

Abstract
Background and Aims
Although prevalence of chronic hepatitis B (CHB) in the USA includes 0.42 million (range, 0.28‐0.67) U.S.‐born persons, foreign‐born (FB) persons contribute a substantially larger number to the burden of CHB in the USA. Over the past decade, patterns of U.S. immigration have changed and many countries have implemented HBV prevention programs. This study aims to estimate the number of FB persons with CHB in the USA by country of origin, updating our 2011 study.
Approach and Results
We performed systematic searches for articles published in 2009–2019 reporting HBsAg seroprevalence in emigrants and in‐country populations of 117 countries. Data meeting inclusion criteria were combined with data from our 2011 study to calculate pooled prevalence estimates for 99 countries using meta‐analyses (total 2,800 surveys involving 112 million subjects). Combining country‐specific CHB rate estimates with the number of FB in the USA in 2018, by country of origin from the U.S. Census Bureau, we estimate that the number of FB with CHB in the USA in 2018 was 1.47 million (95% CI, 1.21‐1.73), substantially higher than previously reported. The weighted average CHB prevalence for all FB in the USA in 2018 was 3.07%. Approximately 59% of FB with CHB in the USA in 2018 emigrated from Asia, 19% from the Americas, and 15% from Africa. Subgroup analyses found that for many countries, CHB rates are higher in males than females and have declined over the past three decades, but no consistent pattern is observed between emigrant and in‐country rates.
Conclusions
Including FB and U.S.‐born persons, the total prevalence of CHB in the USA may be as high as 2.4 million.
Abbreviations
- ACS
American Community Survey
- CHB
chronic hepatitis B
- CLDF
Chronic Liver Disease Foundation
- FB
foreign‐born
- FE
fixed effect
- M
million
- NHANES
National Health and Nutrition Examination Surveys
- PUMS
Public Use Microdata Sample
- RE
random effects
Foreign‐born (FB) persons contribute disproportionately to the burden of chronic hepatitis B (CHB) in the USA, comprising 14% of the population and 60%‐90% of persons living with CHB.( 1, 2, 3, 4 ) Few reports enumerating this large at‐risk population have been published, and existing estimates are likely underestimates because of the difficulties in capturing accurate survey data from the culturally, socially, and linguistically diverse groups that make up the FB population.( 3 )
In 2009, we estimated that 1.3 million (M) FB with CHB were living in the USA based on systematic review and meta‐analysis of reports of HBsAg seroprevalence in 102 countries from which FB emigrate to the USA.( 5 ) In the past decade, the number of FB persons living in the USA has increased by 25% and patterns of immigration have changed, with a larger proportion of FB originating in Asia, Africa, and other regions with high HBV endemicity. In addition, HBsAg prevalence in many countries has likely declined given that countries have implemented immunization programs, routine antenatal testing, and other HBV prevention measures.( 6 )
The aim of this study was to estimate the number of FB persons living with CHB in the USA in 2018 by country of origin. The 2011 analysis was updated by incorporating changes in the size and composition of FB populations in the USA from 2009 to 2018 and country‐specific HBV epidemiological data published during the past decade. The update includes a systematic review of articles published from 1980 to 2019 reporting HBsAg seroprevalence in 102 countries, calculation of country‐specific prevalence rates using meta‐analytical methods, and a combination of these rates with the 2018 FB populations from each country reported by the U.S. Census Bureau to estimate the number of FB with CHB living in the USA in 2018. These estimates of CHB among diverse FB communities and cultural characteristics of the affected populations can guide providers and policy makers to allocate the necessary resources to prevent, test, and treat CHB in the USA.
Materials and Methods
Results of the systematic review are reported using applicable components of the Meta‐Analysis of Observational Studies in Epidemiology recommendations.( 7 ) Components are shown in aggregate for country‐specific searches and reviews. Results for individual countries are available in Supporting Table S1 and at Plan A website https://www.plan‐a.com/data.html.
Foreign‐Born Populations Living in the United States
FB populations by country of birth and decade of entry are from the 2018 U.S. Census Bureau American Community Survey (ACS) Public Use Microdata Sample (PUMS).( 1 ) The PUMS includes persons living in housing units and group quarters without regard to legal status. The ACS assumes that undocumented persons participate and adjusts for 10% undercounting.( 1, 8 )
Search Strategy
Country‐specific PubMed searches were conducted March 20, 2020 to identify articles reporting HBsAg seroprevalence surveys published January 1, 2009 to December 31, 2019. Country searches were organized into 17 world regions as defined in the PubMed geographical locations tree (Table 1). Each search combined a country name and corresponding demonym(s) with free‐text search terms: hepatitis B or HBsAg and epidemiological studies, prevalence, or seroprevalence, migrant, immigrant, or refugee, used individually and in combination separated by logical operators “AND” or “OR” as appropriate (Supporting Table S2). For Japan, Northern America, Australia, New Zealand, and Southern, Northern, and Western Europe, which have low CHB rates, rates from reviews were used instead of rates from systematic reviews and meta‐analyses.( 9 )
TABLE 1.
CHB Prevalence Estimates From RE Meta‐Analyses and Number of FB With CHB Living in the USA by Country of Origin
| Country/Region | FB Living in the USA, 2018 (PUMS) | CHB Prevalence Estimate (%) | No. of FB With CHB in the USA | ||||
|---|---|---|---|---|---|---|---|
| RE Pooled Prevalence Rate | Lower 95% CI | Upper 95% CI | Mid‐Range Prevalence | Lower 95% CI | Upper 95% CI | ||
| Asia | 14,785,266 | 5.88% | 5.34% | 6.43% | 869,787 | 789,155 | 950,279 |
| Americas | 24,410,150 | 1.12% | 0.65% | 1.60% | 274,081 | 159,137 | 389,343 |
| Oceania | 297,510 | 4.46% | 3.40% | 5.51% | 13,261 | 10,120 | 16,400 |
| Africa | 2,575,550 | 8.65% | 6.98% | 10.32% | 222,779 | 179,724 | 265,782 |
| Europe | 5,894,567 | 1.54% | 1.22% | 1.86% | 90,649 | 71,806 | 109,655 |
| All regions | 47,963,043 | 3.07% | 2.52% | 3.61% | 1,470,557 | 1,209,942 | 1,731,458 |
| Asia | 14,785,266 | 5.88% | 5.34% | 6.43% | 869,787 | 789,155 | 950,279 |
| Eastern Asia | 4,639,824 | 7.00% | 6.75% | 7.25% | 324,967 | 313,269 | 336,455 |
