

Abstract
Introduction:
Patients with end-stage liver disease (ESLD) have impaired physical, psychological, and social functions, which can diminish patient quality of life, burden family caregivers, and increase healthcare utilization. For those with a life expectancy of less than six months, these impairments and their downstream effects can be addressed effectively through high-quality hospice care, delivered by multidisciplinary teams and focused on the physical, emotional, social, and spiritual wellbeing of patients and caregivers, with a goal of improving quality of life.
Areas Covered:
In this review, we examine the evidence supporting hospice for ESLD, we compare this evidence to that supporting hospice more broadly, and we identify potential criteria that may be useful in determining hospice appropriateness.
Expert Opinion:
Despite the potential for hospice to improve care for those at the end of life, it is underutilized for patients with ESLD. Increasing the appropriate utilization of hospice for ESLD requires a better understanding of patient eligibility, which can be based on predictors of high short-term mortality and liver transplant ineligibility. Such hospice criteria should be data-driven and should accommodate the uncertainty faced by patients and physicians.
Keywords: end stage liver disease, hospice, liver transplant, palliative care, prognosis
1.0. INTRODUCTION
Liver cirrhosis is a life-threatening disease characterized by progressive hepatic fibrosis that can lead to portal hypertension and liver failure. The resulting clinical manifestations include ascites, hepatic encephalopathy, variceal hemorrhage, infections, and hepatocellular carcinoma (HCC). The appearance of these complications denotes the onset of decompensated cirrhosis or “end stage liver disease” (ESLD). These complications comprise the proximate cause of death for many patients with cirrhosis, and overall cirrhosis is the 12th leading cause of death in the US [1]. In addition to the high associated mortality, the complications of ESLD contribute to impairments in physical, cognitive, psychological, and social functions [2–4]. The resultant poor quality of life is linked to further burdens on patients’ caregivers (stress, loss of productivity) and society (health care utilization, costs) [3,5,6].
The physical, psychosocial, and spiritual needs of patients suffering from life-threatening illnesses can be addressed through high-quality palliative care, a team-based approach that cares for patients with serious illness. The field of palliative care has experienced rapid growth in recent years, much of which has focused on patients with cancer [7]. In the cancer population and others, extensive research has documented the positive impact of palliative care on a host of outcomes [8–10], and this success has spurred interest in expanding the role of palliative care for patients with ESLD [11]. A few recent and ongoing studies are examining the impact of palliative care in this population [12–14].
As more attention is paid to palliative care for patients with cirrhosis, it is important to understand the role of hospice care for these patients. Hospice refers to a subset of palliative care reserved for patients with limited life expectancy, typically six months or less (the prognosis required for Medicare beneficiaries to enroll in hospice) [15]. In contrast to the broader field of palliative care, which may be delivered concurrently alongside disease-directed, even potentially curative therapy, in hospice care, patients forgo treatments with curative intent and focus on comfort care and support for patients and their families. Several reviews have been written on palliative care in ESLD in recent years, but none have focused on the unique role of hospice care [11,16,17]. In this review, we aim to examine the role of hospice care for patients with ESLD in the United States, with a focus on potential eligibility criteria that may aid in determining the appropriateness of hospice for specific patients.
2.0. DESCRIPTION OF HOSPICE FOR PATIENTS WITH ESLD
Hospice is a model of care that provides medical and supportive care for patients with life-limiting illnesses and their families. Hospice care focuses on meeting patients’ and caregivers’ physical, emotional, social, and spiritual needs with an emphasis on maximizing quality of life. To achieve these goals, hospice programs leverage the expertise of an interdisciplinary team of doctors, nurses, social workers, counselors, home health aides, chaplains, therapists, and volunteers to deliver comprehensive services focused on patients’ and caregivers’ individual needs. In the US, this care is delivered for patients with an estimated life expectancy of less than six months and is delivered by certified hospice programs, typically in the home setting and also in nursing homes and assisted living. Hospice care can also be delivered in inpatient hospice facilities; however, such care is not common in the US compared to other countries where it is the dominant mode of hospice delivery. Lastly, hospice can be delivered in the hospital when necessary, though short-term hospital care is typically reserved only for symptoms that cannot be controlled outside of the hospital setting or for respite for caregivers. Patients enrolled in hospice typically must forego curative therapies, and often receive their medical care primarily from the hospice team. Financing of hospice care is largely through the Medicare hospice benefit, which is a capitated per diem payment mechanism. Because hospices provide all of the care needed for the primary diagnosis through this per diem payment, costly interventions can be financially problematic.
Patients with cirrhosis suffer from a variety of issues that can be addressed by the hospice team (Table 1). Physical symptoms frequently include pain, breathlessness, muscle cramps, and sleep disturbances [30]. Pain can be a difficult symptom to treat in this population due to the increased propensity for adverse effects from many commonly-used analgesics. For instance, non-steroidal anti-inflammatory drugs are typically avoided due to the risk of gastrointestinal toxicity, renal impairment, and worsening of ascites [31,32]. Opioids are often used, but are impacted by reduced hepatic metabolism and sedating effects interacting with underlying hepatic encephalopathy [33]. Reduced cognitive reserve related to encephalopathy can also limit the use of sleep aids and anti-pruritic therapy with anticholinergic properties due to an increased risk of adverse effects.
Table 1.
Issues Facing Patients with End Stage Liver Disease and How They Can Be Addressed by Hospice
| Domain | Issues | Hospice Services |
|---|---|---|
| Physical | Abdominal symptoms[18] Ascites Hepatic encephalopathy Hepatic hydrothorax Impaired functional status[19] Medical comorbidities[20] Muscle cramps[21] Nausea[22] Pain[22] Pruritis[23] |
Medications Home nursing care Inpatient care Occupational therapy Paracentesis Peritoneal catheter Pleural catheter Physical therapy Thoracentesis |
| Emotional | Anxiety[24] Depression[24] Distress[25] |
Counseling Medications Support |
| Social | Isolation[2] Poverty[26] Substance abuse[26] Unemployment[3] |
Community resources |
| Spiritual | Hope Love Meaning Purpose Religion |
Chaplaincy Counseling Support |
| Caregiver | Anxiety[27] Bereavement[28] Depression[27] Financial burden[3] Impaired health[3] Time burden[29] |
Bereavement care Counseling Respite care |
In addition to the general, non-liver-specific symptoms of advanced illness, patients with end stage liver disease also experience the liver-specific symptoms of ascites and hepatic encephalopathy. Ascites is generally managed by dietary sodium restriction and diuretics. For those with ascites refractory to medications, large volume paracentesis can be used to reduce painful abdominal distention, and repeated paracenteses are often needed [34]. In the hospice setting, patients can avoid repeated trips to the hospital and pain from serial paracentesis with an indwelling peritoneal catheter for home drainage, which is associated with reduced healthcare resource utilization and adequate patient and caregiver acceptability [35,36]. Outside of the hospice setting, such catheters are typically avoided due to high rates of infection and leakage [37]. Ascites also can pass through small defects in the diaphragm into the pleural space, resulting in hepatic hydrothorax. When hepatic hydrothorax accumulates, thoracentesis and indwelling pleural catheters may be used. Refractory hepatic hydrothorax or ascites also can be managed with transjugular intrahepatic portosystemic shunts (TIPS). However, these shunts can cause deterioration in liver function and hepatic encephalopathy, and therefore they are typically not appropriate for those on hospice care, in whom these risks outweigh the short-term potential benefits [38,39]. Hepatic encephalopathy is treated with ammonia-lowering therapies, including synthetic disaccharides (e.g. lactulose) and nonabsorbable antibiotics (e.g. rifaximin). Although effective, lactulose is often limited by side effects, which include abdominal cramping, flatulence, and diarrhea [40]. Adherence to lactulose can also be challenging, as the dosing is titrated to achieve two to three soft bowel movements per day. Rifaximin does not have the same gastrointestinal side effects; however, it is costly.
In addition to physical symptoms, patients with end stage liver disease commonly have mental health disorders such as depression, anxiety, and alcohol and substance use disorders [24]. These disorders may be amplified by the psychological distress accompanying the knowledge of limited life expectancy. Emotional symptoms can be addressed by the medical team through pharmacotherapy and psychotherapy, as well as involvement of other hospice team members who can provide additional community resources. Community resources may also be employed in aiding patients with social troubles: social isolation, poverty, and substance use disorders are common in patients with ESLD and can be addressed by the hospice team [41]. Lastly, hospice can provide resources to address patients’ spiritual concerns, which are aspects related to meaning, purpose, and connectedness in patients’ lives [42]. In this respect, hospice clinicians are trained to complete a spiritual screening, and to collaborate with the multidisciplinary team, including chaplain support, to assess and treat spiritual distress through the biopsychosocial model and involvement of the patient’s spiritual community.
Finally, aside from addressing the needs of patients suffering from life-limiting illness, hospice can also serve family caregivers. Caregivers of patients with ESLD experience burdens on their schedules, finances, personal health, mental health, and social functioning [3,27]. Patients’ hepatic encephalopathy is especially burdensome to caregivers, who develop expertise in the day in, day out management of the disease, but who also suffer from diminished quality of life and psychological distress [29,43–45]. By assuming some of the home health assistance that would otherwise be the responsibility of caregivers, hospice can reduce caregiver burden. Caregiver burden can also be lightened through taking advantage of respite care that is available for hospice beneficiaries. Caregivers, along with patients, prefer the introduction of non-hospice palliative care early in the disease course to assist with illness understanding and coping [46]. Lastly, following the patient’s death, bereavement can result in deterioration in caregivers’ physical and mental health, leading to complicated grief in some and an increase in mortality [47]. Bereavement support is another benefit of hospice care that is covered for 13 months after the patient’s death.
