

Abstract
Background:
Studies examining gender-based differences in outcomes of out-of-hospital cardiac arrest patients have demonstrated that despite a higher likelihood of return of spontaneous circulation, women do not have higher survival.
Methods:
Patients successfully resuscitated from out-of-hospital cardiac arrest enrolled in the Continuous Chest Compression trial were included. Hierarchical multivariable logistic regression models were constructed to evaluate the association between gender and survival after adjustment for age, gender, cardiac arrest rhythm, witnessed status, bystander cardiopulmonary resuscitation, episode location, epinephrine dose, emergency medical services response time and duration of resuscitation. Do Not Resuscitate (DNR) and withdrawal of life-sustaining therapy (WLST) order status were used to assess whether differences in post resuscitation outcomes were modified by baseline prognosis. The analysis was replicated among Amiodarone, Lidocaine, or Placebo Cardiac Arrest trial participants.
Results:
Among 4,875 successfully resuscitated patients, 1,825 (37.4%) were women and 3,050 (62.6%) were men. Women were older (67.5 vs. 65.3 years), received less bystander cardiopulmonary resuscitation (49.1% vs. 54.9%), and had a lower proportion of cardiac arrests that were witnessed (55.1% vs. 64.5%) or had shockable rhythm (24.3% vs. 44.6%, p<0.001 for all). A significantly higher proportion of women received DNR orders (35.7% vs. 32.1%, p=0.009) and had WLST (32.8% vs. 29.8%, p=0.03). Discharge survival was significantly lower in women (22.5% vs. 36.3%, p<0.001, adjusted odds ratio [OR] 0.78, 95% confidence interval [C.I.] 0.66 – 0.93, p=0.005). The association between gender and discharge survival was modified by DNR and WLST order status such that women had significantly reduced discharge survival among patients who were not made DNR (31.3% vs. 49.9%, p=0.005, adjusted OR 0.74, 95% C.I. 0.60 – 0.91) or did not have WLST (32.3% vs. 50.7%, p=0.002, adjusted OR 0.73, 95% C.I. 0.60 – 0.89). In contrast, no gender difference in survival was noted among patients receiving a DNR order (6.7% vs. 7.4%, p=0.90) or had WLST (2.8% vs. 2.4%, p=0.93). Consistent patterns of association between gender and post-resuscitation outcomes were observed in the secondary cohort.
Conclusions:
Among resuscitated out-of-hospital cardiac arrest patients, discharge to survival was significantly lower in women compared with men especially among patients considered to have a favorable prognosis.
Keywords: Out-of-hospital cardiac arrest, gender differences, outcomes research
Introduction
There are over 350,000 out-of-hospital cardiac arrests annually in the United States.1 Studies examining gender-based differences in outcomes after out-of-hospital cardiac arrest have consistently demonstrated that women have more poor prognostic factors related to cardiac arrest compared with men. They are older, less frequently experience cardiac arrest that is witnessed, in a public location, or have an initial shockable rhythm.2, 3 Additionally, women receive sub-optimal resuscitation care with less likelihood of receiving bystander cardiopulmonary resuscitation (CPR) compared with men affecting their discharge survival and survival with good neurological function.4 Despite this, women have a higher likelihood of return of spontaneous circulation (ROSC) compared with men after accounting for baseline characteristics.3, 5, 6 Thus, women might be expected to have higher survival since ROSC is an intermediary to surviving to hospital discharge. However, most studies have not observed increased survival to hospital discharge for women.3, 5, 6
To better understand this discordance between ROSC and survival to discharge, we evaluated gender differences in outcomes in patients successfully resuscitated from out-of-hospital cardiac arrest, using data from two large, multicenter, randomized trials.7, 8 Both trials contain robust data on important cardiac arrest variables required for risk assessment and information regarding in-hospital procedures. They also captured valuable data on the use of Do Not Resuscitate (DNR) and withdrawal of life-sustaining therapy (WLST) orders. This information is relevant since prior studies have demonstrated across multiple acute care settings e.g. sepsis, heart failure and after in-hospital cardiac arrest that women tend to receive DNR orders earlier and more frequently compared with men9–11 and receiving a DNR order or having WLST is associated with worse outcomes.12–14 Additionally, the absence of a DNR or WLST order, after excluding patient preferences would to a certain degree reflect a favorable prognosis as perceived by the treatment team allowing for a more robust comparison in outcomes among resuscitated men and women taking into account unmeasured factors that better capture the severity of illness.
Methods
Data Source
The (CCC) trial and Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest (ALPS) trial datasets are publicly available and were obtained from the National Institute of Health’s Biologic Specimen and Data Repository Information Coordinating Center (https://biolincc.nhlbi.nih.gov/home/). Both clinical trials were conducted by the Resuscitation Outcomes Consortium network across 10 major sites within the United States and Canada and completed patient enrollment in May 2015 and October 2015 respectively. The detailed study design, baseline characteristics, and trial results have been previously reported.7, 8
Study Cohorts
We constructed two study cohorts: Primary study cohort consisting of patients successfully resuscitated from the CCC trial dataset, and a secondary cohort consisting of resuscitated patients from the ALPS dataset. Figure 1 demonstrates the primary study cohort derivation flow diagram: The Continuous Chest Compression trial enrolled 26,148 adults with non–trauma-related out-of-hospital cardiac arrest who received chest compressions performed by emergency medical services (EMS) providers. We excluded patients with missing data on gender, age, initial rhythm, witnessed status, application of bystander cardiopulmonary resuscitation, location of arrest, EMS response time, and duration of resuscitation attempt. To identify co-enrolled patients in the two de-identified data sets we indirectly matched the patients by age, gender, EMS response time and duration of resuscitation attempt. Given the smaller size of the ALPS trial used to construct the secondary cohort, patients matching on these variables were excluded from the primary study cohort and counted towards the secondary cohort to allow for adequate sample size. Finally, we restricted our cohort to successfully resuscitated patients. The final primary study cohort consisted of 4,875 unique patients.
