Garuccio J., Le A., Pinkston J., Yelowitz A. Strong social distancing measures in the United States reduced the COVID-19 growth rate. Health Affairs. 2020;39(7):1237–1246. doi: 10.1377/hlthaff.2020.00608. [DOI] [PubMed] [Google Scholar]
- 24.Deng W., Bao L., Gao H., et al. Ocular conjunctival inoculation of SARS-CoV-2 can cause mild COVID-19 in rhesus macaques. Nature Communications. 2020;11(1):1–7. doi: 10.1038/s41467-020-18149-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wang Y., Tian H., Zhang L., et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Global Health. 2020;5(5, article e002794) doi: 10.1136/bmjgh-2020-002794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ran L., Chen X., Wang Y., Wu W., Zhang L., Tan X. Risk factors of healthcare workers with coronavirus disease 2019: a retrospective cohort study in a designated hospital of Wuhan in China. Clinical Infectious Diseases. 2020;71(16):2218–2221. doi: 10.1093/cid/ciaa287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.van Kampen J. J., van de Vijver D. A., Fraaij P. L., et al. Shedding of infectious virus in hospitalized patients with coronavirus disease-2019 (COVID-19): duration and key determinants. 2020. MedRxiv. [DOI] [PMC free article] [PubMed]
- 28.Cheng H.-Y., Jian S.-W., Liu D.-P., Ng T.-C., Huang W.-T., Lin H.-H. Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset. JAMA Internal Medicine. 2020;180(9):1156–1163. doi: 10.1001/jamainternmed.2020.2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Alzamora M. C., Paredes T., Caceres D., Webb C. M., Valdez L. M., La Rosa M. Severe COVID-19 during pregnancy and possible vertical transmission. American Journal of Perinatology. 2020;37(8):861–865. doi: 10.1055/s-0040-1710050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Patanè L., Morotti D., Giunta M. R., et al. Vertical transmission of coronavirus disease 2019: severe acute respiratory syndrome coronavirus 2 RNA on the fetal side of the placenta in pregnancies with coronavirus disease 2019-positive mothers and neonates at birth. American Journal of Obstetrics & Gynecology MFM. 2020;2(3, article 100145) doi: 10.1016/j.ajogmf.2020.100145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Baud D., Greub G., Favre G., et al. Second-trimester miscarriage in a pregnant woman with SARS-CoV-2 infection. JAMA. 2020;323(21):2198–2200. doi: 10.1001/jama.2020.7233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Vivanti A. J., Vauloup-Fellous C., Prevot S., et al. Transplacental transmission of SARS-CoV-2 infection. Nature Communications. 2020;11(1):1–7. doi: 10.1038/s41467-020-17436-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Alamar I., Abu-Arja M. H., Heyman T., et al. A possible case of vertical transmission of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a newborn with positive placental in situ hybridization of SARS-CoV-2 RNA. Journal of the Pediatric Infectious Diseases Society. 2020;9(5):636–639. doi: 10.1093/jpids/piaa109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Li W., Moore M. J., Vasilieva N., et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. 2003;426(6965):450–454. doi: 10.1038/nature02145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Wrapp D., Wang N., Corbett K. S., et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020;367(6483):1260–1263. doi: 10.1126/science.abb2507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Udugama B., Kadhiresan P., Kozlowski H. N., et al. Diagnosing COVID-19: the disease and tools for detection. ACS Nano. 2020;14(4):3822–3835. doi: 10.1021/acsnano.0c02624. [DOI] [PubMed] [Google Scholar]
- 37.Emery S. L., Erdman D. D., Bowen M. D., et al. Real-time reverse transcription–polymerase chain reaction assay for SARS-associated coronavirus. Emerging Infectious Diseases. 2004;10(2):311–316. doi: 10.3201/eid1002.030759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wyllie A. L., Fournier J., Casanovas-Massana A., et al. Saliva is more sensitive for SARS-CoV-2 detection in COVID-19 patients than nasopharyngeal swabs. 2020. Medrxiv.
- 39.Billingsley A. The latest in coronavirus (COVID-19) testing methods and availability. 2020;10:p. 2020. [Google Scholar]
- 40.Wyllie A. L., Fournier J., Casanovas-Massana A., et al. Saliva or nasopharyngeal swab specimens for detection of SARS-CoV-2. New England Journal of Medicine. 2020;383(13):1283–1286. doi: 10.1056/NEJMc2016359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Vogels C. B., Brito A. F., Wyllie A. L., et al. Analytical sensitivity and efficiency comparisons of SARS-CoV-2 RT-qPCR primer-probe sets. Nature Microbiology. 2020;5(10):1299–1305. doi: 10.1038/s41564-020-0761-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Han M., Byun J., Cho Y., Rim J. RT-PCR for SARS-CoV-2: quantitative versus qualitative. The Lancet Infectious Diseases. 2021;21(2):p. 165. doi: 10.1016/S1473-3099(20)30424-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zhang W., Du R.-H., Li B., et al. Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerging Microbes & Infections. 2020;9(1):386–389. doi: 10.1080/22221751.2020.1729071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Green K., Graziadio S., Turner P., Fanshawe T., Allen J. Molecular and antibody point-of-care tests to support the screening, diagnosis and monitoring of COVID-19. Oxford: COVID-19 Evidence Service; 2020. [Google Scholar]
- 45.Zhang F., Abudayyeh O. O., Gootenberg J. S. A protocol for detection of COVID-19 using CRISPR diagnostics. A protocol for detection of COVID-19 using CRISPR diagnostics. 2020;8 [Google Scholar]
- 46.Jalandra R., Yadav A. K., Verma D., et al. Strategies and perspectives to develop SARS-CoV-2 detection methods and diagnostics. Biomedicine & Pharmacotherapy. 2020;129, article 110446 doi: 10.1016/j.biopha.2020.110446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mitra A. Harnessing science, technology and innovation in India for tackling COVID-19. RIS Diary 3rd Special Issue on COVID-19. 2020;16(4):1–35. [Google Scholar]
