

Abstract
Studies of posttraumatic stress disorder (PTSD) report volume abnormalities in multiple regions of the cerebral cortex. However, findings for many regions, particularly regions outside commonly studied emotion-related prefrontal, insular, and limbic regions, are inconsistent and tentative. Also, few studies address the possibility that PTSD abnormalities may be confounded by comorbid depression. A mega-analysis investigating all cortical regions in a large sample of PTSD and control subjects can potentially provide new insight into these issues. Given this perspective, our group aggregated regional volumes data of 68 cortical regions across both hemispheres from 1379 PTSD patients to 2192 controls without PTSD after data were processed by 32 international laboratories using ENIGMA standardized procedures. We examined whether regional cortical volumes were different in PTSD vs. controls, were associated with posttraumatic stress symptom (PTSS) severity, or were affected by comorbid depression. Volumes of left and right lateral orbitofrontal gyri (LOFG), left superior temporal gyrus, and right insular, lingual and superior parietal gyri were significantly smaller, on average, in PTSD patients than controls (standardized coefficients = −0.111 to −0.068, FDR corrected P values < 0.039) and were significantly negatively correlated with PTSS severity. After adjusting for depression symptoms, the PTSD findings in left and right LOFG remained significant. These findings indicate that cortical volumes in PTSD patients are smaller in prefrontal regulatory regions, as well as in broader emotion and sensory processing cortical regions.
Introduction
Posttraumatic stress disorder (PTSD) affects millions of people globally [1]. PTSD is characterized by intrusive memories of a traumatic event, avoidance of trauma-related circumstances, hyperarousal, and negative alterations in mood and cognition. PTSD is also frequently comorbid with depression and other psychiatric disorders [2, 3]. The personal suffering associated with PTSD, coupled with residual symptoms and functional impairments that persist even after pharmacological and behavioral treatments, results in major financial and societal costs [4, 5]. A better understanding of brain abnormalities that underlie PTSD is needed to develop more effective treatments.
Behavioral and functional neuroimaging studies have linked posttraumatic stress symptom (PTSS) to abnormal fear extinction learning, exaggerated threat detection, deficient context processing, and impaired emotion regulation [6]. Several structural magnetic resonance imaging (sMRI) studies comparing PTSD patients to controls report smaller volumes of brain regions related to these emotion functions, such as the hippocampus [7], cingulate, insula, and prefrontal cortices [8–13]; however, these results are inconsistent [14–16]. In some studies, volumes of emotion-related regions were also negatively correlated with PTSS severity, suggesting that smaller volumes of emotion-related cortical regions may underlie PTSD pathophysiology [12]. Far less is known about effects of PTSD on volumes of other cortical regions. Some evidence points to reduced volumes in regions of parietal, temporal, and occipital cortices of PTSD patients [13, 17, 18]. However, these findings have not been replicated and remain tentative [19], possibly due to small sample sizes or heterogeneity of samples and analyses across studies. Identification of cortical regions with PTSD-related structural differences may be improved with analyses of large samples from multiple PTSD cohorts, which can provide greater statistical power, robust results, improved generalizability, and precise effect size estimates. Large samples also permit nuanced analyses that can uncover underlying diagnostic heterogeneity by testing interactions with clinical variables.
Existing PTSD meta-analyses, based on group descriptive statistics of volumetric data, focus only on emotion-related prefrontal, limbic, and insular cortical regions frequently reported in individual studies. These meta-analyses report, for example, smaller anterior cingulate cortex (ACC) [20, 21] and total brain volume [22, 23] in PTSD patients, but most cortical regions remain largely unstudied. This has resulted in limited understanding of regional effects of PTSD over the full extent of cortex. Meta-analyses using voxel based morphometry (VBM), from either group descriptive statistics or whole brain data, report lower gray matter density (GMD) in PTSD patients not only in ACC [24–28], superior frontal (SFG) [26–28], and insular (IG) [24, 26] gyri, but also in middle temporal (MTG) [26–28], lingual (LING) [27], fusiform [27], and parahippocampal [24] gyri. These GMD findings suggest that PTSD structural abnormalities may extend beyond emotion-related cortical regions. However, spatial normalization, smoothing, and statistical approaches used in group VBM comparisons can introduce confounds [29]. Consequently, VBM findings of structural differences provide indirect evidence that requires confirmation with more direct volumetric measurements [30].
It is also important to consider that existing meta-analyses using descriptive statistics have limited capacity to investigate confounding factors. For example, depression is frequently comorbid with PTSD and has been independently associated with reductions in cortical volume [31–33], GMD [34], and/or thickness [35] in prefrontal, cingulate, insular, and temporal lobe regions. Thus, depression-related cortical alterations may overlap with PTSD-related alterations [25] and may be a possible confound in PTSD studies. However, volumetric meta-analyses have not addressed interactions of depression with PTSD.
In an attempt to more comprehensively investigate cortical regional volume abnormalities in PTSD patients, we performed a multi-cohort analysis of volumetric data of all cortical regions in 1379 PTSD patients and 2192 controls without PTSD. In contrast to previous meta-analyses using published data that may be biased by the “file drawer problem”, i.e., contradictory and null results are less likely to be published, we harmonized participants’ whole cortical data irrespective of prior publication status to preclude inflation of effect size due to exclusion of non-significant or contradictory findings. To minimize noise from variability in neuroimaging processing methods, all laboratories implemented a standardized image processing and quality control pipeline developed by the ENIGMA Consortium which has been used in large-scale studies to successfully identify cortical structural abnormalities in many psychiatric disorders [35–37]. Furthermore, unlike previous meta-analysis approaches that tested effects across cohorts using group statistics for each cohort, we used a mega-analysis approach in which the data of individual subjects were centralized, and the effect of cohort was modeled using multiple linear regression [38]. This mega-analysis approach enhanced detection of PTSD-related volumetric differences and increased power to account for factors that may confound PTSD differences. Almost all (42 of 44) cohorts in the current study included evaluations of depression symptoms, permitting study of potential confounding effects of comorbid depression on cortical volumes of PTSD patients to test the specificity of PTSD effects. Overall, we attempted to systematically examine all cortical regions for volumetric abnormalities in PTSD patients.
Methods
Samples
Clinical and imaging data from 3571 individuals were collected from 44 cohorts assessed in 32 laboratories across seven countries. Descriptive information on the samples is summarized in Supplementary Table 1. Inclusion and exclusion criteria for each cohort are summarized in Supplementary Table 2. Depending on the cohort, current PTSD was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (DSM) IV or V criteria, using the following standard instruments: Clinician-Administered PTSD Scale-IV (CAPS-4; 24 cohorts, DSM-IV), CAPS-5 (7 cohorts, DSM-V), Structured Clinical Interview (SCID-4; 5 cohorts, DSM-IV), Mini International Neuropsychiatric Interview 6.0.0 (3 cohorts, DSM-IV), PTSD Checklist-4 (PCL-4; 3 cohorts; DSM-IV), PCL-5 (2 cohorts; DSM-V), PTSD Symptom Scale (1 cohort, DSM-IV), Schedule for Affective Disorders and Schizophrenia for School-Age Children (1 cohort, DSM-IV), Diagnostic Interview Schedule for Children (1 cohort, DSM-IV), UCLA PTSD Reaction Index (1 cohort, DSM-IV), and Anxiety Disorders Interview Schedule (1 cohort, DSM-IV). The anonymized data were aggregated at the University of Michigan with prior approval of the Institutional Review Board.