Figure 1. Derivation of primary study cohort.
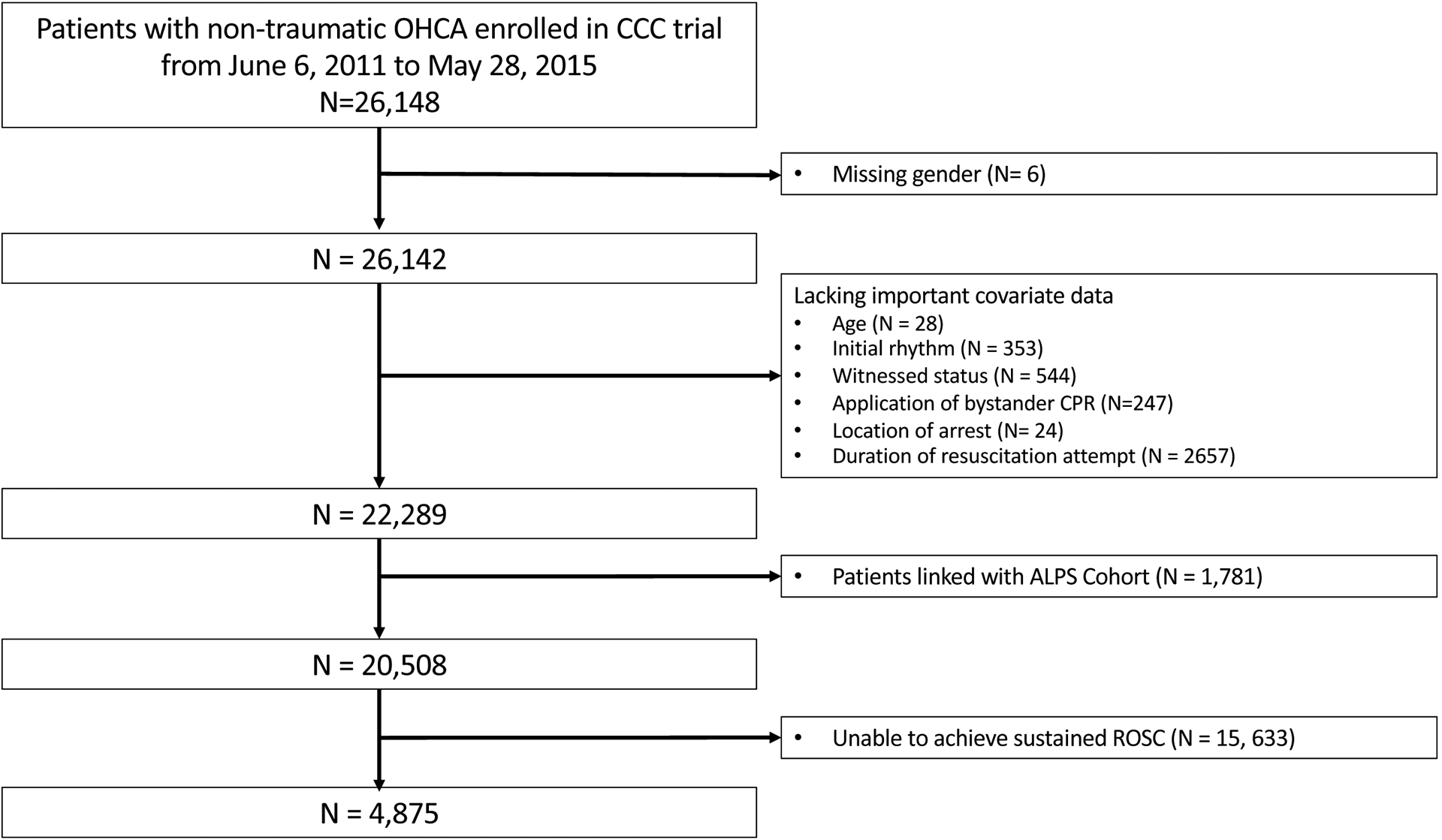
OHCA: Out-of-hospital cardiac arrest; CCC: Continuous Chest Compression; ALPS: Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest
The secondary cohort consisting of ALPS trial participants was constructed using a similar approach (Figure I in the Supplement). The study received an exemption from University of Texas at Southwestern IRB as it did not involve human research.
