

Description
A young student was resistance training at the gym when he developed a headache and collapsed. On waking, there was left-sided facial weakness, visual extinction and sensory loss. Investigations revealed a right internal carotid artery dissection (ICAD) and M1 thrombus. Intravenous thrombolysis was given, but he deteriorated (National Institutes of Health Stroke Scale, 14 to 20). He was referred to interventional radiology and successfully treated with mechanical clot retrieval and ICAD stenting (figure 1). A right frontal lobe infarct was evident on CT (figure 2). Dual antiplatelets were prescribed for 3 months followed by lifelong single antiplatelet. He had no stroke risk factors or medical history. On reviewing his CT images, bilateral elongated styloid processes (ESP) were identified; 7.4 cm for the right and 7.0 cm for the left (normal less than 3 cm) (figure 1). The patient declined stylectomy, but he made a full recovery and the only problem at 3 years is low mood.
Figure 1.
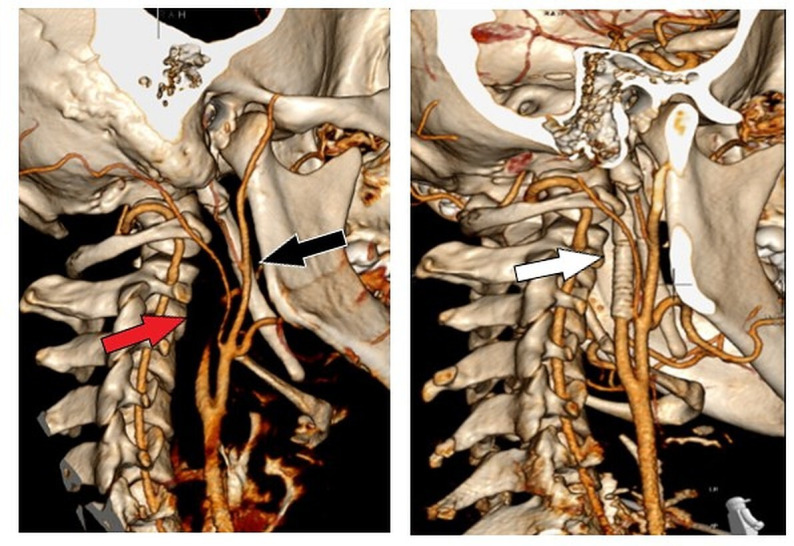
Left: reconstructed CT image demonstrating absence of flow in right internal carotid artery (red arrow) and right-sided elongated styloid process which has two pseudoarticulations (black arrow). Right: Postprocedure reconstructed image demonstrating stent adjacent to styloid process (white arrow).
Figure 2.
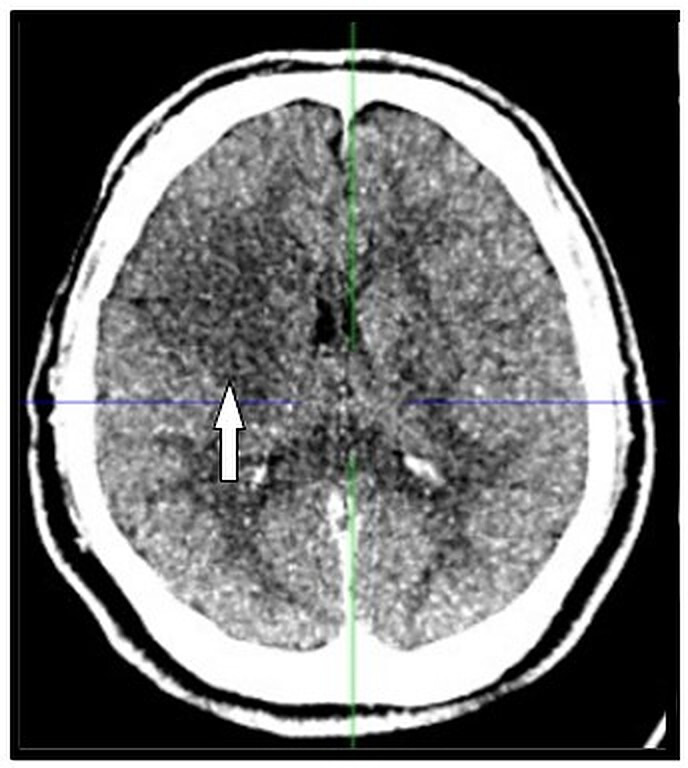
Head CT demonstrating evolving infarction of right frontal lobe (white arrow).
