

Abstract
Background
The prognosis of pancreatic cancer (PC) has been improved by new chemotherapy regimens (combination of 5-fluorouracil, oxaliplatin, irinotecan, and leucovorin (FOLFIRINOX) or gemcitabine plus nab-paclitaxel (GnP)). Unfortunately, chemotherapy-induced peripheral neuropathy (CIPN) is a common adverse event of these two regimens. The efficacy of pregabalin for CIPN has been reported in previous studies. However, the efficacy of mirogabalin for CIPN remains unknown. Thus, in this study, we aimed to clarify which drug (mirogabalin or pregabalin) was more valuable for improving CIPN.
Methods
A total of 163 PC patients who underwent FOLFIRINOX or GnP between May 2014 and January 2021 were enrolled. Among them, 34 patients were diagnosed with CIPN. Thirteen patients were treated with mirogabalin (mirogabalin group), and twenty-one patients were treated with pregabalin (pregabalin group). Treatment efficacy was compared between the two groups.
Results
In both the mirogabalin group and the pregabalin group, the grade of patients with CIPN at 2, 4, and 6 weeks after the initiation of treatment showed significant improvement compared to the pretreatment grade. Notably, the rate of CIPN improvement was higher in the mirogabalin group than in the pregabalin group (2 weeks: 84.6% (11/13) vs 33.3% (7/21), P value = 0.005; 4 weeks, 6 weeks: 92.3% (12/13) vs 33.3% (7/21), P value = 0.001).
Conclusions
Although both mirogabalin and pregabalin were effective at improving CIPN, mirogabalin might be a suitable first choice for CIPN in PC patients.
Trial registration
Not applicable
Keywords: chemotherapy-induced peripheral neuropathy, mirogabalin, pregabalin, pancreatic cancer
Background
Pancreatic cancer (PC) is a lethal disease that has become a major cause of cancer-related death worldwide [1–3]. The poor prognosis of most PC patients is due to the advanced stage of the disease at diagnosis, making resection difficult [4–6]. Thus, chemotherapy has become the general treatment strategy for PC patients. Recently, new chemotherapy regimens have been developed, such as the combination of 5-fluorouracil, oxaliplatin, irinotecan, and leucovorin (FOLFIRINOX) or gemcitabine plus nab-paclitaxel (GnP). Although the prognosis of PC patients is very poor, it has been dramatically improved by FOLFIRINOX or GnP [7–35]. On the other hand, many adverse events are also reported for these regimens. Chemotherapy-induced peripheral neuropathy (CIPN) is a common side effect of both FOLFIRINOX and GnP. In past reports, the frequency of grade 3-4 CIPN was 0 - 25% for FOLFIRINOX [7–9, 11, 12, 14, 15, 17, 18, 21–23, 36] and 1.8 – 30.4% for GnP [27–31, 35, 37]. Oxaliplatin and paclitaxel represent a class of neurotoxic drugs [38–40]. When CIPN becomes severe, it could influence the decision to continue chemotherapy, affecting patient prognosis. Therefore, adequate management of CIPN is necessary.
Regarding drug treatments for CIPN, the efficacy of duroxetine was demonstrated in a past large double-blind randomized controlled trial [41]. In addition, pregabalin was found to be more valuable for treating CIPN than duroxetine in some reports [42, 43]. On the other hand, the efficacy of mirogabalin for diabetic peripheral neuropathy has also been reported [44]. Recently, mirogabalin treatment for CIPN was covered by medical insurance in Japan. Unfortunately, the efficacy of mirogabalin for CIPN is unknown. Therefore, in this study, we compared mirogabalin and pregabalin for the treatment of CIPN.
Methods
Study design and ethics
This was a retrospective study comparing the efficacy of mirogabalin and pregabalin for the treatment of CIPN. This study was approved by the Institutional Review Board of Fukushima Medical University (approval number: 29254). The analysis used anonymous clinical data obtained after all the participants agreed to treatment by written consent, so patients were not required to give informed consent for the study. Informed consent was obtained from all participants or, if participants were under 18, from a parent and/or legal guardian. The details of the study can be found on the homepage of Fukushima Medical University. All methods were carried out in accordance with relevant guidelines and regulations.
Patients
A total of 163 PC patients who underwent FOFIRINOX or GnP therapy at Fukushima Medical University between May 2014 and January 2021 were enrolled. Among them, 34 patients were diagnosed with CIPN based on its clinical course. When a PC patient who was administered a neurotoxic drug reported new pain or numbness on the extremities, the patient was diagnosed with CIPN [45]. Thirteen patients were treated with mirogabalin (mirogabalin group), and twenty-one patients were treated with pregabalin (pregabalin group) (Fig. 1). PC was diagnosed by endoscopic ultrasonography-guided fine needle aspiration, abdominal ultrasonography-guided biopsy, bile cytology, or biliary biopsy.
Fig. 1.
