

Abstract
Background
The Revised Cardiac Risk Index (RCRI) is a widely acknowledged prognostic model to estimate preoperatively the probability of developing in‐hospital major adverse cardiac events (MACE) in patients undergoing noncardiac surgery. However, the RCRI does not always make accurate predictions, so various studies have investigated whether biomarkers added to or compared with the RCRI could improve this.
Objectives
Primary: To investigate the added predictive value of biomarkers to the RCRI to preoperatively predict in‐hospital MACE and other adverse outcomes in patients undergoing noncardiac surgery.
Secondary: To investigate the prognostic value of biomarkers compared to the RCRI to preoperatively predict in‐hospital MACE and other adverse outcomes in patients undergoing noncardiac surgery.
Tertiary: To investigate the prognostic value of other prediction models compared to the RCRI to preoperatively predict in‐hospital MACE and other adverse outcomes in patients undergoing noncardiac surgery.
Search methods
We searched MEDLINE and Embase from 1 January 1999 (the year that the RCRI was published) until 25 June 2020. We also searched ISI Web of Science and SCOPUS for articles referring to the original RCRI development study in that period.
Selection criteria
We included studies among adults who underwent noncardiac surgery, reporting on (external) validation of the RCRI and:
‐ the addition of biomarker(s) to the RCRI; or
‐ the comparison of the predictive accuracy of biomarker(s) to the RCRI; or
‐ the comparison of the predictive accuracy of the RCRI to other models.
Besides MACE, all other adverse outcomes were considered for inclusion.
Data collection and analysis
We developed a data extraction form based on the CHARMS checklist. Independent pairs of authors screened references, extracted data and assessed risk of bias and concerns regarding applicability according to PROBAST. For biomarkers and prediction models that were added or compared to the RCRI in ≥ 3 different articles, we described study characteristics and findings in further detail. We did not apply GRADE as no guidance is available for prognostic model reviews.
Main results
We screened 3960 records and included 107 articles.
Over all objectives we rated risk of bias as high in ≥ 1 domain in 90% of included studies, particularly in the analysis domain. Statistical pooling or meta‐analysis of reported results was impossible due to heterogeneity in various aspects: outcomes used, scale by which the biomarker was added/compared to the RCRI, prediction horizons and studied populations.
Added predictive value of biomarkers to the RCRI
Fifty‐one studies reported on the added value of biomarkers to the RCRI. Sixty‐nine different predictors were identified derived from blood (29%), imaging (33%) or other sources (38%). Addition of NT‐proBNP, troponin or their combination improved the RCRI for predicting MACE (median delta c‐statistics: 0.08, 0.14 and 0.12 for NT‐proBNP, troponin and their combination, respectively). The median total net reclassification index (NRI) was 0.16 and 0.74 after addition of troponin and NT‐proBNP to the RCRI, respectively. Calibration was not reported. To predict myocardial infarction, the median delta c‐statistic when NT‐proBNP was added to the RCRI was 0.09, and 0.06 for prediction of all‐cause mortality and MACE combined. For BNP and copeptin, data were not sufficient to provide results on their added predictive performance, for any of the outcomes.
Comparison of the predictive value of biomarkers to the RCRI
Fifty‐one studies assessed the predictive performance of biomarkers alone compared to the RCRI. We identified 60 unique predictors derived from blood (38%), imaging (30%) or other sources, such as the American Society of Anesthesiologists (ASA) classification (32%). Predictions were similar between the ASA classification and the RCRI for all studied outcomes. In studies different from those identified in objective 1, the median delta c‐statistic was 0.15 and 0.12 in favour of BNP and NT‐proBNP alone, respectively, when compared to the RCRI, for the prediction of MACE. For C‐reactive protein, the predictive performance was similar to the RCRI. For other biomarkers and outcomes, data were insufficient to provide summary results. One study reported on calibration and none on reclassification.
Comparison of the predictive value of other prognostic models to the RCRI
Fifty‐two articles compared the predictive ability of the RCRI to other prognostic models. Of these, 42% developed a new prediction model, 22% updated the RCRI, or another prediction model, and 37% validated an existing prediction model. None of the other prediction models showed better performance in predicting MACE than the RCRI. To predict myocardial infarction and cardiac arrest, ACS‐NSQIP‐MICA had a higher median delta c‐statistic of 0.11 compared to the RCRI. To predict all‐cause mortality, the median delta c‐statistic was 0.15 higher in favour of ACS‐NSQIP‐SRS compared to the RCRI. Predictive performance was not better for CHADS2, CHA2DS2‐VASc, R2CHADS2, Goldman index, Detsky index or VSG‐CRI compared to the RCRI for any of the outcomes. Calibration and reclassification were reported in only one and three studies, respectively.
Authors' conclusions
Studies included in this review suggest that the predictive performance of the RCRI in predicting MACE is improved when NT‐proBNP, troponin or their combination are added. Other studies indicate that BNP and NT‐proBNP, when used in isolation, may even have a higher discriminative performance than the RCRI. There was insufficient evidence of a difference between the predictive accuracy of the RCRI and other prediction models in predicting MACE. However, ACS‐NSQIP‐MICA and ACS‐NSQIP‐SRS outperformed the RCRI in predicting myocardial infarction and cardiac arrest combined, and all‐cause mortality, respectively. Nevertheless, the results cannot be interpreted as conclusive due to high risks of bias in a majority of papers, and pooling was impossible due to heterogeneity in outcomes, prediction horizons, biomarkers and studied populations.
Future research on the added prognostic value of biomarkers to existing prediction models should focus on biomarkers with good predictive accuracy in other settings (e.g. diagnosis of myocardial infarction) and identification of biomarkers from omics data. They should be compared to novel biomarkers with so far insufficient evidence compared to established ones, including NT‐proBNP or troponins. Adherence to recent guidance for prediction model studies (e.g. TRIPOD; PROBAST) and use of standardised outcome definitions in primary studies is highly recommended to facilitate systematic review and meta‐analyses in the future.
Keywords: Adult, Humans, Bias, Biomarkers, Heart Arrest, Myocardial Infarction, Peptide Fragments, Predictive Value of Tests, Prognosis, Risk Assessment
Plain language summary
Can biomarkers improve predictions of the RCRI tool to predict heart‐related complications in patients undergoing surgery other than heart surgery?
Background and review question
Although patients undergo surgery to maintain or increase life expectancy or to improve quality of life, surgery is not without risks. Some patients will develop a heart‐related complication after surgery other than heart surgery, such as a heart infarction. Several tools try to predict someone's chance of developing a heart complication after surgery using information collected in the period before surgery. The Revised Cardiac Risk Index (RCRI) is such a tool that tries to estimate the chance of developing a heart complication during hospital admission in patients undergoing surgery other than heart surgery. It uses information on whether the patient has in the past experienced a heart infarction, heart failure and/or a stroke during his/her life, their use of insulin for the treatment of diabetes mellitus, their current renal (kidney) function and whether he/she will undergo high or non‐high risk surgery. The RCRI is commonly used by physicians, but the predictions are not always very accurate. Therefore, several researchers have attempted to improve these predictions by adding extra information to this tool. This information can be derived from so‐called biomarkers, which are, for example, measurements from blood, imaging techniques or other characteristics, such as age, smoking status or physical condition of the patient.
The aim of this systematic review was to investigate whether the addition of such biomarkers to the RCRI improves predictions of heart‐related complications during hospitalisation in patients undergoing surgery other than heart surgery. In addition, we investigated whether biomarkers and other prediction tools resulted in better predictions of heart‐related complications during hospitalisation compared to the predictions of the RCRI in patients undergoing surgery other than heart surgery.
Key results
We identified 69 different predictors that were added to the RCRI tool to improve predictions of these heart‐related complications. The evidence is current to 25 June 2020. Predictions seem to improve with the addition of some biomarkers derived from blood. These are troponin (which measures muscular damage of the heart), brain natriuretic peptide (BNP) and (NT‐pro)brain natriuretic peptide (NT‐proBNP) (which both measure severity of heart failure).
In addition, there were 60 biomarkers that were studied to compare their predictions to the RCRI. Other studies included in this review suggest that BNP and NT‐proBNP alone may predict heart‐related complications even better than the RCRI. Sixty‐five prediction tools other than the RCRI tried to improve its predictions. The American College of Surgeons National Surgical Quality Improvement (ACS‐NSQIP) and ACS‐NSQIP‐MICA (myocardial infarction or cardiac arrest) surgical risk score tools could make better predictions than the RCRI, but this was only true for certain outcomes, and not for heart‐related complications. However, for all of these research questions, we are not confident in the results due to large variation in the research methods applied and signs of less accurate research approaches having been used.
Authors' conclusions
Troponin, BNP and NT‐proBNP may improve the ability of the RCRI to predict heart‐related complications. The ACS‐NSQOP‐MICA and ACS‐NSQIP surgical risk score tools seem to be better at predicting postoperative complications than the RCRI tool, but not heart‐related complications. However, due to deficiencies in how the studies were conducted, we are uncertain whether the results we found apply to all patients undergoing surgery other than heart surgery. We need more and better research on biomarkers with promising predictive performance in other settings.
Summary of findings
Summary of findings 1. Summary of findings ‐ objective 1: added value of biomarkers to the RCRI.
|
Population: patients undergoing noncardiac surgery Index model: Revised Cardiac Risk Index (RCRI) Comparator: RCRI extended with biomarker(s) Outcome: postoperative occurrence of (in‐hospital) major adverse cardiac events (MACE), all‐cause mortality and other adverse outcomes Timing: time point of prognostication: before surgery; prediction horizon: in‐hospital, but all time spans are included Setting: to inform physicians of the patient's risk of developing in‐hospital events after noncardiac surgery | ||||||
| Outcomes | Biomarker | № of participants (studies) | Measure | Pooled result | Comments | |
| Summary measure | Median (range) | |||||
| MACE | Troponin | 3 studies 810 patients 77 MACE | Discrimination | Delta c‐statistic | 0.14 (0.06 to 0.33) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was 30‐day MACE. |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 577 patients 70 MACE | Reclassification | NRI | 0.16 (0.09 to 0.22) | Surgical specialty was vascular surgery. Prediction horizon was 30‐day MACE and long‐term MACE (> 30 days). | ||
| 1 study 122 patients 29 MACE | — | IDI | 0.05 | Surgical specialty was vascular surgery. Prediction horizon was long‐term MACE (> 30 days). | ||
| NT‐proBNP | 7 studies 13,687 patients 1710 MACE | Discrimination | Delta c‐statistic | 0.08 (0.04 to 0.22) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was 30‐day MACE. | |
| 1 study 10,402 patients 1269 MACE | Calibration | Calibration plot | Good calibration | Surgical specialty was noncardiac surgery. Prediction horizon was 30‐day MACE. | ||
| 2 studies 10,524 patients 1560 MACE | Reclassification | NRI | 0.74 (0.26 to 1.22) | Surgical specialty was noncardiac and vascular surgery. Prediction horizon was 30‐day MACE and long‐term MACE (> 30 days). | ||
| 1 study 122 patients 29 MACE | — | IDI | 0.23 | Surgical specialty was vascular surgery. Prediction horizon was long‐term MACE (> 30 days). | ||
| Troponin + NT‐proBNP | 3 studies 575 patients 120 MACE | Discrimination | Delta c‐statistic | 0.12 (0.1 to 0.34) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| BNP | 0 studies | Discrimination | — | — | — | |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 874 patients unknown MACE | Reclassification | NRI | 0.72 (0.47 to 0.96) | Results are based on two studies as one study did not report the total NRI. Surgical specialty was orthopaedic and vascular surgery. Prediction horizon was 30‐day MACE. For one study, the number of outcomes was not reported. | ||
| All‐cause mortality and MACE | NT‐proBNP | 3 study 12,214 patients 548 events | Discrimination | Delta c‐statistic | 0.06 (0.06 to 0.07) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was 30‐day events. |
| 1 study 411 patients 74 events | Calibration | Hosmer Lemeshow | P = 0.03 | Surgical specialty was vascular surgery. Prediction horizon was 30‐day events. | ||
| 2 study 1812 patients 102 events | Reclassification | NRI | 0.19 (0.13 to 0.25) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was 30‐day events. | ||
| 1 study 411 patients 74 events | — | IDI | 0.06 | Surgical specialty was vascular surgery. Prediction horizon was 30‐day events. | ||
| Myocardial infarction | NT‐proBNP | 2 studies 2626 patients 132 MI | Discrimination | Delta c‐statistic | 0.09 (0.06 to 0.11) | Surgical specialty was noncardiac surgery. Prediction horizon was within 3 days after surgery and in‐hospital events. |
| 0 studies | Calibration | — | — | — | ||
| 1 study 572 patients 30 MI | Reclassification | NRI | 0.46 | Surgical specialty was noncardiac surgery. Prediction horizon was within 3 days after surgery. | ||
IDI: integrated discrimination index; MACE: major adverse cardiac event(s); MI: myocardial infarction; NRI: net reclassification index
Troponin is a cardiac biomarker that reflects myocardial ischaemia.
Both BNP (B‐type natriuretic peptide) and NT‐proBNP (N‐terminal (NT)‐pro hormone BNP) are released by cardiomyocytes due to myocardial stretch and used in clinical practice as a marker for heart failure.
Summary of findings 2. Summary of findings ‐ objective 2: comparison of predictive performance of biomarkers to the RCRI.
|
Population: patients undergoing noncardiac surgery Index model: Revised Cardiac Risk Index (RCRI) Comparator: predictive performance of biomarker(s) alone Outcome: postoperative occurrence of (in‐hospital) major adverse cardiac events (MACE), all‐cause mortality and other adverse outcomes Timing: time point of prognostication: before surgery; prediction horizon: in‐hospital, but all time spans are included Setting: to inform physicians of the patient's risk of developing in‐hospital events after noncardiac surgery | ||||||
| Outcomes | Biomarker | № of participants (studies) | Measure | Pooled result | Comments | |
| Summary measure | Median (range) | |||||
| MACE | ASA | 6 studies 84,145 patients 5415 MACE | Discrimination | Delta c‐statistic | ‐0.02 (‐0.18 to 0.03) | Surgical specialty was orthopaedic, vascular and noncardiac surgery. One study reported on intraoperative MACE (hypotension, hypertension, bradycardia and tachycardia), which contributed most outcomes. Prediction horizon was intraoperative or in‐hospital or 30‐day MACE. |
| 1 study 29,437 patients 5249 MACE | Calibration | Calibration plot | Poor calibration | Poor calibration for both RCRI and ASA. This study reported on intraoperative MACE. Surgical specialty was noncardiac surgery. | ||
| 1 study 29,437 patients 5249 MACE | — | Hosmer Lemeshow | P < 0.0001 | This study reported on intraoperative MACE. Surgical specialty was noncardiac surgery. | ||
| 0 studies | Reclassification | — | — | — | ||
| BNP | 6 studies 1451 patients NA MACE | Discrimination | Delta c‐statistic | 0.15 (0.0 to 0.24) | For one study, the number of outcomes was not reported. Surgical specialties were orthopaedic, general, vascular and noncardiac surgery. Prediction horizon was in‐hospital or 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| NT‐proBNP | 6 studies 3256 patients 457 MACE | Discrimination | Delta c‐statistic | 0.15 (0.02 to 0.22) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was in‐hospital, 30‐day and 6‐month MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| CRP | 2 studies 145 patients 15 MACE | Discrimination | Delta c‐statistic | ‐0.01 (‐0.12 to 0.10) | Surgical specialty was vascular and noncardiac surgery. Prediction horizon was in‐hospital and 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| All‐cause mortality and MACE | BNP | 2 studies 248 patients 27 events | Discrimination | Delta c‐statistic | 0.21 (0.18 to 0.23) | Surgical specialty was noncardiac surgery. Prediction horizon was in‐hospital or 30 day events. |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Troponin | 2 studies 1154 patients 52 events | Discrimination | Delta c‐statistic | 0.09 (0.09 to 0.10) | Surgical specialty was noncardiac surgery. Prediction horizon was in‐hospital and 30‐ay events. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Myocardial infarction | ASA | 2 studies 52,638 patients 106 MI | Discrimination | Delta c‐statistic | 0.02 (‐0.07 to 0.12) | Surgical specialty was neurosurgery and noncardiac surgery. Prediction horizon was within 7 days or 30 days after surgery. |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| All‐cause mortality | ASA | 5 studies 124,400 patients 1040 deaths | Discrimination | Delta c‐statistic | 0.05 (‐0.05 to 0.24) | Surgical specialty was general, neurosurgery, vascular and noncardiac surgery. Prediction horizon was in‐hospital or 30‐day all‐cause mortality. |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| BNP | 2 studies 825 patients unknown deaths | Discrimination | Delta c‐statistic | 0.14 (0.08 to 0.21) | Surgical specialty was orthopaedic and vascular surgery. For one study, the number of deaths was not reported. Prediction horizon for one study was 30 days and the other was 1‐year all‐cause mortality. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| NT‐proBNP | 2 studies 1314 patients 74 deaths | Discrimination | Delta c‐statistic | 0.10 (0.09 to 0.11) | Surgical specialty was orthopaedic and vascular surgery. Prediction horizon for one study was in‐hospital and within 6 weeks after surgery. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Other | ASA | 6 studies 126,963 patients | Discrimination | Delta c‐statistic | ‐ a | Surgical specialty was neurosurgery and noncardiac surgery. Prediction horizon was within 7 days or 30 days after surgery. |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
IDI: integrated discrimination index; MACE: major adverse cardiac event(s); MI: myocardial infarction; NRI: net reclassification index
ASA: American Society of Anesthesiologists physical status, which is a tool commonly used to classify a patient's physical fitness before surgery.
Troponin is a cardiac biomarker that reflects myocardial ischaemia.
Both BNP (B‐type natriuretic peptide) and NT‐proBNP (N‐terminal (NT)‐pro hormone BNP) are released by cardiomyocytes due to myocardial stretch and used in clinical practice as a marker for heart failure.
C‐reactive protein (CRP) is a sensitive systemic marker of inflammation and tissue damage.
Summary of findings 3. Summary of findings ‐ objective 3: comparison of predictive performance of other prediction models to the RCRI.
|
Population: patients undergoing noncardiac surgery Index model: Revised Cardiac Risk Index (RCRI) Comparator: other prediction models Outcome: postoperative occurrence of (in‐hospital) major adverse cardiac events (MACE), all‐cause mortality and other adverse outcomes Timing: time point of prognostication: before surgery; prediction horizon: in‐hospital, but all time spans are included Setting: to inform physicians of the patient's risk of developing in‐hospital events after noncardiac surgery | ||||||
| Outcomes | Prediction model | № of participants (studies) | Measure | Pooled result | Comments | |
| Summary measure | Median (range) | |||||
| MACE | ACS‐NSQIP‐MICA | 3 studies 1567 patients 95 MACE | Discrimination | Delta c‐statistic | 0.00 (‐0.09 to 0.04) | Surgical specialty was neurosurgery, vascular and noncardiac surgery. Prediction horizon was in‐hospital or 30‐day MACE. The prediction horizon was not reported in one study. |
| 1 study 870 patients 76 MACE | Calibration | Calibration plot | Poor calibration | Poor calibration for both RCRI and NSQIP MACE. Calibration improved after recalibration of NSQIP MACE. Surgical specialty was noncardiac surgery. | ||
| Calibration intercept | 0.95 for RCRI and 2.37 for NSQIP‐MICA | — | ||||
| Calibration slope | 0.29 for RCRI and 0.70 for NSQIP‐MICA | — | ||||
| 0 studies | Reclassification | — | — | — | ||
| ACS‐NSQIP‐SRS | 2 studies 1087 patients 26 MACE | Discrimination | Delta c‐statistic | 0.06 (0.00 to 0.11) | Surgical specialty was noncardiac surgery. Prediction horizon was in‐hospital or 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Detsky | 3 studies 3361 patients 191 MACE | Discrimination | Delta c‐statistic | 0.05 (‐0.07 to 0.11) | Surgical specialty was orthopaedic, vascular and noncardiac surgery. Prediction horizon was in‐hospital or 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Goldman | 3 studies 3361 patients 191 MACE | Discrimination | Delta c‐statistic | ‐0.03 (‐0.07 to 0.08) | Surgical specialty was orthopaedic, vascular and noncardiac surgery. Prediction horizon was in‐hospital or 30‐day MACE. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| VSG‐CRI | 3 studies 2023 patients 208 MACE | Discrimination | Delta c‐statistic | 0.03 (0.00 to 0.05) | Surgical specialty was vascular surgery. Prediction horizon was in‐hospital MACE. In one study, the prediction horizon was not reported. | |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| Myocardial infarction or cardiac arrest | ACS‐NSQIP‐MICA | 6 studies 243,896 patients unknown MICA | Discrimination | Delta c‐statistic | 0.11 (‐0.05 to 0.39) | Surgical specialty was general, vascular, orthopaedic and noncardiac surgery. Prediction horizon was 30‐day MICA. The prediction horizon was not reported in one study. |
| 2 studies 181,920 patients 1889 MICA | Calibration | Calibration plot | Poor calibration | Calibration was poor for both scores, however calibration was better for the RCRI compared to the NSQIP‐MICA. Calibration improved after recalibration of NSQIP‐MICA. Surgical specialty was noncardiac surgery. Prediction horizon was 30‐day MICA, but was not reported in one study. | ||
| 2 studies 43,047 patients 463 MICA | — | Hosmer Lemeshow | RCRI: P = 0.018 to P < 0.001 ACS‐NSQIP‐MICA P < 0.001 |
Surgical specialty was general and noncardiac surgery. Prediction horizon was 30‐day MICA, but was not reported in one study. | ||
| 0 studies | Reclassification | — | — | — | ||
| ACS‐NSQIP‐SRS | 2 studies 9678 patients 94 MICA | Discrimination | Delta c‐statistic | 0.18 (0.13 to 0.22) | Surgical specialty was noncardiac surgery or not specified. Prediction horizon was 30‐day MICA. The prediction horizon was not reported in one study. | |
| 1 study 9015 patients 91 MICA | Calibration | Calibration plot | RCRI: poor calibration, ACS‐NSQIP‐SRS: acceptable calibration | Surgical specialty was noncardiac surgery. Prediction horizon was not reported. | ||
| 1 study 9015 patients 91 MICA | Hosmer Lemeshow | RCRI: P < 0.001 ACS‐NSQIP‐SRS P = 0.07 |
Surgical specialty was noncardiac surgery. Prediction horizon was not reported. | |||
| 0 studies | Reclassification | — | — | — | ||
| All‐cause mortality | ACS‐NSQIP‐SRS | 3 studies 2461 patients 155 deaths | Discrimination | Delta c‐statistic | 0.15 (0.12 to 0.47) | Surgical specialty was neurosurgery or noncardiac surgery. The prediction horizon was in‐hospital or 30‐day events. In one study the prediction horizon was not reported. |
| 0 studies | Calibration | — | — | — | ||
| 0 studies | Reclassification | — | — | — | ||
| CHADS2 | 3 studies 35129 patients 1177 deaths | Discrimination | Delta c‐statistic | 0.00 (‐0.02 to 0.01) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | |
| 0 studies | Calibration | — | — | — | ||
| 3 studies 35129 patients 1177 deaths | Reclassification | NRI | 0.07 (0.01 to 0.12) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| CHADS2VASc | 2 studies 2969 patients 121 deaths | Discrimination | Delta c‐statistic | 0.00 (‐0.02 to 0.02) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 2969 patients 121 deaths | Reclassification | NRI | 0.09 (0.01 to 0.17) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| R2CHADS2 | 3 studies 35129 patients 1177 deaths | Discrimination | Delta c‐statistic | ‐0.03 (‐0.03 to 0.03) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | |
| 0 studies | Calibration | — | — | — | ||
| 3 studies 35129 patients 1177 deaths | Reclassification | NRI | 0.03 (‐0.09 to 0.13) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| Stroke | CHADS2 | 4 studies unknown patients unknown events | Discrimination | Delta c‐statistic | 0.02 (‐0.01 to 0.11) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study the number of included patients and number of events were not reported. |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 33121 patients 391 events | Reclassification | NRI | 0.05 (‐0.06 to 0.17) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| CHADS2VASc | 3 studies unknown patients unknown events | Discrimination | Delta c‐statistic | 0.04 (0.00 to 0.12) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study the number of included patients and number of events were not reported. | |
| 0 studies | Calibration | — | — | — | ||
| 1 studies 961 patients 11 events | Reclassification | NRI | 0.07 | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| R2CHADS2 | 3 studies unknown patients unknown events | Discrimination | Delta c‐statistic | 0.05 (0.01 to 0.12) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study the number of included patients and number of events were not reported. | |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 33,121 patients 391 events | Reclassification | NRI | ‐0.06 (‐0.14 to 0.01) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. | ||
| All‐cause mortality or stroke | CHADS2 | 3 studies 33,748 patients unknown events | Discrimination | Delta c‐statistic | 0.03 (0.02 to 0.07) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. |
| 0 studies | Calibration | — | — | — | ||
| 3 studies 33,748 patients unknown events | Reclassification | NRI | 0.31 (0.14 to 0.35) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. | ||
| CHADS2VASc | 2 studies 1588 patients unknown events | Discrimination | Delta c‐statistic | 0.04 (0.01 to 0.07) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. | |
| 0 studies | Calibration | — | — | — | ||
| 2 studies 1588 patients unknown events | Reclassification | NRI | 0.30 (0.24 to 0.36) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. | ||
| R2CHADS2 | 3 studies 33,748 patients unknown events | Discrimination | Delta c‐statistic | 0.03 (0.01 to 0.06) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. | |
| 0 studies | Calibration | — | — | — | ||
| 3 studies 33,748 patients unknown events | Reclassification | NRI | 0.17 (0.11 to 0.44) | Surgical specialty was noncardiac surgery. The prediction horizon was 30‐day events. For one study, the number of outcomes was not reported. | ||
MACE: major adverse cardiac event(s); MICA: composite outcome of myocardial infarction and cardiac arrest; NRI: net reclassification index; RCRI: Revised Cardiac Risk Index.
ACS‐NSQIP‐MICA provides a risk estimate of 30‐day myocardial infarction or cardiac arrest (MICA) in patients undergoing noncardiac surgery (Gupta 2011).
The ACS‐NSQIP surgical risk score (ACS‐NSQIP‐SRS) is a decision‐support tool based, which can be used to estimate the risks of multiple outcomes (including myocardial infarction) for most operations (Bilimoria 2013).
The CHADS2, CHA2DS2‐VASc and R2CHA2DS2 are risk scores that predict stroke in patients diagnosed with atrial fibrillation (Gage 2001; Lip 2010; Piccini 2013).
The Goldman index represents a multivariable approach to estimate cardiac risk in patients undergoing noncardiac procedures (Goldman 1977).
The Detsky index is a modified version of an index that was previously generated by Goldman in 1977 (Detsky 1986).
Vascular Study Group of New England Cardiac Risk Index (VSG‐CRI) is a prediction model to predict a composite cardiac outcome of in‐hospital myocardial infarction, clinically significant new arrhythmia or congestive heart failure (CHF) in patients undergoing vascular surgery (Bertges 2010).
Background
Description of the condition
Worldwide, over 300 million patients undergo intermediate‐ to high‐risk noncardiac surgery every year (Rose 2015), and this number has been increasing continuously (Weiser 2015). Despite the beneficial aspects of surgery, approximately 19% of these patients will suffer an in‐hospital major adverse event (ISOSG 2016). The most common complications are infectious (33%) or have a cardiovascular origin (19%), with the highest mortality rates in the latter (7%). However, such complications are difficult to diagnose, as typical symptoms are often not present in most postoperative patients (e.g. chest pain may be masked by pain medication). Therefore, preoperative risk stratification of these patients using available clinical information is an important component of any strategy to prevent these complications and has been recommended by clinical guidelines (Fleisher 2014; Kristensen 2014). Informing patients and physicians about perioperative risks by, for example, performing additional diagnostic tests or interventions aimed at preventing postoperative complications might enhance patient management and optimisation before surgery.
Description of the prognostic model
The Revised Cardiac Risk Index (RCRI) is a predictive tool to be applied before surgery (Lee 1999). It estimates the postoperative probability of a major adverse cardiac events (MACE) in patients undergoing noncardiac surgery. The RCRI is specially developed for patients undergoing noncardiac surgery and contains six equally weighted predictors, including high‐risk surgery, history of ischaemic heart disease, history of cerebrovascular disease, chronic heart failure, renal insufficiency and insulin‐dependent diabetes (Table 4). Although the RCRI was published over two decades ago, it is still commonly recommended and used in daily clinical practice (Duceppe 2017; Fleisher 2014; Kristensen 2014), as the predictors are easy to collect and calculation of the score and probability are convenient. A systematic review that examined the performance of the RCRI in external validation studies concluded that the RCRI discriminated moderately well between patients at low versus high risk in predicting cardiac events after noncardiac surgery (Ford 2010). However, the predictive ability of the RCRI for patients undergoing vascular surgery was less accurate (Ford 2010).
1. Scoring of the Revised Cardiac Risk Index.
| Predictor | Definition | Point distribution |
| High‐risk surgery | Intraperitoneal, intrathoracic, or suprainguinal vascular surgery | 1 |
| Ischaemic heart disease | History of myocardial infarction, positive exercise test, current complaint of ischaemic chest pain or use of nitrate therapy, or ECG with Q waves. Patients with prior CABG surgery or PTCA were included in this definition only if they had current complaints of chest pain that were presumed to be due to ischaemia. | 1 |
| History of congestive heart failure | History of congestive heart failure, pulmonary oedema, or paroxysmal nocturnal dyspnoea, physical examination showing bilateral rales or S3 gallop, or chest radiograph showing pulmonary vascular redistribution. | 1 |
| History of cerebrovascular disease | History of transient ischaemic attack or stroke. | 1 |
| Insulin therapy for diabetes mellitus | — | 1 |
| Preoperative serum creatinine > 2.0 mg/dL | — | 1 |
Complication rates in patients with none of these predictors is 0.4%, with 1 point is 1.0%, 2 points is 7% and 3 or more points is 11%.
CSBG: coronary artery bypass graft; ECG: electrocardiogram; PTCA: percutaneous transluminal coronary angioplasty
To improve the predictive performance of the RCRI, the added value of different biomarkers to the RCRI has been extensively studied in recent years. These biomarkers could originate from blood, such as troponin (Gillmann 2014; Kopec 2017), (NT‐pro)brain natriuretic peptide (BNP) (Choi 2010; Scrutinio 2014) and C‐reactive protein (CRP) (Choi 2010; Scrutinio 2014). Besides biomarkers derived from blood, many imaging markers, such as electrocardiography (Noordzij 2006; van Klei 2007), and coronary computed tomographic angiography (Sheth 2015), have also been used to assess their added predictive value to the RCRI. Altogether, addition of new biomarkers to the RCRI seems to improve the predictive performance of the RCRI (Choi 2010; Gillmann 2014; Kopec 2017; Scrutinio 2014).
Besides the addition of new biomarkers to the RCRI, various studies have compared the predictive ability of biomarkers to the RCRI. Again, the biomarkers compared were most commonly derived from blood, such as (NT‐pro) BNP (Katsanos 2015; Mercantini 2012) and troponin (Weber 2013), and from imaging, such as thoracic echocardiography (Park 2011).
Finally, the predictive ability of the RCRI has also been compared to other prediction models to predict various outcomes, including the ACS‐NSQIP Surgical Risk Score (Bilimoria 2013; Cohn 2018; Gupta 2011; Markovic 2018) and the NSQIP‐MICA model (Asuzu 2018; Gupta 2011).
Health outcomes
The RCRI was originally developed to predict postoperative in‐hospital occurrence of MACE. Annually, over 10 million patients undergoing noncardiac surgery develop a MACE (Devereaux 2017; ISOSG 2016; van Waes 2016; Weiser 2015). MACE are a leading cause of morbidity and mortality in this patient population (Devereaux 2012; Devereaux 2017; Ekeloef 2016). Additionally, MACE have been associated with prolonged hospitalisation and increased medical costs (Mackey 2006). In cardiovascular research, MACE are most commonly used as a composite outcome and include, among others, cardiac death, (non)fatal myocardial infarction, cardiac arrest, arrhythmias, congestive heart failure or emergent coronary bypass graft surgery. However, varying composites of cardiac outcomes to define MACE are still used within different research groups and publications, which hampers comparison of results over different studies (Kip 2008). As a response to this phenomenon, the systematic review and consensus definitions for the Standardized Endpoints in Perioperative Medicine (StEP) initiative recently published a consensus statement on standardised definitions of cardiovascular outcomes in anaesthesia research (Beattie 2020). In this consensus statement, a MACE was defined as the composite of myocardial infarction, nonfatal cardiac arrest, cardiac death and coronary revascularisation within 30 days of surgery (Beattie 2020).
Besides the use of the RCRI to predict in‐hospital MACE occurrence, several other outcomes have been studied, notably all‐cause mortality (Katsanos 2015; Weber 2013), and noncardiac complications such as sepsis, respiratory failure, renal failure, readmission, discharge to a nursing facility etc. (Bronheim 2018; Ehlert 2016; Makary 2010; Press 2006).
Why it is important to do this review of these prognostic models
Elderly and multi‐morbid patients undergoing noncardiac surgery are more likely to develop perioperative complications (Jammer 2015; Wolff 2002). This suggests that preoperative risk stratification in such patients is essential to direct healthcare towards those that most need it. Preoperative risk stratification of noncardiac surgical patients could easily be performed during the pre‐anaesthesia outpatient clinic visit using routine measurements of biomarkers and/or the use of prognostic models including, for example, the RCRI and ACS‐NSQIP‐MICA model (Lee 1999; Mayhew 2019). More intensified monitoring of noncardiac surgery patients at increased postoperative risk of MACE or other major complications might result in better prevention of such complications and their consequences in the long term.
To date, many authors have aimed to improve predictions of cardiovascular outcomes in the perioperative period by reporting on the added predictive value of biomarkers to the RCRI (Choi 2010; Gillmann 2014; Kopec 2017; Scrutinio 2014). In addition, others have compared the predictive performance of biomarkers themselves or other prediction models to the RCRI (Bronheim 2018; Park 2011; Weber 2013). As no systematic review has currently been conducted on this topic, we aimed to provide a comprehensive overview of all the evidence.
Objectives
Primary objective
The primary objective of this systematic review is to quantify the added predictive value of biomarkers to the RCRI to preoperatively predict the in‐hospital occurrence of MACE and other adverse outcomes in patients undergoing noncardiac surgery (see Table 5 for the PICOTS).
2. PICOTS for the objectives based on the CHARMS checklist.
| Population | Patients undergoing noncardiac surgery |
| Index Model | Revised Cardiac Risk Index (RCRI) |
| Comparator | Biomarker(s) added or compared to the RCRI; other prediction models compared to the RCRI |
| Outcome(s) | Postoperative occurrence of (in‐hospital) major adverse cardiac events, all‐cause mortality and other adverse outcomes |
| Timing | Time point of prognostication: before surgery Prediction horizon: in‐hospital, but all time spans are included |
| Setting | To inform physicians of the patient's risk of developing in‐hospital events after noncardiac surgery |
Other objectives
The secondary objective is to investigate the prognostic value of biomarkers as compared to the RCRI to preoperatively predict the in‐hospital occurrence of MACE and other adverse outcomes in patients undergoing noncardiac surgery.
The third objective is to examine the prognostic value of other prediction models as compared to the RCRI to preoperatively predict the in‐hospital occurrence of MACE and other adverse outcomes in patients undergoing noncardiac surgery.
Investigation of sources of heterogeneity between studies
The RCRI was originally developed for the preoperative prediction of in‐hospital MACE in the noncardiac, nonvascular surgical population (Lee 1999). We expected various sources of heterogeneity that we planned to investigate where possible:
Differences in studied noncardiac surgical subpopulations, such as vascular (Gillmann 2014; Scrutinio 2014) and orthopaedic surgical patients (Katsanos 2015; Vetrugno 2014).
Variation in the composites used to define MACE.
Prediction of other outcomes besides MACE, including all‐cause mortality and noncardiac complications.
Prediction horizons varying from intraoperative events to long‐term events (i.e. one year).
Use of other definitions for the RCRI predictors or unclear predictor definitions, especially for the predictors ischaemic heart disease, congestive heart failure and high‐risk surgery (Feringa 2007; Gualandro 2018; Katsanos 2015).
Where biomarkers have been added or compared to the RCRI, variations in the assay used to measure a particular biomarker, the threshold used to define elevation and the way the biomarkers have been entered into the prediction model (i.e. continuous, categorical or dichotomous).
Methods
Criteria for considering studies for this review
Types of studies
We considered all original research reports that studied the predictive accuracy of the RCRI for inclusion regardless of study design, or language. We excluded studies that were only published as conference abstracts because of the lack of sufficient information.
Types of participants (target population)
We included studies on adult (≥ 18 years) patients undergoing any type of noncardiac surgery.
Types of prognostic models
To address the three separate objectives of this review, we included all studies reporting on either:
the addition to the RCRI of one or more preoperatively measured biomarker, including blood, imaging or other type of predictor(s);
the comparison of the predictive accuracy of the RCRI model to one or more of these preoperatively measured biomarker(s);
the comparison of the predictive accuracy of the RCRI model to other prognostic models.
We defined a biomarker as a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes or pharmacologic responses to a therapeutic intervention (Biomarkers Definitions Working Group 2001). In essence, this broad definition includes all predictors that have been added or compared to the RCRI, including, for example, predictors from demographics, history taking, physical examination, blood or urine measurements, imaging and omics. We excluded studies reporting solely on the external validation of the original RCRI without any addition or comparison of a biomarker or another model, respectively, from this review.
Types of outcomes
The primary outcome of interest was in‐hospital MACE, as used for the original RCRI model development paper (Lee 1999). For this definition, we made no distinction between fatal and nonfatal MACE. As secondary outcomes, we included all other outcomes that were studied for the external validation of the RCRI, such as all‐cause mortality, myocardial infarction and noncardiac complications.
In addition, there is a wide variation in the prediction horizons, ranging from studies reporting on prediction of intraoperative events (Rohrig 2004) to long‐term post‐discharge events (Subramaniam 2011). Altogether, we made no a priori restrictions based on the type of outcome and prediction horizon used for inclusion in this review.
Search methods for identification of studies
Electronic searches
The original development study for the RCRI was published in 1999 (Lee 1999). Therefore, all our searches started from 1999 onwards. We searched the following databases on 25 June 2020: MEDLINE and Embase (Ovid, 1 January 1999 to 25 June 2020). We used a prediction model search filter developed by Geersing et al (Geersing 2012), and extended the filter to also identify studies reporting on the validation or updating of prediction models, as well as the added value of variables to existing prediction models. The Geersing search filter was originally designed for searches in Ovid MEDLINE (Geersing 2012); however, for this review we also adapted the search strategy for use in Ovid Embase. Further, we used synonyms of the RCRI, including 'revised Goldman index' and 'Lee index'. The search strategies are reported in Appendix 1 and Appendix 2.
In addition, we searched in both ISI Web of Science and SCOPUS (1 January 1999 to 25 June 2020) for articles referring to the original RCRI development study (Lee 1999). As the RCRI is a revised model of the Cardiac Risk Index by Goldman (Goldman 1977) and Detsky (Detsky 1986), we also searched all references referring to these publications from 1999 onwards. We searched the clinical trial registers ClinicalTrials.gov (www.clinicaltrials.gov; searched 27 July 2020) and World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (apps.who.int/trialsearch; searched 27 July 2020; Appendix 3) for ongoing trials. We checked Retraction Watch Database for retractions of included articles (retractiondatabase.org/RetractionSearch) (searched 27 July 2020). There was no language restriction so as to reduce language bias.
We checked all identified ongoing studies for completion and published results on 25 November 2021.
Searching other resources
We carried out a cross‐reference check of all retrieved articles in PubMed and relevant review articles to identify other eligible articles, including the review by Ford published in 2010 (Ford 2010).
Data collection and analysis
Selection of studies
Two review authors (JAD, LMV) independently screened the results of the searches for eligibility based on title and abstract. In case of disagreement, abstracts were included for full text screening.
In contrast with the protocol (Vernooij 2018), selection of studies based on full text was performed in two stages. In the first step, one review author (LMV) assessed whether the RCRI was mentioned in the 'Results' and/or 'Methods' section of the article. This was done by searching for the terms 'RCRI' or often used synonyms, i.e. 'revised Goldman index' and 'Lee index', or by searching where in the report the original paper was referenced. If this was not the case, these articles were excluded.
We screened the remaining studies for inclusion in the review. This screening was performed independently by two review authors from a team of four (JAD, TT, JAvW, LMV) according to the above criteria using a predefined electronic spreadsheet. Any disagreements were resolved through discussion or by involving a third review author (JAD or JAvW) when necessary.
Data extraction and management
We developed a predefined electronic data extraction form containing items based on the CHARMS checklist (Debray 2017; Moons 2014; Riley 2019). These items address potential critical appraisal issues and issues that may affect the applicability of the results in relation to the intended use of the prediction model. The data extraction form was first piloted on five included articles by three review authors (JAD, JAvW and LMV) and subsequently updated to optimise it to the final format. Two review authors from a team of four (JAD, TT, JAvW, LMV) independently extracted the data from the selected articles. In case of any disagreement, this was resolved by discussion or a third review author was involved to reach consensus.
We extracted data for the following items (see Appendix 4 for a detailed data extraction list): study design, participant eligibility criteria, study dates, case mix (such as age, sex), outcome definition and measurement, prediction horizon, RCRI predictor definitions and measurement, predictors that were added or compared, number of participants and events, details on (handling of) missing data, and model performance in terms of calibration, discrimination, reclassification and other measures for the original and extended model, and the biomarker and prediction model to which the model was compared.
Assessment of risk of bias of included studies
We used the Prediction model Risk of Bias Assessment Tool (PROBAST) for risk of bias and applicability assessment (Moons 2019; Wolff 2019). In short, we assessed risk of bias according to four domains, i.e. participants, predictors, outcomes and analysis. For each domain, we rated risk of bias as either 'Low risk of bias', 'High risk of bias' or 'Unclear risk of bias' based on signalling questions provided by the PROBAST tool (Moons 2019; Wolff 2019). Based on the domain level assessments, we established overall risk of bias and judgements per study as follows:
'low risk of bias': for studies in which all four domains were scored as low risk of bias;
'high risk of bias': for studies in which at least one domain was assessed as high risk of bias;
'unclear risk of bias': for studies in which at least one domain was rated as 'unclear' and the other domains were scored as 'low risk of bias'.
Besides assessment of risk of bias, PROBAST also provides judgement of the applicability of the included studies to the review question with the following response options: 'low concern', 'high concern' or 'unclear concern' regarding applicability. A similar approach as used for the risk of bias assessment holds for the overall judgement for applicability.
Risk of bias and applicability were independently assessed by two review authors in a team of four (JAD, TT, JAvW and LMV) for each included article. Consensus was reached by discussion or, in case of any disagreements, a third review author was involved for the final judgement (JAD, JAvW).
Measures of predictive performance to be extracted
For all three objectives, we extracted the reported predictive performance measures from each of the selected articles including calibration, discrimination and reclassification measures and the uncertainty around these measures (standard errors or confidence intervals). Calibration indicates the extent to which the expected number of outcomes (i.e. the probability of the outcome as predicted by the prediction model) and the observed frequency of the outcome agree (Harrell 2015; Riley 2019; Steyerberg 2009). Extracted calibration performance measures – if reported ‐ were calibration plots, calibration slopes and observed to expected ratios (O:E ratio). Discrimination refers to the ability of the prediction model to discriminate between those with and without the outcome event (Harrell 2015; Riley 2019; Steyerberg 2009). The most commonly used discrimination measure is the concordance‐statistic, i.e. c‐statistic, which we also extracted for this review. We also extracted the delta c‐statistic, i.e. the difference between the c‐statistic of the RCRI model alone versus the RCRI model added with the biomarker(s) (for objective 1) and for the comparison between biomarkers or prediction models to the RCRI (objective 2 and 3). Furthermore, we extracted reclassification measures including the integrated discrimination improvement (IDI) and the net reclassification index (NRI), when reported.
Dealing with missing data
In case of any missing data about the predictive performance measures of the RCRI, extended RCRI and other prediction models, we planned to contact the original investigators to provide this missing information. However, in contrast to the protocol (Vernooij 2018), we concluded that contacting authors for missing information would not lead to different review findings as we encountered large heterogeneity in the study population, outcome definitions, prediction horizons and studied biomarkers or prediction models. Missing data for the confidence intervals around the C‐statistic were estimated using the guidance and formulas described by Debray et al (Debray 2017).
Assessment of heterogeneity
We investigated clinical and statistical heterogeneity based on the items mentioned in the section 'Investigation of sources of heterogeneity between studies'. In particular, we discussed differences in surgical populations studied, in the composition of MACE and other predicted outcomes, and in prediction horizons within the author team. To assess between‐study heterogeneity across the included studies, we inspected the forest plots of the extracted predicted performance measures. To further explore causes of heterogeneity, we predefined subgroup analyses (specified in further detail below under 'Subgroup analysis and investigation of heterogeneity').
Assessment of reporting deficiencies
Current guidelines (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis; TRIPOD) recommend the reporting of calibration and discrimination measures for all prediction models (Collins 2015; Moons 2015). However, several systematic reviews focusing on the methodological conduct and reporting of prognostic models found that these performance measures are frequently not reported (Bouwmeester 2012; Collins 2013; Collins 2014; Heus 2018; Laupacis 1997; Mallett 2010). Therefore, we also evaluated which predictive performance measures were reported and which were not reported in the selected studies. Most studies reporting on prognostic models are not prospectively registered and no protocol has been published (Peat 2014), which makes a formal assessment of potential reporting bias difficult. We used sensitive search strategies to increase retrieval (Geersing 2012).
Data synthesis
Data synthesis and meta‐analysis approaches
An overview of all included articles was created, sorted by the biomarker added to the RCRI and on the predicted outcomes. This overview included parameters such as publication year, type of surgery, number of patients included, biomarker(s) added and outcome definition. We created a similar overview for the articles reporting on the comparison of the predictive accuracy of one or more biomarkers to the RCRI (objective 2), and for the articles comparing the predictive performance of other prediction models to the RCRI (objective 3). As one article could have reported more than one validation of the RCRI, e.g. by using multiple outcomes or study populations, the number of validations may not correspond to the number of included articles. Therefore, results on study characteristics and (composite) outcomes are presented per uniquely reported outcome for each objective separately. Risk of bias and concern regarding applicability, and reporting rates of predictive performance measures, are reported per included article.
We planned to perform a meta‐analysis of the predictive performance (O:E ratio, c‐statistic and net reclassification index) of the RCRI model across the various validation studies as compared to the RCRI with the biomarker(s) added (objective 1). However, this turned out to be impossible due to the low number of studies reporting on the added value of the same biomarker and due to the differences in included study populations and in the outcome definitions between studies.
Instead, we presented the performance measures (c‐statistic) for RCRI models extended with biomarkers that were studied in at least three studies in forest plots, without presenting a pooled estimate. Meta‐analysis of the c‐statistic was also planned for the studies that compared the RCRI to biomarkers alone (objective 2), if there were at least three studies reporting on the same biomarker and with a similar outcome definition, prediction horizon and scale on how the predictor was studied (i.e. continuous, categorical or dichotomous). As there was no set of studies fulfilling these criteria, meta‐analysis of the c‐statistic for objective 2 also turned out not to be possible. We therefore visualised the results in forest plots without presenting a pooled estimate.
Similar to objective 1 and 2, meta‐analysis of the c‐statistics was not possible for the studies that compared the predictive performance of other prediction models to the RCRI. For prediction models for which the predictive performance was compared to the RCRI at least three times, we made forest plots to visualise the results without presenting a pooled estimate.
Meta‐analysis of the O:E ratio had also been planned, but turned out not to be possible due to the low number of studies reporting any calibration measures. We performed all analyses in Rstudio using the packages metafor (Viechtbauer 2010) and metamisc (Debray 2018).
Subgroup analysis and investigation of heterogeneity
The following subgroup analyses were planned:
vascular surgery patients versus other noncardiac surgery patients;
patients undergoing elective versus emergency surgery;
different prediction horizons, e.g. in‐hospital, 30‐day and long‐term events;
patients in different age categories.
For the same reasons as mentioned above, meta‐analysis in these subgroups was not possible. Again, we stratified the forest plots according to the subgroups based on outcome, and reported the prediction horizon in the plot. Details on the surgical population and age categories are reported in the 'Description of included studies' table. We explored potential sources of heterogeneity by assessing case mix variation and differences in study characteristics (e.g. study design and prospective versus retrospective data collection). We had planned meta‐regression to explore the cause and extent of the between‐study heterogeneity but this turned out not to be possible (Debray 2017; Riley 2011).
Sensitivity analysis
We had planned sensitivity analyses excluding studies with high risk of bias (at least four domains rated 'high') and excluding unpublished studies and studies with missing data but we did not perform these due to the large heterogeneity between studies.
Rating the certainty of evidence and summary of findings
We had planned a summary of findings table using GRADE to present the body of evidence of the included prognostic studies. However, GRADE guidance for grading the certainty of results from prognostic studies is currently not available (Kreuzberger 2020). Therefore, the summary of findings table presents descriptive results (i.e. without pooled estimates) for studies reporting on biomarkers/prediction models that were added or compared to the RCRI in at least three different studies and were validated using a similar outcome in at least two different studies. This means that outcomes that were only validated once in any of the included studies were not included in the summary of findings table.
Results
Description of studies
Results of the search
We identified a total of 3672 records through database searching and an additional 4251 records from citations to the development study of the RCRI (Lee 1999) and the studies of Goldman and Detsky (Detsky 1986; Goldman 1977). After removal of 2715 duplicates and 1248 articles that were published before the development study for the RCRI in 1999, we screened 3960 articles based on title and abstract, of which 1061 articles were selected for full‐text screening. As mentioned before, we performed full‐text screening in two stages. In the first stage, we characterised 43 articles as 'Awaiting classification' as the full text could not be retrieved. We discarded another 630 articles because they did not mention the RCRI in either the 'Methods' or 'Results' section of the article. In the second stage, we assessed the remaining 388 full‐text articles for eligibility resulting in the inclusion of 106 articles. Cross‐referencing of these 106 articles yielded the identification of one additional article leading to the inclusion of a total of 107 articles.
Of these 107 articles, 51 reported on the added value of predictors to the RCRI, 51 compared the predictive performance of the RCRI to biomarkers and 52 compared the RCRI to other prediction models. We found 30 (28%) articles reporting on both the added value of a certain predictor to the RCRI and comparison of the predictive performance of this biomarker. In 11 (10%) articles, the added value of a particular biomarker to the RCRI and the comparison of another prediction model was reported. Finally, the comparison of both a biomarker and a prediction model to the RCRI was presented in 13 (12%) articles. For further details of our search results, see Figure 1.
1.

Study flow diagram
The search of databases of ongoing trials (clinicaltrials.gov and WHO ICTRP; searched 27 July 2020) revealed 22 records (Figure 1). No duplicates were identified. Four ongoing trials aim to investigate the added value of biomarkers to the RCRI (NCT03436238: hsTnT, NTproBNP, copeptin, MR‐proADM and CT‐proET1; NCT02860754: six‐minute walking test and self‐reported METS, NCT03016936: METs estimated by questionnaire and NT‐proBNP; NCT02146560: BNP, HbA1c and others) and two other ongoing trials will compare the predictive ability of the RCRI alone to biomarkers (NCT01280253: NT‐proNP, lactate, pro‐calcitonin, adrenomedullin, copeptin, cystatin c; CTRI/2019/02/017668: hand grip strength, Modified Frailty Index). More detailed information is provided in Characteristics of ongoing studies.
Risk of bias and concern regarding applicability
We observed no differences in terms of assessment of risk of bias and concern regarding applicability among articles studying the added value of predictors or comparing the predictive performance of predictors or prediction models to the RCRI. Therefore, we evaluated the risk of bias and concern regarding applicability per domain (i.e. selection of participants, predictors, outcome and analysis) as described by the PROBAST tool (Moons 2019; Wolff 2019) for all included articles at once.
Overall, we rated risk of bias as high in at least one domain in 96 (90%) of all included articles. There was an overall 'high' concern regarding applicability in 84 (78%) articles. More detailed information is presented in Figure 2 and Figure 3.
2.
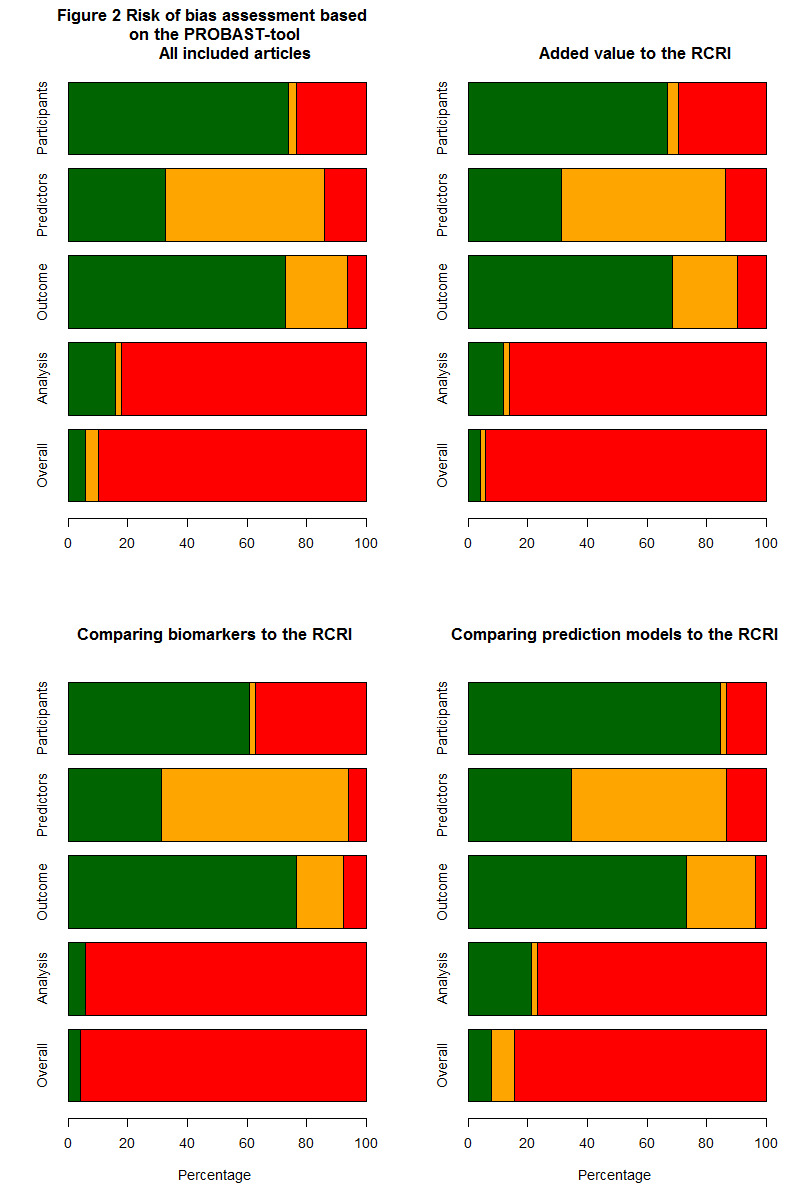
Green refers to 'low' risk of bias; orange is 'unclear' risk of bias and red represents 'high' risk of bias.
3.
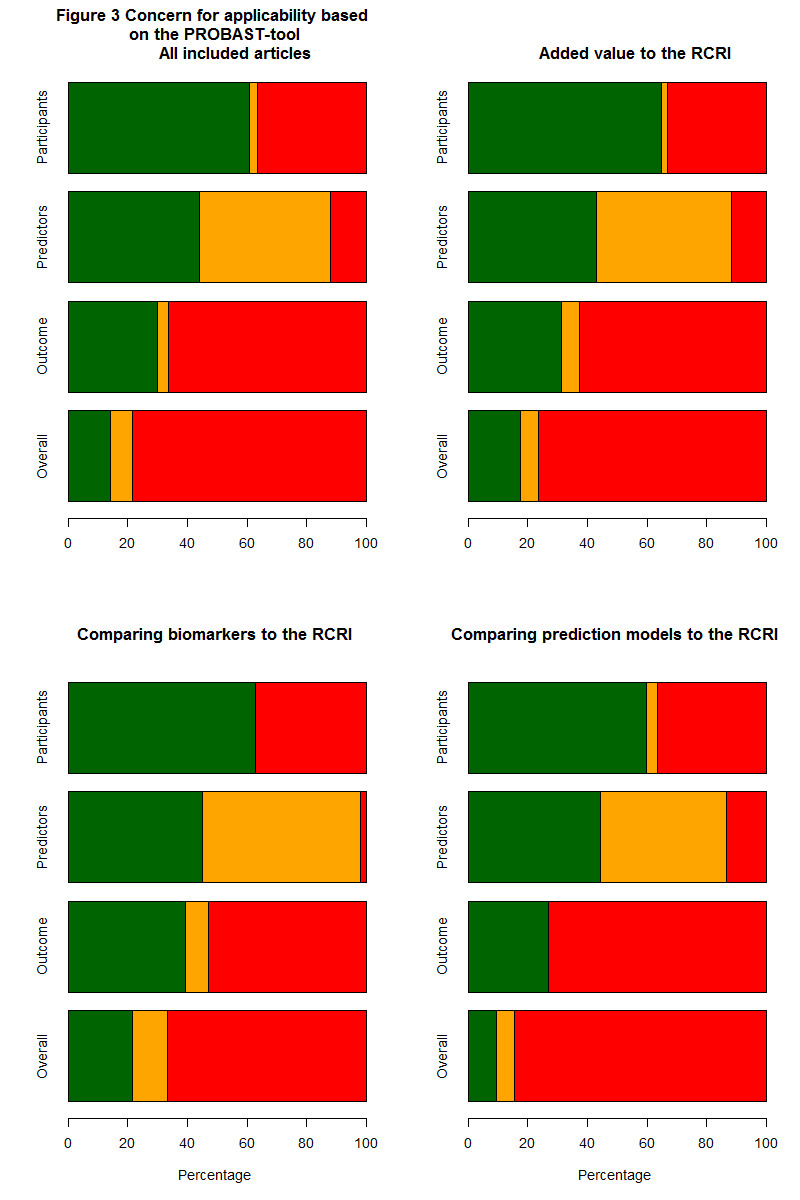
Green refers to 'low' risk of bias; orange is 'unclear' risk of bias and red represents 'high' risk of bias.
