

Abstract
Justice-involved youth experience high rates of Adverse Childhood Experiences (ACEs), placing them in great need of behavioral health treatment and risk for continued justice involvement. Policy makers, government agencies, and professionals working with justice-involved youth have called for trauma-informed juvenile justice reform. Yet, there is currently no available review of the literature on ACEs and their impact on justice-involved youths’ psychological, legal and related (e.g., academic) outcomes to rigorously guide such reform efforts. The current systematic scoping review synthesizes existing literature related to the impact of ACEs on justice-involved youth and offers recommendations for data-driven intervention along the Sequential Intercept Model, which describes five different points of justice system contact (i.e., first arrest, court diversion, detention, community supervision) in which there is opportunity to intervene and improve youth behavioral health, legal and associated outcomes. Eight unique studies were included in 40 articles examining ACEs among justice-involved youth; 38% were longitudinal/prospective analyses and none were intervention studies. Studies included delinquency (e.g., recidivism; n=5), psychiatric (n=4), substance use (n=3), and other (n=2; e.g., academic, pregnancy) outcomes, documenting high prevalence of ACEs and significant associations between ACEs and a variety of outcomes. Implications for clinical services (e.g., targeting youth dysregulation and aggression), agency context (e.g., training police officers in trauma-responsive practices), and system-level changes (e.g., intervening at the time of first ACE documentation such as parent’s arrest) are discussed.
Keywords: adverse childhood experiences, child maltreatment, delinquency, juvenile justice, sequential intercept model
Editor’s note.
This article is part of a special issue, “Adverse Childhood Experiences (ACEs): Translation to Action,” published in the Xxxxxx 2021 issue of American Psychologist. Sharon G. Portwood and Michael J. Lawler served as editors of the special issue, with Michael C. Roberts as advisory editor.
Introduction
A plethora of research documents the link between adverse childhood experiences (ACEs) and health outcomes, including heart disease, alcoholism, drug use, depression, sexually transmitted diseases, and premature death among adults. Ten ACEs within three broad categories: abuse (physical, emotional, sexual), neglect (physical, emotional), and household dysfunction (caregiver substance abuse, caregiver mental illness, caregiver divorce/separation, caregiver incarceration, domestic violence) comprise the framework for characterizing and quantifying effects of childhood adversity across different settings and populations (Felitti et al., 1998; Hughes et al., 2017; Oral et al., 2016). Justice-involved youth report particularly high rates of ACEs (Baglivio et al., 2014), which place them in greater need of behavioral health intervention (Clements-Nolle & Waddington, 2019) and at greater risk for continued justice involvement (Fox, Perez, Cass, Baglivio, & Epps, 2015; Wolff & Baglivio, 2017).
Policy makers have begun recognizing the broad and profound impact of ACEs and responded by launching initiatives such as California’s new ACEs screening program for publicly-insured (i.e., Medi-Cal) youth. The U.S. Department of Justice has also called for trauma-informed juvenile justice system reform, yet there is little agreement on the specific trauma-informed practices and policies that should be implemented when a youth endorses exposure to ACEs or “screens positive” for ACEs (Branson, Baetz, Horwitz, & Hoagwood, 2017). In part, this is due to a lack of rigorous review of the empirical literature required to best inform data-driven approaches to intervention and lack of a coherent framework for applying data-driven recommendations. The current study addresses this gap by 1) synthesizing existing literature among justice-involved youth on the prevalence of ACEs and their impact on behavioral health, legal and associated (e.g., academic) outcomes and 2) offering data-driven recommendations for action along the Sequential Intercept Model (SIM) (Munetz & Griffin, 2006) and considering three primary domains of trauma-informed care for justice-involved youth: clinical services (e.g., screening and assessment, interventions), agency context (e.g., workforce development and support, promoting a safe agency environment), and system-level (e.g., system-level policies and procedures, cross-system collaboration) (Branson et al., 2017).
The Sequential Intercept Model
The SIM began as a conceptual framework to organize the discussion regarding overcriminalization of adults with behavioral health concerns and how to identify and divert these individuals to needed behavioral health services while holding them accountable for criminal behavior (Griffin, Munetz, Bonfire, & Kemp, 2013). Through collaborative discussions, policy experts from the Ohio Center of Excellence and the GAINS Center identified five original intercepts: Intercept 1: Law enforcement, emergency services; Intercept 2: Initial detention, initial court hearings; Intercept 3: Jails, collaborative/specialty courts, forensic evaluation/hospitalization; Intercept 4: Re-entry; and Intercept 5: Community corrections and supports (Munetz & Griffin, 2006). The horizontal graphic of the SIM in Figure 1 illustrates that movement through the system is linear and predictable. With growing recognition that a robust community-based behavioral health system will prevent justice involvement, Intercept 0: Hospital, Crisis, Respite, Peer and Community Services was added and refined (Abreu, Parker, Noether, Steadman, & Case, 2017). Grounded in the principle that community-based treatment is more effective and cost efficient, the goal is to divert individuals from further penetration into the justice system by providing community-based treatment alternatives (Heilbrun et al., 2012). As such, SIM Intercepts correspond to criminal justice decision junctures and are available intervention points to prevent further entrenchment in the justice system. The SIM’s use has expanded beyond adults with severe mental illness to other populations at increased risk for justice involvement, such as those with primary substance use disorders, women with a history of trauma, and young adults (Griffin et al., 2013).
Figure 1.
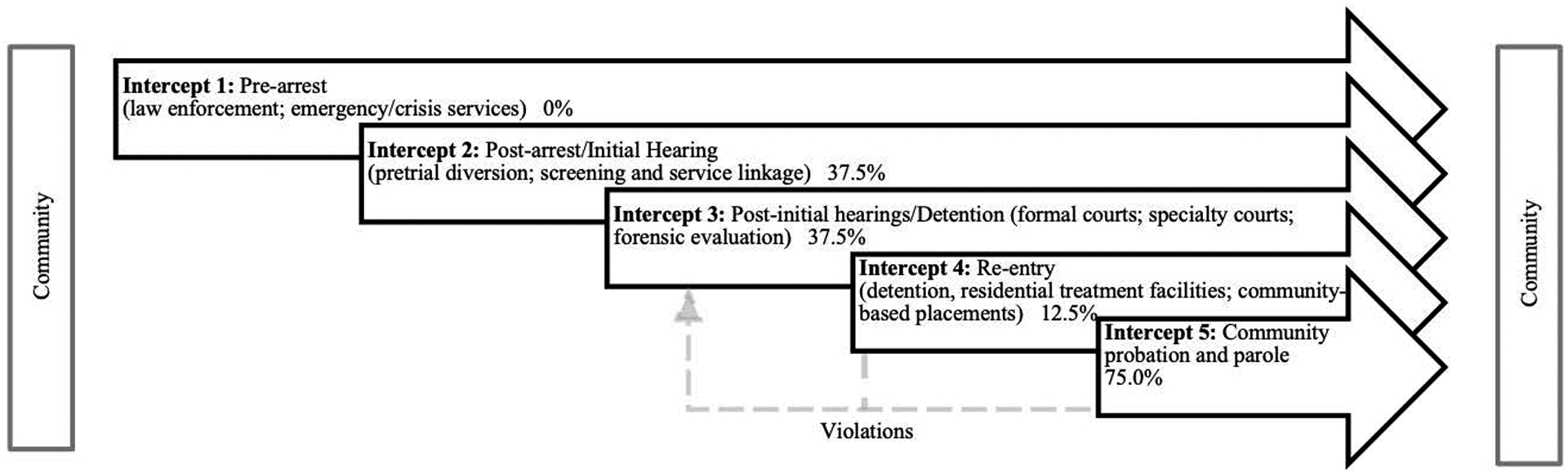
Sequential intercept model
Note. Percentages represent the proportion of articles including justice-involved youth at this intercept. Violations are one example of how youth may re-enter the system at different intercepts.
The SIM is highly relevant to the juvenile justice system given its focus on rehabilitation and community-based intervention (Heilbrun et al., 2017). A prior review of the SIM application to juvenile justice identified Intercepts 1, 3, and 5 as particularly relevant (Heilbrun et al., 2017). Intercept 1 is the point at which youth come into contact with the justice system, often by exhibiting disruptive behavior at school that could be considered offending (e.g., fighting). Schools often have “zero tolerance policies” mandating suspension or expulsion, and at times reporting to the police; these practices ultimately promote the school-to-prison pipeline. At Intercept 3, collaborative/specialty courts are most applicable to the juvenile justice system. Juvenile courts were initially established to be rehabilitative, though have become more punitive over time (Mears, 2002); these alternative models promote more specialized and rehabilitation-oriented attention to youth. Lastly, at Intercept 5, most youth who have been placed in residential facilities receive probation supervision post-release.
The SIM has also been applied to court-involved youth using substances (Dauria, McWilliams, & Tolou-Shams, 2018), highlighting the potential for developing and testing brief substance use interventions for delivery at Intercept 2 when the youth’s substance use may be less severe and contact with the court briefer than those who have become further entrenched. Re-entry (Intercept 4) also maps well onto the juvenile justice process for youth returning to the community from detention or longer-term incarceration, as well as court-ordered residential treatment programs with many of the same community re-integration challenges.