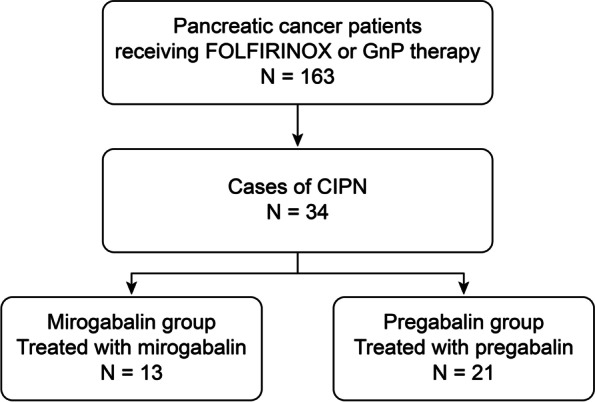
Flowchart of patient selection
Dose of mirogabalin, pregabalin
The dosages of mirogabalin and pregabalin were determined by each doctor, and the effect of mirogabalin or pregabalin was evaluated every one or two weeks. If CIPN did not improve, the dose of mirogabalin or pregabalin was increased. On the other hand, when a side effect of mirogabalin or pregabalin was observed, the dose was decreased. When a side effect became severe or CIPN was sufficiently improved, mirogabalin or pregabalin was stopped. The actual dosage of mirogabalin was as follows (10 mg/day for 4-6 weeks: six patients, 10 mg/day for a week→20 mg/day for a week→30 mg/day for four weeks: a patient, 10 mg/day for a week→ 15 mg/day for a week→20 mg/day for four weeks: a patient, 5 mg/day for a week→15 mg/day for two weeks→10 mg/day for a week→20 mg/day for two weeks: a patient, 10 mg/day for two weeks→20 mg/day for four weeks: a patient, 10 mg/day for four weeks→20 mg/day for two weeks: a patient, 10 mg/day for a week→20 mg/day for five weeks: a patient, 5 mg/day for two weeks→10 mg/day for four weeks: a patient). The actual dosage of pregabalin was as follows (150 mg/day for 2-6 weeks: 18 patients, 75 mg/day for 6 weeks: a patient, 150 mg/day for three weeks→75 mg/day for three weeks: a patient, 150 mg/day for four weeks→75 mg for two weeks: a patient).
Examination items
Patient characteristics and background (age, sex, tumor stage based on the Union for International Cancer Control (UICC) classification 8th edition [46], neurotoxic regimen, concomitant drugs for CIPN, pretreatment CIPN grade) were compared between the mirogabalin group and the pregabalin group. CIPN grade was compared between pretreatment and at 2 weeks after treatment, 4 weeks after treatment, or 6 weeks after treatment. The grade of CIPN was classified by Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. The number of patients with improvement in CIPN at 2, 4, or 6 weeks after treatment was compared between the mirogabalin group and the pregabalin group. If a patient stopped taking medicine for several reasons (CIPN was sufficiently improved, drugs were ineffective, adverse events), the evaluation of improvement in CIPN was continued until 6 weeks after drug initiation.
Statistical analysis
Continuous variables following a normal distribution (age) were analyzed with Welch’s t-test. Ordinal variables and continuous variables that did not follow a normal distribution were analyzed with the Mann-Whitney U test. Nominal variables were analyzed with Fisher’s exact test. The treatment effect of each group was compared between pretreatment and posttreatment with the Wilcoxon signed-rank test. P < 0.05 was defined as statistically significant. All statistical analyses were performed using EzR (Saitama Medical Centre, Jichi Medical University, Saitama, Japan).
Results
Patient characteristics and clinical background
Age, sex, UICC stage, neurotoxic regimen, and concomitant drugs for CIPN were not different between the two groups (Table 1). In both groups, the majority of patients underwent GnP. The pretreatment CIPN grade was significantly higher in the mirogabalin group than in the pregabalin group (3 (2-3) vs 2 (2-3), P < 0.01).
Table 1.
Comparison of patient characteristics and clinical background
| Mirogabalin group (N = 13) |
Pregabalin group (N = 21) |
P value | |
|---|---|---|---|
| Age, years | 61.3 ± 13.6 | 65.4 ± 7.2 | 0.33 |
| Sex, male/female | 8/5 | 9/12 | 0.48 |
| UICC stage, median (range) | 4 (3-4) | 4 (2-4) | 0.74 |
| II, n (%) | 0 (0) | 1 (4.8) | |
| III, n (%) | 5 (38.5) | 8 (38.1) | |
| IV, n (%) | 8 (61.5) | 12(57.1) | |
| Neurotoxic regimen, n (%) | 0.68 | ||
| FOLFIRINOX | 2 (15.4) | 5 (23.8) | |
| GnP | 11 (84.6) | 16 (76.2) | |
| Concomitant drugs for CIPN, n (%) | 3 (23.1) | 5 (23.8) | 1.0 |
| Duroxetine | 1 (7.7) | 1 (4.8) | |
| Vitamin B12 | 2 (15.4) | 1 (4.8) | |
| Duroxetine, goshajinkigan | 1 (4.8) | ||
| Goshajinkigan | 2 (9.5) | ||
| Pretreatment CIPN grade, median (range) | 3 (2-3) | 2 (2-3) | < 0.01 |
| 2, n (%) | 1 (7.7) | 13 (61.9) | |
| 3, n (%) | 12 (92.3) | 8 (38.1) |
Values are shown as the mean ± standard deviation, median (range) or n (%)
UICC Union for International Cancer Control classification; FOLFIRINOX combination of 5-fluorouracil, oxaliplatin, irinotecan, and leucovorin; GnP gemcitabine plus nab-paclitaxel; CIPN chemotherapy-induced peripheral neuropathy
Treatment effect for CIPN
CIPN showed improvement in both the mirogabalin group and pregabalin group (Figure 2). In each group, the grade of CIPN at 2 weeks, 4 weeks, and 6 weeks after drug initiation showed significant improvement over the pretreatment grade.
Fig. 2.

