

Abstract
Background
Considering the widespread risk of collider bias and confounding by indication in previous research, the associations between renin‐angiotensin aldosterone system (RAAS) inhibitor use and COVID‐19 remain unknown. Accordingly, this study tested the hypothesis that RAAS inhibitors influence the summation effect of COVID‐19 and its progression to severe outcomes.
Methods and Results
This nationwide cohort study compared all residents of Sweden, without prior cardiovascular disease, in monotherapy (as of January 1, 2020) with a RAAS inhibitor to those using a calcium channel blocker or a thiazide diuretic. Comparative cohorts were balanced using machine‐learning‐derived propensity score methods. Of 165 355 people in the analysis (51% women), 367 were hospitalized or died with COVID‐19 (246 using a RAAS inhibitor versus 121 using a calcium channel blocker or thiazide diuretic; Cox proportional hazard ratio [HR], 0.97; 95% CI, 0.74–1.27). When each outcome was assessed separately, 335 people were hospitalized with COVID‐19 (HR, 0.92; 95% CI, 0.70–1.22), and 64 died with COVID‐19 (HR, 1.22; 95% CI, 0.68–2.19). The severity of COVID‐19 outcomes did not differ between those using a RAAS inhibitor and those using a calcium channel blocker or thiazide diuretic (ordered logistic regression odds ratio, 1.01; 95% CI, 0.89–1.14).
Conclusions
Despite potential limitations, this study is among the best available evidence that RAAS inhibitor use in primary prevention does not increase the risk of severe COVID‐19 outcomes; presenting strong data from which scientists and policy makers alike can base, with greater confidence, their current position on the safety of using RAAS inhibitors during the COVID‐19 pandemic.
Keywords: angiotensin II receptor blocker, angiotensin‐converting enzyme inhibitor, COVID‐19, hypertension, SARS‐CoV‐2
Subject Categories: Epidemiology, Pharmacology, ACE/Angiotension Receptors/Renin Angiotensin System, Hypertension, Mortality/Survival
Nonstandard Abbreviations and Acronyms
- ATC
Anatomical Therapeutic Chemical
- RAAS
renin‐angiotensin aldosterone system
- TZD
thiazide diuretic
Clinical Perspective
What Is New?
In contrast to previous studies that have evaluated the associations between renin‐angiotensin aldosterone system inhibitor use and COVID‐19 outcomes, this study limits the influence of collider, indication, and confounding biases to provide the best available evidence that the use of renin‐angiotensin aldosterone system inhibitors in primary prevention is not associated with COVID‐19 outcomes.
What Are the Clinical Implications?
Previously, scientists and policy makers alike were basing their current position regarding the safety of using renin‐angiotensin aldosterone system inhibitors during the COVID‐19 pandemic on data where the associations between renin‐angiotensin aldosterone system inhibitor use and COVID‐19 outcomes could be highly distorted by several types of bias.
This study provides data where those biases have been limited, fortunately supporting advice from the authorities that antihypertensive therapies should not be altered due to of the COVID‐19 pandemic.
SARS‐CoV‐2 gains entry into its target cells via angiotensin‐converting enzyme (ACE) 2.1 Renin‐angiotensin aldosterone system (RAAS) inhibitors, such as ACE inhibitors and angiotensin II type‐I receptor blockers (ARBs), may upregulate the expression of ACE2,2, 3, 4 establishing a basis for the hypothesis that their use may increase the risk of a SARS‐CoV‐2 infection.2
As of February 2021, at least 118 studies have attempted to test variants of this hypothesis.5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123 However, nearly all of them have assessed the associations between RAAS inhibitor use and COVID‐19 outcomes exclusively in people with a confirmed SARS‐CoV‐2 infection, mainly in those hospitalized with COVID‐19, introducing a high risk of collider bias.124 Collider bias creates a spurious within‐sample association between 2 variables (eg, in the context of this study: frailty caused by cardiovascular disease, with a high likelihood of being prescribed a RAAS inhibitor, and frailty caused by an adverse COVID‐19 course) that affects the probability of being included in the sample (eg, being hospitalized).124 To understand if RAAS inhibitors can increase the risk of COVID‐19, a primary prevention sample of yet uninfected people using RAAS inhibitors or a relevant comparator drug class must be studied, not those already impacted by the virus.124 Considering this, the findings of those biased studies need to be treated with caution,124 with the total effect of RAAS inhibitors on the risk of COVID‐19 remaining unknown.
Given that RAAS inhibitors are widely used in age groups where the incidence and case fatality of COVID‐19 are disproportionally high,125 there is an urgent need to provide definitive data about the safety of using these drugs during the ongoing COVID‐19 pandemic. Accordingly, the present study tested the hypothesis that RAAS inhibitors influence the summation effect of a SARS‐CoV‐2 infection and its progression to severe COVID‐19 outcomes.
Methods
Use of the analytical methods and data that support the findings of this study can be arranged with the corresponding author upon reasonable request.
Sample
The study was set in Sweden, where all residents have universal access to health care with a negligible copayment for healthcare visits, hospitalizations, and medications.126 Following approval by the Swedish Ethical Review Authority (approval no. 2020‐01556), the 12‐digit personal identity number,127 unique to all Swedish residents, was used to link a variety of nationwide socioeconomic and health registries (classifying diagnoses using the International Classification of Diseases , Tenth Revision [ICD‐10] system,128 surgical procedures using the Nordic Medico‐Statistical Committee Classification of Surgical Procedures system,129 and filled drug prescriptions using the Anatomical Therapeutic Chemical [ATC] classification system130), whose only loss to follow‐up was by emigration. The need for informed consent was waived.
A nationwide cohort study of all residents of Sweden in monotherapy with an antihypertensive drug as of January 1, 2020 was formed. To minimize confounding by indication, people using an ACE inhibitor (ATC code C09A), an ARB (ATC code C09C), a vascular selective calcium channel blocker (CCB; ATC code C08CA), or a thiazide diuretic (TZD; ATC codes C03AA or C03BA04) in monotherapy were included, because these are first‐line choices in current European hypertension guidelines.131 Among these, the group using a RAAS inhibitor (ie, an ACE inhibitor or an ARB) was compared with the group not using a RAAS inhibitor (ie, a CCB or TZD) in the primary analysis. Additionally, acknowledging that different classes of RAAS inhibitors do not share the same mechanistic actions, those using an ACE inhibitor and those using an ARB were also compared separately, in a secondary analysis, with the group using a CCB or TZD.
To further minimize confounding by disease severity, people using other blood pressure–lowering drugs (ATC codes C02CA04, C03DA, C07), combination pills including blood pressure–lowering drugs, or other cardiovascular drugs (ATC codes C01, C02D, C02K, C03C, C03X, C08D) were excluded. Additionally, people with preexisting cardiovascular and kidney diseases (ICD‐10 codes I20, I21, I22, I24, I25.2, Z95.1, Z95.5, I60, I61, I62, I63.0‐I63.5, I63.8‐I63.9, I64, I65, I66, I69.0‐I69.4, G45.0‐3, G45.8‐9, G46.0‐7, I50, I11.0, I13.0, I13.2, I25.5, I42.0, I42.6, I42.9, I43.1, Z99.4, I70.2, I73.0, I73.1, I73.9, I73.9, I74, or Z49; or procedure codes AAL10, AAL15, DF005, DF009, DF019, DF020, DR016, DR024, F, KAS, PA, PB, PC, PD, PE, PF, PG, or QF006) were excluded.
Follow‐Up and Outcomes
Participants were followed in the registries from January 1, 2020 until June 23, 2020 covering the first wave of the COVID‐19 pandemic in Sweden, in which around 100 to 800 new cases were recorded each day for the majority of the follow‐up period, before infection rates peaked at around 1000 to 1500 cases per day in June 2020.132 The primary outcome was defined as hospitalization and/or death with COVID‐19 (ICD‐10 code U07.1 [COVID‐19, virus identified] as either the main or underlying cause). A person who was hospitalized with COVID‐19 and then died with COVID‐19 was included in both the hospitalization and the death event counts. Mortality attributable to causes unrelated to COVID‐19 was used as a negative control. An ordered outcome, reflecting the severity of the SARS‐CoV‐2 disease course, was defined at the end of follow‐up as: (1) no event during follow‐up, (2) hospitalization with COVID‐19 without the need for intensive care, (3) hospitalization with COVID‐19 requiring intensive care (U07.1 as the main cause as well as procedure codes DG021, DG022, and DG023), (4) death with COVID‐19, and (5) death attributable to causes unrelated to COVID‐19. Participants were assigned to the most severe category of disease course experienced.
Statistical Analysis
Associations between exposures and the outcomes were analyzed using an intention‐to‐treat approach (ie, exposure groups were defined once, January 1, 2020) and an as‐treated approach. Patients were considered to have stopped or changed their RAAS inhibitor therapy if they did not refill their prescription within 120 days of their previous refill. Subsequently, in the as‐treated model, those patients were censored from the analyses.
Bias‐minimized models investigating total effects were identified using the directed acyclic graphs approach (Figure S1), considering subject matter knowledge and all factors listed in the Summary of Product Characteristics for the most commonly used of the studied drugs (Table S1). Potential confounding was handled by weighting patients on a propensity score and by multivariable adjustment.
The propensity score was estimated using gradient‐boosted classification and regression trees to determine the probability of being prescribed a RAAS inhibitor or not. More information about the use of gradient‐boosted classification and regression trees can be found in Data S1. The resulting propensity score was used to calculate an inverse probability of treatment weight for each individual:
where Z i is a binary indicator taking the value 1 if individual i was treated with a RAAS inhibitor and 0 otherwise, and where p i is the propensity score for individual i.
The associations between the use of RAAS inhibitors and the COVID‐19 outcomes during the 6‐month follow‐up period were assessed in the primary analysis using Cox models weighted with this inverse probability weight, further adjusting for age, sex, income, country of birth, use of drugs affecting the immune system, diabetes mellitus, antidiabetic drug use, renal disease, hepatic disease, neoplasms, and previous RAAS inhibitor use. Proportionality of the hazards was assessed by visually examining the smoothed association of the scaled Schoenfeld residuals with time. The Aalen‐Johansen estimate of the cumulative incidence function was also presented. This was repeated in the secondary analysis to evaluate the relationships between COVID‐19 outcomes and the use of an ACE inhibitor or an ARB, separately.