Study definitions
Baseline patient, event characteristics and outcomes were abstracted based on standardized Utstein definitions.15 To capture the data point of man vs woman or male vs female in this data set, paramedics made judgements based on socially constructed and enacted roles as well as behaviors that occur in a clinical and cultural context at the public or private scene of the cardiac arrest. They used not only secondary sex characteristics but also the language used by bystanders and family members to identify the individual. Additionally, the data point was further validated by the prehospital data guardian who reviewed the source documents for language such as he or she or male patient or female patient. Since there was no biological confirmation of sex and the data was captured retrospectively based on judgement and as such gender was felt to be the most appropriate term within the context of our study. Initial cardiac arrest rhythm was considered to be shockable if ventricular tachycardia, ventricular fibrillation or automated external defibrillator advised “shockable” was observed and as non-shockable if asystole, pulseless electrical activity or automated external defibrillator advised “no-shock” was observed.7, 8 EMS response time was defined as the interval from initial 9-1-1 call to first vehicle arrival on scene.7, 8 Duration of resuscitation attempt was defined as the time interval from initiation of emergency medical provider chest compressions to one of the following two end points: 1) time of ROSC for those with ROSC in the field and 2) time of termination of resuscitation or time of hospital arrival with ongoing resuscitation for those without ROSC in the field. Successful resuscitation was defined as presence of a pulse at hospital arrival. The dataset includes information on whether there was a DNR order or if the patient had withdrawal of life-sustaining therapy. Finally, we calculated the Cardiac Arrest Hospital Prognosis Score (CAHP) which predicts unfavorable outcome among resuscitated patients from out-of-hospital cardiac arrest.16
Outcomes
The primary study outcome was survival to hospital discharge. We also examined rate of survival with favorable neurological function at discharge; defined as a Modified Rankin score ≤3. We also compared DNR order rates, WLST rates, and rates of guideline-recommended procedures such as targeted temperature management (TTM) and coronary angiography (CAG).
Statistical Analysis
Baseline characteristics by gender were compared using chi-square tests for categorical variables and Student’s t-test or Wilcoxon-Mann-Whitney test for continuous variables.
To examine the relationship between gender and survival to hospital discharge, we constructed a hierarchical logistic regression model using data from the primary study cohort. In this model we included trial randomization cluster as a random effect, and patient level covariates as fixed effects. These included covariates that have previously been shown to be associated with survival of resuscitated patients such as age, gender, initial cardiac arrest rhythm (shockable or non-shockable), witnessed arrest status, bystander CPR before EMS arrival, episode location (public or not), epinephrine dose, EMS response time, and duration of the resuscitation attempt.17–19 Given prior data demonstrating that age was a modifying factor on survival,3 we tested for interaction between gender and age for survival to hospital discharge and if interaction was present, stratified analyses were performed. Separate hierarchical logistic regression models were constructed for survival with favorable neurological function.
We performed a number of explanatory analyses to check the robustness of our findings. First, to examine patterns of care, we examined rates of TTM and CAG among select, eligible subsets of resuscitated patients that included patients with ST segment elevation, those who had an initial shockable rhythm, and patients who were not made DNR or did not have life-sustaining therapy withdrawn. Second, since DNR order status and WLST are reflective of perceived patient prognosis, we stratified our analyses based on these variables. Third, given the prognostic importance of ST elevation on subsequent rates of CAG as well as survival after cardiac arrest,20 we performed stratified analysis based on baseline ST elevation status. Fourth, we examined the interaction between CAHP score and gender using logistic regression and restricted cubic splines with further adjustment for witnessed cardiac arrest and bystander chest compressions.16 Finally, we replicated our primary analysis in the secondary cohort.
For the primary analysis, no patient data was imputed for missingness since patients with missing covariate data were excluded during cohort construction. Missing data regarding the variable arterial pH required for calculation of CAHP score was imputed using random forest imputation.21 All analyses were performed using SAS University edition 3.8 (SAS Institute Inc., Cary, North Carolina) and R version 3.6.0. Statistical tests were 2-sided, and a p-value below 0.05 was considered statistically significant.
Results
Patient characteristics
Of 26,148 patients enrolled in the CCC trial, 20,508 unique patients remained after excluding patients with missing data and patients co-enrolled in the Amiodarone, Lidocaine, and Placebo trial dataset (Table I in the Supplement). Of the 4,875 successfully resuscitated patients in the primary study cohort, 1,825 (37.4%) were women and 3,050 (62.6%) were men. Overall, women were older, less frequently received bystander CPR, and had a lower proportion of witnessed arrests, arrests in public locations, or arrests with an initial shockable rhythm (Table 1). The EMS response time, epinephrine dose and amount of fluid administered during resuscitation were similar in men and women. Women had a marginally longer duration of resuscitation (14.6 vs. 13.5 minutes, p<0.001) compared with men. While rates of electrocardiogram performed were similar (91.6% for women; 93.4% for men, p=0.03), ST segment elevation was less frequent in women (19.4% for women compared with 32.4% for men, p<0.001). The secondary cohort baseline rates are similar (Table II in the Supplement).
Table 1.