Grade of CIPN before and after treatment. a, b, The grade of CIPN at 2, 4, and 6 weeks after treatment initiation showed significant improvement compared to that before treatment initiation in both groups. CIPN, chemotherapy-induced peripheral neuropathy; CTCAE, Common Terminology Criteria for Adverse Events. * p<0.05, ** p<0.01
The rate of improvement in CIPN at 2, 4 or 6 weeks after drug initiation was significantly higher in the mirogabalin group than in the pregabalin group (2 weeks: 84.6% (11/13) vs 33.3% (7/21), P value = 0.005; 4 weeks, 6 weeks: 92.3% (12/13) vs 33.3% (7/21), P value = 0.001) (Fig. 3).
Fig. 3.
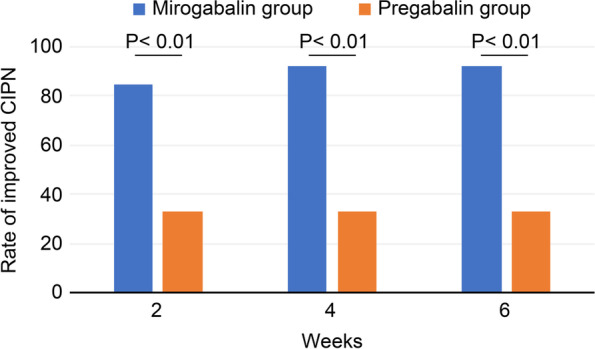
Rate of improvement in CIPN. The rates of improvement in CIPN at 2, 4, and 6 weeks after treatment initiation were significantly higher in the mirogabalin group than in the pregabalin group. CIPN, chemotherapy-induced peripheral neuropathy
Drug discontinuation and adverse events
Drug discontinuation are shown in Table 2. Mirogabalin was stopped in two (15.4%) patients 4 weeks after it was initiated; one patient reported dizziness, and CIPN was found to improve very well in the other patient. Pregabalin was stopped in eleven (52.4%) patients. Seven (33.3%) patients stopped taking pregabalin 2 weeks after pregabalin was initiated. Sufficient improvement in CIPN was not observed in two patients, and side effects were observed in the other five patients. Four (19.0%) patients stopped taking pregabalin four weeks after pregabalin was initiated. Sufficient improvement in CIPN was not observed in three patients, and CIPN was found to improve very well in the other patient. The change in CTCAE grade was not observed after drug discontinuation.
Table 2.
The reasons for drug discontinuation
| Reason for drug discontinuation, n (%) | Mirogabalin group (N = 13) |
Pregabalin group (N = 21) |
|---|---|---|
| 2 weeks after initiation | 0 (0) | 7 (33.3) |
| Ineffective | 0 (0) | 2 (9.5) |
| Adverse events | 0 (0) | 5 (23.8) |
| 4 weeks after initiation | 2 (15.4) | 4 (19.0) |
| CIPN sufficiently improved | 1 (7.7) | 1 (4.8) |
| Adverse events | 1 (7.7) | 0 (0) |
| Ineffective | 0 (0) | 3 (14.3) |
Values are shown as n (%)
CIPN, chemotherapy-induced peripheral neuropathy
Adverse events were not significantly different between the mirogabalin group and the pregabalin group (Table 3).
Table 3.
The comparison of adverse events
| Mirogabalin group (N = 13) |
Pregabalin group (N = 21) |
P value | |
|---|---|---|---|
| Adverse events, n (%) | 2 (15.4) | 7 (33.3) | 0.43 |
| Dizziness | 1 (7.7) | 2 (9.5) | |
| Edema | 1 (7.7) | 2 (9.5) | |
| Sleepiness | 0 | 3 (14.3) |
Values are shown as n (%)
Discussion
In this study, the majority of CIPN occurred by GnP. The therapeutic effect for CIPN was compared between mirogabalin and pregabalin. Both drugs were effective at improving CIPN in PC patients. Although the effect of mirogabalin on CIPN was unknown, the rate of improved CIPN was significantly higher in the mirogabalin group than in the pregabalin group.
In a recent meta-analysis that compared treatment outcomes between FOLFIRINOX and GnP, CIPN occurred much more frequently in patients who were treated with GnP than in patients who were treated with FOLFIRINOX [47]. Therefore, it was reasonable that the regimen responsible for most CIPN was GnP in this study.
Several drugs have been reported for treating CIPN. In these reports, calcium and magnesium, goshajinkigan, duloxetine, vitamin B12, pregabalin, and gabapentin were used [41–43, 48–62]. However, calcium/magnesium, goshajinkigan, and gabapentin were found to be ineffective at treating CIPN in the largest double-blind randomized controlled trials (RCTs) for each drug. Vitamin B12 was used as a control group in the study to investigate the efficacy of goshajinkigan and duroxetine. In the largest RCT, duroxetine was found to be effective at treating CIPN. In addition, the efficacy of pregabalin for CIPN was reported to be better than that of duroxetine in two reports. In 2018, Avan et al. [42] performed a double-blind RCT that targeted 82 breast cancer patients with taxane-induced peripheral neuropathy (pregabalin group: n = 40, duroxetine group: n = 42). In their study, pregabalin provided the greatest improvement in insomnia and pain scores [42]. In 2019, Salehifar et al. [43] reported that pregabalin was more valuable for improving the sensory and pain scores of CIPN than duroxetine. In both reports, CIPN was improved after 6 weeks of pregabalin treatment. In this study, CIPN was significantly improved after pregabalin treatment. Although mirogabalin was reported to be useful for diabetic neuropathy [44], it was also found to be useful for CIPN in this study.
