

Abstract
Background
Personal health records (PHRs) are eHealth tools designed to support patient engagement, patient empowerment, and patient- and person-centered care. Endorsement of a PHR by health care providers (HCPs) facilitates patient acceptance. As health care organizations in the Kingdom of Saudi Arabia begin to adopt PHRs, understanding the perspectives of HCPs is important because it can influence patient adoption. However, no studies evaluated HCPs’ acceptance of PHRs in the Kingdom of Saudi Arabia.
Objective
The aim of this study was to identify predictors of HCPs’ acceptance of PHRs using behavioral intention to recommend as a proxy for adoption.
Methods
This cross-sectional study was conducted among HCPs (physicians, pharmacists, nurses, technicians, others) utilizing a survey based on the Unified Theory of Acceptance and Use of Technology. The main theory constructs of performance expectancy, effort expectancy, social influence, facilitating conditions, and positive attitude were considered independent variables. Behavioral intention was the dependent variable. Age, years of experience, and professional role were tested as moderators between the main theory constructs and behavioral intention using partial least squares structural equation modeling.
Results
Of the 291 participants, 246 were included in the final analysis. Behavioral intention to support PHR use among patients was significantly influenced by performance expectancy (β=.17, P=.03) and attitude (β=.61, P<.01). No moderating effects were present.
Conclusions
This study identified performance expectancy and attitude as predictors of HCPs’ behavioral intention to recommend PHR to patients. To encourage HCPs to endorse PHRs, health care organizations should involve HCPs in the implementation and provide training on the features available as well as expected benefits. Future studies should be conducted in other contexts and include other potential predictors.
Keywords: personal health records, patient portals, Ministry of National Guard Health Affairs, UTAUT, eHealth, Middle East
Introduction
Overview
A wide range of eHealth technologies has become available over the past 2 decades as countries have introduced eHealth initiatives to support the goals for patient engagement and person-centered care [1]. Legislation around the world advocates for patients to have electronic access to their health information through personal health records (PHRs) [2]. PHRs are an eHealth tool to increase patient engagement and empowerment by allowing individuals to keep track of their personal health information. The Markle Foundation defined PHRs as “an Internet-based set of tools that allows people to access and coordinate their lifelong health information and make appropriate parts of it available to those who need it” [3]. Person-centered care and patient engagement are considered pillars of any high-functioning health care system, and PHRs can contribute to both [4,5]. While various terms have been used interchangeably with PHR in the literature (eg, patient portal, patient web portal, computerized patient portal, patient accessible electronic health record [EHR], tethered PHR, electronic PHR), the broader term of PHR will be used predominantly throughout this paper.
PHR adoption has been associated with a wide range of benefits, including better patient–provider relationships, improvements in patient engagement, better medication adherence, positive health outcomes (eg, blood pressure and glycemic control), and increased organizational efficiencies [6]. As the benefits of PHR adoption are achieved, health care costs potentially decrease as individuals become empowered to take better control of their health and rely less on interactions with the health care system [6]. However, multiple studies have shown low adoption rates [7-9]. Even though the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act and its Meaningful Use criteria accelerated PHR access in the United States [10], only 15%-30% of patients use PHRs while 90% of health care systems offer them [11]. Outside of the United States, a systematic review showed adoption rates of around 0.13% in the United Kingdom and 5% in other European countries [7].
Various barriers to PHR adoption have been identified [7,9,12,13]. In the systematic review by Niazkhani et al [13], the barriers were characterized as patient demographic factors (eg, age, gender); environment/medical practice (eg, providers’ communication about PHRs, physician resistance); technological (eg, perceived PHR usefulness, perceived PHR complexity); and chronic disease characteristics (eg, patients’ feeling of control over the disease, number of comorbidities). Health care providers’ (HCPs) attitudes are a major contributing factor in patients’ adoption of PHRs [14-16]. HCPs play a key role in supporting and engaging patients through their attitudes, behavior, and endorsement of services [17]. Although studies have shown a high level of patient interest in PHRs [5,18-20], there has been a disconnect between interest and uptake. This is partially due to HCPs’ reticence toward the acceptance and promotion of their use [5,21,22].
Researchers around the world have studied HCPs’ attitudes and perceptions of PHRs. Nazi [22] explored the experiences and perspectives of HCPs (physicians, nurses, and pharmacists) related to patients’ use of the My HealtheVet PHR in the United States and found that many HCPs had limited familiarity with the PHR features, contributing to its underutilization [22]. The author identified the following 8 factors to be key in the implementation, adoption, and use of PHRs: (1) showing the relevance of PHRs; (2) increasing the perceived value by focusing on unique services; (3) providing education and training; (4) integrating PHRs into the existing technology; (5) aligning PHR functions with the workflow; (6) offering incentives to individuals or teams; (7) making information accessible; and (8) supporting asynchronous and bidirectional communication.
A study in Finland, which included a wide range of HCPs (eg, nurses, social workers, dentists, physicians, physical therapists, and psychologists), found that the most important factors influencing HCPs’ support for a national patient portal were expected positive influences on their work, the usability of the portal, and benefits for the patients [17]. However, only few (13%) respondents felt they had received adequate information about the portal. The authors recommended HCPs be informed about PHR benefits to garner their support. In Canada, Wiljer et al [23] endorsed institutional strategies such as “continuous organizational reassurance,” education, and a physician champion to stimulate a paradigm shift to patient-centered care for successful PHR implementation. In a Swedish study of oncology HCPs (nurses and physicians), the authors compared HCPs working in outpatient clinics with those working in primary care units [24]. A greater proportion of HCPs in primary care believed there were benefits of patients using PHRs such as better adherence (50% vs. 35%), greater ability to clarify important information (50% vs. 26%), and improved patient communication (36% vs. 20%) [25].
In the Kingdom of Saudi Arabia, enhancing patient-centered care through patient involvement with technology is an objective of The National Transformation Program, a component of Vision 2030. The Ministry of National Guard Health Affairs (MNGHA) implemented the MNGHA Care PHR in 2018. No studies have evaluated HCPs’ acceptance of PHRs in the country.
The aim of this study was to identify a set of factors that affect the intention to recommend the use of MNGHA Care PHR among HCPs. To promote patient engagement and patient-centered care, a better understanding of how HCPs perceive PHRs is needed.
Theoretical Background
In 2003, Venkatesh et al [26] developed the Unified Theory of Acceptance and Use of Technology (UTAUT) to provide a comprehensive framework to explain acceptance, intention, and usage of information technology in organizations. It is an integration of 8 theories—theory of reasoned action, technology acceptance model (TAM), motivational model, theory of planned behavior (TPB), combined TAM–TPB, model of personal computer utilization, diffusion of innovation theory, and social cognitive theory [26]. The core constructs of performance expectancy, effort expectancy, social influence, and facilitating conditions directly act on behavioral intention and, ultimately, predict the use of the technology. Gender, age, voluntariness, and experience are moderators in the framework. The model explained approximately 77% of the variance in behavioral intention and 52% of the variance in technology use [26]. Since its development, UTAUT has been used to explain technology acceptance in different user groups in a wide range of contexts with various technologies, strengthening the generalizability [27]. UTAUT has also been used broadly in other health care areas, including telemedicine [28,29], electronic medical/health records [30-34], electronic documentation systems [35], picture archiving and communication systems [36], and health information systems [37,38].