PROBAST domain 1: Participants
In 79 (74%) included articles, we judged the risk of participant selection bias as low. We rated risk of bias as high for 25 articles (23%) due to inappropriate exclusion of participants (e.g. exclusion of patients with preoperative severe cardiac comorbidities, who underwent coronary revascularisation or patients who were unsuitable for exercise testing) or inappropriate inclusion of participants (e.g. only inclusion of patients who were referred to a cardiologist, had a transthoracic echocardiography or without any known cardiovascular disease). We rated the remaining three articles (3%) as having unclear risk of bias as no eligibility criteria for inclusion in the study were described.
We judged concern regarding applicability for the domain 'Selection of participants' as low in 65 (61%) of all included articles. We rated 39 (36%) articles as having high concern regarding applicability because of the inclusion of patients undergoing a single procedure or with one particular comorbidity (e.g. atrium fibrillation), inclusion of very high‐risk patients (i.e. high incidence of comorbidities) and inclusion of patients with a either broad or small age range. The three (3%) articles that we rated as having unclear risk of bias were also judged as having unclear concern regarding applicability for the same reasons.
PROBAST domain 2: Predictors
For the domain 'Predictors', we rated the majority of articles (57, 53%) as having unclear risk of bias as no information was provided on how the individual RCRI predictors were defined or measured. This was most often the case for 'history of congestive heart failure' (76%), 'history of ischaemic heart disease' (73%) and 'history of cerebrovascular disease' (64%). We judged a high risk of bias for this domain in 15 (14%) articles because of different predictor definitions compared to the definitions of the development study. Differences were most often observed for the definition of 'history of ischaemic heart disease' (19%) and 'history of congestive heart failure' (15%).
We rated concern regarding applicability as low in 47 (44%), unclear in 47 (44%) and high in 13 (12%) articles. Judgement was based on similar reasons as mentioned above for risk of bias.
PROBAST domain 3: Outcome
We rated seven (6%) of the included articles as having high risk of bias for the domain 'Outcome', mostly due to inappropriate assessment of the outcome. We judged 22 (21%) articles to have unclear risk of bias as in many studies there was no clear outcome definition, or no information on how the outcome was assessed or whether outcome assessors were blinded to predictor information. We rated the remaining 78 (72%) articles as low risk of bias for this domain.
The RCRI has been developed to predict postoperative in‐hospital MACE. However, many articles used the RCRI for predicting other outcomes, including all‐cause mortality and noncardiac complications, and therefore we judged these articles (71, 66%) as having high concern regarding applicability for this domain. We rated concern regarding applicability as unclear in four (4%) articles due to unclear outcome definitions.
PROBAST domain 4: Analysis
We rated risk of bias for the domain 'Analysis' as high in the majority of the included articles (88, 82%), mainly due to low numbers of outcome events. The PROBAST‐tool recommends at least 100 outcome events as otherwise biased estimates of model performance become more likely (Moons 2019; Wolff 2019). Other reasons for scoring risk of bias as high were dichotomisation of predictors, and not reporting appropriate performance measures (i.e. discrimination and/or calibration) at all or without uncertainty measures (i.e. confidence intervals or standard errors). In addition, none of the included articles used multiple imputation for handling of missing data. Only 30 (28%) articles reported that they did complete case analysis and the remaining articles did not mention handling of missing data. We rated the remaining articles (17, 16%) as low risk of bias.
Included studies
Some articles reported on the validation of the RCRI for different outcomes (i.e. multiple validations are described in one article). Accordingly, the number of validations is higher than the number of included articles. Therefore, study characteristics and (composite) outcomes are presented uniquely per reported outcome for each objective separately. Risk of bias and concern regarding applicability, and reporting rates of predictive performance measures, are reported per article. In addition, lists of biomarkers and prediction models that have been added and/or compared to the RCRI are provided. Biomarkers or prediction models, i.e. predictors that were reported in at least three separate included studies, are described in more detail. The summary of findings tables presents descriptive results (i.e. without pooled estimates) for studies reporting on biomarkers/prediction models that were added or compared to the RCRI in at least three different studies and were validated using a similar outcome in at least two different studies (Table 1; Table 2; Table 3).
Objective 1: the added predictive value of biomarkers to the RCRI
Study design and study population
In the 51 included articles reporting on the added value of biomarkers to the RCRI, 62 validations of the RCRI were observed. Most validations were done in cohort study data (n = 57, 92%) and 44 (71%) had their data collected prospectively. Study participants most often underwent noncardiac surgery (n = 36, 58%) followed by vascular surgery (n = 19, 30%) (Table 6). In one study, the surgical specialty was not specified (Makary 2010). Participants originated most frequently from Europe (n = 22, 36%) and Asia or North America (n = 14, 23% and n = 12, 19%, respectively). The number of included participants per validation ranged from 77 to 108,593 (median (interquartile range, IQR); 442 (223 to 1389)) and the number of events ranged from 11 to 1269 (38 (21 to 84)). In one study, the number of events was not reported. The most frequently used prediction horizons were either during hospital admission (n = 12, 19%), 30 days (n = 29, 47%) or within the first seven days after surgery (n = 6, 10%). However, there was a broad width in prediction horizons, ranging from one day to four years after surgery. In terms of predicted outcomes, MACE was most frequently the outcome of interest (n = 31, 50%) followed by all‐cause mortality (n = 6, 10%) or a combination of both (n = 8, 13%). Although the RCRI was developed to predict MACE, 14 (23%) validations used all‐cause mortality as an outcome and four validations used other complications (e.g. discharge to a nursing facility; 7%). The number of published articles on the added value of predictors to the RCRI increased over time with a peak in the most recent period, i.e. 2018 to June 2020 (Figure 4).
3. Study characteristics of included studies.
| All validations | Added value of biomarkers | Comparison of biomarkers | Comparison of prediction models | |
| N | 172 | 62 | 89 | 79 |
| Geographical area (%) | ||||
| Europe | 51 (29.8) | 22 (35.5) | 24 (27.3) | 28 (35.9) |
| North America | 63 (36.8) | 12 (19.4) | 42 (47.7) | 27 (34.6) |
| Asia | 20 (11.7) | 14 (22.6) | 10 (11.4) | 3 (3.8) |
| Africa | 2 (1.2) | 1 (1.6) | 1 (1.1) | 1 (1.3) |
| Australia | 1 (0.6) | 0 (0.0) | 1 (1.1) | 0 (0.0) |
| South America | 5 (2.9) | 1 (1.6) | 1 (1.1) | 4 (5.1) |
| Combination | 29 (17.0) | 12 (19.4) | 9 (10.2) | 15 (19.2) |
| Data collection (%) | ||||
| Prospective | 124 (72.5) | 44 (71.0) | 66 (74.2) | 25 (32.1) |
| Retrospective | 41 (24.0) | 15 (24.2) | 18 (20.2) | 54 (68.4) |
| Unclear | 6 (3.5) | 3 (4.8) | 5 (5.6) | 0 (0.0) |
| Study design (%) | ||||
| Cohort | 130 (75.6) | 57 (91.9) | 57 (64.0) | 68 (86.1) |
| Existing registry | 35 (20.3) | 2 (3.2) | 26 (29.2) | 9 (11.4) |
| Case‐control | 1 (0.6) | 0 (0.0) | 0 (0.0) | 1 (1.3) |
| Existing RCT | 1 (0.6) | 1 (1.6) | 1 (1.1) | 1 (1.3) |
| Individual patient data meta‐analysis | 5 (2.9) | 2 (3.2) | 5 (5.6) | 0 (0.0) |
| Surgical specialty (%) | ||||
| Noncardiac | 77 (44.8) | 36 (58.1) | 30 (33.7) | 37 (46.8) |
| Vascular | 47 (27.2) | 19 (30.2) | 23 (25.6) | 25 (31.6) |
| ENT and dental | 2 (1.2) | 1 (1.6) | 1 (1.1) | 1 (1.3) |
| General | 5 (2.9) | 0 (0.0) | 2 (2.2) | 4 (5.1) |
| Neurological | 25 (14.5) | 0 (0.0) | 24 (26.7) | 1 (1.3) |
| Orthopaedic | 8 (4.6) | 3 (4.8) | 5 (5.6) | 5 (6.3) |
| Other | 5 (2.9) | 1 (1.6) | 2 (2.2) | 3 (3.8) |
| Not specified | 3 (1.7) | 2 (3.2) | 2 (2.2) | 3 (3.8) |
| Prediction horizon (%) | ||||
| Intraoperative events | 1 (0.6) | 0 (0.0) | 1 (1.1) | 1 (1.3) |
| 1 to 7 days | 7 (4.1) | 6 (9.7) | 7 (7.9) | 1 (1.3) |
| In‐hospital events | 25 (14.5) | 12 (19.4) | 13 (14.6) | 14 (17.7) |
| In‐hospital or within 30 days | 10 (5.8) | 8 (12.9) | 2 (2.2) | 2 (2.5) |
| 30‐day events | 109 (63.4) | 29 (46.8) | 59 (66.3) | 52 (65.8) |
| > 30 days (long‐term) | 12 (7.0) | 6 (9.7) | 5 (5.6) | 4 (5.1) |
| Not reported | 8 (4.6) | 1 (1.6) | 2 (2.2) | 5 (6.3) |
| Outcome (%) | ||||
| MACE | 70 (40.7) | 31 (50.0) | 35 (39.3) | 32 (40.5) |
| MICA | 8 (4.7) | 2 (3.2) | 0 (0.0) | 7 (8.9) |
| Myocardial infarction | 5 (2.9) | 3 (4.8) | 3 (3.4) | 0 (0.0) |
| Cardiovascular mortality | 6 (3.5) | 3 (4.8) | 1 (1.1) | 2 (2.5) |
| Troponin elevation/myocardial injury | 6 (3.5) | 5 (8.1) | 4 (4.5) | 3 (3.8) |
| All‐cause mortality | 22 (12.8) | 6 (9.7) | 10 (11.2) | 13 (16.5) |
| All‐cause mortality and MACE | 15 (8.7) | 8 (12.9) | 7 (7.9) | 6 (7.6) |
| Other | 40 (23.3) | 4 (6.5) | 29 (32.6) | 16 (20.3) |
| Number of participants (median (IQR)) | 922 (244 to 9267) | 442 (223 to 1389) | 594 (227 to 52066) | 941 (251 to 2284) |
| Number of events (median (IQR)) | 49 (23 to 112) | 38 (21 to 84) | 39 (19 to 77) | 64 (21 to 132) |
| Incidence (median (IQR)) | 0.06 (0.02 to 0.13) | 0.09 (0.05 to 0.14) | 0.06 (0.02 to 0.13) | 0.06 (0.03 to 0.14) |
RCT: randomised controlled trial; noncardiac: patients of multiple (noncardiac) surgical specialties were included in the analysis; ENT: ear, nose and throat; MACE: major adverse cardiac events; MICA: myocardial infarction and cardiac arrest; IQR: interquartile range
4.
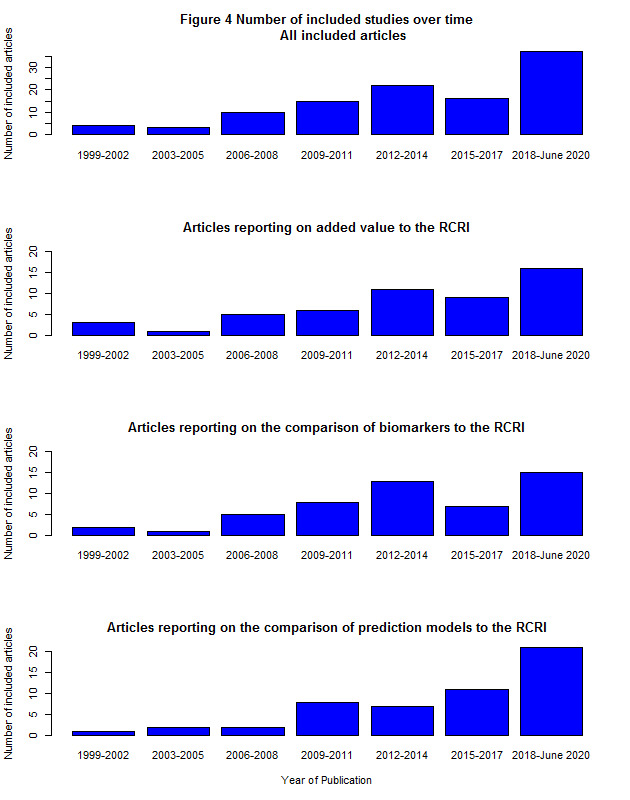
As the search was performed on June 25th, results are shown for the period between January 2018 and June 2020
Outcomes and composition of MACE
The majority of all included articles used MACE including MICA (composite outcome including myocardial infarction and cardiac arrest; n = 78, 45%) as an outcome or combined MACE with all‐cause mortality (n = 15, 9%). However, MACE composition varied noticeably with 80 different definitions. Table 7 shows an overview of the outcome composites of MACE (i.e. MACE and combination of MACE and all‐cause mortality). For the studies reporting on the added value of biomarkers to the RCRI, all but eight (81%) included myocardial infarction as one of the composites of MACE. Most definitions for MACE (22/33; 67%) did not specify if it concerned either fatal or nonfatal myocardial infarction. Besides myocardial infarction, there was no other outcome used as a composite in more than half of the definitions used. Other frequently used included outcomes as part of MACE were heart failure (29%), cardiac death (35%), cardiovascular death (22%), cardiac arrest (15%), myocardial injury (24%) and pulmonary oedema (20%) (Table 7).
4. Composites used to define major adverse cardiac events (MACE).
| Overall | Added value of biomarkers | Comparison of biomarkers | Comparison of prediction models | |
| n | 93 | 41 | 42 | 45 |
| Cardiac death | 28 (30.1) | 14 (34.5) | 16 (38.1) | 11 (24.4) |
| Cardiovascular death | 16 (17.2) | 9 (22.0) | 8 (19.0) | 6 (13.3) |
| All cause mortality | 17 (18.3) | 9 (22.0) | 8 (19.0) | 6 (13.3) |
| Nonfatal myocardial infarction | 22 (23.7) | 11 (26.8) | 12 (28.6) | 8 (17.8) |
| Fatal myocardial infarction | 1 (1.1) | 0 (0.0) | 1 (2.4) | 0 (0.0) |
| Myocardial infarction (not specified) | 44 (47.3) | 22 (53.7) | 23 (54.8) | 18 (40.0) |
| Myocardial infarction (any) | 66 (70.1) | 33 (80.5) | 35 (83.3) | 26 (57.8) |
| Heart failure | 33 (35.5) | 12 (29.3) | 17 (40.5) | 19 (42.2) |
| Cardiac arrest | 27 (29.0) | 6 (14.6) | 8 (19.0) | 18 (40.0) |
| Complete heart block | 7 (7.5) | 2 (4.9) | 4 (9.5) | 3 (6.7) |
| Pulmonary oedema | 18 (19.4) | 8 (19.5) | 9 (21.4) | 8 (17.8) |
| Ventricular arrhythmia | 12 (12.9) | 4 (9.8) | 8 (19.0) | 7 (15.6) |
| Atrial arrhythmia | 4 (4.3) | 1 (2.4) | 3 (7.1) | 2 (4.4) |
| Arrhythmia, not specified | 17 (18.3) | 7 (17.1) | 8 (19.0) | 8 (17.8) |
| Revascularisation | 6 (6.5) | 4 (9.8) | 3 (7.1) | 2 (4.4) |
| Acute coronary syndrome | 6 (6.5) | 4 (9.8) | 4 (9.5) | 2 (4.4) |
| Unstable angina | 8 (8.6) | 2 (4.8) | 6 (14.3) | 4 (8.9) |
| Myocardial injury | 15 (16.1) | 10 (24.4) | 10 (23.8) | 4 (8.9) |
| Stroke | 14 (15.1) | 4 (9.5) | 5 (11.9) | 9 (20.0) |
| Hypertensive crisis | 2 (2.2) | 0 (0.0) | 2 (4.8) | 0 (0.0) |
| ST‐T changes on ECG | 1 (1.1) | 0 (0.0) | 0 (0.0) | 1 (2.2) |
| Intraoperative hemodynamic adversity | 1 (1.1) | 0 (0.0) | 1 (2.4) | 1 (2.2) |
| Systemic embolism | 1 (1.1) | 1 (2.4) | 1 (2.4) | 0 (0.0) |
Risk of bias and concern regarding applicability
We rated overall risk of bias as high in at least one domain in 48 (94%) articles reporting on the added value of predictors to the RCRI. More detailed information is described under the subheading 'Risk of bias and concern regarding applicability' and presented in Figure 2 and Figure 3. We rated most articles as having unclear risk of bias for predictors (n = 28, 55%) due to no information on the definitions of the individual RCRI items or no description on how the 'new' biomarkers were measured or added to the RCRI. For the domains 'outcome' and 'analyses', we rated n = 5 (10%) and n = 44 (86%) articles as having high risk of bias, respectively. We rated concern regarding applicability as high in at least one of the domains in 39 (76%) of the included articles. This was mainly because of high concern regarding applicability in the domain 'outcome' (n = 32, 63%) due to inappropriate outcomes used to be predicted (Figure 2; Figure 3).
We observed no differences in the reasons for judgement of high or unclear risk of bias and concern regarding applicability among the different objectives. More detailed information on this topic is described below under the subheading 'Risk of bias and concern regarding applicability'.
Predictive performance measures reported
All included articles but one (n = 106, 99%) reported at least one performance measure (Table 8). For studies on the added value of biomarkers to the RCRI, discrimination was reported in 48 (94%) articles, for which the majority of articles presented a c‐statistic (n = 40, 78%). Compared to all included studies, c‐statistics were reported less often for studies on the added value of biomarkers to the RCRI (92% and 79%, respectively). Calibration was presented in 39 (36%) articles by means of an observed/expected ratio (n = 22, 21%), calibration plot (n = 14, 13%) or a Hosmer Lemeshow test (n = 7, 7%). Again, calibration measures were less frequently reported in articles evaluating the added value of predictors to the RCRI compared to all included articles (20% versus 36%, respectively). In total, 36 articles (34%) reported both discrimination and calibration measures, of which nine (18%) investigated the added value of predictors to the RCRI. Reclassification measures, presented as integrated discrimination improvement (IDI) or net reclassification index (NRI), were more often reported in articles investigating the added value of biomarkers to the RCRI compared to all included articles, as expected (35% versus 22%, respectively).
5. Reporting of performance measures in included studies.
| All included studies | Added value to the RCRI | Comparison of biomarkers | Comparison of prediction models | |
| N | 107 | 51 | 51 | 52 |
| Performance category (%) | ||||
| Discrimination | 102 (95.3) | 48 (94.1) | 49 (96.1) | 50 (96.2) |
| Calibration | 39 (36.4) | 10 (19.6) | 15 (29.4) | 22 (42.3) |
| Reclassification | 23 (21.5) | 18 (35.3) | 2 (4.0) | 5 (9.6) |
| C‐statistic (%) | 98 (91.6) | 40 (78.4) | 45 (88.2) | 48 (92.3) |
| O/E (%) | 22 (20.6) | 6 (11.8) | 12 (23.5) | 8 (15.4) |
| Calibration plot (%) | 14 (13.1) | 4 (7.8) | 1 (2.0) | 10 (19.2) |
| Hosmer Lemeshow test (%) | 7 (6.5) | 1 (2.0) | 3 (5.9) | 7 (13.5) |
| IDI (%) | 7 (6.5) | 7 (13.7) | 1 (2.0) | 0 (0.0) |
| NRI (%) | 22 (20.6) | 17 (33.3) | 2 (3.9) | 5 (9.6) |
| Other reported measures (%) | ||||
| Sensitivity | 41 (38.3) | 6 (11.8) | 27 (52.9) | 14 (26.9) |
| Specificity | 40 (37.4) | 6 (11.8) | 27 (52.9) | 13 (25.0) |
| Negative predictive value | 19 (17.8) | 3 (5.9) | 12 (23.5) | 5 (9.6) |
| Positive predictive value | 18 (16.8) | 3 (5.9) | 11 (21.6) | 5 (9.6) |
| Accuracy | 3 (2.8) | 0 (0.0) | 2 (3.9) | 1 (1.9) |
O/E: observed/expected ratio; IDI: integrated discrimination improvement; NRI: net reclassification improvement.
Discrimination includes the following performance measures: c‐statistics/AUC, sensitivity, specificity, negative predictive value, positive predictive value, positive predictive value and accuracy.
Calibration includes O:E ratio, calibration plot and Hosmer Lemeshow test.
Reclassification includes IDI and NRI.
Added biomarkers
In Table 9, an overview of the biomarkers added to the RCRI is provided sorted by the number of studies reporting on a particular biomarker. We identified 69 different added predictors of which 20 (29%) were derived from blood, 23 (33%) from imaging and 26 (38%) from other sources including patient characteristics, such as smoking or age. In most instances, one predictor was added (n = 47, 68%) to the RCRI to improve risk prediction followed by two (n = 16, 23%) and three predictors (n = 6, 9 %) in the same model.
6. Biomarkers/predictors added to the RCRI.
| Number of studies | Derivation | |
| NT‐proBNP | 13 | Blood |
| Troponin | 7 | Blood |
| NT‐proBNP + troponin | 5 | Blood |
| BNP | 4 | Blood |
| Copeptin | 3 | Blood |
| Coronary artery calcium score (CACS) | 2 | Imaging |
| CRP | 2 | Blood |
| fQRS of an ECG | 2 | Imaging |
| NT‐proBNP + CRP | 2 | Blood |
| V‐POSSUM | 2 | Other |
| V‐POSSUM + NTproBNP | 2 | Blood |
| V‐POSSUM + troponin | 2 | Blood |
| 6 minute walking test | 1 | Other |
| Abdominal aortic aneurysm size | 1 | Other |
| Age | 1 | Other |
| Age + abdominal aortic aneurysm size | 1 | Other |
| Age + sex + copeptin | 1 | Other |
| Age > 70 years | 1 | Other |
| Anaerobic threshold | 1 | Other |
| Anaemia | 1 | Other |
| Angina pectoris | 1 | Other |
| ASA | 1 | Other |
| ASA + SORT + NSQIP‐MICA | 1 | Other |
| Atrial fibrillation | 1 | Other |
| Copeptin + NT‐proBNP | 1 | Blood |
| Coronary CT angiography | 1 | Imaging |
| Duke Activity Status Index | 1 | Other |
| ECG abnormalities | 1 | Imaging |
| Echocardiography | 1 | Imaging |
| Echocardiography + beta blockers | 1 | Imaging |
| EE ratio of echocardiography | 1 | Imaging |
| Frailty | 1 | Other |
| Jeopardy score | 1 | Imaging |
| Left bundle branch block on ECG | 1 | Imaging |
| Left ventricular ejection fraction | 1 | Imaging |
| Male sex | 1 | Other |
| Metabolic equivalent (METS) | 1 | Other |
| METS + positive stress test with no false negatives | 1 | Other |
| METS + stress test | 1 | Imaging |
| Multi vessel disease | 1 | Imaging |
| Multi vessel disease + CACS | 1 | Imaging |
| Peak oxygen | 1 | Other |
| Polygenic risk score for coronary artery disease | 1 | Other |
| Presepsin | 1 | Blood |
| Presepsin + NT‐proBNP | 1 | Blood |
| Presepsin + troponin | 1 | Blood |
| Presepsin + troponin + NT‐proBNP | 1 | Blood |
| Reactive hyperaemia peripheral arterial tonometry | 1 | Other |
| Regulatory T cells | 1 | Blood |
| Regulatory T cells + troponin + NT‐proBNP | 1 | Blood |
| Right bundle branch block on ECG | 1 | Imaging |
| Segment involvement + Jeopardy score | 1 | Imaging |
| Segment involvement score | 1 | Imaging |
| Smoking | 1 | Other |
| ST2 + troponin | 1 | Blood |
| ST2 cardiac biomarker | 1 | Blood |
| Stenosis of CTA + CACS | 1 | Imaging |
| Stenosis on CTA | 1 | Imaging |
| Stress echocardiography | 1 | Imaging |
| Survivin | 1 | Blood |
| Thallium scan | 1 | Imaging |
| Total joint arthroplasty risk score | 1 | Other |
| Type of surgery | 1 | Other |
| Type of surgery + age | 1 | Other |
| Type of surgery + age + hypertension | 1 | Other |
| Valve sclerosis | 1 | Imaging |
| Valve stenosis | 1 | Imaging |
| V‐POSSUM + troponin + NT‐proBNP | 1 | Blood |
| Wall abnormalities on an echocardiography | 1 | Imaging |
ASA: American Society of Anesthesiologists; BNP: brain natriuretic peptide; CRP: C‐reactive protein; CT: computed tomography; E/e' ratio: ratio between early mitral inflow velocity and mitral annular early diastolic velocity; fQRS of an ECG: fragmented QRS of an electrocardiogram (ECG); NSQIP‐MICA: National Surgical Quality Improvement Program score for the prediction of myocardial infarction and cardiac arrest; NT‐prBNP: N‐terminal prohormone of brain natriuretic peptide; SORT: Surgical Outcome Risk Tool; V‐POSSUM: Vascular Physiologic and Operative Severity Score for the enUmeration of Mortality and Morbidity
For the biomarkers that have been added to the RCRI in at least three different studies, study characteristics and findings are described in further detail below. These biomarkers are brain natriuretic peptide (BNP), copeptin, N‐terminal pro‐B type natriuretic peptide (NT‐proBNP), troponin and the combination of NT‐proBNP and troponin.
N‐terminal pro‐B type natriuretic peptide (NT‐proBNP)
N‐terminal pro‐B type natriuretic peptide (NT‐proBNP) is generated by cardiomyocytes in the context of numerous triggers, most notably myocardial stretch. NT‐proBNP has been increasingly used as a marker to establish the presence and severity of heart failure in both chronic ambulatory or acute decompensated heart failure settings (Yancy 2013). We included 12 articles reporting on the added predictive value of NT‐proBNP to the RCRI in 17 different analyses. Three articles showed added value for multiple outcomes (Choi 2010; Duceppe 2020; Wijeysundera 2018). Patients underwent either mixed noncardiac (n = 7) or vascular surgery (n = 5). NT‐proBNP was added to the RCRI on a continuous scale in six articles, on a dichotomous scale using a predefined threshold in four articles and on a categorical scale in two articles. Figure 5 represents the added predictive value of NT‐proBNP to the RCRI by means of the c‐statistics to predict MACE, myocardial infarction, all‐cause mortality, cardiovascular mortality or pulmonary oedema. The majority of predictions were performed for the in‐hospital and/or 30‐day events (n = 14). The number of reported events was relatively low in the majority of the studies, i.e. median 43, range 13 to 1269. Addition of NT‐proBNP to the RCRI to predict MACE was reported in seven studies including 13,687 patients of whom 1710 suffered MACE (Biccard 2012; Binh 2019; Borges 2013; Choi 2010; Duceppe 2020; Golubovic 2018; Handke 2020; Yang 2012). The delta c‐statistic was median 0.08 (range 0.04 to 0.22). Calibration was presented in one study and showed good calibration (Duceppe 2020). Reclassification was better for the model including NT‐proBNP (n = 2 studies, 10,524 included patients with 1560 MACE, median NRI (range) 0.74 (0.26 to 1.22)) (Duceppe 2020; Golubovic 2018). For the composite outcome all‐cause mortality and MACE, the delta c‐statistic was 0.06 (range 0.06 to 0.07) and reported in three studies that included 12,214 patients of whom 548 suffered either all‐cause mortality or MACE (Duceppe 2020; Scrutinio 2014; Wijeysundera 2018). The Hosmer Lemeshow test was reported in one study showing some overall miscalibration (P = 0.03) (Scrutinio 2014). The median NRI was 0.19 (0.13 to 25) (Scrutinio 2014; Wijeysundera 2018). For the prediction of myocardial infarction (MI), two studies (n = 2626, 131 MIs) showed improved discrimination (delta c‐statistic; 0.09, range 0.06 to 0.11) (Choi 2010; Kopec 2017). No calibration was reported in these studies. In the study Kopec 2017, the total NRI was 0.46.
5.
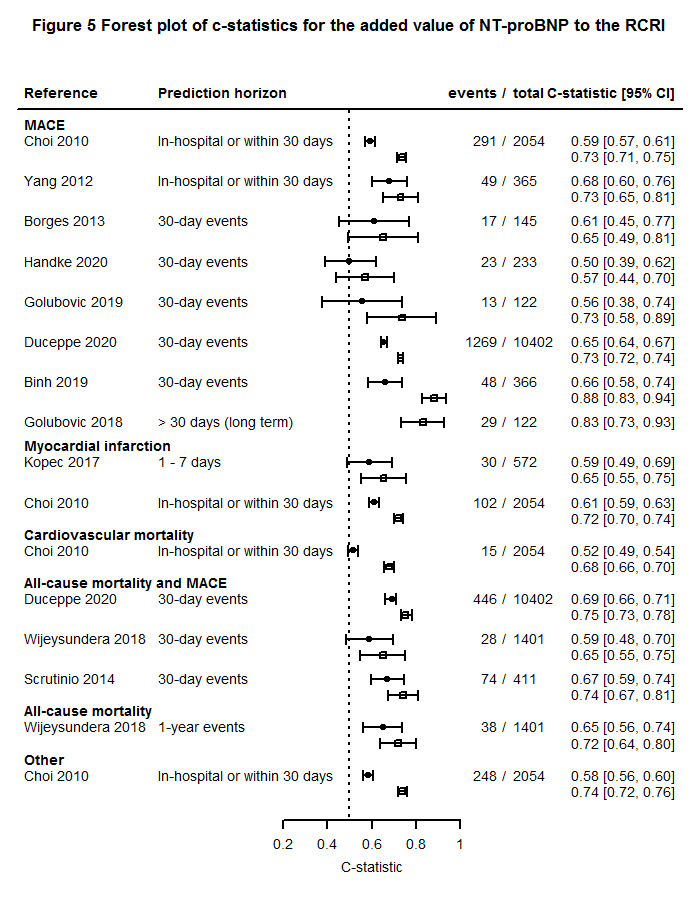
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents RCRI + NT‐proBNP.
Brain natriuretic peptide (BNP)
Similar to NT‐proBNP, BNP is released by cardiomyocytes in case of myocardial stretch. BNP is used in clinical practice as a marker to establish the presence and severity of both chronic ambulatory or acute decompensated heart failure (Yancy 2013). BNP was added to the RCRI in six analyses over five articles (Biccard 2011; Biccard 2012; Cuthbertson 2007; Katsanos 2015; Rodseth 2011), with one article describing two analyses using different outcomes and prediction horizons (i.e. in‐hospital MACE and one‐year all‐cause mortality) (Katsanos 2015). Included articles reported most frequently on patients undergoing vascular surgery (n = 3). The outcome of interest in these articles was MACE (n = 3), all‐cause mortality (n = 1), a combination of both (n = 1) or troponin elevation (n = 1). Prediction horizons ranged from in‐hospital to one‐year events. As none of the articles reported the c‐statistics of the extended model (i.e. BNP added to the RCRI), no forest plot was provided. Two studies reported reclassification in terms of the NRI after addition of BNP to the RCRI to predict MACE (n = 1724 patients, unknown number of MACE) (Katsanos 2015; Rodseth 2011). The median NRI was 0.72 with a range of 0.47 to 0.96. None of the included studies reported on calibration.
Troponin
Troponin is a protein that is involved in the contraction of cardiac muscle and is released by injured cardiomyocytes. Release of troponin may be due to myocardial cell death caused by ischaemia but also by, for example, normal turnover of myocardial cells, apoptosis or increased permeability of the cell wall (Mair 2018; Thygesen 2018). We included five articles reporting on the added predictive value of troponin to the RCRI in six analyses, of which one article analysed two populations separately (Gualandro 2018). However, no c‐statistics were reported for this study. Included populations concerned patients undergoing vascular (n = 4) or mixed noncardiac surgery (n = 3). Troponin was added on a continuous scale, dichotomous scale or not reported in two and four and one studies, respectively. Included studies aimed to predict 30‐day MACE (n = 4), long‐term MACE (n = 1), 30‐day MACE or all‐cause mortality (n = 1) or myocardial infarction within three days of surgery (n = 1). The extracted confidence intervals were wide, the studied patient populations (i.e. vascular and noncardiac) heterogeneous, and the numbers of included participants and events for the studies investigating the added value of troponin were low, i.e. median 238 (range 122 to 797) and median 30 (range 13 to 58), respectively. Three studies (n = 810, 77 MACE) investigated the incremental discriminative value of troponin to the RCRI model to predict MACE (delta c‐statistic 0.14 (range 0.06 to 0.33); Figure 6) (Gillmann 2014; Golubovic 2018; Handke 2020). Reclassification was reported in two studies (n = 577, 70 MACE) resulting in a delta NRI of 0.16 (range 0.09 to 0.22) (Gillmann 2014; Golubovic 2018). None of the studies investigating the incremental value of troponin to the RCRI reported on calibration.
6.
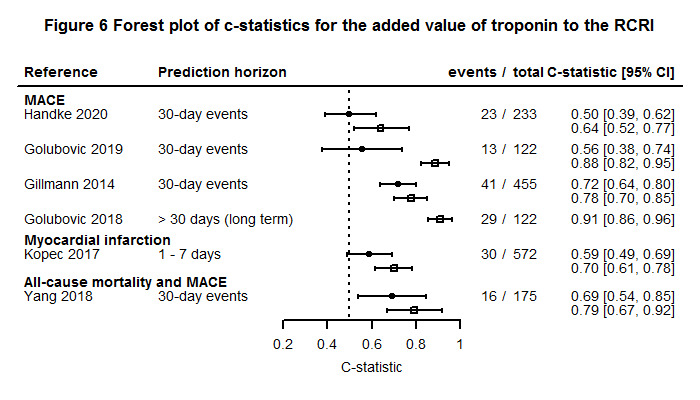
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents RCRI + troponin. As Golubovic 2018 solely reported on the c‐statistics for the additive model, no c‐statistic for RCRI alone is provided for this study.
Copeptin
Copeptin is a novel marker of vasopressin activity, an antidiuretic hypothalamo‐pituitary hormone, mainly regulated by changes in plasma osmolality, blood volume and blood pressure (Mauermann 2016). Copeptin was added to the RCRI in three articles of which two studies reported on either the prediction of 30‐day or long‐term MACE in the vascular surgical population (Jarai 2011; Schrimpf 2015). The other study investigated the added value of copeptin to the RCRI to predict troponin elevation within two days after surgery in noncardiac surgical patients (Mauermann 2016). The NRI in this study was 0.78. The c‐statistic for the RCRI alone and the extended model to predict MACE was reported in one article, i.e. 0.714 and 0.752, respectively (n = 477, 41 MACE) (Schrimpf 2015). The NRI was reported in one study (n = 198, 40 MACE) to evaluate reclassification of the incremental value of copeptin to the RCRI to predict MACE at 24 months after surgery (NRI; 0.33) (Jarai 2011). None of the selected studies reported on calibration. There was not sufficient information to summarise these studies in a forest plot.
NT‐proBNP + troponin
We included four studies reporting on the added predictive value of the combination of NT‐proBNP and troponin to the RCRI (Golubovic 2018; Handke 2020; Kopec 2017; Scholz 2019). Patients underwent vascular (n = 2) or mixed noncardiac surgery (n = 3). The scale used to add troponin and NT‐proBNP to the RCRI was either continuous (n = 3) or dichotomous (n = 2). Reported outcomes were 30‐day MACE (n = 3), long‐term MACE (n = 1) or myocardial infarction within three days of surgery (n = 1). The number of included patients and events was low (i.e. median 227; range 122 to 572 and median 30; range 13 to 84, respectively) resulting in wide confidence intervals. In addition, the composition of MACE varied among the included studies and the patient populations (i.e. vascular and noncardiac) were heterogeneous. The addition of troponin and NT‐proBNP to the RCRI to predict 30‐day MACE resulted in a delta c‐statistic of median 0.12 with a range of 0.10 to 0.34 (3 studies, n = 572, 120 MACE; Figure 7) (Golubovic 2018; Handke 2020; Scholz 2019). The added value of troponin and NT‐proBNP to the RCRI to predict myocardial infarction was investigated by Kopec 2017). They reported a delta c‐statistic of 0.13 and an NRI of 0.66 (n = 572, 30 MIs). None of the selected studies reported on calibration.
7.
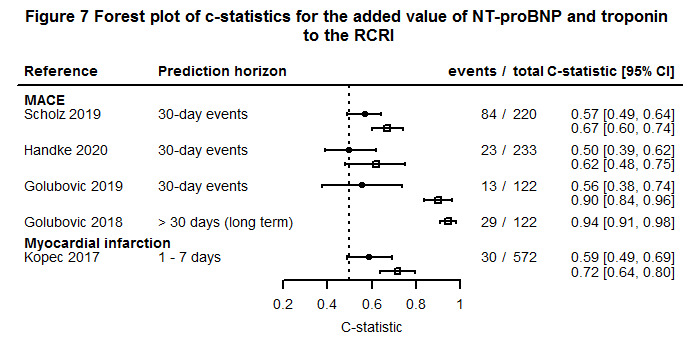
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents NT‐proBNP+troponin+RCRI. As Golubovic 2018 solely reported on the c‐statistics for the additive model, no c‐statistic for RCRI alone is provided for this study.
Objective 2: comparison of the predictive value of single biomarkers to the RCRI
Study design and study population
In total, 51 studies compared the predictive performance of biomarkers to the RCRI and reported 89 validations (Table 6). Most articles reported on the validation of one outcome (n = 37), two outcomes (n = 8) or three or more (n = 4). One article reported on 24 validations of primarily noncardiac complications (Bronheim 2018). Similar to studies reporting on the added value of biomarkers to the RCRI, most studies were cohort studies (n = 57, 64%) and data were collected prospectively in 66 (74%) validations. In 24 (27%) and 42 (48%) validations, patients originated from Europe and North America, respectively. Most included patients who underwent noncardiac surgery (n = 30, 34%) followed by vascular surgery (n = 23, 26%). Bronheim et al validated 24 different outcomes in a neurosurgical population (Bronheim 2018). The surgical specialty was not specified in one study (Makary 2010). The median number of included participants was 594 (227, 52,066). The number of events was not reported in one study, which reported four validations (Rodseth 2011). The most frequently used prediction horizons were during hospital admission (n = 13, 15%), within the first seven days (n = 7, 8%) or 30 days (n = 59, 66%) after surgery. In 39% (n = 35) of the studies, MACE was the outcome to be predicted followed by all‐cause mortality (n = 10, 11%) or a combination of both (n = 7, 8%). Five articles (10%) reporting on 29 validations predicted other outcomes than MACE or all‐cause mortality, of which Bronheim et al reported predictions for 21 different (noncardiac) outcomes (Bronheim 2018). The number of published articles on the comparison of the predictive accuracy of biomarkers to the RCRI increased over time with a peak in 2018 to June 2020 (Figure 4).
Composition of MACE
For the 38 articles that used MACE as the outcome to be predicted, we found 42 validations that compared the prognostic ability of biomarkers to the RCRI alone (Table 7). Within these 42 validations, 21 different MACE definitions were reported using composites ranging from intraoperative haemodynamic adversity to cardiac death. Myocardial infarction was the most frequently used composite of MACE (n = 35, 83%).
Risk of bias and concern regarding applicability
We rated an overall high risk of bias in 49 (96%) articles that compared the predictive performance of biomarkers to the RCRI. Compared to articles included in the other objectives, we rated risk of bias for participants as high more often (n = 19, 37%). Most articles scored unclear risk of bias for predictors (n = 32, 63%) due to no information on the definitions of the individual RCRI items. For the domain 'outcome' and for the domain 'analyses', n = 4(8%) and n = 48(94%) articles scored high for risk of bias, respectively. Concern regarding applicability scored high in at least one of the domains in 34 (67%) of the included articles. This was mainly because of high concern regarding applicability in the domain 'outcome' (n = 27, 53%) due to inappropriate outcomes used to be predicted (Figure 2; Figure 3).
As we did not observe differences in the reasons for judgements of high or unclear risk of bias and concern regarding applicability among the different objectives, more detailed information on this topic is described below under the subheading 'Risk of bias and concern regarding applicability' as part of the first objective.
Predictive performance measures reported
For studies comparing the prognostic ability of biomarkers to the RCRI alone, predictive performance measures on discrimination, calibration and reclassification were reported in 96%, 29% and 4%, respectively (Table 8). The c‐statistic was presented in 88% of the included articles. Half of the articles that compared the predictive ability of biomarkers to the RCRI reported sensitivity and specificity. The negative and positive predictive value were reported in 24% and 22% of the included studies, respectively. Calibration was presented as an observed/expected ratio (24%), calibration plot (2%) or a Hosmer Lemeshow test (6%).
Comparison of biomarkers
An overview of biomarkers for which the predictive performance was compared to the RCRI is presented in Table 10. We identified 60 unique predictors derived from blood (n = 23, 38%), imaging (n = 18, 30%) or other type of characteristics (n = 19, 32%; e.g. age or metabolic equivalent (METS)). For biomarkers for which the predictive performance was compared to the RCRI in at least three different studies, the study characteristics are described in further detail below. These predictors were the American Society of Anesthesiologists classification (ASA), BNP, NT‐proBNP, troponin and C‐reactive protein (CRP).
7. Biomarkers/predictors for which the predictive performance was compared to the RCRI.
| Number of studies | Derivation | |
| ASA | 14 | Other |
| NT‐proBNP | 11 | Blood |
| BNP | 10 | Blood |
| Troponin | 6 | Blood |
| CRP | 3 | Blood |
| Coronary artery calcium score (CACS) | 2 | Imaging |
| Dobutamine stress echocardiography | 2 | Imaging |
| EE ratio on an echocardiography | 2 | Imaging |
| Left ventricular ejection fraction | 2 | Imaging |
| METS | 2 | Other |
| NT‐proBNP + troponin | 2 | Blood |
| Positive stress test | 2 | Imaging |
| Presepsin | 2 | Blood |
| 6 minute walking test | 1 | Other |
| Abnormal echocardiography | 1 | Imaging |
| Age | 1 | Other |
| Age + surgical complexity | 1 | Other |
| Anaerobic threshold | 1 | Other |
| Ankle arm index | 1 | Other |
| Ankle arm index ≤ 0.9 | 1 | Other |
| Ankle arm index ≥ 1.2 | 1 | Other |
| Aortic arch calcification | 1 | Imaging |
| ASA + frailty | 1 | Other |
| CD40 | 1 | Blood |
| Copeptin | 1 | Blood |
| Coronary artery stenosis | 1 | Imaging |
| Coronary CT angiography | 1 | Imaging |
| eGFR | 1 | Blood |
| Estimated blood loss + estimated surgical duration | 1 | Other |
| Estimated blood loss + estimated surgical duration + type of surgery | 1 | Other |
| Functional capacity | 1 | Other |
| H‐FABP | 1 | Blood |
| H‐FABP + survivin | 1 | Blood |
| High age + ischaemic heart disease | 1 | Other |
| Jeopardy score | 1 | Imaging |
| Karnofsky score | 1 | Other |
| KDIGO stage 3 | 1 | Other |
| Left atrial volume index | 1 | Imaging |
| Left ventricular ejection fraction + wall motion abnormalities | 1 | Imaging |
| NT‐proBNP + high creatinine | 1 | Blood |
| NT‐proBNP + high creatinine + ischaemic heart disease | 1 | Blood |
| Peak VO2 | 1 | Other |
| Pedal pulses absent on ankle arm index | 1 | Other |
| Platelet factor V | 1 | Blood |
| Platelet P‐selectin | 1 | Blood |
| Positive stress test without false positives | 1 | Imaging |
| Reactive hyperaemia peripheral arterial tonometry | 1 | Other |
| Regional wall motion abnormalities | 1 | Imaging |
| Regulatory T cells | 1 | Blood |
| sCD40L | 1 | Blood |
| Segment involvement in echocardiography | 1 | Imaging |
| St2 | 1 | Blood |
| Survivin | 1 | Blood |
| Survivin + CRP | 1 | Blood |
| Systolic dysfunction | 1 | Imaging |
| Systolic dysfunction + left hypertrophy | 1 | Imaging |
| Troponin + CK‐MB | 1 | Blood |
| Troponin + CRP | 1 | Blood |
| Troponin + CRP + NT‐proBNP | 1 | Blood |
| Wall motion abnormalities | 1 | Imaging |
ASA: American Society of Anesthesiologists classification; BNP: brain natriuretic peptide; NT‐proBNP: N‐terminal prohormone of brain natriuretic peptide; CRP: C‐reactive protein; E/e' ratio: ratio between early mitral inflow velocity and mitral annular early diastolic velocity; METS: metabolic equivalent; CD40: co‐stimulatory protein found on antigen‐presenting cells and is required for their activation; eGFR: estimated glomerular filtration rate; H‐FABP; heart‐type fatty acid binding protein; KDIGO stage 3: Kidney Disease Improving Global Outcomes stage 3 indicates severity of kidney injury; VO2: rate of oxygen consumption; St2: soluble interleukin 1 receptor like‐1, protein that signals the presence and severity of adverse cardiac remodeling; CT scan: computed tomography scan
American Society of Anesthesiologists (ASA) physical status
The ASA physical status is a tool commonly used to classify a patient's physical fitness before surgery. It describes five classes of physical status ranging from ASA1 (i.e. healthy, non‐smoking patient) to ASA5 (patient is expected to die within 24 hours). ASA6 is sometimes used to describe a brain‐death organ donor. The ASA classification is not a prediction model, but a subjective and rapid assessment tool mostly based on the experience of the anaesthesiologist (Mayhew 2019). The predictive ability of ASA was compared to the RCRI in 53 analyses over 14 included articles. Patients underwent a variety of surgical procedures, i.e. neurosurgery (number of studies = 3), vascular (n = 3), general (n = 1), orthopaedic (n = 1), mixed noncardiac surgery (n = 5) or unspecified (n = 1). The prediction horizon was most commonly within 30 days (n = 9) followed by in‐hospital events (n = 4). MACE was the outcome to be predicted in six articles over seven analyses (Bronheim 2018; James 2014; Parmar 2010; Press 2006; Rohrig 2004; Vetrugno 2014). The delta c‐statistic was 0.02 with a range of ‐0.03 to 0.18 in favour of the RCRI (n = 84,145, 5415 MACE). Rohrig 2004 reported on intraoperative MACE (hypotension, hypertension, bradycardia and tachycardia), which contributed most of the MACE outcomes. The prediction horizon was intraoperative or in‐hospital or 30‐day MACE (Rohrig 2004). Calibration was poor as presented in a calibration plot and Hosmer Lemeshow test (P < 0.001) reported in one study (Rohrig 2004). Other predicted outcomes were myocardial infarction (n = 2) and all‐cause mortality (n = 6 articles, 10 validations). The delta c‐statistic was 0.02 (range ‐0.07 to 0.12) and 0.05 (‐0.05 to 0.24) in favour of ASA, respectively. Other noncardiac events were predicted in six articles over 34 validations (Table 11). Bronheim 2018 compared the ASA to the RCRI to predict 21 different outcomes, and Press 2006 predicted four different noncardiac outcomes. Figure 8 and Table 11 show the reported c‐statistics for the ASA and RCRI. Besides the study by Rohrig 2004, none of the studies reported on calibration or reclassification.
8. C‐statistics for the comparison of the predictive performance of ASA classification to the RCRI using outcomes other than cardiovascular.
| Author | Outcome | Prediction horizon | N events | N total | c‐statistic RCRI | CI (95%) c‐statistic RCRI | c‐statistic ASA | CI (95%) c‐statistic RCRI |
| Bronheim 2018 | Any noncardiac complication | 30 days | 3399 | 52,066 | 0.62 | (0.61 to 0.63) | 0.77 | (0.73 to 0.82) |
| Bronheim 2018 | Unplanned intubation | 30 days | 111 | 52,066 | 0.84 | (0.83 to 0.84) | 0.74 | (0.74 to 0.75) |
| Bronheim 2018 | Pulmonary embolism | 30 days | 149 | 52,066 | 0.41 | (0.4 to 0.42) | 0.81 | (0.81 to 0.82) |
| Bronheim 2018 | Ventilated > 48 hours | 30 days | 65 | 52,066 | 0.85 | (0.84 to 0.85) | 0.74 | (0.74 to 0.75) |
| Bronheim 2018 | Acute renal failure | 30 days | 36 | 52,066 | 0.88 | (0.88 to 0.89) | 0.79 | (0.78 to 0.79) |
| Bronheim 2018 | Cerebrovascular accident | 30 days | 42 | 52,066 | 0.75 | (0.74 to 0.75) | 0.84 | (0.84 to 0.84) |
| Bronheim 2018 | Coma > 24 hours | 30 days | 8 | 52,066 | 0.90 | (0.87 to 0.93) | 0.65 | (0.65 to 0.66) |
| Bronheim 2018 | Sepsis | 30 days | 259 | 52,066 | 0.83 | (0.82 to 0.83) | 0.91 | (0.9 to 0.91) |
| Bronheim 2018 | Septic shock | 30 days | 50 | 52,066 | 0.85 | (0.84 to 0.85) | 0.76 | (0.76 to 0.76) |
| Bronheim 2018 | Reoperation | 30 days | 912 | 52,066 | 0.85 | (0.85 to 0.86) | 0.87 | (0.86 to 0.87) |
| Bronheim 2018 | Superficial surgical site infection | 30 days | 452 | 52,066 | 0.72 | (0.71 to 0.72) | 0.84 | (0.84 to 0.85) |
| Bronheim 2018 | Deep incisional surgical site infection | 30 days | 297 | 52,066 | 0.88 | (0.88 to 0.88) | 0.95 | (0.95 to 0.95) |
| Bronheim 2018 | Organ space surgical site infection | 30 days | 104 | 52,066 | 0.88 | (0.87 to 0.88) | 0.78 | (0.77 to 0.78) |
| Bronheim 2018 | Wound dehiscence | 30 days | 102 | 52,066 | 0.72 | (0.71 to 0.72) | 0.79 | (0.79 to 0.8) |
| Bronheim 2018 | Pneumonia | 30 days | 177 | 52,066 | 0.74 | (0.73 to 0.74) | 0.82 | (0.82 to 0.83) |
| Bronheim 2018 | Progressive renal insufficiency | 30 days | 35 | 52,066 | 0.85 | (0.84 to 0.85) | 0.81 | (0.81 to 0.82) |
| Bronheim 2018 | Urinary tract infection | 30 days | 558 | 52,066 | 0.74 | (0.73 to 0.74) | 0.83 | (0.82 to 0.83) |
| Bronheim 2018 | Peripheral nerve injury | 30 days | 21 | 52,066 | 0.07 | (0.07 to 0.08) | 0.51 | (0.51 to 0.52) |
| Bronheim 2018 | Bleeding transfusions | 30 days | 1621 | 52,066 | 0.71 | (0.71 to 0.72) | 0.80 | (0.8 to 0.8) |
| Bronheim 2018 | Deep vein thrombosis/thrombophlebitis | 30 days | 165 | 52,066 | 0.71 | (0.7 to 0.71) | 0.78 | (0.78 to 0.79) |
| Bronheim 2018 | Readmission | 30 days | NR | 52,066 | 0.84 | (0.83 to 0.84) | 0.91 | (0.9 to 0.91) |
| Ehlert 2016 | Clavien Dindo class IV complications | In‐hospital | 800 | 5621 | 0.56 | NR | 0.55 | NR |
| Ehlert 2016 | Clavien Dindo class IV complications | In‐hospital | 541 | 15,354 | 0.59 | NR | 0.56 | NR |
| Ehlert 2016 | Clavien Dindo class IV complications | In‐hospital | 455 | 8367 | 0.56 | NR | 0.57 | NR |
| Ehlert 2016 | Clavien Dindo class IV complications | In‐hospital | 32 | 1833 | 0.56 | NR | 0.59 | NR |
| Ehlert 2016 | Clavien Dindo class IV complications | In‐hospital | 835 | 40,803 | 0.69 | NR | 0.56 | NR |
| Farina‐Castro 2020 | Postoperative complications (CCI 0 vs CCI ≥ 1) | Not reported | 179 | 244 | 0.69 | (0.60 to 0.79) | 0.65 | (0.56 to 0.74) |
| James 2014 | Surgical complications | 30 days | 40 | 83 | 0.53 | (0.4 to 0.65) | 0.60 | (0.48 to 0.72) |
| Makary 2010 | Surgical complications | 30 days | 34 | 594 | 0.72 | NR | 0.71 | NR |
| Makary 2010 | Discharge to a nursing facility | In‐hospital | 14 | 594 | 0.75 | NR | 0.78 | NR |
| Press 2006 | All‐cause mortality or nonfatal stroke | 30 days | 64 | 1998 | 0.61 | NR | 0.53 | NR |
| Press 2006 | Noncardiac complications | 30 days | 63 | 1998 | 0.66 | NR | 0.62 | NR |
| Press 2006 | Minor neurological complications | 30 days | 138 | 1998 | 0.56 | NR | 0.53 | NR |
| Press 2006 | Wound complications | 30 days | 119 | 1998 | 0.61 | NR | 0.54 | NR |
NR: not reported
8.
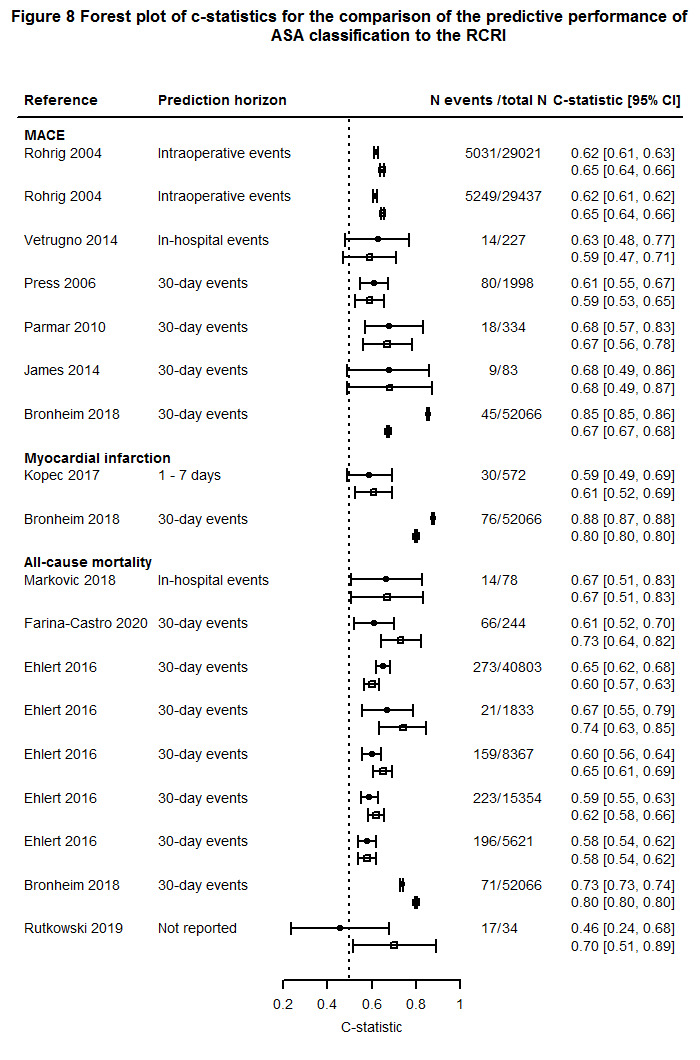
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents ASA.