Although mirogabalin and pregabalin were both valuable for improving CIPN, the treatment effect was different between the two groups. Although no significant difference in adverse events was observed, adverse events were more common in the pregabalin group than in the mirogabalin group. Pregabalin and mirogabalin combine with the α2δ subunit of Ca channels in the back horn of the spinal cord and impede the inflow of calcium, which is required for neurotransmitter release [44, 63–66]. However, the two drugs show different connectivity to the subtypes of the α2δ subunit of the Ca channel. Among these subtypes, the α2δ-1 subunit is related to analgesic effects [67], and the α2δ-2 subunit is related to central nervous system disorders [68]. In a past report written by Domon et al. [69], the dissociation half-life between mirogabalin and the α2δ-1 subunit was 11.1 (8.3-16.4) hours, and the dissociation half-life between mirogabalin and the α2δ-2 subunit was 2.4 (2.1-2.8) hours. On the other hand, the dissociation half-life between pregabalin and α2δ-1 and α2δ-2 subunits was 1.4 hours (α2δ-1: 1.4 (1.3-1.4) hours, α2δ-2: 1.4 (0.9-2.7) hours) [69]. Because the dissociation half-life between mirogabalin and the α2δ-1 subunit was longer than that between mirogabalin and the α2δ-2 subunit, the analgesic effect is expected to be durable, and adverse events caused by central nervous system disorder are expected to be reduced by mirogabalin. This difference in the connection to the α2δ subunit leads to differences in not only the treatment effects but also the adverse events elicited by mirogabalin and pregabalin.
There were some limitations to this study that should be mentioned. First, this was a retrospective study with a small sample size conducted at a single institution. However, this study is the first to compare the efficacy of mirogabalin and pregabalin for the treatment of CIPN. We hope that multicenter RCTs will be conducted in the future to confirm the results reported in this study. Second, the doses of mirogabalin and pregabalin were not uniform. The results showed that both drugs were effective at treating CIPN, even though a low dose was used for both drugs.
Conclusions
Although both mirogabalin and pregabalin were effective at improving CIPN, a higher rate of improved CIPN was observed in patients who were treated with mirogabalin. Mirogabalin might be a suitable first choice for CIPN in PC patients.
Acknowledgements
We thank all the staff at the Department of Gastroenterology of Fukushima Medical University, the Department of Endoscopy of Fukushima Medical University Hospital, and the gastroenterology ward of Fukushima Medical University Hospital. We also thank American Journal Experts for providing English language editing.
Informed consent
The analysis used anonymous clinical data obtained after all the participants agreed to treatment by written consent, so patients were not required to give informed consent for the study. Informed consent was obtained from all participants or, if participants were under 18, from a parent and/or legal guardian.
Abbreviations
- PC
Pancreatic cancer
- FOLFIRINOX
The combination of 5-fluorouracil, oxaliplatin, irinotecan, and leucovorin
- GnP
Gemcitabine plus nab-paclitaxel
- CIPN
Chemotherapy-induced peripheral neuropathy
Authors’ contributions
MS wrote the paper and designed and performed the research; TT designed and oversaw the research; RS, NK, HA, YS, HI, YO, JN, MT, MH, TK, RK, and TH provided clinical advice; and HO supervised the report and the writing of the paper. All authors have read and approved the final manuscript.
Funding
Department of Gastroenterology, Fukushima Medical University
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
Ethics approval and consent to participate
The study protocol was reviewed and approved by the Institutional Review Board of Fukushima Medical University (Number 29254). The analysis used anonymous clinical data obtained after all the participants agreed to treatment by written consent, so patients were not required to give informed consent for the study. The details of the study can be found on the homepage of Fukushima Medical University.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests to report.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi: 10.3322/caac.21492. [DOI] [PubMed] [Google Scholar]
- 2.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. doi: 10.3322/caac.21590. [DOI] [PubMed] [Google Scholar]
- 3.Afshar N, English DR, Chamberlain JA, Blakely T, Thursfield V, Farrugia H, et al. Differences in cancer survival by remoteness of residence: an analysis of data from a population-based cancer registry. Cancer Causes Control. 2020;31:617–629. doi: 10.1007/s10552-020-01303-2. [DOI] [PubMed] [Google Scholar]
