

ABSTRACT
Background
Previous diet findings in Hispanics/Latinos rarely reflect differences in commonly consumed and culturally relevant foods across heritage groups and by years lived in the United States.
Objectives
We aimed to identify and compare a posteriori heritage-specific dietary patterns (DPs) and evaluate their associations with “healthfulness” [using the Alternative Healthy Eating Index–2010 (AHEI-2010)] and years living in the United States.
Methods
We used baseline data from a population-based cohort of 14,099 Hispanics/Latinos aged 18–74 y in the Hispanic Community Health Study/Study of Latinos. We performed principal factor analysis using two 24-h recalls to derive DPs, separately, in each heritage group (Cuban, Dominican, Mexican, Puerto Rican, Central American, and South American), and identified overarching DPs based on high-loading foods shared by ≥2 groups. We used multivariable linear regression to test associations of DPs with AHEI-2010 and years living in the United States.
Results
We identified 5 overarching DPs (Burgers, Fries, & Soft Drinks; White Rice, Beans, & Red Meats; Fish; Egg & Cheese; and Alcohol). All Burgers, Fries, & Soft Drinks DPs were inversely associated with AHEI-2010, whereas all Fish DPs (except Dominican) were positively associated with this index (all P-trend < 0.001). White Rice, Beans, & Red Meats DPs showed inverse associations in Cuban and Central American groups and positive associations in Mexican-origin individuals (all P-trend < 0.001). Fewer years living in the United States was associated with higher scores for White Rice, Beans, & Red Meats DPs in Cuban and Mexican heritage groups and lower scores on Burgers, Fries, & Soft Drinks DPs in Cuban, Mexican, and Puerto Rican groups (all P-trend < 0.01).
Conclusions
Our findings show substantial variation in DPs across Hispanics/Latinos and adherence to DPs by time in the United States, which could inform dietary interventions targeting this diverse US population. This trial was registered at clinicaltrials.gov as NCT02060344.
Keywords: diet, dietary patterns, a posteriori, heritage, nativity, Hispanics/Latinos, HCHS/SOL, dietary acculturation, principal factor analysis
See corresponding editorial on page 2505.
Introduction
In the United States, ∼20% of individuals are Hispanic/Latino (1). The term “Hispanic/Latino” encompasses >20 nationalities with substantial social, cultural, behavioral, geographic, and genetic heterogeneity (2–4). Hispanics/Latinos constitute the largest US ethnic minority (1), and the population as a whole is projected to double by 2060 (5). Compared to non-Hispanic whites, Hispanics/Latinos are disproportionately affected by cardiometabolic conditions such as obesity and diabetes (6, 7). Among US Hispanics/Latinos, obesity and type 2 diabetes disparities have also been documented by heritage (8, 9). For instance, Hispanics/Latinos of Mexican and Puerto Rican heritage had the highest diabetes prevalence (both 18%), whereas those of South American heritage had the lowest (10%) (8). Identifying effective strategies against chronic disease development tailored to different groups in this diverse US population is therefore warranted.
Diet is strongly linked to health but has been shown to vary across US Hispanics/Latinos. For instance, dietary differences by heritage have been documented at the component level (foods/nutrients) (10, 11) in Hispanics/Latinos, but unlike dietary patterns (DPs), these do not comprehensively and realistically reflect the way people eat, considering foods and nutrients are consumed together (12). Other studies have used a priori, or predefined, DPs based on other populations (13, 14), but these may not necessarily capture commonly consumed and culturally relevant foods, possibly missing important dietary aspects relevant to health among Hispanics/Latinos. A posteriori (data-driven) approaches such as exploratory factor analysis empirically derive DPs typically using foods specific to the population under study (15). The scarce a posteriori diet findings in Hispanics/Latinos, however, have been specific to those of Mexican and Puerto Rican heritage and may not generalize to other heritage groups (16, 17). No study has compared a posteriori DPs across heritage, which may provide insights about differences in dietary behaviors and diet compositions across this diverse population.
Immigrants from Latin America and the Caribbean comprise 50% of the foreign-born population living in the United States (18). Hispanics/Latinos are also the second-largest immigrant group (34%) in the United States, carrying with them dietary preferences and behaviors developed in their country of origin. Over time, however, these dietary practices may be replaced with those of the host country (19–21). For instance, as foreign-born Hispanics/Latinos spend more time living in the United States, studies suggest they undergo an acculturation process in which they lose health-protective aspects of their culture and adopt US “American” or “Western” diet (dietary acculturation) and other obesogenic behaviors (22–24). Indeed, greater years living in the United States has generally been associated with higher intakes of obesogenic dietary components (e.g., fast food, snacks, added fats, added sugars) and lower intakes of those characteristically traditional or healthy (e.g., corn tortillas, fiber, β-carotene) (20, 22, 25–28). The few studies evaluating a posteriori findings by years living in the United States have been specific to Hispanics/Latinos of Mexican (17) and Puerto Rican (29) heritage and generally show greater years in the United States associated with lower adherence to a characteristically traditional DP and higher adherence to a characteristically obesogenic DP. Determining whether patterning is similar in other heritage groups warrants evaluation.
This study fills important gaps in the literature by addressing the following objectives: 1) compare heritage-specific diets across 6 large Hispanic/Latino heritage groups (Cuban, Dominican, Mexican, Puerto Rican, Central American, and South American); 2) assess whether heritage-specific diets correlate with a measure of “healthfulness” using the Alternative Healthy Eating Index–2010 (AHEI-2010), a diet quality indicator; and 3) examine differences in DP scores (dietary adherence) by years living in the United States in each heritage group.
Methods
Study population
The Hispanic Community Health Study/Study of Latinos (HCHS/SOL) is a population-based, multisite cohort study of 16,415 Hispanic/Latino adults living in 4 US field sites (Bronx, New York; Chicago, Illinois; Miami, Florida; and San Diego, California) with baseline examinations (2008–2011) and annual telephone follow-up assessments (30). Recruitment included a stratified 2-stage probability representative sample of households at each center site (31). Individuals from selected households were contacted and screened for eligibility (living in the household, aged 18–74 y, ability to attend a clinic visit for baseline data collection, and not planning to move from the study area within 6 mo). Of the 16,415, we excluded participants who did not self-identify as a member of 1 of the 6 larger heritage groups (Cuban, Dominican, Mexican, Puerto Rican, Central American, and South American) in HCHS/SOL (n = 650) or had missing data on heritage (n = 87). In addition, we excluded participants if they had any missing or only 1 dietary recall (n = 85 and n = 762, respectively), had any recalls with implausible energy intakes (<1st or >99th sex-specific HCHS/SOL percentiles) or recalls deemed unreliable by the interviewer (n = 681), or had missing data on education (n = 14) or years living in the United States (n = 37). Figure 1 displays a flowchart of HCHS/SOL study participants for overall and heritage-specific analytic samples. Approval by the institutional review boards from all participating institutions involved in the study and written consent from all participants were received.
FIGURE 1.

Flowchart of baseline study participants overall and by heritage in HCHS/SOL. Estimated energy intake was <1st or >99th sex-specific percentiles in HCHS/SOL or deemed unreliable by the interviewer. HCHS/SOL, Hispanic Community Health Study/Study of Latinos.
Sociodemographics
Questionnaires were interviewer-administered in either Spanish or English. Hispanic/Latino heritage was self-reported from a list of cultural origin/descendent groups, including Cuban, Dominican, Mexican, Puerto Rican, Central American, South American, more than one heritage, and other. Other self-reported data collected included age at time of examination (years), sex (men, women), highest education achieved (less than high school diploma, high school or equivalent, or greater than high school), lived years in the United States, and place of birth/nativity (US-born including 50 states and District of Columbia/foreign-born) (32). For this analysis, we combined nativity and years living in the United States to form a more nuanced variable representing time in the United States (<10 y, ≥10 y, and US-born) (20).
Dietary assessment and food group formation
Two nonconsecutive 24-h recalls were administered in person at baseline (first interview) and via telephone ≤30 d from baseline (second interview) in the participant's preferred language (English or Spanish) by trained interviewers using the Nutrition Data System for Research (NDS-R) software (version 11), which includes the multiple-pass method (33), food-amounts booklet, and food models for estimating portion sizes. The NDS-R database includes thousands of common foods, brand-name products, and Hispanic/Latino foods, and it provides values for nutrients, food-group serving counts, and other food components. Participants were given a food-amounts booklet to estimate portion sizes during the subsequent telephone interview.