Research Model and Hypotheses
Most studies have not examined the full UTAUT with the moderation effects but rather the main effects alone, combined with a subset of the moderators, or with new constructs or mechanisms [39]. Venkatesh et al [39] proposed that future research should use UTAUT as the baseline model to transform the theory from static to dynamic. New endogenous mechanisms or new moderation mechanisms are the most common types of extensions [39]. While UTAUT includes the technological dimension (performance expectancy and effort expectancy) and organizational/environmental dimension (social influence and facilitating conditions), the individual dimension is not included. Nonetheless, individual traits (attitude, personal innovativeness, computer self-efficacy) may significantly predict the acceptance of technology [27,40,41]. Constructs representing individual traits are frequently used as endogenous mechanisms to extend UTAUT.
The research model for this study includes the 4 core UTAUT constructs: performance expectancy, effort expectancy, social influence, and facilitating conditions (Figure 1). The construct of attitude was added as an individual characteristic. Unlike the original UTAUT model, we did not include behavior in the proposed model because we were unable to objectively assess use. Instead, we measured intention to recommend PHR, using it as a proxy for HCPs’ acceptance. Behavioral intention is frequently a proxy for actual technology adoption in the literature [42-44].
Figure 1.
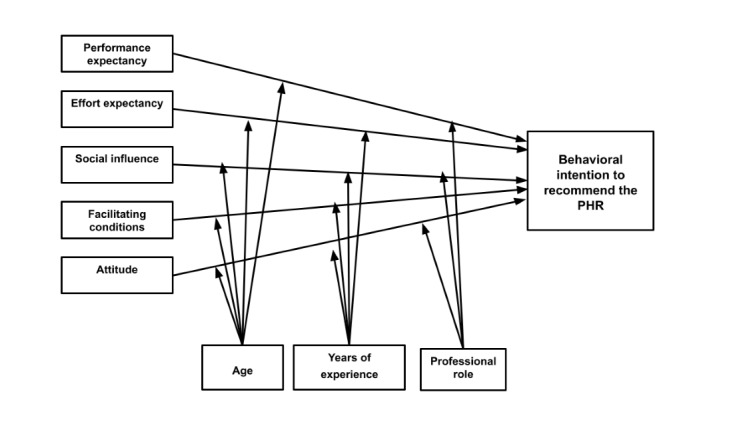
Adapted UTAUT model. PHR: personal health record; UTAUT: Unified Theory of Acceptance and Use of Technology.
Proposed differences between this model and the original UTAUT model are shown in Table 1. The moderators chosen for this study were age, years of experience, and professional role. Previous literature indicated that age was inversely associated with eHealth adoption. For example, electronic medical record use was inversely associated with physician age [45]. A potential explanation is that, in the initial stages of technology use, older users are believed to be more influenced by experience, and ease of use is more important [26]. Next, years in practice has been associated with acceptance of eHealth [45]. As the number of years since medical school graduation increased, physicians became less likely to accept eHealth technologies [45]. There have also been differences in eHealth acceptance by professional role [45]. Nonphysicians used advanced EHR features less than physicians, and specialists (eg, obstetrician/gynecologists) were less likely to use an EHR in their practices [45]. Voluntariness of use and gender were dropped as moderators in the proposed model. PHR use is not mandatory; therefore voluntariness of use is not relevant [26]. In the health care context, professional role takes precedence over gender and no differences in acceptance by gender were expected [34].
Table 1.
Original Unified Theory of Acceptance and Use of Technology (UTAUT) versus adapted UTAUT for health care providers.
| Construct | Original UTAUTa moderators | Adapted UTAUT moderators | |||||
|
|
Gender | Age | Experience | Voluntariness | Age | Years of experience | Professional role |
| PEb → BIc | ✓ | ✓ |
|
|
✓ |
|
✓ |
| EEd → BI | ✓ | ✓ | ✓ |
|
✓ | ✓ |
|
| SIe → BI | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| BI → Usef |
|
|
|
|
|
|
|
| FCg → Use |
|
✓ | ✓ |
|
|
|
|
| FC → BI |
|
|
|
|
✓ | ✓ |
|
| ATTh → BI |
|
|
|
|
✓ | ✓ | ✓ |
aUTAUT: Unified Theory of Acceptance and Use of Technology.
bPE: performance expectancy.
cBI: behavioral intention.
dEE: effort expectancy.
eSI: social influence.
fUse: actual usage.
gFC: facilitating conditions.
hATT: attitude.
This study tested the following hypotheses:
H1: Performance expectancy positively influences behavioral intention to recommend the PHR
H2: Effort expectancy positively influences behavioral intention to recommend the PHR
H3: Social influence positively influences behavioral intention to recommend the PHR
H4: Facilitating conditions positively influence behavioral intention to recommend the PHR
H5: Attitude positively influences behavioral intention to recommend the PHR
H6: Age, years of experience, and professional role selectively moderate the relationships between the main constructs and behavioral intention to recommend the PHR
Methods
Study Design
A cross-sectional study utilizing a survey was conducted at a large, integrated health care system in the Kingdom of Saudi Arabia. The survey was administered to HCPs across the organization to assess acceptance of the PHR. Since 2018, patients have had access to the MNGHA Care PHR, which includes the following features: scheduling appointments, requesting medical reports and prescription refills, viewing radiology reports, checking laboratory results, and receiving vaccination reminders [46]. Additionally, personal health information such as weight, blood pressure, blood sugar, and exercise details can be uploaded. Finally, MNGHA Care contains links to health education information and a self-assessment feature permitting patients to enter information related to pain control, performance status, and quality of life.
Setting and Participants
The study population consisted of HCPs from MNGHA hospitals and primary health care centers in Dammam, Riyadh, Jeddah, Madinah, Al Ahsa, and Qassim, including physicians, dentists, pharmacists, nurses, physical and occupational therapists, optometrists, technicians (pharmacy, medical imaging, medical and pathology laboratory, dental), paramedics, and dietitians.
Instrument and Data Collection
Data were collected using an anonymous self-administered online survey between April and May 2021. The initial version of the survey included 63 items adapted from previously published technology acceptance surveys used in health care in 3 parts [26,47-51]. The first part captured demographic characteristics including age, gender, region, facility type, profession, specialty area (for physicians), years in profession, years at MNGHA, and nationality. The second part contained 4 general PHR questions: (1) Have you heard of MNGHA Care?; (2) Do you have an MNGHA Care account?; (3) Have you used MNGHA Care yourself?; and (4) Have you recommended patients to use MNGHA? This section also included Likert-scale statements associated with PHR acceptance along with an open-ended question and a checklist. The third section related to acceptance of secure messaging and included Likert-scale statements, an open-ended question, and a checklist.
The instrument was built on QuestionPro [52] and pilot tested with 7 HCPs (2 physicians, 3 pharmacists, and 2 nurses) working within MNGHA. The QuestionPro survey link and a cover letter explaining the purpose of the study were emailed to these 7 HCPs to obtain feedback regarding survey length, clarity, and flow of the questionnaire. After comments were compiled, 12 items were removed, and some were modified to improve clarity and to decrease survey length. The final version of the survey included 51 items and was approved by the institutional review boards at the Virginia Commonwealth University and King Abdullah International Medical Research Center.