Imaging acquisition and processing
High resolution T1-weighted brain sMRI scans were acquired at contributing laboratories and processed with standardized ENIGMA Consortium protocols. In brief, sMRI images were processed using the automated FreeSurfer processing stream (version 5.3 in 36 cohorts, 6.0 in 7 cohorts, and 5.1 in 1 cohort) to create individual subject thickness maps. Each hemisphere was parcellated into 34 cortical regions of interest (ROIs) using the Desikan–Killiany atlas. FreeSurfer defines the volume of each ROI by multiplying cortical thicknesses at vertices in the region by the surface area across all vertices. ROI volumes and intracranial volume (ICV) were derived in subjects’ native space. Segmentations of gray and white matter and parcellations of ROIs were visually inspected using ENIGMA imaging quality control protocols (http://enigma.ini.usc.edu/protocols/genetics-protocols). ROIs with segmentation or parcellation errors were excluded from analysis. Five cohorts included 391 children (6–17 years, 12.6 ± 3.0 years). Previous studies of PTSD effects on cortical volumes in children have also yielded inconsistent findings [12, 18], so we studied PTSD abnormalities across all ages. Children’s data were processed and inspected in the same way as adults, based on previous validations of FreeSurfer processing for the above age range [39, 40].
Statistical analyses
First, a mixed effects model mega-analysis of individual subject data from all cohorts was used to test for cortical volume differences in each ROI between PTSD and control groups. Age, sex, and ICV were included as fixed-effect covariates. A random intercept was fitted for each cohort and scanner. Interactions of age by PTSD and sex by PTSD were added to the model to examine effects of these factors on group differences. The “lmer” function in the R package “lme4” was used.
Second, associations between ROI volumes and a dimensional PTSS severity were examined. Instruments for assessing PTSS varied by cohort. Score homogenization was accomplished by calculating the percentage of the severity score relative to the maximum score possible for each instrument (Supplementary Table 3). Most (36 of 44, Supplementary Table 2) cohorts included trauma-exposed control subjects whose PTSS severities were assessed. Consistent with distributions of PTSS of other trauma-exposed populations [41], the homogenized PTSS severity scores of 2535 subjects from both PTSD and control groups were continuously distributed and the number of subjects declined progressively with increasing scores (Supplementary Fig. 1A). The Spearman’s rank-order correlation was used in a partial correlation analysis to examine associations between cortical volume and PTSS severity, with adjustments for cohort, scanner, age, sex, ICV, and assessment instrument.
Third, the effects of comorbid depression on PTSD-related cortical volume alterations were examined. A binary index distinguishing high vs. low depression symptom severity was defined based on the questionnaire-specific severe depression cut-off scores or the depression diagnosis provided by SCID (Supplementary Table 3). Subjects with depression information were divided into high (n = 499) vs. low (n = 2713) depression symptom severity groups. Cortical volumes of PTSD vs. control subjects from these cohorts were compared using the same mixed effects model mega-analysis with and without an additional fixed factor of the depression symptom severity index to study the confounding effect of depression on PTSD group differences. Then, the interaction between PTSD and depression symptom index was further examined.
All measures are reported as mean ± standard deviation. Effect size was calculated using a standardized coefficient, which was the coefficient from the model with all continuous variables standardized [42]. A false discovery rate (FDR) was used for multiple comparisons correction across 68 cortical regions. FDR is preferred over Bonferroni correction for multiple testing correction in many fields, including imaging research [27, 28, 35–37], because Bonferroni correction is overly conservative and likely leads to false negative results [43]. An FDR corrected P value (often known as a q value) was calculated using the Benjamini–Hochberg procedure [44]. An FDR corrected P value < 0.05 was considered significant. All statistical analyses were performed using R v3.3.1.
Results
Sample characteristics
Male and female subjects between 6 and 85 years old were studied. The number of male and female subjects in PTSD and control groups did not differ significantly, but mean age was significantly higher in the PTSD group (Table 1). The PTSD group had significantly greater PTSS scores and higher comorbid depression than controls (Table 1). Homogenized PTSS scores were significantly greater in the high vs. low depression symptom group (51.5 ± 20.6 vs. 22.4 ± 22.2; T = 25.6, degree of freedom (df) = 622.2, p < 0.00001), but did not differ between males vs. females (27.0 ± 24.2 vs. 28.7 ± 25.1, T = 1.65, df = 1675.8, p = 0.099) and were not correlated with age (Pearson correlation R = −0.014, df = 2525, P = 0.49).
Table 1.
Demographics, symptoms and ICV of PTSD and control groups.
| PTSD | Control | Difference | P value | |
|---|---|---|---|---|
| N (%) | 1379 (39.5%) | 2192 (60.5%) | ||
| Female N (%) | 554 (40.4%) | 923 (42.2%) | χ2=1.02 (df = 1) | 0.31 |
| Age (years) | 36.0 ± 14.1 | 34.3 ± 15.5 | T = 3.35 (df = 3101) | P = 0.0008* |
| Age range (years) | 6‐82 | 6‐85 | ||
| PTSD severity | 49.8 ± 16.7 | 10.5 ± 12.8 | T = 64.91 (df = 2009) | <0.0001* |
| N of depression High/Low | 397/860 | 102/1852 | χ2 = 403.04 (df = 1) | <0.0001* |
| N of cohorts | 43 | 42 | ||
| N of scanners | 63 | 60 | ||
| ICV (mm3) | 1491977 ± 212659 | 1492371 ± 223097 | T = 0.05 (dfa = 2813.2) | P = 0.959 |
Data are reported as mean ± standard deviation.
df degree of freedom.
Significant at P < 0.05 level.
Welch approximation to the degrees of freedom (df) is used.
Cortical volume differences between PTSD and control groups
ROI volume means, standard deviations, effect sizes, and significance levels for differences between PTSD and control groups are reported in Table 2 and Supplementary Table 4. After adjusting for age, sex, ICV, cohort, and scanner, PTSD subjects had significantly smaller volumes bilaterally in the lateral and medial orbitofrontal gyrus (LOFG and MOFG), IG, precuneus, and superior temporal gyrus (STG). PTSD patients also had smaller volumes in left rostral middle frontal gyrus (RMFG), rostral and caudal ACC (RACC and CACC), posterior cingulate cortex (PCC), and banks of the superior temporal sulcus (STS-banks). Finally, PTSD patients had smaller volumes in right SFG, pars orbitalis of inferior frontal gyrus (IFG-PORB), MTG, superior and inferior parietal gyrus (SPG and IPG), and LING (Fig. 1). ICV did not differ between groups (Table 1). The I2 from Higgins Heterogeneity tests ranged between 0 and 48.3 across all regions, indicating low to moderate heterogeneity across cohorts (Supplementary Table 5).
Table 2.