The SIM’s utility and flexibility as an organizing model makes it useful to understand the current state of research about ACEs among justice-involved youth and to offer data-driven trauma-informed behavioral health practices and policies at each intercept of the juvenile justice system. The current study systematically reviews literature on the prevalence and impact of ACEs among justice-involved youth at Intercepts 1–5; Intercept 0 is not included because reviews regarding the impact of ACEs on youth prior to justice contact exist (e.g., Felitti et al., 1998; Hughes et al., 2017; Oral et al., 2016). Grounded in the principle that agencies and systems must respond to the impact and consequences of trauma in all services and policies (American Association of Children’s Residential Centers, 2014) and stemming directly from this research synthesis, data-driven recommendations for practice and policy at each intercept are offered.
Method
Search Strategy
A systematic search for articles involving adverse childhood experiences and justice-involved youth published from January 1, 1990 to January 14, 2020, and updated on September 16, 2020, was conducted in PubMed, PsycINFO, Embase, Web of Science, Sociological Abstracts, Social Services Abstracts, and Google Scholar. Our search was limited to 1990–2020 as the first article describing the ACEs framework was published in 1998 (Felitti et al., 1998). A search strategy was developed in collaboration with a clinical librarian (J.B.Y) using a three step process. First, key articles were identified and term harvesting was conducted to identify relevant terms included therein. Next, search terms were tested by reviewing the unique results for each in order to determine that term’s relevance and subsequent inclusion in the search. Finally, a search strategy was developed by applying Boolean logic to combine similar keywords and controlled vocabulary (e.g. MeSH and Emtree terms) with OR and using AND between the three concepts, for example, (“court involved” OR offender) AND (juvenile OR “young adult”) AND (“Adverse Childhood Experiences”[Mesh] OR “childhood trauma”). Because the focus of the current review is on the ACEs framework broadly, we did not include search terms that focused on individual types of adverse childhood experiences (e.g., parental incarceration). Detailed search strategies for each database can be found in Appendix 1.
Study Selection
Study screening progress was documented in a PRISMA flow chart (Figure 2). Our literature search yielded 1,657 articles. After excluding duplicates, 898 articles underwent title and abstract screening. Two reviewers (J.F. & A.Y.) independently screened a random sample (n=50) and collaboratively reviewed decisions to ensure inter-rater reliability. Studies were then divided and screened by the two reviewers to determine if they met inclusion criteria for full-text review; 642 were eliminated because of irrelevance to the topic. Full-text screening of 256 articles was conducted independently by three reviewers (J.F., K.K., & A.Y.). Inclusion criteria were: (1) peer-reviewed empirical article; (2) U.S.-only population; (3) youth ages 10–18 years at the time of study enrollment (i.e., longitudinal studies may have continued assessment of youth beyond 18 years of age); (4) participants were justice-involved at the time of study enrollment (e.g., arrestees, court-involved, community-supervised, detained); and (5) all three main ACEs categories (i.e., abuse, neglect, and household dysfunction) were measured and included in results. Studies were excluded if they were not published in English. Of the 256 full texts reviewed, 216 did not meet inclusion criteria [e.g., sample was not justice-involved (n=50); did not include all ACEs (n=72); not peer-reviewed empirical article (n=52); sample outside U.S. (n=39); article not in English (n=6); other (n=1)]. A team of four reviewers (J.F., K.K., A.Y., & M.T.S.) assessed and summarized findings from the final 39 articles. Any disagreements in the full text review were resolved collectively after consultation and detailed examination of the study. One additional article from a special issue related to ACEs in juvenile justice which did not appear in the updated search was also added, bringing the overall total for final analysis to 40 articles.
Figure 2.
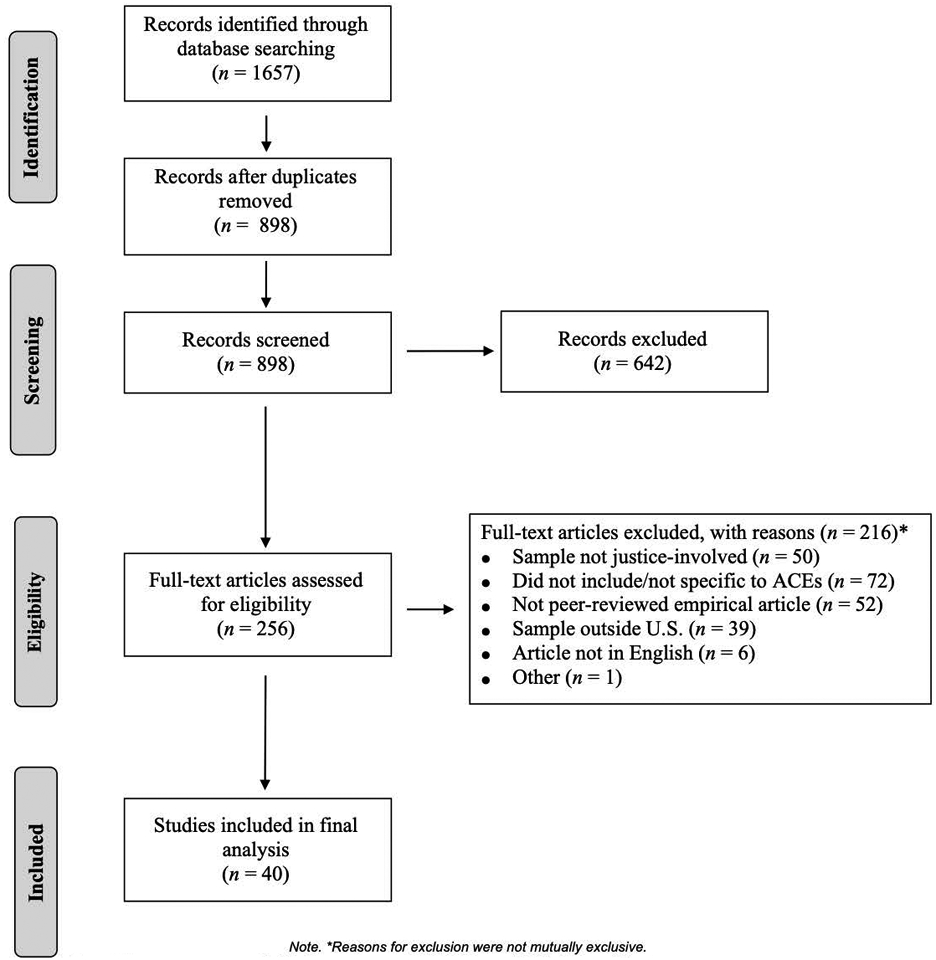
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart Note.
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi: 10.1371/journal.pmed1000097
Results
Substantial overlap in samples was found across the 40 articles examining ACEs among justice-involved youth; 28 articles drew their samples from a single large dataset of youth in Florida, 3 articles each used the same sample of youth from Washington and Texas. Samples across the 28 articles using youth data from Florida were not identical (e.g., a focus on different years of data collection or different subsets of justice-involved youth), but our review discovered substantial overlap in youth data included across the articles. Counting these articles as unique studies could bias summaries. Thus, for the purposes of this review, all Florida dataset findings, Washington dataset findings, and Texas dataset findings, are each considered a single study, resulting in a total of 8 unique studies for review and summary. The term “study” is used to refer to the 8 unique datasets (some including multiple articles), while “article” reflects 40 published articles.
Study designs were 62.5% (n=5) cross-sectional and 37.5% (n=3) longitudinal/prospective; none involved intervention trials. Assessment time periods varied and included data examining youth from the period of initial system entry to discharge and/or aging out; repeated yearly assessments; 1-year following discharge or treatment/service completion; and 3 years post-release from detention. Sample size ranged from 104 to 104,267. All samples involved youth up to age 18. Consistent with higher representation of males and disproportionate representation of racial and ethnic minority youth in the juvenile justice system (Office of Juvenile Justice and Delinquency Prevention, 2019), samples were largely male, and Black and Latinx youth were overrepresented across studies. Two studies focused solely on cisgender females and none focused on sexual or gender minority youth. Level of justice-involvement ranged from initial court appearance or detention, or diversion (Intercept 2) to community supervision (Intercept 5). As shown in Figure 1, no studies included youth at Intercept 1 (law enforcement, emergency services) and Intercept 5 (community corrections/supervision or probation) was most commonly studied (75%).