For this study, the focus was on parts 1 and 2 of the instrument. However, the open-ended question and checklist from part 2 are not included in this paper. Responses to the PHR acceptance items were provided on a 5-point Likert scale from strongly disagree (1) to strongly agree (5). Acceptance was operationalized as the intention to recommend patients use the PHR using the statement “I will probably recommend patients use MNGHA Care in the future” [49].
Performance expectancy was defined as the degree to which the HCP believes a PHR will be beneficial in the health care delivery process [20]. It was measured with the following 4 items:
MNGHA Care is a useful tool to help patients feel more involved in their care [47,53].
I believe MNGHA Care helps patients to better manage their health [48].
MNGHA Care will increase patient satisfaction with their health care [48].
MNGHA Care can improve the quality of patient care [51].
Effort expectancy is the degree of ease associated with use of the PHR [20]. It was measured with the following 3 items:
Information in MNGHA Care should be easy for our patients to understand [48,53].
I believe most patients have the skills needed to use MNGHA Care [47].
I think it is not difficult for our patients to learn to use MNGHA Care [47].
Social influence is the degree to which an individual perceives important others believe the PHR should be used [20]. It was measured with the following 2 items:
I believe our patients support the use of MNGHA Care [48].
In general, the organization has supported the use of MNGHA Care [26].
Facilitating conditions was defined as the degree to which an individual believes an organizational and technical infrastructure exists to support use of the PHR [20]. It was measured with the following 3 items:
Attitude was defined as positive feelings related to patients using the PHR [54]. It was measured with the following 4 items:
MNGHA Care is a positive advancement in this digital age [47].
I believe MNGHA Care will be used by many patients [47].
Although behavioral intention and social influence used less than 3 items, partial least squares structural equation modeling (PLS) supports using single-item measures [55] and earlier research using PLS has used less than 3 items for measuring constructs [56,57].
Sampling
A snowball and convenience sampling strategy was used to recruit HCPs from across the organization. HCPs were initially recruited through the hospital’s email list in combination with WhatsApp as it is a widely used social media platform for professional communication. They were asked to forward the survey to other HCPs. Follow-up reminders were also sent out. The target sample size for this study was 200 HCPs, which has been considered a fair sample size for statistical analysis with structural equation modeling [58]. To encourage participation, there was a random drawing for twenty five 37.5 Saudi Arabian Riyal (US $10) Amazon gift cards.
Statistical Analyses
Descriptive statistics were analyzed using SPSS version 25 (IBM) [59]. PLS was used to test the research model using SmartPLS version 3.0 [60]. The advantage of PLS is the ability to estimate complex research models without distributional assumptions [61]. Compared with traditional SEM, PLS has greater statistical power, which means that there is a higher likelihood of identifying significant relationships if they are actually present in the population [61]. Furthermore, PLS has been widely used in empirical studies of technology acceptance, including with UTAUT [26,27,34] and with PHR acceptance [50,62]. To test the research model, a measurement model was used to evaluate construct reliability, indicator reliability, convergent validity, and discriminant validity. A structural model was tested after ensuring reliability and validity.
Results
Demographic Characteristics
Overall, 291 HCPs participated in the survey. However, after removing the data for missing values, a usable sample of 246 was used for further analysis. Table 2 presents the demographic characteristics. Most were 40-49 years old (95/246, 38.6%), female (158/246, 64.2%), non-Saudi (132/246, 53.7%), nurses (106/246, 43.1%), in Riyadh (81/246, 32.9%), over 10 years of experience (167/246, 67.9%) and over 10 years at MNGHA (128/246, 52.0%), and hospital based (228/246, 92.7%).
Table 2.
Demographic characteristics (N=246).
| Variables | Values, n (%) | |
| Age |
|
|
|
|
20-29 years | 37 (15.0) |
|
|
30-39 years | 77 (31.3) |
|
|
40-49 years | 95 (38.6) |
|
|
50 years and above | 37 (15.0) |
| Gender |
|
|
|
|
Male | 88 (35.8) |
|
|
Female | 158 (64.2) |
| Nationality |
|
|
|
|
Saudi | 114 (46.3) |
|
|
Non-Saudi | 132 (53.7) |
| Health care provider |
|
|
|
|
Physician | 40 (16.3) |
|
|
Pharmacist | 57 (23.2) |
|
|
Nurse | 106 (43.1) |
|
|
Technician | 33 (13.4) |
|
|
Other | 10 (4.1) |
| Years in profession |
|
|
|
|
Less than 5 years | 33 (13.4) |
|
|
5-10 years | 46 (18.7) |
|
|
Greater than 10 years | 167 (67.9) |
| Years working at MNGHAa |
|
|
|
|
<1 year | 13 (5.3) |
|
|
1-4 years | 40 (16.3) |
|
|
5-10 years | 65 (26.4) |
|
|
>10 years | 128 (52.0) |
| Location |
|
|
|
|
Dammam | 46 (18.7) |
|
|
Madinah | 35 (14.2) |
|
|
Al Ahsa | 51 (20.7) |
|
|
Jeddah | 33 (13.4) |
|
|
Riyadh | 81 (32.9) |
| Type of facility |
|
|
|
|
Hospital | 228 (92.7) |
|
|
Primary health care clinic | 18 (7.3) |
aMNGHA: Ministry of National Guard Health Affairs.
General PHR Use Characteristics
The majority of HCPs were aware of MNGHA Care (225/246, 91.5%), had an account (213/246, 86.6%), used MNGHA Care (202/246, 82.1%), and recommended it to patients (198/246, 80.5%).
Measurement Model
The measurement model testing results are summarized in Table 3. After removing missing data, the usable sample for hypothesis testing was 246. The variance inflation factor of all items was below the threshold of 5, showing no evidence of multicollinearity. Item loadings were all above 0.40 and in the range of 0.70-0.93. Composite reliability was above the threshold of 0.70, showing good internal consistency. Moreover, the average variance extracted (AVE) of the constructs were greater than 0.50 and in the range of 0.55-0.81, indicating convergent validity.
Table 3.
Measurement model statistics.
| Construct and items | Mean | SD | VIFa | Loadings | CRb | AVEc | |
| Performance expectancy (PE) | 4.09 | 0.73 |
|
|
0.95 | 0.81 | |
|
|
PE1 |
|
|
2.526 | 0.87 |
|
|
|
|
PE2 |
|
|
3.792 | 0.92 |
|
|
|
|
PE3 |
|
|
3.711 | 0.92 |
|
|
|
|
PE4 |
|
|
3.462 | 0.90 |
|
|
| Effort expectancy (EE) | 3.75 | 0.67 |
|
|
0.79 | 0.55 | |
|
|
EE1 |
|
|
1.099 | 0.81 |
|
|
|
|
EE2 |
|
|
1.473 | 0.70 |
|
|
|
|
EE3 |
|
|
1.465 | 0.72 |
|
|
| Facilitating conditions (FC) | 3.60 | 0.78 |
|
|
0.88 | 0.71 | |
|
|
FC1 |
|
|
1.756 | 0.85 |
|
|
|
|
FC2 |
|
|
1.547 | 0.77 |
|
|
|
|
FC3 |
|
|
2.023 | 0.90 |
|
|
| Social influence (SI) | 3.82 | 0.69 |
|
|
0.85 | 0.74 | |
|
|
SI1 |
|
|
1.3 | 0.84 |
|
|
|
|
SI2 |
|
|
1.3 | 0.88 |
|
|
| Attitude (ATT) | 4.08 | 0.63 |
|
|
0.94 | 0.80 | |
|
|
ATT1 |
|
|
4.171 | 0.93 |
|
|
|
|
ATT2 |
|
|
3.603 | 0.92 |
|
|
|
|
ATT3 |
|
|
3.486 | 0.91 |
|
|
|
|
ATT4 |
|
|
2.029 | 0.83 |
|
|
| Behavioral intention (BI) |
|
|
|
|
|
|
|
|
|
BI | 4.18 | 0.68 |
|
1 | 1 | 1 |
aVIF: variance inflation factor.
bCR: composite reliability.
cAVE: average variance extracted.