Associations between RAAS inhibitor use and an ordinal variable indicating the severity of the outcome at the end of the 6‐month follow‐up period were analyzed using ordered logistic regression, using the same weights and adjustments as above.
The balance of the cohorts was assessed using the standardized mean difference between the groups, and with a falsification outcome of mortality by causes unrelated to COVID‐19, which is not supposed to differ between the groups.133 All analyses were made using R version 4.0.0 and the twang and survival add‐on packages (R Foundation for Statistical Computing, Vienna, Austria).134, 135, 136
Results
Of the 1 997 479 residents of Sweden with an active blood pressure–lowering drug prescription as of January 1, 2020, there were 165 355 people who met the inclusion criteria of this study and were eligible for inclusion in the primary analysis. After removal of missing values in the adjusted variables and nonoverlapping weights, the final sample sizes included in the regressions for the primary and secondary analyses were 164 611 and 164 655, respectively (Figure 1). Of those people included in the primary analysis, 115 684 were on monotherapy with a RAAS inhibitor, and 48 927 were on monotherapy with a CCB or a TZD. In the secondary analysis, 47 998 people were on monotherapy with an ACE inhibitor, 68 239 with an ARB, and 48 418 with a CCB or TZD. The characteristics of the cohort in the primary analysis is detailed in Table 1. Characteristics of the cohort in the secondary analysis are detailed in Tables S2 and S3. Excellent balance between the weighted study groups was achieved; the standardized mean difference for all variables was near 0, and the hazard ratio for the association of RAAS inhibitor use with the falsification outcome, death by causes unrelated to COVID‐19, was 1.03 (95% CI, 0.84–1.27).
Figure 1. Flowchart detailing the identification of the study population.
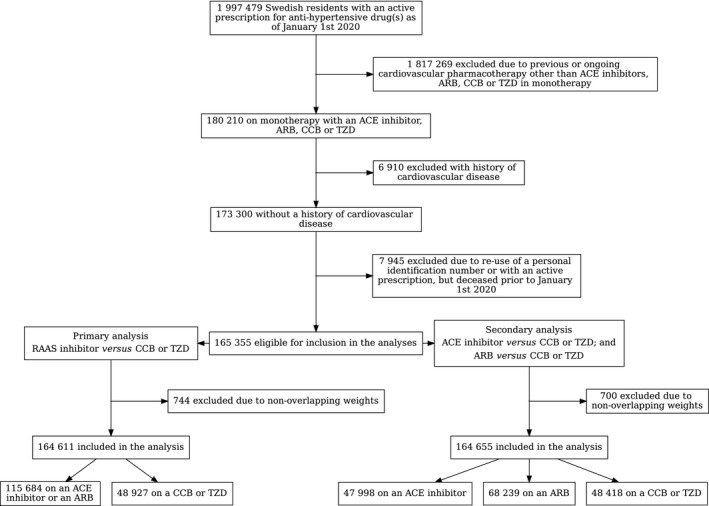
ACE indicates angiotensin‐converting enzyme; ARB, angiotensin II type‐I receptor blocker; CCB, calcium channel blocker; RAAS, renin‐angiotensin aldosterone system; and TZD, thiazide diuretic.
Table 1.
Baseline Characteristics of the Study Groups
| Unweighted | Weighted | |||||
|---|---|---|---|---|---|---|
| RAAS Inhibitor, | CCB or TZD, | SMD | RAAS Inhibitor, | CCB or TZD, | SMD | |
| N=115 684 | N=48 927 | N=164 358.5 | N=161 041.5 | |||
| Women, n (%) | 56 214 (48.6) | 26 316 (53.8) | 0.104 | 82 295.6 (50.1) | 81 500.2 (50.6) | 0.011 |
| Age, y, median [IQR] | 62.0 [54.0–71.0] | 66.0 [56.0–74.0] | 0.229 | 63.0 [54.0–72.0] | 64.0 [55.0–72.0] | 0.029 |
| Yearly income in SEK, median [IQR] | 3 268 600 [207 700–443 800] | 279 800 [176 200–406 200] | 0.186 | 314 400 [197 100–433 700] | 310 700 [195 300–429 200] | 0.032 |
| Education, n (%) | 0.113 | 0.020 | ||||
| Elementary school | 21 148 (18.4) | 11 065 (22.8) | 32 107.3 (19.7) | 32 275.0 (20.2) | ||
| High school | 55 684 (48.5) | 22 810 (47.0) | 78 469.5 (48.1) | 77 338.7 (48.4) | ||
| Academic | 33 802 (32.0) | 14 185 (29.2) | 50 880.7 (31.2) | 48 782.0 (30.5) | ||
| Postgraduate | 1278 (1.1) | 452 (0.9) | 1720.9 (1.1) | 1514.8 (0.9) | ||
| Marital status, n (%) | 0.123 | 0.008 | ||||
| Unmarried | 25 511 (22.1) | 9868 (20.2) | 25 702.8 (15.7) | 25 610.3 (15.9) | ||
| Married | 64 394 (55.7) | 25 824 (52.8) | 90 064.5 (54.9) | 88 063.1 (54.7) | ||
| Divorced | 17 663 (15.3) | 8064 (16.5) | 35 352.7 (21.5) | 34 359.7 (21.4) | ||
| Widow | 8006 (6.9) | 5110 (10.5) | 13 074.6 (8.0) | 12 823.4 (8.0) | ||
| Region of birth, n (%) | 0.060 | 0.006 | ||||
| Africa | 964 (0.8) | 628 (1.3) | 1559.3 (0.9) | 1569.0 (1.0) | ||
| Asia | 4085 (3.5) | 2061 (4.2) | 6092.1 (3.7) | 6038.4 (3.7) | ||
| Nordic countries | 3935 (3.4) | 1850 (3.8) | 5757.5 (3.5) | 5660.3 (3.5) | ||
| North America | 275 (0.2) | 121 (0.2) | 405.1 (0.2) | 407.1 (0.3) | ||
| Rest of Europe | 5354 (4.6) | 2460 (5.0) | 7718.0 (4.7) | 7539.6 (4.7) | ||
| South America | 589 (0.5) | 223 (0.5) | 827.9 (0.5) | 866.2 (0.5) | ||
| Sweden | 100 467 (86.8) | 41 579 (85.0) | 141 978.9 (86.4) | 138 943.7 (86.3) | ||
| Medical history, n (%) | ||||||
| Angioedema | 203 (0.2) | 200 (0.4) | 0.043 | 394 (0.2) | 394.6 (0.2) | 0.001 |
| Diabetes mellitus | 1313 (1.1) | 453 (0.9) | 0.021 | 1769.4 (1.1) | 1859.3 (1.2) | 0.007 |
| Renal disease | 1092 (0.9) | 5571 (1.2) | 0.022 | 1625.2 (1.0) | 1452.4 (0.9) | 0.009 |
| Hepatic disease | 1143 (1.0) | 559 (1.1) | 0.015 | 1672.6 (1.0) | 1668.6 (1.0) | 0.002 |
| Psychiatric disease | 6595 (5.7) | 3401 (7.0) | 0.051 | 9929.7 (6.0) | 9847.7 (6.1) | 0.003 |
| Neuropsychiatric disease | 1954 (1.7) | 912 (1.9) | 0.013 | 2838.1 (1.7) | 2811.1 (1.7) | 0.001 |
| Neoplasms | 6800 (5.9) | 3084 (6.3) | 0.018 | 9896.6 (6.0) | 9766.0 (6.1) | 0.002 |
| Autoimmune disease | 741 (0.6) | 310 (0.6) | 0.001 | 1061.1 (0.6) | 1103.8 (0.7) | 0.005 |
| Obesity | 3037 (2.6) | 1077 (2.2) | 0.028 | 4091.9 (2.5) | 4173.6 (2.6) | 0.006 |
| Heart valve disease | 1092 (0.9) | 423 (0.9) | 0.008 | 1510.6 (0.9) | 1276.2 (0.8) | 0.014 |
| Hypertrophic cardiomyopathy | 23 (0.0) | 8 (0.0) | 0.003 | 30.3 (0.0) | 26.0 (0.0) | 0.002 |
| Pharmacotherapy, n (%) | ||||||
| Antidiabetic drugs | 1791 (1.5) | 539 (1.1) | 0.039 | 2333.4 (1.4) | 2358.4 (1.5) | 0.004 |
| NSAID | 77 917 (67.4) | 32 727 (66.9) | 0.010 | 110 422.5 (67.2) | 108 776.5 (67.5) | 0.008 |
| Immune system–affecting drugs | 1817 (1.6) | 847 (1.7) | 0.009 | 2682.6 (1.5) | 2657.5 (1.7) | 0.001 |
| Previous ACE inhibitor/ARB | 84 157 (72.7) | 13 963 (28.5) | 0.986 | 98 204.5 (59.8) | 94 748.3 (58.9) | 0.018 |
Unweighted and weighted characteristics of the study groups included in the primary analysis, composed of all Swedish residents using an antihypertensive drug in monotherapy as of January 1, 2020. ACE indicates angiotensin‐converting enzyme; ARB, angiotensin II type‐I receptor blocker; CCB, calcium channel blocker; IQR, interquartile range; NSAID, nonsteroidal anti‐inflammatory drug; RAAS, renin‐angiotensin aldosterone system; SEK, Swedish Kronor (currency of Sweden: 8.5 SEK=1.0 USD); SMD, standardized mean difference; and TZD, thiazide diuretic.
Focusing on the primary analysis, 228 people using a RAAS inhibitor had been hospitalized with COVID‐19, 30 had been admitted to an intensive care unit with COVID‐19, 324 had died from causes unrelated to COVID‐19, and 35 had died with COVID‐19 at the end of the 6‐month follow‐up period. Of those on monotherapy with a CCB or TZD, 107 people were hospitalized with COVID‐19, 15 were admitted to an intensive care unit with COVID‐19, 229 died from causes unrelated to COVID‐19, and 29 died with COVID‐19.
There were no statistical differences in the rates of all COVID‐19 outcomes between those using a RAAS inhibitor and those using a CCB or TZD (Table 2 and Figure 2). Additionally, there was no difference in the severity of the COVID‐19 outcomes between these groups (odds ratio, 1.01; 95% CI, 0.89–1.14, from an ordered logistic regression). There were also no statistical differences in the rates of all COVID‐19 outcomes when those using an ACE inhibitor and those using an ARB were compared separately to those using a CCB or TZD (Table 3). These findings did not change when using either an intention‐to‐treat or as‐tread approach. Hazard ratios did not vary with adjustment (Table S4). Although the proportionality test indicated potentially nonproportional hazards, the plot of the smoothed association of the scaled Schoenfeld residuals with time revealed little (Figure S2).
