

Abstract
Objective
To provide a comprehensive, evidence-based overview of the risk factors, prevention, diagnosis, imaging, treatment and prognosis for Achilles tendinopathy. To make clinical recommendations for healthcare practitioners and patients.
Design
Comprehensive multidisciplinary guideline process funded by the Quality Foundation of the Dutch Federation of Medical Specialists. This process included a development, commentary and authorisation phase. Patients participated in every phase.
Data sources
Multiple databases and existing guidelines were searched up to May 2019. Information from patients, healthcare providers and other stakeholders were obtained using a digital questionnaire, focus group interview and invitational conference.
Study eligibility criteria
Studies on both insertional and/or midportion Achilles tendinopathy were eligible. Specific eligibility criteria were described per module.
Data extraction and synthesis
To appraise the certainty of evidence, reviewers extracted data, assessed risk of bias and used the Grading of Recommendations Assessment, Development and Evaluation method, where applicable. Important considerations were: patient values and preferences, costs, acceptability of other stakeholders and feasibility of implementation. Recommendations were made based on the results of the evidence from the literature and the considerations.
Primary outcome measure
The primary and secondary outcome measures were defined per module and defined based on the input of patients obtained in collaboration with the Netherlands Patient Federation and healthcare providers from different professions.
Results
Six specific modules were completed: risk factors and primary prevention, diagnosis, imaging, treatment prognosis and secondary prevention for Achilles tendinopathy.
Summary/conclusion
Our Dutch multidisciplinary guideline on Achilles tendinopathy provides six modules developed according to the standards of the Dutch Federation of Medical Specialists. Evidence-based recommendations for clinical practice are given for risk factors, prevention, diagnosis, imaging, treatment and prognosis. This guideline can assist healthcare providers and patients in clinical practice.
Keywords: achilles tendon, risk factor, injury prevention, ultrasonography, treatment
General introduction
Background to this guideline
Sports medicine was finally recognised as a clinical medical specialty in Holland in 2014. Following this recognition, the Dutch Association of Sports Medicine could apply for funding to develop clinical guidelines. This guideline is the result of a successful funding application and was produced according to the official process. This is very similar to the National Institute for Health and Care Excellence process in the UK. Achilles tendinopathy was chosen as it is common in clinical practice, seriously impacts patients and there is a significant body of scientific literature on the subject.
An Achilles tendon injury is a frequent problem in both active athletes and inactive individuals. In athletes, this may be caused by the external load being too high and in inactive individuals relative overload may be caused by a very low baseline capacity. In Dutch general practice, Achilles tendon symptoms occur in 2–3 per 1000 adult patients.1 Runners have a 52% chance (cumulative incidence) of having an Achilles tendon injury in their lifetime.2 The symptoms are often longstanding and lead to disability, thus being the main reason that people present to clinical practice.
The terminology used to describe and diagnose tendon injuries has changed in recent decades.3 According to the current consensus, local pain in a tendon in association with tendon-loading activities is referred to as ‘tendinopathy’.4 The use of clear unambiguous terminology is important because it ensures clear communication between healthcare providers and reduces the risk of confusing patients.
The exact pathophysiology of Achilles tendinopathy is still unknown; it is thought to have a multifactorial origin. A better understanding of risk factors can help develop more effective (preventive) interventions.
The diagnosis of Achilles tendinopathy is usually made using clinical findings. The exact diagnostic criteria are not sufficiently described. The role of imaging in making a diagnosis is also not agreed on.4 In addition, there are a number of (systemic) conditions that should be considered in patients with pain in the Achilles tendon region.5 6 Recognition of these disorders by healthcare providers is important, as this strongly affects treatment and prognosis.
Imaging is frequently used in patients with Achilles tendon complaints. X-rays, ultrasound and MRI scans have prominent roles in imaging.7 In clinical practice, prognostic value is often attributed to the findings on imaging. On the other hand, imaging can have negative effects through radiation risks, misinterpretation by healthcare providers (leading to unnecessary additional imaging and interventions) and patients (leading to confusion, catastrophising, fear and avoidance of movement, and low expectations of recovery).8 It is important that the additional value and potential negative consequences of using imaging for healthcare providers and patients is clear.
Treatment of Achilles tendinopathy is initially non-surgical.9 If non-surgical treatment fails, surgical interventions may be considered. In current clinical practice, the use of treatment options is often variable and suboptimal. There are also no clear guidelines on load management during sports.
Achilles tendinopathy seems to have an unfavourable long-term prognosis. In clinical practice, it is desirable to be able to predict which patients recover and who will continue to experience chronic symptoms. Knowledge of prognostic factors is important to be able to do this. Finally, preventiing recurrent symptoms is important. A practical, step-by-step treatment strategy for Achilles tendinopathy is necessary based on existing guidelines and evidence. The complete guideline process is described in online supplemental file ‘Guideline process’.
bjsports-2020-103867supp002.pdf (208KB, pdf)
Aim of the guideline
The aim was to develop a multidisciplinary evidence-based guideline on the risk factors, diagnosis, imaging, treatment, prognosis and prevention of Achilles tendinopathy. The guideline provides guidance on how to manage the challenges for patients with Achilles tendinopathy in the primary and secondary healthcare settings.
A multidisciplinary working group was set up to develop this guideline. The working group consisted of representatives of relevant specialties involved in the care of Achilles tendinopathy. The online supplemental file ‘Guideline process’ shows the composition of the working group.
