

Supplemental Digital Content is available in the text.
Keywords: blood pressure, hyperkalemia, kidney, hypertension, mineralocorticoid receptor antagonist
Abstract
In patients with resistant or poorly controlled hypertension and advanced chronic kidney disease, mineralocorticoid receptor antagonists are recommended; however, hyperkalemia limits their use. BLOCK-CKD was a phase 2b, multicenter, randomized, double-blind, placebo-controlled, parallel-group study that evaluated the safety, efficacy, and pharmacokinetics of KBP-5074, a nonsteroidal mineralocorticoid receptor antagonist, for uncontrolled hypertension in patients with stage 3b/4 chronic kidney disease. The study tested the hypothesis that addition of KBP-5074 to standard treatment lowers blood pressure without increased risk of hyperkalemia. Patients (N=162) were randomly assigned 1:1:1 to once-daily oral treatment with placebo, KBP-5074 0.25 mg, or KBP-5074 0.5 mg. The primary end point was systolic blood pressure change from baseline at day 84. Baseline mean (SD) systolic blood pressure was 155.3 (13.55) mm Hg. After 84 days, the placebo-subtracted treatment mean difference (SE) was −7.0 (3.37) mm Hg with KBP-5074 0.25 mg (P=0.0399) and −10.2 (3.32) mm Hg with KBP-5074 0.5 mg (P=0.0026). Hyperkalemia incidence, ≥5.6 <6 mmol/L, were similar among groups 5 (8.8%) placebo, 6 (11.8%) 0.25 mg, and 9 (16.7%) 0.5 mg patients. No hyperkalemia ≥6.0 mmol/L was observed. We conclude that KBP-5074 effectively lowers blood pressure with some risk of hyperkalemia in individuals with advanced chronic kidney disease and uncontrolled blood pressure.
Registration:
URL: https://www.clinicaltrials.gov; Unique identifier: NCT03574363.
Poorly controlled and resistant hypertension (RH), that is, blood pressure (BP) that is not at goal in patients already receiving 2 to 3 antihypertensive drugs, are prevalent in people with advanced chronic kidney disease (CKD). RH is especially prevalent among individuals with an estimated glomerular filtration rate (eGFR) <45 mL/(min·1.73 m2).1,2 The estimated prevalence of CKD in 2017 was roughly 844 million worldwide,3 with 31 to 34 million in the United States with CKD between 2015 and 2016.3–5 Of individuals with CKD in the United States between 2015 and 2016, 15 to 18 million had evidence of CKD stage 3b or 4.5 This high prevalence of stage 3b or 4 CKD also portends a high RH prevalence, with true RH occurring in about 23% of individuals with CKD compared with about 10% of individuals in the general population of treated patients with hypertension.6
Sustained BP reduction to levels <140/90 mm Hg slows kidney disease progression,7 and levels <130/80 mm Hg also reduce the risk for cardiovascular events.8 The most recent American Heart Association Consensus Report on RH mandates addition of a steroidal mineralocorticoid receptor antagonist (MRA), spironolactone, to established antihypertensive triple therapy that includes a renin-angiotensin system blocker, calcium antagonist, and thiazide-type diuretic, at maximal or maximally tolerated doses.1 Data for this recommendation, however, come from a study in patients with normal kidney function,9 whereas spironolactone’s major limitation in advanced CKD (eGFR, 15–44 mL/[min·1.73 m2]) is increased risk for hyperkalemia.10
Hyperkalemia risk increases when eGFR is <45 mL/(min·1.73 m2) or serum potassium at the start of therapy is >4.8 mmol/L even while on an appropriate diuretic.2,11 Moreover, currently available steroidal MRAs are contraindicated for treating hypertension in patients with advanced CKD (creatinine clearance <50 mL/min).12,13
Several new nonsteroidal MRAs are being studied. Three are being investigated in patients with hypertension and stage 3 CKD (esaxerenone, Japan only14; apararenone, in Asia15; and KBP-5074, internationally16). A fourth nonsteroidal MRA, finerenone, was recently shown to reduce diabetic kidney disease progression and cardiovascular outcomes in patients with diabetic nephropathy but had only a minimal effect on BP reduction.17
KBP-5074 is a highly selective nonsteroidal MRA with a higher binding affinity to the mineralocorticoid receptor than steroidal MRAs (ie, spironolactone and eplerenone). In clinical studies, KBP-5074 exhibited a half-life of ≈60 hours, which was not affected by dialysis. The current phase 2b study was designed to evaluate the BP-lowering efficacy, safety, and pharmacokinetics of KBP-5074 in patients with uncontrolled hypertension (failure to achieve target BP, despite taking ≥2 antihypertensive medications, one of which must have been a high ceiling diuretic) and who have stage 3b or 4 CKD.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request.
