

Abstract
Objective:
Failing to account for temporal dynamics can hinder our understanding of suicidal ideation and the potential mechanisms underlying increased risk for suicide death and suicide attempts associated with posttraumatic stress disorder (PTSD). To address these limitations, this study used an analytic approach based on Dynamical Systems Theory to describe temporal patterns associated with multiple dimensions of suicidal ideation in a treatment-seeking sample of military personnel diagnosed with PTSD.
Method:
We performed a secondary analysis of archived data from 742 active duty military personnel (90% male, 57% white, mean age = 33 ± 7.4 years) enrolled in three clinical trials to examine the dimensional measurement properties of the first 5 items of the Scale for Suicidal Ideation (SSI).
Results:
Findings indicated two change dynamics for suicidal ideation: homeostatic (i.e., the tendency for suicidal ideation to return to a stable point) and cyclical (i.e., the tendency for suicidal ideation to switch back and forth between higher and lower values). Cycling was the dominant dynamic, and was related to variables other from suicidal ideation.
Conclusion:
The cyclic nature of suicidal ideation suggests that assessment timing and context could influence observed associations with other variables. Analytic approaches and clinical methods that do not account for the temporal dynamics of suicide risk could miss these properties, thereby hindering efforts to identify mechanisms underlying the relationship between PTSD and suicidal thoughts and behaviors, and limiting opportunities for proactive and timely intervention.
Clinical Impact Statement:
Suicidal ideation is multidimensional, with each dimension following different time courses. Cycling of suicidal ideation is pronounced among military personnel receiving treatment for PTSD. Recognizing these patterns could improve assessment and treatment by identifying critical periods of time during treatment that warrant suicide-focused interventions.
Keywords: Dynamical Systems Theory, Posttraumatic Stress Disorder, Suicide, Military
The fluid vulnerability theory (FVT) of suicide (Bryan & Rudd, 2016; Rudd, 2006) conceptualizes suicide as a phenomenon that results from complex interactions among multiple risk and protective factors. Owing to these interactions, suicide risk is an ever-changing construct, a characteristic that has been recognized for decades (e.g., Maris, 1972; Schiepek et al., 2011) but only recently been examined using data collection and analysis methods sufficient to describe this property. These studies underscore how meaningful, dynamic fluctuations in suicidal ideation occur within several days or in some cases a few hours (Bryan et al., 2019; Bryan & Rudd, 2018; Kleiman et al., 2017). Measurement methods that fail to account for these change processes could lead to mixed or apparently contradictory results about how PTSD and suicide risk are related.
Of the numerous assessment scales developed to measure various aspects of suicide ideation (Brown, 2001), the Scale for Suicidal Ideation (SSI; Beck et al, 1979) has been used extensively by clinical researchers and is recommended as the PhenX Toolkit measure (www.phenxtoolkit.org). The scale has 19 items that each use a 3-point ordinal response scale to assess suicide-related thoughts, attitudes, and behaviors during the preceding week (Beck et al., 1979). The SSI is designed such that the first five items are administered to all respondents as a screening tool (Beck & Steer, 1991) and the remaining 14 items are administered only if a respondent positively endorses either item 4 (active suicide ideation) or item 5 (passive suicide ideation). The SSI’s internal consistency, interrater reliability, and construct validity are supported (Beck et al., 1979; Beck et al., 1988). Although the SSI is typically scored and used as a unidimensional measure of suicidal ideation, factor analyses have yielded inconsistent results (Beck et al., 1979; Holden et al., 1985), suggesting suicidal ideation may be better understood as a multidimensional construct. Insufficient attention to the temporal dynamics associated with multiple dimensions or facets of suicidal ideation may contribute to these mixed findings. SSI items may therefore reflect distinct aspects of suicidal thinking that change in unique ways; some aspects of suicidal ideation may, for example, fluctuate faster than others. If true, intercorrelations among multiple items could vary depending on when the scale is completed.
To our knowledge, no studies have examined how these temporal processes might influence the assessment and measurement of suicidal ideation. Research focused on identifying and describing temporal patterns in item responses could provide clues about how to optimally use and/or interpret suicide risk assessment tools within clinical practice, advance the measurement of suicidal ideation (and potentially other constructs), and improve our conceptual understanding of suicidal thoughts and behaviors. Dynamical Systems Theory (DST) , a branch of mathematics that focuses on understanding and describing change processes through the examination of multiple levels of change (Butner et al., 2015), provides a conceptual approach that is well-suited to these objectives. Recent conceptual work informed by DST suggests that simultaneously thinking about the measurement of a particular construct’s value and the measurement of change in the construct’s value over repeated measurements can provide unique insight into how an assessment scale functions through time (Estabrook, 2015; Butner et al., 2014) and, by extension, how its measured construct behaves over time.
If the measurement of suicidal ideation over time is conceptualized in this manner, we need to think of SSI item responses with respect to their values at a given point in time (also referred to as position, or the zeroth derivative), the change in values from one time point to the next (commonly referred to as velocity, or the first derivative), and the change in each item’s change values (commonly referred to as acceleration, or the second derivative). A useful example to illustrate these three levels is to think of driving a car between work and home. If we wanted to estimate when a person might arrive at one location or the other, it would be useful to know where on the route a person resides (position), how fast they are going and their direction of travel (velocity), and if they are speeding up or slowing down (acceleration). Together these can provide invaluable information as to know when to arrive or if you are going to be late stuck in traffic. Because each item of the SSI is assumed to measure a separate facet of suicide risk, it is possible for each item to have distinct values, velocities, and accelerations for each respondent at each point in time, just as a group of individuals commuting from one location to another can follow different roads, drive at different speeds, and speed up or slow down at different times and to different degrees.
It is possible that all of the positions, velocities, and accelerations are the same for all of the SSI items, just as the positions, velocities, and accelerations of multiple individuals would be the same if they were commuting together in a single vehicle. If this condition were true, this would imply the SSI’s many items truly do measure a single underlying construct that changes within individuals and across individuals in a fixed and/or uniform way, meaning that the conventional approach to summing all item values as an aggregate indicator of suicidal ideation would be appropriate for monitoring suicide risk within individual patients over time as well as monitoring suicide risk across many patients (Molenaar, 2004). Clinically, this would be ideal because it provides a simple and straightforward method for assessing and monitoring suicide risk. In reality, this ideal condition is improbable, implicating the need for alternative approaches that more accurately reflect the ever-changing nature of suicide risk. Such approaches could improve suicide risk screening, assessment, and monitoring during the course of treatment.
