

Summary
Initially, it was reported that coronavirus 2019 disease (Covid‐19) affects respiratory, gastrointestinal and neurological systems, but the oral, olfactory and integumentary systems are also involved. This review discusses various oral manifestations of Covid‐19 reported in the literature along with possible underlying mechanisms. The reported manifestations include taste impairment, oral mucosal changes (petechiae, ulcers, plaque‐like lesions, reactivation of herpes simplex virus 1(HSV1), geographical tongue and desquamative gingivitis) and dry mouth. The prominent location for mucosal lesions are tongue, palate and labial mucosa. The exact pathogenesis of these oral symptoms is not known. Angiotensin‐converting enzyme 2 (ACE2) cell receptors are expressed in abundance on oral mucosa allowing severe acute respiratory syndrome‐coronavirus‐2 (SARS‐CoV‐2) to infect them. Gustatory impairment along with olfactory changes is now listed as a symptom of Covid‐19 by the World Health Organization, but further research is needed to confirm a link between reported additional oral symptoms and Covid‐19. Dental professionals may encounter individuals with Covid‐19 and be called upon to identify various oral manifestations of this disease.
Keywords: Covid‐19, dry mouth, gustatory changes, mucosal lesions, oral manifestations
Abbreviations
- HSV1
herpes simplex virus 1
- PHEIC
Public Health Emergency of International Concern
- SARS‐CoV‐2
severe acute respiratory syndrome‐coronavirus‐2
- TNF
tumour necrosis factor
- WHO
World Health Organization; CN, Cranial Nerve; PCR, Polymerase Chain Reaction; RT‐PCR, Reverse transcription‐ polymerase chain reaction; HSV‐1, Herpes Simplex Virus type 1
1. INTRODUCTION
‘Wuhan Pneumonia of unknown origin’ was identified as a novel coronavirus, the seventh member of the coronavirus family, by Chinese researchers through sequencing its genome. 1 On 30 January 2020, the World Health Organization (WHO) declared this outbreak a Public Health Emergency of International Concern (PHEIC) due to its spread across 18 countries till that date. WHO named this disease as ‘Covid‐19’, which is short for ‘coronavirus disease 2019’. 2 The virus was named severe acute respiratory virus syndrome coronavirus 2 (SARS‐CoV‐2) by the International Committee on Taxonomy of Viruses. 3
Coronavirus comprises a single plus strand of RNA (+ssRNA). SARS‐CoV‐2 is a β‐CoV and mainly infects the respiratory, gastrointestinal, and central nervous systems of humans and mammals. It is transmitted through respiratory droplets, aerosols, contact and fomites. 4 Bilateral lung ground‐glass opacity on computed tomography is found in many patients infected with this virus. Fever, dyspnea, body aches and dry cough are common presenting symptoms, whereas sputum production, hemoptysis, diarrhea and headache are less common symptoms. 5 , 6 Along with these symptoms, this virus can affect other organs including skin, olfactory system and oral cavity. 7 , 8 Various manifestations in the oral cavity such as mucosal lesions, taste changes and gingivitis are reported in the literature. 9 , 10 , 11 Oral lesions can be an inaugural sign of Covid‐19 or a warning sign of peripheral thrombosis. 7 , 12 To avoid more serious complications arising as a result of peripheral thrombosis, it is suggested to start anticoagulant therapy as soon as possible after emergence of these oral lesions. 12
As dental practices throughout the world have opened or are preparing to open, it is quite possible that dentists may encounter oral manifestations of Covid‐19 in their patients. The objective of this review is to report various oral manifestation of Covid‐19 described in the literature. This will help dental professionals to focus on detailed intraoral examination before initiating any dental treatment on Covid‐19 suspected or confirmed patients.
2. METHODOLOGY
2.1. Search strategy
Online database PubMed was searched for all publications related to oral manifestation of Covid‐19 with a combination of following keywords:
‘Covid‐19’ or ‘2019 novel Coronavirus’ or ‘2019‐nCoV’ or ‘SARS‐CoV‐2’,
and ‘oral manifestation’
(1) and ‘oral sign and symptoms’
(1) and ‘oral mucosal changes’
(1) and ‘taste impairment’
(1) and ‘gustatory changes’
2.2. Inclusion criteria
Publications in English language only.
Publications from January 2020 to February 2021.
Type of publications (letter to the editors, correspondence, case report, case series, observational studies, clinical studies, clinical trials and reviews).
2.3. Exclusion criteria
The publications addressing Covid‐19 symptoms in general or challenges in dentistry without reference to oral manifestations or oral symptoms.
The studies presenting oral mucosal changes without reference to Covid‐19.
In cases, where both the review and research articles present in that review were retrieved, a review article was selected instead of individual studies (Duplication removal).
2.4. Article selection
Publications screening and selection was divided into two phases: an initial screening of titles and abstracts, and final screening of full‐text publications. Authors (Huma Farid, Madiha Khan, Shizrah Jamal) independently screened the titles and abstracts of retrieved publications from the initial search strategy. In this stage, articles were included if they reported the above‐mentioned keywords in title or abstract. Full‐text reading was carried out at initial screening stage only if the content of the title/abstract was unclear or abstract was not provided.
