

Abstract
Mucous membrane pressure injury (MMPI) is associated with a history of medical device use at the site of injury. The current international guideline recommends they should be reported in incidence and prevalence studies. The aim of this systematic review was to analyse the incidence and prevalence of hospital‐acquired MMPI in adults admitted to acute hospital settings. Database searches (EBSCO CINAHL Complete, EBSCO Medline Complete, Embase, Scopus and Web of Science) were undertaken between October 2019 and February 2021, using search terms related to hospital‐acquired, mucosal and device‐related pressure injury/ulcer incidence and prevalence. Searches were limited to the English language. Articles published between 2008 and 2020, reporting incidence or prevalence of mucous membrane or medical device‐related pressure injury in non‐interventional samples were selected. Two authors assessed study bias and extracted data, with a third reviewer as arbitrator. Twenty‐one studies met inclusion criteria; most provided incidence data. No studies were found that specifically reported MMPI incidence or prevalence. It was possible to calculate incidence or prevalence from four studies; all were in intensive care settings. MMPI incidence of 0.8% and 30.4%, and prevalence of 1.7% and 3.7% were found. One study provided data that enabled calculation of prevalence of 0.1% in a non‐intensive care sample. Only one other study provided specific data about MMPI. It is concluded that there is insufficient evidence available to enable estimation of MMPI incidence or prevalence in either acute hospital or intensive care settings.
Keywords: incidence, mucous membrane, pressure injury, prevalence, systematic review
1. INTRODUCTION
Hospitalised adults are susceptible to adverse events such as pressure injuries (PI), which usually form over bony prominences. 1 Because these injuries are considered to be largely preventable, they are routinely reported as an indicator of the quality of care provided to hospital inpatients. 2 Mucous membrane pressure injuries (MMPI) differ, however. They are defined as PI located on mucous membranes with an associated history of medical device use at the site of the injury. 3 Thus, by definition, MMPI are medical device‐related pressure injuries (MDRPI). Medical devices associated with PI development include, among others, endotracheal tubes, oxygen tubing, bite blocks, nasogastric and orogastric tubes, urinary catheters, and faecal containment devices. 1
1.1. Background
Mucous membranes lack the protective keratinised layer of the skin and do not undergo reepithelialisation, 4 and are so delicate that depth of ulceration is not visible to the naked eye. 5 Several risk factors are associated with MDRPI and MMPI development. For example, patients with impaired sensory perception such as neuropathy, those with difficulty communicating their discomfort because of a language barrier or cognitive impairment, and orally intubated and/or unconscious/sedated patients are at greater risk. 6 Critically ill patients are more susceptible to PI because they tend to require more medical devices for therapeutic and monitoring purposes. 4 Risk factors for MMPI relate to management of the medical device in use, including tightness of the device securement method, rigidity or inelasticity of the device or its securement, improper use, poor positioning or ill‐fitment of the device, increased heat, moisture, and humidity, absence of practice guidelines, and the workload and experience levels of staff. 7 , 8 , 9 , 10 Because of the necessary use of various medical devices, MMPI are found more commonly in patients admitted to intensive care units (ICU).
In 2016, the National Pressure Ulcer Advisory Panel (NPUAP) clarified that MDRPI should not be considered as a separate category of PI and should be classified by stage using the same criteria as other PI. 5 However, MMPI should not be staged 1 as the international staging system is based on skin anatomy. Rather, they should be classified based on aetiology, that is, pressure associated with a history of medical device use at the site of injury. 5 Since publication of the 2014 international guideline, it has been recommended that MMPI are included in prevalence and incidence studies. 11 (p30) The current international guideline also states that MMPI should be “identified, monitored, reported and tracked in prevalence and incidence surveys”. 1 (p182) And, yet, there has been limited reporting of MMPI in the research literature to date. The tendency has been to report incidence and prevalence of all MDRPI without distinguishing those that are mucosal, thus it is difficult to determine the magnitude of their occurrence. For example, a recent systematic review and meta‐analysis of MDRPI identified a pooled incidence of 14% (95% CI 8%‐21%) and pooled prevalence of 11% (95% CI 6%‐18%) in adult patients across 10 heterogeneous studies. 12 Medical device type was identified separately, but occurrence of MMPI per se was not specified. Similarly, a large United States and Canadian point prevalence survey from 2016 reported an acute care setting MDRPI prevalence of 0.6% in a sample of 88 896 (including community‐acquired MDRPI) but did not identify those that were mucosal, as MMPI was not included as an option on the data collection form. 13 Furthermore, the sample was filtered, and included only patients with complete PI data. In a recent systematic review of ICU patients, a pooled MDRPI incidence across four studies of 3.9% (95% CI 0%‐16.7%) and a pooled prevalence across seven studies of 6.5% (95% CI 2.0%‐13.1%) were reported. 14 Again, MMPI was not reported separately. In summary, to date, there has been very limited reporting of the incidence or prevalence of MMPI.
2. METHODS AND REVIEW PROCESS
2.1. Aims
The aim of this systematic review was to analyse research studies that reported either the incidence or prevalence of hospital‐acquired MMPI in adults admitted to acute hospital settings.
The following research question guided this review:
What is the incidence and prevalence of MMPI in adults admitted to acute hospital settings?
2.2. Design
This systematic review was conducted based on Joanna Briggs Institute guidelines 15 and in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐analysis (PRISMA) guidelines. 16 The protocol was registered prospectively with PROSPERO, the International Prospective Register of Systematic Reviews. 17
2.3. Search methods
2.3.1. Search strategy
A preliminary literature search was undertaken in October 2019, with search terms formulated with the assistance of a university health services specialist librarian. The search terms and subject headings (exploded where relevant) were finalised and the following databases were systematically searched in October 2020 and again in February 2021: EBSCO CINAHL Complete, EBSCO Medline Complete, Embase, Scopus, and Web of Science. The search was limited to articles published in the English language between the years 2008 and 2020. This timeframe was selected because MMPI was first recognised internationally as a specific category of PI in 2008 when NPUAP produced its position statement about this injury. 3 The EBSCO Medline Complete search strategy is presented in Figure 1. Search results were exported to EndNote™ for collation and duplicate removal, and then imported into Covidence™ for screening, data extraction, and risk of bias assessment by two independent reviewers. Reviewers were blinded to each other's assessments during each stage. Any conflicting opinions were resolved through consultation with a third reviewer.
FIGURE 1.
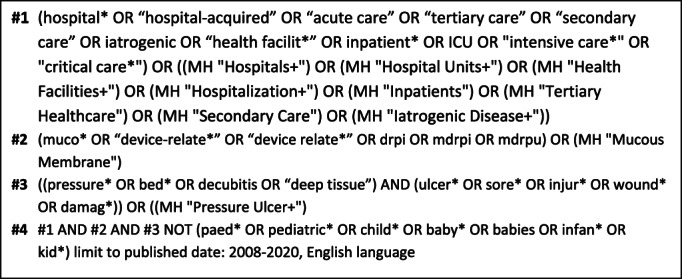
EBSCO Medline Complete search strategy
2.3.2. Eligibility criteria
Primary research that reported hospital‐acquired MMPI in adults admitted to acute hospital settings was included. Primary research reports of MDRPI were also included, as MMPI may be reported in combination with MDRPI. All studies were then scrutinised to identify MMPI incidence or prevalence data. For the purpose of this review, incidence and prevalence were defined as the number of patients with MMPI (numerator) divided by the number of patients sampled (denominator) × 100%. Studies that reported incidence in other formats, for example, PI per 1000 bed days were included in the review, and where possible incidence was calculated. In prevalence studies that reported prevalence for more than one time point, overall prevalence was calculated.