Cortical regions with significant volume differences between PTSD and control subjects.
| Brain regionsa | PTSD | Control | PTSD vs. Control | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean (mm3) | SD (mm3) | N | Mean (mm3) | SD (mm3) | Diff. (mm3) | Effect sizeb | FDR P | |
| Frontal regions | |||||||||
| R LOFG | 1259 | 7368.940 | 1137.590 | 2079 | 7562.397 | 1234.104 | −193.456 | −0.111 | 0.000* |
| R MOFG | 1232 | 5131.391 | 819.555 | 2071 | 5222.223 | 844.395 | −90.831 | −0.067 | 0.039* |
| R IFG-PORB | 1269 | 2696.327 | 497.214 | 2092 | 2764.559 | 515.613 | −68.232 | −0.086 | 0.020* |
| R SFG | 1211 | 21834.360 | 3438.285 | 2017 | 22431.852 | 3589.712 | −597.492 | −0.082 | 0.008* |
| L LOFG | 1265 | 7565.540 | 1102.285 | 2089 | 7765.323 | 1162.551 | −199.783 | −0.107 | 0.001* |
| L MOFG | 1250 | 5160.526 | 889.396 | 2082 | 5288.258 | 907.856 | −127.733 | −0.068 | 0.038* |
| L RMFG | 1256 | 15829.645 | 2737.385 | 2081 | 16311.831 | 2959.738 | −482.186 | −0.062 | 0.039* |
| Insular regions | |||||||||
| R IG | 1118 | 6780.865 | 1006.828 | 1880 | 6847.068 | 974.675 | −66.203 | −0.073 | 0.039* |
| L IG | 1197 | 6853.961 | 1050.529 | 2014 | 6962.180 | 1112.211 | −108.219 | −0.066 | 0.036* |
| Cingulate regions | |||||||||
| L RACC | 1258 | 2684.630 | 589.660 | 2090 | 2758.639 | 596.734 | −74.009 | −0.074 | 0.047* |
| L CACC | 1266 | 1848.427 | 495.657 | 2090 | 1939.267 | 525.090 | −90.840 | −0.098 | 0.030* |
| L PCC | 1270 | 3242.812 | 590.116 | 2095 | 3341.209 | 626.234 | −98.397 | −0.078 | 0.039* |
| Temporal regions | |||||||||
| R STG | 1209 | 11434.388 | 1684.942 | 2035 | 11652.213 | 1787.315 | −217.825 | −0.081 | 0.021* |
| R MTG | 1249 | 11768.208 | 1932.620 | 2074 | 11941.835 | 2240.106 | −173.627 | −0.075 | 0.020* |
| L STG | 1207 | 12107.253 | 1911.582 | 1989 | 12438.862 | 1913.769 | −331.609 | −0.089 | 0.018* |
| L STS-banks | 1122 | 2538.936 | 513.020 | 1879 | 2631.318 | 562.580 | −92.382 | −0.084 | 0.039* |
| Parietal regions | |||||||||
| R precuneus | 1258 | 10119.110 | 1660.468 | 2091 | 10336.908 | 1758.257 | −217.798 | −0.065 | 0.038* |
| R SPG | 1153 | 13072.242 | 2171.277 | 1974 | 13293.998 | 2176.036 | −221.756 | −0.068 | 0.039* |
| R IPG | 1239 | 15102.197 | 2586.341 | 2066 | 15469.810 | 2754.932 | −367.613 | −0.065 | 0.041* |
| L precuneus | 1263 | 9713.105 | 1606.806 | 2093 | 9909.710 | 1672.397 | −196.605 | −0.061 | 0.041* |
| Occipital regions | |||||||||
| R LING | 1186 | 6786.013 | 1187.746 | 1973 | 6994.104 | 1187.540 | −208.091 | −0.110 | 0.006* |
PTSD vs. control difference significant at FDR corrected P < 0.05 level.
“L” refers to left hemisphere, and “R” means right hemisphere.
The standardized coefficients of linear mixed model were reported for effect sizes.
Fig. 1. Cortical volume differences between PTSD and control subjects.
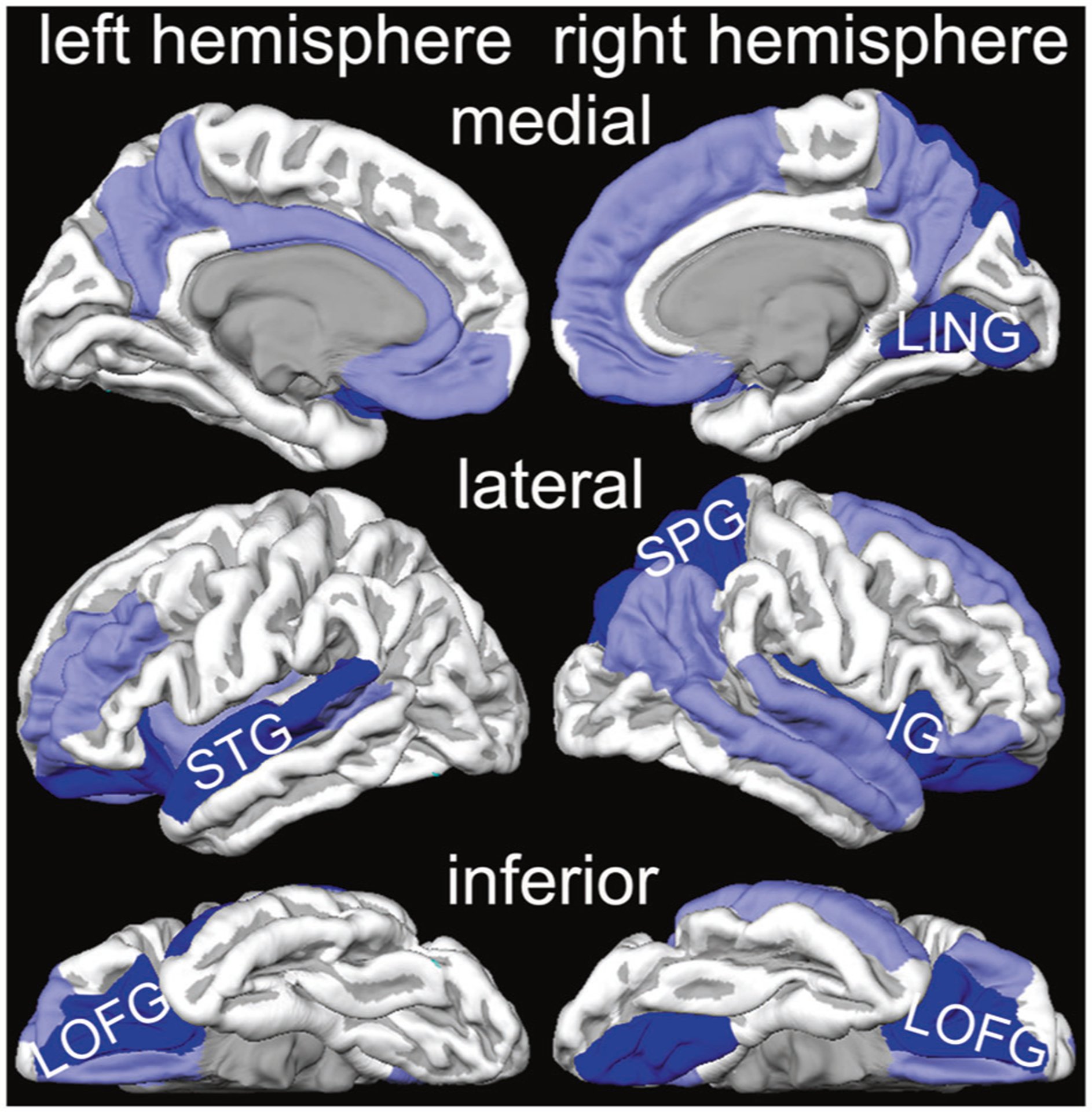
Light blue indicates regions with smaller volume in PTSD group. Dark blue indicates regions which are smaller in PTSD group, and their volumes are negatively associated with harmonized PTSS severity scores.