The initial screening phase was followed by full‐text publication screening. In this phase, publications were screened and selected on the basis of pre‐determined inclusion and exclusion criteria. There was no disagreement between the authors during screening process.
Except for the taste impairment, all other oral manifestations were mostly reported in the form of cross sectional studies, letters to the editors, case reports or short communications. Due to scarcity of literature on this topic, we were not able to report a systematic review. Still to make a structured narrative review and ensured standardization, PRISMA flowchart was followed for literature search and selection (Figure 1: Literature search flowchart).
FIGURE 1.
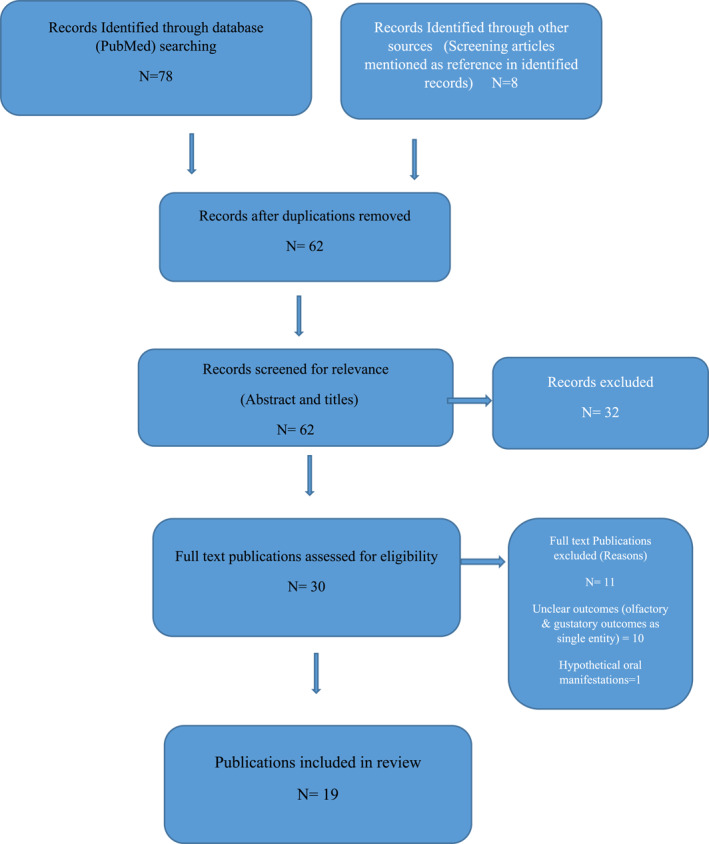
Literature search flowchart
3. RESULTS
Using the described search strategy, a total of 86 publications were retrieved. After removing the duplicate publications, the total number reduced to 62. These 62 publications underwent titles and abstract screening and 30 were selected for full‐text screening. On full‐text review, 11 publications were excluded. In addition to the above‐mentioned exclusion criteria, at this stage, the studies that did not distinguish between olfactory and gustatory impairment and considered them one entity were excluded. Similarly, a publication with hypothesized oral manifestations that can arise as a result of Covid‐19 was excluded. A total of 19 publications were selected. Among these, there was one systematic review and meta‐analysis on gustatory changes associated with Covid‐19. For the remaining oral manifestations, mostly case report, case series, letters to the editors and short communications were found. The summary of included publications including type of study, demographics of patients (age and gender), oral manifestations, treatment provided, duration of symptoms and Covid‐19 confirmation status is presented in Table 1. The reported oral manifestations are briefly discussed under the discussion section.
TABLE 1.