3.0. HOSPICE ELIGIBILITY OF PATIENTS WITH ESLD
For patients in the United States (U.S) who are Medicare beneficiaries, hospice is covered by the Medicare hospice benefit. To be eligible for this benefit, a patient’s physician must certify a life expectancy of less than six months, which can be based on either a decline in clinical status or a combination of both non-disease- and disease-specific guidelines [15]. The non-disease-specific guidelines focus both on impairment in functional status and on dependence on assistance for activities of daily living. Liver disease-specific guidelines, most recently updated in 2019, are listed in Table 2. Although these criteria include many of the pertinent features of ESLD, they are not data-driven, they lack important prognostic factors (e.g., Model for End-stage Liver Disease [MELD]), and they include some factors that are dated and no longer clinically relevant (e.g. hepatitis C refractory to interferon treatment). In addition, they do not address liver transplant (LT) eligibility criteria. Transplant eligibility is a critical component when considering hospice, as opting for care under the hospice benefit of Medicare, for example, includes forgoing such life-prolonging or curative therapies typically covered by Medicare Part A, the hospital insurance portion [48]. In contrast, non-hospice palliative care, which can benefit patients with serious life-threatening illness pursuing curative therapies, can be delivered concurrently with LT evaluation and listing.
Table 2.
Medicare Guidelines to Support Hospice Eligibility for Patients with Liver Disease[15]
| Patients will be considered to be in the terminal stage of liver disease (life expectancy of six months or less) if they meet the following criteria. (1 and 2 should be present, factors from 3 will lend supporting documentation.) |
| 1. The patient should show both a and b: |
| a. Prothrombin time prolonged more than 5 seconds over control, or International Normalized Ratio (INR) > 1.5; |
| b. Serum albumin < 2.5 gm/dl. |
| 2. End stage liver disease is present and the patient shows at least one of the following: |
| a. Ascites, refractory to treatment or patient non-compliant; |
| b. Spontaneous bacterial peritonitis; |
| c. Hepatorenal syndrome (elevated creatinine and BUN with oliguria (< 400 ml/day) and urine sodium concentration < 10 mEq/l); |
| d. Hepatic encephalopathy, refractory to treatment, or patient non-compliant; |
| e. Recurrent variceal bleeding, despite intensive therapy. |
| 3. Documentation of the following factors will support eligibility for hospice care: |
| a. Progressive malnutrition; |
| b. Muscle wasting with reduced strength and endurance; |
| c. Continued active alcoholism (> 80 gm ethanol/day); |
| d. Hepatocellular carcinoma; |
| e. HBsAg (Hepatitis B) positivity; |
| f. Hepatitis C refractory to interferon treatment. |
In determining hospice eligibility, it is therefore important to consider both (1) factors that are predictive of high short-term mortality, and (2) factors that would prevent a patient from being eligible for transplant (Figure).
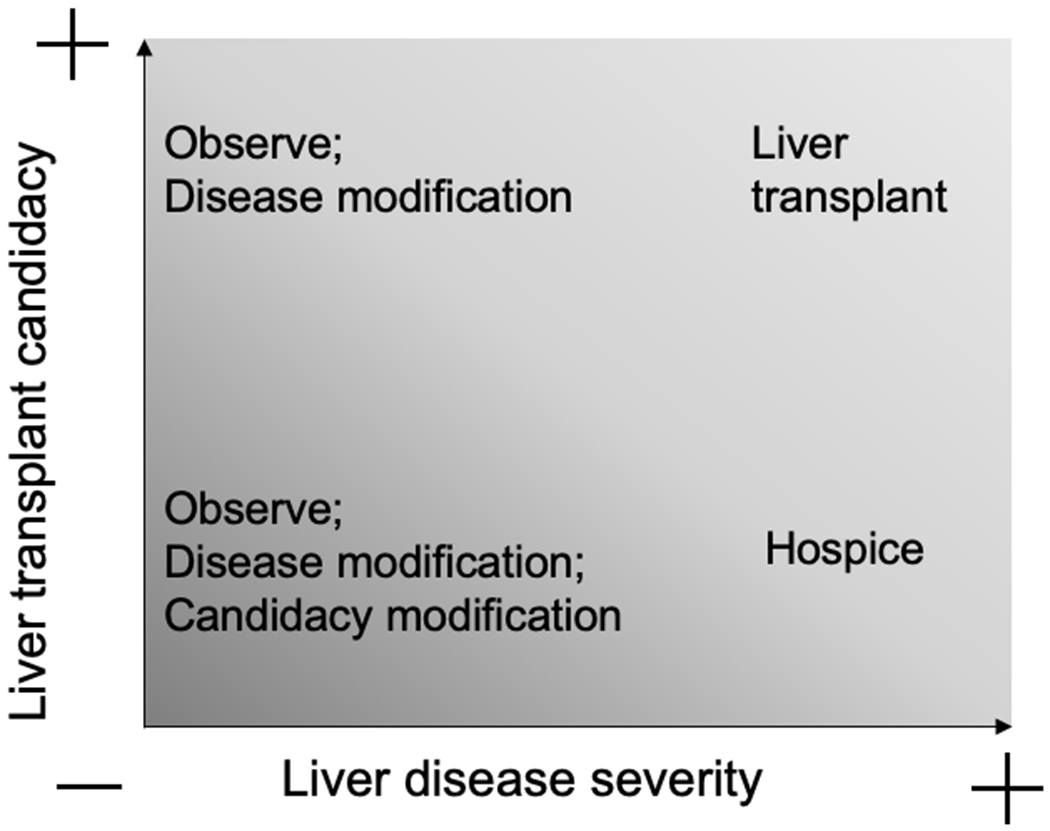
Relationship between liver disease severity, transplant candidacy, and hospice.
3.1. Prognostic Factors (Table 3)
Table 3.
Prognostic Factors That May Be Used to Help Determine Hospice Eligibility
| Factor | Parameter | Outcome | Population |
|---|---|---|---|
| MELD | MELD ≥ 20 | 3-month mortality 81%[49] | Hospitalized patients |
| MELD ≥ 20 | 3-month mortality 50%[49] | Ambulatory patients | |
| MELD ≥ 30 | 3-month mortality 53%[50] | Waitlisted patients | |
| MELD ≥ 30 | 6-month mortality 75%[51] | Hospitalized patients | |
| MELD-Na | MELD-Na ≥ 32 | 3-month mortality 65%[52] | Waitlisted patients |
| Child-Pugh | Child-Pugh C | 3-month mortality 51%[49] | Hospitalized patients |
| Child-Pugh C | 6-month mortality 42%[51] | Hospitalized patients | |
| Acute-on-Chronic Liver Failure | ACLF (CLIF) | 3-month mortality 48–63%[53] | Hospitalized patients |
| ACLF (NACSELD) | 30-day mortality 49%[54] | Hospitalized patients (infection) | |
| Refractory Ascites | Refractory ascites | 12-month mortality 37–48%[55] | Individual patient meta-analysis |
| Hepatorenal Syndrome | HRS Type 1 | 3-month mortality 81%[56] | Meta-analysis |
| HRS Type 2 | 3-month mortality 46%[56] | Meta-analysis | |
| Hepatopulmonary Syndrome | PaO2 ≤ 60 mmHg | 6-month mortality 75%[57] | Transplant evaluation |
| Frailty/Sarcopenia | Liver frailty index ≥ 4.5 (with HE and/or ascites) | 12-month mortality 39%[58] | Waitlisted patients |
| Psoas muscle thickness/height ≤ 16.8 mm/m | 6-month mortality 42%[59] | Waitlisted patients | |
| Sarcopenia (skeletal muscle index ≤38.5 cm2/m2 for women; ≤52.4 cm2/m2 for men) | 12-month mortality 47%[60] | Ambulatory patients | |
| Sarcopenia in women (skeletal muscle index <39 cm2/m2) | 6-month mortality ~50%[61] | Waitlisted patients | |
| Bristol Prognostic Screening Tool | BPST ≥3 | 12-month mortality 81%[62] | Hospitalized patients |
| Supportive and Palliative Indicators Tool | SPICT | 6-month mortality 37%[63] | Hospitalized patients |
Abbreviations: MELD, model for end-stage liver disease; ACLF, acute-on-chronic liver failure; CLIF, chronic liver failure consortium; NACSELD, North American Consortium for the Study of End Stage Liver Disease; HRS, hepatorenal syndrome; HE, hepatic encephalopathy; BPST, Bristol Prognostic Screening Tool; SPICT, Supportive and Palliative Indicators Tool
3.1.1. MELD
MELD is a laboratory-based scoring system based on serum bilirubin, creatinine, and INR that predicts mortality and has been validated repeatedly in different populations of patients with cirrhosis [49,50,64]. It is used ubiquitously in clinical care for liver disease, primarily in organ allocation to prioritize patients on the transplant waitlist, but also for prognostication in other situations including TIPS placement, alcoholic hepatitis, and non-transplant surgery. Initial studies examining MELD showed very high 3-month mortality with MELD ≥ 20, but more recent data suggest a higher threshold of ≥ 30 to best identify those at high risk of short-term mortality [49,50].
The well-known contribution of hyponatremia to poor prognosis in cirrhosis led investigators to revise the MELD score to include serum sodium concentration (MELD-Na), which more accurately predicts outcomes and has therefore supplanted MELD in organ allocation [65]. One study of US transplant registry data showed 3-month mortality of 65% in patients with MELD-Na ≥ 32 [52].
3.1.2. Child-Pugh Score
The Child-Pugh classification is a simple metric that has been in use for 50 years. It is comprised of serum albumin, bilirubin, and prothrombin time; and the presence of ascites and hepatic encephalopathy [66]. The resulting score is used to classify patients as “A”, “B”, or “C”, corresponding to a one-year survival of 100%, 80%, and 45%, respectively [67]. Studies examining shorter-term outcomes have found patients with Child-Pugh class C cirrhosis have 3–6 month mortality rates of 42–51% [49,51].
3.1.3. Acute-on-Chronic Liver Failure
Acute-on-chronic liver failure (ACLF) is a syndrome of acute decompensation of chronic liver disease in association with extrahepatic organ failures. Although the definition of ACLF has not been standardized, it is clear that the presence of extrahepatic organ failures is associated with high short-term mortality [68]. One European study of patients with ACLF from the Chronic Liver Failure Consortium identified 3-month mortality of 48–63% [53]. Another US-based study in hospitalized patients with infections showed 30-day mortality of 49% [54].