- 48.Abreu A. L., Souza R. P., Gimenes F., Consolaro M. E. A review of methods for detect human Papillomavirus infection. Virology Journal. 2012;9(1):p. 262. doi: 10.1186/1743-422X-9-262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Zou L., Ruan F., Huang M., et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. The New England Journal of Medicine. 2020;382(12):1177–1179. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Young B. E., Ong S. W. X., Kalimuddin S., et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. 2020;323(15):1488–1494. doi: 10.1001/jama.2020.3204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Pan Y., Zhang D., Yang P., Poon L. L., Wang Q. Viral load of SARS-CoV-2 in clinical samples. The Lancet Infectious Diseases. 2020;20(4):411–412. doi: 10.1016/S1473-3099(20)30113-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Yuan J., Kou S., Liang Y., Zeng J., Pan Y., Liu L. Polymerase Chain Reaction assays Reverted to positive in 25 discharged Patients With COVID-19. Clinical Infectious Diseases. 2020;71(16):2230–2232. doi: 10.1093/cid/ciaa398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tang X., Zhao S., He D., et al. Positive RT-PCR tests among discharged COVID-19 patients in Shenzhen, China. Infection Control and Hospital Epidemiology. 2020;41(9):1110–1112. doi: 10.1017/ice.2020.134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ma H., Hu J., Tian J., et al. A single-center, retrospective study of COVID-19 features in children: a descriptive investigation. BMC Medicine. 2020;18:1–11. doi: 10.1186/s12916-020-01596-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Xiao A. T., Tong Y. X., Zhang S. False negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: rather than recurrence. Journal of Medical Virology. 2020;92(10):1755–1756. doi: 10.1002/jmv.25855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Liu R., Han H., Liu F., et al. Positive rate of RT-PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clinica Chimica Acta. 2020;505:172–175. doi: 10.1016/j.cca.2020.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Zheng S., Fan J., Yu F., et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang Province, China, January-March 2020: retrospective cohort study. BMJ. 2020;369, article m1443 doi: 10.1136/bmj.m1443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lescure F.-X., Bouadma L., Nguyen D., et al. Clinical and virological data of the first cases of COVID-19 in Europe: a case series. The Lancet Infectious Diseases. 2020;20(6):697–706. doi: 10.1016/S1473-3099(20)30200-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Xing Y.-H., Ni W., Wu Q., et al. Prolonged viral shedding in feces of pediatric patients with coronavirus disease 2019. Journal of Microbiology, Immunology and Infection. 2020;53(3):473–480. doi: 10.1016/j.jmii.2020.03.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Wang W., Xu Y., Gao R., et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020;323(18):1843–1844. doi: 10.1001/jama.2020.3786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Wong M. C., Huang J., Lai C., Ng R., Chan F. K., Chan P. K. Detection of SARS-CoV-2 RNA in fecal specimens of patients with confirmed COVID-19: a meta-analysis. Journal of Infection. 2020;81(2):e31–e38. doi: 10.1016/j.jinf.2020.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Chen W., Lan Y., Yuan X., et al. Detectable 2019-nCoV viral RNA in blood is a strong indicator for the further clinical severity. Emerging Microbes & Infections. 2020;9(1):469–473. doi: 10.1080/22221751.2020.1732837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Chen X., Zhao B., Qu Y., et al. Detectable serum Severe Acute Respiratory Syndrome Coronavirus 2 viral load (RNAemia) is closely correlated with drastically elevated interleukin 6 level in critically ill Patients With Coronavirus Disease 2019. Clinical Infectious Diseases. 2020;71(8):1937–1942. doi: 10.1093/cid/ciaa449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Corman V. M., Rabenau H. F., Adams O., et al. SARS-CoV-2 asymptomatic and symptomatic patients and risk for transfusion transmission. Transfusion. 2020;60(6):1119–1122. doi: 10.1111/trf.15841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.To K. K.-W., Tsang O. T.-Y., Leung W.-S., et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. The Lancet Infectious Diseases. 2020;20(5):565–574. doi: 10.1016/S1473-3099(20)30196-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Williams E., Bond K., Zhang B., Putland M., Williamson D. A. Saliva as a non-invasive specimen for detection of SARS-CoV-2. Journal of Clinical Microbiology. 2020;58(8) doi: 10.1128/JCM.00776-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.McCormick-Baw C., Morgan K., Gaffney D., et al. Saliva as an alternate specimen source for detection of SARS-CoV-2 in symptomatic patients using Cepheid Xpert Xpress SARS-CoV-2. Journal of Clinical Microbiology. 2020;58(8) doi: 10.1128/JCM.01109-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Colavita F., Lapa D., Carletti F., et al. SARS-CoV-2 isolation from ocular secretions of a patient with COVID-19 in Italy with prolonged viral RNA detection. Annals of Internal Medicine. 2020;173(3):242–243. doi: 10.7326/M20-1176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Xia J., Tong J., Liu M., Shen Y., Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. Journal of Medical Virology. 2020;92(6):589–594. doi: 10.1002/jmv.25725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Wu P., Duan F., Luo C., et al. Characteristics of ocular findings of patients with coronavirus disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmology. 