Publications regarding oral manifestations associated with COVID 19
| Type of study | Author, year | No. of patients, age & gender | Oral manifestation | Covid‐19 confirmed/suspected | Treatment provided | Symptoms resolved |
|---|---|---|---|---|---|---|
| Letter to the editor | Chaux‐bodard 7 | 1 patient | Irregular ulcer on the dorsal side of the tongue | Confirmed at 8 days (RT‐PCR) | Not mentioned | Healing of ulcer without scar after 10 days |
| 2020 | 45 years female | |||||
|
Case series |
Martín Carreras‐Presas C 10 | 3 patients | *Dysgeusia, *Multiple ulcers on palate and internal lip *Mucosal blisters, *Desquamative gingivitis, *Pain in tongue. | 1 confirmed | Valaciclovir 500 mg every 8 h for 10 days, and topical antiseptics with chlorhexidine and hyaluronic acid, Predinolone | Within 7–10 days |
| 2020 |
56 years Male |
2 suspected | ||||
| 58 years Male | ||||||
| 65 years Female | ||||||
| Letter to the editor | Patel J, Woolley J 11 | 1 patient | *Severe halitosis, | Suspected | 400 mg metronidazole three times daily for 5 days and 0.12% chlorhexidine mouthwash twice daily for 10 days. | Complete resolution of oral and Covid‐19 symptoms after 5 days |
| 2020 | 35 years | *Generalized erythematous and edematous gingivae, | ||||
| Female | *Necrotic interdental papillae in both the maxillary and mandibular labial sextants. | |||||
| Cross–sectional study | Favia G 12 | 123 patients | *Geographic tongue (5) | Confirmed‐PCR | Hyaluronic acid gel and chlorhexidine 2% mouthwash or gel (twice a day) for 14 days in patients with ulcero‐erosive lesions | Days of appearance of symptoms mentioned. |
| 2021 | 70 male | *Fissured tongue (4) | Miconazole nitrate twice a day in patients with cytological diagnosis of candidiasis tranexamic acid for local hemorrhages | No information regarding resolution of symptoms. | ||
| 53 female | *Ulcerative lesion (51) | |||||
| Median age = 72 years | *Blisters (14) | |||||
| (Patients were classified as moderate, severe and critical form of Covid‐19) | *Hyperplasia of papillae (33) | |||||
| *Angina bullosa (8) | ||||||
| *Candidiasis (18) | ||||||
| *Ulcero‐necrotic gingivitis (1) | ||||||
| *Petechiae (4) | ||||||
| *Above 80% of patients in each form of Covid‐19 presented with taste disorders | ||||||
| Case report | Zarch et al. 13 | 1 patient, | *Vesicles | Confirmed (PCR) | Azithromycin, levofloxacin | 7 days |
| 2021 | 56 year old female | *Dry mouth | Anti‐inflammatory and antiasmathic drugs (montelukast, naproxen and acetaminophen) | |||
| *Dysgeusia | ||||||
| Case series | Riad et al. 14 | 26 patients mean age = 37 | *Ageusia = 3 | Confirmed (PCR) | Chlorhexidine, paracetamol | 21 patients = 7 days |
| 2020 | Male = 9 | *Painful tongue ulcers (all cases) | 5 patients = 14 days | |||
| Female = 17 | ||||||
| Systematic review | Tong JY & colleagues 15 | 1390 patients (9 studies) | 626 reported gustatory dysfunction | Majority were hospitalized & RT‐PCR was done | Not mentioned in review | Not mentioned in review |
| 2020 | ||||||
| Case report | Hjelmesæth J, Skaare D 16 |
2 patients male in sixties |
Ageusia for 9 days | Confirmed (RT‐PCR) | No treatment for taste disturbance | On 10 days, sweet & sour flavor was detected On 13th day umami flavor was detected |
| 2020 | ||||||
| Male in ninties | Dysgeusia | Not mentioned | Not mentioned | Not mentioned | ||
| Case report | Santos JA dos et al. 17 | 1 patient | *White plaque and multiple tiny yellow ulcers on dorsum of the tongue (resemble to late stage of herpetic recurrent oral lesions associated with candidiasis) | Confirmed (RT‐PCR) | *Intravenous fluconazole (Zoltec® 200 mg/100 ml, one bag a day for 10 days) and oral nystatin (100,000 IU/ml, 8/8h, for 30 days), but no regression was observed. Then | Complete lesion of white lesion after 14 days of oral examination |
| 2020 | 67 years | *asymptomatic geographical tongue | *Antifungals, chlorhexidine digluconate (0.12%), 1% hydrogen peroxide. | Over the time recession in size of geographical tongue | ||
| Male | *Lower lip nodule (reactive reaction) | |||||
| *Hypogeusia | ||||||
| Correspondence | J Jimenez‐Cauhe et al. 29 | Total 4 patients | Palatal macules and petechiae | Confirmed (PCR) | Systemic corticosteroids | Within 2–3 weeks. |
| 2020 | Oral manifestations in 3 | |||||
| Mean age | ||||||
| 66.75 years all female | ||||||
| Case series | Orcina F et al. 30 | 4 patients, | Apthous ulcers | Confirmed (PCR) | Phtalox mouth wash | 12 h–4 days |
| 2021 | 52 year old male | |||||
| 32 year old male | ||||||
| 30 year old female | ||||||
| 29 year old male | ||||||