Discriminant validity was tested using the Fornell–Larcker criterion. The square roots of the corresponding AVE are shown in italics, with each construct’s AVE higher than its highest correlation with any other construct (Table 4). Results in Tables 3 and 4 provide evidence of the validity and reliability of the constructs used in the model.
Table 4.
Discriminant validity of the constructs.a
| Constructs | 1 | 2 | 3 | 4 | 5 |
| Attitude | 0.896 |
|
|
|
|
| Effort expectancy | 0.697 | 0.742 |
|
|
|
| Facilitating conditions | 0.596 | 0.570 | 0.843 |
|
|
| Performance expectancy | 0.742 | 0.708 | 0.527 | 0.901 |
|
| Social influence | 0.646 | 0.671 | 0.645 | 0.602 | 0.860 |
aSquare roots of the corresponding average variance extracted are shown in italics.
Structural Model
The R2 was used to assess the structural model. Overall, the model explained 70% of the variance in the intention to recommend the PHR among HCPs (Figure 2). Table 5 presents the structural model results, while Table 6 presents the test for moderating effects.
Figure 2.
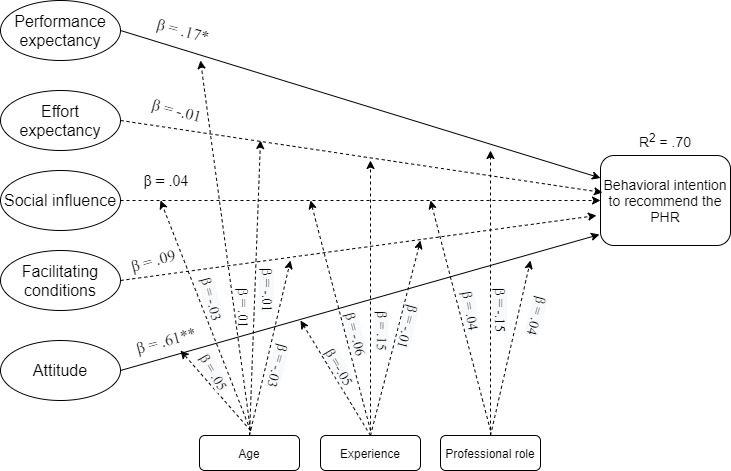
Structural model showing path coefficients (β) and coefficient of determination (R2) (*P<.05, **P<.01). PHR: personal health record.
Table 5.
Structural model results.
| Structural model | β | t-statisticsa (df) | P value | f 2 |
| PEb → BIc | .17 | 2.132 (499) | .03d | 0.035 |
| EEe → BI | –.01 | 0.166 (499) | .87 | 0 |
| SIf → BI | .04 | 0.473 (499) | .63 | 0.002 |
| FCg → BI | .09 | 1.241 (499) | .21 | 0.013 |
| ATTh → BI | .61 | 6.385 (499) | <.01 | 0.369 |
aTwo tailed.
bPE: performance expectancy.
cBI: intention to recommend PHR.
dP<.05.
eEE: effort expectancy.
fSI: social influence.
gFC: facilitating conditions.
hATT: attitude.
Table 6.
Moderation analysis results.
| Analysis | β | t-statisticsa (df) | P value | f 2 | |
| Moderation of age |
|
|
|
|
|
|
|
PEb × AGEc → BId | .01 | 0.118 (499) | .91 | 0 |
|
|
EEe × AGE → BI | –.01 | 0.159 (499) | .87 | 0 |
|
|
FCf × AGE → BI | –.03 | 0.360 (499) | .72 | 0.001 |
|
|
SIg × AGE → BI | .05 | 0.633 (499) | .53 | 0.003 |
|
|
ATTh × AGE → BI | –.03 | 0.307 (499) | .76 | 0.001 |
| Moderation of experience |
|
|
|
|
|
|
|
EE × EXPi → BI | .15 | 1.688 (499) | .09 | 0.016 |
|
|
SI × EXP → BI | –.06 | 0.609 (499) | .54 | 0.003 |
|
|
FC × EXP → BI | –.01 | 0.205 (499) | .84 | 0 |
|
|
ATT × EXP → BI | –.05 | 0.597 (499) | .55 | 0.003 |
| Moderation of professional role |
|
|
|
|
|
|
|
PE × HCPj → BI | –.15 | 1.598 (499) | .11 | 0.023 |
|
|
SI × HCP → BI | .04 | 0.620 (499) | .54 | 0.003 |
|
|
ATT × HCP → BI | .04 | 0.441 (499) | .66 | 0.002 |
aTwo tailed.
bPE: performance expectancy.
cAGE: age.
dBI: intention to recommend PHR.
eEE: effort expectancy.
fFC: facilitating conditions.
gSI: social influence.
hATT: attitude.
iEXP: experience.
jHCP: health care provider.
Discussion
Principal Findings
To the best of our knowledge, this is the first study to examine factors that influence HCPs’ intention to recommend PHRs to patients in the Kingdom of Saudi Arabia. Prior studies in the country evaluated the challenges in implementing PHRs and identified HCP resistance as a barrier [63,64]. Although HCPs are not the primary users of PHRs, their endorsement can positively influence patient engagement with this technology [12]. While some providers find promoting the PHR to be an additional burden, those providers who present a PHR to their patients as a tool to supplement their care can facilitate patient adoption [9]. Our study found a high level of awareness among HCPs, with 88.2% (217/246) having an account and 82.1% (202/246) recommending patients use the PHR. In our previous study in patients, HCPs and hospital staff were primarily responsible for recommending the PHR in 58.7% of patients who reported using MNGHA Care [18].
Predictors of patient adoption of PHRs may differ from those that affect HCPs to endorse a PHR [7,12]. Therefore, the research model for HCPs was slightly different from the one used for patients [18]. The proposed theoretical model explained 70% of the variance in HCPs’ behavioral intention to recommend PHRs to patients. Performance expectancy and attitude were significantly associated with behavioral intention to recommend the PHR. Much of the literature has shown performance expectancy as the strongest predictor of intention to use technology among HCPs [30,38,47]. In patient and consumer studies of PHRs, performance expectancy has also been a positive predictor of adoption [50,65-67]. However, the attitude was the strongest predictor of behavioral intention in our study. Other studies on PHR adoption have also found attitude to be an important predictor [47,51].
Our findings did not support the hypothesis that age, years of experience, and professional role moderate behavioral intention. Several studies have shown that older and more experienced HCPs are more resistant to health information technology and are less comfortable with using technology [35]. Physicians also have been found to be less enthusiastic about the introduction of eHealth services [33]. In our study, most had over 10 years of experience as an HCP (190/289, 65.7%) and more than 10 years in MNGHA (149/289, 51.6%). Furthermore, while Moll and Cajander [25] found differences in attitudes of HCPs who worked in primary care units compared with outpatient clinics, most HCPs in this study were from the hospital (265/284, 93.3%), limiting the ability to draw comparisons.
