

Abstract
Background
Long hair follicular unit excision (FUE) is the most state‐of‐the‐art surgical technique in the field of hair transplantation surgery. Long hair FUE reduces the signs of surgery by camouflaging the recipient area with long hair, and allows hair curl identification when placing grafts. In addition, donor area shaving can be omitted.
Methods
This article presents the surgical approach and methods of long hair FUE. Patients were categorized by sex, age, recipient site, purpose of the surgery, and history of previous hair transplantation. Medical charts and photographs were reviewed to obtain the transection rate and calculated density for each patient.
Results
Long hair FUE was applied to 134 patients (112 women and 22 men). Thirty‐four patients received eyebrow hair transplantation, 73 underwent female hairline correction surgery, nine patients underwent sideburn reconstruction, two were treated for female pattern hair loss, and 19 were treated for male pattern baldness (MPB). Four of the patients with MPB also underwent eyebrow transplant surgery. Of the patients with MPB, 17 (89%) had Norwood type III baldness, and two (11%) had type IV hair loss. The mean number of grafts required was 292 for eyebrow transplantation, 1,214 for female hairline correction, 251 for sideburn reconstruction, 1,344 for female pattern hair loss, and 1,567 for MPB. The mean follicle transection rate was 9.2%, and the mean calculated number of follicles per graft achieved was 2.23.
Conclusion
This long hair FUE method introduced by the authors is an excellent surgical method when performed by surgeons with sufficient skill and expertise.
Introduction
Follicular unit transplantation (FUT) was developed in the 1990s, 1 and follicular unit excision (FUE) was first reported in 2002. 2 FUE has progressively gained in popularity owing to the absence of a linear scar and less postoperative pain than FUT. 3 However, shaving of the donor area for FUE was the biggest obstacle for patients because of social, occupational, and personal reasons; thus, the demand for non‐shaven FUE (NS‐FUE) began to increase. 4
In 2006, the concept of recipient area preview long hair transplantation was introduced. 5 The technique involves graft harvest by FUT and transplantation of the donor hair while maintaining its natural length. Surgical results expected at more than 1 year postoperatively are visualized immediately after surgery, which makes it less obvious that the patient has undergone surgery.
Long hair FUE was introduced in 2016 6 and has the advantage of donor area preview. With no need for donor area shaving, long hair FUE allows the surgeon to control the donor area density to prevent overharvesting.
The direct NS‐FUE procedure was first introduced in 2014. 7 NS‐FUE is classified as a pre‐trimming (PT) method, direct method (DM), and long hair FUE. 4 , 8 The PT method is a two‐step technique in which the target follicles in the donor area are trimmed to a length of about 1 mm and later located for excision. In contrast, the DM is a one‐step method in which hair is cut by a punch tip during graft dissection. In addition to the recipient and donor area previews provided by NS‐FUE, this procedure enables the surgeon to identify hair curl upon graft placement.
Long hair FUE overcomes the shortcomings of FUT including linear donor scars and severe postoperative pain, reduces the signs of surgery by camouflaging the recipient area with long hair, and allows hair curl identification when placing grafts. Indications for long hair FUE include hair transplant surgeries in areas requiring meticulous hair curl matching, such as the eyebrows and hairline (including temporal and sideburn area reconstruction), and when patients desire the surgery to be unnoticeable immediately postoperatively. This article presents the surgical approach and methods of long hair FUE.
Materials and methods
Overall, 134 patients underwent long hair FUE from January 2016 to December 2019. Those that received a combination of FUE and FUT or minor touch‐up procedures complementary to the primary surgery were excluded from the present study. Patients were categorized by sex, age, recipient site, purpose of the surgery, and history of previous hair transplantation. Medical charts and photographs were reviewed to obtain the transection rate and calculated density for each patient.
Surgical planning
Each surgery was meticulously planned through preoperative consultation with the patient, considering factors such as previous surgical history, donor and recipient area status, patient expectations and wants, hair characteristics such as curl and caliber, hairstyle, and occupation. The surgical design was confirmed while the patient was looking into a mirror and was marked with a surgical pen.
Patient positioning
Punching and extraction were performed with the patient in a sitting position. Graft placement was carried out with the patient in a supine position. The forehead of the patient rested on a forehead support system known as the graFUEt™ (Seson Medical Company, Seoul, Korea), which is easily controlled by a foot pedal or remote control system to adjust the position of the patient's head (Fig. 1).
Figure 1.