The conclusions in this guideline indicate the level of evidence. The recommendations are aimed at optimal care and are based on the results of both scientific research and the considerations of the working group, in which the patient perspective has an important role. Ultimately, this should lead to the overall aim, which is to reduce pain and improve the function and activity level in patients with Achilles tendinopathy by optimising care.
Scope of the guideline
This guideline is intended for the broad group of patients with Achilles tendinopathy. Initially, efforts were made to work with four subcategories of Achilles tendinopathy, based on the most recent literature.10 11 Location and duration of Achilles tendinopathy played a prominent role in this subclassification. Reactive tendinopathy was defined as symptom duration shorter than 6 weeks and a chronic tendinopathy for 3 months or longer.11 It became clear during the process of development that there was little literature on and inconsistent definitions of reactive Achilles tendinopathy. There were also differing views on the definition of this entity within the working group. Consequently, it was chosen not to use this subclassification based on symptom duration. The subclassification based on the location of the condition was maintained in the guideline (figure 1).
Figure 1.

Distinguishing Achilles tendinopathy based on location of the symptoms. Insertional Achilles tendinopathy is localised within the first 2 cm of the attachment of the Achilles tendon on the calcaneus (left side figure) and midportion Achilles tendinopathy is localised >2 cm above this attachment (right side figure).
The working group defined insertional tendinopathy as symptoms localised within the first 2 cm of the attachment of the Achilles tendon to the calcaneus. There may be a tendinopathy of the Achilles tendon insertion, an associated prominence of the calcaneus (Haglund morphology) and/or an associated retrocalcaneal bursitis.12 The working group defined midportion tendinopathy as symptoms localised >2 cm above the distal attachment and according to the current consensus this concerns an isolated tendinopathy of the middle part of the Achilles tendon.12 The distinction between these two subclassifications is also justified, because there seems to be a difference in prognosis during non-surgical treatment.13
In contrast to the 2007 Dutch guideline,9 the patient group in this guideline included both active and sedentary people. This guideline also includes identification of patients with a systemic cause of tendinopathy, for example, an enthesitis because of a rheumatic disease or a tendon xanthoma as a result of familial hypercholesterolaemia. However, the major clinical questions in the guideline will not be covered specifically for these uncommon patient groups. This guideline is not intended for patients younger than 18. Achilles tendon symptoms in patients under the age of 18 are usually caused by extra-articular osteochondrosis (Morbus Sever or Sever’s disease). Complete Achilles tendon ruptures are also excluded from this guideline.
The current challenges in practice and key outcome measures have been identified in collaboration with patients who have been diagnosed with Achilles tendinopathy. There is currently no specific patient association for Achilles tendinopathy. We initially formed a patient panel (n=9), collecting information on which challenges in practice they had experienced. In this analysis, six challenges in practice were prioritised, which were developed into the guideline modules:
There is insufficient knowledge about the causes of Achilles tendinopathy and what can be done to prevent it.
The criteria for determining the diagnosis of Achilles tendinopathy are not sufficiently known.
The role of imaging in Achilles tendinopathy is unclear.
There is insufficient knowledge about the natural course and which treatments should be used for patients with Achilles tendinopathy.
There is a lack of knowledge about the long-term prognosis in patients with Achilles tendinopathy.
There is a lack of knowledge about preventing recurrent symptoms after recovery from Achilles tendinopathy.
A national survey was then launched in collaboration with the Netherlands Patient Federation. Ninety-seven patients with Achilles tendinopathy responded to this digital questionnaire. A total of 85 (88%) of these patients described their treatment aims. The most common aims were: participation in sports without mentioning pain status (36%), pain-free sports participation (27%), pain-free functioning in activities of daily living (ADL) (22%), pain reduction without further specification and restoration of function in ADL without specific mentioning pain status.14
In a recent international consensus meeting, a similar process was conducted with the broad aim of determining the main outcome measures of tendinopathy for healthcare providers (n=29) and patients with tendinopathy in different locations (n=32). In this consensus meeting, the domains 'degree of pain in relation to loading' and 'participation' emerged as patient-relevant outcome measures.15
Based on this feedback from patients, this guideline defines the validated and disease-specific Victorian Institute of Sports Assessment-Achilles (VISA-A) score, return to sports rate, patient satisfaction and subjective recovery as crucial and important outcome measures. The validated VISA-A questionnaire consists of eight questions that cover three domains: pain during ADL, during functional testing and (sports) activities.16 17 A score of 100 points is optimal and represents a fully loadable Achilles tendon without symptoms, a score of 0 points represents a very low load bearing capacity of the Achilles tendon with severe symptoms. This questionnaire is included in online supplemental file ‘VISA-A questionnaire’. The return to sports rate, patient satisfaction and subjective recovery should always be patient-reported, with the type of scale used not being further specified in the guideline.
bjsports-2020-103867supp001.pdf (169.4KB, pdf)
The guideline contains six separate modules. Each module contains different sections and submodules. The make-up of the guideline is shown in figure 2. A full description of the guideline accountability and process is provided in online supplemental file ‘Guideline process’.
Figure 2.

Overview of the Dutch multidisciplinary guideline process and the six modules.
Module 1 risk factors and primary prevention of Achilles tendinopathy
Scoping question
Which individuals are at increased risk of developing Achilles tendinopathy and how can this be prevented?
This scoping question includes the following two subquestions
Which modifiable and non-modifiable factors increase the risk of Achilles tendinopathy?
Which primary prevention strategy is most effective for Achilles tendinopathy?