2020;138(5):575–578. doi: 10.1001/jamaophthalmol.2020.1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Zhou Y., Duan C., Zeng Y., et al. Ocular findings and proportion with conjunctival SARS-COV-2 in COVID-19 patients. Ophthalmology. 2020;127(7):982–983. doi: 10.1016/j.ophtha.2020.04.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Zhang X., Chen X., Chen L., et al. The Evidence of SARS-Cov-2 Infection on Ocular Surface. Elsevier; 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Ling Y., Xu S.-B., Lin Y.-X., et al. Persistence and clearance of viral RNA in 2019 novel coronavirus disease rehabilitation patients. Chinese Medical Journal. 2020;133(9):1039–1043. doi: 10.1097/CM9.0000000000000774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Nomoto H., Ishikane M., Katagiri D., et al. Cautious handling of urine from moderate to severe COVID-19 patients. American Journal of Infection Control. 2020;48(8):969–971. doi: 10.1016/j.ajic.2020.05.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Li D., Jin M., Bao P., Zhao W., Zhang S. Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Network Open. 2020;3(5):e208292–e208292. doi: 10.1001/jamanetworkopen.2020.8292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Paniz-Mondolfi A., Bryce C., Grimes Z., et al. Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) Journal of Medical Virology. 2020;92(7):699–702. doi: 10.1002/jmv.25915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Moriguchi T., Harii N., Goto J., et al. A first case of meningitis/encephalitis associated with SARS-coronavirus-2. International Journal of Infectious Diseases. 2020;94:55–58. doi: 10.1016/j.ijid.2020.03.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Huang Y., Chen S., Yang Z., et al. SARS-CoV-2 viral load in clinical samples from critically ill patients. American Journal of Respiratory and Critical Care Medicine. 2020;201(11):1435–1438. doi: 10.1164/rccm.202003-0572LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Sutjipto S., Lee P. H., Tay J. Y., et al. Open Forum Infectious Diseases. Oxford University Press US; 2020. The effect of sample site, illness duration, and the presence of pneumonia on the detection of SARS-CoV-2 by real-time reverse transcription PCR; p. p. ofaa335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lai C. K., Chen Z., Lui G., et al. Prospective study comparing deep throat saliva with other respiratory tract specimens in the diagnosis of novel coronavirus disease 2019. The Journal of Infectious Diseases. 2020;222(10):1612–1619. doi: 10.1093/infdis/jiaa487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Hammitt L. L., Kazungu S., Welch S., et al. Added value of an oropharyngeal swab in detection of viruses in children hospitalized with lower respiratory tract infection. Journal of Clinical Microbiology. 2011;49(6):2318–2320. doi: 10.1128/JCM.02605-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Ek P., Böttiger B., Dahlman D., Hansen K. B., Nyman M., Nilsson A. C. A combination of naso- and oropharyngeal swabs improves the diagnostic yield of respiratory viruses in adult emergency department patients. Infectious Diseases. 2019;51(4):241–248. doi: 10.1080/23744235.2018.1546055. [DOI] [PubMed] [Google Scholar]
- 83.Winichakoon P., Chaiwarith R., Liwsrisakun C., et al. Negative nasopharyngeal and oropharyngeal swabs do not rule out COVID-19. Journal of Clinical Microbiology. 2020;58(5) doi: 10.1128/JCM.00297-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.W H Organization. Clinical management of COVID-19: interim guidance, 27 May 2020. World Health Organization; 2020. [Google Scholar]
- 85.Hamid H., Khurshid Z., Adanir N., Zafar M. S., Zohaib S. COVID-19 pandemic and role of human saliva as a testing biofluid in point-of-care technology. European Journal of Dentistry. 2020;14(S 01):S123–S129. doi: 10.1055/s-0040-1713020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Alizargar J., Etemadi Sh M., Aghamohammadi M., Hatefi S. Saliva samples as an alternative for novel coronavirus (COVID-19) diagnosis. Journal of the Formosan Medical Association. 2020;119(7):1234–1235. doi: 10.1016/j.jfma.2020.04.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Ceron J. J., Lamy E., Martinez-Subiela S., et al. Use of saliva for diagnosis and monitoring the SARS-CoV-2: a general perspective. Journal of Clinical Medicine. 2020;9(5):p. 1491. doi: 10.3390/jcm9051491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Chen L., Zhao J., Peng J., et al. Detection of 2019-nCoV in saliva and characterization of oral symptoms in COVID-19 patients. SSRN Electronic Journal. 2020;3556665 doi: 10.2139/ssrn.3556665. [DOI] [Google Scholar]
- 89.Ng S. C., Chan F. K., Chan P. K. Screening FMT donors during the COVID-19 pandemic: a protocol for stool SARS- CoV-2 viral quantification. The Lancet Gastroenterology & Hepatology. 2020;5(7):642–643. doi: 10.1016/S2468-1253(20)30124-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Tang J. W., To K. F., Lo A. W., Sung J. J., Ng H., Chan P. K. Quantitative temporal-spatial distribution of severe acute respiratory syndrome-associated coronavirus (SARS-CoV) in post-mortem tissues. Journal of Medical Virology. 2007;79(9):1245–1253. doi: 10.1002/jmv.20873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Pomara C., Volti G. L., Cappello F. COVID-19 deaths: are we sure it is pneumonia? Please, autopsy, autopsy, autopsy! Multidisciplinary Digital Publishing Institute; 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Salerno M., Sessa F., Piscopo A., et al. No autopsies on COVID-19 deaths: a missed opportunity and the lockdown of science. Journal of Clinical Medicine. 2020;9(5):p. 1472. doi: 10.3390/jcm9051472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Hanley B., Lucas S. B., Youd E., Swift B., Osborn M. Autopsy in suspected COVID-19 cases. Journal of Clinical Pathology. 2020;73(5):239–242. doi: 10.1136/jclinpath-2020-206522. [DOI] [PubMed] [Google Scholar]
