

Notes
Editorial note
There is a more recent Cochrane review on this topic: https://doi.org/10.1002/14651858.CD013667.pub2
Abstract
Background
Self‐harm (SH; intentional self‐poisoning or self‐injury) is common in children and adolescents, often repeated, and strongly associated with suicide. This is an update of a broader Cochrane review on psychosocial and pharmacological treatments for deliberate SH first published in 1998 and previously updated in 1999. We have now divided the review into three separate reviews; this review is focused on psychosocial and pharmacological interventions for SH in children and adolescents.
Objectives
To identify all randomised controlled trials of psychosocial interventions, pharmacological agents, or natural products for SH in children and adolescents, and to conduct meta‐analyses (where possible) to compare the effects of specific treatments with comparison types of treatment (e.g., treatment as usual (TAU), placebo, or alternative pharmacological treatment) for children and adolescents who SH.
Search methods
For this update the Cochrane Depression, Anxiety and Neurosis Group (CCDAN) Trials Search Co‐ordinator searched the CCDAN Specialised Register (30 January 2015).
Selection criteria
We included randomised controlled trials comparing psychosocial or pharmacological treatments with treatment as usual, alternative treatments, or placebo or alternative pharmacological treatment in children and adolescents (up to 18 years of age) with a recent (within six months) episode of SH resulting in presentation to clinical services.
Data collection and analysis
Two reviewers independently selected trials, extracted data, and appraised study quality, with consensus. For binary outcomes, we calculated odds ratios (OR) and their 95% confidence intervals (CI). For continuous outcomes measured using the same scale we calculated the mean difference (MD) and 95% CI; for those measured using different scales we calculated the standard mean difference (SMD) and 95% CI. Meta‐analysis was only possible for two interventions: dialectical behaviour therapy for adolescents and group‐based psychotherapy. For these analyses, we pooled data using a random‐effects model.
Main results
We included 11 trials, with a total of 1,126 participants. The majority of participants were female (mean = 80.6% in 10 trials reporting gender). All trials were of psychosocial interventions; there were none of pharmacological treatments. With the exception of dialectical behaviour therapy for adolescents (DBT‐A) and group‐based therapy, assessments of specific interventions were based on single trials. We downgraded the quality of evidence owing to risk of bias or imprecision for many outcomes.
Therapeutic assessment appeared to increase adherence with subsequent treatment compared with TAU (i.e., standard assessment; n = 70; k = 1; OR = 5.12, 95% CI 1.70 to 15.39), but this had no apparent impact on repetition of SH at either 12 (n = 69; k = 1; OR 0.75, 95% CI 0.18 to 3.06; GRADE: low quality) or 24 months (n = 69; k = 1; OR = 0.69, 05% CI 0.23 to 2.14; GRADE: low quality evidence). These results are based on a single cluster randomised trial, which may overestimate the effectiveness of the intervention.
For patients with multiple episodes of SH or emerging personality problems, mentalisation therapy was associated with fewer adolescents scoring above the cut‐off for repetition of SH based on the Risk‐Taking and Self‐Harm Inventory 12 months post‐intervention (n = 71; k = 1; OR = 0.26, 95% CI 0.09 to 0.78; GRADE: moderate quality). DBT‐A was not associated with a reduction in the proportion of adolescents repeating SH when compared to either TAU or enhanced usual care (n = 104; k = 2; OR 0.72, 95% CI 0.12 to 4.40; GRADE: low quality). In the latter trial, however, the authors reported a significantly greater reduction over time in frequency of repeated SH in adolescents in the DBT condition, in whom there were also significantly greater reductions in depression, hopelessness, and suicidal ideation.
We found no significant treatment effects for group‐based therapy on repetition of SH for individuals with multiple episodes of SH at either the six (n = 430; k = 2; OR 1.72, 95% CI 0.56 to 5.24; GRADE: low quality) or 12 month (n = 490; k = 3; OR 0.80, 95% CI 0.22 to 2.97; GRADE: low quality) assessments, although considerable heterogeneity was associated with both (I2 = 65% and 77% respectively). We also found no significant differences between the following treatments and TAU in terms of reduced repetition of SH: compliance enhancement (three month follow‐up assessment: n = 63; k = 1; OR = 0.67, 95% CI 0.15 to 3.08; GRADE: very low quality), CBT‐based psychotherapy (six month follow‐up assessment: n = 39; k = 1; OR = 1.88, 95% CI 0.30 to 11.73; GRADE: very low quality), home‐based family intervention (six month follow‐up assessment: n = 149; k = 1; OR = 1.02, 95% CI 0.41 to 2.51; GRADE: low quality), and provision of an emergency card (12 month follow‐up assessment: n = 105, k = 1; OR = 0.50, 95% CI 0.12 to 2.04; GRADE: very low quality). No data on adverse effects, other than the planned outcomes relating to suicidal behaviour, were reported.
Authors' conclusions
There are relatively few trials of interventions for children and adolescents who have engaged in SH, and only single trials contributed to all but two comparisons in this review. The quality of evidence according to GRADE criteria was mostly very low. There is little support for the effectiveness of group‐based psychotherapy for adolescents with multiple episodes of SH based on the results of three trials, the evidence from which was of very low quality according to GRADE criteria. Results for therapeutic assessment, mentalisation, and dialectical behaviour therapy indicated that these approaches warrant further evaluation. Despite the scale of the problem of SH in children and adolescents there is a paucity of evidence of effective interventions. Further large‐scale trials, with a range of outcome measures including adverse events, and investigation of therapeutic mechanisms underpinning these interventions, are required. It is increasingly apparent that development of new interventions should be done in collaboration with patients to ensure that these are likely to meet their needs. Use of an agreed set of outcome measures would assist evaluation and both comparison and meta‐analysis of trials.
Plain language summary
Interventions for children and adolescents who self‐harm
Why is this review important?
Self‐harm (SH), which includes intentional self‐poisoning/overdose and self‐injury, is a major problem in children and adolescents in many countries and is strongly linked to risk of future suicide. It is therefore important that effective treatments for SH patients are developed.
Who will be interested in this review?
Clinicians working with young people who engage in SH, policy makers, young people who themselves have self‐harmed or may be at risk of doing so, and their families and relatives.
What questions does this review aim to answer?
This review is an update of a previous Cochrane review from 1999 which found little evidence of beneficial effects of interventions for SH aimed specifically at children and adolescents. This update aims to further evaluate the evidence for the effectiveness of psychosocial and pharmacological treatments for children and adolescents who engage in SH with a broader range of outcomes, particularly with regards to investigating whether there are specific treatments for children and adolescents who SH which have greater benefit compared to routine care in terms of treatment adherence and improvements in psychological well‐being.
Which studies were included in the review?
To be included in the review, studies had to be randomised controlled trials of either psychosocial or pharmacological treatments for children and adolescents up to 18 years of age who had recently engaged in SH and presented to clinical services.
What does the evidence from the review tell us?
There have been surprisingly few investigations of treatments for SH in children and adolescents, despite the size of this problem in many countries. Providing therapeutic assessment may improve attendance at subsequent treatment sessions. Only one therapeutic approach ‐ mentalisation ‐ was associated with a reduction in frequency of repetition of SH. However this effect was only modest and the trial was small, which prevents us from being able to make firm conclusions about the effectiveness of this treatment. There was no clear evidence of effectiveness for compliance enhancement, individual cognitive behavioral therapy (CBT)‐based psychotherapy, home‐based family intervention, or provision of an emergency card, nor was there clear evidence for group therapy for adolescents with a history of multiple episodes of SH.
What should happen next?
Therapeutic assessment, mentalisation, and dialectical behaviour therapy warrant further investigation. While in a single small study, individual CBT‐based psychotherapy appeared ineffective, further evaluation of this treatment is also desirable given the favourable results found in adults who SH. Given the extent of SH in children and adolescents, greater attention should be paid to the development and evaluation of specific therapies for this population.
Summary of findings
Summary of findings 1. Comparison 1: individual CBT‐based psychotherapy versus treatment as usual.
| CBT‐based psychotherapy compared to treatment as usual | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatient. Intervention: individual CBT‐based psychotherapy. Comparison: treatment as usual. | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | CBT‐based psychotherapy | |||||
| Repetition of SH at six months | Study population | OR 1.88 (0.3 to 11.73) | 39 (1 RCT) | ⊕⊝⊝⊝ VERY LOW1,2 | Quality was downgraded as information on allocation concealment, participant blinding, outcome assessor blinding, and selective outcome reporting was not adequately described. The trial was further downgraded as the same therapists delivered both the intervention and control treatments leading to possible confounding which could have led to a reduction in the demonstrated effect. | |
| 111 per 1000 | 190 per 1000 (36 to 595) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CBT: cognitive behavioural therapy; CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as VERY SERIOUS as information on allocation concealment, participant blinding, outcome assessor blinding, and selective outcome reporting was not adequately described raising the possibility of selection bias, performance bias, detection bias, and reporting bias. Given that the same therapists delivered both the intervention and control treatments in this trial, there is also the possibility of confounding which could have led to a reduction in the demonstrated effect.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Summary of findings 2. Comparison 2: interventions for patients with multiple episodes of SH or emerging personality problems versus treatment as usual or routine management.
| Dialectical behaviour therapy or mentalisation for adolescents compared to treatment as usual or other routine management | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatients. Intervention: dialectical behaviour therapy or mentalisation for adolescents. Comparison: treatment as usual or other routine management (i.e., enhanced usual care) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | Interventions for patients with multiple episodes of SH or emerging personality problems | |||||
| Dialectical behaviour therapy for adolescents (DBT‐A) | ||||||
| Repetition of SH at post‐intervention | 151 per 1000 |
113 per 1000 (21 per 439) |
OR 0.72 (0.12 to 4.40) |
105 (2 RCTs) |
⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as neither participants nor clinical personnel were blind as to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. |
| Frequency of SH at post‐intervention | The mean frequency of SH episodes at post‐intervention in the intervention group was 0.79 lower (2.78 lower to 1.20 higher) | ‐ | 104 (2 RCTs) |
⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as neither participants nor clinical personnel were blind as to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. | |
| Mentalisation | ||||||
| Repetition of SH at post‐intervention | 829 per 1000 |
557 per 1000 (303 to 790) |
OR 0.26 (0.09 to 0.78) |
71 (1 RCT) |
⊕⊕⊕⊝ MODERATE1 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. |
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as SERIOUS as the nature of the intervention means that clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Summary of findings 3. Comparison 5: group‐based psychotherapy versus treatment as usual.
| Group‐based psychotherapy compared to treatment as usual | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatient. Intervention: group‐based psychotherapy. Comparison: treatment as usual | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | Group‐based psychotherapy | |||||
| Repetition of SH at six months | Study population | OR 1.72 (0.56 to 5.24) | 430 (2 RCTs) | ⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. | |
| 726 per 1000 | 820 per 1000 (597 to 933) | |||||
| Repetition of SH at 12 months | Study population | OR 0.8 (0.22 to 2.97) | 490 (3 RCTs) | ⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. | |
| 588 per 1000 | 533 per 1000 (239 to 809) | |||||
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as SERIOUS as the nature of the intervention means that clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Summary of findings 4. Comparison 6: therapeutic assessment versus treatment as usual (i.e., standard assessment).
| Therapeutic assessment compared to treatment as usual (i.e., standard psychosocial assessment) for self‐harm in children and adolescents | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatients. Intervention: therapeutic assessment. Comparison: treatment as usual (i.e., standard psychosocial assessment). | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Standard psychosocial assessment | Therapeutic assessment | |||||
| Repetition of SH at 12 months | Study population | OR 0.75 (0.18 to 3.06) | 69 (1 RCT) | ⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. | |
| 147 per 1000 | 115 per 1000 (30 to 345) | |||||
| Repetition of SH at 24 months | Study population | OR 0.69 (0.23 to 2.14) | 69 (1 RCT) | ⊕⊕⊝⊝ LOW1,2 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. Quality was further downgraded due to imprecision in the effect size estimate. | |
| 265 per 1000 | 199 per 1000 (76 to 435) | |||||
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as SERIOUS as the nature of the intervention means that clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Summary of findings 5. Comparison 7: compliance enhancement plus treatment as usual (i.e., standard disposition planning) versus treatment as usual.
| Compliance enhancement plus treatment as usual (i.e., standard disposition planning) compared to treatment as usual | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatient. Intervention: compliance enhancement plus standard disposition planning. Comparison: treatment as usual (i.e., standard disposition planning). | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | Standard disposition planning | |||||
| Repetition of SH by six months | Study population | OR 0.67 (0.15 to 3.08) | 63 (1 RCT) | ⊕⊝⊝⊝ VERY LOW1,2 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. Quality was further downgraded as details on blinding of outcome assessors, incomplete data and selective reporting was not adequately described. Lastly, due to imprecision in the effect size estimate, quality was further downgraded. | |
| 147 per 1000 | 104 per 1000 (25 to 347) | |||||
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as VERY SERIOUS as the nature of the intervention means that participants and clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present. Additionally, details on blinding of outcome assessors, incomplete data and selective reporting was not adequately described.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Summary of findings 6. Comparison 8: home‐based family intervention versus treatment as usual.
| Home‐based family intervention compared to treatment as usual | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatients. Intervention: home‐based family intervention. Comparison: treatment as usual. | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | Home‐based family intervention | |||||
| Repetition of SH at six months | Study population | OR 1.02 (0.41 to 2.51) | 149 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Quality was downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation. | |
| 147 per 1000 | 149 per 1000 (66 to 301) | |||||
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as SERIOUS as the nature of the intervention means that participants and clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present.
Summary of findings 7. Comparison 9: remote contact interventions versus treatment as usual.
| Remote contact interventions compared to treatment as usual | ||||||
| Patient or population: children and adolescents who engage in SH. Settings: outpatients. Intervention: remote contact interventions (emergency card). Comparison: treatment as usual. | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Treatment as usual | Emergency card | |||||
| Repetition of SH at 12 months | Study population | OR 0.5 (0.12 to 2.04) | 105 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1,2 | Quality was downgraded as an open random numbers table was used to generate the allocation sequence and, as allocation was not concealed, there is possible selection bias. Quality was further downgraded as the nature of this intervention means it is unlikely participants and clinical personnel would have been blind to treatment allocation and, as no details on outcome assessor blinding were provided, performance and detection bias cannot be ruled out. Lastly, there was an error in the randomisation sequence such that five participants in the intervention group either did not receive emergency cards, or alternatively, received them only after a delay thereby invalidating follow‐up data for these five individuals. | |
| 121 per 1000 | 64 per 1000 (16 to 219) | |||||
| *The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial; SH: self‐harm. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Risk of bias was rated as VERY SERIOUS as the nature of the intervention means that participants and clinical personnel could not have remained blind to treatment allocation suggesting that performance and detection bias may have been present. Additionally, as an open random numbers table was used to generate the allocation sequence and, as allocation was not concealed, there is possible selection bias. There was also an error in the randomisation sequence resulting in five participants in the intervention group either not receiving the cards, or alternatively, not receiving them until after a substantial delay thereby invalidating follow‐up data for these individuals.
2 Imprecision was rated as SERIOUS owing to the wide confidence interval associated with the estimate of treatment effect.
Background
Description of the condition
The term ‘self‐harm’ is used to describe all intentional acts of self‐poisoning (such as overdoses) or self‐injury (such as self‐cutting), irrespective of degree of suicidal intent or other types of motivation (Hawton 2003). Thus it includes acts intended to result in death (‘attempted suicide’), those without suicidal intent (for example, to communicate distress, to temporarily reduce unpleasant feelings), and those with mixed motivation (Hjelmeland 2002; Scoliers 2009). The term ‘parasuicide’ was introduced by Kreitman 1969 to include the same range of behaviour. However, ‘parasuicide’ has been used in the USA to refer specifically to acts of self‐harm without suicidal intent (Linehan 1991), and the term has largely fallen into disuse in the UK and other countries. In the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM‐5; American Psychiatric Association 2013), two types of self‐harming behaviour are included as conditions for further study, namely "Non‐Suicidal Self Injury" (NSSI) and "Suicidal Behavior Disorder" (SBD). Many researchers and clinicians, however, believe this to be an artificial and somewhat misleading categorisation (Kapur 2013), and recent research has shown a high level of co‐occurance between NSSI and attempted suicide, in particular among young people (Andover 2012). We have therefore used the approach favoured in the UK and some other countries of conceptualising all intentional self‐harm in a single category, namely self‐harm (SH).
SH is a major problem in children and adolescents (Hawton 2012a). Unlike suicide, in most countries SH in young people occurs far more commonly in females than males (Evans 2005). SH is uncommon below the age of 12 years (Hawton 2003); from age 12 years onwards, SH becomes increasingly frequent in girls such that the female:male ratio between 12 and 15 years of age is as high as five or six to one. This is thought to be due to the increased prevalence of depression in young adolescent females, and alcohol consumption and engagement in sexual activity in both genders (Patton 2007). The gender ratio decreases in the older teenage years as the behaviour becomes more frequent in boys and rates level off in girls. SH is more frequent in adolescents from lower socioeconomic groups (Burrows 2010). In the UK, SH has become more common in adolescents in recent decades, at least as reflected in hospital presentations (Hawton 2003). However, only about one in eight adolescents in the community who self‐report engaging in SH ever presents to hospital (Hawton 2002; McMahon 2014; Ystgaard 2009). In fact, it has become increasingly apparent that SH in adolescents in the community (without hospital presentation) is extremely common (Hawton 2012a; Madge 2008; McMahon 2014), although less is known about these individuals.
In children and adolescents who present to hospital, the most common method of SH is self‐poisoning, with overdoses of analgesics (especially paracetamol) being common in some countries, particularly those of high income (Hawton 2012b; Sheen 2002). In a multicentre study of child and adolescent SH presentations to hospitals in England, three‐quarters of individuals were girls and self‐poisoning occurred in just over three‐quarters of episodes (Hawton 2012b). Self‐cutting is the next most frequent method for those who present to hospital. In the community, however, self‐cutting and other forms of self‐mutilation are far more frequent than self‐poisoning (Madge 2008).
SH (and suicide) in adolescents is the result of a complex interplay between genetic, biological, psychiatric, psychosocial, social, and cultural factors (Hawton 2012a). Relationship problems are common in adolescents who engage in SH, especially problems with family members. Relationship problems with partners are more common in older adolescents than in younger adolescents (Hawton 2012b); there may also be a history of emotional, physical, or sexual abuse (Madge 2011). Bullying, including cyberbullying, can also increase the risk of SH (Hinduja 2010). Psychiatric disorders are common in adolescents who present to hospital because of SH, with depression, anxiety, ADHD, and eating disorders being particularly frequent (Hawton 2013). While personality disorders should not be diagnosed in adolescents, emergent pathological personality traits may be apparent during this phase of development, with traits similar to those in adult borderline personality disorder being found in some adolescents who engage in frequent repetition of SH (Crowell 2012). Poor emotion regulation abilities or poor emotional intelligence may also contribute to the risk of SH in this population (Mikolajczak 2009).
SH in adolescence often has a 'contagious' quality, and exposure to SH (and suicide) in friends and family members can be a strong influence (Hawton 2002; McMahon 2013; O'Connor 2014). Adolescents are also vulnerable to media influences; SH in both traditional media, such as films and television soaps, and new media, especially the Internet and social networking (Daine 2013), are important.
Psychological influences on SH in young people include feelings of entrapment, lack of belonging, and perceiving oneself as a burden (O'Connor 2012). Deficiencies in problem‐solving skills may also be relevant (Speckens 2005). Other contributors include perfectionism, low self‐esteem, social isolation, impulsivity, hopelessness, and poor parent‐child attachment (Hawton 2012a). On the other hand, social attachment to family (Carter 2007), friends, and school may be protective (King 2008; Stallard 2013).
Repetition of SH is common in adolescents, with 15‐25% of individuals who present to hospital following SH returning to the same hospital following a repeat episode within a year (Hawton 2008b). There may also be other repeat episodes that do not result in hospital presentation. Repetition is also common in adolescents who do not present to clinical care (Hawton 2002).
While suicide is relatively uncommon in younger adolescents, SH generally increases the risk of future suicide, especially in adolescent males. Risk is also increased in those who repeat SH and, contrary to clinical opinion, possibly in those who cut themselves (compared to those who engage in self‐poisoning) (Hawton 2012c).
Of particular concern regarding after‐care of adolescents who engage SH and who present to hospital is the fact that adherence to recommended treatment tends to be relatively poor; between 25% and 50% of adolescents will not attend any follow‐up sessions (Granboulan 2001; Taylor 1984).
Description of the intervention
Treatment for SH in children and adolescents may involve psychosocial interventions, pharmacological interventions, or a combination of the two approaches.
Psychosocial interventions
Given the role of psychological influences, and particularly problem‐solving deficits (Speckens 2005), in children and adolescents who engage in SH, psychological approaches used in the treatment of these individuals typically involve brief individual or group‐based psychological therapy (such as cognitive‐behavioural therapy or problem‐solving therapy), family therapy, and contact interventions; enhanced assessment interventions may also be used. Treatment may vary in terms of initial management, location of treatment, continuity, and intensity or frequency of contact with therapists. There is also considerable variation among countries in the availability of services to provide such interventions. Consequently, there is no standard psychosocial treatment for SH in children and adolescents. However, in high income countries treatment generally consists of a combination of assessment, support, involvement of relatives, and individual psychological therapies.
Pharmacological interventions
Given the prevalence of depression in children and adolescents who present to hospital following an episode of SH (Hawton 2013), pharmacological treatments may include antidepressants. Other pharmacological agents, such as benzodiazepines and other anxiolytics, may also be prescribed. However, treatment with pharmacological agents is generally less common than treatment with psychosocial interventions, partly due to concerns about the risk of exacerbating suicidality (Miller 2014).
How the intervention might work
Psychosocial interventions
The mechanisms of action of psychosocial interventions might include helping adolescents improve their coping skills and tackle specific problems, overcoming psychiatric disorders, improving self‐esteem, increasing a sense of social connectedness, and reducing impulsivity, aggression, and unhelpful reactions to distressing situations.
Cognitive behavioural therapy‐based psychotherapy
This intervention includes both cognitive behavioural therapy (CBT) and problem‐solving therapy (PST). CBT helps patients identify and critically evaluate the ways in which they interpret and evaluate disturbing emotional experiences and events (Westbrook 2011), and aims to help them change the ways in which they deal with problems. This is achieved in three steps: first, patients are helped to change the ways in which they interpret and evaluate distressing emotions; second, patients learn strategies to help them change the way in which they think about the meanings and consequences of these emotions; finally, with the benefit of modified interpretation of emotions and events, patients are helped to change their behaviour and develop positive functional behaviour (Jones 2012).
PST, which is an integral part of CBT, assumes that ineffective and maladaptive coping behaviours might be overcome by helping patients learn skills to actively, constructively, and effectively solve the problems they face in their daily lives (Nezu 2010), and that this will reduce SH. PST consists of encouraging patients to consciously and rationally appraise problems, reduce or modify the negative emotions generated by problems, and develop a range of possible solutions to address problems (D'Zurilla 2010). Treatment goals include helping patients to develop a positive problem‐solving orientation, use rational problem‐solving strategies, reduce the tendency to avoid problem‐solving, and reduce the use of impulsive problem‐solving strategies (Washburn 2012). Homework assignments are an essential component of CBT‐based psychotherapy.
Interventions for patients with multiple episodes of SH or emerging personality problems
Dialectical behaviour therapy
Dialectical behaviour therapy (DBT) in adults combines problem‐solving training, skills training, cognitive modification training, and mindfulness techniques (Washburn 2012), encouraging patients to accept their thoughts, feelings, and behaviours without necessarily attempting to change, suppress, or avoid these experiences (Lynch 2006). Within this framework, the aim of DBT is to help patients better regulate their emotions, achieve a sense of interpersonal effectiveness, become more tolerant of distressing thoughts or feelings, and become better at managing their own thoughts and behaviours (Linehan 1993; Linehan 2007). The primary treatment goals of DBT are therefore threefold: to reduce SH, behaviours that interfere with the success of treatment (such as treatment non‐adherence), and any other factors which may adversely affect the patent's quality of life (such as frequency or duration of psychiatric hospitalizations) (Linehan 1993).
Dialectical Behaviour Therapy for Adolescents (DBT‐A) is a clinical programme for adolescents with severe personality difficulties and co‐morbid mental health problems. DBT‐A has been adapted by Miller 2007 from Linehan’s initial conceptualisation of DBT which was developed for adults diagnosed with borderline personality disorder. DBT‐A typically includes a combination of individual and family sessions (Mehlum 2014). As the aim of DBT‐A is to help adolescents change or adjust to maladaptive personality characteristics, the treatment is intensive and relatively prolonged, although usually less so than in adults (James 2008; Miller 2007).
Mentalisation
Mentalisation refers to the ability to understand the actions of both the self and of others as meaningful given knowledge of the desires, beliefs, feelings, emotions, and motivations that underscore the behaviour (Bateman 2004; Choi‐Kain 2008). During times of interpersonal stress, however, individuals may fail to represent experiences in terms of mental states, and instead become overwhelmed with negative thoughts and feelings about the self (Rossouw 2013). Behaviours such as SH may therefore represent an escape from these negative self‐evaluations. Mentalisation therapy aims to improve patients’ ability to empathise with others by developing an understanding of how their own behaviours may impact on the feelings of others, and to regulate their own emotions more effectively (Rossouw 2013).
Group‐based psychotherapy
In the treatment of adolescents who have engaged in SH, group psychotherapy has included the integration of techniques from several therapies, including CBT, DBT‐A, and specific group techniques (Green 2011; Wood 2001a). In adolescents, group‐based psychotherapy may be more effective than individual psychotherapy as it provides patients with a chance to work on skills related to developing interpersonal relationships and problem‐solving, which are deficient in some suicidal adolescents (Evans 2004; Speckens 2005).
Enhanced assessment approaches
Therapeutic assessment combines standard psychosocial history and risk assessment techniques with cognitive‐analytic therapy and PST (Ougrin 2011a). Adolescents learn to identify sources of psychological pain and their connection to problem behaviours such as SH, and identify ways to break this cycle. The aim is to enhance adherence with subsequent treatment and therefore potential benefit from it.
Compliance enhancement approaches
Given the known poor treatment adherence of adolescents who engage in SH (Granboulan 2001; Taylor 1984), efforts to maintain contact with patients, such as following up patients in the community, as well as efforts to address factors likely to impede attendance at treatment sessions may be used to enhance treatment engagement and adherence (Spirito 2002).
Home‐based family interventions
Home‐based family intervention typically involves conjoint therapy sessions with the child or adolescent and family members. It includes negotiation of goals, exploration of the SH episode, communication between family members, problem solving, and discussion of developmental issues and their impact on the family. The basis of this therapy is that SH in young people may relate to family dysfunction and that this therapeutic approach could help families function better and hence reduce the risk of suicidal ideation and SH (Harrington 1998).
Remote contact interventions
Contact interventions, particularly emergency card interventions, can be used to encourage patients to seek help when they feel distressed as well as offering provision of on‐demand emergency contact with psychiatric services (Kapur 2010). In adolescents this has been used as a means of gaining admission to psychiatric inpatient care (Cotgrove 1995). The aim is to reduce the risk of SH by facilitating rapid access to care.