| Case report and narrative review | Hockova et al. 31 | Total = 210, | *Perioral pressure ulcers = 179 | Confirmed (PCR) | Dressings, position adjustment, antifungals, antivirals, and surgical interventions, full thickness excisions | Healed after 1–2 weeks |
| 2021 | 23 female | *Intraoral candidiasis = 27, | ||||
| 62 male | *Other intraoral ulcers = 3 | |||||
| *macroglossia = 1, | ||||||
| Prospective, observational study | Fidan et al. 32 | 74 patients | *Apthous ulcers = 27 | Confirmed (PCR) | Not reported | Not reported |
| 2021 | 49 males, 25 females | *Erythema = 19 | ||||
| *Lichen planus = 12 | ||||||
| Descriptive cross sectional study (Questionnaire based) | C. Galván Casas et al. 39 | Total 375 cases | Maculopapular eruption on palatal and lower lip mucosa | 1 confirmed | Not available | Not mentioned |
| 2020 | Oral manifestation in 2 | 1 suspected | ||||
| Age and gender not specify | (Method of Covid‐19 confirmation not mentioned) | |||||
| Descriptive cross sectional study (Web based questionnaire) | Biadsee A 41 | Total 128 | *Impaired sense of taste = 67 | Confirmed (RT‐PCR) | Not mentioned | Not mentioned |
| 2020 | Mean age 36.25 | *Dry mouth = 72 | ||||
| 58 male | *Facial pain = 18 | |||||
| 70 female | *Masticatory muscles pain = 15 | |||||
| *Change in tongue sensation = 20 | ||||||
| *plaque‐like changes in the tongue = 9 | ||||||
| *Swelling in the oral cavity = 9 | ||||||
| *Swelling in palate = 4 | ||||||
| *Swelling in tongue = 4 | ||||||
| *Swelling in gums = 2 | ||||||
| Prospective Cohort study | M Hedou et al. 42 | Total 103 patients | Oral herpes simplex virus‐type 1 (HSV‐1) reactivation | Confirmed (PCR) | Not available | Cutaneous manifestations disappeared with median time of 48 h (from 24 h to 6 days). Oral manifestation disappearance not mentioned. |
| 2020 | Oral manifestation in 1 | |||||
| Age & gender not mentioned | ||||||
| Descriptive, cross sectional study (in two phases) Active phase (A) and 15 days after RT‐PCR ‐(B) | Freni F et al. 43 | 50 patients | *Gustatory disorders | Confirmed | Not mentioned | 15 days after RT‐PCR became negative, |
| 2020 | Mean age 37.7 | A = 35 | (Autoimmune RT‐PCR) | Gustatory disorder in 4 | ||
| 30 male | B = 4 | Xerostomia in 1 patient | ||||
| 20 female | *Xerostomia | |||||
| A = 16 | ||||||
| B = 1 | ||||||
| Case report | Villalba LN et al. 44 | 2 patients | 5‐days history of taste loss preceding smelling problems and fatigue. | Confirmed (PCR) | Asymptomatic treatment and an oxygen supply. | Not mentioned |
| 2020 | 1 with oral manifestations | |||||
| 80 years female | ||||||
| Letter to editor | Ansari et al. 45 | 2 patients with oral manifestations | *Painful, red ulcerations on hard palate = 1 | Confirmed (PCR) | Diphenhydramine, dexamethasone, tetracycline, and lidocaine | Healed after 1 week |
| 2020 | *Several small painful ulcers on the anterior tongue = 1 |
4. DISCUSSION
4.1. Gustatory changes or taste impairment
Gustatory and olfactory changes can be the only symptom in mild cases of Covid‐19 or the initial symptom in patients who ultimately present with more severe respiratory failure. The reported gustatory changes associated with Covid‐19 are hypogeusia, dysgeusia and ageusia. 10 , 13 , 14 , 15 , 16 , 17 The exact pathogenesis of SARS‐CoV‐2 and olfactory and gustatory dysfunction is not known. It is reported that angiotensin‐converting enzyme 2 (ACE2) cell receptors are expressed in abundance on respiratory epithelium and oral mucosa especially tongue. 16 , 18 SARS‐CoV‐2 has a great affinity for these receptors. 19 , 20 Direct damage to nasal and oral epithelium and neuroinvasive nature of this virus can result in olfactory and gustatory disorders. It is reported that 95% of the cases with taste disturbances are secondary to olfactory dysfunction. 21 Olfactory dysfunction should be considered as a primary cause if patient complaints of both smell and taste disturbances. Most of the studies had considered smell and taste disturbances as a single entity rather than two separate entities. 22 , 23 , 24 In fact, it is often very difficult for the patient to delineate between taste and smell dysfunctions. There is a need to highlight Covid‐19 cases presented with gustatory dysfunction (hypogeusia, dysgeusia and ageusia) in the absence of olfactory changes. Investigations such as whole mouth and spatial taste tests can be employed to identify the presence of gustatory dysfunctions along with localization of area of impairment and threshold sensitivity to a particular taste. 25 Different mechanisms proposed in the literature for taste alterations are shown in the Figure 2.
FIGURE 2.