3.1.4. Refractory Ascites
Ascites that cannot be mobilized with medications is termed refractory ascites. Refractory ascites is typically managed with large volume paracentesis, TIPS, and transplant where possible. Historically, refractory ascites has been associated with a median survival of 6 months [69]. More contemporary data from TIPS clinical trials show 25–35% mortality at 6 months and 37–48% mortality at 1 year [55].
3.1.5. Hepatorenal Syndrome
Hepatorenal syndrome (HRS) is a dreaded consequence of cirrhosis in which patients with portal hypertension and ascites develop progressive renal failure as a result of splanchnic arterial vasodilatation with accompanying decreased renal perfusion [70]. HRS has classically been divided into two types: type 1 characterized by rapid acute kidney injury occurring in less than two weeks, and type 2 characterized by a more slowly progressive decline in renal function typically seen in the setting of diuretic-refractory ascites. Recently updated consensus recommendations have more precisely defined type 1 HRS [71]. In a systematic review and meta-analysis of outcomes in cirrhosis and concurrent renal failure, type 1 and type 2 HRS were associated with 3-month mortality rates of 81% and 46%, respectively [56].
3.1.6. Hepatopulmonary Syndrome
Hepatopulmonary syndrome refers to hypoxemia due to intrapulmonary vascular dilatations in the setting of chronic liver disease or portal hypertension. It occurs in up to 30% of patients evaluated for LT and is associated with reduced quality of life and survival [72]. Mortality in hepatopulmonary syndrome is directly related to the degree of hypoxemia; patients with PaO2 ≤ 60 mmHg have extremely high short-term mortality (75% at 6 months) [57]. Transplant-eligible patients with this degree of hypoxemia are therefore eligible for priority placement on the waitlist, even with lower MELD scores [73].
3.1.7. Frailty
Frailty is a condition characterized by diminished physiologic reserve, in which patients are highly vulnerable to stress, with an increased risk of poor outcomes. Multiple measures of frailty have been studied in patients with cirrhosis, including both general frailty measures, as well as liver disease-specific frailty measures [74]. These measures have largely focused on physical frailty, including direct physical assessment of gait speed, lower extremity function, and grip strength [75–77], as well as indirect assessment of daily activities and performance [19,78]. Frailty is common in patients with ESLD, and it is associated with increased mortality [19,58,76,79]. Although most studies have not identified extremely high short-term mortality in frail patients, one large multicenter study of patients listed for transplant showed that physically frail patients (identified using the Liver Frailty Index) with either ascites or HE had a one-year mortality of 39% [58].
3.1.8. Sarcopenia
Sarcopenia is a syndrome closely related to frailty, characterized by decreased muscle mass and function [80]. It is also common in patients with cirrhosis, and it can be quantified on the basis of skeletal muscle area on cross-sectional imaging at the L3 vertebral level [61]. Muscle mass cutoffs for defining sarcopenia vary widely between studies and are typically sex-specific, with men having a higher threshold than women [81]. Sarcopenia in patients on the LT waitlist has been associated with increased mortality independent of liver disease severity (as measured by MELD or Child-Pugh score) [81]. Notably, sarcopenia has been associated with 6–12 month mortality rates approaching 40–50% [59–61].
3.1.9. Novel Tools
Due to the limitations of established prognostic factors, newer approaches to identify patients in need of palliative care and potentially hospice are being developed and tested. One, the Bristol Prognostic Screening Tool, is based on Child-Pugh score, performance status, hospital admissions, ongoing alcohol use, and suitability for LT [62]. It can predict 1-year mortality with a positive predictive value of 81%. The Supportive and Palliative Care Indicators Tool is based on the presence of cirrhosis complications (refractory ascites, hepatic encephalopathy, hepatorenal syndrome, bacterial peritonitis, or variceal bleeding) or contraindication to LT [63]. Preliminary data of this tool shows 6- and 12-month mortality of 37% and 54%, respectively. Both of these tools, developed in the United Kingdom, still require further developmental work, but they are promising tools to fill this important need.
3.2. Transplant Ineligibility Factors (Table 4)
Table 4.
Transplant Ineligibility Factors
| Factor | Rationale |
|---|---|
| Obstructive coronary artery disease not amenable to revascularization | Patients with medically-managed obstructive coronary artery disease without revascularization have nearly 100% intra-operative and post-operative morbidity and mortality.[82] |
| Systolic heart failure | Profound hemodynamic changes during LT require adequate compensatory cardiac function.[83] |
| Pulmonary hypertension (mPAP ≥ 35 mmHg) not correctable with medical therapy | Perioperative mortality associated with mPAP ≥ 50 mmHg is 100%; mortality for mPAP 35–50 mmHg is 50%.[84] |
| Severe intrinsic pulmonary disease | Impaired pulmonary function is associated with increased post-transplant length of stay and ventilator time.[85] |
| Class 3 obesity (BMI ≥ 40 kg/m2) | Obesity is associated with increased transplant operative time, wound infections and dehiscence, overall infections, postoperative respiratory failure, and hospital length of stay.[86] |
| Inability to maintain abstinence from alcohol or illicit substances | A short duration of abstinence before transplant is associated with post-transplant recidivism, which results in decreased survival.[87,88] |
| Persistent nonadherence to medical recommendations | Pre-transplant nonadherence predicts post-transplant nonadherence, which results in organ rejection and graft loss.[89,90] |
| Lack of adequate social support | Social support is necessary to aid the transplant recipient in maintaining their health through assisting with appointments, necessary testing, and medications. |
| Hepatocellular carcinoma with extrahepatic spread | Patients with advanced HCC have a limited life expectancy that cannot be corrected with LT. |
| Intrahepatic cholangiocarcinoma | Following LT with intrahepatic cholangiocarcinoma, recurrence was found in 57%, and 5-year survival was 51%.[91] |
| Active extrahepatic malignancy | Post-transplant cancer recurrence rates are associated with the duration of remission and vary based on the type of cancer. Cancers treated after transplant are associated with very high recurrence rates.[92] |
| Poorly-controlled HIV infection | Patients with poorly-controlled HIV (CD4+ T-cell count < 200 cells/mm3 and/or detectable HIV viral load) have a high incidence of HIV-related complications following LT, and 3/11 patients in one report died rapidly of HIV.[93] |
| Uncontrolled sepsis | Patients with active sepsis are generally too unstable to safely undergo LT. |
| Anatomic abnormality that precludes transplant | Anatomic features may prohibit the ability to perform LT (e.g. extensive mesenteric thrombosis). |
| Patient preference to decline transplant | Autonomy is a central principle of biomedical ethics, and fully informed patients may wish to decline LT in favor of hospice.[94] |
Abbreviations: LT, liver transplantation; mPAP, mean pulmonary arterial pressure; BMI, body mass index; HCC, hepatocellular carcinoma; HIV, human immunodeficiency virus
Despite increasing numbers of transplants performed in the US, the demand for donor livers continues to outstrip supply, with thousands of patients dying of ESLD each year [95]. Therefore, as a scarce resource, LT must necessarily be rationed, accounting for principles of justice (equity and fairness) and utility (maximization of benefit) [96]. In promoting utility, transplant programs evaluate patient transplant candidacy with regard to the likelihood of a good post-transplant outcome [97]. Determination of transplant candidacy, typically performed by a multidisciplinary committee, is a complex decision. This decision-making process typically involves identifying factors that might render a patient unsuitable for transplant (i.e., having a high probability of excessive morbidity and mortality following transplant) [97]. However, clear contraindications for transplant are often not present, and eligibility decisions therefore frequently require inductive reasoning, with detailed discussions among committee members. Despite the limitations of contraindications in facilitating decisions, when present they can still play an important role, and may be useful in hospice discussions, too.
3.2.1. Cardiac Disease
LT is a major surgical procedure associated with a high risk of major cardiovascular events and perioperative death, and cardiovascular risk stratification is an essential component of the LT evaluation [98]. Patients found to have significant coronary artery disease typically undergo percutaneous coronary intervention to reduce their risk, and those who are not candidates for coronary revascularization are usually not eligible for transplant [82,99]. Similarly, patients with significant systolic heart failure are also not transplant candidates (except in the rare circumstance where combined heart-liver transplant is an option) [83].
3.2.2. Pulmonary Hypertension
Patients with portal hypertension frequently have coexisting pulmonary arterial hypertension (portopulmonary hypertension), with associated perioperative mortality directly related to the baseline mean pulmonary artery pressure (mPAP). Transplant can be performed safely when the mPAP is less than 35 mmHg; for patients with mPAP > 45–50 mmHg, mortality is excessive and transplant is contraindicated [84,100]. Patients with moderate to severe pulmonary hypertension can be treated with vasodilator therapy to reduce the mPAP and thus facilitate safe transplantation [101].
3.2.3. Obesity
Obesity is associated with increased transplant operative time, wound infections and dehiscence, overall infections, postoperative respiratory failure, and hospital length of stay [86]. Historically, obese patients also had increased post-transplant mortality, but contemporary data suggest similar mortality rates compared to normal-weight recipients [102]. Efforts to induce weight loss prior to transplant are complicated by coexisting sarcopenia and nutritional needs of patients with ESLD. Additionally, bariatric surgery in patients with ESLD is associated with very high mortality [103]. Outcomes from a single-center experience with simultaneous LT and sleeve gastrectomy are encouraging [104]. Class 3 obesity (BMI ≥ 40 kg/m2) is considered a relative contraindication to transplant in clinical practice guidelines [73], though this recommendation is controversial, and there is a lack of consensus on strict cutoffs for obesity to preclude transplant [86].
3.2.4. Advanced Age
Older patients are more likely to carry cardiopulmonary comorbidities and physical frailty that may preclude transplant. However, older age alone is not associated with worse post-transplant outcomes, and elderly patients should not be excluded from transplant consideration solely on the basis of age [105].