- 94.Basso C., Calabrese F., Sbaraglia M., et al. Feasibility of postmortem examination in the era of COVID-19 pandemic: the experience of a Northeast Italy University Hospital. Virchows Archiv. 2020;477(3):341–347. doi: 10.1007/s00428-020-02861-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Tian S., Xiong Y., Liu H., et al. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Modern Pathology. 2020;33(6):1007–1014. doi: 10.1038/s41379-020-0536-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Kadkhoda K. COVID-19: an immunopathological view. Msphere. 2020;5(2) doi: 10.1128/mSphere.00344-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Lega S., Naviglio S., Volpi S., Tommasini A. Recent insight into SARS-CoV2 immunopathology and rationale for potential treatment and preventive strategies in COVID-19. Vaccine. 2020;8(2):p. 224. doi: 10.3390/vaccines8020224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Dai W., Zhang B., Jiang X.-M., et al. Structure-based design of antiviral drug candidates targeting the SARS-CoV-2 main protease. Science. 2020;368(6497):1331–1335. doi: 10.1126/science.abb4489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Prajapat M., Sarma P., Shekhar N., et al. Drug targets for corona virus: a systematic review. Indian Journal of Pharmacology. 2020;52(1):56–65. doi: 10.4103/ijp.IJP_115_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Gorse G. J., Patel G. B., Vitale J. N., O'Connor T. Z. Prevalence of antibodies to four human coronaviruses is lower in nasal secretions than in serum. Clinical and Vaccine Immunology. 2010;17(12):1875–1880. doi: 10.1128/CVI.00278-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Walls A. C., Park Y.-J., Tortorici M. A., Wall A., McGuire A. T., Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell. 2020;183(6):p. 1735. doi: 10.1016/j.cell.2020.11.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Luo P., Liu Y., Qiu L., Liu X., Liu D., Li J. Tocilizumab treatment in COVID-19: a single center experience. Journal of Medical Virology. 2020;92(7):814–818. doi: 10.1002/jmv.25801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Mastroianni A., Greco S., Apuzzo G., et al. Subcutaneous tocilizumab treatment in patients with severe COVID-19-related cytokine release syndrome: An observational cohort study. EClinicalMedicine. 2020;24:p. 100410. doi: 10.1016/j.eclinm.2020.100410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Kaye A. G., Siegel R. The efficacy of IL-6 inhibitor tocilizumab in reducing severe COVID-19 mortality: a systematic review. PeerJ. 2020;8, article e10322 doi: 10.7717/peerj.10322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Guaraldi G., Meschiari M., Cozzi-Lepri A., et al. Tocilizumab in patients with severe COVID-19: a retrospective cohort study. The Lancet Rheumatology. 2020;2(8):e474–e484. doi: 10.1016/S2665-9913(20)30173-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Aziz M., Fatima R., Assaly R. Elevated interleukin-6 and severe COVID-19: a meta-analysis. Journal of Medical Virology. 2020;92(11):2283–2285. doi: 10.1002/jmv.25948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Zhu J., Pang J., Ji P., et al. Elevated interleukin-6 is associated with severity of COVID-19: a meta-analysis. Journal of Medical Virology. 2021;93(1):35–37. doi: 10.1002/jmv.26085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Varga Z., Flammer A. J., Steiger P., et al. Endothelial cell infection and endotheliitis in COVID-19. The Lancet. 2020;395(10234):1417–1418. doi: 10.1016/S0140-6736(20)30937-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Ackermann M., Verleden S. E., Kuehnel M., et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. New England Journal of Medicine. 2020;383(2):120–128. doi: 10.1056/NEJMoa2015432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Giamarellos-Bourboulis E. J., Netea M. G., Rovina N., et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host & Microbe. 2020;27(6):992–1000.e3. doi: 10.1016/j.chom.2020.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Ruan Q., Yang K., Wang W., Jiang L., Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Medicine. 2020;46(5):846–848. doi: 10.1007/s00134-020-05991-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Rubbert-Roth A., Furst D. E., Nebesky J. M., Jin A., Berber E. A review of recent advances using tocilizumab in the treatment of rheumatic diseases. Rheumatology and Therapy. 2018;5(1):21–42. doi: 10.1007/s40744-018-0102-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Cellina M., Orsi M., Bombaci F., Sala M., Marino P., Oliva G. Favorable changes of CT findings in a patient with COVID-19 pneumonia after treatment with tocilizumab. Diagnostic and Interventional Imaging. 2020;101(5):323–324. doi: 10.1016/j.diii.2020.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Zhang X., Song K., Tong F., et al. First case of COVID-19 in a patient with multiple myeloma successfully treated with tocilizumab. Blood Advances. 2020;4(7):1307–1310. doi: 10.1182/bloodadvances.2020001907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Antwi-Amoabeng D., Kanji Z., Ford B., Beutler B. D., Riddle M. S., Siddiqui F. Clinical outcomes in COVID-19 patients treated with tocilizumab: an individual patient data systematic review. Journal of Medical Virology. 2020;92(11):2516–2522. doi: 10.1002/jmv.26038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Xu X., Han M., Li T., et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proceedings of the National Academy of Sciences. 2020;117(20):10970–10975. doi: 10.1073/pnas.2005615117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Somers E. C., Eschenauer G. A., Troost J. P., et al. Tocilizumab for treatment of mechanically ventilated patients with COVID-19. Clinical Infectious Diseases. 