Brain natriuretic peptide (BNP)
As mentioned before, BNP is released by cardiomyocytes due to myocardial stretch and used in clinical practice as a marker for heart failure (Yancy 2013). We included 10 articles that compared the predictive ability of BNP to the RCRI over 14 different analyses. Rodseth et al reported predictions for BNP and RCRI alone using four different outcomes (Rodseth 2011), and Katsanos et al used two different outcomes (i.e. MACE and all‐cause mortality; Figure 9; Katsanos 2015). Predictions were made for seven different outcome categories, i.e. MACE (n = 6), myocardial infarction (n = 1), all‐cause mortality (n = 2), a combination of the latter two (n = 1), cardiovascular mortality (n = 1), troponin elevation (n = 1) and other (noncardiac) outcomes (n = 2). The number of included patients was low (i.e. less than 50) resulting in wide confidence intervals. The delta c‐statistic was 0.15 (0.0 to 0.24) in favour of BNP compared to the predictive discriminative performance of the RCRI to predict MACE (6 studies, n = 2301, unknown number of MACE). For one study, the number of outcomes was not reported (Rodseth 2011). Surgical specialties were orthopaedic, general, vascular and noncardiac surgery. The prediction horizon was in‐hospital or 30‐day MACE. None of the included studies reported on calibration or reclassification measures.
9.
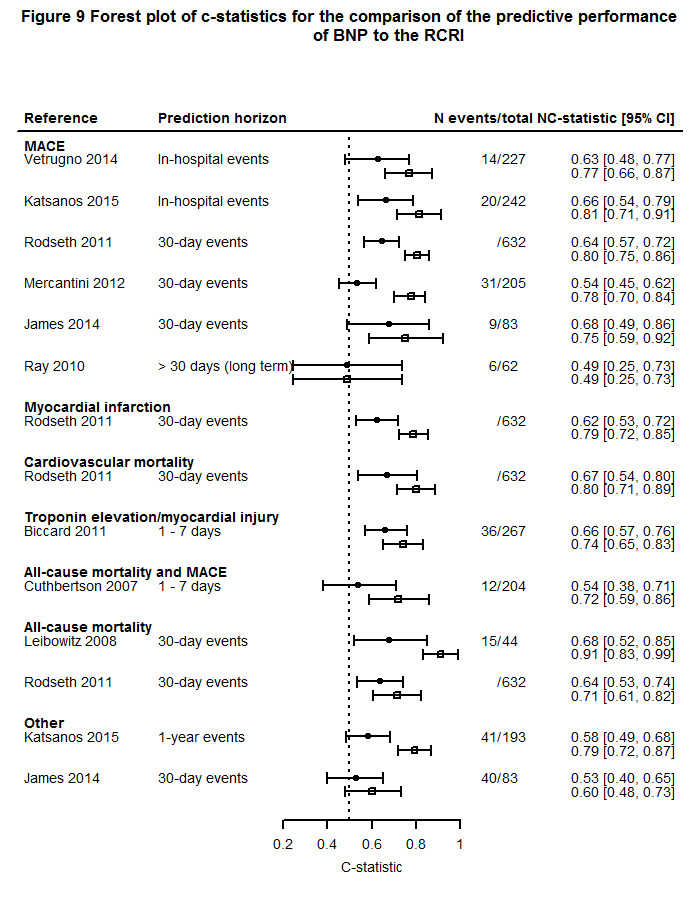
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents BNP alone.
NT‐proBNP
NT‐proBNP is used as marker for heart failure in clinical practice (Yancy 2013). The predictive performance of NT‐proBNP was compared to the RCRI alone in 15 validations over 11 included articles (Figure 10). Feringa et al reported four different analyses on two different outcomes (i.e. all‐cause mortality and MACE) in two different patient populations (Feringa 2007). Weber et al reported prediction for two different outcomes (i.e. all‐cause mortality and all‐cause mortality and MACE) (Weber 2013). MACE was predicted in nine different validations, however the prediction horizon varied from in‐hospital to long‐term events in either vascular or noncardiac surgical patients. Six articles studied NT‐proBNP on a continuous scale, one on a categorical scale (Biccard 2011), and three on a dichotomous scale. For one article, the method of handling NT‐proBNP was unclear (Feringa 2007). The confidence intervals were wide and there was large heterogeneity between included studies due to the different study populations, outcome composition and prediction horizons. Using MACE as an outcome, the delta c‐statistic was 0.15 (range 0.02 to 0.22) in favour of NT‐proBNP (6 studies, n = 3256, 457 MACE) (Binh 2019; Borges 2013; Feringa 2007; Golubovic 2018; Park 2011; Yang 2012). In these studies, the surgical specialty was vascular and noncardiac surgery and the prediction horizons varied between in‐hospital, 30‐day and 6 months. None of the included studies reported on calibration or reclassification measures.
10.
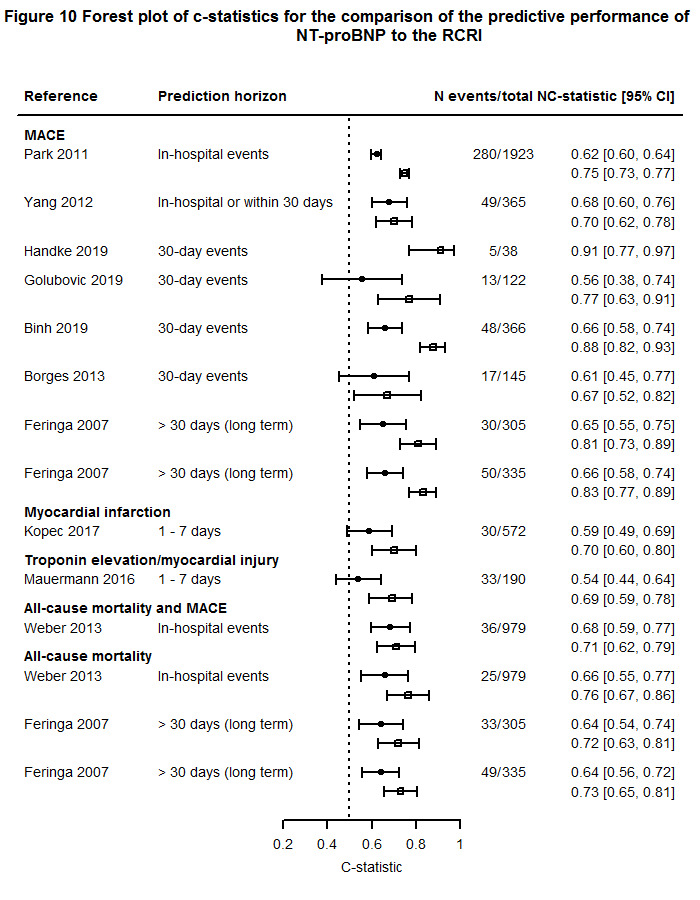
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents NT‐proBNP alone. As Handke 2019 solely reported on the c‐statistics for the additive model, no c‐statistic for RCRI alone is provided for this study.
Troponin
Troponin is a protein released by cardiomyocytes in case of myocardial ischaemia (Mair 2018; Thygesen 2018). We included six articles reporting on eight validations (Figure 11). Gualandro et al predicted MACE using troponin in two different populations (i.e. vascular and nonvascular patients) (Gualandro 2018). Although the aim in that study was to compare the predictive performance of troponin to the RCRI, only the c‐statistic for troponin alone was reported. Included patients underwent either vascular (n = 2) or noncardiac surgery (n = 4). For the prediction of all‐cause mortality and MACE (2 studies, n = 1154, 52 events), higher c‐statistics were observed for troponin alone compared to the RCRI (median delta c‐statistic 0.09, range 0.09 to 0.10) (Weber 2013; Yang 2018). None of the included studies reported on calibration or reclassification measures.
11.
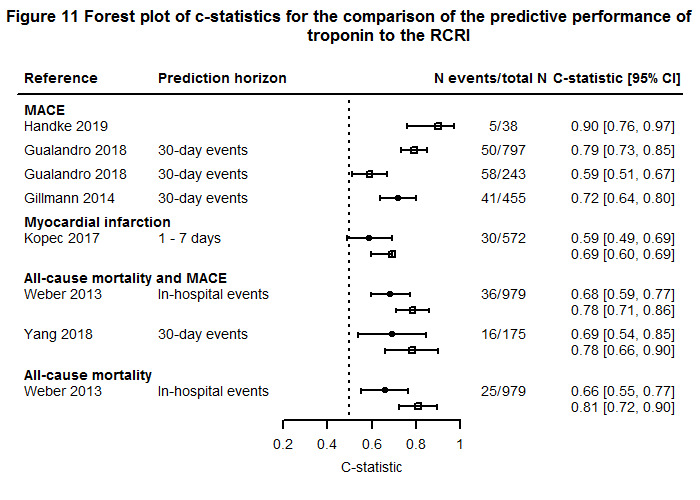
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents troponin alone. As Handke 2019 and Gualandro 2018 solely reported on the c‐statistics for the additive model, no c‐statistic for RCRI alone is provided for this study. Gillmann 2014 only reported c‐statistics for RCRI alone.
C‐reactive protein (CRP)
C‐reactive protein (CRP) is a sensitive systemic marker of inflammation and tissue damage. The acute‐phase response comprises the nonspecific physiological and biochemical responses of tissue damage, infection, inflammation and malignant neoplasia (Pepys 2003). Three articles compared the predictive ability of CRP to the RCRI (Figure 12). James et al made predictions for two different outcomes (i.e. MACE and postoperative complications) (James 2014). All included patients underwent noncardiac surgery except for patients included in the study Ray 2010, who underwent orthopaedic surgery. Two studies compared the predictive discriminative performance of CRP to the RCRI to predict MACE resulting in a delta c‐statistic of ‐0.01 with a range of ‐0.12 to 0.10 (n = 306, 15 MACE) (James 2014; Ray 2010). None of the included studies reported on calibration or reclassification measures.
12.
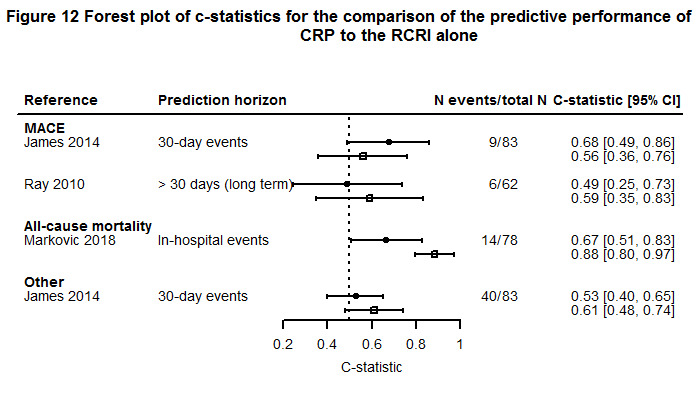
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents CRP alone.
Objective 3: Comparison of predictive value of prediction models to the RCRI
Study design and study population
Fifty‐one articles compared the predictive ability of the RCRI to another prediction model, reporting on 79 validations of the RCRI with a unique outcome (Table 6). Most validations were based on cohort study data (n = 68, 86%). Retrospective study data were most common (n = 54, 68%). Included patients originated most commonly from Europe (36%) or North America (35%) and most frequently underwent noncardiac (47%) or vascular surgery (32%). The median number of included patients was higher for this objective compared to articles reporting on the added value or the predictive performance of biomarkers to the RCRI (median (IQR)): 941 (251 to 2284), 442 (223 to 1389) and 594 (227 to 52,066), respectively). The most frequently used prediction horizons were during hospital admission (18%) or 30 days (66%) after surgery. The outcome of interest was most often MACE (41%) followed by other outcomes (e.g. stroke, transient ischaemic attack (TIA), systemic embolism (20%), all‐cause mortality (17%) and myocardial infarction or cardiac arrest (9%). The number of publications increased over time with most included articles in the 2018 to June 2020 period (Figure 4).
Composition of MACE
For included studies that used MACE (also in combination with all‐cause mortality) as an outcome, all validations used a different definition meaning that the composition of MACE varied among the included validations (Table 7). We found 19 different composites for MACE. Similar to the articles reporting on the added value or the predictive performance of biomarkers to the RCRI, the most frequently used composite of MACE was myocardial infarction, i.e. in 26 out of 45 different definitions. The MACE definition also commonly included heart failure (42%), cardiac arrest (40%), cardiac death (24%) or stroke (20%).
Risk of bias and concern regarding applicability
We judged 44 (85%) articles that compared the predictive performance of the RCRI to other prediction models as having overall high risk of bias. Most articles scored as having low risk of bias for participants (n = 44, 85%). For predictors, 27 (52%) articles scored as having unclear risk of bias, for outcome 2 (4%) and for analyses 40 (77%) articles scored as having high risk of bias. Comparable to articles included in the other objectives, most articles had high concern regarding applicability (n = 44, 85%) (Figure 2; Figure 3). We observed no differences in the reasons for judgements of high or unclear of risk of bias and concern regarding applicability among the different objectives. Accordingly, more detailed information is described below under the subheading 'Risk of bias and concern regarding applicability' as part of the first objective.
Performance measures reported
Discrimination measures were reported in 50 (96%) articles mostly using a c‐statistic (n = 48, 92%) (Table 8). Calibration was more often reported in articles that compared the predictive performance of other prediction models to the RCRI than articles that studied the added value or the comparison of the predictive ability of biomarker to the RCRI (42%, 20% and 29%, respectively). This was in particular by means of the calibration plot and observed/expected ratio. Reclassification measures were reported in five (10%) articles using a NRI.
Prediction models compared to the RCRI
An overview of prediction models for which the predictive performance was compared to the RCRI is presented in Table 12. Fifty‐two articles compared the predictive ability of the RCRI to other prediction models. In these 52 studies, 27 (42%) addressed the development of a new prediction model, 14 (22%) updated the RCRI or another prediction model, and 24 (37%) addressed the validation of an existing prediction model.
9. Prediction models for which the predictive performance was compared to the RCRI.
| Number of studies | |
| NSQIP‐MICA | 10 |
| NSQIP surgical risk score | 9 |
| CHADS2 score | 4 |
| Detsky index | 4 |
| Goldman index | 4 |
| CHADS2VASc | 3 |
| R2CHADS2 score | 3 |
| Vascular Study Group of New England Cardiac Risk Index | 3 |
| AUB‐HAS2 Cardiovascular Risk Index | 2 |
| Charlson Index | 2 |
| Glasgow Aneurysm Risk score | 2 |
| Halm score | 2 |
| Individual items of the RCRI | 2 |
| POSSUM | 2 |
| P‐POSSUM | 2 |
| RCRI without insulin use with low eGFR | 2 |
| Reiss Index | 2 |
| South African Vascular Surgical Cardiac Risk Index | 2 |
| Surgical Mortality Probability Model | 2 |
| Thoracic RCRI | 2 |
| Tu score | 2 |
| V‐POSSUM | 2 |
| Adult Comorbidity Evaluation‐27 score | 1 |
| Adult Comorbidity Evaluation‐27 score + high age | 1 |
| Age + type of admission + RCRI + arrhythmia + electrolyte disorder + hypertension | 1 |
| Age + type of admission + RCRI + arrhythmia + electrolyte disorder + hypertension + polygenic risk score for coronary artery disease | 1 |
| ANESCARDIOCAT | 1 |
| ASA + NSQIP surgical risk score | 1 |
| ASA + Surgical Outcome Risk Tool | 1 |
| Ashton | 1 |
| Biochemistry and Haematology Outcome Model | 1 |
| Coronary artery disease + atrium fibrillation + diabetes mellitus + mechanical ventilation + heart rate | 1 |
| CR‐POSSUM | 1 |
| Detsky score + type of surgery | 1 |
| Dilated cardiomyopathy + ischaemic cardiopathy + CVA | 1 |
| Eagle score | 1 |
| Geriatric Sensitive Perioperative Cardiac Risk Index | 1 |
| Insulin use + open surgery + high fibrinogen + CRP + NT‐proBNP | 1 |
| Long Term Survival Score | 1 |
| MASHOUR | 1 |
| Modified Frailty Index | 1 |
| Myocardial infarction + sex + insulin‐dependent diabetes mellitus + low BMI + high age + atrium fibrillation | 1 |
| New model 1 | 1 |
| New model 2 | 1 |
| New model 3 | 1 |
| NSQIP score "Death" | 1 |
| NT‐proBNP + high creatinine + ischaemic heart disease + congestive heart failure | 1 |
| Patient Outcomes in Renal Transplant model | 1 |
| Preoperative risk score of the estimation of physiological ability + surgical stress score | 1 |
| RCRI with redefined high‐risk surgery | 1 |
| RCRI with redefined high‐risk surgery and clinical characteristics | 1 |
| RCRI without insulin use and creatinine > 2.0 mg/dL | 1 |
| Recalibrated NSQIP surgical risk score | 1 |
| Recalibrated RCRI | 1 |
| Regulatory T cells + age + sex + ASA + previous PCI + creatinine | 1 |
| Surgical Outcome Risk Tool | 1 |
| Surgical risk score | 1 |
| TJA individual factors | 1 |
| TJA risk score | 1 |
| Updated Cardiac Risk Score | 1 |
| Vascular Biochemistry and Haematology Outcome Model | 1 |
| Vascular Quality Initiative Cardiac Risk Index | 1 |
| Vascular Study Group of New England Cardiac Risk Index + anaemia | 1 |
| V‐POSSUM + troponin | 1 |
| V‐POSSUM + troponin + NT‐proBNP | 1 |
ACE‐27: adult comorbidity evaluation‐27; ACS‐NSQIP: American College of Surgeons National Surgical Quality Improvement Program; CHADS2 score: congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus, stroke (double weight); CHADS2VASc: CHADS2 added with vascular disease, age 65 to 74 years and sex; CR‐POSSUM: POSSUM score for colorectal surgical patients; MICA: myocardial infarction and cardiac arrest; New model 1: age, sex, history of coronary revascularisation, aortic or mitral valve disease, arrhythmia, hypertension, carotid artery stenosis, hypovolaemia, chronic renal failure, emergency surgery, neurosurgery, thoracic surgery, major vascular surgery, haematopoietic/lymphatic surgery, gastro‐intestinal surgery; New model 2: age, ASA, neurosurgery, thoracic surgery, major vascular surgery, haematopoietic/lymphatic surgery, gastro‐intestinal surgery; New model 3: history of myocardial infarction, age > 70, insulin dependent diabetes mellitus, female, BMI < 18, operation time > 2.5 hours, atrium fibrillation, intraoperative hypotension; P‐POSSUM: Portsmouth‐POSSUM; POSSUM: Physiologic and Operative Severity Score for the enUmeration of Mortality and Morbidity; R2CHADS2: CHADS2 score added with renal failure (double weighted); SORT: Surgical Outcome Risk Tool; TJA: total joint arthroplasty; V‐POSSUM: POSSUM for vascular surgical patients
For prediction models for which the predictive performance was compared head‐to‐head to the RCRI in at least three different studies, the study characteristics are described in further detail below. These prediction models were ACS‐NSQIP‐MICA, ACS‐NSQIP‐SRS, CHADS2 score, Goldman index, Detsky index, CHADS2VASc, R2CHADS and Vascular Study Group of New England Cardiac Risk Index.
ACS‐NSQIP‐MICA
The ACS‐NSQIP‐MICA was developed in 2011 and provides a risk estimate of 30‐day myocardial infarction or cardiac arrest (MICA) in patients undergoing noncardiac surgery. Data from the ACS‐NSQIP was used for the development of the model (Gupta 2011). Predictions for MACE were made in four articles describing 11 validations. The delta c‐statistic was reported in three studies (n = 1567, 95 MACE) and not different between both models (delta median c‐statistic 0, range ‐0.09 to 0.04) (Cohn 2018; Fronczek 2019; Rutkowski 2019). One study showed poor calibration for both RCRI and ACS‐NSQIP‐MICA in a calibration plot with an intercept of 0.95 and 2.37 and slope of 0.29 and 0.70 for the RCRI and ACS‐NSQIP‐MICA, respectively (Fronczek 2019). Cohn 2018 reported on six validations (i.e. all elective noncardiac patients, patients with short (≤ 2 days) and long (> 2 days) hospital stay using both prediction horizons for in‐hospital and 30‐day events). Rutkowski 2019 presented three validations (i.e. patients undergoing elective craniotomy, deceased patients and surviving patients) and Fronczek 2019 and Glance 2018 reported on the validation in a vascular and noncardiac surgical population, respectively. Six articles (n = 243,896, unknown MICAs) predicted 30‐day MICA in nine analyses, which resulted in higher predictive performance of the ACS‐NSQIP‐MICA compared to the RCRI alone (delta median c‐statistic 0.11, range ‐0.05 to 0.39). In one study, the number of events was not reported (Gupta 2011). Calibration was poor for both scores, however calibration was better for the RCRI compared to the ACS‐NSQIP‐MICA (2 studies, n = 181,920, 1889 MICAs) (Alrezk 2017; Glance 2018). The Hosmer Lemeshow for the RCRI ranged from P = 0.018 to P < 0.001 and was P < 0.001 for the ACS‐NSQIP‐MICA. Calibration improved after recalibration of the NSQIP‐MICA (Asuzu 2018; Glance 2018). Asuzu 2018 reported three validations among patients undergoing open procedures, laparoscopic procedures or all included procedures and Alrezk 2017 studied geriatric and non‐geriatric patients. None of the included studies reported on reclassification measures. Information regarding the c‐statistics is presented in Figure 13.
13.
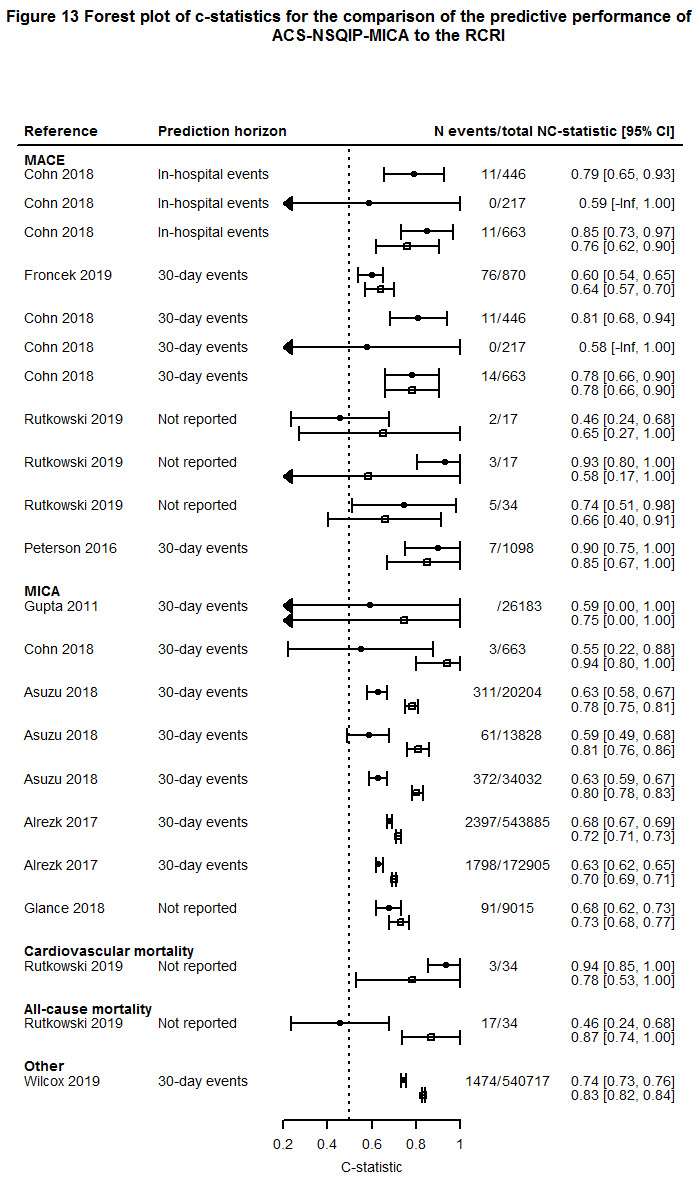
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the ASC‐NSQIP surgical risk score. As Cohn 2018 solely reported on the c‐statistics for the RCRI, no c‐statistic for NSQIP MICA is provided for this study.
ACS‐NSQIP surgical risk score (ACS‐NSQIP‐SRS)
The American College of Surgeons National Surgical Quality Improvement Program surgical risk score (ACS‐NSQIP‐SRS) is a decision‐support tool based on multi‐institutional clinical data, which can be used to estimate the risks of multiple outcomes (including myocardial infarction) for most operations (Bilimoria 2013). We included 10 articles reporting 18 different validations (Figure 14). Two studies compared the discriminative performance of the RCRI to the ACS‐NSQIP‐SRS for predicting MACE, resulting in a median delta c‐statistic of 0.06 with a range of 0.00 to 0.11 in favour of the ACS‐NSQIP‐SRS (n = 1087, 26 MACE) (Cohn 2018; Yap 2018). To predict MICA (2 studies, n = 9678, 94 MICA), the ACS‐NSQIP‐SRS had a higher c‐statistic compared to the RCRI (delta median c‐statistic 0.18 with range 0.13 to 0.22) (Cohn 2018; Glance 2018). Calibration was reported in one study and showed poor calibration for the RCRI and acceptable calibration for the ACS‐NSQIP‐SRS (Hosmer Lemeshow RCRI: P < 0.001; ACS‐NSQIP‐SRS, P = 0.07). However, data from the NSQIP database was used in this study (Glance 2018). Using all‐cause mortality as an outcome (3 studies, n = 2461, 155 deaths), the ACS‐NSQIP‐SRS had a higher discriminative performance compared to the RCRI (median delta c‐statistic 0.14, range 0.11 to 0.15) (Markovic 2018; Neary 2007; Rutkowski 2019). One article predicted the 30‐day risk of stroke in a large cohort originating from the NSQIP registry, showing better predictive performance for the ACS‐NSQIP‐SRS compared to the RCRI (delta c‐statistic 0.10; Wilcox 2019). None of the included studies reported on reclassification measures.
14.
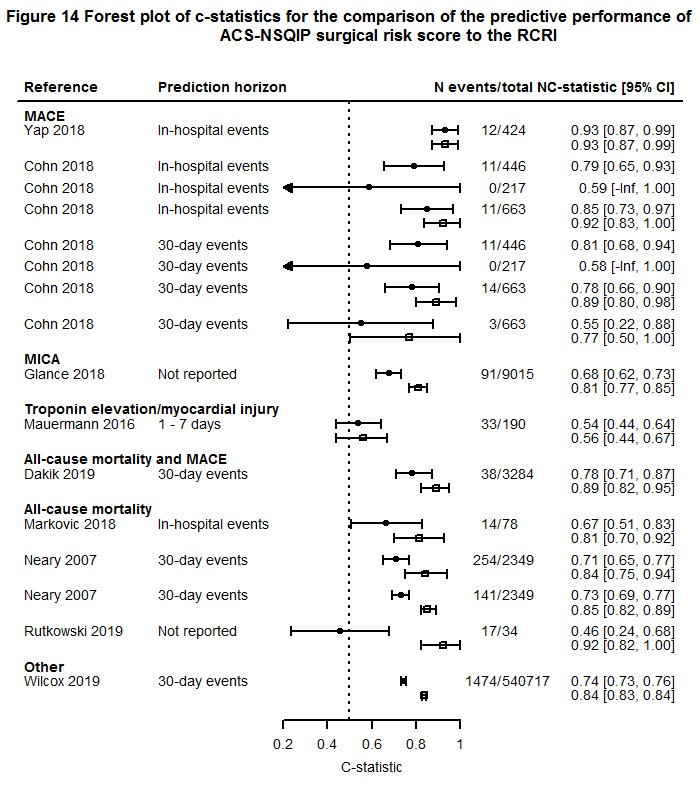
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the NSQIP surgical risk score.
CHADS2
The CHADS2 is a combination of two existing risk scores to predict stroke in patients diagnosed with atrial fibrillation. CHADS2 is an acronym for its risk factors and their scoring. The score is calculated adding one point each for any of the following: recent congestive heart failure, hypertension, age 75 years or older and diabetes mellitus, and two points for a history of stroke or TIA (Gage 2001). Four articles reported on 17 validations of which nine were described by McAlister et al (McAlister 2020). Eight of these validations reported on varying outcomes including MACE, all‐cause mortality, vascular death, stroke, myocardial injury, congestive heart failure and nonfatal cardiac arrest in a noncardiac surgical population derived from the VISION study (Devereaux 2017). The other validation by McAlister et al was in patients undergoing only high‐risk surgery to predict all‐cause mortality and stroke (delta c‐statistic 0.07) (McAlister 2015). The predictive performance in terms of the c‐statistics are presented in Figure 15. CHADS2 was compared to the RCRI to predict 30‐day all‐cause mortality in three studies (n = 35,129, 1177 deaths), resulting in a median delta c‐statistic of 0.00 (range ‐0.02 to 0.01) and a median NRI of 0.07 (range 0.01 to 0.12) (McAlister 2015; McAlister 2020; van Diepen 2014). Using stroke as an outcome, the median delta c‐statistic was 0.02 (range ‐0.01 to 0.11; 4 studies, n = unknown, unknown events) with NRI 0.05 (range ‐0.06 to 0.17; 2 studies, n = 33,121, 391 events) in favour of CHADS2 (McAlister 2015; McAlister 2020; van Diepen 2014; Wilcox 2019). Three studies (n = 33,748, unknown events) compared the CHADS2 to the RCRI to predict all‐cause mortality or stroke resulting in a median delta c‐statistic of 0.03 (range 0.02 to 0.07) and a median NRI of 0.31 (range 0.14 to 0.35) (McAlister 2015; McAlister 2020; van Diepen 2014). None of the included studies reported on calibration measures.
15.
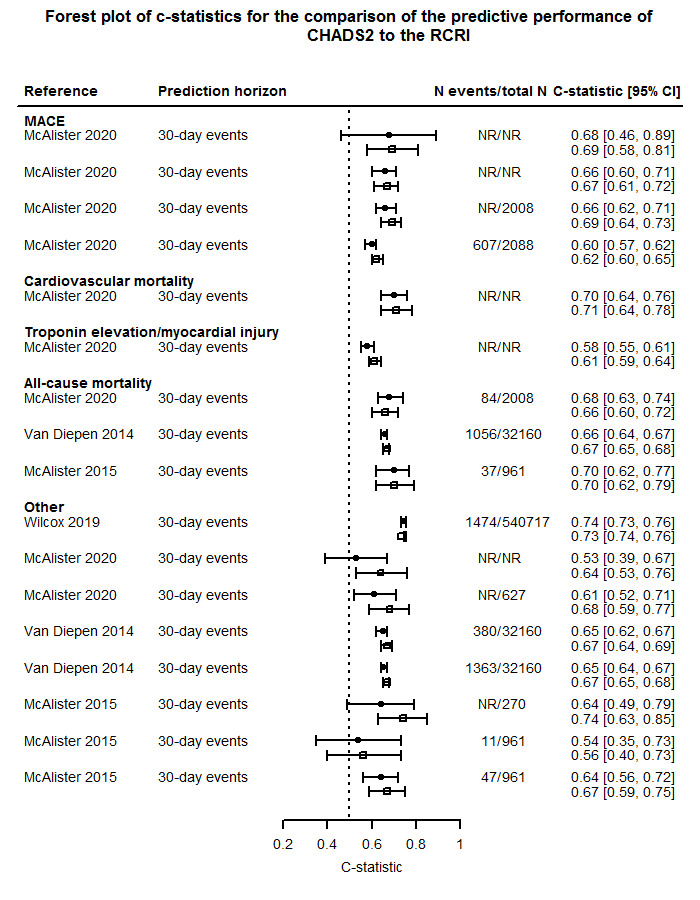
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the CHADS2.
Goldman index
The Goldman index represents a multivariable approach to estimate cardiac risk in patients undergoing noncardiac procedures (Goldman 1977). The model was developed in 1977 and can be considered as a previous version of the RCRI. The RCRI and Goldman index were validated in three articles reporting on eight validations (Figure 16). Press et al reported on predictions of five different outcomes (i.e. MACE and four noncardiac outcomes) in patients undergoing vascular surgery (Press 2006). No difference in c‐statistic was found, which could be explained by the fact that both models were not originally developed to predict noncardiac outcomes. Katsanos et al compared the RCRI to the Goldman index to predict in‐hospital MACE and one‐year all‐cause mortality in patients undergoing orthopaedic surgery (Katsanos 2015), and Pantoja Muñoz et al used both models to predict in‐hospital MACE (Pantoja 2014). For the latter, only sensitivity and specificity measures were reported and therefore the data were not sufficient to be presented in a forest plot. Three studies (n = 3361 patients, 191 MACE) compared the discriminative performance of the Goldman index to the RCRI, which resulted in a median delta c‐statistic of ‐0.03 with a range of ‐0.07 to 0.08 in favour of the RCRI (Katsanos 2015; Kumar 2001; Press 2006). Reclassification or calibration were not reported in any of the included studies.
16.
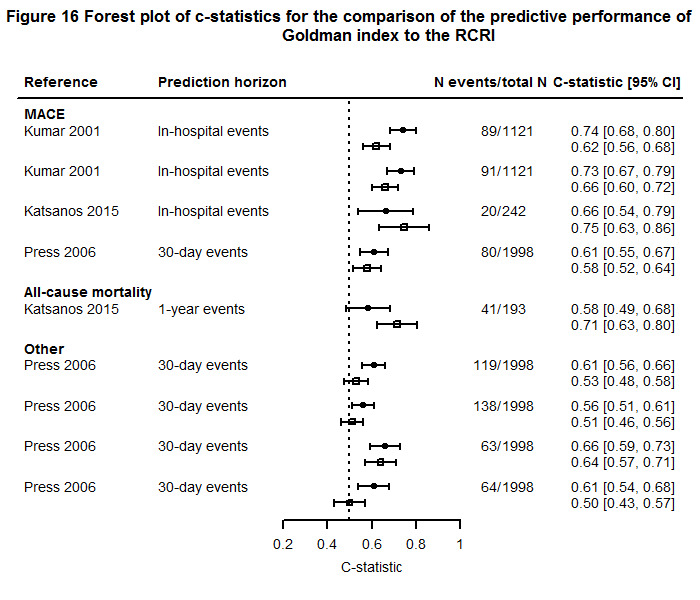
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the Goldman index.
Detsky index
The Detsky index is a modified version of an index that was previously generated by Goldman in 1977 (Detsky 1986). This model was developed in 1986 and revised to the RCRI by Lee et al in 1999 (Lee 1999). The same articles that were identified for the Goldman index also compared the discriminative performance of the Detsky index to the RCRI, resulting in a median delta c‐statistic of 0.05 with a range of ‐0.07 to 0.11 in favour of the Detsky index (Figure 17) (Katsanos 2015; Kumar 2001; Press 2006). Again, reclassification or calibration were not reported in any of the included studies.
17.
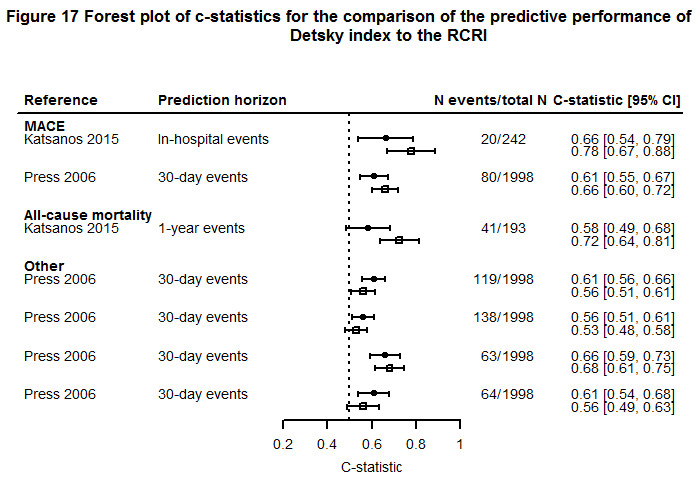
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the Detsky index.
CHA2DS2‐VASc
In 2010, the CHADS2 was updated and additional new risk factors were incorporated. For the CHA2DS2‐VASc, one point is assigned to congestive heart failure/left ventricular dysfunction, hypertension, age between 65 and 74 years, diabetes mellitus, vascular disease (prior myocardial infarction, peripheral artery disease or aortic plaque) and sex category, and two points for age ≥ 75 years and history of stroke, TIA or thromboembolism (Lip 2010). Similar articles were identified that reported on the validation of the CHADS2 (McAlister 2015; McAlister 2020; Wilcox 2019). Comparison of the predictive performance of the CHA2DS2‐VASc to the RCRI is presented in Figure 18. CHADS2‐VAScwas compared to the RCRI to predict 30‐day all‐cause mortality in two studies (n = 2969, 121 deaths), resulting in a median delta c‐statistic of 0.00 (range ‐0.02 to 0.02) and a median NRI of 0.09 (range 0.01 to 0.17) (McAlister 2015; McAlister 2020). Using stroke as an outcome, the median delta c‐statistic was 0.04 (range 0.00 to 0.12; 3 studies, n = unknown, unknown events) with a NRI of 0.05 (range ‐0.06 to 0.17; 1 study, n = 961, 11 events) in favour of CHADS2‐VASc (McAlister 2015; McAlister 2020; Wilcox 2019). Two studies (n = 1588, unknown events) compared the CHADS2‐VASc to the RCRI to predict all‐cause mortality or stroke, resulting in a median delta c‐statistic of 0.04 (range 0.01 to 0.07) and a median NRI of 0.30 (range 0.14 to 0.35) (McAlister 2015; McAlister 2020). None of the included studies reported on calibration measures.
18.
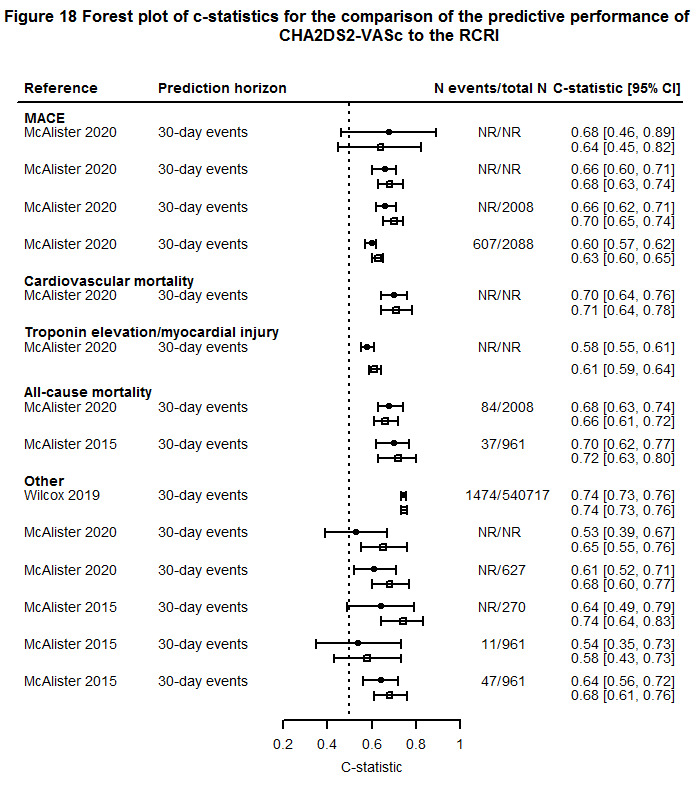
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the CHA2DS2‐VASc.
R2CHADS2
A new update of the CHADS2 was published in 2013. In this version, two points were added to the CHADS2 score for creatinine clearance < 60 mL/min to designate the R2CHADS2. The outcome to be predicted was stroke (both ischaemic and haemorrhagic) and systemic embolism (Piccini 2013). The model was compared to the RCRI by three different articles describing 16 validations (McAlister 2015; McAlister 2020; van Diepen 2014). In three different validations, Van Diepen et al predicted all‐cause mortality, the composite of stroke, TIA and systemic embolism, and the combination of all these outcomes in a noncardiac surgical population (van Diepen 2014). Comparison of the predictive performance of the R2CHADS2 to the RCRI is shown in Figure 19. R2CHADS2 was compared to the RCRI to predict MACE in one study resulting in a delta c‐statistic of 0.02 and a NRI of 0.21 (McAlister 2020). All‐cause mortality was predicted in three studies (n = 35,129, 1177 deaths) and resulted in a median delta c‐statistic of ‐0.03 (range ‐0.03 to 0.03) and a total NRI of 0.03 (range ‐0.09 to 0.13) in favour of R2CHADS2. For the prediction of stroke, the median delta c‐statistic was 0.05 with a range of 0.01 to 0.12 (3 studies, n = unknown, unknown events) and the NRI was ‐0.06 with a range of ‐0.14 to 0.01 (2 studies, n = 33,121, 391 events) (McAlister 2015; McAlister 2020; van Diepen 2014). Three studies reported on the comparison of R2CHADS2 to the RCRI to predict all‐cause mortality or stroke (n = 33,748, unknown events), which resulted in a median delta c‐statistic of 0.03 with a range of 0.01 to 0.06 and a median NRI of 0.17 with a range of 0.11 to 0.44 (McAlister 2015; McAlister 2020; van Diepen 2014). None of the included studies reported on calibration measures.
19.
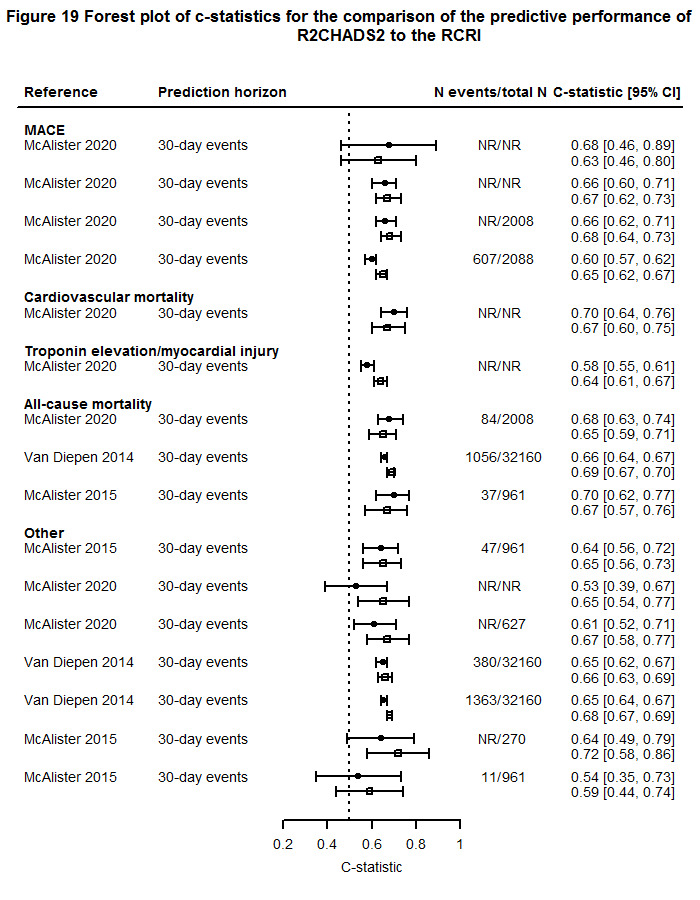
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the R2CHADS2.
Vascular Study Group of New England Cardiac Risk Index (VSG‐CRI)
In response to the fact that the RCRI does not accurately predict cardiac events in vascular surgery patients, a new prediction model was developed to predict a composite cardiac outcome of in‐hospital myocardial infarction (MI), clinically significant new arrhythmia or congestive heart failure (CHF). The model was developed in patients undergoing a broad range of vascular surgery, i.e. carotid endarterectomy, open abdominal aortic aneurysm repair, endovascular abdominal aortic aneurysm repair and lower extremity bypass (Bertges 2010). Eight validations were reported by three articles in vascular surgical patients (Avena 2015; Gualandro 2018; Reis 2019). Comparison of the discriminative performance of the VSG‐CRI to the RCRI is presented in Figure 20. Three studies (n = 2023, 208 MACE) compared the VSG‐CRI to the RCRI resulting in a delta c‐statistic of 0.03 with a range of 0.00 to 0.05 (Avena 2015; Gualandro 2018; Reis 2019). The surgical specialty in all studies was vascular surgery. The prediction horizon was in‐hospital MACE, but in one study the prediction horizon was not reported. None of the included studies reported on calibration or reclassification measures.
20.
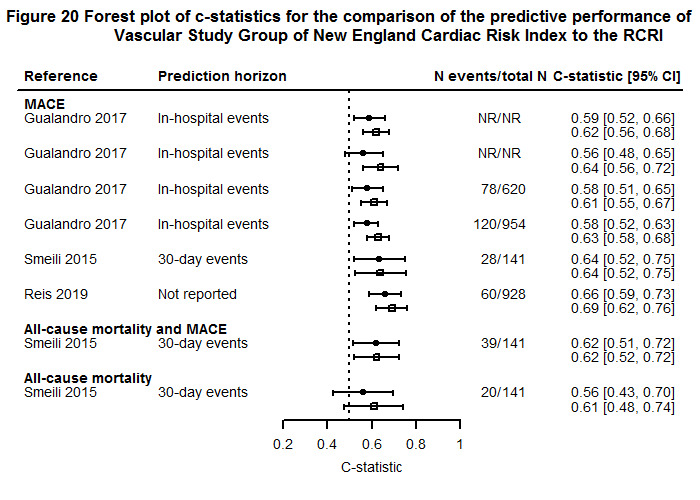
Per article, two c‐statistics with confidence intervals are presented. The upper (filled circle) represents the RCRI alone and the lower (open square) represents the Vascular Study Group of New England Cardiac Risk Index.
Discussion
Summary of main results
We screened 3962 studies resulting in a final inclusion of 107 studies. In general, over the three objectives, 'concern regarding applicability' and 'risk of bias' were rated as high in at least one domain in 78% and 90% of the included studies, respectively, the latter particularly in the analysis domain. Furthermore, the composition of predicted outcomes was very heterogeneous, especially for major adverse cardiac events (MACE) for which 80 different definitions were reported. Also the number of included patients and outcome events was relatively low in the majority of the studies. We deemed pooling of the results (delta c‐statistic) impossible due to large heterogeneity in various aspects; i.e. in the (composition of the) used outcomes, the scale by which the biomarker was added to the model (i.e. dichotomous, continuous or categorical) and in the patient populations (e.g. vascular and noncardiac surgery).
In total, 51 articles reported on the added value of predictors to the Revised Cardiac Risk Index (RCRI) in 62 outcome validations. We identified 69 unique predictors that were added to the RCRI, which were derived from blood (29%), imaging (33%) or other types of predictors such as age, anaemia or six‐metre walking test (38%). Addition of N‐terminal pro‐B type natriuretic peptide (NT‐proBNP), troponin or a combination of both improved the RCRI model for the prediction of MACE with a median delta c‐statistic ranging from 0.04 to 0.22, 0.06 to 0.33 and 0.10 to 0.34 for NT‐proBNP, troponin and their combination, respectively, as compared to the c‐statistic for the RCRI alone. The total net reclassification index (NRI) ranged from 0.09 to 0.22 and 0.26 to 1.22 in favour of troponin and NT‐proBNP, respectively, as compared to the classification of the RCRI alone. Data on (improved) calibration of the biomarkers when added to the RCRI was not reported. For the prediction of myocardial infarction, the median delta c‐statistic range when NT‐proBNP was added to the RCRI was 0.06 to 0.07 and 0.06 to 0.11 for the prediction of all‐cause mortality and MACE combined. For BNP and copeptin, the data were not sufficient to provide median results on their added predictive performance, for any of the outcomes.
The predictive performance of biomarkers alone was compared to the RCRI in 51 articles reporting on 89 validations. Sixty unique biomarkers were identified that were compared to the RCRI. Predictors were derived from blood (38%), imaging (30%) or other types of characteristics such as the American Society of Anesthesiologists classification (ASA), functional capacity or ankle‐to‐arm‐index (32%). Regarding ASA, predictions were similar to the RCRI for each of the studied outcomes (median delta c‐statistics ‐0.02, 0.02 and 0.05 for MACE, myocardial infarction and all‐cause mortality, respectively). In studies different from those identified in objective 1, the median delta c‐statistic was 0.15 and 0.12 in favour of BNP and NT‐proBNP alone, respectively, when compared to the RCRI, for the prediction of MACE. For C‐reactive protein (CRP), the predictive performance was similar to the RCRI in predicting MACE. For other biomarkers and outcomes, no summary results could be given due to insufficient data. Only one study reported on calibration and none on reclassification measures.
For the third objective, in 52 articles we found 65 different prediction models that were compared to the RCRI. In these 52 studies, 27 (42%) addressed the development of a new prediction model, 14 (22%) updated the RCRI or another prediction model and 24 (37%) reported on the validation of an existing prediction model. None of the prediction models that were compared to the RCRI showed better predictive performance for the prediction of MACE compared to the RCRI. For the prediction of myocardial infarction and cardiac arrest, the ACS‐NSQIP‐MICA had a higher median delta c‐statistic of 0.11 (range ‐0.05 to 0.39) compared to the RCRI. Using all‐cause mortality as an outcome, the predictive performance of the ACS‐NSQIP surgical risk score was higher compared to the RCRI (median delta c‐statistic 0.15, range 0.12 to 0.47). The predictive performance was not better for the CHADS2, CHA2DS2‐VASc, R2CHADS2, Goldman index, Detsky index or Vascular Study Group of New England Cardiac Risk Index compared to the RCRI for any of the validated outcomes. Only one study reported on calibration measures; reclassification measures were reported in three studies.
Certainty of the evidence
There is currently no official GRADE guidance available for grading summarised results of prognostic model studies. Therefore, we did not perform rating of the certainty of evidence (Kreuzberger 2020).
Limitations of the included studies
We rated risk of bias as 'high' in at least one domain in 96 (90%) of all included studies. The reasons for judgements of high risk of bias were mainly the inappropriate in‐ or exclusion of participants, low numbers of events, not reporting of relevant performance measures at all or without uncertainty measures. TRIPOD recommends reporting of both discrimination and calibration measures in all prediction model papers (Collins 2015; Moons 2015). Discrimination was reported in most studies, however calibration measures were not. Evaluation of calibration is highly important since the model predictions are actually used to inform patients and physicians to make decisions (Van Calster 2019). In addition, none of the included articles used proper methods for handling of missing data. Only four studies (4%) reported on handling of missing data by assumption of normal values (n = 2, e.g. in case of missing postoperative creatinine measurement), last measurement carried forward or mean imputation. We judged concerns regarding applicability to be 'high' in 84 (79%) of all included studies, mainly due to strict in‐ and exclusion criteria and the use of other outcomes than the outcome that was used in the development study, i.e. MACE. Many included articles, for example, reported predictions for other cardiac complications, noncardiac complications and all‐cause mortality.
Finally, meta‐analyses of the predictive performance measures (including c‐statistics) were not possible due to extreme clinical and methodological heterogeneity across studies. This heterogeneity included a wide variety in biomarkers and prediction models added or compared to the RCRI, outcome definitions and prediction horizons, and there was no uniformity in the scales by which the predictor was added/compared to the RCRI (i.e. continuous, categorical or dichotomous).
Limitations of the review
Several limitations should be addressed. Firstly, we excluded articles for which the full text was not available (4%). This may have led to an underestimation of the number of predictors that are added or compared to the RCRI. Secondly, we encountered missing data for many of the included studies especially in the predictive performance measures. However, we did not contact study authors for additional information (e.g. on performance measures) as we anticipated that this would not result in different conclusions, given the expectation that this information would not be available to them in any case. The main reason why pooling of the results was not possible was less the lack of data than the extreme heterogeneity and high risk of bias in the majority of the included studies. Thirdly, we did not extract clinical utility measures such as decision curves or net benefit since almost none of the papers reported these measures.
Currently, there is no established standard for assessing the likelihood of publication bias in research on prognostic models. In addition, publication bias could also not be assessed due to the low number of included papers reporting on a particular biomarker. However, many studies in this research field have measured biomarkers and collected the items of the RCRI and/or other prediction models, but have not published results on their predictive performance.
Applicability of findings to clinical practice and policy
In more than half of the included articles, the outcome of interest was MACE. The definition of MACE, however, varied greatly: we found 80 different definitions. One reason for this heterogeneity could be the fact that many studies included, for example, atrial fibrillation or myocardial ischaemia (or myocardial injury after noncardiac surgery (MINS)) in the MACE definition, whereas others did not. As the incidence of these outcomes is much higher than the occurrence of a myocardial infarction (MI) or (fatal) cardiac arrest, comparison of these studies is complicated, which could explain the reported model calibration inconsistencies of the RCRI or extended RCRI across studies. In addition, some studies added the occurrence of stroke and/or pulmonary embolism as components of MACE. Hence, the aetiology of such complications is, in essence, different from the aetiology of cardiac complications such as myocardial infarction. Recently, guidance on standardised definitions of cardiovascular endpoints has come out as part of the 'Standardized Endpoint for Perioperative Medicine' (StEP) initiative (Beattie 2020; Myles 2016). In this guidance paper, MACE was described as a composite outcome including cardiac death, myocardial infarction, nonfatal cardiac arrest and coronary revascularisation within 30 days of the index surgery. Cardiac death is defined as death with a vascular cause and included those deaths after a myocardial infarction, nonfatal cardiac arrest and cardiac revascularisation procedure. Myocardial infarction is defined in accordance with the fourth universal definition of myocardial infarction. Cardiac arrest is defined as successful resuscitation from either documented or presumed ventricular fibrillation, sustained ventricular tachycardia, asystole or pulseless electrical activity requiring cardiopulmonary resuscitation, pharmacological therapy or cardiac defibrillation. Finally, coronary revascularisation is defined as percutaneous coronary intervention or coronary artery bypass graft surgery within 30 days of the index surgery (Beattie 2020). Unfortunately, none of the included studies used MACE as defined in the StEP guidance paper. Adherence to guidelines, such as StEP but also such as reporting guidelines for prediction model papers (TRIPOD), is recommended when designing new studies to enhance comparability between studies, enhance meta‐analysis of multiple studies and thus improve the generalisability of study and review results to a broader patient population (Beattie 2020; Collins 2015; Moons 2015). In addition, studies should consider calibration and clinical utility measures to assess its impact on clinical practice (Collins 2015; Moons 2015).
Furthermore, the original RCRI development paper based the diagnosis of MI on serial CK/CK‐MB measurements, while (high‐sensitivity) troponin measurements are currently used (Lee 1999). As troponin assays are more sensitive, more MIs are detected resulting in a higher incidence of MI compared to the data used to develop the RCRI model. This could lead to substantial miscalibration in the more recent validation studies, resulting in underestimation of risk by the RCRI. Therefore, the Canadian Cardiovascular Society updated the RCRI risk estimates based on external validation studies that were published in the past 15 years, systematically monitored perioperative troponin measurements and reported event rates for the various RCRI scores (Duceppe 2017).
Besides the variety in predicted outcomes, we identified a large amount of different biomarkers and other prediction models added or compared to the RCRI. Most biomarkers and prediction models that were added or compared to the RCRI were only studied once, meaning that selecting promising predictors from the existing literature is currently not possible. The focus of the current studies in the literature was mainly on the (incremental) predictive accuracy of cardiac biomarkers such as NT‐proBNP or high‐sensitivity troponins, however the superiority of other biomarker(s) cannot be ruled out as the available evidence is currently not sufficient. Extra complexity in the comparison of different studies arises when biomarkers are studied on a different scale (i.e. continuous, categorical or dichotomous) or using different thresholds. Imaging biomarkers might in turn be exposed to the subjective interpretation of the assessor.
In addition, we found 51 articles that compared the predictive performance of a single biomarker to the RCRI. However, treatment decisions are normally based on information from multiple predictors and, therefore, making predictions based on a single biomarker is less relevant (Moons 1999; Moons 2009; Riley 2019). Subsequently, demonstrating incremental value in model performance by adding a certain biomarker to the RCRI is more challenging than comparing the RCRI model to a single biomarker. Due to the substantial miscalibration and the explained variance of the RCRI model itself, improvement of predictive performance by the addition of a biomarker may be harder than assessing the predictive performance of a single biomarker, which may be optimally modelled in the dataset under investigation (Moons 2015; Riley 2019; Steyerberg 2009).
The RCRI has been externally validated in numerous and therefore very heterogeneous patient populations, ranging from a broad variety of noncardiac surgical procedures to specific surgical procedures such as posterior lumbar decompressions or kidney transplants. Furthermore, populations with specific characteristics (e.g. patients with a history of ischaemic heart disease or known atrial fibrillation) have been studied. The RCRI has only moderate predictive performance in vascular surgery patients, probably due to the presence of its items in high‐risk patients (Ford 2010). This implies that the predictive performance of prediction models could vary in different populations, which should be taken into account when implementing such models in clinical practice.
Agreements and disagreements with other studies or reviews
To our knowledge, this is the first systematic review that provides a comprehensive overview of all biomarkers and prediction models that have been added or compared to the RCRI to improve risk prediction in patients undergoing noncardiac surgery. However, there is one individual patient data meta‐analysis including data from six studies comparing the predictive performance of BNP to the RCRI in vascular surgical patients (Rodseth 2011). They found higher c‐statistics for BNP compared to the RCRI (0.62, 95% CI 0.55 to 0.69 and 0.81, 95% CI 0.75 to 0.86). However, the authors attribute this difference to the fact that the RCRI was derived from a population of predominantly noncardiac and nonvascular surgery patients. Therefore, they recommended that further research should be undertaken to determine whether the RCRI improves pre‐operative risk stratification in patients primarily risk stratified using BNP (Rodseth 2011). In addition, the findings from this review are in line with international guidelines on cardiac risk assessment in patients undergoing noncardiac surgery, that recommend considering (NT‐pro)BNP and troponin for further preoperative risk stratification in high‐risk patients (Duceppe 2017; Kristensen 2014).