3.2.5. Frailty/Sarcopenia
Both pre-transplant frailty and sarcopenia are associated with post-transplant complications and mortality [81,106,107]. However, the evidence for frailty as a predictor of post-transplant mortality remains underdeveloped, with modest absolute risk differences. One series described 90-day post-transplant mortality in up to 12% of high-risk patients (compared to 3% in low-risk patients) [106] while the larger experience of the US national transplant registry showed one-year post-transplant mortality of 13% in severely impaired patients (compared to 7% in non-impaired patients) [107]. For patients with sarcopenia, a meta-analysis has suggested increased post-transplant mortality (HR 1.84; 95% CI 1.11–3.05), but study heterogeneity is significant, and absolute mortality estimates vary widely [81]. Uncertainty is compounded by the inherent selection bias in post-transplant observational studies (which exclude those severely impaired patients not offered transplant). Due to the significant uncertainty surrounding the impact of frailty and sarcopenia on post-transplant outcomes, consensus statements do not support the use of a one-time assessment of frailty to exclude a patient for transplant [74].
3.2.6. Ongoing Alcohol or Illicit Substance Abuse
A key consideration in the transplant candidacy of patients with alcoholic liver disease is the status of patients’ underlying alcohol use disorder. In addition to addiction treatment, a 6-month period of abstinence has traditionally been required prior to transplant listing to allow for potential recovery of liver function and to reduce the risk of post-transplant relapse [73]. Indeed, the risk of post-transplant recidivism is directly related to the duration of pre-transplant abstinence [87]. Rarely, patients with alcoholic hepatitis with extremely high risk of short-term mortality can benefit from early transplantation despite recent alcohol use, with low rates of recidivism [108,109]. However, patients who do not meet the rigorous psychosocial criteria for early transplantation and others who are unable to maintain continuous abstinence are not candidates for transplant [73].
3.2.7. Persistent Nonadherence
Nonadherence to medical recommendations (including immunosuppressive regimens) is closely associated with a variety of poor outcomes including organ rejection and graft loss, and therefore patient selection for post-transplant adherence is an important component of optimizing transplant outcomes [89]. Post-transplant nonadherence can be predicted by pre-transplant nonadherence [90], and thus patients with persistent nonadherence to medical recommendations are not eligible for transplant [73].
3.2.8. Lack of Adequate Social Support
Organ transplant recipients require intensive medical care, including frequent laboratory testing and office visits to monitor and maintain their health. Coordinating this care requires the assistance of informal caregivers, and therefore a lack of adequate social support is considered a contraindication to LT in US clinical practice guidelines [73]. However, the relationship between social support and post-transplant outcomes is not well-established [110]. In addition, use of social support criteria to exclude patients for transplant may violate principles of fairness, consistency, and equity; and it may exacerbate racial and socioeconomic disparities in access to transplant [111].
3.2.9. Malignancy
Cirrhosis is a strong risk factor for HCC, and screening for HCC is recommended for all patients with cirrhosis [112]. When diagnosed at an early stage, patients are candidates for curative therapy, including LT [73]. Indeed, patients with HCC within the “Milan criteria” (one lesion ≤ 5cm or three lesions each ≤ 3cm) receive priority on the transplant list. Those with intrahepatic disease beyond the Milan criteria can get locoregional therapy for downstaging to within the Milan criteria for potential transplant. Patients with more advanced HCC (either macrovascular invasion or extrahepatic metastases, corresponding to BCLC stage C) are not candidates for LT.
Cholangiocarcinoma is a rare cancer with an increased incidence in the setting of chronic liver disease [113]. Patients with intrahepatic cholangiocarcinoma who have undergone LT have very high recurrence rates and low post-transplant survival [91]. Therefore, intrahepatic cholangiocarcinoma is considered a contraindication to transplant.
After transplant, organ recipients have an increased risk of both solid and hematological cancers, and outcomes for these patients are worse than for the general population with cancer [114,115]. Transplant is contraindicated in those with active extrahepatic malignancies. In those with a prior history of cancer, the risk of recurrence is associated with duration of remission and varies based on the type of cancer [92]. These factors should be carefully considered when determining individual transplant candidacy.
3.2.10. Patient Preference
Autonomy is a central principle of biomedical ethics that allows for fully informed, competent patients to make their own medical decisions [94]. Some patients may not want to undergo the pain of major abdominal surgery or the subsequent recuperation, and some may not want to risk the well-known complications of LT [116]. For these patients with a limited life expectancy, hospice is a reasonable alternative.
4.0. BENEFITS OF HOSPICE FOR PATIENTS WITH ESLD
For patients with cancer at the end of life, hospice has been associated with multiple benefits. Benefits for patients include better emotional support and an improved quality of death, and benefits for caregivers include a reduced risk of prolonged grief disorder and posttraumatic stress disorder [117–119]. Hospice is also associated with reduced healthcare utilization, including lower hospitalization rates, use of intensive care and invasive procedures, and healthcare costs [120]. Similar benefits have been shown in other chronic illnesses including heart failure and kidney disease [117,121–125].
In contrast to these favorable data, there has been relatively little research on the benefits of hospice for patients with cirrhosis. Of the studies that have been performed in this population, most have been specifically in patients with HCC. For patients with HCC, hospice has been associated with decreased healthcare services utilization, including costs and invasive procedures, and with fewer in-hospital deaths [126–129]. One study of patients with cirrhosis regardless of HCC presence found that hospice was associated with patient decisions to place limitations on their resuscitation (code) status [130]. No studies of patients with cirrhosis have examined the impact of hospice on patient-reported outcomes. In contrast, one study of patients with cirrhosis showed that non-hospice palliative care is associated with improvements in symptoms and depression [131]. Notwithstanding the paucity of evidence for hospice for ESLD, clinical practice guidelines are starting to support timely referrals for eligible patients [17].
5.0. UTILIZATION OF HOSPICE FOR PATIENTS WITH ESLD
Despite the potential of hospice to improve patients’ and caregivers’ experiences and to reduce healthcare utilization at the end of life, hospice in this population remains underutilized. One study of all decedents in the US found that only 6% of patients with cirrhosis died while enrolled in hospice, a figure considerably lower than that for Medicare beneficiaries in general [132,133]. Another study of hospitalized patients with 50% one-year mortality showed only 18% referred to hospice [130]. Compared to patients who do not enroll in hospice, hospice enrollees are more likely to have HCC and to have a greater comorbidity burden [130,134]. In addition, patients with HCC are more likely to use hospice when they are seen by an oncologist (as opposed to a gastroenterologist) [128]. Together, these findings suggest that concurrent conditions (such as HCC) drive hospice referral decisions for patients with ESLD and that hospice referrals are not driven by the underlying liver disease. For patients with cirrhosis who do enroll in hospice, most enroll very late, a median of 9 days before death [135].
6.0. BARRIERS TO INCREASING HOSPICE UTILIZATION
6.1. Requirement of Forgoing Life-Prolonging Treatment
Under the Medicare hospice benefit, hospices receive a daily payment, which is intended to cover all services provided for the terminal illness. This payment is fixed, regardless of the amount of services provided. Therefore, expensive diagnostics and therapeutics that may prolong life (while also offering palliation) are often not financially feasible in the hospice setting [136]. Examples of such care include blood transfusions, palliative radiation, and chemotherapy [137–139]. In cirrhosis, paracentesis may not be available, and hospices may require placement of a peritoneal catheter prior to enrollment [140]. Patients benefiting from these services therefore often delay hospice enrollment, and this delay accounts in part for the short duration of hospice enrollment among decedents in the US [133].
Whether or not models allowing for non-hospice (even potentially curative) concurrent care can improve patient-reported outcomes or costs remains unclear. Several studies of such models in predominantly cancer populations have shown positive impacts on beneficiary quality of life, as well as potential reductions in intensive care utilization and costs, though robust data are still lacking [141,142]. For patients with ESLD, a pilot study demonstrated the feasibility of providing hospice care to patients actively listed for LT, and this approach was associated with a longer duration of hospice care [143].
6.2. Dealing with Uncertainty
Despite the evidence supporting specific predictors of high short-term mortality and transplant ineligibility, there remains uncertainty that complicates patient end-of-life decisions. This uncertainty not only impacts patients; providers also experience uncertainty in assigning prognosis [28,144]. This uncertainty is well-founded; physicians may remain overly optimistic about prognosis [145]. In addition, the dynamic nature of liver disease can result in shifting prognosis for an individual patient; today’s good prognosis may be tomorrow’s poor prognosis.
Uncertainty may be even greater when considering transplant eligibility factors. Many of the listed contraindications for LT are based on low-quality evidence, and studies assessing factors associated with poor transplant outcomes are hampered by the significant selection bias inherent in post-transplant cohorts [73]. These limitations contribute to the complexity of LT committee decisions, the frequent need for judgment-based reasoning in determining eligibility, and the perception among committee members that the process lacks consistency and fairness [97]. Even when supported by specific criteria for hospice, patients and providers must maintain flexibility as conditions change. Although the Medicare hospice benefit requires that a physician certify a life-expectancy of less than six months, enrollees may revoke the hospice benefit at any time, and enrollees are occasionally discharged from hospice alive [48]. From a transplant standpoint, patients deemed ineligible at one point may be able to address LT barriers at a later date (e.g., improved social support network). Patients ineligible for hospice may also benefit from non-hospice palliative care, which can also facilitate transitions to hospice care when appropriate. Such care can be particularly helpful for patients on the LT waiting list, who have significant palliative care needs, substantial mortality risk, and risk of delisting [146]. Notably, patients and caregivers often confuse hospice care with non-hospice palliative care [46]. Therefore, hospice eligibility criteria can play an important role in guiding decision-making, recognizing that any decisions to pursue hospice need not be final.