Table 2.
Associations of RAAS Inhibitor Use With COVID‐19 Outcomes
| Outcome | Rate of Outcome With RAAS Inhibitor Use vs Use of a CCB or TZD | |||||
|---|---|---|---|---|---|---|
| Intention‐to‐Treat | As‐Treated | |||||
| RAAS Inhibitor, n=115 684, No. of Events | CCB or TZD, n=48 927, No. of Events | HR (95% CI) |
RAAS Inhibitor, n=115 684, No. of Events |
CCB or TZD, n=48 927, No. of Events |
HR (95% CI) | |
| Hospitalization with COVID‐19 | 228 | 107 | 0.92 (0.70–1.22) | 210 | 100 | 0.93 (0.67–1.29) |
| Death with COVID‐19 | 35 | 29 | 1.22 (0.68–2.19) | 34 | 28 | 1.44 (0.64–3.27) |
| Hospitalization or death with COVID‐19 combined | 246 | 121 | 0.97 (0.74–1.27) | 228 | 114 | 0.98 (0.72–1.34) |
Swedish residents on antihypertensive monotherapy with a RAAS inhibitor were compared with those on monotherapy with either a CCB or a TZD, in both intention‐to‐treat and as‐treated models. CCB indicates calcium channel blocker; HR, inverse probability of treatment‐weighted and multivariate‐adjusted Cox proportional hazard ratio; RAAS, renin‐angiotensin aldosterone system; and TZD, thiazide diuretic.
Figure 2. The Aalen‐Johansen estimate of the cumulative incidence function for death unrelated to COVID‐19 and for a combination of hospitalization or death with COVID‐19, in people on monotherapy with a renin‐angiotensin aldosterone system (RAAS) inhibitor and those on monotherapy with either a calcium channel blocker (CCB) or a thiazide diuretic (TZD).
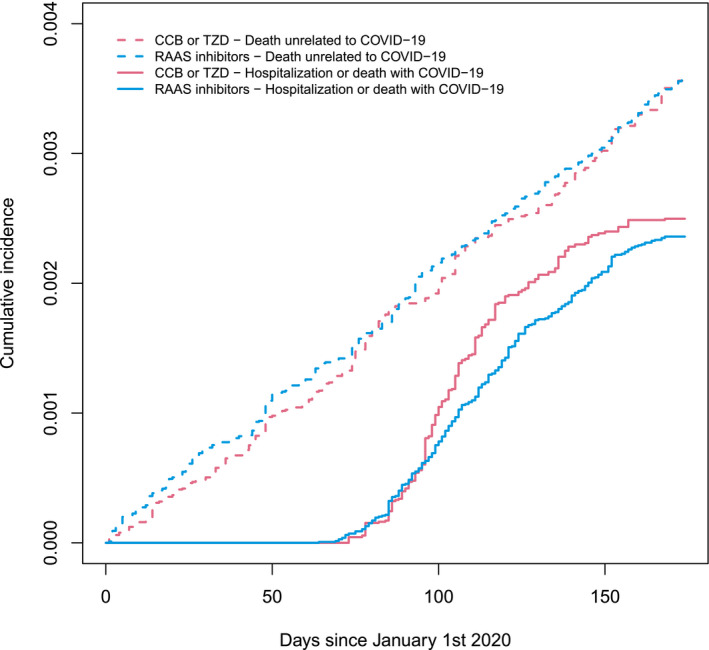
Table 3.
Associations of ACE Inhibitor or ARB Use With COVID‐19 Outcomes
| Outcome | Rate of Outcome With ACE Inhibitor or ARB Use vs Use of a CCB or TZD | |||||
|---|---|---|---|---|---|---|
| Intention‐to‐Treat | As‐Treated | |||||
|
ACE Inhibitor, n=47 998, No. of Events |
CCB or TZD, n=48 418, No. of Events |
HR (95% CI) |
ACE Inhibitor, n=47 998, No. of Events |
CCB or TZD, n=48 418, No. of Events |
HR (95% CI) | |
| Hospitalization with COVID‐19 | 94 | 107 | 0.89 (0.64–1.23) | 85 | 100 | 0.85 (0.60–1.19) |
| Death with COVID‐19 | 16 | 26 | 0.97 (0.48–1.93) | 15 | 25 | 0.94 (0.46–1.92) |
| Hospitalization or death with COVID‐19 combined | 104 | 118 | 0.95 (0.69–1.29) | 95 | 111 | 0.91 (0.65–1.26) |
|
ARB, n=68 239, No. of Events |
CCB or TZD, n=48 418, No. of Events |
HR (95% CI) |
ARB, n=68 239, No. of Events |
CCB or TZD, n=48 418, No. of Events |
HR (95% CI) | |
|---|---|---|---|---|---|---|
| Hospitalization with COVID‐19 | 135 | 107 | 0.94 (0.70–1.27) | 126 | 100 | 0.93 (0.67–1.27) |
| Death with COVID‐19 | 19 | 26 | 1.25 (0.63–2.49) | 19 | 25 | 1.68 (0.69–2.77) |
| Hospitalization or death with COVID‐19 combined | 143 | 118 | 0.99 (0.73–1.32) | 134 | 111 | 0.98 (0.72–1.33) |
Swedish residents on antihypertensive monotherapy with an ACE inhibitor or an ARB were compared with those on monotherapy with either a CCB or TZD, in both intention‐to‐treat and as‐treated models. ACE indicates angiotensin‐converting enzyme; ARB, angiotensin II type‐I receptor blocker; CCB, calcium channel blocker; HR, inverse probability of treatment weighted and multivariate adjusted Cox proportional hazard ratio; and TZD, thiazide diuretic.
Discussion
In this nationwide cohort study of initially uninfected people, there is no evidence to support that RAAS inhibitor use increases the risk of severe COVID‐19 outcomes including hospitalization, admission to an intensive care unit, or death.
Of the 118 previous studies of RAAS inhibition and COVID‐19 associations,5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123 at least 102 were restricted to patients who were tested for/tested positive for a SARS‐CoV‐2 infection or who had been hospitalized because of COVID‐19. Such inclusion strategies produce samples that are not representative of the general population and carry a high risk of collider bias, thus distorting any true associations between the use of RAAS inhibitors and the incidence of COVID‐19 outcomes.124 Unfortunately, even the more influential studies published to date suffer from this bias.84, 95 The most comprehensive overview of this methodological problem stresses an urgent need for COVID‐19 studies that use representative population samples and thus avoid collider bias to provide reliable evidence.124 Results from biased studies should be treated with caution by scientists and policy makers alike.124
Four case‐control studies and 10 cohort studies provided stronger study designs than most of the other RAAS inhibitor–COVID‐19 research, but each study included people with prior cardiovascular and/or renal disease, which renders them highly susceptible to confounding by indication, the main pitfall in comparative effectiveness and drug‐safety studies. Considering the methodological limitations in previous studies, as well as the burden that a potential inaccurate conclusion could have on patients and healthcare systems worldwide, it was warranted that the potential associations between RAAS inhibitor use and the summation effect of SARS‐CoV‐2 infection and the progression to severe COVID‐19 outcomes be studied further and settled.
Accordingly, Semenzato et al recognized the methodological limitations in the previous research, providing the strongest study design to date by limiting the potential for collider, indication, and confounding biases.102 In a nationwide cohort that identified patients in France being treated for uncomplicated hypertension, they found that long‐term use of an ACE inhibitor or ARB may lower COVID‐19 risk when compared with those using a CCB.102 This present study addresses a major limitation of that research, extending upon it by including an as‐treated analysis. Given the similarities in study design and the event rates, it is not entirely clear why the associations between RAAS inhibitor use and COVID‐19 outcomes differ from the study by Semenzato et al102 to this present research. Potentially, the difference in the effect may be simply explained by how France and Sweden have managed the COVID‐19 pandemic, with approaches that varied greatly between the 2 countries (eg, nationwide lockdowns versus no lockdowns, respectively). Nevertheless, each study provides strong data that do not indicate a harmful interaction between RAAS inhibitor use and COVID‐19.
The initial doubt cast over the safety of using RAAS inhibitors was driven by the finding that SARS‐CoV‐2 gains entry to human cells by binding its viral spike protein to ACE2.1, 2 In brief, it was hypothesized that RAAS inhibitors could increase one's susceptibility to a SARS‐CoV‐2 infection, as well as potentiate a more severe disease course, by increasing the expression of ACE2 on the surface of the cell.2 Potential protective effects of RAAS inhibition have also been proposed. RAAS inhibition may potentiate the lung protective function of ACE2.137 Given that either of these potential effects, protective or harmful, would affect the probability of infection and the probability of symptomatic disease, the most relevant population for studying the totality of the safety of RAAS inhibition should be noninfected people. Randomized clinical trials of RAAS inhibition in people with established COVID‐19 are ongoing, but these cannot shed light on the total effect on COVID‐19.
Several limitations must be considered when interpreting these data. The external validity of these findings to people on combination therapy with antihypertensive drugs, as well as to other geographic or ethnic contexts, is unknown. Given that people with preexisting cardiovascular and kidney diseases were excluded, whether these findings extend to those with underlying comorbidities is also unknown. However, exclusion of these patients was necessary to avoid collider bias and to isolate any interaction between RAAS inhibitors and COVID‐19. Given that the definition for COVID‐19 cases in this present study was based on admission to hospital or death (ie, a severity criterion), nonsevere cases of COVID‐19 were not included in this study, meaning that the association between RAAS inhibition in primary prevention and a combination of the risk for infection and progression to severe disease was studied. However, severe COVID‐19 cases are a good representation of (proportional to) all cases but are detected with much better precision because they are not subject to differences and biases in testing. Indeed, virus polymerase chain reaction testing strategies were constant in inpatient care, but changed substantially in outpatient care during follow‐up, with unknown potential for bias. Furthermore, severe COVID‐19 cases are more relevant considering that they are the burden to health care and that they reflect COVID‐19 mortality risk in affected patients. Finally, it must be acknowledged that there was a low number of COVID‐19–related events (particularly for deaths with COVID‐19) in this study's sample, which limits the power to detect weak associations in each outcome of interest.