Research aimed at understanding and describing the temporal dynamics of suicide risk could provide novel insights relevant to the well-established link among PTSD, suicidal ideation, and suicidal behaviors (Gradus et al., 2010; May & Klonsky, 2016). Unlike many other psychological and behavioral disorders, PTSD is associated with increased risk for suicidal behaviors among individuals with suicidal ideation (May & Klonsky, 2016), suggesting the condition is characterized by properties or features that facilitate the transition from ideation to action. Although the mechanisms underlying increased risk for suicidal thoughts and behaviors among individuals with PTSD remain unknown, recent theoretical and empirical work (Bryan et al., 2020) suggest certain temporal patterns in suicidal ideation, especially those characterized by rapid and/or large fluctuations in ideation, are associated with increased risk for suicidal behaviors (Bryan et al., 2019; Bryan & Rudd, 2016). These preliminary studies considered suicidal ideation as a unidimensional construct, however, and were not conducted in clinical settings that allowed for the examination of temporal processes within specific patient subgroups (e.g., those with particular diagnoses).
In the present study, we address these knowledge gaps by analyzing data from three separate longitudinal clinical trials (Foa et al., 2018; Resick et al., 2015, 2017) that repeatedly administered the SSI to patients during and after treatment. The SSI is especially well-suited for these analyses because the scale measures multiple components of suicidal ideation. Our primary aim was to describe temporal change processes in suicidal ideation among treatment-seeking adults diagnosed with PTSD. In contrast to previous research, we examined change patterns associated with each SSI item separately, consistent with our conceptualization of suicidal ideation as a multidimensional (versus unidimensional) construct.
Methods
Participants and Procedures
Participants were 742 treatment-seeking active duty U.S. military personnel who had deployed to Iraq or Afghanistan, were at least 18 years of age, and met full diagnostic criteria for PTSD according to the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994) as assessed using the PTSD Symptom Scale Interview (PSS-I; Foa et al., 1993). Participants meeting these criteria provided consent to participate in clinical research. This military sample was primarily male (89.8%), Caucasian (56.5%) or African American (25.2%) race, non-Hispanic ethnicity (79.8%), E4 – E6 grade (noncommissioned officer; 79.8%), active duty component (98.5%), and Army branch of service (99.6%). Average age was 33 (SD = 7.42 years) with average service of 131 months (SD = 76.19 months) and two deployments during time in service (SD = 1.06 deployments). The severity of PTSD symptoms assessed by the PCL-5 averaged 41 (SD = 17). A full listing of sample demographics can be found in the Supplementary Materials. A previous examination of this sample evaluated the frequency of trauma types reported in the cohort of service members seeking treatment for PTSD (Litz et al., 2018). The results indicated the following trauma types: Life Threat to Self (41%), Life Threat to Others (14%), Aftermath of Violence (20%), Traumatic Loss (9%), Moral injury by Self (7%), and moral injury by Others (9%). Demographic characteristics did not differ across the three studies. This study was approved by the University of Utah Institutional Review Board.
The present study entailed secondary data analyses of archived de-identified data from the STRONG STAR Consortium Data Repository. Data were compiled from three separate randomized clinical trials testing the comparative effectiveness of various outpatient psychotherapies for reducing PTSD symptoms among U.S. military personnel (clinicaltrials.gov identifiers: NCT02173561, NCT01286415, and NCT01049516). Details about the procedures used for each study can be found elsewhere (Foa et al., 2018; Resick et al., 2015, 2017). Relevant to the present study, participants in these trials were repeatedly administered the SSI up to 16 times total (the assessment schedule for each study can be found in the Supplementary Materials).
Measure
The SSI (Beck et al., 1988) is a 19-item, self-report measure that assesses the intensity of suicide-related thoughts, urges, and behaviors during the preceding week using a 3-point ordinal scale, with higher scores indicating more severe suicide risk. The first 5 items assess the wish to die, wish to live, relative balance of wish to die to wish to live, active suicide ideation, and passive suicide ideation, and were administered to all participants at all time points. Because the scale’s remaining 14 items were only completed by the subset of patients endorsing active or passive suicidal ideation (Beck & Steer, 1991), we restricted our analyses to the first 5 items.
Data Analyses
For all calculations and analyses, we collapsed data sources across all three studies. Data were first transformed into estimates of the three levels of derivatives (zeroth, first, and second) for each of the five SSI items using Deboeck’s (2020) Empirical Bayesian derivative procedure in R. We used a window size of four measures and the number of days between each measurement as the indicator of time, thereby accounting for differing lengths of time between repeated measurements. Data were then randomized into equal halves with analyses applied to both datasets separately.
We captured measurement and dynamics at the same time by calculating derivative-based equations and then examining the eigenvalues of the coefficients from these equations (Butner et al., 2017). In this case, we calculated the first derivative for the first SSI item at each assessment point and used the first derivative values as our criterion. This process can be repeated for multiple items within a scale. In the present study, we used the first five SSI items because these items are administered to all patients or research participants, whereas items 6–19 are administered only if a respondent endorses a non-zero value on either item 4 or item 5. Full data were therefore available for the first 5 items only. We generated five separate equations, one for each item, wherein item values (i.e., zeroth derivatives) at each point in time are used as the predictors of item velocities (i.e., first derivatives) at the next point in time. When the relationship between an item’s value and its velocity are negative in value, a homeostatic relationship is implied, which means that when an item value at a given time point is lower than the homeostatic point, we would expect the item’s value to increase at the following time point, whereas when an item value at a given time point is higher than the homeostatic point, we would expect the item’s value to decrease at the following time point.
An item’s value can also be used to predict a different item’s velocity. The statistical association between items forms a relationship commonly called coupling. Coupling terms capture the unique push/pull relationships that exist among multiple items, thereby providing information about how one dimension of suicidal ideation might be temporally related to another dimension of suicidal ideation. It is possible that all items function identically through time; alternatively, it is possible that some (but not necessarily all) items function differently. In the case where all five items function identically through time, which would support the perspective that suicidal ideation is unidimensional, collinearity among the various coefficients must be considered. To account for this possibility, we examined the eigenvalues of the set of all coefficients, with non-zero eigenvalues indicating unique dimensions.
This eigenvalue procedure is similar to the first step of an exploratory factor analysis, albeit with the primary difference that eigenvalues can be complex numbers, with the imaginary portion of the eigenvalue implying a cyclical change pattern. A cycle is a circumstance where item values form steady, pattern-like fluctuations between higher and lower values that occur irrespective of natural fluctuations. In cycles, the association between an item’s value and its velocity cancel each other out over time, but a consistent negative association between an item’s value and its acceleration (i.e., second derivative). The cycle is a noteworthy change pattern because it implies that an item’s value changes as a function of two competing or countering forces (Abraham & Shaw, 2005; Huckfeldt et al., 1982) that may be related to other dimensions of suicidal ideation or some other variable(s). To account for this possibility, we also tested associations among item values and accelerations as well consistent with published recommendations (Butner et al., 2017). Although the relationship between acceleration and velocity has some redundancies with the relationship between velocity and value, this issue is resolved by the eigenvalue procedure. Finally, the absolute values of the complex numbers derived from the eigenvalue procedure were used to determine the dominant dynamics across the 5 items—homeostatic or cyclical.