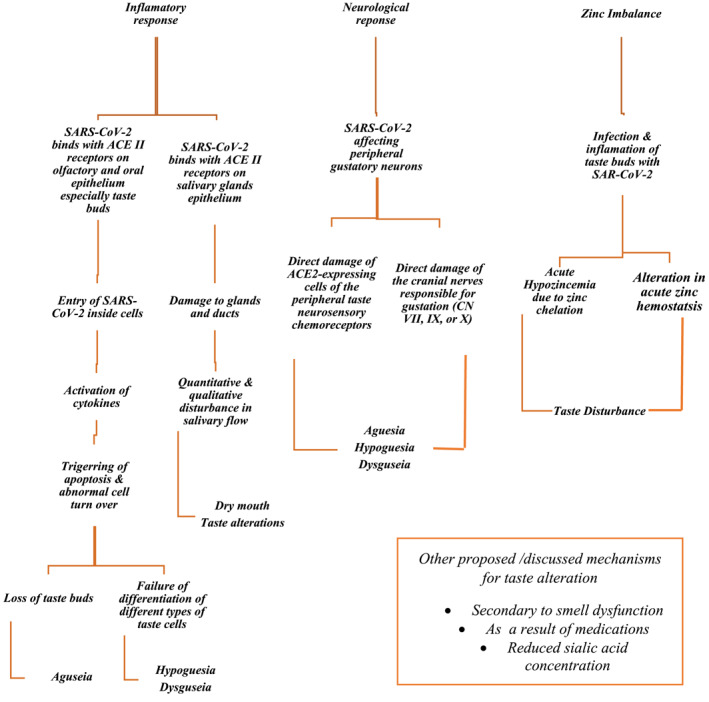
Proposed mechanisms for taste alteration in Covid‐19. ACE2, angiotensin‐converting enzyme 2; SARS‐CoV‐2, severe acute respiratory virus syndrome coronavirus 2
Based on the frequent presence of these symptoms in Covid‐19 positive and suspected patients, the American Academy of Otolaryngology recommended the addition of anosmia, hyposmia, and dysgeusia to the list of screening tools for COVID‐19 in asymptomatic individuals. 26 The US Centers for Disease Control and Prevention officially added olfactory and gustatory dysfunctions as an important Covid‐19 symptom whereas the WHO listed them as less common symptoms of Covid‐19. 27 , 28
4.2. Oral mucosal lesions
Many oral mucosal lesions are reported in Covid‐19 confirmed and suspected individuals. They include ulcers, erosions, blisters, plaque‐like lesions, reactivation of herpes simplex virus 1(HSV1), and geographical tongue. 10 , 13 , 14 , 29 , 30 , 31 , 32 , 33 Oral mucosal lesions are presented along with common symptoms of Covid‐19 or with other cutaneous manifestations. The lesions appear either before or along with systemic manifestations of Covid‐19. A clear relationship between Covid‐19 and oral mucosal lesions has yet to be established. It is stated in few publications that only oral symptom associated with Covid‐19 is taste impairment and other oral lesions arise as a result of decreased immunity due to viral infection, opportunistic or secondary infection or treatment for Covid‐19. 8 , 14 , 32 , 34 , 35 Oral mucosal lesions are reported to disappear (6 days–2 weeks) or regress in size with time. 7 , 17 , 29 Different possible mechanisms proposed in the literature for oral mucosal lesions are shown in Figure 3. Following is the brief description of different oral mucosal lesions as reported in the literature.
FIGURE 3.
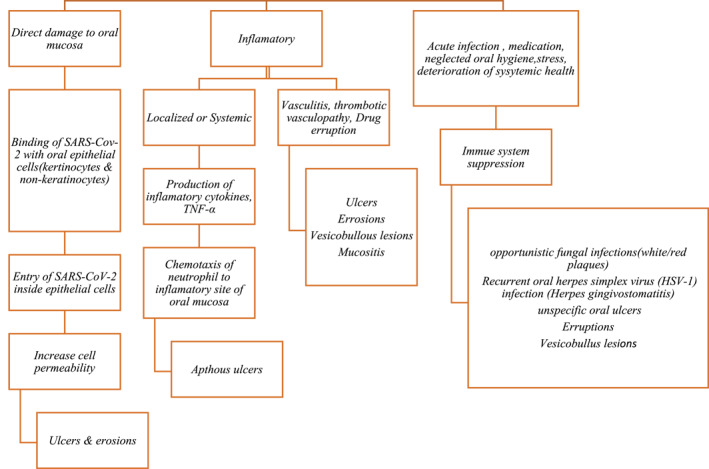
Proposed mechanisms of oral mucosal lesion due to Covid‐19. SARS‐CoV‐2, severe acute respiratory virus syndrome coronavirus 2; TNF, tumour necrosis factor
4.2.1. Ulcers and erosions
One of the most common oral complication associated with Covid‐19 confirmed or suspected individuals is ulcerative lesions of the oral cavity. 7 , 13 , 14 , 17 , 29 , 32 , 36 , 37 , 38 The site, pattern and presentation varies in different reported papers. Tongue (dorsum and lateral boarder) is the most common reported site followed by hard palate and buccal mucosa. Irregular and painful ulcers either appear alone (single ulcers) or in the form of multiple tiny ulcers. Clusters of ulcers either resemble herpetiform ulcers or multiple apthoid ulcers with diffuse erythematous base. These multiple apthoid ulcer later on coalesce to form large ulcers with yellowish fibrin covering them, resembling erythema multiform‐like disease. 12 Ulcers, erosions and blood crust on labial mucosa along with palatal and gingival petechiae are also reported in one study. 38
4.2.2. Vesicobullous lesions
These lesions mostly appear in association with cutaneous manifestations and show a range of presentation such as blisters, petechiae, erythematous lesions and erythema multiform‐like lesions. 10 , 17 , 29 , 31 , 36 , 38 , 39 , 40 Tounge and palate (soft and hard) are the most common reported location of these lesions. Erythema multiform‐like lesions are most commonly reported lesions accompanied by skin target lesions. 29
4.2.3. Plaques (white or red)
Candidal plaque‐like lesions are also observed in association with Covid‐19. Both red and white plaques were observed. They are located on the dorsum of the tongue and palate. They were also observed along with multiple tiny ulcers, taste changes, tongue and masticatory muscles pain. 12 , 17 , 41 Immune system suppression as a result of antibiotic therapy, deteriorating general health and neglected oral hygiene can be possible causes of these plaques.