BLOCK-CKD is a phase 2b, international, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. It evaluates the safety, efficacy, and pharmacokinetics of the nonsteroidal MRA KBP-5074 for uncontrolled hypertension in patients with stage 3b/4 CKD already receiving background antihypertensive medication. The rationale and design of this study were previously published.16 Details of the inclusion/exclusion criteria are published elsewhere16 and are provided in Table S1 in the Data Supplement.
Briefly, male and female patients aged 18 through 85 years with body mass index of 19 to 45 kg/m2, stage 3b/4 CKD (defined as eGFR ≥15 and ≤44 mL/[min·1.73 m2]), and uncontrolled grade 1 and 2 systolic hypertension (defined as resting trough cuff seated systolic BP [SBP] ≥140 and ≤179 mm Hg18 at screening and the end of the placebo run-in period) were enrolled. Blood measurement was performed according to American Heart Association guidelines and described in our design article and added to the Data Supplement (Table S2) to this article.1,16 Approximately 30% of patients enrolled in the study were to have eGFR in the range of ≥15 and ≤29 mL/(min·1.73 m2). Patients were concurrently receiving ≥2 antihypertensive medications (ie, diuretics [except potassium-sparing diuretics] that were mandated by the protocol unless there was documented intolerance or contraindication in diuretic therapy, renin-angiotensin system blockers, or calcium channel blockers) at stable doses for 30 days before randomization, per guidelines.1
Trial Conduct
The study was initially planned to enroll 240 patients; however, 162 subjects were subsequently enrolled. Recruitment ended earlier than expected due to the coronavirus disease 2019 (COVID-19) pandemic. The Independent Data Monitoring Committee, including 2 physicians and one statistician, periodically reviewed safety data per the Independent Data Monitoring Committee charter. An independent statistical team conducted an interim administrative analysis for a manufacturing decision in June 2020. A specific blinding plan, including a robust firewall, was created and shared with the US Food and Drug Administration. Participating investigators and regulatory and clinical team members did not have access to the administrative interim analysis data results, thereby ensuring equipoise and ongoing protection of patient data.
Patients gave written informed consent to participate in this study, which was conducted in compliance with Helsinki Declaration. A central institutional review board and several local independent ethics committees reviewed and approved all appropriate study documentation to safeguard patients’ rights, safety, and well-being.
Statistics
For this phase 2b study, the primary objective was to evaluate the antihypertensive effect of KBP-5074 compared with placebo in patients with advanced CKD. The primary analysis was based on the intent-to-treat population, which consisted of all randomized patients who took at least one dose of study drug, had a baseline SBP measurement, and had at least one postrandomization SBP measurement. In addition, the per-protocol population was used to assess the robustness of the primary analysis results. The per-protocol population included all intent-to-treat patients who had completed the 84-day double-blind treatment period without any significant protocol deviations.
The primary efficacy analysis was performed using a 2-way ANCOVA model, with treatment, baseline eGFR level (≥30 mL/[min·1.73 m2] versus <30 mL/[min·1.73 m2]), and background antihypertensive medications (3 or more) as factors, and baseline SBP value as a covariate. Model-adjusted least-squares mean, SE, and 2-tailed 95% CI were estimated for each treatment group. A similar approach (using the ANCOVA model) was taken to compare the treatment difference between each KBP-5074 dose versus placebo.
The supportive analysis was carried out for the primary efficacy variable based on the per-protocol population to examine the impact of premature dropouts or significant protocol deviations or violations.
Secondary end point analysis of diastolic BP (DBP) was evaluated similarly to SBP. Given the trial’s short duration and the considerable variation among fewer patients, the analysis of urinary albumin-to-creatinine ratio (UACR) focused on the median value trend from baseline through day 84.