All primary research designs, in which incidence or prevalence data were reported in a non‐interventional sample, were included. Quantitative, observational, or epidemiological studies (prospective and retrospective) were included. The before group of before and after studies, or control groups of trials, were included if there were no selection criteria applied, that is, the sample was representative of the general population. Intervention groups were excluded, as PI incidence would have been influenced by the tested intervention.
Studies that were limited to PI occurring at a single body site or associated with a specific device, studies limited to specific groups of patients (eg, burns, spinal injury), and those that reported mucosal wounds that were not pressure‐related, such as traumatic injuries, were excluded. Studies reported in the grey literature, such as conference abstracts, were also excluded.
2.3.3. Screening
Abstracts were screened against the eligibility criteria, and then full‐text records of abstracts assessed as potentially eligible were retrieved to confirm whether they met inclusion criteria. The reference lists of any systematic reviews that were identified in the abstract screening and all full‐text articles that were retrieved following screening were examined to identify other studies for potential inclusion.
2.4. Search outcome
The search identified 1261 potentially eligible articles, once duplicates were removed. Following abstract screening and full‐text review, 17 studies met the criteria for inclusion. A further 26 full‐text articles were reviewed following screening of reference lists, resulting in the inclusion of a further four studies. In total, 21 studies met the inclusion criteria for full review (see Figure 2).
FIGURE 2.
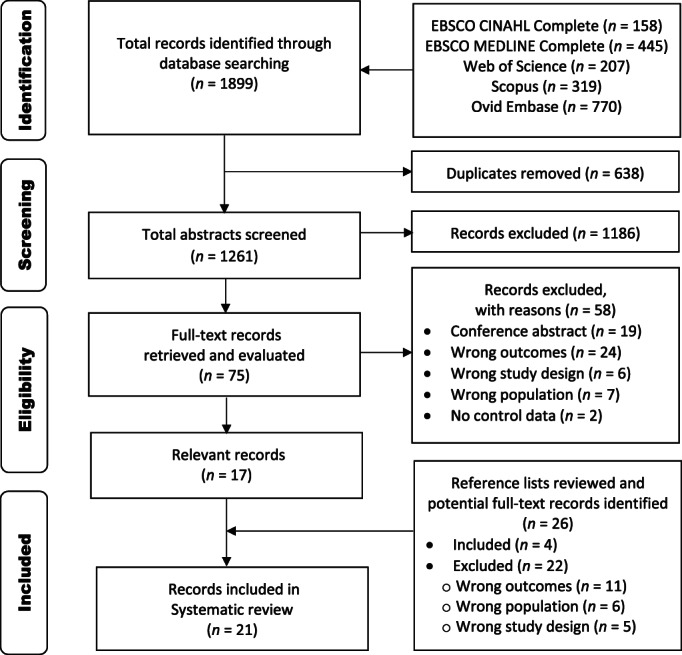
Preferred reporting items for systematic reviews and meta‐analysis (PRISMA) flow diagram: search and study selection
2.5. Data extraction
The Covidence™ data extraction form was customised for this review. Where necessary, authors were contacted to identify additional information. Data extracted included general information (author, year, country), study characteristics (design, setting, sample size, year of data collection), intervention (described if applicable), and outcomes (hospital‐acquired PI, MDRPI, MMPI overall and by body site, and associated devices).
2.6. Quality appraisal
Risk of bias assessment was undertaken using a slightly modified version of the tool developed by Hoy et al, 18 to ensure congruence with PI as an outcome measure, which was input into the Covidence™ risk of bias platform. The tool has four items that examine external validity and six that assess internal validity. Each item is scored as either 0 or 1. Studies scoring ≥8 were considered to be at low risk of bias, with those scoring 6 to 7 and ≤5 considered to be at moderate risk and high risk, respectively. With respect to internal validity, provided that a relevant international PI guideline was cited by the authors, it was accepted that an appropriate tool was used to define and diagnose PI. Quality appraisal was not used to exclude studies from the review.
2.7. Synthesis
It was anticipated that extracted data would be heterogeneous in relation to population, setting, and method of reporting MDRPI and MMPI incidence and prevalence. Consequently, meta‐analysis was inappropriate, and a narrative synthesis was undertaken based on the extracted data.
3. RESULTS
3.1. Study characteristics
The characteristics of the included studies are described in Table 1. Of the 21 studies included in this review, nearly all followed an observational design (n = 17). Control data from one cluster randomised trial, 36 one before and after study, 28 and two quality improvement studies 26 , 35 were included. Seven studies reported data from the United States, four from Australia, three from Saudi Arabia, and two from Indonesia. The majority of studies were prospective (n = 13) and most (n = 13) provided incidence data, although it was necessary to calculate incidence for some studies, and most collected data directly from subjects (n = 15). Ten studies were multi‐hospital‐site. Over half of all studies (n = 13) reported MDRPI and/or MMPI in ICU samples only. In three single site studies, data were reported from five, 30 four, 20 and three 33 ICUs. Sample size ranged from very small (n = 32) 32 to very large (n = 102 865). 13 Three studies included only patients with medical devices in situ, 24 , 32 , 34 therefore true cross‐sectional incidence was unable to be calculated for these studies. The four largest studies, with sample sizes in excess of 2000, reported prevalence data. 13 , 23 , 25 , 38 In three studies, 21 , 22 , 31 the sample size (denominator) was not reported.
TABLE 1.
