

Abstract
Background
Pathophysiology of rosacea is not completely understood and involves a complex interaction among genetics, ultraviolet (UV) light, microorganisms, impaired skin barrier, neuronal and vascular dysfunction, and immune system disruption.
Aims
To describe the etiology of rosacea with an emphasis on the role of UV radiation and exposome, and to review the importance of non‐pharmacologic strategies focusing on photoprotection.
Methods
We conducted a narrative review of the literature. We performed literature searches with PubMed from January 1990 to November 2020 using the keywords “rosacea”, “pathogenesis”, “ultraviolet radiation”, “exposome”, “photoprotection”, “sunscreens” and “non‐pharmacologic agents”. The search was limited to English, Spanish, and French language articles.
Results
Several environmental factors such as UV light, diverse microorganisms, air pollution, tobacco smoking, nutrition, and psychological stress showed to trigger or worsen rosacea. UV radiation was reported to induce pro‐inflammatory, pro‐angiogenic, and pro‐fibrotic responses. We found 6 original articles about the impact of sunscreens on rosacea. The use of sunscreens containing ingredients with emollient, anti‐inflammatory, and/or vasoregulatory properties was shown to significantly improve symptomatology.
Conclusion
UV radiation and the exposome play a key role in the development of rosacea. UV light is implicated in all significant aspects of rosacea: skin inflammation, neoangiogenesis, telangiectasia, and fibrosis, and may even initiate rosacea. While the use of sunscreens is widely recommended, the literature on the impact of photoprotection in rosacea is scarce. Adequately formulated sunscreens could not only provide the required level of photoprotection, but may also help to mitigate the barrier dysfunction, neutralize facial redness (tinted sunscreens), and decrease inflammation and vascular dysfunction.
Keywords: exposome, photoprotection, rosacea, sunscreens, ultraviolet radiation
1. INTRODUCTION
Rosacea is a chronic, inflammatory skin disorder, which most frequently affects fair‐skinned women. Rosacea prevalence can be highly variable, ranging from 1% to >20%. Rosacea is characterized by facial erythema, telangiectasia, erythematous papules, pustules, and flushing, among other manifestations. Patients complain about skin dryness, edema, stinging, itching, and burning sensations, 1 along with embarrassment and impairment of social life. Rosacea can produce a negative impact on quality of life and self‐esteem. 2
Pathophysiology of rosacea is not completely understood and involves a complex interaction among genetics, environmental factors, microorganisms, impaired skin barrier, neuronal and vascular dysfunction, and immune system disruption. 3 The exposome can be defined as the totality of environmental exposures in a lifetime, which can induce or modify diverse dermatoses. 4 The role of the exposome in rosacea must be highlighted: UV light, air pollution, tobacco smoking, nutrition, and psychological stress can trigger or worsen rosacea. Although UV exposure is one of the most commonly reported triggers and UV radiation can play a significant role in the pathogenesis of rosacea, 5 the literature on photoprotection in rosacea is relatively scarce. Furthermore, affected individuals typically react to diverse cosmetics and skincare products with stinging, burning, and worsening of rosacea. 6 While there is a wide range of available sunscreens, it can be difficult for patients and dermatologists to determine which sunscreens will be beneficial. The use of sunscreens containing ingredients with emollient, anti‐inflammatory, and vasoregulatory properties could not only ensure the required level of photoprotection, but may also have the potential to mitigate the barrier dysfunction, neutralize facial redness (using green pigment as camouflage), and decrease inflammation and vascular dysfunction.
Here, we discuss the etiology of rosacea with emphasis on the role of UV radiation and the exposome, and review the importance of non‐pharmacologic strategies with a focus on photoprotection.
2. METHODS
We conducted a narrative review of the literature. We performed literature searches with PubMed from January 1990 to November 2020 using the keywords (non‐MeSH) “rosacea”, “pathogenesis”, “ultraviolet radiation”, “exposome”, “photoprotection”, “sunscreens” and “non‐pharmacologic agents”. The search was limited to English, Spanish, and French language articles. Articles were selected depending on their relevance.