Implications for Theory
This research adds to the literature on HCPs’ acceptance of PHR using an adapted UTAUT model. To our knowledge, this is the first study to extend UTAUT with the construct of attitude in the context of HCPs’ acceptance of PHR. Only few studies evaluating HCPs’ acceptance of PHRs have used theory [68]. This study revealed that the adapted UTAUT model was a good predictive model of HCPs’ behavioral intention to recommend PHR use. While our model found that performance expectancy and attitude individually influence behavioral intention, it may also be the case that attitude mediates the relationship between performance expectancy and behavioral intention, as proposed by Dwivedi et al [40].
The original UTAUT explained 76% of the variance in behavioral intention. No studies on PHR adoption have used the original UTAUT model [50,65,66,69,70]. The advantage of the adapted model is a similar predictive power while parsimoniously eliminating the construct “use behavior” and the moderator “voluntariness” in the original model. Although the model explained 70% of the variance in behavioral intention and provided support for the proposed theoretical model, other factors may be important for HCPs’ acceptance of PHR. In the health care setting, UTAUT has been criticized for its focus on general technology acceptance factors and the inability to completely explain health information technology adoption [71]. Therefore, it is recommended that UTAUT be adapted to fit the health care context by incorporating health behavior theories, privacy and security issues, and negative factors that inhibit technology adoption [71].
Implications for Practice
This study provides practical contributions based on the proposed relationships and supports the need to focus on strategies to enhance perceived usefulness and a positive attitude toward the PHR in HCPs. While some patients view self-management as a burden and prefer the status quo [9], others will respond to HCP’s endorsement of the use of PHRs. Several studies identified HCP recommendation as an important factor in patients’ choosing to use PHRs [2,22,23,72,73]. Lyles et al [11] found one-on-one training to be the most effective intervention in PHR implementation in the United States. Providing short educational sessions to individuals or teams can facilitate acceptance among HCPs [48]. These training sessions could be conducted by each department. Training HCPs on the features available supports successful implementation by increasing skills and knowledge. Campaigns can also be directed at promoting awareness among HCPs. Through these interventions, HCPs will perceive the usefulness of PHRs and develop more positive attitudes regarding the benefits. Consequently, they will be more inclined to recommend PHRs to patients. Through their interactions with HCPs, patients will perceive PHRs as useful and are more likely to adopt them [66].
Limitations
There are several limitations to this study. While cross-sectional studies are useful for examining associations, a causal relationship cannot be established [74]. Snowball and convenience sampling, both nonprobability sampling strategies, were used to select participants, limiting generalizability; however, participants from multiple sites were selected to attain good representation across MNGHA. Self-administered online surveys are associated with various biases, including social desirability response bias, self-selection, and nonresponse bias [75]. To minimize social desirability response bias, participants had the option of not answering any question that made them uncomfortable. To minimize nonresponse bias, HCPs were contacted multiple times and offered an incentive to encourage a high response rate.
Recommendations for Future Research
Future studies should evaluate the proposed model in other contexts. This study involved a large integrated health care organization. Research in other organizations within the country and in this part of the world will increase the generalizability of our findings. Research should also be conducted in individual HCP groups. Differences in PHR acceptance have been observed based on a variety of characteristics, including age, gender, professional role, and practice setting. Future researchers should focus on HCP group–specific interventions. Finally, while this study used an open-ended question and checklist (analyzed separately) to achieve greater depth, one-on-one interviews would provide valuable data on the motivation of HCPs and nuances within this context.
Conclusion
This study examined factors affecting HCPs’ behavioral intention to recommend PHRs to patients in the Kingdom of Saudi Arabia. The proposed model accounted for 70% of the variance in behavioral intention, indicating significant predictive power. Performance expectancy and attitude were significant predictors of HCPs’ behavioral intention to support PHR use. Our results suggest that health care organizations should focus on strategies associated with these factors to improve HCP support and decrease barriers to patient use of PHRs. Future research should test this model and explore other predictors in order to develop successful interventions to encourage the adoption and continued use of the PHR among patients.
Acknowledgments
We thank the health care providers who participated in this study and acknowledge Dr Sherine Esmail and Mr Mansoor Ahmed Khan for their assistance in participant recruitment.
Abbreviations
- EHR
electronic health record
- HCP
health care provider
- HITECH
Health Information Technology for Economic and Clinical Health
- MNGHA
Ministry of National Guard Health Affairs
- PHR
personal health record
- TAM
technology acceptance model
- TPB
theory of planned behavior
- UTAUT
Unified Theory of Acceptance and Use of Technology
Footnotes
Conflicts of Interest: None declared
References
- 1.Petrovskaya O, Lau F, Antonio M. Synthesising evidence on patient portals: a protocol for an umbrella review. BMJ Open. 2019 Mar 30;9(3):e024469. doi: 10.1136/bmjopen-2018-024469. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=30928933 .bmjopen-2018-024469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gagnon M, Payne-Gagnon J, Breton E, Fortin J, Khoury L, Dolovich L, Price D, Wiljer D, Bartlett G, Archer N. Adoption of Electronic Personal Health Records in Canada: Perceptions of Stakeholders. Int J Health Policy Manag. 2016 Jul 01;5(7):425–433. doi: 10.15171/ijhpm.2016.36. http://europepmc.org/abstract/MED/27694670 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Markle Foundation Connecting for Health: A Public-Private Collaborative. The Personal Health Working Group Final Report. 2003. [2021-10-05]. https://www.markle.org/sites/default/files/final_phwg_report1.pdf .