| Mainland China (including Hong Kong) | 2,527,241 | 8.46% | 8.30% | 8.62% | 213,805 | 209,761 | 217,848 |
| Taiwan | 404,329 | 12.93% | 12.32% | 13.53% | 52,280 | 49,813 | 54,706 |
| Korea | 1,133,728 | 4.61% | 4.16% | 5.05% | 52,265 | 47,163 | 57,253 |
| Japan | 560,538 | 1.02% | 1.01% | 1.02% | 5,717 | 5,661 | 5,717 |
| Eastern Asia, other/n.s. | 13,988 | 6.44% | 6.22% | 6.65% | 901 | 870 | 930 |
| South Eastern Asia | 4,529,616 | 8.43% | 7.51% | 9.35% | 382,021 | 340,180 | 423,623 |
| Philippines | 2,168,566 | 7.03% | 6.13% | 7.92% | 152,450 | 132,933 | 171,750 |
| Vietnam | 1,365,908 | 11.71% | 10.92% | 12.50% | 159,948 | 149,157 | 170,739 |
| Thailand | 289,335 | 6.04% | 5.51% | 6.56% | 17,476 | 15,942 | 18,980 |
| Laos | 189,131 | 9.43% | 7.80% | 11.05% | 17,835 | 14,752 | 20,899 |
| Cambodia | 144,093 | 9.00% | 6.96% | 11.04% | 12,968 | 10,029 | 15,908 |
| Indonesia | 101,501 | 4.06% | 3.39% | 4.74% | 4,121 | 3,441 | 4,811 |
| Myanmar | 145,864 | 8.46% | 6.79% | 10.14% | 12,340 | 9,904 | 14,791 |
| Malaysia | 84,316 | 3.07% | 2.47% | 3.67% | 2,589 | 2,083 | 3,094 |
| Singapore | 40,902 | 5.61% | 4.74% | 6.48% | 2,295 | 1,939 | 2,650 |
| South Central Asia | 4,264,431 | 2.84% | 2.45% | 3.24% | 121,067 | 104,354 | 138,001 |
| India | 2,670,106 | 2.50% | 2.30% | 2.69% | 66,753 | 61,412 | 71,826 |
| Iran | 397,203 | 2.34% | 1.96% | 2.73% | 9,295 | 7,785 | 10,844 |
| Pakistan | 400,978 | 3.78% | 3.28% | 4.29% | 15,157 | 13,152 | 17,202 |
| Bangladesh | 281,578 | 4.51% | 3.67% | 5.36% | 12,699 | 10,334 | 15,093 |
| Afghanistan | 119,003 | 4.06% | 3.04% | 5.08% | 4,832 | 3,618 | 6,045 |
| Uzbekistan | 74,008 | 6.34% | 4.22% | 8.46% | 4,692 | 3,123 | 6,261 |
| Nepal | 151,248 | 1.58% | 1.18% | 1.98% | 2,390 | 1,785 | 2,995 |
| Sri Lanka | 52,894 | 2.41% | −0.72% | 5.53% | 1,275 | 0 | 2,925 |
| Kazakhstan | 30,431 | 4.95%† | 3.34% | 6.56% | 1,506 | 1,016 | 1,996 |
| South Central Asia, other/n.s. | 86,982 | 2.84% | 2.45% | 3.24% | 2,469 | 2,129 | 2,815 |
| Western Asia | 1,257,218 | 2.88% | 2.09% | 3.67% | 36,191 | 26,325 | 46,147 |
| Iraq | 250,435 | 1.19% | 0.62% | 1.76% | 2,980 | 1,553 | 4,408 |
| Israel | 163,156 | 0.77% | 0.64% | 0.90% | 1,256 | 1,044 | 1,468 |
| Lebanon | 135,345 | 1.42% | 1.00% | 1.84% | 1,922 | 1,353 | 2,490 |
| Turkey | 150,341 | 4.47% | 4.08% | 4.86% | 6,720 | 6,134 | 7,307 |
| Armenia | 92,327 | 0.71% | 0.29% | 1.13% | 656 | 268 | 1,043 |
| Syria | 113,654 | 1.75% | 1.30% | 2.21% | 1,989 | 1,478 | 2,512 |
| Jordan | 87,888 | 6.36% | 3.72% | 9.00% | 5,590 | 3,269 | 7,910 |
| Saudi Arabia | 91,085 | 5.51% | 4.93% | 6.09% | 5,019 | 4,490 | 5,547 |
| Yemen | 64,556 | 10.44% | 7.88% | 13.00% | 6,740 | 5,087 | 8,392 |
| Kuwait | 39,318 | 2.66% | −0.19% | 5.52% | 1,046 | 0 | 2,170 |
| Azerbaijan | 23,015 | 3.38% | 2.71% | 4.04% | 778 | 624 | 930 |
| Georgia | 20,125 | 3.72% | 2.39% | 5.05% | 749 | 481 | 1,016 |
| Western Asia, other/n.s. | 25,973 | 2.88% | 2.09% | 3.67% | 748 | 544 | 953 |
| Asia, not specified | 94,177 | 5.88% | 5.34% | 6.43% | 5,540 | 5,027 | 6,053 |
| Americas | 24,410,150 | 1.12% | 0.65% | 1.60% | 274,081 | 159,137 | 389,343 |
| Central America | 15,275,916 | 0.45% | 0.30% | 0.61% | 68,882 | 45,163 | 92,685 |
| Mexico | 11,549,703 | 0.38% | 0.26% | 0.49% | 43,889 | 30,029 | 56,594 |
| El Salvador | 1,452,848 | 0.44% | 0.33% | 0.55% | 6,393 | 4,794 | 7,991 |
| Guatemala | 1,038,393 | 1.05% | 0.66% | 1.44% | 10,903 | 6,853 | 14,953 |
| Honduras | 663,876 | 0.51% | 0.35% | 0.68% | 3,386 | 2,324 | 4,514 |
| Nicaragua | 270,471 | 0.68% | −0.41% | 1.78% | 1,839 | 0 | 4,814 |
| Panama | 153,402 | 0.83% | 0.52% | 1.13% | 1,273 | 798 | 1,733 |
| Costa Rica | 96,525 | 0.57%† | −0.07% | 1.20% | 550 | 0 | 1,158 |
| Belize | 50,698 | 1.28% | 0.72% | 1.83% | 649 | 365 | 928 |
| Caribbean | 4,656,720 | 3.19% | 1.72% | 4.67% | 148,600 | 80,035 | 217,321 |
| Cuba | 1,372,576 | 0.90% | 0.70% | 1.10% | 12,353 | 9,608 | 15,098 |
| Dominican Republic | 1,234,737 | 5.04% | 2.84% | 7.25% | 62,231 | 35,067 | 89,518 |
| Jamaica | 776,242 | 3.94% | 0.81% | 7.07% | 30,584 | 6,288 | 54,880 |
| Haiti | 718,111 | 4.60% | 3.24% | 5.96% | 33,033 | 23,267 | 42,799 |
| Trinidad and Tobago | 229,145 | 0.71% | 0.49% | 0.94% | 1,627 | 1,123 | 2,154 |
| Barbados | 58,522 | 0.41% | 0.15% | 0.67% | 240 | 88 | 392 |
| Caribbean, other/n.s. | 267,387 | 3.19% | 1.72% | 4.67% | 8,533 | 4,596 | 12,478 |
| South America | 3,479,059 | 1.41% | 0.76% | 2.05% | 48,946 | 26,566 | 71,304 |
| Colombia | 825,787 | 0.84% | 0.00% | 1.68% | 6,937 | 0 | 13,873 |
| Ecuador | 457,873 | 0.47% | 0.42% | 0.51% | 2,152 | 1,923 | 2,335 |
| Peru | 488,139 | 1.82% | 1.28% | 2.36% | 8,884 | 6,248 | 11,520 |
| Brazil | 513,965 | 1.37% | 1.23% | 1.52% | 7,041 | 6,322 | 7,812 |
| Guyana | 287,911 | 3.96%* | 2.21% | 5.70% | 11,401 | 6,363 | 16,411 |
| Argentina | 203,915 | 0.41% | 0.20% | 0.62% | 836 | 408 | 1,264 |
| Venezuela | 422,418 | 1.93% | 1.13% | 2.73% | 8,153 | 4,773 | 11,532 |
| Chile | 111,774 | 0.40%† | 0.11% | 0.69% | 447 | 123 | 771 |
| Bolivia | 85,723 | 3.03% | 0.08% | 5.98% | 2,597 | 69 | 5,126 |
| Uruguay | 50,626 | 0.38% | 0.30% | 0.46% | 192 | 152 | 233 |
| Paraguay | 20,806 | 0.78% | 0.52% | 1.05% | 162 | 108 | 218 |
| South America, other/n.s. | 10,122 | 1.41% | 0.76% | 2.05% | 142 | 77 | 207 |
| Northern America | 980,525 | 0.76% | 0.74% | 0.79% | 7,452 | 7,256 | 7,746 |
| Canada | 963,388 | 0.76% | 0.74% | 0.79% | 7,322 | 7,129 | 7,611 |
| Northern America, other/n.s. | 17,137 | 0.76% | 0.74% | 0.79% | 130 | 127 | 135 |
| Americas, not specified | 17,930 | 1.12% | 0.65% | 1.60% | 201 | 117 | 286 |
| Oceania | 297,510 | 4.46% | 3.40% | 5.51% | 13,261 | 10,120 | 16,400 |
| Australia | 107,071 | 0.37% | 0.36% | 0.38% | 396 | 385 | 407 |
| New Zealand | 36,252 | 4.11% | 4.04% | 4.18% | 1,490 | 1,465 | 1,515 |
| Fiji | 49,573 | 4.63% | 3.26% | 6.00% | 2,295 | 1,616 | 2,974 |
| Tonga | 17,636 | 12.00% | 8.04% | 15.97% | 2,116 | 1,418 | 2,816 |
| Micronesia | 32,438 | 14.28% | 10.77% | 17.79% | 4,632 | 3,494 | 5,771 |
| Samoa | 12,682 | 3.67% | 2.52% | 4.81% | 465 | 320 | 610 |
| Oceania, other/n.s. | 41,858 | 4.46% | 3.40% | 5.51% | 1,866 | 1,423 | 2,306 |
| Africa | 2,575,550 | 8.65% | 6.98% | 10.32% | 222,779 | 179,724 | 265,782 |
| Eastern Africa | 741,178 | 7.84% | 6.24% | 9.45% | 58,143 | 46,243 | 70,030 |
| Ethiopia | 295,970 | 7.44% | 6.50% | 8.38% | 22,020 | 19,238 | 24,802 |
| Kenya | 163,398 | 5.99% | 4.59% | 7.38% | 9,788 | 7,500 | 12,059 |
| Somalia | 101,011 | 10.42% | 8.05% | 12.79% | 10,525 | 8,131 | 12,919 |
| Uganda | 35,836 | 9.25% | 7.06% | 11.45% | 3,315 | 2,530 | 4,103 |
| Eritrea | 45,878 | 8.20% | 4.25% | 12.15% | 3,762 | 1,950 | 5,574 |