3. RESULTS AND DISCUSSIONS
3.1. Pathophysiology of rosacea
Rosacea seems to develop from dysregulation of innate and adaptive immune systems and/or neurovascular dysfunction, disrupted skin barrier, and genetic predisposition. The exposome can play a significant role in inducing this impaired immune or neurovascular response.
3.1.1. Genetic predisposition
The genetic contribution to the development of this disorder is estimated to be 46%. 7 Chang et al. 8 identified one single nucleotide polymorphism (rs763035) and three major histocompatibility complex class II alleles (HLA‐DRB1*, HLA‐DQB1*, and HLA‐DQA1*) associated with rosacea.
3.1.2. Microorganisms and the gut‐skin axis
Recent evidence suggests a significant role of the cutaneous and gut microbiome. Small intestinal bacterial overgrowth, Helicobacter pylori infection, presence of b‐hemolytic Staphylococcus epidermidis, and increased density of Demodex folliculorum, among other microorganisms, have been implicated in chronic skin inflammation and in the genesis of rosacea. 9
3.1.3. Impaired skin barrier
The lesional skin of rosacea patients can present lower skin conductivity, lower water content, and higher transepidermal water loss. 10 Impaired barrier function may promote skin bacterial colonization and inflammation. 10
3.1.4. Dysregulation of Immune response
Rosacea patients present higher levels of metalloproteinases (MMPs) and overexpression of Toll‐like receptor 2 (TLR2). TLR2 activates the innate immune system in response to infection/infestation, such as the presence of Demodex. 3 Activation of the innate immune system leads to the release of pro‐inflammatory cytokines and antimicrobial proteins such as cathelicidin. Cathelicidin is then cleaved into its active form, LL37, which induces degranulation of mast cells and secretion of multiple pro‐inflammatory and pro‐angiogenic molecules. 3
3.1.5. Neurovascular dysregulation
Activation of transient receptor potential (TRP) cation channels leads to the release of vasoregulatory neuropeptides calcitonin gene‐related peptide and substance P. Both peptides can induce flushing. The TRP vanilloid 1 (TRPV1) is overexpressed in rosacea patients and is activated by heat, capsaicin, and inflammation. TRP ankyrin 1 (TRPA1) can be activated by cold, mustard oil, and formalin. 11
3.1.6. The exposome
As stated before, the exposome can be defined as the totality of environmental exposures of an individual in a lifetime and how those exposures relate to health. Herein, we will describe the most relevant exposome factors involved in the pathophysiology of rosacea.
The role of ultraviolet radiation
UV radiation is one of the most frequently reported triggers of rosacea. 2 The tendency of this disorder to affect the central face may be influenced by the exposure of convex surfaces of the face to UV light. 3 Sun‐protected areas, such as the submental and supraorbital areas, are usually spared. Lifetime UV radiation exposure has been shown to be significantly associated with the presence of rosacea and is the single most important environmental variable. 7
UVB radiation has significant angiogenic properties and can upregulate the expression of vascular endothelial growth factor, and increase endothelial cell proliferation within existing blood vessels, leading to telangiectasia and new blood vessels in animal models. 3 Chronic UVA exposure can induce MMP‐1 overexpression, a metalloproteinase associated with dermal collagen degeneration in rosacea. 11
UV irradiation can induce an imbalance between oxidant and antioxidant pathways, such as increased serum peroxide and decreased tissue superoxide dismutase observed in rosacea. 12 UV radiation produces reactive oxygen species (ROS), which can induce the release of pro‐inflammatory cytokines by fibroblasts and keratinocytes. ROS levels are higher in patients with rosacea than in controls, and ROS can increase inflammatory response in these individuals. 11 UV irradiation can also induce endoplasmic reticulum stress leading to activation of TLR2, a mechanism through which UV could trigger innate immune responses in rosacea. Furthermore, UV irradiation may increase the expression of myeloid differentiation factor 88 (MyD88), an adaptor molecule for TLR signaling. 11
Cathelicidin LL‐37 contributes to enhanced photosensitivity in rosacea: It augments the pro‐inflammatory and pro‐angiogenic effects of UV radiation, increasing the release of IL‐1β and augmenting the angiogenic potential of endothelial cells. 13 The link between UV radiation and the onset of inflammation mediated by the innate immune system has recently been described by Kulkarny et al. 5 : UVB induces keratinocyte damage, leading to the release of cathelicidin LL‐37 and double‐stranded RNA. This complex increases endothelial cell expression of adhesion molecules such as ICAM and VCAM, promoting an influx of neutrophils and monocytes into the dermis (Figure 1). These findings suggest that UV light can not only act as a trigger, but it may also initiate rosacea.