The study has several advantages, including the availability of 2 million people using antihypertensive drugs, which allowed us to select the sample least prone to several biases. Additionally, we have complete coverage of all individuals in a society with universal access to health care with a negligible copayment, we have data on both in‐hospital and out‐of‐hospital mortality and could study the need for intensive care, and we used state‐of‐the‐art methods for causal assumptions and development of bias‐minimized models.
The importance of the findings from this study are only emphasized by the way in which much of the world is currently struggling under the burden of subsequent waves of the COVID‐19 pandemic, with infection and mortality rates far surpassing those seen during the initial wave during the first half of 2020.132 Furthermore, there is now an urgent need for research that can properly inform and support healthcare systems by providing reliable information on associations of readily modifiable factors with COVID‐19 outcomes.
In conclusion, despite potential limitations in the data, this study is among the best available evidence that the use of RAAS inhibitors in primary prevention does not increase the risk of severe COVID‐19 outcomes; stronger data from which scientists and policy makers alike can base, with greater confidence, their current position on the safety of using RAAS inhibitors during the COVID‐19 pandemic. A corresponding randomized clinical trial is unlikely to ever be executed.
Sources of Funding
This research was supported by funding from the Swedish Heart‐Lung Foundation and Anders Wiklöf.
Disclosures
None.
Supporting information
Supplementary Material for this article is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.120.021154
For Sources of Funding and Disclosures, see page 8.
References
- 1.Hoffmann M, Kleine‐Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu N‐H, Nitsche A, et al. SARS‐CoV‐2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–280.e8. DOI: 10.1016/j.cell.2020.02.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nishiga M, Wang DW, Han Y, Lewis DB, Wu JC. COVID‐19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nat Rev Cardiol. 2020;17:543–558. DOI: 10.1038/s41569-020-0413-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ferrario CM, Jessup J, Chappell MC, Averill DB, Brosnihan KB, Tallant EA, Diz DI, Gallagher PE. Effect of angiotensin‐converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin‐converting enzyme 2. Circulation. 2005;111:2605–2610. DOI: 10.1161/CIRCULATIONAHA.104.510461. [DOI] [PubMed] [Google Scholar]
- 4.Ishiyama Y, Gallagher PE, Averill DB, Tallant EA, Brosnihan KB, Ferrario CM. Upregulation of angiotensin‐converting enzyme 2 after myocardial infarction by blockade of angiotensin II receptors. Hypertension. 2004;43:970–976. DOI: 10.1161/01.HYP.0000124667.34652.1a. [DOI] [PubMed] [Google Scholar]
- 5.Adrish M, Chilimuri S, Sun H, Mantri N, Yugay A, Zahid M. The association of renin‐angiotensin‐aldosterone system inhibitors with outcomes among a predominantly ethnic minority patient population hospitalized with COVID‐19: the Bronx experience. Cureus. 2020;12:e10217. DOI: 10.7759/cureus.10217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aghaaliakbari F, Abbasi MA, Ranjbar M, Jamshidi Makiani M, Farrokhpour M, Safarnezhad Tameshkel F, Karbalaie Niya MH, Doltkhah S, Yaghoobzadeh K, Savaj S. Angiotensin converting enzyme inhibitors, a risk factor of poor outcome in diabetic patients with COVID‐19 infection. Iran J Kidney Dis. 2020;14:482–487. [PubMed] [Google Scholar]
- 7.Ahlström B, Frithiof R, Hultström M, Larsson I‐M, Strandberg G, Lipcsey M. The Swedish Covid‐19 intensive care cohort: risk factors of ICU admission and ICU mortality. Acta Anaesthesiol Scand. 2021;65:525–533. DOI: 10.1111/aas.13781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Akchurin O, Meza K, Biswas S, Greenbaum M, Licona‐Freudenstein AP, Goyal P, Choi JJ, Choi ME. COVID‐19 in patients with CKD in New York City. Kidney360. 2021;2:63–70. DOI: 10.34067/KID.0004142020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.An J, Wei R, Zhou H, Luong TQ, Gould MK, Mefford MT, Harrison TN, Creekmur B, Lee M‐S, Sim JJ, et al. Angiotensin‐converting enzyme inhibitors or angiotensin receptor blockers use and COVID‐19 infection among 824 650 patients with hypertension from a US integrated healthcare system. J Am Heart Assoc. 2021;10:e019669. DOI: 10.1161/JAHA.120.019669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Anzola GP, Bartolaminelli C, Gregorini GA, Coazzoli C, Gatti F, Mora A, Charalampakis D, Palmigiano A, De Simone M, Comini A, et al. No harm from angiotensin‐converting enzyme inhibitors or angiotensin receptor inhibitors in patients with COVID‐19. Results of a prospective study on a hospital‐based cohort. Ital J Med. 2020;14:162–166. DOI: 10.4081/itjm.2020.1313. [DOI] [Google Scholar]
- 11.Bae DJ, Tehrani DM, Rabadia SV, Frost M, Parikh RV, Calfon‐Press M, Aksoy O, Umar S, Ardehali R, Rabbani A, et al. Angiotensin converting enzyme inhibitor and angiotensin II receptor blocker use among outpatients diagnosed with COVID‐19. Am J Cardiol. 2020;132:150–157. DOI: 10.1016/j.amjcard.2020.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bae S, Kim JH, Kim Y‐J, Lim JS, Yun S‐C, Kim Y‐H, Lee S‐O, Kim S‐H. Effects of recent use of renin‐angiotensin system inhibitors on mortality of patients with coronavirus disease 2019. Open Forum Infect Dis. 2020;7:ofaa519. DOI: 10.1093/ofid/ofaa519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bauer AZ, Gore R, Sama SR, Rosiello R, Garber L, Sundaresan D, McDonald A, Arruda P, Kriebel D. Hypertension, medications, and risk of severe COVID‐19: a Massachusetts community‐based observational study. J Clin Hypertens (Greenwich). 2021;23:21–27. DOI: 10.1111/jch.14101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bean DM, Kraljevic Z, Searle T, Bendayan R, Kevin O, Pickles A, Folarin A, Roguski L, Noor K, Shek A, et al. Angiotensin‐converting enzyme inhibitors and angiotensin II receptor blockers are not associated with severe COVID‐19 infection in a multi‐site UK acute hospital trust. Eur J Heart Fail. 2020;22:967–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Boari G, Chiarini G, Bonetti S, Malerba P, Bianco G, Faustini C, Braglia‐Orlandini F, Turini D, Guarinoni V, Saottini M, et al. Prognostic factors and predictors of outcome in patients with COVID‐19 and related pneumonia: a retrospective cohort study. Biosci Rep. 2020;40:BSR20203455. DOI: 10.1042/BSR20203455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Braude P, Carter B, Short R, Vilches‐Moraga A, Verduri A, Pearce L, Price A, Quinn TJ, Stechman M, Collins J, et al. The influence of ACE inhibitors and ARBs on hospital length of stay and survival in people with COVID‐19. Int J Cardiol Heart Vasc. 2020;31:100660. DOI: 10.1016/j.ijcha.2020.100660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bravi F, Flacco ME, Carradori T, Volta CA, Cosenza G, De Togni A, Acuti Martellucci C, Parruti G, Mantovani L, Manzoli L. Predictors of severe or lethal COVID‐19, including angiotensin converting enzyme inhibitors and angiotensin II receptor blockers, in a sample of infected Italian citizens. PLoS One. 2020;15:e0235248. DOI: 10.1371/journal.pone.0235248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cannata F, Chiarito M, Reimers B, Azzolini E, Ferrante G, My I, Viggiani G, Panico C, Regazzoli D, Ciccarelli M, et al. Continuation versus discontinuation of ACE inhibitors or angiotensin II receptor blockers in COVID‐19: effects on blood pressure control and mortality. Eur Heart J Cardiovasc Pharmacother. 2020;6:412–414. DOI: 10.1093/ehjcvp/pvaa056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cariou B, Hadjadj S, Wargny M, Pichelin M, Al‐Salameh A, Allix I, Amadou C, Arnault G, Baudoux F, Bauduceau B, et al. Phenotypic characteristics and prognosis of inpatients with COVID‐19 and diabetes: the CORONADO study. Diabetologia. 2020;63:1500–1515. DOI: 10.1007/s00125-020-05180-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chaudhri I, Koraishy FM, Bolotova O, Yoo J, Marcos LA, Taub E, Sahib H, Bloom M, Ahmad S, Skopicki H, et al. Outcomes associated with the use of renin‐angiotensin‐aldosterone system blockade in hospitalized patients with SARS‐CoV‐2 infection. Kidney360. 2020;1:801–809. DOI: 10.34067/KID.0003792020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chen C, Wang F, Chen P, Jiang J, Cui G, Zhou N, Moroni F, Moslehi JJ, Ammirati E, Wang DW. Mortality and pre‐hospitalization use of renin‐angiotensin system inhibitors in hypertensive COVID‐19 patients. J Am Heart Assoc. 2020;9:e017736. DOI: 10.1161/JAHA.120.017736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chen F‐F, Zhong M, Liu Y, Zhang Y, Zhang K, Su D‐Z, Meng X, Zhang Y. The characteristics and outcomes of 681 severe cases with COVID‐19 in China. J Crit Care. 2020;60:32–37. DOI: 10.1016/j.jcrc.2020.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chen R, Yang J, Gao X, Ding X, Yang Y, Shen Y, He C, Xiang H, Ke J, Yuan F, et al. Influence of blood pressure control and application of renin‐angiotensin‐aldosterone system inhibitors on the outcomes in COVID‐19 patients with hypertension. J Clin Hypertens (Greenwich). 2020;22:1974–1983. DOI: 10.1111/jch.14038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chen Y, Yang D, Cheng B, Chen J, Peng A, Yang C, Liu C, Xiong M, Deng A, Zhang YU, et al. Clinical characteristics and outcomes of patients with diabetes and COVID‐19 in association with glucose‐lowering medication. Diabetes Care. 2020;43:1399–1407. DOI: 10.2337/dc20-0660. [DOI] [PubMed] [Google Scholar]