We formed 35 food groups based on nutritional, cultural, and behavioral relevance; previous work (e.g., corn-based foods, burgers, meat and vegetable stews) (17, 22, 34); and consumption patterns in the data (Table 1). We grouped ingredients (e.g., corn tortilla, beef, onion) constituting a recipe (e.g., taco) and same-named nonrecipe foods to reflect real eating behaviors. To maintain consistent food group assignment across heritage, recipes with overlapping food groups (e.g., rice and beans) were not disaggregated. Instead, we labeled these recipes under the food group best reflected by the predominant recipe ingredient (>50% total g). For remaining nonrecipe whole foods (e.g., fluid milk, cheese), we initially applied the University of North Carolina food grouping system, which disaggregates the major US Department of Agriculture's food groups by fat and fiber (35). Due to low consumption of several foods across heritage groups, however, we aggregated low- and high-nutrient specific food groups (e.g., high- and low-fat milk into milk). In addition, we separated fried from nonfried foods (e.g., fried compared with grilled chicken) across food groups except for corn-based foods, which traditionally include fried/grilled corn tortillas. Finally, dietary intakes (g/d) (36, 37) of each food group were first summed in their respective 24-h recalls and then averaged across recalls for each participant.
TABLE 1.
Examples, median intakes, and percentage of nonconsumers by food group in HCHS/SOL (n = 14,099)1
| Food group, g/d | Examples2 | Median (IQR)3 | NCs (%) |
|---|---|---|---|
| Cheese | Queso fresco, queso blanco, mozzarella cheese | 31.3 (40.3) | 88.6 |
| Milk | Unflavored milk,4 yogurt, smoothies | 305.0 (226.7) | 51.1 |
| Fruit | Bananas, apples, oranges, grapes | 182.0 (164.0) | 45.8 |
| Nonstarchy vegetables | Tomato, mixed vegetables, lettuce, cactus pads (nopales) | 96.0 (135.8) | 70.4 |
| Starchy vegetables | Plantains, yuca blanca, mashed potatoes, potatoes | 167.0 (181.1) | 68.2 |
| Salads | Tossed salads, lettuce salads, Caesar salads | 134.6 (168.0) | 69.0 |
| Fish | Tilapia, shrimp, salmon, cod, catfish, calamari | 125.0 (97.9) | 85.2 |
| Poultry | Chicken (breast, drumstick, leg, wing) | 98.0 (75.5) | 58.9 |
| Pork | Pork (chops, steak, ribs, cubes) | 103.0 (95.0) | 86.2 |
| Beef | Beefsteak, beef (steak, sirloin, meatballs), ropa vieja | 92.8 (97.8) | 72.6 |
| Processed meats | Bacon, sausage, ham, salami, corned beef | 45.3 (44.4) | 85.6 |
| Burgers | Hamburger or ground beef and buns | 165.3 (136.0) | 90.9 |
| Fries | French fries,4 hashed brown potatoes | 80.0 (78.5) | 85.9 |
| Fried dishes | Other fried foods (e.g., empanadas, fried chicken) | 103.0 (108.8) | 83.1 |
| Pizza | Pizza | 204.0 (195.9) | 88.4 |
| Dessert | Pan dulce, ice cream, cookies, cake | 76.0 (89.3) | 46.1 |
| Sweets | Chocolate candy, ice popsicle, gelatin | 41.0 (74.0) | 84.2 |
| Salty snacks | Crackers, tortilla/nacho chips, potato chips | 27.0 (34.1) | 66.6 |
| Refined grains | White breads and toppings (e.g., cream cheese)4 and rolls | 60.9 (70.3) | 54.4 |
| Cereal | Ready-to-eat cereals and milk,4 oatmeal ± milk | 255.5 (185.1) | 64.1 |
| Whole grains | Whole wheat bread4 and toppings (e.g., cream cheese, butter) | 61.4 (47.6) | 82.1 |
| Corn-based foods | Corn tortillas,4 tacos, tamales | 142.0 (176.0) | 55.9 |
| Meat and vegetable stew | Carne guisada (beef stew), picadillo de carne | 189.0 (203.0) | 76.7 |
| Beans | Beans (pinto, black, red),4 lentils | 125.0 (143.3) | 58.3 |
| Eggs | Scrambled eggs, fried eggs, boiled eggs | 92.9 (75.3) | 67.7 |
| Rice | White rice,4 rice and beans | 177.8 (179.8) | 34.5 |
| Noodle-based foods | Spaghetti noodles and sauce, ramen, macaroni and cheese | 255.0 (243.0) | 78.3 |
| Sandwiches and rolls | Sandwiches, hot dogs, burritos | 161.1 (119.4) | 52.5 |
| Soups | Chicken/vegetable soup, pozole, caldo de res (beef soup) | 394.8 (396.8) | 69.0 |
| Soft beverages | Coke,4 Pepsi,4 Sprite,4 diet soda | 369.6 (275.4) | 47.5 |
| Flavored drinks | Fruit juices/drinks, Gatorade, fruit punch, horchata | 373.5 (386.6) | 36.6 |
| Coffee/tea | Coffee and milk/cream,4 tea ± milk or cream | 360.0 (328.7) | 27.2 |
| Alcoholic beverages | Beer,4 wine, spirits | 356.4 (477.6) | 85.5 |
| Water | Tap water, bottled water | 896.2 (866.5) | 07.6 |
| Miscellaneous5 | Herbalife products (e.g., shakes), dairy alternatives | 255.0 (362.9) | 90.7 |
Food groups (n = 34) are total intakes (g) averaged across 2 nonconsecutive 24-h recalls in HCHS/SOL (n = 14,099). HCHS/SOL, Hispanic Community Health Study/Study of Latinos; NCs, nonconsumers.
Examples are listed in descending order of frequency in their food group.
Median intakes (g) in the overall sample defined 3-level ordinal intake variables (NCs, below and above median intakes).
Most represented food in their food group.
Dropped from analysis due to consumption <5% found in ≥1 Hispanic/Latino heritage group.
Episodically consumed foods are typically not well captured by 24-h recalls, resulting in high proportions of nonconsumers and skewed distributions for some food groups. To address this, we used food group intakes in the overall sample to generate a 3-level ordinal intake categorical variable for each food group (nonconsumers, below and above the median). Last, food groups with consumption <5% in ≥1 heritage group were either merged with another food group or dropped from analysis (Table 1) (38, 39).
AHEI-2010
To evaluate the healthfulness of each heritage-specific DP, we used AHEI-2010, a diet quality indicator previously linked to cardiometabolic disease risk (40–42). To construct the AHEI-2010, which consists of 11 dietary components, 4 steps were followed: 1) at the 24-h recall level, each component was generated by summing the corresponding NDS-R food subgroups (40); 2) predicted usual intakes for each component were created using the National Cancer Institute method, which considers within- and between-person variation in each component and accounts for the high intraindividual variation innate in 24-h recalls (43); 3) scores for each component were generated ranging from 0 (worst) to 10 (best); and then 4) scores were summed with a range from 0 to 110, with higher scores indicating diet healthfulness.
Dietary pattern derivation and statistical analysis
We performed all analyses in Stata version 14.2 (Stata Corp). To test whether the 34 ordinal food group variables had too little in common to warrant factor analysis, we evaluated Kaiser–Meyer–Olkin (KMO) indices and Barlett's tests for sphericity separately in each heritage group (44) and found acceptable results in all groups (all KMOs > 0.50 and Barlett's tests P < 0.001). Thus, we proceeded with exploratory factor analysis to empirically derive DPs separately in each heritage group (45). We first used the 34 ordinal food group variables to generate 6 heritage-specific matrixes of polychoric correlations (46). We then performed principal factor analysis (PFA) on the correlation matrices of each heritage group to identify the smallest number of unique factors that best account for the common variance across food groups (44, 45). Because PFA only analyzes the common variance across food group input variables, it best suited our research objectives to understand which foods are “consumed together/hang together,” in comparison to principal component analysis (PCA), which analyzes the total variance and is not typically used to identify underlying latent variables (e.g., DPs) (47).
To guide factor retention in each heritage group, we used a modified Delphi approach, which is a widely used method that solicits the opinions of experts through a series of carefully designed questionnaires interspersed with information and opinion feedback in order to establish a convergence of opinion (48). Three investigators with experience involving exploratory factor analysis independently evaluated factors in each heritage group based on heritage-specific scree plots (Supplemental Figure 1), factor loadings, variance explained by each factor, interpretability of factors, and consistency with the extant literature (45, 49, 50). Investigators then met to compare, discuss, and reconcile differences related to independent conclusions about the final number of factors retained in each heritage group. Despite high uniqueness in some food groups in some heritage groups, all food groups were included for consistency (49, 51). To improve the interpretability and minimize correlations among derived heritage-specific factors, we used orthogonal (varimax) rotation (44). We initially identified heritage-specific DPs based on food groups with the largest positive and negative factor loadings (>0.20) (45, 52–54). To identify commonality among heritage-specific DPs, we identified overarching DPs based on similarly high loadings for the same food groups in ≥2 heritage groups. We then generated DP scores for everyone by multiplying the scoring coefficient of each food group by the individual's corresponding food group intake category (nonconsumer, below or above the median) and summing across food groups. Finally, we divided DP scores into quintiles and evaluated mean AHEI-2010 scores at each DP quintile to evaluate healthfulness and further characterize overarching DPs (45, 52).