Characteristics of included studies
| Author, year, country | Design, setting, sample size n, year of data collection | Primary outcome measure | Comparator (if applicable) | Outcomes: hospital‐acquired incidence/prevalence | Comments | ||
|---|---|---|---|---|---|---|---|
| HAPI | MDRPI | MMPI | |||||
|
Alves et al., 2017 19 Portugal |
Retrospective audit ICU n = 1 n = 600 2012‐2013 |
HAPI | NA |
Incidence = 9.7% (58/600) PI n = 130 (includes POA) |
aIncidence = 2.5% (15/600) aMDRPI (hospital‐acquired) n = 15 |
aIncidence = 0.8% (5/600) aMMPI n = 5 MMPI proportion of MDRPI = 33.3% (5/15) aMMPI by site: oral (ETT) n = 3; nasal (NGT) n = 2. |
aConfirmed via personal correspondence with author ICU subjects only Only PI reported after 24 hours hospitalisation counted as HAPI. |
|
Amirah et al., 2017 20 Saudi Arabia |
Retrospective, cross‐sectional cohort study Acute hospital n = 1; ICU n = 4 n = 431 2015‐2016 |
MDRPI | NA |
NR Unable to calculate incidence |
Incidence = 26.7% (115/431) MDRPI n = 128 MDRPI proportion of HAPI = 32.4% (128/395). |
Unable to calculate incidence Possible MMPI by device: ETT‐related n = 47; UC‐related n = 47; NGT‐related n = 12. |
ICU subjects only Adults >16 years of age MMPI not reported specifically but authors stated most MDRPI were MMPI Only three devices were reported, which may cause MMPI: ETT, NGT, UC. |
|
Arnold‐Long et al., 2017 21 United States |
Retrospective cross‐sectional Long‐term acute care hospital n = 3 n = NR 2009‐2010 |
MDRPI | NA |
Unable to calculate incidence HAPI n = 304 |
Unable to calculate incidence MDRPI n = 142 MDRPI proportion of HAPI = 46.7% (142/304). |
Unable to calculate incidence Possible MMPI by device: oxygen tubing/BiPAP/ CPAP n = 21, tubing (urine or faecal) n = 21, PEG tube flange n = 8 Possible MMPI by site: nose n = 7; penis n = 4; mouth n = 1. |
MMPI NR Only the total n of patients with HAPI/MDRPI were reported Sample denominator not reported. |
|
Barakat‐Johnson et al., 2017 22 Australia |
Prospective exploratory descriptive Acute hospital n = 1 n = NR 2015‐2016 |
MDRPI | NA |
Unable to calculate incidence HAPI n = 179. |
Unable to calculate incidence MDRPI total n = 50: ICU n = 34; non‐ICU n = 16 MDRPI proportion of HAPI = 27.9% (50/179). |
Unable to calculate incidence Patients with MMPI n = 20 MMPI (ICU) n = 17; MMPI non‐ICU n = 3 MMPI proportion of MDRPI = 40% (20/50) MMPI by site: mouth/lips n = 10; nose n = 9; tongue n = 1 MMPI by device: ETT n = 11; NGT n = 4; oxygen tubing n = 3; others n = 2 |
Only the total n of patients with HAPI/MDRPI/MMPI were reported: patient denominators n NR. Number of adults in sample unclear. At least three children (neonates) were included |
|
Black et al., 2010 23 United States |
Retrospective cross‐sectional prevalence: secondary data analysis Acute hospital n = 1 ICU, medical/ surgical, step‐down patient sub‐set n = 2079 2004‐2006 |
MDRPI | NA |
Prevalence = 5.4% (113/2079) HAPI n = 113 |
Prevalence = 1.3% (27/2079) MDRPI n = 39 MDRPI proportion of HAPI = 34.5% (39/113). |
Unable to calculate prevalence Possible MMPI by site: nose (n = 3); mouth/lips (n = 2). |
MMPI NR Adults aged ≥17 Total number of MMPI unclear. Unclear which devices caused PI of nose and mouth. |
|
Bubun et al., 2020 24 Indonesia |
Prospective observational study ICU n = 1 n = 50 Year NR |
MDRPI | NA |
NR Unable to calculate incidence |
Incidence = 26.0% (13/50) MDRPI n = 13. |
bIncidence = 0% |
bMMPI confirmed via personal correspondence with author ICU subjects only Only patients with medical devices in situ were included |
|
Clark et al., 2017 25 Wales |
Prospective observational prevalence audit Acute and community hospitals n = 66 n = 8365 2015 |
PI | NA |
Prevalence = 4.0% (337/8365) Visually verified prevalence = 3.1% (259/8365). |
Visually verified prevalence = 0.2% (20/8365). | Unable to calculate prevalence |
MMPI NR Origin of 68 PI unreported. |
|
Cooper et al., 2015 26 United States |
Retrospective prevalence surveys (monthly) ICU n = 1 n = 134 2012‐2015 |
HAPI Pre‐quality improvement programme n = 134 (2012) |
Post‐quality improvement programme n = 329 (2013‐2015) |
Unable to calculate prevalence HAPI n = 23 (2012 baseline). |
Unable to calculate prevalence MDRPI n = 12 (2012 baseline) MDRPI proportion of HAPI = 52.2% (12/23). |
Unable to calculate prevalence Possible MMPI by device: ETT n = 5; NGT n = 2; nasal cannula n = 1; FMS n = 1. |
MMPI NR Cardiac ICU subjects only Quality improvement programme commenced in 2013 Inconsistent reporting of PI n. |
|
Coyer et al., 2014 27 Australia, United States |
Prospective cross‐sectional prevalence Acute hospital n = 2, ICU n = 6 n = 483 Year NR |
MDRPI | NA |
Prevalence = 9.9% (48/483) HAPI n = 61 |
Prevalence = 3.1% (15/483) MDRPI n = 20 MDRPI proportion of HAPI = 32.9% (20/61). |
cPrevalence = 1.7% (8/483) MMPI n = 9 MMPI by site: mouth/lip n = 5; nose n = 4 MMPI by device: ETT n = 7; NGT n = 2. |
cMMPI prevalence calculated ICU subjects only Adults in Australia aged ≥16 years; adults in United States aged ≥18 years Patients with MDRPI followed up for 7 days. |
|
Coyer et al., 2015 28 Australia |
Prospective before‐after study ICU n = 1 n = 102 Year NR |
HAPI Before: standard care n = 102 |
After: skin integrity protocol n = 105 |
Incidence = 30.4% (31/102) HAPI n = 64 |
Unable to calculate incidence MDRPI NR. |
dIncidence = 30.4% (31/102) MMPI n = 39 MMPI by site: nare n = 22 (56.4%); lip n = 14 (35.9%); tongue n = 2 (5.1%). |
dMMPI incidence calculated ICU subjects only Reported MMPI n = 39 however ear PI included (n = 1) MMPI reduced following intervention. |
|
Coyer et al., 2017 29 Australia |
Retrospective secondary data analysis: prevalence Acute hospital n = 18 Overall n = 7291 ICU n = 296 Non‐ICU n = 6995 2012‐2014 |
HAPI | NA |
Overall prevalence = 3.3% (244/7291) ICU prevalence = 11.5% (34/296) ICU HAPI n = 49 Non‐ICU HAPI prevalence = 3.0% (210/6995) Non‐ICU HAPI n = 282 |
Unable to calculate prevalence MDRPI NR. |
eOverall prevalence = 0.2% (16/7291) eICU prevalence = 3.7% (11/296) ICU MMPI n = 11 ICU MMPI proportion of HAPI = 22.4% (11/49) eNon‐ICU prevalence = 0.1% (5/6995) Non‐ICU MMPI n = 5 Non‐ICU MMPI proportion of HAPI = 1.8% (5/282). |