- 4.Berwick D, Snair M, Nishtar S. Crossing the Global Health Care Quality Chasm: A Key Component of Universal Health Coverage. JAMA. 2018 Oct 02;320(13):1317–1318. doi: 10.1001/jama.2018.13696.2701790 [DOI] [PubMed] [Google Scholar]
- 5.Shah SD, Liebovitz D. It Takes Two to Tango: Engaging Patients and Providers With Portals. PM R. 2017 May;9(5S):S85–S97. doi: 10.1016/j.pmrj.2017.02.005.S1934-1482(17)30207-1 [DOI] [PubMed] [Google Scholar]
- 6.Tapuria A, Porat T, Kalra D, Dsouza G, Xiaohui S, Curcin V. Impact of patient access to their electronic health record: systematic review. Inform Health Soc Care. 2021 Jun 02;46(2):192–204. doi: 10.1080/17538157.2021.1879810. [DOI] [PubMed] [Google Scholar]
- 7.Abd-Alrazaq Alaa A, Bewick BM, Farragher T, Gardner P. Factors that affect the use of electronic personal health records among patients: A systematic review. Int J Med Inform. 2019 Jun;126:164–175. doi: 10.1016/j.ijmedinf.2019.03.014.S1386-5056(18)31225-5 [DOI] [PubMed] [Google Scholar]
- 8.Fraccaro V, Balatsoukas B, Peek VDV. MEDINFO 2017: Precision Health Care Through Informatics. Hangzhou, China: International Medical Informatics Association; 2017. [2021-10-05]. Patient portal adoption rates: A systematic literature review and meta-analysis. https://livrepository.liverpool.ac.uk/3043795/1/patient portal.pdf . [PubMed] [Google Scholar]
- 9.Zhao JY, Song B, Anand E, Schwartz D, Panesar M, Jackson GP, Elkin PL. Barriers, Facilitators, and Solutions to Optimal Patient Portal and Personal Health Record Use: A Systematic Review of the Literature. AMIA Annu Symp Proc. 2017;2017:1913–1922. http://europepmc.org/abstract/MED/29854263 . [PMC free article] [PubMed] [Google Scholar]
- 10.Ammenwerth E. From eHealth to ePatient: The Role of Patient Portals in Fostering Patient Empowerment. ejbi. 2018;14(2):20–23. doi: 10.24105/ejbi.2018.14.2.4. [DOI] [Google Scholar]
- 11.Lyles C, Nelson E, Frampton S, Dykes P, Cemballi A, Sarkar U. Using Electronic Health Record Portals to Improve Patient Engagement: Research Priorities and Best Practices. Annals of Internal Medicine. 2020 Jun 02;172(11_Supplement):S123–S129. doi: 10.7326/m19-0876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thompson M, Reilly J, Valdez R. Work system barriers to patient, provider, and caregiver use of personal health records: A systematic review. Appl Ergon. 2016 May;54:218–42. doi: 10.1016/j.apergo.2015.10.010.S0003-6870(15)30095-8 [DOI] [PubMed] [Google Scholar]
- 13.Niazkhani Z, Toni E, Cheshmekaboodi M, Georgiou A, Pirnejad H. Barriers to patient, provider, and caregiver adoption and use of electronic personal health records in chronic care: a systematic review. BMC Med Inform Decis Mak. 2020 Jul 08;20(1):153. doi: 10.1186/s12911-020-01159-1. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-020-01159-1 .10.1186/s12911-020-01159-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Agarwal R, Anderson C, Zarate J, Ward C. If we offer it, will they accept? Factors affecting patient use intentions of personal health records and secure messaging. J Med Internet Res. 2013 Feb 26;15(2):e43. doi: 10.2196/jmir.2243. https://www.jmir.org/2013/2/e43/ v15i2e43 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Assadi V, Hassanein K. Consumer Adoption of Personal Health Record Systems: A Self-Determination Theory Perspective. J Med Internet Res. 2017 Jul 27;19(7):e270. doi: 10.2196/jmir.7721. https://www.jmir.org/2017/7/e270/ v19i7e270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liu L, Miguel Cruz Antonio, Rios Rincon Adriana, Buttar V, Ranson Q, Goertzen D. What factors determine therapists' acceptance of new technologies for rehabilitation – a study using the Unified Theory of Acceptance and Use of Technology (UTAUT) Disabil Rehabil. 2015;37(5):447–55. doi: 10.3109/09638288.2014.923529. [DOI] [PubMed] [Google Scholar]
- 17.Kujala S, Hörhammer Iiris, Kaipio J, Heponiemi T. Health professionals' expectations of a national patient portal for self-management. Int J Med Inform. 2018 Sep;117:82–87. doi: 10.1016/j.ijmedinf.2018.06.005. https://linkinghub.elsevier.com/retrieve/pii/S1386-5056(18)30348-4 .S1386-5056(18)30348-4 [DOI] [PubMed] [Google Scholar]
- 18.Yousef CC, Thomas A, Alenazi AO, Elgadi S, Abu Esba LC, AlAzmi A, Alhameed AF, Hattan A, Almekhloof S, AlShammary MA, Alanezi NA, Alhamdan HS, Eldegeir M, Abulezz R, Khoshhal S, Masala CG, Ahmed O. Adoption of a Personal Health Record in the Digital Age: Cross-Sectional Study. J Med Internet Res. 2020 Oct 28;22(10):e22913. doi: 10.2196/22913. https://www.jmir.org/2020/10/e22913/ v22i10e22913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yousef CC, Salgado TM, Farooq A, Burnett K, McClelland LE, Thomas A, Alenazi AO, Abu Esba LC, AlAzmi A, Alhameed AF, Hattan A, Elgadi S, Almekhloof S, AlShammary MA, Alanezi NA, Alhamdan HS, Khoshhal S, DeShazo JP. Predicting Patients' Intention to Use a Personal Health Record Using an Adapted Unified Theory of Acceptance and Use of Technology Model: Secondary Data Analysis. JMIR Med Inform. 2021 Aug 17;9(8):e30214. doi: 10.2196/30214. https://medinform.jmir.org/2021/8/e30214/ v9i8e30214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Patel V, Abramson E, Edwards A, Cheung M, Dhopeshwarkar RV, Kaushal R. Consumer attitudes toward personal health records in a beacon community. Am J Manag Care. 2011 Apr;17(4):e104–20. https://www.ajmc.com/pubMed.php?pii=48672 .48672 [PubMed] [Google Scholar]
- 21.Kaelber DC, Jha AK, Johnston D, Middleton B, Bates DW. A research agenda for personal health records (PHRs) J Am Med Inform Assoc. 2008;15(6):729–36. doi: 10.1197/jamia.M2547. http://europepmc.org/abstract/MED/18756002 .M2547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nazi KM. The personal health record paradox: health care professionals' perspectives and the information ecology of personal health record systems in organizational and clinical settings. J Med Internet Res. 2013 Apr 04;15(4):e70. doi: 10.2196/jmir.2443. https://www.jmir.org/2013/4/e70/ v15i4e70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wiljer D, Urowitz S, Apatu E, DeLenardo C, Eysenbach G, Harth T, Pai H, Leonard KJ, Canadian Committee for Patient Accessible Health Records Patient accessible electronic health records: exploring recommendations for successful implementation strategies. J Med Internet Res. 2008 Oct 31;10(4):e34. doi: 10.2196/jmir.1061. https://www.jmir.org/2008/4/e34/ v10i4e34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wass S, Vimarlund V. Same, same but different: Perceptions of patients' online access to electronic health records among healthcare professionals. Health Informatics J. 2019 Dec;25(4):1538–1548. doi: 10.1177/1460458218779101. https://journals.sagepub.com/doi/10.1177/1460458218779101?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PubMed] [Google Scholar]