To account for data dependency, we used multilevel models in R using the lme4 package (Bates et al., 2015) with the inclusion of a random intercept, which allows us to assume that the coupling terms account for any remaining dependency across equations. Finally, because our expectation of cycles was drawn from preliminary data inspections described below, we split the dataset randomly into two equal subsamples to provide cross-validation of our findings. A more detailed explanation of these steps can be found in the Supplementary Materials.
Data were available for 99.7% of expected measurements for all 5 items over time. Data were more likely to be missing during follow-up (i.e., posttreatment) measurements, which accounted for only a small percentage of all expected measurements. The most common incomplete data pattern was to skip or omit the SSI item 3, which occurred in 9 (0.1%) of expected assessments. Due to the rarity of missing data, we relied on the maximum likelihood procedure within multilevel modeling to account for missing data.
Results
We first inspected time series plots for each SSI item over time, which revealed a pattern suggesting the possibility of cycling. To illustrate, SSI item 1 values are depicted as a time series plot in Figure 1a, and reveal that for many individuals, item values tended to fluctuate over time. Figure 1b is a scatterplot of these SSI item 1 values on the x-axis, with the item’s estimated velocities on the y-axis and a loess smoother (a flexible type of regression slope; Cohen et al, 2003) overlaid. In Figure 1b, the loess smoother crosses the axis of zero change (i.e., y = 0) at a value of x that corresponds with the lowest SSI item response option (i.e., x = 0). At this point, the loess smoother has a negative slope, which implies a homeostatic change process (Butner et al., 2015). When an item’s value was higher than the homeostatic point, the item’s value typically decreased at the next assessment; conversely, when the item’s value was lower than the homeostatic point, the item’s value typically increased at the next assessment. The scatterplot implies a second dynamic beyond the homeostatic pattern, however. This second pattern appears as a circle in Figure 1b, implicating the cyclical change pattern wherein item responses fluctuate between higher and lower values in a steady pattern, akin to a sinusoidal wave. Taken together, these two figures suggest the simultaneous existence of homeostatic and cyclical change patterns.
Figure 1. Participant Responses on the Scale for Suicide Ideation (SSI) Item 1 Implicate a Cyclical Change Process.
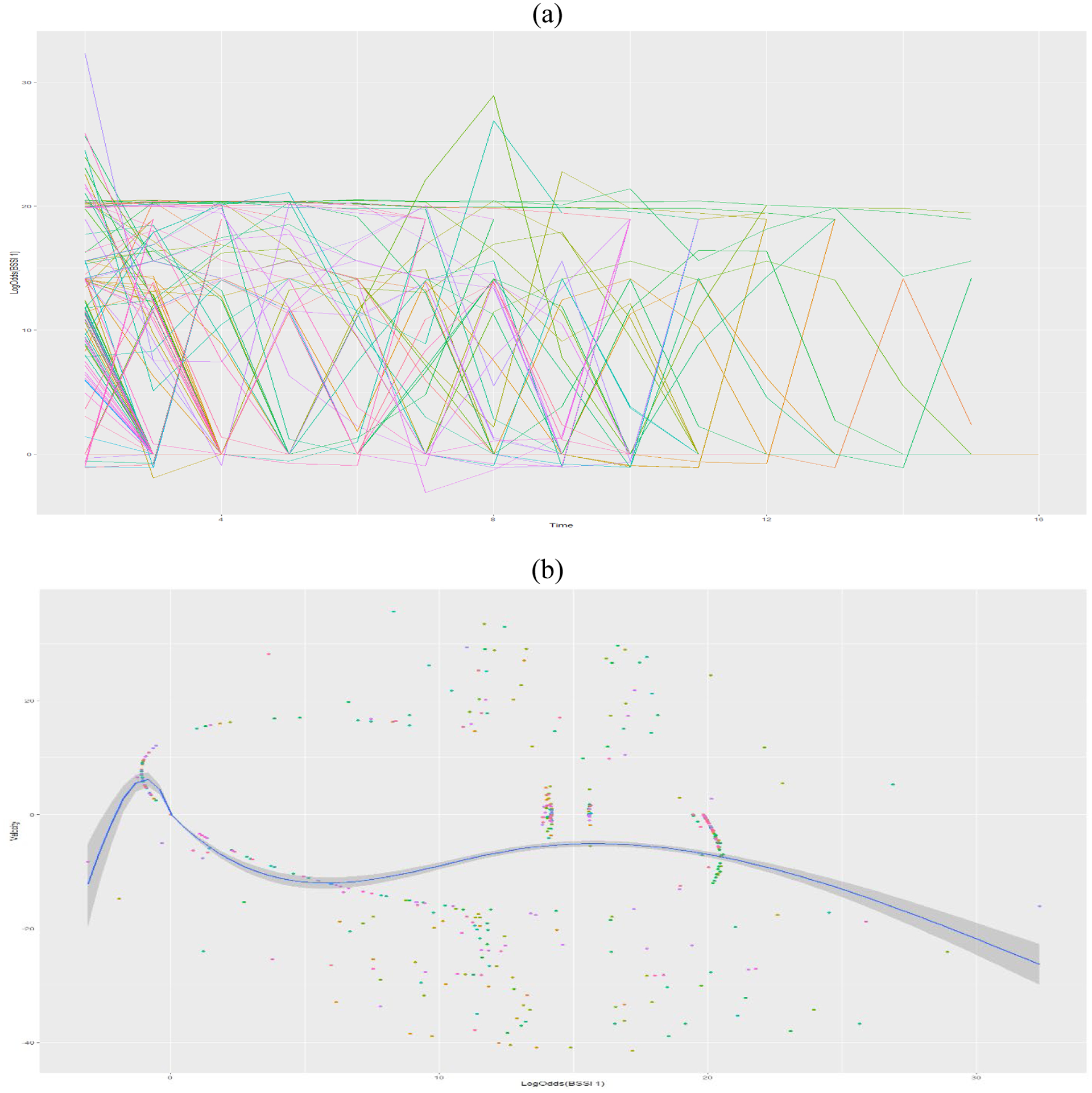
Note. (a) The sawtooth pattern in log-odds SSI item 1 scores over time indicates suicidal ideation switched between lower and higher values during and after treatment. (b) When change in the log-odds SSI item 1 response from time t to time t+1 (i.e., the first derivative, or velocity) is plotted as a function of the log-odds SSI item 1 value at time t (i.e., the zeroth derivative, or value) an elliptical region of empty values is observed, which indicates the relationship between the value and velocity of suicidal ideation was sometimes positive and sometimes negative.