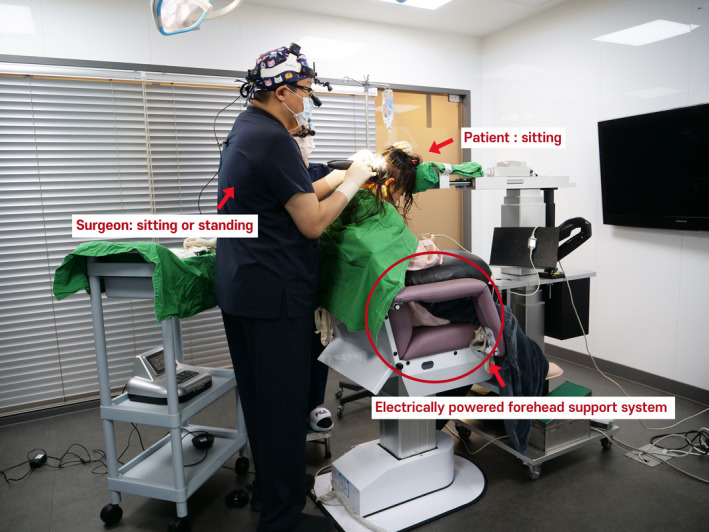
Forehead support system for non‐shaven follicular unit excision. A patient resting on an electrically powered forehead support. A foot pedal (not shown) is used by the surgeon to move the support in the horizontal and vertical planes
Anesthesia
The donor area was prepared with a ring block of local anesthesia (1 : 100,000 epinephrine mixed with lidocaine) along the inferior margin. A tumescent solution composed of 100 ml normal saline, 10 ml 2% lidocaine, and 0.3 ml epinephrine was intradermally injected into the punching site. Tumescent solution was intermittently injected intradermally to ensure that the skin remained firm and turgid. The recipient site was injected with 1 : 50,000 epinephrine mixed with lidocaine. Abbasi solution was used for tumescence (100 ml normal saline, 8 ml 2% lidocaine, 1 ml epinephrine, and 1 ml triamcinolone). 7
Long hair FUE procedure
Punching
We used a motorized FUE machine with a 0.85–0.9 mm open window punch (graMAX™, Seson Medical Company). A 5.5× magnifying loupe was used intraoperatively.
Punching in male patients
The surgeon held microteeth forceps in the left hand and the punching handpiece in the right hand. The patient's hair was swept up with the forceps in the left hand while the hair follicles were dissected with the handpiece in the right hand (Fig. 2).
Figure 2.

Long hair follicular unit excision procedure. The forceps are held in the left hand while the punch handpiece is held in the right hand. The hair is swept up with the left hand, and the grafts are excised with the right hand
The procedure involved two assistants, with one assistant standing on each side of the surgical chair. When the surgeon worked on the right side, the assistant standing on the right of the patient swept the hair up while applying upward scalp traction to increase both the skin firmness and hair exit angle. When the surgeon finished punching one zone on the right, the assistant on the right started extracting the punched grafts. The surgeon then moved to the left to perform punching, and the assistant on the left side performed upward traction and hair sweeping. Overlapping the processes of punching and scored graft extraction helped minimize the operation time. The harvesting process was carried out repeatedly on alternate sides (Fig. 3).
Figure 3.

Teamwork for long hair follicular unit excision. The assistant standing on the same side as the surgeon sweeps up the hair and simultaneously applies upward traction while the assistant on the opposite side extracts the excised hair follicles
Punching in female patients with long hair
In patients with long hair, only 0.7–1.0‐cm sections of the scalp were exposed using multiple hair clips (Fig. 4). To obtain a better visual field and minimize hindrance caused by the long hair and bleeding, punch insertion was performed within the 0.7–1.0‐cm long zone exposed at the proximal end of hairs fixed with the lowermost clip. Grafts were scored from the bottom, and the clips were unclipped one at a time. The assistant standing on the same side as the surgeon moved the hair aside using a narrow sterile stick and applied upward traction. The open window slot was preferably situated at the 10 o'clock position. Approaching from the right side of the graft maximized the surgeon's view of the target graft until the actual punch insertion (for a right‐handed surgeon) while approaching from the left side of the graft would have temporarily blocked the surgeon's view of the target graft. The 10 o'clock direction was preferred over the 9 o'clock direction because the direction of progress in harvesting was toward the left and upwards (Fig. 5).
Figure 4.

Multiple clips used to expose the scalp of a female patient with long hair. To minimize hindrance to the surgeon and the tangling of long hairs, punch insertion is performed within the exposed working zone
Figure 5.