Pharmacological interventions
Antidepressants
Antidepressants might be expected to have general benefits on mood in young people with depression and, hence, reduce thoughts and acts of SH. Commonly used antidepressants include tricyclics and newer generation antidepressants (such as selective serotonin reuptake inhibitors (SSRIs)). Tricyclic antidepressants primarily inhibit both serotonin and norepinephrine reuptake, whereas SSRIs specifically target synaptic serotonergic reuptake (Feighner 1999). Given the link between serotonin activity, impulsivity, and suicidal behaviour (van Heeringen 2014), both tricyclic and SSRI antidepressants might be expected to be associated with a serotonin‐mediated reduction in impulsivity which could reduce the likelihood that an individual will engage in SH. However, there have been significant concerns that SSRIs (apart from fluoxetine) may increase suicidality in young people, resulting in warnings from regulatory agencies in both the UK (Medicines and Healthcare products Regulatory Agency; MHRA 2003) and the USA (Food and Drug Administration 2004). Guidance from the National Institute for Clinical Excellence (NICE) suggests that only fluoxetine has been shown to be of benefit for depression in children and young people (NICE 2005). Recent studies, however, indicate that warnings from regulatory agencies may have had unintended consequences, such as increases in suicide attempts among young people (Lu 2014).
Antipsychotics
One risk factor for SH, including repetition of the behaviour, may be heightened arousal, especially in relation to stressful life events. The rationale for the use of antipsychotics is that by reducing this arousal, the urge to engage in SH may also be reduced. Case series data suggest some benefit for low potency second generation antipsychotics (such as quetiapine) in reducing suicidality in adolescents diagnosed with major depression (e.g., Good 2006).
Mood stabilisers (including antiepileptics)
Mood stabilisers may have specific benefits for children and adolescents diagnosed with bipolar disorder or unipolar disorder, especially in terms of preventing recurrence of episodes of mood disorder. It might therefore be anticipated that these drugs would offer benefits in terms of reducing the risk of suicidal behaviour. To date, however, such an effect has only been found for lithium in adults (Cipriani 2013). Lithium may also reduce the risk of suicidal behaviour via a serotonin‐mediated reduction in impulsivity and aggression. It is also possible that the long‐term clinical monitoring that all patients prescribed lithium treatment must undergo contributes to a reduction in SH (Cipriani 2013).
Other pharmacological agents
Benzodiazepines and other anxiolytics might be expected to reduce suicidal behaviour through their specific effects on anxiety (Tyrer 2012). However, because of their GABAminergic effects, benzodiazepines may also increase aggression and disinhibition (Albrecht 2014). In adolescents, furthermore, case series data also describe an increased risk of suicidality and SH in those prescribed benzodiazepines (e.g., Kandemir 2008). Other pharmacological agents, such as the N‐Methyl‐D‐aspartate receptor antagonist ketamine, may also have beneficial effects in patients with major depression. However, it is presently unclear whether ketamine has a specific antisuicidal effect, or rather whether its effectiveness is due to a reduction in depressive symptomatology more generally (Fond 2014).
Natural products
In adults, the main focus with regard to natural products and suicidal behaviour has been on dietary supplementation of omega‐3 fatty acids (fish oils; Tanskanen 2001). Omega‐3 fatty acids have been implicated in the neural network shown to correlate with the lethality of recent suicidal behaviour (Mann 2013). Blood plasma polyunsaturated fatty acid levels have also been implicated in the serotonin‐mediated link between low cholesterol and suicidal behaviour, suggesting that low omega‐3 fatty acid levels may have a negative impact on serotonin function (Sublette 2006). For those in whom SH is impulsive, omega‐3 supplementation may stimulate serotonin activity, thereby reducing the likelihood of engaging in SH (Brunner 2002).
Why it is important to do this review
SH in adolescents is a major social and healthcare problem. It represents significant morbidity, is often repeated, and has strong links to suicide. It also leads to substantial healthcare costs (Sinclair 2011). Many countries now have suicide prevention strategies (World Health Organization 2014); all include a focus on improved management of patients presenting with SH because of their greatly elevated suicide risk and high levels of psychopathology and distress. The National Suicide Prevention Strategy for England (Her Majesty's Government Department of Health 2012) and the national suicide prevention strategy for the USA (Office of the Surgeon General (US) 2012), for example, highlight adolescent SH patients as a key high risk group for special attention. In recent years there has been considerable focus on improving the standards of general hospital care for SH patients. In 2014 in the UK, the Royal College of Psychiatrists published a guideline on services (including assessment and treatment) for young people who engage in SH (Royal College of Psychiatrists 2014). In 2004, NICE produced a guideline on SH which focused on its short‐term physical and psychological management (NCCMH 2004). More recently it produced a second guideline focused particularly on longer‐term management (NICE 2011), using some interim data from the present review as the evidence base on therapeutic interventions. A similar guideline was produced in Australia and New Zealand (Boyce 2003). We had previously conducted a systematic review of treatment interventions for SH patients of all ages in terms of reducing repetition of SH which had highlighted the paucity of evidence for effective treatments, at least in terms of this outcome (Hawton 1998; Hawton 1999). The first NICE guideline essentially reinforced this conclusion (NCCMH 2004). Using interim data from the present review, the second NICE guideline concluded that there was no evidence showing that specific treatments for adolescent patients were more effective than routine care (NICE 2011).
We have now fully updated our original review in order to provide contemporary evidence to guide clinical policy and practice. Because of the increasing number treatment types and the need for a special focus on adolescents who engage in SH, we have divided the original review into three reviews: the present review which focuses on interventions for children and adolescents, a second review on pharmacological interventions in adults, and a third review on psychosocial interventions for adults. In the earlier review we focused on repetition of SH and suicide as the main outcomes. In this update we have now also included data on treatment adherence, depression, hopelessness, suicidal ideation, and problem‐solving.
Objectives
To identify all randomised controlled trials (RCTs) of psychosocial or pharmacological interventions for SH in children and adolescents (up to 18 years of age), and to conduct meta‐analyses (where possible) to compare the effects of specific treatments with comparison types of care (such as treatment as usual, routine psychiatric care, enhanced usual care, placebo, or alternative pharmacological treatment) for children and adolescents who SH.
Methods
Criteria for considering studies for this review
Types of studies
We included RCTs, including cluster randomised and cross‐over trials, of specific psychosocial or pharmacological treatments versus treatment as usual, routine psychiatric care, enhanced usual care, placebo, or any other pharmacological comparison in the treatment of child and adolescent SH patients.
Types of participants
Participant characteristics
Participants were males and females up to 18 years of age of all ethnicities. We also included trials where there was a small minority (<15%) of adult participants, providing these participants had been referred to child and adolescent mental health services. However, we undertook sensitivity analyses to assess the effect of inclusion of such trials.
Diagnosis
Participants who had engaged in any type of non‐fatal intentional self‐poisoning or self‐injury resulting in presentation to child and adolescent mental health services in the six months prior to trial entry were included. There were no restrictions on the frequency with which patients engaged in SH; thus, for example, we included studies where participants had frequently repeated SH (for example, those with SH behaviour associated with emergent borderline personality disorder).
We defined SH as any intentional act of self‐poisoning or self‐injury, irrespective of degree of suicidal intent or other types of motivation. Thus it includes acts intended to result in death (‘attempted suicide’), those without suicidal intent (for example, to communicate distress or temporarily reduce unpleasant feelings), and those with mixed motivation. Self‐poisoning includes both overdoses of medicinal drugs and ingestion of substances not intended for consumption (such as pesticides). Self‐injury includes acts such as self‐cutting, self‐mutilation, attempted hanging, and jumping in front of moving vehicles. We only included trials where participants presented to clinical services as a result of SH.
Co‐morbidities
There were no restrictions in terms of whether or not patients had psychiatric disorders, or the nature of those disorders, with the exception of intellectual disability (where any SH behaviour, such as head‐banging, is likely to be repetitive, as the purpose of this behaviour is usually different from that involved in SH; NICE 2004).
Setting
Interventions delivered in inpatient or outpatient settings were eligible for inclusion, as were trials from any country.
Subset data
We did not include trials in which only some participants had engaged in SH or studies of people with psychiatric disorders in which SH was an outcome variable but was not an inclusion criterion for entry into the trial.
Types of interventions
Categorisation of the interventions included in this review was informed by the trials themselves and was based on consensus discussions among the review team who have considerable experience in both research and clinical practice related to SH.
Psychosocial interventions
Experimental interventions
This could include:
individual CBT‐based psychotherapy;
interventions for patients with multiple episodes of SH or emerging personality problems;
group‐based psychotherapy;
enhanced assessment approaches;
compliance enhancement approaches;
home‐based family interventions;
remote contact interventions.
Comparator interventions
As treatment as usual (TAU) is likely to vary widely between settings, following previous work we defined TAU as routine clinical service provision that the patient would receive had they not been included in the study (i.e., routine care or 'standard disposition'; Hunt 2013). Other routine management comparators could include no specific treatment or enhanced usual care which refers to TAU that has in some way been supplemented, such as through the provision of psychoeducation, assertive outreach or more regular contact with case managers, and standard assessment approaches.
Pharmacological interventions
Experimental interventions
This could include:
tricyclic antidepressants (TADs; e.g., amitriptyline);
newer generation antidepressants (NGAs) such as SSRIs (e.g., fluoxetine), serotonin and noradrenaline reuptake inhibitors (SNRIs; e.g., venlafaxine), norepinephrine reuptake inhibitors (NRIs; e.g., reboxetine), tetracyclic antidepressants (e.g., maprotiline), noradrenergic specific serotonergic antidepressants (NaSSAs; e.g., mirtazapine), serotonin antagonist or reuptake inhibitors (SARIs; e.g., trazodone), or reversible inhibitors of monoamine oxidase type A (RIMAs; e.g., moclobemide)
any other antidepressants such as irreversible monoamine oxidase inhibitors (MAOIs; e.g., bupropion);
antipsychotics (e.g., quetiapine);
mood stabilisers, including antiepileptics (e.g., sodium valporate) and lithium;
other pharmacological agents (e.g., benzodiazepines, ketamine);
natural products (e.g., omega‐3 essential fatty acid supplementation).
Comparator interventions
In pharmacological trials, where a comparison with the specific effects of a drug is being made, the comparator is typically placebo, which consists of any pharmacologically inactive treatment such as sugar pills or injections with saline, although in some trials another comparator pharmacological intervention (such as another standard pharmacological agent or reduced dose of the intervention agent) may be used.
Types of outcome measures
Primary outcomes
The primary outcome measure in this review was the occurrence of repeated SH (defined above) over a maximum follow‐up period of two years. Repetition was identified through self‐report, collateral report, clinical records, or research monitoring systems. As we wished to incorporate the maximal amount of data from each trial, we included both self‐reported and hospital records of SH where available. We report both proportions of participants repeating SH and frequency of repeat episodes.
Secondary outcomes
1. Treatment adherence
This was assessed using a range of measures of adherence, including pill counts, changes in blood measures, and the proportion of participants that both started and completed treatment.
2. Depression
This was assessed either continuously, as scores on psychometric measures of depression symptoms (for example total scores on the Beck Depression Inventory (BDI; Beck 1961) or scores on the depression sub‐scale of the Hospital Anxiety and Depression Scale (HADS; Zigmond 1983)), or dichotomously as the proportion of patients reaching defined diagnostic criteria for depression.
3. Hopelessness
This was assessed as scores on psychometric measures of hopelessness, for example, total scores on the Beck Hopelessness Scale (BHS; Beck 1974).
4. Suicidal ideation
This was assessed either continuously, as scores on psychometric measures of suicidal ideation (for example, total scores on the Beck Scale for Suicidal Ideation (BSS; Beck 1988)), or dichotomously, as the proportion of patients reaching a defined cut‐off for ideation.
5. Problem‐solving
This was assessed either continuously, as scores on a psychometric measure of problem‐solving ability (for example total scores on the Problem Solving Inventory (PSI; Heppner 1988)), or dichotomously, as the proportion of patients with improved problems.
6. Suicide
This included both register‐recorded deaths and reports from collateral informants such as family members or neighbours.
Timing of outcome assessment
We have reported outcomes for the following time periods.
At the conclusion of the treatment period.
Between zero and six months after the conclusion of the treatment period.
Between six and 12 months after the conclusion of the treatment period.
Between 12 and 24 months after the conclusion of the treatment period.
Where there was more than one outcome assessment within a time period, we only used data from the last assessment in the time period, unless different outcomes were assessed at different points. For treatment adherence, we also used within‐treatment period results.
Hierarchy of outcome measures
Where a trial measured the same outcome (for example, depression) in two or more ways, we used the most common measure across trials in any meta‐analysis, but we also reported scores from the other measure in the text of the review.
Search methods for identification of studies
Electronic searches
Electronic searches
The Cochrane Depression, Anxiety and Neurosis Review Group's Specialised Register (CCDANCTR)
The Cochrane Depression, Anxiety and Neurosis Group (CCDAN) maintains two clinical trials registers at their editorial base in Bristol, UK: a references register and a studies‐based register. The CCDANCTR‐References contains over 37,500 reports of RCTs on depression, anxiety, and neurosis. Approximately 60% of these references have been tagged to individual, coded trials. The coded trials are held in the CCDANCTR‐Studies and records are linked between the two registers through the use of unique study ID tags. Coding of trials is based on the EU‐Psi coding manual. Please contact the CCDAN Trials Search Coordinator for further details.
Reports of trials for inclusion in the group's registers are collated from weekly generic searches of MEDLINE (1950 to date), EMBASE (1974 to date), and PsycINFO (1967 to date), as well as quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL).
The CCDANCTR (Studies and References) was searched on 30 January 2015 using terms for self‐harm (condition only), as outlined in Appendix 1. No restrictions on date, language, or publication status were applied to the search.
Additional electronic database searches
Complementary searches of MEDLINE (1998 to 2013), EMBASE (1998 to 2013), PsycINFO (1998 to 2013), and CENTRAL (The Cochrane Library, Issue 10, 2013) were conducted by Sarah Stockton, librarian at the University of Oxford, following the search strategy outlined in Appendix 2. Additionally, KW searched the Australian Suicide Prevention RCT Database (Christensen 2014). KW also conducted electronic searches of ClinicalTrials.gov and the ISRCTN registry using the keywords random* AND suicide attempt* OR self$harm* to identify relevant ongoing trials.
Both the original version of this review and an unpublished version also incorporated searches of the following databases: SIGLE (1980 to March 2005) and Sociofile (1963 to July 2006).
Searching other resources
Hand searching
For the original version of this review, the authors hand searched ten specialist journals within the fields of psychology and psychiatry, including all English language suicidology journals as outlined in Appendix 3. As these journals are now indexed in major electronic databases, we did not repeat hand searching for this update of the review.
Reference lists
The reference lists of all relevant papers known to the investigators were checked, as were the reference lists of major reviews which included a focus on interventions for SH in children and adolescents (Brausch 2012; Brent 2013; Burns 2000; Daniel 2009; Gould 2003; Hawton 2012a; Newton 2010; Nock 2007; Ougrin 2011b; Ougrin 2015; Robinson 2011).
Correspondence
We consulted the authors of trials and other experts in the field of suicidal behaviour to find out if they were aware of any ongoing or unpublished RCTs concerning the treatment of adolescent SH patients.
Data collection and analysis
For details of the data collection and analysis methods used in the original version of this review see Appendix 4.
Selection of studies
For this update of the review, all authors independently assessed the titles of trials identified by the systematic search for eligibility. We made a distinction between:
eligible trials, in which any psychosocial or psychopharmacological treatment was compared with a control (treatment as usual, standard or less intensive types of aftercare, placebo medication, or comparator drug/dose);
ineligible general treatment trials (without any control treatment).
All trials identified as potentially eligible for inclusion then underwent a second screening. Pairs of review authors, working independently from one another, screened the full text of relevant trials to identify whether the trial met our inclusion criteria.
Disagreements were resolved following consultation with KH. Where disagreements could not be resolved from the information reported within the trial, or where it was unclear whether the trial satisfied our inclusion criteria, we contacted study authors to provide additional clarification.
Data extraction and management
In the current update, data from included trials were extracted by KW and one of either TTS, EA, DG, PH, ET, or KvH using a standardised extraction form. Review authors extracted data independently of one another. Where there were any disagreements, these were resolved through consensus discussions with KH.
Data extracted from each eligible trial included participant demographics, details of the treatment and control interventions, and information on the outcome measures used to evaluate the efficacy of the intervention. Study authors were contacted to provide raw data for outcomes that were not reported in the full text of included trials.
Both dichotomous and continuous outcome data were extracted from eligible trials. As the use of non‐validated psychometric scales is associated with bias, we extracted continuous data only if the psychometric scale used to measure the outcome of interest had been previously published in a peer‐reviewed journal (Marshall 2000), and was not subjected to item, scoring, or other modification by the trial authors.
We planned the following main comparisons.
Individual CBT‐based psychotherapy (e.g., CBT, PST) versus TAU or other routine management.
Interventions for patients with multiple episodes of SH or emerging personality problems versus TAU or other routine management.
Group‐based psychotherapy versus TAU or other routine management.
Enhanced assessment approaches versus TAU or other routine management.
Compliance enhancement approaches versus TAU or other routine management.
Home‐based family interventions versus TAU or other routine management.
Remote contact interventions versus TAU or other routine management.
Tricyclic antidepressants versus placebo or other comparator drug/dose.
Newer generation antidepressants versus placebo or other comparator drug/dose.
Any other antidepressants versus placebo or other comparator drug/dose.
Antipsychotics versus placebo or other comparator drug/dose.
Mood stabilisers versus placebo or other comparator drug/dose.
Other pharmacological agents versus placebo or other comparator drug/dose.
Natural products versus placebo or other comparator drug/dose.
Assessment of risk of bias in included studies
Given that highly biased studies are more likely to overestimate treatment effectiveness (Moher 1998), the quality of included studies was evaluated independently by KW and one of either TTS, EA, DG, PH, ET, or KvH using the criteria described in Higgins 2011. This tool encourages consideration of the following domains.
Random sequence generation.
Allocation concealment.
Blinding of participants and personnel.
Blinding of outcome assessment.
Incomplete outcome data.
Selective outcome reporting.
Other bias.
Each source of potential bias was judged as contributing to at "low," "high," or "unclear" risk of each potential bias independently by two reviewers. Where inadequate details of the randomisation, blinding, or outcome assessment procedures were provided in the original report, we contacted authors to provide clarification. Disagreements were resolved following discussion with KH. Risk of bias for each included trial is reported in the text of the review, as well as in the 'Risk of bias' tables, along with supporting quotations from the trial report to justify each judgment.
Measures of treatment effect
Dichotomous outcomes
We summarised dichotomous outcomes, such as the number of participants engaging in a repeat SH episode and deaths by suicide, using the summary odds ratios (OR) and the accompanying 95% confidence interval (CI), as the OR is the most appropriate effect size statistic for summarising associations between two dichotomous groups (Fleiss 1994).
Continuous outcomes
For outcomes measured on a continuous scale, we used mean differences (MD) and accompanying 95% CI where the same outcome measure was employed. Where different outcome measures were employed, we used the standardised mean difference (SMD) and its accompanying 95% CI.
Trials were aggregated for the purposes of meta‐analysis only if treatments were sufficiently similar. For trials that could not be included in a meta‐analysis, we have instead provided narrative descriptions of the results.
Unit of analysis issues
Zelen design trials
Trials in this area are increasingly employing Zelen's method in which consent is obtained subsequent to randomisation and treatment allocation. This design may lead to bias if, for example, participants allocated to one particular arm of the trial disproportionally refuse to provide consent for participation or, alternatively, if participants only provide consent provided they are allowed to cross‐over to the active treatment arm (Torgerson 2004). No trial included in this review used Zelen's design. Given the uncertainty of whether to use data based on those randomised or those consenting to participation, should a trial using Zelen's method be identified in future updates of this review we plan to extract data using both sources where possible. We also plan to conduct sensitivity analyses to investigate what impact, if any, the inclusion of these trials may have on the pooled estimate of treatment effect.
Cluster randomised trials
Cluster randomisation, for example by clinician or practice, can lead to overestimation of the significance of a treatment effect, resulting in an inflation of the nominal type I error rate, unless appropriate adjustment is made for the effects of clustering (Donner 2002; Kerry 1998). One trial included in the review used clustering (Ougrin 2011a). As the study authors were unable to provide us with the values of either the inter‐cluster correlation coefficient or the design effect to enable us to statistically account for the effects of clustering (as per the guidance in Higgins 2011), for this trial we have used unadjusted data, but have commented on the impact this may have had on the results observed in the text of the review.
In future updates of this review, should we be able to obtain information on either the inter‐cluster correlation coefficient or the design effect, we will use the formula given in Higgins 2011 to account for the effects of clustering.
Cross‐over trials
A primary concern with cross‐over trials is the "carry‐over" effect in which the effect of the intervention treatment (pharmacological, physiological, or psychological) influences the participant's response to the subsequent control condition (Elbourne 2002). As a consequence, on entry to the second phase of the trial, participants may differ systematically from their initial state despite a wash‐out phase. This, in turn, may result in a concomitant underestimation of the effectiveness of the treatment intervention (Curtin 2002a; Curtin 2002b). No trials in the current review included cross‐over methodology. However, should we identify any such trials in future updates, only data from the first phase of the study, prior to cross‐over, will be included to protect against the carry‐over effect.
Studies with multiple treatment groups
No trials in the current review included multiple treatment groups. In future updates, however, should trials with multiple treatment groups be identified, all relevant treatment arms will be included in the review. For binary data we will combine data or use the data from the comparison arm in two or more analyses as appropriate. For continuous data, we will combine data following the formula given in Higgins 2011, section 7.7.3.8.
Studies with adjusted effect sizes
None of the trials included in the current update provided adjusted effect sizes. In future updates, however, where trials reported both unadjusted and adjusted effect sizes, we will include only unadjusted effect sizes.
Dealing with missing data
We did not impute missing data as we considered that the bias that would be introduced by doing this would have outweighed any benefit (in terms of increased statistical power) that may have been gained by the inclusion of imputed data. However, where authors omitted standard deviations (SD) for continuous measures, we planned to estimate these using the method described in Townsend 2001.
Dichotomous data
Although some authors said they conducted intention‐to‐treat analyses, few presented such analyses as defined by Higgins 2011. Therefore, outcome analyses for both dichotomous and continuous data were based on all information available on study participants. For dichotomous outcomes, we included data on only those participants whose results were known, using as the denominator the total number of participants with data for the particular outcome of interest, as recommended (Higgins 2011).
Continuous data
For continuous outcomes, we have included data only on observed cases.
Missing data
Where data on outcomes of interest were incomplete or were excluded from the text of the trial, we contacted study authors in order to try to obtain further information.
Assessment of heterogeneity
Between‐study heterogeneity can be assessed using either the Chi2 or I2 statistics. In this review, however, we used only the I2 statistic to determine heterogeneity as this is considered to be more reliable (Higgins 2011). The I2 statistic indicates the percentage of between‐study variation due to chance (Higgins 2011), and can take any value from 0% to 100%. We used the following values to denote relative importance of heterogeneity: 0% to 40% (unimportant), 30% to 60% (moderate), 50% to 90% (substantial), and 75% to 100% (considerable), as per the guidance in the Cochrane Handbook (Higgins 2011). Where we found substantial levels of heterogeneity (i.e., ≥ 75%), we explored reasons for this heterogeneity. We also planned to investigate heterogeneity when the I2 statistic was lower than 75% where either the direction or magnitude of a trial effect size was clearly discrepant from that of other trials included in the meta‐analysis (see Subgroup analysis and investigation of heterogeneity for further information on these analyses).
Assessment of reporting biases
Reporting bias occurs when the decision to publish a particular trial is influenced by the direction and significance of its results (Egger 1997). Research suggests, for example, that trials with statistically significant findings are more likely to be submitted for publication and to subsequently be accepted for publication (Hopewell 2009), leading to possible overestimation of the true treatment effect. To assess whether trials included in any meta‐analysis were affected by reporting bias, we planned to enter data into a funnel plot when a meta‐analysis included results of at least ten trials. Should evidence of any small study effects be identified, we planned to explore reasons for funnel plot asymmetry, including the presence of publication bias (Egger 1997).
Data synthesis
For the purposes of meta‐analysis, we calculated the pooled OR and accompanying 95% CI using the random‐effects model as this is the most appropriate model for incorporating heterogeneity between studies (Higgins 2011). Specifically, for dichotomous data, the Mantel‐Haenszel method was used, whilst the inverted variance method was used for continuous data. However, a fixed‐effect analysis was also undertaken to investigate the potential effect of method choice on the estimates of treatment effect. Any material differences in ORs between these two methods are reported descriptively in the text of the review. All analyses were undertaken in RevMan, version 5.3 (RevMan 2014).
Subgroup analysis and investigation of heterogeneity
Subgroup analyses
In the original version of this review, we planned to undertake subgroup analyses by repeater status and gender but found there were insufficient data. Consequently, in this update we only undertook a priori subgroup analyses by gender or repeater status where there were sufficient data to do so.
Given the increasing use of enhanced usual care rather than TAU in trials in this area, we also planned to undertake sub‐group analyses to determine whether comparator choice influenced the pattern of results observed.
Investigation of heterogeneity
We planned that should any meta‐analysis be associated with substantial levels of between‐study heterogeneity (i.e., I2 ≥ 75%), KH and KW would independently triple‐check data to ensure these had been correctly entered. Assuming data had been entered correctly, we would investigate the source of this heterogeneity by visually inspecting the forest plot and removing each trial which has a very different result to the general pattern of the others until homogeneity was restored as indicted by an I2 statistic < 75%. We planned to report the results of this sensitivity analysis in the text of the review alongside hypotheses regarding the likely causes of the heterogeneity.
Sensitivity analysis
We planned to undertake sensitivity analyses, where appropriate, as outlined below.
Where a trial made use of Zelen's method of randomisation (see Unit of analysis issues section).
Where a trial contributed to substantial between‐study heterogeneity (see Subgroup analysis and investigation of heterogeneity section).
Where a trial included a mixture of both adolescent and adult participants.
'Summary of findings' table
A 'Summary of findings' table was prepared for the primary outcome measure, repetition of SH, following recommendations outlined in Schünemann 2008a, section 11.5. This table provides information concerning the overall quality of evidence from each included trial. The 'Summary of findings' table was prepared using GRADEpro software (GRADEpro). Quality of the evidence was assessed following recommendations in the Cochrane Handbook (Higgins 2011).
Results
Description of studies
Results of the search
For this update, a total of 23,763 citations were found using the search strategies outlined in Appendix 1 and Appendix 2. A further 10 trials were identified through correspondence with researchers in the field; these trials were ongoing at the time of the systematic search. All but one have subsequently been published and a report on the remaining trial is currently in preparation. We were able to include data for this unpublished trial, however, by correspondence with and permission from study authors. In consultation with CCDAN, we have divided the original review into three separate reviews: the present review which focuses on psychosocial or pharmacological interventions for children and adolescents, a second review on psychosocial interventions for adults, and the third on pharmacological interventions for adults. All but one of the 10 additional trials identified through correspondence with study authors have evaluated psychosocial interventions in adults and these have therefore been included in the corresponding review. The remaining trial is one of a psychosocial intervention for children and adolescents (Cooney 2010) and has therefore been included in the present review.
After deduplication, the overall figure for citations was reduced to 16,736. Of these, 16,491 were excluded after screening, whilst a further 221 were excluded after reviewing the full texts (Figure 1).
1.