To examine the relative predominance of both dynamics across items, we used the eigenvalue procedure in both random subsamples; Figure 2 shows the resulting scree plots. Using conventional interpretation rules for scree plots (Cattell, 1966), both subsamples suggested two non-zero eigenvalues, implicating the existence of two change dimensions. Table 1 contains the actual eigenvalues from each sample. Within each sample, the first two eigenvalues were complex numbers characterized by real (and negative) values, indicating homeostatic dynamics, and imaginary values with inverse signs, indicating cyclical dynamics. For each eigenvalue, the absolute values of the imaginary components were much larger than the real components, indicating that cyclicity was a much larger contributor to change in item responses over time. We next bootstrapped this procedure, drawing 5000 samples and keeping only the results that ran without errors or warnings (98.0% of all draws). Histograms of the first eigenvalue are displayed in Figures 3a and 3b, broken down by real and imaginary components. Similar to the results of the scree plot, for the real component most samples had a negative value, consistent with homeostatic dynamics, but the absolute value of the imaginary component was much larger in magnitude in all cases, implicating the predominance of cycles.
Figure 2. Scree Plot of the Modulus of the Eigenvalues From the Two Random Samples.
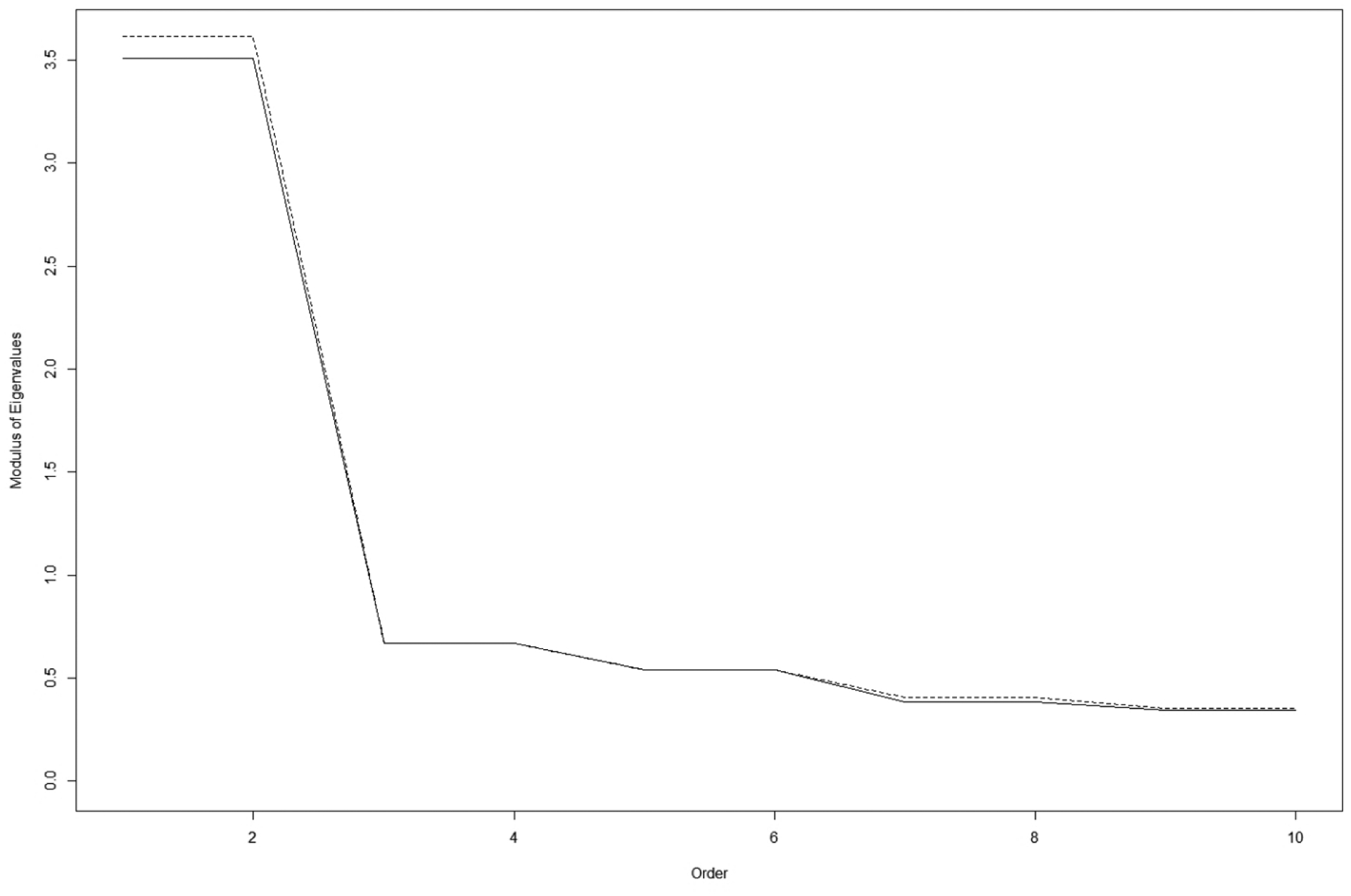
Note. Separate lines (solid and hashed) appear for each random sample. Non-zero eigenvalues for both random samples suggest the existence of two change dimensions in each random sample.
Table 1.
Eigenvalues From the Two Random Samples
| Sample 1 | Sample 2 | |||
|---|---|---|---|---|
| Real | Imaginary | Real | Imaginary | |
| 1 | −0.500 | 3.472 | −0.051 | 3.613 |
| 2 | −0.500 | −3.472 | −0.051 | −3.613 |
| 3 | 0.381 | 0.548 | 0.378 | 0.550 |
| 4 | 0.381 | −0.548 | 0.378 | −0.550 |
| 5 | 0.149 | 0.519 | 0.223 | 0.491 |
| 6 | 0.149 | −0.519 | 0.223 | −0.491 |
| 7 | −0.151 | 0.355 | −0.209 | 0.348 |
| 8 | −0.151 | −0.355 | −0.209 | −0.348 |
| 9 | −0.213 | 0.269 | −0.291 | 0.203 |
| 10 | −0.213 | −0.269 | −0.291 | −0.203 |
Note. These eigenvalues are unrotated because no rotation method has yet been developed that accounts for complex numbers.
Figure 3. Histogram of 5,000 Bootstrapped Samples.