Introduction
Problem
The onset of Achilles tendinopathy is generally related to ageing and overuse.18 In addition, biomechanical factors, genetic factors, specific health problems, medication use and imaging abnormalities are thought to be associated with the onset of Achilles tendinopathy. There is currently insufficient knowledge about modifiable and non-modifiable risk factors for the onset of Achilles tendinopathy. This is important because it can inform (preventive) interventions.
Primary prevention aims to prevent an initial disease episode, and this is an important topic especially in sports. By applying primary prevention in specific populations at high risk of Achilles tendinopathy, both the incidence and long-term symptoms may be reduced.
There is insufficient knowledge about the effectiveness of primary prevention strategies for Achilles tendinopathy. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 1.
bjsports-2020-103867supp003.pdf (712.1KB, pdf)
Recommendations
Midportion and insertional Achilles tendinopathy
Consider informing individuals with a history of lower limb tendinopathy who are going to become active or increase their training load about the increased risk of Achilles tendinopathy.
A gradual training build-up, taking into account the type, frequency, size and intensity of the training.
Targeted calf muscle strengthening exercises prior to the sports season, in which the exercise dosage should be tailored to the individual.
Wearing enough warm clothing during training in the winter.
In the context of the importance of preventing Achilles tendinopathy, consider advising individuals to avoid the use of fluoroquinolone antibiotics if alternative antibiotics are available and the clinical picture allows.
Module 2 diagnosis of Achilles tendinopathy
Scoping question
How is Achilles tendinopathy diagnosed?
The scoping question includes the following two subquestions
What are the criteria for diagnosing Achilles tendinopathy?
Which differential diagnoses of posterior ankle pain should be considered and which underlying pathology might be related to Achilles tendinopathy?
Introduction
Problem
Achilles tendinopathy is often diagnosed based on clinical findings. When a healthcare provider is confronted with posterior ankle pain suggestive of Achilles tendinopathy, several differential diagnoses should be considered. Imaging can be added to aid the diagnostic process. In most cases, Achilles tendinopathy is suggested to be caused by overload, but it can also be related to other (systemic) disorders.19 Recognition of these disorders is important, because different causes of Achilles tendinopathy might require different treatment strategies. It is important to know how to diagnose Achilles tendinopathy and which differential diagnoses and possible related disorders should be considered. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 2.
bjsports-2020-103867supp004.pdf (389.8KB, pdf)
Recommendations
Midportion Achilles tendinopathy and insertional Achilles tendinopathy
Diagnose midportion Achilles tendinopathy based on the presence of all the following findings:
Symptoms localised 2–7 cm proximal to the Achilles tendon insertion.
Painful Achilles tendon midportion on (sports) loading.
Local thickening of the Achilles tendon midportion (this may be absent in cases with short symptom duration).
Pain on local palpation of the Achilles tendon midportion.
Diagnose insertional Achilles tendinopathy based on the presence of all the following findings:
Symptoms localised to the Achilles tendon insertional region (within 2 cm of the insertion of the Achilles tendon).
Painful Achilles tendon insertional region on (sports) loading.
Local thickening of the Achilles tendon insertion (this may be absent in cases with short symptom duration).
Pain on local palpation of the Achilles tendon insertion.
No additional imaging studies are needed if the presenting case fits all four diagnostic criteria.
Consider additional imaging examinations (X-ray of the calcaneus, ultrasound of the Achilles tendon or MRI of the ankle) if:
The symptoms do not fit with all four diagnostic criteria.
The symptoms match all four diagnostic criteria, but there is an unexpected course or change of symptoms during follow-up.
Surgery is being considered.
Consider a referral to a sports medicine physician or an orthopaedic surgeon if:
There is continued uncertainty about the diagnosis.
There is an unexpected course or change of symptoms during follow-up.
Consider a referral to a rheumatologist if:
There is insertional Achilles tendinopathy or an established diagnosis of spondylarthritis or a suspicion of this condition (chronic low back pain that started before the age of 45 or psoriasis).
Consider a referral to a general medical consultant if:
There is midportion Achilles tendinopathy and a demonstrated familial hypercholesterolaemia or suspicion of this condition (an untreated low-density lipoprotein (LDL) cholesterol value higher than 5.0mmol/L or an untreated total cholesterol value higher than 8.0mmol/L, a first degree relative with cardiovascular disease before the age of 60, a first-degree relative with an untreated total cholesterol level higher than 8.0mmol/L (approximately equivalent to an LDL cholesterol level higher than 5.0 mmol/l mmol/L), presence of cardiovascular disease under the age of 60 and/or the presence of an arcus lipoides under the age of 45.
In patients with posterior ankle pain, consider alternative diagnoses (online supplemental table 2.5).
In patients with the clinical diagnosis of Achilles tendinopathy, consider underlying causes and associated pathologies (online supplemental table 2.6).
bjsports-2020-103867supp006.pdf (3.9MB, pdf)
Module 3 imaging of Achilles tendinopathy
Scoping question
What is the role of imaging in Achilles tendinopathy?
This scoping question includes the following four submodules
Which imaging techniques can be used for assessing Achilles tendinopathy in clinical practice?
Which qualifications are required to perform imaging?
Which imaging findings are characteristic for Achilles tendinopathy?
Which imaging findings have prognostic value in Achilles tendinopathy?
Submodule 3.1 types of imaging
Which imaging techniques can be used for assessing Achilles tendinopathy in clinical practice?