Unadjusted baseline characteristics and rates of in-hospital procedures among resuscitated patients in primary study cohort
| Characteristics* | Women (N= 1,825) |
Men (N= 3,050) |
P-Value |
|---|---|---|---|
| Age, years | 67.5 (16.9) | 65.3 (15.7) | <0.001 |
| Bystander cardiopulmonary resuscitation, % | 49.1 | 54.9 | <0.001 |
| Witnessed, % | 55.1 | 64.5 | <0.001 |
| Initial shockable rhythm, % | 24.3 | 44.6 | <0.001 |
| Public location, % | 10.8 | 26.6 | <0.001 |
| EMS response time, minutes | 5.8 (2.5) | 5.7 (2.5) | 0.22 |
| Amount of fluids administered, mL | 549 (411.6) | 577 (465.4) | 0.33 |
| Epinephrine dose, mg | 2.7 (1.6) | 2.8 (1.8) | 0.39 |
| Duration of resuscitation, minutes | 14.6 (8.3) | 13.5 (8.6) | <0.001 |
| 12-lead electrocardiogram | 91.6 | 93.4 | 0.03 |
| ST-Elevation present, % | 19.4 | 32.4 | <0.001 |
| In-hospital procedures | |||
| Targeted temperature management, % | 35.1 | 44.6 | <0.001 |
| Coronary angiography, % | 14.3 | 30.2 | <0.001 |
All continuous measures are reported as means with standard deviations, and categorical measures as percentages.
The unadjusted rates of DNR order placement (35.7% vs 32.1%, p=0.009) as well as WLST (32.8% vs. 29.8%, p=0.03) were higher in women compared with men (Table 2). Similarly, the unadjusted rates of receiving a DNR order or having WLST within 3 days of admission were higher in women (75.0% vs. 70.4%, p=0.04 for DNR orders; 65.5% vs. 59.0, p=0.01 for WLST). Results were similar in the secondary study cohort (Table III in the Supplement).
Table 2.
Unadjusted rates of withdrawal of life-sustaining therapy and Do Not Resuscitate orders among resuscitated patients in primary study cohort
| Clinical Characteristics | Women (N= 1,825) |
Men (N= 3,050) |
P-Value |
|---|---|---|---|
| DNR order received (N=1,630), (%) | 652/1,825 (35.7) |
978/3,050 (32.1) |
0.009 |
| DNR order received within 3 days of admission (N=1,615), (%)* | 487/649 (75.0) |
680/966 (70.4) |
0.04 |
| Withdrawal of life-sustaining therapy (N=1,508), (%) | 599/1,825 (32.8) |
909/3,050 (29.8) |
0.03 |
| Withdrawal of life-sustaining therapy within 3 days of admission (N=1,489), (%)* | 390/595 (65.5) |
528/894 (59.0) |
0.01 |
Among patients who were made DNR or had life-sustaining care withdrawn respectively
Clinical Outcomes
Primary Study Cohort
In the primary study cohort, the unadjusted rate of survival to hospital discharge was lower in women compared with men (22.5% vs. 36.3%, p<0.001), a finding that persisted after accounting for age, gender, initial cardiac arrest rhythm, witnessed status, bystander CPR, episode location, response time and duration of the resuscitation attempt (OR for women 0.78, 95% C.I. 0.66 – 0.93, p=0.005). Similarly, unadjusted rate of survival with favorable neurological function was significantly lower among women compared with men (17.6% vs. 31.0%, p<0.001) that persisted on multivariable adjustment (OR for women 0.79, 95% C.I. 0.65 – 0.95, p=0.01). The relationship between gender and discharge survival was not modified by age (pinteraction =0.94).
The use of in-hospital procedures was different among men vs. women. The unadjusted rates of guideline-directed therapy such as TTM and CAG were significantly lower in women compared with men (Table 1). Rates of angiography were significantly lower in women regardless of ST segment elevation on the initial electrocardiogram (Table 3). Additionally, women continued to receive CAG less frequently compared with men when the primary cohort was limited to patients with initial shockable rhythm who were not made DNR or did not have life-sustaining therapy withdrawn and met the criteria for guideline directed CAG (Table 3). With regards to TTM, among patients with initial shockable rhythm, women had numerically lower proportion of TTM utilization not meeting statistical significance (54.5% vs. 58.9%, P = 0.10). In contrast, among patients with initial non-shockable rhythm, the use of TTM was significantly lower in women (vs. men) post ROSC (28.9 vs. 33.1%, P = 0.01) (Table 3).
Table 3.
Rates of coronary angiography and targeted temperature management among select group of resuscitated patients in primary study cohort based on presence of ST elevation on electrocardiogram, initial rhythm, and Do Not Resuscitate or withdrawal of life-sustaining status
| Cohort | Women | Men | P-Value |
|---|---|---|---|
| Coronary angiography | |||
| ST elevation present (N= 1,331), (%) | 125/349 (35.8) |
573/982 (58.3) |
<0.001 |
| ST elevation absent (N= 3,346), (%) | 120/1,385 (8.6) |
317/1,961 (16.1) |
<0.001 |
| Shockable & DNR order not placed (N= 1,350), (%) | 139/305 (45.5) |
628/1,045 (60.1) |
<0.001 |
| Shockable & No WLST (N= 1,396), (%) | 139/322 (43.2) |
634/1,074 (59.0) |
<0.001 |
| ST elevation present & DNR order not placed (N= 931), (%) | 89/232 (38.3) |
443/699 (63.4) |
<0.001 |
| ST elevation present & No WLST (N= 961), (%) | 86/233 (36.9) |
453/728 (62.2) |
<0.001 |
| Targeted temperature management | |||
| Shockable rhythm (N= 1,803), (%) | 242/444 (54.5) |
801/1,359 (58.9) |
0.10 |
| Non-shockable rhythm (N= 3,072), (%) | 400/1,381 (28.9) |
561/1,691 (33.1) |
0.01 |
We observed that among patients who were assigned a DNR order or had WLST there were no gender related differences in survival (Figure 2). In contrast, among patients who did not have WLST nor were assigned DNR status, women had significantly lower survival to discharge (Figure 2). Similar patterns of results for survival to discharge were observed after stratifying for baseline ST segment status. In patients with ST elevation on baseline electrocardiogram, women had significantly lower survival to discharge compared with men (OR for women 0.54, 95% C.I. 0.40 – 0.74, p<0.001). There were no significant differences in survival in men versus women with no ST elevation (OR for women 0.88, 95% C.I. 0.72 – 1.08, p=0.22). Finally, in restricted cubic spline analysis, there was a significant interaction between CAHP score and gender with association with survival to hospital discharge (pinteraction = 0.001, Figure 3).