eMMPI prevalence calculated following confirmation of patient numerator via personal correspondence with author Cumulative data from three point prevalence studies Adults aged ≥16 years MMPI sites unclear. |
|
Hanonu et al., 2016 30 Turkey |
Prospective cohort study Acute hospital n = 1, ICU n = 5 n = 175 2013‐2014 |
MDRPI | NA | Incidence = 55.4% (97/175) |
Incidence = 40.0% (70/175) MDRPI n = 211. |
Unable to calculate incidence Possible MMPI by device: ETT n = 95; nasal cannula n = 14; NGT n = 10; UC n = 6 Possible MMPI by site: lips n = 93; nose n = 33; mouth n = 2. |
MMPI NR ICU subjects only ICUs with low PI prevalence excluded. |
|
Kayser et al., 2018 13 Canada, United States |
Secondary analysis: prospective prevalence survey data Acute hospitals n = 1115, n = 102 865 5Acute care setting n = 88 896 2016 |
MDRPI | NA |
Overall prevalence = 3.7% (3763/102865) HAPI n = 5370 |
Overall prevalence = 0.5% (499/102865) MDRPI n = 660 MDRPI proportion of HAPI = 12.2% (660/5370) f,gAcute setting prevalence = 0.6% (527/88896) MDRPI n = NR |
Unable to calculate MMPI prevalence Possible MMPI by device: ETT n = 54; nasal oxygen n = 36; NGT n = 35 Possible MMPI proportion of MDRPI = 20.7% (125/604). |
MMPI NR fSample filtered: only patients with complete records included gIncludes MDRPI POA 28% of MDRPI within ICU settings. |
|
Kim et al., 2019 31 South Korea |
Retrospective secondary data analysis Acute hospital n = 5 n = NR 2016 |
MDRPI | NA |
Incidence = 16.9% (n/N NR) Incidence rate per 1000 hospital days = 1.7 hHAPI n = 4142 |
Incidence = 0.8% (n/N NR) Incidence rate per 1000 hospital days = 0.1 MDRPI n = 227 MDRPI proportion of HAPI = 5.5% |
Unable to calculate incidence Possible MMPI by device: NGT n = 40; nasal cannula n = 27; ETT n = 9; UC n = 4 Possible MMPI proportion of MDRPI = 35.2% (80/227). |
MMPI NR hCalculated based on MDRPI reported proportion. |
|
Masyitha et al., 2020 32 Indonesia |
Prospective cohort study ICU n = 1 n = 32 2019 |
MDRPI | NA | Incidence unable to be calculated |
Incidence = 21.9% (7/32) MDRPI n = 7 |
Unable to calculate incidence Possible MMPI by site: lip n = 1; nose n = 1 Possible MMPI proportion of MDRPI = 28.6% (2/7). |
MMPI NR ICU subjects only Only patients with medical devices in situ were included Data collected for only 5 days Outdated PI staging system reported (2009). |
|
Mehta et al., 2019 33 India |
Prospective cross‐sectional point prevalence Acute hospital n = 1, ICU n = 3 n = 146 Year NR |
MDRPI | NA |
Prevalence = 26.0% (38/146) |
Prevalence = 19.2% (28/146) MDRPI n = 33 MDRPI proportion within HAPI = 73.7% (28/38). |
Unable to calculate prevalence Possible MMPI by device: NGT n = 10; ETT n = 3; nasal prongs n = 2. |
MMPI NR ICU subjects only Unclear whether all MDRPI were hospital‐acquired. |
|
Rashvand et al., 2020 34 Iran |
Prospective cross‐sectional audit Acute hospital n = 3 n = 404 2019 |
MDRPI | NA | Incidence unable to be calculated |
iIncidence = 20.5% (83/404) MDRPI n = 87. |
Unable to calculate incidence Possible MMPI by device: nasal oxygen tubing n = 31; ETT n = 17; NGT n = 5; tracheostomy n = 2. |
MMPI NR: all MDRPI were categorised by stage suggesting that either there were no MMPI or some MMPI were categorised incorrectly iOnly patients with at least one medical device in situ were included Discrepancy in n of ICU patients with MDRPI (38 vs 39) Assessors relied upon referrals from participating sites. |
|
Swafford et al., 2016 35 United States |
Quality improvement study ICU n = 1 n = 461 2011‐2013 |
HAPI Pre‐PI prevention programme n = 461 (retrospective) |
Post‐PI prevention programme n = 997 | Incidence = 9.8% (45/461) |
Incidence = 2.0% (9/461) MDRPI n = NR. |
Unable to calculate incidence |
MMPI NR ICU subjects only Site and device associated with MDRPI NR MDRPI reduced following quality improvement programme. |
|
Tayyib et al., 2015 36 Saudi Arabia |
Prospective cluster RCT Tertiary hospital n = 2, ICU n = 2 n = 70 2013‐2014 |
HAPI Control group: usual care n = 70 |
PI prevention bundle n = 70 |
Incidence = 32.9% (23/70) HAPI n = 37 |
Incidence = 10.0% (7/70) | Unable to calculate incidence |
MMPI NR ICU subjects only PI within 24 hours excluded Most common MDRPI = nare MDRPI reduced in intervention group. |
|
Tayyib et al., 2016 37 Saudi Arabia |
Prospective observational study Tertiary hospital n = 2, ICU n = 2 n = 84 2013 |
HAPI | NA |
Incidence = 39.3% (33/84) HAPI n = 41 |
Incidence = 8.3% (7/84) MDRPI n = 8 MDRPI proportion of HAPI = 19.5% (8/41). |
Unable to calculate incidence Possible MMPI n = 2 (nare and lip). |
MMPI NR ICU subjects only. |
|
VanGilder et al., 2009 38 United States |
Prospective prevalence surveys Acute care facilities n = NR n = 86 932 2009 |
HAPI | NA |
Prevalence = 5.0% (N = 86 932) HAPI n = 6589 jAcute care unit prevalence = 5.5% (4144/75189) |
jPrevalence = 1.0% (740/75189) MDRPI n = 785 MDRPI proportion of HAPI = 11.9% (785/6589). |
Unable to calculate prevalence |
MMPI NR jCalculated with reduced sample size reported for acute care units. |
Abbreviations: CPAP, continuous positive airways pressure; ETT, endotracheal tube; FMS, faecal management system; HAPI, hospital‐acquired pressure injury; MDRPI, medical device‐related pressure injury; MMPI, mucous membrane pressure injury; NA, not applicable; NGT, nasogastric tube; NR, not reported; PEG, percutaneous endoscopic gastrostomy; PI, pressure injury; POA, present on admission; RCT, randomised controlled trial; UC, urinary catheter.
3.2. Quality appraisal
The majority of studies included in the review were judged to be at low risk of bias (n = 14) with the remainder at moderate risk (see Table 2). Across studies, the main areas of bias were data collection from medical records, as opposed to directly from subjects (n = 6), and absence of subject numerator/denominator to enable calculation of incidence/prevalence (n = 5). A lack of consistency was noted across the studies regarding the reporting and documentation of PI, and several studies involved nurses from multiple hospitals in which different data collection/recording methods were used.
TABLE 2.