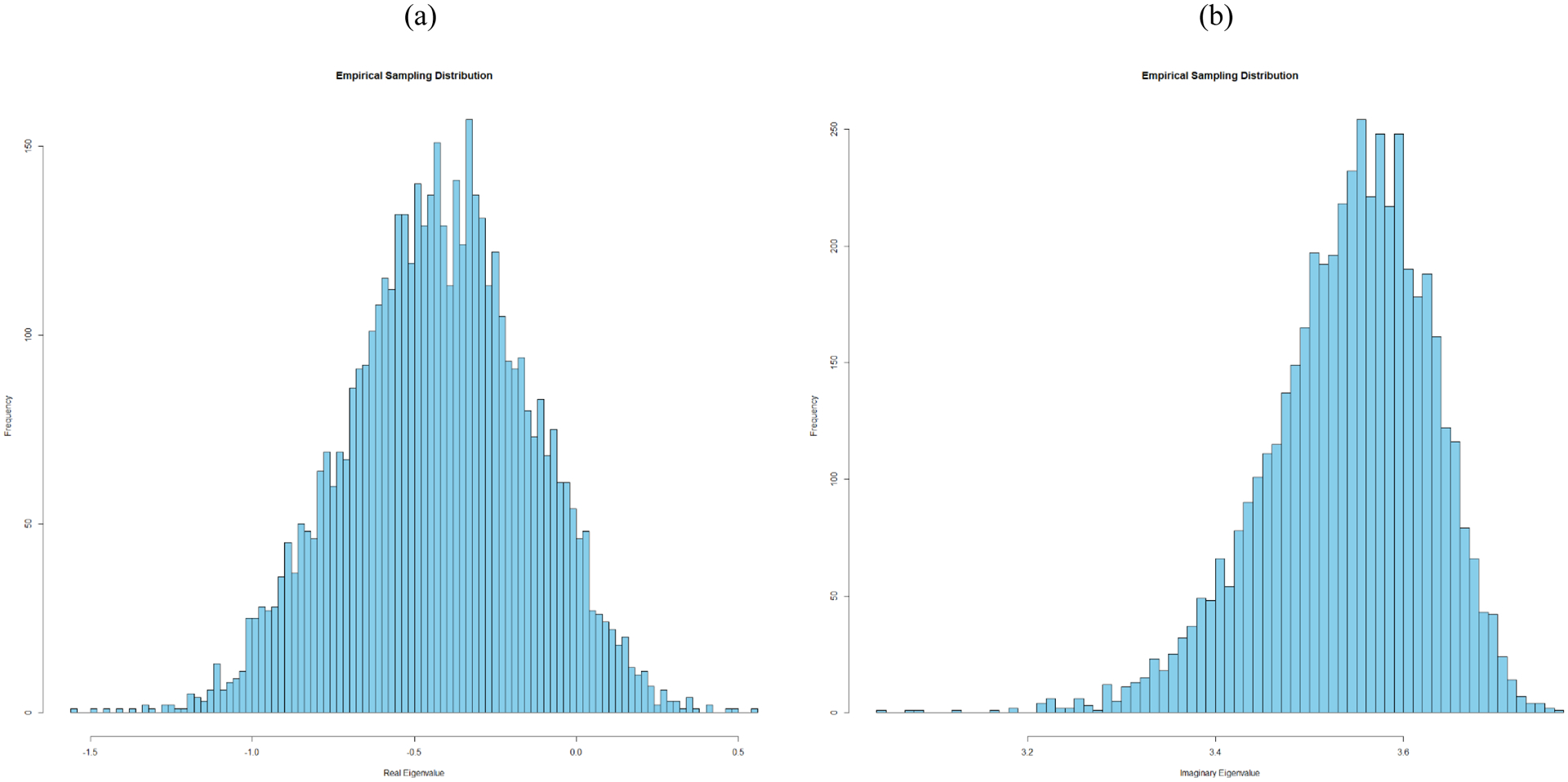
Note. This represents the (a) real component and the (b) imaginary component of the eigenvalue from the first random subsample. The real component of the eigenvalue reflects the attractor dynamic whereas the imaginary component of the eigenvalue represents the cycling dynamic. The magnitude of the eigenvalues, represented by the x-axis, is larger in value for the imaginary component than the real component, implicating the predominance of cycles relative to attraction.
To assess the extent to which the observed cycles were a function of the different SSI items interacting with one another, we repeated the eigenvalue procedure using only the five equations with velocity as the criterion. In both random subsamples, the scree plot of the eigenvalues suggested a maximum of two dimensions of change (Figure 4a). The real component of the first two eigenvalues were positive (Figure 4b) but the imaginary components were zero.1 Only the third and higher eigenvalues yielded a non-zero imaginary component, implying that the cyclic nature of SSI item responses was attributable to something other than the 5 variables considered in this study.
Figure 4. Scree Plot and Histogram of Eigenvalues.
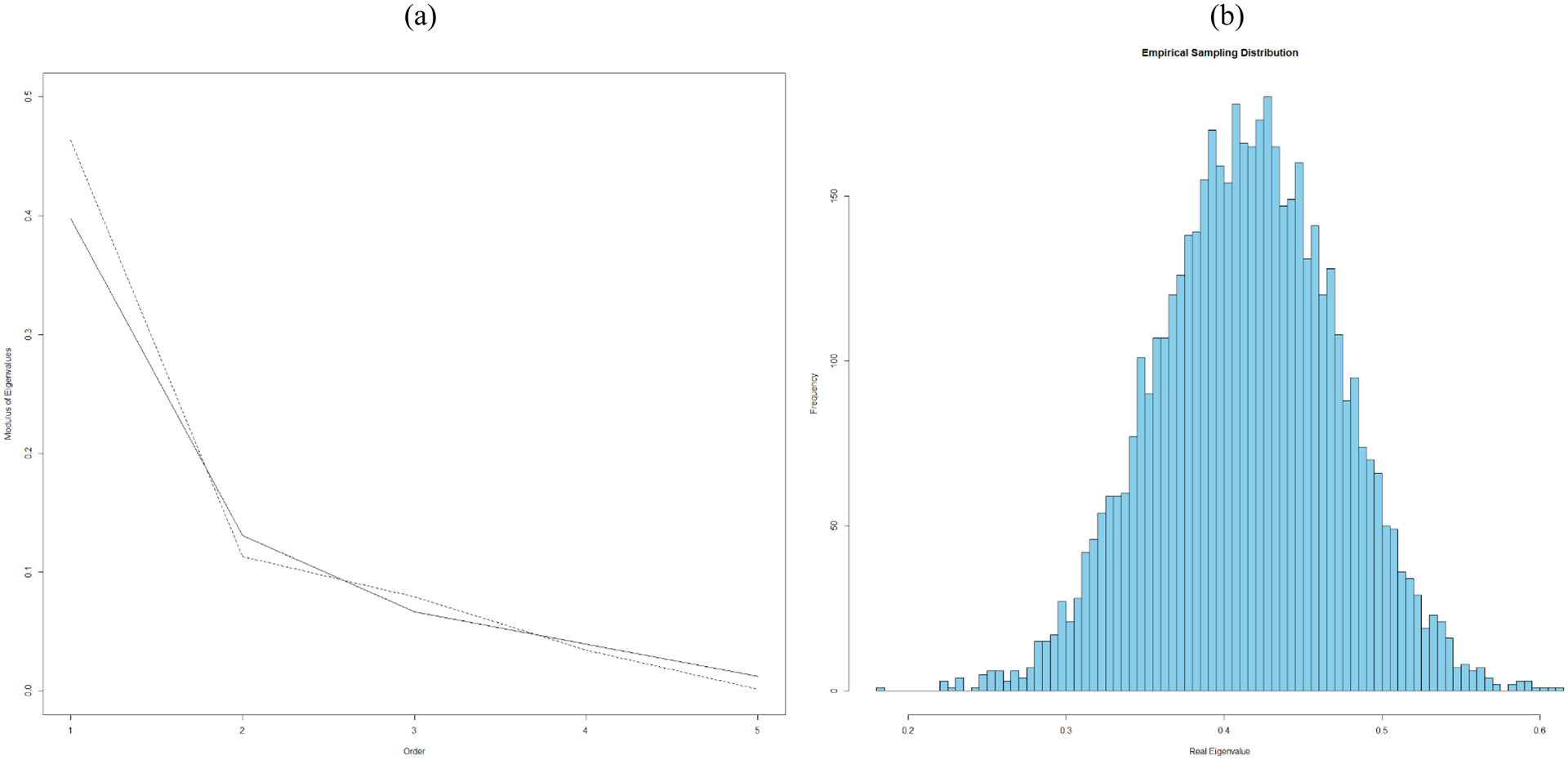
Note. (a) Scree plot of the modulus of the eigenvalues for two random subsamples based on only the five equations using velocity as the criterion. Separate lines (solid and hashed) appear for each random sample. This scree plot suggests a maximum of two dimensions of change. (b) Histogram of the bootstrapped first real eigenvalue from the full sample based on the five equations that use velocity as the criterion.
Discussion
Although the inherently dynamic nature of suicide risk has been recognized for decades, the assessment of suicide risk has not taken these dynamics into account. The present results support two key conclusions about suicidal ideation among treatment-seeking military personnel with PTSD: first, fluctuations in suicidal ideation are dominated by cycles and, second, suicidal ideation is better understood as a multidimensional rather than a unidimensional construct. This cyclic nature holds several implications relevant to measurement issues and the assessment of suicide risk using the SSI and (potentially) other measures. For example, cycling may explain mixed findings regarding the SSI’s factor structure, which has typically been examined using cross-sectional data (e.g., Beck et al., 1979; Holden et al., 1985). This is because, in the case of cycles, an item’s response value at a given time point would not enough to distinguish whether item responses, and possibly suicide risk more generally, are on the upswing or downswing. For example, a patient who reports a weak wish to die on SSI item 1 (i.e., a response value of 1) could signify either an increase in risk (e.g., moving from a value of 0 to 1) or a decrease in risk (i.e., moving from a value of 2 to 1)—two very different clinical circumstances. Analyses that do not account for temporal dynamics treat these two opposing circumstances as the same, however.
Multidimensionality increases the complexity of these considerations because it introduces the possibility that different aspects of suicide risk may be moving in different directions with different velocities at any given point in time. Indeed, our results suggest that among patients with PTSD, this circumstance is very likely to be true. Future work should therefore take care to consider both value and change when developing scales designed to measure an inherently dynamic construct and when using these scales in research and, more importantly, clinical settings. Such research could provide more nuanced and accurate methods for suicide risk screening and assessment than prevailing methods that often represent suicide risk as a unidimensional construct.