Figure 2. Association of women with survival to hospital discharge stratified by Do Not Resuscitate order status and Withdrawal of life-sustaining therapy.

*Hierarchical multivariable logistic regression modeling was performed after adjustment for age, witnessed status, initial presenting rhythm, public location, bystander cardiopulmonary resuscitation, resuscitation duration and response time as covariates
Figure 3. Association of men vs women with survival to hospital discharge across Cardiac Arrest Hospital Prognosis scores.
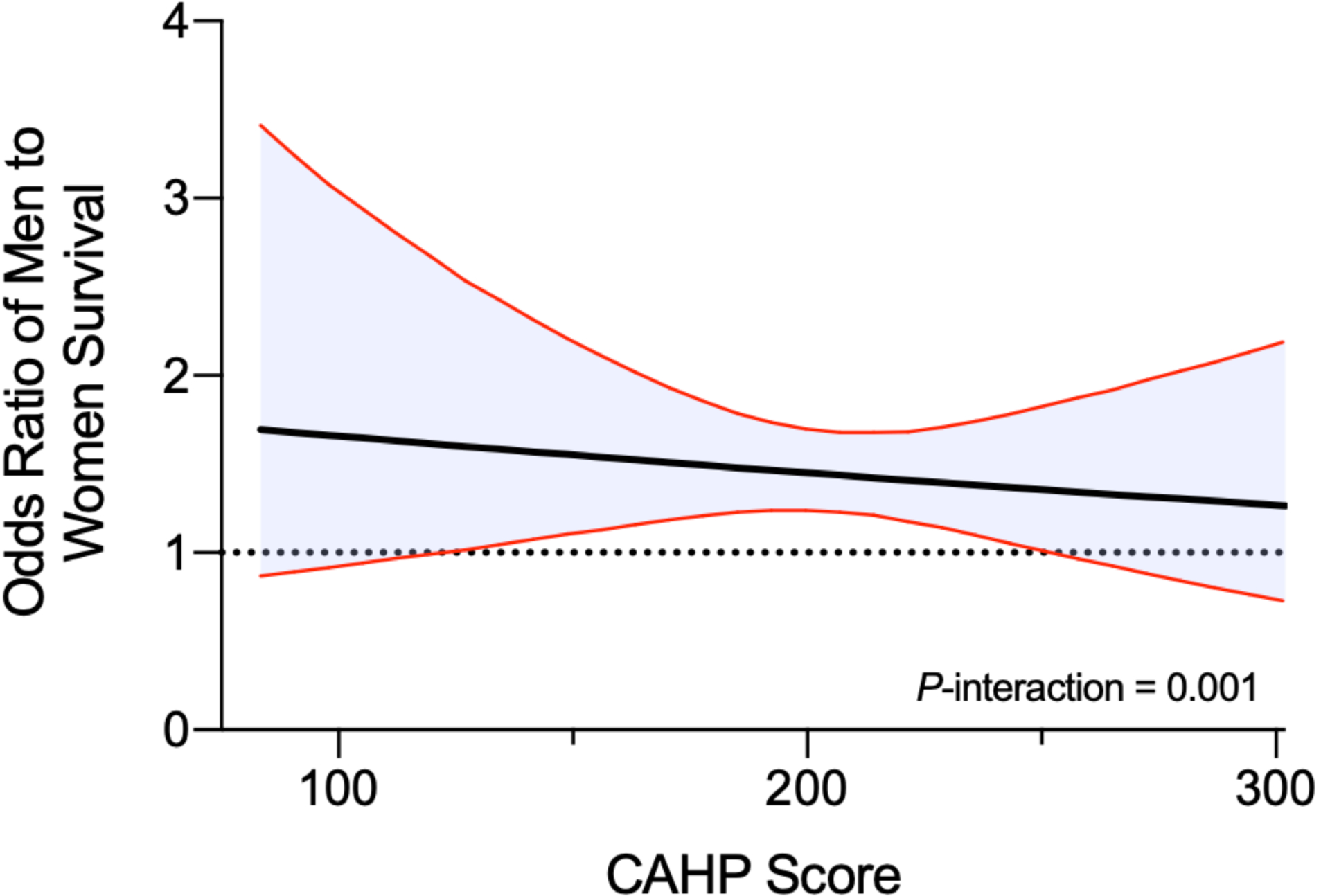
Restricted cubic spline showing adjusted association between Cardiac Arrest Hospital Prognosis (CAHP) score and odds of men to women survival to hospital discharge. The shaded area shows the 95% confidence interval for the odds ratio point estimate. The model was adjusted for CAHP score, gender, witnessed cardiac arrest, and bystander CPR
Comparison with the secondary study cohort
Our replication of primary analysis in the 1,307 resuscitated patients enrolled in the ALPS trial yielded similar results. Unadjusted survival to discharge was lower among women compared with men (41% vs 50%, p=0.005). After multivariable adjustment, women continued to have significantly reduced likelihood of survival to hospital discharge compared with men (OR for women 0.72, 95% C.I. 0.54 – 0.97, p=0.03). Similarly, the rate of discharge survival with good neurological function was lower among women compared with men (29.6% vs. 38.9%, p=0.002), that persisted after multivariable adjustment (OR for women 0.67, 95% C.I. 0.49 – 0.92, p=0.03).