Assessment of and reporting on ACEs was variable. Range of ACEs assessed across studies was 4 to 11 and there was significant variability within studies on number of ACEs examined; for example, of the articles using the Florida dataset, ACEs reported were 7 (n=1 article), 9 (n=5 articles), 10 (n=20 articles), and 11 (n=2 articles). ACEs were most commonly derived from the Positive Assessment Change Tool (PACT; 37.5% of studies), which has multiple versions (e.g., Pre-Screen, Community-PACT, Residential-PACT), and record review (37.5% of studies). Rates of exposure to individual ACEs were reported in 7 studies; prevalence ranged widely: 10–52% emotional abuse; 16–40% physical abuse; 5–26% sexual abuse; 9%−35% emotional neglect; 7–83% physical neglect; 29–75% caregiver or household incarceration; 14–63% caregiver, family, or household substance use; 5–93% caregiver, family, household mental illness1; 17–85% domestic violence; and 14–93% caregiver separation or divorce.
Study outcomes included descriptive differences in ACEs (e.g., differences by race and ethnicity, gender; n=1 study), delinquency (e.g., recidivism, institutional misconduct; n=5), psychiatric (n=4), substance use (n=3), and other (n=2; academic, pregnancy, victimization); some studies examined multiple outcomes so categories are not mutually exclusive (see Table 1). Regarding the three articles from the Washington study, one solely reported prevalence, one focused on psychiatric outcomes, and one examined psychiatric, substance use, delinquency, academic and family/social outcomes. The three articles from the Texas study all examined delinquency outcomes. Results from the Washington and Texas studies are presented within the other non-Florida studies in the Other Remaining Studies subsection below.
Table 1.
Characteristics of Studies Focused on Adverse Childhood Experiences among Justice-Involved Youth
| Sample Characteristics | ACEs | Study Design | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Age | % Female | Race/Ethnicity | # | M | Assessment | Sampling Frame | Longitudinal/cross-sectional | Outcome | |
| Baglivio et al. (2015) | 64,329a | – | 22 | 39% White/other, 46% Black, 15% Latinx | 10 | 2.8 | Full C-PACT | 18 years old 1/1/07–12/31/12 | longitudinal | delinquency |
| Baglivio et al. (2016) | 12,955a | - | 15 | 4% White, 55% Black, 11% Latinx | 10 | 3.2 | Full C-PACT and R-PACT | Completed residential program 1/1/10–6/30/13 | longitudinal | delinquency |
| Baglivio & Epps (2016) | 64,329a | – | 22 | 38% White, 43% Black, 15% Latinx | 10 | - | Full C-PACT | Turned 18 1/1/07–12/31/12 | longitudinal | descriptive |
| Baglivio, Wolff, Epps & Nelson (2017) | 59,432a | 17.7 | 21 | 38% White, 43% Black, 15% Latinx | 10 | 3.6 | Full C-PACT | Turned 18 1/1/07–12/31/12 | cross-sectional | descriptive |
| Baglivio, Wolff, Piquero et al. (2017) | 10,110a | - | 13 | 37% White, 57% Black; 6% Latinx | 10 | - | Full C-PACT and R-PACT | Completed residential program 12/1/11–12/1/14 | cross-sectional | psychiatric |
| Baglivio et al. (2020) | 64,007a | 22 | 39% White/other, 46% Black, 15% Latinx | 10 | 2.8 | Full PACT | 18 years old 1/1/07–12/31/12 | longitudinal | delinquency | |
| Barnert et al. (2019) | 360 | 16.4 | 100 | 6% White/other, 70% Black, 23% Latinx | 4 | - | record review | Specialty court for CSEC 2012–2016 | cross-sectional | physical health |
| Bright et al. (2018) | 81,171a | - | 22 | 38% White, 46% Black, 16% Latinx | 10 | 2.8 | Full PACT | Adjudicated 12/05–12/14 | cross-sectional | psychiatric |
| Clements-Nolle & Waddington (2019) | 429 | - | 27 | 34% White, 17% Black, 42% Latinx | 8 | 3.7 | BRFSS ACEs Module | Supervised or unsupervised, 2014 | cross-sectional | psychiatric |
| Craig & Trulson (2019) | 1,061c | 15.4 | 100 | 29% White, 35% Black, 34% Latinx | 9 | 3.2 | record review; risk assessments | Incarcerated 2005–2013 | cross-sectional | delinquency |
| Craig & Zettler (2020) | 11,788c | 18.1 | 9 | 21% White, 35% Black, 44% Latinx | 9 | 2.2 | record review; risk assessments | Incarcerated 2005–2013 | longitudinal | delinquency |
| Craig et al. (2017) | 28,169a | 17.0 | 23 | 39% White/other, 46% Black, 15% Latinx | 10 | 2.6 | Full PACT | Community-based placement 7/1/09–6/30/12 | longitudinal | delinquency |
| Craig et al. (2020) | 621c | 16.4 | 3 | 18% White, 37% Black, 45% Latinx | 9 | 2.0 | record review, risk assessments | Incarcerated 2005–2013; Serious and violent delinquent offense | longitudinal | delinquency |
| Craig, Intravia et al. (2019) | 28,169a | 17.0 | 23 | 39% White/other, 46% Black, 15% Latinx | 10 | 2.6 | Full PACT | Community-based placement 7/1/09–6/30/12 | longitudinal | delinquency |
| Craig, Zettler et al. (2019) | 28,047a | 17.0 | 23 | 39% White, 46% Black, 15% Latinx | 10 | 2.6 | Full PACT | Community-based placement 7/1/09–6/30/12 | longitudinal | psychiatric, substance use, delinquency |
| Dargis et al. (2019) | 104 | 16.4 | 0 | 31% White, 66% Black, 2% Latinx | 5 | - | chart review; semi-structured interview | Detained youth; year not specified | cross-sectional | prevalence |
| Fox et al. (2015) | 22,575a | - | 16 | 33% White, 67% non-White | 9 | - | Full PACT | Felony offenders 1/1/07–12/31/12 | longitudinal | delinquency |
| Johnson (2017) | 2,367a | 13.9 | 16 | 29% White, 61% Black, 10% Latinx | 11 | 4.1 | Full PACT | Official referral before age 16, completed PACT in 2007 and 2008, turned 18 by 2016 | longitudinal | psychiatric |
| Johnson (2018a) | 2,558a | 14.0 | 18 | 31% White,58% Black, 10% Latinx | 10 | 3.1 | Full PACT | Official referral before age 16, completed PACT in 2007 and 2008, turned 18 by 2016 | longitudinal | academic |
| Johnson (2018b) | 3,284a | - | 18 | 38% White, 58% Black, 10% Latinx | 11 | 4.0 | Full PACT | Official referral before age 16, completed PACT in 2007 and 2008, turned 18 by 2016 | cross-sectional | delinquency |
| Kowalski (2019) | 50,862 | - | 26 | 61% White, 14% Black, 16% Latinx | 10 | - | Full PACT | Community supervision or probation 12/03–6/17 | longitudinal | delinquency |
| Lee & Taxman (2020) | 16,402 | 15.9 | 25 | 43% White, 42% Black, 10% Latinx | 9 | YASI | Youth beginning probation 2011–2013 | cross-sectional | psychiatric, substance use, delinquency | |
| Levenson et al. (2017) | 89,045a | 16.2 | 22 | 42% White, 25% Black, 15% Latinx | 10 | 2.8 | Full C-PACT | Turned 18 1/1/07–12/31/15 | cross-sectional | descriptive |
| Logan-Greene et al. (2016) | 5,378b | 15.5 | 24 | 56% White, 24% Black, 6% Latinx | 8 | - | Full PACT | Probation 2003–2013 | cross-sectional | prevalence |
| Logan-Greene et al. (2017) | 5,378b | 15.5 | 24 | 60% White, 26% Black, 6% Latinx | 9 | - | Full PACT | Probation 2003–2013 | cross-sectional | psychiatric |
| Logan-Greene et al. (2020) | 5,378b | 15.5 | 24 | 60% White, 26% Black, 6% Latinx | 9 | - | Full PACT | Probation 2003–2013 | cross-sectional | psychiatric, substance use, delinquency, academic, family/social |
| Meldrum et al. (2020) | 8,296a | 16.4 | 13 | 35% White, 65% non-White | 10 | 3.4 | Full C-PACT | Completed residential program 7/1/10–6/30/15 | cross-sectional | psychiatric |
| Muniz et al. (2019) | 30,909a | – | 22 | 38% White, 62% non-White | 9 | – | Full PACT | High risk and turned 18 1/1/07–12/31/12 | cross-sectional | psychiatric |
| Naramore et al. (2017) | 64,329a | - | 22 | 38% White, 43% Black, 15% Latinx | 10 | 3.7 | Full PACT | Turned 18 1/1/07–12/31/12 | longitudinal | descriptive |
| Narvey et al. (2020) | 11,053a | 16.5 | 14 | 53% Black, 12% Latinx | 10 | 3.4 | R-PACT | Completed residential program 2009–2012 | longitudinal | delinquency |
| Perez et al. (2016) | 64,329a | 17.0 | 22 | 38% White, 43% Black, 15% Latinx | 9 | 2.3 | Full PACT | Turned 18 1/1/07–12/31/12 | cross-sectional | psychiatric, substance use, academic |
| Perez et al. (2018) | 64,329a | - | 22 | 38% White, 43% Black, 15% Latinx | 9 | 2.3 | Full PACT | Turned 18 1/1/07–12/31/12 | cross-sectional | psychiatric, substance use, delinquency |
| Reid et al. (2017) | 68,218a | - | 24 | 36% White, 48% Black, 15% Latinx | 10 | 4.1 | Full C-PACT | Arrested 2007–2015 | longitudinal | victimization |
| Reid et al. (2019) | 68,218a | - | 24 | 36% White, 48% Black, 15% Latinx | 10 | - | Full C-PACT | Arrested 2007–2015 | cross-sectional | descriptive, psychiatric, substance use, delinquency |
| Wolff & Baglivio (2017) | 27,720a | - | 23 | 39% White, 46% Black, 15% Latinx | 10 | 2.6 | Full PACT | Community-based service 7/1/09–6/30–12 | longitudinal | delinquency |
| Wolff et al. (2017) | 27,867a | 16.3 | 23 | 38% White, 46% Black, 15% Latinx | 10 | 2.6 | Full C-PACT | Community-based service 7/1/09–6/30–12 | longitudinal | delinquency |
| Wolff et al. (2018) | 92,017a | 16.2 | 48 | 37% White, 47% Black, 16% Latinx | 9 | 2.8 | Full PACT | Turned 18 1/1/07–6/30/16 | cross-sectional | descriptive |
| Wolff et al. (2020) | 104,26a | 16.1 | 24 | 38% White, 46% Black, 16% Latinx | 10 | 2.8 | Full C-PACT | Turned 18 1/1/07–12/31/17 | longitudinal | delinquency |
| Zettler et al. (2018) | 4,733a | – | 32 | 40% White, 45% Black, 15% Latinx | 7 | – | Pre-screen C-PACT | Age 12 at first arrest 1/1/07–12/31/09 | longitudinal | delinquency |
Note. – indicates information was not reported; when descriptives were presented by subgroup, full sample descriptives were calculated;
Drawn from the same dataset of justice-involved youth in Florida;
Drawn from the same sample of justice-involved youth in Washington.