- 4.Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev Clin Oncol. 2010;7:163–172. doi: 10.1038/nrclinonc.2009.236. [DOI] [PubMed] [Google Scholar]
- 5.Warsame R, Grothey A. Treatment options for advanced pancreatic cancer: a review. Expert Rev Anticancer Ther. 2012;12:1327–1336. doi: 10.1586/era.12.115. [DOI] [PubMed] [Google Scholar]
- 6.Fogel EL, Shahda S, Sandrasegaran K, DeWitt J, Easler JJ, Agarwal DM, et al. A multidisciplinary approach to pancreas cancer in 2016: a review. Am J Gastroenterol. 2017;112:537–554. doi: 10.1038/ajg.2016.610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Conroy T, Paillot B, François E, Bugat R, Jacob JH, Stein U, et al. Irinotecan plus oxaliplatin and leucovorin-modulated fluorouracil in advanced pancreatic cancer--a Groupe Tumeurs Digestives of the Federation Nationale des centres De Lutte Contre le Cancer study. J Clin Oncol. 2005;23:1228–1236. doi: 10.1200/JCO.2005.06.050. [DOI] [PubMed] [Google Scholar]
- 8.Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–1825. doi: 10.1056/NEJMoa1011923. [DOI] [PubMed] [Google Scholar]
- 9.Assaf E, Verlinde-Carvalho M, Delbaldo C, Grenier J, Sellam Z, Pouessel D, et al. 5-fluorouracil/leucovorin combined with irinotecan and oxaliplatin (FOLFIRINOX) as second-line chemotherapy in patients with metastatic pancreatic adenocarcinoma. Oncology. 2011;80:301–306. doi: 10.1159/000329803. [DOI] [PubMed] [Google Scholar]
- 10.Peddi PF, Lubner S, McWilliams R, Tan BR, Picus J, Sorscher SM, et al. Multi-institutional experience with FOLFIRINOX in pancreatic adenocarcinoma. JOP. 2012;13:497–501. doi: 10.6092/1590-8577/913. [DOI] [PubMed] [Google Scholar]
- 11.Hosein PJ, Macintyre J, Kawamura C, Maldonado JC, Ernani V, Loaiza-Bonilla A, et al. A retrospective study of neoadjuvant FOLFIRINOX in unresectable or borderline-resectable locally advanced pancreatic adenocarcinoma. BMC Cancer. 2012;12:199. doi: 10.1186/1471-2407-12-199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lorgis V, Chauffert B, Gentil J, Ghiringhelli F. Influcence of localization of primary tumor on effectiveness of 5-fluorouracil/leucovorin combined with irinotecan and oxaliplatin (FOLFIRINOX) in patients with metastatic pancreatic adenocarcinoma: a retrospective study. Anticancer Res. 2012;32:4125–4130. [PubMed] [Google Scholar]
- 13.Mahaseth H, Brutcher E, Kauh J, Hawk N, Kim S, Chen Z, et al. Modified FOLFIRINOX regimen with improved safety and maintained efficacy in pancreatic adenocarcinoma. Pancreas. 2013;42:1311–1315. doi: 10.1097/MPA.0b013e31829e2006. [DOI] [PubMed] [Google Scholar]
- 14.Faris JE, Blaszkowsky LS, McDermott S, Guimaraes AR, Szymonifka J, Huynh MA, et al. FOLFIRINOX in locally advanced pancreatic cancer: the Massachusetts General Hospital Cancer Center experience. Oncologist. 2013;18:543–548. doi: 10.1634/theoncologist.2012-0435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gunturu KS, Yao X, Cong X, Thumar JR, Hochster HS, Stein SM, et al. FOLFIRINOX for locally advanced and metastatic pancreatic cancer: single institution retrospective review of efficacy and toxicity. Med Oncol. 2013;30:361. doi: 10.1007/s12032-012-0361-2. [DOI] [PubMed] [Google Scholar]
- 16.Hohla F, Hopfinger G, Romeder F, Rinnerthaler G, Bezan A, Stättner S, et al. Female gender may predict response to FOLFIRINOX in patients with unresectable pancreatic cancer: a single institution retrospective review. Int J Oncol. 2014;44:319–326. doi: 10.3892/ijo.2013.2176. [DOI] [PubMed] [Google Scholar]
- 17.Moorcraft SY, Khan K, Peckitt C, Watkins D, Rao S, Cunningham D, et al. FOLFIRINOX for locally advanced or metastatic pancreatic ductal adenocarcinoma: the Royal Marsden experience. Clin Colorectal Cancer. 2014;13:232–238. doi: 10.1016/j.clcc.2014.09.005. [DOI] [PubMed] [Google Scholar]
- 18.Marthey L, Sa-Cunha A, Blanc JF, Gauthier M, Cueff A, Francois E, et al. FOLFIRINOX for locally advanced pancreatic adenocarcinoma: results of an AGEO multicenter prospective observational cohort. Ann Surg Oncol. 2015;22:295–301. doi: 10.1245/s10434-014-3898-9. [DOI] [PubMed] [Google Scholar]
- 19.Mellon EA, Hoffe SE, Springett GM, Frakes JM, Strom TJ, Hodul PJ, et al. Long-term outcomes of induction chemotherapy and neoadjuvant stereotactic body radiotherapy for borderline resectable and locally advanced pancreatic adenocarcinoma. Acta Oncol. 2015;54:979–985. doi: 10.3109/0284186X.2015.1004367. [DOI] [PubMed] [Google Scholar]
- 20.Sadot E, Doussot A, O'Reilly EM, Lowery MA, Goodman KA, Do RK, et al. FOLFIRINOX induction therapy for stage 3 pancreatic adenocarcinoma. Ann Surg Oncol. 2015;22:3512–3521. doi: 10.1245/s10434-015-4647-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zahir MN, Jabbar AA. Metastatic pancreatic carcinoma and experience with FOLFIRINOX - a cross sectional analysis from a developing country. Asian Pac J Cancer Prev. 2015;16:6001–6006. doi: 10.7314/apjcp.2015.16.14.6001. [DOI] [PubMed] [Google Scholar]