Discussion
In a large, contemporary cohort of successfully resuscitated cardiac arrest patients (shockable and non-shockable initial rhythms), we demonstrate that women have significantly decreased likelihood of survival after accounting for baseline differences, compared with men. These findings were replicated in a second cohort of cardiac arrest patients with refractory, shockable rhythms. Gender differences in survival appear to be primarily driven by differences in patients with favorable prognosis. Finally, we demonstrate that eligible women less frequently receive guideline-directed therapy such as coronary angiography and targeted temperature management compared with men.
Numerous studies have been published over the last decade regarding gender differences in cardiac arrest.2, 3, 5, 6, 22 Few studies have focused on outcomes of resuscitated patients or explored the impact of ICU decision making on outcomes.5, 23, 24 Blom et al. demonstrated worse outcomes for women after hospital admission5 without evaluating DNR or WLST order rates.5 Perman et al. demonstrated that women were made DNR more frequently and earlier compared to men.23 However, the lack of important variables such as application of bystander CPR and initial rhythm limits the generalizability of their results. Our study extends the findings of these studies. First, our study used a large, contemporary, North America wide data set, that improves generalizability. Second, we used robust risk adjusted multivariable models that included known predictive cardiac arrest event variables.17, 18 Third, we included information on whether a patient received DNR orders or had life-sustaining therapy withdrawn. We observed that there was no gender-based survival differences among resuscitated patients who were made DNR or had life-sustaining therapy withdrawn. In contrast, there were significant gender-based differences in survival among resuscitated patients that did not receive a DNR order nor had life-sustaining therapy withdrawn with women having a decreased likelihood of survival compared with men. This important observation highlights that gender-based differences in survival outcomes are to an extent driven by patients who were viewed to have a more favorable prognosis as they did not have life-sustaining treatment withdrawn. Finally, we observed consistent results on replicating our study analysis in a secondary cohort of patients from the ALPS trial. In contrast to our primary study cohort patients that largely experienced initial non-shockable rhythms, secondary study cohort patients predominantly experienced cardiac arrest with initial refractory, shockable rhythm and had significantly superior survival outcomes especially survival with good neurological function.8 This allowed us to confirm the robustness of our findings across the spectrum of cardiac arrest patients with varying prognosis.
In adjusted analysis, women (vs. men) were less likely to have survival to hospital discharge as well as survival with good neurological function after accounting for potential confounders in both primary and secondary study cohorts. The latter outcome is particularly relevant as survival with good neurological function represents a meaningful clinical outcome and has been associated with better quality of life, less burden on care givers, and lower resource utilization in the long-term.25
A third of our study population had DNR orders, or had life-sustaining treatment withdrawn, with an overwhelming majority experiencing these decisions within 72 hours of admission, highlighting the need for further investigation in the circumstances leading to early WLST compared with the recommended 72 hour window for neuroprognostication as well as an opportunity to improve post resuscitation outcomes.14, 26. A significantly higher proportion of women in our study were made DNR and had WLST within 3 days of admission. This appears to be consistent with prior studies by Perman et al. demonstrating increased rates of DNR order use among women after in-hospital and out-of-hospital cardiac arrest.11, 23 We speculate that this is due to a number of factors including differences in end-of-life preferences across gender27 and known provider level disparities in approaching goals of care discussions with men and women.28 Future qualitative studies examining these sorts of social factors and the broader contexts in which treatment decisions are made would help improve understanding of these differences.
Consistent with prior literature, we observed that rates of in-hospital procedures such as CAG and TTM were lower in women.2, 23, 29, 30 However, these prior studies were limited by small sample size,29 absence of cardiac arrest variables that affect outcomes,27, 30 and lack of important prognostic information such as application of DNR orders and WLST that might have affected the use of these in-hospital procedures.2 These differences persisted on examining CAG rates in select patients with presumed cardiac cause of arrest e.g., ST segment elevation or initial shockable rhythm highlighting the need to explore the surrounding contexts and mechanisms underlying the gender based differences in post resuscitation care. Similarly, women received TTM less frequently compared with men. This difference was more pronounced in the non-shockable group where the strength of recommendation for use of TTM is weaker and use is driven by provider clinical judgment.26
A novel finding in our study was that differences in survival in men and women occurred in patients who were expected to have more favorable outcomes i.e. those who were not made DNR or had life-sustaining therapy withdrawn or those with a lower CAHP Score. Finally, survival differences favoring men were also noted in patients with ST elevation compared with no ST elevation on their electrocardiogram further illustrating differences in outcomes among men and women contingent on baseline risk.