4.2.4. Reactivation of Herpes Simplex 1(HSV 1)
Hedou et al. while reporting cutaneous manifestations of Covid‐19 in 103 patients found reactivation of Herpes Simplex in one intubated patient in intensive care. Although cutaneous manifestations disappeared with median time of 48 h (from 24 h to 6 days), no information regarding resolution of Herpes simplex is provided. 42 Another study also reported multiple tiny yellow ulcers on dorsum of the tongue that resembled to late stage of herpetic recurrent infection along with geographical tongue. Both cases in above‐mentioned studies were confirmed Covid‐19.
4.2.5. Angina bullosa
These blood filled blisters are observed on soft palate, tongue and cheek. They are brown–black single or multiple lesions and may appear after initiation of therapies for Covid‐19. 12
4.2.6. Gingival changes
Gingival changes such as generalized erythematous and edematous gingivae, gingivo‐paradontal bleeding, necrotic interdental papillae and desquamative gingivitis are reported in the literature. 10 , 11 , 12 They are reported in critically ill patients with neglected oral hygiene. In a Covid‐19 suspected patient symptoms disappeared within 10 days of antibiotics and topical antiseptic mouthwash usage.
4.3. Dry mouth
Dry mouth is also reported in association with Covid‐19 positive patients. 13 , 41 , 43 In a study, 16 patients reported dry mouth along with other symptoms (PCR positive for Covid‐19). 43 This number reduced to 1 when PCR for the disease became negative. In another cross‐sectional study, 72 patients with Covid‐19 reported dry mouth. 41
4.4. Other manifestations
Symptoms such as halitosis, tongue and masticatory muscle pain and swelling, geographical tongue, hyperplasia of papilla associated with taste changes and macroglossia are also reported along with fatigue and major symptoms of Covid‐19 in few case reports. 11 , 31 , 43
5. CONCLUSION
This paper reports various oral manifestations associated with Covid‐19 confirmed and suspected patients. Gustatory impairment along with olfactory changes is now listed as a symptom of Covid‐19 by the WHO. Covid‐19 patients may present with ulcerative, erosive, vesicobullous and plaque‐like oral lesions. Further research is needed to confirm a link between reported mucosal lesions and Covid‐19, as these lesions may be the first sign of the disease or secondary to medications, reduced immunity, vascular compromise, localized or generalized inflammation and neglected oral hygiene. Dental professionals should be aware of oral manifestations, predisposing factors and underlying mechanisms while examining and before initiating any treatment in patients.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
AUTHOR CONTRIBUTION STATEMENT
Huma Farid presented the idea, conducted literature search and designed the first draft.
Madiha Khan and Shizrah Jamal conducted the literature search (independent screening and selection of publications).
Robia Ghafoor provided advice to improve the manuscript.
All authors have read and approved the submitted version.
ACKNOWLEDGEMENT
We are thankful to Dr. Muhammad Saad Shinwari for his support and expert opinion while preparing the final version of the manuscript.
Farid H, Khan M, Jamal S, Ghafoor R. Oral manifestations of Covid‐19‐A literature review. Rev Med Virol. 2022;32(1):e2248. 10.1002/rmv.2248
DATA AVAILABILITY STATEMENT
This is a narrative review and data sharing is not applicable to this article as no new data was created in this study. The analyzed data (studies included in the review along with variable of interest are presented in the Table 1 whereas literature search flow chart in presented in Figure 1).