Except for PFA, all statistical analyses accounted for complex survey design using HCHS/SOL survey weights and survey procedures in Stata (version 14.2; StataCorp). We tested differences in baseline sociodemographics by heritage group using t test for continuous variables and Pearson chi-square test for categorical variables. To assess whether DPs correlate with a measure of diet healthfulness, we separately performed multiple linear regressions in each heritage group to test mean differences in AHEI-2010 scores by quintiles of each heritage-specific DP, adjusting for relevant covariates known to be linked to diet, including age, sex, and education, and other heritage-specific DPs (quintiles) that account for scoring in other DPs. We also assessed linear relations between DPs and AHEI-2010 by using the midpoint of each quintile as a continuous measure. Last, we separately conducted multivariate linear regressions in each heritage group to test mean differences in heritage-specific DP scores by categories of years living in the United States, adjusting for age, sex, and education. We also tested linear trends between heritage-specific DPs and years living in the United States in each heritage group by using the midpoint of each heritage-specific category of years living in the United States as a continuous measure. We adjusted statistical significance for multiple pairwise comparisons with a Bonferroni correction. As a result, we considered P < 0.01 significant for all analyses.
Results
Table 2 displays demographic characteristics by heritage. Overall, Hispanics/Latinos of Mexican heritage were the largest group (41.7%), followed by those of Puerto Rican (16.6%), Cuban (15.2%), Central American (11%), Dominican (8.4%), and South American (7%) heritage. On average, Hispanics/Latinos of Mexican heritage were the youngest (38.6 y), whereas individuals of Cuban heritage were the oldest (46.8 y). Regardless of heritage, most HCHS/SOL participants were foreign-born. Among the foreign-born, most had reported living in the United States >10 y in all groups except individuals of Cuban heritage (50.3%). Regarding education, most reported having achieved at most a high school or equivalent education in all groups except the South American group (48.1%). Finally, although mean AHEI-2010 (scores) were the highest among Mexican-origin Hispanics/Latinos (48.6) and lowest among those of Puerto Rican heritage (41.8), all heritage groups scored poorly on this diet quality measure given total AHEI-2010 scores are out of 110.
TABLE 2.
Baseline sociodemographics and AHEI-2010 score by Hispanic/Latino heritage group in HCHS/SOL (n = 14,099)1
| Cuban | Dominican | Mexican | Puerto Rican | Central American | South American | ||
|---|---|---|---|---|---|---|---|
| Sociodemographics | n = 2140 | n = 1189 | n = 5883 | n = 2343 | n = 1553 | n = 991 | P |
| Age, y | 46.8 (13.0) | 39.7 (14.4) | 38.6 (14.4) | 43.6 (15.9) | 40.3 (17.2) | 42.8 (16.6) | <0.001 |
| Women, % | 48.7 | 59.4 | 53.1 | 50.8 | 51.2 | 55.3 | <0.001 |
| Years living in the United States, % | <0.001 | ||||||
| US-born | 06.6 | 16.3 | 23.1 | 48.5 | 06.7 | 05.1 | |
| ≥10 y | 43.1 | 60.0 | 53.0 | 45.0 | 56.2 | 55.0 | |
| <10 y | 50.3 | 23.7 | 24.0 | 06.5 | 37.1 | 39.9 | |
| Education status, % | <0.001 | ||||||
| Less than high school | 21.6 | 36.9 | 35.2 | 34.2 | 39.2 | 20.8 | |
| High school or equivalent | 29.7 | 23.5 | 30.6 | 28.9 | 25.1 | 27.3 | |
| Greater than high school | 48.7 | 39.7 | 34.2 | 36.9 | 35.8 | 51.9 | |
| Center site, % | <0.001 | ||||||
| Bronx, New York | 01.3 | 94.0 | 08.3 | 69.5 | 17.9 | 22.5 | |
| Chicago, Illinois | 00.8 | 01.0 | 27.1 | 23.5 | 15.7 | 21.0 | |
| Miami, Florida | 97.4 | 04.7 | 01.1 | 04.8 | 62.5 | 52.0 | |
| San Diego, California | 00.5 | 00.3 | 63.4 | 02.2 | 03.9 | 04.6 | |
| AHEI-2010 (scores) | 44.0 (4.6) | 48.6 (6.4) | 52.1 (7.0) | 41.8 (5.9) | 47.4 (7.3) | 46.1 (7.6) | <0.001 |
Values are survey-weighted means (SE) unless otherwise specified; sample sizes are unweighted. AHEI-2010, Alternative Healthy Eating Index–2010; HCHS/SOL, Hispanic Community Health Study/Study of Latinos.
Table 3 shows derived heritage-specific factors and factor loadings by overarching DPs based on shared high loadings on the same foods in ≥2 heritage groups. The number of derived factors in each heritage group ranged from 3 to 5 for a total of 21 heritage-specific factors. The percentage variance explained by heritage-specific factors ranged from a low of 6% in the Central American group to a high of 28% in the Mexican group. The first factor, which accounts for the largest portion of variation in PFA, derived in all heritage groups was characterized by the highest positive loadings on burgers, fries, and soft drinks. We classified these heritage-specific factors under an overarching Burgers, Fries, & Soft Drinks DP, which was the only common DP including findings from all heritage groups.
TABLE 3.
Heritage-specific principal factors and factor loadings by overarching common dietary patterns in HCHS/SOL (n = 14,099)1
| Burgers , Fries, & Soft Drinks | White Rice, Beans, & Red Meats | Fish | Egg & Cheese | Alcohol | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CB | DM | MX | PR | CA | SA | CB | DM | MX | PR | CA | CB | DM | MX | SA | DM | PR | CA | DM | CA | SA | |
| Food groups (n = 34) | F1 | F1 | F1 | F1 | F1 | F1 | F2 | F3 | F3 | F2 | F3 | F3 | F4 | F2 | F2 | F2 | F3 | F2 | F5 | F4 | F3 |
| Cheese | −0.21 | −0.33 | 0.22 | 0.29 | 0.46 | 0.26 | 0.54 | −0.22 | 0.31 | ||||||||||||
| Milk | −0.21 | ||||||||||||||||||||
| Fruit | −0.26 | −0.27 | −0.35 | −0.33 | 0.23 | 0.31 | −0.28 | ||||||||||||||
| Nonstarchy vegetables | −0.21 | −0.35 | −0.30 | 0.27 | 0.35 | 0.36 | 0.25 | 0.21 | |||||||||||||
| Starchy vegetables | 0.28 | 0.40 | 0.67 | 0.25 | 0.21 | ||||||||||||||||
| Salads | −0.22 | −0.28 | 0.25 | 0.44 | −0.21 | ||||||||||||||||
| Fish | −0.32 | −0.35 | −0.23 | 0.48 | 0.73 | 0.23 | 0.31 | 0.23 | 0.35 | ||||||||||||
| Poultry | 0.29 | 0.24 | 0.23 | 0.36 | −0.27 | 0.27 | –0.34 | ||||||||||||||
| Pork | 0.32 | 0.37 | 0.21 | 0.47 | 0.28 | −0.45 | −0.23 | 0.22 | |||||||||||||
| Beef | 0.39 | 0.27 | 0.24 | 0.56 | 0.68 | ||||||||||||||||
| Processed meats | 0.28 | 0.28 | 0.43 | 0.48 | 0.20 | ||||||||||||||||
| Burgers | 0.68 | 0.57 | 0.67 | 0.60 | 0.74 | 0.77 | –0.28 | −0.31 | |||||||||||||
| Fries | 0.55 | 0.73 | 0.70 | 0.61 | 0.72 | 0.61 | |||||||||||||||
| Fried dishes | 0.23 | 0.46 | 0.24 | 0.21 | 0.26 | ||||||||||||||||
| Pizza | 0.35 | 0.43 | 0.27 | 0.32 | 0.27 | 0.25 | −0.51 | −0.22 | −0.23 | −0.26 | 0.27 | −0.24 | |||||||||
| Dessert | 0.21 | 0.23 | |||||||||||||||||||
| Sweets | −0.22 | −0.25 | 0.36 | ||||||||||||||||||
| Salty snacks | 0.23 | 0.24 | |||||||||||||||||||
| Refined grains | 0.20 | −0.24 | |||||||||||||||||||
| Cereal | −0.24 | 0.25 | 0.36 | −0.38 | −0.20 | −0.31 | |||||||||||||||
| Whole grains | −0.21 | −0.30 | −0.42 | −0.23 | 0.24 | 0.32 | 0.48 | −0.30 | |||||||||||||
| Corn-based | -0.25 | 0.27 | −0.47 | 0.63 | |||||||||||||||||
| Meat and vegetable stew | 0.27 | 0.31 | 0.21 | −0.39 | −0.26 | 0.24 | −0.30 | ||||||||||||||
| Beans | −0.22 | −0.20 | 0.42 | 0.37 | 0.33 | 0.56 | 0.26 | −0.22 | −0.28 | 0.31 | |||||||||||
| Eggs | 0.31 | 0.23 | 0.52 | 0.45 | 0.50 | 0.24 | |||||||||||||||
| White rice | −0.28 | 0.61 | 0.41 | 0.29 | 0.77 | 0.64 | −0.27 | −0.29 | |||||||||||||
| Noodle dishes | 0.22 | −0.26 | −0.29 | −0.21 | 0.44 | ||||||||||||||||
| Sandwiches/rolls | 0.39 | 0.40 | 0.31 | 0.27 | 0.21 | 0.35 | −0.32 | 0.29 | |||||||||||||
| Soups | −0.23 | −0.21 | −0.22 | −0.20 | −0.39 | −0.28 | −0.24 | 0.28 | −0.32 | ||||||||||||
| Soft drinks | 0.64 | 0.78 | 0.43 | 0.60 | 0.61 | 0.40 | 0.29 | −0.38 | −0.51 | 0.21 | |||||||||||