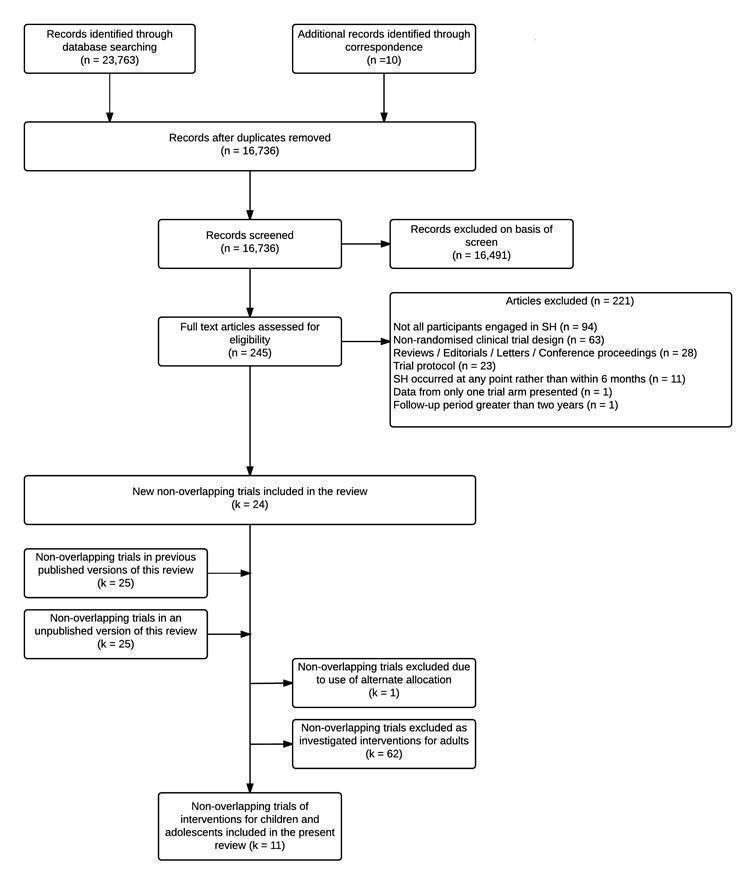
Prisma flow diagram
Included studies
In the previous versions of this review (Hawton 1998; Hawton 1999; NICE 2011), six trials of psychosocial interventions for adolescent SH patients were included (Cotgrove 1995; Donaldson 2005; Harrington 1998; Hazell 2009; Spirito 2002; Wood 2001a). The present update includes information from an additional five trials (Cooney 2010; Green 2011; Mehlum 2014; Ougrin 2011a; Rossouw 2012a). The present review therefore includes 11 non‐overlapping trials. A further report (Ougrin 2013) provided two‐year follow‐up data for one of the previously‐included trials (Ougrin 2011a).
None of the included trials were unpublished, however unpublished data were obtained from study authors for eight of the 11 included trials (Cooney 2010; Cotgrove 1995; Donaldson 2005; Green 2011; Ougrin 2011a; Rossouw 2012a; Spirito 2002; Wood 2001a).
Five ongoing trials of interventions for SH in children and adolescents were also identified (see Characteristics of ongoing studies for further information on these trials).
Design
Of the 11 trials, all were described as randomised controlled trials. Most (k = 10) employed a simple randomisation procedure based on individual allocation to the intervention and control groups. In one trial, clinicians rather than participants were randomised (Ougrin 2011a).
Participants
The included trials comprised a total of 1,126 child and adolescent participants. All had engaged in at least one episode of SH in the six months prior to randomisation.
Participant characteristics
Of the nine trials in which information on age was provided, the average age of participants at randomisation was 15.3 years (SD 0.5). All participants had been referred to child and adolescent mental health services. Of the 10 trials that recorded information on gender, the majority of participants were female (80.6%), reflecting the typical pattern for SH in children and adolescents (Hawton 2008a).
Diagnosis
A history of SH prior to the index episode (i.e., multiple episodes of SH) was a requirement for participation in five trials (Cooney 2010; Green 2011; Hazell 2009; Mehlum 2014; Wood 2001a). In one trial, over half of the sample (58.6%) had a history of multiple episodes of SH (Ougrin 2011a), whilst in a further trial just under half of the sample (48.4%) had a history of multiple episodes (Donaldson 2005). For four trials, information on the proportion of participants with a history of SH prior to the index episode was not reported (Cotgrove 1995; Harrington 1998; Rossouw 2012a; Spirito 2002). Two trials included participants who had made a "suicide attempt" (i.e., with evidence of suicidal intent) (Donaldson 2005; Spirito 2002); however, most trials (k = 7) included adolescents irrespective of intent (Cooney 2010; Harrington 1998; Hazell 2009; Mehlum 2014; Ougrin 2011a; Rossouw 2012a; Wood 2001a). In the two remaining trials, information on intent was not reported (Cotgrove 1995; Green 2011).
Information on the method of SH for the index episode was not reported in two trials (Cooney 2010; Mehlum 2014). In three trials, information on methods used in all lifetime episodes of SH (including the index episode) was reported (Hazell 2009; Rossouw 2012a; Wood 2001a). In the latter two trials, 64.0% and 94.4% respectively had a history of self‐poisoning whilst 95.5% and 74.6% respectively had a history of self‐injury. In Hazell 2009, 97.0% had a history of self‐cutting, 71.0% of head banging, 57.0% of self‐poisoning with prescription medication, 36.0% of self‐smothering, 25.0% of self‐strangulation, 19.0% of other forms of self‐injury, 19.0% of self‐drowning, 17.0% of jumping from a height, and 35.0% some other form of SH. Information on methods used for the index episode only for the remaining six trials is presented in Table 8. In these trials, the majority of participants (k = 6; 67.1%) had engaged in self‐poisoning.
1. Methods used for the index episode of self‐harm in included studies.
| Reference | Method 1 | |||
| Self‐poisoning (any) n (%) |
Self‐poisoning (alcohol) n (%) |
Self‐injury (any) n (%) |
Combined self‐ poisoning and self‐injury n (%) |
|
| Cotgrove 19952 | 94 (89.6) | 7 (6.6) | 2 (1.9) | |
| Donaldson 20053 | 33 (84.6) | |||
| Green 2011 | 5 (2.7) | 67 (36.6) | 111 (60.7) | |
| Harrington 1998 | 162 (100) | |||
| Ougrin 2011a | 28 (40.0) | 37 (52.8) | 5 (7.2) | |
| Spirito 20024 | 54 (85.7) | |||
1 Refers to method used for the index episode.
2 The method used by the remaining two (1.9%) participants was not reported.
3 The method used by the remaining six (15.4%) participants was not reported.
4 The method used by the remaining nine (14.3%) participants was not reported.
Co‐morbidities
Information on current psychiatric diagnoses was reported in 10 trials (see Table 9). In these trials, the most common psychiatric diagnoses were major depression (k = 8; mean 65.2%) and behavioural disorders (k = 4; mean 35.8%). One trial included a high proportion of adolescents diagnosed as having features of emerging borderline personality disorder (72.5%; Rossouw 2012a).
2. Psychiatric diagnoses in included studies.
| Reference | Psychiatric diagnosis1 | |||||||||||
| Major depression n (%) |
Any other
mood disorder n (%) |
Any anxiety disorder n (%) |
Post‐ traumatic stress disorder n (%) |
Any eating disorder n (%) |
Alcohol use disorder/ dependence n (%) |
Drug use disorder/ dependence n (%) |
Substance use disorder/ dependence n (%) |
Oppositional defiance disorder n (%) |
Conduct disorder n (%) |
Any other behaviour disorder n (%) |
Borderline personality disorder n (%) |
|
| Cooney 2010 | 23 (79.3) | 24 (82.7) | 7 (24.1) | 9 (31.0) | 8 (27.6) | |||||||
| Cotgrove 1995 | Information on psychiatric diagnosis not provided. | |||||||||||
| Donaldson 2005 | 9 (29.0) | 6 (19.3) | 14 (45.2) | 14 (45.2) | ||||||||
| Green 2011 | 227 (62.0) | 122 (22.2) | ||||||||||
| Harrington 1998 | 109 (67.3) | 17 (10.5) | ||||||||||
| Hazell 2009 | 41 (56.9) | 3 (4.2) | 5 (6.9)2 | |||||||||
| Mehlum 2014 | 17 (22.1) | 29 (37.7) | 33 (42.9) | 13 (16.9) | 6 (7.8) | 2 (2.6) | 15 (20.5) | |||||
| Ougrin 2011a3 | ||||||||||||
| Rossouw 2012a | 77 (96.2) | 35 (43.7) | 27.5 (28.0) | 58 (72.5) | ||||||||
| Spirito 20024 | 1 (2.2) | 6 (13.0) | 4 (8.7) | 6 (13.0) | 5 (10.9) | 6 (13.0) | ||||||
| Wood 2001a | 52 (83.9) | 42 (68.8)2 | ||||||||||
1 All diagnoses refer to current, rather than lifetime, diagnoses. The total percentages were more than 100% in some studies due to comorbidity.
2 Conduct disorder or oppositional defiance disorder.
3 The authors state that 53/70 (75.7%) participants had previous contact with mental health services. Diagnoses are only provided in broad categories, however. Specifically, 42/70 (60.0%) were diagnosed with an "emotional disorder," 9/70 (12.8%) were diagnosed with a "disruptive disorder," and 2/70 (2.8%) were diagnosed with "another disorder."
4 Information on psychiatric diagnoses were available for only 46 of the 63 participants.
Details on comorbid diagnoses were not reported in eight of the 11 trials (Cotgrove 1995; Green 2011; Harrington 1998; Hazell 2009; Mehlum 2014; Ougrin 2011a; Rossouw 2012a; Wood 2001a). In the remaining three trials, between 7.3% (Spirito 2002) and 93.1% (Cooney 2010) of participants were diagnosed with two or more psychiatric disorders. However, further information on specific diagnoses was not provided.
Setting
Of the 11 non‐overlapping RCTs included in this review, five were from the UK (Cotgrove 1995; Green 2011; Ougrin 2011a; Rossouw 2012a; Wood 2001a), three were from the US (Donaldson 2005; Harrington 1998; Spirito 2002), and one was from each of Australia (Hazell 2009), New Zealand (Cooney 2010), and Norway (Mehlum 2014). Although all participants were identified following a clinical presentation for SH, treatment was delivered on an outpatient basis or in the patient's home in nine trials. In the remaining trials of brief (one hour) compliance enhancement (Spirito 2002) and therapeutic assessment (Ougrin 2011a), the intervention was delivered whilst the adolescent was receiving treatment in hospital.
Interventions
All 11 trials included in this review investigated the effectiveness of various forms of psychosocial therapy.
Individual CBT‐based psychotherapy versus TAU (Donaldson 2005).
Interventions for patients with multiple episodes of SH or emerging personality problems versus TAU or other routine management (i.e., enhanced usual care) (Cooney 2010; Mehlum 2014; Rossouw 2012a).
Group‐based psychotherapy versus TAU (Green 2011; Hazell 2009; Wood 2001a).
Therapeutic assessment versus TAU (i.e., standard assessment) (Ougrin 2011a).
Compliance enhancement plus standard disposition planning versus TAU (i.e., standard disposition) (Spirito 2002).
Home‐based family intervention versus TAU (Harrington 1998).
Remote contact interventions plus TAU versus TAU (Cotgrove 1995).
There were no trials in which pharmacological treatments were investigated.
Outcomes
All 11 trials reported information on the primary outcome: repetition of SH. In the majority of these trials (k = 8), this was based on self‐reported information (Cooney 2010; Donaldson 2005; Harrington 1998; Hazell 2009; Mehlum 2014; Rossouw 2012a; Spirito 2002; Wood 2001a), whilst in one further trial, self‐reported information was combined with information from a collateral informant such as a parent (Green 2011). In one trial, information on repetition of SH was obtained from clinical or hospital notes supplemented by information from general practitioners, social workers, and psychologists (where relevant) (Cotgrove 1995). In only one trial, information on repetition of SH was based solely on representation to accident and emergency departments (Ougrin 2011a).
In the seven trials that recorded information on treatment adherence, this was assessed using a variety of methods including: the proportion of participants that completed the full course of treatment (Donaldson 2005; Harrington 1998; Rossouw 2012a), the proportion attending their first appointment (Ougrin 2011a), the proportion attending at least one treatment session (Spirito 2002), and the total number of treatment sessions attended (Cooney 2010; Mehlum 2014; Spirito 2002). Depression was assessed using the Mood and Feelings Questionnaire (MFQ; Angold 1995) in five trials (Green 2011; Hazell 2009; Mehlum 2014; Rossouw 2012a; Wood 2001a), the Montgomery‐Åsberg Depression Rating Scale (MADRS; Montgomery 1979) in one trial (Mehlum 2014), and the Center for Epidemiologic Studies Depression Scale (CES‐D; Radloff 1991) in one trial (Donaldson 2005). Hopelessness was assessed using the Hopelessness Scale (HS; Kazdin 1986) in one trial (Harrington 1998), the BHS in a second trial (Mehlum 2014), and by the future optimism sub‐scale score on the Reasons for Living Inventory‐Adolescent (RFL‐A; Osman 1998), which was reverse coded in the present review to indicate a perceived lack of optimism about the future (Cooney 2010). In six trials, information on suicidal ideation was assessed using the Suicidal Ideation Questionnaire (SIQ; Reynolds 1985; Reynolds 1988; Reynolds 1999) whilst in a further trial (Cooney 2010) suicidal ideation was assessed using the Beck Scale for Suicide Ideation (Beck 1991). For the two trials that reported information on problem‐solving, this was assessed using the Social Problem‐Solving Inventory (SPSI; Maydeu‐Olivares 1996) and the Means Ends Problem‐Solving test (MEPS; Platt 1971) in one trial (Donaldson 2005) and by the Generation of Alternative Solutions subscale of the SPSI in a second (Harrington 1998). Suicide was assessed using medical or health service records (Green 2011; Hazell 2009) or via interviews with parents (Donaldson 2005). In the majority of trials (k = 6), however, it was unclear how suicide was assessed (Harrington 1998; Mehlum 2014; Ougrin 2011a; Rossouw 2012a; Spirito 2002; Wood 2001a).
Excluded studies
A total of 221 articles were excluded from this update: 94 were excluded because not all patients engaged in SH, 63 used a non‐randomised clinical trial design, 28 were reviews, editorials, letters to the editor, or conference proceedings that were not relevant to the treatment of SH in children and adolescents, and 23 were trial protocols. In addition, 11 were excluded as SH could have occurred at any time rather than within six months of randomisation, and one each were excluded either because only data from one trial arm was presented (however, a related publication in which data for both the intervention and control arms were presented was eligible for inclusion), or because the data reported in the article was for a period beyond two years (however, articles reporting data for earlier follow‐up periods for this trial were eligible for inclusion).
Details on the reasons for exclusion of 32 trials clearly related to interventions for suicidality in children and adolescents can be found in the Characteristics of excluded studies section.
Ongoing studies
Five ongoing trials of psychosocial interventions for SH in children and adolescents were identified. In these trials, the effectiveness of the following treatments are being investigated: family therapy (Asarnow 2014; Cottrell 2014; Diamond 2014), a crisis card in conjunction with individualised psychotherapy (Fischer 2013), and combined individual and group sessions of DBT‐A (Linehan 2014). Full details of these studies are provided in the Characteristics of ongoing studies.
Studies awaiting classification
There were no potentially eligible studies which have not been incorporated into the review.
Risk of bias in included studies
Summaries of the overall risk of bias for the included studies are presented in Figure 2 and Figure 3. Risk of bias for each included study is also considered within the text of the review and in the 'Risk of bias' tables.
2.

Risk of bias graph: Review authors' judgements for each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary graph: Review authors' judgements about each risk of bias item for each included study.
Sequence generation
Of the 11 independent trials included in this review, all used random allocation. We rated the majority (k = 9; 81.8%) as having a low risk of bias for this item. Four used a random numbers table to allocate adolescents to the intervention and control groups (Donaldson 2005; Hazell 2009; Spirito 2002; Wood 2001a), three used permuted block randomisation (Mehlum 2014; Ougrin 2011a; Rossouw 2012a), one used a minimisation algorithm (Green 2011), and one used a computerised randomisation sequence (Cooney 2010). We rated one trial as having an unclear risk of bias for this item as although opaque, sealed envelopes were used, it is unclear whether these were shuffled to ensure random sequence generation (Harrington 1998). We rated one trial as having a high risk of bias for this item as an open numbers table was used (Cotgrove 1995).
Allocation concealment (selection bias)
We rated the majority of trials as having a low risk of bias for allocation concealment (k = 8; 72.7%). Allocation was by an offsite researcher in four trials (Green 2011; Hazell 2009; Mehlum 2014; Rossouw 2012a), by a third party researcher working independently of the trial team in one trial (Ougrin 2011a), and by using opaque, sealed envelopes in two further trials (Cooney 2010; Harrington 1998). In one trial, "[t]reatment allocation was concealed from the outcome assessors" (Wood 2001a, p.1247), although details of the method used to conceal allocation were not provided. We rated two trials as having an unclear risk of bias for this item as no details on allocation concealment were provided (Donaldson 2005; Spirito 2002), whilst we rated the remaining trial as having a high risk of bias for this item as an open numbers table was used (Cotgrove 1995).
Blinding (performance bias and detection bias)
We assessed blinding separately for participants, clinical personnel, and outcome assessors.
Blinding of participants
Overall, we classified blinding of participants as resulting in a high risk of bias for the majority of trials included in this review (k = 9; 81.8%), as psychosocial interventions predominated and we contend that it is generally not possible to blind participants to psychosocial therapy. We rated one trial as having a low risk of bias for this item as it was reported that participants were blind to the treatment allocation; however, further details on the method of achieving participant blinding were not reported (Rossouw 2012a). We rated the remaining trial as having an unclear risk of bias for this item as, although no information on participant blinding was provided, both treatments were so similar it remains possible that participants may have been blind to treatment allocation (Donaldson 2005).
Blinding of personnel
Again, we classified blinding of clinical personnel as resulting in a high risk of bias for the majority of trials included in this review (k = 10; 90.9%), as we contend that it is not possible to blind clinicians to the psychosocial therapy they are delivering. We rated one trial, however, as having an unclear risk of bias for this item as, although no information on personnel blinding was reported, the intervention consisted of a one‐off emergency card which could have been given to participants in private (Cotgrove 1995).
Blinding of outcome assessors
As outcome assessors were blind to treatment allocation in eight trials (72.7%), we rated this item as having a low risk of bias for the majority of trials. We rated the remaining three trials, however, as having an unclear risk of bias for this item as no information on blinding of outcome assessors was provided (Cotgrove 1995; Donaldson 2005; Spirito 2002).
Incomplete outcome data (attrition bias)
For four trials, the authors reported having conducted analyses on an intention‐to‐treat basis we therefore classified them as having a low risk of bias for this item (36.4%); although the methods used to conduct these analyses were not clear (Donaldson 2005; Harrington 1998; Mehlum 2014; Wood 2001a). Although the authors of one trial undertook per protocol analyses (Cooney 2010), as there was a 0% drop‐out rate we nevertheless rated it as having a low risk of bias for this item. Two trials used the last observation carried forward method (Hazell 2009; Ougrin 2011a), which we understand may introduce bias (Engles 2003). We therefore rated these trials as having an unclear risk of bias for this item. We also rated three additional trials as having an unclear risk of bias for this item as there were insufficient details to confirm whether intention‐to‐treat or per protocol analyses had been undertaken (Green 2011; Rossouw 2012a; Spirito 2002). We rated one trial as having a high risk of bias for this item as around one‐fifth of the consecutive admissions during this period were not included in the trial and the reasons for excluding these participants were not clearly stated.
Selective reporting (reporting bias)
As we did not have access to trial protocols for the trials included in this review, it is difficult to assess the degree to which selective outcome reporting could have occurred. Consequently, we rated all 11 trials as having an unclear risk of bias for this item.
Other potential sources of bias
We classified most trials as having a low risk of bias for this item as no evidence of other bias was apparent (k = 9; 81.8%). In one trial, however, some participants randomised to the control group mistakenly received the intervention treatment and yet were included in the control group for all subsequent analyses (Cotgrove 1995), whilst in another there was the potential for contamination as therapists delivered both the intervention and control therapy (Donaldson 2005). We therefore classified both of these trials as having a high risk of bias for this item.
The source of funding was not indicated in three trials (Cooney 2010; Cotgrove 1995; Rossouw 2012a). For the remaining trials, funding was received from a variety of sources, including: government (Harrington 1998), health promotion foundations (Wood 2001a), joint university and suicide prevention or health promotion foundations (Donaldson 2005; Green 2011), joint charitable and research foundations (Ougrin 2011a), and a combination of government, university, and health promotion foundations (Mehlum 2014; Spirito 2002). For one, no specific funding was received for the trial (Hazell 2009).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
As only two interventions, DBT‐A and group‐based therapy, were evaluated in more than one independent trial, meta‐analyses were only undertaken for these two interventions. We have reported all other interventions, which were evaluated in only single trials, in the text.
There were no trials of pharmacological agents.
Comparison 1: Individual CBT‐based psychotherapy versus TAU
The effectiveness of brief (i.e., up to 10 sessions) skills‐based psychological therapy (mainly involving training in problem‐solving and affect management) versus supportive relationship therapy, which was designed to be as close as possible to usual care for this population, was assessed in one small study of 12 to 17 year olds presenting to paediatric general or psychiatric facilities following self‐injury in which an intent to die was indicated (N = 39; Donaldson 2005).
Primary outcome
1.1 Repetition of SH
There was no evidence of a significant treatment effect for brief psychological therapy on repetition of SH during the six month follow‐up period (4/21 versus 2/18; OR 1.88, 95% CI 0.30 to 11.73; k = 1; N = 39). The evidence contributing to this outcome was of moderate quality according to the GRADE criteria (Table 1).
Secondary outcomes
1.2 Treatment adherence
There was no evidence of a significant treatment effect on the proportion of participants who completed the full course of treatment (13/21 versus 13/18; OR 0.63, 95% CI 0.16 to 2.43; k = 1; N = 39).
Data on the number of treatment sessions attended was only available for those who completed the three and six month follow‐up assessments. There was no evidence of a significant treatment effect on the number of sessions attended (mean 9.70, SD 2.40, n = 15 versus mean 9.50, SD 1.30, n = 16; MD 0.20, 95% CI ‐1.17 to 1.57; k = 1; N = 31).
1.3 Depression
There was no evidence of a significant treatment effect of brief psychological therapy on depression scores at six months (mean 10.92, SD 15.21, n = 15 versus mean 16.81, SD 15.10, n = 16; MD ‐5.89, 95% CI ‐16.57 to 4.79; k = 1; N = 31) or 12 months (mean 10.33, SD 11.45, n = 15 versus mean 13.89, SD 8.28, n = 15; MD ‐3.56, 95%CI ‐10.71 to 3.59; k = 1; N = 30).
1.4 Hopelessness
There were no data available for this outcome.
1.5 Suicidal ideation
There was also no evidence of a significant treatment effect on suicidal ideation scores at six months (mean 27.08, SD 39.82, n = 15 versus mean 32.19, SD 30.45, n = 15; MD ‐5.11, 95% CI ‐30.48 to 20.26; k = 1; N = 30) or 12 months (mean 24.89, SD 28.52, n = 15 versus mean 33.33, SD 30.42, n = 15; MD ‐8.44, 95% CI ‐29.54 to 12.66; k = 1; N = 30).
1.6 Problem‐solving
Similarly, no clear evidence of a significant treatment effect was found for problem‐solving scores according to either the SPSI or MEPS at the six month follow up assessment (SPSI: mean 126.69, SD 39.92, n = 15 versus mean 108.81, SD 31.00, n = 15; MD 17.88, 95% CI ‐7.70 to 43.46; k = 1; N = 30; MEPS: mean 7.00, SD 4.24, n = 15 versus mean 7.56, SD 3.41, n = 15; MD ‐0.56, 95% CI ‐3.31 to 2.19; k = 1; N = 30). However, by the 12 month assessment there was evidence of a significant treatment effect of psychological therapy according to scores on the SPSI (mean 139.00, SD 31.39, n = 15 versus mean 105.00, SD 29.48, n = 15; MD 34.00, 95% CI 12.21 to 55.79; k = 1; N = 30) but not on the MEPS (mean 9.44, SD 4.72, n = 15 versus mean 9.89, SD 2.47, n = 15; MD ‐0.45, 95% CI ‐3.15 to 2.25; k = 1; N = 30).
1.7 Suicide
No participants died by suicide in either arm during the 12 month follow‐up period.
Comparison 2: interventions for patients with multiple episodes of SH or emerging personality problems versus TAU or other routine management
Dialectical behaviour therapy for adolescents (DBT‐A)
Two trials evaluated the effectiveness of a dialectical behaviour therapy program specially adapted for adolescents, comprising individual, group‐based, and family therapy sessions, in adolescents (between 12 and 19 years) with a history of multiple episodes of SH (Cooney 2010; N = 29; Mehlum 2014; N = 77). The comparator was TAU in Cooney 2010 and enhanced usual care in Mehlum 2014.
Primary outcome
2.1 Repetition of SH
There was no evidence of a significant treatment effect of DBT‐A at the post‐intervention assessment when compared to either TAU or enhanced usual care (Analysis 1.1; k = 2; N = 105). There was also no evidence of a significant difference based on which comparator condition DBT‐A was compared against (i.e., TAU or enhanced usual care; test for subgroup differences: Chi² = 1.70; df = 1; p = 0.19; I² = 41.0%).
1.1. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 1: Repetition of SH post‐intervention
With respect to frequency of SH episodes, there was no evidence of a treatment effect of DBT‐A at the post‐intervention assessment (Analysis 1.2; k = 2; N = 104). Once again, there was no evidence of a significant difference based on the comparator condition (i.e., TAU or enhanced usual care; test for subgroup differences: Chi² = 2.86; df = 1; p = 0.09; I² = 65.1%). The quality of evidence for both outcomes was low (Table 2).
1.2. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 2: Frequency of SH post‐intervention
The study authors of one of these trials measured longitudinal changes in frequency of SH over a 15 week period, based on comparisons of assessments "from baseline to week 9 and from week 10 to week 15," and reported that "[t]he average drop on logarithmic scale in self‐harm frequency in the DBT‐A group (slope ‐1.28, 95% CI ‐1.77 to ‐0.80, P < 0.001) was highly significant, whereas the drop in the [enhanced usual care] group (slope ‐0.36, 95% CI ‐0.99 to 0.26, P = 0.254) was not. The between‐group difference was statistically significant (Δ slope = ‐0.92, 95% CI ‐1.69 to ‐0.15, P = 0.021)" (Mehlum 2014, p.7).
Secondary outcomes
2.2 Treatment adherence
Although adolescents randomised to the DBT‐A treatment group attended a greater number of individual therapy sessions, there was no evidence of a significant treatment effect (Analysis 1.3; k = 2; N = 106). However, there was evidence of a significant treatment effect based on comparator condition (i.e., TAU versus enhanced usual care; Analysis 1.3; test for subgroup differences: Chi² = 30.01; df = 1; P < 0.001; I² = 96%). Compared against TAU, participants randomised to DBT‐A attended a significantly greater number of individual therapy sessions (MD 16.10, 95% CI 12.16 to 20.04; k = 1; N = 29).
1.3. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 3: Number of individual psychotherapy sessions attended
There was no evidence that adolescents randomised to the DBT‐A group attended a significantly greater number of family therapy sessions overall (Analysis 1.4; k = 2; N = 106). Once again, however, there was evidence of a significant difference by comparator condition (Analysis 1.4; test for subgroup differences: Chi² = 16.14; df = 1; P < 0.001; I² 93.8%). Compared against TAU, participants randomised to DBT‐A attended a significantly greater number of family therapy sessions (MD 4.90, 95% CI 2.57 to 7.23; k = 1; N = 29).
1.4. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 4: Number of family therapy sessions attended
Participants in the DBT‐A group in Mehlum 2014 attended significantly more group sessions compared to those in the enhanced usual care group (mean 11.2, SD 5.9, n = 39 versus mean 0.50, SD 2.10, n = 38; MD 10.70, 95% CI 8.73 to 12.67; k = 1; N = 77). As adolescents randomised to TAU in Cooney 2010 were not required to attend group therapy sessions, it was not possible to assess the effectiveness of DBT‐A in this trial with respect to this outcome.