FIGURE 1.
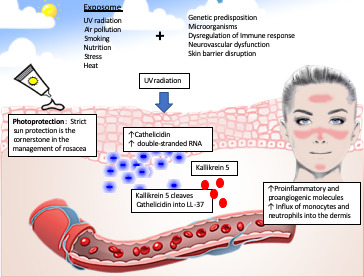
Role of ultraviolet radiation and exposome in the pathophysiology of rosacea. Pathophysiology of rosacea includes a complex interaction among genetics, ultraviolet light (UV), microorganisms, impaired skin barrier, neuronal and vascular dysfunction, and immune system disruptions. UVB radiation induces keratinocyte damage, leading to the release of cathelicidin LL‐37 and double‐stranded RNA. This complex increases endothelial cell expression of adhesion molecules, promoting an influx of neutrophils and monocytes into the dermis. Cathelicidin LL‐37 also promotes angiogenesis, the release of pro‐inflammatory cytokines and metalloproteinases, and leukocyte chemotaxis
The contribution of visible light (VL) in the pathogenesis of rosacea needs to be addressed. We have not found studies on the role of VL in this dermatosis, although VL has been linked to diverse photoaggravated disorders such as melasma, postinflammatory hyperpigmentation, cutaneous porphyrias, and solar urticaria. 14 Furthermore, VL can trigger immediate erythema in light‐skinned individuals, through a synergistic effect with UVA1. 15
In summary, UV radiation is implicated in all key aspects of rosacea (Table 1): skin inflammation, neoangiogenesis, telangiectasia, and fibrosis.
TABLE 1.
The role of ultraviolet radiation in the pathogenesis of rosacea
| Epidemiological characteristics |
UV radiation is one of the most frequently reported triggers of rosacea Lifetime UV radiation exposure is the single most important environmental variable associated with rosacea |
| Pro‐angiogenic and pro‐inflammatory effects |
Augmented expression of VEGF, and increase endothelial cell proliferation within existing blood vessels Cathelicidin LL‐37 augments the pro‐inflammatory and pro‐angiogenic effects of UV radiation, increasing the release of IL‐1β and incrementing the angiogenic potential of endothelial cells |
| Activation of innate immune system | UVB radiation induces keratinocyte damage, leading to the release of cathelicidin LL‐37 and double‐stranded RNA. This complex increases endothelial cell expression of adhesion molecules such as ICAM and VCAM, promoting an influx of neutrophils and monocytes into the dermis |
| Induction of collagen dermal degeneration and fibrosis | Chronic UVA exposure can induce MMP‐1 overexpression |
| Generation of reactive oxygen species |
UV irradiation can induce an imbalance between oxidant and antioxidant pathways: increased serum peroxide and decreased tissue superoxide dismutase ROS levels are higher in patients with rosacea than in controls |
Abbreviations: ICAM, intracellular adhesion molecule‐1; IL, interleukin; MMP, metalloproteinase; ROS, reactive oxygen species; UV, ultraviolet; VEGF, vascular endothelial growth factor.
Air pollution and smoking
The impact of air pollution on skin aging, pigmentation, and cutaneous diseases has been highlighted in recent years. 4 Outdoor air pollutants can be significantly associated with increased severity of symptoms in atopic dermatitis. 16 Traffic exhaust emissions seem to affect both skin barrier function and activation of immune responses. 16 UV light and air pollutants can have a synergic detrimental effect on the skin; this combination can induce significant cytotoxic and genotoxic damage. 4 While the impact of air pollution in rosacea remains to be determined, a recent study found a significantly increased risk of developing erythematous telangiectatic rosacea among smokers. 17 Volatile substances contained in cigarettes are likely to induce this erythematous condition (Table 2). 17
TABLE 2.