Although suicidal ideation primarily cycles, there may nonetheless be circumstances where it functions homeostatically, meaning that responses tend to gravitate towards or cling to a particular value. Our results suggest this homeostatic dynamic is probably associated with lower risk states, and would manifest as repeated zero-value responses across the 5 SSI items used in our analyses. This aligns with previous research showing that suicidal behaviors are associated with larger and more rapid fluctuations in suicidal ideation (Bryan et al., 2019). From a clinical perspective, these patterns suggest that among patients with PTSD, switching from a homeostatic to a cycling dynamic may signal the emergence of suicidal behavior and warrant the use of empirically-supported suicide-focused interventions like the crisis response plan, a brief intervention that has been shown to significantly reduce suicidal behavior (Bryan et al., 2017) and can be integrated into trauma-focused therapies (Rozek & Bryan, 2020). Conversely, switching from a cycling to a homeostatic dynamic may signal risk stabilization, a pattern implicated in previous research with treatment-seeking military personnel (Bryan et al., 2019). If patients differ or can switch between homeostatic and cycling dynamics around a particular level of suicide risk, there may be times when clinicians should not merely examine the values of the SSI (possibly other scales as well) through time, but should also consider change processes including velocity and acceleration. Further research building upon the present results could potentially lead to improved suicide risk assessment and monitoring methods that can better guide clinical decision-making. If, for example, clinicians repeatedly assess suicide risk at each clinical encounter, temporal dynamics could potentially be calculated by an automated system that could distinguish between multiple dynamics, which could potentially improve clinical decision-making.
Our results further suggest that cycles in SSI item responses were related to the items’ interactions with something (or some things) external to suicidal ideation. Given all of the participants included in these analyses were diagnosed with PTSD, one obvious hypothesis involves PTSD symptomatology, although it is also possible that one or more other variables (e.g., depression, alcohol use, emotion dysregulation) play a role, whether in isolation or combination. Unfortunately, further analyses aimed at exploring of all of the many possible candidates, which could play a role either in isolation or in combination with one another, extends beyond the scope of the present paper, but this is a clear direction for further investigation. Such research could uncover key mechanisms underlying increased risk for suicide-related morbidity in people with PTSD, thereby leading to treatment refinement.
Strengths and Limitations
Pulling from multiple archived studies provided a unique opportunity to test our hypotheses in a large sample that was followed over time, anchoring the generalizability of these findings. Further scaffolding was generated by splitting the sample for cross-validation. Despite these strengths, several key limitations warrant discussion. Foremost, we did not entertain the possibility of cycling until after we completed an initial inspection of the data, notably the scatterplots of item responses, to include Figure 1b; the inclusion of second order derivatives was therefore a reaction to this observation in our preliminary analyses and was not hypothesized a priori. That said, our cross-validation efforts, made possible by the suitably large sample size, mitigates concerns about replicability of findings based on a post-hoc decision. Second, we chose to use a normal theory approach for estimating velocity and acceleration because we had difficulty estimating acceleration using analytic methods that are more appropriate to the SSI items’ zero-inflated distributions. This difficulty was likely related to peculiarities that can occur in estimation as a function of how time is scaled in the Empirical Bayesian procedure (Deboeck, P. R., personal communication, April 3, 2020). Our reliance on normal theory derivatives may therefore have over-emphasized the observed cycles as regular divergences from the lowest possible endorsement values. Additional research using the SSI and/or other measures of suicide risk would therefore be valuable for considering the generalizability and consistency of the present findings.