Drawn from the same sample of justice-involved youth in Texas.
Results from Florida Study
Most articles (72%; n=28) used a single large dataset of justice-involved youth in Florida. In Florida (Florida Department of Juvenile Justice, 2012), youth found to be participating in a delinquent act by law enforcement are taken into custody and assessed to determine whether they should be placed in secure, non-secure, or home detention prior to a detention hearing. Youth are assessed by juvenile probation officers during intake with the PACT pre-screen and if determined to be at moderate-high or high risk to re-offend, with the PACT Full Assessment. Youth being considered for residential placement, day treatment, or family therapy with probation supervision, also receive the Full PACT. Youth on probation are assessed with the PACT every 180 days. All articles with Florida youth used the PACT Full Assessment except one which used the pre-screen (Zettler, Wolff, Baglivio, Craig, & Epps, 2018).
Descriptive differences.
Six articles focused on descriptive differences in ACEs among justice-involved youth in Florida (67% cross-sectional). Sub-samples from the Florida study used in each article varied in size (range=59,342–92,017) and gender representation (% female=21–48%); all but one article included 10 ACEs (Wolff et al., 2018 used nine ACEs). Analyses of demographic differences revealed females and White youth report a greater number of ACEs (Baglivio & Epps, 2016; Wolff et al., 2018). White youth were most likely to report exposure to four or more ACEs, though Black youth were least likely to report no ACEs (Baglivio & Epps, 2016). Latent class analysis (Wolff et al., 2018) revealed females and White youth were more likely to be in the high ACEs exposure group, whereas older youth, males, Black, and Latinx youth were less likely to be in the high ACEs exposure group. Females had the strongest odds of membership in the group in which sexual abuse was most prevalent and level of ACE exposure was moderate. Youth who experienced more ACEs were more likely to have a history of child welfare placement and to have parents who experience employment problems.
Neighborhood factors also contributed to ACEs. Living in a disadvantaged neighborhood increased risk for experiencing more ACEs, above and beyond youth-level attributes, whereas living in a neighborhood with a larger concentration of affluent families was associated with lower levels of ACEs (Baglivio, Wolff, Epps, et al., 2017; Wolff et al., 2018). In particular, concentrated affluence was related to less household incarceration and substance use (Wolff et al., 2018), and youth who live in neighborhoods with higher concentration of immigrant populations tended to experience fewer ACEs (Wolff et al., 2018). Level of residential instability within a neighborhood was related to moderate levels of ACEs (Wolff et al., 2018).
Youth who experienced human trafficking were at particularly high risk for experiencing more ACEs (Naramore et al., 2017; Reid et al., 2019). In addition to higher overall levels of ACEs, youth arrested for sex-trafficking violations, who were disproportionately female and Black youth, tended to experience higher levels of every type of ACE (Naramore et al., 2017).
Regarding legal offense history, youth who committed sexual offenses experienced more ACEs than youth who committed non-sexual offenses (Levenson et al., 2017). Specifically, female youth who committed sexual offenses reported more ACEs and higher rates of physical and sexual abuse, and physical neglect than youth who committed non-sexual offenses. Compared to adult females who committed sexual offenses, female youth had higher rates of physical neglect, family violence, parental separation/divorce, and household incarceration, and lower rates of household substance abuse and mental illness. Male youth who committed sexual offenses experienced more ACEs and higher rates of emotional, physical, and sexual abuse, emotional and physical neglect, household mental illness, parental separation/divorce, and household incarceration than youth who committed non-sexual offenses; compared to adult males who committed sexual offenses, male youth experienced more physical abuse, family violence, parental separation/divorce, and household incarceration, and less emotional and sexual abuse, emotional and physical neglect, and household substance abuse and mental illness.
Psychiatric outcomes.
Nine articles focused on psychiatric outcomes (78% cross-sectional). Sample size (range=2,367–81,171), gender representation (% female range=13–24), and number of ACEs (range=9–11; 45% used 10) varied. Articles examined the impact of ACEs on psychiatric symptoms or mental health problems (n=2; Muniz et al., 2019; Perez et al., 2018), mental health diagnosis (n=2; Baglivio, Wolff, Piquero, et al., 2017; Craig, Zettler, et al., 2019), suicidal ideation and/or behavior (n=3; Johnson, 2017; Perez et al., 2016; Reid et al., 2019), and other psychological factors (n=4; e.g., aggression, self-control).
ACEs are associated with increased psychiatric symptoms or mental health problems (Muniz et al., 2019; Perez et al., 2018). Muniz et al. (2019) examined the association between specific types of ACEs and internalizing and externalizing problems, finding emotional abuse, household member incarceration, physical abuse, emotional neglect, and household violence or substance abuse predicted externalizing (e.g., behavioral aggression) outcomes, while only sexual abuse predicted internalizing (e.g., depression) outcomes; physical neglect and parental mental illness did not correlate with either outcome. Perez et al. (2018) found aggression and impulsivity mediated the association between ACEs and general mental health problems (i.e., binary variable reflecting symptoms of general mental health problems, depression, somatic complaints, or thought disturbances).
Experiencing more ACEs is associated with the likelihood of being diagnosed with a mental health condition or prescribed medication by a professional (Craig, Zettler, et al., 2019). Among youth in detention, however, experiencing more ACEs was related to a lower likelihood of having a conduct disorder diagnosis for White and Black males and an increased likelihood of an oppositional defiant disorder diagnosis for Black males and White females; when accounting for prior history of justice involvement, ACEs no longer predicted diagnosis (Baglivio, Wolff, Piquero, et al., 2017).
Higher levels of ACEs are also associated with lower levels of self-control (Meldrum et al., 2020), higher levels of aggression and impulsivity (Perez et al., 2018, 2016) and animal cruelty (Bright et al., 2018), and increased risk for suicidal ideation (Johnson, 2017) and suicide attempts (Perez et al., 2016). Although not examining the relationship between ACEs and suicidal ideation or behavior explicitly, one study found that youth who had history of being trafficked tended to experience more ACEs and were more likely to experience suicidal ideation and attempt suicide (Reid et al., 2019). Aggression and impulsivity mediate the association between ACEs and suicide attempts (Perez et al., 2016).
Substance use outcomes.
Four articles examined the impact of ACEs on substance use (75% cross-sectional). Sample size (range=1,061–67,305) and gender representation (% female range=22–100) varied; three articles assessed nine ACEs and one assessed 10. Results indicated a greater number of ACEs was associated with current alcohol and drug use (Craig, Zettler, et al., 2019) and substance abuse problems (Perez et al., 2018, 2016). Youth who had been trafficked (and had higher rates of ACEs) were more likely to use alcohol and/or drugs (Reid et al., 2019).
Two articles with identical samples supported aggression and impulsivity as mediators of the relationship between ACEs and substance abuse problems (Perez et al., 2018, 2016). Two articles examined substance use as a mediator between ACEs and delinquency outcomes. Results indicated current drug use (for males and non-Latinx youth) and the co-occurrence of drug use and mental health problems (for White youth, and males and females) mediated the relationship between ACEs and recidivism (Craig, Zettler, et al., 2019). Substance abuse problems did not mediate the relationship between ACEs and suicidal behavior (Perez et al., 2016).