| Tanzania | 21,483 | 5.80% | 4.85% | 6.75% | 1,246 | 1,042 | 1,450 |
| Zimbabwe | 29,875 | 12.53% | 9.62% | 15.44% | 3,743 | 2,874 | 4,613 |
| Eastern Africa, other/n.s. | 47,727 | 7.84% | 6.24% | 9.45% | 3,744 | 2,978 | 4,509 |
| Middle Africa | 162,788 | 9.36% | 7.57% | 11.14% | 15,237 | 12,323 | 18,135 |
| Cameroon | 81,190 | 9.36% | 7.57% | 11.14% | 7,599 | 6,146 | 9,045 |
| Middle Africa, other/n.s. | 81,598 | 9.36% | 7.57% | 11.14% | 7,638 | 6,177 | 9,090 |
| Northern Africa | 433,036 | 5.52% | 4.29% | 6.74% | 23,888 | 18,595 | 29,176 |
| Egypt | 224,905 | 4.14% | 3.57% | 4.71% | 9,311 | 8,029 | 10,593 |
| Morocco | 84,690 | 1.93% | 1.44% | 2.41% | 1,635 | 1,220 | 2,041 |
| Sudan | 70,223 | 14.06% | 11.48% | 16.64% | 9,873 | 8,062 | 11,685 |
| Algeria | 23,307 | 6.09% | 0.00% | 12.19% | 1,419 | 0 | 2,841 |
| Northern Africa, other/n.s. | 29,911 | 5.52% | 4.29% | 6.74% | 1,650 | 1,284 | 2,015 |
| Southern Africa | 128,640 | 5.68% | 4.42% | 6.93% | 7,307 | 5,686 | 8,915 |
| South Africa | 108,660 | 5.68% | 4.42% | 6.93% | 6,172 | 4,803 | 7,530 |
| Southern Africa, other/n.s. | 19,980 | 5.68% | 4.42% | 6.93% | 1,135 | 883 | 1,385 |
| Western Africa | 960,077 | 10.96% | 9.00% | 12.92% | 105,244 | 86,422 | 124,065 |
| Nigeria | 397,555 | 10.24% | 9.27% | 11.21% | 40,710 | 36,853 | 44,566 |
| Ghana | 205,277 | 9.82% | 7.91% | 11.73% | 20,158 | 16,237 | 24,079 |
| Liberia | 90,793 | 16.54% | 11.55% | 21.53% | 15,017 | 10,487 | 19,548 |
| Cape Verde | 38,435 | 5.65% | 0.16% | 11.14% | 2,172 | 61 | 4,282 |
| Sierra Leone | 54,671 | 12.51% | 10.64% | 14.38% | 6,839 | 5,817 | 7,862 |
| Senegal | 32,863 | 12.38% | 10.41% | 14.35% | 4,068 | 3,421 | 4,716 |
| Guinea | 22,337 | 14.90% | 13.03% | 16.77% | 3,328 | 2,911 | 3,746 |
| Western Africa, other/n.s. | 118,146 | 10.96% | 9.00% | 12.92% | 12,951 | 10,635 | 15,267 |
| Africa, not specified | 149,831 | 8.65% | 6.98% | 10.32% | 12,960 | 10,455 | 15,462 |
| Europe | 5,894,567 | 1.54% | 1.22% | 1.86% | 90,649 | 71,806 | 109,655 |
| Eastern Europe | 2,166,197 | 3.05% | 2.25% | 3.85% | 66,105 | 48,698 | 83,432 |
| Poland | 415,200 | 1.33% | 0.97% | 1.68% | 5,522 | 4,027 | 6,975 |
| Russia | 396,680 | 2.73% | 2.28% | 3.18% | 10,829 | 9,044 | 12,614 |
| Ukraine | 343,192 | 1.68% | 0.55% | 2.80% | 5,766 | 1,888 | 9,609 |
| Romania | 170,493 | 6.41% | 5.90% | 6.91% | 10,929 | 10,059 | 11,781 |
| Yugoslavia | 36,223 | 3.98% | 1.32% | 6.64% | 1,442 | 478 | 2,405 |
| Bosnia and Herzegovina | 111,510 | 1.51% | 0.73% | 2.30% | 1,684 | 814 | 2,565 |
| Hungary | 72,307 | 1.07% | 0.03% | 2.12% | 774 | 22 | 1,533 |
| Albania | 95,436 | 10.89% | 9.78% | 11.99% | 10,393 | 9,334 | 11,443 |
| Czech Republic and Slovakia | 65,787 | 1.43% | 0.97% | 1.90% | 941 | 638 | 1,250 |
| Belarus | 74,057 | 2.97% | 1.68% | 4.27% | 2,199 | 1,244 | 3,162 |
| Bulgaria | 80,429 | 4.14% | 2.81% | 5.47% | 3,330 | 2,260 | 4,399 |
| Moldova | 47,170 | 9.75% | 7.55% | 11.96% | 4,599 | 3,561 | 5,642 |
| Croatia | 38,807 | 1.34% | 0.76% | 1.92% | 520 | 295 | 745 |
| Former USSR | 70,258 | 3.83% | 2.74% | 4.91% | 2,691 | 1,925 | 3,450 |
| Lithuania | 33,237 | 2.03% | 1.37% | 2.69% | 675 | 455 | 894 |
| Latvia | 24,665 | 1.39% | 1.10% | 1.67% | 343 | 271 | 412 |
| Macedonia | 25,940 | 5.75%* | 3.56% | 7.93% | 1,492 | 923 | 2,057 |
| Eastern Europe, other/n.s. | 64,806 | 3.05% | 2.25% | 3.85% | 1,978 | 1,458 | 2,495 |
| Southern Europe | 878,517 | 1.56% | 1.49% | 1.64% | 13,738 | 13,119 | 14,439 |
| Italy | 394,857 | 2.52% | 2.49% | 2.54% | 9,950 | 9,832 | 10,029 |
| Portugal | 183,628 | 1.02% | 0.78% | 1.31% | 1,873 | 1,432 | 2,406 |
| Greece | 141,937 | 0.97% | 0.95% | 1.00% | 1,377 | 1,348 | 1,419 |
| Spain | 158,095 | 0.34% | 0.32% | 0.37% | 538 | 506 | 585 |
| Northern/Western Europe | 2,816,583 | 0.37% | 0.34% | 0.40% | 10,295 | 9,584 | 11,165 |
| UK | 882,828 | 0.01% | 0.01% | 0.01% | 88 | 88 | 88 |
| Germany | 1,149,413 | 0.70% | 0.65% | 0.76% | 8,046 | 7,471 | 8,736 |
| France | 253,868 | 0.26% | 0.25% | 0.27% | 660 | 635 | 685 |
| Ireland | 141,434 | 0.03% | 0.01% | 0.07% | 42 | 14 | 99 |
| Netherlands | 104,658 | 0.40% | 0.39% | 0.41% | 419 | 408 | 429 |
| No./West Europe, other/n.s. | 284,382 | 0.37% | 0.34% | 0.40% | 1,039 | 968 | 1,127 |
| Europe, not specified | 33,270 | 1.54% | 1.22% | 1.86% | 512 | 405 | 619 |
Rate shown for subregion or region and for “other/n.s.” is the weighted average for subregion or region.
Rates have been rounded to two decimal places.
Northern America = FB from Canada and Bermuda living in the USA.
For Northern America, Japan, Australia, New Zealand, and Northern and Western Europe, which have low CHB rates and relatively modest numbers of emigrants to the USA, rates from a few large population studies were used instead of rates from a systematic review and meta‐analysis.
Only one study available; rates are as reported with 95% CIs from standard error.
RE rate cannot be calculated because tau2 <0; FE rate is shown.
Abbreviations: n.s., not specified; USSR, Union of Soviet Socialist Republics.
Study Selection and Data Extraction
Search results were downloaded to country‐specific EndNote libraries (EndNote X8.2; Clarivate Analytics, Philadelphia, PA); records were labeled by country and aggregated with search results from other countries into regional libraries for screening and review. No duplicates were present in country‐specific libraries; duplicates within regional libraries were retained to allow tabulation of reviews for each country. Regional libraries were screened at title and abstract level and potentially relevant full‐text articles accessed and examined for eligibility. Relevant data extracted into standardized country‐specific Excel databases included: country, location and date of survey, description of sample population(s), sampling method, age and sex composition of sample, HBsAg seroprevalence and assay method, bibliographical information, comments, and source of article. Resources precluded retrieval of all potentially relevant articles in languages other than English; articles were included if an English abstract provided sufficient data. A best effort was made to translate accessible full‐text non‐English articles using Google Translate. Additional eligible articles were identified from reviews and citations in articles from PubMed searches. Many articles report data from more than one HBsAg serosurvey (e.g., different groups and/or locations within a country or from persons from multiple countries). Where possible, data were parsed into separate surveys for the meta‐analyses (e.g., as a survey for each location sampled). When multiple parsing options were possible (e.g., by sex or by location), parsing by sex was given priority.