2020 doi: 10.1093/cid/ciaa954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Gremese E., Cingolani A., Bosello S. L., et al. Sarilumab use in severe SARS-CoV-2 pneumonia. EClinicalMedicine. 2020;27:p. 100553. doi: 10.1016/j.eclinm.2020.100553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Stone J. H., Frigault M. J., Serling-Boyd N. J., et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. New England Journal of Medicine. 2020;383(24):2333–2344. doi: 10.1056/NEJMoa2028836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Hermine O., Mariette X., Tharaux P.-L., et al. Effect of tocilizumab vs usual care in adults hospitalized with COVID-19 and moderate or severe pneumonia: a randomized clinical trial. JAMA Internal Medicine. 2021;181(1):32–40. doi: 10.1001/jamainternmed.2020.6820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Salvarani C., Dolci G., Massari M., et al. Effect of tocilizumab vs standard care on clinical worsening in patients hospitalized with COVID-19 pneumonia: a randomized clinical trial. JAMA Internal Medicine. 2021;181(1):24–31. doi: 10.1001/jamainternmed.2020.6615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Rosas I. O., Bräu N., Waters M., et al. Tocilizumab in hospitalized patients with severe Covid-19 pneumonia. New England Journal of Medicine. 2021;384(16):1503–1516. doi: 10.1056/NEJMoa2028700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Veiga V. C., Prats J. A., Farias D. L., et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: randomised controlled trial. BMJ. 2021;372 doi: 10.1136/bmj.n84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Kalil A. C., Patterson T. F., Mehta A. K., et al. Baricitinib plus remdesivir for hospitalized adults with Covid-19. New England Journal of Medicine. 2021;384(9):795–807. doi: 10.1056/NEJMoa2031994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Cantini F., Niccoli L., Matarrese D., Nicastri E., Stobbione P., Goletti D. Baricitinib therapy in COVID-19: a pilot study on safety and clinical impact. The Journal of Infection. 2020;81(2):318–356. doi: 10.1016/j.jinf.2020.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Cantini F., Niccoli L., Nannini C., et al. Beneficial impact of baricitinib in COVID-19 moderate pneumonia; multicentre study. Journal of Infection. 2020;81(4):647–679. doi: 10.1016/j.jinf.2020.06.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Stebbing J., Nievas G. S., Falcone M., et al. JAK inhibition reduces SARS-CoV-2 liver infectivity and modulates inflammatory responses to reduce morbidity and mortality. Science Advances. 2021;7(1):p. eabe4724. doi: 10.1126/sciadv.abe4724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Uzunova K., Filipova E., Pavlova V., Vekov T. Insights into antiviral mechanisms of remdesivir, lopinavir/ritonavir and chloroquine/hydroxychloroquine affecting the new SARS-CoV-2. Biomedicine & Pharmacotherapy. 2020;131:p. 110668. doi: 10.1016/j.biopha.2020.110668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Lamontagne F., Agoritsas T., Macdonald H., et al. A living WHO guideline on drugs for COVID-19. BMJ. 2020;370 doi: 10.1136/bmj.m3379. [DOI] [PubMed] [Google Scholar]
- 130.Sciascia S., Aprà F., Baffa A., et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in patients with severe COVID-19. Clinical and Experimental Rheumatology. 2020;38(3):529–532. [PubMed] [Google Scholar]
- 131.Lan S.-H., Lai C.-C., Huang H.-T., Chang S.-P., Lu L.-C., Hsueh P.-R. Tocilizumab for severe COVID-19: a systematic review and meta-analysis. International Journal of Antimicrobial Agents. 2020;56(3):p. 106103. doi: 10.1016/j.ijantimicag.2020.106103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Sandeep S., McGregor K. Energetics Based Modeling of Hydroxychloroquine and Azithromycin Binding to the SARS-CoV-2 Spike (S)Protein - ACE2 Complex. 2020. [DOI]
- 133.Sterne J. A., Murthy S., Diaz J. V., et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 2020;324(13):1330–1341. doi: 10.1001/jama.2020.17023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Villar J., Ferrando C., Martínez D., et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. The Lancet Respiratory Medicine. 2020;8(3):267–276. doi: 10.1016/S2213-2600(19)30417-5. [DOI] [PubMed] [Google Scholar]
- 135.Hamming I., Timens W., MLC B., Lely A. T., Navis G. J., van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. The Journal of Pathology. 2004;203(2):631–637. doi: 10.1002/path.1570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Wan Y., Shang J., Sun S., et al. Molecular mechanism for antibody-dependent enhancement of coronavirus entry. Journal of Virology. 2020;94(5) doi: 10.1128/jvi.02015-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Walls A. C., Xiong X., Park Y.-J., et al. Unexpected receptor functional mimicry elucidates activation of coronavirus fusion. Cell. 2019;176(5):1026–1039.e15. doi: 10.1016/j.cell.2018.12.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Channappanavar R., Zhao J., Perlman S. T cell-mediated immune response to respiratory coronaviruses. Immunologic Research. 2014;59(1-3):118–128. doi: 10.1007/s12026-014-8534-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Liu W. J., Zhao M., Liu K., et al. T-cell immunity of SARS-CoV: implications for vaccine development against MERS-CoV. Antiviral Research. 2017;137:82–92. doi: 10.1016/j.antiviral.2016.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Navas-Martín S., Weiss S. R. Coronavirus replication and pathogenesis: implications for the recent outbreak of severe acute respiratory syndrome (SARS), and the challenge for vaccine development. Journal of Neurovirology. 2004;10(2):75–85. doi: 10.1080/13550280490280292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Saif L. Animal coronavirus vaccines: lessons for SARS. Developments in Biologicals. 2004;119:129–140. [PubMed] [Google Scholar]