Delinquency.
Fifteen articles (80% longitudinal) assessed the impact of ACEs on delinquency (e.g., recidivism, institutional misconduct). Samples varied widely in size (range=3,284–104,267), gender representation (% female range=15–24), and number of ACEs assessed (range=7–11; 73% assessed 10). Recidivism was the primary outcome for 11 of the 15 articles. Higher levels of ACEs predicted recidivism (Craig et al., 2017; Craig, Intravia, et al., 2019; Craig, Zettler, et al., 2019; Johnson, 2018b; Narvey, Yang, Wolff, Baglivio, & Piquero, 2020; Wolff & Baglivio, 2017), as well as shorter time to recidivism for White and Black youth (Wolff et al., 2017). Mediators of the relationship between ACEs and recidivism included negative emotionality (Wolff & Baglivio, 2017); drug use (for males and non-Latinx youth), mental health problems (for Black youth), and co-occurring drug use and mental health problems (for males and females, and White non-Latinx youth) (Craig, Zettler, et al., 2019). One article focused on youth completing a juvenile justice commitment program found no direct effect of ACEs on recidivism, but found an indirect relationship through child welfare involvement history (for White and Latinx youth). Moderators of this relationship included substance use (Craig, Intravia, et al., 2019) and empathy (Narvey et al., 2020); social bonds was also explored as a moderator, though this was not significant (Craig et al., 2017). The link between ACEs and increased likelihood of recidivism was only found among youth who engage in moderate to high substance use (Craig, Intravia, et al., 2019). Empathy moderated the association between ACEs, rearrest and readjudication, attenuating the association among youth who experienced increased empathy over the course of residential treatment (Narvey et al., 2020).
ACEs were also related to serious violent and chronic (SVC) delinquency (Baglivio, Wolff, DeLisi & Jackowski, 2020; Fox et al., 2015; Perez et al., 2018); one article found physical abuse and having an incarcerated household member had the greatest impact on SVC delinquency, whereas emotional neglect and household mental illness were unrelated (Fox et al., 2015). Mediators of the relationship between ACEs and SVC delinquency included aggression, impulsivity, deviant peer imitation, school difficulties, substance abuse, and mental health problems (Perez et al., 2018), as well as psychopathic features (e.g., callousness, detachment; Baglivio et al., 2020).
Additional outcomes examined were offending trajectory (Baglivio et al., 2015), residential placement (Baglivio et al., 2020; Zettler et al., 2018), gang involvement (Wolff et al., 2020), and history of violent behavior and weapons use (Reid et al., 2019). Youth exposed to more ACEs began offending at a younger age (Baglivio et al., 2015; Baglivio et al., 2020) and tended to have a higher number of juvenile arrests (Baglivio et al., 2020). Experiencing more ACEs by the age of 12 significantly increased the odds of residential placement prior to age 17 (Zettler et al., 2018) and by age 18 (Baglivio et al., 2020); ACEs differentially predicted odds of residential placement, with significant higher odds of placement emerging only for Black and Latinx males and Black females (Zettler et al., 2018). Psychopathic features or “dispositional tendencies” mediated a moderate-to-large proportion of the association between ACEs and a range of juvenile justice outcomes, including SVC delinquency, first time justice involvement by age 12, residential placement by age 18, and total number of juvenile arrests (Baglivio et al., 2020). Higher levels of ACEs were linked to gang involvement, and temperament and drug use mediated this association (Wolff et al., 2020). The article examining trafficked youth (who also experienced more ACEs) found they were more likely to have a history of violent behavior and to use weapons (Reid et al., 2019).
Other outcomes.
Three articles (67% longitudinal) examined the impact of ACEs on other outcomes, including academic (n=2; Johnson, 2018a; Perez et al., 2016) and victimization (n=1; Reid, Baglivio, Piquero, Greenwald, & Epps, 2017). Sample size (range=2,558–68,218), gender representation (% female range=18–24), and number of ACEs assessed (range=9–10; 67% assessed 10) varied. Higher levels of ACEs were associated with more toxic relationships with school personnel and lower expectations for graduating from high school (Johnson, 2018a) and greater difficulties in school (e.g., suspensions) (Perez et al., 2016); aggression and impulsivity mediated the relationship between ACEs and school difficulties (Perez et al., 2016). In a comparison of a matched sample who had and had not experienced human trafficking, ACEs were also significantly higher among youth with human trafficking (Reid et al., 2017); all ACEs except physical and emotional abuse predicted human trafficking for females (controlling for other ACEs, for females, odds of human trafficking were lower for those who experienced physical abuse, but higher for those who experienced sexual and physical abuse). For males, only emotional and sexual abuse increased risk of human trafficking.
Results from Remaining Studies
Psychiatric outcomes.
Three studies, including two articles from the Washington dataset, examined the impact of ACEs on psychiatric symptoms (Clements-Nolle & Waddington, 2019; Lee & Taxman, 2020) or mental health problems (e.g., mental health diagnosis, suicidal thoughts, mental health problems interfering with court personnel’s work with the youth; Logan-Greene et al., 2017; Logan-Greene, Kim, & Nurius, 2020;). Consistent with the Florida study, ACEs were associated with increased psychiatric symptoms or mental health problems (Clements-Nolle & Waddington, 2019; Logan-Greene et al., 2017; Logan-Greene et al., 2020). One study documented increased risk of psychiatric symptoms specifically for youth who experienced four or more ACEs (Clements-Nolle & Waddington, 2019). Internal resilience and school connectedness attenuated the association between ACEs and psychiatric symptoms or mental health problems (Clements-Nolle & Waddington, 2019). Youth identified as having elevated mental health treatment needs in a latent class analysis had higher than average exposure to ACEs, including abuse, neglect, domestic violence, and household mental illness (Lee & Taxman, 2020).
Substance use.
Two studies examined the association between ACEs and substance use (Lee & Taxman, 2020; Logan-Greene et al., 2020) as part of latent class analyses. One study found youth classified into the elevated substance use treatment needs group tended to have lower than average exposure to abuse, neglect, domestic violence, and family history of mental illness (Lee & Taxman, 2020). In a separate latent class analysis, youth in the maltreatment class tended to have lower levels of substance use compared to youth in other classes (Logan-Greene et al., 2020).
Delinquency.
Two studies, including the three articles from the Texas dataset, examined the link between ACEs and delinquency. Consistent with the Florida study, higher ACEs predicted recidivism among youth on probation (Kowalski, 2019). Participating in family-based programming and aggression replacement training did not moderate the relationship between ACEs and recidivism (Kowalski, 2019); of note, this study was not designed as an intervention trial to address ACEs. Higher levels of ACEs were unrelated to violent misconduct among detained females (Craig & Trulson, 2019) or to re-arrest during later adolescent years and early adulthood (Craig et al., 2020). One study found gender and racial differences in the link between ACEs and recidivism; exposure to more ACEs increased the odds of arrest for a violent felony for White males and Black females (and marginally for White females), but not Black males or Hispanic males or females (Craig & Zettler, 2020).
Other outcomes.
One study examined the association between ACEs and pregnancy (Barnert et al., 2019) among females impacted by commercial sexual exploitation of children (CSEC) in a collaborative/specialty court (Intercept 3). Experiencing parental incarceration and maternal substance abuse were associated with pregnancy (Barnert et al., 2019).
Discussion
The purpose of this review was to synthesize existing literature examining ACEs among justice-involved youth and provide recommendations for data-driven, trauma-informed responses across the SIM intercepts. Together, studies documented significant associations among justice-involved youth between ACEs and a variety of behavioral health and legal outcomes including mental health or psychiatric symptoms, substance use, and delinquency, as well pregnancy, victimization and limited academic achievement. These relationships were researched across four of the five SIM intercepts, highlighting the importance of screening for and intervening upon ACEs at any and all points of contact with the juvenile justice system. Findings from this review are consistent with the broader literature linking ACEs to poor mental and physical health outcomes (e.g., Liming & Grube, 2018), as well as theories such as general strain theory (Agnew, 1992), which posits that a range of stressors (e.g., child abuse) increase the likelihood of future illicit behavior. Results have clear implications for practice (clinical services, agency context, system-level) and policy in behavioral health and juvenile justice.