| Fruit and vegetable drinks | |||||||||||||||||||||
| Coffee/tea | −0.21 | 0.28 | 0.38 | 0.28 | |||||||||||||||||
| Alcoholic drinks | 0.24 | 0.25 | 0.24 | 0.20 | 0.22 | 0.37 | 0.29 | 0.45 | 0.60 | 0.41 | |||||||||||
| Water | −0.22 | −0.22 | 0.39 | 0.25 | −0.28 | ||||||||||||||||
| Variance explained, % | 16.8 | 16.2 | 28.4 | 18.0 | 8.89 | 15.8 | 12.7 | 8.52 | 15.2 | 12.2 | 6.64 | 9.64 | 8.39 | 18.6 | 15.5 | 9.65 | 9.88 | 6.68 | 8.39 | 5.97 | 11.4 |
Values are orthogonally (varimax) rotated factors and food group loadings derived in each heritage group separately using principal factor analysis on heritage-specific matrices holding polychoric correlations between 34 three-level ordinal food group intake variables (nonconsumers, below and above the median in the overall sample) with original daily total intakes (g) averaged across 2 nonconsecutive 24-h recalls in HCHS/SOL. Factor loadings in absolute values >0.20 only shown for simplicity. CB, n = 2140; DM, n = 1189; MX, n = 5883; PR, n = 2343; SA, n = 991. CA, Central American; CB, Cuban; DM, Dominican; F, factor; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; MX, Mexican; PR, Puerto Rican; SA, South American.
After this first common DP, DPs became less similar and heritage-specific, showing fewer shared food groups with high loadings among ≥2 heritage groups. For instance, all heritage groups, except South American, shared largest loadings on white rice, beans, and red meats (pork or beef). We classified these heritage-specific factors under an overarching White Rice, Beans, & Red Meats DP. We identified 3 additional overarching DPs, including an overarching Fish DP showing high loadings on fish shared by Cuban, Dominican, Mexican, and South American groups; an overarching Egg & Cheese DP showing high loadings on eggs and cheese shared by Dominican, Puerto Rican, and Central American groups; and an overarching Alcohol DP showing high loadings on alcohol shared by those of Dominican, Central American, and South American heritage.
Although overarching DPs were based on ≥1 food group showing high loadings shared by ≥2 heritage groups, some groups additionally shared several other food groups within these overarching DPs. For example, among Burgers, Fries, & Soft Drinks DPs, Hispanics/Latinos of Dominican, Mexican, Puerto Rican, and Central American heritage additionally shared high positive loadings on pizza and sandwiches and rolls and large negative loadings on fruit. In addition to these foods, Puerto Rican and Central American groups shared large negative loadings on nonstarchy vegetables, salads, fish, and whole grains. Among White Rice, Beans, & Red Meats DPs, all groups, except Dominican, additionally shared high positive loadings on beef. Furthermore, Cuban, Dominican, and Central American groups additionally shared large positive loadings for meat and vegetable stews, and Dominican, Mexican, and Puerto Rican groups additionally shared high positive loadings on poultry. Fish DPs among Cuban, Mexican, and South American groups additionally shared high positive loadings only for whole grains. Mexican and South American heritage groups for this same overarching DP shared, in addition to whole grains, high positive loadings on cereal and fruit and negative loadings on soft drinks, and Mexican and Cuban groups also shared similar findings for salads and poultry (both positive) and meat and vegetable stews (negative). Last, Egg & Cheese DPs in Dominican and Puerto Rican groups additionally shared high positive loadings for starchy vegetables and processed meats, and Alcohol DPs in those of Central and South American heritage shared high positive loadings for coffee/tea.
Figure 2 displays mean AHEI-2010 scores (95% CIs) for each quintile of each heritage-specific DP from models adjusting for age, sex, education, and other heritage-specific DPs. AHEI-2010 score differences comparing higher with lowest quintiles (quintiles 2–5 compared with quintile 1) are marked with an asterisk (all Bonferroni-corrected pairwise comparisons P < 0.01; all P-trend < 0.001). Higher scores on all Burgers, Fries, & Soft Drinks DPs across heritage [all quintiles 2–5, except Dominican (quintiles 3–5) and South American (quintiles 4–5) groups] were consistently and significantly associated with lower mean AHEI-2010 scores. In contrast, higher scores on all Fish DPs across heritage (Cuban, quintiles 2–5; Dominican, quintiles 4 and 5; Mexican, quintile 5; and South American, quintiles 3–5) were significantly associated with greater mean AHEI-2010 scores. Among the remaining overarching DPs, findings were mixed and showed significant associations for the White Rice, Beans, & Red Meats DPs among Cuban, Central American, and Mexican groups; Egg & Cheese DP in those of Puerto Rican heritage; and Alcohol DP in the Dominican group. Whereas White Rice, Beans, & Red Meats DPs in Cuban (quintiles 3–5) and Central American (quintile 5) groups were inversely associated with AHEI-2010, findings for this same overarching DP among individuals of Mexican heritage showed the opposite (quintiles 2–5). Last, only the Puerto Rican Egg & Cheese (quintiles 2–5) and Dominican Alcohol (quintiles 3–5) DPs were significantly associated with higher and lower AHEI-2010 scores, respectively.
FIGURE 2.

Mean AHEI-2010 scores by quintiles of heritage-specific a posteriori dietary patterns in HCHS/SOL (n = 14,099). Data are weighted mean AHEI-2010 scores (95% CIs) by quintiles of each heritage-specific dietary pattern from multivariable linear regression models showing significant mean AHEI-2010 score differences comparing higher with lowest quintiles (Q2–Q5 compared with Q1), adjusting for age (y), sex (men, women), highest education achieved (less than high school, high school or equivalent, beyond high school), and other heritage-specific dietary patterns (quintiles) (all Bonferroni-corrected for pairwise comparisons, P < 0.01; all P-trend < 0.001). Asterisks indicate significant pairwise comparisons for higher to lowest quintiles of each heritage-specific dietary pattern. Linear trends were tested by using the midpoint of each dietary pattern quintile as a continuous measure. CB, n = 2140; DM, n = 1189; MX, n = 5883; PR, n = 2343; SA, n = 991. AHEI-2010, Alternative Healthy Eating Index–2010; CA, Central American; CB, Cuban; DM, Dominican; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; MX, Mexican; PR, Puerto Rican; Q, quintile; SA, South American.
Figure 3 presents significant mean heritage-specific dietary pattern score differences (95% CIs) by lived years in the United States (<10 y, ≥10 y) compared with US-born adjusting for age, sex, and education (all Bonferroni-corrected pairwise comparisons P < 0.01). Fewer years living in the United States was consistently and significantly associated with lower mean scores for the Burgers, Fries, & Soft Drinks DPs only in Cuban, Mexican, Puerto Rican (all P-trend < 0.001), and Dominican (P-trend = 0.036) groups. Findings for Fish and Egg & Cheese DPs were significant only in Mexican (only <10 y) and Puerto Rican groups, respectively, and showed similar patterning (both P-trend = 0.001). In contrast, fewer years living in the United States was significantly associated with higher mean scores for the White Rice, Beans, & Red Meats DPs only among those of Cuban (P-trend < 0.001) and Mexican (P-trend = 0.021) heritage. Findings for Alcohol DPs were nonsignificant. Last, null findings for Burgers, Fries, & Soft Drinks, Fish, and White Rice, Beans, & Red Meats DPs, on average, tracked similarly, whereas the Egg & Cheese DPs in Dominican and Central American groups showed opposite findings.