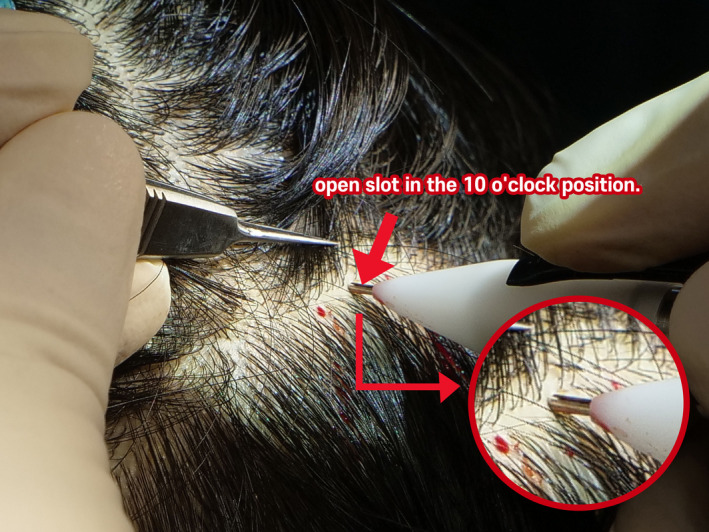
Location of the open slot of the open window punch. It is advantageous for a right‐handed surgeon to place the slot in the 10 o'clock position
The oscillation movement was started with the target hair close to the slot or even completely encased in the tip, which helped to neatly dissect the grafts and allow long hair to readily move in through the slot.
Extraction
After punching, the aid to extraction forceps were used for extraction (Fig. 6). To minimize the operation time, two assistants alternately performed the hair sweeping and upward traction and the extraction of scored grafts using 5× magnifying surgical loupes.
Figure 6.

Graft extraction using the aid to extraction forceps
Graft inspection
All harvested grafts were inspected under a high‐powered microscope. Partially transected grafts were trimmed. Grafts were divided into one‐, two‐, and three‐hair follicular units (Fig. 7). One‐hair follicular units were then further divided into thin, thick, and very thick one‐hair grafts. The entire process of dividing grafts by caliber was carefully done under the microscope. One hundred extracted follicular units were randomly selected and examined under a microscope.
Figure 7.
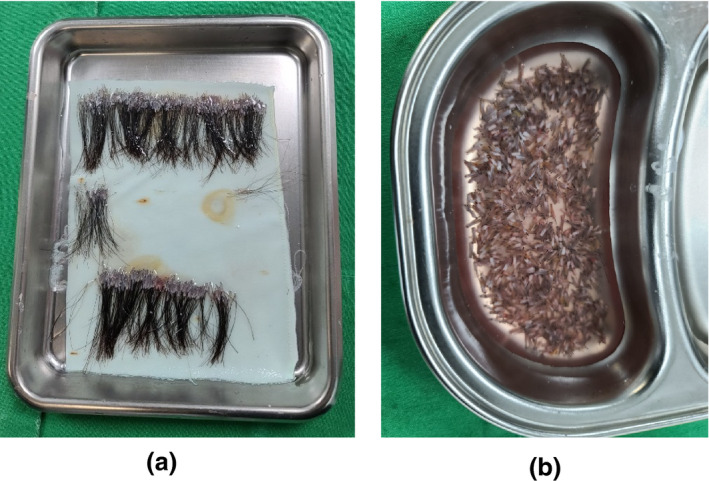
Extracted long hair follicular unit excision grafts. (a) Long hair grafts extracted by the long hair follicular unit excision technique. (b) Conventional follicular unit excision grafts with short hair
Graft insertion
Graft insertion was mostly performed with the patient in a supine position. A sharp implanter was used for transplantation. To minimize the out‐of‐body time, the concept of “first out, first in” was applied so that harvested grafts were inserted sequentially in order of harvesting. Two or three assistants loaded implanters while another assistant stood immediately next to the operator to circulate the implanters.
Grafts were loaded into the implanters with the curl bending away from the bevel tip and toward the bevel face. The surgeon wears highly magnified loupes and does not need to check the curl every time; the curl can be perceived just by checking where the bevel is facing.
Results
Long hair FUE was applied to 134 patients (112 women and 22 men). Thirty‐four patients received eyebrow hair transplantation, 73 underwent female hairline correction surgery, nine patients underwent sideburn reconstruction, two were treated for female pattern hair loss, and 19 were treated for male pattern baldness (MPB). Four of the patients with MPB also underwent eyebrow transplant surgery. Of the patients with MPB, 17 (89%) had Norwood type III baldness, and two (11%) had type IV hair loss.