Per the original study design, assuming an observed treatment difference of SBP change between the KBP-5074 group and the placebo group is 5 mm Hg, and an SD of change from baseline of 15 mm Hg, with 80 patients/group, the CI of the observed difference would not include 0. Assuming 10% to 15% dropout postrandomization, 80 patients/group, or a total of 240 patients, would be needed for this phase 2b study. No multiple comparison adjustment was applied. The final number of patients enrolled in the study was 162 due to the impact of the COVID-19 pandemic. The reduced final sample size could have impacted the estimate’s accuracy, but as a phase 2b estimation study, it was not powered to detect a treatment effect.
Results
Baseline Characteristics
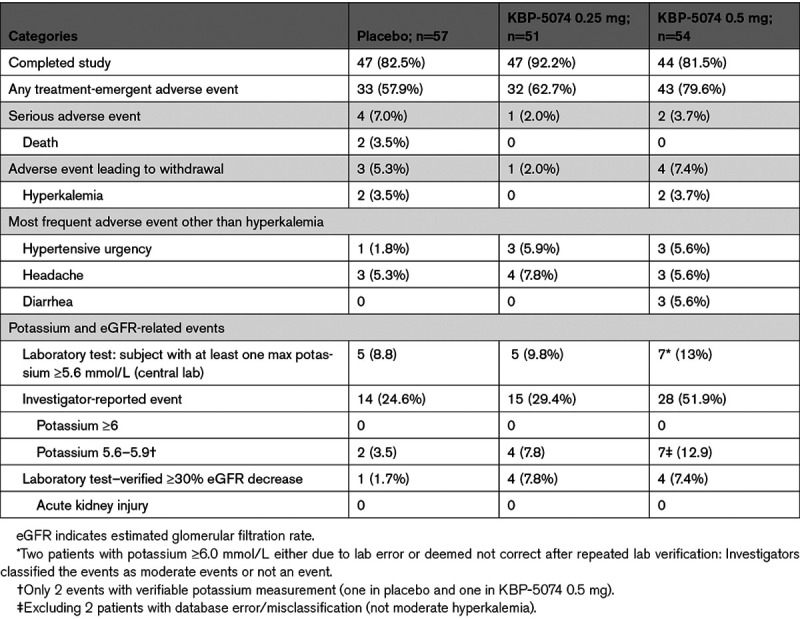
A total of 162 patients were randomized, including 57 patients to the placebo group, 51 to the KBP-5074 0.25 mg group, and 54 patients to the KBP-5074 0.50 mg group (Table 1). One hundred thirty-eight (138) of 162 (85.2%) patients enrolled completed the study, including 47 patients in the placebo group, 47 in the KBP-5074 0.25 mg group, and 44 patients in the KBP-5074 0.50 mg group (Table 2). Eight patients in total (3 placebo, 1 KBP-5074 0.25 mg, and 4 KBP-5074 0.5 mg) withdrew due to adverse events, and 2 deaths occurred, both in the placebo group (Table 2).
Table 1.
Baseline Demographics and Characteristics

Table 2.
Investigator-Reported Treatment-Emergent Adverse Events Across Different Treatment Groups
Upon the completion of enrollment, 162 stage 3b/4 CKD patients randomized in the clinical trial had a mean SBP at baseline of 155.3 mm Hg, and a DBP of 87.7 mm Hg; 64 (39.5%) patients had stage 4 CKD and 125 (77.2%) patients had proteinuria as defined by UACR ≥30 mg/g (Table 1) with the median baseline UACR for placebo, KBP-5074 0.25 mg, and KBP-5074 0.5 mg of 611.9 mg/g, 1003.7 mg/g, and 558.9 mg/g, respectively. eGFR (SD) at baseline was 31.9 (9.90) mL/(min·1.73 m2), and 144 (88.9%) patients were taking at least 3 antihypertensive medications (Table 1).