Introduction
Problem
The diagnosis of Achilles tendinopathy can be made based on clinical criteria. Additional imaging may be used if the diagnosis is uncertain or in case of an unexpected course of symptoms or during a pre-operative workup. There are several imaging modalities that are used in Achilles tendinopathy and some modalities are performed by different healthcare providers. There is currently no adequate overview for healthcare providers on the imaging modalities they can use for Achilles tendinopathy. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 3.
bjsports-2020-103867supp005.pdf (534.8KB, pdf)
Recommendations
Midportion Achilles tendinopathy
If imaging is deemed necessary, consider the following imaging modalities:
Ultrasound is the preferred imaging investigation
-
MRI if:
Ultrasound is not available.
There is a discrepancy between the ultrasound results and the clinical findings.
An additional specific diagnosis is expected which cannot be detected by ultrasound.
Surgery is being considered.
Insertional Achilles tendinopathy
If imaging is deemed necessary, consider the following imaging modalities:
Ultrasound is the preferred imaging investigation
X-ray of the calcaneus (lateral view) for the exclusion of bony abnormalities
-
MRI if:
Ultrasound is not available.
There is a discrepancy between the ultrasound results and the clinical findings.
An additional specific diagnosis is expected which cannot be detected by ultrasound.
Surgery is being considered.
Submodule 3.2 required qualifications
Which qualifications are required to perform imaging?
Introduction
Problem
There are several imaging techniques used in Achilles tendinopathy and some of these techniques are performed by different healthcare providers. There is insufficient knowledge of which qualifications are needed to apply, assess and communicate the results of an imaging modality to a patient with Achilles tendinopathy. The literature search, selection conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 3.
Recommendations
Midportion and insertional Achilles tendinopathy
Ensure additional imaging studies are performed and assessed by the healthcare provider with the highest possible qualification for performing them.
When applying imaging, consider the following competencies:
The healthcare provider referring for imaging (or performing the imaging themselves) is able to critically consider the added value of the imaging technique. Using the technique should be clinically important for the patient.
The healthcare provider who performs and assesses the imaging has sufficient training and experience. For the maintenance and renewal of knowledge, regular further training and continued medical education is recommended.
The healthcare provider who communicates the results of the imaging has sufficient knowledge of the clinical picture and the relationship between imaging findings and the outcome in Achilles tendinopathy.
Submodule 3.3 diagnostic findings
Which imaging findings are characteristic for Achilles tendinopathy?
Introduction
Problem
Multiple findings on imaging have been described that can be present in Achilles tendinopathy. However, it is unknown which findings are more frequent in patients with Achilles tendinopathy compared with an asymptomatic population. Diagnostic criteria for imaging are currently lacking. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 3.
Recommendations
Midportion Achilles tendinopathy
When using ultrasound or MRI in clinically diagnosed Achilles tendinopathy, report the following parameters as a minimum:
Increased thickness of the Achilles tendon (anterior-posterior diameter).
Altered structure of the Achilles tendon (altered echogenicity on ultrasound and altered signal intensity on MRI).
Presence of parameters for vascularisation (peritendinous or intratendinous).
Insertional Achilles Tendinopathy
For X-ray of the calcaneus in clinically diagnosed insertional Achilles tendinopathy, report the following characteristic as a minimum:
Calcifications located at the insertion of the Achilles tendon.
When using ultrasound or MRI in clinically diagnosed Achilles tendinopathy, report the following parameters as a minimum:
Increased thickness of the Achilles tendon (anterior-posterior diameter).
Altered structure of the Achilles tendon (altered echogenicity on ultrasound and altered signal intensity on MRI).
Presence of parameters for vascularisation (peritendinous or intratendinous).
Submodule 3.4 prognostic factors
Which imaging findings have prognostic value in Achilles tendinopathy?
Introduction
Problem
Imaging is often used in the diagnostic process. In clinical practice, imaging is sometimes used to provide the prognosis, but it is unknown whether imaging findings have a prognostic value. It is important to have this information. The literature search, selection, conclusions, considerations, and summary with tables and/or figures are presented in online supplemental file module 3.
Recommendations
Midportion Achilles Tendinopathy and insertional Achilles tendinopathy
Do not perform imaging to determine the prognosis of Achilles tendinopathy.
Inform patients with Achilles tendinopathy who have had imaging that their findings have no prognostic value.
Module 4 treatment of Achilles tendinopathy
Scoping question
What is the effectiveness of current treatments for Achilles tendinopathy?
This scoping question includes the following six submodules
Which measurement instruments are best suited for monitoring a treatment effect?
What is the effect of a wait-and-see policy in Achilles tendinopathy?
Which non-surgical treatment is most effective for Achilles tendinopathy?
Is surgery more effective than non-surgical treatment for Achilles tendinopathy?
Which factors influence treatment effects in Achilles tendinopathy?
What advice (self-management and patient education) should be given to patients with Achilles tendinopathy regarding lifestyle, work and sports loading?
Submodule 4.1 measurement instruments
Which measurement instruments are best suited for monitoring a treatment effect?
Introduction
Problem
There are many potential outcome measures for evaluating Achilles tendinopathy. This makes comparing different treatment modalities very difficult. Consensus on the outcome measures to be used is therefore important. The outcome measures should be considered relevant by both patients and healthcare providers and it is important to include both perspectives when advising a ‘core outcome set’ for Achilles tendinopathy. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion Achilles tendinopathy and insertional Achilles tendinopathy
Consider using the VISA-A questionnaire to evaluate the course of Achilles tendinopathy.