Sex and age interactions with PTSD
Main effects of age and sex were significant in almost all regions (Supplementary Table 5). Interactions between sex and PTSD were not significant in any region; however, interactions between age and PTSD were significant bilaterally in MTG, left inferior temporal gyrus (ITG), and right fusiform and parahippocampal gyri (Table 3). To eliminate the effect of age difference between groups, the analysis was repeated in an age-matched subsample (35.2 ± 11.1 years in PTSD vs. 34.4 ± 12.1 years in control, T = 1.80, df = 2776.3, p = 0.07) obtained by excluding the two youngest cohorts and the one eldest cohort. PTSD by age interactions were no longer significant in any region, but volumes of bilateral LOFG and STG, left PCC, and right SFG, IFG-PORB, LING, and MTG remained significantly smaller in the PTSD patients vs. age-matched controls across ages (Table 3).
Table 3.
Significant interaction of age and PTSD diagnosis in cortical volumes.
| All subjects | Age-matched subsamplea | |||||||
|---|---|---|---|---|---|---|---|---|
| Age effect | Age effect | PTSD vs. control | ||||||
| Brain regions | Effect sizeb | FDR P | Interaction FDR P | Effect sizeb | FDR P | Interaction FDR P | Effect sizeb | FDR P |
| Frontal regions | ||||||||
| R LOFG | −0.371 | 3.0 × 10−95* | 0.070 | −0.302 | 5.4 × 10−99* | 0.918 | −0.093 | 0.012† |
| R IFG-PORB | −0.388 | 1.3 × 10−82* | 0.096 | −0.314 | 1.8 × 10−80* | 0.876 | −0.083 | 0.046† |
| R SFG | −0.436 | 1.4 × 10−137* | 0.959 | −0.350 | 9.1 × 10−130* | 0.930 | −0.090 | 0.012† |
| L LOFG | −0.413 | 9.8 × 10−111* | 0.121 | −0.329 | l.O× 10−111* | 0.918 | −0.085 | 0.023† |
| Cingulate regions | ||||||||
| L PCC | −0.353 | 6.1 × 10−62* | 0.504 | −0.277 | 2.9 × 10−58* | 0.821 | −0.088 | 0.046† |
| Temporal regions | ||||||||
| R STG | −0.342 | 1.1 × 10−67* | 0.305 | −0.273 | 7.2 × 10−68* | 0.975 | −0.080 | 0.046† |
| R MTG | −0.358 | 1.6 × 10−89* | 0.041# | −0.282 | 2.2 × 10−87* | 0.803 | −0.080 | 0.029† |
| R fusiform | −0.273 | 2.6 × 10−42* | 0.040# | −0.206 | 1.4 × 10−38* | 0.876 | −0.064 | 0.111 |
| R parahippocampal | −0.126 | 7.1 × 10−15* | 0.040# | −0.091 | 4.3 × 10−13* | 0.821 | −0.010 | 0.702 |
| L STG | −0.360 | 2.8 × l0−71* | 0.437 | −0.285 | 7.0 × 10−69* | 0.930 | −0.084 | 0.046† |
| L MTG | −0.355 | 2.2 × l0−73* | 0.040# | −0.281 | 7.5 × 10−72* | 0.821 | −0.050 | 0.179 |
| L ITG | −0.301 | 4.5 × 10−52* | 0.040# | −0.237 | 1.5 × 10−49* | 0.599 | −0.059 | 0.127 |
| Occipital regions | ||||||||
| R LING | −0.286 | 1.0 × 10−39* | 0.119 | −0.217 | 1.0 × 10−35* | 0.881 | −0.118 | 0.012† |
Significant age main effects at FDR corrected p < 0.05 level.
Significant interaction of age and PTSD diagnosis at FDR corrected P < 0.05 level.
Significant PTSD main effect at FDR corrected P < 0.05 level in age-matched subsamples.
Analysis after matching mean ages of PTSD and control groups by excluding the single cohort on older adults, ADNIDOD, and two youngest cohorts, NIRL and FEAR.
The standardized coefficients of linear mixed model were reported for effect sizes.
Correlations between PTSS severity and cortical volumes
Cortical volumes of bilateral LOFG, left STG, and right SPG, IG and LING were significantly negatively correlated with PTSS severity scores from the pooled PTSD and control subjects (Table 4, Supplementary Table 6, Supplementary Fig. 2). The correlations for bilateral LOFG, left STG, and right SPG were consistent with significant negative associations of cortical ROI volume and PTSS severity in the same linear mixed effects model analyses used for group comparisons (Supplementary Table 6, Supplementary Fig. 1B–F). When further examining the same correlation in the PTSD group alone, the above ROI volumes remained negatively correlated with PTSS severity, but no correlations were significant after FDR correction (Supplementary Table 6). This might be attributed to the reduced number of subjects and range of symptom severity.
Table 4.
Cortical regions with significant correlations of PTSS severity and regional volumes.
| Brain regions | N | R a | FDR P |
|---|---|---|---|
| Frontal regions | |||
| R LOFG | 2475 | −0.060 | 0.039* |
| L LOFG | 2479 | −0.066 | 0.038* |
| Insular regions | |||
| R IG | 2210 | −0.065 | 0.038* |
| Temporal regions | |||
| L STG | 2362 | −0.066 | 0.038* |
| Parietal regions | |||
| R SPG | 2295 | −0.059 | 0.050* |
| Occipital regions | |||
| R LING | 2319 | −0.065 | 0.038* |
Significant at FDR corrected P < 0.05 level.
Spearman correlation coefficients of cortical volume and homogenized PTSS severity scores in partial correlation analyses adjusting for cohort, scanner, age, sex, ICV, and the assessment instrument that was used.
Effect of depression on PTSD-related differences in cortical volumes
When the binary index of depression symptom severity was added to the analytical model, PTSD effects remained significant bilaterally in the LOFG, whereas differences in right SFG and LING, and left CACC became non-significant (Table 5, Supplementary Table 7). Depression symptom severity and ROI volumes were significantly inversely related in left pars opercularis of IFG (IFG-POPE) and STG, and right IG and SPG. Negative effect sizes in the above regions for both PTSD and depression suggested greater symptom severity was associated with smaller volumes for both conditions. Interaction of PTSD and depression on cortical volume was not significant in any region. Finally, for subjects with low depression symptoms, the PTSD-associated difference remained significant in left LOFG (Supplementary Table 7).
Table 5.