6.3. A Lack of Evidence and Guidance
Hospice, and palliative care more generally, has been more broadly adopted for other chronic disease states due in part to a more robust evidence base and resultant endorsement in clinical practice guidelines [147–149]. Until recently, such guidance for ESLD has been lacking, leaving a gap in the “road map” that providers can use to help patients navigate their illness. This gap highlights the urgent need for prospective studies, including randomized trials, to better support the efficacy of both palliative care and hospice in improving patients’ and caregivers’ lives. Indeed, patients and caregivers welcome the opportunity to participate in research on end-of-life care, and such work is needed to cement the role of hospice for this population [150]. Notably, recent gastroenterology society guidelines are just now starting to recognize the roles of both palliative care and hospice [17,151].
6.4. Patient Marginalization
Patients with ESLD are relatively young compared to those with other end-stage diseases, with a high burden of comorbid substance use disorders and a frequent lack of social support [152,153]. This group is therefore vulnerable and marginalized, with a high burden of self-perceived stigma [154]. Such marginalization is a barrier to all medical care, including palliative care and hospice, and certainly serves to reduce hospice utilization for ESLD [155]. Future work should focus on building trust with marginalized communities to improve access to this care.
6.5. Provider Resistance
The complications of ESLD often require hospitalization and intensive care, and such care, focused on disease modification, is often not compatible with symptom control and support for other aspects of advanced disease (Table 1) [156]. Specialists who provide care for this population, often at tertiary care centers, tend to focus less on such supportive care for symptoms and quality of life. Continued attention to the topic of palliative care and hospice, with a growing body of literature, may help shift provider attitudes and practices to bring hospice to more patients when appropriate.
7.0. CONCLUSION
Patients with cirrhosis at the end of life suffer from multiple physical, emotional, social, and spiritual troubles that result in poor quality of life, high caregiver burden, and high rates of healthcare utilization. These issues can be addressed holistically through appropriate hospice care, which leverages the expertise of an interdisciplinary team to deliver comprehensive services focused on patients’ and caregivers’ individual needs. Despite the potential for hospice to benefit this population, it remains underutilized. Barriers to increasing hospice utilization include the requirement to forgo life-prolonging treatment as well as uncertainty in assessing prognosis and transplant eligibility. These factors need to be considered in formulating up-to-date, evidence-based criteria for hospice suitability.
8.0. Expert opinion
As for those with other serious conditions, patients with ESLD and a limited life expectancy can avail themselves of hospice care to support their end-of-life needs and their families. Hospice is well-placed to provide the comprehensive care to address the range of issues facing this population (Table 1). However, in contrast to the cancer population, there are limited data to show how hospice benefits patients with ESLD. More research is necessary in this area to better define the role of hospice in ESLD and how it might positively impact patient-reported outcomes as well as caregiver outcomes. Collection of these outcome measures in combination with hospice-provided services may also help identify which interventions have greatest impact. For example, patients may benefit disproportionately from linkage to community resources to help address the social troubles that are highly prevalent in this population. In turn, hospice for ESLD in the future could be more refined and patient-centered, addressing patients’ unique needs. Beyond individual patients and families, future work also needs to examine how hospice can impact the healthcare system more broadly, including its effects on acute healthcare utilization (e.g., hospitalizations, ED visits) and overall costs.
Current Medicare guidelines for hospice eligibility rely on dated, non-data-driven criteria, lacking contemporary prognostic markers and consideration of LT eligibility. Efforts to increase the appropriate use of hospice must include a better delineation of current, relevant criteria, focused on high short-term mortality and ineligibility for LT. Data-driven development of such criteria are urgently needed to improve healthcare for this vulnerable population. In this review, we have summarized many of the factors that should be considered in this work. Moving forward, it will be important to consider how these factors could be further developed and codified to be useful for clinicians and patients. Of note, many of the proposed factors are not absolute, and considerable uncertainty can remain, even with the best available evidence. In addition to further developing evidence to more accurately assess prognosis, the existing evidence can be used in formal consensus methodology, such as the modified Delphi process, in which expert opinion can help guide the development of hospice criteria. In clinical practice, hospice can also play a more prominent role in transplant committee deliberations, where transplant eligibility is often a primary topic of discussion.
Hospice is woefully underutilized for patients with ESLD, and more work is needed to increase the use of hospice for appropriate patients. In addition to better defining clear criteria for hospice eligibility, increasing awareness of hospice among providers and patients may serve to increase its use. Other work focused on early non-hospice palliative care involvement for ESLD may also offer opportunities for patients to learn about hospice and to establish relationships with providers who can help with the goals of care discussions that are integral to hospice. Indeed, much can be learned from non-hospice palliative care in regards to tackling physical, psychological, and spiritual needs for these patients, and many of the same best practices can applied to those in hospice care. Lastly, the current fixed hospice payment model serves as a barrier for many patients to obtain the complex medical care they need at the end of life. Further work emphasizing concurrent non-hospice care or alternative payment models may help hospice reach more patients at earlier time points, improving care for patients and families and reducing the burden of ESLD on the healthcare system.
Article highlights.
Patients with ESLD near the end of life have numerous physical, emotional, social, and spiritual concerns that can be addressed through high-quality hospice care.
Current liver-specific Medicare hospice eligibility guidelines rely on dated, non-data-driven criteria.
Future hospice criteria for ESLD should be based on accurate, contemporary prognostic markers and liver transplant eligibility.
For patients with ESLD near the end of life, hospice is underutilized, and several barriers exist to increase timely hospice referrals.
Acknowledgments
Funding
This paper was partly funded by the National Institutes of Health under award number K23DK109202. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Declaration of Interests
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer Disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
REFERENCES
Papers of special note have been highlighted as either of interest (*) or of considerable interest (**) to readers.
- [1].Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999–2017 on CDC WONDER Online Database [Internet]. [cited 2020. September 3]. Available from: http://wonder.cdc.gov/ucd-icd10.html.
- [2].Marchesini G, Bianchi G, Amodio P, et al. Factors associated with poor health-related quality of life of patients with cirrhosis. Gastroenterology. 2001;120:170–178. [DOI] [PubMed] [Google Scholar]
- [3].Bajaj JS, Wade JB, Gibson DP, et al. The multi-dimensional burden of cirrhosis and hepatic encephalopathy on patients and caregivers. Am J Gastroenterol. 2011;106:1646–1653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Samoylova ML, Covinsky KE, Haftek M, et al. Disability in patients with end-stage liver disease: Results from the functional assessment in liver transplantation study. Liver Transpl. 2017;23:292–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Orman ES, Ghabril M, Emmett TW, et al. Hospital readmissions in patients with cirrhosis: A systematic review. J Hosp Med. 2018;13:490–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Stepanova M, De Avila L, Afendy M, et al. Direct and Indirect Economic Burden of Chronic Liver Disease in the United States. Clin Gastroenterol Hepatol. 2017;15:759–766.e5. [DOI] [PubMed] [Google Scholar]
- [7].Lupu D, Quigley L, Mehfoud N, et al. The Growing Demand for Hospice and Palliative Medicine Physicians: Will the Supply Keep Up? J Pain Symptom Manag. 2018;55:1216–1223. [DOI] [PubMed] [Google Scholar]
- [8].Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363:733–742. [DOI] [PubMed] [Google Scholar]
- [9].Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. Jama. 2009;302:741–749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Kavalieratos D, Corbelli J, Zhang D, et al. Association Between Palliative Care and Patient and Caregiver Outcomes: A Systematic Review and Meta-analysis. Jama. 2016;316:2104–2114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Mazzarelli C, Prentice WM, Heneghan MA, et al. Palliative care in end-stage liver disease: Time to do better? Liver Transplant. 2018;24:961–968. [DOI] [PubMed] [Google Scholar]
- [12].Low JTS, Rohde G, Pittordou K, et al. Supportive and palliative care in people with cirrhosis: International systematic review of the perspective of patients, family members and health professionals. J Hepatol. 2018;69:1260–1273. [DOI] [PubMed] [Google Scholar]
- [13].Rush B, Walley KR, Celi LA, et al. Palliative care access for hospitalized patients with end-stage liver disease across the United States. Hepatology. 2017;66:1585–1591. [DOI] [PubMed] [Google Scholar]