Inclusion Criteria
Studies included in the meta‐analyses reported original data on HBsAg seroprevalence in general populations of countries of origin and emigrants to other countries. HBsAg seroprevalence was assumed to represent prevalence of chronic HBV infection; data using any HBsAg assay were allowed. In‐country studies included surveys of the general population (e.g., national surveys and groups such as pregnant women, military recruits, factory workers, university students, persons attending routine health checkups or community screening events). Emigrant surveys included immigrants, refugees, or asylum seekers who left their home country for other destination countries. Surveys in blood donors, who generally have lower HBV infection rates than the general population, were not used unless other data were limited. Surveys in persons at higher risk for HBV infection (e.g., health‐care workers, injection drug users, persons with immunodeficiency, or certain infectious diseases) were excluded. Data were parsed to include only rates for adults and teens; surveys reporting on children only were excluded. Studies in indigenous populations (e.g., Inuit and Amazonian tribes) with HBsAg prevalence higher than the nonindigenous population were excluded. An exception was made for the Hmong, a proportion of whom emigrated from Laos and may self‐identify as Laotian in census surveys.( 10 ) Other inclusion criteria include a minimum sample size of 50 and publication in 1980 or later in peer‐reviewed journals, except as noted (e.g., government reports). Complete criteria are shown in Supporting Table S3.
Statistical Analysis
Pooled CHB prevalence estimates were calculated for each country of origin using random effects (RE) meta‐analyses based on all surveys that met inclusion criteria, including surveys used in our 2011 study and new surveys from the 2019 systematic review. RE meta‐analysis, which assumes heterogeneity among surveys (i.e., that true CHB rates differ among different populations), was considered appropriate for studies conducted in different populations in different locations and at different times within a country. Between‐survey heterogeneity for meta‐analyses for each country was assessed using the I2 statistic (Supporting Table S5; 10‐12). Country‐specific pooled prevalence rates using fixed effect (FE) meta‐analysis, which assumes observed differences in seroprevalence are attributable to sampling error only, were calculated for comparison with RE results and for country data sets where RE analysis was not possible (e.g., RE tau2 <0). Subgroup analyses compared pooled RE CHB rates for emigrants versus in‐country populations, males versus females, and surveys conducted in four different decades from before 1990‐2019. Differences between subgroups were assessed using a Z‐test.( 11 )
To estimate the number of FB with CHB in the USA in 2018 by country of origin, pooled CHB rates from country‐specific RE meta‐analyses were multiplied by the number of FB from each country living in the USA in 2018.( 1 ) Prevalence estimates for FB by world region and for the total FB population from all countries were calculated from country‐specific rates weighted by the number of FB from each country living in the USA in 2018.
Results
Search Results
Table 2 summarizes results of the 2019 systematic review aggregated in major world regions. A Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) diagram (Fig. 1) shows the aggregated results for all country‐specific searches and includes duplicates, retained to allow tabulations for each country. Data for 17 subregions and individual countries are available in Supporting Table S1. More than 20,000 articles were identified in the 2019 PubMed searches. After exclusions at the title and abstract level, 3,184 full‐text articles were assessed (including 605 duplicates), and 723 articles (638 unique articles reporting HBsAg survey data from 974 surveys involving 94.3M subjects) met criteria for inclusion in the meta‐analyses. These surveys, combined with 1,826 surveys from our 2011 meta‐analyses, provided 2,800 HBsAg seroprevalence surveys involving 112M subjects for the updated meta‐analyses (Table 3). Of these, 457 were surveys in emigrants (involving 1.2M subjects from 65 countries) and 2,343 were surveys of populations living in countries of origin (involving 110.8M subjects in 98 countries). Approximately 21% of the surveys were conducted before 1990, 25% from 1990 to 1999, 33% from 2000 to 2009, and 20% in 2010 and later. Overall, 27% of the 112.0M survey participants were male and 58% female; sex was not reported for 15% of the sample. Greater representation of females reflects antenatal screening. In some surveys, data are reported in aggregate without sex distribution, and rates by sex could not be quantified. Data by country are shown in Supporting Table S4.
TABLE 2.
Results of Systematic Review: HBsAg Seroprevalence Articles Identified in PubMed (2009‐2019) by World Region
| Country/Region | 2019 Country‐Specific PubMed Searches | 2009 Meta‐Analysis | 2019 Meta‐Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Articles Identified in Country Searches | Articles Excluded at Title Abstract | Full‐Text Articles Evaluated | Articles Excluded at Full‐Text Review | Eligible Articles From 2019 Country Searches | Eligible Articles From Other Sources | Total Eligible Articles From 2019 Searches | Eligible Articles From 2009 Meta‐Analysis | Total Articles in 2019 Country Meta‐Analysis | No. of Surveys in Country Meta‐Analysis | |
| Asia | 16,103 | 14,218 | 1,885 | 1,525 | 360 | 85 | 445 | 705 | 1,150 | 1,685 |
| Americas | 1,007 | 743 | 264 | 229 | 35 | 6 | 41 | 155 | 196 | 286 |
| Oceania | 26 | 0 | 26 | 21 | 5 | 5 | 10 | 20 | 30 | 62 |
| Africa | 2,347 | 1,570 | 777 | 635 | 142 | 48 | 190 | 226 | 416 | 578 |
| Europe | 830 | 598 | 232 | 208 | 24 | 13 | 37 | 109 | 146 | 189 |
| All regions | 20,313 | 17,129 | 3,184 | 2,618 | 566 | 157 | 723 | 1,215 | 1,938 | 2,800 |
Totals shown are the sum of country results and are not deduplicated.
Individual country searches contain no duplicate records; regional duplicates were retained to allow tabulation of reviews for each country.
Other sources for a given country include articles found in searches for other countries and citations from reviews and articles found in PubMed searches.
For Japan, Northern America, Australia, New Zealand, and Southern, Northern, and Western Europe, which have low CHB rates and relatively modest numbers of emigrants to the USA, rates from reviews were used instead of rates from systematic reviews and meta‐analyses. Male‐specific data and female‐specific data from the same survey were entered separately and counted as two surveys.
FIG. 1.
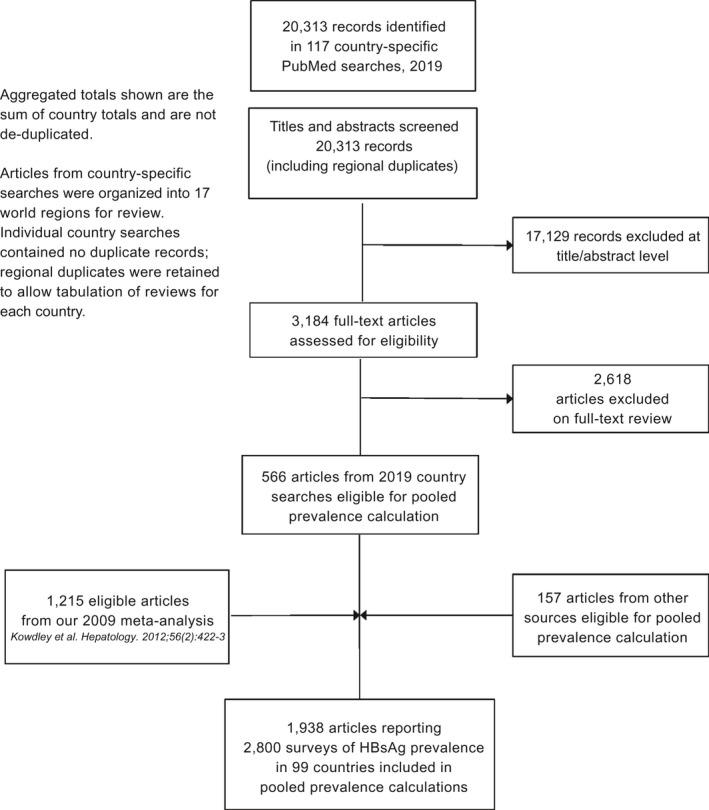
Flowchart of PubMed searches and study selection for 2019 systematic review (aggregate results for 99 country‐specific searches).
TABLE 3.