REFERENCES
- 1. Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265‐269. 10.1038/s41586-020-2008-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Gorbalenya AE, Baker SC, Baric RS, et al. Coronaviridae study group of the International Committee on Taxonomy of Viruses. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5:536–544. 10.1038/s41564-020-0695-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Gorbalenya AE, Baker SC, Baric RS, et al. Severe Acute Respiratory Syndrome‐related Coronavirus: The Species And its Viruses ‐ A Statement of the Coronavirus Study Group. Biorxiv (Cold Spring Harb Lab). Published online. 2020;1‐15. 10.1101/2020.02.07.937862 [DOI] [Google Scholar]
- 4. Maier HJ, Bickerton E, Britton P, eds. Coronaviruses: Methods and Protocols (1282). 2015;1‐282. 10.1007/978-1-4939-2438-7 [DOI] [PubMed] [Google Scholar]
- 5. Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus (2019‐nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill. 2020;25(5):1‐6. 10.2807/1560-7917.ES.2020.25.5.2000062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Jiang F, Deng L, Zhang L, Cai Y, Cheung CW, Xia Z. Review of the clinical characteristics of coronavirus disease 2019 (COVID‐19). J Gen Intern Med. 2020;35(5):1545‐1549. 10.1007/s11606-020-05762-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bodard C, Gaëlle A, Deneuve S, Desoutter A. Oral manifestation of Covid‐19 as an inaugural symptom? J Oral Med Oral Surg. 2020;26(2):18. 10.1051/mbcb/2020011 [DOI] [Google Scholar]
- 8. Marzano AV, Cassano N, Genovese G, Moltrasio C, Vena GA. Cutaneous manifestations in patients with COVID‐19: a preliminary review of an emerging issue. Br J Dermatol. 2020;183:431‐442. 10.1111/bjd.19264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Gautier JF, Ravussin Y. A new symptom of COVID‐19: loss of Taste and smell. Obesity. 2020;28(5):848. 10.1002/oby.22809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Carreras‐Presas CM, Sánchez JA, López‐Sánchez AF, Jané‐Salas E, Somacarrera Pérez ML. Oral vesiculobullous lesions associated with SARS‐CoV‐2 infection. Oral Dis. 2020;(April):1‐3. 10.1111/odi.13382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Patel J, Woolley J. Necrotizing periodontal disease: oral manifestation of COVID‐19. Oral Dis. 2020;27:768‐769. 10.1111/odi.13462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Favia G, Tempesta A, Barile G, et al. Covid‐19 symptomatic patients with oral lesions: clinical and histopathological study on 123 cases of the university hospital policlinic of bari with a purpose of a new classification. J Clin Med. 2021;10(4):757. 10.3390/jcm10040757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Zarch RE. COVID‐19 from the perspective of dentists : a case report and brief review of more than 170 cases. Dermatol Ther. 2021;34:1‐6:e14717. 10.1111/dth.14717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Riad A, Kassem I, Hockova B, Badrah M, Klugar M. Tongue ulcers associated with SARS‐CoV‐2 infection: a case series. Oral Dis. 2020;00(August):1‐3. 10.1111/odi.13635 [DOI] [PubMed] [Google Scholar]
- 15. Tong JY, Wong A, Zhu D, Fastenberg JH, Tham T. The prevalence of olfactory and gustatory dysfunction in COVID‐19 patients: a systematic review and meta‐analysis. Otolaryngol Head Neck Surg. 2020;163(1):3‐11. 10.1177/0194599820926473 [DOI] [PubMed] [Google Scholar]
- 16. Hjelmesæth J, Skaare D. Loss of smell or taste as the only symptom of COVID‐19. Tidsskr Nor Laegeforen. 2020;140(7). 10.4045/tidsskr.20.0287 [DOI] [PubMed] [Google Scholar]
- 17. Santos JAdos, Normando AGC, da Silva RLC, et al. Oral mucosal lesions in a COVID‐19 patient: new signs or secondary manifestations? Int J Infect Dis. Published online. 2020. 10.1016/j.ijid.2020.06.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019‐nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12(1):1‐5. 10.1038/s41368-020-0074-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Lozada‐Nur F, Chainani‐Wu N, Fortuna G, Sroussi H. Dysgeusia in COVID‐19: possible mechanisms and implications. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130(3):344‐346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Mahmoud MM, Abuohashish HM, Khairy DA, Bugshan AS, Khan AM, Moothedath MM. Pathogenesis of dysgeusia in COVID‐19 patients: a scoping review. Eur Rev Med Pharmacol Sci. 2021;25(2):1114‐1134. 10.26355/eurrev_202101_24683 [DOI] [PubMed] [Google Scholar]
- 21. Malaty J, Malaty IAC. Smell and taste disorders in primary care. Am Fam Physician. 2013;88(12):852‐859. [PubMed] [Google Scholar]
- 22. Kaye R, Chang CWD, Kazahaya K, Brereton J, Denneny JC. COVID‐19 anosmia reporting tool: initial findings. Otolaryngol Head Neck Surg. 2020;163(1):132‐134. 10.1177/0194599820922992 [DOI] [PubMed] [Google Scholar]
- 23. Vinayachandran D, Balasubramanian S. Is gustatory impairment the first report of an oral manifestation in COVID‐19? Oral Dis. 2020;27(April):748‐749. 10.1111/odi.13371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Giacomelli A, Pezzati L, Conti F, et al. Self‐reported olfactory and Taste disorders in patients with severe acute respiratory coronavirus 2 infection: a cross‐sectional study. Clin Infect Dis. 2020;71:889‐890.ciaa330. 10.1093/cid/ciaa330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Ambaldhage V, Puttabuddi J, Nunsavath P, Tummuru Y. Taste disorders: a review. J Indian Acad Oral Med Radiol. 2014;26(1):69‐76. 10.4103/0972-1363.141864 [DOI] [Google Scholar]