- 25.Cheung KS, Hung IFN, Leung WK. Association between angiotensin blockade and COVID‐19 severity in Hong Kong. CMAJ. 2020;192:E635. DOI: 10.1503/cmaj.75865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chodick G, Nutman A, Yiekutiel N, Shalev V. Angiotensin‐converting enzyme inhibitors and angiotensin‐receptor blockers are not associated with increased risk of SARS‐CoV‐2 infection. J Travel Med. 2020;27:taaa069. DOI: 10.1093/jtm/taaa069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Choi MH, Ahn H, Ryu HS, Kim B‐J, Jang J, Jung M, Kim J, Jeong SH. Clinical characteristics and disease progression in early‐stage COVID‐19 patients in South Korea. J Clin Med. 2020;9:1959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Christiansen CF, Pottegård A, Heide‐Jørgensen U, Bodilsen J, Søgaard OS, Maeng M, Vistisen ST, Schmidt M, Lund LC, Reilev M, et al. SARS‐CoV‐2 infection and adverse outcomes in users of ACE inhibitors and angiotensin‐receptor blockers: a nationwide case‐control and cohort analysis. Thorax. 2020; 76:370–379. DOI: 10.1136/thoraxjnl-2020-215768. [DOI] [PubMed] [Google Scholar]
- 29.Chung SM, Lee YY, Ha E, Yoon JS, Won KC, Lee HW, Hur J, Hong KS, Jang JG, Jin HJ, et al. The risk of diabetes on clinical outcomes in patients with coronavirus disease 2019: a retrospective cohort study. Diabetes Metab J. 2020;44:405–413. DOI: 10.4093/dmj.2020.0105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cippà PE, Cugnata F, Ferrari P, Brombin C, Ruinelli L, Bianchi G, Beria N, Schulz L, Bernasconi E, Merlani P, et al. A data‐driven approach to identify risk profiles and protective drugs in COVID‐19. Proc Natl Acad Sci USA. 2021;118:e2016877118. DOI: 10.1073/pnas.2016877118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Conversano A, Melillo F, Napolano A, Fominskiy E, Spessot M, Ciceri F, Agricola E. Renin‐angiotensin‐aldosterone system inhibitors and outcome in patients with SARS‐CoV‐2 pneumonia: a case series study. Hypertension. 2020;76:e10–e12. DOI: 10.1161/HYPERTENSIONAHA.120.15312. [DOI] [PubMed] [Google Scholar]
- 32.Cordeanu E‐M, Jambert L, Severac F, Lambach H, Tousch J, Heitz M, Mirea C, Hamadé A, Younes W, Frantz A‐S, et al. Outcomes of COVID‐19 hospitalized patients previously treated with renin‐angiotensin system inhibitors. J Clin Med. 2020;9:3472. DOI: 10.3390/jcm9113472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.COVID‐19 RISk and Treatments (CORIST) Collaboration . RAAS inhibitors are not associated with mortality in COVID‐19 patients: findings from an observational multicenter study in Italy and a meta‐analysis of 19 studies. Vascul Pharmacol. 2020;135:106805. DOI: 10.1016/j.vph.2020.106805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Covino M, De Matteis G, Burzo ML, Santoro M, Fuorlo M, Sabia L, Sandroni C, Gasbarrini A, Franceschi F, Gambassi G; Gemelli Against COVID‐19 Group . Angiotensin‐converting enzyme inhibitors or angiotensin II receptor blockers and prognosis of hypertensive patients hospitalised with COVID‐19. Intern Med J. 2020;50:1483–1491. DOI: 10.1111/imj.15078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Dalan R, Ang LW, Tan WYT, Fong S‐W, Tay WC, Chan Y‐H, Renia L, Ng LFP, Lye DC, Chew DEK, et al. The association of hypertension and diabetes pharmacotherapy with COVID‐19 severity and immune signatures: an observational study. Eur Heart J Cardiovasc Pharmacother. 2021;7:e48–e51. DOI: 10.1093/ehjcvp/pvaa098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Daniels LB, Sitapati AM, Zhang J, Zou J, Bui QM, Ren J, Longhurst CA, Criqui MH, Messer K. Relation of statin use prior to admission to severity and recovery among COVID‐19 inpatients. Am J Cardiol. 2020;136:149–155. DOI: 10.1016/j.amjcard.2020.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.de Abajo FJ , Rodríguez‐Martín S, Lerma V, Mejía‐Abril G, Aguilar M, García‐Luque A, Laredo L, Laosa O, Centeno‐Soto GA, Ángeles Gálvez M, et al. Use of renin‐angiotensin‐aldosterone system inhibitors and risk of COVID‐19 requiring admission to hospital: a case‐population study. Lancet. 2020;395:1705–1714. DOI: 10.1016/S0140-6736(20)31030-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.De Spiegeleer A, Bronselaer A, Teo JT, Byttebier G, De Tré G, Belmans L, Dobson R, Wynendaele E, Van De Wiele C, Vandaele F, et al. The effects of ARBs, ACEis, and statins on clinical outcomes of COVID‐19 infection among nursing home residents. J Am Med Dir Assoc. 2020;21:909–914.e2. DOI: 10.1016/j.jamda.2020.06.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.De Vito A, Geremia N, Princic E, Fanelli C, Panu Napodano CM, Muredda AA, Fiore V, Maida I, Fois AG, Babudieri S, et al. Does angiotensin II receptor blockers increase the risk of SARS‐CoV‐2 infection? A real‐life experience. Eur Rev Med Pharmacol Sci. 2021;25:523–526. [DOI] [PubMed] [Google Scholar]
- 40.Desai A, Voza G, Paiardi S, Teofilo FI, Caltagirone G, Pons MR, Aloise M, Kogan M, Tommasini T, Savevski V, et al. The role of anti‐hypertensive treatment, comorbidities and early introduction of LMWH in the setting of COVID‐19: a retrospective, observational study in Northern Italy. Int J Cardiol. 2021;324:249–254. DOI: 10.1016/j.ijcard.2020.09.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Díaz‐Guardiola P, Martín‐Borge V, García‐Fernández C, Ramírez‐Prieto MT, Ramírez‐Belmar MI, García‐Romero G, de la Calle E , Balsa JA. Association of use of angiotensin‐converting enzyme inhibitors and angiotensin II receptor blockers with coronavirus disease 2019 severity and mortality. Am J Intern Med. 2020;8:204. DOI: 10.11648/j.ajim.20200805.12. [DOI] [Google Scholar]
- 42.Dublin S, Walker R, Floyd JS, Shortreed SM, Fuller S, Albertson‐Junkans L, Harrington LB, Greenwood‐Hickman MA, Green BB, Psaty BM. Renin‐angiotensin‐aldosterone system inhibitors and COVID‐19 infection or hospitalization: a cohort study. Am J Hypertens. 2021;34:339–347. DOI: 10.1093/ajh/hpaa168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Felice C, Nardin C, Di Tanna GL, Grossi U, Bernardi E, Scaldaferri L, Romagnoli M, Tonon L, Cavasin P, Novello S, et al. Use of RAAS inhibitors and risk of clinical deterioration in COVID‐19: results from an Italian cohort of 133 hypertensives. Am J Hypertens. 2020;33:944–948. DOI: 10.1093/ajh/hpaa096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Feng Z, Li J, Yao S, Yu Q, Zhou W, Mao X, Li H, Kang W, Ouyang X, Mei JI, et al. Clinical factors associated with progression and prolonged viral shedding in COVID‐19 patients: a multicenter study. Aging Dis. 2020;11:1069–1081. DOI: 10.14336/AD.2020.0630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ferrante G, Fazzari F, Cozzi O, Maurina M, Bragato R, D’Orazio F, Torrisi C, Lanza E, Indolfi E, Donghi V, et al. Risk factors for myocardial injury and death in patients with COVID‐19: insights from a cohort study with chest computed tomography. Cardiovasc Res. 2020;116:2239–2246. DOI: 10.1093/cvr/cvaa193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Fosbøl EL, Butt JH, Østergaard L, Andersson C, Selmer C, Kragholm K, Schou M, Phelps M, Gislason GH, Gerds TA, et al. Association of angiotensin‐converting enzyme inhibitor or angiotensin receptor blocker use with COVID‐19 diagnosis and mortality. JAMA. 2020;324:168–177. DOI: 10.1001/jama.2020.11301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Fröhlich GM, Jeschke E, Eichler U, Thiele H, Alhariri L, Reinthaler M, Kastrati A, Leistner DM, Skurk C, Landmesser U, et al. Impact of oral anticoagulation on clinical outcomes of COVID‐19: a nationwide cohort study of hospitalized patients in Germany. Clin Res Cardiol. 2021;9:1–10. DOI: 10.1007/s00392-020-01783-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gao C, Cai Y, Zhang K, Zhou L, Zhang Y, Zhang X, Li QI, Li W, Yang S, Zhao X, et al. Association of hypertension and antihypertensive treatment with COVID‐19 mortality: a retrospective observational study. Eur Heart J. 2020;41:2058–2066. DOI: 10.1093/eurheartj/ehaa433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Genet B, Vidal J‐S, Cohen A, Boully C, Beunardeau M, Marine Harlé L, Gonçalves A, Boudali Y, Hernandorena I, Bailly H, et al. COVID‐19 In‐hospital mortality and use of renin‐angiotensin system blockers in geriatrics patients. J Am Med Dir Assoc. 2020;21:1539–1545. DOI: 10.1016/j.jamda.2020.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Georges J‐L, Gilles F, Cochet H, Bertrand A, De Tournemire M, Monguillon V, Pasqualini M, Prevot A, Roger G, Saba J, et al. Positive association of angiotensin II receptor blockers, not angiotensin‐converting enzyme inhibitors, with an increased vulnerability to SARS‐CoV‐2 infection in patients hospitalized for suspected COVID‐19 pneumonia. PLoS One. 2020;15:e0244349. DOI: 10.1371/journal.pone.0244349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Giorgi Rossi P, Marino M, Formisano D, Venturelli F, Vicentini M, Grilli R; Reggio Emilia COVID‐19 Working Group . Characteristics and outcomes of a cohort of COVID‐19 patients in the Province of Reggio Emilia, Italy. PLoS One. 2020;15:e0238281. DOI: 10.1371/journal.pone.0238281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Gnavi R, Demaria M, Picariello R, Dalmasso M, Ricceri F, Costa G. Therapy with agents acting on the renin‐angiotensin system and risk of severe acute respiratory syndrome coronavirus 2 infection. Clin Infect Dis. 2020;71:2291–2293. DOI: 10.1093/cid/ciaa634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gobbato M, Calagnan E, Burba I, Rizzi L, Grassetti L, Del Zotto S, Dal Maso L, Serraiono D, Tonutti G. Clinical, demographical characteristics and hospitalisation of 3,010 patients with Covid‐19 in Friuli Venezia Giulia Region (Northern Italy). A multivariate, population‐based, statistical analysis. Epidemiol Prev. 2020;44:226–234. [DOI] [PubMed] [Google Scholar]