Primary Outcome
Systolic BP
The primary end point was the change in resting trough cuff seated SBP from baseline to day 84. Figure 1A shows that the reduction of the trough cuff seated SBP was observed as early as day 7. The change in SBP from baseline to day 84 for patients in the 0.5 mg KBP-5074 cohort was −15.9 mm Hg compared with −5.3 mm Hg for the placebo cohort, representing a significant difference of −10.2 mm Hg based on a model-adjusted mean difference (P=0.0029). For patients in the 0.25 mg KBP-5074 cohort, the change in SBP was −11.5 mm Hg compared with −5.3 mm Hg for the placebo cohort, representing a statistically significant difference of −7.0 mm Hg based on a model-adjusted mean difference (P=0.0399).
Figure 1.
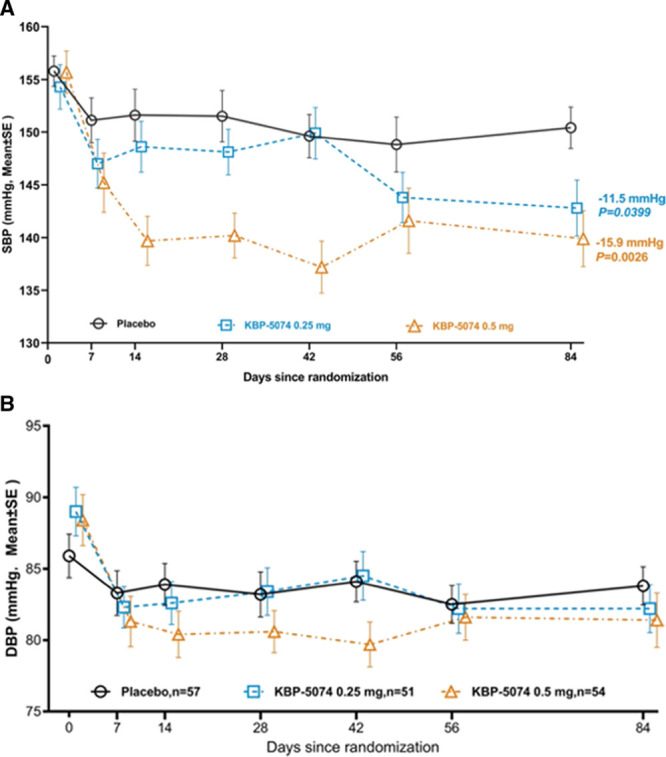
The effect of KBP-5074 on blood pressure in CKD cohort. A) Systolic blood pressure (SBP) from baseline to end of treatment (intent-to-treat [ITT] population/last observation carried forward [LOCF], N=162). P values were calculated based on ANCOVA model. B, Diastolic blood pressure (DBP) from baseline to end of treatment (ITT population/LOCF, N=162).
The per-protocol population analysis showed similar results. A significant reduction of −10.6 mm Hg versus placebo based on a model-adjusted mean difference (P=0.0058) and a significant reduction of −8.3 mm Hg versus placebo based on a model-adjusted mean difference (P=0.0266) were shown for the 0.5 mg and 0.25 mg dose groups, respectively.
In addition, we assessed changes in SBP in groups taking <2 versus ≥3 medications as an exploratory analysis. The SBP reduction in KBP-5074 dose groups versus placebo in 2 subgroups is comparable.
Secondary Outcomes
The key prespecified secondary outcome variables included change in trough cuff seated DBP from baseline at day 84 and change and percentage change in UACR from baseline at day 84.
Diastolic BP
As depicted in Figure 1B, the overall mean (SE) changes in trough cuff seated DBP to day 84 was −2.0 mm Hg (1.41) for the placebo group, −6.7 mm Hg (2.02) for the KBP-5074 0.25 mg group, and −7.0 mm Hg (2.23) for the KBP-5074 0.5 mg group. The treatment differences were not significant. The baseline mean for all groups was 87.7 mm Hg.