Authors' conclusions
Implications for practice
A large number of studies have externally validated the Revised Cardiac Risk Index (RCRI) with the aim of improving its predictive performance by adding biomarkers or by comparing its predictive accuracy to biomarkers or other prediction models. The studies included in this review suggest that the predictive performance of the RCRI in predicting major adverse cardiac events (MACE) is improved when N‐terminal pro‐B type natriuretic peptide (NT‐proBNP), troponin, or the combination of both, are added. Furthermore, other studies included in this review have indicated that BNP and NT‐proBNP, when used in isolation, may even have a higher discriminative performance than the RCRI. There was insufficient evidence of a difference between the predictive accuracy of the RCRI and other prediction models in predicting MACE. However, the ACS‐NSQIP‐MICA and ACS‐NSQIP surgical risk scores outperformed the RCRI in predicting myocardial infarction and cardiac arrest, and all‐cause mortality, respectively. Nevertheless, the results cannot be interpreted as conclusive due to high risk of bias in a majority of the studies. We also deemed pooling to be impossible due to heterogeneity in outcomes, prediction horizons, biomarkers and studied populations. Furthermore, we scored risk of bias and concern regarding applicability as high in the majority of studies and reporting of predictive performance measures was poor, particularly on calibration measures.
Implications for research
Future research on the added prognostic value of biomarkers to existing prediction models for the preoperative prediction of in‐hospital adverse outcomes of patients undergoing noncardiac surgery should focus on biomarkers that demonstrated good predictive accuracy (i.e. diagnosis of myocardial infarction or heart failure) to assess their predictive value in the perioperative setting. In addition, research using omics data could be useful to identify new biomarkers for this purpose. Such new biomarkers should be compared to novel biomarkers with so far insufficient evidence compared to established ones such as NT‐proBNP or troponins. Adherence to recent guidance for prediction studies is recommended, such as TRIPOD and PROBAST, and the use of standardised outcome definitions (StEP) is highly recommended to improve generalisability and comparability between studies. This would facilitate individual patient data meta‐analyses, as well as comparison of different prediction models to the RCRI. Besides the identification of patients at risk of adverse outcomes by the use of the RCRI or other prediction models, future studies should also focus on prophylactic measures to optimise high‐risk patients in order to prevent such postoperative adverse outcomes.
History
Protocol first published: Issue 10, 2018
Acknowledgements
This project was supported by the NIHR via Cochrane Infrastructure funding to the Heart Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care. The background and methods section of this review is based on a standard template provided by Cochrane Heart.
The authors thank Nicole Martin (Managing Editor, Cochrane Heart), Andrea Takeda (Systematic Review Specialist, Cochrane Heart), Charlene Bridges (Information Specialist, Cochrane Heart) and Adrian Hernandez (Contact Editor, Cochrane Heart) for their assistance regarding the review. We would like to acknowledge René Spijker (Information Specialist, Cochrane Netherlands) for his valuable input in setting up the search strategies for this review. We are grateful to the following peer reviewers for their time and valuable input: Jan Larmann (Department of Anesthesiology, Heidelberg University Hospital, Heidelberg, Germany), Lotty Hooft (Cochrane Netherlands, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands) and one reviewer who wishes to remain anonymous.
Appendices
Appendix 1. MEDLINE Ovid search strategy
1 ("Revised Cardiac risk index" or RCRI or "Lee index" or "Lee‐index" or "Lee's index" or "revised goldman index" or goldman or detsky or LCRI or RCI or "revised cardiac index" or "pre‐operative variable*" or "preoperative variable*" or "revised cardiac risk" or "cardiac risk factor*").ti,ab,kf.
2 Reproducibility of Results/ or calibration/ or Area Under Curve/ or Validation Studies.pt. or (validat* or stratification or overfit* or overpredict* or underfit* or underpredict* or overestimation or underestimation or pooled or recalibration or re‐calibration or calibration or discrimination or cohort or discriminate or c‐statistic* or "c statistic*" or "Area under the curve*" or AUC or Indices or Algorithm or Multivariable or "added value" or incremental or "receiver operating curve" or roc or "receiver operating characteristic" or "c index" or "c‐index" or "predictive accuracy" or "prognostic accuracy" or "reclassifi*" or "prognostic value" or "predictive value" or MACE).ti,ab,kf.
3 1 and 2
4 (exp animals/ not humans/) or (equine or cattle or bovine or canine or mice or mouse or rat or rats or guinea‐pig* or dog).ti.
5 3 not 4
Appendix 2. Ovid Embase search strategy
1 ("Revised Cardiac risk index" or RCRI or "Lee index" or "Lee‐index" or "Lee's index" or "revised goldman index" or goldman or detsky or LCRI or RCI or "revised cardiac index" or "pre‐operative variable*" or "preoperative variable*" or "revised cardiac risk" or "cardiac risk factor*").ti,ab,kw.
2 reproducibility/ or validation study/ or validation process/ or calibration/ or area under the curve/ or (validat* or stratification or overfit* or overpredict* or underfit* or underpredict* or overestimation or underestimation or pooled or recalibration or re‐calibration or calibration or discrimination or cohort or discriminate or c‐statistic* or "c statistic*" or "Area under the curve*" or AUC or Indices or Algorithm or Multivariable or "added value" or incremental or "receiver operating curve" or roc or "receiver operating characteristic" or "c index" or "c‐index" or "predictive accuracy" or "prognostic accuracy" or "reclassifi*" or "prognostic value" or "predictive value" or MACE).ti,ab,kw.
3 1 and 2
4 ((exp experimental organism/ or animal tissue/ or animal cell/ or exp animal disease/ or exp carnivore disease/ or exp bird/ or exp experimental animal welfare/ or exp animal husbandry/ or animal behavior/ or exp animal cell culture/ or exp mammalian disease/ or exp mammal/ or exp marine species/ or nonhuman/ or animal.hw.) not human/) or (equine or cattle or bovine or canine or mice or mouse or rat or rats or guinea‐pig* or dog).ti.
5 3 not 4
6 limit 5 to (conference abstract or conference paper or "conference review")
7 5 not 6
Appendix 3. ClinicalTrials.gov and World Health Organization International Clinical Trials Registry platform (WHO‐ICTRP) search strategy up to 27 July 2020
Clinicaltrials.gov
Advanced search
Condition or disease:
Other terms: RCRI OR revised cardiac risk index
Study type: all studies
Study results: all studies
WHO‐ICTRP
RCRI OR revised cardiac risk index
Appendix 4. Data extraction form
| General items | |
| Author | |
| Year | |
| Journal | |
| Study ID | |
| Validation ID | Example: if 1 study reports results using multiple outcomes, the first extraction (MACE) receives number studynumber‐1 and the second (mortality) studynumber‐2 |
| Reviewer | |
| Validation details | If there are multiple outcomes, a single outcome per column. E.g. if both results for mortality and MACE are reported, extract data in two columns (i.e. one per outcome) |
| Type of study | Predesigned validation study: study is prospectively designed with the aim to validate the model |
| Was data collection prospective or retrospective? | |
| Participant selection | |
| Study design | |
| Comment on study design | |
| In‐ and exclusion criteria for the analyses | |
| Lower age limit | Enter number |
| Surgical specialty | Only information on eligibility criteria for surgical specialty |
| Surgical procedure if specified | Specify only when a particular surgical procedure is performed within a surgical specialty. E.g. some studies might only report patients undergoing AAA repair and not include patients undergoing other vascular procedures |
| Emergency surgery | Only information on eligibility criteria for emergency surgery |
| Other specific patient characteristics | e.g. patients undergoing vascular surgery with COPD and heart failure |
| Eligibility criteria for participants comparable to RCRI | ≥ 50 years, non‐emergent and non‐cardiac procedures |
| Case mix | For continuous variables: if reported extract mean and SD (other information is not needed), if these are not reported, extract median and IQR. If these are not reported specify any other information that is reported (e.g. a plot). |
| Is case mix solely reported for 2 separate groups (e.g. for cases and non‐cases)? | If yes, extract numbers at the bottom of this DE table. |
| If yes, specify which table. | |
| Age >70 years | % |
| Age | Mean |
| SD | |
| Median | |
| IQR ‐ 25th percentile | |
| IQR ‐ 75th percentile | |
| If NR: other (specify) | |
| Gender | % men |
| Type of procedure ‐ thoracic | % |
| Type of procedure ‐ orthopaedic | % |
| Type of procedure ‐ vascular | % |
| Type of procedure ‐ general/abdominal | % |
| Type of procedure ‐ gynaecological/urological | |
| Type of procedure ‐ other | % |
| High‐risk procedure | %, more information tab High‐risk surgical procedures |
| Similar definition used as in RCRI (intraperitoneal, intrathoracic or suprainguinal vascular procedures) | |
| If no, which definition has been used? | |
| Diabetes | % |
| Insulin dependent diabetes | % |
| History of ischaemic heart disease | % |
| History of myocardial infarction | % ‐ part of definition of ischaemic heart disease |
| Patients with prior CABG or PTCA | % ‐ part of definition of ischaemic heart disease |
| History of congestive heart failure | % |
| History of cerebrovascular disease | % both TIA and CVA |
| Serum creatinine > 2.0 mg/dL or > 177 µmol/L | % |
| Continue creatinine if no threshold reported | report mean (SD) |
| Renal insufficiency | % |
| Hypertension | % |
| Chronic medication use – beta blockers | % more information tab ‐ Medication |
| Chronic medication use ‐ calcium antagonists | % more information tab ‐ Medication |
| Chronic medication use ‐ diuretics | % more information tab ‐ Medication |
| Chronic medication use ‐ ACE of ARB | % more information tab ‐ Medication |
| Chronic medication use ‐ anticoagulation | % more information tab ‐ Medication |
| Chronic medication use ‐ platelet aggregation medication | % more information tab ‐ Medication |
| Chronic medication use ‐ nitrates | % more information tab ‐ Medication |
| Chronic medication use – anti‐hypertensives | %, report only if not specified in detail |
| Chronic medication use ‐ cardiac medication | %, report only if not specified in detail |
| Smoking | % Never |
| % Past | |
| % Current | |
| % Ever | |
| % not specified/other (specify) | |
| Atrial fibrillation | % |
| RCRI | Mean |
| SD | |
| Median | |
| IQR ‐ 25th percentile | |
| IQR ‐ 75th percentile | |
| RCRI 0 factor | % |
| RCRI 1 factor | % |
| RCRI 2 factor | % |
| RCRI 3 factor | % |
| RCRI 4 factor | % |
| RCRI 5 factor | % |
| RCRI 3 or more | % |
| RCRI ‐ other information/classification | |
| Study dates | |
| Start date recruitment period (dd‐mm‐yyyy) | If day is not reported enter 00. So July 2010 is 00‐07‐2010 |
| End date recruitment period (dd‐mm‐yyyy) | |
| End date of follow up (dd‐mm‐yyyy) | |
| Follow‐up time ‐ median (days) | |
| Follow‐up time ‐ range (days) min | |
| Follow‐up time ‐ range (days) max | |
| Follow‐up time ‐ mean (days) | |
| Prediction horizon ‐ category | In‐hospital events/30‐day/1‐year/other |
| Follow‐up time ‐ other information (specify) | |
| Location | |
| Number of centres | |
| Location of centres ‐ continent | |
| Location of centres ‐ country | |
| Data collection in academic or peripheral hospital? | |
| Risk of Bias ‐ Participant selection | Be strict on signalling questions, but less strict on risk of bias. If there is no information, answer 'No information' to the signalling question, but you might score Low risk of bias, if you think it didn't cause bias. |
| 1. Were appropriate data sources used, e.g. cohort, RCT or nested case‐control study data? | YES: Cohort, RCT, Case cohort, nested case‐control PROBABLY YES registry or existing cohort studies. In case RCT data is used and treatment is accounted for, score Yes. NO: case‐control, cross‐sectional Consider scoring NO if data collection was not intended for research purposes. |
| 2. Were all inclusions and exclusions based on characteristics of participants appropriate (e.g. comorbidities, treatment)? | The key issue is whether any inclusion or exclusion criteria, or the recruitment strategy, could have made the included study participants unrepresentative of the intended target population, e.g. selection of participants was based on the outcome at time of predictor measurement or specific subgroups are excluded that may alter the performance of the prediction model. This item is NOT on loss to follow‐up or missing data, but rather on eligibility criteria and exclusions made before entrance in the cohort used for the validation. This is really about the people that were selected for the analyses (although, exclusion of people with missing data should be scored below in 'sample size and participant flow'). |
| Risk of bias introduced by selection of participants | |
| Justification of bias rating | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Applicability | |
| 1. Were participants enrolled at a similar state of health compared to the development population? | |
| Concern that the included participants and setting do not match the review question | Studies might have reduced applicability to our review if they included a study population different from the original development study, e.g. if they included only young people, or a more diseased population with 50% diabetes or cancer (see separate file). |
| Justification of applicability rating | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Predictors | |
| Actions to blind assessment of predictors for the outcome | |
| Actions to blind assessment of predictors for each other | |
| Was there a general statement that predictor definitions were the same as in the development study? If not, answer the following question for every predictor. | |
| For the following predictors: was the same definition used? If not, copy the definition in the box below. (if the same definition is used, you don't have to copy it) | |
| High‐risk surgery intraperitoneal, intrathoracic, or suprainguinal vascular procedures | Yes/No/NR/NA Score NA if predictor was not included in the model |
| Definition | |
| Ischaemic heart disease history of myocardial infarction, positive exercise test, current complaint of ischaemic chest pain or use of nitrate therapy, or ECG with pathological Q waves. Patients with previous revascularisation (i.e. CABG or PCI or PTCA) were included in this definition only if they had current chest pain | Yes/No/NR/NA Score NA if predictor was not included in the model. |
| Definition | |
| History of congestive heart failure history of congestive heart failure, pulmonary oedema or paroxysmal nocturnal dyspnoea, physical examination showing bilateral rales or S3 gallop or chest radiograph showing pulmonary vascular redistribution | Yes/No/NR/NA Score NA if predictor was not included in the model. |
| Definition | |
| History of cerebrovascular disease history of transient ischaemic attack or stroke | Yes/No/NR/NA Score NA if predictor was not included in the model. |
| Definition | |
| Insulin therapy for the treatment of diabetes | Yes/No/NR/NA Score NA if predictor was not included in the model |
| Definition | |
| Preoperative creatinine > 2.0 mg/dl or > 177 µmol/L | Yes/No/NR/NA Score NA if predictor was not included in the model |
| Definition | |
| Were predictors deleted? | |
| If yes, which ones? | |
| Was the number of predictors or the individual predictors used for validation of the model? | |
| For each biomarkers that was added to the RCRI | |
| Which biomarker was added to the RCRI? | |
| How was the biomarker derived? | Blood derived/imaging/patient characteristic/prediction model/other |
| How was the biomarker added to the model? | Continuous/categorical/dichotomous |
| What threshold of the biomarker was used to define elevation? | Only insert the number, for patient characteristic use NA, if not reported use NR |
| Entity of the threshold | |
| Which assay/device was used? | |
| For each biomarkers that was compared to the RCRI | |
| Which biomarker alone was compared to the RCRI? | |
| How was the biomarker derived? | Blood derived/imaging/patient characteristic/prediction model/other |
| How was the biomarker added to the model? | Continuous/categorical/dichotomous |
| What threshold of the biomarker was used to define elevation? | Only insert the number, for patient characteristic use NA, if not reported use NR |
| Entity of the threshold | |
| Which assay/device was used? | |
| Risk of Bias ‐ predictors | Be strict on signalling questions, but less strict on risk of bias. If there is no information, answer 'No information' to the signalling question, but you might score Low risk of bias, if you think it didn't cause bias. |
| 1. Were predictors defined and assessed in a similar way for all participants? | |
| 2. Were predictor assessments made without knowledge of outcome data? | |
| 3a. Are all predictors available at the time the model is used? | Score No if it is stated that not all predictors were measured at baseline, or if not all predictors were available. |
| 3b. Were predictors defined and assessed in the same way as in the original RCRI model? | Score Yes if it is stated that the same definitions were used. Score No if there is at least one definition different. |
| Risk of bias introduced by predictors or their assessment | |
| Justification of bias rating: | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Applicability | |
| Concern that the definition, assessment or timing of assessment of predictors in the model do not match the review question | |
| Justification of applicability rating | Justification is not always necessary when you score LOW (although it might be helpful), but ís necessary when you score HIGH or UNCLEAR. |
| Outcome | |
| Is the outcome definition the same as the development study? RCRI: major cardiac complications This composite outcome included myocardial infarction, pulmonary oedema, ventricular fibrillation or primary cardiac arrest, and complete heart block. Myocardial infarction was diagnosed if CK‐MB was > 5% of an elevated total CK or the peak CK‐MB was > 3% of an elevated total CK in the presence of ECG changes consistent with ischaemia or infarction. Diagnosis of pulmonary oedema required a formal reading of a chest radiograph by a radiologist | |
| Outcome ‐ main category | MACE/cardiovascular mortality/all‐cause mortality/myocardial infarction/myocardial injury (troponin elevation)/Other |
| Outcome ‐ full definition | Copy/paste information |
| Outcome ‐ full definition ‐ other information | |
| Outcome ‐ measurement method | E.g. expert panel, death register |
| If a composite outcome was used, enter the relative or absolute frequency/distribution of each contributing outcome | Format: outcome number, outcome number. E.g. MI 250, stroke 302 |
| Actions to blind outcome assessment for the predictors | |
| Risk of bias ‐ Outcome | Be strict on signalling questions, but less strict on risk of bias. If there is no information, answer 'No information' to the signalling question, but you might score Low risk of bias, if you think it didn't cause bias. |
| 1. Was the outcome determined appropriately? | |
| 2. Was a prespecified or standard outcome definition used? | |
| 3. Were predictors excluded from the outcome definition? | |
| 3. Was the outcome defined and determined in a similar way for all participants? | Score Yes if it was stated that patients were diagnosed using a panel diagnosis. |
| 4. Was the outcome determined without knowledge of predictor information? | |
| 5. Was the time interval between predictor assessment and outcome determination appropriate? | |
| Risk of bias introduced by the outcome or its determination | You might score HIGH if outcomes were self‐reported. |
| Justification of bias rating | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Applicability | |
| Concern that the definition, assessment or timing of assessment of the outcome in the model does not match the review question | |
| Justification of applicability rating | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Sample size and participant flow | |
| Number of participants included in the full cohort | Enter number |
| Number of events in the full cohort | Enter number |
| Number of participants included in the analysis | Enter number |
| Number of events included in the analysis | Enter number |
| Missing data | |
| Number of participants with any missing value | Enter number |
| Number of participants with missing data for outcome | Enter number |
| Number of participants with missing data for predictors | Enter number |
| Method used to account for missing data | |
| Type of missing data | |
| Comment on missing data | |
| Analysis | |
| How were predictors calculated | |
| Comment on calculating predictors | |
| Type of validation ‐ Investigators Is this a validation by different investigators? Is there NO overlap between the researchers of the validation study and the development study? | Score YES if there was NO overlap, score NO if there was overlap between authors. Thomas H. Lee, MD, SM; Edward R. Marcantonio, MD, SM; Carol M. Mangione, MD, SM; Eric J. Thomas, MD, SM; Carisi A. Polanczyk, MD; E. Francis Cook, ScD; David J. Sugarbaker, MD; Magruder C. Donaldson, MD; Robert Poss, MD; Kalon K.L. Ho, MD, SM; Lynn E. Ludwig, MS, RN; Alex Pedan, PhD; Lee Goldman, MD, MPH |
| Risk of bias ‐ analysis | Be strict on signalling questions, but less strict on risk of bias. If there is no information, answer 'No information' to the signalling question, but you might score Low risk of bias, if you think it didn't cause bias. |
| 1. Were there a reasonable number of outcome events? | Yes: >=100 (ref: Vergouwe) |
| 2. Were continuous and categorical predictors handled appropriately? | |
| 3. Were all enrolled participants included in the analysis? | This question is on exclusions made after study entrance (e.g. participants with missing data were excluded, or people with short follow‐up time were excluded), so not on eligibility criteria. Score YES if all enrolled participants were included in the analysis. |
| 4. Were participants with missing data handled appropriately? | Yes: probabilistic imputation approach such as multiple imputation, or explicit mentioning of no missing data. Probably yes: single imputation Probably no: no information on missing data reported anywhere in the paper No: deterministic (e.g. mean) imputation, complete case analysis |
| 5. Was selection of predictors based on univariable analysis avoided? | This is for development studies only. |
| 6. Were any complexities in the data (e.g. censoring, competing risks) accounted for appropriately? | Score No if it was a multicentre study and this was not taken into account, or if it was a case‐cohort/nested case‐control study and this was not taken into account. Score Probably yes if you have no reason to believe there were any complexities in the data. |
| 7. Were relevant model performance measures evaluated appropriately? | |
| 8. Were model overfitting, underfitting, and optimism in model performance accounted for? | For development studies only A model extension, where new predictors are added to an existing model, would be assessed as new model development. |
| 9. Do predictors and their assigned weights in the final model correspond to the results from the reported multivariable analysis? | For development studies only A model extension, where new predictors are added to an existing model, would be assessed as new model development. |
| Risk of bias introduced by the analysis | If it was a multicentre study and this was not taken into account you might score Low if there was protocolised data collection. |
| Justification of bias rating | Justification is not always necessary when you score LOW (although it might be helpful), but is necessary when you score HIGH or UNCLEAR. |
| Results | |
| Performance RCRI alone | |
| C‐statistic ‐ type | |
| C‐statistic | |
| C‐statistic ‐ 95% CI Lower bound | |
| C‐statistic ‐ 95% CI Upper bound | |
| C‐statistic ‐ SE | |
| C‐statistic ‐ P value | Report only if confidence interval and/or SE is not reported |
| C‐statistic ‐ other information | Specify |
| Observed rate | % |
| Observed rate ‐ 95% CI Lower bound | |
| Observed rate ‐ 95% CI Upper bound | |
| Expected rate | % |
| Expected rate ‐ 95% CI Lower bound | |
| Expected rate ‐ 95% CI Upper bound | |
| Observed/expected | |
| Observed/expected ‐ 95% CI Lower bound | |
| Observed/expected ‐ 95% CI Upper bound | |
| Observed/expected ‐ SE | |
| Observed/expected ‐ P value | |
| Observed/expected ‐ IQR Lower bound | |
| Observed/expected ‐ IQR Upper bound | |
| Expected/observed | |
| Expected/observed ‐ 95% CI Lower bound | |
| Expected/observed ‐ 95% CI Upper bound | |
| Expected/observed ‐ SE | |
| Expected/observed ‐ P value | |
| Expected/observed ‐ IQR Lower bound | |
| Expected/observed ‐ IQR Upper bound | |
| Calibration plot ‐ calibration table is available | If yes, mention which table in the article |
| Sensitivity | % |
| Specificity | % |
| Negative predictive value | % |
| Positive predictive value | % |
| In case sensitivity, specificity, negative predictive value or positive predictive value is reported, what threshold is used? | |
| Hosmere Lemeshow X2 | |
| Hosmere Lemeshow X2 ‐ P value | |
| Calibration ‐ other | |
| Performance after updating ‐ addition for each biomarker | |
| Which biomarker(s) is (are) added? | In case, multiple biomarkers are added at once, name all biomarkers |
| C‐statistic ‐ type | |
| C‐statistic | |
| C‐statistic ‐ 95% CI Lower bound | |
| C‐statistic ‐ 95% CI Upper bound | |
| C‐statistic ‐ SE | |
| C‐statistic ‐ P value | Report only if confidence interval and/or SE is not reported |
| C‐statistic ‐ P value difference in c‐statistic | |
| C‐statistic ‐ other information | Specify |
| Observed rate | % |
| Observed rate ‐ 95% CI Lower bound | |
| Observed rate ‐ 95% CI Upper bound | |
| Expected rate | % |
| Expected rate ‐ 95% CI Lower bound | |
| Expected rate ‐ 95% CI Upper bound | |
| Observed/expected | |
| Observed/expected ‐ 95% CI Lower bound | |
| Observed/expected ‐ 95% CI Upper bound | |
| Observed/expected ‐ SE | |
| Observed/expected ‐ P value | |
| Observed/expected ‐ IQR Lower bound | |
| Observed/expected ‐ IQR Upper bound | |
| Expected/observed | |
| Expected/observed ‐ 95% CI Lower bound | |
| Expected/observed ‐ 95% CI Upper bound | |
| Expected/observed ‐ SE | |
| Expected/observed ‐ P value | |
| Expected/observed ‐ IQR Lower bound | |
| Expected/observed ‐ IQR Upper bound | |
| Calibration plot ‐ calibration table is available | If yes, mention which table in the article |
| Sensitivity | % |
| Specificity | % |
| Negative predictive value | % |
| Positive predictive value | % |
| Accuracy | % |
| In case sensitivity, specificity, negative predictive value or positive predictive value is reported, what threshold is used? | |
| Hosmer Lemeshow X2 | |
| Hosmer Lemeshow X2 ‐ P value | |
| IDI | |
| IDI ‐ 95% CI lower bound | |
| IDI ‐ 95% CI upper bound | |
| IDI ‐ P value | Report only if confidence interval and/or SE is not reported |
| NRI ‐ cases | |
| NRI ‐ 95% CI lower bound ‐ cases | |
| NRI ‐ 95% CI upper bound ‐ cases | |
| NRI – non‐cases | |
| NRI ‐ 95% CI lower bound – non‐cases | |
| NRI ‐ 95% CI upper bound – non‐cases | |
| NRI ‐ total | |
| NRI ‐ 95% CI lower bound ‐ total | |
| NRI ‐ 95% CI upper bound ‐ total | |
| NRI ‐ category‐free or thresholds | Category free NRI or thresholds were used? |
| NRI ‐ if thresholds, which thresholds were used? | |
| NRI ‐ table available with thresholds | If yes, mention which table in the article |
| NRI ‐ other information | |
| Performance after updating ‐ for each biomarker that is compared to the RCRI | |
| Which biomarker(s) is (are) compared to RCRI? | In case, multiple biomarkers are added at once, name all biomarkers |
| C‐statistic ‐ type | |
| C‐statistic | |
| C‐statistic ‐ 95% CI Lower bound | |
| C‐statistic ‐ 95% CI Upper bound | |
| C‐statistic ‐ SE | |
| C‐statistic ‐ P value | Report only if confidence interval and/or SE is not reported |
| C‐statistic ‐ P value difference in c‐statistic | |
| C‐statistic ‐ other information | Specify |
| Observed rate | % |
| Observed rate ‐ 95% CI Lower bound | |
| Observed rate ‐ 95% CI Upper bound | |
| Expected rate | % |
| Expected rate ‐ 95% CI Lower bound | |
| Expected rate ‐ 95% CI Upper bound | |
| Observed/expected | |
| Observed/expected ‐ 95% CI Lower bound | |
| Observed/expected ‐ 95% CI Upper bound | |
| Observed/expected ‐ SE | |
| Observed/expected ‐ P value | |
| Observed/expected ‐ IQR Lower bound | |
| Observed/expected ‐ IQR Upper bound | |
| Expected/observed | |
| Expected/observed ‐ 95% CI Lower bound | |
| Expected/observed ‐ 95% CI Upper bound | |
| Expected/observed ‐ SE | |
| Expected/observed ‐ P value | |
| Expected/observed ‐ IQR Lower bound | |
| Expected/observed ‐ IQR Upper bound | |
| Calibration plot ‐ calibration table is available | If yes, mention which table in the article |
| Sensitivity | % |
| Specificity | % |
| Negative predictive value | % |
| Positive predictive value | % |
| Accuracy | % |
| In case sensitivity, specificity, negative predictive value or positive predictive value is reported, what threshold is used? | |
| Hosmer Lemeshow X2 | |
| Hosmer Lemeshow X2 ‐ P value | |
| IDI | |
| IDI ‐ 95% CI lower bound | |
| IDI ‐ 95% CI upper bound | |
| IDI ‐ P value | Report only if confidence interval and/or SE is not reported |
| NRI ‐ cases | |
| NRI ‐ 95% CI lower bound ‐ cases | |
| NRI ‐ 95% CI upper bound ‐ cases | |
| NRI – non‐cases | |
| NRI ‐ 95% CI lower bound – non‐cases | |
| NRI ‐ 95% CI upper bound – non‐cases | |
| NRI ‐ total | |
| NRI ‐ 95% CI lower bound ‐ total | |
| NRI ‐ 95% CI upper bound ‐ total | |
| NRI ‐ category‐free or thresholds | Category free NRI or thresholds were used? |
| NRI ‐ if thresholds, which thresholds were used? | |
| NRI ‐ table available with thresholds | If yes, mention which table in the article |
| NRI ‐ other information | |
| Addition information | |
| Additional information regarding conflict of interest | E.g. funding of biomarker assay manufacturers |
| Comments | |
| Extra baseline table when characteristics are not reported for the whole population. Baseline characteristics for cases and non‐cases were collected separately similar to the baseline characteristics previously reported in this data extraction form | |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Adar 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular accidents
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Aortic arch calcification
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Only orthopaedic patients were included and patients with malignancy and previous cardiac surgery were excluded. In addition, patients from 18 years onwards were eligible. Domain 2: Predictors
Justification: No information on the definition of the individual RCRI predictor definitions. Domain 3: Outcome
Justification: Although outcome is MACE, it also includes stroke, atrial fibrillation and unstable angina pectoris. Overall judgement
Justification: Only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | ||
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing orthopaedic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on the definition of the individual RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and no information on handling missing data. |
| Overall judgement | No | Low number of outcomes and no information on handling missing data and no information on the definition of the individual RCRI predictor definitions. However, patient selection was appropriate and outcome definitions were clearly defined and assessed. |
Ahn 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular accidents
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Coronary artery calcium scores (CACS)
Predictor 2: Multi‐vessel disease
Predictor 3: Coronary artery calcium scores (CACS) + multi‐vessel disease
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Domain 2: Predictors
Domain 3: Outcome
Overall judgement:
Patient selection was appropriate; predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients with severe cardiac morbidities such as previous myocardial infarction, severe heart failure or severe valvular disease were excluded from the analysis. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Small number of outcomes. No information on how missing data were handled. |
| Overall judgement | No | Patients with severe cardiac morbidities were excluded from the analysis. In addition, there was a small number of outcomes and no information on handling of missing data. However, predictor and outcome definitions were clearly reported and assessed. |
Ahn 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular accidents
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Dobutamine stress test
Predictor 2: Coronary artery stenosis
Predictor 3: Coronary artery calcium scores
Predictor 4: Coronary artery calcium scores + significant coronary artery stenosis ≥ 50%
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Patients with at least 1 RCRI factor were included, patients were excluded if they had active cardiac conditions including recent MI, decompensated heart failure, more than moderate valvular heart disease and significant arrhythmia. Domain 2: Predictors
Justification: No information on the definition of the individual RCRI predictor definitions. Domain 3: Outcome
Justification: MACE includes MINS and pulmonary embolism and stroke Overall judgement
Justification: Only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 2: Predictors | Unclear | No information on the definition of the individual RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Small number of outcomes. No information on how missing data were handled. |
| Overall judgement | No | No information on the definition of the individual RCRI predictor definitions. In addition, the number of outcomes was low and there was no information on handling missing data. However, patient selection was appropriate and outcomes were clearly defined and assessed. |
Alrezk 2017.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular accidents
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: GSCRI Objective: Prediction model compared
Predictor 2: ACS‐NSQIP‐MICA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Not applicable Domain 2: Predictors
Justification: Not applicable Domain 3: Outcome
Justification: Outcome is different from MACE in the development study Overall judgement
Justification: Patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Yes | Appropriate patient selection and number of outcomes, clear predictor and outcome definitions and study methodology. |
Archan 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Age Objective: biomarker compared
Predictor 2: Glasgow Aneurysm Risk score (GAS)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not applicable Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: Outcome is different from MACE in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Other (more advanced) performance measures could have been calculated and reported including confidence intervals and/or standard error; low number of outcomes. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, the number of outcomes was low and other performance measures should have been calculated with confidence intervals and/or standard error. |
Asuzu 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Weighted RCRI score
Predictor 2: ASC‐NSQIP‐MICA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients were eligible if they underwent a single procedure, were > 18 years and had a lower incidence of comorbidities Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: outcome does not match outcome of the development study Overall judgement
Justification: only a selected group of patients was used. Predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing general surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Patients with missing data were excluded from the analyses (> 50%), however they did provide the right performance measures. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, handling of missing data was inappropriate as > 50% of patients were excluded from the analysis. |
Avena 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Vascular study group of New England cardiac risk index (VSG‐CRI) Objective: prediction model compared
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: included patients have very high incidence of comorbidities Domain 2: Predictors
Justification: no information on predictor definitions Domain 3: Outcome
Justification: outcome does not match outcome of the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on predictor definitions |
| Domain 3: Outcome | Unclear | No standardised definition of composite outcomes; no information how outcomes were assessed. |
| Domain 4: Analysis | No | Low number of outcomes; no estimate reported; no handling of missing data. |
| Overall judgement | No | Patient selection was appropriate. However, predictors and outcomes definitions were unclear. In addition, the number of outcomes was low, no performance measures were reported and no information on handling of missing data. |
Bae 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Fragmented QRS complex (fQRS)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients underwent noncardiac vascular surgery and no information is reported on baseline characteristics of included patients Domain 2: Predictors
Justification: no information was provided how the items of the RCRI were interpreted and defined Domain 3: Outcome
Justification: outcome does not match outcome of the development study Overall judgement
Justification: no information on baseline characteristics of included patients was reported. There was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information was provided how the items of the RCRI were interpreted and defined. |
| Domain 3: Outcome | Unclear | No information on how the SPECT images were assessed and how the outcome was determined based on the SPECT. |
| Domain 4: Analysis | No | Low number of outcomes and no information on the handling of missing data. |
| Overall judgement | No | Patient selection was appropriate. However, predictors and outcomes definitions were unclear. In addition, the number of outcomes was low and no information on handling of missing data. |
Bae 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Fragmented QRS complex (fQRS)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients underwent vascular surgery and underwent SPECT before being considered for inclusion Domain 2: Predictors
Justification: for some items, no information on the definition was provided. High‐risk surgery was not inserted into the RCRI and the definition of diabetes was different compared to the development paper Domain 3: Outcome
Justification: outcome does not match outcome of the development study Overall judgement
Justification: patient selection was appropriate. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. Furthermore, outcome definition was different compared to the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | No | For some items, no information on the definition was provided. High‐risk surgery was not inserted into the RCRI and the definition of diabetes was different compared to the development paper. |
| Domain 3: Outcome | Unclear | No information how the outcomes were assessed and if the assessors were blinded for predictor values. |
| Domain 4: Analysis | No | Low number of outcomes and no information on the handling of missing data. |
| Overall judgement | No | Patient selection was appropriate. However, there was no information on how outcomes were assessed. Prediction definitions were unclear or were different compared to definitions used in the RCRI development study. In addition, the number of outcomes was low, no performance measures were reported and no information on handling of missing data. |
Biccard 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: BNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients underwent vascular surgery; no age limit was provided Domain 2: Predictors
Justification: no information on the definition of the individual RCRI predictor definitions Domain 3: Outcome
Justification: outcome assessed is troponin elevation and not MACE as defined in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Post hoc decision to exclude a selective group of patients. |
| Domain 2: Predictors | Unclear | No information on the definition of the individual RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Very low number of events; calibration not assessed; limited information on discrimination. |
| Overall judgement | No | Inappropriate exclusion of a selective group of patients, predictor definitions were not reported and the number of events was low and no calibration measures were assessed. However, outcome definitions were clearly defined and assessed. |
Biccard 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: BNP or NT‐proBNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients underwent vascular surgery, no age limit was provided Domain 2: Predictors
Justification: no information on the definition of the individual RCRI predictor definitions Domain 3: Outcome
Justification: no clear definition of the outcome measure MACE Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was not clearly defined |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Unclear | Almost no information reported about participants. |
| Domain 2: Predictors | Unclear | No information on the definition of the individual RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No clear definition of the outcome measure MACE. |
| Domain 4: Analysis | No | Low number of outcomes (with no definition) and no information on the handling of missing data. |
| Overall judgement | No | There was no/limited information on participants included in the analysis, and on how predictors and outcomes were defined and assessed. In addition, the number of outcomes was low and there was no information on handling of missing data. |
Binh 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: NT‐proBNP + high creatinine (> 2 mg/L)
Predictor 3: NT‐proBNP + high creatinine (> 2 mg/L) + ischaemic heart disease
Predictor 4: NT‐proBNP + high creatinine (> 2 mg/L) + ischaemic heart disease+ congestive heart failure
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not applicable Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: not applicable Overall judgement:
Patient selection was appropriate; predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on handling missing data; only discrimination reported. |
| Overall judgement | No | Appropriate patient selection and predictors and outcomes were clearly defined. However, the number of outcome was low, there was no information on handling of missing data and only discrimination was reported as performance measure. |
Boersma 2001.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 or more RCRI factors
|
|
| Predictors | Predictor 1: Dobutamine stress echocardiography (DES) + betablocker use
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: population very different from the development study; only high‐risk patients included Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: outcome is cardiovascular death with myocardial infarction in this study and MACE in the development study Overall judgement
Justification: only high‐risk patients were included. Predictors were clearly defined. However, the outcome used was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only patients with at least one cardiac risk factor had a DSE meaning that only high‐risk patients were assessed. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and no information on handling missing data. |
| Overall judgement | No | Only high‐risk patients were included. Predictors and outcomes were clearly defined. However, the number of outcomes was low and there was no information on handling missing data. |
Boersma 2005.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Type of surgery + laparoscopic procedure + emergency surgery
Predictor 2: Type of surgery + type of surgery + laparoscopic procedure + emergency surgery + age
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients were included from 15 years onwards meaning that the percentage with comorbidities is much lower compared to development study Domain 2: Predictors
Justification: ICD codes were used as RCRI predictor definitions and high‐risk surgery was defined as retroperitoneal, intrathoracic or suprainguinal vascular procedures Domain 3: Outcome
Justification: outcome is cardiovascular death in this study and MACE in the development study Overall judgement
Justification: the inclusion criteria were broader compared to the development study. ICD codes were used as RCRI predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | ||
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | ICD codes were used as RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | However, no confidence intervals or standard error for the c‐statistics. |
| Overall judgement | No | Appropriate selection of patients and clearly defined outcomes with proper methodology. However, ICD codes were used as RCRI predictor definitions. |
Borges 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients with at least one RCRI factor were eligible for inclusion Domain 2: Predictors
Justification: definition of high‐risk surgery is according to the American College of Cardiology/American Heart Association and no definition for ischaemic heart disease and congestive heart failure was reported. Domain 3: Outcome
Justification: not applicable Overall judgement
Justification: only a selected group of patients was included. There was no/unclear information on predictor definitions or different predictor definitions were used. Outcome definition used was clearly defined and comparable to the RCRI development study outcome definition. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients with at least one RCRI factor were eligible for inclusion. |
| Domain 2: Predictors | No | Definition of high‐risk surgery is according to the American College of Cardiology/American Heart Association and no definition for ischaemic heart disease and congestive heart failure was reported. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and no information on how missing data were handled. |
| Overall judgement | No | Justification: only a selected group of patients was included. There was no/unclear information on predictor definitions or different predictor definitions were used. Outcome used was appropriate and clearly defined. However, the number of outcomes was low and there was no information on handling missing data. |
Bronheim 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient underwent posterior lumbar decompression Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: the RCRI was not developed to predict noncardiac complications Overall judgement
Justification: only a selected group of patients was included. Predictors were clearly defined. However, many (noncardiac) outcomes were assessed and therefore different compared to the outcome used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing neurosurgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Depending on the outcome, low number of outcomes. Only discrimination is reported and no other performance measures. Multiple testing issue. No information on handling missing data. |
| Overall judgement | No | Appropriate patient selection and outcomes and predictors were clearly defined. However, many outcomes were tested and there was no correction for multiple testing; only discrimination measures were reported and there was no information on handling missing data. |
Brunelli 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors Not reported |
|
| Predictors | Predictor 1: Thoracic RCRI, including serum creatinine, cerebrovascular disease, cardiac ischaemia, pneumonectomy
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: very selective group of patients included Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: not applicable
Justification: only a selected group of patients was included. However, predictors and outcomes were clearly defined and comparable as used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing thoracic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of events; no information on missing data and calibration. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Bryce 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Glasgow aneurysm score
Predictor 2: V(p)‐POSSUM score
Predictor 3: Vascular biochemical and haematological outcome model
Predictor 4: Preoperative risk score of the estimation of physiological ability and surgical stress score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: most RCRI predictor definitions not reported Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: patient selection was appropriate. However, there was no/unclear information on predictor definitions. In addition, the outcome used was different from MACE in the development study. |
|
| Notes | ||
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | Most predictor definitions not reported including RCRI definition factors. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Very low sample size; calibration not assessed. |
| Overall judgement | No | Appropriate patient selection and clearly defined outcome. However, there was no/unclear information on predictor definitions. In addition, the sample size was low and calibration was not assessed. |
Canbolat 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NSQIP surgical risk score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not sure if patients who underwent liver transplantation were involved in the original study. Domain 2: Predictors
Justification: no definition of RCRI factors was reported Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing general surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No definition of RCRI factors was reported. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Very low sample size, no information on missing data, no information on discrimination and limited information on calibration. |
| Overall judgement | No | Appropriate patient selection and clearly defined outcome. However, there was no/unclear information on predictor definitions. In addition, the sample size was low and calibration was not assessed. |
Carabini 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Age + surgical complexity
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no definition of RCRI factors were reported Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: appropriate patient selection. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing general surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on predictor definitions. |
| Domain 3: Outcome | Unclear | Time horizon is unclear; limited information on
outcome measurement. |
| Domain 4: Analysis | No | Low sample size and complete‐case analysis but only 3 patients excluded because of missing data. |
| Overall judgement | No | Appropriate patient selection. However, predictors definitions and outcome assessments were unclear. In addition, the sample size and number of outcomes was low. |
Che 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon 30‐day events |
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only participants with CAD were included Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: only a selected group of patients was included and the outcome definition was different compared to the development study. However, predictor definitions were clearly defined and comparable to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of events; 15% of participants excluded due to missing data. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, the number of outcomes was low and complete case analysis was performed. |
Cho 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Atrial fibrillation
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: MACE definition varies from definition of MACE in development cohort Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients without cardiac evaluation were excluded (approximately 80% of sample). |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | However, no information on handling missing data, only c‐statistic reported. No measures of calibration or reclassification. |
| Overall judgement | No | Only a selected group of patients were included in the analysis and no information on the handling of missing data. In addition, only discrimination was reported and no other performance measures. However, outcomes and predictors were clearly defined and assessed. |
Choi 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: CRP
Predictor 3: NT‐proBNP + CRP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients were required to have ≥ 1 cardiovascular risk factor such as hypertension, diabetes, angina, history of revascularisation, heart failure or stroke, or abnormal preoperative electrocardiography with pathological Q wave or non‐sinus rhythm. In addition patients with creatinine > 2.0 mg/dL were excluded from the analysis. Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: not applicable Overall judgement
Justification: only a selected group of patients was included. However, predictors and outcomes were clearly defined and comparable as used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Data were dichotomised for all predictors of interest; no information on the handling of missing data. No calibration or reclassification measures were reported. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, data were dichotomised, there was no information on the handling of missing data and no information on calibration and reclassification measures were reported. |
Cohn 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Reconstructed RCRI, defined as high‐risk surgery, ischaemic heart disease, congestive heart failure, cerebrovascular disease, renal insufficiency (GFR < 30) Objective: prediction model compared
Predictor 2: ACS‐NSQIP‐MICA
Predictor 3: ACS‐NSQIP surgical risk score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Eligibility criteria were not described Domain 2: Predictors
Justification: limited information on predictor definitions and measurement Domain 3: Outcome
Justification: not applicable Overall judgement
Justification: there was no information on eligibility criteria and predictor definitions. Outcome used was comparable to the outcome used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Unclear | Eligibility criteria were not described. |
| Domain 2: Predictors | Unclear | Limited information on predictor definitions and measurement. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Very low number of events; no information about missing values; calibration not assessed. |
| Overall judgement | No | No information on eligibility criteria and predictor definitions. In addition, the number of events was low, there was no information on the handling of missing values and calibration measures were not reported. However, the outcome was clearly defined and assessed. |
Cuthbertson 2007.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
2 or more RCRI factors
|
|
| Predictors | Outcome category
Full outcome definition
Prediction horizon
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not applicable Domain 2: Predictors
Justification: no information on predictor definitions Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: patient selection was appropriate. However, there was no/unclear information on predictor definitions. In addition, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | The number of events was low; there was no information on handling missing data. |
| Overall judgement | No | Appropriate patient selection and outcomes definitions were clearly defined and assessed. However, there was no/unclear information on predictor definitions, the number of outcomes was low and no information on handling of missing data was reported. |
Dakik 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: AUB‐HAS2 Cardiovascular Risk Index, which includes age > 75 years, history of heart disease, symptoms of angina or dyspnoea, haemoglobin < 12 mg/dl, vascular surgery and emergency surgery
Predictor 2: NSQIP surgical risk score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on how RCRI items were defined Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: patient selection was appropriate. However, there was no/unclear information on predictor definitions. In addition, the outcome used was different from MACE in the development study. |
|
| Notes | ||
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how RCRI items were defined. |
| Domain 3: Outcome | No | There was no routine troponin monitoring so some MIs could be missed. |
| Domain 4: Analysis | No | Low number of outcome; predictor selection for new prediction model based on significant univariable factors; only c‐statistic was reported. |
| Overall judgement | No | Patient selection was appropriate. However, predictor definition were not reported/unclear. In addition, outcomes assessment was inappropriate, the number of outcomes was low and no calibration measures were reported. |
Dakik 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: AUB‐HAS2 Cardiovascular Risk Index, which includes age > 75 years, history of heart disease, symptoms of angina or dyspnoea, haemoglobin < 12 mg/dl, vascular surgery and emergency surgery
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: also patients < 50 years are included and lower incidence of comorbidities are reported. This might be a more healthy population compared to the population of the development study. Domain 2: Predictors
Justification: no information on how RCRI items were defined Domain 3: Outcome
Justification: outcome different from the development study Overall judgement
Justification: patient selection was appropriate. However, there was no/unclear information on predictor definitions. In addition, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how RCRI items were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | No measures or calibration or reclassification were reported and no information on handling of missing data. |
| Overall judgement | No | Patient selection was appropriate and outcomes were clearly defined and assessed. However, there was no information on RCRI predictor definitions and no calibration and/or reclassification measures were reporting. |
Datema 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Age
Predictor 2: Adult comorbidity evaluation (ACE‐27)
Predictor 3: Adult comorbidity evaluation (ACE‐27) + age ≥ 70 years
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not applicable Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: not applicable Overall judgement:
Patient selection was appropriate, predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing head and neck surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and only c‐statistic reported without any confidence intervals or standard errors. |
| Overall judgement | No | Appropriate patient selection and clearly defined predictors and outcomes. However, the number of outcomes was low and no calibration was reported. |
Davis 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: RCRI without insulin‐dependent diabetes and preoperative creatinine > 2.0 mg/dL
Predictor 2: RCRI without insulin‐dependent diabetes and eGFR < 30 instead of preoperative creatinine > 2.0 mg/dL
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not applicable Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: not applicable Overall judgement:
Patient selection was appropriate, predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Yes | Patient selection was appropriate; predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. In addition, methodology used was appropriate including the number of outcomes. |
Dhillon 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: 6‐minute walking test
Predictor 2: METs
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: the definition of each predictor was not clarified Domain 3: Outcome
Justification: the outcome is troponin elevation which is not similar to the outcome used in the RCRI development paper Overall judgement
Justification: patient selection was appropriate. However, predictor definitions were unclear/not reported. Furthermore, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | The definition of the RCRI predictors was not clarified. |
| Domain 3: Outcome | No | Troponin was only measured on the morning of postoperative day 1 meaning that many outcomes could have been missed. |
| Domain 4: Analysis | No | Low number of outcomes and only c‐statistics are reported; no measures of calibration or reclassification. |
| Overall judgement | No | Patient selection was appropriate. However, predictor definitions were not clear/not reported. In addition, outcome assessment was inappropriate, the number of outcomes was low and no calibration/reclassification measures were reported. |
Dillon 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Estimated blood loss + operation time
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: there was no definition of the RCRI items; predictors compared are intraoperative predictors meaning that the model cannot be used preoperatively Domain 3: Outcome
Justification: no information on how the outcomes were assessed and whether predefined definitions were used; no reporting of event per individual item of the composite outcome Overall judgement
Justification: patient selection was appropriate. However, predictor and outcome definitions were not clear/not reported and outcome assessment was inappropriate. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing ENT surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | There was no definition of the RCRI items; predictors compared are intraoperative predictors meaning that the model cannot be used preoperatively. |
| Domain 3: Outcome | Unclear | No information on how the outcomes were assessed and whether predefined definitions were used, no reporting of event per individual item of the composite outcome. |
| Domain 4: Analysis | No | Low number of outcomes; only c‐statistic reported and not interpreted in the right way. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported. There was no information on how outcomes were assessed. In addition, the number of outcomes was low and no calibration measures were reported. |
Douville 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Polygenic risk score (CAD)
Predictor 2: Preoperative model (age, admission type, composite RCRI, arrhythmia, fluid/electrolyte disorder, hypertension)
Predictor 3: Preoperative model + Polygenic Risk Score (CAD)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: However, patients might be healthier compared to the patients included in the development study Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: troponin elevation is not similar to the outcome MACE in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | No | Troponins are not routinely drawn on all patients, but rather drawn when a clinical suspicion of MINS exists. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | No | Appropriate patient selection, clearly defined predictors and proper methodology. However, outcomes could have been missed due to inappropriate outcome assessment. |
Duceppe 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no definition for the RCRI items was reported Domain 3: Outcome
Justification: composite outcome that is different from MACE in the development study. In addition, the severity of the composites is very different compared to MACE in the development study. Overall judgement
Justification: patient selection was appropriate. However, there was no information on how predictors were defined. Furthermore, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No definition for the RCRI items was reported. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Unclear | Patient selection was appropriate, outcome definitions were clearly defined and assessed and proper methodology was used. However, there was no/unclear information on predictor definitions. |
Dunn 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASC‐NSQIP‐MICA
Predictor 2: PORT model
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only kidney transplants Domain 2: Predictors
Justification: definition of ischaemic heart disease is different from the definition in the development study and no information on blinding Domain 3: Outcome
Justification: outcome is myocardial infarction and cardiac arrest, which is different from the definition from the development study Overall judgement
Justification: only a selected group of patients was included; predictor definitions were different from the predictor definitions used in the development study. In addition, outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing kidney transplant surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | No | Definition of ischaemic heart disease is different from the definition in the development study and no information on blinding. |
| Domain 3: Outcome | Unclear | No information on how myocardial infarction is defined/diagnosed. |
| Domain 4: Analysis | No | Low number of outcomes; complete case analyses; c‐statistic was not provided for the RCRI alone; no information on calibration and reclassification. |
| Overall judgement | No | Patient selection was appropriate. However, predictors were defined differently compared to predictor definitions used in the development study. In addition, the number of outcomes was low, complete case analysis was performed and no calibration and reclassification was reported. |
Ehlert 2016.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: Modified frailty index
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only kidney transplants Domain 2: Predictors
Justification: some of the definitions of the RCRI were not similar to the predictor definitions of the development study Domain 3: Outcome
Justification: outcome was all‐cause mortality or Clavien Dindo Class IV complications, which is different from the definition from the development study (MACE) Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | No | Some of the definitions of the RCRI were not similar to the predictor definitions of the development study. |
| Domain 3: Outcome | Yes | Clear (RCRI) outcomes definitions were described with appropriate assessment. |
| Domain 4: Analysis | No | Complete case analysis while there were missing data and only c‐statistic without accuracy measures (CI or SE). |
| Overall judgement | No | Patient selection and outcome definitions/assessment was appropriate. However, different predictor definitions were used compared to predictor definitions in the development study. In addition, complete case analysis was performed and no calibration and/or reclassification was reported. |
Farina‐Castro 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: S‐MPM (surgical mortality probability model)
Predictor 3: Charlson Comorbidity Index
Predictor 4: Reiss Index
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients with age > 90 years were included Domain 2: Predictors
Justification: the definition of each item of RCRI was unclear Domain 3: Outcome
Justification: outcome is all‐cause mortality or Comprehensive Complication Index, which is different from the definition from the development study (MACE) Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | The definition of each item of RCRI was unclear. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no information on calibration and reclassification. |
| Overall judgement | No | Patient selection and outcome definitions with their assessment was appropriate. However, there was no/unclear information on predictor definitions. In addition, the number of outcomes was low, complete case analysis was performed and no calibration and reclassification measures were reported. |
Feringa 2007.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: Dobutamine stress echocardiography
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients underwent vascular surgery and high incidences of comorbidities Domain 2: Predictors
Justification: not applicable Domain 3: Outcome
Justification: outcome is all‐cause mortality or MACE, which is different to the definition from the development study (MACE) Overall judgement
Justification: predictor definitions were clearly defined and comparable to definitions used in the development study. However, patient selection was inappropriate and the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients who underwent coronary artery revascularisation were excluded. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on the handling of missing data; no information how many outcomes have occurred for the 6‐month outcome; no calibration or reclassification measures reported. |
| Overall judgement | No | Predictors and outcomes were clearly defined and assessed. However, patient selection was inappropriate, the number of outcomes was low. there was no information on missing data and no calibration or reclassification measures were reported. |
Ferrante 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Prediction model made by the authors including dilated cardiopathy, ischaemic cardiopathy, cerebrovascular disease, peripheral artery disease
Predictor 2: Prediction model made by the authors including previous MI, congestive heart failure and COPD
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only AAA patients were included Domain 2: Predictors
Justification: several RCRI items, including high creatinine value and congestive heart failure, had a different definition compared to the development paper Domain 3: Outcome
Justification: not applicable Overall judgement
Justification: only a selected group of patients was included. Predictor definitions were defined differently from the predictor definitions in the development study. However, the outcome used was comparable to the development study. |
|
| Notes | ||
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | No | Several RCRI items, including high creatinine value and congestive heart failure, had a different definition compared to the development paper. |
| Domain 3: Outcome | Unclear | No information on how the endpoints were defined and assessed. |
| Domain 4: Analysis | No | Complete case analysis; low number of outcomes; no predictive performance measures were reported. |
| Overall judgement | No | Patient selection was appropriate. Furthermore, the number of outcomes was low, complete case analysis was performed and no predictive performance measures were reported. |
Fisher 2008.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
2 or more RCRI factors
|
|
| Predictors | Predictor 1: All 4 pedal pulses absent or any palpated ankle‐to‐arm blood pressure index (AAI)
Predictor 2: Doppler ankle to arm blood pressure index
Predictor 3: All 4 pedal pulses absent
Predictor 4: Ankle to arm blood pressure index AAI ≥ 1.2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on the handling of missing data; dichotomisation of AAI and RCRI; patients in which it was not possible to perform an AAI were excluded from the analysis |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low and there was no information on handling of missing data and dichotomisation of predictors. |
Fronczek 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASC‐NSQIP‐MICA
Predictor 2: Recalibrated RCRI by Canadian Cardiovascular Society
Predictor 3: Recalibrated ASC‐NSQIP‐MICA after logistic recalibration
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients selected were generalisable to the patients included in the RCRI development studies Domain 2: Predictors
Justification: predictor definitions were clearly defined/assessed and comparable to the predictor definitions used in the RCRI development study Domain 3: Outcome
Justification: predictor definitions were clearly defined/assessed and comparable to the predictor definitions used in the RCRI development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | No information on handling missing data and low number of outcomes. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low and there was no information on handling of missing data. |
Gillmann 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 or more RCRI factors
2 or more RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin T
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selected were generalisable to the patient population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: the outcome definition MACE is different from the definition in the development study as it includes troponin elevation Overall judgement
Justification: patient selection was appropriate, there was no/unclear information on predictor definitions/assessments and outcome definition was different compared to the RCRI development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | No | Outcome definition is unclear and no information on the assessment of outcomes and blinding of assessors. |
| Domain 4: Analysis | No | Low number of outcomes; no information on missing data; exclusion of patients without blood samples; no calibration measures. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcomes definitions were unclear and there was no information on predictor and outcome assessments. In addition, the number of outcomes was low, there was no information on missing data and no calibration was reported. |
Glance 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ACS‐NSQIP surgical risk score
Predictor 2: ACS‐NSQIP‐MICA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selected were generalisable to the patient population used in the RCRI development study Domain 2: Predictors
Justification: there is no information on predictor definitions and measurement Domain 3: Outcome
Justification: MICA (myocardial infarction and cardiac arrest) differs from outcome used in development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | There is no information on predictor definitions and measurement. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and exclusion of patients due to missing values or assumption of normal value in case of missing creatinine values. However, discrimination and calibration measures were appropriately reported. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, there was no/unclear information on predictor definitions/assessment. Furthermore, the number of outcomes was low and inappropriate exclusion of patients with missing values. |
Golubovic 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: V‐POSSUM
Predictor 2: NT‐proBNP
Predictor 3: High‐sensitivity troponin I
Predictor 4: V‐POSSUM + NT‐proBNP
Predictor 5: NT‐proBNP + high‐sensitivity troponin I
Predictor 6: V‐POSSUM + high‐sensitivity troponin I
Predictor 7: V‐POSSUM + NT‐proBNP + high‐sensitivity troponin I
Predictor 8: High‐sensitivity troponin I + high‐sensitivity CRP
Predictor 9: High‐sensitivity troponin I + CK‐MB
Predictor 10: NT‐proBNP + high‐sensitivity troponin I + high‐sensitivity CRP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: definition of MACE varies from the development cohort (includes cardiac arrhythmias) Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No information how the individual items of the composite outcome were defined and whether blinding occurred. |
| Domain 4: Analysis | No | Low number of events, dichotomisation of continuous variable and no information on handling missing data. |
| Overall judgement | No | Patient selection was appropriate. There was no/unclear information on how predictors were defined/assessed. However, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Gualandro 2017.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Anaemia
Predictor 2: Smoking
Predictor 3: Vascular Study Group of New England Cardiac Risk Index (VSG‐score)
Predictor 4: Vascular Study Group of New England Cardiac Risk Index (VSG‐score) + anaemia
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients in which no preoperative cardiologic consultation was performed were excluded Domain 2: Predictors
Justification: Predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: Outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selection was inappropriate and not generalisable to the patient population used in the RCRI development study. However, predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | However, no information on the handling of missing data. |
| Overall judgement | Yes | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. Study methodology was appropriate and clear. |
Gualandro 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin T
Predictor 2: High‐sensitivity troponin I
Predictor 3: Sensitive cardiac troponin I
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon 30‐day events |
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selected were generalisable to the patient population used in the RCRI development study Domain 2: Predictors
Justification: unclear what definitions for the RCRI has been used Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement
Patient selected were generalisable to the patient population used in the RCRI development study. Outcomes definitions were clearly defined and comparable to definitions used in the RCRI development study. However, there was no information on the definition of predictors and their assessment. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | Unclear what definitions for the RCRI has been used. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; exclusion of patients (> 50%) without preoperative troponin; no measures of calibration or reclassification reported. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictors definitions were not clear/reported. Furthermore, the number of outcomes was low, inappropriate exclusion of patients with missing data and no calibration/reclassification measures were reported. |
Gupta 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ACS‐NSQIP‐MICA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on how the RCRI predictors were defined Domain 3: Outcome
Justification: outcome is myocardial infarction and cardiac arrest, which is not the outcome for which the RCRI is developed Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI predictors were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Number of outcomes is not reported; calibration and discrimination was reported. Development of a new model was reported and validated in a new model. However, no calibration plot was reported for the NSQIP‐MICA model in the validation set and no information on the confidence intervals or standard errors was reported. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were not clear/reported. Furthermore, the number of outcomes was not reported and inappropriate reporting of performance measures. |
Handke 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin T
Predictor 2: NT‐proBNP
Predictor 3: eGFR (KDIGO stage ≥ 3)
Predictor 4: Presepsin
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only included participants with coronary artery disease Domain 2: Predictors
Justification: no information on how the RCRI predictors were defined Domain 3: Outcome
Justification: outcome definition of MACE is different from the outcome in the development study as it includes e.g. stroke and myocardial ischaemia Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI predictors were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of included patients and outcomes, dichotomisation of continuous variables, no predictive performance measures reported that compared the RCRI with predictors. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictors definitions were not clear/reported. Furthermore, the number of outcomes was low, dichotomisation of continuous variables and inappropriate reporting of performance measures. |
Handke 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin T
Predictor 2: NT‐proBNP
Predictor 3: Presepsin
Predictor 4: High‐sensitivity troponin T + NT‐proBNP
Predictor 5: High‐sensitivity troponin T + presepsin
Predictor 6: NT‐proBNP + presepsin
Predictor 7: NT‐proBNP + high‐sensitivity troponin T + presepsin
Assay/device: Immulite, Siemens Health care Diagnostics, Erlangen, Germany and Cobas E4111, Roche Diagnostics, Mannheim, Germany and noncompetitive immunoassay on the PATHFAST analyser (LSI Medience, Tokyo, Japan) |
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only included participants with coronary artery disease Domain 2: Predictors
Justification: no information on how the RCRI predictors were defined Domain 3: Outcome
Justification: outcome definition of MACE is different from the outcome in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI predictors were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of events and dichotomisation of continuous predictors. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictors definitions were not clear/reported. Furthermore, the number of outcomes was low and dichotomisation of continuous variables. |