Surveys in Emigrants and in General In‐Country Populations Included in the Meta‐Analyses by World Region
| World Region | FB Living in USA, 2018 | Total No. of Surveys | Surveys by Date | Total Sample No. | Survey Sample Composition by Sex | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before 1990 | 1990‐1999 | 2000‐2009 | 2010‐2019 | Males | Females | Sex Not Specified | ||||
| All surveys | ||||||||||
| Asia | 14,785,266 | 1,685 | 310 | 395 | 637 | 343 | 106,772,038 | 29,956,751 | 63,921,096 | 12,894,191 |
| Americas | 24,410,150 | 286 | 51 | 128 | 81 | 26 | 2,868,724 | 101,004 | 334,515 | 2,433,205 |
| Oceania | 297,510 | 62 | 28 | 15 | 18 | 1 | 77,311 | 4,529 | 37,315 | 35,467 |
| Africa | 2,575,550 | 578 | 165 | 115 | 123 | 175 | 632,984 | 251,468 | 261,742 | 119,774 |
| Europe | 5,894,567 | 189 | 42 | 56 | 65 | 26 | 1,642,136 | 50,162 | 526,312 | 1,065,662 |
| All regions | 47,963,043 | 2,800 | 596 | 709 | 924 | 571 | 111,993,193 | 30,363,914 | 65,080,980 | 16,548,299 |
| Surveys in emigrants from country of origin to USA and elsewhere | ||||||||||
| Asia | 14,785,266 | 305 | 58 | 41 | 135 | 71 | 994,475 | 183,971 | 371,223 | 439,281 |
| Americas | 24,410,150 | 27 | 11 | 3 | 11 | 2 | 37,033 | 278 | 3,074 | 33,681 |
| Oceania | 297,510 | 11 | 1 | 3 | 7 | — | 45,470 | — | 14,003 | 31,467 |
| Africa | 2,575,550 | 66 | 9 | 8 | 21 | 28 | 54,837 | 5,422 | 13,277 | 36,138 |
| Europe | 5,894,567 | 48 | 4 | 20 | 14 | 10 | 29,768 | 2,483 | 8,906 | 18,379 |
| All regions | 47,963,043 | 457 | 83 | 75 | 188 | 111 | 1,161,583 | 192,154 | 410,483 | 558,946 |
| Surveys in general populations living in country of origin | ||||||||||
| Asia | 14,785,266 | 1,380 | 252 | 354 | 502 | 272 | 105,777,563 | 29,772,780 | 63,549,873 | 12,454,910 |
| Americas | 24,410,150 | 259 | 40 | 125 | 70 | 24 | 2,831,691 | 100,726 | 331,441 | 2,399,524 |
| Oceania | 297,510 | 51 | 27 | 12 | 11 | 1 | 31,841 | 4,529 | 23,312 | 4,000 |
| Africa | 2,575,550 | 512 | 156 | 107 | 102 | 147 | 578,147 | 246,046 | 248,465 | 83,636 |
| Europe | 5,894,567 | 141 | 38 | 36 | 51 | 16 | 1,612,368 | 47,679 | 517,406 | 1,047,283 |
| All regions | 47,963,043 | 2,343 | 513 | 634 | 736 | 460 | 110,831,610 | 30,171,760 | 64,670,497 | 15,989,353 |
Northern America = FB from Canada and Bermuda living in the USA.
For Japan, Northern America, Australia, New Zealand, and Southern, Northern, and Western Europe, which have low CHB rates and relatively modest numbers of emigrants to the USA, rates from reviews were used instead of rates from systematic review and meta‐analyses. Male‐specific data and female‐specific data from the same survey were entered separately and counted as two surveys.
Results for individual countries are available in Supporting Table S4 (Supporting Information).
FB Population
The FB population in the USA increased by 25% (from 38.4M to 48.0M) from 2009 to 2018 and patterns of immigration shifted, with larger numbers of FB originating in Asia, Africa, and Oceania—regions with intermediate and high HBV endemicity.( 1 ) From 2009 to 2018, FB from Africa, Oceania, and Asia living in the USA increased by 75%, 59%, and 39%, respectively. Nearly half (4.1M) of the 9.5M additional FB persons living in the USA in 2018 compared to 2009 were born in Asia, including 1.6M from South Central Asia; an additional 1.2M originated in the Caribbean and 1.1M in Africa (Table 1).
Seroprevalence Surveys by Country
Data from surveys used in each country‐specific meta‐analysis are available at https://www.plan‐a.com/data.html. Availability of HBsAg seroprevalence data varied by region and was sparse for many countries. For the 99 countries for which CHB rates were calculated, the median number of surveys per country was 11 (mean, 28.3; range, 1‐362); for 22 countries, five or fewer surveys were found. More than half (60%; 1,685) of all surveys were from Asia, including 598 from mainland China and Taiwan. Although Central Americans comprise the largest FB population in the USA, only 72 surveys from this region (27 from Mexico) were found. Most surveys from El Salvador, Honduras, Panama, and Belize were in blood donors and likely under‐represent HBV prevalence in the general population. Surveys from Eastern Europe and Oceania were sparse and small.
For most countries, reported HBsAg seroprevalence varied substantially from survey to survey. For example, HBsAg seroprevalence reported in 39 new surveys for India ranged from 0.33% among emigrants to Australia to 6.1% among adults in the Ladakh region. Wide variations in rates were observed in surveys among emigrants as well as in‐country populations; this heterogeneity was expected, given that surveys were conducted in different populations at different times in different locations using different sampling methods.
CHB Pooled Prevalence Estimates From Meta‐Analyses
Country‐specific CHB pooled prevalence rates were calculated for each country using RE meta‐analyses (Table 1). Rates were <1% in northern and western Europe, Australia, Canada, and most of Central and South America. The highest CHB rate estimates were in Africa: Liberia 16.5%, Guinea 14.9%, Sudan 14.1%, Zimbabwe 12.5%, Sierra Leone 12.5%, and Senegal 12.4%. Relatively high rates were also found for Oceania (Micronesia 14.3%; Tonga 12.0%) and for countries in Eastern and South Eastern Asia (Taiwan 12.9%, Vietnam 11.7%), Western Asia (Yemen 10.4%), and Eastern Europe (Albania 10.9%). In the Americas, the highest pooled CHB rates were in the Dominican Republic (5.0%) and Haiti (4.6%).
Consistent with the wide variation in reported prevalence within each country, confidence intervals for country‐specific RE pooled CHB rate estimates are broad (Table 1). Cochran’s Q test and I2 statistic for each country‐specific RE meta‐analysis support high heterogeneity among surveys for most countries (Supporting Table S5). The I2 statistic was ≥55% (indicating substantial heterogeneity) for the meta‐analyses for all except two countries.( 12, 13 )
Country‐Specific Prevalence Estimates in Emigrants and In‐Country Populations
To compare CHB rates in emigrants to rates in populations who remain in their country of origin, country‐specific CHB pooled rates were calculated using surveys from emigrants only and in‐country populations only. Data were found for emigrants from 65 countries and in‐country data for 98 countries (Supporting Table S6). For 38 of the 64 countries for which comparison was possible, RE pooled CHB prevalence rates in emigrant surveys did not differ significantly from rates in in‐country surveys (P > 0.05). For nine countries, rates were significantly higher (P < 0.05) in emigrant surveys (China, Laos, Cambodia, Myanmar, Nepal, Armenia, Azerbaijan, Ethiopia, and Albania). For 17 countries, rates from in‐country surveys were significantly higher (P < 0.05).
Country‐Specific CHB Prevalence Estimates by Survey Date
To assess time trends in CHB rates, country‐specific RE pooled prevalence rates were calculated for surveys conducted in each of the past four decades (i.e., before 1990, 1990‐1999, 2000‐2009, and 2010‐2019; Supporting Table S7). Data were sufficient to compare rates for 49 countries (516 surveys conducted 2010‐2019; 503 surveys conducted before 1990). Pooled CHB rates from surveys conducted 2010‐2019 were significantly lower (P < 0.05) than those conducted before 1990 for 31 countries and significantly higher for two countries (Indonesia, Czech Republic/Slovakia). Significant decreases over these decades were noted for mainland China, Taiwan, and Korea and for all assessable countries in South Eastern and Western Asia except Azerbaijan and Lebanon. Data from Central America were insufficient for analysis. Data from Africa were sparse; significant decreases were noted for Egypt, Morocco, Sudan, Ethiopia, Cameroon, South Africa, and Nigeria.
Country‐Specific CHB Prevalence Estimates by Sex
Higher HBsAg prevalence has been reported in males than in females in many populations.( 14 ) Country‐specific, sex‐specific RE pooled CHB rates were calculated for males and females for 64 countries for which sex‐specific data were available. We found 1,086 surveys in 83 countries reporting female‐specific data and 554 surveys in 66 countries reporting male‐specific data (Supporting Table S8). Pooled CHB rates were higher in males than females in surveys from 49 of 64 assessable countries, although this difference reached statistical significance (P < 0.05) in only 28 of 64 countries. Rates were significantly higher for females in surveys from two countries (Yemen and Mexico).