Recommendations for Practice
Studies consistently demonstrated the association between ACEs and adverse outcomes for justice-involved youth. In general, the more ACEs youth reported, the higher their risk for mental health and other behavioral concerns including delinquency (Clements-Nolle & Waddington, 2019; Craig, Zettler, et al., 2019; Fox et al., 2015; Johnson, 2018a; Logan-Greene et al., 2017; Perez et al., 2018); this suggests ACEs directly impact youths’ increased likelihood of initial and future juvenile justice involvement. Findings regarding the link between ACEs and substance use were mixed, with one study (Florida dataset) finding ACEs was associated with more substance use (Craig, Zettler, et al., 2019; Perez et al., 2018, 2016; Reid et al., 2019) and two suggesting ACEs was associated with less substance use (Lee & Taxman, 2020; Logan-Greene et al., 2020); of note, the latter studies included youth on probation (Intercept 5), whereas the former included youth across Intercepts 2 through 5. It is critical to note the significant differences with respect to race, ethnicity, and gender in the association of ACEs and behavioral health and legal outcomes. Given well-documented disproportionate minority contact in the juvenile and adult justice systems (e.g., associated with systemic racial bias and profiling; Rovner, 2014), as well as the racial, ethnic, and gender differences observed in psychiatric and legal outcomes associated with ACEs, clinical practice must address the differential cultural (broadly defined) needs of Black, Latinx and other non-majority youth and families, and tailor psychological and recidivism reduction intervention approaches accordingly. Alongside studies demonstrating independent associations between ACEs and outcomes, studies assessing mediators and moderators of the relationships provide additional insight into the clinical implications of these associations. For instance, evidence suggests different ACEs are associated with specific types of psychiatric problems (externalizing vs. internalizing; Muniz et al., 2019) and co-occurring mental health and substance use problems, as well as psychopathic features, mediate the relationship between ACEs and recidivism (Baglivio et al., 2020; Craig, Zettler, et al., 2019).
From a clinical standpoint, our review highlights the importance of targeting youth dysregulation, aggression, and degree of empathy/callousness, within behavioral health treatments, but also heavily acknowledging the role trauma plays in the origin of these symptoms. For example, ACEs are associated with more aggressive and impulsive behaviors among justice-involved youth, and this accounts for a large part of the association of ACEs and mental health and substance use problems (Perez et al., 2018). Similarly, ACEs are related to higher levels of callousness and lower levels of empathy, which in turn is associated with delinquency (Baglivio et al., 2020). The Risk Needs Responsivity (RNR) model (Brogan, Haney-Caron, NeMoyer, & DeMatteo, 2015) highlighting youth criminogenic factors associated with recidivism includes aggressive and impulsive behaviors, as well as low empathy and callousness. While more research in this area is needed, probation officers and other systems stakeholders who use the RNR model should consider conceptualizing the impact of trauma on these behaviors as the risk factor instead of viewing youth simply as aggressive, detached, cold or defiant, even if youth do not meet diagnostic criteria for Post-Traumatic Stress Disorder (PTSD).
Individuals serving justice-involved youth (i.e., practitioners, police officers) may want to consider becoming more knowledgeable about the consequences associated with ACEs and how trauma might influence behaviors commonly displayed by justice-involved youth. Programs and trainings at the agency- and system-level presenting data such as these for psychoeducational purposes, along with proposing a trauma-informed response or creating a trauma-informed environment, should be provided to all staff at each intercept, including law enforcement, judges, probation officers, and treatment staff. Because resiliency and school connectedness have been found to protect against the influence of ACEs on psychiatric outcomes (Clements-Nolle & Waddington, 2019), prevention and intervention programs may want to focus on increasing school and academic engagement when working with justice-involved youth.
Lastly at the system-level, given the high prevalence of ACEs among justice-involved youth (at any intercept) and their association with worse outcomes, the mental health field is in desperate need of large-scale clinical workforce development opportunities and incentives. Learning systems collaboratives and other innovative models of dissemination and implementation to build capacity for trauma-informed care (e.g., statewide; Connell, Lang, Zorba, & Stevens, 2019) can help address this. For example, taking a public health approach to children’s mental health and leveraging technology to support workforce learning and development (Schoenwald, Hoagwood, Atkins, Evans, & Ringeisen, 2010) as well as engaging community coalitions (Hoge et al., 2009) and system champions (Connell et al., 2019) are needed to expand professionals’ evidence-based knowledge and skills in how to address trauma exposure, treat associated symptoms (e.g., emotion dysregulation) and prevent long-term negative justice-involved youth outcomes.
Recommendations for Policy
The reviewed literature highlights the importance of developing community-engaged public mental health and juvenile justice partnerships to coordinate efforts for infusing trauma-informed approaches and care across the intercepts. Though Intercept 0 was not the focus of the current paper, primary prevention of ACEs is likely to be one of the most successful ways of diverting juvenile justice system contact. Juvenile justice and behavioral health stakeholders can offer unique insights to their adult behavioral health and criminal justice counterparts that would support system-wide policies and programs to identify children in need through parent system contact. For example, adult-based programs might provide services for their children at the occurrence of a known ACE risk factor such as parent’s arrest or incarceration, as well as at the time child welfare agencies file abuse and neglect petitions against parents. Intervening at these early stages may prevent the occurrence of additional ACEs and future contact with the juvenile justice system.
Our review also suggests if opportunities for intervention are missed in the community prior to justice involvement, ACEs screening and intervention at the earliest point of justice system contact may still reduce psychiatric and substance use treatment needs and further justice system entrenchment. Over the past two decades, Grisso and colleagues’ work (2012) has led to systemic change in juvenile detention and probation settings with large-scale, ongoing implementation of the MAYSI-2, a brief mental health (including trauma) and substance use screening measure specifically designed for systems to understand the imminent behavioral health needs of youth in their care. Our findings are a call to action to consider incorporating ACEs screening, in addition to typically implemented MAYSI and RNR assessments, for all justice-involved youth at all intercepts. Juvenile justice systems should carefully consider expanding policies to include universal ACEs screening across intercepts.
Thoughtful consideration of such policy shift would include understanding the limitations to ACEs screenings and potential unintended consequences versus benefits. There are noteworthy limitations to the use of the ACEs score (Anda, Porter, & Brown, 2020), including its failure to account for the frequency, intensity, and chronicity of exposure to each ACE. Further, the ACEs score does not provide information about the developmental timing of an experience or account for protective factors that can influence biological stress responses and lead to different outcomes following ACEs. An ACEs score alone is not sufficient for clinical decision-making purposes. Beyond these limitations, universal screening procedures have the potential to flood child welfare systems with calls from mandated reporters and perpetuate new or repeat system involvement, which may be counter to desired outcomes. Information sharing through memorandums of understanding may present some solutions to reduce repetitive child welfare calls, but also raises ethical questions. Specific solutions will likely vary by community. An example at Intercept 1 may include co-responder models at schools where school resource officers respond to calls with mental health professionals, who maintain confidentiality and make informed referrals. ACEs screening and potential associated increase in mandated calls to the child welfare system could also lead to the collateral consequence of further perpetuating systemic racial bias and disproportionate system contact for Black and Latinx youth and families, which is the direct opposite of utilizing ACEs to reduce system contact, particularly for overrepresented Black and Latinx youth.
An additional consequence to universal screening is increased identification of intervention need without the corresponding resources and workforce to deliver empirically-supported care. Current billing for mental health (including substance use) treatment for publicly insured youth requires a “medical necessity” determination and while some U.S. states have broad definitions of medical necessity, others are highly restrictive. For example, a first-time justice-involved youth who screens with 3–4 ACEs, for whom the literature suggests would have significant behavioral health needs and increased risk for continued justice involvement, would not be covered by public health insurance to receive mental health intervention if they do not also meet diagnostic criteria for PTSD or another psychiatric diagnosis. Advocacy for policy shifts in treatment delivery and reimbursement is key to improving these youth’s lives and reducing costs to medical, social, school and legal systems. System and program policies and procedures must integrate a broader approach to trauma-informed care beyond the often traditional and more limited definition of trauma. The SIM provides a framework for systems to examine their trauma-informed policies and practices at each intercept, identify gaps and resources, and strategically plan enhancements.
Limitations to Existing Literature and Directions for Future Research
Our review highlighted that while ACEs are related to a variety of adverse outcomes across four of the five SIM intercepts, certain methodological limitations must be acknowledged. First, there were no discernible studies with youth at Intercept 1 (police contact). The generalizability of findings to justice-involved youth living outside of Florida might be limited due to the fact that youth participants in 28 out of the 40 available reports came from Florida’s juvenile justice system. Many of the studies and reports lacked basic demographic characteristics and/or clear descriptions of the level of justice involvement for the youth under study.
There was also variation and inconsistent measurement of ACEs across studies. Studies differed in the number and types of ACEs assessed, as well as the measurement tools used. These assessment variations across studies make synthesis and interpretation challenging. Of note, some studies used trauma symptom measures as a proxy for exposure to ACEs. Although trauma exposure is the primary etiologic risk factor for trauma symptoms, not all youth exposed to trauma will exhibit PTSD symptoms; as such, findings from these studies may inherently differ from those assessing ACEs directly and may not be representative of justice-involved youth.
The findings reviewed and the inherent methodological limitations of prior research highlight a call-to-action for future research to better understand the relationship between childhood adversity and justice involvement. Future research should more clearly describe sample characteristics, including demographics and stage of justice involvement, to support more robust practice and policy recommendations. It is important for future research to address intersectionality and consider how structural inequities and systemic oppression of minoritized groups may compound the impact of ACEs. More research on individual-, family-, community-, and societal-level factors that mediate the relationship between childhood adversity, justice, and behavioral health-related outcomes will hone our knowledge of protective mechanisms of change to incorporate in future interventions. For example, understanding ways the field can intervene to prevent child-welfare involved youth from engaging in delinquent behavior that can result in dual involvement in the juvenile justice system will be an important area for future research.