The mean age of the patients in the overall study cohort was 36.5 years (range: 20–73 years). There was a large difference in age by type of surgery. The mean age was 36.9 years (range: 25–68 years) for patients who underwent eyebrow surgery, 32.3 years (range: 24–43 years) for patients who received female hairline correction surgery, 33.7 years (range: 24–36 years) for patients who underwent sideburn reconstruction, 40.0 years (range: 20–60 years) for patients treated for female pattern hair loss, and 39.8 years (range: 32–61 years) for patients treated for MPB.
One complete long hair FUE cycle took approximately 3–4 hours. The process of punching and extraction lasted about 2 hours, while graft implantation took about 1–2 hours. About 600–1,200 grafts (mean 800 grafts) were punched in 1 hour. A patient requiring about 1,500 grafts would require about 2–3 hours of punching and extraction. Considering the preparation time required for patient positioning and various surgical equipment and devices as well as the 2 hours of implantation, the total surgery time was approximately 5 hours. The maximum number of grafts implanted by long hair FUE was about 2,500 per day.
The mean follicle transection rate was 9.2%, and the mean calculated follicles per graft achieved was 2.23.
The mean number of grafts required was 292 for eyebrow transplantation, 1,214 for female hairline correction, 251 for sideburn reconstruction, 1,344 for female pattern hair loss, and 1,567 for MPB.
Case presentations
A 39‐year‐old woman with a high forehead and M‐shaped frontotemporal recess areas received female hairline correction surgery with 1,533 grafts transplanted by long hair FUE (Fig. 8).
Figure 8.

Female hairline correction surgery by long hair follicular unit excision. (a) Preoperative view. (b) Preoperative design. (c) Immediate postoperative view. (d) Twelve days postoperatively. (e) Two months postoperatively. Transplanted hairs undergoing partial shedding. (f) Eight months postoperatively
Discussion
The three main NS‐FUE methods are PT, DM, and long hair FUE. 4 , 8 In the PT method, the target grafts are cut to a length of 1 mm prior to surgery, and the trimmed grafts are then located for graft dissection. In the DM method, a rotating or oscillating punch tip cuts the hair shaft and dissects around the hair follicle at the same time. Using the PT method, the hair strand length can be controlled to some degree during preoperative cutting. However, when the target graft has a hair shaft longer than 3 mm, it is difficult for the surgeon to insert all the strands of multifollicular units into the punch tip. Grafts harvested by the DM method have shorter hair shafts (approximately 0.3–0.5 mm) than those harvested by the PT method. The authors usually combine the PT method and the DM to minimize the operation time.
Long hair FUE does not require preoperative trimming. Long hair FUE grafts are harvested at the natural length and are later cut as needed. For eyebrow reconstruction, hair shafts are cut to lengths of around 10 mm. For other types of hair transplantation, the grafts are about 30–40 mm long.
Advantages and disadvantages of long hair FUE
The main advantage of long hair FUE is the immediate visualization of the probable result at 1 year postoperatively. In addition, the recipient area looks natural and is camouflaged by long hair, making the surgery inconspicuous; that is, a recipient area preview is plausible. 8 The second advantage of long hair FUE is the concept of donor area preview. 5 However, the authors consider such a concept to be limited to extreme cases with donor area depletion due to several previous hair transplant sessions. The surgeon can generally predict and control the degree of donor area depletion while proceeding with graft punching. The third advantage of long hair FUE is the concept of previewing hair curl. This has great clinical importance in hair transplantation in the eyebrows, sideburns, and the temples, where it is critical that the hair curls are matched. Fourth, the advantages of NS‐FUE include less postoperative pain, no linear donor scar, and no need for donor area shaving. Lastly, even during the resting period of hair follicles after the shedding of transplanted hairs, the hairs that were not shed help create a natural appearance in the recipient area.
The disadvantages of the long hair FUE method include the prolonged operation time, necessity for more surgical staff (graft harvesting and preparation for long hair FUE require more manpower and time than for other FUE methods), prolonged learning curve, and requirement for a higher degree of expertise.