Number of FB With CHB Living in the USA
Using FB populations from ACS and country‐specific CHB pooled rates from the mid‐range RE meta‐analyses, we estimate that the number of FB with CHB living in the USA in 2018 was 1.47M persons (95% CI, 1.21‐1.73; Table 1). Approximately 59% (0.87M; 95% CI, 0.79‐0.95) of FB with CHB emigrated from Asia, 19% (0.27M; 95% CI, 0.16‐0.39) from the Americas—the majority from the Caribbean, and 15% (0.22M; 95% CI, 0.18‐0.27) from Africa (Fig. 2). The six countries from which the largest number of FB with CHB originated were mainland China including Hong Kong (213,805; 8.46% of 2.53M FB), Vietnam (159,948; 11.7% of 1.37M FB), Philippines (152,450; 7.0% of 2.17M FB), India (66,753; 2.5% of 2.67M FB), Dominican Republic (62,231; 5.04% of 1.23M FB), and Taiwan (52,280; 12.9% of 404,329 FB). In 2018, FB from these six countries comprise 707,466 persons or 48% of the total FB with CHB. The weighted average CHB prevalence for FB in the USA from each world region was calculated using country‐specific CHB rates weighted by the number of FB from each country in the region living in the USA in 2018 (Table 1). The highest regional CHB prevalence was found for Africa (8.65%; 95% CI, 6.98‐10.32), followed by Asia (5.88%; 95% CI, 5.34‐6.43) and Oceania (4.46%; 95% CI, 3.40‐5.51). The weighted average CHB prevalence estimate for all FB from all world regions living in the USA in 2018 from RE meta‐analysis was 3.07% (95% CI, 2.52‐3.61).
FIG. 2.
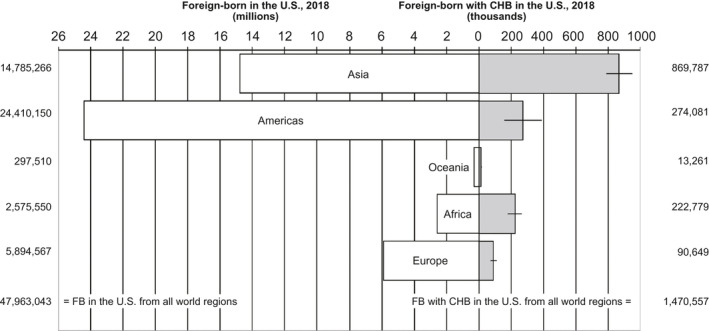
FB populations living in the USA and number of FB with CHB living in the USA from RE meta‐analysis by world region of origin, 2018. *Northern America = FB from Canada and Bermuda living in the USA.
An alternative calculation using country‐specific CHB rates from FE meta‐analyses combined with the number of FB by country of origin yields an estimate of 924,857 (95% CI, 870,623‐980,684) FB with CHB in the USA in 2018, ~37% lower than the estimate of 1.47M using rates from RE meta‐analyses (Fig. 3). The weighted average CHB prevalence estimate for all FB from all world regions living in the USA in 2018 was 1.93% (95% CI, 1.82‐2.04). The large difference from the RE estimate results from the different methods used for weighting the studies in FE versus RE meta‐analyses.( 11 )
FIG. 3.
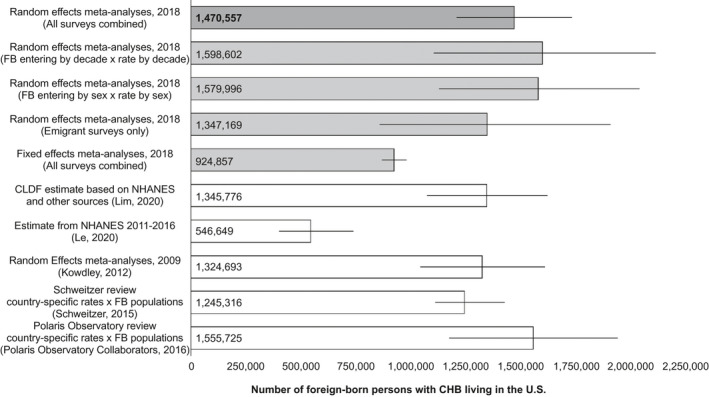
Number of FB persons with CHB living in the USA: comparison of estimates. *Northern America = FB from Canada and Bermuda living in the USA.
Number of FB With CHB Estimated From Emigrant Surveys
Based on the assumption that prevalence rates in emigrants better represent rates among FB in the USA than rates in persons who remain in their home countries, the number of FB living with CHB in the USA was calculated using country‐specific RE pooled prevalence rates from surveys of emigrants only (Fig. 3). Substituting emigrant‐only CHB rates (available for 65 countries) yields an estimate of 1.35M (95% CI, 0.86‐1.91) FB with CHB living in the USA in 2018, ~8% lower than the number calculated using all surveys combined (emigrants and in‐country populations). The weighted average CHB prevalence for all FB in the USA in 2018 using available emigrant‐only surveys is 2.81% (95% CI, 1.79‐3.97).
Number of FB With CHB Estimated From Decade‐Specific Prevalence Rates and Populations
Subgroup analyses above found that country‐specific pooled CHB rates were significantly lower in surveys conducted 2010‐2019 than in surveys conducted before 1990 for 31 of 49 assessable countries. To assess the impact of these changes over time, an alternative calculation was done based on the assumption that CHB rates in FB persons living in the USA in 2018 were comparable to rates in their home countries at the time they emigrated. The number of FB living in the USA in 2018 who arrived from each country during each of the past four decades (i.e., before 1990, 1990‐1999, 2000‐2009, and 2010‐2019) was combined with country‐specific RE CHB rates calculated from surveys conducted in the corresponding decade. Approximately 31% of all FB living in the USA in 2018 arrived before 1990 and 21%‐25% in each succeeding decade (Supporting Table S9); proportions vary by country of origin, with a greater percentage of emigrants from Africa and Asia arriving in later decades. The calculation stratified by decade yields an estimate of 1.60M (95% CI, 1.11‐2.11) FB with CHB in the USA in 2018 (Fig. 3)—within the confidence interval of the estimate of 1.47M (95% CI, 1.21‐1.73) using pooled rates from all surveys from all decades and all FB arriving in all years. Because few surveys were available for many countries, prevalence estimates for decade‐stratified calculations have greater uncertainty (Fig. 3). The weighted average pooled CHB prevalence rate for all FB arriving each decade shows a nonsignificant trend toward decline over time: 4.25% (95% CI, 2.79‐5.75), 3.34% (95% CI, 2.27‐4.46), 2.84% (95% CI, 2.11‐3.59), and 2.63% (95% CI, 1.89‐3.43).
Number of FB With CHB Estimated From Sex‐Specific Surveys
Approximately 48% of the FB living in the USA in 2018 were male and 52% female. Male‐specific survey data were available for 66 countries and female‐specific data for 83 countries. A calculation substituting available country‐specific, sex‐specific CHB rates from RE meta‐analyses (Supporting Table S8) combined with the number of FB of each sex by country of origin yields an estimate of 1.58M (95% CI, 1.13‐2.04) FB with CHB in the USA in 2018, within the confidence interval of the estimate of 1.47M using rates from RE meta‐analyses with all surveys for each country combined (Fig. 3). Based on this sex‐specific calculation, males made up 56% of the FB with CHB in 2018.
Total Number of Persons With CHB in the USA
The National Health and Nutrition Examination Survey (NHANES) from 2011 to 2016 estimates 0.30M (range, 0.20‐0.47) U.S.‐born persons with CHB in the USA( 2 ) Adjusting for the increase in the 2018 U.S. population, the Chronic Liver Disease Foundation (CLDF) estimated 0.42M (range, 0.28‐0.67) U.S.‐born with CHB in the USA in 2018.( 15 ) Combining the estimate of 1.47M (95% CI, 1.21‐1.73) FB with CHB from this analysis with the CLDF estimate for U.S.‐born with CHB suggests as many as 1.89M (range, 1.49‐2.40) persons chronically infected with HBV (FB and U.S.‐born) living in the USA in 2018.
Discussion
Our updated systematic review and meta‐analysis from 1980 to 2019 incorporated changes that have occurred over the past decade, including an increase in the FB population in the USA, increased immigration from HBV endemic regions, and changes in country‐specific CHB prevalence rates resulting from HBV prevention programs. We estimate that the number of FB with CHB living in the U.S. in 2018 was 1.47M (95% CI, 1.21‐1.73), an increase of 11% from 1.32M (95% CI, 1.04‐1.61) in 2009.( 5 ) Assuming 0.42M (95% CI, 0.28‐0.67) U.S.‐born persons with CHB in 2018, as many as 1.89M (range, 1.49‐2.40) persons with CHB (FB and U.S.‐born) may be living in the USA in 2018—80% of whom acquired their infection in their country of birth.
The increase in FB with CHB in the USA in 2018 can be attributed to a 25% increase in the FB population over the past decade and a greater proportion of FB from regions with high HBV endemicity.( 1 ) Offsetting the population increase, CHB rates likely declined in many countries. Comparisons of country‐specific pooled CHB rates by survey decade showed that rates from surveys conducted in 2010‐2019 are significantly lower than rates from surveys conducted before 1990 for many countries in Asia and for a few countries in Africa. Although limited by lack of data for many countries, these results are generally consistent with studies using more robust methods to measure time changes in CHB rates (e.g., modeling rate trends).( 16 ) For the FB population in the USA as a whole, a nonsignificant trend toward lower prevalence over time was observed. The weighted average CHB prevalence for all FB from all countries living in the USA in 2018 of 3.07% (95% CI, 2.52‐3.61) is similar to what we found for 2009 (3.45%; 95% CI, 2.72‐4.19),( 5 ) which was not unexpected given the large number of surveys common to both analyses.