Hwang 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Duke Jeopardy score
Predictor 2: Segment involvement score
Predictor 3: Duke Jeopardy score + segment involvement score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: coronary CTA was performed when the patient had not been evaluated for coronary artery disease, had > 1 clinical cardiovascular risk factors or taking cardiovascular medications, and had no contraindication for CT, such as renal failure, any potential of pregnancy, contraindications to β‐blockade or nitroglycerin. Patients with previous revascularisation were excluded. Domain 2: Predictors
Justification: pulmonary oedema was used for item in RCRI of congestive heart failure, definition of other items were not reported and no statement was made on how the CTA results were assessed. Domain 3: Outcome
Justification: outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study Overall judgement
Justification: only a selected group of patients was included. Some predictor definitions were different compared to the RCRI development study and others were not defined at all. However, outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Coronary CTA was performed when the patient had not been evaluated for coronary artery disease, had > 1 clinical cardiovascular risk factors or taking cardiovascular medications, and had no contraindication for CT, such as renal failure, any potential of pregnancy, contraindications to β‐blockade or nitroglycerin. Patients with previous revascularisation were excluded. |
| Domain 2: Predictors | No | Pulmonary oedema was used for item in RCRI of congestive heart failure, definition of other items were not reported and no statement was made on how the CTA results were assessed. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no handling of missing data and dichotomisation of predictor data. No calibration reported. |
| Overall judgement | No | Outcome was clearly defined and assessed. However, patient selection was inappropriate. Predictor definitions were defined differently compared to the definitions used in the RCRI development study. Furthermore, the number of outcomes was low, dichotomisation of continuous variables and inappropriate reporting of performance measures. |
James 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 or 1 RCRI factor
2 or 3 RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: BNP
Predictor 3: CRP
Predictor 4: eGFR
Predictor 5: Anaerobic threshold
Predictor 6: Peak VO2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on how the RCRI predictors were defined Domain 3: Outcome
Justification: Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, this was not the case for predictors. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients unsuitability for CPET (cardiopulmonary exercise testing) were not included. |
| Domain 2: Predictors | Unclear | No information on how the RCRI predictors were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and no handling of missing data; calibration and reclassification were not reported. |
| Overall judgement | No | Outcomes were clearly defined and assessed. However, patient selection was inappropriate, there was no/unclear information on predictor definitions and assessments. Furthermore, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Jarai 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 or more RCRI factors
|
|
| Predictors | Predictor 1: Copeptin
Predictor 2: NT‐proBNP + copeptin
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: preoperative creatinine was deleted from the model as all patients with creatinines > 1.4 were excluded Domain 3: Outcome
Justification: the outcome definition differed from the MACE definition in the development study Overall judgement
Justification: patient selected were generalisable to the patient population used in the RCRI development study. There was no/unclear information on predictor definitions and outcome definition was different compared to the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Excluded were patients with acute coronary syndromes or evidence of myocardial ischaemia on stress tests (n = 4), decompensated heart failure (n = 2), aortic stenosis (n 2), atrial fibrillation (n = 17), kidney dysfunction (serum creatinine 1.4 mg/dl; n = 26), reduced left ventricular function (left ventricular ejection fraction 40%; n = 10) |
| Domain 2: Predictors | No | Preoperative creatinine was deleted from the model as all patients with creatinines > 1.4 were excluded |
| Domain 3: Outcome | No | Independent cardiologist had access to all available documents and clinical charts of each patient. |
| Domain 4: Analysis | No | Low number of outcomes, dichotomisation of predictors and no handling of missing data. |
| Overall judgement | No | Patient selection and outcome and predictor definitions/assessments were inappropriate. In addition, the number of outcomes was low, there was no information on the handling of missing data and predictors were dichotomised. |
Karkos 2002.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: Left ventricular ejection fraction
Predictor 2: Wall abnormalities
Predictor 3: Left ventricular ejection fraction + wall abnormalities
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only patients undergoing the MUGA scan were included over a 4‐year period. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; dichotomisation of predictors; no handling of missing data; no reporting of appropriate performance measures |
| Overall judgement | No | Inappropriate exclusion of patients without a MUGA scan. In addition, the number of outcomes was low, dichotomisation of prediction, no information on handling missing data and no reporting of appropriate performance measures. However, predictors and outcomes were clearly defined and assessed. |
Katsanos 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: BNP
Predictor 2: Goldman index
Predictor 3: Fleisher/Eagle index
Predictor 4: Detsky index
Predictor 5: Functional capacity index
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: unclear what definitions for each of the RCRI predictors were used Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Outcome definition was clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, there was no/unclear information on predictor definitions. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing orthopaedic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | Unclear what definitions for each of the RCRI predictors were used. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, dichotomisation of predictors and no handling of missing data. |
| Overall judgement | No | Appropriate patient selection and outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported, number of outcomes was low, dichotomisation of predictors and no information on handling missing data. |
Kaw 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: Estimated metabolic equivalents (METS)
Predictor 2: METS + positive stress test
Predictor 3: METSe + positive stress test with no false negatives
Predictor 4: Positive stress test
Predictor 5: Positive stress test with no false negatives
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients who underwent preoperative stress testing were included which seems to be less healthy compared to development population Domain 2: Predictors
Justification: no information on how the RCRI items were defined and on how the predictors added/compared were assessed Domain 3: Outcome
Justification: outcome differs from outcome in development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI items were defined and on how the predictors added/compared were assessed. |
| Domain 3: Outcome | No | No information on how endpoints were defined apart from ICD‐codes and no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes and no information on handling missing outcomes. |
| Overall judgement | No | Patient selection was appropriate. However, outcome assessment was through ICD codes and there was no information on blinding. Predictor definitions were unclear/not reported, number of outcomes was low and no information on handling missing data. |
Kertai 2005.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: RCRI with redefined high‐risk surgery
Predictor 2: RCRI with redefined high‐risk surgery + clinical characteristics
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome is all‐cause mortality Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clear methodology and appropriate number of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Yes | Patient selection was appropriate, predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. In addition, methodology used was appropriate including the number of outcomes. |
Kopec 2017.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin T
Predictor 2: NT‐proBNP
Predictor 3: High‐sensitivity troponin T +NT‐proBNP
Predictor 4: ASA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: the definition of each item of RCRI was unclear Domain 3: Outcome
Justification: outcome is myocardial infarction, which is different from the MACE definition in the development study Overall judgement
Justification: patient selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only patients with known coronary artery disease or multiple risk factors for coronary artery disease were included. |
| Domain 2: Predictors | Unclear | The definition of each item of RCRI was unclear. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, patients with missing biomarker data were excluded and dichotomisation of predictor information. |
| Overall judgement | No | Patient selection was inappropriate and predictor definitions were unclear/not reported. In addition, the number of outcomes was low, inappropriate exclusion of patients with missing data and dichotomisation of predictors. However, outcomes were clearly defined and assessed. |
Kumar 2001.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: DVAMC (new prediction model)
Predictor 2: Goldman index
Predictor 3: Detsky index
Predictor 4: Ashton
Predictor 5: DVAMC + type of surgery
Predictor 6: Detsky index + type of surgery
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: all included patients had known or suspected cardiac disease Domain 2: Predictors
Justification: different definitions of RCRI items compared to development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement
Justification: only a selected group of patients was included; predictor definitions were different compared to definitions used in the RCRI development study. However, outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | All included patients had known or suspected cardiac disease. |
| Domain 2: Predictors | No | Different definitions of RCRI items compared to development study. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcome, no information on handling missing data and no measures on calibration. |
| Overall judgement | No | Outcome was clearly defined and assessed. However, patient selection was inappropriate. Predictor definitions were defined differently compared to the definitions used in the RCRI development study. Furthermore, the number of outcomes was low, no information on handling missing data and inappropriate reporting of performance measures. |
Leibowitz 2008.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: BNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patients were included if they had a clinical history of congestive heart failure on physical examination or known ejection fraction < 40% or severe aortic stenosis Domain 2: Predictors
Justification: the definition of each item of RCRI was unclear Domain 3: Outcome
Justification: composition of MACE is very different from the definition of MACE in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients were included if they had a clinical history of congestive heart failure on physical examination or known ejection fraction < 40% or severe aortic stenosis. |
| Domain 2: Predictors | Unclear | The definition of each item of RCRI was unclear. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on the handling of missing data; no information on calibration measures. |
| Overall judgement | No | Outcome was clearly defined and assessed. However, patient selection was inappropriate. Predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on handling missing data and inappropriate reporting of performance measures. |
Makary 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: Frailty
Predictor 2: ASA
Predictor 3: ASA + frailty
Predictor 4: Eagle score
Predictor 5: Eagle score + frailty
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: not specified what type of surgery the patients underwent and patients with previous stroke were excluded from the analysis Domain 2: Predictors
Justification: the definition of each item of RCRI was unclear Domain 3: Outcome
Justification: outcome includes surgical complications and presumably this also involves noncardiac complications, which differs from the MACE definition from the development study Overall judgement
Justification: the type of surgery was not specified and inappropriate exclusion of patients with stroke. In addition, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Not specified what type of surgery the patients underwent and patients with previous stroke were excluded from the analysis. |
| Domain 2: Predictors | Unclear | The definition of each item of RCRI was unclear. |
| Domain 3: Outcome | No | No outcome definitions and no information on blinding. |
| Domain 4: Analysis | No | No information on the number of outcomes, how missing data were handled and no reporting of calibration measures. |
| Overall judgement | No | Patient selection was inappropriate. Predictor and outcome definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on handling missing data and inappropriate reporting of performance measures. |
Markovic 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: Survivin
Predictor 2: Heart‐type fatty acid binding protein (H‐FABP)
Predictor 3: High‐sensitivity CRP
Predictor 4: Survivin + high‐sensitivity CRP
Predictor 5: Survivin + H‐FABP
Predictor 6: ASA
Predictor 7: ASA + SORT + ACS‐NSQIP surgical risk score
Predictor 8: ACS‐NSQIP surgical risk score
Predictor 9: SORT
Predictor 10: ASA + SORT
Predictor 11: ASA + ACS‐NSQIP surgical risk score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on the handling of missing data; multiple testing issue; no information on calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low, multiple comparisons were reported, there was no information on missing data and no calibration was reported. |
Mauermann 2016.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: Copeptin
Predictor 2: Age + sex + copeptin
Predictor 3: NT‐proBNP
Predictor 4: ACS‐NSQIP MICA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on RCRI predictor definition Domain 3: Outcome
Justification: outcome is myocardial injury (MINS) and not MACE |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only high‐risk patients, i.e. patients with a history of coronary artery disease or patients having two risk factors for coronary artery disease were included. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definition. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and dichotomisation of predictors. |
| Overall judgement | No | Outcome was clearly defined and assessed. However, patient selection was inappropriate as only high‐risk patients were included. Predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, dichotomisation of continuous variables and complete case analysis was performed. |
McAlister 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0‐1 RCRI factors
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: CHADS2
Predictor 2: CHADS2‐Vasc
Predictor 3: R2CHADS2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: all patients had preoperative history of AF Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome is composite of stroke and all‐cause mortality and not MACE Overall judgement
Justification: predictors were clearly defined and comparable as used in the development study. However, only a selected group of patients were included and the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no calibration measures reported. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low, complete case analysis was reported and no calibration was reported. |
McAlister 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 to 1 RCRI factors
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: CHADS2
Predictor 2: CHADS2‐Vasc
Predictor 3: R2CHADS2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: all patients had preoperative history of AF Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: MACE outcome also includes stroke and troponin elevation (MINS) and is therefore different from the MACE definition in the development study Overall judgement
Justification: predictors were clearly defined and comparable as used in the development study. However, only a selected group of patients were included and the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Complete case analysis and categorisation of prediction models. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, complete case analysis was reported and categorisation of prediction models. |
McIlroy 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: RH‐PAT index (endothelial function)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on predictor definition of the RCRI items Domain 3: Outcome
Justification: outcome is troponin elevation (MINS) or all‐cause mortality and MACE, which is different from the MACE definition in the development study Overall judgement:
Patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on predictor definition of the RCRI items. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no reporting of calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, prediction definitions were unclear/not reported. In addition, the number of outcomes was low, complete case analysis was performed and no calibration was reported. |
Mercantini 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: BNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on predictor definition of the RCRI items and for history of ischaemic disease, another definition was used Domain 3: Outcome
Justification: MACE definition is highly different from the MACE definition in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. In addition, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on predictor definition of the RCRI items and for history of ischaemic disease, another definition was used. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing data and no reporting of calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. In addition, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Moodley 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: SAVS‐CRI (South African Vascular Surgery Cardiac Risk Index)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: outcome used in this study is highly different from the MACE definition in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Yes | Patient selection was appropriate, predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. In addition, methodology used was appropriate including the number of outcomes. |
Neary 2007.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: POSSUM
Predictor 2: ACS‐NSQIP surgical risk score
Predictor 3: Biochemistry and Haematology Outcome Models
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: inclusion of emergency surgery patients and broad range in ages Domain 2: Predictors
Justification: predictor definitions not described Domain 3: Outcome
Justification: outcome was all‐cause mortality and not MACE Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | Predictor definitions not described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Adequate sample size, no information on missing data but likely there were no missing data because of the prospective nature of the study. |
| Overall judgement | Unclear | Patient selection was appropriate. Outcome definition was clearly defined/assessed and clear study methodology used was used with appropriate the number of outcomes. However, there was no/unclear information on predictor definitions. |
Noordzij 2006.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: ECG abnormalities
Predictor 2: Age
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients at high risk for CAD included Domain 2: Predictors
Justification: predictor definitions very different from the development study Domain 3: Outcome
Justification: outcome was cardiovascular death and not MACE Overall judgement
Justification: only a selected group of patients was included; predictors of the original RCRI were not included or had a different definition. In addition, the outcome definition used was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | Predictor definitions very different from the development study. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | No information on handling of missing data and calibration/reclassification not assessed. |
| Overall judgement | No | Patient selection was appropriate and outcomes was clearly defined and assessed. Predictor definitions were defined differently compared to the definitions used in the RCRI development study. Furthermore, there was no information on handling of missing data and inappropriate reporting of performance measures. |
Pandey 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: History of preoperative stable angina
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only participants with recent myocardial infarction were included Domain 2: Predictors
Justification: no information on predictor definitions Domain 3: Outcome
Justification: outcome was different from the MACE definition used in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on handling missing data; no reporting of calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate and outcomes was clearly defined and assessed. Predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, there was no information on handling of missing data and inappropriate reporting of performance measures. |
Pantoja 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Goldman index
Predictor 2: Detsky index
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on how the RCRI predictors were defined, when the model was used Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Outcome definition was clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, there was no/unclear information on predictor definitions. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI predictors were defined and when the model was used. |
| Domain 3: Outcome | Unclear | No definitions for each of the composite outcomes and no information whether the assessors were blinded for the predictor variables. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis, only sensitivity and specificity reported and no performance measures on discrimination, calibration and reclassification. |
| Overall judgement | No | Patient selection was appropriate. However, outcome and predictor definitions were unclear/not reported. In addition, the number of outcomes was low, complete case analysis was performed and inappropriate reporting on performance measures. |
Park 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: Left ventricular ejection fraction
Predictor 3: Regional wall motion index
Predictor 4: Left atrial volume index
Predictor 5: E/E' (transmitral early diastolic velocity/tissue Doppler mitral annular early diastolic velocity)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients referred for cardiac testing were included in this study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement
Justification: only a selected group of patients was included, that was not generalisable to the patient population used in the RCRI development study. However, predictors and outcomes were clearly defined/assessed and comparable as used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Patients without an echocardiography, with moderate to severe valvular stenosis and with a preoperative creatinine ≥ 2.0 mg/dL were excluded. Patients underwent echocardiography at the discretion of the physician or if they had 2 or more of the following cardiovascular risk factors: diabetes mellitus, hypertension, aged 65 years and older, current smoking status or hypercholesterolaemia. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | However, no information on handling missing data and no reporting of calibration and reclassification measures. |
| Overall judgement | No | Patient selection was inappropriate resulting in a more high‐risk population compared to the RCRI development study. However, predictor and outcome definitions were clearly defined and assessed. In addition, methodology used was appropriate, although there was no information on the handling of missing data and no reporting of calibration/reclassification measures. |
Parmar 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 of more RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: Eagle score
Predictor 3: P‐POSSUM
Predictor 4: Age > 80 years old + ischaemic heart disease
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: all patients were started on statins and beta‐blockade was initiated if not contraindicated. Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement
Justification: only a selected group of patients was included, that was not generalisable to the patient population used in the RCRI development study. However, predictors and outcomes were clearly defined/assessed and comparable as used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | All patients were started on statins and beta‐blockade was initiated if not contraindicated. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on the handling of missing data; a new prediction model was developed based on univariable analysis; no reporting of calibration/reclassification measures. |
| Overall judgement | No | Predictors and outcomes were clearly defined and assessed. However, patient selection was inappropriate, as all patients were initiated on drug therapy. In addition, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Peterson 2016.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
2 or more RCRI factors
|
|
| Predictors | Outcome category
Full outcome definition
Prediction horizon
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: definition of MACE is different to the definition of MACE in the RCRI development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing orthopaedic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no handling of missing data; no reporting of calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low and there was no information on missing data and no calibration was reported. |
Press 2006.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: Goldman index
Predictor 3: Detsky index
Predictor 4: Score by Halm et al
Predictor 5: Score by Tu et al
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: No information on predictor definitions Domain 3: Outcome
Justification: concern regarding applicability is low for outcome MACE, but high for the other validated outcomes Overall judgement:
Patients selected were generalisable to the patient population used in the RCRI development study. Outcome definition was clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, there was no/unclear information on predictor definitions. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no handling of missing data; only c‐statistics reported. Many models are compared to each other without adjustment for multiple testing. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, there was no/unclear information on predictor definitions. In addition, the number of outcomes was low and there was no information on missing data, multiple testing issue and no calibration was reported. |
Ray 2010.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Platelet CD40 ligand
Predictor 2: Platelet factor V/Va
Predictor 3: Platelet P‐selectin
Predictor 4: High‐sensitivity CRP
Predictor 5: BNP
Predictor 6: sCD40L
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Outcome definition was clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, there was no/unclear information on predictor definitions. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing orthopaedic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No outcome definitions were provided. |
| Domain 4: Analysis | No | Low number of outcomes, no information on the handling of missing data and no reporting on calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported. In addition, the number of outcomes was low, there was no information on missing data and no calibration was reported. |
Reis 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Vascular Surgery Group Cardiac Risk Index (VSG‐CRI)
Predictor 2: Vascular Quality Initiative Cardiac Risk Index (VQI‐CRI)
Predictor 3: South African Vascular Surgical Cardiac Risk Index (SAVS‐CRI)
Predictor 4: New model ‐ coronary artery disease, atrial fibrillation, diabetes mellitus, mechanical ventilation and heart rate ordinal
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: although MACE was used as the outcome, it was different from the MACE outcome used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No information on how the outcomes were determined, what definitions were used and what prediction horizon was used. |
| Domain 4: Analysis | No | Low number of outcomes and no information on handling missing data. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported including their assessment. In addition, the number of outcomes was low and there was no information on missing data. |
Rodseth 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 ‐2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: BNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: no clear definition of the outcome measure MACE, which could be different among the included studies + outcome is different compared to development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No clear definition of the outcome measure MACE, which could be different among the included studies. |
| Domain 4: Analysis | No | Low number of outcomes, no information on the handling of missing data and no reporting of calibration measures |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported including their assessment. In addition, the number of outcomes was low, there was no information on missing data and no reporting calibration measures. |
Rohde 2001.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 ‐2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Abnormal echocardiography
Predictor 2: Any degree of systolic dysfunction on echocardiography
Predictor 3: Any degree of systolic dysfunction or moderate to severe left ventricular hypertrophy on echocardiography
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients who underwent preoperative TTE were included in the analysis Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement
Justification: only a selected group of patients was included, that was not generalisable to the patient population used in the RCRI development study. However, predictors and outcomes were clearly defined/assessed and comparable as used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only patients who underwent preoperative TTE were included in the analysis. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on the handling of missing data and no reporting on calibration/reclassification measures. |
| Overall judgement | No | Predictors and outcomes was clearly defined and assessed. However, patient selection was inappropriate, the number of outcomes was low, no information on handling of missing data and inappropriate reporting of performance measures. |
Rohrig 2004.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ASA
Predictor 2: Model 1 – age, male gender, coronary bypass/PTCA, valvular heart disease, arrhythmia, arterial hypertension, carotid stenosis, hypervolaemia, chronic renal failure, emergency surgery, neurosurgery, major vascular surgery, haematopoietic/lymphatic surgery and gastrointestinal surgery
Predictor 3: Model 2 – age, ASA, neurosurgery, thoracic surgery, major vascular surgery, haematopoietic/lymphatic surgery and gastrointestinal surgery
|
|
| Outcome | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: the RCRI was not developed to predict intraoperative events and the outcome is very different from the MACE outcome used in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | Yes | Patient selection was appropriate, predictor and outcome definitions were clearly defined and comparable to the definitions used in the development study. In addition, methodology used was appropriate including the number of outcomes. |
Rutkowski 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ACS‐NSQIP‐MICA
Predictor 2: ACS‐NSQIP‐Cardiac death score
Predictor 3: ACS‐NSQIP‐Death score
Predictor 4: ACS‐NSQIP‐Cardiac complications score
Predictor 5: Karnofsky performance score
Predictor 6: ASA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients who underwent craniotomy were included Domain 2: Predictors
Justification: craniotomy was considered as high‐risk surgery, however this procedure is not considered high‐risk in the RCRI predictor definitions. No definition was provided for history of ischaemic heart disease and congestive heart failure. Domain 3: Outcome
Justification: MACE definition was different from its definition used in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on some predictor definitions and other had different definitions compared to the RCRI development study. In addition, outcome definition used was different compared to the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | This study was a case‐control study, which is not the appropriate design for prediction research. |
| Domain 2: Predictors | No | Craniotomy was considered as high‐risk surgery, however this procedure is not considered high‐risk in the RCRI predictor definitions. No definition was provided for history of ischaemic heart disease and congestive heart failure. |
| Domain 3: Outcome | Unclear | No information on the definition, how it was determined and whether it was blinded. |
| Domain 4: Analysis | No | Low number of events; no reporting of calibration/reclassification measures; use of a case‐control design is not appropriate for prediction research analysis. |
| Overall judgement | No | This study was a case‐control study, which is not the appropriate design for prediction research. Predictor definitions were defined differently compared to the definitions used in the RCRI development study. Outcome definitions with their assessment were unclear/not reported. Furthermore, the number of outcomes was low and inappropriate reporting of performance measures. |
Sabate 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Outcome category
Full outcome definition
Prediction horizon
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: definition of IHD and CHF are unclear and definition of high‐risk surgery is different Domain 3: Outcome
Justification: MACE definition also includes cerebrovascular events and is therefore different from its definition used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. In addition, outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | Definition of IHD and CHF are unclear and definition of high‐risk surgery is different. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | No | Patient selection was appropriate, outcome definitions with their assessment were clearly defined and comparable to the definitions used in the development study. In addition, methodology used was appropriate including the number of outcomes. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. |
Saito 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: E/E'
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patients selected were generalisable to the patient population used in the RCRI development study. Outcome definition was clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, there was no/unclear information on predictor definitions. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Only those who underwent TTE were eligible for study participation. |
| Domain 2: Predictors | Unclear | No/unclear information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | Outcome definitions for, among others, myocardial infarction and heart failure are not clear and no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes; no predictive performance measures are reported; no information on handling of missing data. |
| Overall judgement | No | Patient selection was inappropriate as only a selected group of high‐risk patients were included. Predictor and outcome definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Scholz 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Regulatory T cells
Predictor 2: NT‐proBNP + high‐sensitivity troponin
Predictor 3: NT‐proBNP + high‐sensitivity troponin + regulatory T‐cells
Predictor 4: Regulatory T cells + age + sex +ASA + history of PCI + creatinine
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: all included patients had coronary artery disease Domain 2: Predictors
Justification: no information on how the RCRI items were defined Domain 3: Outcome
Justification: outcome also includes troponin elevation (MINS), which is not included in the original RCRI outcome definition Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information on how the RCRI items were defined. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcome and no information on missing data. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low and there was no information on missing data. |
Schouten 2006.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: AAA size
Predictor 2: AAA size + age
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on blinding in retrospective study and no information on the definition of CHF and IHD Domain 3: Outcome
Justification: outcome is composite of cardiovascular death and nonfatal myocardial infarction which differs from outcome in development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on blinding in retrospective study and no information on the definition of CHF and IHD. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing values and no reporting of calibration/reclassification measures. |
| Overall judgement | No | Outcome was clearly defined and assessed. Patient selection was appropriate. Predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Schrimpf 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Copeptin
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on RCRI predictor definitions Domain 3: Outcome
Justification: composite endpoint of MACE is very different from the outcome used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | Individual items of MACE composite are not reported; no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes; no information on handling missing outcome; no reporting on calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Scorcu 2020.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Updated Cardiac Risk Score (UCRS) ‐ high‐risk surgery, preoperative estimate glomerular filtration rate < 30 ml/min/1.73 m2, age ≥ 75 years and history of heart failure
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: definitions of high‐risk surgery and ischaemic heart disease were different from the development study Domain 3: Outcome
Justification: although stroke was included in the outcome definition, it is only a small contribution to the number of events Overall judgement:
Patients selected were generalisable to the patient population used in the RCRI development study. Outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | Definition of high‐risk surgery and ischaemic heart disease were different from the development study. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on the handling of missing data and no reporting of calibration/reclassification measures. |
| Overall judgement | No | Patient selection was appropriate and outcome was clearly defined and assessed. However, predictor definitions were defined differently compared to the definitions used in the RCRI development study. Furthermore, the number of outcomes was low, no information on handling missing data and inappropriate reporting of performance measures. |
Scrutinio 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: High‐sensitivity CRP
Predictor 3: NT‐proBNP+ high‐sensitivity CRP
Predictor 4: New developed prediction model including insulin therapy for diabetes, open surgery and the highest tertiles of fibrinogen (> 377 mg/dL), hs‐CRP (> 3.2 mg/L) and NT‐proBNP (> 221 ng/L)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes and no information on handling missing data. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, the number of outcomes was low and there was no information on missing data. |
Sheth 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Coronary CT angiography
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: many exclusion criteria including persistent atrium fibrillation, patients with previous stent implantation. However, they could not have done it differently as these exclusions were due to CTA measurements. Domain 2: Predictors
Justification: no information for each of the RCRI predictor definitions Domain 3: Outcome
Justification: outcome MACE differs from the definition of MACE in the development study Overall judgement
Justification: only a selected group of patients was included, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | No information for each of the RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on handling missing outcome; no reporting on calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcome was clearly defined and assessed. However, predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Stonelake 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors Not reported |
|
| Predictors | Predictor 1: ASA
Predictor 2: POSSUM
Predictor 3: P‐POSSUM
Predictor 4: CR‐POSSUM
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: no information on each of the RCRI predictor definitions Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE |
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on each of the RCRI predictor definitions Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Exclusion of some surgical procedure as described in figure 1 seems inappropriate. |
| Domain 2: Predictors | Unclear | No information on each of the RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing data and no reporting of performance measures, only percentages. |
| Overall judgement | No | Outcome was clearly defined and assessed. However, patient selection was inappropriate and predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Subramaniam 2011.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: LTSS ‐ age > 65 years, diabetes mellitus, history of cerebrovascular disease, history of ischaemic heart disease, history of congestive heart failure, ST‐depression on preoperative ECG and renal insufficiency
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: definition of ischaemic heart disease and congestive heart failure unclear and probable exclusion of high‐risk surgery Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE. In addition, outcomes were assessed at 6 months and at 1 and 3 years after surgery, whereas the RCRI has a prediction horizon of 30 days Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | Definition of ischaemic heart disease and congestive heart failure unclear and probable exclusion of high‐risk surgery. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no handling of missing data and no reporting on calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcome was clearly defined and assessed. However, predictor definitions were unclear/not reported. Furthermore, the number of outcomes was low, no information on the handling of missing data and inappropriate reporting of performance measures. |
Valentijn 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 to 1 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Aortic value function (aortic valve sclerosis)
Predictor 2: Aortic value function (aortic valve stenosis)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: some of the echocardiographies were performed in the 30 days after surgery Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE |
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: some of the echocardiographies were performed in the 30 days after surgery Domain 3: Outcome
Justification: outcome is all‐cause mortality and not MACE Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, some predictors were measures after surgery and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | No | Some of the echocardiographies were performed in the 30 days after surgery. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Categorisation of predictors; no performance measures for additive predictive performance are reported; complete case analysis. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, some predictors were not preoperatively available. Furthermore, predictors were categorised, complete case analysis was performed and no reclassification measures were reported. |
van Diepen 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 to 1 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: CHADS2
Predictor 2: CHADS2‐Vasc
Predictor 3: R2CHADS2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: only patients with nonvalvular atrium fibrillation were included Domain 2: Predictors
Justification: some definitions of the RCRI did not match the definitions used for this article Domain 3: Outcome
Justification: outcome is composite of mortality, stroke, TIA and systemic embolism and not MACE Overall judgement
Justification: only a selected group of patients was included which are not generalisable to the RCRI development cohort. No/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. Outcome definition was different compared to the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | Some definitions of the RCRI did not match the definitions used for this article. |
| Domain 3: Outcome | Yes | some definitions of the RCRI did not match the definitions used for this article. |
| Domain 4: Analysis | Yes | Clear methodology and appropriate number of outcomes. |
| Overall judgement | No | Patient selection was appropriate, outcome definitions were clearly defined and comparable to the definitions used in the development study. Methodology used was appropriate including the number of outcomes. However, some predictor definitions were defined differently compared to the definitions used in the RCRI development study. |
van Klei 2007.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Left bundle branch block on ECG
Predictor 2: Right bundle branch block on ECG
Predictor 3: Male gender
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome is myocardial infarction and not MACE Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | No | Troponin, ECG and echocardiography were not measured in all patients, only on clinical indication. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no reporting on calibration and reclassification measures. |
| Overall judgement | No | Patient selection was appropriate. Predictors were clearly defined and assessed. However, troponin, ECG and echocardiography were only measured on clinical indication. In addition, the number of outcomes was low, complete case analysis and no calibration was reported. |
Vetrugno 2014.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: BNP
Predictor 2: ASA
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Exclusion criteria were atrial fibrillation, a recent history (within 6 months) of unstable coronary syndrome, or decompensate heart failure. Since severe aortic valve stenosis and impaired renal function are associated with increased serum levels of natriuretic peptides, patients with these preoperative diagnoses were also excluded. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | No | AV block counted as MACE, but this was not predefined. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no reporting on calibration measures. |
| Overall judgement | No | Predictor definitions were clearly defined/reported and assessed. However, patient selection was inappropriate as only a selected group of patients were included. Outcome definition was inconsistent with the MACE definition reported. Furthermore, the number of outcomes was low, complete case analysis and inappropriate reporting of performance measures. |
Vilarino‐Rico 2015.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Halm score
Predictor 2: Tu score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on individual RCRI predictor definitions Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on individual RCRI predictor definitions. |
| Domain 3: Outcome | Unclear | No definitions were provided for the separate composite outcomes and no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes, complete case analysis and no reporting on calibration measures. |
| Overall judgement | No | Patient selection was appropriate. However, predictor and outcome definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, complete case analysis was performed and inappropriate reporting of performance measures. |
Waterman 2016.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Total joint arthroplasty model (TJA) ‐ risk score (age > 80, hypertension, history of cardiac disease)
Predictor 2: Total joint arthroplasty model (TJA) ‐ individual risk factors (age > 80, hypertension, history of cardiac disease)
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information on individual RCRI predictor definitions Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing orthopaedic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information on individual RCRI predictor definitions. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | The analysis performed is not clear; no reporting on calibration measures; no information on handling missing data. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported including their assessment. Furthermore, the analysis performed is not clear, no information on handling missing data and inappropriate reporting of performance measures. |
Weber 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: NT‐proBNP
Predictor 2: High‐sensitivity troponin T
Assay/device: Roche Diagnostics, Mannheim, Germany |
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Domain 1: Participant selection
Justification: Domain 2: Predictors
Justification: Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study |
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: the authors state that they used the definitions by the original Lee paper, however the definition of CAD is different and others are not specified Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Unclear | The authors state that they used the definitions by the original Lee paper, however the definition of CAD is different and others are not specified. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes; no information on handling missing outcomes; no calibration/reclassification measures were reported. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, no information on handling missing data and inappropriate reporting of performance measures. |
Welten 2007.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Type of surgery + age + history of hypertension (low, low‐intermediate, high‐intermediate and high risk of surgery; < 55, age 56 to 65, age 66 to 75 and > 70)
Assay/device: not applicable |
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: MACE outcome is different from the MACE definition used in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | No measures of calibration/reclassification were reported and no information on handling missing data. |
| Overall judgement | No | Patient selection was appropriate. Predictors and outcomes were clearly defined and assessed. However, there was no information on missing data and no calibration/reclassification measures was reported. |
Wijeysundera 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Peak oxygen consumption
Predictor 2: Anaerobic threshold
Predictor 3: DASI
Predictor 4: NT‐proBNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: RCRI predictor definitions were not reported Domain 3: Outcome
Justification: outcome used is different from the MACE definition used in the development study Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, there was no/unclear information on predictor definitions and outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing vascular surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | RCRI predictor definitions were not reported. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Complete case analysis, low number of outcomes and no reporting on calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, complete case analysis and inappropriate reporting of performance measures. |
Wilcox 2019.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ACS‐NSQIP surgical risk score
Predictor 2: ACS‐NSQIP MICA
Predictor 3: MASHOUR
Predictor 4: CHADS2‐VASC
Predictor 5: CHADS2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: different definition for ischaemic heart disease and unclear definition for high‐risk surgery and congestive heart failure Domain 3: Outcome
Justification: outcome is stroke and not MACE Overall judgement
Justification: patients selected were generalisable to the patient population used in the RCRI development study. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. In addition, outcome definition was different compared to the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | No | Different definition for ischaemic heart disease and unclear definition for high‐risk surgery and congestive heart failure. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | Yes | However, method of handling missing data was not appropriate and no reporting of calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcome definitions were clearly defined and comparable to the definitions used in the development study. However, no/unclear information on predictor definitions for some items and other predictors of the original RCRI were not included or had a different definition. In addition, method of handling missing data was not appropriate and no reporting of calibration measures. |
Wotton 2013.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ThRCRI
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: no information regarding the definition of some of the RCRI variables Domain 3: Outcome
Justification: definition differs from outcome in development study (mainly because of addition of atrial fibrillation and all‐cause mortality to the composite outcome) |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Although only patients undergoing thoracic surgery were included, participant selection was appropriate and the RCRI model can be applied in these patients. |
| Domain 2: Predictors | Unclear | No information regarding the definition of some of the RCRI variables. |
| Domain 3: Outcome | Yes | Clearly defined outcome definitions and appropriate adjudication of outcomes. |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing outcomes, no information on blinding and no reporting on calibration measures. |
| Overall judgement | No | Patient selection was appropriate. Outcomes were clearly defined and assessed. However, predictor definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, no information on handling of missing data and inappropriate reporting of performance measures. |
Yang 2012.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 to 2 RCRI factors
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: Ischaemia on a thallium scan
Predictor 2: NT‐proBNP
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definitions were clearly defined and comparable to the definitions used in the development study Overall judgement:
Patient selected were generalisable to the patient population used in the RCRI development study. Predictor and outcome definitions were clearly defined/assessed and comparable to the definitions used in the RCRI development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Eligible patients needed to be referred to the cardiologist before surgery. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | No | The authors defined myocardial infarction solely as a rise in troponin and no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing data, no information on blinding and dichotomisation of the predictors. |
| Overall judgement | No | Predictor definitions were clearly defined/reported and assessed. However, patient selection was inappropriate as only a selected group of high‐risk patients were included. Outcome definition was inappropriate as myocardial infarction was solely defined as a rise in troponin. Furthermore, the number of outcomes was low, no information on the handling of missing data and dichotomisation of predictors. |
Yang 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: High‐sensitivity troponin I
Predictor 2: sST2 (soluble suppression of tumorigenicity‐2)
Predictor 3: High‐sensitivity troponin I +sST2
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: no information on how the composite outcomes were defined and whether assessors were blinded Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome definitions were unclear/not reported including their assessment. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | No | Inappropriate exclusion of many patients: 150 who did not provide informed consent and 71 patients who could not undergo biomarker testing. Only 10% of the original sample was included in the study. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Unclear | No information on how the composite outcomes were defined and whether assessors were blinded |
| Domain 4: Analysis | No | Low number of outcomes, no information on handling missing outcomes, no information on blinding and dichotomisation of the predictors. |
| Overall judgement | No | Predictor definitions were clearly defined and assessed. However, patient selection was inappropriate as only a selected group of high‐risk patients were included. Outcome definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, no information on the handling of missing data and dichotomisation of predictors. |
Yap 2018.
| Study characteristics | ||
| General information | Objective
Journal
Country
Study design
|
|
| Participants | Number of included patients
Surgical specialty
Age
Male sex
High‐risk surgery
Insulin‐dependent diabetes mellitus
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular events
Elevated creatinine
0 RCRI factors
1 RCRI factor
2 RCRI factors
3 or more RCRI factors
|
|
| Predictors | Predictor 1: ACS‐NSQIP surgical risk score
|
|
| Outcome | Outcome category
Full outcome definition
Prediction horizon
|
|
| Analysis | Number of outcomes
Handling missing data
Discrimination reported?
Calibration reported?
Reclassification reported?
|
|
| PROBAST: Applicability | Domain 1: Participant selection
Justification: patient selection was appropriate and generalisable to the population used in the RCRI development study Domain 2: Predictors
Justification: predictor definitions were clearly defined and comparable to the definitions used in the development study Domain 3: Outcome
Justification: outcome definition of MACE is different from the outcome used in the development study Overall judgement
Justification: patient selection was appropriate and predictor definitions were clearly defined and comparable to definitions used in the development study. However, the outcome used was different from MACE in the development study. |
|
| Notes | — | |
| Item | Authors' judgement | Support for judgement |
| Domain 1: Participant selection | Yes | Appropriate participant selection in which patients were selected in whom the RCRI model can be applied. |
| Domain 2: Predictors | Yes | Clear (RCRI) predictor definitions were described. |
| Domain 3: Outcome | Unclear | No composite outcome definitions and no information on blinding. |
| Domain 4: Analysis | No | Low number of outcomes, no information on missing data and no calibration measures were reported. |
| Overall judgement | No | Patient selection was appropriate. Predictors were clearly defined and assessed. However, outcome definitions were unclear/not reported including their assessment. Furthermore, the number of outcomes was low, there was no information on missing data and no calibration was reported. |
AAA: abdominal aortic aneurysm; AAI: ankle‐to‐arm blood pressure index; ACS‐NSQIP: American College of Surgeons National Surgical Quality Improvement; AF: atrial fibrillation; ASA: American Society of Anesthesiologists; BNP: brain natriuretic peptide; CACS: Coronary artery calcium scores; CAD: coronary artery disease; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; CPR: Cardiopulmonary resuscitation; CRP: C‐reactive protein; CT: computed tomography; CTA: computed tomography angiography; DSE: dobutamine stress echocardiography; DVAMC: Durham Veterans Administration Hospital; ECG: electrocardiogram; eGFR: estimated glomerular filtration rate; ICD: International Classification of Diseases; IHD: ischaemic heart disease; IPD: individual patient data; IQR: interquartile range; LTSS: long term survival score; LVEF: left ventricular ejection fraction; MACE: major adverse cardiac events; MET: metabolic equivalents; MI: myocardial infarction; MICA: myocardial infarction or cardiac arrest; MINS: myocardial injury after noncardiac surgery; MUGA: multigated acquisition scan; NSQIP: National Surgical Quality Improvement; NT‐proBNP: (NT‐pro)brain natriuretic peptide; PCI: percutaneous coronary intervention; PTCA: percutaneous transluminal coronary angioplasty; RCRI: Revised Cardiac Risk Index; RCT: randomised controlled trial; SD: standard deviation; SORT: Surgical Outcome Risk Tool; SPECT: single photon emission computed tomography; STEMI: ST‐elevation myocardial infarction; TTE: transthoracic echocardiography; UAP: unstable angina pectoris
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abbott 2017 | No prediction |
| Abbott 2019 | No prediction |
| Abdelmalak 2018 | No external validation of RCRI |
| Abdullah 2017 | No prediction |
| Abdullaha 2018 | No external validation of RCRI |
| Abelha 2009 | No prediction |
| Abelha 2010 | No prediction |
| Abelha 2012 | No prediction |
| Ackland 2007 | No prediction |
| Ackland 2010 | Other prediction model |
| Ackland 2011 | No prediction |
| Ackland 2018 | No prediction |
| Agarwal 2013 | No prediction |
| Albaladejo 2011 | No prediction |
| Alcock 2012 | No prediction |
| Alcock 2013 | No prediction |
| Alvarez 2016 | No prediction |
| Ambler 2014 | No prediction |
| Andersson 2015 | External validation only without added value or comparison |
| Anghelescu 2018 | No external validation of RCRI |
| Arain 2016 | No prediction |
| Armstrong 2017 | No prediction |
| Azevedo 2017 | No prediction |
| Bae 2014 | No external validation of RCRI |
| Baer‐Bositis 2018 | No prediction |
| Bajaj 2013 | No prediction |
| Bakker 2012 | No prediction |
| Bakker 2013 | No prediction |
| Barisione 2016 | No prediction |
| Barrett 2007 | No prediction |
| Batsis 2009 | No prediction |
| Belmont 2014 | No external validation of RCRI |
| Bertges 2010 | No external validation of RCRI in the same cohort |
| Biccard 2007 | No prediction |
| Biccard 2010 | No prediction |
| Biccard 2012a | No external validation of RCRI |
| Biccard 2013 | Non‐original research (review, comment, guideline etc.) |
| Biccard 2014 | Non‐original research (review, comment, guideline etc.) |
| Biccard 2015 | Non‐original research (review, comment, guideline etc.) |
| Biteker 2011 | No prediction |
| Biteker 2011a | No prediction |
| Biteker 2012 | No prediction |
| Biteker 2014 | No prediction |
| Biteker 2014a | No prediction |
| Bolliger 2009 | No external validation of RCRI |
| Bolliger 2012 | No prediction |
| Borges 2013a | No external validation of the RCRI |
| Butt 2009 | No prediction |
| Calvillo‐King 2010 | No external validation of RCRI |
| Canter 2008 | No external validation of RCRI |
| Cassagneau 2012 | No external validation of RCRI |
| Chan 2018 | Other prediction model |
| Chang 2019 | No external validation of RCRI |
| Chen 2002 | No external validation of RCRI |
| Christiansen 2017 | No external validation of RCRI |
| Cicarelli 2001 | External validation only without added value or comparison |
| Cloney 2017 | No prediction |
| Cook 2017 | No external validation of RCRI |
| Crowther 2018 | No external validation of RCRI |
| Cullen 2020 | No external validation of RCRI |
| Cuthbertson 2007a | No external validation of RCRI |
| Cuthbertson 2007b | No external validation of RCRI |
| Davies 2015 | No prediction |
| Davies 2015a | No prediction |
| Davis 2018 | No prediction |
| de Campos 2012 | No external validation of RCRI |
| Dernellis 2006 | Other prediction model |
| Devereaux 2011 | External validation only without added value or comparison |
| de Virgilio 2009 | No prediction |
| Dover 2013 | External validation only without added value or comparison |
| Drake 2016 | No external validation of RCRI |
| Drudi 2016 | No external validation of RCRI |
| Duceppe 2018 | No external validation of RCRI |
| Duceppe 2019 | No external validation of RCRI |
| Edelmuth 2018 | No external validation of RCRI |
| Ekeloef 2017 | No prediction |
| Ekeloef 2020 | No external validation of RCRI |
| Ekeloef 2020a | Postoperative biomarker was evaluated |
| Erol 2019 | No prediction |
| Eyraud 2000 | No external validation of RCRI |
| Faggiano 2012 | No prediction |
| Fayad 2011 | No external validation of RCRI |
| Feringa 2006 | No prediction |
| Feringa 2006a | No prediction |
| Feringa 2007a | No external validation of RCRI |
| Feringa 2009 | No prediction |
| Ferrante 2018 | No external validation of the RCRI |
| Filipovic 2003 | No prediction |
| Filipovic 2005 | No external validation of RCRI |
| Flu 2009 | No external validation of RCRI |
| Flu 2010 | Other prediction model |
| Flu 2010a | No external validation of RCRI |
| Galal 2010 | No prediction |
| Garcia 2009 | External validation only without added value or comparison |
| Garcia 2013 | No external validation of RCRI |
| Ghadri 2012 | No external validation of RCRI |
| Ghazali 2017 | No external validation of RCRI |
| Gibson 2007 | No external validation of RCRI |
| Gillmann 2019 | No external validation of RCRI |
| Go 2017 | No external validation of RCRI |
| Goei 2009 | No external validation of RCRI |
| Goh 2000 | No external validation of RCRI |
| Gómez 2012 | No prediction |
| Goodman 2015 | No prediction |
| Gu 2018 | No prediction |
| Gundes 2017 | No prediction |
| Halm 2005 | No prediction |
| Halm 2009 | No prediction |
| Halm 2009a | No prediction |
| Hammill 2008 | No prediction |
| Hansen 2016 | No prediction |
| Hanss 2008 | RCRI was part of the inclusion criteria |
| Harland 2020 | No external validation of RCRI |
| Hawn 2013 | No prediction |
| Hennis 2012 | No external validation of RCRI |
| Hietala 2014 | No prediction |
| Hirano 2014 | No prediction |
| Hirpara 2019 | No external validation of RCRI |
| Hoeks 2007 | No prediction |
| Hoeks 2008 | No prediction |
| Hoeks 2009 | No prediction |
| Hoeks 2009a | No prediction |
| Hoeks 2010 | No external validation of RCRI |
| Hofer 2018 | Other prediction model |
| Hoftman 2013 | External validation only without added value or comparison |
| Hokari 2015 | Other prediction model |
| Holcomb 2016 | No prediction |
| Holcomb 2016a | No prediction |
| Hollis 2016 | No prediction |
| Huang 2017 | No prediction |
| Jakobson 2014 | No prediction |
| Kamber 2018 | No external validation of RCRI |
| Kanakaraj 2017 | Other prediction model |
| Karakas 2013 | Non‐original research (review, comment, guideline etc.) |
| Kazimierczak 2015 | Other prediction model |
| Kerry 2011 | Non‐original research (review, comment, guideline etc.) |
| Kertai 2004 | No prediction |
| Khambalia 2015 | No prediction |
| Kikura 2008 | No prediction |
| Kim 2013 | No prediction |
| Kim 2016 | No external validation of RCRI |
| Kim 2016a | No external validation of RCRI |
| Kim 2018 | No external validation of RCRI |
| Kim 2019 | No external validation of RCRI |
| Kistan 2018 | No external validation of RCRI |
| Koh 2012 | No prediction |
| Kougias 2013 | No prediction |
| Kougias 2017 | No prediction |
| Kronzer 2016 | Non‐original research (review, comment, guideline etc.) |
| Kronzer 2016a | No prediction |
| Kumar 2017 | No prediction |
| Küpper 2015 | Other prediction model |
| Ladha 2018 | No external validation of RCRI |
| Lau 2013 | No external validation of RCRI |
| Lee 1999 | Development study, external validation only without added value or comparison |
| Leibowitz 2009 | No prediction |
| Levitan 2016 | No prediction |
| Li 2016 | No external validation of RCRI |
| Licker 2011 | Other prediction model |
| Licker 2013 | No external validation of RCRI |
| Liem 2018 | No external validation of RCRI |
| Lin 2005 | No prediction |
| Lin 2016 | Other prediction model |
| Lin 2017 | No prediction |
| Lindenauer 2004 | No prediction |
| Lindenauer 2005 | No prediction |
| Liu 2013 | No external validation of RCRI |
| Lo 2014 | No prediction |
| Long 2016 | No prediction |
| Lucreziotti 2007 | No prediction |
| Lupei 2014 | No prediction |
| Maas 2007 | No external validation of RCRI |
| MacIntyre 2018 | No prediction |
| Mahmoud 2016 | No prediction |
| Mann 2020 | No external validation of RCRI |
| Marinho 2018 | No prediction |
| Marsman 2020 | No external validation of RCRI |
| Marston 2013 | No prediction |
| Martins 2011 | No external validation of RCRI |
| Mases 2014 | No prediction |
| Matsumoto 2016 | No prediction |
| May 2019 | No prediction |
| McIlroy 2015 | No prediction |
| Meershoek 2020 | No external validation of RCRI |
| Mendonca 2014 | No prediction |
| Mitropoulos 2006 | Other prediction model |
| Moitra 2011 | No external validation of RCRI |
| Moodley 2015 | No prediction |
| Moodley 2015a | No prediction |
| Mooney 2016 | No prediction |
| Moran 2008 | External validation only without added value or comparison |
| Moses 2018 | Other prediction model |
| Mureddu 2017 | Non‐original research (review, comment, guideline etc.) |
| Nagayoshi 2012 | No prediction |
| Nepogodiev 2015 | Non‐original research (review, comment, guideline etc.) |
| Noordzij 2010 | No external validation of RCRI |
| Noordzij 2015 | No external validation of RCRI |
| Nordling 2016 | No external validation of RCRI |
| Nutt 2012 | No external validation of RCRI |
| O'Neill 2016 | No prediction |
| Oberweis 2015 | No prediction |
| Ochroch 2006 | No prediction |
| Oliveros 2005 | No external validation of RCRI |
| Oscarsson 2009 | No external validation of RCRI |
| Oscarsson 2009a | No external validation of RCRI |
| Oshin 2013 | No prediction |
| Padayachee 2018 | No prediction |
| Paladugu 2020 | Non‐original research (review, comment, guideline etc.) |
| Parente 2013 | No prediction |
| Parikh 2020 | No external validation of RCRI |
| Park 2018 | No external validation of RCRI |
| Patel 2018 | No prediction |
| Patorno 2015 | No prediction |
| Patorno 2016 | No prediction |
| Payne 2011 | No external validation of RCRI |
| Payne 2013 | External validation only without added value or comparison |
| Pereira 2016 | No external validation of RCRI |
| Pili‐Floury 2012 | No external validation of RCRI |
| Pinho 2016 | No prediction |
| Puelacher 2018 | No prediction |
| Rajagopalan 2008 | No external validation of RCRI |
| Rao 2012 | External validation only without added value or comparison |
| Redman 2014 | No prediction |
| Reeh 2016 | No prediction |
| Reeve 2018 | No prediction |
| Reis 2018 | No external validation of RCRI |
| Richards 2015 | No prediction |
| Richardson 2018 | No external validation of RCRI |
| Rinfret 2004 | No prediction |
| Rodriguez 2018 | No prediction |
| Rodseth 2014 | No external validation of RCRI |
| Rosenberg 2016 | No prediction |
| Roshanov 2017 | Non‐original research (review, comment, guideline etc.) |
| Roxburgh 2011 | No prediction |
| Sakuma 2010 | No prediction |
| Salinas 2012 | No prediction |
| Sankar 2014 | Other prediction model |
| Sankar 2019 | No external validation of RCRI |
| Schier 2012 | No external validation of RCRI |
| Schier 2013 | No prediction |
| Shalaeva 2016 | No external validation of RCRI |
| Silva 2020 | No prediction |
| Simeoni 2016 | No prediction |
| Skaro 2016 | No prediction |
| Smilowitz 2016 | No prediction |
| Smilowitz 2018 | No prediction |
| Smolock 2012 | No prediction |
| Snowden 2010 | No external validation of RCRI |
| Snowden 2013 | No external validation of RCRI |
| Sousa 2016 | No prediction |
| Stevens 2017 | No prediction |
| Sunny 2018 | External validation only without added value or comparison |
| Tao 2008 | Other prediction model |
| Tashiro 2014 | External validation only without added value or comparison |
| Tavakoli 2009 | Other prediction model |
| Teixeira 2014 | No prediction |
| Toda 2018 | No prediction |
| Tong 2015 | Wrong population |
| Toyonaga 2017 | No external validation of RCRI |
| Valentijn 2013 | No prediction |
| Valentijn 2013a | No prediction |
| van Kuijk 2009 | No prediction |
| Vanniyasingam 2016 | No external validation of RCRI |
| van Waes 2017 | Postoperative biomarker measurement |
| Vanwagner 2012 | No prediction |
| VanWagner 2014 | No external validation of RCRI |
| Veiga 2012 | No prediction |
| Venkatraghavan 2015 | No prediction |
| Vetrugno 2018 | Non‐original research (review, comment, guideline etc.) |
| Waliszek 2011 | No prediction |
| Ward 2006 | No prediction |
| Warnakulasuriya 2017 | No prediction |
| Weissman 2011 | No external validation of RCRI |
| Widmer 2018 | No prediction |
| Wijeysundera 2010 | No prediction |
| Wijeysundera 2011 | No prediction |
| Wijeysundera 2012 | No prediction |
| Wijeysundera 2020 | No external validation of RCRI |
| Wilson 2010 | No external validation of RCRI |
| Xara 2015 | No external validation of RCRI |
| Yun 2008 | No external validation of RCRI |
| Yurtlu 2016 | No prediction |
RCRI: Revised Cardiac Risk Index
Characteristics of studies awaiting classification [ordered by study ID]
Alexander 2008.
| Notes | No full text available |
Andreenko 2003.
| Notes | No full text available |
Author unknown 2010.
| Notes | No full text available |
Author unknown 2011.
| Notes | No full text available |
Barbarash 2012.
| Notes | No full text available |
Can 2018.
| Notes | No full text available |
Caruso 2006.
| Notes | No full text available |
Dobrushina 2012.
| Notes | No full text available |
Domínguez 2014.
| Notes | No full text available |
Faris 1999.
| Notes | No full text available |
Ghorra 1999.
| Notes | No full text available |
Gnocchi 2000.
| Notes | No full text available |
Grabowska‐Gawel 2004.
| Notes | No full text available |
Kapma 2017.
| Notes | No full text available |
Kavarana 2003.
| Notes | No full text available |
Kertai 2003.
| Notes | No full text available |
Khan 2010.
| Notes | No full text available |
Khoronenko 2009.
| Notes | No full text available |
Kim 2017.
| Notes | No full text available |
Knaak 2020.
| Notes | No full text available |
Kozlov 2016.
| Notes | No full text available |
Kuznetsov 2018.
| Notes | No full text available |
Law 2014.
| Notes | No full text available |
Leo 2005.
| Notes | No full text available |
Li 2016a.
| Notes | No full text available |
Li 2018.
| Notes | No full text available |
Macan 2004.
| Notes | No full text available |
Martinez 2018.
| Notes | No full text available |
Maruoka 2018.
| Notes | No full text available |
Moodley 2018.
| Notes | No full text available |
Mori 2014.
| Notes | No full text available |
Peretich (year of publication unknown).
| Notes | No full text available |
Ray 2013.
| Notes | No full text available |
Shevchenko 2005.
| Notes | No full text available |
Stelzner 2003.
| Notes | No full text available |
Sumin 2012.
| Notes | No full text available |
Sumin 2013.
| Notes | No full text available |
Vanzetto 1999.
| Notes | No full text available |
Wolf 2001.
| Notes | No full text available |
Wunderlich 2005.
| Notes | No full text available |
Yamada 2019.
| Notes | No full text available |
Yi 2015.
| Notes | No full text available |
Zarich 2001.
| Notes | No full text available |
Characteristics of ongoing studies [ordered by study ID]
CTRI/2019/02/017668.
| Study name | To predict 30‐day in hospital mortality and morbidity using preoperative hand grip strength and comparing it with existing Revised Cardiac Risk Index and Modified Frailty Index |
| Starting date | February 2019 |
| Contact information | Kompal Jain, Department of Anaesthesia and Intensive Care, Government Medical College and Hospital, Sector ‐ 32, Chandigarh, India |
| Notes | To predict 30‐day in hospital mortality and morbidity using preoperative hand grip strength and comparing it with existing Revised Cardiac Risk Index and Modified Frailty Index |
NCT01280253.
| Study name | Preoperative biochemical predictors of outcome in patients with hip fracture |
| Starting date | January 2011 |
| Contact information | Peter Bentzer, MD, PhD, Skane University Hospital |
| Notes | The objective of the study is to identify biochemical predictors of morbidity and mortality in patients suffering from hip fracture. Biochemical predictors include pro‐brain natriuretic peptide, lactate, pro‐calcitonin, adrenomedullin, copeptin, cystatin c. The predictive value of the potential markers will be compared to that of ASA, RCRI and POSSUM. |
NCT02146560.
| Study name | TEAMS (Troponin Elevation After Major Surgery) Study (TEAMS) |
| Starting date | August 2014 |
| Contact information | University Health Network, Toronto |
| Notes | This study will compare postoperative health‐related
quality of life of patients who did or did not
experience perioperative myocardial injury (defined
by troponin‐I > 0.07 ng/ml) after noncardiac
surgery. Clinically based risk stratification tools used in noncardiac surgery (e.g. Revised Cardiac Risk Index) are of moderate utility and assign patients only to broad risk categories. This study will examine the usefulness of pre‐operative biomarkers (BNP, HbA1c and others) in supporting cardiac risk stratification and will address the question: Is there a set of preoperative criteria that can accurately inform the decision to monitor troponin postoperatively? |
NCT02860754.
| Study name | The prognostic capabilities of a preoperative six‐minute walk test to independently inform cardiovascular risk after major noncardiac surgery |
| Starting date | August 2016 |
| Contact information | Amal Bessissow, MD, McGill University Health Centre/Research Institute of the McGill University Health Centre |
| Notes | This prospective cohort study aims to determine whether the addition of the 6MWT to the RCRI score improves the risk prediction of postoperative cardiovascular outcomes after noncardiac surgery. In addition, this study will assess whether the patients' reported MET score corresponds to the determined MET score from the 6MWT distance completed. |
NCT03016936.
| Study name | MET: REevaluation for Perioperative cArdIac Risk (MET‐REPAIR) |
| Starting date | 1 August 2017 |
| Contact information | Giovanna Lurati Buse, PD Dr, University Hospital, Düsseldorf, Germany |
| Notes | Multicentre international prospective cohort study
designed to answer the question: "In patients
undergoing elevated risk noncardiac surgery, are
METs estimated by questionnaire associated with
perioperative major adverse cardiovascular events or
cardiovascular mortality?" If so:
MET‐REPAIR will examine the ability of MET estimated using a questionnaire to predict perioperative cardiovascular events correcting for preoperative risk factors, (e.g. comorbidity and type of surgery) and calculate the effect on risk stratification (net reclassification improvement) by the addition of METs estimated by questionnaire to established risk scores, such as the Revised Cardiac Risk Score (Lee‐index) and the NSQIP MICA. |
NCT03436238.
| Study name | Myocardial Injury in Noncardiac Surgery in Sweden (MINSS) |
| Starting date | 15 May 2017 |
| Contact information | Michelle Chew, Professor, Senior Consultant, Linkoeping University |
| Notes | The purpose of this multicentre, prospective,
observational study is to identify robust
biochemical markers that predict adverse
cardiovascular outcomes and mortality in patients
undergoing major abdominal surgery. Plasma levels of hsTnT, NTproBNP, copeptin, MR‐proADM and CT‐proET1 will be measured. Receiver operating curve analysis will be used to determine the optimal threshold of each biomarker in predicting mortality/MACCE. The net reclassification index will be used to assess if biomarkers confer added value to the RCRI for the classification of MACCE. |
6MWT: six‐minute walk test; ASA: American Society of Anesthesiologists; BNP: brain natriuretic peptide; MACCE: major adverse cardiac and cerebrovascular events; MET: metabolic equivalents; MICA: myocardial infarction or cardiac arrest; NSQIP: National Surgical Quality Improvement; POSSUM: Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity; RCRI: Revised Cardiac Risk Index
Differences between protocol and review
Several differences between the protocol and review should be addressed:
Initially, we aimed to identify all biomarkers that were compared or added to the RCRI to improve risk prediction. As we found many studies that compared the RCRI to a new or existing prediction model, we added a third aim that specifically focused on the comparison of the predictive performance of the RCRI to other prediction models.