- 142.Saif L. Animal coronaviruses: what can they teach us about the severe acute respiratory syndrome? Revue Scientifique et Technique-Office International des Épizooties. 2004;23(2):643–660. doi: 10.20506/rst.23.2.1513. [DOI] [PubMed] [Google Scholar]
- 143.Subbarao K., McAuliffe J., Vogel L., et al. Prior infection and passive transfer of neutralizing antibody prevent replication of severe acute respiratory syndrome coronavirus in the respiratory tract of mice. Journal of Virology. 2004;78(7):3572–3577. doi: 10.1128/JVI.78.7.3572-3577.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Cheng V., Hung I., Tang B., et al. Viral replication in the nasopharynx is associated with diarrhea in patients with severe acute respiratory syndrome. Clinical Infectious Diseases. 2004;38(4):467–475. doi: 10.1086/382681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Greenough T. C., Babcock G. J., Roberts A., et al. Development and characterization of a severe acute respiratory syndrome—associated coronavirus—neutralizing human monoclonal antibody that provides effective immunoprophylaxis in mice. The Journal of Infectious Diseases. 2005;191(4):507–514. doi: 10.1086/427242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Sui J., Li W., Roberts A., et al. Evaluation of human monoclonal antibody 80R for immunoprophylaxis of severe acute respiratory syndrome by an animal study, epitope mapping, and analysis of spike variants. Journal of Virology. 2005;79(10):5900–5906. doi: 10.1128/JVI.79.10.5900-5906.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Almeida J., Berry D., Cunningham C., et al. Coronaviruses. Nature. 1968;220(5168):p. 650. doi: 10.1038/220650b0. [DOI] [Google Scholar]
- 148.Liu S., Xiao G., Chen Y., et al. Interaction between heptad repeat 1 and 2 regions in spike protein of SARS- associated coronavirus: implications for virus fusogenic mechanism and identification of fusion inhibitors. The Lancet. 2004;363(9413):938–947. doi: 10.1016/S0140-6736(04)15788-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Liu Y.-C., Huang V., Chao T.-C., et al. Screening of drugs by FRET analysis identifies inhibitors of SARS-CoV 3CL protease. Biochemical and Biophysical Research Communications. 2005;333(1):194–199. doi: 10.1016/j.bbrc.2005.05.095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Yang H., Yang M., Ding Y., et al. The crystal structures of severe acute respiratory syndrome virus main protease and its complex with an inhibitor. Proceedings of the National Academy of Sciences. 2003;100(23):13190–13195. doi: 10.1073/pnas.1835675100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Barnard D. L., Hubbard V. D., Burton J., et al. Inhibition of severe acute respiratory syndrome-associated coronavirus (SARSCoV) by calpain inhibitors and β-D-N4-hydroxycytidine. Antiviral Chemistry and Chemotherapy. 2004;15(1):15–22. doi: 10.1177/095632020401500102. [DOI] [PubMed] [Google Scholar]
- 152.Bosch B. J., Martina B. E., van der Zee R., et al. Severe acute respiratory syndrome coronavirus (SARS-CoV) infection inhibition using spike protein heptad repeat-derived peptides. Proceedings of the National Academy of Sciences. 2004;101(22):8455–8460. doi: 10.1073/pnas.0400576101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Weiss S. R., Navas-Martin S. Coronavirus pathogenesis and the emerging pathogen severe acute respiratory syndrome coronavirus. Microbiology and Molecular Biology Reviews. 2005;69(4):635–664. doi: 10.1128/MMBR.69.4.635-664.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Groneberg D. A., Poutanen S. M., Low D. E., Lode H., Welte T., Zabel P. Treatment and vaccines for severe acute respiratory syndrome. The Lancet Infectious Diseases. 2005;5(3):147–155. doi: 10.1016/S1473-3099(05)70022-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.de Haan C. A., van Genne L., Stoop J. N., Volders H., Rottier P. J. Coronaviruses as vectors: position dependence of foreign gene expression. Journal of Virology. 2003;77(21):11312–11323. doi: 10.1128/JVI.77.21.11312-11323.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Haijema B. J., Volders H., Rottier P. J. Live, attenuated coronavirus vaccines through the directed deletion of group-specific genes provide protection against feline infectious peritonitis. Journal of Virology. 2004;78(8):3863–3871. doi: 10.1128/JVI.78.8.3863-3871.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Bosch B. J., de Haan C. A., Rottier P. J. Coronavirus spike glycoprotein, extended at the carboxy terminus with green fluorescent protein, is assembly competent. Journal of Virology. 2004;78(14):7369–7378. doi: 10.1128/JVI.78.14.7369-7378.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Fischer F., Stegen C. F., Koetzner C. A., Masters P. S. Analysis of a recombinant mouse hepatitis virus expressing a foreign gene reveals a novel aspect of coronavirus transcription. Journal of Virology. 1997;71(7):5148–5160. doi: 10.1128/JVI.71.7.5148-5160.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Goebel S. J., Hsue B., Dombrowski T. F., Masters P. S. Characterization of the RNA components of a putative molecular switch in the 3′ untranslated region of the murine coronavirus genome. Journal of Virology. 2004;78(2):669–682. doi: 10.1128/JVI.78.2.669-682.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Marra M. A., Jones S. J., Astell C. R., et al. The genome sequence of the SARS-associated coronavirus. Science. 2003;300(5624):1399–1404. doi: 10.1126/science.1085953. [DOI] [PubMed] [Google Scholar]