Impact of the exposome on rosacea patients
| Exposure | |
|---|---|
| UV radiation |
Can exacerbate or initiate rosacea: Triggers the inflammasome Increases oxidative stress Induces vasodilation |
| Air pollution |
UV light and air pollutants have a synergistic detrimental effect Induces significant cytotoxic and genotoxic damage |
| Tobacco smoking | Increased risk of developing rosacea |
| Nutrition |
Triggers: alcohol, hot beverages, spicy food (capsaicin), fatty food, and those containing cinnamaldehyde such as chocolate, tomatoes, and citrus Protectors: increased coffee consumption |
| Psychological factors |
Stress is a frequently reported trigger Can induce an hyper‐responsiveness in sympathetic nerve activity in the supraorbital skin |
It seems reasonable to advise patients to avoid ambient air pollutants when possible.
Nutrition
Regarding the impact of nutrition on rosacea, patients report certain foods as triggers such as spicy food (capsaicin), fatty food, those containing cinnamaldehyde (chocolate tomatoes and citrus 15 ), alcohol, and hot beverages 18 as triggers. 19 Capsaicin and cinnamaldehyde can trigger TRP and promote vasodilation and flushing. 11 In contrast, increased coffee consumption seems to be inversely associated with the risk of incident rosacea, perhaps due to the high concentration of polyphenols found in coffee, which have antioxidant, anti‐inflammatory, and vascular effects. 20
Stress
Mental stress is one of the most frequently reported triggers by rosacea patients. Stress can increase the levels of corticosterone and the adrenocorticotropic hormone and activate the hypothalamic‐pituitary‐adrenal axis. Cortisol‐releasing hormone (CRH) acts as a direct vasodilator and induces the degranulation of mast cells and the release of vasodilatory mediators, such as nitric oxide and histamine. CRH increases the levels of pro‐inflammatory cytokines including IL‐6, IL‐8, and IL‐18. 11 IL‐8 impairs collagen production and stimulates the activity of MMP and epidermal water loss. 4 Mental stress can induce a hyper‐responsiveness in sympathetic nerve activity in the supraorbital skin of rosacea patients and may cause neurovascular dysregulation and local inflammation. 11
Heat
Heat is commonly reported as an exacerbating factor in rosacea. Individuals exposed to heat from using a tandoor oven exhibited a significantly higher incidence of rosacea than control subjects. 21 Heat can activate TRPV1 and ankyrin 1, leading to vascular deregulation, flushing, and neurogenic leukocyte inflammation. 11
3.2. Non‐pharmacologic treatment
3.2.1. Cleansers
Recent evidence suggests that excessive cleansing can induce rosacea. High frequency of cleansing (more than once daily), 22 , 23 the usage of foaming cleansers, 23 a high quantity of cleansers, 22 long baths (≥11 min), 24 overuse of cleansing tool (more than four times/week), 22 daily exfoliating activity, 22 or sessions of deep cleansing treatment in beauty salons 22 presented a positive correlation with rosacea. Excessive cleansing may induce mechanical damage and chemical irritation to the stratum corneum and alter the normal cutaneous pH. 23
As general skin care, the use of soap‐free gentle facial cleansers, no more than once daily, must be encouraged. 23 As the skin barrier is already damaged in rosacea, any procedure or ingredient known to disrupt it should be avoided. Products containing ingredients likely to induce irritant or allergic contact dermatitis (camphor, menthol, eucalyptus oil, peppermint, witch hazel, or antiseptics) should not be recommended. 25
3.2.2. Moisturizers
Rosacea patients often suffer from dry facial skin, and non‐oily moisturizers must be indicated. These products can repair the damaged skin barrier, relieve dry skin, improve skin homeostasis, 19 , 26 and may reduce the risk of rosacea onset. 23 Unfortunately, these individuals frequently report worsening of symptoms or heightened cutaneous sensitivity to skin care products, and allergic contact dermatitis is identified in 30% to 40% of cases. 27 , 28 This is why a skin care regimen should be as simple as possible, preferring cosmetically pleasing moisturizers without fragrance that have been developed to minimize the risk of irritant or allergic contact dermatitis. 23
3.2.3. Photoprotection