Risk of bias
| Risk of bias items | Authors, year | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alves et al., 2017 19 | Amirah et al., 2017 20 | Arnold‐Long et al., 2017 21 | Barakat‐Johnson et al., 2017 22 | Black et al., 2010 23 | Bubun et al., 2020 24 | Clark et al., 2017 25 | Cooper et al., 2015 26 | Coyer et al., 2014 27 | Coyer et al., 2015 28 | Coyer et al., 2017 29 | Hanonu et al., 2016 30 | Kayser et al., 2018 13 | Kim et al., 2019 31 | Masyitha et al., 2020 32 | Mehta et al., 2019 33 | Rashvand et al., 2020 34 | Swafford et al., 2016 35 | Tayyib et al., 2015 36 | Tayyib et al., 2016 37 | VanGilder et al., 2009 38 | ||
| External validity | Representative sample | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 |
| Sampling frame | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | |
| Random selection or census | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Non‐response bias minimal | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | |
| Internal validity | Data collected directly from subjects | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Acceptable definition of PI | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | |
| Accepted diagnosis method for PI | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | |
| Same data collection method used for all subjects | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | |
| Appropriate prevalence period | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Numerator(s) and denominator(s) appropriate | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | |
| Total score | 9 | 7 | 7 | 9 | 9 | 7 | 10 | 7 | 10 | 8 | 10 | 8 | 10 | 8 | 7 | 10 | 6 | 9 | 9 | 9 | 6 | |
| Overall risk of bias | Low | Mod | Mod | Low | Low | Mod | Low | Mod | Low | Low | Low | Low | Low | Low | Mod | Low | Mod | Low | Low | Low | Mod | |
3.3. Results of studies
No studies were found that reported MMPI incidence or prevalence as a primary outcome. In 12 studies, MDRPI was the primary outcome. 13 , 20 , 21 , 22 , 23 , 24 , 27 , 30 , 31 , 32 , 33 , 34
3.3.1. Mucous membrane pressure injury incidence and prevalence
Only two studies were found that provided sufficient data to enable calculation of MMPI incidence or prevalence. 27 , 28 In two other studies incidence 19 and prevalence 29 were able to be calculated following personal communication with authors. In another study, personal communication confirmed that none of the 13 MDRPI that were reported were MMPI. 24 However, only subjects with a medical device in situ were included in this study. These five studies all reported ICU samples, although Coyer et al 29 also reported a non‐ICU sample. In an earlier study by Coyer et al, 27 data were collected from Australia and United States. In their relatively large sample (n = 483), the prevalence of MDRPI was low (3.1%). Of the 20 MDRPI that were reported in 15 patients, nine MMPI were reported in eight patients, giving a calculated MMPI prevalence of 1.7%. Of the nine MMPI found, most were associated with the use of an endotracheal tube (n = 7) and were found on the mouth or lip (n = 5). In another study, using an Australian sample, 28 a prospective before and after trial of a skin integrity protocol, sufficient data were provided to enable calculation of MMPI incidence in the before group (30.4%). In this study, 39 MMPI were reported in 31 patients, however, the site for one of these was given as the ear. Most MMPI were found on the nares (n = 22) or lips (n = 14) and were associated with the presence of an endotracheal tube or nasogastric tube. MDRPI were not reported per se, and some of the skin injuries may have been device‐related. Significantly, MMPI (n = 39) represented 61% of all reported PI (n = 64). In contrast, non‐MMPI (n = 25) were reported in only 24 patients. On the other hand, in a Portuguese study with an ICU sample (n = 600), 19 only five MMPI were found, giving a considerably lower incidence of 0.8%. Three MMPI were found in the mouth (endotracheal tube‐related) and two were in the nose (nasogastric tube‐related). In a secondary analysis of state‐wide prevalence data in Australia, 29 11 MMPI were found in 11 patients in an ICU sample of 296 patients, giving an MMPI prevalence of 3.7%. In this sample, MDRPI were not reported; however, of the 49 hospital‐acquired PI that were reported, 22% were MMPI. In this study, MMPI in the non‐ICU sample were also reported. Personal correspondence with one of the authors confirmed that five patients each had one MMPI, enabling calculation of non‐ICU MMPI prevalence of 0.1% (5/6995).
In one other study, some data were presented about the number of MMPI. 22 In this Australian study, 50 MDRPI were reported, of which 20 (40%) MMPI were reported in the same number of patients. The majority was found in ICU (n = 17). However, MDRPI “incidence” was reported as the proportion of hospital‐acquired PI that were device‐related (27.9%). In this study, most MMPI were found on the mouth or lips (n = 10) or nose (n = 9), and most were associated with the presence of an endotracheal tube (n = 11) or nasogastric tube (n = 4). Calculation of true MMPI incidence was not possible because only patients with hospital‐acquired PI were sampled; the denominator, that is, total number of hospital patients during the data collection period was not reported.
3.3.2. Intensive care settings: medical device‐related and mucous membrane pressure injuries
In several studies, where MDRPI was categorised by body site or medical device association, some information was reported that provides an approximation of possible MMPI (see Table 1). Three studies 30 , 32 , 37 provided some relevant ICU data by body site and four studies 20 , 26 , 30 , 33 provided information related to medical device association. In the study by Hanonu et al, 30 211 MDRPI were found in a sample of 175 ICU patients. Of these, 128 PI were found on the lips, nose or mouth, suggesting that the majority (61%) may have been MMPI. In the smallest study included in this review, 32 which only included ICU patients with medical devices in situ for up to 5 days, MDRPI incidence of 21.9% was calculated. Of the seven MDRPI that were reported, 29% (n = 2; lip and nose) may have been MMPI. Similarly, in another small ICU study, 37 25% (2/8) of MDRPI were possible MMPI (nare and lip). In Saudi Arabia, Amirah et al 20 sampled four ICUs, reporting a total of 128 MDRPI in 431 patients, with an MDRPI incidence of 26.7%. Of the MDRPI, 83% were associated with a medical device (endotracheal tube, urinary catheter, nasogastric tube) that could have caused an MMPI. Similarly, in the ICU quality improvement project reported by Cooper et al, 26 in a baseline sample of 134 patients, 12 MDRPI were found of which 75% were associated with medical devices (endotracheal tubes, nasogastric tubes, nasal cannula, faecal management system) that could have caused MMPI. In the prospective study of five ICUs by Hanonu et al, 30 125 possible MMPI associated with four medical devices (endotracheal tube, nasogastric tube, nasal cannula, urinary catheter) were reported, representing a significant proportion (59%) of all MDRPI. In a similar‐sized prevalence study of three ICUs in India, Mehta et al 33 reported 15 possible MMPI associated with three devices (nasogastric tube, endotracheal tube, nasal prongs) representing 45% of all MDRPI.
3.3.3. Acute care settings: medical device‐related and mucous membrane pressure injuries
No studies were found across an acute hospital setting that reported, or provided, data that enabled calculation of MMPI incidence, whereas prevalence (0.1%) was able to be calculated from only one study 29 following correspondence with one of the authors. However, similarly to the ICU studies described above, several studies provided some information in terms of the MMPI as a proportion of MDRPI. In the study by Barakat‐Johnson et al, 22 16 MDRPI were reported in non‐ICU patients, of which three (19%) were MMPI. In a relatively large study in the United States, in which a subset of adults in ICU, medical surgical, and step‐down units was analysed, Black et al 23 reported only 39 MDRPI in 2079 patients, of which only 13% (n = 5) were possible MMPI (nose and lips). The lower level of MDRPI reporting may be because of the relatively recent revision of its definition by the NPUAP. 5 In a later secondary analysis of Canada/United States prevalence data, Kayser et al 13 reported 499 patients with a facility‐acquired MDRPI in a large sample of 102 865 from 1115 hospitals, giving a prevalence of 0.5%. Of 99 876 patients with complete data, 89% (n = 88 896) were from acute care settings, with an MDRPI prevalence of 0.6% (including non‐facility‐acquired MDRPI) within this subset. A total of 604 facility‐acquired MDRPI were reported in the filtered dataset, and 28% of all MDRPI (n = 804) were recorded in ICU settings. When analysed by associated medical device (endotracheal tube, nasal cannula, nasogastric tube), potentially 125 (21%) of facility‐acquired MDRPI may have been MMPI. As well, some of the 26 MDRPI associated with tracheostomy neck plates may have been MMPI. In another large study reporting data from the United States, MDRPI prevalence of 1.0% was calculated from an acute care unit sample of 75 189 but neither the site of the injury or the associated device was reported. 38 Similarly, in a South Korean analysis of PI incidence across five hospitals, an MDRPI incidence of 0.8% was reported. 31 Of 227 MDRPI, up to 80 (35%) that were associated with nasogastric tubes, nasal cannula, endotracheal tubes, or urinary catheters may have been MMPI. When reported by site (nose, mouth), a similar number (n = 82; 36%) may have been MMPI. In another study, within three hospital settings, an MDRPI incidence of 21% (n = 83) was reported in a sample of 404 patients with at least one medical device. 34 Of the 87 MDRPI that were recorded, around two‐thirds (63%, n = 55) that were associated with three medical devices (nasal cannulae, endotracheal tubes, nasogastric tubes) may have been MMPI. In an earlier study across three long‐term acute care hospitals, in which 142 MDRPI were reported, 8% (n = 12; nose, penis, mouth) may have been MMPI. 21
4. DISCUSSION
To our knowledge, this is the first systematic review that has been conducted to investigate MMPI incidence and prevalence. The review has highlighted a significant gap in knowledge. The limited data available about MMPI incidence are consistent with the finding of a recent systematic review of MDRPI in the acute hospital setting, in which none of the included studies reported mucosal injuries. 39 As there were no studies found that directly reported either incidence or prevalence of MMPI, heterogeneity was unable to be assessed. However, as shown in Table 1, a large proportion of studies that reported MDRPI as a primary outcome were within the ICU setting.