- [14].Verma M, Kosinski AS, Volk ML, et al. Introducing Palliative Care within the Treatment of End-Stage Liver Disease: The Study Protocol of a Cluster Randomized Controlled Trial. J Palliat Med. 2019;22:34–43. [DOI] [PubMed] [Google Scholar]
- [15].Centers for Medicare & Medicaid Services. Local Coverage Determination (LCD): Hospice - Determining Terminal Status (L33393) [Internet]. Baltimore, MD; 2019. [cited 2020 Sep 3]. Available from: https://www.cms.gov/medicare-coverage-database/details/lcd-details.aspx?LCDId=33393&ver=5&CntrctrSelected=272*1&Cntrctr=272&name=National+Government+Services%2C+Inc.+(06004%2C+HHH+MAC)&DocType=All&s=56&bc=AggAAAIAgAAA&. [Google Scholar]
- [16].Langberg KM, Kapo JM, Taddei TH. Palliative care in decompensated cirrhosis: A review. Liver Int. 2018;38:768–775. [DOI] [PubMed] [Google Scholar]
- [17].Tandon P, Walling A, Patton H, et al. AGA Clinical Practice Update on Palliative Care Management in Cirrhosis: Expert Review. Clin Gastroenterol Hepatol. 2020; [DOI] [PubMed] [Google Scholar]
- [18].Younossi ZM, Boparai N, Price LL, et al. Health-related quality of life in chronic liver disease: the impact of type and severity of disease. Am J Gastroenterol. 2001;96:2199–2205. [DOI] [PubMed] [Google Scholar]
- [19].Orman ES, Ghabril M, Chalasani N. Poor Performance Status Is Associated With Increased Mortality in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2016;14:1189–1195.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Rakoski MO, McCammon RJ, Piette JD, et al. Burden of cirrhosis on older Americans and their families: analysis of the health and retirement study. Hepatology. 2012;55:184–191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Chatrath H, Liangpunsakul S, Ghabril M, et al. Prevalence and morbidity associated with muscle cramps in patients with cirrhosis. Am J Med. 2012;125:1019–1025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Poonja Z, Brisebois A, van Zanten SV, et al. Patients with cirrhosis and denied liver transplants rarely receive adequate palliative care or appropriate management. Clin Gastroenterol Hepatol. 2014;12:692–698. [DOI] [PubMed] [Google Scholar]
- [23].Bunchorntavakul C, Reddy KR. Pruritus in chronic cholestatic liver disease. Clin Liver Dis. 2012;16:331–346. [DOI] [PubMed] [Google Scholar]
- [24].Buganza-Torio E, Mitchell N, Abraldes JG, et al. Depression in cirrhosis – a prospective evaluation of the prevalence, predictors and development of a screening nomogram. Aliment Pharmacol Ther. 2019;49:194–201. [DOI] [PubMed] [Google Scholar]
- [25].Russ TC, Kivimaki M, Morling JR, et al. Association Between Psychological Distress and Liver Disease Mortality: A Meta-analysis of Individual Study Participants. Gastroenterology. 2015;148:958–966.e4. [DOI] [PubMed] [Google Scholar]
- [26].Scaglione S, Kliethermes S, Cao G, et al. The Epidemiology of Cirrhosis in the United States: A Population-based Study. J Clin Gastroenterol. 2015;49:690–696. [DOI] [PubMed] [Google Scholar]
- [27].Nguyen DL, Chao D, Ma G, et al. Quality of life and factors predictive of burden among primary caregivers of chronic liver disease patients. Ann Gastroenterol. 2015;28:124–129. [PMC free article] [PubMed] [Google Scholar]
- [28].Kimbell B, Boyd K, Kendall M, et al. Managing uncertainty in advanced liver disease: a qualitative, multiperspective, serial interview study. BMJ Open. 2015;5:e009241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Kunzler-Heule P, Beckmann S, Mahrer-Imhof R, et al. Being an informal caregiver for a relative with liver cirrhosis and overt hepatic encephalopathy: a phenomenological study. J Clin Nurs. 2016;25:2559–2568. [DOI] [PubMed] [Google Scholar]
- [30].Peng JK, Hepgul N, Higginson IJ, et al. Symptom prevalence and quality of life of patients with end-stage liver disease: A systematic review and meta-analysis. Palliat Med. 2019;33:24–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].De Ledinghen V, Heresbach D, Fourdan O, et al. Anti-inflammatory drugs and variceal bleeding: a case-control study. Gut. 1999;44:270–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Wong F, Massie D, Hsu P, et al. Indomethacin-induced renal dysfunction in patients with well-compensated cirrhosis. Gastroenterology. 1993;104:869–876. [DOI] [PubMed] [Google Scholar]
- [33].Moon AM, Jiang Y, Rogal SS, et al. Opioid prescriptions are associated with hepatic encephalopathy in a national cohort of patients with compensated cirrhosis. Aliment Pharmacol Ther. 2020;51:652–660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Cheng Y-W, Sandrasegaran K, Cheng K, et al. A dedicated paracentesis clinic decreases healthcare utilization for serial paracenteses in decompensated cirrhosis. Abdom Radiol (New York). 2018;43:2190–2197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Macken L, Bremner S, Gage H, et al. Randomised clinical trial: palliative long-term abdominal drains vs large-volume paracentesis in refractory ascites due to cirrhosis. Aliment Pharmacol Ther. 2020;52:107–122. [DOI] [PubMed] [Google Scholar]
- [36].Cooper M, Pollard A, Pandey A, et al. Palliative Long-Term Abdominal Drains Versus Large Volume Paracentesis in Refractory Ascites Due to Cirrhosis (REDUCe Study): Qualitative Outcomes. J Pain Symptom Manage. 2020; [DOI] [PubMed] [Google Scholar]
- [37].Caldwell J, Edriss H, Nugent K. Chronic peritoneal indwelling catheters for the management of malignant and nonmalignant ascites. Proc (Bayl Univ Med Cent). 2018;31:297–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Casadaban LC, Parvinian A, Couture PM, et al. Characterization of liver function parameter alterations after transjugular intrahepatic portosystemic shunt creation and association with early mortality. Am J Roentgenol. 2014;203:1363–1370. [DOI] [PubMed] [Google Scholar]
- [39].Riggio O, Nardelli S, Moscucci F, et al. Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt. Clin Liver Dis. 2012;16:133–146. [DOI] [PubMed] [Google Scholar]
- [40].Sharma BC, Sharma P, Agrawal A, et al. Secondary prophylaxis of hepatic encephalopathy: an open-label randomized controlled trial of lactulose versus placebo. Gastroenterology. 2009;137:885–891, 891.e1. [DOI] [PubMed] [Google Scholar]
- [41].Singh GK, Hoyert DL. Social epidemiology of chronic liver disease and cirrhosis mortality in the United States, 1935-1997: trends and differentials by ethnicity, socioeconomic status, and alcohol consumption. Hum Biol. 2000;72:801–820. [PubMed] [Google Scholar]
- [42].Puchalski C, Ferrell B, Virani R, et al. Improving the quality of spiritual care as a dimension of palliative care: the report of the Consensus Conference. J Palliat Med. 2009;12:885–904. [DOI] [PubMed] [Google Scholar]
- [43].Hareendran A, Devadas K, Sreesh S, et al. Quality of life, caregiver burden and mental health disorders in primary caregivers of patients with Cirrhosis. Liver Int Off J Int Assoc Study Liver. 2020 [DOI] [PubMed] [Google Scholar]
- [44].Fabrellas N, Moreira R, Carol M, et al. Psychological Burden of Hepatic Encephalopathy on Patients and Caregivers. Clin Transl Gastroenterol. 2020;11:e00159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Hansen L, Chang MF, Lee CS, et al. Physical and Mental Quality of Life in Patients With End-Stage Liver Disease and Their Informal Caregivers. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2021;19:155–161.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Donlan J, Ufere NN, Indriolo T, et al. Patient and Caregiver Perspectives on Palliative Care in End-Stage Liver Disease. J Palliat Med. 2020; [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Stroebe M, Schut H, Stroebe W. Health outcomes of bereavement. Lancet. 2007;370:1960–1973. [DOI] [PubMed] [Google Scholar]
- [48].Johnson KS, Kuchibhatla M, Tanis D, et al. Racial differences in hospice revocation to pursue aggressive care. Arch Intern Med. 2008;168:218–224. [DOI] [PubMed] [Google Scholar]
- [49].Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. [DOI] [PubMed] [Google Scholar]
- [50].Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124:91–96. [DOI] [PubMed] [Google Scholar]
- [51].Mishra P, Desai N, Alexander J, et al. Applicability of MELD as a short-term prognostic indicator in patients with chronic liver disease: an Indian experience. J Gastroenterol Hepatol. 2007;22:1232–1235. [DOI] [PubMed] [Google Scholar]
- [52].Kim WR, Biggins SW, Kremers WK, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359:1018–1026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Jalan R, Saliba F, Pavesi M, et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. J Hepatol. 2014;61:1038–1047. [DOI] [PubMed] [Google Scholar]
- [54].Bajaj JS, O’Leary JG, Reddy KR, et al. Survival in infection-related acute-on-chronic liver failure is defined by extrahepatic organ failures. Hepatology. 2014;60:250–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Salerno F, Cammà C, Enea M, et al. Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites: A Meta-analysis of Individual Patient Data. Gastroenterology. 2007;133:825–834. [DOI] [PubMed] [Google Scholar]
- [56].Fede G, D’Amico G, Arvaniti V, et al. Renal failure and cirrhosis: A systematic review of mortality and prognosis. J Hepatol. 2012;56:810–818. [DOI] [PubMed] [Google Scholar]
- [57].Schenk P, Schoniger-Hekele M, Fuhrmann V, et al. Prognostic significance of the hepatopulmonary syndrome in patients with cirrhosis. Gastroenterology. 2003;125:1042–1052. [DOI] [PubMed] [Google Scholar]
- [58].Lai JC, Rahimi RS, Verna EC, et al. Frailty Associated With Waitlist Mortality Independent of Ascites and Hepatic Encephalopathy in a Multicenter Study. Gastroenterology. 2019;156:1675–1682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Durand F, Buyse S, Francoz C, et al. Prognostic value of muscle atrophy in cirrhosis using psoas muscle thickness on computed tomography. J Hepatol. 2014;60:1151–1157. [DOI] [PubMed] [Google Scholar]
- [60].Montano-Loza AJ, Meza-Junco J, Prado CM, et al. Muscle wasting is associated with mortality in patients with cirrhosis. Clin Gastroenterol Hepatol. 2012;10:166–173, 173.e1. [DOI] [PubMed] [Google Scholar]