Shaving methods
Various methods are used to shave the donor area. A buzz cut refers to shaving the entire head. A marine cut or crew cut refers to leaving the hairs on top of the head about 6–9 mm long but shaving the donor area to about 1 mm long. For an undercut, only the donor area is shaved. In the partial shaving method, the donor area is shaved in a box form and covered with the uncut, long hair from above the donor area. The line‐cut or microstrip shaving method may leave multiple linear strip scars; therefore, the authors recommend avoiding this method for patients requiring more than 600–800 grafts.
The non‐shaving method is an excellent harvesting method that spaces out the FUE scars in random and homogeneous patterns. There is no donor shaving, but the short hair shafts in the recipient area make the surgery quite noticeable and make it difficult to identify hair curl. In addition, NS‐FUE has a long learning curve.
Long hair FUE is an upgraded version of NS‐FUE that overcomes the disadvantages of the short hair strands in NS‐FUE grafts.
Devices and equipment
The key point of long hair FUE is the harvest of intact hair follicles without cutting the hair shaft and the prevention of the hair shaft from wrapping around the punch tip. This procedure requires a specialized device that differs from the device used in standard FUE. A slot in the form of an open window is created at the edge of the punch tip (Fig. 9). The hair shaft enters this slot and is harvested uncut without altering its length. Long hair FUE necessitates more than a punch tip with a slot. The oscillation arcs must be less than approximately 270° to prevent the hair strands from wrapping around the punch tip, and the open slot must return to the original starting location with every punch to help enclose hair strands in the tip lumen. The speed of the oscillation may differ by the type of the scalp and the surgeon's preference. In general, it is set at a slightly low to moderate speed but changes by case.
Figure 9.

Open window punch for long hair follicular unit excision
A small slot is made at the edge of the punch tip, which may be long or short, single or multiple, sharp or blunt, or partially sharp and partially blunt (Fig. 10).
Figure 10.
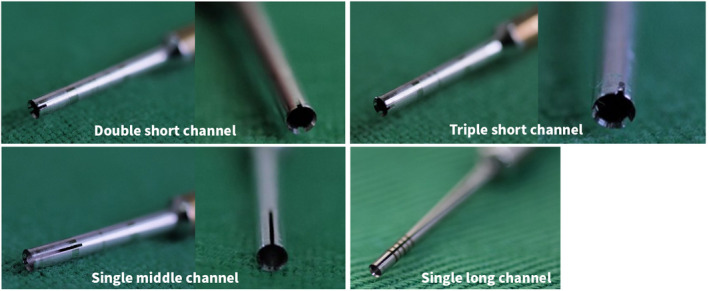
Variations of the open window punch
Patient positioning
A sitting position is preferred to a prone position for long hair FUE harvesting. However, the patient's and surgeon's positions largely depend on the surgeon's preference, surgical system, and experience. The biggest obstacle in long hair FUE is the presence of long hair in the donor area. The long hair strands also make the process of graft extraction extremely difficult. With the patient in a prone position, the blood oozing from the punched sites forms blood clots that cause the long hair to tangle and stick together. However, unlike the sitting position, operating with the patient in a prone position does not let blood trickle downward, thus maintaining a clear visual field. To overcome this problem, grafts can be deeply dissected to allow punching and immediate extraction with forceps. However, such a deeper punch depth may lead to increased follicular injury.
Ergonomics
Because of the long operation time required for long hair FUE, the ergonomics of the patient and the surgeon must be considered. 9 The prone position can be challenging for patients with extreme central obesity or with back or neck troubles. Fixation of the forehead is also crucial in maintaining a seated posture for a long period. Forehead fixation has even more clinical importance when working at very acute angles, especially when harvesting from below the occipital protuberance or from the temporal areas of the donor site. It is easier to insert the punch tip at acute angles when the patient's neck is flexed. However, it is impossible for the patient to maintain such a posture for a long period without forehead fixation. The graFUEt system, the FUE apparatus that is currently used by the authors, is very conveniently controlled with a remote control as well as a foot pedal, enabling the forehead fixture to be moved up, down, forward, and backward, and the chair to be moved up and down (Fig. 11). 10
Figure 11.

Motorized forehead supporting follicular unit excision chair system
Tumescent injection
Adequate application of a tumescent solution mixed with epinephrine is very important. 11 The tumescent injection reduces intraoperative bleeding, changes the hair exit angle from an acute to a more vertical angle, and hardens the scalp. The tumescent solution must infiltrate the intradermal layer to tense the scalp tissue. However, the tense turgor of the scalp tissue only lasts 5–10 minutes. Therefore, it is best to administer the tumescent solution frequently and to only cover a small surface area.