In most studies in this review, an international PI guideline relevant to the year of data collection was cited for the purpose of diagnosis and categorisation of PI. The earliest guideline, which was cited in several studies, was from 2009. 40 It states that ulcers on mucous membranes should not be classified. In the absence of further guidance about their reporting, this may have been interpreted to mean that they should not be reported at all. However, MMPI were recognised as a specific category of PI in the preceding year, 3 when it was clarified that they should be “labelled as mucosal pressure ulcers without a stage identified.” And, since publication of the 2014 international guideline, it has been recommended that MMPI are included in prevalence and incidence studies. 11 Despite this, only four studies were found in this systematic review, all conducted within ICU settings, that enabled calculation of MMPI prevalence or incidence. 19 , 27 , 28 , 29 However, the results were quite different. In the earlier study, 27 MMPI prevalence of only 1.7% was found. However, in the later studies, MMPI incidence of 0.8% 19 and 30.4% 28 and prevalence of 3.7% 29 was found. Based on these data, no conclusions can be drawn about the true incidence of MMPI in ICU settings, and further research is required.
Several studies conducted within an ICU setting have provided some useful information about the possible incidence of MMPI as a proportion of MDRPI. 19 , 20 , 26 , 30 , 33 , 37 Our estimates indicate a broad range, suggesting that as many as one in every three MDRPI may be a MMPI. In a very recent study, which investigated predictors of PI in ICU from the records of 1587 patients, a hospital‐acquired PI incidence of 5.1% (n = 81) was reported. 41 Of the 114 PI documented, 39.5% (n = 45) were MDRPI of which 21 were MMPI. These data indicate that nearly half (47%) of all MDRPI were MMPI.
In broader hospital settings, given the relatively lower use of medical devices and consequent incidence of MDRPI, estimations of MMPI incidence are much lower than ICU settings, as indicated by the prevalence of only 0.1% in the study by Coyer et al. 29 Importantly, there is a notable absence of reported data about MMPI in acute hospital settings.
In this review, we found 12 studies that reported MDRPI incidence or prevalence as a primary outcome, of which eight were prospective studies. 13 , 22 , 24 , 27 , 30 , 32 , 33 , 34 Despite being prospective, only two of these studies reported MMPI data, 22 , 27 of which only one provided sufficient data to enable calculation of incidence. 27 This finding suggests that the recommendation to collect MMPI data in incidence and prevalence studies is not being adhered to. This represents a gap in knowledge about these types of PI, which makes it difficult for health care institutions to benchmark their own data. Furthermore, the lack of data about the scope and nature of the problem means identification of targeted interventions to reduce MMPI development in clinical practice is challenging.
The MDRPI incidence and prevalence found in the studies included in this review were wide‐ranging. In the acute setting, MDRPI incidence ranged from 0.8% 31 to 20.5% 34 and prevalence ranged from 0.2% 25 to 1.3%. 23 However, an inclusion criterion for the study by Rashvand et al 34 was that patients had at least one medical device in situ for at least 1 hour. Thus, the incidence in this study does not represent true hospital cross‐sectional incidence. In a recent systematic review, MDRPI incidence was reported to be 28.1% in the acute hospital setting, 39 which may represent a closer approximation. In ICU settings, MDRPI incidence ranged from 2.0% 35 to 40.0% 30 and prevalence ranged from 3.1% 27 to 19.2%. 33 When only patients with medical devices in situ were included in the sample, MDRPI incidence was between 22% and 26%. 24 , 32 Given that the proportions of possible MMPI reported in these studies were also wide‐ranging, it is not possible to even broadly estimate either MMPI incidence or prevalence from the data currently available.
Previous systematic reviews have reported pooled MDRPI incidence and prevalence across all settings 12 and ICU settings. 14 In the former study, 12 pooled incidence of adult patients was 14% (95% CI 8%‐21%) and pooled prevalence was 11% (95% CI 6%‐18%); however, specialty samples were included (eg, patients with spinal injury/disease), and eligibility criteria included studies that pre‐dated the 2008 NPUAP statement. 3 In the latter study, 14 which presents a more contemporary analysis as the included studies were published between 2007 and 2017, pooled incidence was 3.4% (95% CI 0%‐14.4%) and pooled prevalence was 33.7% (95% CI 22.6%‐45.8%). Nevertheless, the pooled estimates of incidence and prevalence were quite different. These two systematic reviews provide further evidence that good quality cross‐sectional incidence and prevalence studies are needed to enable a more accurate estimation of both MDRPI and MMPI incidence and prevalence.
The limited data derived from our review indicate that patients in ICU settings are at greater risk for MMPI development compared with others in general hospital settings. Primarily, this is associated with the large number of medical devices required for these patients. Our data indicate that the most common medical devices likely to be associated with MMPI development are nasogastric tubes, endotracheal tubes, and nasal cannulae. In one study, 31 a large number of MDRPI were reported as associated with urinary catheter use, whereas in other studies 21 , 26 , 31 the number was relatively small. The fact that only four of the studies in this review reported urinary catheter‐related MDRPI suggests that these may be under‐reported. Some studies have investigated risk factors and incidence of MMPI of the mouth or lips 42 , 43 , 44 , 45 and several studies have investigated the use of various dressings or support devices to reduce oral 46 , 47 , 48 , 49 or nasal 50 , 51 MDRPI or both. 52 The SKINCARE bundle, which includes guidance about management of medical devices and prevention of PI, was shown to be effective in reducing MMPI 28 and MDRPI. 53 A recent evidence review 54 provides recommendations for practice about medical device management to reduce MDRPI, and an international expert consensus statement has proposed an MDRPI prevention pathway. 55 However, discussion of the efficacy of measures to prevent MDRPI or MMPI is beyond the scope of this paper, and further rigorous trials are required to establish their effectiveness.
4.1. Limitations
This review utilised a comprehensive search strategy that covered all years since MMPI was first defined, and included MDRPI studies. Overall, the methodological quality of the included studies was good. However, only English language articles were included in this review, which may have introduced an element of bias.
Although most studies reported MDRPI data, only two published sufficient information to enable calculation of MMPI incidence or prevalence. Furthermore, only two other studies reported specific data about MMPI. Although it was possible, to some extent, to estimate the proportion of MDRPI that were MMPI, the degree of accuracy was low as many of the MDRPI reported on the mouth or nose, or those associated with oral or nasal medical devices, may have been skin PI.