Conference proceedings for abstracts were eventually not searched, because the lack of information would not allow us to perform a risk of bias assessment.
The review protocol stated that we would include studies reporting on patients of all ages, however we eventually selected studies including only adult patients (≥ 18 years). As the RCRI has been developed for patients ≥ 50 years, we do not expect to have missed studies that reported on patients < 18 years.
In the protocol, we stated that PubMed would be searched to check for any comments or retractions, however we only searched the Retraction Watch Database for retractions. We used PubMed to identify new studies during the cross‐referencing procedure.
In contrast with the protocol, selection of studies based on full text assessment was performed in two stages. In the first step, one review author assessed whether the RCRI was mentioned in the 'Results' and/or 'Methods' section of the article. This was done by searching for the terms 'RCRI' or often used synonyms, i.e. 'revised Goldman index' and 'Lee index', or by searching where in the report the original paper was referenced. If this was not the case, these articles were excluded. The remaining studies were screened for inclusion in the review as planned. We planned to contact the original investigators to provide this missing information in case of any missing data about the predictive performance measures of the RCRI, extended RCRI and other prediction models. However, we concluded that contacting authors for missing information would not lead to different review findings as we encountered large heterogeneity in the study population, outcome definitions, prediction horizons and studied biomarkers or prediction models.
We planned to perform a meta‐analysis of the predictive performance of the RCRI model only as compared to the RCRI with the biomarker(s) added, across the various RCRI validation studies. However, this turned out to be impossible due to the low number of studies reporting on the added value of the same biomarker, and due to the differences in included study populations and in outcome definitions between these RCRI validation studies. Meta‐analysis of the c‐statistic was also planned for the studies that compared the RCRI to biomarkers alone (objective 2), where there were at least three studies reporting on the same biomarker for predicting a similar outcome (using a similar definition), with a similar prediction horizon and scale on how the biomarker was studied. As there was no set of studies fulfilling these criteria, meta‐analysis of the c‐statistic for objective 2 also turned out to be not possible. Finally, meta‐analysis of the c‐statistics was also not possible for objective 3 for the same reason. Instead, the performance measures (c‐statistic) for RCRI models extended with biomarkers that were studied in at least three studies were presented in forest plots, without presenting a pooled estimate.
Several subgroup analyses were planned, including vascular surgery patients versus other noncardiac surgery patients, elective versus emergency surgery, different prediction horizons and patients in different age categories. For the same reasons as mentioned above, meta‐analysis in these subgroups was not possible. Again, we stratified the forest plots according to the subgroups based on outcome, and reported the prediction horizon in the plot.
Sensitivity analyses excluding studies with high risk of bias (at least four domains judged to be 'high') and excluding unpublished studies and studies with missing data were planned but not performed due to the large heterogeneity between studies.
We planned a summary of findings table using GRADE to present the body of evidence for the included prognostic studies. However, GRADE guidance for grading the certainty of results from prognostic model studies is currently not available.
Contributions of authors
Lisette M Vernooij: protocol development, screening and selection of studies, development of data extraction form and data extraction, characteristics of studies, risk of bias assessment, statistical analysis, writing and drafting of the review, communication with and between authors.
Wilton A van Klei: medical and content input.
Karel G Moons: methodological, statistical and content input.
Toshihiko Takada: selection of studies, data extraction, risk of bias assessment.
Judith AR van Waes: selection of studies, data extraction, risk of bias assessment, medical and content input.
Johanna AAG Damen: screening and selection of studies, data extraction, risk of bias assessment, methodological, statistical and content input.
Sources of support
Internal sources
No sources of support provided
External sources
-
NIHR, UK
This project was supported by the NIHR via Cochrane Infrastructure funding to the Heart Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care.
Declarations of interest
Lisette M Vernooij: none known.
Wilton A van Klei: none known.
Karel G Moons: none known.
Toshihiko Takada: none known.
Judith AR van Waes: none known.
Johanna A Damen: none known.
New
References
References to studies included in this review
Adar 2019 {published data only}
- Adar A, Onalan O, Cakan F, Akbay E, Colluoglu T, Dasar U, et al. A strong and reliable indicator for early postoperative major cardiac events after elective orthopedic surgery: aortic arch calcification. Heart and Lung 2019;48(5):446-51. [DOI] [PubMed] [Google Scholar]
Ahn 2013 {published data only}
- Ahn JH, Park JR, Min JH, Sohn JT, Hwang SJ, Park Y, et al. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgery. Journal of the American College of Cardiology 2013;61(6):661-8. [DOI] [PubMed] [Google Scholar]
Ahn 2020 {published data only}
- Ahn JH, Jeong YH, Park Y, Kwak CH, Jang JY, Hwang JY, et al. Head-to-head comparison of prognostic accuracy in patients undergoing noncardiac surgery of dobutamine stress echocardiography versus computed tomography coronary angiography (PANDA trial): a prospective observational study. Journal of Cardiovascular Computed Tomography 2020;14(6):471-7. [DOI] [PubMed] [Google Scholar]
Alrezk 2017 {published data only}
- Alrezk R, Jackson N, Al Rezk M, Elashoff R, Weintraub N, Elashoff D, et al. Derivation and validation of a geriatric-sensitive perioperative cardiac risk index. Journal of the American Heart Association 2017;6(11):e006648. [DOI] [PMC free article] [PubMed] [Google Scholar]
Archan 2010 {published data only}
- Archan S, Roscher CR, Fairman RM, Fleisher LA. Revised cardiac risk index (Lee) and perioperative cardiac events as predictors of long-term mortality in patients undergoing endovascular abdominal aortic aneurysm repair. Journal of Cardiothoracic and Vascular Anesthesia 2010;24(1):84-90. [DOI] [PubMed] [Google Scholar]
Asuzu 2018 {published data only}
- Asuzu DT, Chao GF, Pei KY. Revised cardiac risk index poorly predicts cardiovascular complications after adhesiolysis for small bowel obstruction. Surgery 2018;164(6):1198-203. [DOI] [PubMed] [Google Scholar]
Avena 2015 {published data only}
- Avena Smeili LA, Lotufo PA. Incidence and predictors of cardiovascular complications and death after vascular surgery. Arquivos Brasileiros De Cardiologia 2015;105(5):510-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bae 2012 {published data only}
- Bae MH, Choi WS, Kim KH, Park SH, Kim HW, Lee JH, et al. The implications of a fragmented QRS complex and newly reclassified revised cardiac risk index including fragmented QRS in patients undergoing non-cardiac vascular surgery. International Journal of Cardiology 2012;157(2):276-8. [DOI] [PubMed] [Google Scholar]
Bae 2013 {published data only}
- Bae MH, Jang SY, Choi WS, Kim KH, Park SH, Lee JH, et al. A new revised cardiac risk index incorporating fragmented QRS complex as a prognostic marker in patients undergoing noncardiac vascular surgery. American Journal of Cardiology 2013;112(1):122-7. [DOI] [PubMed] [Google Scholar]
Biccard 2011 {published data only}
- Biccard BM, Naidoo P. The role of brain natriuretic peptide in prognostication and reclassification of risk in patients undergoing vascular surgery. Anaesthesia 2011;66(5):379-85. [DOI] [PubMed] [Google Scholar]
Biccard 2012 {published data only}
- Biccard BM, Naidoo P, Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia 2012;67(4):389-95. [DOI] [PubMed] [Google Scholar]
Binh 2019 {published data only}
- Binh TQ, Trang DV, Vuong NL, Khoi NV, Elfaituri MK, Huu Loc TT, et al. NT-proBNP incorporated in prediction rule of major peri-operative adverse cardiac event in non-cardiac surgery. Surgeon Journal of the Royal Colleges of Surgeons of Edinburgh & Ireland 2019;17(3):127-32. [DOI] [PubMed] [Google Scholar]
Boersma 2001 {published data only}
- Boersma E, Poldermans D, Bax JJ, Steyerberg EW, Thomson IR, Banga JD, et al. Predictors of cardiac events after major vascular surgery - role of clinical characteristics, dobutamine echocardiography, and beta-blocker therapy. JAMA 2001;285(14):1865-73. [DOI] [PubMed] [Google Scholar]
Boersma 2005 {published data only}
- Boersma E, Kertai MD, Schouten O, Bax JJ, Noordzij P, Steyerberg EW, et al. Perioperative cardiovascular mortality in noncardiac surgery: validation of the Lee cardiac risk index. American Journal of Medicine 2005;118(10):1134-41. [DOI] [PubMed] [Google Scholar]
Borges 2013 {published data only}
- Borges FK, Furtado MV, Webber RA, Bertoluci C, Gonzalez VL, Bertoldi EG, et al. Prognostic value of perioperative N-terminal pro-B-type natriuretic peptide in noncardiac surgery. Arquivos Brasileiros De Cardiologia 2013;100(6):561-70. [DOI] [PubMed] [Google Scholar]
Bronheim 2018 {published data only}
- Bronheim RS, Oermann EK, Bronheim DS, Caridi JM. Revised cardiac risk index as a predictor for myocardial infarction and cardiac arrest following posterior lumbar decompression. Spine 2019;44(3):E187-93. [DOI] [PubMed] [Google Scholar]
- Bronheim RS, Oermann EK, Bronheim DS, Caridi JM. Revised cardiac risk index vs. ASA status as a predictor for non-cardiac events following posterior lumbar decompression. World Neurosurgery 2018;120:e1175-84. [DOI] [PubMed] [Google Scholar]
Brunelli 2010 {published data only}
- Brunelli A, Varela G, Salati M, Jimenez MF, Pompili C, Novoa N, et al. Recalibration of the revised cardiac risk index in lung resection candidates. Annals of Thoracic Surgery 2010;90(1):199-203. [DOI] [PubMed] [Google Scholar]
Bryce 2012 {published data only}
- Bryce GJ, Payne CJ, Gibson SC, Kingsmore DB, Byrne DS, Delles C. Risk stratification scores in elective open abdominal aortic aneurysm repair: are they suitable for preoperative decision making? European Journal of Vascular and Endovascular Surgery 2012;44(1):55-61. [DOI] [PubMed] [Google Scholar]
Canbolat 2018 {published data only}
- Canbolat IP, Erdogan Y, Adali G, Kaplan O, Dayangac M, Yuzer Y, et al. The predictive value of risk indices for cardiac complications in living donor liver transplantation. Bratislava Medical Journal-Bratislavske Lekarske Listy 2018;119(5):289-93. [DOI] [PubMed] [Google Scholar]
Carabini 2014 {published data only}
- Carabini LM, Zeeni C, Moreland NC, Gould RW, Hemmer LB, Bebawy JF, et al. Predicting major adverse cardiac events in spine fusion patients. Spine 2014;39(17):1441-8. [DOI] [PubMed] [Google Scholar]
Che 2018 {published data only}
- Che L, Xu L, Huang Y, Yu C. Clinical utility of the revised cardiac risk index in older Chinese patients with known coronary artery disease. Clinical Interventions in Aging 2018;13:35-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cho 2020 {published data only}
- Cho MS, Lee CH, Kim J, Ahn JM, Han M, Nam GB, et al. Clinical implications of preoperative nonvalvular atrial fibrillation with respect to postoperative cardiovascular outcomes in patients undergoing non-cardiac surgery. Sunhwangi 2020;50(2):148-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
Choi 2010 {published data only}
- Choi JH, Cho DK, Song YB, Hahn JY, Choi S, Gwon HC, et al. Preoperative NT-proBNP and CRP predict perioperative major cardiovascular events in non-cardiac surgery. Heart 2010;96(1):56-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cohn 2018 {published data only}
- Cohn SL, Fernandez RN. Comparison of 4 cardiac risk calculators in predicting postoperative cardiac complications after noncardiac operations. American Journal of Cardiology 2018;121(1):125-30. [DOI] [PubMed] [Google Scholar]
Cuthbertson 2007 {published data only}
- Cuthbertson BH, Almiri AR, Croal BL, Rajagopalan S, Alozairi O, Brittenden J, et al. Utility of B-type natriuretic peptide in predicting perioperative cardiac events in patients undergoing major non-cardiac surgery. British Journal of Anaesthesia 2007;99(2):170-6. [DOI] [PubMed] [Google Scholar]
Dakik 2019 {published data only}
- Dakik HA, Chehab O, Eldirani M, Sbeity E, Karam C, Abou Hassan O, et al. A new index for pre-operative cardiovascular evaluation. Journal of the American College of Cardiology 2019;73(24):3067-78. [DOI] [PubMed] [Google Scholar]
Dakik 2020 {published data only}
- Dakik HA, Sbaity E, Msheik A, Kaspar C, Eldirani M, Chehab O, et al. AUB-HAS2 cardiovascular risk index: performance in surgical subpopulations and comparison to the revised cardiac risk index. Journal of the American Heart Association 2020;9(10):e016228. [DOI] [PMC free article] [PubMed] [Google Scholar]
Datema 2010 {published data only}
- Datema FR, Poldermans D, Baatenburg de Jong RJ. Incidence and prediction of major cardiovascular complications in head and neck surgery. Head and Neck-Journal for the Sciences and Specialties of the Head and Neck 2010;32(11):1485-93. [DOI] [PubMed] [Google Scholar]
Davis 2013 {published data only}
- Davis C, Tait G, Carroll J, Wijeysundera DN, Beattie WS. The revised cardiac risk index in the new millennium: a single-centre prospective cohort re-evaluation of the original variables in 9,519 consecutive elective surgical patients. Canadian Journal of Anesthesia-Journal Canadien D Anesthesie 2013;60(9):855-63. [DOI] [PubMed] [Google Scholar]
Dhillon 2018 {published data only}
- Dhillon AK, Disque AA, Nguyen-Buckley CT, Grogan TR, Russell DL, Gritsch HA, et al. Does a low 6-minute walk distance predict elevated postoperative troponin? Anesthesia and Analgesia 2018;127(2):E1-E3. [DOI] [PubMed] [Google Scholar]
Dillon 2011 {published data only}
- Dillon JK, Liu SY, Patel CM, Schmidt BL. Identifying risk factors for postoperative cardiovascular and respiratory complications after major oral cancer surgery. Head and Neck-Journal for the Sciences and Specialties of the Head and Neck 2011;33(1):112-6. [DOI] [PubMed] [Google Scholar]
Douville 2020 {published data only}
- Douville NJ, Surakka I, Leis A, Douville CB, Hornsby WE, Brummett CM, et al. Use of a polygenic risk score improves prediction of myocardial injury after non-cardiac surgery. Circulation. Genomic and Precision Medicine 2020;13(4):e002817. [DOI] [PMC free article] [PubMed] [Google Scholar]
Duceppe 2020 {published data only}
- Duceppe E, Patel A, Chan MT, Berwanger O, Ackland G, Kavsak P, et al. Preoperative n-terminal pro-b-type natriuretic peptide and cardiovascular events after noncardiac surgery: a cohort study. Annals of Internal Medicine 2020;172(2):96-104. [DOI] [PubMed] [Google Scholar]
Dunn 2019 {published data only}
- Dunn CP, Emeasoba EU, Holtzman AJ, Hung M, Kaminetsky J, Alani O, et al. Comparing the predictive power of preoperative risk assessment tools to best predict major adverse cardiac events in kidney transplant patients. Surgery Research & Practice Print 2019;2019:9080856. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ehlert 2016 {published data only}
- Ehlert BA, Najafian A, Orion KC, Malas MB, Black JH III, Abularrage CJ. Validation of a modified Frailty Index to predict mortality in vascular surgery patients. Journal of Vascular Surgery 2016;63(6):1595-601.e2. [DOI] [PubMed] [Google Scholar]
Farina‐Castro 2020 {published data only}
- Farina-Castro R, Roque-Castellano C, Artiles-Armas M, Conde-Martel A, Marchena-Gomez J. Usefulness of pre- and intraoperative risk scores in nonagenarian surgical patients. Journal of Anesthesia 2020;34(5):650-7. [DOI] [PubMed] [Google Scholar]
Feringa 2007 {published data only}
- Feringa HH, Schouten O, Dunkelgrun M, Bax JJ, Boersma E, Elhendy A, et al. Plasma N-terminal pro-B-type natriuretic peptide as long-term prognostic marker after major vascular surgery. Heart 2007;93(2):226-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ferrante 2019 {published data only}
- Ferrante AM, Moscato U, Snider F, Tshomba Y. Controversial results of the Revised Cardiac Risk Index in elective open repair of abdominal aortic aneurysms: Retrospective analysis on a continuous series of 899 cases. International Journal of Cardiology 2019;277:224-8. [DOI] [PubMed] [Google Scholar]
Fisher 2008 {published data only}
- Fisher BW, Ramsay G, Majumdar SR, Hrazdil CT, Finegan BA, Padwal RS, et al. The ankle-to-arm blood pressure index predicts risk of cardiac complications after noncardiac surgery. Anesthesia and Analgesia 2008;107(1):149-54. [DOI] [PubMed] [Google Scholar]
Fronczek 2019 {published data only}
- Fronczek J, Polok K, Devereaux PJ, Gorka J, Archbold RA, Biccard B, et al. External validation of the Revised Cardiac Risk Index and National Surgical Quality Improvement Program Myocardial Infarction and Cardiac Arrest calculator in noncardiac vascular surgery. British Journal of Anaesthesia 2019;123(4):421-9. [DOI] [PubMed] [Google Scholar]
Gillmann 2014 {published data only}
- Gillmann HJ, Meinders A, Grosshennig A, Larmann J, Buente C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Critical Care Medicine 2014;42(6):1498-506. [DOI] [PubMed] [Google Scholar]
Glance 2018 {published data only}
- Glance LG, Faden E, Dutton RP, Lustik SJ, Li Y, Eaton MP, et al. Impact of the choice of risk model for identifying low-risk patients using the 2014 American college of cardiology/American Heart Association perioperative guidelines. Anesthesiology 2018;129(5):889-900. [DOI] [PubMed] [Google Scholar]
Golubovic 2018 {published data only}
- Golubovic M, Peric V, Stanojevic D, Lazarevic M, Jovanovic N, Ilic N, et al. Potential new approaches in predicting adverse cardiac events one month after major vascular surgery. Medical Principles & Practice 2019;28(1):63-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Golubovic M, Stanojevic D, Lazarevic M, Peric V, Kostic T, Djordjevic M, et al. A risk stratification model for cardiovascular complications during the 3-month period after major elective vascular surgery. Biomed Research International 2018;2018:4381527. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gualandro 2017 {published data only}
- Gualandro DM, Puelacher C, LuratiBuse G, Llobet GB, Yu PC, Cardozo FA, et al. Prediction of major cardiac events after vascular surgery. Journal of Vascular Surgery 2017;66(6):1826-35.e1. [DOI] [PubMed] [Google Scholar]
Gualandro 2018 {published data only}
- Gualandro DM, Puelacher C, LuratiBuse G, Lampart A, Strunz C, Cardozo FA, et al. Comparison of high-sensitivity cardiac troponin I and T for the prediction of cardiac complications after non-cardiac surgery. American Heart Journal 2018;203:67-73. [DOI] [PubMed] [Google Scholar]
Gupta 2011 {published data only}
- Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011;124(4):381-7. [DOI] [PubMed] [Google Scholar]
Handke 2019 {published data only}
- Handke J, Scholz AS, Gillmann HJ, Janssen H, Dehne S, Arens C, et al. Elevated presepsin is associated with perioperative major adverse cardiovascular and cerebrovascular complications in elevated-risk patients undergoing noncardiac surgery: the leukocytes and cardiovascular perioperative events study. Anesthesia & Analgesia 2019;128(6):1344-53. [DOI] [PubMed] [Google Scholar]
Handke 2020 {published data only}
- Handke J, Scholz AS, Dehne S, Krisam J, Gillmann HJ, Janssen H, et al. Presepsin (sCD14-ST) for pre-operative prediction of major adverse cardiovascular events in coronary heart disease patients undergoing noncardiac surgery: post hoc analysis of the Leukocytes and Cardiovascular Peri-operative Events-2 (LeukoCAPE-2) Study. European Journal of Anaesthesiology 2020;37(10):908-19. [DOI] [PubMed] [Google Scholar]
Hwang 2015 {published data only}
- Hwang J, Kim EK, Yang JH, Chang SA, Bin SY, Hahn JY, et al. Assessment of perioperative cardiac risk of patients undergoing noncardiac surgery using coronary computed tomographic angiography. Circulation-Cardiovascular Imaging 2015;8(3):e002582. [DOI] [PubMed] [Google Scholar]
James 2014 {published data only}
- James S, Jhanji S, Smith A, O'Brien G, Fitzgibbon M, Pearse RM. Comparison of the prognostic accuracy of scoring systems, cardiopulmonary exercise testing, and plasma biomarkers: a single-centre observational pilot study. British Journal of Anaesthesia 2014;112(3):491-7. [DOI] [PubMed] [Google Scholar]
Jarai 2011 {published data only}
- Jarai R, Mahla E, Perkmann T, Jarai R, Archan S, Tentzeris I, et al. Usefulness of pre-operative copeptin concentrations to predict post-operative outcome after major vascular surgery. American Journal of Cardiology 2011;108(8):1188-95. [DOI] [PubMed] [Google Scholar]
Karkos 2002 {published data only}
- Karkos CD, Thomson GJ, Hughes R, Hollis S, Hill JC, Mukhopadhyay US. Prediction of cardiac risk before abdominal aortic reconstruction: comparison of a revised Goldman Cardiac Risk Index and radioisotope ejection fraction. Journal of Vascular Surgery 2002;35(5):943-9. [DOI] [PubMed] [Google Scholar]
Katsanos 2015 {published data only}
- Katsanos S, Babalis D, Kafkas N, Mavrogenis A, Leong D, Parissis J, et al. B-type natriuretic peptide vs. cardiac risk scores for prediction of outcome following major orthopedic surgery. Journal of Cardiovascular Medicine 2015;16(6):465-71. [DOI] [PubMed] [Google Scholar]
Kaw 2019 {published data only}
- Kaw R, Nagarajan V, Jaikumar L, Halkar M, Mohananey D, Hernandez AV, et al. Predictive value of stress testing, revised cardiac risk index, and functional status in patients undergoing noncardiac surgery. Journal of Cardiothoracic & Vascular Anesthesia 2019;33(4):927-32. [DOI] [PubMed] [Google Scholar]
Kertai 2005 {published data only}
- Kertai MD, Boersma E, Klein J, Urk H, Poldermans D. Optimizing the prediction of perioperative mortality in vascular surgery by using a customized probability model. Archives of Internal Medicine 2005;165(8):898-904. [DOI] [PubMed] [Google Scholar]
Kopec 2017 {published data only}
- Kopec M, Duma A, Helwani MA, Brown J, Brown F, Gage BF, et al. Improving prediction of postoperative myocardial infarction with high-sensitivity cardiac troponin T and NT-proBNP. Anesthesia and Analgesia 2017;124(2):398-405. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kumar 2001 {published data only}
- Kumar R, McKinney WP, Raj G, Heudebert GR, Heller HJ, Koetting M, et al. Adverse cardiac events after surgery - assessing risk in a veteran population. Journal of General Internal Medicine 2001;16(8):507-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
Leibowitz 2008 {published data only}
- Leibowitz D, Planer D, Rott D, Elitzur Y, Chajek-Shaul T, Weiss AT. Brain natriuretic peptide levels predict perioperative events in cardiac patients undergoing noncardiac surgery: a prospective study. Cardiology 2008;110(4):266-70. [DOI] [PubMed] [Google Scholar]
Makary 2010 {published data only}
- Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. Journal of the American College of Surgeons 2010;210(6):901-8. [DOI] [PubMed] [Google Scholar]
Markovic 2018 {published data only}
- Markovic D, Jevtovic-Stoimenov T, Stojanovic M, Vukovic A, Dinic V, Markovic-Zivkovic B, et al. Addition of clinical risk scores improves prediction performance of American Society of Anesthesiologists (ASA) physical status classification for postoperative mortality in older patients: a pilot study. European Geriatric Medicine 2018;9(1):51-9. [DOI] [PubMed] [Google Scholar]
- Markovic DZ, Jevtovic-Stoimenov T, Cosic V, Stosic B, Zivkovic BM, Jankovic RJ. Addition of biomarker panel improves prediction performance of American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) calculator for cardiac risk assessment of elderly patients preparing for major non-cardiac surgery: a pilot study. Aging Clinical and Experimental Research 2018;30(5):419-31. [DOI] [PubMed] [Google Scholar]
Mauermann 2016 {published data only}
- Mauermann E, Bolliger D, Seeberger E, Puelacher C, Corbiere S, Filipovic M, et al. Incremental value of preoperative copeptin for predicting myocardial injury. Anesthesia and Analgesia 2016;123(6):1363-71. [DOI] [PubMed] [Google Scholar]
McAlister 2015 {published data only}
- McAlister FA, Jacka M, Graham M, Youngson E, Cembrowski G, Bagshaw SM, et al. The prediction of postoperative stroke or death in patients with preoperative atrial fibrillation undergoing non-cardiac surgery: a VISION sub-study. Journal of Thrombosis and Haemostasis 2015;13(10):1768-75. [DOI] [PubMed] [Google Scholar]
McAlister 2020 {published data only}
- McAlister FA, Youngson E, Jacka M, Graham M, Conen D, Chan M, et al. A comparison of four risk models for the prediction of cardiovascular complications in patients with a history of atrial fibrillation undergoing non-cardiac surgery. Anaesthesia 2020;75(1):27-36. [DOI] [PubMed] [Google Scholar]
McIlroy 2014 {published data only}
- McIlroy DR, Chan MT, Wallace SK, Symons JA, Koo EG, Chu LC, et al. Automated preoperative assessment of endothelial dysfunction and risk stratification for perioperative myocardial injury in patients undergoing non-cardiac surgery. British Journal of Anaesthesia 2014;112(1):47-56. [DOI] [PubMed] [Google Scholar]
Mercantini 2012 {published data only}
- Mercantini P, Di Somma S, Magrini L, Nava AK, Scarinci A, La Torre M, et al. Preoperative brain natriuretic peptide (BNP) is a better predictor of adverse cardiac events compared to preoperative scoring system in patients who underwent abdominal surgery. World Journal of Surgery 2012;36(1):24-30. [DOI] [PubMed] [Google Scholar]
Moodley 2013 {published data only}
- Moodley Y, Naidoo P, Biccard BM. The South African Vascular Surgical Cardiac Risk Index (SAVS-CRI): a prospective observational study. Samj South African Medical Journal 2013;103(10):746-50. [DOI] [PubMed] [Google Scholar]
Neary 2007 {published data only}
- Neary WD, Prytherch D, Foy C, Heather BP, Earnshaw JJ. Comparison of different methods of risk stratification in urgent and emergency surgery. British Journal of Surgery 2007;94(10):1300-5. [DOI] [PubMed] [Google Scholar]
Noordzij 2006 {published data only}
- Noordzij PG, Boersma E, Bax JJ, Feringa HH, Schreiner F, Schouten O, et al. Prognostic value of routine preoperative electrocardiography in patients undergoing noncardiac surgery. American Journal of Cardiology 2006;97(7):1103-6. [DOI] [PubMed] [Google Scholar]
Pandey 2015 {published data only}
- Pandey A, Sood A, Sammon JD, Abdollah F, Gupta E, Golwala H, et al. Effect of preoperative angina pectoris on cardiac outcomes in patients with previous myocardial infarction undergoing major noncardiac surgery (data from ACS-NSQIP). American Journal of Cardiology 2015;115(8):1080-4. [DOI] [PubMed] [Google Scholar]
Pantoja 2014 {published data only}
- Pantoja MH, Fernández RH, Guevara TW. Sensitivity, specificity and predictive values of the Goldman, Detsky and Lee cardiac indices. Revista Colombiana de Anestesiologia 2014;42(3):184-91. [Google Scholar]
Park 2011 {published data only}
- Park SJ, Choi JH, Cho SJ, Chang SA, Choi JO, Lee SC, et al. Comparison of transthoracic echocardiography with N-terminal pro-brain natriuretic peptide as a tool for risk stratification of patients undergoing major noncardiac surgery. Korean Circulation Journal 2011;41(9):505-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Parmar 2010 {published data only}
- Parmar CD, Torella F. Prediction of major adverse cardiac events in vascular surgery: are cardiac risk scores of any practical value? Vascular and Endovascular Surgery 2010;44(1):14-9. [DOI] [PubMed] [Google Scholar]
Peterson 2016 {published data only}
- Peterson B, Ghahramani M, Harris S, Suchniak-Mussari K, Bedi G, Bulathsinghala C, et al. Usefulness of the myocardial infarction and cardiac arrest calculator as a discriminator of adverse cardiac events after elective hip and knee surgery. American Journal of Cardiology 2016;117(12):1992-5. [DOI] [PubMed] [Google Scholar]
Press 2006 {published data only}
- Press MJ, Chassin MR, Wang J, Tuhrim S, Halm EA. Predicting medical and surgical complications of carotid endarterectomy - comparing the risk indexes. Archives of Internal Medicine 2006;166(8):914-20. [DOI] [PubMed] [Google Scholar]
Ray 2010 {published data only}
- Ray MJ, Calabro LJ, Sirisena T, Crawford SA, Crawford RW, Walters DL. Pre-operative platelet-bound CD40 ligand is probably associated with peri-operative cardiac events in hip and knee arthroplasty. European Journal of Clinical Investigation 2010;40(6):497-503. [DOI] [PubMed] [Google Scholar]
Reis 2019 {published data only}
- Reis PV, Lopes AI, Leite D, Moreira J, Mendes L, Ferraz S, et al. Major cardiac events in patients admitted to intensive care after vascular noncardiac surgery: a retrospective cohort. Seminars in Cardiothoracic & Vascular Anesthesia 2019;23(3):293-9. [DOI] [PubMed] [Google Scholar]
Rodseth 2011 {published data only}
- Rodseth RN, Buse GA, Bolliger D, Burkhart CS, Cuthbertson BH, Gibson SC, et al. The predictive ability of pre-operative B-type natriuretic peptide in vascular patients for major adverse cardiac events an individual patient data meta-analysis. Journal of the American College of Cardiology 2011;58(5):522-9. [DOI] [PubMed] [Google Scholar]
Rohde 2001 {published data only}
- Rohde LE, Polanczyk CA, Goldman L, Cook EF, Lee RT, Lee TH. Usefulness of transthoracic echocardiography as a tool for risk stratification of patients undergoing major noncardiac surgery. American Journal of Cardiology 2001;87(5):505-9. [DOI] [PubMed] [Google Scholar]
Rohrig 2004 {published data only}
- Rohrig R, Junger A, Hartmann B, Klasen J, Quinzio L, Jost A, et al. The incidence and prediction of automatically detected intraoperative cardiovascular events in noncardiac surgery. Anesthesia and Analgesia 2004;98(3):569-77. [DOI] [PubMed] [Google Scholar]
Rutkowski 2019 {published data only}
- Rutkowski M, Sankaran S. Preoperative risk stratification of patient mortality following elective craniotomy; a comparative analysis of prediction algorithms. Journal of Clinical Neuroscience 2019;67:24-31. [DOI] [PubMed] [Google Scholar]
Sabate 2011 {published data only}
- Sabate S, Mases A, Guilera N, Canet J, Castillo J, Orrego C, et al. Incidence and predictors of major perioperative adverse cardiac and cerebrovascular events in non-cardiac surgery. British Journal of Anaesthesia 2011;107(6):879-90. [DOI] [PubMed] [Google Scholar]
Saito 2012 {published data only}
- Saito S, Takagi A, Kurokawa F, Ashihara K, Hagiwara N. Usefulness of tissue Doppler echocardiography to predict perioperative cardiac events in patients undergoing noncardiac surgery. Heart and Vessels 2012;27(6):594-602. [DOI] [PubMed] [Google Scholar]
Scholz 2019 {published data only}
- Scholz AS, Handke J, Gillmann HJ, Zhang Q, Dehne S, Janssen H, et al. Frontline science: low regulatory T cells predict perioperative major adverse cardiovascular and cerebrovascular events after noncardiac surgery. Journal of Leukocyte Biology 2019;107(5):717-30. [DOI] [PubMed] [Google Scholar]
Schouten 2006 {published data only}
- Schouten O, Kok NF, Hoedt MT, Laanen JH, Poldermans D. The influence of aneurysm size on perioperative cardiac outcome in elective open infrarenal aortic aneurysm repair. Journal of Vascular Surgery 2006;44(3):435-41. [DOI] [PubMed] [Google Scholar]
Schrimpf 2015 {published data only}
- Schrimpf C, Gillmann HJ, Sahlmann B, Meinders A, Larmann J, Wilhelmi M, et al. Renal function interferes with copeptin in prediction of major adverse cardiac events in patients undergoing vascular surgery. PloS One 2015;10(4):e0123093. [DOI] [PMC free article] [PubMed] [Google Scholar]
Scorcu 2020 {published data only}
- Scorcu G, Pilleri A, Contu P, Faggiano P, Floris R, Mereu A, et al. Preoperative assessment of cardiovascular risk in patients undergoing noncardiac surgery: the Orion study. Monaldi Archives for Chest Disease 2020;90(1):21-8. [DOI] [PubMed] [Google Scholar]
Scrutinio 2014 {published data only}
- Scrutinio D, Guido G, Guida P, Passantino A, Angiletta D, Santoro D, et al. Combined use of high-sensitivity C-reactive protein and N-terminal pro-B-type natriuretic peptide for risk stratification of vascular surgery patients. Annals of Vascular Surgery 2014;28(6):1522-9. [DOI] [PubMed] [Google Scholar]
Sheth 2015 {published data only}
- Sheth T, Chan M, Butler C, Chow B, Tandon V, Nagele P, et al. Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study. BMJ 2015;350:h1907. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stonelake 2015 {published data only}
- Stonelake S, Thomson P, Suggett N. Identification of the high risk emergency surgical patient: which risk prediction model should be used? Annals of Medicine and Surgery 2015;4(3):240-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Subramaniam 2011 {published data only}
- Subramaniam B, Meroz Y, Talmor D, Pomposelli FB, Berlatzky Y, Landesberg G. A long-term survival score improves preoperative prediction of survival following major vascular surgery. Annals of Vascular Surgery 2011;25(2):197-203. [DOI] [PubMed] [Google Scholar]
Valentijn 2012 {published data only}
- Valentijn TM, Hoeks SE, Bakker EJ, Voute MT, Chonchol M, de Luijtgaarden KM, et al. Influence of aortic valve calcium on outcome in patients undergoing peripheral vascular surgery. American Journal of Cardiology 2012;110(8):1195-9. [DOI] [PubMed] [Google Scholar]
van Diepen 2014 {published data only}
- Diepen S, Youngson E, Ezekowitz JA, McAlister FA. Which risk score best predicts perioperative outcomes in nonvalvular atrial fibrillation patients undergoing noncardiac surgery? American Heart Journal 2014;168(1):60-7. [DOI] [PubMed] [Google Scholar]
van Klei 2007 {published data only}
- Klei WA, Bryson GL, Yang H, Kalkman CJ, Wells GA, Beattie WS. The value of routine preoperative electrocardiography in predicting myocardial infarction after noncardiac surgery. Annals of Surgery 2007;246(2):165-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vetrugno 2014 {published data only}
- Vetrugno L, Langiano N, Gisonni R, Rizzardo A, Venchiarutti PE, Divella M, et al. Prediction of early postoperative major cardiac events after elective orthopedic surgery: the role of B-type natriuretic peptide, the revised cardiac risk index, and ASA class. BMC Anesthesiology 2014;14:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vilarino‐Rico 2015 {published data only}
- Vilarino-Rico J, Pita-Fernandez S, Joaquin Segura-Iglesias R. Clinical predictors of major adverse cardiovascular events during long-term follow-up after carotid endarterectomy. Annals of Vascular Surgery 2015;29(3):419-25. [DOI] [PubMed] [Google Scholar]
Waterman 2016 {published data only}
- Waterman BR, Belmont PJ Jr, Bader JO, Schoenfeld AJ. The total joint arthroplasty cardiac risk index for predicting perioperative myocardial infarction and cardiac arrest after primary total knee and hip arthroplasty. Journal of Arthroplasty 2016;31(6):1170-4. [DOI] [PubMed] [Google Scholar]
Weber 2013 {published data only}
- Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. European Heart Journal 2013;34(11):853-62. [DOI] [PubMed] [Google Scholar]
Welten 2007 {published data only}
- Welten GM, Schouten O, Domburg RT, Feringa HH, Hoeks SE, Dunkelgrun M, et al. The influence of aging on the prognostic value of the revised cardiac risk index for postoperative cardiac complications in vascular surgery patients. European Journal of Vascular and Endovascular Surgery 2007;34(6):632-8. [DOI] [PubMed] [Google Scholar]
Wijeysundera 2018 {published data only}
- Wijeysundera DN, Pearse RM, Shulman MA, Abbott TE, Torres E, Ambosta A, et al. Assessment of functional capacity before major non-cardiac surgery: an international, prospective cohort study. Lancet 2018;391(10140):2631-40. [DOI] [PubMed] [Google Scholar]
Wilcox 2019 {published data only}
- Wilcox T, Smilowitz NR, Xia Y, Berger JS. Cardiovascular risk scores to predict perioperative stroke in noncardiac surgery. Stroke 2019;50(8):2002-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wotton 2013 {published data only}
- Wotton R, Marshall A, Kerr A, Bishay E, Kalkat M, Rajesh P, et al. Does the revised cardiac risk index predict cardiac complications following elective lung resection? Journal of Cardiothoracic Surgery 2013;8:220. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yang 2012 {published data only}
- Yang JH, Choi JH, Ki YW, Kim DI, Kim DK, Park JR, et al. Plasma n-terminal pro-B-type natriuretic peptide is predictive of perioperative cardiac events in patients undergoing vascular surgery. Korean Journal of Internal Medicine 2012;27(3):301-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yang 2018 {published data only}
- Yang HS, Hur M, Yi A, Kim H, Kim J. Prognostic role of high-sensitivity cardiac troponin I and soluble suppression of tumorigenicity-2 in surgical intensive care unit patients undergoing non-cardiac surgery. Annals of Laboratory Medicine 2018;38(3):204-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yap 2018 {published data only}
- Yap MK, Ang KF, Gonzales-Porciuncula LA, Esposo E. Validation of the American College of Surgeons Risk Calculator for preoperative risk stratification. Heart Asia 2018;10(2):e010993. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Abbott 2017 {published data only}
- Abbott TE, Minto G, Lee AM, Pearse RM, Ackl GL. Elevated preoperative heart rate is associated with cardiopulmonary and autonomic impairment in high-risk surgical patients. British Journal of Anaesthesia 2017;119(1):87-94. [DOI] [PubMed] [Google Scholar]
Abbott 2019 {published data only}
- Abbott TE, Pearse RM, Cuthbertson BH, Wijeysundera DN, Ackland GL. Cardiac vagal dysfunction and myocardial injury after non-cardiac surgery: a planned secondary analysis of the measurement of Exercise Tolerance before surgery study. British Journal of Anaesthesia 2019;122(2):188-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Abdelmalak 2018 {published data only}
- Abdelmalak BB, Abd-Elsayed AA, Dalton JE, Abdelmalak JB, Lawrence JP, Doyle DJ, et al. The association between preinduction arterial blood pressure and postoperative cardiovascular, renal, and neurologic morbidity, and in-hospital mortality in elective noncardiac surgery: an observational study. Journal of Hypertension 2018;36(11):2251-9. [DOI] [PubMed] [Google Scholar]
Abdullah 2017 {published data only}
- Abdullah HR, Sim YE, Hao Y, Lin GY, Liew GH, Lamoureux EL, et al. Association between preoperative anaemia with length of hospital stay among patients undergoing primary total knee arthroplasty in Singapore: a single-centre retrospective study. BMJ Open 2017;7(6):e016403. [DOI] [PMC free article] [PubMed] [Google Scholar]
Abdullaha 2018 {published data only}
- Abdullah HR, Sim YE, Sim YT, Ang AL, Chan YH, Richards T, et al. Preoperative red cell distribution width and 30-day mortality in older patients undergoing non-cardiac surgery: a retrospective cohort observational study. Scientific Reports 2018;8(1):6226. [DOI] [PMC free article] [PubMed] [Google Scholar]
Abelha 2009 {published data only}
- Abelha F, Jose O, Botelho M, Fernes V, Barros H. Determinants of postoperative acute kidney injury. Critical Care (London, England) 2009;13(3):R79. [DOI] [PMC free article] [PubMed] [Google Scholar]
Abelha 2010 {published data only}
- Abelha F, Jose O, Botelho M, Fern V, Barros H. Quality of life and mortality assessment in patients with major cardiac events in the postoperative period. Revista Brasileira De Anestesiologia 2010;60(3):268-78. [DOI] [PubMed] [Google Scholar]
Abelha 2012 {published data only}
- Abelha F, Jose O, Fernes V, Botelho M, Santos P, Santos A, et al. Apolipoprotein E e4 allele does not increase the risk of early postoperative delirium after major surgery. Journal of Anesthesia 2012;26(3):412-21. [DOI] [PubMed] [Google Scholar]
Ackland 2007 {published data only}
- Ackland GL, Scollay JM, Parks RW, Beaux I, Mythen MG. Pre-operative high sensitivity C-reactive protein and postoperative outcome in patients undergoing elective orthopaedic surgery. Anaesthesia 2007;62(9):888-94. [DOI] [PubMed] [Google Scholar]
Ackland 2010 {published data only}
- Ackland GL, Harris S, Ziabari Y, Grocott M, Mythen M, SOuRCe Investigators. Revised cardiac risk index and postoperative morbidity after elective orthopaedic surgery: a prospective cohort study. British Journal of Anaesthesia 2010;105(6):744-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ackland 2011 {published data only}
- Ackland GL, Moran N, Cone S, Grocott MP, Mythen MG. Chronic kidney disease and postoperative morbidity after elective orthopedic surgery. Anesthesia & Analgesia 2011;112(6):1375-81. [DOI] [PubMed] [Google Scholar]
Ackland 2018 {published data only}
- Ackland GL, Abbott TE, Cain D, Edwards MR, Sultan P, Karmali SN, et al. Preoperative systemic inflammation and perioperative myocardial injury: prospective observational multicentre cohort study of patients undergoing non-cardiac surgery. British Journal of Anaesthesia 2018;122(2):180-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Agarwal 2013 {published data only}
- Agarwal S, Rajamanickam A, Bajaj NS, Griffin BP, Catacutan T, Svensson LG, et al. Impact of aortic stenosis on postoperative outcomes after noncardiac surgeries. Circulation: Cardiovascular Quality and Outcomes 2013;6(2):193-200. [DOI] [PubMed] [Google Scholar]
Albaladejo 2011 {published data only}
- Albaladejo P, Marret E, Samama CM, Collet JP, Abhay K, Loutrel O, et al. Non-cardiac surgery in patients with coronary stents: the RECO study. Heart 2011;97(19):1566-72. [DOI] [PubMed] [Google Scholar]
Alcock 2012 {published data only}
- Alcock RF, Kouzios D, Naoum C, Hillis GS, Brieger DB. Perioperative myocardial necrosis in patients at high cardiovascular risk undergoing elective non-cardiac surgery. Heart 2012;98(10):792-8. [DOI] [PubMed] [Google Scholar]
Alcock 2013 {published data only}
- Alcock RF, Naoum C, Alipri-Costa B, Hillis GS, Brieger DB. The peri-operative management of anti-platelet therapy in elective, non-cardiac surgery. International Journal of Cardiology 2013;167(2):374-7. [DOI] [PubMed] [Google Scholar]
Alvarez 2016 {published data only}
- Alvarez ZC, Planas RA, Alday ME, Vega PL, Ramasco RF. High levels of preoperative and postoperative N terminal B-type natriuretic propeptide influence mortality and cardiovascular complications after noncardiac surgery: a prospective cohort study. European Journal of Anaesthesiology 2016;33(6):444-9. [DOI] [PubMed] [Google Scholar]
Ambler 2014 {published data only}
- Ambler GK, Dapaah A, Al ZN, Hayes PD, Gohel Manjit S, Boyle Jonathan R, et al. Independence and mobility after infrainguinal lower limb bypass surgery for critical limb ischemia. Journal of Vascular Surgery 2014;59(4):983-7.e2. [DOI] [PubMed] [Google Scholar]
Andersson 2015 {published data only}
- Andersson C, Wissenberg M, Jorgensen ME, Hlatky MA, Merie C, Jensen PF, et al. Age-specific performance of the revised cardiac risk index for predicting cardiovascular risk in elective noncardiac surgery. Circulation Cardiovascular Quality & Outcomes 2015;8(1):103-8. [DOI] [PubMed] [Google Scholar]
Anghelescu 2018 {published data only}
- Anghelescu D, Popescu E, Mihalcea D, Carstocea L, Gherghiceanu F, Cursaru A, et al. The influence of preoperative cardiovascular assessment and time to surgery on postoperative mortality after surgery for femoral neck fractures in elderly patients. Archives of the Balkan Medical Union 2018;53(4):551-6. [Google Scholar]
Arain 2016 {published data only}
- Arain AM, Azar NJ, Lagrange AH, McLean M, Singh P, Sonmezturk H, et al. Temporal lobe origin is common in patients who have undergone epilepsy surgery for hypermotor seizures. Epilepsy & Behavior 2016;64:57-61. [DOI] [PubMed] [Google Scholar]
Armstrong 2017 {published data only}
- Armstrong EJ, Graham L, Waldo SW, Valle JA, Maddox TM, Hawn MT. Patient and lesion-specific characteristics predict risk of major adverse cardiovascular events among patients with previous percutaneous coronary intervention undergoing noncardiac surgery. Catheterization & Cardiovascular Interventions 2017;89(4):617-27. [DOI] [PubMed] [Google Scholar]
Azevedo 2017 {published data only}
- Azevedo PS, Gumieiro DN, Polegato BF, Pereira GJ, Silva IA, et al. Goldman score, but not Detsky or Lee indices, predicts mortality 6 months after hip fracture. BMC Musculoskeletal Disorders 2017;18(1):134. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bae 2014 {published data only}
- Bae MH, Lee JH, Yang DH, Park HS, Cho Y, Chae SC. Usefulness of surgical parameters as predictors of postoperative cardiac events in patients undergoing non-cardiac surgery. Circulation Journal 2014;78(3):718-23. [DOI] [PubMed] [Google Scholar]
Baer‐Bositis 2018 {published data only}
- Baer-Bositis HE, Hicks TD, Haidar GM, Sideman MJ, Pounds LL, Davies MG. Outcomes of isolated tibial endovascular intervention for rest pain in patients on dialysis. Annals of Vascular Surgery 2018;46:118-26. [DOI] [PubMed] [Google Scholar]
Bajaj 2013 {published data only}
- Bajaj NS, Agarwal S, Rajamanickam A, Parashar A, Poddar KL, Griffin BP, et al. Impact of severe mitral regurgitation on postoperative outcomes after noncardiac surgery. American Journal of Medicine 2013;126(6):529-35. [DOI] [PubMed] [Google Scholar]
Bakker 2012 {published data only}
- Bakker EJ, de Luijtgaarden KM, Lier F, Valentijn TM, Hoeks SE, Klimek M, et al. General anaesthesia is associated with adverse cardiac outcome after endovascular aneurysm repair. European Journal of Vascular & Endovascular Surgery 2012;44(2):121-5. [DOI] [PubMed] [Google Scholar]
Bakker 2013 {published data only}
- Bakker EJ, Valentijn TM, de Luijtgaarden KM, Hoeks SE, Voute MT, Goncalves FB, et al. Type 2 diabetes mellitus, independent of insulin use, is associated with an increased risk of cardiac complications after vascular surgery. Anaesthesia & Intensive Care 2013;41(5):584-90. [DOI] [PubMed] [Google Scholar]
Barisione 2016 {published data only}
- Barisione C, Garibaldi S, Brunelli C, Balbi M, Spallarossa P, Canepa M, et al. Prevalent cardiac, renal and cardiorenal damage in patients with advanced abdominal aortic aneurysms. Internal and Emergency Medicine 2016;11(2):205-12. [DOI] [PubMed] [Google Scholar]
Barrett 2007 {published data only}
- Barrett TW, Mori M, De Boer D. Association of ambulatory use of statins and beta-blockers with long-term mortality after vascular surgery. Journal of Hospital Medicine (Online) 2007;2(4):241-52. [DOI] [PubMed] [Google Scholar]
Batsis 2009 {published data only}
- Batsis JA, Huddleston JM, Melton LJ, Huddleston PM, Lopez-Jimenez F, Larson DR, et al. Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: a population-based study. Journal of the American Geriatrics Society 2009;57(3):419-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Belmont 2014 {published data only}
- Belmont PJ Jr, Goodman GP, Kusnezov NA, Magee C, Bader JO, Waterman BR, et al. Postoperative myocardial infarction and cardiac arrest following primary total knee and hip arthroplasty: rates, risk factors, and time of occurrence. Journal of Bone and Joint Surgery-American Volume 2014;96(24):2025-31. [DOI] [PubMed] [Google Scholar]
Bertges 2010 {published data only}
- Bertges DJ, Goodney PP, Zhao Y, Schanzer A, Nolan BW, Likosky DS, et al. The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients. Journal of Vascular Surgery 2010;52(3):674-83, 683.e1-e3. [DOI] [PubMed] [Google Scholar]
Biccard 2007 {published data only}
- Biccard BM. Clinical risk predictors associated with cardiac mortality following vascular surgery in South African patients. Cardiovascular Journal of Africa 2007;18(4):216-20. [PMC free article] [PubMed] [Google Scholar]
Biccard 2010 {published data only}
- Biccard BM, Nepaul S. Risk factors associated with intermediate and long-term mortality following vascular surgery in South African patients. Cardiovascular Journal of Africa 2010;21(5):263-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biccard 2012a {published data only}
- Biccard BM, Naidoo P, Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia 2012;67(4):389-95. [DOI] [PubMed] [Google Scholar]
Biccard 2013 {published data only}
- Biccard BM, Rodseth RN. What evidence is there for intraoperative predictors of perioperative cardiac outcomes? A systematic review. Perioperative Medicine 2013;2(1):14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biccard 2014 {published data only}
- Biccard BM. Myocardial injury after non-cardiac surgery: a new clinical entity. Southern African Journal of Anaesthesia and Analgesia 2014;20(1):24. [Google Scholar]
Biccard 2015 {published data only}
- Biccard B. Proposed research plan for the derivation of a new Cardiac Risk Index. Anesthesia & Analgesia 2015;120(3):543-53. [DOI] [PubMed] [Google Scholar]
Biteker 2011 {published data only}
- Biteker M, Duman D, Dayan A, Ilhan E. Increased aortic stiffness can predict perioperative cardiovascular outcomes in patients undergoing noncardiac, nonvascular surgery. World Journal of Surgery 2011;35(11):2411-6. [DOI] [PubMed] [Google Scholar]
Biteker 2011a {published data only}
- Biteker M, Dayan A, Can MM, Ilhan E, Biteker FS, Tekkesin A, et al. Impaired fasting glucose is associated with increased perioperative cardiovascular event rates in patients undergoing major non-cardiothoracic surgery. Cardiovascular Diabetology 2011;10:63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biteker 2012 {published data only}
- Biteker M, Duman D, Tekkesin AI. Predictive value of preoperative electrocardiography for perioperative cardiovascular outcomes in patients undergoing noncardiac, nonvascular surgery. Clinical Cardiology 2012;35(8):494-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biteker 2014 {published data only}
- Biteker M, Dayan A, Tekkesin AI, Can MM, Tayci I, Ilhan E, et al. Incidence, risk factors, and outcomes of perioperative acute kidney injury in noncardiac and nonvascular surgery. American Journal of Surgery 2014;207(1):53-9. [DOI] [PubMed] [Google Scholar]
Biteker 2014a {published data only}
- Biteker M, Kayatas K, Turkmen FM, Misirli CH. Impact of perioperative acute ischemic stroke on the outcomes of noncardiac and nonvascular surgery: a single centre prospective study. Canadian Journal of Surgery 2014;57(3):E55-E61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bolliger 2009 {published data only}
- Bolliger D, Seeberger MD, Lurati BG, Christen P, Rupinski B, Gurke L, et al. A preliminary report on the prognostic significance of preoperative brain natriuretic peptide and postoperative cardiac troponin in patients undergoing major vascular surgery. Anesthesia & Analgesia 2009;108(4):1069-75. [DOI] [PubMed] [Google Scholar]
Bolliger 2012 {published data only}
- Bolliger D, Seeberger MD, Lurati BG, Christen P, Seeberger E, Ruppen W, et al. The influence of pre-admission hypoglycaemic therapy on cardiac morbidity and mortality in type 2 diabetic patients undergoing major non-cardiac surgery: a prospective observational study. Anaesthesia 2012;67(2):149-57. [DOI] [PubMed] [Google Scholar]
Borges 2013a {published data only}
- Borges FK, Furtado MV, Rossini AP, Bertoluci C, Gonzalez VL, Bertoldi EG, et al. Clinical use of ultrasensitive cardiac troponin I assay in intermediate- and high-risk surgery patients. Disease Markers 2013;35(6):945-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Butt 2009 {published data only}