Hair sweeping and upward traction
Application of upward traction as the assistant sweeps up the hair greatly aids the surgeon during long hair FUE (Fig. 12), as this maneuver helps remove the hair that is visually blocking the surgical field. Furthermore, upward traction reduces the gap between the hair exit angle and the internal angle and makes the punch insertion angle more vertical. 12 , 13 Acute punching angles leave wounds with a larger surface area and cause more follicular injuries. 14 Upward traction also tenses the skin by tightening the scalp tissue, allowing a more stable punch insertion.
Figure 12.

Hair sweeping and upward traction. The assistant sweeps up the long hair falling from above the working area to acquire a clear surgical view while applying upward traction
Extraction
In long hair FUE, the final surgical results are greatly influenced by the punching process as well as a safe and swift graft extraction. With the patient in a sitting position, aid to extraction forceps are more useful than jeweler's forceps for long hair FUE. Maximally overlapping the processes of punching and extraction minimizes the overall operation time. It is also beneficial to proceed from the bottom and work upwards. Highly skilled assistants are required for long hair FUE, especially when treating female patients with very long hair.
Conclusion
The primary objective of hair transplantation is to safely transfer hair follicles from the donor area to the recipient area without side effects to obtain a natural‐looking result and restore hair volume. Patients' expectations are continually increasing, and the field is technologically advancing rapidly. This long hair FUE method introduced by the authors is an excellent surgical method that meets such needs when performed by surgeons with sufficient skill and expertise.
Acknowledgments
We thank Kelly Zammit, BVSc, and J. Ludovic Croxford, PhD, from Edanz Group (https://en‐author‐services.edanz.com/ac) for editing a draft of this manuscript.
Conflict of interest: J. H. Park has patents and ownership interest of Seson Medical Company. For the remaining authors, none were declared.
Funding source: None.
References
- 1. Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. Dermatol Surg Oncol 1994; 20: 789–793. [DOI] [PubMed] [Google Scholar]
- 2. Rassman WR, Bernstein RM. Follicular unit extraction: minimally invasive surgery for hair transplantation. Dermatol Surg 2002; 28: 720–727. [DOI] [PubMed] [Google Scholar]
- 3. Kim YS, Na YC, Park JH. Comparison of postoperative pain according to the harvesting method used in hair restorative surgery. Arch Plast Surg 2019; 46: 241–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Park JH, You SH, Kim NR. Nonshaven follicular unit extraction: personal experience. Ann Plast Surg 2019; 82: 262–268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Pitchon M. Preview long‐hair follicular unit transplantation: an immediate temporary vision of the best possible final result. Hair Transpl Forum Int 2006; 16: 113–119. [Google Scholar]
- 6. Boaventura O. Long hair FUE and the donor area preview. Hair Transpl Forum Int 2016; 26: 200–202. [Google Scholar]
- 7. Park JH. Direct non‐shaven FUE technique. Hair Transpl Forum Int 2014; 24: 103–104. [Google Scholar]
- 8. Park JH, You SH. Pre‐trimmed versus direct non‐shaven follicular unit extraction. Plast Reconstr Surg Glob Open 2017; 5: e1261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Williams KL Jr, Gupta AK, Schultz H. Ergonomics in hair restoration surgeons. J Cosmet Dermatol 2016; 15: 66–71. [DOI] [PubMed] [Google Scholar]
- 10. Park JH, You SH, Kim N. Forehead‐supporting chair system for follicular unit extraction hair transplantation. Arch Aesthetic Plast Surg 2019; 25: 42–44. [Google Scholar]
- 11. Ahmad M. Follicular unit extraction: technique to aid graft extraction—how I do it? Am J Cosmet Surg 2017; 34: 173–174. [Google Scholar]
- 12. Rose PT, Canales M, Zontos M. Examination of the exit angle of hair at the skin surface versus the internal angle of hair as it relates to the FUE/FIT harvesting method. Hair Transpl Forum Int 2017; 27: 8–10. [Google Scholar]
- 13. Zontos G, Williams KL Jr, Nikiforidis G. Minimizing injury to the donor area in follicular unit extraction (FUE) harvesting. J Cosmet Dermatol 2017; 16: 61–69. [DOI] [PubMed] [Google Scholar]
- 14. Zontos G, Rose PT, Nikiforidis G. A mathematical proof of how the outgrowth angle of hair follicles influences the injury to the donor area in FUE harvesting. Dermatol Surg 2014; 40: 1147–1150. [DOI] [PubMed] [Google Scholar]