5. CONCLUSIONS
This systematic review has demonstrated clearly that there is a significant lack of studies available to enable estimation of MMPI incidence or prevalence in either acute hospital or ICU settings. This severely limits the ability of health care institutions to benchmark their own data, as well as providing little guidance about the focus for quality improvement programmes in this area. As concluded by Brophy et al, “the uptake of classifying appropriate MDRPIs as mucosal injuries requires further attention.” 39 (p11) Based on our findings, we wish to strongly emphasise the international guideline recommendation that MMPI should be included in incidence or prevalence studies. 1 Further good quality research is needed in which MMPI are both counted and reported as incidence data. The latter is especially important in ICU settings, where it is common for a single patient to require several medical devices. Furthermore, the body site and the device associated with the MMPI should also be reported. 1
In conclusion, further good quality incidence and prevalence studies are needed in which MMPI are both counted and reported as incidence data, including their site location and associated medical device. In MDRPI studies, MMPI should be reported clearly.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONS
All authors agreed on the final version and met at least one of the following criteria (recommended by ICMJE): made substantial contributions to the conception and design of the study, acquisition of data, analysis, and interpretation of data, drafting the article, and revising it critically for important intellectual content.
SYSTEMATIC REVIEW PROTOCOL REGISTRATION (PROSPERO INTERNATIONAL)
Fulbrook P, Miles S, Lovegrove J (2020). Incidence and prevalence of mucosal pressure injury in adults admitted to acute hospital settings: A systematic review. PROSPERO 2020 CRD42020214127 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020214127.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the assistance of health specialist librarian Virginia Corfield (Australian Catholic University) with development of the search strategy. The contribution of Michaelina Anderson (Australian Catholic University) to our preliminary search strategy development and initial searches is also acknowledged.
Fulbrook P, Lovegrove J, Miles S, Isaqi B. Systematic review: Incidence and prevalence of mucous membrane pressure injury in adults admitted to acute hospital settings. Int Wound J. 2022;19(2):278–293. 10.1111/iwj.13629
DATA AVAILABILITY STATEMENT
Data available on request from the authors.
REFERENCES
- 1. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance . In: Haesler E, ed. Prevention and Treatment of Pressure Injuries/Ulcers: Clinical Practice Guideline; the International Guideline. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance; 2019. [Google Scholar]
- 2. Kottner J, Hahnel E, Lichterfeld‐Kottner A, Blume‐Peytavi U, Büscher A. Measuring the quality of pressure ulcer prevention: a systematic mapping review of quality indicators. Int Wound J. 2017;15(2):218‐224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. National Pressure Ulcer Advisory Panel . Mucosal Pressure Ulcers: A NPUAP Position Statement. National Pressure Ulcer Advisory Panel; 2008. https://cdn.ymaws.com/npuap.site-ym.com/resource/resmgr/position_statements/mucosal_pressure_ulcer_posit.pdf. [Google Scholar]
- 4. Delmore BA, Ayello EA. Pressure injuries caused by medical devices and other objects: a clinical update. Am J Nurs. 2017;117(12):36‐45. [DOI] [PubMed] [Google Scholar]
- 5. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585‐597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Apold J, Rydrych D. Preventing device‐related pressure ulcers: using data to guide statewide change. J Nurs Care Qual. 2012;27(1):28‐34. [DOI] [PubMed] [Google Scholar]
- 7. Black J, Alves P, Brindle C, et al. Use of wound dressings to enhance prevention of pressure ulcers caused by medical devices. Int Wound J. 2015;12(3):322‐327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Campbell N. Electronic SSKIN pathway: reducing device‐related pressure ulcers. Br J Nurs. 2016;25(15):S14‐S26. [DOI] [PubMed] [Google Scholar]
- 9. Dyer A. Ten top tips: preventing device‐related pressure ulcers. Wounds Int. 2015;6(1):9‐13. [Google Scholar]
- 10. Mulgrew S, Khoo A, Newton RM, Rajan R, Kumar K. Pressure necrosis secondary to negative pressure dressing. Ann R Coll Surg Engl. 2011;93(5):e27‐e28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance . In: Haesler E, ed. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Osborne Park, Australia: Cambridge Media; 2014. [Google Scholar]
- 12. Jackson D, Sarkic AM, Betteridge R, Brooke J. Medical device‐related pressure ulcers: a systematic review and meta‐analysis. Int J Nurs Stud. 2019;92:109‐120. [DOI] [PubMed] [Google Scholar]
- 13. Kayser SA, VanGilder CA, Ayello EA, Lachenbruch C. Prevalence and analysis of medical device‐related pressure injuries: results from the international pressure ulcer prevalence survey. Adv Skin Wound Care. 2018;31(6):276‐285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Bakarat‐Johnson M, Lai M, Wand T, Li M, White K, Coyer F. The incidence and prevalence of medical device‐related pressure ulcers in intensive care: a systematic review. J Wound Care. 2019;28(8):512‐521. [DOI] [PubMed] [Google Scholar]
- 15. Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. https://wiki.jbi.global/display/MANUAL/Downloadable+PDF+-+current+version. [Google Scholar]
- 16. PRISMA . Transparent reporting of systematic reviews and meta‐analyses; 2015. http://www.prisma-statement.org/.
- 17. Fulbrook P, Miles S, Lovegrove J. Incidence and prevalence of mucosal pressure injury in adults admitted to acute hospital settings: A systematic review. PROSPERO 2020;CRD42020214127. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020214127. [DOI] [PMC free article] [PubMed]
- 18. Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934‐939. [DOI] [PubMed] [Google Scholar]
- 19. Alves P, Eberhardt T, Soares R, et al. Differential diagnosis in pressure ulcers and medical devices. Česká Slov Neurol Neurochir. 2017;80/113(Suppl. 1):S29‐S35. [Google Scholar]
- 20. Amirah MF, Rasheed AM, Parameaswari PJ, Nu'man OS, Al Muteb M. A cross‐sectional study on medical device‐related pressure injuries among critically ill patients in Riyadh, Kingdom of Saudi Arabia. WCET J. 2017;37(1):8‐11. [Google Scholar]
- 21. Arnold‐Long M, Ayer M, Borchert K. Medical device‐related pressure injuries in long‐term acute care hospital setting. J Wound Ostomy Continence Nurs. 2017;44(4):325‐330. [DOI] [PubMed] [Google Scholar]
- 22. Barakat‐Johnson M, Barnett C, Wand T, White K. Medical device‐related pressure injuries: an exploratory descriptive study in an acute tertiary hospital in Australia. J Tissue Viability. 2017;26(4):246‐253. [DOI] [PubMed] [Google Scholar]
- 23. Black J, Cuddigan J, Walko M, Didier L, Lander M, Kelpe M. Medical device related pressure ulcers in hospitalized patients. Int Wound J. 2010;7(5):358‐365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Bubun J, Yusuf S, Darwis M. Relationship between skin moisture and medical device related pressure injury (MDRPI) in intensive care units: prospective study. Enferm Clín. 2020;30(Suppl. 2):420‐423. [Google Scholar]