There was no evidence of a significant treatment effect for the number of medication review meetings attended in Cooney 2010 (mean 2.40, SD 2.20, n = 14 versus mean 1.60, SD 2.90, n = 15; MD 0.80, 95% CI ‐1.07 to 2.67; k = 1; N = 29) or for the number of telephone contacts received in Mehlum 2014 (mean 3.30, SD 4.50, n = 39 versus mean 3.50, SD 4.40, n = 38; MD ‐0.20, 95% CI ‐2.19 to 1.79; k = 1; N = 77).
2.3 Depression
No data on depression scores were reported in Cooney 2010.
In Mehlum 2014, depression was measured in two ways: as scores on the depression sub‐scale of the MFQ and as total scores on the MADRS. There was no clear evidence of a difference in treatment effect for DBT‐A according to either measure at the post‐treatment assessment (MFQ: Analysis 1.6; MD ‐2.39, 95% CI ‐5.02 to 0.24; k = 1; N = 77; MADRS: mean 12.29, SD 7.52, n = 39 versus mean 15.76, SD 8.14, n = 38; MD ‐3.47, 95% CI ‐6.97 to 0.03; k = 1; N = 77).
1.6. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 6: Depression scores post‐intervention
The authors of this trial also analysed longitudinal changes in depression scores, based on the assessments at baseline and at nine, 15, and 19 weeks. They reported that whilst "[b]oth patient groups displayed a significant reduction in self‐reported symptoms of depression...only the DBT‐A group showed a significant reduction in interviewer‐rated depression..." (Mehlum 2014, p.7).
2.4 Hopelessness
There was no evidence of a treatment effect of DBT‐A on hopelessness at the post‐intervention assessment (Analysis 1.7; k = 2; N = 101). There was, however, evidence of a significant difference by comparator condition (i.e., TAU versus enhanced usual care; Analysis 1.7; test for subgroup differences: Chi² = 5.13; df = 1; p = 0.02; I² = 80.5%). When compared to enhanced usual care, DBT‐A was associated with a significant improvement in hopelessness scores at the post‐intervention assessment (SMD ‐0.47, 95% CI ‐0.93 to ‐0.02; k = 1; N = 77).
1.7. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 7: Hopelessness scores post‐intervention
2.5 Suicidal ideation
There was evidence of an overall benefit of DBT‐A on suicidal ideation at the post‐intervention assessment (Analysis 1.8; SMD ‐0.62, 95% CI ‐1.07 to ‐0.16; k = 2; N = 100), but with no evidence of a significant difference by comparator condition (i.e., TAU versus enhanced usual care; Analysis 1.8; test for subgroup differences: Chi² = 1.15; df = 1; p = 0.28; I² = 13.3%).
1.8. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 8: Suicidal ideation scores post‐intervention
2.6 Problem‐solving
There were no data available for this outcome.
2.7 Suicide
Data obtained by correspondence with study authors indicated that there were no suicides in either group during the treatment period or over the 12 month follow‐up period. Correspondence with study authors for Mehlum 2014 further indicated that although information on outcomes over a 24 month follow‐up period are still being collected, of those participants followed until the date of correspondance, none had died by suicide.
Mentalisation
One study investigated the effectiveness of mentalisation‐based therapy in 12 to 17 year olds diagnosed with comorbid depression presenting to emergency departments or community psychiatric services following an episode of self‐injury or self‐poisoning, irrespective of whether suicidal intent was present (Rossouw 2012a; N = 80).
Primary outcome
2.8 Repetition of SH
At the 12 month (post‐intervention) assessment, significantly fewer adolescents scored above the cut‐point on the Risk‐Taking and Self‐Harm Inventory (RTSHI), indicating that they had engaged in fewer episodes of SH behaviour based on information recorded over the preceding three months (Analysis 1.1; OR 0.26, 95% CI 0.09 to 0.78; k = 1; N = 71). The quality of evidence was moderate (Table 2).
The study authors also measured longitudinal changes in scores on the RTSHI and found that although "[b]oth groups showed significant reductions in self‐harm...following both a linear and a quadratic pattern. The interaction term for group x time was also significant...indicating that the linear decrease in RTSHI was significantly greater for the [mentalisation‐based therapy for adolescents] group" (Rossouw 2012a, p.1308).
Secondary outcomes
2.9 Treatment adherence
There was no evidence of a significant treatment effect in terms of the number of adolescents in each group who completed all 12 months of treatment (Analysis 1.5).
1.5. Analysis.

Comparison 1: Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management, Outcome 5: Number completing full course of treatment
2.10 Depression
Adolescents in the intervention group had significantly lower scores on the depression sub‐scale of the MFQ at the 12 month (post‐intervention) assessment (Analysis 1.6; MD ‐2.28, 95% CI ‐2.81 to ‐1.75; k = 1; N = 80).
Depression was also measured dichotomously as the proportion of participants scoring above the cut‐point on the depression sub‐scale of the MFQ. Although fewer adolescents in the intervention group scored above the cut‐point for depression, there was no evidence of a significant treatment effect at the 12 month (post‐intervention) assessment (19/39 versus 25/37; OR 0.46, 95% CI 0.18 to 1.16; k = 1; N = 76).
Changes in depression scores were also measured longitudinally in the original report of this trial. The study authors found that "[t]he level of self‐rated depression decreased for participants in both groups...The linear rate of decrease was somewhat greater for the MBT‐A group (P < 0.04) and the model yielded a significant difference at 12 months" (Rossouw 2012a, p.1308).
2.11 Hopelessness
There were no data available for this outcome.
2.12 Suicidal ideation
There were no data available for this outcome.
2.13 Problem‐solving
There were no data available for this outcome.
2.14 Suicide
Correspondence with study authors confirmed that no participant died by suicide during the 12 month follow‐up period.
Comparison 3: group‐based psychotherapy versus TAU
The effectiveness of group therapy was assessed in three studies of 12 to 17 year olds referred to child and adolescent services following an episode of intentional self‐injury or self‐poisoning, irrespective of intent, over a follow‐up period of seven months (Wood 2001a; N = 63) or 12 months (Green 2011 N = 366; Hazell 2009 N = 68).
Given that Hazell 2009 and Green 2011 were based in a large part on Wood 2001a, employed the same treatment manual (Wood 2001b), and involved the authors of the earlier trial in the design of the therapeutic intervention, we grouped these trials within a single analysis. In all three trials, the content of group therapy involved a variety of techniques, including CBT, PST, DBT, and group psychodynamic psychotherapy. Therapy consisted of six weekly acute group sessions, followed by weekly or bi‐weekly group therapy sessions continuing until the adolescent felt ready to leave the service.
Primary outcome
3.1 Repetition of SH
There was no clear evidence of a difference in treatment effect of group therapy on repetition of SH during either the six month (Analysis 2.1; k = 2; N = 430) or 12 month (Analysis 2.2; k = 3; N = 490) intervals after entry to treatment. A low quality of evidence was found for both analyses (Table 3). Additionally, both of these analyses were associated with considerable heterogeneity (I2 = 65% and 77%, respectively) with, at six months, evidence of a significant adverse effect apparent in Hazell 2009. While we were unable to undertake formal investigation into the source of heterogeneity, it should be noted that in Wood 2001a, the definition of repetition of SH was based on there being two or more further episodes whilst in Hazell 2009 and Green 2011, repetition was based on there being any further episodes of SH. Also, Wood 2001a and Hazell 2009 were relatively small such that chance findings may be more likely.
2.1. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 1: Repetition of SH at six months
2.2. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 2: Repetition of SH at 12 months
Secondary outcomes
3.2 Treatment adherence
There were no data available for this outcome.
3.3 Depression
There was no clear evidence of a difference in treatment effect for depression at either the six month (Analysis 2.3; k = 2; N = 420) or 12 month (Analysis 2.4; k = 3; N = 473) assessments.
2.3. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 3: Depression scores at six months
2.4. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 4: Depression scores at 12 months
3.4 Hopelessness
There were no data available for this outcome.
3.5 Suicidal ideation
There was also no clear evidence of a difference in treatment effect for suicidal ideation at either the six month (Analysis 2.5; k = 2; N = 421) or 12 month (Analysis 2.6; k = 3; N = 471) assessments.
2.5. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 5: Suicidal ideation scores at six months
2.6. Analysis.

Comparison 2: Group‐based psychotherapy vs. Treatment as usual or other routine management, Outcome 6: Suicidal ideation scores at 12 months
3.6 Problem‐solving
There were no data available for this outcome.
3.7 Suicide
There were no suicides in either group in any of the three studies.
Comparison 4: therapeutic assessment versus TAU (standard assessment)
One cluster randomised controlled trial examined the effectiveness of therapeutic assessment for the treatment of SH in adolescent patients in terms of repetition of SH in a sample of 12 to 18 year olds referred for a psychological assessment following an episode of self‐injury or self‐poisoning irrespective of intent at both 12 months (Ougrin 2011a, ISRCTN 81605131, N = 70) and 24 months following entry to the study (Ougrin 2013, ISRCTN 81605131; N = 70).
As the study authors were unable to provide us with the values of the either the inter‐cluster correlation coefficient or the design effect that would enable us to statistically account for the effects of clustering (as per the guidance in Higgins 2011), results presented in this section may overestimate the effectiveness of this intervention.
Primary outcome
4.1 Repetition of SH
There was no evidence for a difference in treatment effect following an episode of SH during either the 12 month (4/35 versus 5/34; OR 0.75, 95% CI 0.18 to 3.06; k = 1; N = 69) or 24 month (7/35 versus 9/34; OR 0.69, 95% CI 0.23 to 2.14; k = 1; N = 69) follow‐up periods. Quality of evidence was very low for both time points (Table 4).
Secondary outcomes
4.2 Treatment adherence
Adolescents in the therapeutic assessment group were significantly more likely to attend their first appointment (29/35 versus 17/35; OR 5.12, 95% CI 1.70 to 15.39; k = 1; N = 70).
4.3 Depression
There were no data available for this outcome.
4.4 Hopelessness
There were no data available for this outcome.
4.5 Suicidal ideation
There were no data available for this outcome.
4.6 Problem‐solving
There were no data available for this outcome.
4.7 Suicide
Correspondence with study authors confirmed that no participants died by suicide in either the intervention or control arms during follow‐up.
Comparison 5: compliance enhancement plus TAU (standard disposition) versus TAU
One study investigated the effectiveness of standard disposition (i.e., aftercare) planning with and without an added compliance enhancement intervention over a three month follow‐up period in a sample of 12 to 19 year olds admitted to the emergency department of a general hospital following an episode of self‐injury irrespective of intent (Spirito 2002 N = 76).
Primary outcome
5.1 Repetition of SH
There was no clear evidence of a difference in treatment effect for repetition of SH by the six month follow‐up assessment (3/29 versus 5/34; OR 0.67, 95% CI 0.15 to 3.08; k = 1; N = 63). Patients in the compliance enhancement group did, however, "engage in fewer repeat SH episodes" compared to participants in the control group (mean 0.10 versus 0.15; Spirito 2002), although no more details were available to allow formal testing of this. The quality of evidence for this outcome was very low (Table 5).
Secondary outcomes
5.2 Treatment adherence
No clear evidence of a difference was found between the experimental and control groups in relation to the number of participants attending at least one treatment session (27/29 versus 31/34; OR 1.31, 95% CI 0.20 to 8.41; k = 1; N = 63), the average number of sessions attended (mean 7.70, SD 5.80, n = 29 versus mean 6.40, SD 4.40, n = 34; MD 1.30, 95% CI ‐1.28 to 3.88; k = 1; N = 63), and completion of the full course of treatment (17/29 versus 16/34; OR 1.59, 95% CI 0.59 to 4.33; k = 1; N = 63).
5.3 Depression
There were no data available for this outcome.
5.4 Hopelessness
There were no data available for this outcome.
5.5 Suicidal ideation
There were no data available for this outcome.
5.6 Problem‐solving
There were no data available for this outcome.
5.7 Suicide
No participants died by suicide in either arm.
Comparison 6: home‐based family intervention versus TAU
The effectiveness of a home‐based family intervention was compared with treatment as usual over a six month follow‐up period in one study in a sample of adolescents aged 16 years or younger referred to child and adolescent mental health services following an episode of self‐poisoning irrespective of intent (Harrington 1998; N = 162).
Primary outcome
6.1 Repetition of SH
There was no evidence of a difference in treatment effect at the six month assessment on the proportion of participants repeating SH (11/74 versus 11/75; OR 1.02, 95% CI 0.41 to 2.51; k = 1; N = 149). The quality of evidence for this outcome was low (Table 6).
Secondary outcomes
6.2 Treatment adherence
Although more participants in the home‐based group completed the full course of treatment, there was no clear evidence of a difference in treatment effect between the two groups (39/84 versus 28/77; OR 1.52, 95% CI 0.81 to 2.85; k = 1; N = 161).
6.3 Depression
There were no data available for this outcome.
6.4 Hopelessness
There was no evidence of a difference in treatment effect on hopelessness at the six month assessment (mean 4.40, SD 3.30, n = 74 versus mean 4.20, SD 3.60, n = 74; MD 0.20, 95% CI ‐0.91 to 1.31; k = 1; N = 148).
6.5 Suicidal ideation
There was also no evidence of a difference in treatment effect on suicidal ideation at the six month assessment (mean 23.60, SD 40.00, n = 74 versus mean 28.70, SD 36.30, n = 75; MD ‐5.10, 95% CI ‐17.37 to 7.17; k = 1; N = 149).
6.6 Problem‐solving
There was also no evidence of a difference in treatment effect on problem‐solving at the six month assessment (mean 17.60, SD 7.40, n = 73 versus mean 17.90, SD 7.30, n = 74; MD ‐0.30, 95% CI ‐2.68 to 2.08; k = 1; N = 149).
6.7 Suicide
There was no evidence of a difference in treatment effect for suicide. One patient in the experimental treatment group died by suicide; none died by suicide in the control group. As the denominator for intervention and control groups for this outcome are not known, however, we could not calculate ORs.
Comparison 7: remote contact interventions versus TAU
Emergency cards
One study investigated the effectiveness of an emergency card enabling adolescents aged 16 years or younger who were admitted to hospital following an episode of self‐injury or self‐poisoning to re‐admit themselves to a paediatric ward in the local hospital on demand if they felt suicidal over a 12 month follow‐up period (Cotgrove 1995 N = 105). The control group participants in this trial received treatment as usual, as did the experimental group (in conjunction with the emergency card).
Primary outcome
7.1 Repetition of SH
There was no clear evidence of a difference in treatment effect of emergency cards on repetition of SH by the 12 month assessment (3/47 versus 7/58; OR 0.50, 95% CI 0.12 to 2.04; k = 1; N = 105). The quality of evidence for this outcome was very low (Table 7).
Secondary outcomes
7.2 Treatment adherence
There were no data available for this outcome.
7.3 Depression
There were no data available for this outcome.
7.4 Hopelessness
There were no data available for this outcome.
7.5 Suicidal ideation
There were no data available for this outcome.
7.6 Problem‐solving
There were no data available for this outcome.
7.7 Suicide
There were no data available for this outcome.
Discussion
This systematic review is an update of previous versions of a Cochrane review (Hawton 1998; Hawton 1999). It also adds to raw data we provided to the UK's National Institute for Clinical Excellence in 2010 to contribute to its guidance on the longer‐term management of self‐harm (NICE 2011). Whilst those versions included psychosocial and pharmacological interventions for adults as well as children and adolescents who engage in SH, this update is solely focused on interventions for children and adolescents. Previously we commented on the small number of trials that have focused on interventions for this population. Although for this update we identified five additional trials, it is still surprising that there have been so few trials in this population, especially given the size of the problem of SH in young people in many countries and the known association between SH and suicide.
In our previous review we commented on the fact that the majority of trials included either solely patients who had taken overdoses, or samples in which the majority had. However, there are other important patient subgroups, especially those who cut themselves. None of the trials included in this review specifically focused on these patients. However, such patients were included in many of the trials, especially those where a large proportion (or all) of the participants had a history of multiple episodes of SH at trial entry (e.g., Green 2011; Hazell 2009; Mehlum 2014; Rossouw 2012a; Wood 2001a). It should be noted that individuals who repeat SH may change from one method of SH to another method in subsequent episodes (Lilley 2008).
None of the included trials evaluated the effectiveness of pharmacological agents in this patient group. Additionally, only one included information on adverse effects of the intervention therapies other than those relating to further suicidal behaviour (Hazell 2009).
We have used the intention‐to‐treat method where data allowed. This was usually possible when examining the outcomes of repetition of SH and suicide. Where outcomes relied on patient interview, this was generally not possible and we have instead used all available case data.
Summary of main results
Individual CBT‐based psychotherapy
In a single trial of brief psychological therapy consisting of problem‐solving and affect management training skills compared with supportive relationship therapy (Donaldson 2005), no beneficial effects of the psychological therapy were found in terms of repetition of SH, treatment adherence, depression, and suicidal ideation. There was evidence of improved problem‐solving on one measure at 12 months but not on a second measure.
Interventions for patients with multiple episodes of SH or emerging personality disorder
There was no apparent benefit for DBT‐A, compared with either TAU (Cooney 2010) or enhanced usual care (Mehlum 2014), using cross‐sectional analyses of the proportion of participants repeating SH (Cooney 2010) or the numbers of SH episodes per patient by the end of the therapy period (Cooney 2010; Mehlum 2014). However, in Mehlum 2014, the authors analysed the longitudinal slope of decline in mean number of SH episodes per participant based on information reported at the baseline, nine week, and 15 week assessments, and reported a significant benefit for DBT‐A. It is difficult to rationalise these two sets of results. The results of our analyses suggest that any differences between the groups following treatment were not marked.
There was no apparent treatment effect in the second trial on depression using data from both the Self‐report Mood and Feelings Questionnaire (SMFQ) and the Montgomery‐Åsberg Depression Rating Scale (MADRS) based on analyses of the post‐intervention scores. However, again when the authors of the Mehlum 2014 trial used a longitudinal analysis based on scores from the SMFQ, it suggested significant positive benefits of DBT‐A on depression. Again, the difference between the result of this analysis and ours based on post‐treatment results would suggest that any treatment effect was not marked. Our analyses showed significant benefits of DBT‐A for both hopelessness and suicidal ideation at the 19 week (post‐intervention) assessment in Mehlum 2014 but not at the post‐intervention assessment in Cooney 2010. There is therefore some evidence of beneficial effects for DBT‐A, although the evidence regarding repetition of SH and depression must currently be regarded as equivocal.
In a single trial of mentalisation‐based therapy, there was a significant effect on repetition of SH in favour of mentalisation at the post‐intervention assessment (Rossouw 2012a). However, this was based on fewer adolescents scoring above the cut‐point on the Risk Taking and Self‐Harm Inventory (RTSHI) and it is unclear how this scale may relate to actual SH behaviour.
There was no apparent beneficial effect of mentalisation on depression as measured by the Mood and Feelings Questionnaire at the post‐intervention assessment. However, it is worth noting that considerably fewer adolescents in the mentalisation group scored above the cut‐point for depression at the 12‐month assessment, although the study was relatively underpowered for this outcome criterion (n = 40 per treatment arm). Changes in depression scores were also measured longitudinally in the original report of this trial. The study authors found that "[t]he level of self‐rated depression decreased for participants in both groups...The linear rate of decrease was somewhat greater for the MBT‐A group (P < 0.04) and the model yielded a significant difference at 12 months" (Rossouw 2012a, p.1308). These results suggest there might be benefits for mentalisation over usual care, but this treatment approach requires evaluation in further trials before a stronger conclusion can be reached.
Group‐based therapy
Three trials investigated group‐based therapy in adolescents with a history of multiple SH episodes (Green 2011; Hazell 2009; Wood 2001a). There was no overall evidence of apparent benefit of group psychotherapy on repetition of SH. However, considerable heterogeneity was associated with the results of the earlier two studies (Hazell 2009; Wood 2001a), whilst the results of the third much larger trial indicated no superiority of group‐based therapy compared with treatment as usual (Green 2011).
Therapeutic assessment
Given the known poor treatment adherence of adolescents who engage in SH (Granboulan 2001; Taylor 1984), efforts have been made to increase adherence through therapeutic assessment following SH. In a single trial a therapeutic assessment approach appeared to considerably increase treatment adherence in terms of the number of participants who attended the first treatment session as compared to treatment as usual (Ougrin 2011a). There were, however, no apparent beneficial effects in terms of repetition of SH at 12 or 24 months. These results are based on a single cluster randomised trial, which may overestimate the effectiveness of this intervention.
Compliance enhancement
In a single small trial, compliance enhancement did not result in improved outcomes compared with standard treatment in terms of treatment adherence or repetition of SH (Spirito 2002). However, the trial was probably underpowered to evaluate these outcomes. The findings of this study are at odds with that of therapeutic assessment (Ougrin 2011a), which also focused on enhancing treatment adherence. However, the latter trial appeared to involve a more intensive and pro‐active therapeutic approach as part of the assessment.
Home‐based family intervention
A home‐based family intervention did not appear to produce a better outcome than standard treatment in terms of repetition of SH, suicidal ideation, problem solving, and hopelessness. However, Harrington 1998 did report that parents were more satisfied with the home‐based family intervention at initial follow‐up.
Remote contact interventions
In a single study to assess the effects of provision of an emergency card allowing patients to re‐admit themselves to hospital (Cotgrove 1995), there was no difference in repetition of SH between the intervention and control groups. However, the study appeared to be underpowered to properly test this outcome. Few adolescents made use of the emergency card, but none of those who did repeated SH.
Overall completeness and applicability of evidence
Completeness of evidence
There have been relatively few trials of interventions for adolescent SH patients (we identified just 11), especially compared with the numbers of trials of psychosocial treatments for adults. Therefore our conclusions are limited to a small range of interventions and outcomes. Additionally, as there were no eligible trials of pharmacological interventions, perhaps due to concerns about safety in this clinical population, our findings are limited to psychosocial interventions.
A range of interventions have been investigated, including modifications of existing assessment procedures and attempts to increase participant adherence, as well as specific aftercare interventions. Mostly, however, these evaluations have been limited to single trials. Three trials focused on group‐based psychotherapy, which is perhaps unsurprising given the initial optimism associated with the publication of the first trial of group‐based therapy in 2001 (Wood 2001a). There were two trials of DBT‐A; all other interventions, including brief psychological therapy and mentalisation, were evaluated only in single trials.
In the previous versions of this review we only focused on a single clinical outcome, namely repetition of SH and suicide. In this update we have considerably expanded the range of clinically relevant outcomes that have been examined to include treatment adherence, depression, hopelessness, suicidal ideation, and problem‐solving where available. We have also reported on the frequency of SH where these data were available. However, limited data were available on secondary outcomes. Only four trials included information on depression, five on suicidal ideation, three on hopelessness and two on problem‐solving. Information on suicide had to be requested from study authors for all 11 trials.
Applicability of evidence
The participants in the included trials appear to have been reasonably representative of adolescents who present to hospital following SH, including a greater proportion of female participants in all trials that recorded information on gender. Four trials focused specifically on individuals with a history of multiple episodes of SH, which is a particular concern in this clinical population given its association with subsequent repetition (Hawton 2012c). In two further trials around one‐half of participants had a history of multiple episodes of SH.
It should be noted that this review is focused exclusively on children and adolescents who have engaged in SH. As a result, we have excluded patients with conditions such as emergent borderline personality disorder who have not engaged in SH, and mixed trials of patients with either SH or suicidal ideation in the absence of suicidal behaviour.
Quality of the evidence
The trials included in this review were, in general, relatively small to detect significant differences in proportions of patients who engaged in a repeat episode of SH. Additionally, quality of evidence, as assessed using the GRADE approach, was, in general, low suggesting that further research is likely to have an important impact on our confidence in the estimate of treatment effectiveness, and may, in fact, change the estimate. This is particularly likely to affect results on those interventions that have so far only been assessed in single trials. However, it should be noted that because of the virtual impossibility of blinding participants and clinical personnel to treatment condition in psychosocial intervention trials such, studies are always likely to receive relatively low quality ratings.
Limitations in design and implementation
All trials included in this review possessed high risk of bias in relation to at least one aspect of trial design, with weaknesses most commonly observed with respect to blinding of both participants and clinical personnel. In part this may be due to the fact that psychological interventions predominated in this review and we believe it is generally not possible to blind participants or clinical personnel to psychological therapy. Such trials are therefore always likely to receive relatively low ratings. Nevertheless, performance and detection bias cannot be ruled out.
Indirectness of evidence
Repetition of SH was measured using self‐reported information, medical records, or representation to hospital in all trials included in this review. Secondary outcomes were assessed using widely validated psychometric measures (such as MFQ, SIQ) that were not subjected to modification in scoring.
Unexplained heterogeneity of inconsistency of results
Meta‐analysis was only undertaken for two interventions: DBT‐A and group‐based therapy. Considerable heterogeneity was, however, found for the three trials included in the latter analyses, particularly with respect to the primary outcome of repetition of SH (I2= 65% for repetition at six months and I2= 77% for repetition of SH at 12 months). I2 values for all other secondary outcome measures equalled zero. It is possible that differences in available services, and hence in treatment as usual more broadly, might be one explanation for this heterogeneity. Another might be that a different definition of repetition was used in the first trial (Wood 2001a), namely two or more further SH episodes. However, it may also be that group‐based therapy does not adequately address the psychological needs of young people who have a history of multiple SH episodes (Townsend 2014) or, possibly, treatment of adolescent repeaters of SH in a group may carry risks of encouraging repetition through contagious influences (Hawton 2012a).
Imprecision of results
Results of the individual trials included in this review were associated with a high level of imprecision as indicated by the wide confidence intervals around the effect size estimates.
Probability of publication bias
Presence of publication bias could not be formally evaluated in this review as no meta‐analysis included ten or more trials. However, it is notable that one trial was not published in full in a peer‐reviewed journal (Cooney 2010).
Potential biases in the review process
We have no reason to believe we have not identified all relevant trials of interventions for SH in children and adolescents. By using the random‐effects model in all analyses, our results possess greater generalisability than if we had used the fixed‐effect model (Erez 1996). However, because our review criteria included only studies of patients who had all engaged in SH and presented to child and adolescent clinical services in the preceding six months, we excluded trials where only some of the patients had engaged in SH. Thus, for example, trials of adolescents with suicidal ideation were excluded. Positive results of some trials which have included such participants suggest a possible preventive role of more intensive forms of psychotherapy, including, for example, multisystemic therapies in adolescents who SH (e.g., Huey 2004). However, such an assumption requires further evaluative research, especially given the recognised differences between adolescents who have ideas of SH and those that actually engage in SH (O'Connor 2012). We also excluded studies where SH was an outcome in studies of general interventions for patients with psychiatric disorders. Data on repetition of SH were available for all the included trials and information on suicides was available for all but one trial (although there was only one such event recorded).
We only included trials in which adolescents engaged in SH and presented to clinical services. For those who do not present to services possible therapeutic approaches include online/bibliotherapy interventions, or screening adolescents to identify those at risk.
We categorised the interventions in this review based on consensus discussions among the review team who have considerable experience in both research and clinical practice related to SH. We believe this approach is more informative and far less misleading than where reviewers have combined disparate therapies in an attempt to evaluate whether psychosocial therapy in general might be effective, irrespective of the specific content of the interventions, which provides little useful information for clinicians. Nevertheless, we have combined interventions only where the therapeutic model is similar between trials. For this reason, meta‐analysis was undertaken for only two interventions (i.e., DBT‐A and group‐based psychotherapy). Both trials of DBT‐A, Cooney 2010 and Mehlum 2014, refer to the original manualised adaption of DBT for adolescents (Miller 2007). We therefore believe that these two trials are based on the same therapeutic model and are sufficiently similar to justify pooling within meta‐analysis. The latter two replications of group‐based psychotherapy, Green 2011 and Hazell 2009, refer to the original trial of this therapy (Wood 2001a); all three trials were based on the same therapeutic model and all recruited adolescents with a history of multiple episodes of SH. We therefore believe that these three trials are also sufficiently similar to justify pooling within a second meta‐analysis.