Do not request imaging to monitor treatment response and/or predict the course of symptoms of Achilles tendinopathy.
Submodule 4.2: wait-and-see policy
What is the effect of a wait-and-see policy in Achilles tendinopathy?
Introduction
Problem
The initial advice for Achilles tendinopathy often consists of temporarily adjusting or stopping the (sports) load that probably caused the injury and wait and see. There is currently insufficient insight into the natural course of Achilles tendinopathy in the absence of active treatment. The search question is therefore whether active treatment should be used or whether a wait-and-see policy is also sufficient. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion and insertional Achilles tendinopathy
Inform patients with chronic Achilles tendinopathy that no, or only limited improvements, are expected in the short term as a result of a wait-and-see policy.
Submodule 4.3: non-surgical treatment options
Which non-surgical treatment is most effective for Achilles tendinopathy?
Introduction
Problem
Non-surgical treatment is usually the first choice for Achilles tendinopathy. Non-surgical treatments can be divided into several categories. The effectiveness of non-surgical treatments can be evaluated using different control groups. For this reason, the following non-surgical intervention categories were defined: a wait-and-see policy, placebo treatment, exercise therapy, orthoses, shockwave therapy, medication, acupuncture, injection therapy and multimodal treatments. From our national patient survey, we found that the majority of patients receive multiple treatments from these categories. This results in significant healthcare consumption.20 This is mainly due to the lack of knowledge about the comparative effectiveness of the different treatment options. The literature search, selection, conclusions, considerations, and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion Achilles tendinopathy and insertional Achilles tendinopathy
Advise active treatment.
Treatment should be provided by a healthcare provider who is sufficiently qualified (medical or paramedical healthcare provider).
Discuss the initial active treatment options together with the patient. Start treatment of midportion and insertional Achilles tendinopathy with:
-
Patient education:
Explanation about the condition.
Explanation about the prognosis.
Pain education and addressing psychological factors.
-
Loading advice:
Temporary cessation of pain provoking (sports) activities.
Temporary replacement of provocative (sports) activities with non-provocative (sports) activities.
Gradual increase of the load of (sports) activities.
Use a pain scale to monitor the level of complaints related to (sports) activities and adjust these activities based on the pain scale.
Progressive calf muscle strengthening exercises for at least 12 weeks (figure 3). The form of exercise therapy should be suitable for the individual patient. Consider the role of: motivation, time constraints, pain monitoring and availability of facilities and resources. For insertional Achilles tendinopathy, consider initially performing exercises on a flat surface.
After 3 months of patient education, structural exercise therapy and following loading advice, if there is still no improvement discuss additional treatment options. Discuss the uncertainty surrounding of the additional effect and the advantages and disadvantages of any additional treatment. The best treatment option can then be decided together with the patient.
The following additional treatment options can be considered in case of insufficient effectiveness of patient education and loading advice in combination with continued exercise therapy:
Extracorporeal shockwave therapy.
Other passive modalities (the use of a night splint, inlays, use of collagen supplements, application of ultrasound and friction massages, laser therapy and light therapy).
Injection therapies (injections with polidocanol, lidocaine, autologous blood, platelet-rich plasma, stromal vascular fraction, hyaluronic acid, prolotherapy or high-volume injection) and acupuncture (or intratendinous needling).
Be cautious with the following additional treatment options:
Non-steroidal anti-inflammatory drugs.
Corticosteroid injections.
Figure 3.
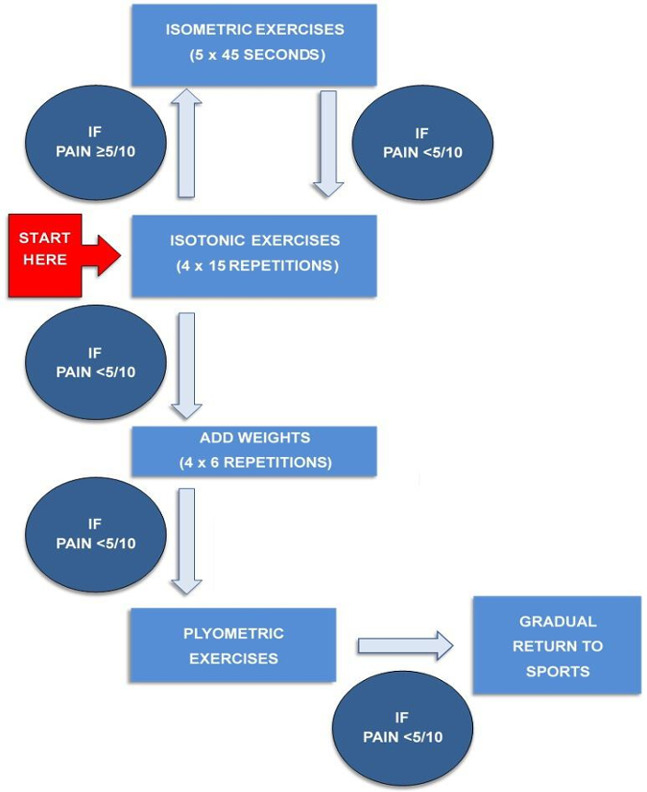
Proposed flow chart for designing the progressive calf muscle strengthening exercises (gastrocnemius and soleus muscles) and plyometric exercises. The degree of pain (measured by a Visual Analogue Scale or Numeric Rating Scale) during and after the exercises and the muscle fatigue are leading for the speed of the progression. Note that for insertional Achilles tendinopathy, exercises are initially advised on a flat surface.