Strict sun protection is the cornerstone of management of rosacea. Daily use of a very high‐tolerance broad‐spectrum sunscreen with a minimum SPF of 30 is necessary. 1 , 29 Studies comparing the effects of different sunscreens on rosacea are lacking. Some authors recommend sunscreens containing physical or mineral filters with zinc oxide and/or titanium dioxide. 29 These physical sunscreens are usually well‐tolerated, although patient adherence can be low, because some can leave a white layer on the skin after application. The selection of the texture of the sunscreen is relevant so as to ensure that the product is easy and gentle to apply and cosmetically acceptable. In facial care of rosacea, hydrophilic formulations such as water‐based sunscreens are recommended more than oil‐enriched formulations, which can lead to heat accumulation and a worsening of dermatosis. Additives such as emollients and/or ingredients with anti‐inflammatory, skin‐calming, or vessel‐stabilizing properties should be considered. 6 Among these substances, dimethicone or Cyclomethicone can mitigate facial irritation. 25 Facial cosmeceuticals such as derivatives from Ginkgo biloba, Aloe vera, allantoin, feverfew, Glycyrrhiza inflata, and niacinamide have anti‐inflammatory/antioxidant properties and can be useful in the treatment of rosacea 30 and may be added to sunscreen formulations. Topically applied polyphenols extracted from green tea or other plants present anti‐inflammatory, antiangiogenic, and antioxidant properties. Polyphenols such as Silybum marianum (Silymarin), Chrysanthemum indicum, Quassia amara extract, and Glycyrrhiza Inflata root extract may be beneficial in reducing rosacea symptoms. 31 Topically applied kinetin (N6‐furfuryladenine), a plant cytokinin that may help to restore the skin barrier function, has demonstrated a beneficial effect in reducing erythema in mild‐to‐moderate rosacea. 32 Ectoine, a marine‐derived molecule, is an effective long‐term moisturizer, which prevents epidermal dehydration, reduces cutaneous inflammation, and protects DNA from damage by ionizing radiation, 33 and can be found in high‐tolerance sunscreens.
We found six original articles about the impact of sunscreens on rosacea. A recent open‐label study using a novel water‐based sunscreen SPF 50+ containing two emollients found significantly less erythema, dryness, and scaling after 21 days of use. Subjects reported significantly less tension, dryness, and tickling. 34 A sunscreen containing sodium sulfacetamide 10% and sulfur 5% cream showed a greater percentage reduction in inflammatory lesions in a clinical trial compared with metronidazole 0.75% cream, as well as a significantly greater percentage of subjects with improved erythema. 35 A tinted daily SPF 30 facial moisturizer showed to improve the skin appearance and symptoms of skin dryness of rosacea‐prone patients, reduced transepidermal water loss, and increased electrical capacitance. 36 A skin care regimen (cleanser, day care with SPF25 and night care) containing Glycyrrhiza Inflata root extract and 4‐t‐butylcyclohexanol was effective in improving signs of rosacea in patients with rosacea subtype I. 37 4‐t‐butylcyclohexanol and Glycyrrhiza Inflata root extract can significantly reduce TRPV1 activation and prostaglandin E2 secretion, respectively. 38 An open‐label study showed that the combination of UV filters together with cholesterol, trehalose, and ceramide, and anti‐inflammatory ingredients such as bisabolol, Echinacea angustifolia extract, Boswellia serrate resin extract, and esculin significantly reduced the erythema index and mean transepidermal water loss. 39 Tinted sunscreens using different concentrations of iron oxide, pigmentary titanium dioxide, and/or zinc oxide have shown to be effective in protecting against visible light. 14
Cosmetic camouflage can be very important in patients with rosacea. Camouflage therapy can give immediate satisfaction to patients and may reduce the impact of the disease on the quality of life. The use of green pigment as an ingredient in sunscreens can also impact positively on patient appearance. 30
The use of oral photoprotection has not yet been evaluated in rosacea. Polypodium leucotomos (PL) extract in combination with green tea polyphenols presents anti‐inflammatory, anticarcinogenic, and antioxidant properties and has been used in photoaggravated dermatoses. This combination allows better tolerance to ultraviolet exposure and increases the minimal erythema dose, 40 and so might be an option for rosacea patients who have intolerance to sun exposure or engage in extensive outdoor activities.