- 26.American Academy of Otolaryngology ‐ Head and Neck Surgery. 2020. Anosmia, Hyposmia, and Dysgeusia Symptoms of Coronavirus Disease. https://www.entnet.org/content/aao-hns-anosmia-hyposmia-and-dysgeusia-symptoms-coronavirus-disease [Google Scholar]
- 27. Center for Disease Control and Prevention . Symptoms of Coronavirus. 2020. https://www.cdc.gov/coronavirus/2019‐ncov/symptoms‐testing/symptoms.html. Accessed July 19, 2020. [Google Scholar]
- 28. World Health Organization . Coronavirus Disease (COVID 19) Pandemic. 2020. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019. Accessed July 19, 2020. [Google Scholar]
- 29. Jimenez‐Cauhe J, Ortega‐Quijano D, Carretero‐Barrio I, et al. Erythema multiforme‐like eruption in patients with COVID‐19 infection: clinical and histological findings. Clin Exp Dermatol. Published online. 2020;45(7):0‐2. 10.1111/ced.14281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. da Fonseca Orcina B , Vilhena FV, Cardoso de Oliveira R. A Phthalocyanine Derivate Mouthwash to Gargling/Rinsing as an Option to Reduce Clinical Symptoms of COVID‐19. Case Series. Clin Cosmet Investig Dent. 2021;13:47-50. 10.2147/CCIDE.S295423. Accessed Feb 18, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hockov B, Riad A, Valky J, et al. Oral Complications of ICU Patients with COVID‐19 : Case‐Series and Review of Two Hundred Ten Cases. J Clin Med. 2021;10(4):581. 10.3390/jcm10040581. Accessed Feb 4, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Fidan V, Koyuncu H, Akin O. Oral lesions in Covid 19 positive patients. Am J Otolaryngol Neck Med Surg. 2020;42(January):2020‐2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Ansari R, Gheitani M, Heidari F, Heidari F. Oral cavity lesions as a manifestation of the novel virus (COVID‐19). Oral Dis. 2021;27:771‐772. Epub ahead of print. 10.1111/odi.13465 [DOI] [PubMed] [Google Scholar]
- 34. Halboub E, Al‐Maweri SA, Alanazi RH, Qaid NM, Abdulrab S. Orofacial manifestations of COVID‐19: a brief review of the published literature. Braz Oral Res. 2020;34:1‐10. 10.1590/1807-3107bor-2020.vol34.0124 [DOI] [PubMed] [Google Scholar]
- 35. La Rosa GRM, Libra M, De Pasquale R, Ferlito S, Pedullà E. Association of viral infections with oral cavity lesions: Role of SARS‐CoV‐2 infection. Front Med. 2021;7(January):1‐8. 10.3389/fmed.2020.571214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Vieira AR. Oral manifestations in coronavirus disease 2019 (COVID‐19). Oral Dis. 2020;27:770. 10.1111/odi.13463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Al‐Khatib A. Oral manifestations in COVID‐19 patients. Oral Dis. 2020;27(3):779‐780. 10.1111/odi.13477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Ciccarese G, Drago F, Boatti M, Porro A, Muzic SI, Parodi A. Oral erosions and petechiae during SARS‐CoV‐2 infection. J Med Virol. 2021;93(1):129‐132. 10.1002/jmv.26221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Casas CG, Català A, Hernández GC, et al. Classification of the cutaneous manifestations of COVID‐19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol. 2020;183(1):71‐77. 10.1111/bjd.19163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Wollina U, Karadağ AS, Rowland‐Payne C, Chiriac A, Lotti T. Cutaneous signs in COVID ‐19 patients: a review. Dermatol Ther. 2020;33(May). 10.1111/dth.13549 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Biadsee A, Biadsee A, Kassem F, Dagan O, Masarwa S, Ormianer Z. Olfactory and oral manifestations of COVID‐19: sex‐related symptoms‐A potential pathway to early diagnosis. Otolaryngol Head Neck Surg. 2020;163:722‐728.Published online. 10.1177/0194599820934380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Hedou M, Carsuzaa F, Chary E, Hainaut E, Cazenave‐Roblot F, Masson Regnault M. Comment on 'Cutaneous manifestations in COVID‐19: a first perspective' by Recalcati S. J Eur Acad Dermatol Venereol. 2020;34:0‐2. 10.1111/jdv.16519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Freni F, Meduri A, Gazia F, et al. Symptomatology in head and neck district in coronavirus disease (COVID‐19): a possible neuroinvasive action of SARS‐CoV‐2. Am J Otolaryngology. 2020;41(5):102612. 10.1016/j.amjoto.2020.102612 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Lorenzo Villalba N, Maouche Y, Alonso Ortiz MB, et al. Anosmia and dysgeusia in the absence of other respiratory disease: should COVID‐19 infection be considered? No Title. Eur J Case Reports Intern Med. 2020;7(4). 10.12890/2020_001641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Ansari R, Gheitani M, Heidari F, Heidari F. Oral cavity lesions as a manifestation of the novel virus (COVID‐19). Oral Dis. 2020;27:771‐772. 10.1111/odi.13465 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This is a narrative review and data sharing is not applicable to this article as no new data was created in this study. The analyzed data (studies included in the review along with variable of interest are presented in the Table 1 whereas literature search flow chart in presented in Figure 1).