Our study has several limitations. First, we cannot exclude residual confounding related to unmeasured risk factors that led women to have decreased survival or decreased rates of post arrest related procedures. Second, we lacked information on patient’s race which has been shown to affect cardiac arrest outcomes.31 Third, we lacked patient level variables or comorbidities such as existing cardiovascular disease that could have influenced the classification of etiology as well as clinical outcomes. The reasons for this difference observed in survival could be a result of women having a different distribution of causes that are all lumped under “no obvious or presumed cardiac cause” in this dataset.32, 33 Finally, we lacked important information about the specific medical circumstances leading to placement of DNR orders or WLST e.g. if they were placed as a reflection of poor prognosis perceived by the treatment team or if they were placed after discovery of patient’s prior wishes.
Conclusions
In a large, contemporary cohort of patients with out-of-hospital cardiac arrest who were successfully resuscitated, we observed that women less frequently survive to hospital discharge despite higher likelihood of return of spontaneous circulation compared with men. This difference in survival is most evident among women who were expected to have a favorable prognosis. Additionally, women less frequently receive in-hospital procedures known to improve survival after cardiac arrest. Future studies focused on strategies to optimize compliance with post arrest guidelines after successful resuscitation are required to understand and improve gender-based differences in outcome.
Supplementary Material
Clinical Perspective.
What is new?
Among patients resuscitated from out-of-hospital cardiac arrest, women have lower likelihood of survival to hospital discharge and survival with good neurological function compared with men.
This difference in survival outcome is more pronounced among patients considered to have a favorable prognosis.
What are the clinical implications?
Our study demonstrates the existence of gender disparities in post resuscitation care and highlights the need for future qualitative studies focused on decision-making and care being provided in the post-resuscitation phase to narrow gender-based differences in cardiac arrest outcomes.
Non-standard Abbreviations and Acronyms
- CPR
cardiopulmonary resuscitation
- ROSC
Return of Spontaneous circulation
- DNR
Do Not Resuscitate
- WLST
Withdrawal of life-sustaining therapy
- CCC
Continuous Chest Compression
- ALPS
Amiodarone, Lidocaine, or Placebo
- EMS
Emergency medical services
- CAHP
Cardiac Arrest Hospital Prognosis Score
- TTM
Targeted temperature management
- CAG
Coronary angiography
Footnotes
Conflicts of Interests: None
References
- 1.Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. [DOI] [PubMed] [Google Scholar]
- 2.Karlsson V, Dankiewicz J, Nielsen N, Kern KB, Mooney MR, Riker RR, Rubertsson S, Seder DB, Stammet P, Sunde K et al. Association of gender to outcome after out-of-hospital cardiac arrest--a report from the International Cardiac Arrest Registry. Crit Care. 2015;19:182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Morrison LJ, Schmicker RH, Weisfeldt ML, Bigham BL, Berg RA, Topjian AA, Abramson BL, Atkins DL, Egan D, Sopko G et al. Effect of gender on outcome of out of hospital cardiac arrest in the Resuscitation Outcomes Consortium. Resuscitation. 2016;100:76–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blewer AL, McGovern SK, Schmicker RH, May S, Morrison LJ, Aufderheide TP, Daya M, Idris AH, Callaway CW, Kudenchuk PJ et al. Gender Disparities Among Adult Recipients of Bystander Cardiopulmonary Resuscitation in the Public. Circ Cardiovasc Qual Outcomes. 2018;11:e004710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Blom MT, Oving I, Berdowski J, van Valkengoed IGM, Bardai A and Tan HL. Women have lower chances than men to be resuscitated and survive out-of-hospital cardiac arrest. Eur Heart J. 2019; 40: 3824–3834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bray JE, Stub D, Bernard S and Smith K. Exploring gender differences and the “oestrogen effect” in an Australian out-of-hospital cardiac arrest population. Resuscitation. 2013;84:957–963. [DOI] [PubMed] [Google Scholar]
- 7.Nichol G, Leroux B, Wang H, Callaway CW, Sopko G, Weisfeldt M, Stiell I, Morrison LJ, Aufderheide TP, Cheskes S et al. Trial of Continuous or Interrupted Chest Compressions during CPR. N Engl J Med. 2015;373:2203–2214. [DOI] [PubMed] [Google Scholar]
- 8.Kudenchuk PJ, Brown SP, Daya M, Rea T, Nichol G, Morrison LJ, Leroux B, Vaillancourt C, Wittwer L, Callaway CW et al. Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2016;374:1711–1722. [DOI] [PubMed] [Google Scholar]
- 9.Chang DW and Brass EP. Patient and hospital-level characteristics associated with the use of do-not-resuscitate orders in patients hospitalized for sepsis. J Gen Intern Med. 2014;29:1256–1262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Phadke A and Heidenreich PA. Differences and Trends in DNR Among California Inpatients With Heart Failure. J Card Fail. 2016;22:312–315. [DOI] [PubMed] [Google Scholar]