Agreements and disagreements with other studies or reviews
We identified 11 reviws of interventions for children and adolescents following SH. Ten were systematic reviews (Brausch 2012; Daniel 2009; Gonzales 2013; Gould 2003; Newton 2010; Nock 2007; Ougrin 2011b; Ougrin 2012; Ougrin 2015; Robinson 2011), and one was a narrative review (Brent 2013). All reviews included both randomised and non‐randomised trials and some also included findings relating to adults who had self‐harmed. Only two included meta‐analyses (Ougrin 2011b; Ougrin 2015). However, these pooled very disparate treatment approaches with likely differing therapeutic mechanisms of action and patients with different characteristics (especially in terms of frequency of prior repetition of SH).
A number of these reviews focused specifically on engagement with treatment, although no one intervention was found to be significantly better than treatment as usual for engaging adolescents in subsequent treatment (Ougrin 2011b; but see Ougrin 2011a in the present review). With respect to repetition of SH, several reviews suggest that DBT‐A (Brausch 2012; Gonzales 2013; Gould 2003; Nock 2007), hospital‐based interventions (Brent 2013), transitional interventions (Newton 2010), or those with a brief cognitive behavioural or problem‐solving orientation (Daniel 2009; Robinson 2011), may show promise for the treatment of suicidal behaviour in adolescents. However, these recommendations are typically based on data from non‐randomised trials, or from trials in adults.
Group‐based therapy was also identified as a potentially useful treatment in one review (Gonzales 2013), on the basis of data from one RCT in adolescents (Green 2011). However, we found no evidence of a significant treatment effect for this trial, including in terms of reduced repetition of SH, at either six or 12 months follow‐up (we also found no evidence of a significant treatment effect for all other outcomes in this trial). Multisystemic therapy was also found to be effective in one review for reducing suicide attempts in adolescents experiencing a variety of psychiatric crises, but not in those with a history of SH specifically (Ougrin 2012).
For the trial by Mehlum 2014, Ougrin 2015 reported data on the proportions of participants who repeated SH, irrespective of whether this resulted in hospital presentation (the only data available for the present review) or not. This apparently showed a significant difference, with fewer participants in the DBT‐A group repeating SH than in the control group. However, correspondence with the study author indicated that these data have not been released. The only relevant data were presented in an interim analysis on an initial sample of participants, not the full study population. We were unable to obtain the final study data for this outcome.
The lack of evidence for the effectiveness of pharmacological interventions for SH in adolescents is also highlighted in several of these reviews. However, as noted in the How the intervention might work section, concerns about safety of drug therapy in young people may partly explain this.
Authors' conclusions
Implications for practice.
There have been relatively few investigations into interventions for children and adolescents who engage in SH. Thus there is not much evidence on which to draw conclusions on effects of interventions for SH in this population. While there were some very limited positive findings regarding DBT‐A, mentalisation, and therapeutic assessment, these approaches require further evaluation before any definitive conclusions about their use in clinical practice can be made. Results of this review would suggest that a comprehensive therapeutic assessment may increase engagement with subsequent treatment. Although this finding is based on a single cluster randomised trial which may overestimate the effectiveness of the intervention, this result suggests that a comprehensive therapeutic assessment might be a useful part of a clinical intervention.
However, on the strength of the evidence from three trials, including one recent larger trial, there is little support for group‐based therapy for adolescents with a history of multiple episodes of SH. Additionally, it is notable that the authors of one of these trials reports an incident in which one participant posted confidential information about another participant on an online blog (Hazell 2009), highlighting the potential risks associated with group‐based therapy in this clinical population.
Implications for research.
While there were no very strong positive findings from the review, some of the results regarding therapeutic assessment, mentalisation, and DBT‐A suggests that these approaches warrant further evaluation.
Given the evidence for its benefit in adults who engage in SH (NICE 2011), individual CBT‐based psychotherapy needs to be further developed and evaluated in children and adolescents. The development of this type of treatment could benefit from being based on detailed investigation of the psychological factors contributing to SH in children and adolescents, including factors that might enhance resilience and thereby reduce the risk of further SH, as well as having benefits for other outcomes. Ideally, the development of new treatments should ensure their feasibility and suitability for the young people for whom they are designed (Craig 2008); children and adolescents with experience of SH and their carers should be involved in this process. Heed should also be paid to the principles of development and evaluation of treatments as laid out in the UK Medical Research Council guidance regarding complex interventions.
In trials of interventions for children and adolescents who engage in SH, investigations of treatment could focus on subgroups of adolescents, including those with a history of multiple episodes of SH and those with a single or only few episodes, those with clearly identified psychiatric disorders, especially depression, and those with emergent borderline personality disorder. Specific treatments for self‐cutting and other forms of self‐mutilation, which are common in adolescents, also merit development and evaluation.
In several trials in this review, especially the more recent trials, a relatively broad range of outcome measures have been investigated. This is to be encouraged in future trials. Any trial of an intervention for SH in children and adolescents should include a range of outcome measures; not just SH and suicide, but also adherence, mood, and attitudes towards treatment, as this may help to identify contributors to any apparent benefits or lack of impact. Investigation of the mechanisms through which treatments might work is also desirable to assist with the identification of clinically relevant sub‐groups of patients who may benefit from certain more intensive forms of intervention. It is also important that any adverse effects of treatment, such as the release of confidential information described in the Hazell 2009 trial, are carefully evaluated. It is essential that future trials in this patient population are adequately powered to detect differences in key clinical outcomes, especially repetition of SH.
The interventions we found to warrant further investigation given some positive findings regarding frequency of repetition of SH ‐ mentalisation and DBT‐A ‐ both involve a core component of intensive, relatively prolonged, one‐on‐one therapy suggesting that where novel therapies for this population are considered, those involving extended contact may be particularly valuable.
It is essential that future trials in this patient population are adequately powered to detect differences in key clinical outcomes, especially repetition of SH.
What's new
| Date | Event | Description |
|---|---|---|
| 14 September 2021 | Amended | There is a more recent Cochrane review on this topic: https://doi.org/10.1002/14651858.CD013667.pub2 An editorial note has been added to redirect readers. |
History
Review first published: Issue 12, 2015
| Date | Event | Description |
|---|---|---|
| 5 January 2016 | Amended | Minor edit to title of analysis 1. |
Notes
Acknowledgements
We thank Emily Cooney, Andrew Cotgrove, Jonathon Green, Philip Hazell, Lars Mehlum, Dennis Ougrin, Trudie Rossouw, and Anthony Spirito for providing us with unpublished data.
We also thank Andrea Cipriani, Jane Dennis, Jessica Sharp, and Catriona Shatford for advice on data extraction and management issues.
This project has previously been supported by the National Co‐ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO). KH is funded by Oxford Health NHS Foundation Trust. He is a National Institute for Health Research (NIHR) Senior Investigator and personal funding from NIHR helped support this update. The opinions expressed are solely those of the authors.
Appendices
Appendix 1. CCDANCTR Search Strategy
Search Strategy 1956 to 2015:
CCDANCTR
Date range searched: 01.01.56 to 30.01.15. #1. ((deliberat* or self*) NEXT (destruct* or harm* or injur* or mutilat* or poison*)):ab,ti,kw,ky,emt,mh,mc #2. DSH:ab #3. (parasuicid* or “para suicid*”) #4. (suicid* NEAR2 (attempt* or episod* or frequen* or future or histor* or multiple or previous* or recur* or repeat* or repetition)):ab,ti,kw,ky,emt,mh,mc #5. “post suicid*” #6. (suicid* and (BPD or “borderline personality disorder”)) #7. (overdos* or “over dos*”) #8. ((crisis or suicid*) NEAR (emergenc* or hospital or outpatient or “repeat* attend*” or “frequent* attend*” )):ab,ti,kw,ky,emt,mh,mc #9. (#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8) Notes: ab: abstract; ti: title; kw: keywords; ky: additional keywords; emt: EMTREE headings; mh: MeSH headings; mc: MeSH checkwords.
Appendix 2. EMBASE, MEDLINE, PreMEDLINE, PsycINFO and CENTRAL Search Strategies
Search Strategy 1998 to 2013:
EMBASE, MEDLINE, PreMEDLINE, PsycINFO (OVID SP interface)
Date range searched: 01.01.1998 to 13.10.2013. 1. automutilation/ or drug overdose/ or exp suicidal behavior/ 2. 1 use emez 3. overdose/ or self‐injurious behavior/ or self mutilation/ or suicide/ or suicidal ideation/ or suicide, attempted/ 4. 3 use mesz, prem 5. drug overdoses/ or self destructive behavior/ or exp self injurious behavior/ or attempted suicide/ or suicidal ideation/ or suicide/ or suicide prevention/ or suicide prevention centers/ or suicidology/ 6. 5 use psyh 7. (auto mutilat$ or automutilat$ or cutt$ or head bang$ or head bang$ or overdos$ or (self adj2 cut$) or self destruct$ or selfdestruct$ or self harm$ or selfharm$ or self immolat$ or selfimmolat$ or self inflict$ or selfinflict$ or self injur$ or selfinjur$ or selfmutilat$ or self mutilat$ or self poison$ or selfpoison$ or suicid$).ti,ab. 8. or/2,4,6‐7 9. exp "clinical trial (topic)"/ or exp clinical trial/ or crossover procedure/ or double blind procedure/ or placebo/ or randomization/ or random sample/ or single blind procedure/ 10. 9 use emez 11. exp clinical trial/ or exp "clinical trials as topic"/ or cross‐over studies/ or double‐blind method/ or placebos/ or random allocation/ or single‐blind method/ 12. 11 use mesz, prem 13. (clinical trials or placebo or random sampling).sh,id. 14. 13 use psyh 15. (clinical adj2 trial$).ti,ab. 16. (crossover or cross over).ti,ab. 17. (((single$ or doubl$ or trebl$ or tripl$) adj2 blind$) or mask$ or dummy or doubleblind$ or singleblind$ or trebleblind$ or tripleblind$).ti,ab. 18. (placebo$ or random$).ti,ab. 19. treatment outcome$.md. use psyh 20. animals/ not human$.mp. use emez 21. animal$/ not human$/ use mesz 22. (animal not human).po. use psyh 23. (or/10,12,14‐19) not (or/20‐22) 24. 8 and 23
CENTRAL (Wiley interface)
Date range searched: 01.01.1998 to 13.10.2013.
#1. MeSH descriptor: [Drug Overdose], this term only #2. MeSH descriptor: [Self‐Injurious Behavior], this term only #3. MeSH descriptor: [Self Mutilation], this term only #4. MeSH descriptor: [Suicide], this term only #5. MeSH descriptor: [Suicide, Attempted], this term only #6. MeSH descriptor: [Suicidal Ideation], this term only #7. auto mutilat*" or automutilat* or cutt* or "head bang*" or headbang* or overdos* or "self destruct*" or selfdestruct* or "self harm*" or selfharm* or "self immolat*" or selfimmolat* or "self inflict*" or selfinflict* or "self injur*" or selfinjur* or selfmutilat* or "self mutilat*" or "self poison*" or selfpoison* or suicid*:ti #8. "auto mutilat*" or automutilat* or cutt* or "head bang*" or "head bang*" or overdos* or "self destruct*" or selfdestruct* or "self harm*" or selfharm* or "self immolat*" or selfimmolat* or "self inflict*" or selfinflict* or "self injur*" or selfinjur* or selfmutilat* or "self mutilat*" or "self poison*" or selfpoison* or suicid*:ab #9. #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8
Appendix 3. Journals hand‐searched for relevant literature in the original version of this review
1. Archives of Suicide Research (1995‐1998); 2. Crisis (1980‐1998); 3. Suicide and Life‐Threatening Behavior (1971‐1998); 4. Der Nervenarzt (1950‐1979); 5. Journal of Adolescence (1978‐1996); 6. Journal of Affective Disorders (1994‐1996); 7. Journal of the American Academy of Child and Adolescent Psychiatry (1978‐1996); 8. Journal of Clinical Psychiatry (1978‐1996); 9. Journal of Psychiatric Research (1961‐1972) and (1985‐1996); 10. Social Psychiatry (1966‐1987), and 11. Social Psychiatry & Psychiatric Epidemiology (1988‐1996).
Appendix 4. Data collection and analysis methods used for the original review
Selection of studies
In the original version of this review, Sarah Stockton, Librarian at the University of Oxford, conducted the systematic search for trials. Two out of TTS, EA, ET, and KH then independently screened the titles of identified trials for relevancy. A distinction was made between:
1) eligible studies, in which any psychological and/or psychopharmacological treatment was compared with a control (e.g. standard or less intensive types of aftercare or medication), and;
2) ineligible general treatment studies, without any control treatment.
A second screening was then undertaken in which two of TTS, EA, ET, and KH independently screened the full text of relevant studies with reference to the following inclusion criteria:
1. All participants must have engaged in SH (self‐poisoning or self‐injury) shortly prior to randomisation;
2. Studies must have reported the number of participants engaging in a repeat episode of SH as an outcome measure;
3. Study participants must have been randomised to the treatment and control groups.
Data extraction and management
Data extraction was carried out by EA and second member of the review group (TTS, ET, or KH) using a standardised data extraction form. Members of the review team extracted data independently from one another. Disputes were resolved through consensus discussions with a third member of the review group, with assistance from the CCDAN editorial base.
We extracted data from each eligible trial concerning the characteristics of patients, the details of the interventions used, and information on the number of participants engaging in a repeat episode of SH during the follow‐up period. Where these details were unclear, corresponding authors were contacted to provide additional clarification.
Assessment of risk of bias
For the original version of this review, the quality of the studies was rated by three independent review authors (EA and ET plus another member of the review group). Review authors were blind to authorship according to the recommended Cochrane criteria for quality assessment (Sackett 1997).
Given that the quality of concealment of allocation can affect the results of trials (Schulz 1995), studies were assigned a quality of concealment rating ranging from C (poor quality) to A (high quality). Trials rated as inadequately concealed, for example via reference to an open random number table, were given a rating of C. Trials that did not provide adequate details about how the randomisation procedure was carried out were given a rating of B, and trials that were deemed to have taken adequate measures to conceal allocation, for example through the use of serially numbered, opaque, sealed envelopes and numbered or coded bottles or containers, were rated as A quality. Where the concealment of allocation was not clearly reported (i.e. where trials were initially in category B), we contacted corresponding authors for more information. Where raters disagreed as to the category to which a trial should be been allocated, the final rating was made by consensus discussion in consultation with TTS, KH, and a third member of the review group.
Measures of treatment effect
RevMan, version 3.0, was used to calculate summary odds ratios and accompanying 95% CIs for the number of participants engaging in a repeat episode of SH during the follow‐up period.
Unit of analysis issues
1. Cluster trials
Clustering was an issue in one included study (Bennewith 2002), however, as the authors reported adjusting for the effects of clustering in their primary analyses, we reproduced the data from this study as if it came from a non‐cluster randomised study.
2. Studies with multiple treatment groups
One included study presented data for multiple treatment groups (Hirsch 1982). As both treatment groups were prescribed antidepressants in this study, we combined the data from these two treatment arms.
Dealing with missing data
Where data on the primary outcome measure were incomplete or excluded from the study, corresponding author(s) were contacted to obtain further information. Some authors used intention to treat analyses to account for missing data using a variety of different methods which are discussed within the 'Risk of bias' tables. We as review authors did not attempt to impute data for those studies in which intention‐to‐treat analyses had not been conducted, however. Instead, the effects of missing data were discussed in the text of the review.
Assessment of heterogeneity
Clinical heterogeneity was examined using the Chi2 test. Where this statistic was significant, potential causes of heterogeneity were investigated as outlined in the "Subgroup analysis and investigation of heterogeneity" section below.
Assessment of reporting biases
To assess whether any meta‐analysis reported in this review are affected by reporting bias, we planned to construct funnel plots to investigate the likelihood that the results of our meta‐analysis were affected by reporting bias. We were unable to undertake these analyses, however, due to the very small number of trials included in our meta‐analyses.
Data synthesis
The Mantel‐Haenszel fixed‐effect method was used to calculate pooled summary ORs and accompanying 95% CIs.
Subgroup analysis and investigation of heterogeneity
In analyses resulting in significant heterogeneity, as indicated by the Chi2 test, an investigation into the source of this heterogeneity was conducted. We had planned to conduct subgroup analyses by repeater status and gender, however, there were insufficient studies with appropriate data to enable these analyses to be undertaken.
Sensitivity analysis
Sensitivity analyses were undertaken where appropriate (e.g., in relation to risk of bias of included trials in the relative intensity of treatment).
Data and analyses
Comparison 1. Dialectical behaviour therapy/mentalisation for adolescents vs. Treatment as usual or other routine management.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Repetition of SH post‐intervention | 3 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1.1 DBT‐A | 2 | 105 | Odds Ratio (M‐H, Random, 95% CI) | 0.72 [0.12, 4.40] |
| 1.1.2 Mentalisation | 1 | 71 | Odds Ratio (M‐H, Random, 95% CI) | 0.26 [0.09, 0.78] |
| 1.2 Frequency of SH post‐intervention | 2 | 104 | Mean Difference (IV, Random, 95% CI) | ‐0.79 [‐2.78, 1.20] |
| 1.2.1 DBT‐A | 2 | 104 | Mean Difference (IV, Random, 95% CI) | ‐0.79 [‐2.78, 1.20] |
| 1.3 Number of individual psychotherapy sessions attended | 2 | 106 | Mean Difference (IV, Random, 95% CI) | 9.14 [‐4.39, 22.66] |
| 1.3.1 DBT‐A | 2 | 106 | Mean Difference (IV, Random, 95% CI) | 9.14 [‐4.39, 22.66] |
| 1.4 Number of family therapy sessions attended | 2 | 106 | Mean Difference (IV, Random, 95% CI) | 0.93 [‐7.01, 8.86] |
| 1.4.1 DBT‐A | 2 | 106 | Mean Difference (IV, Random, 95% CI) | 0.93 [‐7.01, 8.86] |
| 1.5 Number completing full course of treatment | 1 | 80 | Odds Ratio (M‐H, Random, 95% CI) | 1.35 [0.56, 3.27] |
| 1.5.1 Mentalisation | 1 | 80 | Odds Ratio (M‐H, Random, 95% CI) | 1.35 [0.56, 3.27] |
| 1.6 Depression scores post‐intervention | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.6.1 DBT‐A | 1 | 77 | Mean Difference (IV, Random, 95% CI) | ‐2.39 [‐5.02, 0.24] |
| 1.6.2 Mentalisation | 1 | 80 | Mean Difference (IV, Random, 95% CI) | ‐2.28 [‐2.81, ‐1.75] |
| 1.7 Hopelessness scores post‐intervention | 2 | 101 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.93, 0.67] |
| 1.7.1 DBT‐A | 2 | 101 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.93, 0.67] |
| 1.8 Suicidal ideation scores post‐intervention | 2 | 100 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.07, ‐0.16] |
| 1.8.1 DBT‐A | 2 | 100 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.07, ‐0.16] |
Comparison 2. Group‐based psychotherapy vs. Treatment as usual or other routine management.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Repetition of SH at six months | 2 | 430 | Odds Ratio (M‐H, Random, 95% CI) | 1.72 [0.56, 5.24] |
| 2.2 Repetition of SH at 12 months | 3 | 490 | Odds Ratio (M‐H, Random, 95% CI) | 0.80 [0.22, 2.97] |
| 2.3 Depression scores at six months | 2 | 420 | Mean Difference (IV, Random, 95% CI) | 0.40 [‐2.76, 3.55] |
| 2.4 Depression scores at 12 months | 3 | 473 | Mean Difference (IV, Random, 95% CI) | ‐0.93 [‐4.03, 2.17] |
| 2.5 Suicidal ideation scores at six months | 2 | 421 | Mean Difference (IV, Random, 95% CI) | 1.27 [‐7.74, 10.28] |
| 2.6 Suicidal ideation scores at 12 months | 3 | 471 | Mean Difference (IV, Random, 95% CI) | ‐1.51 [‐9.62, 6.59] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Cooney 2010.
| Study characteristics | ||
| Methods |
Allocation: random allocation using a computerised sequence. Follow‐up period: 6 months. N lost to follow up: 0/29 (0%) for the primary outcome measure of repetition of SH. |
|
| Participants |
Inclusion criteria: i) between 13 and 19 years of age; ii) at least one suicide attempt or one episode of intentional self‐injury within the 3 months preceding the pre‐treatment assessment; iii) in regular contact with at least one adult who was also willing and able to attend treatment sessions as required; iv) proficient in English. Exclusion criteria: i) meets diagnostic criteria for an intellectual disability; ii) meets diagnostic criteria for a psychotic disorder. Numbers: Of the 29 participants, 14 were allocated to the experimental arm and 15 to the control arm. Profile: 75.9% (n = 22) were female, 93.1% (n = 27) were diagnosed with comorbid psychiatric disorders. Source of participants: patients referred to services following a suicide attempt or an episode of intentional self‐injury within the preceding 3 months. Location: Auckland, New Zealand. |
|
| Interventions |
Experimental: dialectical behaviour therapy specially adapted for adolescents composed of weekly individual therapy sessions (50‐60 minutes), weekly group skills training (110 minutes), and family therapy sessions and telephone counselling as required. Control: treatment as usual comprising individual and family sessions provided by a multidisciplinary treatment team, medication management, and hospital or respite care as required. Therapist: therapists with experience in delivering DBT. Type of therapy offered: dialectical behaviour therapy for adolescents. Length of treatment: 26 weeks. |
|
| Outcomes |
Included: i) repetition of SH according to self‐report; ii) treatment adherence; iii) suicidal ideation. Excluded: i) reasons for living; ii) emotion regulation; iii) treatment burden. |
|
| Notes |
Source of funding: no details on funding were provided. Declaration of author interests: "Dr. Emily Cooney and Dr. Kirsten Davis are both directors of a training company (DBTNZ) that is affiliated with Behavioral Tech LLC, the training organisation mandated by the developer of dialectical behaviour therapy. DBTNZ provides training in this therapy within New Zealand. Dr. Emily Cooney, Dr. Kirsten Davis and Pania Thompson are all employed by the Kari Centre child and adolescent mental health service within the Auckland District Health Board. This service provides a DBT programme as a treatment for young people with emotion dysregulation and repeated self‐harm" (p.4). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: “Participants were randomly assigned…via a computerised randomisation procedure…” (p.10). Comment: Use of a computerised randomisation procedure is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk |
Quote: “Each treatment assignment was placed in a sealed numbered envelope (32 envelopes in total) by the assistant…” (p.10). Comment: Use of opaque sealed envelopes would ensure that allocation was adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: As this was a single, assessor‐blinded trial, we can assume that the participants were not blinded as to treatment allocation. |
| Blinding (performance bias and detection bias) Of personnel | High risk | Comment: As this was a single, assessor‐blinded trial, we can assume that clinical personnel were not blinded as to treatment allocation. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: “All subsequent assessments were administered by an assessor…who was also blind to treatment condition” (p.10). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: Not stated. Although data for all 29 participants randomised to the intervention or control groups is reported at the mid‐treatment assessment, at longer follow‐up periods only data on those available for assessment were presented. |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Cotgrove 1995.
| Study characteristics | ||
| Methods |
Allocation: random allocation using open number table. Follow‐up period: 12 months. N lost to follow up: 0/105 (0%) for repetition of SH data. |
|
| Participants |
Inclusion criteria: i) aged 16 years or under. Exclusion criteria: i) records of original suicide attempt missing or those with "insufficient follow‐up data" (p.572). Numbers: Of the 105 participants, 47 were allocated to the experimental arm and 58 to the control arm. Profile: 85% (n = 89) were female, 6% (n = 6) were diagnosed with a major psychiatric disturbance (not specified). Source of participants: patients admitted to hospital following SH. Location: North London, UK. |
|
| Interventions |
Experimental: emergency green card in addition to usual care. The green card acted as a passport to re‐admission into a paediatric ward at the local hospital. Control: standard follow‐up including treatment from a clinic or child psychiatry department as required. Therapist: no details provided. Type of therapy offered: emergency green card. Length of treatment: 12 months. |
|
| Outcomes |
Included: i) repetition of SH according to clinical and hospital notes. Excluded: i) use of emergency card. |
|
| Notes |
Source of funding: no details on funding were provided. Declaration of author interests: no details on author interests were provided. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk |
Quote: “Adolescents were allocated randomly” (p.570). Following correspondence with the study authors, it became apparent that a random open numbers table had been used to generate the sequence. Comment: As the numbers table was open, it is possible there may have been bias in the generation of the random sequence. |
| Allocation concealment (selection bias) | High risk | Comment: As the numbers table was open, it is unlikely allocation could have been adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk |
Quote: “Those in the treatment group received a token, a green card, which acted as a passport to re‐admission into a paediatric ward in their local hospital” (p.570) Comment: The nature of this study means that participants could have known to which group they had been allocated. |
| Blinding (performance bias and detection bias) Of personnel | Unclear risk | Comment: No details on blinding of clinical personnel provided. |
| Blinding (performance bias and detection bias) Of outcome assessors | Unclear risk | Comment: No details on blinding of outcome assessors provided. |
| Incomplete outcome data (attrition bias) All outcomes | High risk |
Quote: Of the eligible 134 consecutive admissions only "105 were included in the follow‐up study..." Comment: Unclear as to why these participants were excluded. |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | High risk |
Quote: "Forty seven adolescents (45%) were randomly allocated to the treatment group and 58 (55%) to the control.... The reasons there were larger numbers in the control group was partly due to chance, and partly due to an error in one centre in the way five of the green cards were issued; either several weeks after discharge without adequate explanation, or in a couple of cases, not at all. This invalidated the follow‐up data from this centre for these five cases in the treatment group, but not on those in the control group." (p. 572) Comment: The inclusion of participants who may have received the treatment intervention within the control group may lead to bias in the estimation of the treatment effect, particularly as it is unclear how these five cases were assessed. Additionally, the authors claim the intervention was effective even though comparison of repetition rates was not significantly different between groups. |
Donaldson 2005.