- 22.Rombouts SJ, Mungroop TH, Heilmann MN, van Laarhoven HW, Busch OR, Molenaar IQ, et al. FOLFIRINOX in locally advanced and metastatic pancreatic cancer: a single centre cohort study. J Cancer. 2016;7:1861–1866. doi: 10.7150/jca.16279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chllamma MK, Cook N, Dhani NC, Giby K, Dodd A, Wang L, et al. FOLFIRINOX for advanced pancreatic cancer: the Princess Margaret Cancer Centre experience. Br J Cancer. 2016;115:649–654. doi: 10.1038/bjc.2016.222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Orlandi A, Calegari MA, Martini M, Cocomazzi A, Bagalà C, Indellicati G, et al. Gemcitabine versus FOLFIRINOX in patients with advanced pancreatic adenocarcinoma hENT1-positive: everything was not too bad back when everything seemed worse. Clin Transl Oncol. 2016;18:988–995. doi: 10.1007/s12094-015-1471-z. [DOI] [PubMed] [Google Scholar]
- 25.Hann A, Bohle W, Egger J, Zoller WG. Improvement in advanced pancreatic cancer survival with novel chemotherapeutic strategies - experience of a community based hospital. Z Gastroenterol. 2016;54:1138–1142. doi: 10.1055/s-0042-110793. [DOI] [PubMed] [Google Scholar]
- 26.Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–1703. doi: 10.1056/NEJMoa1304369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang DS, Wang DS, Wang ZQ, Wang FH, Luo HY, Qiu MZ, et al. Phase I/II study of albumin-bound nab-paclitaxel plus gemcitabine administered to Chinese patients with advanced pancreatic cancer. Cancer Chemother Pharmacol. 2013;71:1065–1072. doi: 10.1007/s00280-013-2102-4. [DOI] [PubMed] [Google Scholar]
- 28.Goldstein D, El-Maraghi RH, Hammel P, Heinemann V, Kunzmann V, Sastre J, et al. nab-paclitaxel plus gemcitabine for metastatic pancreatic cancer: long-term survival from a phase III trial. J Natl Cancer Inst. 2015;107:dju413. [DOI] [PubMed]
- 29.Ueno H, Ikeda M, Ueno M, Mizuno N, Ioka T, Omuro Y, et al. Phase I/II study of nab-paclitaxel plus gemcitabine for chemotherapy-naive Japanese patients with metastatic pancreatic cancer. Cancer Chemother Pharmacol. 2016;77:595–603. doi: 10.1007/s00280-016-2972-3. [DOI] [PubMed] [Google Scholar]
- 30.Ahn DH, Krishna K, Blazer M, Reardon J, Wei L, Wu C, et al. A modified regimen of biweekly gemcitabine and nab-paclitaxel in patients with metastatic pancreatic cancer is both tolerable and effective: a retrospective analysis. Ther Adv Med Oncol. 2017;9:75–82. doi: 10.1177/1758834016676011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cho IR, Kang H, Jo JH, Lee HS, Chung MJ, Park JY, et al. Efficacy and treatment-related adverse events of gemcitabine plus nab-paclitaxel for treatment of metastatic pancreatic cancer "in a Korean" population: a single-center cohort study. Semin Oncol. 2017;44:420–427. doi: 10.1053/j.seminoncol.2018.01.001. [DOI] [PubMed] [Google Scholar]
- 32.Ko AH, Murphy PB, Peyton JD, Shipley DL, Al-Hazzouri A, Rodriguez FA, et al. A randomized, double-blinded, phase II trial of gemcitabine and nab-paclitaxel plus apatorsen or placebo in patients with metastatic pancreatic cancer: the RAINIER trial. Oncologist. 2017;22:1427–e129. doi: 10.1634/theoncologist.2017-0066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Xu R, Yu X, Hao J, Wang L, Pan H, Han G, et al. Efficacy and safety of weekly nab-paclitaxel plus gemcitabine in Chinese patients with metastatic adenocarcinoma of the pancreas: a phase II study. BMC Cancer. 2017;17:885. doi: 10.1186/s12885-017-3887-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kang J, Hwang I, Yoo C, Kim KP, Jeong JH, Chang HM, et al. Nab-paclitaxel plus gemcitabine versus FOLFIRINOX as the first-line chemotherapy for patients with metastatic pancreatic cancer: retrospective analysis. Invest New Drugs. 2018;36:732–741. doi: 10.1007/s10637-018-0598-5. [DOI] [PubMed] [Google Scholar]
- 35.You MS, Ryu JK, Choi YH, Choi JH, Huh G, Paik WH, et al. Efficacy of nab-paclitaxel plus gemcitabine and prognostic value of peripheral neuropathy in patients with metastatic pancreatic cancer. Gut Liver. 2018;12:728–735. doi: 10.5009/gnl18220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Boone BA, Steve J, Krasinskas AM, Zureikat AH, Lembersky BC, Gibson MK, et al. Outcomes with FOLFIRINOX for borderline resectable and locally unresectable pancreatic cancer. J Surg Oncol. 2013;108:236–241. doi: 10.1002/jso.23392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ottaiano A, Capozzi M, Divitiis CDE, Arx CV, Girolamo EDI, Nasti G, et al. Nab-paclitaxel and gemcitabine in advanced pancreatic cancer: the one-year experience of the National Cancer Institute of Naples. Anticancer Res. 2017;37:1975–1978. doi: 10.21873/anticanres.11539. [DOI] [PubMed] [Google Scholar]