- Butt ZM, Fazili A, Tan W, Wilding GE, Filadora V, Kim HL, et al. Does the presence of significant risk factors affect perioperative outcomes after robot-assisted radical cystectomy? BJU International 2009;104(7):986-90. [DOI] [PubMed] [Google Scholar]
Calvillo‐King 2010 {published data only}
- Calvillo-King L, Xuan L, Zhang S, Tuhrim S, Halm EA. Predicting risk of perioperative death and stroke after carotid endarterectomy in asymptomatic patients derivation and validation of a clinical risk score. Stroke 2010;41(12):2786-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
Canter 2008 {published data only}
- Canter RJ, Qin LX, Maki RG, Brennan MF, Ladanyi M, Singer S. A synovial sarcoma-specific preoperative nomogram supports a survival benefit to ifosfamide-based chemotherapy and improves risk stratification for patients. Clinical Cancer Research 2008;14(24):8191-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cassagneau 2012 {published data only}
- Cassagneau P, Jacquier A, Giorgi R, Amabile N, Gaubert JY, Cohen F, et al. Prognostic value of preoperative coronary computed tomography angiography in patients treated by orthotopic liver transplantation. European Journal of Gastroenterology & Hepatology 2012;24(5):558-62. [DOI] [PubMed] [Google Scholar]
Chan 2018 {published data only}
- Chan DX, Sim YE, Chan YH, Poopalalingam R, Abdullah HR. Development of the Combined Assessment of Risk Encountered in Surgery (CARES) surgical risk calculator for prediction of postsurgical mortality and need for intensive care unit admission risk: a single-center retrospective study. BMJ Open 2018;8(3):e019427. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chang 2019 {published data only}
- Chang HY, Chang WT, Liu YW. Application of transthoracic echocardiography in patients receiving intermediate- or high-risk noncardiac surgery. PLoS ONE 2019;14(4):e0215854. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chen 2002 {published data only}
- Chen T, Kuwabara Y, Tsutsui H, Sasaki M, Nakagawa M, Koga H, et al. The usefulness of dipyridamole thallium-201 single photon emission computed tomography for predicting perioperative cardiac events in patients undergoing non-cardiac vascular surgery. Annals of Nuclear Medicine 2002;16(1):45-53. [DOI] [PubMed] [Google Scholar]
Christiansen 2017 {published data only}
- Christiansen MN, Andersson C, Gislason GH, Torp-Pedersen C, Sers RD, Jensen PF, et al. Risks of cardiovascular adverse events and death in patients with previous stroke undergoing emergency noncardiac, nonintracranial surgery: the importance of operative timing. Anesthesiology 2017;127(1):9-19. [DOI] [PubMed] [Google Scholar]
Cicarelli 2001 {published data only}
- Cicarelli DD, Marumo CK, Esteves RG. Postoperative myocardial ischemia in patients undergoing abdominal aortic aneurysm repair. A retrospective study. Revista Brasileira de Anestesiologia 2001;51(4):319-24. [Google Scholar]
Cloney 2017 {published data only}
- Cloney MB, Sonabend AM, Yun J, Yang J, Iwamoto F, Singh S, et al. The safety of resection for primary central nervous system lymphoma: a single institution retrospective analysis. Journal of Neuro-Oncology 2017;132(1):189-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cook 2017 {published data only}
- Cook KA, Maclntyre RA, McAlpine JR. A retrospective observational study of patients with dilated cardiomyopathy undergoing non-cardiac surgery. Anaesthesia and Intensive Care 2017;45(5):619-23. [DOI] [PubMed] [Google Scholar]
Crowther 2018 {published data only}
- Crowther M, Spuy K, Roodt F, Nejthardt MB, Davids JG, Roos J, et al. The relationship between pre-operative hypertension and intra-operative haemodynamic changes known to be associated with postoperative morbidity. Anaesthesia 2018;73(7):812-8. [DOI] [PubMed] [Google Scholar]
Cullen 2020 {published data only}
- Cullen MW, McCully RB, Widmer RJ, Schroeder DR, Salonen BR, Raslau D, et al. Preoperative dobutamine stress echocardiography and clinical factors for assessment of cardiac risk after noncardiac surgery. Journal of the American Society of Echocardiography 2020;33(4):423-32. [DOI] [PubMed] [Google Scholar]
Cuthbertson 2007a {published data only}
- Cuthbertson BH, Amiri AR, Croal BL, Rajagopalan S, Brittenden J, Hillis GS. Utility of B-type natriuretic peptide in predicting medium-term mortality in patients undergoing major non-cardiac surgery. American Journal of Cardiology 2007;100(8):1310-3. [DOI] [PubMed] [Google Scholar]
Cuthbertson 2007b {published data only}
- Cuthbertson BH, Card G, Croal BL, McNeilly J, Hillis GS. The utility of B-type natriuretic peptide in predicting postoperative cardiac events and mortality in patients undergoing major emergency non-cardiac surgery. Anaesthesia 2007;62(9):875-81. [DOI] [PubMed] [Google Scholar]
Davies 2015 {published data only}
- Davies MG, El-Sayed HF. Objective performance goals after endovascular intervention for critical limb ischemia. Journal of Vascular Surgery 2015;62(6):1555-63. [DOI] [PubMed] [Google Scholar]
Davies 2015a {published data only}
- Davies MG, El-Sayed HF. Outcomes of isolated tibial endovascular interventions for tissue loss in CLI patients on hemodialysis. Journal of Endovascular Therapy 2015;22(5):681-9. [DOI] [PubMed] [Google Scholar]
Davis 2018 {published data only}
- Davis FM, Park YJ, Grey SF, Boniakowski AE, Mansour MA, Jain KM, et al. The clinical impact of cardiology consultation prior to major vascular surgery. Annals of Surgery 2018;267(1):189-95. [DOI] [PubMed] [Google Scholar]
de Campos 2012 {published data only}
- Campos JE, Cardinalli-Neto A, Borim AA, Bestetti RB. Cardiovascular complications in patients with megaesophagus due to Chagas disease undergoing the Serra-Doria operation. Acta Tropica 2012;122(2):219-23. [DOI] [PubMed] [Google Scholar]
Dernellis 2006 {published data only}
- Dernellis J, Panaretou M. Assessment of cardiac risk before non-cardiac surgery: brain natriuretic peptide in 1590 patients. Heart 2006;92(11):1645-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Devereaux 2011 {published data only}
- Devereaux PJ, Bradley D, Chan MT, Walsh M, Villar JC, Polanczyk CA, et al. An international prospective cohort study evaluating major vascular complications among patients undergoing noncardiac surgery: the VISION Pilot Study. Open Medicine 2011;5(4):e193-200. [PMC free article] [PubMed] [Google Scholar]
de Virgilio 2009 {published data only}
- Virgilio C, Yaghoubian A, Nguyen A, Lewis RJ, Dauphine C, Sarkisyan G, et al. Peripheral vascular surgery using targeted beta blockade reduces perioperative cardiac event rate. Journal of the American College of Surgeons 2009;208(1):14-20. [DOI] [PubMed] [Google Scholar]
Dover 2013 {published data only}
- Dover M, Tawfick W, Hynes N, Sultan S. Cardiac risk assessment, morbidity prediction, and outcome in the vascular intensive care unit. Vascular & Endovascular Surgery 2013;47(8):585-94. [DOI] [PubMed] [Google Scholar]
Drake 2016 {published data only}
- Drake TM, Nepogodiev D, Chapman SJ, Glasbey JC, Khatri C, Kong CY, et al. Multicentre prospective cohort study of body mass index and postoperative complications following gastrointestinal surgery. British Journal of Surgery 2016;103(9):1157-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Drudi 2016 {published data only}
- Drudi LM, Phung K, Ades M, Zuckerman J, Mullie L, Steinmetz OK, et al. Psoas muscle area predicts all-cause mortality after endovascular and open aortic aneurysm repair. European Journal of Vascular & Endovascular Surgery 2016;52(6):764-9. [DOI] [PubMed] [Google Scholar]
Duceppe 2018 {published data only}
- Duceppe E, Lussier AR, Beaulieu-Dore R, LeManach Y, Laskine M, Fafard J, et al. Preoperative antihypertensive medication intake and acute kidney injury after major vascular surgery. Journal of Vascular Surgery 2018;67(6):1872-80.e1. [DOI] [PubMed] [Google Scholar]
Duceppe 2019 {published data only}
- Duceppe E, Studzinska D, Devereaux PJ, Polok K, Gajdosz A, Lewandowski K, et al. Incidence and predictors of myocardial and kidney injury following endovascular aortic repair: a retrospective cohort study. Canadian Journal of Anaesthesia 2019;66(11):1338-46. [DOI] [PubMed] [Google Scholar]
Edelmuth 2018 {published data only}
- Edelmuth SV, Sorio GN, Sprovieri FA, Gali JC, Peron SF. Comorbidities, clinical intercurrences, and factors associated with mortality in elderly patients admitted for a hip fracture. Revista Brasileira de Ortopedia 2018;53(5):543-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ekeloef 2017 {published data only}
- Ekeloef S, Larsen MH, Schou-Pedersen AM, Lykkesfeldt J, Rosenberg J, Gogenur I. Endothelial dysfunction in the early postoperative period after major colon cancer surgery. British Journal of Anaesthesia 2017;118(2):200-6. [DOI] [PubMed] [Google Scholar]
Ekeloef 2020 {published data only}
- Ekeloef S, Bjerrum E, Kristiansen P, Wahlstrøm K, Burcharth J, Gögenur I. The risk of post-operative myocardial injury after major emergency abdominal surgery: a retrospective cohort study. Acta Anaesthesiologica Scandinavica 2020;64(8):1073-81. [DOI] [PubMed] [Google Scholar]
Ekeloef 2020a {published data only}
- Ekeloef S, Oreskov JO, Falkenberg A, Burcharth J, Schou-Pedersen AM, Lykkesfeldt J, et al. Endothelial dysfunction and myocardial injury after major emergency abdominal surgery: a prospective cohort study. BMC Anesthesiology 2020;20(1):67. [DOI] [PMC free article] [PubMed] [Google Scholar]
Erol 2019 {published data only}
- Erol Y, Ergönül AG, Özdil A, Nalbantgil S, Çağırıcı U, Turhan K, et al. Assessment of cardiac complications in patients undergoing pulmonary resection. Heart Lung and Circulation 2019;28(7):1099-101. [DOI] [PubMed] [Google Scholar]
Eyraud 2000 {published data only}
- Eyraud D, Bertr, M, Fleron MH, Godet G, Riou B, Kieffer E, et al. Perioperative mortality in abdominal aortic surgery. Annales Francaises D Anesthesie Et De Reanimation 2000;19(6):452-8. [DOI] [PubMed] [Google Scholar]
Faggiano 2012 {published data only}
- Faggiano P, Bonardelli S, De Feo S, Valota M, Frattini S, Cervi E, et al. Preoperative cardiac evaluation and perioperative cardiac therapy in patients undergoing open surgery for abdominal aortic aneurysms: effects on cardiovascular outcome. Annals of Vascular Surgery 2012;26(2):156-65. [DOI] [PubMed] [Google Scholar]
Fayad 2011 {published data only}
- Fayad AA, Yang HY, Ruddy TD, Watters JM, Wells GA. Perioperative myocardial ischemia and isolated systolic hypertension in non-cardiac surgery. Canadian Journal of Anesthesia-Journal Canadien D Anesthesie 2011;58(5):428-35. [DOI] [PubMed] [Google Scholar]
Feringa 2006 {published data only}
- Feringa HH, Bax JJ, Jonge R, Elhendy A, Domburg RT, Dunkelgrun M, et al. Impact of glomerular filtration rate on minor troponin T elevations for risk assessment in patients undergoing operation for abdominal aortic aneurysm or lower extremity arterial obstruction. American Journal of Cardiology 2006;98(11):1515-8. [DOI] [PubMed] [Google Scholar]
Feringa 2006a {published data only}
- Feringa HH, Bax JJ, Elhendy A, Jonge R, Lindemans J, Schouten O, et al. Association of plasma N-terminal pro-B-type natriuretic peptide with postoperative cardiac events in patients undergoing surgery for abdominal aortic aneurysm or leg bypass. American Journal of Cardiology 2006;98(1):111-5. [DOI] [PubMed] [Google Scholar]
Feringa 2007a {published data only}
- Feringa HH, Vidakovic R, Karagiannis SE, Jonge R, Lindemans J, Goei D, et al. Baseline natriuretic peptide levels in relation to myocardial ischemia, troponin T release and heart rate variability in patients undergoing major vascular surgery. Coronary Artery Disease 2007;18(8):645-51. [DOI] [PubMed] [Google Scholar]
Feringa 2009 {published data only}
- Feringa HH, Bax JJ, Karagiannis SE, Noordzij P, Domburg R, Klein J, et al. Elderly patients undergoing major vascular surgery: risk factors and medication associated with risk reduction. Archives of Gerontology & Geriatrics 2009;48(1):116-20. [DOI] [PubMed] [Google Scholar]
Ferrante 2018 {published data only}
- Ferrante AM, Moscato U, Snider F, Tshomba Y. Controversial results of the Revised Cardiac Risk Index in elective open repair of abdominal aortic aneurysms: Retrospective analysis on a continuous series of 899 cases. International Journal of Cardiology 2018;277:224-8. [DOI] [PubMed] [Google Scholar]
Filipovic 2003 {published data only}
- Filipovic M, Jeger R, Probst C, Girard T, Pfisterer M, Gurke L, et al. Heart rate variability and cardiac troponin I are incremental and independent predictors of one-year all-cause mortality after major noncardiac surgery in patients at risk of coronary artery disease. Journal of the American College of Cardiology 2003;42(10):1767-76. [DOI] [PubMed] [Google Scholar]
Filipovic 2005 {published data only}
- Filipovic M, Jeger RV, Girard T, Probst C, Pfisterer M, Gurke L, et al. Predictors of long-term mortality and cardiac events in patients with known or suspected coronary artery disease who survive major non-cardiac surgery. Anaesthesia 2005;60(1):5-11. [DOI] [PubMed] [Google Scholar]
Flu 2009 {published data only}
- Flu WJ, Kuijk JP, Hoeks SE, Kuiper R, Schouten O, Goei D, et al. Intima media thickness of the common carotid artery in vascular surgery patients: a predictor of postoperative cardiovascular events. American Heart Journal 2009;158(2):202-8. [DOI] [PubMed] [Google Scholar]
Flu 2010 {published data only}
- Flu WJ, Kuijk JP, Voute MT, Kuiper R, Verhagen HJ, Bax JJ, et al. Asymptomatic low ankle-brachial index in vascular surgery patients: a predictor of perioperative myocardial damage. European Journal of Vascular & Endovascular Surgery 2010;39(1):62-9. [DOI] [PubMed] [Google Scholar]
Flu 2010a {published data only}
- Flu WJ, Gestel YR, Kuijk JP, Hoeks SE, Kuiper R, Verhagen HJ, et al. Co-existence of COPD and left ventricular dysfunction in vascular surgery patients. Respiratory Medicine 2010;104(5):690-6. [DOI] [PubMed] [Google Scholar]
Galal 2010 {published data only}
- Galal W, Hoeks SE, Flu WJ, Kuijk JP, Goei D, Galema T, et al. Relation between preoperative and intraoperative new wall motion abnormalities in vascular surgery patients: a transesophageal echocardiographic study. Anesthesiology 2010;112(3):557-66. [DOI] [PubMed] [Google Scholar]
Garcia 2009 {published data only}
- Garcia S, Moritz TE, Goldman S, Littooy F, Pierpont G, Larsen GC, et al. Perioperative complications after vascular surgery are predicted by the Revised Cardiac Risk Index but are not reduced in high-risk subsets with preoperative revascularization. Circulation: Cardiovascular Quality and Outcomes 2009;2(2):73-7. [DOI] [PubMed] [Google Scholar]
Garcia 2013 {published data only}
- Garcia S, Marston N, Soval Y, Pierpont G, Adabag S, Brenes J, et al. Prognostic value of 12-lead electrocardiogram and peak troponin I level after vascular surgery. Journal of Vascular Surgery 2013;57(1):166-72. [DOI] [PubMed] [Google Scholar]
Ghadri 2012 {published data only}
- Ghadri JR, Fiechter M, Veraguth K, Gebhard C, Pazhenkottil AP, Fuchs TA, et al. Coronary calcium score as an adjunct to nuclear myocardial perfusion imaging for risk stratification before noncardiac surgery. Journal of Nuclear Medicine 2012;53(7):1081-6. [DOI] [PubMed] [Google Scholar]
Ghazali 2017 {published data only}
- Ghazali N, Caldroney S, Dyalram D, Lubek JE. Cardiovascular complications in head & neck microvascular flap reconstruction: a retrospective risk stratification and outcomes assessment. Journal of Cranio-Maxillo-Facial Surgery 2017;45(12):2120-7. [DOI] [PubMed] [Google Scholar]
Gibson 2007 {published data only}
- Gibson SC, Payne CJ, Byrne DS, Berry C, Dargie HJ, Kingsmore DB. B-type natriuretic peptide predicts cardiac morbidity and mortality after major surgery. British Journal of Surgery 2007;94(7):903-9. [DOI] [PubMed] [Google Scholar]
Gillmann 2019 {published data only}
- Gillmann HJ, Meinders A, Larmann J, Sahlmann B, Schrimpf C, Aper T, et al. Adrenomedullin is associated with surgical trauma and impaired renal function in vascular surgery patients. Journal of Intensive Care Medicine 2019;34(1):67-76. [DOI] [PubMed] [Google Scholar]
Go 2017 {published data only}
- Go G, Davies KT, O'Callaghan C, Senior W, Kostner K, Fagermo N, et al. Negative predictive value of dobutamine stress echocardiography for perioperative risk stratification in patients with cardiac risk factors and reduced exercise capacity undergoing non-cardiac surgery. Internal Medicine Journal 2017;47(12):1376-84. [DOI] [PubMed] [Google Scholar]
Goei 2009 {published data only}
- Goei D, Hoeks SE, Boersma E, Winkel TA, Dunkelgrun M, Flu WJ, et al. Incremental value of high-sensitivity C-reactive protein and N-terminal pro-B-type natriuretic peptide for the prediction of postoperative cardiac events in noncardiac vascular surgery patients. Coronary Artery Disease 2009;20(3):219-24. [DOI] [PubMed] [Google Scholar]
Goh 2000 {published data only}
- Goh MH, Yo SL, Ip-Yam PC. The predictive value of intraoperative ST-segment monitoring as a marker of myocardial injury. Annals of the Academy of Medicine, Singapore 2000;29(2):173-6. [PubMed] [Google Scholar]
Gómez 2012 {published data only}
- Gómez TR, Legarreta CG, Brea FJ, Martínez PM, Cardozo R, Martínez P. Frecuencia de complicaciones respiratorias en cirugía electiva general: Experiencia en un hospital universitario Experience of a University Hospital. Revista Americana de Medicina Respiratoria 2012;12(3):79-85. [Google Scholar]
Goodman 2015 {published data only}
- Goodman BA, Batterham AM, Kothmann E, Cawthorn L, Yates D, Melsom H, et al. Validity of the Postoperative Morbidity Survey after abdominal aortic aneurysm repair-a prospective observational study. Perioperative Medicine 2015;4:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gu 2018 {published data only}
- Gu Z, Sun C, Xiang D. Postoperative adverse cardiovascular events associated with leptin and adverse age after elective major non-cardiac surgery: an Asian single-center study. Medical Science Monitor 2018;24:2119-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gundes 2017 {published data only}
- Gundes E, Aday U, Ciyiltepe H, Cetin DA, Senger AS, Bozdag E, et al. Effects of left ventricular ejection fraction on morbidity and mortality in major abdominal surgery. International Journal of Clinical and Experimental Medicine 2017;10(12):16632-8. [Google Scholar]
Halm 2005 {published data only}
- Halm EA, Hannan EL, Rojas M, Tuhrim S, Riles TS, Rockman CB, et al. Clinical and operative predictors of outcomes of carotid endarterectomy. Journal of Vascular Surgery 2005;42(3):420-8. [DOI] [PubMed] [Google Scholar]
Halm 2009 {published data only}
- Halm EA, Tuhrim S, Wang JJ, Rojas M, Rockman C, Riles TS, et al. Racial and ethnic disparities in outcomes and appropriateness of carotid endarterectomy impact of patient and provider factors. Stroke 2009;40(7):2493-501. [DOI] [PMC free article] [PubMed] [Google Scholar]
Halm 2009a {published data only}
- Halm EA, Tuhrim S, Wang JJ, Rockman C, Riles TS, Chassin MR. Risk factors for perioperative death and stroke after carotid endarterectomy: results of the New York Carotid Artery Surgery Study. Stroke 2009;40(1):221-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hammill 2008 {published data only}
- Hammill BG, Curtis LH, Bennett-Guerrero E, O'Connor CM, Jollis JG, Schulman KA, et al. Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology 2008;108(4):559-67. [DOI] [PubMed] [Google Scholar]
Hansen 2016 {published data only}
- Hansen PW, Gislason GH, Jorgensen ME, Kober L, Jensen PF, Torp-Pedersen C, et al. Influence of age on perioperative major adverse cardiovascular events and mortality risks in elective non-cardiac surgery. European Journal of Internal Medicine 2016;35:55-9. [DOI] [PubMed] [Google Scholar]
Hanss 2008 {published data only}
- Hanss R, Block D, Bauer M, Ilies C, Magheli A, Schildberg-Schroth H, et al. Use of heart rate variability analysis to determine the risk of cardiac ischaemia in high-risk patients undergoing general anaesthesia. Anaesthesia 2008;63(11):1167-73. [DOI] [PubMed] [Google Scholar]
Harland 2020 {published data only}
- Harland TA, Wang M, Gunaydin D, Fringuello A, Freeman J, Hosokawa PW, et al. Frailty as a predictor of neurosurgical outcomes in brain tumor patients. World Neurosurgery 2020;133:e813-8. [DOI] [PubMed] [Google Scholar]
Hawn 2013 {published data only}
- Hawn MT, Graham LA, Richman JS, Itani KM, Henderson WG, Maddox TM. Risk of major adverse cardiac events following noncardiac surgery in patients with coronary stents. JAMA 2013;310(14):1462-72. [DOI] [PubMed] [Google Scholar]
Hennis 2012 {published data only}
- Hennis PJ, Meale PM, Hurst RA, O'Doherty AF, Otto J, Kuper M, et al. Cardiopulmonary exercise testing predicts postoperative outcome in patients undergoing gastric bypass surgery. British Journal of Anaesthesia 2012;109(4):566-71. [DOI] [PubMed] [Google Scholar]
Hietala 2014 {published data only}
- Hietala P, Stroberg M, Kiviniemi T, Stroberg N, Airaksinen KE. Usefulness of troponin T to predict short-term and long-term mortality in patients after hip fracture. American Journal of Cardiology 2014;114(2):193-7. [DOI] [PubMed] [Google Scholar]
Hirano 2014 {published data only}
- Hirano Y, Takeuchi H, Suda K, Oyama T, Nakamura R, Takahashi T, et al. Clinical utility of the Revised Cardiac Risk Index in non-cardiac surgery for elderly patients: a prospective cohort study. Surgery Today 2014;44(2):277-84. [DOI] [PubMed] [Google Scholar]
Hirpara 2019 {published data only}
- Hirpara DH, Kidane B, Rogalla P, Cypel M, Perrot M, Keshavjee S, et al. Frailty assessment prior to thoracic surgery for lung or esophageal cancer: a feasibility study. Supportive Care in Cancer 2019;27(4):1535-40. [DOI] [PubMed] [Google Scholar]
Hoeks 2007 {published data only}
- Hoeks SE, Scholteop RW, Urk H, Jörning PJ, Boersma E, Simoons ML, et al. Increase of 1-year mortality after perioperative beta-blocker withdrawal in endovascular and vascular surgery patients. European Journal of Vascular and Endovascular Surgery 2007;33(1):13-9. [DOI] [PubMed] [Google Scholar]
Hoeks 2008 {published data only}
- Hoeks SE, Scholte OR, Schouten O, Lenzen MJ, Urk H, Poldermans D. Statin use in the elderly: results from a peripheral vascular survey in The Netherlands. Journal of Vascular Surgery 2008;48(4):891-5; discussion 895-6. [DOI] [PubMed] [Google Scholar]
Hoeks 2009 {published data only}
- Hoeks SE, op Reimer WJ, Gestel YR, Smolderen KG, Verhagen H, Domburg RT, et al. Preoperative cardiac risk index predicts long-term mortality and health status. American Journal of Medicine 2009;122(6):559-65. [DOI] [PubMed] [Google Scholar]
Hoeks 2009a {published data only}
- Hoeks SE, Smolderen KG, Reimer WJ, Verhagen HJ, Spertus JA, Poldermans D. Clinical validity of a disease-specific health status questionnaire: The Peripheral Artery Questionnaire. Journal of Vascular Surgery 2009;49(2):371-7. [DOI] [PubMed] [Google Scholar]
Hoeks 2010 {published data only}
- Hoeks SE, op Reimer WJ, Lingsma HF, Gestel Y, Urk H, Bax JJ, et al. Process of care partly explains the variation in mortality between hospitals after peripheral vascular surgery. European Journal of Vascular and Endovascular Surgery 2010;40(2):147-54. [DOI] [PubMed] [Google Scholar]
Hofer 2018 {published data only}
- Hofer IS, Cheng D, Grogan T, Fujimoto Y, Yamada T, Beck L, et al. Automated assessment of existing patient's revised cardiac risk index using algorithmic software. Anesthesia & Analgesia 2019;128:909-16. [DOI] [PubMed] [Google Scholar]
Hoftman 2013 {published data only}
- Hoftman N, Prunean A, Dhillon A, Danovitch GM, Lee MS, Gritsch HA. Revised Cardiac Risk Index (RCRI) is a useful tool for evaluation of perioperative cardiac morbidity in kidney transplant recipients. Transplantation 2013;96(7):639-43. [DOI] [PubMed] [Google Scholar]
Hokari 2015 {published data only}
- Hokari S, Ohshima Y, Nakayama H, Suzuki R, Kajiwara T, Koya T, et al. Superiority of respiratory failure risk index in prediction of postoperative pulmonary complications after digestive surgery in Japanese patients. Respiratory Investigation 2015;53(3):104-10. [DOI] [PubMed] [Google Scholar]
Holcomb 2016 {published data only}
- Holcomb CN, Graham LA, Richman JS, Itani KM, Maddox TM, Hawn MT. The incremental risk of coronary stents on postoperative adverse events: a matched cohort study. Annals of Surgery 2016;263(5):924-30. [DOI] [PubMed] [Google Scholar]
Holcomb 2016a {published data only}
- Holcomb CN, Hollis RH, Graham LA, Richman JS, Valle JA, Itani KM, et al. Association of coronary stent indication with postoperative outcomes following noncardiac surgery. JAMA Surgery 2016;151(5):462-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hollis 2016 {published data only}
- Hollis RH, Holcomb CN, Valle JA, Smith BP, DeRussy AJ, Graham LA, et al. Coronary angiography and failure to rescue after postoperative myocardial infarction in patients with coronary stents undergoing noncardiac surgery. American Journal of Surgery 2016;212(5):814-22.e1. [DOI] [PubMed] [Google Scholar]
Huang 2017 {published data only}
- Huang Y, Lee M, Chong HC, Ning Y, Lo NN, Yeo SJ. Reasons and factors behind post-total knee arthroplasty dissatisfaction in an Asian population. Annals of the Academy of Medicine, Singapore 2017;46(8):303-9. [PubMed] [Google Scholar]
Jakobson 2014 {published data only}
- Jakobson T, Karjagin J, Vipp L, Padar M, Parik AH, Starkopf L, et al. Postoperative complications and mortality after major gastrointestinal surgery. Medicina (Kaunas, Lithuania) 2014;50(2):111-7. [DOI] [PubMed] [Google Scholar]
Kamber 2018 {published data only}
- Kamber F, Mauermann E, Seeberger E, Guerke L, Mueller C, Bolliger D, et al. Peri-operative copeptin concentrations and their association with myocardial injury after vascular surgery: a prospective observational cohort study. European Journal of Anaesthesiology 2018;35(9):682-90. [DOI] [PubMed] [Google Scholar]
Kanakaraj 2017 {published data only}
- Kanakaraj M, Yates DR, Wilson RJ, Baroni ML, Davies SJ. Prognostic markers of outcome in patients undergoing infra-inguinal revascularisation: a prospective observational pilot study. European Journal of Vascular and Endovascular Surgery 2017;54(2):212-9. [DOI] [PubMed] [Google Scholar]
Karakas 2013 {published data only}
- Karakas M, Koenig W. Improved peri-operative risk stratification in non-cardiac surgery: going beyond established clinical scores. European Heart Journal 2013;34(11):796-8. [DOI] [PubMed] [Google Scholar]
Kazimierczak 2015 {published data only}
- Kazimierczak A, Szumilowicz P, Wiernicki I, Gutowski P, Samad R, Kupicz H, et al. Leucocytosis as a specific risk predictor after abdominal aortic aneurysm open repair. Pomeranian Journal of Life Sciences 2015;61(1):5-11. [DOI] [PubMed] [Google Scholar]
Kerry 2011 {published data only}
- Kerry R, Pouchet B. Revised cardiac risk index and postoperative morbidity after elective orthopaedic surgery. British Journal of Anaesthesia 2011;106(5):750. [DOI] [PubMed] [Google Scholar]
Kertai 2004 {published data only}
- Kertai MD, Bountioukos M, Boersma E, Bax JJ, Thomson IR, Sozzi F, et al. Aortic stenosis: an underestimated risk factor for perioperative complications in patients undergoing noncardiac surgery. American Journal of Medicine 2004;116(1):8-13. [DOI] [PubMed] [Google Scholar]
Khambalia 2015 {published data only}
- Khambalia HA, Moinuddin Z, Summers AM, Tavakoli A, Pararajasingam R, Campbell T, et al. A prospective cohort study of risk prediction in simultaneous pancreas and kidney transplantation. Annals of the Royal College of Surgeons of England 2015;97(6):445-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kikura 2008 {published data only}
- Kikura M, Oikawa F, Yamamoto K, Iwamoto T, Tanaka KA, Sato S, et al. Myocardial infarction and cerebrovascular accident following non-cardiac surgery: differences in postoperative temporal distribution and risk factors. Journal of Thrombosis and Haemostasis 2008;6(5):742-8. [DOI] [PubMed] [Google Scholar]
Kim 2013 {published data only}
- Kim TY, Yun WS, Park K. Cardiac risk factors of revascularization in chronic atherosclerotic lower extremity ischemia. Journal of The Korean Surgical Society 2013;84(3):178-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2016 {published data only}
- Kim S, Marsh AP, Rustowicz L, Roach C, Leng X I, Kritchevsky SB, et al. Self-reported mobility in older patients predicts early postoperative outcomes after elective noncardiac surgery. Anesthesiology 2016;124(4):815-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2016a {published data only}
- Kim IJ, Moon JY, Ko EJ, Lim YM, Kim SH, Yang WI, et al. Prognostic value of preoperative N-terminal pro-brain natriuretic peptide in non-cardiac surgery of elderly patients with normal left ventricular systolic function. Geriatrics & Gerontology International 2016;16(10):1109-16. [DOI] [PubMed] [Google Scholar]
Kim 2018 {published data only}
- Kim BS, Kim TH, Oh JH, Kwon CH, Kim SH, Kim HJ, et al. Association between preoperative high sensitive troponin I levels and cardiovascular events after hip fracture surgery in the elderly. Journal of Geriatric Cardiology 2018;15(3):215-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2019 {published data only}
- Kim KS, Park YS, Moon YJ, Jung KW, Kang J, Hwang GS. Preoperative myocardial ischemia detected with electrocardiography is associated with reduced 1-year survival rate in patients undergoing liver transplant. Transplantation Proceedings 2019;51(8):2755-60. [DOI] [PubMed] [Google Scholar]
Kistan 2018 {published data only}
- Kistan K, Moodley Y. Are abnormal pre-operative platelet counts a risk factor for major adverse cardiovascular events following non-cardiac surgery? Online Journal of Health and Allied Sciences 2018;17(3):1. [Google Scholar]
Koh 2012 {published data only}
- Koh AS, Flores JL, Keng FY, Tan RS, Chua TS. Correlation between clinical outcomes and appropriateness grading for referral to myocardial perfusion imaging for preoperative evaluation prior to non-cardiac surgery. Journal of Nuclear Cardiology 2012;19(2):277-84. [DOI] [PubMed] [Google Scholar]
Kougias 2013 {published data only}
- Kougias P, Orcutt S, Pak T, Pisimisis G, Barshes NR, Lin PH, et al. Impact of postoperative nadir hemoglobin and blood transfusion on outcomes after operations for atherosclerotic vascular disease. Journal of Vascular Surgery 2013;57(5):1331-7; discussion. [DOI] [PubMed] [Google Scholar]
Kougias 2017 {published data only}
- Kougias P, Sharath S, Barshes NR, Chen M, Mills JL Sr. Effect of postoperative anemia and baseline cardiac risk on serious adverse outcomes after major vascular interventions. Journal of Vascular Surgery 2017;66(6):1836-43. [DOI] [PubMed] [Google Scholar]
Kronzer 2016 {published data only}
- Kronzer VL, Ben AA, McKinnon SL, Wildes TS, Avidan MS. Ability of preoperative falls to predict postsurgical outcomes in non-selected patients undergoing elective surgery at an academic medical centre: protocol for a prospective cohort study. BMJ Open 2016;6(9):e011570. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kronzer 2016a {published data only}
- Kronzer VL, Jerry MR, Ben AA, Wildes TS, Stark SL, McKinnon SL, et al. Preoperative falls predict postoperative falls, functional decline, and surgical complications. Ebiomedicine 2016;12:302-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kumar 2017 {published data only}
- Kumar P, Renuka MK, Kalaiselvan MS, Arunkumar AS. Outcome of noncardiac surgical patients admitted to a multidisciplinary intensive care unit. Indian Journal of Critical Care Medicine 2017;21(1):17-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Küpper 2015 {published data only}
- Kuepper S, Karvellas CJ, Khadaroo RG, Widder S. Increased health services use by severely obese patients undergoing emergency surgery: a retrospective cohort study. Canadian Journal of Surgery 2015;58(1):41-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ladha 2018 {published data only}
- Ladha KS, Beattie WS, Tait G, Wijeysundera DN. Association between preoperative ambulatory heart rate and postoperative myocardial injury: a retrospective cohort study. British Journal of Anaesthesia 2018;121(4):722-9. [DOI] [PubMed] [Google Scholar]
Lau 2013 {published data only}
- Lau WC, Froehlich JB, Jewell ES, Montgomery DG, Eng KM, Shields TA, et al. Impact of adding aspirin to beta-blocker and statin in high-risk patients undergoing major vascular surgery. Annals of Vascular Surgery 2013;27(4):537-45. [DOI] [PubMed] [Google Scholar]
Lee 1999 {published data only}
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100(10):1043-9. [DOI] [PubMed] [Google Scholar]
Leibowitz 2009 {published data only}
- Leibowitz D, Rivkin G, Schiffman J, Rott D, Weiss AT, Mattan Y, et al. Effect of severe aortic stenosis on the outcome in elderly patients undergoing repair of hip fracture. Gerontology 2009;55(3):303-6. [DOI] [PubMed] [Google Scholar]
Levitan 2016 {published data only}
- Levitan EB, Graham LA, Valle JA, Richman JS, Hollis R, Holcomb CN, et al. Pre-operative echocardiography among patients with coronary artery disease in the United States Veterans Affairs healthcare system: a retrospective cohort study. BMC Cardiovascular Disorders 2016;16(1):173. [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2016 {published data only}
- Li Y, Xing H, Xie G. Predicative value of preoperative C-reactive protein for postoperative adverse cardiac events in patients undergoing major abdominal surgery. International Journal of Clinical and Experimental Pathology 2016;9(11):11904-10. [Google Scholar]
Licker 2011 {published data only}
- Licker M, Cartier V, Robert J, Diaper J, Villiger Y, Tschopp JM, et al. Risk factors of acute kidney injury according to RIFLE criteria after lung cancer surgery. Annals of Thoracic Surgery 2011;91(3):844-51. [DOI] [PubMed] [Google Scholar]
Licker 2013 {published data only}
- Licker M, Christoph E, Cartier V, Mugnai D, Murith N, Kalangos A, et al. Impact of anesthesia technique on the incidence of major complications after open aortic abdominal surgery: a cohort study. Journal of Clinical Anesthesia 2013;25(4):296-308. [DOI] [PubMed] [Google Scholar]
Liem 2018 {published data only}
- Liem VG, Hoeks SE, Grune F, Mol KH, Wesdorp FH, Stolker RJ, et al. Prognostic value of postoperative high-sensitivity troponin T in patients with different stages of kidney disease undergoing noncardiac surgery. British Journal of Anaesthesia 2018;120(1):84-93. [DOI] [PubMed] [Google Scholar]
Lin 2005 {published data only}
- Lin M, Haukoos J, Tahernia A, Virgilio C. Cardiac morbidity and mortality after surgery for gastrointestinal carcinomas. American Surgeon 2005;71(10):833-6. [PubMed] [Google Scholar]
Lin 2016 {published data only}
- Lin MJ, Housley BC, Kelly N, Pletcher E, Balshi JD, Stawicki SP, et al. Temporal variability of readmission determinants in postoperative vascular surgery patients. Journal of Postgraduate Medicine 2016;62(4):216-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lin 2017 {published data only}
- Lin H, Peel NM, Scott IA, Vardesh DL, Sivalingam P, McBride RL, et al. Perioperative assessment of older surgical patients using a frailty index-feasibility and association with adverse postoperative outcomes. Anaesthesia and Intensive Care 2017;45(6):676-82. [DOI] [PubMed] [Google Scholar]
Lindenauer 2004 {published data only}
- Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA 2004;291(17):2092-9. [DOI] [PubMed] [Google Scholar]
Lindenauer 2005 {published data only}
- Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. New England Journal of Medicine 2005;353(4):349-61. [DOI] [PubMed] [Google Scholar]
Liu 2013 {published data only}
- Liu Z, Yu C, Xu L, Han W, Jiang J, Huang Y. Risk factors for perioperative major cardiac events in Chinese elderly patients with coronary heart disease undergoing noncardiac surgery. Chinese Medical Journal 2013;126(18):3464-9. [PubMed] [Google Scholar]
Lo 2014 {published data only}
- Lo SP, Chechi T, Gensini GF, Troisi N, Pratesi C, Chiti E, et al. Impact of two different cardiac work-up strategies in patients undergoing abdominal aortic aneurysm repair. International Journal of Cardiology 2014;175(1):E1-E3. [DOI] [PubMed] [Google Scholar]
Long 2016 {published data only}
- Long TE, Helgason D, Helgadottir S, Palsson R, Gudbjartsson T, Sigurdsson GH, et al. Acute kidney injury after abdominal surgery: incidence, risk factors, and outcome. Anesthesia and Analgesia 2016;122(6):1912-20. [DOI] [PubMed] [Google Scholar]
Lucreziotti 2007 {published data only}
- Lucreziotti S, Conforti S, Carletti F, Santaguida G, Meda S, Raveglia F, et al. Cardiac troponin-I elevations after thoracic surgery. Incidence and correlations with baseline clinical characteristics, C-reactive protein and perioperative parameters. Revista Espanola De Cardiologia 2007;60(11):1159-66. [PubMed] [Google Scholar]
Lupei 2014 {published data only}
- Lupei MI, Chipman JG, Beilman GJ, Oancea SC, Konia MR. The association between ASA status and other risk stratification models on postoperative intensive care unit outcomes. Anesthesia & Analgesia 2014;118(5):989-94. [DOI] [PubMed] [Google Scholar]
Maas 2007 {published data only}
- Maas R, Dentz L, Schwedhelm E, Thoms W, Kuss O, Hiltmeyer N, et al. Elevated plasma concentrations of the endogenous nitric oxide synthase inhibitor asymmetric dimethylarginine predict adverse events in patients undergoing noncardiac surgery. Critical Care Medicine 2007;35(8):1876-81. [DOI] [PubMed] [Google Scholar]
MacIntyre 2018 {published data only}
- MacIntyre PA, Scott M, Seigne R, Clark A, Deveer F, Minchin I. An observational study of perioperative risk associated with aortic stenosis in non-cardiac surgery. Anaesthesia & Intensive Care 2018;46(2):207-14. [DOI] [PubMed] [Google Scholar]
Mahmoud 2016 {published data only}
- Mahmoud KD, Sanon S, Habermann EB, Lennon RJ, Thomsen KM, Wood DL, et al. Perioperative cardiovascular risk of prior coronary stent implantation among patients undergoing noncardiac surgery. Journal of the American College of Cardiology 2016;67(9):1038-49. [DOI] [PubMed] [Google Scholar]
Mann 2020 {published data only}
- Mann J, Williams M, Wilson J, Yates D, Harrison A, Doherty P, et al. Exercise-induced myocardial dysfunction detected by cardiopulmonary exercise testing is associated with increased risk of mortality in major oncological colorectal surgery. British Journal of Anaesthesia 2020 Feb 19 [Epub ahead of print]. [DOI] [PubMed]
Marinho 2018 {published data only}
- Marinho R, Lusquinhos J, Carvalho B, Azevedo J, Santos A, Abelha F. Quality of recovery after surgery for cancer treatment. Revista Espanola de Anestesiologia y Reanimacion 2018;65(8):426-33. [DOI] [PubMed] [Google Scholar]
Marsman 2020 {published data only}
- Marsman M, Waes JA, Grobben RB, Weersink CS, Klei WA. Added value of subjective assessed functional capacity before non-cardiac surgery in predicting postoperative myocardial injury. European Journal of Preventive Cardiology 2020;28(3):262-9. [DOI] [PubMed] [Google Scholar]
Marston 2013 {published data only}
- Marston N, Soval Y, Zakharova M, Brenes-Salazar J, Santili S, Adabag S, et al. Troponin elevations following vascular surgery in patients without preoperative myocardial ischemia. Southern Medical Journal 2013;106(11):612-7. [DOI] [PubMed] [Google Scholar]
Martins 2011 {published data only}
- Martins OM, Fonseca VF, Borges I, Martins V, Portal VL, Pella LC. C-Reactive protein predicts acute myocardial infarction during high-risk noncardiac and vascular surgery. Clinics 2011;66(5):773-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mases 2014 {published data only}
- Mases A, Sabate S, Guilera N, Sadurni M, Arroyo R, Fau M, et al. Preoperative estimated glomerular filtration rate and the risk of major adverse cardiovascular and cerebrovascular events in non-cardiac surgery. British Journal of Anaesthesia 2014;113(4):644-51. [DOI] [PubMed] [Google Scholar]
Matsumoto 2016 {published data only}
- Matsumoto S, Takayama T, Wakatsuki K, Tanaka T, Migita K, Ito M, et al. Preoperative cardiac risk assessment and surgical outcomes of patients with gastric cancer. Annals of Surgical Oncology 2016;23:S222-9. [DOI] [PubMed] [Google Scholar]
May 2019 {published data only}
- May SM, Reyes A, Martir G, Reynolds J, Paredes LG, Karmali S, et al. Acquired loss of cardiac vagal activity is associated with myocardial injury in patients undergoing noncardiac surgery: prospective observational mechanistic cohort study. British Journal of Anaesthesia 2019;123(6):758-67. [DOI] [PubMed] [Google Scholar]
McIlroy 2015 {published data only}
- McIlroy DR, Chan MT, Wallace SK, Grover A, Koo EG, Ma J, et al. Is preoperative endothelial dysfunction a potentially modifiable risk factor for renal injury associated with noncardiac surgery? Journal of Cardiothoracic and Vascular Anesthesia 2015;29(5):1220-8. [DOI] [PubMed] [Google Scholar]
Meershoek 2020 {published data only}
- Meershoek AJ, Leunissen TC, Waes JA, Klei WA, Huisman A, Groot MC, et al. Reticulated platelets as predictor of myocardial injury and 30 day mortality after non-cardiac surgery. European Journal of Vascular and Endovascular Surgery 2020;59(2):309-18. [DOI] [PubMed] [Google Scholar]
Mendonca 2014 {published data only}
- Mendonca J, Pereira H, Xara D, Santos A, Abelha FJ. Obese patients: respiratory complications in the post-anesthesia care unit. Revista Portuguesa De Pneumologia 2014;20(1):12-9. [DOI] [PubMed] [Google Scholar]
Mitropoulos 2006 {published data only}
- Mitropoulos D, Banias K, Kotsakou D, Lampadariou K, Tsinari K, Anastasiou I, et al. Delayed surgical treatment of benign prostatic hyperplasia: a subjective estimation of change in the operative risk profile. Journal of Men's Health and Gender 2006;3(3):271-8. [Google Scholar]
Moitra 2011 {published data only}
- Moitra VK, Flynn BC, Mazzeffi M, Bodian C, Bronheim D, Ellis JE. Indication for surgery, the revised cardiac risk index, and 1-year mortality. Annals of Vascular Surgery 2011;25(7):902-8. [DOI] [PubMed] [Google Scholar]
Moodley 2015 {published data only}
- Moodley Y, Biccard BM. The impact of acute preoperative beta-blockade on perioperative cardiac morbidity and all-cause mortality in hypertensive South African vascular surgery patients. SAMJ: South African Medical Journal 2015;105(6):476-9. [DOI] [PubMed] [Google Scholar]
Moodley 2015a {published data only}
- Moodley Y, Biccard BM. Predictors of in-hospital mortality following non-cardiac surgery: Findings from an analysis of a South African hospital administrative database. SAMJ South African Medical Journal 2015;105(2):126-9. [DOI] [PubMed] [Google Scholar]
Mooney 2016 {published data only}
- Mooney JF, Hillis GS, Lee VW, Halliwell R, Vicaretti M, Moncrieff C, et al. Cardiac assessment prior to non-cardiac surgery. Internal Medicine Journal 2016;46(8):932-41. [DOI] [PubMed] [Google Scholar]
Moran 2008 {published data only}
- Moran PJ, Ghidella T, Power G, Jenkins AS, Whittle D. The use of Lee and co-workers' index to assist a risk adjusted audit of perioperative cardiac outcome. Anaesthesia & Intensive Care 2008;36(2):167-73. [DOI] [PubMed] [Google Scholar]
Moses 2018 {published data only}
- Moses DA, Johnston LE, Tracci MC, Robinson WP 3rd, Cherry KJ, Kern JA, et al. Estimating risk of adverse cardiac event after vascular surgery using currently available online calculators. Journal of Vascular Surgery 2018;67(1):272-8. [DOI] [PubMed] [Google Scholar]
Mureddu 2017 {published data only}
- Mureddu GF. Current multivariate risk scores in patients undergoing non-cardiac surgery. Monaldi Archives for Chest Disease 2017;87(2):848. [DOI] [PubMed] [Google Scholar]
Nagayoshi 2012 {published data only}
- Nagayoshi Y, Kawano H, Kojima S, Soejima H, Kaikita K, Nakayama M, et al. Significance of coronary vasospasm in the perioperative management of non-cardiac surgery. Circulation Journal 2012;76(8):1965-71. [DOI] [PubMed] [Google Scholar]
Nepogodiev 2015 {published data only}
- Nepogodiev D, Chapman SJ, Glasbey J, Kelly M, Khatri C, Drake TM, et al. Determining Surgical Complications in the Overweight (DISCOVER): a multicentre observational cohort study to evaluate the role of obesity as a risk factor for postoperative complications in general surgery. BMJ Open 2015;5(7):e008811. [DOI] [PMC free article] [PubMed] [Google Scholar]
Noordzij 2010 {published data only}
- Noordzij PG, Poldermans D, Schouten O, Bax JJ, Schreiner FA, Boersma E. Postoperative mortality in The Netherlands: a population-based analysis of surgery-specific risk in adults. Anesthesiology 2010;112(5):1105-15. [DOI] [PubMed] [Google Scholar]
Noordzij 2015 {published data only}
- Noordzij PG, Geffen O, Dijkstra IM, Boerma D, Meinders AJ, Rettig TC, et al. High-sensitive cardiac troponin T measurements in prediction of non-cardiac complications after major abdominal surgery. British Journal of Anaesthesia 2015;114(6):909-18. [DOI] [PubMed] [Google Scholar]
Nordling 2016 {published data only}
- Nordling P, Kiviniemi T, Stroberg M, Stroberg N, Airaksinen J. Predicting the outcome of hip fracture patients by using N-terminal fragment of pro-B-type natriuretic peptide. BMJ Open 2016;6(2):e009416. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nutt 2012 {published data only}
- Nutt CL, Russell JC. Use of the pre-operative shuttle walk test to predict morbidity and mortality after elective major colorectal surgery. Anaesthesia 2012;67(8):839-49. [DOI] [PubMed] [Google Scholar]
O'Neill 2016 {published data only}
- O'Neill BR, Batterham AM, Hollingsworth AC, Durr JW, Danjoux GR. Do first impressions count? Frailty judged by initial clinical impression predicts medium-term mortality in vascular surgical patients. Anaesthesia 2016;71(6):684-91. [DOI] [PubMed] [Google Scholar]
Oberweis 2015 {published data only}
- Oberweis B, Smilowitz NR, Nukala S, Rosenberg A, Xu J, Stuchin S, et al. Relation of perioperative elevation of troponin to long-term mortality after orthopedic surgery. American Journal of Cardiology 2015;115(12):1643-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ochroch 2006 {published data only}
- Ochroch EA, Gottschalk A, Troxel AB, Farrar JT. Women suffer more short and long-term pain than men after major thoracotomy. Clinical Journal of Pain 2006;22(5):491-8. [DOI] [PubMed] [Google Scholar]
Oliveros 2005 {published data only}
- Oliveros RH, Martínez PF, Lobelo GR, Santrich D. Factores de riesgo determinantes de mortalidad postoperatoria en UCI, en los pacientes quirúrgicos de alto riesgo. Revista Colombiana de Anestesiología 2005;33(1):17-23. [Google Scholar]
Oscarsson 2009 {published data only}
- Oscarsson A, Fredrikson M, Sorliden M, Anskar S, Eintrei C. N-terminal fragment of pro-B-type natriuretic peptide is a predictor of cardiac events in high-risk patients undergoing acute hip fracture surgery. British Journal of Anaesthesia 2009;103(2):206-12. [DOI] [PubMed] [Google Scholar]
Oscarsson 2009a {published data only}
- Oscarsson A, Fredrikson M, Sorliden M, Anskar S, Gupta A, Swahn E, et al. Predictors of cardiac events in high-risk patients undergoing emergency surgery. Acta Anaesthesiologica Scandinavica 2009;53(8):986-94. [DOI] [PubMed] [Google Scholar]
Oshin 2013 {published data only}
- Oshin OA, Torella F. Low hemoglobin concentration is associated with poor outcome after peripheral arterial surgery. Vascular and Endovascular Surgery 2013;47(6):449-53. [DOI] [PubMed] [Google Scholar]
Padayachee 2018 {published data only}
- Padayachee N, Rout C, Moodley Y. Postoperative major adverse cardiovascular events in South African non-cardiac surgery patients: does gender play a role? Surgical Chronicles 2018;23(3):170-3. [Google Scholar]
Paladugu 2020 {published data only}
- Paladugu S, Donato AA. Adding NT-proBNP to the Revised Cardiac Risk Index improved prediction of CV events after noncardiac surgery. Annals of Internal Medicine 2020;172(10):JC59. [DOI] [PubMed] [Google Scholar]
Parente 2013 {published data only}
- Parente D, Luis C, Veiga D, Silva H, Abelha F. Congestive heart failure as a determinant of postoperative delirium. Revista Portuguesa De Cardiologia 2013;32(9):665-71. [DOI] [PubMed] [Google Scholar]
Parikh 2020 {published data only}
- Parikh P, Banerjee K, Ali A, Anumandla A, Patel A, Jobanputra Y, et al. Impact of tricuspid regurgitation on postoperative outcomes after non-cardiac surgeries. Open Heart 2020;7(1):e001183. [DOI] [PMC free article] [PubMed] [Google Scholar]
Park 2018 {published data only}
- Park YS, Moon YJ, Jun IG, Song JG, Hwang GS. Application of the revised cardiac risk index to the model for end-stage liver disease score improves the prediction of cardiac events in patients undergoing liver transplantation. Transplantation Proceedings 2018;50(4):1108-13. [DOI] [PubMed] [Google Scholar]
Patel 2018 {published data only}
- Patel SK, Kacheriwala SM, Duttaroy DD. Audit of postoperative surgical intensive care unit admissions. Indian Journal of Critical Care Medicine 2018;22(1):10-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Patorno 2015 {published data only}
- Patorno E, Wang SV, Schneeweiss S, Liu J, Bateman BT. Patterns of β-blocker initiation in patients undergoing intermediate to high-risk noncardiac surgery. American Heart Journal 2015;170(4):812-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Patorno 2016 {published data only}
- Patorno E, Wang SV, Schneeweiss S, Liu J, Bateman BT. Initiation patterns of statin therapy among adult patients undergoing intermediate to high-risk non-cardiac surgery. Pharmacoepidemiology and Drug Safety 2016;25(1):64-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Payne 2011 {published data only}
- Payne CJ, Gibson SC, Bryce G, Jardine AG, Berry C, Kingsmore DB. B-type natriuretic peptide predicts long-term survival after major non-cardiac surgery. British Journal of Anaesthesia 2011;107(2):144-9. [DOI] [PubMed] [Google Scholar]
Payne 2013 {published data only}
- Payne CJ, Bryce GJ, Gibson SC, Kingsmore DB. The Revised Cardiac Risk Index performs poorly in patients undergoing major vascular surgery: a prospective observational study. European Journal of Anaesthesiology 2013;30(11):713-5. [DOI] [PubMed] [Google Scholar]
Pereira 2016 {published data only}
- Pereira KS, Oliveira JC, Carvalho FC, Bellen B. Complicações cardíacas em cirurgia vascular. Jornal Vascular Brasileiro 2016;15(1):16-20. [Google Scholar]
Pili‐Floury 2012 {published data only}
- Pili-Floury S, Ginet M, Saunier L, Besch G, Bartholin F, Chopard R, et al. Preoperative plasma B-type natriuretic peptide (BNP) identifies abnormal transthoracic echocardiography in elderly patients with traumatic hip fracture. Injury-International Journal of the Care of the Injured 2012;43(6):811-6. [DOI] [PubMed] [Google Scholar]
Pinho 2016 {published data only}
- Pinho C, Cruz S, Santos A, Abelha F. Postoperative delirium: age and low functional reserve as independent risk factors. Journal of Clinical Anesthesia 2016;33:507-13. [DOI] [PubMed] [Google Scholar]
Puelacher 2018 {published data only}
- Puelacher C, Buse GL, Seeberger D, Sazgary L, Marbot S, Lampart A, et al. Perioperative myocardial injury after noncardiac surgery incidence, mortality, and characterization. Circulation 2018;137(12):1221-32. [DOI] [PubMed] [Google Scholar]
Rajagopalan 2008 {published data only}
- Rajagopalan S, Croal BL, Bachoo P, Hillis GS, Cuthbertson BH, Brittenden J. N-terminal pro B-type natriuretic peptide is an independent predictor of postoperative myocardial injury in patients undergoing major vascular surgery. Journal of Vascular Surgery 2008;48(4):912-7. [DOI] [PubMed] [Google Scholar]
Rao 2012 {published data only}
- Rao JY, Yeriswamy MC, Santhosh MJ, Shetty GG, Varghese K, Patil C, et al. A look into Lee's score: peri-operative cardiovascular risk assessment in non-cardiac surgeries-usefulness of revised cardiac risk index. Indian Heart Journal 2012;64(2):134-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Redman 2014 {published data only}