Before the juvenile justice community considers using ACEs screening, scholars emphasize current research does not yet support the use of this population based research tool for individual-level clinical decision making (Anda et al., 2020). A future research priority should be developing screening tools that better account for the frequency, intensity, and duration of childhood adversity and connect these experiences to symptom expression (PTSD and beyond) for treatment planning and intervention development. It is also crucial to examine the longitudinal impact of implementing ACEs screenings to determine whether the potential collateral consequences highlighted above come to pass. Beyond individual level research, systemic integration of trauma-informed practices and policy in juvenile justice are common recommendations. Critical implementation science research on when and how trauma-informed practice and policies across the intercepts (e.g., schools, police, detention center staff, judges, lawyers) can be successfully implemented and to study the efficacy of these practice and policy reforms on the outcomes of justice-involved youth.
Conclusion
This review synthesized the literature regarding the impact of ACEs on justice-involved youth and provided recommendations for future directions in this area. Despite the noted limitations and gaps in the literature, findings from this body of research demonstrates that ACEs are associated with a host of negative outcomes in justice-involved youth that could ultimately be prevented. Therefore, we recommend universal screening of ACEs among this population across the different SIM intercepts, but with careful consideration and concurrent research specifically to examine areas of potential unintended consequences. Future research is required to develop, test and successfully implement tailored evidence-based, culturally-congruent interventions to interrupt the negative effect of ACEs on behavioral health, legal, academic and physical health trajectories for this vulnerable youth population. Significant practice and policy shifts must occur concurrently with this ongoing ACEs assessment and intervention research in order for real-world change to occur.
Supplementary Material
Public Significance Statement:
Systematic scoping review results demonstrate youth in contact with the juvenile justice system have high rates of Adverse Childhood Experiences (ACEs), which are associated with greater behavioral health needs and worse legal outcomes. Studies point to critical public health need for data-driven, trauma-informed responses at multiple levels across the continuum of juvenile justice involvement, including: clinical service (e.g., addressing youth dysregulation and aggression versus requiring trauma diagnosis), agency (e.g., training police officers in trauma-responsive practices), and systems (e.g., intervening at time of first ACE documentation, such as parent’s incarceration).
Acknowledgements:
This work was supported by the National Institute on Drug Abuse (K24DA046569, PI: Tolou-Shams; K23DA046565, PI: Yurasek) and the National Institute of Mental Health (K23MH111606, PI: Kemp; T32MH018261, PI: Pfiffner). None of the authors have any conflicts of interest to disclose.
Biographies





Footnotes
Low and high end of ranges presented in text are drawn from articles using the Florida dataset for caregiver, family, household mental illness (range for non-Florida studies was 9–39%).
Reference
- Abreu D, Parker TW, Noether CD, Steadman HJ, & Case B (2017). Revising the paradigm for jail diversion for people with mental and substance use disorders: Intercept 0. Behavioral Sciences & the Law, 35, 380–395. [DOI] [PubMed] [Google Scholar]
- Agnew R (1992). Foundation for a general strain theory of crime and delinquency. Criminology, 30(1), 47–88. [Google Scholar]
- American Association of Children’s Residential Centers. (2014). Trauma-informed care in residential treatment. Residential Treatment for Children & Youth, 31, 97–104. [Google Scholar]
- Anda RF, Porter LE, & Brown DW (2020). Inside the Adverse Childhood Experience score: Strengths, limitations, and misapplications. American Journal of Preventive Medicine, 000(000), 1–3. [DOI] [PubMed] [Google Scholar]
- Baglivio MT, & Epps N (2016). The interrelatedness of adverse childhood experiences among high-risk juvenile offenders. Youth Violence and Juvenile Justice, 14, 179–198. [Google Scholar]
- Baglivio MT, Epps N, Swartz K, Huq MS, Sheer A, & Hardt NS (2014). The prevalence of Adverse Childhood Experiences (ACE) in the lives of juvenile offenders. OJJDP Journal of Juvenile Justice, 3. [Google Scholar]
- Baglivio MT, Wolff KT, DeLisi M, & Jackowski K (2020). The Role of Adverse Childhood Experiences (ACEs) and Psychopathic Features on Juvenile Offending Criminal Careers to Age 18. Youth Violence and Juvenile Justice, 18, 337–364. [Google Scholar]
- Baglivio MT, Wolff KT, Epps N, & Nelson R (2017). Predicting adverse childhood experiences: The importance of neighborhood context in youth trauma among delinquent youth. Crime & Delinquency, 63, 166–188. [Google Scholar]
- Baglivio MT, Wolff KT, Piquero AR, Bilchik S, Jackowski K, Greenwald MA, & Epps N (2016). Maltreatment, child welfare, and recidivism in a sample of deep-end crossover youth. Journal of Youth and Adolescence, 45, 625–654. [DOI] [PubMed] [Google Scholar]
- Baglivio MT, Wolff KT, Piquero AR, & Epps N (2015). The relationship between Adverse Childhood Experiences (ACE) and juvenile offending trajectories in a juvenile offender sample. Journal of Criminal Justice, 43, 229–241. [Google Scholar]
- Baglivio MT, Wolff KT, Piquero AR, Greenwald MA, & Epps N (2017). Racial/ethnic disproportionality in psychiatric diagnoses and treatment in a sample of serious juvenile offenders. Journal of Youth and Adolescence, 46, 1424–1451. [DOI] [PubMed] [Google Scholar]
- Barnert ES, Godoy SM, Hammond I, Kelly MA, Thompson LR, Mondal S, & Bath EP (2019). Pregnancy outcomes among girls impacted by commercial sexual exploitation. Academic Pediatrics. 10.1016/j.acap.2019.12.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Branson CE, Baetz CL, Horwitz SM, & Hoagwood KE (2017). Trauma-informed juvenile justice systems: A systematic review of definitions and core components. Psychological Trauma, 9, 635–646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bright MA, Huq MS, Spencer T, Applebaum JW, & Hardt N (2018). Animal cruelty as an indicator of family trauma: Using adverse childhood experiences to look beyond child abuse and domestic violence. Child Abuse and Neglect, 76, 287–296. [DOI] [PubMed] [Google Scholar]
- Brogan L, Haney-Caron E, NeMoyer A, & DeMatteo D (2015). Applying the Risk-Needs-Responsivity (RNR) Model to Juvenile Justice. Criminal Justice Review, 40, 277–302. [Google Scholar]
- Clements-Nolle K, & Waddington R (2019). Adverse childhood experiences and psychological distress in juvenile offenders: The protective influence of resilience and youth assets. Journal of Adolescent Health, 64, 49–55. [DOI] [PubMed] [Google Scholar]
- Connell CM, Lang JM, Zorba B, & Stevens K (2019). Enhancing Capacity for Trauma‐informed Care in Child Welfare: Impact of a Statewide Systems Change Initiative. American Journal of Community Psychology, 64, 467–480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craig JM, Trulson CR, DeLisi M, & Caudill JW (2020). Toward an Understanding of the Impact of Adverse Childhood Experiences on the Recidivism of Serious Juvenile Offenders. American Journal of Criminal Justice, 1–16. [Google Scholar]
- Craig JM, Baglivio MT, Wolff KT, Piquero AR, & Epps N (2017). Do social bonds buffer the impact of adverse childhood experiences on reoffending? Youth Violence and Juvenile Justice, 15, 3–20. [Google Scholar]
- Craig JM, Intravia J, Wolff KT, & Baglivio MT (2019). What can help? Examining levels of substance (non)use as a protective factor in the effect of ACEs on Crime. Youth Violence and Juvenile Justice, 17, 42–61. [Google Scholar]
- Craig JM, & Trulson CR (2019). Continuity of the delinquent career behind bars: Predictors of violent misconduct among female delinquents. Aggression and Violent Behavior, 49, 101301. [Google Scholar]
- Craig JM, & Zettler HR (2020). Are the effects of adverse childhood experiences on violent recidivism offense-specific? Youth Violence and Juvenile Justice, 1–18. [Google Scholar]
- Craig JM, Zettler HR, Wolff KT, & Baglivio MT (2019). Considering the mediating effects of drug and alcohol use, mental health, and their co-occurrence on the Adverse Childhood Experiences–recidivism relationship. Youth Violence and Juvenile Justice, 17, 219–240. [Google Scholar]
- Dauria EF, McWilliams MA, & Tolou-Shams M (2018). Substance use prevention and treatment interventions for court-involved, non-incarcerated youth. In Monit PM, Colby SM, & Tevyaw TO (Eds.), Brief Interventions for Adolescent Alcohol and Substance Abuse (pp. 213–241). New York: The Guilford Press. [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, … Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults—The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14, 245–258. [DOI] [PubMed] [Google Scholar]