Third, we chose to focus only on the SSI’s first five items because they were administered and completed by all individuals at all assessments across all of the included studies. The decision to exclude items 6–19 was a practical one reflecting an insufficient amount of item responses to reliably estimate velocities and accelerations. Although this approach minimized missingness and more closely mirrored brief screening and assessment approaches used in many clinical settings, using only 5 items nonetheless limits the number of obtainable dimensions. It is possible, for instance, that the SSI’s additional 14 items would help identify different factor structures consistent with some of the factor structures previously proposed for the SSI (e.g., planning, preparatory behavior). The conditional scoring format of the SSI, which assumes that later items would all have values of zero if items 4 and 5 are not endorsed, severely limits the potential range of change in these later items. This restriction would have created a very sparse analytic structure which would have reduced our confidence in the results, especially if those results were inconsistent with those obtained using only the first 5 items.
Fourth, the amount of time in between adjacent measurements varied both within and across studies, reflective of their different aims and designs. For example, the SSI was administered once per week during active treatment but administered every few months during follow-up. Our derivative estimation procedure accounted for this variability, but the approach makes an assumption that the underlying dynamics are unchanging over time both within and across individuals, and also makes the assumption that the dynamics during shorter time scales (e.g. hours) would merely be an extension of what we observed. In combination, these assumptions place some limitations on our claims. It seems reasonable, for example, to assume that the underlying dynamics within people might change over time (i.e., someone switching from homeostatic to cyclical, or vice versa), or that we might see something different when using a different temporal metric (e.g., cyclical when assessing every few hours versus homeostatic when assessing every few months). These concerns are mitigated in that change in the measurement qualities of the SSI items should not change much even though different assessment schedules might alter the dynamics that can be observed. These results therefore set up a strong foundation for the examination of the temporal dynamics of suicidal ideations on faster time schedules that might be relevant to an active clinical setting and differentiating suicidal ideation dynamics under a range of conditions, such as studies using ecological momentary assessment or daily diaries.
Finally, our sample was limited to active duty military personnel receiving outpatient treatment for PTSD. Our sample was demographically diverse and may generalize to other treatment-seeking active duty military personnel. It is possible that the observed patterns would differ in nonmilitary samples and/or samples with a more equitable distribution of men and women. Homeostatic and cyclical dynamics may, for example, differ by sex and/or other demographic characteristics. Alternatively, it is possible that the observed patterns were influenced in part by the co-occurrence of PTSD or the specific nature of the treatments provided. Treatments that reduce or attenuate cyclical dynamics in suicidal ideation, for instance, may influence the likelihood of suicidal behaviors in different ways that treatments that do not affect this dynamic. Replication with other samples is therefore needed to better understand the generalizability of these findings.
Despite these limitations, our results provide further support for the complexity of suicide risk and its measurement, and suggest that temporal patterns of self-reported suicide ideation among military personnel receiving treatment for PTSD demonstrate a strong component of cycling, implicating a possible mechanism underlying increased risk for suicide death and suicide attempts among people with PTSD. Furthermore, the development and use of self-report measures of suicide risk should explicitly consider the potential impact of temporal dynamics on mechanism-focused research.
Supplementary Material
Acknowledgments
Funding for the original data collection for the projects included in the secondary analyses was made possible by the U.S. Department of Defense through the U.S. Army Medical Research and Materiel Command, Congressionally Directed Medical Research Programs, Psychological Health and Traumatic Brain Injury Research Program awards W81XWH-08-02-0109 (Alan Peterson), W81XWH-08-02-0111 (Edna Foa), W81XWH-08-02-0114 (Brett Litz), and W81XWH-08-02-0116 (Patricia Resick).
Funding for this work was made possible by the National Institute of Mental Health of the National Institutes of Health under award R01MH117600 (Craig Bryan) and by the Assistant Secretary of Defense for Health Affairs under award W81XWH-18-2-0022 (Craig Bryan).
The views expressed herein are solely those of the authors and do not reflect an endorsement by or the official policy or position of the National Institutes of Health, the U.S. Army, the U.S. Air Force, the Department of Defense, the Department of Veterans Affairs, or the U.S. Government.
Footnotes
The authors do not report any conflicts of interest.
This pattern implies a third dynamic not considered in this study: repulsion. Repulsion functions as a sort of “transition state” because it often occurs in between homeostatic and cyclical dynamics. This finding therefore lends further support for the existence of two change dynamics.