- Redman LA, Naidoo P, Biccard BM. HIV, vascular surgery and cardiovascular outcomes: a South African cohort study. Anaesthesia 2014;69(3):208-13. [DOI] [PubMed] [Google Scholar]
Reeh 2016 {published data only}
- Reeh M, Metze J, Uzunoglu FG, Nentwich M, Ghadban T, Wellner U, et al. The PER (Preoperative Esophagectomy Risk) Score: a simple risk score to predict short-term and long-term outcome in patients with surgically treated esophageal cancer. Medicine 2016;95(7):e2724. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reeve 2018 {published data only}
- Reeve TE, Ur R, Craven TE, Kaan JH, Goldman MP, Edwards MS, et al. Grip strength measurement for frailty assessment in patients with vascular disease and associations with comorbidity, cardiac risk, and sarcopenia. Journal of Vascular Surgery 2018;67(5):1512-20. [DOI] [PubMed] [Google Scholar]
Reis 2018 {published data only}
- Reis PV, Sousa G, Lopes AM, Costa AV, Santos A, Abelha F, et al. Severity of disease scoring systems and mortality after non-cardiac surgery. Revista Brasileira De Anestesiologia 2018;68(3):244-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Richards 2015 {published data only}
- Richards CH, Roxburgh CS. Surgical outcome in patients undergoing reversal of Hartmann's procedures: a multicentre study. Colorectal Disease 2015;17(3):242-9. [DOI] [PubMed] [Google Scholar]
Richardson 2018 {published data only}
- Richardson KM, Shen ST, Gupta DK, Wells QS, Ehrenfeld JM. Prognostic significance and clinical utility of intraventricular conduction delays on the preoperative electrocardiogram. American Journal of Cardiology 2018;121(8):997-1003. [DOI] [PubMed] [Google Scholar]
Rinfret 2004 {published data only}
- Rinfret S, Goldman L, Polanczyk CA, Cook EF, Lee TH. Value of immediate postoperative electrocardiogram to update risk stratification after major noncardiac surgery. American Journal of Cardiology 2004;94(8):1017-22. [DOI] [PubMed] [Google Scholar]
Rodriguez 2018 {published data only}
- Rodriguez A, Guilera N, Mases A, Sierra P, Oliva JC, Colilles C. Management of antiplatelet therapy in patients with coronary stents undergoing noncardiac surgery: association with adverse events. British Journal of Anaesthesia 2018;120(1):67-76. [DOI] [PubMed] [Google Scholar]
Rodseth 2014 {published data only}
- Rodseth RN, Biccard BM, Le Manach Y, Sessler DI, Lurati BG, Thabane L, et al. The prognostic value of pre-operative and post-operative B-type natriuretic peptides in patients undergoing noncardiac surgery: B-type natriuretic peptide and N-terminal fragment of pro-B-type natriuretic peptide: a systematic review and individual patient data meta-analysis. Journal of the American College of Cardiology 2014;63(2):170-80. [DOI] [PubMed] [Google Scholar]
Rosenberg 2016 {published data only}
- Rosenberg A, Selounski V, Wardak H, Han J, Gowhari M, Hassan J, et al. Utility of the revised cardiac risk index for predicting postsurgical morbidity in Hb SC and Hb Sβ+-thalassemia sickle cell disease. American Journal of Hematology 2016;91(6):E316-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roshanov 2017 {published data only}
- Roshanov PS, Walsh M, Devereaux PJ, MacNeil SD, Lam NN, Hildebr AM, et al. External validation of the Revised Cardiac Risk Index and update of its renal variable to predict 30-day risk of major cardiac complications after non-cardiac surgery: rationale and plan for analyses of the VISION study. BMJ Open 2017;7(1):e013510. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roxburgh 2011 {published data only}
- Roxburgh CS, Platt JJ, Leitch EF, Kinsella J, Horgan PG, McMillan DC. Relationship between preoperative comorbidity, systemic inflammatory response, and survival in patients undergoing curative resection for colorectal cancer. Annals of Surgical Oncology 2011;18(4):997-1005. [DOI] [PubMed] [Google Scholar]
Sakuma 2010 {published data only}
- Sakuma LM, Machado FS, Martins M. Independent association of smoking with postoperative cardiac events and thirty-day mortality. Arquivos Brasileiros De Cardiologia 2010;94(5):625-32. [DOI] [PubMed] [Google Scholar]
Salinas 2012 {published data only}
- Salinas J, Mendez S, Virseda M, Arance I, Pelaquim H, Moreno Sierra J, et al. Urodynamic aspects of feminine urinary incontinence treated with slings. Actas Urologicas Espanolas 2012;36(2):79-85. [DOI] [PubMed] [Google Scholar]
Sankar 2014 {published data only}
- Sankar A, Johnson SR, Beattie WS, Tait G, Wijeysundera DN. Reliability of the American Society of Anesthesiologists physical status scale in clinical practice. British Journal of Anaesthesia 2014;113(3):424-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sankar 2019 {published data only}
- Sankar A, Beattie WS, Tait G, Wijeysundera DN. Evaluation of validity of the STOP-BANG questionnaire in major elective noncardiac surgery. British Journal of Anaesthesia 2019;122(2):255-62. [DOI] [PubMed] [Google Scholar]
Schier 2012 {published data only}
- Schier R, Hinkelbein J, Marcus H, Mehran R, El-Zein R, Hofstetter W, et al. Preoperative microvascular dysfunction: a prospective, observational study expanding risk assessment strategies in major thoracic surgery. Annals of Thoracic Surgery 2012;94(1):226-33. [DOI] [PubMed] [Google Scholar]
Schier 2013 {published data only}
- Schier R, Hinkelbein J, Marcus H, Smallwood A, Correa AM, Mehran R, et al. A novel technique for the assessment of preoperative cardiovascular risk: reactive hyperemic response to short-term exercise. Biomed Research International 2013;2013:837130. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shalaeva 2016 {published data only}
- Shalaeva EV, Saner H, Janabaev BB, Shalaeva A. Coronary artery calcium score and coronary computed tomographic angiography for major perioperative cardiovascular complications in symptomatic diabetic patients undergoing trans-femoral amputation. International Journal of Cardiology 2016;221:806-11. [DOI] [PubMed] [Google Scholar]
Silva 2020 {published data only}
- Silva DD, Casimiro LG, Oliveira MI, Ferreira LB, Abelha FJ. The very elderly surgical population in a critically ill scenario: clinical characteristics and outcomes. Brazilian Journal of Anesthesiology 2020;70(1):3-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Simeoni 2016 {published data only}
- Simeoni R, Breitenstein K, Eser D, Guntinas-Lichius O. Cardiac comorbidity in head and neck cancer patients and its influence on cancer treatment selection and mortality: a prospective cohort study. European Archives of Oto-Rhino-Laryngology 2016;273(9):2765-72. [DOI] [PubMed] [Google Scholar]
Skaro 2016 {published data only}
- Skaro AI, Gallon LG, Lyuksemburg V, Jay CL, Zhao L, Ladner DP, et al. The impact of coronary artery disease on outcomes after liver transplantation. Journal of Cardiovascular Medicine 2016;17(12):875-85. [DOI] [PubMed] [Google Scholar]
Smilowitz 2016 {published data only}
- Smilowitz NR, Oberweis B, Nukala S, Rosenberg A, Zhao S, Xu J, et al. Association between anemia, bleeding, and transfusion with long-term mortality following noncardiac surgery. American Journal of Medicine 2016;129(3):315-23.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smilowitz 2018 {published data only}
- Smilowitz NR, Gupta N, Guo Y, Beckman JA, Bangalore S, Berger JS. Trends in cardiovascular risk factor and disease prevalence in patients undergoing non-cardiac surgery. Heart 2018;104(14):1180-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smolock 2012 {published data only}
- Smolock CJ, Anaya-Ayala JE, Bismuth J, Naoum JJ, El Sayed HF, Peden EK, et al. Impact of metabolic syndrome on the outcomes of superficial femoral artery interventions. Journal of Vascular Surgery 2012;55(4):985-93.e1. [DOI] [PubMed] [Google Scholar]
Snowden 2010 {published data only}
- Snowden CP, Prentis JM, Anderson HL, Roberts DR, Renton M, Manas DM. Submaximal cardiopulmonary exercise testing predicts complications and hospital length of stay in patients undergoing major elective surgery. Annals of Surgery 2010;251(3):535-41. [DOI] [PubMed] [Google Scholar]
Snowden 2013 {published data only}
- Snowden CP, Prentis J, Jacques B, Anderson H, Manas D, Jones D, et al. Cardiorespiratory fitness predicts mortality and hospital length of stay after major elective surgery in older people. Annals of Surgery 2013;257(6):999-1004. [DOI] [PubMed] [Google Scholar]
Sousa 2016 {published data only}
- Sousa G, Lopes A, Reis P, Carvalho V, Santos A, Abelha F. Major cardiac events after non-cardiac surgery. World Journal of Surgery 2016;40(8):1802-8. [DOI] [PubMed] [Google Scholar]
Stevens 2017 {published data only}
- Stevens SM, Crane R, Pensak ML, Samy RN. Middle ear obliteration with blind-sac closure of the external auditory canal for spontaneous CSF otorrhea. Otolaryngology - Head & Neck Surgery 2017;156(3):534-42. [DOI] [PubMed] [Google Scholar]
Sunny 2018 {published data only}
- Sunny JC, Kumar D, Kotekar N, Desai N. Incidence and predictors of perioperative myocardial infarction in patients undergoing non-cardiac surgery in a tertiary care hospital. Indian Heart Journal 2018;70(3):335-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tao 2008 {published data only}
- Tao LS, Mackenzie CR, Charlson ME. Predictors of postoperative complications in the patient with diabetes mellitus. Journal of Diabetes & its Complications 2008;22(1):24-8. [DOI] [PubMed] [Google Scholar]
Tashiro 2014 {published data only}
- Tashiro T, Pislaru SV, Blustin JM, Nkomo VT, Abel MD, Scott CG, et al. Perioperative risk of major non-cardiac surgery in patients with severe aortic stenosis: a reappraisal in contemporary practice. European Heart Journal 2014;35(35):2372-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tavakoli 2009 {published data only}
- Tavakoli H, Salimi J, Amoli HA, Rezaii J, Hasibi M, Khashayar P. ASA and Goldman Scoring Systems in prediction of open cholecystectomy surgeries. Iranian Red Crescent Medical Journal 2009;11(2):220-1. [Google Scholar]
Teixeira 2014 {published data only}
- Teixeira C, Rosa R, Rodrigues N, Mendes I, Peixoto L, Dias S, et al. Acute kidney injury after major abdominal surgery: a retrospective cohort analysis. Critical Care Research & Practice 2014;2014:132175. [DOI] [PMC free article] [PubMed] [Google Scholar]
Toda 2018 {published data only}
- Toda H, Nakamura K, Nakagawa K, Watanabe A, Miyoshi T, Nishii N, et al. Diastolic dysfunction is a risk of perioperative myocardial injury assessed by high-sensitivity cardiac troponin T in elderly patients undergoing non-cardiac surgery. Circulation Journal 2018;82(3):775-82. [DOI] [PubMed] [Google Scholar]
Tong 2015 {published data only}
- Tong MZ, Pattakos G, He J, Rajeswaran J, Kattan MW, Barsoum WK, et al. Sequentially updated discharge model for optimizing hospital resource use and surgical patients' satisfaction. Annals of Thoracic Surgery 2015;100(6):2174-81. [DOI] [PubMed] [Google Scholar]
Toyonaga 2017 {published data only}
- Toyonaga Y, Asayama K, Maehara Y. Impact of systemic inflammatory response syndrome and surgical Apgar score on post-operative acute kidney injury. Acta Anaesthesiologica Scandinavica 2017;61(10):1253-61. [DOI] [PubMed] [Google Scholar]
Valentijn 2013 {published data only}
- Valentijn TM, Hoeks SE, Martienus KA, Bakker EJ, de Luijtgaarden KM, Verhagen HJ, et al. Impact of haemoglobin concentration on cardiovascular outcome after vascular surgery: a retrospective observational cohort study. European Journal of Anaesthesiology 2013;30(11):664-70. [DOI] [PubMed] [Google Scholar]
Valentijn 2013a {published data only}
- Valentijn TM, Galal W, Hoeks SE, Gestel YR, Verhagen HJ, Stolker RJ. Impact of obesity on postoperative and long-term outcomes in a general surgery population: a retrospective cohort study. World Journal of Surgery 2013;37(11):2560-8. [DOI] [PubMed] [Google Scholar]
van Kuijk 2009 {published data only}
- Kuijk JP, Dunkelgrun M, Schreiner F, Flu WJ, Galal W, Domburg RT, et al. Preoperative oral glucose tolerance testing in vascular surgery patients: long-term cardiovascular outcome. American Heart Journal 2009;157(5):919-25. [DOI] [PubMed] [Google Scholar]
Vanniyasingam 2016 {published data only}
- Vanniyasingam T, Rodseth RN, Lurati BG, Bolliger D, Burkhart CS, Cuthbertson BH, et al. Predicting the occurrence of major adverse cardiac events within 30 days of a vascular surgery: an empirical comparison of the minimum p value method and ROC curve approach using individual patient data meta-analysis. Springerplus 2016;5:304. [DOI] [PMC free article] [PubMed] [Google Scholar]
van Waes 2017 {published data only}
- Waes JA, Peelen LM, Kemperman H, Grobben RB, Nathoe HM, Klei WA. Kinetics of troponin I in patients with myocardial injury after noncardiac surgery. Clinical Chemistry & Laboratory Medicine 2017;55(4):586-94. [DOI] [PubMed] [Google Scholar]
Vanwagner 2012 {published data only}
- Vanwagner LB, Bhave M, Te HS, Feinglass J, Alvarez L, Rinella ME. Patients transplanted for nonalcoholic steatohepatitis are at increased risk for postoperative cardiovascular events. Hepatology 2012;56(5):1741-50. [DOI] [PubMed] [Google Scholar]
VanWagner 2014 {published data only}
- VanWagner LB, Lapin B, Levitsky J, Wilkins JT, Abecassis MM, Skaro AI, et al. High early cardiovascular mortality after liver transplantation. Liver Transplantation 2014;20(11):1306-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Veiga 2012 {published data only}
- Veiga D, Luis C, Parente D, Fernoes V, Botelho M, Santos P, et al. Postoperative delirium in intensive care patients: risk factors and outcome. Revista Brasileira De Anestesiologia 2012;62(4):469-83. [DOI] [PubMed] [Google Scholar]
Venkatraghavan 2015 {published data only}
- Venkatraghavan L, Tan TP, Mehta J, Arekapudi A, Govindarajulu A, Siu E. Neutrophil lymphocyte ratio as a predictor of systemic inflammation - a cross-sectional study in a pre-admission setting. F1000 Research 2015;4:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vetrugno 2018 {published data only}
- Vetrugno L, Orso D, Matellon C, Giaccalone M, Bove T, Bignami E. The possible use of preoperative natriuretic peptides for discriminating low versus moderate-high surgical risk patient. Seminars in Cardiothoracic and Vascular Anesthesia 2018;22(4):395-402. [DOI] [PubMed] [Google Scholar]
Waliszek 2011 {published data only}
- Waliszek M, Waliszek-Iwanicka A, Grycewicz T, Jurowski P, Banach M, Rysz J, et al. Prognostic value of plasma N-terminal pro-B-type natriuretic peptide concentration in patients with normal and impaired left ventricular systolic function undergoing surgery for abdominal aortic aneurysm. Archives of Medical Science 2011;7(4):642-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ward 2006 {published data only}
- Ward HB, Kelly RF, Thottapurathu L, Moritz TE, Larsen GC, Pierpont G, et al. Coronary artery bypass grafting is superior to percutaneous coronary intervention in prevention of perioperative myocardial infarctions during subsequent vascular surgery. Annals of Thoracic Surgery 2006;82(3):795-801. [DOI] [PubMed] [Google Scholar]
Warnakulasuriya 2017 {published data only}
- Warnakulasuriya SR, Yates DR, Wilson JT, Stone M, Redman J, Davies S. Cardiopulmonary exercise testing has no additive incremental value to standard scoring systems when risk stratifying for bariatric surgery. Obesity Surgery 2017;27(1):187-93. [DOI] [PubMed] [Google Scholar]
Weissman 2011 {published data only}
- Weissman C, Kleln N. Pre-operative evaluation using therapeutic intensity scoring. European Journal of Anaesthesiology 2011;28(1):20-8. [DOI] [PubMed] [Google Scholar]
Widmer 2018 {published data only}
- Widmer RJ, Cullen MW, Salonen BR, Sundsted KK, Raslau D, Mohabbat AB, et al. Cardiac events after noncardiac surgery in patients undergoing preoperative dobutamine stress echocardiography: findings from the Mayo Poce-DSE Investigators. American Journal of Medicine 2018;131(6):702.e15-e22. [DOI] [PubMed] [Google Scholar]
Wijeysundera 2010 {published data only}
- Wijeysundera DN, Beattie WS, Austin PC, Hux JE, Laupacis A. Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study. BMJ 2010;340:b5526. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wijeysundera 2011 {published data only}
- Wijeysundera DN, Beattie WS, Karkouti K, Neuman MD, Austin PC, Laupacis A. Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ 2011;342:d3695. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wijeysundera 2012 {published data only}
- Wijeysundera DN, Wijeysundera HC, Yun L, Wasowicz M, Beattie WS, Velianou JL, et al. Risk of elective major noncardiac surgery after coronary stent insertion: a population-based study. Circulation 2012;126(11):1355-62. [DOI] [PubMed] [Google Scholar]
Wijeysundera 2020 {published data only}
- Wijeysundera DN, Beattie WS, Hillis GS, Abbott TE, Shulman MA, Ackland GL, et al. Integration of the Duke Activity Status Index into preoperative risk evaluation: a multicentre prospective cohort study. British Journal of Anaesthesia 2020;124(3):261-70. [DOI] [PubMed] [Google Scholar]
Wilson 2010 {published data only}
- Wilson RJ, Davies S, Yates D, Redman J, Stone M. Impaired functional capacity is associated with all-cause mortality after major elective intra-abdominal surgery. British Journal of Anaesthesia 2010;105(3):297-303. [DOI] [PubMed] [Google Scholar]
Xara 2015 {published data only}
- Xara D, Mendonca J, Pereira H, Santos A, Abelha F. Adverse respiratory events after general anesthesia in patients at high risk of obstructive sleep apnea syndrome. Revista Brasileira De Anestesiologia 2015;65(5):359-66. [DOI] [PubMed] [Google Scholar]
Yun 2008 {published data only}
- Yun KH, Jeong MH, Oh SK, Choi JH, Rhee SJ, Park EM, et al. Preoperative plasma N-terminal pro-brain natriuretic peptide concentration and perioperative cardiovascular risk in elderly patients. Circulation Journal 2008;72(2):195-9. [DOI] [PubMed] [Google Scholar]
Yurtlu 2016 {published data only}
- Yurtlu DA, Aksun M, Ayvat P, Karahan N, Koroglu L, Aran GO. Comparison of risk scoring systems to predict the outcome in ASA-PS V patients undergoing surgery: a retrospective cohort study. Medicine 2016;95(13):e3238. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Alexander 2008 {published data only}
- Alexanderer S, Bosch JL, Hendriks JM, Visser JJ, Van Sambeek MR. The 30-day mortality of ruptured abdominal aortic aneurysms: influence of gender, age, diameter and comorbidities. Journal of Cardiovascular Surgery 2008;49(5):633-7. [PubMed] [Google Scholar]
Andreenko 2003 {published data only}
- Andreenko AA, Polushin IS, Pereloma VI, Shirokov DM, Singaevskii SB, Prishvin AP. Characteristics of hemodynamic reactions during various endoscopic surgeries for cholelithiasis in patients with concurrent cardiovascular pathologies. Anesteziologiia i Reanimatologiia 2003;(4):13-9. [PubMed] [Google Scholar]
Author unknown 2010 {published data only}
- Left ventricular systolic dysfunction and risk of postoperative complications in patients with non-coronary artery basins surgery. Russian Heart Failure Journal 2010;11(6):347-54.
Author unknown 2011 {published data only}
- Comparison of two methods for risk reduction of cardiac complications in vascular surgeries. Byulleten' NTsSSKh im. A.N. Bakuleva RAMN Serdechno-sosudistye zabolevaniya 2011;12(6):70-9.
Barbarash 2012 {published data only}
- Barbarash LS, Sumin AN, Evdokimov DO, Bezdenezhnykh AV, Korok EV, Ivanov SV, et al. Role of coronary angiography in decreasing cardiac complications rate during vascular operations. Angiologiia i Sosudistaia Khirurgiia/Angiology & Vascular Surgery 2012;18(4):33-41. [PubMed] [Google Scholar]
Can 2018 {published data only}
- Can MG, Kocyigit OI, Hayiruoglu MB, Kocyigit M, Kayhan Z. Preoperative evaluation of the patients with cardiovascular disease undergoing noncardiac surgery. Gogus-Kalp-Damar Anestezi ve Yogun Bakim Dernegi Dergisi 2018;24(1):16-22. [Google Scholar]
Caruso 2006 {published data only}
- Caruso GA, Capodanno D, Giannone MT, Giannazzo D, Monte I, Nigro P, et al. The usefulness of clinical indexes in the evaluation of cardiovascular risk in non cardiac surgery. Minerva Cardioangiologica 2006;54(6):763-72. [PubMed] [Google Scholar]
Dobrushina 2012 {published data only}
- Dobrushina OR, Korniyenko AN, Shklovsky BL, Tsarev MI, et al. Assessment of cardiac risk during extensive abdominal surgery in elderly and senile patients. Rossiiskii Meditsinskii Zhurnal 2012;(1):14-8. [Google Scholar]
Domínguez 2014 {published data only}
- Domínguez OD, Narváez PO. Rate of operative risk in noncardiac thoracic surgery. Revista del Instituto Nacional de Enfermedades Respiratorias 2014;73(1):18-23. [Google Scholar]
Faris 1999 {published data only}
- Faris PM, Spence RK, Larholt KM, Sampson AR, Frei D. The predictive power of baseline hemoglobin for transfusion risk in surgery patients. Orthopedics 1999;22(1):s135-40. [DOI] [PubMed] [Google Scholar]
Ghorra 1999 {published data only}
- Ghorra SG, Rzeczycki TP, Natarajan R, Pricolo VE. Colostomy closure: impact of preoperative risk factors on morbidity. American Surgeon 1999;65(3):266-9. [PubMed] [Google Scholar]
Gnocchi 2000 {published data only}
- Gnocchi C, Risso J, Khoury M, Torn A, Noel M, Baredes N, et al. Application of a preoperative evaluation model in patients undergoing elective abdominal surgery. Medicina-Buenos Aires 2000;60(1):125-34. [PubMed] [Google Scholar]
Grabowska‐Gawel 2004 {published data only}
- Grabowska-Gawel A. Combined subarachnoideal-extradural anesthesia for high-risk patients during surgery on the musculo-skeletal system. Ortopedia Traumatologia Rehabilitacja 2004;6(3):350-5. [PubMed] [Google Scholar]
Kapma 2017 {published data only}
- Kapma M, Kahmann O, Stijn I, Zeebregts CJ, Vahl A. Evaluation of risk prediction models, V-POSSUM and GAS, in patients with acute abdominal aortic rupture treated with EVAR or an open procedure. Journal of Cardiovascular Surgery 2017;58(3):439-45. [DOI] [PubMed] [Google Scholar]
Kavarana 2003 {published data only}
- Kavarana MN, Azimuddin K, Agarwal A, Balsano N, Cayten CG, Agarwal N. Hemodynamic monitoring in the elderly undergoing elective colon resection for cancer. American Surgeon 2003;69(5):411-5. [PubMed] [Google Scholar]
Kertai 2003 {published data only}
- Kertai MD, Boersma E, Bax JJ, den Meiracker AH, Urk H, Roel. Comparison between serum creatinine and creatinine clearance for the prediction of postoperative mortality in patients undergoing major vascular surgery. Clinical Nephrology 2003;59(1):17-23. [DOI] [PubMed] [Google Scholar]
Khan 2010 {published data only}
- Khan N, Naeem M, Bangash A, Sadiq M, Ahmad M, Nawaz H, et al. Prognostic indicators of mortality prior to surgery in esophageal cancer. Journal of Medical Sciences 2010;18(3):126-31. [Google Scholar]
Khoronenko 2009 {published data only}
- Khoronenko VE, Osipova NA, Lagutin MB, Shemetova MM. Diagnosis and prediction of the risk of perioperative cardiovascular events in geriatric patients in oncosurgical care. Anesteziologiya i Reanimatologiya 2009;(4):22-7. [PubMed] [Google Scholar]
Kim 2017 {published data only}
- Kim JM, Harris MB, Zurakowski D, Liu W, Jupiter JB, Kim JH, et al. Predictors of carpal tunnel release after open distal radius fracture. Journal of Surgical Orthopaedic Advances 2017;26(4):227-32. [PubMed] [Google Scholar]
Knaak 2020 {published data only}
- Knaak C, Brockhaus WR, Spies C, Borchers F, Piper SK, Radtke FM, et al. Presurgical cognitive impairment is associated with postoperative delirium and postoperative cognitive dysfunction. Minerva Anestesiologica 2020;86(4):394-403. [DOI] [PubMed] [Google Scholar]
Kozlov 2016 {published data only}
- Kozlov IA. Prevention of complications caused by myocardial ischemia-reperfusion in noncardiac surgical procedures. Byulleten Sibirskoy Meditsiny 2016;15(3):102-19. [Google Scholar]
Kuznetsov 2018 {published data only}
- Kuznetsov NA. Prediction of outcomes in elective surgery. Klinicheskaya Meditsina 2018;96(1):49-54. [Google Scholar]
Law 2014 {published data only}
- Law TR, Fludder V, Dizdarevic S, Singh N, Yusuf S, Thorburn P. The value of myocardial perfusion imaging in predicting cardiac events and hospital length of stay in abdominal aortic aneurysm repair. Anaesthesia 2014;69:40. [Google Scholar]
Leo 2005 {published data only}
- Leo E, Biancari F, Hanhela R, Karlqvist K, Romsi P, Ylonen K, et al. Baseline oxygen delivery is associated with an increased risk of severe postoperative complications after elective open repair of abdominal aortic aneurysm. Journal of Cardiovascular Surgery 2005;46(3):279-84. [PubMed] [Google Scholar]
Li 2016a {published data only}
- Li H, Feng G, Lin R, Zhang Y, Yao X. Prognostic value of preoperative D-dimer in metastatic renal cell carcinoma patients with targeted therapy. Chinese Journal of Clinical Oncology 2016;43(22):992-6. [Google Scholar]
Li 2018 {published data only}
- Li CJ, Guo C, Wang BJ, Mu DL, Wang DX. Relationship between preoperative abnormal echocardiography and occurrence of postoperative major adverse cardiac events in non-cardiac surgery patients: a nested case-control study. Medical Journal of Chinese People's Liberation Army 2018;43(2):158-65. [Google Scholar]
Macan 2004 {published data only}
- Macan JS, Karadža V, Kogler J, Majerič Kogler V. Role of transthoracic echocardiography in preoperative evaluation of high risk patients for thoracic surgery. Acta Medica Croatica 2004;58(3):221-4. [PubMed] [Google Scholar]
Martinez 2018 {published data only}
- Martinez M, Sosa C, Velescu A, Llort C, Elosua R, Clara A. Predictive factors of a poor outcome following revascularization for critical limb ischemia: implications for practice. International Angiology 2018;37(5):370-6. [DOI] [PubMed] [Google Scholar]
Maruoka 2018 {published data only}
- Maruoka T, Murashima K, Kayashima K. Factors predicting postoperative complications in patients with severe preoperative co-existing diseases. Japanese Journal of Anesthesiology 2018;67:213-7. [Google Scholar]
Moodley 2018 {published data only}
- Moodley Y. Impact of an unknown HIV serostatus on the risk of postoperative cardiovascular morbidity and mortality. University of Toronto Medical Journal 2018;95(2):32-6. [Google Scholar]
Mori 2014 {published data only}
- Mori S, Choi Y, Park MS, Kim H, Hong G, Yi NJ, et al. Usefulness of preoperative c-reactive protein and alpha-fetoprotein levels for prognostication of patients with hepatocellular carcinoma after living donor liver transplantation. Hepato-Gastroenterology 2014;61(136):2353-8. [PubMed] [Google Scholar]
Peretich (year of publication unknown) {published data only}
- Peretich KT, Engoren M, Jewell ES, Maile MD. Comparison of various preoperative echocardiogram measurements for predicting 30 day mortality after non-cardiac surgery. Anesthesia and Analgesia unknown;122:unknown. [Google Scholar]
Ray 2013 {published data only}
- Ray KK. Erratum: Incremental value of high-sensitive troponin T in addition to the revised cardiac index for perioperative risk stratification in non-cardiac surgery (European Heart Journal (2013) 34:11 (853-862) DOI: 10.1093/eurheartj/ehs445). European Heart Journal 2013;34(24):1777. [DOI] [PubMed] [Google Scholar]
Shevchenko 2005 {published data only}
- Shevchenko YL, Ablitsov YA, Kuznetsov NA, Anisimova OV. Lung carcinoma under combined and competitive pathologies: prognosis of radical surgery. Pul'monologiya 2005;1:16-23. [Google Scholar]
Stelzner 2003 {published data only}
- Stelzner S, Hellmich G, Koch R, Albert W, Ludwig K. Perioperative risk assessment in surgery - an analysis in 10395 patients. Zentralblatt Fur Chirurgie 2003;128(11):963-9. [DOI] [PubMed] [Google Scholar]
Sumin 2012 {published data only}
- Sumin AN, Gayfulin RA, Evdokimov DO, Korok EV, Bezdenezhnykh AV, Ivanov SV, et al. Impact of elder age on perioperative complications risk in non-coronary vascular surgery. Uspekhi Gerontologii 2012;25(1):143-51. [PubMed] [Google Scholar]
Sumin 2013 {published data only}
- Sumin AN, Gayfulin RA, Korok EV, Panfilov SD, Evdokimov DO, Raykh OI, et al. Long-term survival after reconstructive surgery on non-coronary arteries in different age groups. Uspekhi Gerontologii 2013;26(3):501-10. [PubMed] [Google Scholar]
Vanzetto 1999 {published data only}
- Vanzetto G, Sessa C, Magne JL, Guidicelli H, Ormezzano O, Fagret D, et al. Evaluation of a clinical and scintigraphy strategy of management of the cardiological risk before surgery of the abdominal aorta. Results in a series of 982 operated patients. Archives Des Maladies Du Coeur Et Des Vaisseaux 1999;92(2):211-8. [PubMed] [Google Scholar]
Wolf 2001 {published data only}
- Wolf YG, Loersberg G, Mosseri M, Schechter D, Anner H, Weissman C, et al. Preoperative dipyridamole-thallium scanning, selective coronary revascularization and long-term survival in patients with critical lower limb ischemia. Journal of Cardiovascular Surgery 2001;42(1):89-95. [PubMed] [Google Scholar]
Wunderlich 2005 {published data only}
- Wunderlich C, Gossrau G, Wunderlich E, Altmann E. Distinct factors correlating with adverse cardiac events after major vascular surgery. Vasa-Journal of Vascular Diseases 2005;34(1):46-9. [DOI] [PubMed] [Google Scholar]
Yamada 2019 {published data only}
- Yamada S, Osawa T, Abe T, Takada N, Matsumoto R, Ito Y, et al. The development of the preoperative nomogram predicting major perioperative complications after radical cystectomy with ileal conduit or orthotopic neobladder. Hinyokika Kiyo 2019;65(12):495-9. [DOI] [PubMed] [Google Scholar]
Yi 2015 {published data only}
- Yi A, Damodar D, Dacey M, Villacis D, Hatch GF. Quality of life and functional outcomes after multi-ligament knee reconstruction. Orthopaedic Journal of Sports Medicine 2015;3(7):2094-101. [Google Scholar]
Zarich 2001 {published data only}
- Zarich SW, Pierce ET, Nesto RW, Mittleman MA, Bode RH, Kowalchuk G, et al. Age and history of cardiac disease as risk factors for cardiac complications after peripheral vascular surgery in diabetic patients. Mayo Clinic Proceedings 2001;76(1):34-8. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
CTRI/2019/02/017668 {published data only}
- CTRI/2019/02/017668. To predict 30-day in hospital mortality and morbidity using preoperative hand grip strength and comparing it with existing revised cardiac risk index and Modified Frailty Index. ctri.nic.in/Clinicaltrials/showallp.php?mid1=31399&EncHid=&userName=017668 (first received 14 February 2019).
NCT01280253 {published data only}
- NCT01280253. Preoperative biochemical predictors of outcome in patients with hip fracture. clinicaltrials.gov/ct2/show/NCT01280253 (first received 20 January 2011).
NCT02146560 {published data only}
- NCT02146560. TEAMS (Troponin Elevation After Major Surgery) study. clinicaltrials.gov/ct2/show/NCT02146560 (first received 26 March 2014).
NCT02860754 {published data only}
- NCT02860754. The prognostic capabilities of a preoperative six-minute walk test to independently inform cardiovascular risk after major noncardiac surgery. clinicaltrials.gov/ct2/show/NCT02860754 (first received 9 August 2016).
NCT03016936 {published data only}
- NCT03016936. MET: REevaluation for Perioperative cArdIac Risk (MET-REPAIR). clinicaltrials.gov/ct2/show/NCT03016936 (first received 11 January 2017).
NCT03436238 {published data only}
- NCT03436238. Myocardial Injury in Noncardiac Surgery in Sweden (MINSS). clinicaltrials.gov/ct2/show/NCT03436238 (first received 19 February 2018).
Additional references
Beattie 2020
- Beattie WS, Lalu M, Bocock M, Feng S, Wijeysundera DN, Nagele P, et al. Systematic review and consensus definitions for the Standardized Endpoints in Perioperative Medicine (StEP) initiative: cardiovascular outcomes. British Journal of Anaesthesia 2020;126(1):56-66. [DOI] [PubMed] [Google Scholar]
Bertges 2010
- Bertges DJ, Goodney PP, Zhao Y, Schanzer A, Nolan BW, Likosky DS, et al. The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients. Journal of Vascular Surgery 2010;52(3):674-83, 683.e1-e3. [DOI] [PubMed] [Google Scholar]
Biccard 2011
- Biccard BM, Naidoo P. The role of brain natriuretic peptide in prognostication and reclassification of risk in patients undergoing vascular surgery. Anaesthesia 2011;66(5):379-85. [DOI] [PubMed] [Google Scholar]
Bilimoria 2013
- Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. Journal of the American College of Surgery 2013;217(5):833-42.e1-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Biomarkers Definitions Working Group 2001
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clinical and Pharmacological Therapy 2001;69(3):89-95. [DOI] [PubMed] [Google Scholar]
Bouwmeester 2012
- Bouwmeester W, Zuithoff NP, Mallett S, Geerlings MI, Vergouwe Y, Steyerberg EW, et al. Reporting and methods in clinical prediction research: a systematic review. PLoS Medicine 2012;9(5):e1001221. [DOI] [PMC free article] [PubMed] [Google Scholar]
Choi 2010
- Choi JH, Cho DK, Song YB, Hahn JY, Choi S, Gwon HC, et al. Preoperative NT-proBNP and CRP predict perioperative major cardiovascular events in non-cardiac surgery. Heart 2010;96(1):56-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cohn 2018
- Cohn SL, Fernandez RN. Comparison of 4 cardiac risk calculators in predicting postoperative cardiac complications after noncardiac operations. American Journal of Cardiology 2018;121(1):125-30. [DOI] [PubMed] [Google Scholar]
Collins 2013
- Collins GS, Omar O, Shanyinde M, Yu LM. A systematic review finds prediction models for chronic kidney disease were poorly reported and often developed using inappropriate methods. Journal of Clinical Epidemiology 2013;66(3):268-77. [DOI] [PubMed] [Google Scholar]
Collins 2014
- Collins GS, Groot JA, Dutton S, Omar O, Shanyinde M, Tajar A, et al. External validation of multivariable prediction models: a systematic review of methodological conduct and reporting. BMC Medical Research Methodology 2014;14:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Collins 2015
- Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD). Annals of Internal Medicine 2015;162(10):735. [DOI] [PubMed] [Google Scholar]
Debray 2017
- Debray TP, Damen JA, Snell KI, Ensor J, Hooft L, Reitsma JB, et al. A guide to systematic review and meta-analysis of prediction model performance. BMJ 2017;356:i6460. [DOI] [PubMed] [Google Scholar]
Debray 2018
- Debray TP, Jong VMT. Metamisc: diagnostic and prognostic meta-analysis. CRAN.R-project.org/package=metamisc (accessed 1 August 2018).
Detsky 1986
- Detsky AS, Abrams HB, McLaughlin JR, Drucker DJ, Sasson Z, Johnston N, et al. Predicting cardiac complications in patients undergoing non-cardiac surgery. Journal of General Internal Medicine 1986;1(4):211-9. [DOI] [PubMed] [Google Scholar]
Devereaux 2012
- Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012;307(21):2295-304. [DOI] [PubMed] [Google Scholar]
Devereaux 2017
- Devereaux PJ, Biccard BM, Sigamani A, Xavier D, Chan MT, Srinathan SK, et al. Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2017;317(16):1642-51. [DOI] [PubMed] [Google Scholar]
Duceppe 2017
- Duceppe E, Parlow J, MacDonald P, Lyons K, McMullen M, Srinathan S, et al. Canadian Cardiovascular Society guidelines on perioperative cardiac risk assessment and management for patients who undergo noncardiac surgery. Canadian Journal of Cardiology 2017;33(1):17-32. [DOI] [PubMed] [Google Scholar]
Ehlert 2016
- Ehlert BA, Najafian A, Orion KC, Malas MB, Black JH III, Abularrage CJ. Validation of a modified Frailty Index to predict mortality in vascular surgery patients. Journal of Vascular Surgery 2016;63(6):1595-601.e2. [DOI] [PubMed] [Google Scholar]
Ekeloef 2016
- Ekeloef S, Alamili M, Devereaux PJ, Gögenur I. Troponin elevations after non-cardiac, non-vascular surgery are predictive of major adverse cardiac events and mortality: a systematic review and meta-analysis. British Journal of Anaesthesia 2016;117(5):559-68. [DOI] [PubMed] [Google Scholar]
Feringa 2007
- Feringa HH, Schouten O, Dunkelgrun M, Bax JJ, Boersma E, Elhendy A, et al. Plasma N-terminal pro-B-type natriuretic peptide as long-term prognostic marker after major vascular surgery. Heart 2007;93(2):226-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fleisher 2014
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA Guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 2014;130(24):2215-45. [DOI] [PubMed] [Google Scholar]
Ford 2010
- Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Annals of Internal Medicine 2010;152(1):26-35. [DOI] [PubMed] [Google Scholar]
Gage 2001
- Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 2001;285(22):2864-70. [DOI] [PubMed] [Google Scholar]
Geersing 2012
- Geersing GJ, Bouwmeester W, Zuithoff P, Spijker R, Leeflang M, Moons K, et al. Search filters for finding prognostic and diagnostic prediction studies in Medline to enhance systematic reviews. PLoS One 2012;7(2):e32844. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gillmann 2014
- Gillmann HJ, Meinders A, Grohennig A, Larmann J, Bünte C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Critical Care Medicine 2014;42(6):1498-506. [DOI] [PubMed] [Google Scholar]
Goldman 1977
- Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. New England Journal of Medicine 1977;297(16):845-50. [DOI] [PubMed] [Google Scholar]
Gualandro 2018
- Gualandro DM, Puelacher C, LuratiBuse G, Lampart A, Strunz C, Cardozo FA, et al. Comparison of high-sensitivity cardiac troponin I and T for the prediction of cardiac complications after non-cardiac surgery. American Heart Journal 2018;203:67-73. [DOI] [PubMed] [Google Scholar]
Gupta 2011
- Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011;124(4):381-7. [DOI] [PubMed] [Google Scholar]
Harrell 2015
- Harrell FE. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis. Springer International Publishing, 2015. [Google Scholar]
Heus 2018
- Heus P, Damen J, Pajouheshnia R, Scholten R, Reitsma JB, Collins GS, et al. Poor reporting of multivariable prediction model studies: towards a targeted implementation strategy of the TRIPOD statement. BMC Medicine 2018;16(1):120. [DOI] [PMC free article] [PubMed] [Google Scholar]
ISOSG 2016
- International Surgical Outcomes Study Group. Global patient outcomes after elective surgery: prospective cohort study in 27 low-, middle- and high-income countries. British Journal of Anaesthesia 2016;117(5):601-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
James 2014
- James S, Jhanji S, Smith A, O'Brien G, Fitzgibbon M, Pearse RM. Comparison of the prognostic accuracy of scoring systems, cardiopulmonary exercise testing, and plasma biomarkers: a single-centre observational pilot study. British Journal of Anaesthesia 2014;112(3):491-7. [DOI] [PubMed] [Google Scholar]
Jammer 2015
- Jammer I, Wickboldt N, Sander M, Smith A, Schultz M J, Pelosi P, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. European Journal of Anaesthesiology 2015;32(2):88-105. [DOI] [PubMed] [Google Scholar]
Katsanos 2015
- Katsanos S, Babalis D, Kafkas N, Mavrogenis A, Leong D, Parissis J, et al. B-type natriuretic peptide vs. cardiac risk scores for prediction of outcome following major orthopedic surgery. Journal of Cardiovascular Medicine 2015;16(6):465-71. [DOI] [PubMed] [Google Scholar]
Kip 2008
- Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovascular studies. Journal of the American College of Cardiology 2008;51(7):701-7. [DOI] [PubMed] [Google Scholar]
Kopec 2017
- Kopec M, Duma A, Helwani MA, Brown J, Brown F, Gage BF, et al. Improving prediction of postoperative myocardial infarction with high-sensitivity cardiac troponin T and NT-proBNP. Anesthesia and Analgesia 2017;124(2):398-405. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kreuzberger 2020
- Kreuzberger N, Damen JA, Trivella M, Estcourt LJ, Aldin A, Umlauff L, et al. Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: a systematic review and meta-analysis. Cochrane Database of Systematic Reviews 2020, Issue 7. Art. No: CD012022. [DOI: 10.1002/14651858.CD012022.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kristensen 2014
- Kristensen SD, Knuuti J, Saraste A, Anker S, Batker HE, Hert S, et al. 2014 ESC/ESA guidelines on non-cardiac surgery: cardiovascular assessment and management. European Heart Journal 2014;35(35):2383-431. [DOI] [PubMed] [Google Scholar]
Laupacis 1997
- Laupacis A, Sekar N, Stiell IG. Clinical prediction rules. A review and suggested modifications of methodological standards. JAMA 1997;277(6):488-94. [PubMed] [Google Scholar]
Lee 1999
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100(10):1043-9. [DOI] [PubMed] [Google Scholar]
Lip 2010
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest 2010;137(2):263-72. [DOI] [PubMed] [Google Scholar]
Mackey 2006
- Mackey WC, Fleisher LA, Haider S, Sheikh S, Cappelleri JC, Lee WC, et al. Perioperative myocardial ischemic injury in high-risk vascular surgery patients: Incidence and clinical significance in a prospective clinical trial. Journal of Vascular Surgery 2006;43(3):533-8. [DOI] [PubMed] [Google Scholar]
Mair 2018
- Mair J, Lindahl B, Hammarsten O, Muller C, Giannitsis E, Huber K, et al. How is cardiac troponin released from injured myocardium? European Heart Journal. Acute Cardiovascular Care 2018;7(6):553-60. [DOI] [PubMed] [Google Scholar]
Makary 2010
- Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. Journal of the American College of Surgeons 2010;210(6):901-8. [DOI] [PubMed] [Google Scholar]
Mallett 2010
- Mallett S, Royston P, Dutton S, Waters R, Altman DG. Reporting methods in studies developing prognostic models in cancer: a review. BMC Medicine 2010;8:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Markovic 2018
- Markovic D, Jevtovic-Stoimenov T, Stojanovic M, Vukovic A, Dinic V, Markovic-Zivkovic B, et al. Addition of clinical risk scores improves prediction performance of American Society of Anesthesiologists (ASA) physical status classification for postoperative mortality in older patients: a pilot study. European Geriatric Medicine 2018;9(1):51-9. [DOI] [PubMed] [Google Scholar]
Mayhew 2019
- Mayhew D, Mendonca V, Murthy BV. A review of ASA physical status - historical perspectives and modern developments. Anaesthesia 2019;74(3):373-9. [DOI] [PubMed] [Google Scholar]
McAlister 2015
- McAlister FA, Jacka M, Graham M, Youngson E, Cembrowski G, Bagshaw SM, et al. The prediction of postoperative stroke or death in patients with preoperative atrial fibrillation undergoing non-cardiac surgery: a VISION sub-study. Journal of Thrombosis and Haemostasis 2015;13(10):1768-75. [DOI] [PubMed] [Google Scholar]
McAlister 2020
- McAlister FA, Youngson E, Jacka M, Graham M, Conen D, Chan M, et al. A comparison of four risk models for the prediction of cardiovascular complications in patients with a history of atrial fibrillation undergoing non-cardiac surgery. Anaesthesia 2020;75(1):27-36. [DOI] [PubMed] [Google Scholar]
Mercantini 2012
- Mercantini P, Di Somma S, Magrini L, Kazemi NA, Scarinci A, La Torre M, et al. Preoperative brain natriuretic peptide (BNP) is a better predictor of adverse cardiac events compared to preoperative scoring system in patients who underwent abdominal surgery. World Journal of Surgery 2012;36(1):24-30. [DOI] [PubMed] [Google Scholar]
Moons 1999
- Moons KG, Es GA, Michel BC, Büller HR, Habbema JD, Grobbee DE. Redundancy of single diagnostic test evaluation. Epidemiology 1999;10(3):276-81. [PubMed] [Google Scholar]
Moons 2009
- Moons KG, Altman DG, Vergouwe Y, Royston P. Prognosis and prognostic research: application and impact of prognostic models in clinical practice. BMJ 2009;338:b606. [DOI] [PubMed] [Google Scholar]
Moons 2014
- Moons KG, Groot JA, Bouwmeester W, Vergouwe Y, Mallett S, Altman DG, et al. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: the CHARMS checklist. PLoS Medicine 2014;11(10):e1001744. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moons 2015
- Moons KG, Altman DG, Reitsma JB, Ioannidis JP, Macaskill P, Steyerberg EW, et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Annals of Internal Medicine 2015;162(1):W1-73. [DOI] [PubMed] [Google Scholar]
Moons 2019
- Moons KG, Wolff RF, Riley RD, Whiting PF, Westwood M, Collins GS, et al. PROBAST: a tool to assess risk of bias and applicability of prediction model studies: explanation and elaboration. Annals of Internal Medicine 2019;170(1):51-8. [DOI] [PubMed] [Google Scholar]
Myles 2016
- Myles PS, Grocott MP, Boney O, Moonesinghe SR. Standardizing end points in perioperative trials: towards a core and extended outcome set. British Journal of Anaesthesia 2016;116(5):586-9. [DOI] [PubMed] [Google Scholar]
Noordzij 2006
- Noordzij PG, Boersma E, Bax JJ, Feringa HH, Schreiner F, Schouten O, et al. Prognostic value of routine preoperative electrocardiography in patients undergoing noncardiac surgery. American Journal of Cardiology 2006;97(7):1103-6. [DOI] [PubMed] [Google Scholar]
Pantoja 2014
- Pantoja Muñoz HJ, Fernández RH, Guevara TW. Sensitivity, specificity and predictive values of the Goldman, Detsky and Lee cardiac indices. Revista Colombiana de Anestesiologia 2014;42(3):184-91. [Google Scholar]
Park 2011
- Park SJ, Choi JH, Cho SJ, Chang SA, Choi JO, Lee SC, et al. Comparison of transthoracic echocardiography with N-terminal pro-brain natriuretic peptide as a tool for risk stratification of patients undergoing major noncardiac surgery. Korean Circulation Journal 2011;41(9):505-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Peat 2014
- Peat G, Riley RD, Croft P, Morley KI, Kyzas PA, Moons KG, et al. Improving the transparency of prognosis research: the role of reporting, data sharing, registration, and protocols. PLoS Medicine 2014;11(7):e1001671. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pepys 2003
- Pepys MB, Hirschfield GM. C-reactive protein: a critical update. Journal of Clinical Investigation 2003;111(12):1805-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Piccini 2013
- Piccini JP, Stevens SR, Chang Y, Singer DE, Lokhnygina Y, Go AS, et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation 2013;127(2):224-32. [DOI] [PubMed] [Google Scholar]
Press 2006
- Press MJ, Chassin MR, Wang J, Tuhrim S, Halm EA. Predicting medical and surgical complications of carotid endarterectomy - comparing the risk indexes. Archives of Internal Medicine 2006;166(8):914-20. [DOI] [PubMed] [Google Scholar]
Ray 2010
- Ray MJ, Calabro LJ, Sirisena T, Crawford SA, Crawford RW, Walters DL. Pre-operative platelet-bound CD40 ligand is probably associated with peri-operative cardiac events in hip and knee arthroplasty. European Journal of Clinical Investigation 2010;40(6):497-503. [DOI] [PubMed] [Google Scholar]
Reis 2019
- Reis PV, Lopes AI, Leite D, Moreira J, Mendes L, Ferraz S, et al. Major cardiac events in patients admitted to intensive care after vascular noncardiac surgery: a retrospective cohort. Seminars in Cardiothoracic & Vascular Anesthesia 2019;23(3):293-9. [DOI] [PubMed] [Google Scholar]
Riley 2011
- Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta-analyses. BMJ 2011;342:d549. [DOI] [PubMed] [Google Scholar]
Riley 2019
- Riley RD, Windt D, Croft P, Moons KG. Prognosis Research in Health Care: Concepts, Methods, and Impact. Oxford University Press, 2019. [Google Scholar]
Rodseth 2011
- Rodseth RN, Buse GA, Bolliger D, Burkhart CS, Cuthbertson BH, Gibson SC, et al. The predictive ability of pre-operative b-type natriuretic peptide in vascular patients for major adverse cardiac events: an individual patient data meta-analysis. Journal of the American College of Cardiology 2011;58(5):522-9. [DOI] [PubMed] [Google Scholar]
Rohrig 2004
- Rohrig R, Junger A, Hartmann B, Klasen J, Quinzio L, Jost A, et al. The incidence and prediction of automatically detected intraoperative cardiovascular events in noncardiac surgery. Anesthesia and Analgesia 2004;98(3):569-77. [DOI] [PubMed] [Google Scholar]
Rose 2015
- Rose J, Weiser TG, Hider P, Wilson L, Gruen RL, Bickler SW. Estimated need for surgery worldwide based on prevalence of diseases: a modelling strategy for the WHO Global Health Estimate. Lancet. Global Health 2015;3 Suppl 2:S13-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Scrutinio 2014
- Scrutinio D, Guido G, Guida P, Passantino A, Angiletta D, Santoro D, et al. Combined use of high-sensitivity C-reactive protein and N-terminal pro-B-type natriuretic peptide for risk stratification of vascular surgery patients. Annals of Vascular Surgery 2014;28(6):1522-9. [DOI] [PubMed] [Google Scholar]
Sheth 2015
- Sheth T, Chan M, Butler C, Chow B, Tandon V, Nagele P, et al. Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study. BMJ 2015;350:h1907. [DOI] [PMC free article] [PubMed] [Google Scholar]
Steyerberg 2009
- Steyerberg EW. Clinical Prediction Models. New York, NY: Springer New York, 2009. [Google Scholar]
Subramaniam 2011
- Subramaniam B, Meroz Y, Talmor D, Pomposelli FB, Berlatzky Y, Landesberg G. A long-term survival score improves preoperative prediction of survival following major vascular surgery. Annals of Vascular Surgery 2011;25(2):197-203. [DOI] [PubMed] [Google Scholar]
Thygesen 2018
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction. Circulation 2018;138(20):e618-51. [DOI] [PubMed] [Google Scholar]
Van Calster 2019
- Van Calster B, McLernon DJ, Smeden M, Wynants L, Steyerberg EW. Calibration: the Achilles heel of predictive analytics. BMC Medicine 2019;17(1):230. [DOI] [PMC free article] [PubMed] [Google Scholar]
van Diepen 2014
- Diepen S, Youngson E, Ezekowitz JA, McAlister FA. Which risk score best predicts perioperative outcomes in nonvalvular atrial fibrillation patients undergoing noncardiac surgery? American Heart Journal 2014;168(1):60-7. [DOI] [PubMed] [Google Scholar]
van Klei 2007
- Klei WA, Bryson GL, Yang H, Kalkman CJ, Wells GA, Beattie WS. The value of routine preoperative electrocardiography in predicting myocardial infarction after noncardiac surgery. Annals of Surgery 2007;246(2):165-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
van Waes 2016
- Waes JA, Grobben RB, Nathoe HM, Kemperman H, Borst GJ, Peelen LM, et al. One-year mortality, causes of death, and cardiac interventions in patients with postoperative myocardial injury. Anesthesia and Analgesia 2016;123(1):29-37. [DOI] [PubMed] [Google Scholar]
Vernooij 2018
- Vernooij LM, Damen J, Klei WA, Moons K, Peelen LM. The added value of different biomarkers to the Revised Cardiac Risk Index to predict major adverse cardiac events and all‐cause mortality after noncardiac surgery. Cochrane Database of Systematic Reviews 2018, Issue 10. Art. No: CD013139. [DOI: 10.1002/14651858.CD013139] [DOI] [PMC free article] [PubMed] [Google Scholar]
Vetrugno 2014
- Vetrugno L, Langiano N, Gisonni R, Rizzardo A, Venchiarutti PE, Divella M, et al. Prediction of early postoperative major cardiac events after elective orthopedic surgery: the role of B-type natriuretic peptide, the revised cardiac risk index, and ASA class. BMC Anesthesiology 2014;14:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Viechtbauer 2010
- Viechtbauer W. Conducting meta-analyses in R with the metafor package. JSS Journal of Statistical Software 2010;36.
Weber 2013
- Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. European Heart Journal 2013;34(11):853-62. [DOI] [PubMed] [Google Scholar]
Weiser 2015
- Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 2015;385:S11. [DOI] [PubMed] [Google Scholar]
Wilcox 2019
- Wilcox T, Smilowitz NR, Xia Y, Berger JS. Cardiovascular risk scores to predict perioperative stroke in noncardiac surgery. Stroke 2019;50(8):2002-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wolff 2002
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Archives of Internal Medicine 2002;162(20):2269-76. [DOI] [PubMed] [Google Scholar]
Wolff 2019
- Wolff RF, Moons KG, Riley RD, Whiting PF, Westwood M, Collins GS, et al. PROBAST: a tool to assess the risk of bias and applicability of prediction model studies. Annals of Internal Medicine 2019;170(1):51-8. [DOI] [PubMed] [Google Scholar]
Yancy 2013
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013;128(16):e240-327. [DOI] [PubMed] [Google Scholar]