- 38.Loprinzi CL, Reeves BN, Dakhil SR, Sloan JA, Wolf SL, Burger KN, et al. Natural history of paclitaxel-associated acute pain syndrome: prospective cohort study NCCTG N08C1. J Clin Oncol. 2011;29:1472–1478. doi: 10.1200/JCO.2010.33.0308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Reeves BN, Dakhil SR, Sloan JA, Wolf SL, Burger KN, Kamal A, et al. Further data supporting that paclitaxel-associated acute pain syndrome is associated with development of peripheral neuropathy: North Central Cancer Treatment Group trial N08C1. Cancer. 2012;118:5171–5178. doi: 10.1002/cncr.27489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pachman DR, Qin R, Seisler DK, Smith EM, Beutler AS, Ta LE, et al. Clinical course of oxaliplatin-induced neuropathy: results from the randomized phase III trial N08CB (alliance) J Clin Oncol. 2015;33:3416–3422. doi: 10.1200/JCO.2014.58.8533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Smith EM, Pang H, Cirrincione C, Fleishman S, Paskett ED, Ahles T, et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: a randomized clinical trial. JAMA. 2013;309:1359–1367. doi: 10.1001/jama.2013.2813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Avan R, Janbabaei G, Hendouei N, Alipour A, Borhani S, Tabrizi N, et al. The effect of pregabalin and duloxetine treatment on quality of life of breast cancer patients with taxane-induced sensory neuropathy: a randomized clinical trial. J Res Med Sci. 2018;23:52. doi: 10.4103/jrms.JRMS_1068_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Salehifar E, Janbabaei G, Hendouei N, Alipour A, Tabrizi N, Avan R. Comparison of the efficacy and safety of pregabalin and duloxetine in taxane-induced sensory neuropathy: a randomized controlled trial. Clin Drug Investig. 2020;40:249–257. doi: 10.1007/s40261-019-00882-6. [DOI] [PubMed] [Google Scholar]
- 44.Baba M, Matsui N, Kuroha M, Wasaki Y, Ohwada S. Mirogabalin for the treatment of diabetic peripheral neuropathic pain: a randomized, double-blind, placebo-controlled phase III study in Asian patients. J Diabetes Investig. 2019;10:1299–1306. doi: 10.1111/jdi.13013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Loprinzi CL, Lacchetti C, Bleeker J, Cavaletti G, Chauhan C, Hertz DL, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J Clin Oncol. 2020;38:3325–3348. doi: 10.1200/JCO.20.01399. [DOI] [PubMed] [Google Scholar]
- 46.Brierley JD, Gospodarowicz MK, Wittekind C. TNM-classification of malignant tumours. 8th ed. New Jersey, NJ: Wiley-Blackwell; 2017.
- 47.Pusceddu S, Ghidini M, Torchio M, Corti F, Tomasello G, Niger M, et al. Comparative effectiveness of gemcitabine plus nab-paclitaxel and FOLFIRINOX in the first-line setting of metastatic pancreatic cancer: a systematic review and meta-analysis. Cancers (Basel). 2019;11:484. doi: 10.3390/cancers11040484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ishibashi K, Okada N, Miyazaki T, Sano M, Ishida H. Effect of calcium and magnesium on neurotoxicity and blood platinum concentrations in patients receiving mFOLFOX6 therapy: a prospective randomized study. Int J Clin Oncol. 2010;15:82–87. doi: 10.1007/s10147-009-0015-3. [DOI] [PubMed] [Google Scholar]
- 49.Loprinzi CL, Qin R, Dakhil SR, Fehrenbacher L, Flynn KA, Atherton P, et al. Phase III randomized, placebo-controlled, double-blind study of intravenous calcium and magnesium to prevent oxaliplatin-induced sensory neurotoxicity (N08CB/Alliance) J Clin Oncol. 2014;32:997–1005. doi: 10.1200/JCO.2013.52.0536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wesselink E, Winkels RM, van Baar H, Geijsen A, van Zutphen M, van Halteren HK, et al. Dietary intake of magnesium or calcium and chemotherapy-induced peripheral neuropathy in colorectal cancer patients. Nutrients. 2018;10:398. doi: 10.3390/nu10040398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Nishioka M, Shimada M, Kurita N, Iwata T, Morimoto S, Yoshikawa K, et al. The Kampo medicine, Goshajinkigan, prevents neuropathy in patients treated by FOLFOX regimen. Int J Clin Oncol. 2011;16:322–327. doi: 10.1007/s10147-010-0183-1. [DOI] [PubMed] [Google Scholar]
- 52.Kaku H, Kumagai S, Onoue H, Takada A, Shoji T, Miura F, et al. Objective evaluation of the alleviating effects of Goshajinkigan on peripheral neuropathy induced by paclitaxel/carboplatin therapy: a multicenter collaborative study. Exp Ther Med. 2012;3:60–65. doi: 10.3892/etm.2011.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kono T, Hata T, Morita S, Munemoto Y, Matsui T, Kojima H, et al. Goshajinkigan oxaliplatin neurotoxicity evaluation (GONE): a phase 2, multicenter, randomized, double-blind, placebo-controlled trial of goshajinkigan to prevent oxaliplatin-induced neuropathy. Cancer Chemother Pharmacol. 2013;72:1283–1290. doi: 10.1007/s00280-013-2306-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Oki E, Emi Y, Kojima H, Higashijima J, Kato T, Miyake Y, et al. Preventive effect of Goshajinkigan on peripheral neurotoxicity of FOLFOX therapy (GENIUS trial): a placebo-controlled, double-blind, randomized phase III study. Int J Clin Oncol. 2015;20:767–775. doi: 10.1007/s10147-015-0784-9. [DOI] [PubMed] [Google Scholar]