In summary, topical sunscreens must be indicated for all rosacea patients, deciding which, however, among the vast range of products can be challenging. Products with broadband UV protection, water‐based sunscreens, easy to remove, and containing ingredients with emollient, anti‐inflammatory, antioxidant, and vasoregulatory properties should be preferred (Table 3). The use of tinted sunscreens or those containing green pigment for camouflage could be considered and discussed with the patient.
TABLE 3.
Characteristics of recommended sunscreens in rosacea
| Sun protection factor | Broad spectrum (≥SPF 30+) |
| Formula | High‐tolerance water‐based formula, easy to apply, and remove |
| Other active ingredients | Should contain ingredients with emollient, anti‐inflammatory, skin barrier repair activity, or vasoregulatory properties |
| Color |
Sunscreens containing green pigment should be considered as they can impact positively on patient appearance Tinted sunscreens containing formulations of iron oxides, pigmentary titanium dioxide, and zinc oxide can protect against visible light |
| Camouflage | Use of cosmetic camouflage with UV filters can give immediate satisfaction to patients and may reduce the impact of rosacea on quality of life |
4. CONCLUSION
The exposome can negatively impact on rosacea patients. Avoidance and/or protection (when possible) from known triggers such as environmental and emotional stimuli, and certain food should be recommended. Among these factors, UV radiation is crucial in the pathogenesis of rosacea. The appropriate skin care, use of moisturizers, and adequately formulated sunscreens are the cornerstone of treatment. Sunscreens can not only provide the required UV protection, but may also have the potential to moisturize the skin, repair the disrupted cutaneous barrier, reduce inflammation, and provide camouflage.
CONFLICT OF INTEREST
DM reported no conflict of interest, JP is a consultant for ISDIN, and CG and CT are employed by ISDIN who financed the publication expenses.
5. ETHICS STATEMENT
We declare that this is an original and not previously published paper, and all contributions to the work are reported in the manuscript according to ICJME guidelines. There are no conflicts of interest to disclose.
Funding information
ISDIN financed the publication expenses
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- 1. Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269‐1276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: The 2017 update by the national rosacea society expert committee. J Am Acad Dermatol. 2018;78:148‐155. [DOI] [PubMed] [Google Scholar]
- 3. Ahn CS, Huang WW. Rosacea pathogenesis. Dermatol Clin. 2018;36:81‐86. [DOI] [PubMed] [Google Scholar]
- 4. Passeron T, Krutmann J, Andersen ML, Katta R, Zouboulis CC. Clinical and biological impact of the exposome on the skin. J Eur Acad Dermatol Venereol. 2020;34(Suppl 4):4‐25. [DOI] [PubMed] [Google Scholar]
- 5. Kulkarni NN, Takahashi T, Sanford JA, et al. Innate immune dysfunction in rosacea promotes photosensitivity and vascular adhesion molecule expression. J Invest Dermatol. 2020;140:645‐655.e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kresken J, Kindl U, Wigger‐Alberti W, Clanner‐Engelshofen BM, Reinholz M. Dermocosmetics for use in rosacea: guideline of the society for dermopharmacy. Skin Pharmacol Physiol. 2018;31:147‐154. [DOI] [PubMed] [Google Scholar]
- 7. Aldrich N, Gerstenblith M, Fu P, et al. Genetic vs environmental factors that correlate with rosacea: a cohort‐based survey of twins. JAMA Dermatol. 2015;151:1213‐1219. [DOI] [PubMed] [Google Scholar]