Submodule 4.4: surgical treatment options
Is surgery more effective than non-surgical treatment for Achilles tendinopathy?
Introduction
Problem
In some patients with Achilles tendinopathy, non-surgical therapy is not successful and surgery is considered. The goal is to reduce symptoms, which can be done by excising fibrotic adhesions, excising degenerative noduli and/or making longitudinal incisions to induce a recovery response in the extracellular matrix.21 There is insufficient knowledge of how the results of surgical techniques compare with non-surgical treatment options. Understanding this is important in order to be able to make an informed decision to perform a surgical procedure. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion Achilles tendinopathy and insertional Achilles tendinopathy
Consider surgery only in patients who do not recover after at least six months of active treatment. See the recommendations of submodule 4.3 for the definition of active treatment. Discuss the expected effectiveness of surgical intervention compared with active non-surgical treatments and the potential surgical complications.
Submodule 4.5 factors that affect treatment effectiveness
Which factors influence treatment effects in Achilles tendinopathy?
Introduction
Problem
With the rise of so-called ‘big data’, personalisation of care is increasingly considered as the future for the treatment for many patients. This information can be obtained from, for example; electronic medical records, DNA profiles and eHealth apps. In the field of Achilles tendinopathy, there is insufficient knowledge about factors that influence the treatment effect or the natural course (prognosis). Knowledge of these factors could contribute to personalising treatment with possible improvements in clinical outcomes as a result. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion and insertional Achilles tendinopathy
Assess specific patient characteristics (such as activity level and the presence of comorbidities) to personalise treatment, but do not use this information to provide a prognosis. Together with the patient, the best treatment option can be decided.
Submodule 4.6: lifestyle advice, work and sports loading
What advice (self-management and patient education) should be given to patients with Achilles tendinopathy regarding lifestyle, work and sports loading?
Introduction
Problem
Patients with Achilles tendinopathy often report pain and not being able to exercise without pain. Patients, regularly ask about the nature and expected course of the condition and how they themselves can contribute positively or negatively to the recovery. The differing views of healthcare providers frequently causes confusion and uncertainty in patients. It is therefore important that healthcare providers have sufficient knowledge to give the correct instructions on lifestyle, work and sports loading to patients with Achilles tendinopathy. This can potentially contribute to improving self-efficacy and coping strategies which may have a positive contribution to treatment and recovery. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 4.
Recommendations
Midportion and insertional Achilles tendinopathy
The recommendations in submodule 4.3 are also aimed at lifestyle adjustments and loading during work and sports.
Discuss the initial active treatment options. Advise patients with work-related Achilles tendinopathy according to the same principles of patient education, load management advice and exercise therapy as a first step. Identify and temporarily adjust provocative factors related to the work.
Module 5 long-term prognosis of Achilles tendinopathy
Scoping question
What is the prognosis of individuals with Achilles tendinopathy in the long term?
This scoping question includes the following three subquestions
What percentage of patients with Achilles tendinopathy have persistent symptoms for more than 1 year?
What percentage of patients with Achilles tendinopathy return to their original level of sport over a period of more than 1 year?
What factors affect the long-term prognosis (longer than 1 year) in patients with Achilles tendinopathy?
Introduction
Problem
The treatment of Achilles tendinopathy is not always successful. Recovery can be slow and take months to years. There is insufficient knowledge about the exact prognosis. This applies both to the degree of symptoms and the possibility to return to a desired level of sports, without pain. Knowledge about the prognosis is important to provide realistic expectations for patients. Identifying prognostic factors can help to inform a more accurate prognosis for individual patients. In addition, this provides possible openings for optimising treatment. The literature search, selection, conclusions, considerations, and summary with tables and/or figures are presented in online supplemental file module 5.
bjsports-2020-103867supp007.pdf (435.3KB, pdf)
Recommendations
Midportion Achilles tendinopathy and insertional Achilles tendinopathy
Inform patients with Achilles tendinopathy about the following long-term consequences:
The majority of patients recover, but there is a chance that symptoms may persist in the long term (at least up to 10 years with 23-37% having persistent symptoms), despite treatment.
The majority of athletes with Achilles tendinopathy return to sports (85%). It is unknown whether this is at original (performance) level and whether this can be done completely asymptomatically.
Inform patients about the inability to provide a long-term prognosis, as prognostic factors for the long term have not been identified.
Module 6 preventing recurrence of Achilles tendinopathy
Scoping question
How can recurrent symptoms be prevented in patients who have recovered from Achilles tendinopathy?
The scoping question includes the following subquestion
Which prevention strategies are effective in patients who have recovered from Achilles tendinopathy?
Introduction
Problem
After recovery from Achilles tendinopathy it is important to prevent recurrence. As a previous lower limb tendinopathy is the risk factor with the strongest evidence for developing Achilles tendinopathy,22 there is a likelihood of recurring symptoms. There is insufficient knowledge about the effectiveness of prevention strategies aimed at recurrent Achilles tendinopathy. The literature search, selection, conclusions, considerations and summary with tables and/or figures are presented in online supplemental file module 6.
bjsports-2020-103867supp008.pdf (238KB, pdf)
Recommendations
Midportion and insertional Achilles tendinopathy
Discuss that sufficient time should be spent on active treatment before starting with provocative (sports) loading.
As a rule, a return to full symptom-free (sports) loading is only possible after a few months of active treatment at a minimum. A return to sports within days is associated with a greater likelihood of recurrence. Discuss the speed of return to sports with the patient and take the above-mentioned data into account.