Urinary Albumin-to-Creatinine Ratio
One hundred twenty-five (125) of 162 (77.2%) patients in the study had albuminuria at baseline (Table 1). Because baseline UACR values varied widely among patients (range: 31.2–7971 mg/g), the analysis focused on the median UACR through day 84. Although there was a trend in reduction, no significant difference was seen between groups. The median baseline UACR values for the placebo, KBP-5074 0.25 mg, and KBP-5074 0.5 mg dose groups were 611.92, 1003.67, and 558.90 mg/g, respectively, and the median UACR values at day 84 were 678.00, 415.29, and 454.40 mg/g, respectively. A subgroup analysis was completed for subjects with a baseline UACR >300 mg/g in the placebo, KBP-5074 0.25 mg, and KBP-5074 0.5 mg dose groups. The median UACR baseline values were 1687.34, 1372.19, and 1359.36 mg/g, respectively, and the median UACR values at day 84 were 1355.07, 746.24, and 950.14 mg/g, respectively. Changes in SBP, DBP, and UACR are found in Table S3.
Safety Outcomes
KBP-5074 was observed to be well tolerated in patients in the BLOCK-CKD trial, with no reported cases of severe hyperkalemia (potassium levels ≥ 6 mmol/L), acute kidney injury, or hospitalization due to hyperkalemia.
A total of 8 patients discontinued the study due to adverse events, 3 patients in the placebo group, 1 patient in the 0.25 mg group, and 4 patients in the 0.5 mg group. Of these 4 patients, 2 in the placebo group and 2 in the 0.5 mg group were withdrawn by the investigator because of hyperkalemia.
Potassium
Increases in potassium post-treatment were observed in all 3 groups, with the largest increase in the 0.5 mg dose group (Figure 2). Hyperkalemia (based on central laboratory potassium levels ≥5.6 mmol/L) in the placebo, 0.25 mg, and 0.5 mg groups was observed in 5 (8.8%) patients, 5 (9.8%) patients, and 7 (13%) patients, respectively (Table 2). None of the hyperkalemia in any treatment group was considered by investigators to be severe. Investigator-reported hyperkalemia (serum potassium levels, 5.6–5.9 mmol/L) occurred in 15 (9.3%) patients. No investigator-reported hyperkalemia ≥6.0 mmol/L occurred. No study subjects were hospitalized due to hyperkalemia. Additionally, we reviewed the patients with and without diabetes and noted no obvious difference in serum potassium elevation among patients with or without diabetes post-treatment.
Figure 2.
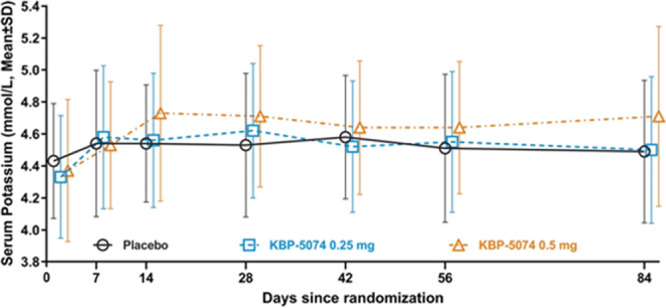
Line plot of potassium over time (safety population). On average, increases in potassium by day 84 were 0.08, 0.19, and 0.33 mmol/L in the placebo, 0.25 mg, and 0.5 mg groups, respectively.
eGFR Changes and Events
eGFR was expected to decrease due to the hemodynamic effect of lowering SBP. No significant change in eGFR was observed in either the 0.25 mg group or the 0.5 mg group compared with placebo, Figure S1. Overall, there was no significant initial decrease in eGFR in both KBP-5074 groups at the beginning of the study. No study subjects withdrew due to worsening eGFR or acute kidney injury.
Discussion
The BLOCK-CKD trial resulted in a significant reduction of SBP in patients with uncontrolled hypertension, 89% of whom had RH. Additionally, in patients with a mean eGFR of 34 mL/(min·1.73 m2), KBP-5074 was comparable to placebo for hyperkalemia resulting in drug discontinuation. The overall mean baseline eGFR was 31.9 mL/(min·1.73 m2). Moreover, there were no hyperkalemia-related serious adverse events or hospitalizations, and there was no use of potassium binders in either group. Thus, the results support the efficacy and safety of KBP-5074 for treating patients with uncontrolled or RH and advanced CKD (CKD stage 3b/4).