FIGURE 3.
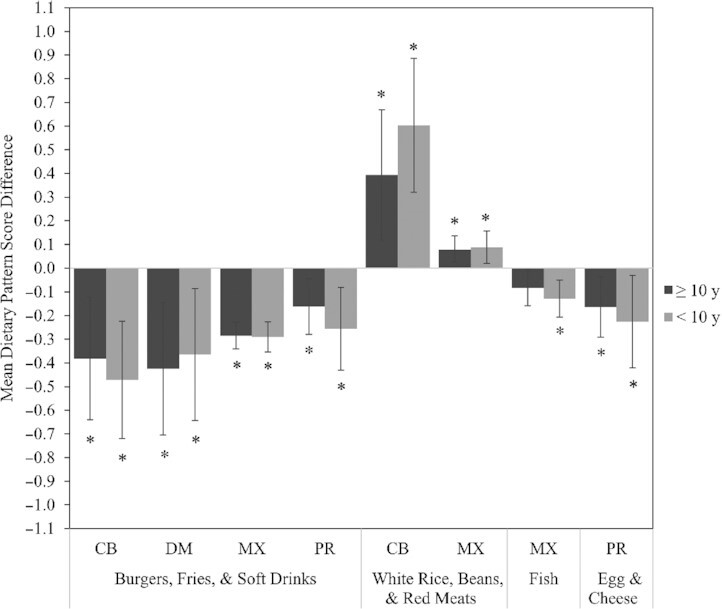
Mean heritage-specific a posteriori dietary pattern scores by years living in the United States in HCH/SOL. Data presented are significant weighted heritage-specific dietary pattern mean score differences (95% CIs) comparing greater years living in the United States categories with US-born (referent, not shown) in HCHS/SOL, adjusting for age (y), sex (men, women), and highest education achieved (less than high school, high school or equivalent, beyond high school) (Bonferroni-corrected P < 0.01). Asterisks indicate significant individual pairwise comparisons for categories of years living in the United States compared with US-born (all Bonferroni-corrected for pairwise comparisons, P < 0.01). Linear trends were significant across all presented heritage-specific findings (P-trend < 0.01), except for the Western dietary pattern in Dominicans (P-trend = 0.036) and traditional dietary pattern in Mexicans (P-trend = 0.021). Linear trends were tested by using the midpoint of each category for years living in the United States in the overall sample as a continuous measure. CB, n = 2140; DM, n = 1189; MX, n = 5883; PR, n = 2343; SA, n = 991. CA, Central American; CB, Cuban; DM, Dominican; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; MX, Mexican; PR, Puerto Rican; SA, South American.
Discussion
Using data from the largest population-based cohort of US Hispanics/Latinos of diverse origin aged 18–74 y, this study identified a total of 21 a posteriori heritage-specific DPs separately derived in 6 large Hispanic/Latino heritage groups. Based on higher intakes of foods shared by ≥2 groups, we first identified the following 5 overarching DPs and foods for which these DPs were labeled: Burgers, Fries, & Soft Drinks; White Rice, Beans, & Red Meats; Fish; Egg & Cheese; and Alcohol. The Burgers, Fries, & Soft Drinks DP was the most salient DP in each heritage group and shared by all groups. Subsequently derived DPs were more heritage-specific, shared by fewer groups, and generally showed higher intakes of traditional compared with nontraditional foods Hispanic/Latino. Second, Burgers, Fries, & Soft Drinks and Fish DPs were all significantly associated with lower and higher healthfulness (as measured by AHEI-2010), respectively. Findings for White Rice, Beans, & Red Meats, Egg & Cheese, and Alcohol DPs were mixed. Last, greater time in the United States was significantly associated with higher adherence to the following DPs: Burgers, Fries, & Soft Drinks only in Cuban, Dominican, Mexican, and Puerto Rican groups; Fish only in those of Mexican heritage; and Egg & Cheese only in Puerto Rican Hispanics/Latinos. Conversely, greater time in the United States was significantly associated with lower adherence to a White Rice, Beans, & Red Meats DP only in Cuban and Mexican groups.
Our findings were fairly consistent with a posteriori DPs derived in previously published studies among Hispanics/Latinos of Puerto Rican and Mexican heritage. Using FFQs from the Boston Puerto Rican Health Study, a cohort of Hispanics/Latinos of Puerto Rican heritage aged 45–75 y living in Boston, Massachusetts, 1 study derived and identified 3 a posteriori DPs using PCA (16). Two of the DPs (meat, processed meat, and French fries; and traditional) showed similarly high food group loadings as the Burgers, Fries, & Soft Drinks and White Rice, Beans, & Red Meats DPs derived among Hispanics/Latinos of Puerto Rican heritage in the current study. Another study also using PCA on FFQs from a nationally representative sample of Hispanics/Latinos of Mexican origin derived 4 a posteriori DPs, the first 3 of which were fairly consistent with those derived in our study among participants of Mexican heritage. For example, similar to the Mexican Burgers, Fries, & Soft Drinks, Fish, and White Rice, Beans, & Red Meats DPs identified in HCHS/SOL, Sofianou and colleagues (17) identified the following 3 DPs: Burgers, Fries, & Soft Drinks (fries, fried foods, pizza, and sweetened beverages); Healthy (vegetables of all types, poultry, fish, and others); and Tomato/Tortilla (tortilla, beans, eggs, and rice). Despite differences between our study and these 2 published studies in terms of dietary assessment (24-h recall compared with FFQ), food group aggregation/disaggregation, factor analysis approach (PFA compared with PCA), and “subjective” decisions about factor retention, findings were relatively consistent, suggesting fair reproducibility of salient a posteriori DPs derived using factor analysis among Hispanics/Latinos of Puerto Rican and Mexican heritage. Future research is needed to verify a posteriori findings of other heritage groups in the current study.
Findings for AHEI-2010 were generally consistent with our expectations of diet healthfulness among DPs. For example, all Burgers, Fries, & Soft Drinks DPs were associated with worse AHEI-2010 scores, whereas all Fish DPs were associated with higher scores. Relatedly, previous work in HCHS/SOL reported significant inverse relations between AHEI-2010 and frequency of consumption of away-from-home foods from fast foods (55), most of which showed the highest loadings on an overarching Burgers, Fries, & Soft Drinks DP identified in all heritage groups in the current study. In addition, White Rice, Beans, & Red Meats DPs were inconsistently related to AHEI-2010, showing positive associations in those of Mexican heritage but the opposite in Cuban and Central American groups. These discrepant findings for the same overarching DP may be due to differences in the overall dietary composition of these DPs by heritage group. For example, compared with those of Mexican heritage, Cuban and Central American groups showed, on average, unfavorable loadings on the White Rice, Beans, & Red Meats DP for the following AHEI dietary components: higher red and processed meats (beef and pork) and soft beverages (Central American only), lower whole grains (Central American only), and no loadings for vegetables without potatoes (i.e., nonstarchy vegetables). In addition, although white rice was the highest loading food for each heritage-specific White Rice, Beans, & Red Meats DP, the Mexican group had the lowest loading or relative intake of this food and relatively greater intakes of AHEI-relevant foods (e.g., vegetables and beans), which could explain why this DP was associated with higher AHEI scores among the Mexican heritage group but not others.
Associations between years living in the United States and DPs, particularly Burgers, Fries, & Soft Drinks and White Rice, Beans, & Red Meats, at the heritage level were roughly similar to previously published findings among individuals of Mexican origin, but less so for those of Puerto Rican heritage. For example, whereas we detected significant associations only for the Burgers, Fries, & Soft Drinks DP in the Puerto Rican group, Mattei and colleagues (29) found significant findings only for a characteristically similar traditional DP (White Rice, Beans, & Red Meats) in the Boston Puerto Rican Health Study. These inconsistencies may be due to differences between Puerto Rican samples related to age and nativity, both of which have been shown to have dietary implications. For instance, older compared with younger immigrants may be more likely to adhere to a White Rice, Beans, & Red Meats DP characterized mostly by characteristically traditional foods (16), whereas US-born individuals have generally been shown to have worse dietary profiles with higher intakes of foods known to be related to chronic disease (20, 22, 56, 57). Compared with Puerto Rican Hispanics/Latinos in HCHS/SOL, those in the Boston Puerto Rican Health Study were relatively older and mostly born in Puerto Rico, with no mainland US-born comparison group (27). For those of Mexican heritage, our findings corroborate previous work for characteristically similar DPs by nativity but not by years living in the United States alone (17). To compare findings, we categorized years living in the United States among the foreign-born consistent with previous work [<10 y, ≥10 y (reference)] (20), but generally and similarly found no significant differences in Burgers, Fries, & Soft Drinks and White Rice, Beans, & Red Meats DP scores by years living in the United States alone (data not shown). Together, these findings suggest nativity may be a stronger predictor of dietary acculturation compared with years living in the United States alone, at least in Puerto Rican and Mexican heritage groups.