Ensure a gradual build-up of the (sports) loading after recovery from Achilles tendinopathy or after a longer period of relative inactivity.
Consider continuing exercise therapy of the calf muscles after symptomatic recovery from Achilles tendinopathy.
Conclusion
Achilles tendinopathy is a common sporting injury that can result in reduced quality of life and is notorious for its long-lasting symptoms.23 The Dutch Association for Sports Medicine initiated this new multidisciplinary clinical guideline on Achilles tendinopathy. We followed the standard national comprehensive multidisciplinary guideline process. Using patient focus group interviews and a national online survey, we identified current barriers for patients with Achilles tendinopathy. The following domains were deemed important: primary prevention strategies, diagnosis, the role of imaging, effectiveness of non-surgical and surgical treatment options, the prognosis and prevention of a recurrence. Standardised scientific approaches were used, including a systematic search, selection of publication, data extraction, assessing risk of bias and appraising the certainty of evidence. This information was combined with other important considerations, including patient values and preferences, costs, acceptability of other stakeholders and feasibility of implementation.
Recommendations were made based on the results of the evidence from the literature and the considerations. All the national associations involved approved the guideline in October 2020.
This guideline provides recommendations on primary prevention, diagnosis, imaging, treatment and prevention of recurrence. It is essential for all involved (para)medical professionals who provide care for this patient group to be aware of knowledge in these different domains. By translating and sharing the guideline, our ultimate aim is to improve healthcare for patients with Achilles tendinopathy across the world.
What is already known.
Achilles tendinopathy is a common, persisting condition that impacts on sports participation and quality of life.
Many patients receive multiple treatments, resulting in high healthcare consumption.
There is inconclusive evidence on risk factors, prevention, diagnosis, imaging, treatment and prognosis for Achilles tendinopathy.
What are the new findings.
Each module contains recommendations for clinical practice—the most important are:
Diagnosis: establish the diagnosis ‘Achilles tendinopathy’ when the following four clinical diagnostic criteria are all present: localised symptoms, symptoms related to (sports) activity, localised thickening and presence of pain on palpation.
Treatment: consider including the following three aspects in basic management for at least 12 weeks: patient education, load management and calf muscle exercise therapy.
Treatment: consider additional therapies in cases of non-response to adequately performed basic management. Be cautious with using non-steroidal anti-inflammatory drugs and/or local corticosteroid injections. Consider surgery only if more than six months of basic management and additional therapies do not improve symptoms.
Acknowledgments
We would like to extend our gratitude to WM Bramer, research librarian at Erasmus MC Medical Library, for his help with developing a sensitive search strategy. The Netherlands Patient Federation assisted in sending, receiving and extracting surveys that were completed online by patients who suffered self-reported Achilles tendinopathy. We are grateful for their help and input in the design of the survey, thereby improving knowledge on important and relevant outcome domains for patients with Achilles tendinopathy. We thank M Winters, C Ardern, NJ Welton and DM Caldwell for their participation in the Treatment Module of this guideline.
Footnotes
Twitter: @rj_devos, @ArcoVlist, @HansZwerver, @ronaldvaningen, @astrid_balemans, @AdamWeirSports
Correction notice: This article has been corrected since it published Online First. The supplementary files have been updated.
Contributors: R-JdV initiated the project. R-JdV, ACvdV and MdO were involved in designing the project. ACvdV and R-JdV coordinated the project. ACvdV, AB, MP and NV provided support for the project by searching the literature, screening trials for inclusion, interpretation of the results of the data analyses and they checked whether the process followed the standards of the Dutch Federation of Medical Specialists. All members from the workgroup (R-JdV, JZ, DEM, FS, RvI, FvdG and EV) were responsible for screening trials, the risk of bias assessment, data extraction, interpretation of the results of the data-analyses and the formulation of the final recommendations. All workgroup members were responsible for one specific Module of Submodule of the guideline and drafted the first version of this Module of Submodule with assistance of R-JdV and ACvdV. AW drafted the translated version of the Dutch guideline into English. R-JdV is project guarantor. All authors reviewed the final guideline and agreed to be accountable for all aspects of the work and approved the final manuscript for submission. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This project received a grant from the Dutch Association of Medical Specialists to develop a clinical guideline for the management of patients with Achilles tendinopathy. The Netherlands Patient Federation is involved in this guideline development and assisted in sending out patient surveys. This non-commercial association is not involved in the planning, conduct or reporting of this project.
Competing interests: The personal financial interests, personal relationships, external research funding, intellectual property and other potential conflicts of all authors are described in the supplementary file.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Ethics statements
Patient consent for publication
Not required.