- 55.Hirayama Y, Ishitani K, Sato Y, Iyama S, Takada K, Murase K, et al. Effect of duloxetine in Japanese patients with chemotherapy-induced peripheral neuropathy: a pilot randomized trial. Int J Clin Oncol. 2015;20:866–871. doi: 10.1007/s10147-015-0810-y. [DOI] [PubMed] [Google Scholar]
- 56.Wang J, Li Q, Xu B, Zhang T, Chen S, Luo Y. Efficacy and safety of duloxetine in Chinese breast cancer patients with paclitaxel-induced peripheral neuropathy. Chin J Cancer Res. 2017;29:411–418. doi: 10.21147/j.issn.1000-9604.2017.05.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Shinde SS, Seisler D, Soori G, Atherton PJ, Pachman DR, Lafky J, et al. Can pregabalin prevent paclitaxel-associated neuropathy?--an ACCRU pilot trial. Support Care Cancer. 2016;24:547–553. doi: 10.1007/s00520-015-2807-5. [DOI] [PubMed] [Google Scholar]
- 58.de Andrade DC, Jacobsen Teixeira M, Galhardoni R, Ferreira KSL, Mileno PB, Scisci N, et al. Pregabalin for the prevention of oxaliplatin-induced painful neuropathy: a randomized, double-blind trial. Oncologist. 2017;22:1154–e105. doi: 10.1634/theoncologist.2017-0235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hincker A, Frey K, Rao L, Wagner-Johnston N, Ben Abdallah A, Tan B, et al. Somatosensory predictors of response to pregabalin in painful chemotherapy-induced peripheral neuropathy: a randomized, placebo-controlled, crossover study. Pain. 2019;160:1835–1846. doi: 10.1097/j.pain.0000000000001577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Rao RD, Michalak JC, Sloan JA, Loprinzi CL, Soori GS, Nikcevich DA, et al. Efficacy of gabapentin in the management of chemotherapy-induced peripheral neuropathy: a phase 3 randomized, double-blind, placebo-controlled, crossover trial (N00C3) Cancer. 2007;110:2110–2118. doi: 10.1002/cncr.23008. [DOI] [PubMed] [Google Scholar]
- 61.Magnowska M, Iżycka N, Kapoła-Czyż J, Romała A, Lorek J, Spaczyński M, et al. Effectiveness of gabapentin pharmacotherapy in chemotherapy-induced peripheral neuropathy. Ginekol Pol. 2018;89:200–204. doi: 10.5603/GP.a2018.0034. [DOI] [PubMed] [Google Scholar]
- 62.Aghili M, Zare M, Mousavi N, Ghalehtaki R, Sotoudeh S, Kalaghchi B, et al. Efficacy of gabapentin for the prevention of paclitaxel induced peripheral neuropathy: a randomized placebo controlled clinical trial. Breast J. 2019;25:226–231. doi: 10.1111/tbj.13196. [DOI] [PubMed] [Google Scholar]
- 63.Xiao W, Boroujerdi A, Bennett GJ, Luo ZD. Chemotherapy-evoked painful peripheral neuropathy: analgesic effects of gabapentin and effects on expression of the alpha-2-delta type-1 calcium channel subunit. Neuroscience. 2007;144:714–720. doi: 10.1016/j.neuroscience.2006.09.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Gauchan P, Andoh T, Ikeda K, Fujita M, Sasaki A, Kato A, et al. Mechanical allodynia induced by paclitaxel, oxaliplatin and vincristine: different effectiveness of gabapentin and different expression of voltage-dependent calcium channel alpha(2)delta-1 subunit. Biol Pharm Bull. 2009;32:732–734. doi: 10.1248/bpb.32.732. [DOI] [PubMed] [Google Scholar]
- 65.Peng P, Xi Q, Xia S, Zhuang L, Gui Q, Chen Y, et al. Pregabalin attenuates docetaxel-induced neuropathy in rats. J Huazhong Univ Sci Technolog Med Sci. 2012;32:586–590. doi: 10.1007/s11596-012-1001-y. [DOI] [PubMed] [Google Scholar]
- 66.Aoki M, Kurauchi Y, Mori A, Nakahara T, Sakamoto K, Ishii K. Comparison of the effects of single doses of elcatonin and pregabalin on oxaliplatin-induced cold and mechanical allodynia in rats. Biol Pharm Bull. 2014;37:322–326. doi: 10.1248/bpb.b13-00735. [DOI] [PubMed] [Google Scholar]
- 67.Boroujerdi A, Zeng J, Sharp K, Kim D, Steward O, Luo DZ. Calcium channel alpha-2-delta-1 protein upregulation in dorsal spinal cord mediates spinal cord injury-induced neuropathic pain states. Pain. 2011;152:649–655. doi: 10.1016/j.pain.2010.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Barclay J, Balaguero N, Mione M, Ackerman SL, Letts VA, Brodbeck J, et al. Ducky mouse phenotype of epilepsy and ataxia is associated with mutations in the Cacna2d2 gene and decreased calcium channel current in cerebellar Purkinje cells. J Neurosci. 2001;21:6095–6104. doi: 10.1523/JNEUROSCI.21-16-06095.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Domon Y, Arakawa N, Inoue T, Matsuda F, Takahashi M, Yamamura N, et al. Binding characteristics and analgesic effects of mirogabalin, a novel ligand for the α(2)δ subunit of voltage-gated calcium channels. J Pharmacol Exp Ther. 2018;365:573–582. doi: 10.1124/jpet.117.247551. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.