- [61].Carey EJ, Lai JC, Wang CW, et al. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl. 2017;23:625–633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [62].Hudson BE, Ameneshoa K, Gopfert A, et al. Integration of palliative and supportive care in the management of advanced liver disease: development and evaluation of a prognostic screening tool and supportive care intervention. Frontline Gastroenterol. 2017;8:45–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Highet G, Crawford D, Murray SA, et al. Development and evaluation of the Supportive and Palliative Care Indicators Tool (SPICT): a mixed-methods study. BMJ Support Palliat Care. 2014;4:285–290. [DOI] [PubMed] [Google Scholar]
- [64].Said A, Williams J, Holden J, et al. Model for end stage liver disease score predicts mortality across a broad spectrum of liver disease. J Hepatol. 2004;40:897–903. [DOI] [PubMed] [Google Scholar]
- [65].Nagai S, Chau LC, Schilke RE, et al. Effects of Allocating Livers for Transplantation Based on Model for End-Stage Liver Disease-Sodium Scores on Patient Outcomes. Gastroenterology. 2018;155:1451–1462.e3. [DOI] [PubMed] [Google Scholar]
- [66].Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60:646–649. [DOI] [PubMed] [Google Scholar]
- [67].Infante-Rivard C, Esnaola S, Villeneuve JP. Clinical and statistical validity of conventional prognostic factors in predicting short-term survival among cirrhotics. Hepatology. 1987;7:660–664. [DOI] [PubMed] [Google Scholar]
- [68].Hernaez R, Solà E, Moreau R, et al. Acute-on-chronic liver failure: an update. Gut. 2017;66:541–553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Salerno F, Borroni G, Moser P, et al. Survival and prognostic factors of cirrhotic patients with ascites: a study of 134 outpatients. Am J Gastroenterol. 1993;88:514–519. [PubMed] [Google Scholar]
- [70].Gines P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009;361:1279–1290. [DOI] [PubMed] [Google Scholar]
- [71].Angeli P, Ginès P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. J Hepatol. 2015;62:968–974. [DOI] [PubMed] [Google Scholar]
- [72].Fallon MB, Krowka MJ, Brown RS, et al. Impact of hepatopulmonary syndrome on quality of life and survival in liver transplant candidates. Gastroenterology. 2008;135:1168–1175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Martin P, DiMartini A, Feng S, et al. Evaluation for liver transplantation in adults: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Hepatology. 2014;59:1144–1165. [DOI] [PubMed] [Google Scholar]
- [74].Lai JC, Sonnenday CJ, Tapper EB, et al. Frailty in liver transplantation: An expert opinion statement from the American Society of Transplantation Liver and Intestinal Community of Practice. Am J Transplant. 2019;19:1896–1906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Carey EJ, Steidley DE, Aqel BA, et al. Six-minute walk distance predicts mortality in liver transplant candidates. Liver Transpl. 2010;16:1373–1378. [DOI] [PubMed] [Google Scholar]
- [76].Lai JC, Feng S, Terrault NA, et al. Frailty predicts waitlist mortality in liver transplant candidates. Am J Transpl. 2014;14:1870–1879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Lai JC, Covinsky KE, Dodge JL, et al. Development of a novel frailty index to predict mortality in patients with end-stage liver disease. Hepatology. 2017;66:564–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [78].Tapper EB, Finkelstein D, Mittleman MA, et al. Standard assessments of frailty are validated predictors of mortality in hospitalized patients with cirrhosis. Hepatology. 2015;62:584–590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [79].Tandon P, Reddy KR, O’Leary JG, et al. A Karnofsky performance status-based score predicts death after hospital discharge in patients with cirrhosis. Hepatology. 2017;65:217–224. [DOI] [PubMed] [Google Scholar]
- [80].Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [81].van Vugt JL, Levolger S, de Bruin RW, et al. Systematic Review and Meta-Analysis of the Impact of Computed Tomography-Assessed Skeletal Muscle Mass on Outcome in Patients Awaiting or Undergoing Liver Transplantation. Am J Transpl. 2016;16:2277–2292. [DOI] [PubMed] [Google Scholar]
- [82].Plotkin JS, Scott VL, Pinna A, et al. Morbidity and mortality in patients with coronary artery disease undergoing orthotopic liver transplantation. Liver Transpl Surg. 1996;2:426–430. [DOI] [PubMed] [Google Scholar]
- [83].Ripoll C, Yotti R, Bermejo J, et al. The heart in liver transplantation. J Hepatol. 2011;54:810–822. [DOI] [PubMed] [Google Scholar]
- [84].Krowka MJ, Plevak DJ, Findlay JY, et al. Pulmonary hemodynamics and perioperative cardiopulmonary-related mortality in patients with portopulmonary hypertension undergoing liver transplantation. Liver Transplant. 2000;6:443–450. [DOI] [PubMed] [Google Scholar]
- [85].Kia L, Cuttica MJ, Yang A, et al. The utility of pulmonary function testing in predicting outcomes following liver transplantation. Liver Transpl. 2016;22:805–811. [DOI] [PubMed] [Google Scholar]
- [86].Spengler EK, O’Leary JG, Te HS, et al. Liver Transplantation in the Obese Cirrhotic Patient. Transplantation. 2017;101:2288–2296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [87].Tandon P, Goodman KJ, Ma MM, et al. A shorter duration of pre-transplant abstinence predicts problem drinking after liver transplantation. Am J Gastroenterol. 2009;104:1700–1706. [DOI] [PubMed] [Google Scholar]
- [88].Pfitzmann R, Schwenzer J, Rayes N, et al. Long-term survival and predictors of relapse after orthotopic liver transplantation for alcoholic liver disease. Liver Transpl. 2007;13:197–205. [DOI] [PubMed] [Google Scholar]
- [89].Laederach-Hofmann K, Bunzel B. Noncompliance in organ transplant recipients: a literature review. Gen Hosp Psychiatry. 2000;22:412–424. [DOI] [PubMed] [Google Scholar]
- [90].Douglas S, Blixen C, Bartucci MR. Relationship between pretransplant noncompliance and posttransplant outcomes in renal transplant recipients. J Transpl Coord. 1996;6:53–58. [DOI] [PubMed] [Google Scholar]
- [91].Sapisochin G, Fidelman N, Roberts JP, et al. Mixed hepatocellular cholangiocarcinoma and intrahepatic cholangiocarcinoma in patients undergoing transplantation for hepatocellular carcinoma. Liver Transpl. 2011;17:934–942. [DOI] [PubMed] [Google Scholar]
- [92].Penn I Evaluation of transplant candidates with pre-existing malignancies. Ann Transpl. 1997;2:14–17. [PubMed] [Google Scholar]
- [93].Bouscarat F, Samuel D, Simon F, et al. An observational study of 11 French liver transplant recipients infected with human immunodeficiency virus type 1. Clin Infect Dis. 1994;19:854–859. [DOI] [PubMed] [Google Scholar]
- [94].Beauchamp TL, Childress JF. Principles of biomedical ethics. Oxford University Press, USA; 2001. [Google Scholar]
- [95].Organ Procurement and Transplantation Network Policies [Internet]. 2020. [cited 2020 May 16]. Available from: https://optn.transplant.hrsa.gov/media/1200/optn_policies.pdf. [Google Scholar]
- [96].Keller EJ, Kwo PY, Helft PR. Ethical considerations surrounding survival benefit-based liver allocation. Liver Transpl. 2014;20:140–146. [DOI] [PubMed] [Google Scholar]
- [97].Volk ML, Biggins SW, Huang MA, et al. Decision making in liver transplant selection committees: a multicenter study. Ann Intern Med. 2011;155:503–508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [98].Smilowitz NR, Gupta N, Ramakrishna H, et al. Perioperative Major Adverse Cardiovascular and Cerebrovascular Events Associated With Noncardiac Surgery. JAMA Cardiol. 2017;2:181–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [99].Maddur H, Bourdillon PD, Liangpunsakul S, et al. Role of cardiac catheterization and percutaneous coronary intervention in the preoperative assessment and management of patients before orthotopic liver transplantation. Liver Transpl. 2014;20:664–672. [DOI] [PubMed] [Google Scholar]
- [100].Krowka MJ, Fallon MB, Kawut SM, et al. International Liver Transplant Society Practice Guidelines: Diagnosis and Management of Hepatopulmonary Syndrome and Portopulmonary Hypertension. Transplantation. 2016;100:1440–1452. [DOI] [PubMed] [Google Scholar]
- [101].Hollatz TJ, Musat A, Westphal S, et al. Treatment with sildenafil and treprostinil allows successful liver transplantation of patients with moderate to severe portopulmonary hypertension. Liver Transpl. 2012;18:686–695. [DOI] [PubMed] [Google Scholar]
- [102].Bambha KM, Dodge JL, Gralla J, et al. Low, rather than high, body mass index confers increased risk for post-liver transplant death and graft loss: Risk modulated by model for end-stage liver disease. Liver Transpl. 2015;21:1286–1294. [DOI] [PubMed] [Google Scholar]
- [103].Mosko JD, Nguyen GC. Increased perioperative mortality following bariatric surgery among patients with cirrhosis. Clin Gastroenterol Hepatol. 2011;9:897–901. [DOI] [PubMed] [Google Scholar]
- [104].Zamora-Valdes D, Watt KD, Kellogg TA, et al. Long-term outcomes of patients undergoing simultaneous liver transplantation and sleeve gastrectomy. Hepatology. 2018;68:485–495. [DOI] [PubMed] [Google Scholar]
- [105].Gomez Gavara C, Esposito F, Gurusamy K, et al. Liver transplantation in elderly patients: a systematic review and first meta-analysis. HPB. 2019;21:14–25. [DOI] [PubMed] [Google Scholar]
- [106].Sundaram V, Lim J, Tholey DM, et al. The Braden Scale, A standard tool for assessing pressure ulcer risk, predicts early outcomes after liver transplantation. Liver Transpl. 2017;23:1153–1160. [DOI] [PubMed] [Google Scholar]
- [107].Thuluvath PJ, Thuluvath AJ, Savva Y. Karnofsky performance status before and after liver transplantation predicts graft and patient survival. J Hepatol. 2018;69:818–825. [DOI] [PubMed] [Google Scholar]
- [108].Mathurin P, Moreno C, Samuel D, et al. Early liver transplantation for severe alcoholic hepatitis. N Engl J Med. 2011;365:1790–1800. [DOI] [PubMed] [Google Scholar]
- [109].Im GY, Kim-Schluger L, Shenoy A, et al. Early Liver Transplantation for Severe Alcoholic Hepatitis in the United States--A Single-Center Experience. Am J Transpl. 2016;16:841–849. [DOI] [PubMed] [Google Scholar]
- [110].Ladin K, Daniels A, Osani M, et al. Is social support associated with post-transplant medication adherence and outcomes? A systematic review and meta-analysis. Transpl Rev. 2018;32:16–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [111].Ladin K, Emerson J, Berry K, et al. Excluding patients from transplant due to social support: Results from a national survey of transplant providers. Am J Transpl. 2019;19:193–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [112].Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68:723–750. [DOI] [PubMed] [Google Scholar]