In general, greater years living in the United States was associated with lower DP healthfulness across all heritage groups, which has concerning health implications across Hispanics/Latinos. These findings may reflect dietary acculturation, a complex and dynamic process by which immigrants typically adopt the cultural practices of the host country and abandon the cultural dietary choices and behaviors practiced in the country of origin (20, 58). Over time, dietary acculturation may lead to relatively unhealthier diets, which in turn may increase diet-related chronic disease risk (58). In the current study, for example, greater time in the United States generally corresponded to lower mean scores for a characteristically traditional White Rice, Beans, & Red Meats DP and greater mean scores for a characteristically unhealthier Burgers, Fries, & Soft Drinks DP. Compared with other overarching DPs, foods highly represented in the Burgers, Fries, & Soft Drinks DPs tended to be relatively more energy-dense and less nutrient-dense and are consistent with those highly represented in previously derived DPs shown to be associated with health outcomes (59, 60). The overarching White Rice, Beans, & Red Meats DP was linked favorably to AHEI-2010 only in the Mexican group, but this DP was also inversely linked to years living in the United States in the same heritage group. Future work could consider identifying environmental influences (e.g., food availability, taste changes, adoption of new foods) related to time in the United States that likely explain these dietary shifts observed among Hispanics/Latinos. In addition, there may be other socioeconomic and psychosocial factors [e.g., income (29), food insecurity, immigrant enclaves, access to characteristically “healthy” foods] interacting with years living in the United States to influence dietary choices differently across heritage groups. Indeed, our findings show increased adherence to a Burgers, Fries, & Soft Drinks DP and lowered adherence to a White Rice, Beans, & Red Meats DP only in Cuban and Mexican groups, suggesting differential dietary acculturation processes by heritage (61).
This study has several notable strengths. The large samples of different heritage groups in HCHS/SOL allowed the separate derivation of DPs in each heritage group through factor analysis, which typically requires a large sample size to achieve stable correlations between input variables (51). In addition, we used 2 nonconsecutive 24-h recalls, which, in comparison to FFQs, have been shown to explain a relatively higher proportion of the variance in derived DPs using exploratory factor analysis (62, 63). Another strength of our approach was the derivation of culturally and behaviorally meaningful DPs by different Hispanics/Latinos, which may inform dietary interventions targeting different Hispanic/Latino groups in this diverse population. Future research should evaluate how these culturally relevant DPs relate to health outcomes. Identifying health-relevant DPs that more closely resembles dietary preferences in this diverse population may improve long-term dietary adherence (64).
This study also had some limitations. Because we relied on only 24-h recalls, we may not have captured episodically consumed foods well. Along with measurement error (65), this may have resulted in underestimation of our findings related to PFA. In addition, misclassification of foods may have introduced nondifferential bias in the relations with AHEI-2010, resulting in estimates toward the null given our behavioral-focused approach of maintaining mixed dishes intact and assigning them (all ingredients) to 1 food group. Despite this food misclassification among mixed dishes, 15 out of the 21 heritage-specific findings were significantly related to the diet quality index, reflecting the robustness of our approach. Another limitation was inadequate sample sizes for deriving and evaluating DPs in Hispanics/Latinos of different cultural origins in Central America (e.g., Guatemala, Costa Rica) and South America (e.g., Argentina, Bolivia), leaving much unpacked dietary heterogeneity in these groups. Therefore, findings for Central and South American groups should be interpreted with caution. Last, we tested only 1 a priori defined diet quality score as a marker of healthfulness because previous work has documented links between AHEI-2010 and cardiometabolic health among Hispanics/Latinos (14). Relations between this score and health outcomes, however, have only been detected in some, but not all, heritage groups (14). Therefore, other indices may be more appropriate to evaluate healthfulness in certain heritage groups. Nevertheless, findings for AHEI provide insights and generate hypotheses about how DPs may be related to health in each heritage group. Future studies should investigate relations among heritage-specific DPs, other indices of healthfulness, and general health outcomes in Hispanics/Latinos.
In summary, our findings suggest 1) substantial heterogeneity in culturally relevant DPs and the types of foods being consumed together across Hispanic/Latinos in the United States; 2) most a posteriori DPs were significantly associated with an a priori nutrient-focused diet quality index (AHEI-2010) despite our behavioral compared with nutrient focus in food group formation, indicating their potential for explaining variation in associations between this diet quality index and cardiometabolic profiles by heritage previously reported in HCHS/SOL (14); and 3) dietary acculturation may be playing a stronger role in some heritage groups compared with others. Given the nutrition transition occurring in many areas of Latin America (58), studies should use multinational data to compare diets between Hispanics/Latinos living in the country of origin and those living in the United States to determine the extent to which dietary shifts (e.g., from White Rice, Beans, & Red Meats to Burgers, Fries, & Soft Drinks) have occurred in those countries (66). As the Hispanic/Latino population continues to grow in the United States, research focused on unpacking dietary heterogeneity across Hispanics/Latinos may help inform dietary and other relevant interventions targeting this diverse US population.
Supplementary Material
Acknowledgments
The authors’ responsibilities were as follows—LEM: reviewed the literature, developed the study design, analyzed and interpreted the data, and wrote the manuscript; LSA and SSA: contributed to the study design, data interpretation, and critically revised and edited the manuscript; DS-A, JM, YM-R, KMP, MLD, LVVH, LCG, and CRI: assisted in data interpretation and reviewed and edited the manuscript; and all authors: read and approved the final manuscript.
Notes
The Hispanic Community Health Study/Study of Latinos (HCHS/SOL) was carried out as a collaborative study supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI) to the University of North Carolina (N01-HC65233), University of Miami (N01-HC65234), Albert Einstein College of Medicine (N01-HC65235), Northwestern University (N01-HC65236), and San Diego State University (N01-HC65237). The following institutes/centers/offices contribute to the HCHS/SOL through a transfer of funds to the NHLBI: National Center on Minority Health and Health Disparities, National Institute of Deafness and Other Communications Disorders, National Institute of Dental and Craniofacial Research, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Neurological Disorders and Stroke, and the Office of Dietary Supplements. This research received support from the NHLBI Global Cardiometabolic Disease Training Grant (1T32HL129969-01A1), the National Institute of Diabetes and Digestive and Kidney Diseases (K01DK107791), and the Population Research Infrastructure Program (R24 HD050924) awarded to the Carolina Population Center at The University of North Carolina at Chapel Hill by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Author disclosures: The authors report no conflicts of interest.
Supplemental Figure 1 is available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/jn/.
Abbreviations used: AHEI, Alternative Healthy Eating Index–2010; DP, dietary pattern; HCHS/SOL, Hispanic Community Health Study/Study of Latinos; KMO, Kaiser–Meyer–Olkin; PCA, principal component analysis; PFA, principal factor analysis.
Contributor Information
Luis E Maldonado, Carolina Population Center, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; Department of Nutrition, Gillings School of Global Public Health, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Linda S Adair, Carolina Population Center, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; Department of Nutrition, Gillings School of Global Public Health, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Daniela Sotres-Alvarez, Carolina Population Center, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; Department of Biostatistics, Gillings School of Global Public Health, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Josiemer Mattei, Department of Nutrition, Harvard TH Chan School of Public Health, Boston, MA, USA.
Yasmin Mossavar-Rahmani, Department of Epidemiology & Population Health, Albert Einstein College of Medicine, Bronx, NY, USA.
Krista M Perreira, Carolina Population Center, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; Department of Social Medicine, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Martha L Daviglus, Institute for Minority Health Research, University of Illinois College of Medicine, Chicago, IL, USA.
Linda V Van Horn, Department of Preventive Medicine, Northwestern University, Chicago, IL, USA.
Linda C Gallo, Department of Psychology, San Diego State University, San Diego, CA, USA.
Carmen R Isasi, Department of Epidemiology & Population Health, Albert Einstein College of Medicine, Bronx, NY, USA.