- 161.Sarma J. D., Scheen E., Seo S.-h., Koval M., Weiss S. R. Enhanced green fluorescent protein expression may be used to monitor murine coronavirus spread in vitro and in the mouse central nervous system. Journal of Neurovirology. 2002;8(5):381–391. doi: 10.1080/13550280260422686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Tetro J. A. Is COVID-19 receiving ADE from other coronaviruses? Microbes and Infection. 2020;22(2):72–73. doi: 10.1016/j.micinf.2020.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.DiLillo D. J., Palese P., Wilson P. C., Ravetch J. V. Broadly neutralizing anti-influenza antibodies require Fc receptor engagement for in vivo protection. The Journal of Clinical Investigation. 2016;126(2):605–610. doi: 10.1172/JCI84428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Du L., He Y., Zhou Y., Liu S., Zheng B.-J., Jiang S. The spike protein of SARS-CoV -- a target for vaccine and therapeutic development. Nature Reviews Microbiology. 2009;7(3):226–236. doi: 10.1038/nrmicro2090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Iwasaki A., Yang Y. The potential danger of suboptimal antibody responses in COVID-19. Nature Reviews Immunology. 2020;20(6):339–341. doi: 10.1038/s41577-020-0321-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Wang S.-F., Tseng S.-P., Yen C.-H., et al. Antibody-dependent SARS coronavirus infection is mediated by antibodies against spike proteins. Biochemical and Biophysical Research Communications. 2014;451(2):208–214. doi: 10.1016/j.bbrc.2014.07.090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Jaume M., Yip M. S., Cheung C. Y., et al. Anti-severe acute respiratory syndrome coronavirus spike antibodies trigger infection of human immune cells via a pH- and cysteine protease-independent Fc R pathway. Journal of Virology. 2011;85(20):10582–10597. doi: 10.1128/JVI.00671-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Wu D., Yang X. O. TH17 responses in cytokine storm of COVID-19: an emerging target of JAK2 inhibitor fedratinib. Journal of Microbiology, Immunology and Infection. 2020;53(3):368–370. doi: 10.1016/j.jmii.2020.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Hoe E., Anderson J., Nathanielsz J., et al. The contrasting roles of Th17 immunity in human health and disease. Microbiology and Immunology. 2017;61(2):49–56. doi: 10.1111/1348-0421.12471. [DOI] [PubMed] [Google Scholar]
- 170.Zhang Y., Li J., Zhan Y., et al. Analysis of serum cytokines in patients with severe acute respiratory syndrome. Infection and Immunity. 2004;72(8):4410–4415. doi: 10.1128/IAI.72.8.4410-4415.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Tseng C.-T., Sbrana E., Iwata-Yoshikawa N., et al. Correction: Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLoS One. 2012;7(8) doi: 10.1371/annotation/2965cfae-b77d-4014-8b7b-236e01a35492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Hotez P. J., Bottazzi M. E., Corry D. B. The Potential Role of TH17 Immune Responses in Coronavirus Immunopathology and Vaccine-Induced Immune Enhancement. Elsevier; 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Zhu X., Liu Q., Du L., Lu L., Jiang S. Receptor-binding domain as a target for developing SARS vaccines. Journal of Thoracic Disease. 2013;5(2):p. S142. doi: 10.3978/j.issn.2072-1439.2013.06.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174.Hoffmann M., Kleine-Weber H., Krüger N., Mueller M. A., Drosten C., Pöhlmann S. The novel coronavirus 2019 (2019-nCoV) uses the SARS-coronavirus receptor ACE2 and the cellular protease TMPRSS2 for entry into target cells. 2020. BioRxiv.
- 175.Cavanagh D. Severe acute respiratory syndrome vaccine development: experiences of vaccination against avian infectious bronchitis coronavirus. Avian Pathology. 2003;32(6):567–582. doi: 10.1080/03079450310001621198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Takasuka N., Fujii H., Takahashi Y., et al. A subcutaneously injected UV-inactivated SARS coronavirus vaccine elicits systemic humoral immunity in mice. International Immunology. 2004;16(10):1423–1430. doi: 10.1093/intimm/dxh143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Thiel V., Herold J., Schelle B., Siddell S. G. Infectious RNA transcribed in vitro from a cDNA copy of the human coronavirus genome cloned in vaccinia virus. Journal of General Virology. 2001;82(6):1273–1281. doi: 10.1099/0022-1317-82-6-1273. [DOI] [PubMed] [Google Scholar]
- 178.Wang Z., Yuan Z., Matsumoto M., Hengge U. R., Chang Y.-F. Immune responses with DNA vaccines encoded different gene fragments of severe acute respiratory syndrome coronavirus in BALB/c mice. Biochemical and Biophysical Research Communications. 2005;327(1):130–135. doi: 10.1016/j.bbrc.2004.11.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Jackson L. A., Anderson E. J., Rouphael N. G., et al. An mRNA vaccine against SARS-CoV-2—preliminary report. New England Journal of Medicine. 2020;383(20):1920–1931. doi: 10.1056/NEJMoa2022483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Liu L., Wei Q., Lin Q., et al. Anti–spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection. JCI Insight. 2019;4(4) doi: 10.1172/jci.insight.123158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Houser K. V., Broadbent A. J., Gretebeck L., et al. Enhanced inflammation in New Zealand white rabbits when MERS-CoV reinfection occurs in the absence of neutralizing antibody. PLoS Pathogens. 2017;13(8, article e1006565) doi: 10.1371/journal.ppat.1006565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Moderna M. S. COVID-19 vaccine candidate meets its primary efficacy endpoint in the first interim analysis of the phase 3 COVE study. Moderna. 2020;16 [Google Scholar]
- 183.Anderson E. J., Rouphael N. G., Widge A. T., et al. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. New England Journal of Medicine. 2020;383(25):2427–2438. doi: 10.1056/NEJMoa2028436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Kolber M. R., Fritsch P., Price M., et al. COVID-19 vaccine fast facts. Canadian Family Physician. 2021;67(3):185–186. doi: 10.46747/cfp.6703185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Vogel A., Kanevsky I., Che Y., et al. A prefusion SARS-CoV-2 spike RNA vaccine is highly immunogenic and prevents lung infection in non-human primates. 2020. BioRxiv.