A direct comparison of KBP-5074 to steroidal MRAs, ie, spironolactone or eplerenone, in patients with uncontrolled hypertension and advanced CKD is not available; however, it should be noted that in the AMBER (Patiromer Versus Placebo to Enable Spironolactone Use in Patients With Resistant Hypertension and Chronic Kidney Disease): a phase 2b, randomized, double-blind, placebo-controlled trial of RH and CKD (mean eGFR, 36 mL/[min·1.73 m2]), patients were all given spironolactone and randomly assigned to receive either placebo or the potassium-lowering drug patiromer.10 Hyperkalemia in the AMBER trial involving patients receiving a placebo with spironolactone resulted in a 23% discontinuation rate.10 In contrast, in the BLOCK-CKD study with a comparable range of eGFR, 3.7% of the subjects in the highest dose group of 0.5 mg permanently discontinued the study due to hyperkalemia versus 3.5% in the placebo group without any use of potassium binders. Moreover, none of the patients in the 0.25 mg group discontinued treatment due to hyperkalemia. A low incidence of hyperkalemia was also seen in the phase 3 trial of finerenone (FIDELIO [Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease]). However, the average eGFR in that study was ≈44 mL/(min·1.73 m2).17 Thus, nonsteroidal MRAs are different from the steroidal MRAs eplerenone and spironolactone concerning hyperkalemia risk.19
Limitations
This trial’s results are limited due to cohort size and restricted duration of follow-up and cannot be generalized to a larger population. Additionally, we had planned an analysis with ambulatory blood pressure monitor, however, the ability to perform 24-hour ambulatory blood pressure monitor in a sufficient number of subjects was dampened by the COVID-19 pandemic and operational issues. This phase 2b trial was designed to assess the effect of the KBP-5074 dose on BP reduction and safety. Although guiding this drug’s use in the subpopulation of individuals with uncontrolled or RH and advanced CKD, the data are unique to this trial. Further study is required for broader extrapolation.
Perspectives
BLOCK-CKD demonstrates that KBP-5074 effectively decreases BP reduction with a lower-than-expected risk of hyperkalemia in a high-risk group. Currently, the only guideline-recommended MRA for RH is very limited in advanced CKD due to high hyperkalemia risk, a safety afforded to KBP-5074. Should BLOCK-CKD results be confirmed in a prospective, randomized, powered phase 3 trial, there would be important implications for the use of KBP-5074 in patients with advanced CKD and resistant or poorly controlled hypertension. Additionally, the BLOCK-CKD trial results may impact patients with heart failure and reduced ejection fraction. In these patients, MRAs are known to reduce cardiovascular mortality and hospitalization, but the initiation of MRAs is not optimized to reduce the risk of hyperkalemia markedly.
Acknowledgments
We are grateful for the contributions of the many investigators (Table S4), without whom this study could not have been conducted, and to the study patients, site staff, and monitors whose dedication to the study resulted in data that bring hope to patients with uncontrolled hypertension and advanced chronic kidney disease (CKD). The authors also thank Tam M. Nguyen-Cao, PhD, CMPP, of Claritas Scientific LLC for medical writing services, and Ann Bledsoe Bollert, MA, CMPP, of y axis Editorial and Terri O’Quin of O’Quin Editorial Services LLC for editing this manuscript. We also express special thanks to Daniel Wilson, MD, who was a medical director for this study and contributed a great deal to experimental design; Xiaojuan Tan, director of project management; Fran Newark, senior clinical trial manager; Jinrong Liu, project manager; and Shuangshuang Chi, biology lab head for their superb management of the BLOCK-CKD study.
Sources of Funding
This study was funded by KBP Biosciences PTE Ltd, the developer of KBP-5074.
Disclosures
G. Bakris is the principal investigator of the FIDELIO trial (Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease; Bayer) and on the steering committee of the Controlling and Lowering Blood Pressure With the MobiusHD trial (Vascular Dynamics). He is a consultant to Merck, KBP Biosciences, Relypsa, and Alnylam. B. Pitt is the coprincipal investigator of the FIGARO trial (Finerenone in Reducing Cardiovascular Mortality and Morbidity in Diabetic Kidney Disease) evaluating the nonsteroidal mineralocorticoid receptor antagonist (MRA) finerenone (Bayer). He is a consultant for Bayer, Astra Zeneca, Sanofi/Lexicon, Amgen, Relypsa/Vifor (stock options), Boehringer Ingelheim, SC Pharmaceuticals (stock options), Sqinnovations (stock options), G3 pharmaceuticals (stock options), KBP Biosciences (stock options), Cereno Scientific (stock options), Tricida (stock options), Phasebio, and holds US Patent 9931412 (site-specific delivery of eplerenone to the myocardium), and US Patent pending 63/045,784—Histone-Acetylation–Modulating Agents for the Treatment and Prevention of Organ Damage. P.E. Pergola was a study investigator and as such his employer received funds from KBP Biosciences USA. Other relevant conflicts include being a consultant for Bayer and Astra Zeneca. F. Yang, V. Benn, and J. McCabe are employees of KBP Biosciences. The other authors report no conflicts.