| Study characteristics | ||
| Methods |
Allocation: Following correspondence with study authors, it became apparent that simple randomisation using a random numbers table had been used to generate the allocation sequence. Follow‐up period: 3 and 6 months. Follow‐up data on functioning for a sub‐sample of participants was available for 12 months. N lost to follow up: 8/39 (21%) for repetition data. |
|
| Participants |
Inclusion criteria: i) aged 12‐17 years; ii) primary language was English; iii) outpatient care indicated; iv) intent to die indicated. Exclusion criteria: i) psychosis indicated on mental status examination; ii) clinician judgement that intellectual functioning precluded outpatient psychotherapy. Numbers: Of the 39 participants, 21 were allocated to the experimental arm and 18 to the control arm. Profile: 48% (15/31) were repeaters, 29% (9/31) were diagnosed with major depression, 19% (6/31) were diagnosed with alcohol use disorder. Source of participants: patients presenting to a general paediatric emergency department or inpatient unit of an affiliated child psychiatric hospital after a suicide attempt. Location: Northeast USA, possibly Providence, RI. |
|
| Interventions |
Experimental: Skills‐based treatment focused on improving problem solving and affect management skills. Additionally, participants were taught problem solving and cognitive and behavioural strategies and given homework assignments to further improve their skills. Treatment comprised two parts: i) active treatment for the first three months which included six individual sessions and one adjunct family session with two additional family sessions and two crisis sessions available at the therapist’s discretion; ii) maintenance treatment for the remaining three months which included three sessions. Control: Supportive relationship therapy focused on addressing the adolescent's mood and behaviour, including unstructured sessions which addressed reported symptoms and problems, and fostered the development of specific skills not otherwise addressed during treatment. This intervention was designed to resemble usual care for this population in this community. Therapist: 5 clinicians and 2 individuals with master’s degrees provided treatment for both study arms. Type of therapy offered: problem solving therapy. Length of treatment: 6 months. |
|
| Outcomes |
Included: i) repetition of SH; ii) suicide; iii) suicidal ideation; iv) depression; v) problem solving; vi) compliance. Excluded: i) anger. |
|
| Notes |
Source of funding: "This project was supported by NIMH (MH05749), the American Foundation for Suicide Prevention, and the Harvard Pilgrim Research Foundation" (p.113). Declaration of author interests: No details on author interests were provided. Other: Data on repetition of SH were obtained from reports from adolescents and parents. Data on suicides were obtained following correspondence with study authors. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: “[Participants were r]andomized to one of two treatment conditions” (p.114) Comment: Correspondence with study authors confirmed that a random numbers table was used to generate the allocation sequence. Use of a random numbers table is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Unclear risk | Comment: No information on allocation concealment was provided. |
| Blinding (performance bias and detection bias) Of participants | Unclear risk | Comment: No information on participant blinding was provided. However, both treatments were so similar that it is possible participants were unaware of which treatment they were receiving. |
| Blinding (performance bias and detection bias) Of personnel | High risk |
Quote: “The same seven therapists provided treatment in both...conditions” (p.114) Comment: Therapists are likely to have known which participant was receiving which treatment. |
| Blinding (performance bias and detection bias) Of outcome assessors | Unclear risk |
Quote: “Outcome measures were administered...by a trained bachelor’s degree level research assistant” (p.115) Comment: No information on outcome assessor blinding was provided. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Quote: “Follow‐up data from all 31 families who completed follow‐ups (regardless of number of treatment sessions attended) were included in data analyses consistent with an intent to‐treat model” (p.115) Comment: In addition to performing analyses in line with the intention‐to‐treat principle, the authors also compared study participants at baseline to those who dropped out of treatment and concluded there were “no significant differences” in the results obtained. Of the 39 randomised participants, 31 completed the 3 or 6 month evaluations. |
| Selective reporting (reporting bias) | Unclear risk | Comment: Suicide data were obtained through correspondence with the study authors, suggesting that selective reporting bias may have been present. |
| Other bias | High risk | Comment: Contamination is possible given that the same seven therapists delivered both the experimental and control treatments. |
Green 2011.
| Study characteristics | ||
| Methods |
Allocation: randomised using a minimisation procedure controlling for: i) frequency of SH; ii) diagnosis of conduct disorder; iii) diagnosis of major depression; iv) psychosocial distress. Follow‐up period: 6 and 12 months. N lost to follow up: "Loss to follow‐up was low (<4%)" (p.1). |
|
| Participants |
Inclusion criteria: i) aged 12 years to 16 years 11 months; ii) presenting to child and adolescent services with a history of at least two episodes of SH in the previous 12 months. Exclusion criteria: i) unable to communicate in English; ii) diagnosed with severe low weight anorexia nervosa; iii) diagnosed with psychosis; iv) attends a special learning disability school; v) currently in secure care. Numbers: of the 366 participants, 183 were allocated to the intervention arm and 183 to the control arm. Profile: 88.5% (n = 324) were female, 100% (n = 366) were multiple repeaters, 62.0% (n = 227) were diagnosed with a depressive disorder; 33.3% (n = 122) were diagnosed with a behavioural disorder. Source of participants: adolescents presenting to local child and adolescent services with a history of at least two episodes of SH within the previous 12 months. Location: Manchester and Chester, UK. |
|
| Interventions |
Experimental: manualised developmental group psychotherapy involving elements of cognitive behavioural therapy, dialectical behavioural therapy, and group psychotherapy. Control: treatment as usual according to the clinical judgement of the adolescents' child and adolescent mental health service team. Treatment as usual excluded any type of group‐based intervention. Therapists: clinicians with a minimum of thee years post‐qualifying experience and who also received training in delivering developmental group psychotherapy. Type of therapy offered: group psychotherapy Length of treatment: Acute treatment phase: 6 weeks. Weekly booster sessions continued for as long as required (maximum theoretical length of treatment unclear in trial report). |
|
| Outcomes |
Included: i) repetition of SH according to self‐ and/or collateral report; ii) suicide; iii) suicidal ideation; iv) depression. Excluded: i) global functioning; ii) health economics information. |
|
| Notes |
Source of funding: "This study was funded by the Health Foundation and sponsored by the University of Manchester" (p.11). Declaration of author interests: none stated. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: "Allocation was by minimisation controlling for: high or low self harm...presence of behavioural disorder...or depressive disorder...and presence or absence of high psychosocial risk..." (p.4). Comment: use of a minimisation algorithm is likely to have minimised the role of bias in the generatioU of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk |
Quote: "Randomisation was by remote telephone..." (p.4). Comment: Randomisation by remote telephone would have enabled the allocation sequence to have remained adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk | Quote: "It was not possible to blind...the participants themselves to treatment allocation" (p.4). |
| Blinding (performance bias and detection bias) Of personnel | High risk | Quote: "It was not possible to blind clinicians...to treatment allocation" (p.4). |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: "The main outcomes were recorded by outcome assessors blinded to treatment allocation...Assessor guesses of allocation following end point were no better than chance" (p.4). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk |
Quote: "Analysis of primary and secondary outcomes was by intention‐to‐treat subject to availability of data" (p.4). Comment: Although the authors describe using an intention‐to‐treat approach to analyses for both primary and secondary outcomes, not all participants allocated to the intervention and control groups are included in subsequent analyses suggesting that outcome reporting may be incomplete. |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Harrington 1998.
| Study characteristics | ||
| Methods |
Allocation: randomisation using a series of opaque sealed envelopes which contained either a blank sheet or one bearing the letter F (for family therapy). Follow‐up period: 6 months. N lost to follow up: 13/162 (8%) for repetition data. |
|
| Participants |
Inclusion criteria: i) 16 years of age or younger; ii) engaged in an episode of self‐poisoning; iii) living in a family. Exclusion criteria: i) engaged in self‐cutting or hanging; ii) in social service care; iii) current investigation of physical or sexual abuse; iv) diagnosed with a contraindicated psychiatric condition (e.g., psychosis); v) currently in inpatient treatment; vi) parent or child diagnosed with a learning disability; vii) parent or child seriously suicidal. Numbers: Of the 162 participants, 85 were allocated to the experimental arm and 77 to the control arm. Profile: 89.5 % (n = 145) were female, 64.5% (n = 104) were diagnosed with major depression, 10.5% (n = 17) were diagnosed with conduct disorder, 100% (n = 162) had a history of self‐poisoning. Source of participants: patients referred to mental health teams in one of four hospitals. Location: Manchester, UK. |
|
| Interventions |
Experimental: manualised home based family therapy intervention involving one assessment session and 4 home visits in addition to treatment as usual. Control: treatment as usual. Therapist: 2 psychiatric social workers with a master’s degree. Type of therapy offered: family therapy. Length of treatment: not stated. |
|
| Outcomes |
Included: i) repetition (data obtained from study authors); ii) suicide; iii) suicidal ideation; iv) compliance; v) hopelessness; vi) problem solving; vii) depression. Excluded: i) family functioning; ii) satisfaction with treatment; iii) cost‐effectiveness; iv) parent General Health Questionnaire. |
|
| Notes |
Source of funding: "This research was supported by the Department of Health, London" (p.517). Declaration of author interests: no details on author interests were provided. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "a series of opaque and sealed envelopes containing either a blank sheet or the letter F were prepared and randomly assorted by an assistant" (p.2). Comment: Although it is likely the random sequence was adequately generated, without further information on the method used, this cannot be ascertained. |
| Allocation concealment (selection bias) | Low risk | Quote: "a series of opaque and sealed envelopes containing either a blank sheet or the letter F were prepared and randomly assorted by an assistant” (p.2). Comment: Use of opaque sealed envelope containing either a blank sheet or a sheet with the letter F printed on it would ensure that allocation was adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: The nature of this study means that participants could have known to which group they had been allocated. |
| Blinding (performance bias and detection bias) Of personnel | High risk |
Quote: “[The envelopes] were opened by the social worker at the time of the assessment, who then assigned the case to the family intervention plus routine care or routine care alone” (p.2) Comment: Personnel were not blinded. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: “Treatment assignment was entered on a register and concealed from the outcome assessors” (p.2) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: “Outcome assessments were conducted with 154 (96%) of 162 cases at two months and 149 (92%) of 162 cases at six months” (p.3). “All the analyses were conducted ‘intent to treat’” (p.3). |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Hazell 2009.
| Study characteristics | ||
| Methods |
Allocation: random allocation conducted by a distant site coordinator. Follow‐up period: 12 months N lost to follow up: 0/72 for repetition data. |
|
| Participants |
Inclusion criteria: i) aged between 12 and 16 years; ii) referred to a child and adolescent mental health service in Newcastle, Brisbane North, or Logan; iii) reported at least two episodes of self‐harm in the past year, one of which occurred within the past 3 months. Exclusion criteria: i) required intensive treatment owing to an imminent risk of SH; ii) diagnosed with acute psychosis; iii) diagnosed with an intellectual disability or other disorder that would indicate the patient was unlikely to benefit from group therapy sessions; iv) current level of SH risk precluded participation in group therapy sessions. Numbers: Of the 72 participants, 35 were allocated to the experimental arm and 37 to the control arm. Profile: 90.3% (n = 65) were female, 100% (n = 72) were multiple repeaters, 4.1% (n = 3) had alcohol problems, 0% (n = 0) had substance misuse problems, 56.9% (n = 41) were diagnosed with depression; 6.9% (n = 5) had a diagnosis of conduct/oppositional defiant disorder. Source of participants: patients referred to a child and adolescent mental health service who had reported at least two episodes of SH in the past year, one within the past 3 months. Setting: Newcastle, Brisbane North, and Logan, New South Wales and Queensland, Australia. |
|
| Interventions |
Experimental: group therapy involving CBT, social skills training, interpersonal psychotherapy, group psychotherapy in addition to treatment as usual. Control: treatment as usual involving individual counselling, family sessions, medication assessment and review, and other care co‐ordination. Therapists: clinicians in community‐based adolescent mental health services. Type of therapy offered: group psychotherapy. Length of treatment: 12 months. |
|
| Outcomes |
Included: i) repetition of SH according to self‐report; ii) suicide; iii) suicidal ideation; iv) depression. Excluded: None |
|
| Notes |
Source of funding: no specific sources of funding were reported for this study. Declaration of author interests: "Prof. Hazell has received research funding from Celltach and Eli Lilly; has served as a consultant to Eli Lilly, Janssen‐Cilag, Novartis, and Shire; and has participated in the speakers' bureaus of Eli Lilly, Janssen‐Cilag, and Pfizer. The other authors report no conflicts of interest" (p.669). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: Correspondence with study authors revealed that a computer generated random number table was used to generate the random sequence. Randomisation by location and by blocks of four were also used to ensure a similar number of adolescents were recruited from each study location. |
| Allocation concealment (selection bias) | Low risk |
Quote: "The local site co‐ordinator emailed the distant site co‐ordinator, who assigned a trial number and randomly allocated that adolescent to group therapy or routine care" (p.664) Comment: Use of a remote site co‐ordinator is likely to have ensured allocation was adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk | Quote: "The adolescent was informed of his or her allocation by a letter and by their routine care therapist" (p.664). |
| Blinding (performance bias and detection bias) Of personnel | High risk | Quote: "The adolescent was informed of his or her allocation by a letter and by their routine care therapist" (p.664) Comment: Given that the therapist is informing participants as to their allocation, this would suggest personnel were also not blinded to allocation. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: "Treatment allocation was concealed from the outcome assessors, who were asked at the end of the study to nominate which treatment had been given to the adolescents" (p.664) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk |
Quote: "Continuous outcome data were analyzed on an intent‐to‐treat basis" (p.664) Comment: Intention‐to‐treat analyses made using the last outcome carried forward method. |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Mehlum 2014.
| Study characteristics | ||
| Methods |
Allocation: random allocation conducted by an external group using a permuted block randomisation procedure. Follow‐up period: 16 weeks (post‐treatment). N lost to follow up: 0/77 (0%). |
|
| Participants |
Inclusion criteria: i) history of at least two prior episodes of SH, one of which must have occurred in the preceding 16 weeks; ii) meets at least two of the DSM‐IV borderline personality disorder criteria including the self‐destructive criterion, or, at least one of the DSM‐IV borderline personality disorder criteria and at least two sub‐threshold level criteria; iii) fluent in Norwegian. Exclusion criteria: i) diagnosed with bipolar disorder (with the exception of bipolar II disorder), schizophrenia, schizoaffective disorder, psychotic disorder not otherwise specified, intellectual disability, or Asperger's syndrome. Numbers: Of the 77 participants, 39 were allocated to the experimental arm and 38 to the control arm. Profile: 88.3% (n = 68) were female, 100% (n = 77) were multiple repeaters, 22.1% (n = 17) were diagnosed with major depression, 37.7% (n = 29) were diagnosed with another depressive disorder, 26.0% (n = 20) were diagnosed with borderline personality disorder, 2.6% (n = 2) were diagnosed with substance use disorder. Source of participants: patients referred to a child and adolescent mental health service who had reported at least two episodes of SH in the past year, one within the past 16 weeks. Setting: Oslo, Norway. |
|
| Interventions |
Experimental: dialectical behaviour therapy specially adapted for adolescents (DBT‐A) involving: weekly sessions of individual therapy, weekly sessions of multifamily skills training, family therapy sessions, and telephone coaching as required. Control: enhanced usual care involving no less than one weekly individual therapy session. Therapists: psychologists and psychiatrists who received training in DBT‐A specially for this trial. Type of therapy offered: dialectical behaviour therapy. Length of treatment: 19 weeks. |
|
| Outcomes |
Included: i) repetition of SH according to self‐report and hospital records; ii) suicidal ideation; iii) depression; iv) hopelessness Excluded: i) borderline personality disorder symptom severity. |
|
| Notes |
Source of funding: "This study was funded by grants from the Norwegian Directorate of Health, the South Eastern Regional Health Authority, the Extra‐Foundation for Health and Rehabilitation, and the University of Oslo" (p.9). Declaration of author interests: no author reported any conflict of interest. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: "Treatment allocation of participants...was based on a permuted block randomisation procedure with an undisclosed and variable blocking factor..." (p.2) Comment: Use of a block randomisation procedure is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk |
Quote: "...management of the randomisation procedures was performed by an external group..." (p.2) Comment: Use of remote site coordinators is likely to have ensured allocation was adequately concealed. |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: This was a single, assessor‐blinded trial. |
| Blinding (performance bias and detection bias) Of personnel | High risk | Comment: This was a single, assessor‐blinded trial. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: "Ten independent assessors, blind to treatment allocation and to results from baseline interviews, conducted interviews at trial completion..." (p.4) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Data analysis was by intention to treat." (p.5) |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Ougrin 2011a.
| Study characteristics | ||
| Methods |
Allocation: randomisation at the clinician level using permuted blocks (block lengths 22 and 4) using web‐based randomisation software. Follow‐up period: 12 and 24 months. Data for the 24 month follow‐up period were extracted from Ougrin 2013. N lost to follow up: 0/70 (0%) for the primary outcome (i.e., attendance at scheduled individual outpatient therapy sessions); 5/70 (7.1%) for secondary outcomes. |
|
| Participants |
Inclusion criteria: i) aged 12‐18 years; ii) presenting to emergency departments following an episode of SH; iii) referred for psychological assessment at one of two Child and Adolescent Mental Health Services. Exclusion criteria: i) currently receiving psychiatric treatment; ii) diagnosed with a disorder causing gross reality distortion (e.g., psychosis, acute intoxication); iii) history of diagnosis for a moderate to severe learning disability; iv) unable to communicate fluently in English; v) at immediate risk of violence or suicide; vi) requiring inpatient psychiatric treatment. Numbers: Of the 26 clinicians, 13 were allocated to the experimental arm and 13 to the control arm. Of the 70 participants, 35 received treatment from clinicians allocated to the experimental arm and 35 received treatment from clinicians allocated to the control arm. Profile: 80.0% (n = 56) were female; 58.6% (n = 41) were multiple repeaters Source of participants: patients admitted to emergency departments following an episode of SH. Location: London, UK. |
|
| Interventions |
Experimental: manualised therapeutic assessment involving standard psychosocial history and suicide risk assessment conducted according to NICE guidelines (NICE 2004), a review of this information, the identification of reciprocal roles, core pain, and maladaptive procedures based on a cognitive analytic therapy paradigm, the identification of target problems, consideration of the ways to change these problems, providing motivation to change these problems, exploring alternatives to solve these problems, and the construction of an "understanding letter" summarising these steps to be sent to the family. Control: standard psychosocial history and suicide risk assessment conducted according to NICE guidelines (NICE 2004). Therapist: clinicians who received a minimum of 5 weeks training in therapeutic assessment. Type of therapy offered: therapeutic assessment. Length of treatment: approximately 1 hour and 40 minutes. |
|
| Outcomes |
Included: i) repetition of SH; ii) suicide; iii) compliance. Excluded: i) functioning; ii) strengths and difficulties. |
|
| Notes |
Funding source: "The study was funded from the following three sources: Psychiatry Research Fund...Maudsley Charitable Fund...and West London Research Consortium" (p.153). Declaration of author interests: "...DO has support from Psychiatry Research Trust, Maudsley Charitable Funds and West London Research Consortium for the submitted work...AN, DO and TZ have royalties paid to them by Hodder Arnold Publishing that might have an interest in the submitted work...DO, TZ, AN, RB, AB and ET have no non‐financial interests that may be relevant to the submitted work" (p.153). Other: Adjustment was made for the effects of clustering within clinicians enabling the inclusion of this study. Data on repetition of SH and suicide were obtained following correspondence with study authors. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: "Randomisation occurred at the assessor level...The randomisation was stratified by centre, and two blocks (block lengths 22 and 4) were created using a permuted block design to ensure equal numbers from each centre being allocated to either intervention or control groups. The randomisation scheme was generated using web‐based randomisation software (http://www.randomization.com)" (pp. 149‐150). Comment: Use of computer‐based randomisation software is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation was conducted by a senior psychiatrist independent of the study clinicians" (pp.149‐150). |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: Correspondence with study authors revealed that participants were not blinded. |
| Blinding (performance bias and detection bias) Of personnel | High risk | Quote: "It was not possible to blind the clinicians to the intervention they were delivering" (p.150). |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: "The study statistician and the researchers conducting follow‐up assessments were unaware of the participants' allocation" (p.150). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "All 70 recruited participants were analysed on the primary and secondary outcome measures. Whenever the data were missing we used the last observation available" (p.150). |
| Selective reporting (reporting bias) | Unclear risk | Comment: Data on repetition of SH had to be requested from study authors, suggesting that selective reporting bias may have been present. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Rossouw 2012a.
| Study characteristics | ||
| Methods |
Allocation: randomisation using a minimisation procedure controlling for: i) age; ii) gender; iii) number of prior hospital admissions for SH. Follow‐up period: 3, 6, 9, and 12 months. N lost to follow up: 9/80 (11.2%) for SH at the 12 month follow‐up. |
|
| Participants |
Inclusion criteria: i) 12‐17 years; ii) presented with at least one episode of SH within the past month; iii) episode of SH was primary reason for referral to psychiatric services. Exclusion criteria: i) required inpatient psychiatric treatment; ii) diagnosed with comorbid psychosis, a severe learning disability, a pervasive developmental disorder, or an eating disorder in the absence of SH; iii) diagnosed with any chemical dependence. Numbers: Of the 80 participants, 40 were allocated to the intervention arm and 40 to the control arm. Profile: 85.0% (n = 68) were female; 96.2% (n = 77) were diagnosed with depression; 72.5% (n = 58) were diagnosed with borderline personality disorder. Source of participants: patients presenting to community health services or acute hospital emergency rooms following an episode of SH. Location: London, UK. |
|
| Interventions |
Experimental: mentalisation‐based treatment adapted for adolescents involving manualised psychodynamic psychotherapy sessions for both the adolescent and his/her family. Control: treatment as usual according to current NICE guidelines (NICE 2004). "The majority of...participants in the TAU group received the following: an individual therapeutic session alone (28%), consisting of counselling (in 38% of cases receiving an individual intervention), generic supportive interventions (24%), cognitive behavioral therapy (19%), or psychodynamic psychotherapy (19%); a combination of individual therapy and family work (25%); or psychiatric review alone (27.5%)" (p.1306). Therapist: 22 therapists from a variety of different professional backgrounds who received 6 days training in delivering mentalisation‐based treatment. Type of therapy offered: mentalisation. Length of treatment: 12 months. |
|
| Outcomes |
Included: i) repetition of SH according to scores on SH scale of the Risk‐Taking and Self‐Harm Inventory; ii) depression; iii) hopelessness; iv) compliance. Excluded: i) borderline personality disorder symptom severity; ii) feelings. |
|
| Notes |
Source of funding: no details on funding are provided. Declaration of author interests: "Dr. Fonagy is the Chief Executive of the Anna Freud Centre, London, which regularly offers training courses in mentalization based treatment...and National Clinical Lead for the Department of Health's Improved Access to Psychological Therapies (IAPT) for Children and Young People Programme. He has received grant income from the National Institute of Clinical Excellence, the UK Mental Health Research Network, the British Academy, the Wellcome Trust, the National Institute of Health Research (Senior Investigator Award and Research for Patient Benefit Programme), the Pulitzer Foundation, the Department for Children, Schools, and Families, the Central and East London Comprehensive Local Research Network (CLRN) Programme, the NHS Health Technology Assessment (HTA) programme, the Department of Health's IAPT Programme, and the Hope for Depression Foundation. Dr. Rossouw reports no biomedical, financial interests, or potential conflicts of interest" (p.1312). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: "Allocation was by minimization, controlling for past hospital admissions, gender, and age." (p.1305). Comment: Use of a minimisation procedure is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk | Quote: "...participants were randomized by an independent statistician working off‐site..." (p.1306). |
| Blinding (performance bias and detection bias) Of participants | Low risk | Quote: "...participants were...blinded to assignment" (p.1305). |
| Blinding (performance bias and detection bias) Of personnel | High risk | Comment: The nature of the study means personnel are likely to have known which participant was receiving which treatment. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: "assessors...were...blinded to assignment" (p.1305). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Data analysis was by intention to treat" (p.1306). |
| Selective reporting (reporting bias) | Unclear risk | Comment: No reason to suspect that all outcomes were not measured, however, in the absence of the trial protocol, this cannot be ascertained. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Spirito 2002.
| Study characteristics | ||
| Methods |
Allocation: randomisation using a random numbers table. Follow‐up period: 3 months. N lost to follow up: 13/76 (17%) for repetition of SH data. |
|
| Participants |
Inclusion criteria: i) aged 12‐18 years; ii) receiving medical care in either the emergency department or paediatric ward of a children's hospital following a suicide attempt. Exclusion criteria: none stated. Numbers: Of the 76 participants, 36 were allocated to the experimental arm and 40 to the control arm. Profile: 63 (90%) were female. Source of participants: patients presenting to hospital following a suicide attempt. Location: Northeast USA, possibly Providence, RI. |
|
| Interventions |
Experimental: compliance enhancement intervention plus standard disposition planning involving a single, one‐hour session that reviewed expectations for outpatient treatment as well as addressing the factors likely to impede attendance and treatment misconceptions, and encouraged both the adolescent and parent to make a verbal contract to attend all treatment sessions. Participants were also contacted by telephone at 1, 2, 4, and 8 weeks post‐discharge to review their compliance with treatment. Control: standard disposition planning involving treatment based on judgment of psychiatric clinician who conducted the evaluation. Some participants in both the experimental and control arms had a brief inpatient psychiatric stay prior to receiving outpatient care. The remainder received outpatient care at local mental health centre. Therapist: 3 post‐doctoral fellows in psychology. Type of therapy offered: compliance enhancement. Length of treatment: 8 weeks. |
|
| Outcomes |
Included: i) repetition of SH according to self‐ and parent‐report, however, only data from self‐report was used; ii) suicide; iii) compliance. Excluded: i) problems concerning therapy sessions. |
|
| Notes |
Source of funding: "This investigation was supported by NIMH grant MH52411 and by a grant from the van Amerigen Foundation" (p.435). Declaration of author interests: not stated. Other: In two cases a parent reported repetition of SH but the adolescent denied this. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: “Randomly assigned” (p.436) Comment: Correspondence with study authors clarified that the method used was a "random numbers table." Use of a random numbers table is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Unclear risk | Comment: no details on allocation concealment were provided. |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: The nature of this study means that participants could have known to which group they had been allocated. |
| Blinding (performance bias and detection bias) Of personnel | High risk | Comment: The nature of the study means personnel are likely to have known which participant was receiving which treatment. |
| Blinding (performance bias and detection bias) Of outcome assessors | Unclear risk | Comment: No details on outcome assessor blinding were provided. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk |
Quote: “Adolescents who refused to participate in the project (n = 6) were compared on age and gender to those who were enrolled. No significant differences were found. In addition, adolescents who were lost to follow‐up (n = 13) were compared to those who remained in the project. There were no significant differences noted on age, gender, race, [socioeconomic status], or any of the baseline psychological measures” (p.437) Comment: Although there was no indication that intention‐to‐treat analyses had been conducted, efforts were clearly made to establish whether results could be affected by attrition bias. |
| Selective reporting (reporting bias) | Unclear risk | Comment: Data on suicides had to be requested from study authors, suggesting that selective reporting bias may have been present. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
Wood 2001a.