- 186.Walsh E. E., Frenck R. W., Jr., Falsey A. R., et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. New England Journal of Medicine. 2020;383(25):2439–2450. doi: 10.1056/NEJMoa2027906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Kyriakidis N. C., López-Cortés A., González E. V., Grimaldos A. B., Prado E. O. SARS-CoV-2 vaccines strategies: a comprehensive review of phase 3 candidates. NPJ Vaccines. 2021;6(1):1–17. doi: 10.1038/s41541-021-00292-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Wu S., Zhong G., Zhang J., et al. A single dose of an adenovirus-vectored vaccine provides protection against SARS-CoV-2 challenge. Nature Communications. 2020;11(1):4081–4087. doi: 10.1038/s41467-020-17972-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.Zhu F.-C., Li Y.-H., Guan X.-H., et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. The Lancet. 2020;395(10240):1845–1854. doi: 10.1016/S0140-6736(20)31208-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 190.Zhu F.-C., Guan X.-H., Li Y.-H., et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: a randomised, double-blind, placebo-controlled, phase 2 trial. The Lancet. 2020;396(10249):479–488. doi: 10.1016/S0140-6736(20)31605-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191.Graham S. P., McLean R. K., Spencer A. J., et al. Evaluation of the immunogenicity of prime-boost vaccination with the replication-deficient viral vectored COVID-19 vaccine candidate ChAdOx1 nCoV-19. NPJ Vaccines. 2020;5(1):1–6. doi: 10.1038/s41541-020-00221-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.van Doremalen N., Lambe T., Spencer A., et al. ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus macaques. Nature. 2020;586(7830):578–582. doi: 10.1038/s41586-020-2608-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Phillips N., Cyranoski D., Mallapaty S. A leading coronavirus vaccine trial is on hold: scientists react. Nature. 2020 doi: 10.1038/d41586-020-02594-w. [DOI] [PubMed] [Google Scholar]
- 194.Voysey M., Clemens S. A. C., Madhi S. A., et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS- CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. The Lancet. 2021;397(10269):99–111. doi: 10.1016/S0140-6736(20)32661-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Logunov D. Y., Dolzhikova I. V., Zubkova O. V., et al. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia. The Lancet. 2020;396(10255):887–897. doi: 10.1016/S0140-6736(20)31866-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196.Corbett K. S., Flynn B., Foulds K. E., et al. Evaluation of the mRNA-1273 vaccine against SARS-CoV-2 in nonhuman primates. New England Journal of Medicine. 2020;383(16):1544–1555. doi: 10.1056/NEJMoa2024671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Sadoff J., Le Gars M., Shukarev G., et al. Interim results of a phase 1–2a trial of Ad26. COV2. S Covid-19 vaccine. New England Journal of Medicine. 2021;384(19):1824–1835. doi: 10.1056/NEJMoa2034201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Ashraf M. U., Kim Y., Kumar S., Seo D., Ashraf M., Bae Y.-S. COVID-19 vaccines (revisited) and oral-mucosal vector system as a potential vaccine platform. Vaccine. 2021;9(2):p. 171. doi: 10.3390/vaccines9020171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Gao Q., Bao L., Mao H., et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science. 2020;369(6499):77–81. doi: 10.1126/science.abc1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200.Zhang Y.-J., Zeng G., Pan H.-X., et al. Immunogenicity and safety of a SARS-CoV-2 inactivated vaccine in healthy adults aged 18-59 years: report of the randomized, double-blind, and placebo-controlled phase 2 clinical trial. 2020 medRxiv.
- 201.Xia S., Duan K., Zhang Y., et al. Effect of an inactivated vaccine against SARS-CoV-2 on safety and immunogenicity outcomes: interim analysis of 2 randomized clinical trials. JAMA. 2020;324(10):951–960. doi: 10.1001/jama.2020.15543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 202.Xia S., Zhang Y., Wang Y., et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a randomised, double-blind, placebo-controlled, phase 1/2 trial. The Lancet Infectious Diseases. 2021;21(1):39–51. doi: 10.1016/S1473-3099(20)30831-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Wang H., Zhang Y., Huang B., et al. Development of an inactivated vaccine candidate, BBIBP-CorV, with potent protection against SARS-CoV-2. Cell. 2020;182(3):713–721.e9. doi: 10.1016/j.cell.2020.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Yadav P., Ella R., Kumar S., et al. Remarkable immunogenicity and protective efficacy of BBV152, an inactivated SARS-CoV-2 vaccine in rhesus macaques. 2020. S0092867420306954
- 205.Ella R., Vadrevu K. M., Jogdand H., et al. Safety and immunogenicity trial of an inactivated SARS-CoV-2 vaccine-BBV152: a phase 1, double-blind, randomised control trial. 2020. S0092867420306954 [DOI] [PMC free article] [PubMed]
- 206.Rajput Z. I., Hu S.-h., Xiao C.-w., Arijo A. G. Adjuvant effects of saponins on animal immune responses. Journal of Zhejiang University. Science. B. 2007;8(3):153–161. doi: 10.1631/jzus.2007.B0153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207.Tian J.-H., Patel N., Haupt R., et al. SARS-CoV-2 spike glycoprotein vaccine candidate NVX-CoV2373 elicits immunogenicity in baboons and protection in mice. 2020. BioRxiv. [DOI] [PMC free article] [PubMed]
- 208.Keech C., Albert G., Cho I., et al. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. New England Journal of Medicine. 2020;383(24):2320–2332. doi: 10.1056/NEJMoa2026920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 209.Kramer D. B., Opel D. J., Parasidis E., Mello M. M. Choices in a crisis—individual preferences among SARS-CoV-2 vaccines. New England Journal of Medicine. 2021;384(17):p. e62. doi: 10.1056/NEJMp2102146. [DOI] [PubMed] [Google Scholar]
- 210.Kreps S., Prasad S., Brownstein J. S., et al. Factors associated with US adults’ likelihood of accepting COVID-19 vaccination. JAMA Network Open. 2020;3(10):p. e2025594. doi: 10.1001/jamanetworkopen.2020.25594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211.Polack F. P., Thomas S. J., Kitchin N., et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. New England Journal of Medicine. 2020;383(27):2603–2615. doi: 10.1056/NEJMoa2034577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 212.Castells M. C., Phillips E. J. Maintaining safety with SARS-CoV-2 vaccines. New England Journal of Medicine. 2021;384(7):643–649. doi: 10.1056/NEJMra2035343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 213.Castells M. Diagnosis and management of anaphylaxis in precision medicine. Journal of Allergy and Clinical Immunology. 2017;140(2):321–333. doi: 10.1016/j.jaci.2017.06.012. [DOI] [PubMed] [Google Scholar]
- 214.Stone C. A., Jr., Rukasin C. R., Beachkofsky T. M., Phillips E. J. Immune-mediated adverse reactions to vaccines. British Journal of Clinical Pharmacology. 2019;85(12):2694–2706. doi: 10.1111/bcp.14112. [DOI] [PMC free article] [PubMed] [Google Scholar]