An elongated styloid process, which can include a calcified stylohyoid ligament, does not usually cause symptoms.1 Rarely, some develop pain due to contact with neurovascular structures in what is known as Eagle syndrome after the otolaryngologist describing it in 1937.2 Our patient never had symptoms of Eagle syndrome. ICAD due to ESP is rare, but well described.3 4 Some authors have identified ESP length or ESP angulation and carotid artery proximity as being important risk factors for ICAD, but others have demonstrated that these factors have no relation.5–7 Triggering events like exercise and neck massage are commonly seen, but most are spontaneous.3 4 The initial treatment of ICAD due to ESP resembles that of ICAD and stroke, with many authors opting for medical management with or without early endovascular intervention.3 4 Like our patient, many with ICAD due to ESP have early deterioration despite medical management, so they should be monitored with a low threshold for referral to interventional radiology or otolaryngology. Definitive treatment of Eagle syndrome is resection, but the role of ESP resection for ICAD is unclear.8 Late complications can occur in patients without ESP resection, namely recurrent stroke, carotid stent fracture, persistent ICA stenosis with dissection flap, stent displacement and pseudoaneurysm formation, so stylectomy or delayed imaging should be considered.9–12
Learning points.
Dissection is a common cause of ischaemic stroke in young patients.
In patients with spontaneous or low energy dissection, review images for an elongated styloid process.
Consider monitoring in these patients as early and late deterioration is reported.
Footnotes
Contributors: MT composed the manuscript. LI directed the project. AS and DJW were responsible for interpreting imaging. All authors were involved in the design and review of the manuscript and the literature.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer-reviewed.
Ethics statements
Patient consent for publication
Obtained.
References
- 1.Gokce C, Sisman Y, Sipahioglu M. Styloid process elongation or Eagle's syndrome: is there any role for ectopic calcification? Eur J Dent 2008;2:224–8. [PMC free article] [PubMed] [Google Scholar]
- 2.Eagle WW. Elongated styloid processes: report of two cases. Arch Otolaryngol 1937;25:584–7. 10.1001/archotol.1937.00650010656008 [DOI] [Google Scholar]
- 3.Zammit M, Chircop C, Attard V, et al. Eagle’s syndrome: a piercing matter. BMJ Case Rep 2018;11:e226611–6. 10.1136/bcr-2018-226611 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ogura T, Mineharu Y, Todo K, et al. Carotid artery dissection caused by an elongated styloid process: three case reports and review of the literature. NMC Case Rep J 2015;2:21–5. 10.2176/nmccrj.2014-0179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Raser JM, Mullen MT, Kasner SE, et al. Cervical carotid artery dissection is associated with styloid process length. Neurology 2011;77:2061–6. 10.1212/WNL.0b013e31823b4729 [DOI] [PubMed] [Google Scholar]
- 6.Tardivo V, Castaldi A, Baldino G, et al. Internal carotid artery dissection related to abnormalities of styloid process: is it only a matter of length? Neurol Sci 2021. 10.1007/s10072-021-05350-8. [Epub ahead of print: 31 May 2021]. [DOI] [PubMed] [Google Scholar]
- 7.Cruddas L, Joffe M, Baker D. Can styloid process and internal carotid artery anatomy be used to predict carotid artery dissection? Ann Vasc Surg 2021;74:105–10. 10.1016/j.avsg.2020.12.034 [DOI] [PubMed] [Google Scholar]
- 8.Ceylan A, Köybaşioğlu A, Çelenk F, et al. Surgical treatment of elongated styloid process: experience of 61 cases. Skull Base 2008;18:289–95. 10.1055/s-0028-1086057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sveinsson O, Kostulas N, Herrman L. Internal carotid dissection caused by an elongated styloid process (Eagle syndrome). BMJ Case Rep 2013:2–5. 10.1136/bcr-2013-009878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hooker JD, Joyner DA, Farley EP, et al. Carotid stent fracture from Stylocarotid syndrome. J Radiol Case Rep 2016;10:1–8. 10.3941/jrcr.v10i6.1618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mann A, Kujath S, Friedell ML, et al. Eagle syndrome presenting after blunt trauma. Ann Vasc Surg 2017;40:295.e5–295.e8. 10.1016/j.avsg.2016.07.077 [DOI] [PubMed] [Google Scholar]
- 12.Shimozato R, Hayashi M, Niimura M, et al. Two patients with cerebral infarction who underwent endovascular treatment for internal carotid artery dissection related to an elongated styloid process. Noushinkei Kekkannai Tiryou 2018;12:355–61. 10.5797/jnet.cr.2017-0102 [DOI] [Google Scholar]