- 25. Clark M, Semple MJ, Ivins N, Mahoney K, Harding K. National audit of pressure ulcers and incontinence‐associated dermatitis in hospitals across Wales: a cross‐sectional study. BMJ Open. 2017;7(e015616):1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Cooper DN, Jones SL, Currie LA. Against all odds: preventing pressure ulcers in high‐risk cardiac surgery patients. Crit Care Nurse. 2015;35(5):76‐82. [DOI] [PubMed] [Google Scholar]
- 27. Coyer F, Stotts N, Blackman V. A prospective window into medical device‐related pressure ulcers in intensive care. Int Wound J. 2014;11(6):656‐664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Coyer F, Gardner A, Doubrovsky A, et al. Reducing pressure injuries in critically ill patients by using a patient skin integrity care bundle (INSPIRE). Am J Crit Care. 2015;24(3):199‐209. [DOI] [PubMed] [Google Scholar]
- 29. Coyer F, Miles S, Gosley S, et al. Pressure injury prevalence in intensive care versus non‐intensive care patients: a state‐wide comparison. Aust Crit Care. 2017;30(5):244‐250. [DOI] [PubMed] [Google Scholar]
- 30. Hanonu S, Karadag A. A prospective, descriptive study to determine the rate and characteristics of and risk factors for the development of medical device‐related pressure ulcers in intensive care units. Ostomy Wound Manage. 2016;62(2):12‐22. [PubMed] [Google Scholar]
- 31. Kim JY, Lee YJ, Korean Association of Wound Ostomy Continence Nurses . Medical device‐related pressure ulcer (MDRPU) in acute care hospitals and its perceived importance and prevention performance by clinical nurses. Int Wound J. 2019;16(Suppl. 1):51‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Masyitha K, Haryanto, Puspita D, Suriadi, Usman. Pressure ulcers related to medical device in intensive care in Indonesia: a prospective study. Enferm Clín. 2020;30(Suppl. 3):87‐91. 10.1016/j.enfcli.2020.01.006. [DOI] [Google Scholar]
- 33. Mehta C, Ali M, Mehta Y, George JV, Singh MK. MDRPU—an uncommonly recognized common problem in ICU: a point prevalence study. J Tissue Viability. 2019;28(1):35‐39. [DOI] [PubMed] [Google Scholar]
- 34. Rashvand F, Shamekhi L, Rafiei H, Nosrataghaei M. Incidence and risk factors for medical device‐related pressure ulcers: the first report in this regard in Iran. Int Wound J. 2020;17(2):436‐442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Swafford K, Culpepper R, Dunn C. Use of a comprehensive program to reduce the incidence of hospital‐acquired pressure ulcers in an intensive care unit. Am J Crit Care. 2016;25(2):152‐155. [DOI] [PubMed] [Google Scholar]
- 36. Tayyib N, Coyer F, Lewis P. A two‐arm cluster randomized control trial to determine the effectiveness of a pressure ulcer prevention bundle for critically ill patients. J Nurs Scholarsh. 2015;47(3):237‐247. [DOI] [PubMed] [Google Scholar]
- 37. Tayyib N, Coyer F, Lewis P. Saudi Arabian adult intensive care unit pressure ulcer incidence and risk factors: a prospective cohort study. Int Wound J. 2016;13(5):912‐919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. VanGilder C, Amlung S, Harrison P, Meyer S. Results of the 2008‐2009 International Pressure Ulcer Prevalence Survey and a 3‐year, acute care, unit‐specific analysis. Ostomy Wound Manage. 2009;55(11):39‐45. [PubMed] [Google Scholar]
- 39. Brophy S, Moore ZEH, Patton D, O'Connor T, Avsar P. What is the incidence of medical device‐related pressure injuries in adults within the acute hospital setting? A systematic review. J Tissue Viability. 2021. 10.1016/j.jtv.2021.03.002. [DOI] [PubMed] [Google Scholar]
- 40. National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel . Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Washington, DC: National Pressure Ulcer Advisory Panel; 2009. [Google Scholar]
- 41. Sala JJ, Mayampurath A, Solmos S, et al. Predictors of pressure injury development in critically ill adults: a retrospective cohort study. Intensive Crit Care Nurs. 2021;62(2021):102924. [DOI] [PubMed] [Google Scholar]
- 42. Choi BK, Kim MS, Kim SH. Risk prediction models for the development of oral‐mucosal pressure injuries in intubated patients in intensive care units: a prospective observational study. J Tissue Viability. 2020;29(2020):252‐257. [DOI] [PubMed] [Google Scholar]
- 43. Kim C‐H, Kim MS, Kang MJ, Kim HH, Park NJ, Jung HK. Oral mucosa pressure ulcers in intensive care unit patients: a preliminary observational study of incidence and risk factors. J Tissue Viability. 2019;28(1):27‐34. [DOI] [PubMed] [Google Scholar]
- 44. Wickberg M, Falk A. The occurrence of pressure damage in the oral cavity caused by endotracheal tubes. Nordic J Nurs Res. 2017;37(1):2‐6. [Google Scholar]
- 45. Shapira‐Galitz Y, Karp G, Cohen O, Halperin D, Lahav Y, Adi N. Evaluation and predictors for nasogastric tube associated pressure ulcers in critically ill patients. Isr Med Assoc J. 2018;20(12):731‐736. [PubMed] [Google Scholar]
- 46. Hampson J, Green C, Stewart J, et al. Impact of the introduction of an endotracheal tube attachment device on the incidence and severity of oral pressure injuries in the intensive care unit: a retrospective observational study. BMC Nurs. 2018;17:4. 10.1186/s12912-018-0274-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Holdman J, Rozansky C, Baldwyn T. Reduction of respiratory device‐related pressure injuries. J Respir Care Pract. 2020;33(1):8‐10. [Google Scholar]
- 48. Kuniavsky M, Vilenchik E, Lubanetz A. Under (less) pressure—facial pressure ulcer development in ventilated ICU patients: a prospective comparative study comparing two types of endotracheal tube fixations. Intensive Crit Care Nurs. 2020;58(2020):102804. [DOI] [PubMed] [Google Scholar]
- 49. Zaratkiewicz SD, Teegardin C, Whitney J. Retrospective review of the reduction of oral pressure ulcers in mechanically ventilated patients: a change in practice. Crit Care Nurs Q. 2012;35(3):247‐254. [DOI] [PubMed] [Google Scholar]
- 50. Ambutas S, Staffileno BA, Fogg L. Reducing nasal pressure ulcers with an alternative taping device. Medsurg Nurs. 2014;23(2):96‐100. [PubMed] [Google Scholar]
- 51. Monarca MC, Marteka P, Breda K. Decreasing incidence of medical device‐related pressure injuries in a small community hospital. J Wound Ostomy Continence Nurs. 2018;45(2):137‐140. [DOI] [PubMed] [Google Scholar]
- 52. Coyer F, Cook J, Brown W, Vann A, Doubrovsky A. Securement to prevent device‐related pressure injuries in the intensive care unit: a randomised controlled feasibility study. Int Wound J. 2020;17(6):1566‐1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Tayyib N, Asiri MY, Danic S, et al. The effectiveness of the SKINCARE bundle in preventing medical device‐related pressure injuries in critical care units: a clinical trial. Adv Skin Wound Care. 2021;34(2):75‐80. [DOI] [PubMed] [Google Scholar]
- 54. Cooper KD, McQueen KM, Halm MA, Flayter R. Prevention and treatment of device‐related hospital‐acquired pressure injuries. Am J Crit Care. 2020;29(2):150‐154. [DOI] [PubMed] [Google Scholar]
- 55. Gefen A, Alves P, Ciprandi G, et al. An international consensus on device‐related pressure ulcers: SECURE prevention. Br J Nurs. 2020;29(5):S36‐S38. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data available on request from the authors.