References
- Abraham RH, & Shaw CD (2005). Dynamics: The geometry of behavior (4th ed.). Aerial Press. [Google Scholar]
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). [Google Scholar]
- Bates D, Mächler M, Bolker B, & Walker S (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software, 67(1), 1–48. 10.18637/jss.v067.i01 [DOI] [Google Scholar]
- Beck AT, Kovacs M, & Weissman A (1979). Assessment of suicidal ideation: The Scale for Suicidal Ideation. Journal of Consulting and Clinical Psychology, 47, 343–352. 10.1037//0022-006x.47.2.343 [DOI] [PubMed] [Google Scholar]
- Beck AT, & Steer RA (1991). Manual for Beck Scale for Suicide Ideation. Psychological Corporation. [Google Scholar]
- Beck AT, Steer RA, & Ranieri WF (1988). Scale for Suicidal Ideation: Psychometric properties of a self-report version. Journal of Clinical Psychology, 44(4), 499–505. [DOI] [PubMed] [Google Scholar]
- Brown GK (2001). A review of suicide assessment measures for intervention research with adults and older adults. National Institute of Mental Health. https://www.sprc.org/sites/default/files/migrate/library/BrownReviewAssessmentMeasuresAdultsOlderAdults.pdf [Google Scholar]
- Bryan CJ, Butner JE, May AM, Rugo KF, Harris JA, Oakey DN, Rozek DC, & Bryan AO (2020). Nonlinear change processes and the emergence of suicidal behavior: A conceptual model based on the fluid vulnerability theory of suicide. New Ideas in Psychology, 57, 100758. 10.1016/j.newideapsych.2019.100758 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan CJ, Mintz J, Clemans TA, Leeson B, Burch TS, Williams SR, Maney E, & Rudd MD (2017). Effect of crisis response planning vs. contracts for safety on suicide risk in U.S. Army Soldiers: A randomized clinical trial. Journal of affective disorders, 212, 64–72. 10.1016/j.jad.2017.01.028 [DOI] [PubMed] [Google Scholar]
- Bryan CJ, Rozek DC, Butner J, & Rudd MD (2019). Patterns of change in suicide ideation signal the recurrence of suicide attempts among high-risk psychiatric outpatients. Behaviour Research and Therapy, 120, 103392. 10.1016/j.brat.2019.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan CJ, & Rudd MD (2016). The importance of temporal dynamics in the transition from suicidal thought to behavior. Clinical Psychology: Science and Practice, 23(1), 21–25. 10.1111/cpsp.12135 [DOI] [Google Scholar]
- Butner JE, Berg CA, Baucom BR, & Wiebe DJ (2014). Modeling coordination in multiple simultaneous latent change scores. Multivariate Behavioral Research, 49(6), 554–570. 10.1080/00273171.2014.934321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butner JE, Deits-Lebehn C, Crenshaw AO, Wiltshire TJ, Perry NS, Kent de Grey RG, Hogan JN, Smith TW, Baucom KJW, & Baucom BRW (2017). A multivariate dynamic systems model for psychotherapy with more than one client. Journal of Counseling Psychology, 64(6), 616–625. 10.1037/cou0000238 [DOI] [PubMed] [Google Scholar]
- Butner JE, Gagnon KT, Geuss MN, Lessard DA, & Story TN (2015). Utilizing topology to generate and test theories of change. Psychological Methods, 20(1), 1–25. 10.1037/a0037802 [DOI] [PubMed] [Google Scholar]
- Cattell RB (1966). The Scree Test for the number of factors. Multivariate Behavioral Research, 1(2), 245–276. 10.1207/s15327906mbr0102_10 [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed.). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Deboeck PR (2020). Empirical Bayes derivative estimates. Multivariate Behavioral Research, 55(3), 382–404. 10.1080/00273171.2019.1642729 [DOI] [PubMed] [Google Scholar]
- Estabrook R (2015). Evaluating measurement of dynamic constructs: Defining a measurement model of derivatives. Psychological Methods, 20(1), 117–141. 10.1037/a0034523 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foa EB, McLean CP, Zang Y, Rosenfield D, Yadin E, Yarvis JS, Mintz J, Young-McCaughan S, Borah EV, Dondanville KA, Fina BA, Hall-Clark BN, Lichner T, Litz BT, Roache JD, Wright EC, & Peterson AL, for the STRONG STAR Consortium. (2018). Effect of prolonged exposure therapy delivered over 2 weeks vs 8 weeks vs present-centered therapy on PTSD symptom severity in military personnel: A randomized clinical trial. Journal of the American Medical Association, 319(4), 354–364. 10.1001/jama.2017.21242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foa E, Riggs D, Dancu C, & Rothbaum B (1993). Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress, 6(4), 459–474. 10.1002/jts.2490060405 [DOI] [Google Scholar]
- Gradus JL, Qin P, Lincoln AK, Miller M, Lawler E, Sørensen HT, & Lash TL (2010). Posttraumatic stress disorder and completed suicide. American Journal of Epidemiology, 171(6), 721–727. 10.1093/aje/kwp456 [DOI] [PubMed] [Google Scholar]
- Holden RR, Mendonca JD, & Mazmanian D (1985). Relation of response set to observed suicide intent. Canadian Journal of Behavioural Science, 17(4), 359–368. 10.1037/h0080048 [DOI] [Google Scholar]
- Huckfeldt RR, Kohfeld CW, & Likens TW (1982). Dynamic modeling: An introduction. Sage Publications. 10.4135/9781412983990 [DOI] [Google Scholar]
- Kleiman EM, Turner BJ, Fedor S, Beale EE, Huffman JC, & Nock MK (2017). Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies [Supplemental material]. Journal of Abnormal Psychology, 126(6), 726–738. 10.1037/abn0000273.supp [DOI] [PubMed] [Google Scholar]
- Litz BT, Contractor AA, Rhodes C, Dondanville KA, Jordan AH, Resick PA, Foa EB, Young-McCaughan S, Mintz J, Yarvis JS, & Peterson AL; for the STRONG STAR Consortium. (2018). Distinct trauma types in military service members seeking treatment for posttraumatic stress disorder. Journal of Traumatic Stress, 31(2), 286–295. 10.1002/jts.22276. [DOI] [PubMed] [Google Scholar]
- Maris R (1972). Current problems in suicide research. Crisis Intervention, 4(3), 84–89. [Google Scholar]
- May AM, & Klonsky ED (2016). What distinguishes suicide attempters from suicide ideators? A meta-analysis of potential factors. Clinical Psychology: Science and Practice, 23(1), 5–20. 10.1111/cpsp.12136 [DOI] [Google Scholar]
- Molenaar PC (2004). A manifesto on psychology as idiographic science: Bringing the person back into scientific psychology, this time forever. Measurement, 2(4), 201–218. 10.1207/s15366359mea0204_1 [DOI] [Google Scholar]
- Resick PA, Wachen JS, Dondanville KA, Pruiksma KE, Yarvis JS, Peterson AL, Mintz J, & the STRONG STAR Consortium. (2017). Effect of group vs individual cognitive processing therapy in active-duty military seeking treatment for posttraumatic stress disorder: A randomized clinical trial. JAMA Psychiatry, 74(1), 28–36. 10.1001/jamapsychiatry.2016.2729 [DOI] [PubMed] [Google Scholar]
- Resick PA, Wachen JS, Mintz J, Young-McCaughan S, Roache JD, Borah AM, Borah EV, Dondanville KA, Hembree EA, Litz BT, & Peterson AL, on behalf of the STRONG STAR Consortium. (2015). A randomized clinical trial of group cognitive processing therapy compared with group present-centered therapy for PTSD among active duty military personnel. Journal of Consulting and Clinical Psychology, 83(6), 1058–1068. 10.1037/ccp0000016 [DOI] [PubMed] [Google Scholar]
- Rozek DC, & Bryan CJ (2020). Integrating crisis response planning for suicide prevention into trauma-focused treatments: A military case example. Journal of clinical psychology, 76(5), 852–864. 10.1002/jclp.22920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rudd MD (2006). Fluid vulnerability theory: A cognitive approach to understanding the process of acute and chronic suicide risk. In Ellis TE (Ed.), Cognition and suicide: Theory, research, and therapy (pp. 355–368). American Psychological Association. 10.1037/11377-016 [DOI] [Google Scholar]
- Schiepek G, Fartacek C, Sturm J, Kralovec K, Fartacek R, & Plöderl M (2011). Nonlinear dynamics: Theoretical perspectives and application to suicidology. Suicide and Life-Threatening Behavior, 41(6), 661–675. 10.1111/j.1943-278X.2011.00062.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.