- 25.Moll J, Cajander Å. Oncology health-care professionals' perceived effects of patient accessible electronic health records 6 years after launch: A survey study at a major university hospital in Sweden. Health Informatics J. 2020 Jun;26(2):1392–1403. doi: 10.1177/1460458219881007. https://journals.sagepub.com/doi/10.1177/1460458219881007?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PubMed] [Google Scholar]
- 26.Venkatesh V, Morris MG, Davis GB, Davis FD. User Acceptance of Information Technology: Toward a Unified View. MIS Quarterly. 2003;27(3):425. doi: 10.2307/30036540. [DOI] [Google Scholar]
- 27.Venkatesh V, Thong JYL, Xu X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Quarterly. 2012;36(1):157. doi: 10.2307/41410412. [DOI] [Google Scholar]
- 28.Kohnke A, Cole ML, Bush R. Incorporating UTAUT Predictors for Understanding Home Care Patients' and Clinician's Acceptance of Healthcare Telemedicine Equipment. Journal of Technology Management & Innovation. 2014 Jul;9(2):29–41. doi: 10.4067/s0718-27242014000200003. [DOI] [Google Scholar]
- 29.Alaboudi A, Atkins A, Sharp B, Alzahrani M, Balkhair A, Sunbul T. Perceptions and attitudes of clinical staff towards telemedicine acceptance in Saudi Arabia. IEEE/ACS 13th International Conference of Computer Systems and Applications (AICCSA); November 29 to December 2, 2016; Agadir, Morocco. New York, NY: IEEE; 2016. pp. 1–8. [DOI] [Google Scholar]
- 30.Kim S, Lee K, Hwang H, Yoo S. Analysis of the factors influencing healthcare professionals' adoption of mobile electronic medical record (EMR) using the unified theory of acceptance and use of technology (UTAUT) in a tertiary hospital. BMC Med Inform Decis Mak. 2016 Jan 30;16:12. doi: 10.1186/s12911-016-0249-8. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-016-0249-8 .10.1186/s12911-016-0249-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nematollahi M, Moosavi A, Lazem M, Aslani N, Kafashi M, Garavand A. Factors Affecting in Adoption and Use of Electronic Medical Record Based on Unified Theory of Acceptance and Use of Technology in Iran. Shiraz E-Med J. 2017 Aug 27;18(9):e57582. doi: 10.5812/semj.57582. [DOI] [Google Scholar]
- 32.Mammen A, Weeks R. Electronic Medical Record (EMR) technology acceptance by healthcare professionals in South Africa. Proceedings of PICMET '14 Conference: Portland International Center for Management of Engineering and Technology; Infrastructure and Service Integration; July 27-31, 2014; Kanazawa, Japan. New York, NY: IEEE; 2014. pp. 3539–3548. [Google Scholar]
- 33.Hossain A, Quaresma R, Rahman H. Investigating factors influencing the physicians’ adoption of electronic health record (EHR) in healthcare system of Bangladesh: An empirical study. International Journal of Information Management. 2019 Feb;44:76–87. doi: 10.1016/j.ijinfomgt.2018.09.016. [DOI] [Google Scholar]
- 34.Venkatesh V, Sykes T, Zhang X. 'Just what the doctor ordered': A revised UTAUT for EMR system adoption and use by doctors. 2011 44th Hawaii International Conference on System Sciences; January 4-7, 2011; Kauai, HI. New York, NY: IEEE; 2011. pp. 1–10. [DOI] [Google Scholar]
- 35.Ibrahim S, Donelle L, Regan S, Sidani S. Predicting Registered Nurses' Behavioural Intention to Use Electronic Documentation System in Home Care: Application of an Adapted Unified Theory of Acceptance and Use of Technology Model. Nurs Leadersh (Tor Ont) 2019 Jun 28;32(2):48–70. doi: 10.12927/cjnl.2019.25961.cjnl.2019.25961 [DOI] [PubMed] [Google Scholar]
- 36.Jahanbakhsh M, Nazemi Z, Mohammadi F, Hasanzadeh A. A study of picture archiving and communication system adoption in one hospital: Applying the unified theory of acceptance and use of technology model. J Educ Health Promot. 2018;7:103. doi: 10.4103/jehp.jehp_149_17. http://www.jehp.net/article.asp?issn=2277-9531;year=2018;volume=7;issue=1;spage=103;epage=103;aulast=Jahanbakhsh .JEHP-7-103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bawack RE, Kala Kamdjoug JR. Adequacy of UTAUT in clinician adoption of health information systems in developing countries: The case of Cameroon. Int J Med Inform. 2018 Jan;109:15–22. doi: 10.1016/j.ijmedinf.2017.10.016.S1386-5056(17)30384-2 [DOI] [PubMed] [Google Scholar]
- 38.Ifinedo P. Technology acceptance by health professionals in Canada: an analysis with a modified UTAUT model. 2012 45th Hawaii International Conference on System Sciences; January 4-7, 2012; Maui, HI. New York, NY: IEEE; 2012. [DOI] [Google Scholar]
- 39.Venkatesh V, Thong J, Xu X. Unified Theory of Acceptance and Use of Technology: A Synthesis and the Road Ahead. JAIS. 2016 May;17(5):328–376. doi: 10.17705/1jais.00428. [DOI] [Google Scholar]
- 40.Dwivedi Y, Rana N, Jeyaraj A, Clement M, Williams M. Re-examining the Unified Theory of Acceptance and Use of Technology (UTAUT): Towards a Revised Theoretical Model. Inf Syst Front. 2017 Jun 8;21(3):719–734. doi: 10.1007/s10796-017-9774-y. [DOI] [Google Scholar]
- 41.Rosen P. The Effect of Personal Innovativeness in the Domain of Information Technology on the Acceptance and Use of Technology: A Working Paper. 2004. Jan, [2021-10-05]. https://www.researchgate.net/publication/228868534_The_effect_of_ personal_innovativeness_in_the_domain_of_information_technology_on_the_acceptance_and_use_of_technology .
- 42.Wu J, Du H. Toward a better understanding of behavioral intention and system usage constructs. European Journal of Information Systems. 2017 Dec 19;21(6):680–698. doi: 10.1057/ejis.2012.15. [DOI] [Google Scholar]
- 43.Williams MD, Rana NP, Dwivedi YK. The unified theory of acceptance and use of technology (UTAUT): a literature review. J Ent Info Manage. 2015 Apr 13;28(3):443–488. doi: 10.1108/JEIM-09-2014-0088. [DOI] [Google Scholar]
- 44.Balau M. Exploring the Link Between Intention and Behavior in Consumer Research. 2018. May, [2021-10-05]. https://www.researchgate.net/publication/325972981_Exploring_the_Link_between_Intention_and_Behavior_in_Consumer_Research .
- 45.Li J, Talaei-Khoei A, Seale H, Ray P, Macintyre CR. Health Care Provider Adoption of eHealth: Systematic Literature Review. Interact J Med Res. 2013;2(1):e7. doi: 10.2196/ijmr.2468. http://www.i-jmr.org/2013/1/e7/ v2i1e7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.MNGHA Organization Profile Ministry of National Guard - Health Affairs. 2018. [2019-09-06]. https://ngha.med.sa/English/AboutNGHA/Pages/profile.aspx .