- 54.Golpe R, Pérez‐de‐Llano LA, Dacal D, Guerrero‐Sande H, Pombo‐Vide B, Ventura‐Valcárcel P. Lugo Covid‐19 team. Risk of severe COVID‐19 in hypertensive patients treated with renin‐angiotensin‐aldosterone system inhibitors. Med Clin (Engl Ed). 2020;155:488–490. DOI: 10.1016/j.medcli.2020.06.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gormez S, Ekicibasi E, Degirmencioglu A, Paudel A, Erdim R, Gumusel HK, Eroglu E, Tanboga IH, Dagdelen S, Sariguzel N, et al. Association between renin‐angiotensin‐aldosterone system inhibitor treatment, neutrophil‐lymphocyte ratio, D‐Dimer and clinical severity of COVID‐19 in hospitalized patients: a multicenter, observational study. J Hum Hypertens. 2020;24:1–10. DOI: 10.1038/s41371-020-00405-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Grasselli G, Greco M, Zanella A, Albano G, Antonelli M, Bellani G, Bonanomi E, Cabrini L, Carlesso E, Castelli G, et al. Risk factors associated with mortality among patients with COVID‐19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020;180:1345–1355. DOI: 10.1001/jamainternmed.2020.3539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gupta R, Agrawal R, Bukhari Z, Jabbar A, Wang D, Diks J, Alshal M, Emechebe DY, Brunicardi FC, Lazar JM, et al. Higher comorbidities and early death in hospitalized African‐American patients with Covid‐19. BMC Infect Dis. 2021;21:78. DOI: 10.1186/s12879-021-05782-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Hakeam HA, Alsemari M, Duhailib ZA, Ghonem L, Alharbi SA, Almutairy E, Sheraim NMB, Alsalhi M, Alhijji A, AlQahtani S, et al. Association of angiotensin‐converting enzyme inhibitors and angiotensin II blockers with severity of COVID‐19: a multicenter, prospective study. J Cardiovasc Pharmacol Ther. 2020;26:244–252. DOI: 10.1177/1074248420976279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hippisley‐Cox J, Young D, Coupland C, Channon KM, Tan PS, Harrison DA, Rowan K, Aveyard P, Pavord ID, Watkinson PJ. Risk of severe COVID‐19 disease with ACE inhibitors and angiotensin receptor blockers: cohort study including 8.3 million people. Heart. 2020;106:1503–1511. DOI: 10.1136/heartjnl-2020-317393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Holt A, Mizrak I, Lamberts M, Lav Madsen P. Influence of inhibitors of the renin‐angiotensin system on risk of acute respiratory distress syndrome in Danish hospitalized COVID‐19 patients. J Hypertens. 2020;38:1612–1613. DOI: 10.1097/HJH.0000000000002515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Iaccarino G, Grassi G, Borghi C, Ferri C, Salvetti M, Volpe M, Cicero AFG, Minuz P, Muiesan ML, Mulatero P, et al. Age and multimorbidity predict death among COVID‐19 patients: results of the SARS‐RAS study of the Italian Society of Hypertension. Hypertension. 2020;76:366–372. DOI: 10.1161/HYPERTENSIONAHA.120.15324. [DOI] [PubMed] [Google Scholar]
- 62.Imam Z, Odish F, Gill I, O’Connor D, Armstrong J, Vanood A, Ibironke O, Hanna A, Ranski A, Halalau A. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID‐19 patients in Michigan, United States. J Intern Med. 2020;288:469–476. DOI: 10.1111/joim.13119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Jung C, Bruno RR, Wernly B, Joannidis M, Oeyen S, Zafeiridis T, Marsh B, Andersen FH, Moreno R, Fernandes AM, et al. Inhibitors of the renin‐angiotensin‐aldosterone system and COVID‐19 in critically ill elderly patients. Eur Heart J Cardiovasc Pharmacother. 2021;7:76–77. DOI: 10.1093/ehjcvp/pvaa083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Jung S‐Y, Choi JC, You S‐H, Kim W‐Y. Association of renin‐angiotensin‐aldosterone system inhibitors with coronavirus disease 2019 (COVID‐19)‐ related outcomes in Korea: a nationwide population‐based cohort study. Clin Infect Dis. 2020;71:2121–2128. DOI: 10.1093/cid/ciaa624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Jurado A, Martín MC, Abad‐Molina C, Orduña A, Martínez A, Ocaña E, Yarce O, Navas AM, Trujillo A, Fernández L, et al. COVID‐19: age, interleukin‐6, C‐reactive protein, and lymphocytes as key clues from a multicentre retrospective study. Immun Ageing. 2020;17:22. DOI: 10.1186/s12979-020-00194-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Khan KS, Reed‐Embleton H, Lewis J, Bain P, Mahmud S. Angiotensin converting enzyme inhibitors do not increase the risk of poor outcomes in COVID‐19 disease. a multi‐centre observational study. Scott Med J. 2020;65:149–153. DOI: 10.1177/0036933020951926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Kim J, Kim DW, Kim KI, Kim HB, Kim JH, Lee YG, Byeon KH, Cheong HK; Korean Society of Hypertension . Compliance of antihypertensive medication and risk of coronavirus disease 2019: a cohort study using big data from the Korean National Health Insurance Service. J Korean Med Sci. 2020;35:e232. DOI: 10.3346/jkms.2020.35.e232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kim JH, Baek Y‐H, Lee H, Choe YJ, Shin HJ, Shin J‐Y. Clinical outcomes of COVID‐19 following the use of angiotensin‐converting enzyme inhibitors or angiotensin‐receptor blockers among patients with hypertension in Korea: a nationwide study. Epidemiol Health. 2021;43:e2021004. DOI: 10.4178/epih.e2021004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Kim MK, Jeon J‐H, Kim S‐W, Moon JS, Cho NH, Han E, You JH, Lee JY, Hyun M, Park JS, et al. The clinical characteristics and outcomes of patients with moderate‐to‐severe coronavirus disease 2019 infection and diabetes in Daegu, South Korea. Diabetes Metab J. 2020;44:602–613. DOI: 10.4093/dmj.2020.0146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Kocayigit I, Kocayigit H, Yaylaci S, Can Y, Erdem AF, Karabay O. Impact of antihypertensive agents on clinical course and in‐hospital mortality: analysis of 169 hypertensive patients hospitalized for COVID‐19. Rev Assoc Med Bras (1992). 2020;66(suppl 2):71–76. DOI: 10.1590/1806-9282.66.s2.71. [DOI] [PubMed] [Google Scholar]
- 71.Kolin DA, Kulm S, Christos PJ, Elemento O. Clinical, regional, and genetic characteristics of Covid‐19 patients from UK Biobank. PLoS One. 2020;15:e0241264. DOI: 10.1371/journal.pone.0241264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lafaurie M, Martin‐Blondel G, Delobel P, Charpentier S, Sommet A, Moulis G. Outcome of patients hospitalized for COVID‐19 and exposure to angiotensin‐converting enzyme inhibitors and angiotensin‐receptor blockers in France: results of the ACE‐CoV study. Fundam Clin Pharmacol. 2021;35:194–203. DOI: 10.1111/fcp.12613. [DOI] [PubMed] [Google Scholar]
- 73.Lahens A, Mullaert J, Gressens S, Gault N, Flamant M, Deconinck L, Joly V, Yazdanpanah Y, Lescure F‐X, Vidal‐Petiot E. Association between renin‐angiotensin‐aldosterone system blockers and outcome in coronavirus disease 2019: analysing in‐hospital exposure generates a biased seemingly protective effect of treatment. J Hypertens. 2021;39:367–375. DOI: 10.1097/HJH.0000000000002658. [DOI] [PubMed] [Google Scholar]
- 74.Lam KW, Chow KW, Vo J, Hou W, Li H, Richman PS, Mallipattu SK, Skopicki HA, Singer AJ, Duong TQ. Continued in‐hospital angiotensin‐converting enzyme inhibitor and angiotensin II receptor blocker use in hypertensive COVID‐19 patients is associated with positive clinical outcome. J Infect Dis. 2020;222:1256–1264. DOI: 10.1093/infdis/jiaa447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Lee J, Jo SJ, Cho Y, Lee JH, Oh I‐Y, Park JJ, Cho Y‐S, Choi D‐J. Effects of renin‐angiotensin system blockers on the risk and outcomes of severe acute respiratory syndrome coronavirus 2 infection in patients with hypertension. Korean J Intern Med. 2021;36:S123–S131. DOI: 10.3904/kjim.2020.390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Li J, Wang X, Chen J, Zhang H, Deng A. Association of renin‐angiotensin system inhibitors with severity or risk of death in patients with hypertension hospitalized for coronavirus disease 2019 (COVID‐19) infection in Wuhan, China. JAMA Cardiol. 2020;5:825–830. DOI: 10.1001/jamacardio.2020.1624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Liabeuf S, Moragny J, Bennis Y, Batteux B, Brochot E, Schmit JL, Lanoix J‐P, Andrejak C, Ganry O, Slama M, et al. Association between renin‐angiotensin system inhibitors and COVID‐19 complications. Eur Heart J Cardiovasc Pharmacother. 2020; pvaa062. DOI: 10.1093/ehjcvp/pvaa062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Lim J‐H, Cho J‐H, Jeon Y, Kim JH, Lee GY, Jeon S, Noh HW, Lee Y‐H, Lee J, Chang H‐H, et al. Adverse impact of renin‐angiotensin system blockade on the clinical course in hospitalized patients with severe COVID‐19: a retrospective cohort study. Sci Rep. 2020;10:20250. DOI: 10.1038/s41598-020-76915-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Liu X, Liu Y, Chen K, Yan S, Bai X, Li J, Liu D. Efficacy of ACEIs/ARBs vs CCBs on the progression of COVID‐19 patients with hypertension in Wuhan: a hospital‐based retrospective cohort study. J Med Virol. 