| Study characteristics | ||
| Methods |
Allocation: randomised allocation using trial numbers. Follow‐up period: 7 months N lost to follow up: for repetition of SH, 1/32 (3.1%) in the experimental arm and 0/31 (0%) in the control arm. |
|
| Participants |
Inclusion criteria: i) 12‐16 years; ii) referred to child and adolescent mental health service following an episode of SH; iii) a history of SH on at least one other occasion during the preceding year. Exclusion criteria: i) diagnosed as too suicidal for ambulatory care by a senior child and adolescent psychiatrist; ii) current situation precludes attendance at group sessions (e.g., incarcerated); iii) diagnosed with any psychosis; iv) diagnosed with learning problems or any other disorder that made it unlikely they would benefit from group‐based interventions. Numbers: of the 63 participants, 32 were allocated to the experimental arm and 31 to the control arm. Profile: 100% (n = 63) were multiple repeaters who had engaged in SH an average of 4 times prior to study entry, most commonly by overdose and cutting, 83.9% (n = 52) were diagnosed with major depression, 38.7% (n = 24) of the experimental group and 30.6% (n = 19) of the control group were diagnosed with conduct and/or oppositional defiance disorder. Source of participants: patients referred to child and adolescent mental health service following an episode of SH. Location: Manchester, UK |
|
| Interventions |
Experimental: developmental group psychotherapy involving a variety of techniques, including: problem solving, CBT, DBT, and group psychodynamic psychotherapy interventions. Treatment comprised a one‐off initial assessment phase, followed by 6 acute group sessions, and weekly group therapy sessions continuing until the young person felt ready to leave the intervention. Treatment as usual was also available as required. Control: treatment as usual delivered by community psychiatric nurses and psychologists involving family sessions, non‐specific counselling, and psychotropic medication where indicated. Therapist: 2 therapists, a senior nurse, and a psychiatrist Type of therapy offered: group psychotherapy. Length of treatment: 6 months. |
|
| Outcomes |
Included: i) repetition of SH; ii) suicide; iii) suicidal ideation; iv) depression; v) compliance. Excluded: i) admissions to hospital; ii) behavioural problems; iii) global outcomes. |
|
| Notes |
Source of funding: "This research was supported by a project grant from the Mental Health Foundation and by a Training Fellowship to Miss Trainor from the National Health Service Executive North West" (p.1246). Declaration of author interests: no details on author interests are provided. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: “An independent statistician at a distant site...assigned a trial number and then randomly allocated participants” (p.1247). Comment: Use of assignment by a random numbers technique is likely to have minimised the role of bias in the generation of the randomisation sequence. |
| Allocation concealment (selection bias) | Low risk | Quote: “Treatment allocation was concealed from the outcome assessors” (p.1247). |
| Blinding (performance bias and detection bias) Of participants | High risk | Comment: The nature of this study means that participants could have known to which group they had been allocated. |
| Blinding (performance bias and detection bias) Of personnel | High risk | Comment: The nature of the study means personnel are likely to have known which participant was receiving which treatment. |
| Blinding (performance bias and detection bias) Of outcome assessors | Low risk | Quote: “Treatment allocation was concealed from the outcome assessors” (p.1247). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "We used the most stringent [method of intention‐to‐treat analyses] in which all randomized cases were included, regardless of whether they started or completed treatment. The analysis was conducted just once, all cases were analyzed as allocated, and no interim or subgroup analyses were permitted" (p.1248). |
| Selective reporting (reporting bias) | Unclear risk | Comment: Data on suicides had to be requested from study authors, suggesting that selective reporting bias may have been present. |
| Other bias | Low risk | Comment: No apparent other sources of bias. |
CBT: cognitive behavioural therapy DBT: dialectical behavior therapy DBT‐A: dialectical behavior therapy for adolescents SH: self‐harm
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Asarnow 2011 | Participants were not required to have engaged in SH prior to study entry. |
| Bjärehed 2013 | Participants were not required to have engaged in SH prior to study entry. |
| Brent 2009 | Not all participants were randomised to the intervention or control groups; some chose to receive the intervention treatment. |
| Carli 2011 | Participants were not required to have engaged in SH prior to study entry. |
| Deykin 1986 | Non‐randomised clinical trial. |
| Diamond 2010 | Participants were not required to have engaged in SH prior to study entry. |
| Donaldson 1997 | Non‐randomised clinical trial. |
| Dubois 1999 | Greater than 10‐15% of the sample were older than 18 years of age at study entry. |
| Emslie 2006a | Participants were not required to have engaged in SH prior to study entry. |
| Emslie 2006b | Participants were not required to have engaged in SH prior to study entry. |
| Emslie 2007 | Participants were not required to have engaged in SH prior to study entry. |
| Emslie 2009 | Participants were not required to have engaged in SH prior to study entry. |
| Esposito‐Smythers 2006 | Participants were not required to have engaged in SH prior to study entry. |
| Esposito‐Smythers 2011 | Participants were not required to have engaged in SH prior to study entry. |
| Findling 2009 | Participants were not required to have engaged in SH prior to study entry. |
| Fleischhaker 2005 | Non‐randomised clinical trial in which data from only the intervention arm are presented. |
| Huey 2004 | Participants were not required to have engaged in SH prior to study entry. |
| King 2006 | Participants were not required to have engaged in SH prior to study entry. |
| King 2009 | |
| Miller 2000 | Non‐randomised clinical trial. |
| Nixon 2003 | Non‐randomised clinical trial. |
| Oldershaw 2012 | Participants were not required to have engaged in SH prior to study entry. |
| Pineda 2013 | Participants were not required to have engaged in SH prior to study entry. |
| Podobnik 2012 | Participants were not required to have engaged in SH prior to study entry. |
| Ramani Perera 2011 | Correspondence with study authors suggested alternate allocation to intervention and control groups, rather than true randomisation. |
| Robinson 2012 | Participants were not required to have engaged in SH prior to study entry. |
| Robinson 2014 | Participants were not required to have engaged in SH prior to study entry. |
| Rotheram‐Borus 1996 | Non‐randomised clinical trial. |
| Sarchiapone 2013 | Participants were not required to have engaged in SH prior to study entry. |
| Vitiello 2009 | Not all participants were randomised to the intervention or control groups; some chose to receive the intervention treatment. |
| Wilkinson 2011 | Participants were not required to have engaged in SH prior to study entry. |
| Xu 2006 | Method of allocation to intervention and control groups unclear. |
SH: self‐harm
Characteristics of ongoing studies [ordered by study ID]
Asarnow 2014.
| Study name | Family‐based intervention for adolescent suicide attempters. Extension: Self‐Harm and Suicide Attempt Risk: Evaluation of an Intervention for Youths with Self‐Harm Behaviour. The SAFETY Study. Trial Registration Number: NCT00692302. |
| Methods |
Allocation: single‐blind randomisation. Design: single‐centre (hospital‐affiliated outpatient psychiatric clinic). Setting: hospital‐affiliated outpatient psychiatric clinic in an academic medical centre. Follow‐up period: 3 months. Location: Los Angeles, USA. |
| Participants | Males and females, between 11 and 18 years of age inclusive, selected for presence of suicide attempt within the previous 3 months, were eligible for participation in this trial. An extension of this protocol also enables those with a history of clinically significant self‐harming behaviour to be included. Clinically significant self‐harming behaviour is defined as: 1) an episode of NSSI in the past 3 months; 2) this episode of NSSI is viewed as indicating the presenting problem or a major part of the presenting problem (e.g., the youth presents with NSSI plus suicidal ideation, or with NSSI plus depression), and 3) a pattern of repeated self‐harm behaviour is present as evident by a total or 2 or more lifetime episodes of NSSI and/or suicidal attempts. |
| Interventions | Those randomised to the intervention group received SAFETY, a cognitive‐behavioural oriented family treatment rooted in socio‐ecological theory. Those randomised to the control group received enhanced treatment as usual. In this study, enhancements included 2 additional elements: 1) parents and the youth attended one session with a study clinician to discuss safety, self‐harm, and suicide risk as well as the importance of outpatient treatment to address these issues; and 2) care linkage support was also offered for a period of 12 weeks with monthly check‐in sessions to support patients in linking up with community treatment through the provision of motivational enhancement and problem‐solving therapy. |
| Outcomes |
Primary outcome: repeat episodes of self‐harming behaviour at 3 months follow‐up. Secondary outcomes: repeat episodes of NSSI and/or attempted suicide as separate outcomes at 3 months follow‐up, scores on a measure of depression for both the youth and his/her parents at 3 months follow‐up, scores on a measure of hopelessness at 3 months follow‐up, scores on a measure of social adjustment at 3 months follow‐up, and patient satisfaction at 3 months follow‐up. |
| Starting date | December 2010. Recruitment period closed: between December 2011 and July 2012. Proposed end date: December 2014. |
| Contact information |
Name: Prof. Joan Asarnow (PI). Affiliation: Department of Psychiatry and Biobehavioral Sciences, University of California, Los Angeles. email:jasarnow@mednet.ucla.edu |
| Notes | Prof. Joan Asarnow very kindly provided unpublished information relating to this trial. Please note that Dr. Jennifer Hughes is the PI for the extension component of this trial focusing on youths presenting with NSSI. |
Cottrell 2014.
| Study name | Self‐harm intervention, family therapy (SHIFT): A randomised controlled trial of family therapy versus treatment as usual for young people seen after second or subsequent episodes of self‐harm. Trial Registration Number: ISRCTN 59793150. |
| Methods |
Allocation: randomised. Design: multi‐centre (hospital and community). Setting: community. Follow‐up period: 18 months. Location: multiple locations around the north of England and London. |
| Participants | Males and females, between 11 and 17 years of age, who have engaged in at least one episode of self‐harm as assessed by the local Child and Adolescent Mental Health team as well as at least one additional episode of self‐harm prior to the index presentation, will be included in this trial. Those diagnosed with severe major depression necessitating psychiatric inpatient care will be excluded from participation. Self‐harming behavior includes any form of non‐fatal self‐poisoning or self‐injury such as cutting, overdose, hanging, self‐strangulation, jumping from a height, and deliberately running in front of traffic regardless of the motive and/or intent to die. N: 832. |
| Interventions | Participants (and their families) randomised to the experimental group will receive up to 8 sessions over a 6 month period of family therapy delivered by qualified family therapists using a modified version of the Leeds Family Therapy and Research Centre Systemic Family Therapy Manual. |
| Outcomes |
Primary outcome: rates of repetition of self‐harm leading to hospital admission within the 18 month follow‐up period. Secondary outcomes: number of participants engaging in self‐harm within 12 months post‐randomisation, cost effectiveness of family therapy as measured by the cost of each self‐harm event avoided due to family therapy, number of subsequent self‐harm episodes, time to subsequent self‐harm episodes, severity of subsequent episodes, dangerousness of the method/s used in any subsequent episode as measured by the Suicide Attempt Self‐Injury Interview, scores on the Beck Scale for Suicide Ideation, and scores on the Paediatric Quality of Life Enjoyment and Satisfaction questionnaire. |
| Starting date | September 2009. First participant recruited April 2010. Recruitment period closed: December 2013. Follow‐up period concludes: June 2015. |
| Contact information |
Name: Prof. David Cottrell (chief investigator). Affiliation: Leeds Institute of Health Sciences, Faculty of Medicine and Health, University of Leeds. email:d.j.cottrell@leeds.ac.uk |
| Notes | Prof. David Cottrell very kindly provided unpublished information relating to this trial. |
Diamond 2014.
| Study name | Family Therapy as Hospital Aftercare for Adolescent Suicide Attempters. Trial Registration Number: NCT01195740. |
| Methods |
Allocation: randomised. Design: single‐centre (mental health inpatient unit). Setting: community. Follow‐up period: 16 weeks. Location: Philadelphia, USA. |
| Participants | Male and female adolescents between 12 and 17 years of age, who made at least one suicide attempt in the previous month were included in this trial. Preliminary results suggest 80% of participants were female, 65% were of African‐American ethnicity. |
| Interventions | Participants randomised to the experimental group received attachment based family therapy alongside enhanced usual care. Enhanced usual care is a facilitated referral process with ongoing clinical monitoring. Each adolescent's treating therapist was ultimately responsible for engaging and retaining the adolescent and their family with treatment. |
| Outcomes |
Primary outcome: scores on the Client Satisfaction Questionnaire and the Cornell Services Index measured at 16 weeks post‐treatment. Secondary Outcomes: scores on various measures of attachment with parents (e.g., the Relatedness Scale and the Relationship Structures Questionnaire), and scores on the Lethality of Suicide Attempt Rating Scale at 16 weeks post‐treatment. Information on future suicide attempts and scores on the Beck Depression Inventory, the Suicide Ideation Questionnaire, the Columbia Suicide‐Severity Scale, and the Suicide Intent Scale were also collected. |
| Starting date | April, 2009. End date: May, 2011. |
| Contact information |
Name: Dr. Guy S. Diamond (PI). Affiliation: Drexel University. email:gd342@drexel.edu |
| Notes | Dr. Suzanne Levy and Dr. Guy Diamond very kindly provided unpublished information relating to this trial. Additionally, Dr. Levy provided the following notes pertaining to the findings of this study: "In 2011, we completed a pilot study testing the feasibility, acceptability and outcomes of Attachment‐Based Family Therapy (ABFT; Diamond et. al, 2002) as an aftercare model. We aimed to build on the gains made during inpatient treatment and reduce risk factors for future suicide attempt. Additionally, we sought to strengthen our partnership with an adolescent inpatient unit, creating an infrastructure for long‐term collaboration in suicide research. Twenty adolescents (80% female, 65% identified as African American), with mean age of 14.9 years, and a parent/caregiver were recruited from inpatient care following a suicide attempt. Of the parents, 8 (40%) had an income under $30,000, 14 (70%) were single or separated/divorced, and 7 (35%) had no more than a high school education. Families were randomised to 16 weeks of either ABFT or Enhanced Usual Care (EUC). As a result of variety of means to build a relationship with a local psychiatric hospital (meeting with hospital staff, holding case conferences, quick response time to referrals [intake within 48 hours of discharge], follow‐up post referral, and hosting free educational presentations) we were able to successfully join with the hospital and create a lasting research infrastructure to support future research projects. ABFT was a welcomed option by all of the social workers, nurses, and psychiatrists on the inpatient unit. In terms of feasibility, we met our recruitment goals, the majority of families were interested in receiving family therapy (74% of those referred) and those that got ABFT attended sessions regularly (mean = 11.2 sessions). Additionally, we were able to collect weekly data from participants the majority of the time and collect post treatment data from 90% of the participants. Participants receiving ABFT indicated they were marginally statistically significantly more satisfied with treatment than those receiving EUC (t(12)=2.02, p=0.07). Related to effectiveness, results show that compared to EUC, ABFT was marginally significantly more effective at preventing future suicide attempts (0% ABFT, 16.7% EUC Chi(1)=3.60, p=0.058; Fisher’s exact p=0.206), reducing attachment related avoidance for mothers (F(1,9)=3.85, p=0.08), and ABFT participants received treatment faster than EUC participants (t(6)=‐2.09, p=.08). Additionally, ABFT compared to EUC, was statistically more effective at reducing attachment related anxiety for fathers (F(1,3)=12.33, p=0.04). Overall, the results of this study demonstrate that ABFT is both a feasible and acceptable treatment as aftercare for youth with a suicide attempt after discharge from inpatient care." |
Fischer 2013.
| Study name | Short‐term psychotherapeutic treatment in adolescents engaging in non‐suicidal self‐injury. Trial Registration Number: DRKS00003605. |
| Methods |
Allocation: single‐blinded randomisation. Design: single‐centre (community adolescent mental health clinic). Setting: community. Follow‐up period: 6 months post line. Location: Heidelberg, Germany. |
| Participants | Male and female adolescents, between 12 and 17 years of age, who had engaged in five or more episodes of nonsuicidal self‐injury in the 6 months prior to randomisation, with at least one episode within the one month prior to screening, will be included in this trial. Expected N: 80. |
| Interventions | Participants randomised to the experimental group will receive a crisis card and 8‐12 weekly sessions of individual psychotherapy using the German version of the Cutting Down Programme. |
| Outcomes |
Primary outcome: 50% (or more) reduction in frequency of self‐harm as assessed by the Self‐Injurious Thoughts and Behaviors Interview‐German version. Secondary outcomes: scores on the Beck Depression Inventory, scores on the KIDSCREEN well being scale, and scores on the Self‐Esteem scale. |
| Starting date | November, 2012. Proposed end date: May, 2015. |
| Contact information |
Name: Dr. Michael Kaess (PI). Affiliation: Department of Child and Adolescent Psychiatry, Center of Psychosocial Medicine, University of Heidelberg. email:michael.kaess@med.uni-heidelberg.de |
| Notes | Dr. Michael Kaess very kindly provided unpublished information relating to this trial. |
Linehan 2014.
| Study name | Collaborative Adolescent Research on Emotions and Suicide (CARES). Trial Registration Number: NCT01528020. |
| Methods |
Allocation: single‐blind randomisation. Design: multi‐centre (community clinics). Setting: community outpatient clinics. Location: Seattle, WA and Los Angeles, CA, USA. |
| Participants | Males and females, between 12 and 18 years of age, diagnosed with emotional dysregulation, who made a suicide attempt and/or engaged in self‐harm within 6 months prior to randomisation will be eligible for inclusion in this study. |
| Interventions | Individuals randomised to the experimental group will receive dialectical behavior therapy and individual and group supportive therapy. |
| Outcomes |
Primary outcomes: repetition of any suicidal behaviour, defined as a suicide attempt, suicide, or self‐injury with suicide intent or ambivalent intent as measured by the SASII, admission to the emergency department or inpatient psychiatric facilities for suicidality as measured by the Columbia Classification Algorithm of Suicide Assessment, days successfully retained in treatment, and quality of family relationships as measured by the child bipolar questionnaire. Secondary outcomes: number of episodes of non‐suicidal self‐injury as measured by the SASII, the highest medical risk and risk/rescue score as measured by the SASII, number of suicidal threats made measured by the Suicide Behaviors Questionnaire‐Revised, and the level of suicidal ideation as measured by the Suicide Ideation Questionnaire‐Junior, number who drop‐out of treatment prematurely, number of treatment sessions attended, number of times late to treatment sessions, number of times treatment sessions left early, scores on the adolescent global functioning scale of the Children's Global Assessment Scale, scores on the depression scale of the Children's Depression Inventory, scores on the anger control, bullying, emotional self‐control, aggression, emotion regulation, and resiliency scales of the Behavior Assessment System for Children, Second Edition, Buss Perry Aggression Questionnaire, and Difficulties in Emotion Regulation Scale, scores on the impulsiveness and substance abuse scales of the Barratt Impulsiveness Scale, and the Daily Drinking Questionnaire, scores on the social adjustment scale of the Social Adjustment Scale–Self‐Report, and school attendance as measured by school records. |
| Starting date | January, 2012. Proposed End Date: January, 2016. |
| Contact information |
Name: Prof. Marsha M. Linehan (PI). Affiliation: Behavioural Research and Therapy Clinics, University of Washington. email:linehan@uw.edu |
| Notes | Ms. Elaine Franks, personal assistant to Marsha Linehan, very kindly provided unpublished information relating to this trial. Ms. Franks also provided the following note about this trial: "...insufficient males have been enrolled and will be removed from the final data set and later presented as a sub‐study." |
NSSI: non‐suicidal self injury SASII: Suicide Attempt Self Injury Interview
Differences between protocol and review
In the original protocol for this review, we planned to assess dichotomous outcome data (i.e., repetition of self‐harm and suicide) using the Peto odds ratio. Following revisions to iterations of the Cochrane Handbook (Higgins 2011) and new statistical advice, however, we have instead used the Mantel‐Haenszel method in this update. For this version of the review we have also expanded the range of outcomes assessed to include depression, hopelessness, problem‐solving, and suicidal ideation. We have also used the I2 statistic, rather than the Chi2 test, to summarise between‐study heterogeneity in this version in light of revisions to the Cochrane Handbook (Higgins 2011).
We also planned to assess methodological quality of included trials by the means recommended by the contemporary version of the Cochrane Handbook (Higgins 2011). For this version of the review we have therefore created 'Risk of bias' and 'Summary of findings' tables as per current recommendations. We have also refined the unit of analysis section, as per current recommendations, to include Zelen designed trials and trials that report adjusted effect sizes.
We have also added three sensitivity analyses: one for trials which employed Zelen's method of randomisation; one for trials that contributed to substantial (> 75%) levels of heterogeneity; and a third for trials that included a small minority (< 15%) of adult participants. Given the increasing use of enhanced usual care, rather than TAU, in trials in this area, we also added one sub‐group analysis to determine whether comparator choice influenced the pattern of results observed.
As we were unable to rank outcomes in a hierarchy in the present review, and given the absence of consensus rankings particularly for hopelessness, suicidal ideation, and problem‐solving, we have instead used the most common measure in any meta‐analysis and report results from any other measure in the text of the review. In future updates of this review, we will adopt any accepted outcome hierarchies.
Contributions of authors
KH had the idea for the review. All authors extracted data and assessed risk of bias for included studies. Both TTS and KW conducted the statistical analyses. KH, TTS, and KW wrote the initial version of the report and all authors contributed to the writing of drafts. All authors also approved the final version of the review for publication.
Sources of support
Internal sources
University Department of Psychiatry, Warneford Hospital, Oxford, UK
Oxford Health NHS Foundation Trust, UK
External sources
NHS Executive Anglia and Oxford Research and Development Program, UK
NIHR Service Delivery and Organisation programme, UK
Personal funding to KH as an NIHR Senior Investigator, UK
Declarations of interest
PH is the author of one of the trials included in the review.