Supplemental Materials
Data Supplement Tables S1–S4
Data Supplement Figure S1
Supplementary Material
{kind=link}
Nonstandard Abbreviation and Acronyms
- AMBER
- Patiromer Versus Placebo to Enable Spironolactone Use in Patients With Resistant Hypertension and Chronic Kidney Disease
- CKD
- chronic kidney disease
- COVID-19
- coronavirus disease 2019
- DBP
- diastolic BP
- eGFR
- estimated glomerular filtration rate
- FIDELIO
- Efficacy and Safety of Finerenone in Subjects With Type 2 Diabetes Mellitus and Diabetic Kidney Disease
- MRA
- mineralocorticoid receptor antagonist
- RH
- resistant hypertension
- SBP
- systolic BP
- UACR
- urinary albumin-to-creatinine ratio
The Data Supplement is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/HYPERTENSIONAHA.121.17073.
For Sources of Funding and Disclosures, see page 80.
Contributor Information
Pablo E. Pergola, Email: ppergola@raparesearch.com.
Belkis Delgado, Email: DrDelgado93@hotmail.com.
Diyan Genov, Email: diyan.genov@comac-medical.com.
Tamar Doliashvili, Email: doliashvilit@gmail.com.
Nam Vo, Email: ndvo@mtnkidney.com.
Y. Fred Yang, Email: fred.yang@kbpbiosciences.com.
James McCabe, Email: james.mccabe@kbpbiosciences.com.
Vincent Benn, Email: vince.benn@kbpbiosciences.com.
Bertram Pitt, Email: bpitt@umich.edu.
Novelty and Significance
What Is New?
A novel nonsteroidal mineralocorticoid receptor antagonist significantly reduces blood pressure in people with advanced-stage 3b and 4 chronic kidney disease with minimal risk of hyperkalemia.
What Is Relevant?
KBP-5074 is a very likely candidate to supplant spironolactone for treatment of resistant hypertension in people with advanced chronic kidney disease.
Summary
The results of the BLOCK-CKD study support the efficacy and safety of KBP-5074 for treating patients with uncontrolled or resistant hypertension and advanced chronic kidney disease (chronic kidney disease stage 3b and stage 4).
References
- 1.Carey RM, Calhoun DA, Bakris GL, Brook RD, Daugherty SL, Dennison-Himmelfarb CR, Egan BM, Flack JM, Gidding SS, Judd E, et al. ; American Heart Association Professional/Public Education and Publications Committee of the Council on Hypertension; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Genomic and Precision Medicine; Council on Peripheral Vascular Disease; Council on Quality of Care and Outcomes Research; and Stroke Council. Resistant hypertension: detection, evaluation, and management: a scientific statement from the American Heart Association. Hypertension. 2018;72:e53–e90. doi: 10.1161/HYP.0000000000000084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lazich I, Bakris GL. Prediction and management of hyperkalemia across the spectrum of chronic kidney disease. Semin Nephrol. 2014;34:333–339. doi: 10.1016/j.semnephrol.2014.04.008 [DOI] [PubMed] [Google Scholar]
- 3.Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases. Nephrol Dial Transplant. 2019;34:1803–1805. doi: 10.1093/ndt/gfz174 [DOI] [PubMed] [Google Scholar]
- 4.Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I, Zhao MH, Lv J, Garg AX, Knight J, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385:1975–1982. doi: 10.1016/S0140-6736(14)61601-9 [DOI] [PubMed] [Google Scholar]
- 5.CDC Chronic Kidney Disease Surveillance System—United States. Prevalence of CKD in the general population: CKD stages among US adults, 1988-1994 vs. 1999-2006 vs. 2007-2014 vs. 2015-2016. Accessed January 14, 2021.https://nccd.cdc.gov/ckd/TopicHome/PrevalenceIncidence.aspx