2021;93:854–862. DOI: 10.1002/jmv.26315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.López‐Otero D, López‐Pais J, Cacho‐Antonio CE, Antúnez‐Muiños PJ, González‐Ferrero T, Pérez‐Poza M, Otero‐García Ó, Díaz‐Fernández B, Bastos‐Fernández M, Bouzas‐Cruz N, et al. Impact of angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers on COVID‐19 in a western population. CARDIOVID registry. Rev Esp Cardiol (Engl Ed). 2021;74:175–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Mancia G, Rea F, Ludergnani M, Apolone G, Corrao G. Renin‐angiotensin‐aldosterone system blockers and the risk of Covid‐19. N Engl J Med. 2020;382:2431–2440. DOI: 10.1056/NEJMoa2006923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Martínez‐Del Río J, Piqueras‐Flores J, Martín N‐S, de la Sierra P , Negreira‐Caamaño M, Águila‐Gordo D, Mateo‐Gómez C, Salas‐Bravo D, Rodríguez‐Martínez M. Comparative analysis between the use of renin‐angiotensin system antagonists and clinical outcomes of hospitalized patients with COVID‐19 respiratory infection. Med Clin (Engl Ed). 2020;155:473–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Mayer MA, Vidal‐Alaball J, Puigdellívol‐Sánchez A, Marín Gomez FX, Leis A, Mendioroz Peña J. Clinical characterization of patients with COVID‐19 in primary care in catalonia: retrospective observational study. JMIR Public Health Surveill. 2021;7:e25452. DOI: 10.2196/25452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Mehta N, Kalra A, Nowacki AS, Anjewierden S, Han Z, Bhat P, Carmona‐Rubio AE, Jacob M, Procop GW, Harrington S, et al. Association of use of angiotensin‐converting enzyme inhibitors and angiotensin II receptor blockers with testing positive for coronavirus disease 2019 (COVID‐19). JAMA Cardiol. 2020;5:1020–1026. DOI: 10.1001/jamacardio.2020.1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Meng X, Liu Y, Wei C, Zhang K, Zhang Y, Zhong M, Zhang C, Zhang Y. Angiotensin converting enzyme inhibitors and angiotensin receptor blockers improved the outcome of patients with severe COVID‐19 and hypertension. Sci China Life Sci. 2021;64:836–839. DOI: 10.1007/s11427-020-1813-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Million M, Lagier J‐C, Gautret P, Colson P, Fournier P‐E, Amrane S, Hocquart M, Mailhe M, Esteves‐Vieira V, Doudier B, et al. Early treatment of COVID‐19 patients with hydroxychloroquine and azithromycin: a retrospective analysis of 1061 cases in Marseille, France. Travel Med Infect Dis. 2020;35:101738. DOI: 10.1016/j.tmaid.2020.101738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Morales DR, Conover MM, You SC, Pratt N, Kostka K, Duarte‐Salles T, Fernández‐Bertolín S, Aragón M, DuVall SL, Lynch K, et al. Renin‐angiotensin system blockers and susceptibility to COVID‐19: an international, open science, cohort analysis. Lancet Digit Health. 2021;3:e98–e114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Mostaza JM, García‐Iglesias F, González‐Alegre T, Blanco F, Varas M, Hernández‐Blanco C, Hontañón V, Jaras‐Hernández MJ, Martínez‐Prieto M, Menéndez‐Saldaña A, et al. Clinical course and prognostic factors of COVID‐19 infection in an elderly hospitalized population. Arch Gerontol Geriatr. 2020;91:104204. DOI: 10.1016/j.archger.2020.104204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Negreira‐Caamaño M, Piqueras‐Flores J, Martínez‐DelRio J, Nieto‐Sandoval‐Martin‐DeLaSierra P, Aguila‐Gordo D, Mateo‐Gomez C, Salas‐Bravo D, Rodriguez‐Martinez M, Negreira‐Caamaño M. Impact of treatment with renin‐angiotensin system inhibitors on clinical outcomes in hypertensive patients hospitalized with COVID‐19. High Blood Press Cardiovasc Prev. 2020;27:561–568. DOI: 10.1007/s40292-020-00409-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Ng JH, Hirsch JS, Wanchoo R, Sachdeva M, Sakhiya V, Hong S, Jhaveri KD, Fishbane S, Abate M, Andrade HP, et al.; Northwell COVID‐19 Research Consortium and the Northwell Nephrology COVID‐19 Research Consortium . Outcomes of patients with end‐stage kidney disease hospitalized with COVID‐19. Kidney Int. 2020;98:1530–1539. DOI: 10.1016/j.kint.2020.07.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Núñez‐Gil IJ, Fernández‐Ortiz A, Maroud Eid C, Huang J, Romero R, Becerra‐Muñoz VM, Uribarri A, Feltes G, Trabatoni D, Fernandez‐Rozas I, et al. Underlying heart diseases and acute COVID‐19 outcomes. Cardiol J. 2021;28:202–214. DOI: 10.5603/CJ.a2020.0183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Palazzuoli A, Mancone M, De Ferrari GM, Forleo G, Secco GG, Ruocco GM, D'Ascenzo F, Monticone S, Paggi A, Vicenzi M, et al. Antecedent administration of angiotensin‐converting enzyme inhibitors or angiotensin II receptor antagonists and survival after hospitalization for COVID‐19 syndrome. J Am Heart Assoc. 2020;9:e017364. DOI: 10.1161/JAHA.120.017364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Raisi‐Estabragh Z, McCracken C, Ardissino M, Bethell MS, Cooper J, Cooper C, Harvey NC, Petersen SE. Renin‐angiotensin‐aldosterone system blockers are not associated with coronavirus disease 2019 (COVID‐19) hospitalization: study of 1,439 UK Biobank cases. Front Cardiovasc Med. 2020;7:138. DOI: 10.3389/fcvm.2020.00138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Ran J, Song Y, Zhuang Z, Han L, Zhao S, Cao P, Geng Y, Xu L, Qin J, He D, et al. Blood pressure control and adverse outcomes of COVID‐19 infection in patients with concomitant hypertension in Wuhan, China. Hypertens Res. 2020;43:1267–1276. DOI: 10.1038/s41440-020-00541-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Reynolds HR, Adhikari S, Pulgarin C, Troxel AB, Iturrate E, Johnson SB, Hausvater A, Newman JD, Berger JS, Bangalore S, et al. Renin‐angiotensin‐aldosterone system inhibitors and risk of Covid‐19. N Engl J Med. 2020;382:2441–2448. DOI: 10.1056/NEJMoa2008975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Rodilla E, Saura A, Jiménez I, Mendizábal A, Pineda‐Cantero A, Lorenzo‐Hernández E, Fidalgo‐Montero MDP, López‐Cuervo JF, Gil‐Sánchez R, Rabadán‐Pejenaute E, et al. Association of hypertension with all‐cause mortality among hospitalized patients with COVID‐19. J Clin Med. 2020;9:3136. DOI: 10.3390/jcm9103136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Rosenthal N, Cao Z, Gundrum J, Sianis J, Safo S. Risk factors associated with in‐hospital mortality in a US national sample of patients With COVID‐19. JAMA Netw Open. 2020;3:e2029058. DOI: 10.1001/jamanetworkopen.2020.29058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Rossi L, Malagoli A, Biagi A, Zanni A, Sticozzi C, Comastri G, Pannone L, Gandolfi S, Vergara P, Villani GQ. Renin‐angiotensin system inhibitors and mortality in patients with COVID‐19. Infection. 2021;49:287–294. DOI: 10.1007/s15010-020-01550-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Sablerolles RSG, Hogenhuis FEF, Lafeber M, van de Loo BPA , Borgsteede SD, Boersma E, Versmissen J, van der Kuy H ; COMET Research Team . No association between use of angiotensin‐converting enzyme inhibitors or angiotensin II receptor blockers prior to hospital admission and clinical course of COVID‐19 in the COvid MEdicaTion (COMET) study. Br J Clin Pharmacol. 2021;1–9. DOI: 10.1111/bcp.14751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Savarese G, Benson L, Sundström J, Lund LH. Association between renin‐angiotensin‐aldosterone system inhibitor use and COVID‐19 hospitalization and death: a 1.4 million patient nationwide registry analysis. Eur J Heart Fail. 2021;23:476–485. DOI: 10.1002/ejhf.2060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Selçuk M, Çınar T, Keskin M, Çiçek V, Kılıç Ş, Kenan B, Doğan S, Asal S, Günay N, Yıldırım E, et al. Is the use of ACE inb/ARBs associated with higher in‐hospital mortality in Covid‐19 pneumonia patients? Clin Exp Hypertens. 2020;42:738–742. DOI: 10.1080/10641963.2020.1783549. [DOI] [PubMed] [Google Scholar]
- 102.Semenzato L, Botton J, Drouin J, Baricault B, Vabre C, Cuenot F, Penso L, Herlemont P, Sbidian E, Weill A, et al. Antihypertensive drugs and COVID‐19 risk: a cohort study of 2 million hypertensive patients. Hypertension. 2021;77:833–842. DOI: 10.1161/HYPERTENSIONAHA.120.16314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Şenkal N, Meral R, Medetalibeyoğlu A, Konyaoğlu H, Kose M, Tukek T. Association between chronic ACE inhibitor exposure and decreased odds of severe disease in patients with COVID‐19. Anatol J Cardiol. 2020;24:21–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Seo J, Son M. Update on association between exposure to renin‐angiotensin‐aldosterone system inhibitors and coronavirus disease 2019 in South Korea. Korean J Intern Med. 2021;36:S114–S212. DOI: 10.3904/kjim.2020.380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Shah P, Owens J, Franklin J, Jani Y, Kumar A, Doshi R. Baseline use of angiotensin‐converting enzyme inhibitor/AT1 blocker and outcomes in hospitalized coronavirus disease 2019 African‐American patients. J Hypertens. 2020;38:2537–2541. DOI: 10.1097/HJH.0000000000002584. [DOI] [PubMed] [Google Scholar]
- 106.Soleimani A, Kazemian S, Karbalai Saleh S, Aminorroaya A, Shajari Z, Hadadi A, Talebpour M, Sadeghian H, Payandemehr P, Sotoodehnia M, et al. Effects of angiotensin receptor blockers (ARBs) on in‐hospital outcomes of patients with hypertension and confirmed or clinically suspected COVID‐19. Am J Hypertens. 2020;33:1102–1111. DOI: 10.1093/ajh/hpaa149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Son M, Seo J, Yang S. Association between renin‐angiotensin‐aldosterone system inhibitors and COVID‐19 infection in South Korea. Hypertension. 2020;76:742–749. DOI: 10.1161/HYPERTENSIONAHA.120.15464. [DOI] [PubMed] [Google Scholar]