- 8. Chang ALS, Raber I, Xu J, et al. Assessment of the genetic basis of rosacea by genome‐wide association study. J Invest Dermatol. 2015;135:1548‐1555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Searle T, Ali FR, Carolides S, Al‐Niaimi F. Rosacea and the gastrointestinal system. Australas J Dermatol. 2020;61:307‐311. [DOI] [PubMed] [Google Scholar]
- 10. Yuan C, Ma Y, Wang Y, et al. Rosacea is associated with conjoined interactions between physical barrier of the skin and microorganisms: a pilot study. J Clin Lab Anal. 2020;34:e23363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Woo YR, Lim JH, Cho DH, Rosacea PHJ. Molecular mechanisms and management of a chronic cutaneous inflammatory condition. Int J Mol Sci. 2016;17:1562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tisma VS, Basta‐Juzbasic A, Jaganjac M, et al. Oxidative stress and ferritin expression in the skin of patients with rosacea. J Am Acad Dermatol. 2009;60:270‐276. [DOI] [PubMed] [Google Scholar]
- 13. Salzer S, Kresse S, Hirai Y, et al. Cathelicidin peptide LL‐37 increases UVB‐triggered inflammasome activation: possible implications for rosacea. J Dermatol Sci. 2014;76:173‐179. [DOI] [PubMed] [Google Scholar]
- 14. Lyons AB, Trullas C, Kohli I, Hamzavi IH, Lim HW. Photoprotection beyond ultraviolet radiation: a review of tinted sunscreens. J Am Acad Dermatol. 2020. 10.1016/j.jaad.2020.04.079. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 15. Kohli I, Zubair R, Lyons AB, et al. Impact of long‐wavelength ultraviolet al and visible light on light‐skinned individuals. Photochem Photobiol. 2019;95:1285‐1287. [DOI] [PubMed] [Google Scholar]
- 16. Krämer U, Behrendt H. Air pollution and atopic eczema: systematic review of findings from environmental epidemiological studies. Hautarzt Z Dermatol Venerol Verwandte Geb. 2019;70:169‐184. [DOI] [PubMed] [Google Scholar]
- 17. Kucukunal A, Altunay I, Arici JE, Cerman AA. Is the effect of smoking on rosacea still somewhat of a mystery? Cutan Ocul Toxicol. 2016;35:110‐114. [DOI] [PubMed] [Google Scholar]
- 18. Yuan X, Huang X, Wang B, et al. Relationship between rosacea and dietary factors: a multicenter retrospective case‐control survey. J Dermatol. 2019;46:219‐225. [DOI] [PubMed] [Google Scholar]
- 19. Draelos ZD, Ertel K, Berge C. Niacinamide‐containing facial moisturizer improves skin barrier and benefits subjects with rosacea. Cutis. 2005;76:135‐141. [PubMed] [Google Scholar]
- 20. Li S, Chen ML, Drucker AM, et al. Association of caffeine intake and caffeinated coffee consumption with risk of incident rosacea in women. JAMA Dermatol. 2018;154:1394‐1400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ozkol HU, Calka O, Akdeniz N, Baskan E, Ozkol H. Rosacea and exposure to tandoor heat: is there an association? Int J Dermatol. 2015;54:1429‐1434. [DOI] [PubMed] [Google Scholar]
- 22. Li G, Wang B, Zhao Z, et al. Excessive cleansing: an underestimating risk factor of rosacea in Chinese population. Arch Dermatol Res. 2020. 10.1007/s00403-020-02095-w. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 23. Huang Y‐X, Li J, Zhao Z‐X, et al. Effects of skin care habits on the development of rosacea: a multi‐center retrospective case‐control survey in Chinese population. PLoS One. 2020;15:e0231078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Zuo Z, Wang B, Shen M, et al. Skincare habits and rosacea in 3,439 Chinese adolescents: a university‐based cross‐sectional study. Acta Derm Venereol. 2020;100:adv00081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. van Zuuren EJ. Rosacea. N Engl J Med. 2017;377:1754‐1764. [DOI] [PubMed] [Google Scholar]