Sandra S Albrecht, Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, NY, USA.
References
- 1.US Census Bureau. QuickFacts: United States. 2019[Internet]. [cited 17, February 17, 2020]. Available from: https://www.census.gov/quickfacts/fact/table/US#. [Google Scholar]
- 2.Gallo LC, Penedo FJ, Carnethon M, Isasi C, Sotres-Alvarez D, Malcarne VL, Roesch SC, Youngblood ME, Daviglus ML, Gonzalez P. The Hispanic Community Health Study/Study of Latinos sociocultural ancillary study: sample, design, and procedures. Ethn Dis. 2014;24(1):77. [PMC free article] [PubMed] [Google Scholar]
- 3.López L, Golden SH. A new era in understanding diabetes disparities among US Latinos—all are not equal. Diabetes Care. 2014;37(8):2081–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.González Burchard E, Borrell LN, Choudhry S, Naqvi M, Tsai H-J, Rodriguez-Santana JR, Chapela R, Rogers SD, Mei R, Rodriguez-Cintron W. Latino populations: a unique opportunity for the study of race, genetics, and social environment in epidemiological research. Am J Public Health. 2005;95(12):2161–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vespa J, Medina L, Armstrong DM. Demographic turning points for the United States: population projections for 2020 to 2060. Washington (DC): US Census Bureau; 2020. [Google Scholar]
- 6.Wang Y, Beydoun MA, Min J, Xue H, Kaminsky LA, Cheskin LJ. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020;49(3):810–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mendola N, Chen T, Gu Q, Eberhardt M, Saydah S. Prevalence of total, diagnosed, and undiagnosed diabetes among adults: United States, 2013–2016. NCHS Data Brief No. 319. 2018:1–8. [PubMed] [Google Scholar]
- 8.Schneiderman N, Llabre M, Cowie CC, Barnhart J, Carnethon M, Gallo LC, Giachello AL, Heiss G, Kaplan RC, LaVange LM. Prevalence of diabetes among Hispanics/Latinos from diverse backgrounds: the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Diabetes Care. 2014;37(8):2233–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Isasi CR, Ayala GX, Sotres-Alvarez D, Madanat H, Penedo F, Loria CM, Elder JP, Daviglus ML, Barnhart J, Siega-Riz AM. Is acculturation related to obesity in Hispanic/Latino adults? Results from the Hispanic Community Health Study/Study of Latinos. J Obes. 2015;2015:186276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Siega-Riz AM, Sotres-Alvarez D, Ayala GX, Ginsberg M, Himes JH, Liu K, Loria CM, Mossavar-Rahmani Y, Rock CL, Rodriguez B. Food-group and nutrient-density intakes by Hispanic and Latino backgrounds in the Hispanic Community Health Study/Study of Latinos. Am J Clin Nutr. 2014;99(6):1487–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Casagrande SS, Sotres-Alvarez D, Avilés-Santa L, O'Brien MJ, Palacios C, Pérez CM, Reina SA, Wang X, Qi Q, Giachello AL. Variations of dietary intake by glycemic status and Hispanic/Latino heritage in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). BMJ Open Diabetes Res Care. 2018;6(1):e000486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13(1):3–9. [DOI] [PubMed] [Google Scholar]
- 13.Corsino L, Sotres-Alvarez D, Butera NM, Siega-Riz AM, Palacios C, Pérez CM, Albrecht SS, Giacinto RAE, Perera MJ, Van Horn L. Association of the DASH dietary pattern with insulin resistance and diabetes in US Hispanic/Latino adults: results from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). BMJ Open Diabetes Res Care. 2017;5(1):e000402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mattei J, Sotres-Alvarez D, Daviglus ML, Gallo LC, Gellman M, Hu FB, Tucker KL, Willett WC, Siega-Riz AM, Van Horn L. Diet quality and its association with cardiometabolic risk factors vary by Hispanic and Latino ethnic background in the Hispanic Community Health Study/Study of Latinos. J Nutr. 2016;146(10):2035–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hodge A, Bassett J. What can we learn from dietary pattern analysis?. Public Health Nutr. 2016;19(2):191–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Noel SE, Newby P, Ordovas JM, Tucker KL. A traditional rice and beans pattern is associated with metabolic syndrome in Puerto Rican older adults. J Nutr. 2009;139(7):1360–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sofianou A, Fung TT, Tucker KL. Differences in diet pattern adherence by nativity and duration of US residence in the Mexican-American population. J Am Diet Assoc. 2011;111(10):1563–1569.e2. [DOI] [PubMed] [Google Scholar]
- 18.Radford J. Key findings about U.S. immigrants. [Internet]. 2019; [cited 17 February, 2020]. Available from: https://www.pewresearch.org/fact-tank/2019/06/17/key-findings-about-u-s-immigrants/.
- 19.Abraido-Lanza AF, Chao MT, Flórez KR. Do healthy behaviors decline with greater acculturation? Implications for the Latino mortality paradox. Soc Sci Med. 2005;61(6):1243–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ayala GX, Baquero B, Klinger S. A systematic review of the relationship between acculturation and diet among Latinos in the United States: implications for future research. J Am Diet Assoc. 2008;108(8):1330–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Maldonado LE, Albrecht SS. Does the immigrant advantage in overweight/obesity persist over time in Mexican American youth? NHANES 1988–1994 to 2005–2014. Obesity. 2018;26(6):1057–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Batis C, Hernandez-Barrera L, Barquera S, Rivera JA, Popkin BM. Food acculturation drives dietary differences among Mexicans, Mexican Americans, and non-Hispanic whites. J Nutr. 2011;141(10):1898–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Barcenas CH, Wilkinson AV, Strom SS, Cao Y, Saunders KC, Mahabir S, Hernández-Valero MA, Forman MR, Spitz MR, Bondy ML. Birthplace, years of residence in the United States, and obesity among Mexican-American adults. Obesity. 2007;15(4):1043–52. [DOI] [PubMed] [Google Scholar]
- 24.Van Hook J, Quiros S, Frisco ML, Fikru E. It is hard to swim upstream: dietary acculturation among Mexican-origin children. Population Res Policy Rev. 2016;35(2):177–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Monroe KR, Hankin JH, Pike MC, Henderson BE, Stram DO, Park S, Nomura AM, Wilkens LR, Kolonel LN. Correlation of dietary intake and colorectal cancer incidence among Mexican-American migrants: the Multiethnic Cohort Study. Nutr Cancer. 2003;45(2):133–47. [DOI] [PubMed] [Google Scholar]
- 26.Norman S, Castro C, Albright C, King A. Comparing acculturation models in evaluating dietary habits among low-income Hispanic women. Ethn Dis. 2004;14(3):399–404. [PubMed] [Google Scholar]
- 27.Van Rompay MI, McKeown NM, Castaneda-Sceppa C, Falcon LM, Ordovás JM, Tucker KL. Acculturation and sociocultural influences on dietary intake and health status among Puerto Rican adults in Massachusetts. J Acad Nutr Diet. 2012;112(1):64–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Himmelgreen DA, Bretnall A, Perez-Escamilla R, Peng Y, Bermudez A. Birthplace, length of time in the US, and language are associated with diet among inner-city Puerto Rican women keywords. Ecol Food Nutr. 2005;44(2):105–22. [Google Scholar]
- 29.Mattei J, McClain AC, Falcón LM, Noel SE, Tucker KL. Dietary acculturation among Puerto Rican adults varies by acculturation construct and dietary measure. J Nutr. 2018;148(11):1804–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sorlie PD, Avilés-Santa LM, Wassertheil-Smoller S, Kaplan RC, Daviglus ML, Giachello AL, Schneiderman N, Raij L, Talavera G, Allison M. Design and implementation of the Hispanic Community Health Study/Study of Latinos. Ann Epidemiol. 2010;20(8):629–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.LaVange LM, Kalsbeek WD, Sorlie PD, Avilés-Santa LM, Kaplan RC, Barnhart J, Liu K, Giachello A, Lee DJ, Ryan J. Sample design and cohort selection in the Hispanic Community Health Study/Study of Latinos. Ann Epidemiol. 2010;20(8):642–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kershaw KN, Giacinto RE, Gonzalez F, Isasi CR, Salgado H, Stamler J, Talavera GA, Tarraf W, Van Horn L, Wu D. Relationships of nativity and length of residence in the US with favorable cardiovascular health among Hispanics/Latinos: the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prev Med. 2016;89:84–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nutrition Data System for Research (NDS-R) version 2011. NDS-R software, 1998–1999 Regents of the University of Minnesota. Minneapolis (MN): Nutrition Coordinating Center, University of Minnesota. [Google Scholar]