- 47.Chung M, Ho C, Wen H. Predicting intentions of nurses to adopt patient personal health records: A structural equation modeling approach. Comput Methods Programs Biomed. 2016 Nov;136:45–53. doi: 10.1016/j.cmpb.2016.08.004.S0169-2607(16)30056-6 [DOI] [PubMed] [Google Scholar]
- 48.Hennemann S, Beutel ME, Zwerenz R. Ready for eHealth? Health Professionals' Acceptance and Adoption of eHealth Interventions in Inpatient Routine Care. J Health Commun. 2017 Mar 19;22(3):274–284. doi: 10.1080/10810730.2017.1284286. [DOI] [PubMed] [Google Scholar]
- 49.Hoogenbosch B, Postma J, de Man-van Ginkel JM, Tiemessen NA, van Delden JJ, van Os-Medendorp H. Use and the Users of a Patient Portal: Cross-Sectional Study. J Med Internet Res. 2018 Sep 17;20(9):e262. doi: 10.2196/jmir.9418. https://www.jmir.org/2018/9/e262/ v20i9e262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tavares J, Oliveira T. Electronic Health Record Patient Portal Adoption by Health Care Consumers: An Acceptance Model and Survey. J Med Internet Res. 2016 Mar;18(3):e49. doi: 10.2196/jmir.5069. http://www.jmir.org/2016/3/e49/ v18i3e49 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Khaneghah P, Miguel-Cruz A, Bentley P, Liu L, Stroulia E, Ferguson-Pell M. Users’ attitudes towards personal health records. Appl Clin Inform. 2017 Dec 16;07(02):573–586. doi: 10.4338/aci-2015-12-ra-0180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.QuestionPro. [2021-10-10]. https://www.questionpro.com/
- 53.Dünnebeil Sebastian, Sunyaev A, Blohm I, Leimeister JM, Krcmar H. Determinants of physicians' technology acceptance for e-health in ambulatory care. Int J Med Inform. 2012 Nov;81(11):746–60. doi: 10.1016/j.ijmedinf.2012.02.002.S1386-5056(12)00034-2 [DOI] [PubMed] [Google Scholar]
- 54.Davis FD, Bagozzi RP, Warshaw PR. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Management Science. 1989 Aug;35(8):982–1003. doi: 10.1287/mnsc.35.8.982. [DOI] [Google Scholar]
- 55.Ringle C, Sarstedt M, Straub D. Editor's Comments: A Critical Look at the Use of PLS-SEM in "MIS Quarterly". MIS Quarterly. 2012;36(1):iii. doi: 10.2307/41410402. [DOI] [Google Scholar]
- 56.Farooq A, Ahmad F, Khadam N, Lorenz B, Isoaho J. The impact of perceived security on intention to use e-learning among students. IEEE 20th International Conference on Advanced Learning Technologies (ICALT) 2020; July 6-9, 2020; Tartu, Estonia. 2020. pp. 360–364. [DOI] [Google Scholar]
- 57.Farooq A, Laato S, Islam A, Isoaho J. Understanding the impact of information sources on COVID-19 related preventive measures in Finland. Technology in Society. 2021 May;65:101573. doi: 10.1016/j.techsoc.2021.101573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kline RB. Principles and Practice of Structural Equation Modeling. New York, NY: Guilford Publications; 2015. [Google Scholar]
- 59.IBM Corporation . IBM SPSS Statistics for Windows. Armonk, NY: IBM Corporation; 2017. [2021-10-05]. https://www.ibm.com/in-en/products/spss-statistics . [Google Scholar]
- 60.Ringle C, Wende S, Becker J. SmartPLS 3.0. Hamburg, Germany: SmartPLS; 2014. [2021-10-05]. https://www.smartpls.com . [Google Scholar]
- 61.Hair JF, Risher JJ, Sarstedt M, Ringle CM. When to use and how to report the results of PLS-SEM. EBR. 2019 Jan 14;31(1):2–24. doi: 10.1108/ebr-11-2018-0203. [DOI] [Google Scholar]
- 62.Tavares J, Oliveira T. Electronic Health Record Portal Adoption: a cross country analysis. BMC Med Inform Decis Mak. 2017 Jul 05;17(1):97. doi: 10.1186/s12911-017-0482-9. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-017-0482-9 .10.1186/s12911-017-0482-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Al-Sahan A, Saddik B. Perceived challenges for adopting the Personal Health Record (PHR) at Ministry of National Guard Health Affairs (MNGHA)- Riyadh. Online J Public Health Inform. 2016;8(3):e205. doi: 10.5210/ojphi.v8i3.6845. http://europepmc.org/abstract/MED/28210426 .ojphi-08-e205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Alanazi A, Al Anazi Y. The challenges in personal health record adoption. Journal of Healthcare Management. 2019;64(2):104–109. doi: 10.1097/jhm-d-17-00191. [DOI] [PubMed] [Google Scholar]
- 65.Abd-Alrazaq A, Bewick B, Farragher T, Gardner P. Factors Affecting Patients' Use of Electronic Personal Health Records in England: Cross-Sectional Study. J Med Internet Res. 2019 Jul 31;21(7):e12373. doi: 10.2196/12373. https://www.jmir.org/2019/7/e12373/ v21i7e12373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Abd-Alrazaq A, Alalwan A, McMillan B, Bewick B, Househ M, Al-Zyadat A. Patients' Adoption of Electronic Personal Health Records in England: Secondary Data Analysis. J Med Internet Res. 2020 Oct 07;22(10):e17499. doi: 10.2196/17499. https://www.jmir.org/2020/10/e17499/ v22i10e17499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Hsieh H, Kuo Y, Wang S, Chuang B, Tsai C. A Study of Personal Health Record User's Behavioral Model Based on the PMT and UTAUT Integrative Perspective. Int J Environ Res Public Health. 2016 Dec 23;14(1):8. doi: 10.3390/ijerph14010008. https://www.mdpi.com/resolver?pii=ijerph14010008 .ijerph14010008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Macintosh CI. Healthcare Provider Attitudes and Experiences with Patient Use of Personal Health Records: Evaluation and Modification of the Unified Theory of Acceptance and Use of Technology. 2017. [2021-10-10]. https://tinyurl.com/3yrmptsh .
- 69.Park H, Kim KI, Soh J, Hyun Y, Jang S, Lee S, Hwang G, Kim H. Factors Influencing Acceptance of Personal Health Record Apps for Workplace Health Promotion: Cross-Sectional Questionnaire Study. JMIR Mhealth Uhealth. 2020 Jun 04;8(6):e16723. doi: 10.2196/16723. https://mhealth.jmir.org/2020/6/e16723/ v8i6e16723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Alsahafi Y, Gay V, Khwaji A. Factors affecting the acceptance of integrated electronic personal health records in Saudi Arabia: The impact of e-health literacy. Health Inf Manag. 2020 Nov 28;:1833358320964899. doi: 10.1177/1833358320964899. [DOI] [PubMed] [Google Scholar]
- 71.Alaiad A, Alsharo M, Alnsour Y. The Determinants of M-Health Adoption in Developing Countries: An Empirical Investigation. Appl Clin Inform. 2019 Oct 30;10(5):820–840. doi: 10.1055/s-0039-1697906. http://europepmc.org/abstract/MED/31667819 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Ryan BL, Brown JB, Terry A, Cejic S, Stewart M, Thind A. Implementing and Using a Patient Portal: A qualitative exploration of patient and provider perspectives on engaging patients. J Innov Health Inform. 2016 Jul 04;23(2):848. doi: 10.14236/jhi.v23i2.848. doi: 10.14236/jhi.v23i2.848. [DOI] [PubMed] [Google Scholar]
- 73.Vreugdenhil M, Ranke S, de Man Yvonne, Haan M, Kool R. Patient and Health Care Provider Experiences With a Recently Introduced Patient Portal in an Academic Hospital in the Netherlands: Mixed Methods Study. J Med Internet Res. 2019 Aug 20;21(8):13743. doi: 10.2196/13743. https://www.jmir.org/2019/8/13743/ v21i8e13743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Hulley S. Designing Clinical Research. Philadelphia, PA: Lippincott Williams & Wilkins; 2007. pp. 85–87. [Google Scholar]
- 75.Timmins F. Nursing Research Generating and Assessing Evidence for Nursing Practice. Nurse Education in Practice. 2013 Nov;13(6):e29. doi: 10.1016/j.nepr.2013.04.001. [DOI] [PubMed] [Google Scholar]