Cortical regions with significant main effects of PTSD or depression in the analysis including both PTSD diagnosis and depression symptom severity classifications.
| PTSD | Depression | |||
|---|---|---|---|---|
| Brain regions | Effect sizea | FDR P | Effect sizea | FDR P |
| Frontal regions | ||||
| R LOFG | −0.093 | 0.020* | −0.057 | 0.322 |
| R SFG | −0.066 | 0.143† | −0.088 | 0.107 |
| L LOFG | −0.094 | 0.020* | −0.065 | 0.300 |
| L IFG-POPE | 0.024 | 0.718 | −0.143 | 0.032# |
| Insular regions | ||||
| R IG | −0.025 | 0.699 | −0.128 | 0.032# |
| Cingulate regions | ||||
| L CACC | −0.106 | 0.114† | 0.005 | 0.971 |
| Temporal regions | ||||
| L STG | −0.049 | 0.319 | −0.128 | 0.032# |
| Parietal regions | ||||
| R SPG | −0.022 | 0.718 | −0.129 | 0.032# |
| Occipital regions | ||||
| R LING | −0.076 | 0.232† | −0.070 | 0.322 |
PTSD effects were significant at FDR corrected P < 0.05 level in analyses with and without the depression variable.
PTSD effects were significant at FDR corrected P < 0.05 level in analyses without the depression variable, but were insignificant in analyses with the depression variable.
Depression effects were significant at FDR corrected P < 0.05 level.
The standardized coefficients of linear mixed model were reported for effect sizes.
Discussion
This study is the first mega-analysis of PTSD effects on volumes of regions that span the entire cortex. PTSD was associated with smaller volumes in emotion-related prefrontal, limbic, and insular regions, but also in temporal, parietal, and occipital regions. Bilateral LOFG, left STG, and right IG, SPG and LING volumes were smaller in the PTSD group using a categorical diagnostic classification, and were negatively associated with PTSS severity, a dimensional variable. The corroborating categorical and dimensional results for these regions strengthen confidence in the findings [45, 46]. In addition, the categorical PTSD classification was associated with smaller volume in MOFG and precuneus bilaterally, SFG, IFG-PORB, STG, MTG, and IPG in the right hemisphere, and RMFG, RACC, CACC, PCC, IG, and STS-banks in the left hemisphere. However, volumes of these regions were not significantly correlated with PTSS severity.
Of the above six regions that had significant associations between cortical volumes and both categorical PTSD diagnosis and dimensional PTSS severities, bilateral LOFG volumes remained significantly negatively associated with PTSD after accounting for depression symptom severity. Left LOFG volume was smaller in PTSD subjects with low depression symptoms. By contrast, right LING volumes were no longer significantly associated with PTSD after accounting for depression. Interestingly, volumes of left STG, right IG and right SPG were significantly smaller in the group with high depression symptoms, suggesting that some variance in the model was attributed to comorbid depression rather than PTSD in these regions. Finally, further comparisons from subgroups of age-matched PTSD and control subjects suggest that smaller PTSD-related volumes of bilateral LOFG, left STG, and right LING were not influenced by between-group differences in age. Smaller LOFG volumes in PTSD patients across all ages are consistent with previous findings in both adults [13, 17] and children [12]. However, the significant interaction of age with PTSD in temporal regions might be attributed to between-group differences in age.
Depression effects on PTSD-related smaller cortical volumes
Studies have reported that PTSD and depression are both associated with smaller LOFG volume [13, 17, 31–33]. We found smaller bilateral LOFG volume was linked to PTSD pathophysiology independently of comorbid depression. Consistent with this possibility, prior studies report that lower GMD in LOFG is negatively associated with cumulative trauma exposure [13], and post-to-pre trauma reduction of GMD in LOFG negatively correlates with PTSS severity [47]. Adding to previously reported volume reduction of STG [17] and IG [8], we found smaller volumes of right SPG and LING in PTSD patients, which are consistent with GMD differences in SPG [48] and LING [27, 48]. When adjusting for depression symptoms, LING volumes were no longer significantly associated with PTSD; moreover, smaller SPG, IG, and STG volumes were significantly related to comorbid depression. These results have different potential interpretations. First, we found greater depression symptom severity in PTSD patients and higher PTSS in depressed subjects, suggesting a positive association between PTSD and depression symptoms. This raises a possibility that shared variance of the two variables lowered the statistical power to true PTSD effects [49]. Second, it is possible that depression symptom and PTSS scales measure symptoms common to both disorders including negative emotions, avoidance symptoms, or other latent construct(s). Third, it is possible that depression symptoms and PTSS are mediated, in part, by shared brain abnormalities. If any or all of these explanations are valid, our findings would suggest that smaller IG, STG, SPG and LING could be associated with PTSD pathophysiology. Alternatively, the current results cannot rule out the possibility that diminished volumes of these regions may be associated with depression, but not PTSD.
Implications for PTSD neurocircuits
Prior evidence supports associations between cortical structural alterations and PTSS [19], and potential links between altered cortical structure and brain function in PTSD patients [50, 51]. Deficits in emotion processing circuits and top-down prefrontal dysregulation of these circuits are linked to PTSD [6]. In this context, LOFG plays an important role in integrating sensory and limbic inputs and in top-down prefrontal inhibitory regulation of emotion and sensory regions [52, 53]. Patients with OFG lesions demonstrate attention deficits and impaired response inhibition to emotional stimuli [54]. Thus, low LOFG volume may impair inhibitory top-down regulation of emotion and sensory attention. If the current findings of smaller IG, STG, SPG, and LING volumes also contribute to PTSD pathophysiology, and if IG, STG, and SPG volumes are not solely related to depression, volume alterations in these regions may also contribute to emotion and/or sensory memory dysfunctions in PTSD. Reduced GMD in anterior IG has been linked to greater PTSS including intrusive memories [55, 56], which may explain anterior IG over-responsiveness to negative emotions in PTSD patients [57]. The present findings of smaller SPG, STG, and LING volumes implicate sensory information processing systems in PTSD. SPG contributes to a dorsal visual processing stream for spatial and movement information [58, 59]. STG is a multimodal region linked to audiovisual integration of emotions and is functionally connected to the amygdala—a subcortical emotion processing region that is fundamental to PTSD pathophysiology [60, 61]. LING is involved in visual memory and processing facial and spatial information. Reduced GMD and functional connectivity with other visual areas co-exist in the LING of sexual assault PTSD patients and are associated with re-experiencing symptoms and self-blame [62]. Lower volumes in SPG, STG, and LING may contribute to PTSD symptoms that involve integration of auditory, visual, and emotional processing. These regions may provide sensory substrates for intrusive memories in PTSD and other psychiatric disorders including depression [63]. Consistent with this hypothesis, lower GMD in temporal, parietal and occipital regions negatively correlates with the severity of intrusive memories [64]. This perspective suggests that cortical contributions to PTSD involves sensory and memory processing regions that have been largely overlooked in PTSD studies.
Limitations
The present study has limitations that are pertinent for the generalization and specificity of findings. Data were derived from cohorts that varied in image acquisition, processing, and clinical assessment instruments. We adjusted for data source statistically and had acceptable heterogeneities of cortical regional volumes across cohorts. Additional factors could affect cortical volume, e.g., cohort stratification, medications, duration of illness, trauma type, age at trauma exposure, trauma exposure of control subjects, and other comorbidities including anxiety disorders and substance abuse, which were not available for many cohorts and not analyzed. The cross-sectional data cannot distinguish the volume differences that occurred before vs. after trauma exposure. Further studies are needed to examine confounding effects of comorbid disorders, and to identify agespecific PTSD abnormalities.