- Florida Department of Juvenile Justice. (2012). Juvenile justice process. Retrieved February 28, 2020, from http://www.djj.state.fl.us/youth-families/juvenile-justice-process#
- Fox BH, Perez N, Cass E, Baglivio MT, & Epps N (2015). Trauma changes everything: Examining the relationship between adverse childhood experiences and serious, violent and chronic juvenile offenders. Child Abuse and Neglect, 46, 163–173. [DOI] [PubMed] [Google Scholar]
- Griffin PA, Munetz MR, Bonfire N, & Kemp K (2013). Development of the Sequential Intercept Model: The search for a conceptual framework addressing criminal justice-behavioral health systems interactions. In Griffin P, Heilbrun K, Mulvey E, DeMatteo D, & Schubert C (Eds.), The Sequential Intercept Model and criminal justice: Promoting community alternatives for individuals with serious mental illness. New York: Oxford University Press. [Google Scholar]
- Grisso T, Paiva-Salisbury M, Williams V, Fusco S, Perrault R, & Barnum R (2012). The Massachusetts Youth Screening Instrument-Version 2 (MAYSI-2): Comprehensive research review (p. 43) Worcester: University of Massachusetts Medical School. [Google Scholar]
- Heilbrun K, DeMatteo D, Yasuhara K, Brooks-Holliday S, Shah S, King C, … Laduke C (2012). Community-based alternatives for justice-involved individuals with severe mental illness: Review of the relevant research. Criminal Justice and Behavior, 39, 351–419. [Google Scholar]
- Heilbrun K, Goldstein NES, DeMatteo D, Newsham R, Gale-Bentz E, Cole L, & Arnold S (2017). The sequential intercept model and juvenile justice: Review and prospectus. Behavioral Sciences & the Law, 35, 319–336. [DOI] [PubMed] [Google Scholar]
- Hoge MA, Morris JA, Stuart GW, Huey LY, Bergeson S, Flaherty MT, … Madenwald K (2009). A National Action Plan for Workforce Development in Behavioral Health. 60, 5. [DOI] [PubMed] [Google Scholar]
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, … Dunne MP (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2, e356–e366. [DOI] [PubMed] [Google Scholar]
- Johnson ME (2017). Childhood trauma and risk for suicidal distress in justice-involved children. Children and Youth Services Review, 83, 80–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson ME (2018a). The effects of traumatic experiences on academic relationships and expectations in justice‐involved children. Psychology in the Schools, 55, 240–249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson ME (2018b). Trauma, race, and risk for violent felony arrests among Florida juvenile offenders. Crime & Delinquency, 64, 1437–1457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kowalski MA (2019). Adverse childhood experiences and justice-involved youth: The Effect of trauma and programming on different recidivistic outcomes. Youth Violence and Juvenile Justice, 17, 354–384. [Google Scholar]
- Lee JS, & Taxman FS (2020). Using latent class analysis to identify the complex needs of youth on probation. Child Youth Serv Rev, 115, 105087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levenson JS, Baglivio M, Wolff KT, Epps N, Royall W, Gomez KC, & Kaplan D (2017). You learn what you live: Prevalence of childhood adversity in the lives of juveniles arrested for sexual offenses. Advances in Social Work, 18, 313–334. [Google Scholar]
- Liming K, & Grube W (2018). Wellbeing Outcomes for Children Exposed to Multiple Adverse Experiences in Early Childhood: A Systematic Review. Child and Adolescent Social Work Journal, 35, 17–335. [Google Scholar]
- Logan-Greene P, Kim BKE, & Nurius PS (2020). Adversity profiles among court-involved youth: Translating system data into trauma-responsive programming. Child Abuse and Neglect, 104, 104465. [DOI] [PubMed] [Google Scholar]
- Logan-Greene P, Tennyson RL, Nurius PS, & Borja S (2017). Adverse childhood experiences, coping resources, and mental health problems among court-involved youth. Child & Youth Care Forum, 46, 923–946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mears DP (2002). Sentencing guidelines and the transformation of juvenile justice in the 21st century. Journal of Contemporary Criminal Justice, 6–19. [Google Scholar]
- Meldrum RC, Young BC, Soor S, Hay C, Copp JE, Trace M, … Kernsmith PD (2020). Are adverse childhood experiences associated with deficits in self-control? A test among two independent samples of youth. Criminal Justice and Behavior, 47, 166–186. [Google Scholar]
- Munetz MR, & Griffin PA (2006). Use of the sequential intercept model as an approach to decriminalization of people with serious mental illness. Psychiatric Services, 57, 544–549. [DOI] [PubMed] [Google Scholar]
- Muniz CN, Fox B, Miley LN, Delisi M, Cigarran GP II, & Birnbaum A (2019). The effects of adverse childhood experiences on internalizing versus externalizing outcomes. Criminal Justice and Behavior, 46, 568–589. [Google Scholar]
- Naramore R, Bright MA, Epps N, & Hardt NS (2017). Youth arrested for trading sex have the highest rates of childhood adversity: A Statewide study of juvenile offenders. Sex Abuse, 29, 396–410. [DOI] [PubMed] [Google Scholar]
- Narvey C, Yang J, Wolff KT, Baglivio M, & Piquero AR (2020). The Interrelationship between empathy and adverse childhood experiences and their impact on juvenile recidivism. Youth Violence and Juvenile Justice, 1541204020939647. [Google Scholar]
- Office of Juvenile Justice and Delinquency Prevention. (2019). Law enforcement and juvenile crime: Juvenile arrests. Retrieved February 28, 2020, from OJJDP Statistical briefing book website: https://www.ojjdp.gov/ojstatbb/crime/qa05101.asp?qaDate=2018&text=yes [Google Scholar]
- Oral R, Ramirez M, Coohey C, Nakada S, Walz A, Kuntz A, … Peek-Asa C (2016). Adverse childhood experiences and trauma informed care: The future of health care. Pediatric Research, 79, 227–233. [DOI] [PubMed] [Google Scholar]
- Perez NM, Jennings WG, & Baglivio MT (2018). A path to serious, violent, chronic delinquency: The harmful aftermath of adverse childhood experiences. Crime & Delinquency, 64, 3–25. [Google Scholar]
- Perez NM, Jennings WG, Piquero AR, & Baglivio MT (2016). Adverse childhood experiences and suicide attempts: The Mediating influence of personality development and problem behaviors. Journal of Youth and Adolescence, 45, 1527–1545. [DOI] [PubMed] [Google Scholar]
- Reid JA, Baglivio MT, Piquero AR, Greenwald MA, & Epps N (2017). Human trafficking of minors and childhood adversity in Florida. American Journal of Public Health, 107, 306–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid JA, Baglivio MT, Piquero AR, Greenwald MA, & Epps N (2019). No youth left behind to human trafficking: Exploring profiles of risk. American Journal of Orthopsychiatry, 89, 704–715. [DOI] [PubMed] [Google Scholar]
- Rovner J (2014). Disproportionate minority contact in the juvenile justice system (Policy brief). Retrieved from https://sentencingproject.org/wp-content/uploads/2015/11/Disproportionate-Minority-Contact-in-the-Juvenile-Justice-System.pdf
- Schoenwald SK, Hoagwood KE, Atkins MS, Evans ME, & Ringeisen H (2010). Workforce development and the organization of work: The Science we need. Administration and Policy in Mental Health and Mental Health Services Research, 37, 71–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolff KT, & Baglivio MT (2017). Adverse childhood experiences, negative emotionality, and pathways to juvenile recidivism. Crime & Delinquency, 63, 1495–1521. [Google Scholar]
- Wolff KT, Baglivio MT, Klein HJ, Piquero AR, DeLisi M, & Howell JC (2020). Adverse childhood experiences (aces) and gang involvement among juvenile offenders: Assessing the mediation effects of substance use and temperament deficits. Youth Violence and Juvenile Justice, 18, 24–53. [Google Scholar]
- Wolff KT, Baglivio MT, & Piquero AR (2017). The relationship between adverse childhood experiences and recidivism in a sample of juvenile offenders in community-based treatment. International Journal of Offender Therapy and Comparative Criminology, 61, 1210–1242. [DOI] [PubMed] [Google Scholar]
- Wolff KT, Cuevas C, Intravia J, Baglivio MT, & Epps N (2018). The effects of neighborhood context on exposure to adverse childhood experiences (ACE) among adolescents involved in the juvenile justice system: Latent classes and contextual effects. Journal of Youth and Adolescence, 47, 2279–2300. [DOI] [PubMed] [Google Scholar]
- Yoder J, Brown A, Grady M, Dillard R, & Kennedy N (2020). Positive Caregiving Styles Attenuating Effects of Cumulative Trauma Among Youth Who Commit Sexual Crimes. International Journal of Offender Therapy and Comparative Criminology, 306624×20952390. (32830582). [DOI] [PubMed] [Google Scholar]
- Zettler HR, Wolff K, Baglivio M, Craig JM, & Epps N (2018). The racial and gender differences in the impact of adverse childhood experiences on juvenile residential placement. Youth Violence and Juvenile Justice, 16, 319–337. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.