- 6.Noubiap JJ, Nansseu JR, Nyaga UF, Sime PS, Francis I, Bigna JJ. Global prevalence of resistant hypertension: a meta-analysis of data from 3.2 million patients. Heart. 2019;105:98–105. doi: 10.1136/heartjnl-2018-313599 [DOI] [PubMed] [Google Scholar]
- 7.Taler SJ, Agarwal R, Bakris GL, Flynn JT, Nilsson PM, Rahman M, Sanders PW, Textor SC, Weir MR, Townsend RR. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for management of blood pressure in CKD. Am J Kidney Dis. 2013;62:201–213. doi: 10.1053/j.ajkd.2013.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cheung AK, Rahman M, Reboussin DM, Craven TE, Greene T, Kimmel PL, Cushman WC, Hawfield AT, Johnson KC, Lewis CE, et al. SPRINT Research Group. Effects of intensive BP control in CKD. J Am Soc Nephrol. 2017;28:2812–2823. doi: 10.1681/A.S.N.2017020148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Williams B, MacDonald TM, Morant S, Webb DJ, Sever P, McInnes G, Ford I, Cruickshank JK, Caulfield MJ, Salsbury J, et al. ; British Hypertension Society’s PATHWAY Studies Group. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386:2059–2068. doi: 10.1016/S0140-6736(15)00257-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Agarwal R, Rossignol P, Romero A, Garza D, Mayo MR, Warren S, Ma J, White WB, Williams B. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a phase 2, randomised, double-blind, placebo-controlled trial. Lancet. 2019;394:1540–1550. doi: 10.1016/S0140-6736(19)32135-X [DOI] [PubMed] [Google Scholar]
- 11.Collins AJ, Pitt B, Reaven N, Funk S, McGaughey K, Wilson D, Bushinsky DA. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am J Nephrol. 2017;46:213–221. doi: 10.1159/000479802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Inspra. Prescribing information. 2020. Pfizer. https://www.pdr.net/drug-summary/Inspra-eplerenone-1817 Accessed January 16, 2021. [Google Scholar]
- 13.Aldactone. Prescribing information. 2020. Pfizer. https://www.pdr.net/drug-summary/Aldactone-spironolactone-978 Accessed January 16, 2021. [Google Scholar]
- 14.Ito S, Itoh H, Rakugi H, Okuda Y, Yamakawa S. Efficacy and safety of esaxerenone (CS-3150) for the treatment of essential hypertension: a phase 2 randomized, placebo-controlled, double-blind study. J Hum Hypertens. 2019;33:542–551. doi: 10.1038/s41371-019-0207-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nakamura T, Kawaguchi A. Phase 1 studies to define the safety, tolerability, and pharmacokinetic and pharmacodynamic profiles of the nonsteroidal mineralocorticoid receptor antagonist apararenone in healthy volunteers. Clin Pharmacol Drug Dev. 2021;10:353–365. doi: 10.1002/cpdd.855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bakris G, Yang YF, Pitt B. Mineralocorticoid receptor antagonists for hypertension management in advanced chronic kidney disease: BLOCK-CKD trial. Hypertension. 2020;76:144–149. doi: 10.1161/HYPERTENSIONAHA.120.15199 [DOI] [PubMed] [Google Scholar]
- 17.Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, Kolkhof P, Nowack C, Schloemer P, Joseph A, et al. ; FIDELIO-DKD Investigators. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383:2219–2229. doi: 10.1056/NEJMoa2025845 [DOI] [PubMed] [Google Scholar]
- 18.Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39:3021–3104. doi: 10.1093/eurheartj/ehy339 [DOI] [PubMed] [Google Scholar]
- 19.Agarwal R, Kolkhof P, Bakris G, Bauersachs J, Haller H, Wada T, Zannad F. Steroidal and nonsteroidal mineralocorticoid receptor antagonists in cardiorenal medicine. Eur Heart J. 2021;42:152–161. doi: 10.1093/eurheartj/ehaa736 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.