Conclusion
This is the largest mega-analysis of cortical volumes in PTSD patients to date. We report smaller LOFG volumes in PTSD patients across all ages that are independent of depression. We found that reduced volumes of SPG and LING, in addition to previously reported IG and STG, may be linked to posttraumatic stress and/or comorbid depressive symptomatology. Collectively, these regions contribute to emotion, memory, and sensory processing circuits, and to top-down regulation of these circuits. Our findings support current thinking on deficits in emotion neurocircuits in PTSD and shed new light on the involvement of sensory processing brain circuits in the pathophysiology of PTSD.
Supplementary Material
Acknowledgements
The individual cohorts were supported by following grants: 1R21MH102634, 5U01AA021681-08, Academic Medical Center Research Council (110614), Anonymous Women’s Health Fund, Barlow Family Fund, BOF 01J05415, CDMRP W81XWH-08-2-0038, Center for Brain and Behavior Research Pilot Grant, CX001600 VA CDA, Dana Foundation, DoD W81XWH08-2-0159, DoD W81XWH-10-1-0925, DoD W81XWH-12-2-0012, F32MH109274, German Research Foundation (DA 1222/4-1 and WA 1539/8-2), German Research Society (Deutsche Forschungsgemeinschaft, DFG; SFB/TRR 58: C06, C07), HD071982, HD085850, K01MH118428, K23MH090366-01, K24DA028773, K24MH71434, K99NS096116, Kasparian Fund, L30MH114379, M01RR00039, MH071537, MH098212, MH101380, MJFF 14848, NARSAD- Young Investigator Grant, National Institute of Child Health and Human Development (P30-HD003352), NCATS (CTSA)-Yale Center for Clinical Investigation, The Netherlands Organization for Health Research and Development (40-00812-98-10041), NHMRC Program Grant (1073041), NIAAA (P50)- Center for the Translational Neuroscience in Alcohol, P30HD003352, P41EB015922, R01AA12479, R01AG059874, R01MH043454, R01MH096987, R01MH103291, R01MH105355, R01MH105535, R01MH110483, R01MH111671, R01MH116147, R01MH117601, R01MH61744, R01MH63407, R21MH097196, R21MH098198, R21MH112956, R56AG058854, South African Medical Research Council, South Dakota Governor’s Research Center Grant, T32MH018931, Trauma Scholars Fund, U54EB020403, UCI-LBVA Biumvirate Grant, UL1TR000153, UL1TR000454, The University of Wisconsin Institute for Clinical and Translational Research, VA CSR&D 1IK2CX001680, VA Merit Review Program, VA National Center for PTSD, VA RR&D1IK2RX000709, VA RR&D1K1RX002325, VA RR&D1K2RX002922, VA RR&DI01RX000622, VISN6 MIRECC.
Footnotes
Supplementary information The online version of this article (https://doi.org/10.1038/s41380-020-00967-1) contains supplementary material, which is available to authorized users.
Conflict of interest Dr CGA has served as a consultant, speaker and/or on advisory boards for FSV7, Lundbeck, Psilocybin Labs, Genentech and Janssen, and editor of Chronic Stress for Sage Publications, Inc.; he has filed a patent for using mTOR inhibitors to augment the effects of antidepressants (filed on August 20, 2018). Dr RJD is the founder and president of, and serves on the board of directors for, the non-profit organization Healthy Minds Innovations, Inc. Dr NJ received partial research support from Biogen, Inc. (Boston, USA) for research unrelated to the content of this paper. Dr JHK is a consultant for AbbVie, Inc., Amgen, Astellas Pharma Global Development, Inc., AstraZeneca Pharmaceuticals, Biomedisyn Corporation, Bristol-Myers Squibb, Eli Lilly and Company, Euthymics Bioscience, Inc., Neurovance, Inc., FORUM Pharmaceuticals, Janssen Research & Development, Lundbeck Research USA, Novartis Pharma AG, Otsuka America Pharmaceutical, Inc., Sage Therapeutics, Inc., Sunovion Pharmaceuticals, Inc., and Takeda Industries; is on the Scientific Advisory Board for Lohocla Research Corporation, Mnemosyne Pharmaceuticals, Inc., Naurex, Inc., and Pfizer; is a stockholder in Biohaven Pharmaceuticals; holds stock options in Mnemosyne Pharmaceuticals, Inc.; holds patents for Dopamine and Noradrenergic Reuptake Inhibitors in Treatment of Schizophrenia, US Patent No. 5,447,948 (issued September 5, 1995), and Glutamate Modulating Agents in the Treatment of Mental Disorders, U.S. Patent No. 8,778,979 (issued July 15, 2014); filed a patent for Intranasal Administration of Ketamine to Treat Depression. U.S. Application No. 14/197,767 (filed on March 5, 2014); filed US application or Patent Cooperation Treaty international application No. 14/306,382 (filed on June 17, 2014); and filed a patent for using mTOR inhibitors to augment the effects of antidepressants (filed on August 20, 2018). Dr PMT received partial research support from Biogen, Inc. (Boston, USA) for research unrelated to the topic of this paper. No other authors reported conflicts of interest.