Subgroup analyses comparing country‐specific, sex‐specific CHB prevalence rates in males and females support previous reports that rates are higher in males than in females in many countries, although this analysis was limited by the small number of surveys for many countries. Comparison of rates from surveys in emigrants versus in‐country populations did not show a consistent pattern. For most countries (38 of 64 for which comparison was possible), CHB rates in emigrants were similar to rates in in‐country populations; for 17 of 64, in‐country prevalence was higher, and for 9 of 64, rates in emigrants were higher. This is not unexpected: Different countries may have differing proportions of emigrants with higher CHB rates (e.g., because they spent time in refugee camps) or with lower CHB rates because they had higher socioeconomic status, better health care, and resources to emigrate.
Our current estimate of 1.47M FB with CHB in the USA is substantially higher than estimates from other sources—2.7 times the estimate of 0.55M (95% CI, 0.40‐0.74) FB with CHB based on NHANES surveys from 2011 to 2016 (Fig. 3).( 2 ) Although NHANES methods were modified in 2011 to oversample Asians, these surveys may still under‐represent FB populations.( 15, 17, 18 ) The CLDF recently adjusted the NHANES estimate for FB with CHB, which is calculated by race and ethnicity, by replacing the NHANES CHB rate for FB Asians (3.5%) with a higher CHB rate (7.2%) from our 2011 study.( 5 ) Using this method, the CLDF estimated 1.08M to 1.62M FB with CHB in the USA in 2018.( 15 )
Few other prevalence estimates of FB with CHB in the USA have been reported. A study estimating the burden of CHB in the USA attributable to immigration multiplied country‐specific prevalence rates by the number of FB persons immigrating to the USA each year. They determined that 1.3M FB persons with CHB entered the USA between 1974 and 2008—4.6% of all FB entering during that time. Data include lawful permanent residents only and were not adjusted for mortality to provide a prevalence estimate. The study estimated that FB persons comprise >90% of all new cases of CHB and 96% of deaths from CHB in the USA.( 3, 19 )
Our current estimate of 1.89M total persons (FB and U.S.‐born) living with CHB in the USA in 2018 is higher than estimates from other sources, with the difference attributable to a larger FB population. NHANES surveys indicate that the total number of persons living with CHB in the USA remained at ~0.85M (range, 0.6‐1.1) from 1999 to 2016.( 2, 17 ) This is almost certainly an underestimate because populations at high risk for HBV are excluded and FB under‐represented.( 18 ) By adjusting NHANES data to include institutionalized, incarcerated, homeless, and military populations and revising the estimate for FB with CHB using a higher CHB rate for FB Asians, the CLDF estimated 1.59M (range, 1.25‐2.49) total persons with CHB (FB and U.S.‐born) in the USA in 2018, ~16% lower than our estimate with the difference attributable to our larger number of FB.( 15 )
Some country‐specific CHB rates calculated in this analysis are higher than rates reported elsewhere. To compare our pooled CHB rates (in aggregate) with country‐specific CHB rates from two recent global HBV reviews, we calculated the number of FB with CHB in the USA using ACS FB populations combined with CHB rates from the reviews.( 1, 9, 20 ) Replacing our pooled CHB rates with rates from a review that were calculated from surveys published 1965‐2013 (from a literature review) yields an estimate of 1.25M (95% CI, 1.11‐1.43) FB with CHB in the USA in 2018, ~15% lower than our mid‐range RE estimate of 1.47M (95% CI, 1.21‐1.73). The weighted average CHB rate among all FB in the USA in 2018 using available rates from this review is 2.60% compared to 3.07% from our analysis. A second review identified surveys published 1960‐2016 from a literature review and selected a rate from a single representative survey for each country based on quality assessment and expert opinion; 83% of the surveys selected for country rates were conducted after 2000 and 50% after 2010.( 20 ) Combining available country‐specific CHB rates from this review with FB populations by country of origin yields 1.56M (95% CI, 1.17‐1.94) FB with CHB in the USA in 2018, which encompasses our estimate of 1.47M (95% CI, 1.21‐1.73). CHB rates for individual countries from these reviews and our work show wide variability, highlighting difficulties inherent in estimating country‐specific prevalence rates based on limited data available. Our analysis identified the three countries from which the largest number of FB with CHB in the USA originate as China, Vietnam, and the Philippines. Our CHB rate estimate for mainland China was 8.5% (95% CI, 8.3‐8.6), compared to 5.5% (95% CI, 5.47‐5.50) for China (excluding Hong Kong) and 7.2% (range, 6.7‐7.7) for China reported in the first and second reviews, respectively. Rates for Vietnam were 11.7% (95% CI, 10.9‐12.5), 10.8% (95% CI, 10.3‐11.3), and 10.0% (range, 7.8‐12.5), and for the Philippines, 7.0% (95% CI, 6.1‐7.9), 4.6% (95% CI, 4.5‐4.7), and 16.7% (range, 14.3‐19.1).
Differences between our rates and others could result from differences in the primary HBsAg seroprevalence data included in the analyses (i.e., survey selection) and/or methods used to calculate country‐specific pooled rates. Unlike the first review, our analysis did not include surveys of children or blood donors, groups that generally have lower seroprevalence rates than adults in the general population.( 9 ) The second review excluded surveys in blood donors, but allowed surveys among persons of all ages. Our higher rates may result from the RE meta‐analysis model we used to calculate pooled country‐specific CHB rates. Other meta‐analytical methods would likely produce different estimates. Using rates from an FE model, we calculated a substantially lower estimate of FB in the USA in 2018 (0.92M vs. 1.47M with an RE model). An RE model was selected based on the heterogeneous nature of the survey data—heterogeneity was expected, observed, and supported by formal heterogeneity assessment of country‐specific meta‐analyses (i.e., I2 values). Other variations of RE models (e.g., using different weighting or data transformations) may produce different results and should be considered for future analyses.
A major limitation to this approach is the scarcity of HBsAg seroprevalence studies in many countries. Data are especially scarce for Central America and the Caribbean, regions from which large numbers of FB migrate to the USA. Literature searches were limited to PubMed; additional, potentially relevant articles may have been found in other databases. In addition, coverage of potentially relevant surveys reported in languages other than English was limited. Country‐specific pooled CHB rates were calculated using all eligible surveys identified for the country; data were not sufficient to calculate rates balanced by sex, age, and other variables to be representative of a country’s demographics. Data were not available to account for CHB‐related deaths among FB who arrived in early decades. Nationally representative surveys were included, but were unavailable for most countries. A crude adjustment for age was made by excluding recent surveys in children from the 2019 update.
Surveys used in the analysis may not be strictly representative of populations likely to immigrate to the USA. Although we included surveys of “general populations,” the demographics (age, sex, education, and economic status) of persons likely to emigrate to the USA vary by country. The limited surveys available precluded development of inclusion criteria based on specific demographics for emigrants from each country. Biases will vary from country to country and depend on the available surveys. Inclusion criteria allowed a broad range of surveys in different populations, settings, and locations. We expected prevalence rates to differ among surveys as a consequence of differences in demographics, locally dominant routes of HBV transmission, history and reach of HBV prevention programs, and other factors. For this reason, RE meta‐analysis was used to calculate a pooled weighted mean seroprevalence for the distribution of seroprevalences reported within each country.
The updated estimates of CHB prevalence among FB in the USA provide information to guide public health policies, set research priorities, and help raise greater awareness of the clinical burden of CHB among FB in the USA. The finding that as many as 1.7M FB with CHB and 2.4M total persons with CHB may be living in the USA highlights the importance of HBV screening, particularly given that >80% of CHB adults in the USA remain undiagnosed and less than half of those diagnosed receive appropriate care.( 21, 22 ). Recent updated recommendations by the U.S. Preventative Services Task Force reaffirm the importance of screening adults and adolescents at increased risk for HBV, including persons born in countries with high prevalence of HBV infection ≥2%.( 23 ) However, risk‐based testing for HBV requires accurate assessment of “risk,” contributing to suboptimal screening rates. Similar to the evolution of testing for HIV and HCV from risk‐based to universal testing, our findings and others emphasize the case for universal HBV testing to close the gap in missed diagnoses and opportunities for early linkage to care and treatment. We advocate for universal screening with HBsAg, hepatitis B surface antibody, and hepatitis B core antibody, given the importance of understanding past HBV exposure and potential risk of reactivation, identifying occult HBV infections, linking those with chronic infection to care and treatment for HBV, and assessing need for HBV vaccination, given that only ~25% of U.S. adults aged ≥19 years are vaccinated against hepatitis B and remain at risk for acute HBV infection.( 24 ) Universal screening and universal adult immunization for HBV are recommendations currently undergoing consideration by the U.S. Centers for Disease Control and Prevention and Advisory Committee on Immunization Practices.