References
- 1.de Jonge S, van den Berg C, de Vos RJ, et al. Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med 2011;45:1026–8. 10.1136/bjsports-2011-090342 [DOI] [PubMed] [Google Scholar]
- 2.Kujala UM, Sarna S, Kaprio J. Cumulative incidence of achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med 2005;15:133–5. 10.1097/01.jsm.0000165347.55638.23 [DOI] [PubMed] [Google Scholar]
- 3.Maffulli N, Khan KM, Puddu G. Overuse tendon conditions: time to change a confusing terminology. Arthroscopy 1998;14:840–3. 10.1016/S0749-8063(98)70021-0 [DOI] [PubMed] [Google Scholar]
- 4.Scott A, Squier K, Alfredson H, et al. Icon 2019: international scientific tendinopathy symposium consensus: clinical terminology. Br J Sports Med 2020;54:260–2. 10.1136/bjsports-2019-100885 [DOI] [PubMed] [Google Scholar]
- 5.Soslowsky LJ, Fryhofer GW. Tendon homeostasis in hypercholesterolemia. Adv Exp Med Biol 2016;920:151–65. 10.1007/978-3-319-33943-6_14 [DOI] [PubMed] [Google Scholar]
- 6.Harman H, Tekeoğlu İbrahim, Tekeoglu I. Ankle pathologies in patients with inflammatory rheumatic diseases: a clinical and ultrasonographic study. Int J Rheum Dis 2017;20:675–84. 10.1111/1756-185X.13007 [DOI] [PubMed] [Google Scholar]
- 7.Bleakney RR, White LM. Imaging of the Achilles tendon. Foot Ankle Clin 2005;10:239–54. 10.1016/j.fcl.2005.01.006 [DOI] [PubMed] [Google Scholar]
- 8.Darlow B, Forster BB, O'Sullivan K, et al. It is time to stop causing harm with inappropriate imaging for low back pain. Br J Sports Med 2017;51:414–5. 10.1136/bjsports-2016-096741 [DOI] [PubMed] [Google Scholar]
- 9.van Linschoten R, den Hoed PT, de Jongh AC. [Guideline 'Chronic Achilles tendinopathy, in particular tendinosis, in sportsmen/sportswomen']. Ned Tijdschr Geneeskd 2007;151:2319–24. [PubMed] [Google Scholar]
- 10.Cook JL, Rio E, Purdam CR, et al. Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? Br J Sports Med 2016;50:1187–91. 10.1136/bjsports-2015-095422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Challoumas D, Kirwan PD, Borysov D, et al. Topical glyceryl trinitrate for the treatment of tendinopathies: a systematic review. Br J Sports Med 2019;53:251–62. 10.1136/bjsports-2018-099552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brukner P, Khan K. Chapter 40: Pain in the Achilles region. In: Brukner & Khan’s Clinical Sports Medicine. 5th edition. Sydney: McGraw-Hill, 2017: 865–92. [Google Scholar]
- 13.Fahlström M, Jonsson P, Lorentzon R, et al. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc 2003;11:327–33. 10.1007/s00167-003-0418-z [DOI] [PubMed] [Google Scholar]
- 14.van der Vlist AC, Winters M, Weir A, et al. Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. Br J Sports Med 2021;55:249–56. 10.1136/bjsports-2019-101872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vicenzino B, de Vos R-J, Alfredson H, et al. Icon 2019-International scientific tendinopathy symposium consensus: there are nine core health-related domains for tendinopathy (core domains): Delphi study of healthcare professionals and patients. Br J Sports Med 2020;54:444–51. 10.1136/bjsports-2019-100894 [DOI] [PubMed] [Google Scholar]
- 16.Robinson JM, Cook JL, Purdam C, et al. The VISA-A questionnaire: a valid and reliable index of the clinical severity of Achilles tendinopathy. Br J Sports Med 2001;35:335–41. 10.1136/bjsm.35.5.335 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sierevelt I, van Sterkenburg M, Tol H, et al. Dutch version of the Victorian Institute of sports Assessment-Achilles questionnaire for Achilles tendinopathy: reliability, validity and applicability to non-athletes. World J Orthop 2018;9:1–6. 10.5312/wjo.v9.i1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yasui Y, Tonogai I, Rosenbaum AJ, et al. The risk of Achilles tendon rupture in the patients with Achilles tendinopathy: healthcare database analysis in the United States. Biomed Res Int 2017;2017:1–4. 10.1155/2017/7021862 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kirwan P, March J, Duffy T. Screend’em before you treat’em. A clinical tool to help identify spondylarthropathy in patients with tendinopathy. Abstract at the International Scientific Tendinopathy Symposium, Groningen, the Netherlands, 2018. [Google Scholar]
- 20.van der Plas A, de Jonge S, de Vos RJ, et al. A 5-year follow-up study of Alfredson's heel-drop exercise programme in chronic midportion Achilles tendinopathy. Br J Sports Med 2012;46:214–8. 10.1136/bjsports-2011-090035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lohrer H, David S, Nauck T. Surgical treatment for achilles tendinopathy - a systematic review. BMC Musculoskelet Disord 2016;17:207. 10.1186/s12891-016-1061-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.van der Vlist AC, Breda SJ, Oei EHG, et al. Clinical risk factors for Achilles tendinopathy: a systematic review. Br J Sports Med 2019;53:1352–61. 10.1136/bjsports-2018-099991 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sleeswijk Visser TSO, van der Vlist AC, van Oosterom RF, et al. Impact of chronic Achilles tendinopathy on health-related quality of life, work performance, healthcare utilisation and costs. BMJ Open Sport Exerc Med 2021;7:e001023. 10.1136/bmjsem-2020-001023 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bjsports-2020-103867supp002.pdf (208KB, pdf)
bjsports-2020-103867supp001.pdf (169.4KB, pdf)
bjsports-2020-103867supp003.pdf (712.1KB, pdf)
bjsports-2020-103867supp004.pdf (389.8KB, pdf)
bjsports-2020-103867supp006.pdf (3.9MB, pdf)
bjsports-2020-103867supp005.pdf (534.8KB, pdf)
bjsports-2020-103867supp007.pdf (435.3KB, pdf)
bjsports-2020-103867supp008.pdf (238KB, pdf)