- 26. Santoro F, Lachmann N. An open‐label, intra‐individual study to evaluate a regimen of three cosmetic products combined with medical treatment of rosacea: cutaneous tolerability and effect on hydration. Dermatol Ther. 2019;9:775‐784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Erdogan HK, Bulur I, Saracoglu ZN, Bilgin M. The evaluation of contact sensitivity with standard and cosmetic patch test series in rosacea patients. Ann Dermatol. 2018;30:290‐295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Corazza M, la Malfa W, Lombardi A, Maranini C, Virgili A. Role of allergic contact dermatitis in rosacea. Contact Dermatitis. 1997;37:40‐41. [DOI] [PubMed] [Google Scholar]
- 29. Reinholz M, Tietze JK, Kilian K, et al. Rosacea ‐ S1 guideline. J Dtsch Dermatol Ges. 2013;11:768‐780; 768‐779. [DOI] [PubMed] [Google Scholar]
- 30. Draelos ZD. Cosmeceuticals for rosacea. Clin Dermatol. 2017;35:213‐217. [DOI] [PubMed] [Google Scholar]
- 31. Saric S, Clark AK, Sivamani RK, Lio PA, Lev‐Tov HA. The role of polyphenols in rosacea treatment: a systematic review. J Altern Complement Med. 2017;23:920‐929. [DOI] [PubMed] [Google Scholar]
- 32. Wu JJ, Weinstein GD, Kricorian GJ, Kormeili T, McCullough JL. Topical kinetin 0.1% lotion for improving the signs and symptoms of rosacea. Clin Exp Dermatol. 2007;32:693‐695. [DOI] [PubMed] [Google Scholar]
- 33. Alves A, Sousa E, Kijjoa A, Pinto M. Marine‐derived compounds with potential use as cosmeceuticals and nutricosmetics. Mol Basel Switz. 2020;25:2536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Grivet‐Seyve M, Santoro F, Lachmann N. Evaluation of a novel very high sun‐protection‐factor moisturizer in adults with rosacea‐prone sensitive skin. Clin Cosmet Investig Dermatol. 2017;10:211‐219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Torok HM, Webster G, Dunlap FE, Egan N, Jarratt M, Stewart D. Combination sodium sulfacetamide 10% and sulfur 5% cream with sunscreens versus metronidazole 0.75% cream for rosacea. Cutis. 2005;75:357‐363. [PubMed] [Google Scholar]
- 36. Baldwin H, Santoro F, Lachmann N, Teissedre S. A novel moisturizer with high sun protection factor improves cutaneous barrier function and the visible appearance of rosacea‐prone skin. J Cosmet Dermatol. 2019;18:1686‐1692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Schoelermann AM, Weber TM, Arrowitz C, Rizer RL, Qian K, Babcock M. Skin compatibility and efficacy of a cosmetic skin care regimen with licochalcone A and 4‐t‐butylcyclohexanol in patients with rosacea subtype I. J Eur Acad Dermatol Venereol. 2016;30(Suppl 1):21‐27. [DOI] [PubMed] [Google Scholar]
- 38. Sulzberger M, Worthmann A‐C, Holtzmann U, et al. Effective treatment for sensitive skin: 4‐t‐butylcyclohexanol and licochalcone A. J Eur Acad Dermatol Venereol. 2016;30(Suppl 1):9‐17. [DOI] [PubMed] [Google Scholar]
- 39. Sparavigna A, Tenconi B, De Ponti I. Preliminary open‐label clinical evaluation of the soothing and reepithelialization properties of a novel topical formulation for rosacea. Clin Cosmet Investig Dermatol. 2014;7:275‐283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Granger C, Aladren S, Delgado J, Garre A, Trullas C, Gilaberte Y. Prospective evaluation of the efficacy of a food supplement in increasing photoprotection and improving selective markers related to skin photo‐ageing. Dermatol Ther. 2020;10:163‐178. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.