References
- 1.Kessler RC, Aguilar-Gaxiola S, Alonso J, Benjet C, Bromet EJ, Cardoso G, et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur J Psychotraumatol. 2017;8(sup5):1353383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rytwinski NK, Scur MD, Feeny NC, Youngstrom EA. The cooccurrence of major depressive disorder among individuals with posttraumatic stress disorder: a meta-analysis. J Trauma Stress. 2013;26:299–309. [DOI] [PubMed] [Google Scholar]
- 3.Spinhoven P, Penninx BW, van Hemert AM, de Rooij M, Elzinga BM. Comorbidity of PTSD in anxiety and depressive disorders: prevalence and shared risk factors. Child Abus Negl. 2014;38:1320–30. [DOI] [PubMed] [Google Scholar]
- 4.Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61(Suppl 5): 4–12. [PubMed] [Google Scholar]
- 5.Andrews G, Issakidis C, Sanderson K, Corry J, Lapsley H. Utilising survey data to inform public policy: comparison of the cost-effectiveness of treatment of ten mental disorders. Br J Psychiatry. 2004;184:526–33. [DOI] [PubMed] [Google Scholar]
- 6.Liberzon I, Abelson JL. Context Processing and the Neurobiology of Post-Traumatic Stress Disorder. Neuron. 2016;92:14–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Logue MW, van Rooij SJH, Dennis EL, Davis SL, Hayes JP, Stevens JS, et al. Smaller Hippocampal Volume in Posttraumatic Stress Disorder: a Multisite ENIGMA-PGC Study: Subcortical Volumetry Results From Posttraumatic Stress Disorder Consortia. Biol Psychiatry. 2018;83:244–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chao L, Weiner M, Neylan T. Regional cerebral volumes in veterans with current versus remitted posttraumatic stress disorder. Psychiatry Res. 2013;213:193–201. [DOI] [PubMed] [Google Scholar]
- 9.Rauch SL, Shin LM, Segal E, Pitman RK, Carson MA, McMullin K, et al. Selectively reduced regional cortical volumes in post-traumatic stress disorder. Neuroreport. 2003;14:913–6. [DOI] [PubMed] [Google Scholar]
- 10.Kitayama N, Quinn S, Bremner JD. Smaller volume of anterior cingulate cortex in abuse-elated posttraumatic stress disorder. J Affect Disord. 2006;90:171–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Levy-Gigi E, Szabo C, Kelemen O, Keri S. Association among clinical response, hippocampal volume, and FKBP5 gene expression in individuals with posttraumatic stress disorder receiving cognitive behavioral therapy. Biol Psychiatry. 2013;74: 793–800. [DOI] [PubMed] [Google Scholar]
- 12.Morey RA, Haswell CC, Hooper SR, De Bellis MD. Amygdala, Hippocampus, and Ventral Medial Prefrontal Cortex Volumes Differ in Maltreated Youth with and without Chronic Posttraumatic Stress Disorder. Neuropsychopharmacology. 2016;41:791–801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Eckart C, Stoppel C, Kaufmann J, Tempelmann C, Hinrichs H, Elbert T, et al. Structural alterations in lateral prefrontal, parietal and posterior midline regions of men with chronic posttraumatic stress disorder. J Psychiatry Neurosci. 2011;36:176–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Richert KA, Carrion VG, Karchemskiy A, Reiss AL. Regional differences of the prefrontal cortex in pediatric PTSD: an MRI study. Depress Anxiety. 2006;23:17–25. [DOI] [PubMed] [Google Scholar]
- 15.Starcevic A, Postic S, Radojicic Z, Starcevic B, Milovanovic S, Ilankovic A et al. Volumetric Analysis of Amygdala, Hippocampus, and Prefrontal Cortex in Therapy-Naive PTSD Participants. Biomed Res Int. 2014;2014: 10.1155/2014/968495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lindauer RJ, Vlieger EJ, Jalink M, Olff M, Carlier IV, Majoie CB, et al. Effects of psychotherapy on hippocampal volume in out-patients with post-traumatic stress disorder: a MRI investigation. Psychol Med. 2005;35:1421–31. [DOI] [PubMed] [Google Scholar]
- 17.Woodward SH, Schaer M, Kaloupek DG, Cediel L, Eliez S. Smaller Global and Regional Cortical Volume in Combat-Related Posttraumatic Stress Disorder. Arch Gen Psychiatry. 2009;66:1373–82. [DOI] [PubMed] [Google Scholar]
- 18.De Bellis MD, Keshavan MS, Frustaci K, Shifflett H, Iyengar S, Beers SR, et al. Superior temporal gyrus volumes in maltreated children and adolescents with PTSD. Biol Psychiatry. 2002;51:544–52. [DOI] [PubMed] [Google Scholar]
- 19.Liberzon I, Wang X, Xie H. Brain structural abnormalities in posttraumatic stress disorder and relations with sleeping problems. In: Vermetten E, Germain A, Neylan TC, editors. Sleep and combat-related post traumatic stress disorder. New York, NY, USA: Springer-Verlag New York; 2018. p. 145–68. [Google Scholar]
- 20.O’Doherty DCM, Chitty KM, Saddiqui S, Bennett MR, Lagopoulos J. A systematic review and meta-analysis of magnetic resonance imaging measurement of structural volumes in posttraumatic stress disorder. Psychiatry Res Neuroimaging. 2015;232:1–33. [DOI] [PubMed] [Google Scholar]
- 21.Karl A, Schaefer M, Malta LS, Dörfel D, Rohleder N, Werner A. A meta-analysis of structural brain abnormalities in PTSD. Neurosci Biobehav Rev. 2006;30:1004–31. [DOI] [PubMed] [Google Scholar]
- 22.Hedges DW, Woon FL. Premorbid brain volume estimates and reduced total brain volume in adults exposed to trauma with or without posttraumatic stress disorder: a meta-analysis. Cogn Behav Neurol. 2010;23:124–9. [DOI] [PubMed] [Google Scholar]
- 23.Milani AC, Hoffmann EV, Fossaluza V, Jackowski AP, Mello MF. Does pediatric post-traumatic stress disorder alter the brain? Systematic review and meta-analysis of structural and functional magnetic resonance imaging studies. Psychiatry Clin Neurosci. 2017;71:154–69. [DOI] [PubMed] [Google Scholar]
- 24.Meng Y, Qiu C, Zhu H, Lama S, Lui S, Gong Q, et al. Anatomical deficits in adult posttraumatic stress disorder: a meta-analysis of voxel-based morphometry studies. Behav Brain Res. 2014; 270:307–15. [DOI] [PubMed] [Google Scholar]
- 25.Bromis K, Calem M, Reinders A, Williams SCR, Kempton MJ. Meta-analysis of 89 structural mri studies in posttraumatic stress disorder and comparison with major depressive disorder. Am J Psychiatry. 2018;175:989–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Meng L, Jiang J, Jin C, Liu J, Zhao Y, Wang W et al. Trauma-specific Grey Matter Alterations in PTSD. Sci Rep. 2016;6: 10.1038/srep33748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Li L, Wu M, Liao Y, Ouyang L, Du M, Lei D, et al. Grey matter reduction associated with posttraumatic stress disorder and traumatic stress. Neurosci Biobehav Rev. 2014;43:163–72. [DOI] [PubMed] [Google Scholar]
- 28.Kuhn S, Gallinat J. Gray matter correlates of posttraumatic stress disorder: a quantitative meta-analysis. Biol Psychiatry. 2013;73:70–4. [DOI] [PubMed] [Google Scholar]
- 29.Salmond CH, Ashburner J, Vargha-Khadem F, Connelly A, Gadian DG, Friston KJ. Distributional Assumptions in Voxel-Based Morphometry. Neuroimage. 2002;17:1027–30. [PubMed] [Google Scholar]
- 30.Mechelli A, Price CJ, Friston KJ, Ashburner J. Voxel-based morphometry of the human brain: methods and applications. Curr Med Imaging Rev. 2005;1:1–9. [Google Scholar]
- 31.Arnone D, McIntosh AM, Ebmeier KP, Munafo MR, Anderson IM. Magnetic resonance imaging studies in unipolar depression: systematic review and meta-regression analyses. Eur Neuropsychopharmacol. 2012;22:1–16. [DOI] [PubMed] [Google Scholar]
- 32.Sexton CE, Mackay CE, Ebmeier KP. A Systematic Review and Meta-Analysis of Magnetic Resonance Imaging Studies in Late-Life Depression. Am J Geriatr Psychiatry. 2013;21:184–95. [DOI] [PubMed] [Google Scholar]