- 11.Perman SM, Beaty BL, Daugherty SL, Havranek EP, Haukoos JS, Juarez-Colunga E, Bradley SM, Fendler TJ and Chan PS. Do Sex Differences Exist in the Establishment of “Do Not Attempt Resuscitation” Orders and Survival in Patients Successfully Resuscitated From In-Hospital Cardiac Arrest? J Am Heart Assoc. 2020;9:e014200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fendler TJ, Spertus JA, Kennedy KF, Chen LM, Perman SM and Chan PS. Alignment of Do-Not-Resuscitate Status With Patients’ Likelihood of Favorable Neurological Survival After In-Hospital Cardiac Arrest. JAMA. 2015;314:1264–1271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Richardson DK, Zive D, Daya M and Newgard CD. The impact of early do not resuscitate (DNR) orders on patient care and outcomes following resuscitation from out of hospital cardiac arrest. Resuscitation. 2013;84:483–487. [DOI] [PubMed] [Google Scholar]
- 14.Elmer J, Torres C, Aufderheide TP, Austin MA, Callaway CW, Golan E, Herren H, Jasti J, Kudenchuk PJ, Scales DC et al. Association of early withdrawal of life-sustaining therapy for perceived neurological prognosis with mortality after cardiac arrest. Resuscitation. 2016;102:127–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, Cassan P, Coovadia A, D’Este K, Finn J et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa). Resuscitation. 2004;63:233–249. [DOI] [PubMed] [Google Scholar]
- 16.Maupain C, Bougouin W, Lamhaut L, Deye N, Diehl JL, Geri G, Perier MC, Beganton F, Marijon E, Jouven X et al. The CAHP (Cardiac Arrest Hospital Prognosis) score: a tool for risk stratification after out-of-hospital cardiac arrest. Eur Heart J. 2016;37:3222–3228. [DOI] [PubMed] [Google Scholar]
- 17.Hallstrom AP, Ornato JP, Weisfeldt M, Travers A, Christenson J, McBurnie MA, Zalenski R, Becker LB, Schron EB and Proschan M. Public-access defibrillation and survival after out-of-hospital cardiac arrest. New Engl J Med. 2004;351:637–646. [DOI] [PubMed] [Google Scholar]
- 18.Hasselqvist-Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P, Ringh M, Jonsson M, Axelsson C, Lindqvist J et al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2015;372:2307–2315. [DOI] [PubMed] [Google Scholar]
- 19.Sasson C, Rogers MA, Dahl J and Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. [DOI] [PubMed] [Google Scholar]
- 20.Behnes M, Mashayekhi K, Weiss C, Nienaber C, Lang S, Reiser L, Bollow A, Taton G, Reichelt T, Ellguth D et al. Prognostic Impact of Acute Myocardial Infarction in Patients Presenting With Ventricular Tachyarrhythmias and Aborted Cardiac Arrest. J Am Heart Assoc. 2018;7:e010004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stekhoven DJ and Bühlmann P. MissForest--non-parametric missing value imputation for mixed-type data. Bioinformatics. 2012;28:112–118. [DOI] [PubMed] [Google Scholar]
- 22.Goodwin G, Picache D, Gaeto N, Louie BJ, Zeid T, Aung PP and Sahni S. Gender Disparities in Out-of-hospital Cardiac Arrests. Cureus. 2018;10:e3233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Perman SM, Siry BJ, Ginde AA, Grossestreuer AV, Abella BS, Daugherty SL and Havranek EP. Sex Differences in “Do Not Attempt Resuscitation” Orders After Out-of-Hospital Cardiac Arrest and the Relationship to Critical Hospital Interventions. Clin Ther. 2019;41:1029–1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Greenwood BN, Carnahan S and Huang L. Patient-physician gender concordance and increased mortality among female heart attack patients. Proc Natl Acad Sci U S A. 2018;115:8569–8574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Geocadin RG, Callaway CW, Fink EL, Golan E, Greer DM, Ko NU, Lang E, Licht DJ, Marino BS, McNair ND et al. Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement From the American Heart Association. Circulation. 2019;140:e517–e542. [DOI] [PubMed] [Google Scholar]
- 26.Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, Leary M, Meurer WJ, Peberdy MA, Thompson TM et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132:S465–S482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Skulason B, Hauksdottir A, Ahcic K and Helgason AR. Death talk: gender differences in talking about one’s own impending death. BMC palliative care. 2014;13:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Crosby MA, Cheng L, DeJesus AY, Travis EL and Rodriguez MA. Provider and Patient Gender Influence on Timing of Do-Not-Resuscitate Orders in Hospitalized Patients with Cancer. J Palliat Med. 2016;19:728–7233. [DOI] [PubMed] [Google Scholar]
- 29.Bosson N, Kaji AH, Fang A, Thomas JL, French WJ, Shavelle D and Niemann JT. Sex Differences in Survival From Out-of-Hospital Cardiac Arrest in the Era of Regionalized Systems and Advanced Post-Resuscitation Care. J Am Heart Assoc. 2016; 5: e004131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kim LK, Looser P, Swaminathan RV, Horowitz J, Friedman O, Shin JH, Minutello RM, Bergman G, Singh H, Wong SC et al. Sex-Based Disparities in Incidence, Treatment, and Outcomes of Cardiac Arrest in the United States, 2003–2012. J Am Heart Assoc. 2016; 5: e003704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Reinier K, Rusinaru C and Chugh SS. Race, ethnicity, and the risk of sudden death. Trends Cardiovasc Med. 2019;29:120–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Albert CM, McGovern BA, Newell JB and Ruskin JN. Sex differences in cardiac arrest survivors. Circulation. 1996;93:1170–1176. [DOI] [PubMed] [Google Scholar]
- 33.Haukilahti MAE, Holmstrom L, Vahatalo J, Kentta T, Tikkanen J, Pakanen L, Kortelainen ML, Perkiomaki J, Huikuri H, Myerburg RJ et al. Sudden Cardiac Death in Women. Circulation. 2019;139:1012–1021. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.