- 108.Stevens JS, King KL, Robbins‐Juarez SY, Khairallah P, Toma K, Alvarado Verduzco H, Daniel E, Douglas D, Moses AA, Peleg Y, et al. High rate of renal recovery in survivors of COVID‐19 associated acute renal failure requiring renal replacement therapy. PLoS One. 2020;15:e0244131. DOI: 10.1371/journal.pone.0244131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Tedeschi S, Giannella M, Bartoletti M, Trapani F, Tadolini M, Borghi C, Viale P. Clinical impact of renin‐angiotensin system inhibitors on in‐hospital mortality of patients with hypertension hospitalized for coronavirus disease 2019. Clin Infect Dis. 2020;71:899–901. DOI: 10.1093/cid/ciaa492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Tetlow S, Segiet‐Swiecicka A, O’Sullivan R, O’Halloran S, Kalb K, Brathwaite‐Shirley C, Alger L, Ankuli A, Baig MS, Catmur F, et al. ACE inhibitors, angiotensin receptor blockers and endothelial injury in COVID‐19. J Intern Med. 2021;289:688–699. DOI: 10.1111/joim.13202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Trifirò G, Massari M, Da Cas R, Menniti Ippolito F, Sultana J, Crisafulli S, Giorgi Rossi P, Marino M, Zorzi M, Bovo E, et al. Renin‐angiotensin‐aldosterone system inhibitors and risk of death in patients hospitalised with COVID‐19: a retrospective Italian cohort study of 43,000 patients. Drug Saf. 2020;43:1297–1308. DOI: 10.1007/s40264-020-00994-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Trump S, Lukassen S, Anker MS, Chua RL, Liebig J, Thürmann L, Corman VM, Binder M, Loske J, Klasa C, et al. Hypertension delays viral clearance and exacerbates airway hyperinflammation in patients with COVID‐19. Nat Biotechnol. 2021;39:705–716. [epub ahead of print]. DOI: 10.1038/s41587-020-00796-1. [DOI] [PubMed] [Google Scholar]
- 113.Vila‐Córcoles A, Ochoa‐Gondar O, Satué‐Gracia EM, Torrente‐Fraga C, Gomez‐Bertomeu F, Vila‐Rovira A, Hospital‐Guardiola I, de Diego‐Cabanes C , Bejarano‐Romero F, Basora‐Gallisà J. Influence of prior comorbidities and chronic medications use on the risk of COVID‐19 in adults: a population‐based cohort study in Tarragona, Spain. BMJ Open. 2020;10:e041577. DOI: 10.1136/bmjopen-2020-041577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Vila‐Corcoles A, Satue‐Gracia E, Ochoa‐Gondar O, Torrente‐Fraga C, Gomez‐Bertomeu F, Vila‐Rovira A, Hospital‐Guardiola I, de Diego‐Cabanes C , Bejarano‐Romero F, Rovira‐Veciana D, et al. Use of distinct anti‐hypertensive drugs and risk for COVID‐19 among hypertensive people: a population‐based cohort study in Southern Catalonia, Spain. J Clin Hypertens (Greenwich). 2020;22:1379–1388. DOI: 10.1111/jch.13948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Xu J, Huang C, Fan G, Liu Z, Shang L, Zhou F, Wang Y, Yu J, Yang L, Xie KE, et al. Use of angiotensin‐converting enzyme inhibitors and angiotensin II receptor blockers in context of COVID‐19 outbreak: a retrospective analysis. Front Med. 2020;14:601–612. DOI: 10.1007/s11684-020-0800-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Yahyavi A, Hemmati N, Derakhshan P, Banivaheb B, Karimi Behnagh A, Tofighi R, TehraniYazdi A, Kabir A. Angiotensin enzyme inhibitors and angiotensin receptor blockers as protective factors in COVID‐19 mortality: a retrospective cohort study. Intern Emerg Med. 2020;1–11. DOI: 10.1007/s11739-020-02523-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Yan F, Huang F, Xu J, Yang P, Qin Y, Lv J, Zhang S, Ye LU, Gong M, Liu Z, et al. Antihypertensive drugs are associated with reduced fatal outcomes and improved clinical characteristics in elderly COVID‐19 patients. Cell Discov. 2020;6:77. DOI: 10.1038/s41421-020-00221-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Yan H, Valdes AM, Vijay A, Wang S, Liang L, Yang S, Wang H, Tan X, Du J, Jin S, et al. Role of drugs used for chronic disease management on susceptibility and severity of COVID‐19: a large case‐control study. Clin Pharmacol Ther. 2020;108:1185–1194. DOI: 10.1002/cpt.2047. [DOI] [PubMed] [Google Scholar]
- 119.Zhang P, Zhu L, Cai J, Lei F, Qin J‐J, Xie J, Liu Y‐M, Zhao Y‐C, Huang X, Lin L, et al. Association of inpatient use of angiotensin‐converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID‐19. Circ Res. 2020;126:1671–1681. DOI: 10.1161/CIRCRESAHA.120.317134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Zhong Y, Zhao L, Wu G, Hu C, Wu C, Xu M, Dong H, Zhang Q, Wang G, Yu BO, et al. Impact of renin‐angiotensin system inhibitors use on mortality in severe COVID‐19 patients with hypertension: a retrospective observational study. J Int Med Res. 2020;48:300060520979151. DOI: 10.1177/0300060520979151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Zhou F, Liu Y‐M, Xie J, Li H, Lei F, Yang H, Qin J‐J, Cai J, Zhang X‐J, Wu B, et al. Comparative impacts of ACE (angiotensin‐converting enzyme) inhibitors versus angiotensin II receptor blockers on the risk of COVID‐19 mortality. Hypertension. 2020;76:e15–e17. DOI: 10.1161/HYPERTENSIONAHA.120.15622. [DOI] [PubMed] [Google Scholar]
- 122.Zhou X, Zhu J, Xu T. Clinical characteristics of coronavirus disease 2019 (COVID‐19) patients with hypertension on renin‐angiotensin system inhibitors. Clin Exp Hypertens. 2020;42:656–660. DOI: 10.1080/10641963.2020.1764018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Zhou Y, Hou Y, Shen J, Mehra R, Kallianpur A, Culver DA, Gack MU, Farha S, Zein J, Comhair S, et al. A network medicine approach to investigation and population‐based validation of disease manifestations and drug repurposing for COVID‐19. PLoS Biol. 2020;18:e3000970. DOI: 10.1371/journal.pbio.3000970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Griffith GJ, Morris TT, Tudball MJ, Herbert A, Mancano G, Pike L, Sharp GC, Sterne J, Palmer TM, Davey Smith G, et al. Collider bias undermines our understanding of COVID‐19 disease risk and severity. Nat Commun. 2020;11:5749. DOI: 10.1038/s41467-020-19478-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Zheng Y‐Y, Ma Y‐T, Zhang J‐Y, Xie X. COVID‐19 and the cardiovascular system. Nat Rev Cardiol. 2020;17:259–260. DOI: 10.1038/s41569-020-0360-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Anell A. The public‐private pendulum—patient choice and equity in Sweden. N Engl J Med. 2015;372:1–3. DOI: 10.1056/NEJMp1411430. [DOI] [PubMed] [Google Scholar]
- 127.Ludvigsson JF, Otterblad‐Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24:659–667. DOI: 10.1007/s10654-009-9350-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.World Health Organization . International classification of disease and related health problems. Available at: http://www.who.int/classifications/icd/en/. Accessed December 11, 2020.
- 129.Nordic Medico‐Statistical Committee . NOMESCO classification of surgical procedures. 2010. Available at: https://norden.diva‐portal.org/smash/get/diva2:970547/FULLTEXT01.pdf. Accessed December 11, 2020.
- 130.World Health Organization . WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2017. Available at: https://www.whocc.no/. Accessed December 11, 2020.
- 131.Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement D, Coca A, De Simone G, Dominiczak A, et al. 2018 practice guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens. 2018;36:2284–2309. [DOI] [PubMed] [Google Scholar]
- 132.Johns Hopkins Coronavirus Resource Center . COVID‐19 map. Available at: https://coronavirus.jhu.edu/map.html. Accessed December 11, 2020.
- 133.Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, Chalmers J, Rodgers A, Rahimi K. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta‐analysis. Lancet. 2016;387:957–967. DOI: 10.1016/S0140-6736(15)01225-8. [DOI] [PubMed] [Google Scholar]
- 134.R Core Team . R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2015. Available at: https://www.r‐project.org/. Accessed December 11, 2020. [Google Scholar]
- 135.Therneau TM. until 2009. Original S‐>R port and R maintainer, Elizabeth A, Cynthia C. Survival: Survival Analysis. Vienna, Austria: R Foundation for Statistical Computing. Available at: https://CRAN.R‐project.org/package=survival. Accessed December 11, 2020. [Google Scholar]
- 136.Ridgeway G, McCaffrey D, Morral A, Griffin BA, Burgette L, Cefalu M. twang: Toolkit for Weighting and Analysis of Nonequivalent Groups. Vienna, Austria: R Foundation for Statistical Computing; 2020. Available at: https://CRAN.R‐project.org/package=twang. Accessed November 30, 2020. [Google Scholar]
- 137.Imai Y, Kuba K, Rao S, Huan YI, Guo F, Guan B, Yang P, Sarao R, Wada T, Leong‐Poi H, et al. Angiotensin‐converting enzyme 2 protects from severe acute lung failure. Nature. 2005;436:112–116. DOI: 10.1038/nature03712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Hastie T, Tibshirani R, Friedman J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction. 2nd ed. New York: Springer‐Verlag; 2009. Available from: https://www.springer.com/gp/book/9780387848570. Accessed November 30, 2020. [Google Scholar]
- 139.McCaffrey DF, Ridgeway G, Morral AR. Propensity score estimation with boosted regression for evaluating causal effects in observational studies. Psychol Methods. 2004;9:403–425. DOI: 10.1037/1082-989X.9.4.403. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.