- 34.Davis NJ, Schechter CB, Ortega F, Rosen R, Wylie-Rosett J, Walker EA. Dietary patterns in blacks and Hispanics with diagnosed diabetes in New York City's South Bronx. Am J Clin Nutr. 2013;97(4):878–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Popkin BM, Haines P, Siega-Riz A. Dietary patterns and trends in the United States: the UNC-CH approach. Appetite. 1999;32(1):8–14. [DOI] [PubMed] [Google Scholar]
- 36.Zhang J, Wang H, Wang Y, Xue H, Wang Z, Du W, Su C, Zhang J, Jiang H, Zhai F. Dietary patterns and their associations with childhood obesity in China. Br J Nutr. 2015;113(12):1978–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gougeon L, Payette H, Morais J, Gaudreau P, Shatenstein B, Gray-Donald K. Dietary patterns and incidence of depression in a cohort of community-dwelling older Canadians. J Nutr Health Aging. 2015;19(4):431–6. [DOI] [PubMed] [Google Scholar]
- 38.Batis C, Mendez MA, Gordon-Larsen P, Sotres-Alvarez D, Adair L, Popkin B. Using both principal component analysis and reduced rank regression to study dietary patterns and diabetes in Chinese adults. Public Health Nutr. 2016;19(2):195–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Batis C, Sotres-Alvarez D, Gordon-Larsen P, Mendez MA, Adair L, Popkin B. Longitudinal analysis of dietary patterns in Chinese adults from 1991 to 2009. Br J Nutr. 2014;111(8):1441–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chiuve SE, Fung TT, Rimm EB, Hu FB, McCullough ML, Wang M, Stampfer MJ, Willett WC. Alternative dietary indices both strongly predict risk of chronic disease. J Nutr. 2012;142(6):1009–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.McCullough ML, Feskanich D, Stampfer MJ, Giovannucci EL, Rimm EB, Hu FB, Spiegelman D, Hunter DJ, Colditz GA, Willett WC. Diet quality and major chronic disease risk in men and women: moving toward improved dietary guidance. Am J Clin Nutr. 2002;76(6):1261–71. [DOI] [PubMed] [Google Scholar]
- 42.Liese AD, Krebs-Smith SM, Subar AF, George SM, Harmon BE, Neuhouser ML, Boushey CJ, Schap TE, Reedy J. The dietary patterns methods project: synthesis of findings across cohorts and relevance to dietary guidance. J Nutr. 2015;145(3):393–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tooze JA, Kipnis V, Buckman DW, Carroll RJ, Freedman LS, Guenther PM, Krebs-Smith SM, Subar AF, Dodd KW. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: the NCI method. Stat Med. 2010;29(27):2857–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.StataCorp. Stata 14 base reference manual. College Station (TX): Stata Press;2015. [Google Scholar]
- 45.Newby P, Tucker KL. Empirically derived eating patterns using factor or cluster analysis: a review. Nutr Rev. 2004;62(5):177–203. [DOI] [PubMed] [Google Scholar]
- 46.Holgado-Tello FP, Chacón-Moscoso S, Barbero-García I, Vila-Abad E. Polychoric versus Pearson correlations in exploratory and confirmatory factor analysis of ordinal variables. Quality Quantity 2010;44(1):153. [Google Scholar]
- 47.UCLA Statistical Consulting Group. Principal component analysis, SPSS annotated output. [Internet]. n.d.; [cited January 5, 2021]. Available from https://stats.idre.ucla.edu/spss/output/principal_components/.
- 48.Humphrey-Murto S, Varpio L, Wood TJ, Gonsalves C, Ufholz L-A, Mascioli K, Wang C, Foth T. The use of the Delphi and other consensus group methods in medical education research: a review. Acad Med. 2017;92(10):1491–8. [DOI] [PubMed] [Google Scholar]
- 49.Judd SE, Letter AJ, Shikany JM, Roth DL, Newby P. Dietary patterns derived using exploratory and confirmatory factor analysis are stable and generalizable across race, region, and gender subgroups in the REGARDS study. Front Nutr. 2015;1:29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Jannasch F, Riordan F, Andersen LF, Schulze MB. Exploratory dietary patterns: a systematic review of methods applied in pan-European studies and of validation studies. Br J Nutr. 2018;120(6):601–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.UCLA Statistical Consulting. Factor analysis, Stata annotated output. [Internet]. 2019[cited January 6, 2021]. Available from: https://stats.idre.ucla.edu/stata/output/factor-analysis/.
- 52.Mohammadifard N, Talaei M, Sadeghi M, Oveisegharan S, Golshahi J, Esmaillzadeh A, Sarrafzadegan N. Dietary patterns and mortality from cardiovascular disease: Isfahan Cohort Study. Eur J Clin Nutr. 2017;71(2):252. [DOI] [PubMed] [Google Scholar]
- 53.Wu F, Wills K, Laslett LL, Oldenburg B, Jones G, Winzenberg T. Associations of dietary patterns with bone mass, muscle strength and balance in a cohort of Australian middle-aged women. Br J Nutr. 2017;118(8):598–606. [DOI] [PubMed] [Google Scholar]
- 54.Pala V, Lissner L, Hebestreit A, Lanfer A, Sieri S, Siani A, Huybrechts I, Kambek L, Molnar D, Tornaritis M. Dietary patterns and longitudinal change in body mass in European children: a follow-up study on the IDEFICS multicenter cohort. Eur J Clin Nutr. 2013;67(10):1042. [DOI] [PubMed] [Google Scholar]
- 55.McClain AC, Ayala GX, Sotres-Alvarez D, Siega-Riz AM, Kaplan RC, Gellman MD, Gallo LC, Van Horn L, Daviglus ML, Perera MJ. Frequency of intake and type of away-from-home foods consumed are associated with diet quality in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). J Nutr. 2018;148(3):453–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Duffey KJ, Gordon-Larsen P, Ayala GX, Popkin BM. Birthplace is associated with more adverse dietary profiles for US-born than for foreign-born Latino adults. J Nutr. 2008;138(12):2428–35. [DOI] [PubMed] [Google Scholar]
- 57.Siega-Riz AM, Pace ND, Butera NM, Van Horn L, Daviglus ML, Harnack L, Mossavar-Rahmani Y, Rock CL, Pereira RI, Sotres-Alvarez D. How well do US Hispanics adhere to the Dietary Guidelines for Americans? Results from the Hispanic Community Health Study/Study of Latinos. Health Equity. 2019;3(1):319–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Satia JA. Dietary acculturation and the nutrition transition: an overview. Appl Physiol Nutr Metab. 2010;35(2):219–23. [DOI] [PubMed] [Google Scholar]
- 59.McEvoy CT, Cardwell CR, Woodside JV, Young IS, Hunter SJ, McKinley MC. A posteriori dietary patterns are related to risk of type 2 diabetes: findings from a systematic review and meta-analysis. J Acad Nutr Diet. 2014;114(11):1759–1775. e4. [DOI] [PubMed] [Google Scholar]
- 60.Schulze MB, Hu FB. Dietary patterns and risk of hypertension, type 2 diabetes mellitus, and coronary heart disease. Curr Atheroscler Rep. 2002;4(6):462–7. [DOI] [PubMed] [Google Scholar]
- 61.Perez-Escamilla R. Acculturation, nutrition, and health disparities in Latinos. Am J Clin Nutr. 2011;93(5):1163S–7S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Asghari G, Rezazadeh A, Hosseini-Esfahani F, Mehrabi Y, Mirmiran P, Azizi F. Reliability, comparative validity and stability of dietary patterns derived from an FFQ in the Tehran Lipid and Glucose Study. Br J Nutr. 2012;108(6):1109–17. [DOI] [PubMed] [Google Scholar]
- 63.Khani BR, Ye W, Terry P, Wolk A. Reproducibility and validity of major dietary patterns among Swedish women assessed with a food-frequency questionnaire. J Nutr. 2004;134(6):1541–5. [DOI] [PubMed] [Google Scholar]
- 64.Sotos-Prieto M, Mattei J. Mediterranean diet and cardiometabolic diseases in racial/ethnic minority populations in the United States. Nutrients. 2018;10(3):352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Mossavar-Rahmani Y, Shaw PA, Wong WW, Sotres-Alvarez D, Gellman MD, Van Horn L, Stoutenberg M, Daviglus ML, Wylie-Rosett J, Siega-Riz AM. Applying recovery biomarkers to calibrate self-report measures of energy and protein in the Hispanic Community Health Study/Study of Latinos. Am J Epidemiol. 2015;181(12):996–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kaiser L. What can binational studies reveal about acculturation, food insecurity, and diet?. J Am Diet Assoc. 2009;109(12):1997–2000. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.