- 33.Kempton MJ, Salvador Z, Munafo MR, Geddes JR, Simmons A, Frangou S, et al. Structural neuroimaging studies in major depressive disorder. Meta-analysis and comparison with bipolar disorder. Arch Gen Psychiatry. 2011;68:675–90. [DOI] [PubMed] [Google Scholar]
- 34.Du MY, Wu QZ, Yue Q, Li J, Liao Y, Kuang WH, et al. Voxelwise meta-analysis of gray matter reduction in major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2012; 36:11–6. [DOI] [PubMed] [Google Scholar]
- 35.Schmaal L, Hibar DP, Samann PG, Hall GB, Baune BT, Jahanshad N, et al. Cortical abnormalities in adults and adolescents with major depression based on brain scans from 20 cohorts worldwide in the ENIGMA Major Depressive Disorder Working Group. Mol Psychiatry. 2017;22:900–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.van Erp TGM, Walton E, Hibar DP, Schmaal L, Jiang W, Glahn DC, et al. Cortical Brain Abnormalities in 4474 Individuals With Schizophrenia and 5098 Control Subjects via the Enhancing Neuro Imaging Genetics Through Meta Analysis (ENIGMA) Consortium. Biol Psychiatry. 2018;84:644–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hibar DP, Westlye LT, Doan NT, Jahanshad N, Cheung JW, Ching CRK, et al. Cortical abnormalities in bipolar disorder: an MRI analysis of 6503 individuals from the ENIGMA Bipolar Disorder Working Group. Mol Psychiatry. 2018;23:932–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Thompson PM, Stein JL, Medland SE, Hibar DP, Vasquez AA, Renteria ME, et al. The ENIGMA Consortium: large-scale collaborative analyses of neuroimaging and genetic data. Brain Imaging Behav. 2014;8:153–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Beelen C, Phan TV, Wouters J, Ghesquiere P, Vandermosten M. Investigating the Added Value of FreeSurfer’s Manual Editing Procedure for the Study of the Reading Network in a Pediatric Population. Front Hum Neurosci. 2020;14:143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ghosh SS, Kakunoori S, Augustinack J, Nieto-Castanon A, Kovelman I, Gaab N, et al. Evaluating the validity of volume-based and surface-based brain image registration for developmental cognitive neuroscience studies in children 4 to 11 years of age. Neuroimage. 2010;53:85–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Shalev AY, Gevonden M, Ratanatharathorn A, Laska E, van der Mei WF, Qi W, et al. Estimating the risk of PTSD in recent trauma survivors: results of the International Consortium to Predict PTSD (ICPP). World Psychiatry. 2019;18:77–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lorah J Effect size measures for multilevel models: definition, interpretation, and TIMSS example. Large-scale Assess Educ. 2018;6:8. [Google Scholar]
- 43.Narum SR. Beyond Bonferroni: less conservative analyses for conservation genetics. Conserv Genet. 2006;7:783–7. [Google Scholar]
- 44.Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: a Practical and Powerful Approach to Multiple Testing. J R Stat Soc: Ser B (Methodol). 1995;57:289–300. [Google Scholar]
- 45.Hengartner MP, Lehmann SN. Why Psychiatric Research Must Abandon Traditional Diagnostic Classification and Adopt a Fully Dimensional Scope: Two Solutions to a Persistent Problem. Front Psychiatry. 2017;8:101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kotov R, Krueger RF, Watson D, Achenbach TM, Althoff RR, Bagby RM, et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. J Abnorm Psychol. 2017;126:454–77. [DOI] [PubMed] [Google Scholar]
- 47.Sekiguchi A, Sugiura M, Taki Y, Kotozaki Y, Nouchi R, Takeuchi H, et al. Brain structural changes as vulnerability factors and acquired signs of post-earthquake stress. Mol Psychiatry. 2012;18:618–23. [DOI] [PubMed] [Google Scholar]
- 48.Tan L, Zhang L, Qi R, Lu G, Li L, Liu J, et al. Brain structure in post-traumatic stress disorder: a voxel-based morphometry analysis. Neural Regen Res. 2013;8:2405–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Miller GA, Chapman JP. Misunderstanding analysis of covariance. J Abnorm Psychol. 2001;110:40–8. [DOI] [PubMed] [Google Scholar]
- 50.Fonzo GA, Flagan TM, Sullivan S, Allard CB, Grimes EM, Simmons AN, et al. Neural functional and structural correlates of childhood maltreatment in women with intimate-partner violence-related posttraumatic stress disorder. Psychiatry Res. 2013;211:93–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bremner JD, Vythilingam M, Vermetten E, Southwick SM, McGlashan T, Nazeer A, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry. 2003;160:924–32. [DOI] [PubMed] [Google Scholar]
- 52.Hooker CI, Knight RT. The role of lateral orbitofrontal cortex in the inhibitory control of emotion. In: Zald D, Rauch S, editors. The orbitofrontal cortex. New York: Oxford University Press, New York; 2006. p. 307–24. [Google Scholar]
- 53.Aupperle RL, Allard CB, Grimes EM, Simmons AN, Flagan T, Behrooznia M, et al. Dorsolateral Prefrontal Cortex Activation During Emotional Anticipation and Neuropsychological Performance in Posttraumatic Stress Disorder Dorsolateral Prefrontal Cortex Activation in PTSD. JAMA Psychiatry. 2012;69:360–71. [DOI] [PubMed] [Google Scholar]
- 54.Rule RR, Shimamura AP, Knight RT. Orbitofrontal cortex and dynamic filtering of emotional stimuli. Cogn Affect Behav Neurosci. 2002;2:264–70. [DOI] [PubMed] [Google Scholar]
- 55.Kasai K, Yamasue H, Gilbertson MW, Shenton ME, Rauch SL, Pitman RK. Evidence for Acquired Pregenual Anterior Cingulate Gray Matter Loss from a Twin Study of Combat-Related Post-traumatic Stress Disorder. Biol Psychiatry. 2008;63:550–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Herringa R, Phillips M, Almeida J, Insana S, Germain A. Post-traumatic stress symptoms correlate with smaller subgenual cingulate, caudate, and insula volumes in unmedicated combat veterans. Psychiatry Res. 2012;203:139–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Pitman RK, Rasmusson AM, Koenen KC, Shin LM, Orr SP, Gilbertson MW, et al. Biological studies of post-traumatic stress disorder. Nat Rev Neurosci. 2012;13:769–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Goodale MA, Milner AD. Separate visual pathways for perception and action. Trends Neurosci. 1992;15:20–5. [DOI] [PubMed] [Google Scholar]
- 59.Kravitz DJ, Saleem KS, Baker CI, Mishkin M. A new neural framework for visuospatial processing. Nat Rev Neurosci. 2011;12:217–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Gao C, Weber CE, Shinkareva SV. The brain basis of audiovisual affective processing: Evidence from a coordinate-based activation likelihood estimation meta-analysis. Cortex. 2019;120:66–77. [DOI] [PubMed] [Google Scholar]
- 61.Deen B, Koldewyn K, Kanwisher N, Saxe R. Functional Organization of Social Perception and Cognition in the Superior Temporal Sulcus. Cereb Cortex. 2015;25:4596–609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Berman Z, Assaf Y, Tarrasch R, Joel D. Assault-related self-blame and its association with PTSD in sexually assaulted women: an MRI inquiry. Soc Cogn Affect Neurosci. 2018;13:775–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Brewin CR, Gregory JD, Lipton M, Burgess N. Intrusive images in psychological disorders: characteristics, neural mechanisms, and treatment implications. Psychol Rev. 2010;117:210–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Kroes MC, Whalley MG, Rugg MD, Brewin CR. Association between flashbacks and structural brain abnormalities in post-traumatic stress disorder. Eur Psychiatry. 2011;26:525–31. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.