Author Contributions
Study concept and design: all authors. Acquisition of data: Welch, Chen, S. Wong. Analysis and interpretation of the data: all authors. Statistical analyses: Welch, Chen, S. Wong. Drafting of the manuscript: R. Wong, Brosgart, Welch, Chen, S. Wong, Gish. Critical revision of the manuscript for important intellectual content: all authors. Study supervision: R. Wong, Brosgart, Gish. Drs. Wong, Brosgart, and Gish had full access to the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis.
Supporting information
Supplementary Material
Supported by an investigator‐sponsored research grant from Gilead Sciences (IN‐US‐988‐5504).
Potential conflict of interest: Dr. R. Wong consults for, advises for, is on the speakers’ bureau for, and received grants from Gilead. He received grants from AbbVie. Dr. Brosgart consults for Dynavax. She is employed by and owns stock in Enochian. Dr. Block is employed by Cirna and Hepion. He owns stock in Arbutus and Glycotest. Dr. Cohen advises for and received grants from Gilead and GlaxoSmithKline. She received grants from Janssen and Arbutus. Dr. Kim consults for and advises for Gilead. Dr. Kowdley advises for, is on the speakers’ bureau for, and received grants from Gilead. He advises for and received grants from High Tide and Intercept. He consults for Altimmune, Roche, and Boehringer Ingelheim. He advises for Assembly and Calliditas. He received grants from Janssen, Allergan, Genfit, Novartis, Enanta, and CymaBay. Dr. Lok consults for and received grants from TARGET. She consults for Ambys, Lilly, CLEAR‐B, and Huahui. She received grants from Bristol‐Myers Squibb and Gilead. Dr. Tsai advises for, is on the speakers’ bureau for, and received grants from AbbVie, Gilead, and Intercept. Dr. Ward received grants from Gilead, AbbVie, Merck, Abbott, Cepheid, Siemens, Roche, Pharco, Zydus, and Cadila. Dr. Gish consults for, advises for, is on the speakers’ bureau for, and received grants from Gilead. He consults for, advises for, and is on the speakers’ bureau for AbbVie, Bayer, Bristol‐Myers Squibb, Eisai, Intercept, and Salix. He consults for, advises for, and is on the data safety monitoring board for Arrowhead. He consults for, advises for, and owns stock in Eiger, Genlantis, and HepQuant. He consults for and advises for Abbott, Access Biologicals, Antios, Dova, Dynavax, Enyo, Forty‐Seven, Fujifilm/Wako, eStudySite, Genentech, Gerson Lehrman, HepaTX, Janssen, Helios, Lilly, Merck, Shionogi, and Viking. He consults for ADMA, AEC, Aligos, Arena, Arterys, Alexion, Altimmune, AprosTx, Cirina, Consumer Health Products Association, DiaSorin, DRG Abacus, DURECT, Echosens, Exelixis, IDLogiq, Intellia, Inotek, Iqvia, KannaLife, Laboratory for Advanced Medicine, Labyrinth Holdings, MedImmune, New Enterprise Associates, Ogilvy, Organovo, Patient Connect, ProdigY Biotech, Prometheus, Refuah Solutions, Regulus, Spring Bank, and Trimaran. He advises for Biocollections, Prodigy, and Quest. He owns stock in RiboSciences, CoCrystal, and AngioCrine.
References
- 1.U.S. Census Bureau . American Community Survey 1‐Year Public Use Microdata Sample (PUMS) Files 2018. Variables Place of birth and decade of entry. Suitland, MD: U.S. Census Bureau; 2019. [Google Scholar]
- 2.Le MH, Yeo YH, Cheung R, Henry L, Lok AS, Nguyen MH. Chronic hepatitis B prevalence among foreign‐born and U.S.‐born adults in the United States, 1999‐2016. Hepatology 2020;71:431‐443. [DOI] [PubMed] [Google Scholar]
- 3.Mitchell T, Armstrong GL, Hu DJ, Wasley A, Painter JA. The increasing burden of imported chronic hepatitis B—United States, 1974‐2008 [published correction appears in PLoS One. 2013 Mar 5;8]. PLoS One 2011;6:e27717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wasley A, Kruszon‐Moran D, Kuhnert W, Simard E, Finelli L, McQuillan G, et al. The prevalence of hepatitis B virus infection in the United States in the era of vaccination. J Infect Dis 2010;202:192‐201. [DOI] [PubMed] [Google Scholar]
- 5.Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic hepatitis B among foreign‐born persons living in the United States by country of origin. Hepatology 2012;56:422‐433. [DOI] [PubMed] [Google Scholar]
- 6.Gomes C, Wong RJ, Gish RG. Global perspective on hepatitis B virus infections in the era of effective vaccines. Clin Liver Dis 2019;23:383‐399. [DOI] [PubMed] [Google Scholar]
- 7.Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta‐analysis of observational studies in epidemiology. Meta‐analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:2008‐2015. [DOI] [PubMed] [Google Scholar]
- 8.Baker B. Estimates of the Illegal Alien Population Residing in the United States: January 2015. Washington, D.C.:U.S. Department of Homeland Security Office of Immigration Statistics; 2018. [Google Scholar]
- 9.Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 2015;386:1546‐1555. [DOI] [PubMed] [Google Scholar]
- 10.Pfeifer ME, Sullivan J, Yang K, Yang W. Hmong population and demographic trends in the 2010 census and 2010 American Community Survey. Hmong Studies J 2012;13:1‐31. [Google Scholar]
- 11.Borenstein M, Hedges IV, Higgins JP, Rothstein HR. Introduction to Meta‐analysis, 1st ed. Chichester, UK: John Wiley & Sons; 2009. [Google Scholar]
- 12.Higgins JP, Thompson SG. Quantifying heterogeneity in meta‐analysis. Stat Med 2002;21:1539‐1558. [DOI] [PubMed] [Google Scholar]
- 13.Fletcher J. What is heterogeneity and is it important? BMJ 2007;334:94‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Blumberg BS. The curiosities of hepatitis B virus: prevention, sex ratio, and demography. Proc Am Thorac Soc 2006;3:14‐20. [DOI] [PubMed] [Google Scholar]
- 15.Lim JK, Nguyen MH, Kim WR, Gish R, Perumalswami P, Jacobson IM. Prevalence of chronic hepatitis B virus infection in the United States. Am J Gastroenterol 2020;115:1429‐1438. [DOI] [PubMed] [Google Scholar]
- 16.Ott JJ, Horn J, Krause G, Mikolajczyk RT. Time trends of chronic HBV infection over prior decades—a global analysis. J Hepatol 2017;66:48‐54. [DOI] [PubMed] [Google Scholar]
- 17.Roberts H, Kruszon‐Moran D, Ly KN, Hughes E, Iqbal K, Jiles RB, et al. Prevalence of chronic hepatitis B virus (HBV) infection in U.S. households: National Health and Nutrition Examination Survey (NHANES), 1988‐2012. Hepatology 2016;63:388‐397. [DOI] [PubMed] [Google Scholar]
- 18.Gish RG, Cohen CA, Block JM, Brosgart CL, Block TM, Clary R, et al. Data supporting updating estimates of the prevalence of chronic hepatitis B and C in the United States. Hepatology 2015;62:1339‐1341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liu SJ, Iqbal K, Shallow S, Speers S, Rizzo E, Gerard K, et al. Characterization of chronic hepatitis B cases among foreign‐born persons in six population‐based surveillance sites, United States 2001‐2010. J Immigr Minor Health 2015;17:7‐12. [DOI] [PubMed] [Google Scholar]
- 20.Razavi‐Shearer D, Gamkrelidze I, Nguyen MH, Chen DS, Van Damme P, Abbas Z, et al. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol 2018;3:383‐403. [DOI] [PubMed] [Google Scholar]
- 21.Kim HS, Rotundo L, Yang JD, Kim D, Kothari N, Feurdean M, et al. Racial/ethnic disparities in the prevalence and awareness of hepatitis B virus infection and immunity in the United States. J Viral Hepat 2017;24:1052‐1066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ogawa E, Yeo YH, Dang N, Le MH, Jeong D, Tran S, et al. Diagnosis rates of chronic hepatitis B in privately insured patients in the United States. JAMA Netw Open 2020;3.e201844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Krist AH, Davidson KW, Mangione CM, Barry MJ, Cabana M, Caughey AB, et al. Screening for hepatitis B virus infection in adolescents and adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020;324:2415‐2422. [DOI] [PubMed] [Google Scholar]
- 24.Hung MC, Williams WW, Lu PJ, Kim DK, Grohskopf LA, Pilishvili T, et al. Vaccination Coverage Among Adults in the United States, National Health Interview Survey. U.S. Centers for Disease Control and Prevention; 2016. https://www.cdc.gov/vaccines/imz‐managers/coverage/adultvaxview/pubs‐resources/NHIS‐2016.html. Accessed November 1, 2020.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material