- [113].Shaib YH, El-Serag HB, Davila JA, et al. Risk factors of intrahepatic cholangiocarcinoma in the United States: a case-control study. Gastroenterology. 2005;128:620–626. [DOI] [PubMed] [Google Scholar]
- [114].Watt KD, Pedersen RA, Kremers WK, et al. Long-term probability of and mortality from de novo malignancy after liver transplantation. Gastroenterology. 2009;137:2010–2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [115].Miao Y, Everly JJ, Gross TG, et al. De novo cancers arising in organ transplant recipients are associated with adverse outcomes compared with the general population. Transplantation. 2009;87:1347–1359. [DOI] [PubMed] [Google Scholar]
- [116].McElroy LM, Daud A, Davis AE, et al. A meta-analysis of complications following deceased donor liver transplant. Am J Surg. 2014;208:605–618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [117].Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. Jama. 2004;291:88–93. [DOI] [PubMed] [Google Scholar]
- [118].Wallston KA, Burger C, Smith RA, et al. Comparing the quality of death for hospice and non-hospice cancer patients. Med Care. 1988;26:177–182. [DOI] [PubMed] [Google Scholar]
- [119].Wright AA, Keating NL, Balboni TA, et al. Place of death: correlations with quality of life of patients with cancer and predictors of bereaved caregivers’ mental health. J Clin Oncol. 2010;28:4457–4464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [120].Obermeyer Z, Makar M, Abujaber S, et al. Association between the Medicare hospice benefit and health care utilization and costs for patients with poor-prognosis cancer. Jama. 2014;312:1888–1896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [121].Connor SR, Pyenson B, Fitch K, et al. Comparing hospice and nonhospice patient survival among patients who die within a three-year window. J Pain Symptom Manage. 2007;33:238–246. [DOI] [PubMed] [Google Scholar]
- [122].Teno JM, Shu JE, Casarett D, et al. Timing of referral to hospice and quality of care: length of stay and bereaved family members’ perceptions of the timing of hospice referral. J Pain Symptom Manage. 2007;34:120–125. [DOI] [PubMed] [Google Scholar]
- [123].Gelfman LP, Barrón Y, Moore S, et al. Predictors of Hospice Enrollment for Patients With Advanced Heart Failure and Effects on Health Care Use. JACC Heart Fail. 2018;6:780–789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [124].Wachterman MW, Hailpern SM, Keating NL, et al. Association Between Hospice Length of Stay, Health Care Utilization, and Medicare Costs at the End of Life Among Patients Who Received Maintenance Hemodialysis. JAMA Intern Med. 2018;178:792–799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [125].Richards CA, Hebert PL, Liu C-F, et al. Association of Family Ratings of Quality of End-of-Life Care With Stopping Dialysis Treatment and Receipt of Hospice Services. JAMA Netw open. 2019;2:e1913115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [126].Hwang SJ, Chang HT, Hwang IH, et al. Hospice offers more palliative care but costs less than usual care for terminal geriatric hepatocellular carcinoma patients: a nationwide study. J Palliat Med. 2013;16:780–785. [DOI] [PubMed] [Google Scholar]
- [127].Chiang JK, Kao YH. The impact of hospice care on survival and cost saving among patients with liver cancer: a national longitudinal population-based study in Taiwan. Support Care Cancer. 2015;23:1049–1055. [DOI] [PubMed] [Google Scholar]
- [128].Sanoff HK, Chang Y, Reimers M, et al. Hospice Utilization and Its Effect on Acute Care Needs at the End of Life in Medicare Beneficiaries With Hepatocellular Carcinoma. J Oncol Pr. 2017;13:e197–e206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [129].Fukui N, Golabi P, Otgonsuren M, et al. Hospice care in Medicare patients with primary liver cancer: the impact on resource utilisation and mortality. Aliment Pharmacol Ther. 2018;47:680–688. [DOI] [PubMed] [Google Scholar]
- **[130].Holden JH, Shamseddeen H, Johnson AW, et al. Palliative Care and Hospice Referrals in Patients with Decompensated Cirrhosis: What Factors Are Important? J Palliat Med. 2020;23:1066–1075. [DOI] [PMC free article] [PubMed] [Google Scholar]; Hospice care for patients with ESLD is delivered infrequently, late, and often only in those with concomitant hepatocellular carcinoma.
- [131].Baumann AJ, Wheeler DS, James M, et al. Benefit of Early Palliative Care Intervention in End-Stage Liver Disease Patients Awaiting Liver Transplantation. J Pain Symptom Manag. 2015;50:882–886.e2. [DOI] [PubMed] [Google Scholar]
- [132].Altaii H, Al-Kindi SG, Yaqoob Z, et al. Place of Death and Hospice Utilization Among Patients Who Die From Cirrhosis in the United States. Clin Gastroenterol Hepatol. 2018;16:142–143. [DOI] [PubMed] [Google Scholar]
- [133].Teno JM, Gozalo P, Trivedi AN, et al. Site of death, place of care, and health care transitions among US medicare beneficiaries, 2000–2015. JAMA - J Am Med Assoc. 2018;320:264–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *[134].Ufere NN, Halford JL, Caldwell J, et al. Health Care Utilization and End-of-Life Care Outcomes for Patients With Decompensated Cirrhosis Based on Transplant Candidacy. J Pain Symptom Manage. 2020;59:590–598. [DOI] [PMC free article] [PubMed] [Google Scholar]; Patients with ESLD have substantial healthcare utilization during the last year of life.
- [135].Brown CL, Hammill BG, Qualls LG, et al. Significant Morbidity and Mortality Among Hospitalized End-Stage Liver Disease Patients in Medicare. J Pain Symptom Manag. 2016;52:412–419.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [136].Wright A, Katz I. Letting Go of the Rope — Aggressive Treatment, Hospice Care, and Open Access. N Engl J Med. 2007;357:324–327. [DOI] [PubMed] [Google Scholar]
- [137].LeBlanc TW, Egan PC, Olszewski AJ. Transfusion dependence, use of hospice services, and quality of end-of-life care in leukemia. Blood. 2018;132:717–726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [138].Yeung HN, Mitchell WM, Roeland EJ, et al. Palliative radiation before hospice: The long and the short of it. J Pain Symptom Manage. 2014;48:1070–1079. [DOI] [PubMed] [Google Scholar]
- [139].Wright AA, Zhang B, Keating NL, et al. Associations between palliative chemotherapy and adult cancer patients’ end of life care and place of death: Prospective cohort study. BMJ. 2014;348:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [140].Zama IN, Edgar M. Management of Symptomatic Ascites in Hospice Patients With Paracentesis: A Case Series Report. Am J Hosp Palliat Med. 2012;29:405–408. [DOI] [PubMed] [Google Scholar]
- [141].Mor V, Wagner TH, Levy C, et al. Association of Expanded VA Hospice Care With Aggressive Care and Cost for Veterans With Advanced Lung Cancer. JAMA Oncol. 2019;5:810–816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [142].Sheedy C, Christopher L, Booker C, et al. Evaluation of the Medicare Care Choices Model: Annual Report 2 [Internet]. Rockville, MD; 2020. Available from: https://downloads.cms.gov/files/mccm-secannrpt.pdf. [Google Scholar]
- **[143].Medici V, Rossaro L, Wegelin JA, et al. The utility of the model for end-stage liver disease score: A reliable guide for liver transplant candidacy and, for select patients, simultaneous hospice referral. Liver Transplant. 2008;14:1100–1106. [DOI] [PubMed] [Google Scholar]; Hospice care can be delivered successfully concurrent with LT evaluation and waitlisting in the US.
- [144].Low J, Davis S, Vickerstaff V, et al. Advanced chronic liver disease in the last year of life: a mixed methods study to understand how care in a specialist liver unit could be improved. BMJ Open. 2017;7:e016887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [145].Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: prospective cohort study. Bmj. 2000;320:469–472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [146].Vijeratnam SS, Candy B, Craig R, et al. Palliative Care for Patients with End-Stage Liver Disease on the Liver Transplant Waiting List: An International Systematic Review. Dig Dis Sci. 2021; [DOI] [PubMed] [Google Scholar]
- [147].Allen LA, Stevenson LW, Grady KL, et al. Decision making in advanced heart failure: a scientific statement from the American Heart Association. Circulation. 2012;125:1928–1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [148].Braun LT, Grady KL, Kutner JS, et al. Palliative Care and Cardiovascular Disease and Stroke: A Policy Statement From the American Heart Association/American Stroke Association. Circulation. 2016;134:e198–e225. [DOI] [PubMed] [Google Scholar]
- [149].Ferrell BR, Temel JS, Temin S, et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35:96–112. [DOI] [PubMed] [Google Scholar]
- [150].Higginson IJ, Evans CJ, Grande G, et al. Evaluating complex interventions in End of Life Care: the MORECare Statement on good practice generated by a synthesis of transparent expert consultations and systematic reviews. BMC Med. 2013;11:111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [151].Aithal GP, Palaniyappan N, China L, et al. Guidelines on the management of ascites in cirrhosis. Gut. 2021;70:9 LP – 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [152].Tapper EB, Parikh ND. Mortality due to cirrhosis and liver cancer in the United States, 1999–2016: Observational study. BMJ. 2018;362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [153].Dang K, Hirode G, Singal AK, et al. Alcoholic Liver Disease Epidemiology in the United States: A Retrospective Analysis of 3 US Databases. Am J Gastroenterol. 2020;115:96–104. [DOI] [PubMed] [Google Scholar]
- [154].Vaughn-Sandler V, Sherman C, Aronsohn A, et al. Consequences of perceived stigma among patients with cirrhosis. Dig Dis Sci. 2014;59:681–686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [155].Stienstra D, Chochinov HM. Palliative care for vulnerable populations. Palliat Support Care. 2012;10:37–42. [DOI] [PubMed] [Google Scholar]
- *[156].Hudson B, Hunt V, Waylen A, et al. The incompatibility of healthcare services and end-of-life needs in advanced liver disease: A qualitative interview study of patients and bereaved carers. Palliat Med. 2018;32:908–918. [DOI] [PubMed] [Google Scholar]; The needs of patients with ESLD at the end of life and their caregivers cannot be met with the current healthcare services available to them.