Edited (no change to conclusions)
References
References to studies included in this review
Cooney 2010 {published and unpublished data}
- Cooney E, Davis K, Thompson P, Wharewera-Mika J, Stewart J. Feasibility of evaluating DBT for self-harming adolescents: A small randomised controlled trial. Auckland, New Zealand: Te Pou o Te Whakaaro Nui and The National Centre of Mental Health Research, Information and Workforce Development, 2010. [Google Scholar]
Cotgrove 1995 {published data only}
- Cotgrove A, Zirnisky L, Black D, Weston D. Secondary prevention of attempted suicide in adolescence. Journal of Adolescence 1995;18:569-77. [Google Scholar]
Donaldson 2005 {published data only}
- Donaldson D, Spirito A, Esposito-Smythers C. Treatment for adolescents following a suicide attempt: Results of a pilot trial. Journal of the American Academy of Child and Adolescent Psychiatry 2005;44:113-20. [DOI] [PubMed] [Google Scholar]
- Donaldson D, Spirito A, Overholser J. Treatment of adolescent suicide attempters. In: Spirito A, Overholser JC, editors(s). Evaluating and Treating Adolescent Suicide Attempters: From Research to Practice. San Diego, CA: Academic Press, 2003:295-321. [Google Scholar]
Green 2011 {published data only}20496110
- Green JM, Wood AJ, Kerfoot MJ, Trainor G, Roberts C, Rothwell J, et al. Group therapy for adolescents with repeated self harm: randomised controlled trial with economic evaluation. British Medical Journal 2011;342:d682. [DOI] [PMC free article] [PubMed] [Google Scholar]
Harrington 1998 {published data only}
- Aglan A, Kerfoot M, Pickles A. Pathways from adolescent deliberate self-poisoning to early adult outcomes: a six-year follow-up. Journal of Child Psychology and Psychiatry 2008;49(5):508-15. [DOI] [PubMed] [Google Scholar]
- Byford S, Harrington R, Torgerson D, Kerfoot M, Dyer E, Harrington V, et al. Cost-effectiveness analysis of a home-based social work intervention for children and adolescents who have deliberately poisoned themselves: Results of a randomised controlled trial. The British Journal of Psychiatry 1999;174:56-62. [DOI] [PubMed] [Google Scholar]
- Chitsabesan P, Harrington R, Harrington V, Tomenson B. Predicting repeat self-harm in children: How accurate can we expect to be? European Child and Adolescent Psychiatry 2003;12:23-9. [DOI] [PubMed] [Google Scholar]
- Harrington R, Kerfoot M, Dyer E, McNiven F, Gill J, Harrington V, et al. Deliberate self-poisoning in adolescence: why does a brief family intervention work in some cases and not others? Journal of Adolescence 2000;23(1):13-20. [DOI] [PubMed] [Google Scholar]
- Harrington R, Kerfoot M, Dyer E, McNiven F, Gill J, Harrington V, Woodham A, Byford S. Randomized trial of a home-based family intervention for children who have deliberately poisoned themselves. Journal of the American Academy of Child and Adolescent Psychiatry 1998;37:512-8. [PubMed] [Google Scholar]
- Harrington R, Pickles A, Aglan A, Harrington V, Burroughs H, Kerfoot M. Early adult outcomes of adolescents who deliberately poisoned themselves. Journal of the American Academy of Childand Adolescent Psychiatry 2006;45:337-45. [DOI] [PubMed] [Google Scholar]
Hazell 2009 {published data only}
- Hazell PL, Martin G, McGill K, Kay T, Wood A, Trainor G, et al. Group therapy for repeated deliberate self-harming adolescents: Failure of replication of a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48:662-70. [DOI] [PubMed] [Google Scholar]
Mehlum 2014 {published and unpublished data}
- Mehlum L, Tømoen AJ, Ramberg M, Haga E, Diep LM, Laberg S, et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior - a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry 2014;53:1082-91. [DOI] [PubMed] [Google Scholar]
Ougrin 2011a {published and unpublished data}81605131
- Ougrin D, Boege I, Stahl D, Banarsee R, Taylor E. Randomised controlled trial of therapeutic assessment versus usual assessment in adolescents with self-harm: 2-year follow-up. Archives of Diseases in Childhood 2013;98:772-6. [DOI] [PubMed] [Google Scholar]
- Ougrin D, Zundel T, Kyriakopoulos M, Banarsee R, Stahl D, Taylor E. Adolescents with suicidal and nonsuicidal self-harm: Clinical characteristics and response to therapeutic assessment. Psychological Assessment 2012;24:11-20. [DOI] [PubMed] [Google Scholar]
- Ougrin D, Zundel T, Ng A, Banarsee R, Bottle A, Taylor E. Trial of therapeutic assessment in London: Randomised controlled trial of therapeutic assessment versus standard psychosocial assessment in adolescents presenting with self-harm. Archives of Disease in Childhood 2011;96:148-53. [DOI] [PubMed] [Google Scholar]
Rossouw 2012a {published and unpublished data}95266816
- Rossouw T. Self-harm in young people: Is MBT the answer? In: Midgley N, Vrouva I, editors(s). Minding the child: Mentalization-based interventions with children, young people and their families. New York, NY: Routledge, 2012:131-44. [Google Scholar]
- Rossouw TI, Fonagy P. Mentalization-based treatment for self-harm in adolescents: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry 2012;51:1304-13. [DOI] [PubMed] [Google Scholar]
Spirito 2002 {published data only}
- Spirito A, Boergers J, Donaldson D, Bishop D, Lewander W. An intervention trial to improve adherence to community treatment by adolescents after a suicide attempt. Journal of Child and Adolescent Psychiatry 2002;41:435-42. [DOI] [PubMed] [Google Scholar]
- Spirito A, Stanton C, Donaldson D, Boergers J. Treatment-as-usual for adolescent suicide attempters: Implications for the choice of comparison groups in psychotherapy research. Journal of Clinical Child and Adolescent Psychology 2002;31:41-7. [DOI] [PubMed] [Google Scholar]
Wood 2001a {published data only}
- Wood A, Trainor G, Rothwell J, Moore A, Harrington R. Randomized trial of group therapy for repeated deliberate self-harm in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 2001;40:1246-53. [DOI] [PubMed] [Google Scholar]
- Wood A, Trainor G. Developmental group psychotherapy for adolescents: A manual for mental health professionals. Manchester, UK: University of Manchester, 2001. [Google Scholar]
References to studies excluded from this review
Asarnow 2011 {published data only}
- Asarnow JR, Porta G, Spirito A, Emslie G, Clarke G, Wagner KD, et al. Suicide attempts and nonsuicidal self-injury in the treatment of resistant depression in adolescents: Findings from the TORDIA Study. Journal of the American Academy of Child and Adolescent Psychiatry 2011;50:772-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bjärehed 2013 {published data only}
- Bjärehed J, Pettersson K, Wångby-Lundh M, Lundh LG. Examining the acceptability, attractiveness, and effects of a school-based validating interview for adolescents who self-injure. The Journal of School Nursing 2014;29:225-34. [DOI] [PubMed] [Google Scholar]
Brent 2009 {published data only}
- Brent DA, Greenhill LL, Compton S, Emslie G, Wells K, Walkup JT, et al. The treatment of adolescent suicide attempters study (TASA): Predictors of suicidal events in an open treatment trial. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48:987-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Carli 2011 {published data only}
- Carli V, Sarchiapone M, Wasserman D on behalf of the SEYLE Research Consortium. Saving and Empowering Young Lives in Europe (SEYLE): Preliminary results. European Psychiatry 2011;26:s520. [Google Scholar]
- Carli V, Wasserman C, Wasserman D, Sarchiapone M, Apter A, Balazs J, et al. The Saving and Empowering Young Lives in Europe (SEYLE) randomised controlled trial (RCT): Methodological issues and participant characteristics. BMC Public Health 2013;13:479. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deykin 1986 {published data only}
- Deykin EY, Hsieh CC, Joshi N, McNamarra JJ. Adolescent suicidal and self-destructive behavior. Results of an intervention study. Journal of Adolescent Health Care 1986;7:88-95. [DOI] [PubMed] [Google Scholar]
Diamond 2010 {published data only}
- Diamond GS, Wintersteen MB, Brown GK, Diamond GM, Gallop R, Shelef K, et al. Attachment-based family therapy for adolescents with suicidal ideation: A randomized controlled trial. American Academy of Child and Adolescent Psychiatry 2010;49:122-31. [DOI] [PubMed] [Google Scholar]
Donaldson 1997 {published data only}
- Donaldson D, Spirito A, Arrigan M, Aspel JW. Structured disposition planning for adolescent suicide attempters in a general hospital: Preliminary findings on short-term outcome. Archives of Suicide Research 1997;3(4):271-282. [Google Scholar]
Dubois 1999 {published data only}
- Dubois L, Walter M, Bleton L, Genest P, Lemonnier E, Lachevre G. Evaluation of a comparative and prospective protocol for suicidal youth: Analysis of psychiatric diagnosis, therapeutic compliance and rate of recurrence over one year (preliminary results) [Evaluation comparative et prospective d'un protocole de prise en charge specifique de jeunes suicidants: Analyse du diagnostic psychiatrique initial, de l'observance therapeutique et du taux de recidive a un an (resultats preliminaires)]. Annales Medico-Psychologiques 1999;157:557-61. [Google Scholar]
Emslie 2006a {published data only}
- Emslie G, Kratochvil C, Vitiello B, Silva S, Mayes T, McNulty S, et al. Treatment for adolescents with depression study (TADS): Safety results. Journal of the American Academy of Child and Adolescent Psychiatry 2006;45:1440-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- March JS, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, et al. The treatment for adolescents with depression study (TADS). Archives of General Psychiatry 2007;64:1132-44. [DOI] [PubMed] [Google Scholar]
Emslie 2006b {published data only}
- Emslie GJ, Wagner KD, Sutcher S, Krulewicz S, Fong R, Carpenter DJ, et al. Paroxetine treatment in children and adolescents with major depressive disorder: A randomized, multicenter, double-blind, placebo-controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry 2006;45:709-19. [DOI] [PubMed] [Google Scholar]
Emslie 2007 {published data only}
- Emslie GJ, Findling RL, Yeung PP, Kunz NR, Li Y. Venlafaxine ER for the treatment of pediatric subjects with depression: Results of two placebo-controlled trials. Journal of the American Academy of Child and Adolescent Psychiatry 2007;46:479-88. [DOI] [PubMed] [Google Scholar]
Emslie 2009 {published data only}
- Emslie GJ, Ventura D, Korotzer A, Tourkodimitris S. Escitalopram in the treatment of adolescent depression: A randomized placebo-controlled multisite trial. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48:721-9. [DOI] [PubMed] [Google Scholar]
Esposito‐Smythers 2006 {published data only}
- Esposito-Smythers C, Spirito A, Uth R, LaChance H. Cognitive behavioral treatment for suicidal alcohol abusing adolescents: Development and pilot testing. The American Journal on Addictions 2006;15:126-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Esposito‐Smythers 2011 {published data only}
- Esposito-Smythers C, Spirito, A, Kahler CW, Hunt J, Monti P. Treatment of co-occurring substance abuse and suicidality among adolescents: A randomized trial. Journal of Consulting and Clinical Psychology 2010;79:728-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
Findling 2009 {published data only}
- Findling RL, Nyilas M, Forbes RA, McQuade RD, Jin N, Iwamoto T, et al. Acute treatment of pediatric bipolar I disorder, manic or mixed episode, with aripiprazole: A randomized, double-blind, placebo-controlled study. Journal of Clinical Psychiatry 2009;70:1441-51. [DOI] [PubMed] [Google Scholar]
Fleischhaker 2005 {published data only}
- Fleischhaker C, Böhme R, Sixt B, Brück C, Schneider C, Schulz E. Dialectical Behavioral Therapy for Adolescents (DBT-A): A clinical trial for patients with suicidal and self-injurious behavior and borderline symptoms with a one-year follow-up. Child and Adolescent Psychiatry and Mental Health 2011;5:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleischhaker C, Böhme R, Sixt B, Schulz E. Suicidal, parasuicidal and self injurious behavior in patients with borderline symptoms. First data of a pilot study on dialectical-behavioral therapy for adolescents (DBT-A). Kindheit und Entwicklung 2005;2:112-27. [Google Scholar]
- Fleischhaker C, Munz M, Bohme R, Sixt B, Schulz E. Dialectical behaviour therapy for adolescents (DBT-A): A pilot study on the therapy of suicidal, parasuicidal, and self-injurious behaviour in female patients with a borderline disorder. Zeitschrift fur Kinderund Jugendpsychiatrie und Psychotherapie 2006;1:15-27. [DOI] [PubMed] [Google Scholar]
Huey 2004 {published data only}
- Henggeler SW, Rowland MD, Randall J, Ward DM, Pickrel SG, Cunningham PB, et al. Home-based multisystemic therapy as an alternative to the hospitalization of youths in psychiatriccrisis: Clinical outcomes. Journal of the American Academy of Child & Adolescent Psychiatry 1999;38(11):1331–9. [DOI] [PubMed] [Google Scholar]
- Huey S, Henggeler S, Rowland M, Halliday-Boykins C, Cunningham P, Pickrel S. Predictors of treatment response for suicidal youth referred for emergency psychiatric hospitalization. Journal of Clinical Child and Adolescent Psychology 2005;34:582-9. [DOI] [PubMed] [Google Scholar]
- Huey SJ, Henggeler SW, Rowland MD, Halliday-Boykins CA, Cunningham PB, Pickerl SG, et al. Multisystemic therapy effects on attempted suicide by youths presenting psychiatric emergencies. Journal of the American Academy of Child and Adolescent Psychiatry 2004;43:183-90. [DOI] [PubMed] [Google Scholar]
King 2006 {published data only}
- King CA, Kramer A, Preuss L, Kerr DCR, Weisse L, Venkataraman S. Youth-nominated support team for suicidal adolescents (Version 1): A randomized controlled trial. Journal of Consulting and Clinical Psychology 2006;74:199-206. [DOI] [PubMed] [Google Scholar]
King 2009 {published data only}
- King CA, Klaus N, Kramer A, Venkataraman S, Quinlan P, Gillespie B. The youth-nominated support team – Version II for suicidal adolescents: A randomized controlled intervention trial [NCT00071617]. Journal of Consulting and Clinical Psychology 2009;77:880-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
Miller 2000 {published data only}
- Miller AL, Glinski J. Youth suicidal behavior: Assessment and intervention. Journal of Clinical Psychology 2000;56:1131-52. [DOI] [PubMed] [Google Scholar]
Nixon 2003 {published data only}
- Nixon MK, Cheng M, Cloutier P. An open trial of auricular acupuncture for the treatment of repetitive self-injury in depressed adolescents. The Canadian Child and Adolescent Psychiatry Review 2003;12:10-12. [PMC free article] [PubMed] [Google Scholar]
Oldershaw 2012 {published data only}
- Oldershaw A, Simic M, Grima E, Jollant F, Richards C, Taylor L, et al. The effect of cognitive behavior therapy on decision making in adolescents who self-harm: A pilot study. Suicide and Life-Threatening Behavior 2012;42:255-65. [DOI] [PubMed] [Google Scholar]
Pineda 2013 {published data only}
- Pineda J, Dadds MR. Family intervention for adolescents with suicidal behavior: A randomized controlled trial and mediation analysis. Journal of the American Academy of Child and Adolescent Psychiatry 2013;52:851-62. [DOI] [PubMed] [Google Scholar]
Podobnik 2012 {published data only}
- Podobnik J, Foller Podobnik I, Grgic N, Marcinko D, Pivac N. The effect of add-on treatment with quetiapine on measures of depression, aggression, irritability and suicidal tendencies in children and adolescents. Psychopharmacology 2012;220:639-41. [DOI] [PubMed] [Google Scholar]
Ramani Perera 2011 {published and unpublished data}
- Ramani Perera EA, Kathriarachchi ST. Problem-solving counseling as a therapeutic tool on youth suicidal behavior in the suburban population in Sri Lanka. Indian Journal of Psychiatry 2011;53:30-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Robinson 2012 {published data only}
- Robinson J, Hetrick S, Gook S, Cosgrave E, Yuen HP, McGorry P, et al. The development of a randomised controlled trial testing a postcard intervention designed to reduce suicide risk among young help-seekers. BMC Psychiatry 2009;9:Art ID 59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson J, Yuen HP, Gook S, Hughes A, Cosgrave E, Killackey E, et al. Can receipt of a regular postcard reduce suicide-related behaviour in young help seekers? A randomized controlled trial. Early Intervention in Psychiatry 2012;6:145-52. [DOI] [PubMed] [Google Scholar]
Robinson 2014 {published data only}
- Robinson J, Hetrick S, Cox G, Bendall S, Yung A, Yuen HP, et al. The development of a randomised controlled trial testing the effects of an online intervention among school students at risk of suicide. BMC Psychiatry 2014;14:155. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rotheram‐Borus 1996 {published data only}
- Rotheram-Borus MJ, Piacentini J, Rossem R, Graae F, Cantwell C, Castro-Blanco D, et al. Enhancing treatment adherence with a specialized emergency room program for adolescent suicide attempters. Journal of the American Academy of Child and Adolescent Psychiatry 1996;35:654-63. [DOI] [PubMed] [Google Scholar]
Sarchiapone 2013 {published data only}
- Basilico F, Carli V, Iosue M, d'Aulerio M, di Domenico A, Recchia L, et al. Internet and the media for the prevention of suicide among European youngs. European Psychiatry 2012;27:Art P-1410. [Google Scholar]
- Sarchiapone M. The use of Internet in prevention. European Psychiatry 2013;28:Art 3026. [Google Scholar]
Vitiello 2009 {published data only}
- Stanley B, Brown G, Brent DA, Wells K, Poling K, Curry J, et al. Cognitive-behavioral therapy for suicide prevention (CBT-SP): Treatment model, feasibility, and acceptability. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48:1005-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vitiello B, Brent DA, Greenhill LL, Emslie G, Wells K, Walkup JT, et al. Depressive symptoms and clinical status during the Treatment of Adolescent Suicide Attempters (TASA) study. Journal of the American Academy of Child & Adolescent Psychiatry 2009;10:997-1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wilkinson 2011 {published data only}
- Wilkinson P, Kelvin R, Roberts C, Dubicka B, Goodyer I. Clinical and psychosocial predictors of suicide attempts and nonsuicidal self-injury in the Adolescent Depression Antidepressants and Psychotherapy Trial (ADAPT). American Journal of Psychiatry 2011;168:495-501. [DOI] [PubMed] [Google Scholar]
Xu 2006 {published data only}
- Xu J, Fu YX, Du ZH. Effect of psychological intervention on adolescent suicide attempters. Journal of Community Medicine 2006;4:7-9. [Google Scholar]
References to ongoing studies
Asarnow 2014 {unpublished data only}
- Asarnow JR. Effectiveness of a Family-Based Intervention for Adolescent Suicide Attempters (The SAFETY Study). https://clinicaltrials.gov/ct2/show/NCT00692302 (Accessed 13 September 2015). [Google Scholar]
Cottrell 2014 {unpublished data only}59793150
- Cottrell D. SHIFT Trial - Family therapy vs treatment as usual for young people seen after second or subsequent episodes of self-harm. http://www.controlled-trials.com/ISRCTN59793150 (Accessed 13 September 2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
Diamond 2014 {unpublished data only}
- Diamond GS. Family Therapy as Hospital Aftercare for Adolescent Suicide Attempters. https://clinicaltrials.gov/ct2/show/NCT01195740 (Accessed 13 September 2015). [Google Scholar]
Fischer 2013 {published and unpublished data}
- Fischer G, Brunner R, Parzer P, Resch F, Kaess M. Short-term psychotherapeutic treatment in adolescents engaging in non-suicidal self-injury: A randomized controlled trial. Trials 2013;14:294. [DOI] [PMC free article] [PubMed] [Google Scholar]
Linehan 2014 {unpublished data only}
- Linehan MM, McCauley EA, Asarnow J, Berk M. Collaborative Adolescent Research on Emotions and Suicide (CARES). https://clinicaltrials.gov/ct2/show/NCT01528020 (Accessed 13 September 2015). [Google Scholar]
Additional references
Albrecht 2014
- Albrecht B, Staiger PK, Hall K, Miller P, Best D, Lubman DI. Benzodiazepine use and aggressive behaviour: A systematic review. Australian and New Zealand Jounral of Psychiatry 2014;48:1096-114. [DOI] [PubMed] [Google Scholar]
American Psychiatric Association 2013
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Association, 2013. [Google Scholar]
Andover 2012
- Andover MS, Morris BW, Wren A, Bruzzese ME. The co-occurance of non-suicidal self-injury and attempted suicide among adolescents: Distinguishing risk factors and psychosocial correlates. Child and Adolescent Psychiatry and Mental Health 2012;6:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Angold 1995
- Angold A, Costello EJ, Messer SC, Pickles A. The development of a short questionnaire for use in epidemiological studies in depression in children and adolescents. International Journal of Methods in Psychiatric Research 1995;5:237-49. [Google Scholar]
Bateman 2004
- Bateman A, Fonagy P. Mentalization-based treatment of BDP. In: Psychotherapy for borderline personality disorder: Mentalization-based treatment. Oxford, UK: Oxford University Press, 2004. [Google Scholar]
Beck 1961
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry 1961;4:561. [DOI] [PubMed] [Google Scholar]
Beck 1974
- Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: The Hopelessness Scale. Journal of Consulting and Clinical Psychology 1974;42:861-865. [DOI] [PubMed] [Google Scholar]
Beck 1988
- Beck AT, Steer RA, Ranieri WF. Scale for Suicide Ideation: Psychometric properties of a self-report version. Journal of Clinical Psychology 1988;44:499-505. [DOI] [PubMed] [Google Scholar]
Beck 1991
- Beck AT. Beck Scale for Suicide Ideation: Manual. San Antonio, TX: Psychological Corporation, 1991. [Google Scholar]
Bennewith 2002
- Bennewith O, Stocks N, Gunnell D, Peters TJ, Evans MO, Sharp DJ. General practice based intervention to prevent repeat episodes of deliberate self harm: Cluster randomised controlled trial. British Medical Journal 2002;324:1254-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boyce 2003
- Boyce P, Carter G, Penrose-Wall J, Wilhelm K, Goldney R. Summary Australian and New Zealand clinical practice guideline for the management of adult deliberate self-harm. Australasian Psychiatry 2003;11:150-5. [Google Scholar]
Brausch 2012
- Brausch AM, Girresch SK. A review of empirical treatment studies for adolescent nonsuicidal self-injury. Journal of Cognitive Psychotherapy: An International Quarterly 2012;26:3-18. [Google Scholar]
Brent 2013
- Brent DA, McMakin DL, Kennard BD, Goldstein TR, Mayes TL, Douaihy AB. Protecting adolescents from self-harm: A critical review of intervention studies. Journal of the American Academy of Child and Adolescent Psychiatry 2013;52:1260-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brunner 2002
- Brunner J, Parhofer KG, Schwandt P, Bronisch T. Cholesterol, essential fatty acids, and suicide. Pharmacopsychiatry 2002;35:1-5. [DOI] [PubMed] [Google Scholar]
Burns 2000
- Burns JM, Patton GC. Preventive interventions for youth suicide: A risk factor-based approach. Australian and New Zealand Journal of Psychiatry 2000;34:388-407. [DOI] [PubMed] [Google Scholar]
Burrows 2010
- Burrows S, Laflamme L. Socioeconomic disparities and attempted suicide: State of knowledge and implications for research and prevention. International Journal of Injury Control and Safety Promotion 2010;17:23-40. [DOI] [PubMed] [Google Scholar]
Carter 2007
- Carter M, McGee R, Taylor B, Williams S. Health outcomes in adolescence: Associations with family, friends and school engagement. Journal of Adolescence 2007;30:51-62. [DOI] [PubMed] [Google Scholar]
Choi‐Kain 2008
- Choi-Kain LW, Gunderson JG. Mentalization: Ontogeny, assessment, and application in the treatment of borderline personality disorder. The American Journal of Psychiatry 2008;165:1127-35. [DOI] [PubMed] [Google Scholar]
Christensen 2014
- Christensen H, Calear AL, Spijker B, Gosling J, Petrie K, Donker T, et al. Psychosocial interventions for suicidal ideation, plans, and attempts: A database of randomised controlled trials. BMC Psychiatry 2014;14:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cipriani 2013
- Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: Updated systematic review and meta-analysis. British Medical Journal 2013;346:f3646. [DOI] [PubMed] [Google Scholar]
Craig 2008
- Craig N, Dieppe P, MacIntyre S, Mitchie S, Nasareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidence. British Medical Journal 2008;337:a1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
Crowell 2012
- Crowell SE, Beauchaine TP, Hsiao RC, Wasilev CA, Yaptangco M, Linehan MM. Differentiating adolescent self-injury from adolescent depression: Possible implications for borderline personality development. Journal of Abnormal Child Psychology 2012;40:45-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
Curtin 2002a
- Curtin F, Elbourne D, Altman DG. Meta-analysis combining parallel and cross-over clinical trials. III: The issue of carry-over. Statistics in Medicine 2002;21:2161-73. [DOI] [PubMed] [Google Scholar]
Curtin 2002b
- Curtin F, Altman DG, Elbourne D. Meta-analysis combining parallel and cross-over clinical trials. I: Continuous outcomes. Statistics in Medicine 2002;21:2131-44. [DOI] [PubMed] [Google Scholar]
D'Zurilla 2010
- D'Zurilla TJ, Nezu AM. Problem-solving therapy. In: Dobson KS, editors(s). Handbook of Cognitive-Behavioral Therapies. 3rd edition. New York, NY: The Guilford Press, 2010:197-225. [Google Scholar]
Daine 2013
- Daine K, Hawton K, Singaravelu V, Stewart A, Simkin S, Montgomery P. The power of the Web: A systematic review of studies of the influence of the Internet on self-harm and suicide in young people. PLoS One 2013;8:e77555. [DOI] [PMC free article] [PubMed] [Google Scholar]
Daniel 2009
- Daniel SS, Goldston DB. Interventions for suicidal youth: A review of the literature and developmental considerations. Suicide and Life-Threatening Behavior 2009;39:252-268. [DOI] [PMC free article] [PubMed] [Google Scholar]
Donner 2002
- Donner A, Klar N. Issues in the meta-analysis of cluster randomized trials. Statistics in Medicine 2002;21:2971-80. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. British Medical Journal 1997;315:629-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington HV, Vail A. Meta-analyses involving cross-over trials: Methodological issues. International Journal of Epidemiology 2002;31:140-49. [DOI] [PubMed] [Google Scholar]
Engles 2003
- Engles JM, Diehr P. Imputation of missing longitudinal data: A comparison of methods. Journal of Clinical Epidemiology 2003;56:968-76. [DOI] [PubMed] [Google Scholar]
Erez 1996
- Erez A, Bloom MC, Wells MT. Using random rather than fixed effects models in meta-analysis: Implications for situation specificity and validity generalization. Personnel Psychology 1996;49:275-306. [Google Scholar]
Evans 2004
- Evans E, Hawton K, Rodham K. Factors associated with suicidal phenomena in adolescents: A systematic review of population-based studies. Clinical Psychology Review 2004;24:957-79. [DOI] [PubMed] [Google Scholar]
Evans 2005
- Evans J, Evans M, Morgan HG, Hayward A, Gunnell D. Crisis card following self-harm: 12-month follow-up of a randomised controlled trial. British Journal of Psychiatry 2005;187:186-7. [DOI] [PubMed] [Google Scholar]
Feighner 1999
- Feighner JP. Mechanism of action of antidepressant medications. Journal of Clinical Psychiatry 1999;60:s4-s11. [PubMed] [Google Scholar]
Fleiss 1994
- Fleiss, JL. Measures of effect size for categorical data. In: Cooper H, Hedges LV, editors(s). The Handbook of Research Synthesis. New York, NY: Russell Sage Foundation, 1994:245-260. [Google Scholar]
Fond 2014
- Fond G, Loundou A, Rabu C, MacGregor A, Lançon C, Brittner M, et al. Ketamine administration in depressive disorders: A systematic review and meta-analysis. Psychopharmacology 2014;231:3663-76. [DOI] [PubMed] [Google Scholar]
Food and Drug Administration 2004
- US Food and Drug Administration. Relationship between psychotropic drugs and pediatric suicidality: Review and evaluation of clinical data. http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004-4065b1-10-TAB08-Hammads-Review.pdf (Accessed 18 September 2014).
Gonzales 2013
- Gonzales AH, Bergstrom L. Adolescent non-suicidal self-injury (NSSI) interventions. Journal of child and Adolescent Psychiatric Nursing 2013;26:124-30. [DOI] [PubMed] [Google Scholar]
Good 2006
- Good CR. Adjunctive quetiapine targets self-harm behaviors in adolescent females with major depressive disorder. Journal of Child and Adolescent Psychopharmacology 2006;16:235-6. [DOI] [PubMed] [Google Scholar]
Gould 2003
- Gould MS, Greenberg T, Velting DM, Shaffer D. Youth suicide risk and preventive interventions: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry 2003;42:386-405. [DOI] [PubMed] [Google Scholar]
GRADEpro [Computer program]
- GRADEpro. Version 24 September 2014. McMaster University, 2014.
Granboulan 2001
- Granboulan V, Roudot-Thoraval F, Lemerle S, Alvin P. Predictive factors of post-discharge follow-up care among adolescent suicide attempters. Acta Psychiatrica Scandinavica 2001;104:31-36. [DOI] [PubMed] [Google Scholar]
Hawton 2002
- Hawton K, Rodham K, Evans E, Weatherall R. Deliberate self-harm in adolescents: Self report survey in schools in England. British Medical Journal 2002;325:1207-1211. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hawton 2003
- Hawton K, Harriss L, Hall S, Simkin S, Bale E, Bond A. Deliberate self-harm in Oxford, 1990-2000: A time of change in patient characteristics. Psychological Medicine 2003;33:987-996. [DOI] [PubMed] [Google Scholar]
Hawton 2008a
- Hawton K, Harriss L. The changing gender ratio in occurrence of deliberate self-harm across the life-cycle. Crisis 2008;29:4-10. [DOI] [PubMed] [Google Scholar]
Hawton 2008b
- Hawton K, Harriss L. Deliberate self-harm by under-15-year-olds: characteristics, trends and outcome. Journal of Child Psychology and Psychiatry 2008;49:441-448. [DOI] [PubMed] [Google Scholar]
Hawton 2012a
- Hawton K, Saunders KEA, O'Connor R. Self-harm and suicide in adolescents. Lancet 2012;379:2373-2382. [DOI] [PubMed] [Google Scholar]
Hawton 2012b
- Hawton K, Bergen H, Waters K, Ness J, Cooper J, Steeg S, Kapur N. Epidemiology and nature of self-harm in children and adolescents: Findings from the multicentre study of self-harm in England. European Child and Adolescent Psychiatry 2012;21:369-377. [DOI] [PubMed] [Google Scholar]
Hawton 2012c
- Hawton K, Bergen H, Kapur N, Cooper J, Steeg S, Ness J, Waters K. Repetition of self-harm and suicide following self-harm in children and adolescents: Findings from the Multicentre Study of self-harm in England. Journal of Child Psychology and Psychiatry 2012;53:1212-1219. [DOI] [PubMed] [Google Scholar]
Hawton 2013
- Hawton, K, Saunders, K E A, Topiwala, A, Haw, C. Psychiatric disorders in patients presenting to hospital following self-harm: A systematic review. Journal of Affective Disorders 2013;151:821-830. [DOI] [PubMed] [Google Scholar]
Heppner 1988
- Heppner, P. The Problem-Solving Inventory. Palo Alto, CA: Consulting Psychologist Press, 1988. [Google Scholar]
Her Majesty's Government Department of Health 2012
- Her Majesty's Government / Department of Health. Preventing suicide in England: A cross-government outcomes strategy to save lives. London: Her Majesty's Government / Department of Health, 2012. [Google Scholar]
Higgins 2011
- Higgins JPT, Deeks JJ. Selecting studies and collecting data. In: Cochrane Handbook for Systematic Reviews of Interventions. Vol. Version 5.1.0. The Cochrane Colloboration: Available from www.cochrane-handbook.org, 2011. [Google Scholar]
Hinduja 2010
- Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of Suicide Research 2010;14:206-221. [DOI] [PubMed] [Google Scholar]
Hirsch 1982
- Hirsch S, Walsh C, Draper R. Parasuicide: A review of treatment interventions. Journal of Affective Disorders 1982;4:299-311. [DOI] [PubMed] [Google Scholar]
Hjelmeland 2002
- Hjelmeland H, Hawton K, Nordvik H, Bille-Brahe U, De Leo D, Fekete S, Grad O, Haring C, Kerkhof JF, Lönnqvist J, Michel K, Renberg ES, Schmidtke A, Heeringen K, Wasserman D. Why people engage in parasuicide: A cross-cultural study of intentions. Suicide and Life-Threatening Behavior 2002;32:380-393. [DOI] [PubMed] [Google Scholar]
Hopewell 2009
- Hopewell S, Loudon K, Clarke MJ, Oxman AD, Dickersin K. Publication bias in clinical trials due to statistical significance or direction of trial results. Cochrane Database of Systematic Reviews 2009;1:MR000006. [DOI] [PMC free article] [PubMed] [Google Scholar]
Huey 2004
- Hury Jr SJ, Henggeler SW, Rowland MD, Halliday-Boykins CA, Cunningham PB, Pickerl SG, Edwards J. Multisystemic therapy effects on attempted suicide by youths presenting psychiatric emergencies. Journal of the American Academy of Child and Adolescent Psychiatry 2004;43:183-90. [DOI] [PubMed] [Google Scholar]
Hunt 2013
- Hunt GE, Siegfried N, Morley K, Sitharthan T, Cleary M. Psychosocial interventions for people with both severe mental illness and substance misuse. Cochrane Database of Systematic Reviews 2013;10:CD001088. [DOI] [PubMed] [Google Scholar]
James 2008
- James AC, Taylor A, Winmill L, Alfoadari K. A preliminary community study of dialectical behavior therapy (DBT) with adolescent females demonstrating persistent, deliberate self-harm (DSH). Child and Adolescent Mental Health 2008;13:7. [DOI] [PubMed] [Google Scholar]
Jones 2012
- Jones C, Hacker D, Cormac I, Meaden A, Irving CB. Cognitive behavioural therapy versus other psychosocial treatments for schizophrenia. Cochrane Database of Systematic Reviews 2012;4:CD008712. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kandemir 2008
- Kandemir H, Yumru M, Kul M, Kandemir SB. Behavioural disinhibition, suicidal ideation, and self-mutilation related to clonazepam. Journal of Child and Adolescent Psychopharmacology 2008;18:409. [DOI] [PubMed] [Google Scholar]
Kapur 2010
- Kapur N, Cooper J, Bennewith O, Gunnell D, Hawton K. Postcards, green cards and telephone calls: Therapeutic contact with individuals following self-harm. British Journal of Psychiatry 2010;197:5-7. [DOI] [PubMed] [Google Scholar]
Kapur 2013
- Kapur N, Cooper J, O'Connor RC, Hawton K. Non-suicidal self-injury v. attempted suicide: New diagnosis or false dichotomy? British Journal of Psychiatry 2013;202:326-328. [DOI] [PubMed] [Google Scholar]
Kazdin 1986
- Kazdin AE, Rodgers A, Coibus D. The Hopelessness Scale for children: Psychometric characteristics and concurrent validity. Journal of Consulting and Clinical Psychology 1986;54:241-245. [DOI] [PubMed] [Google Scholar]
Kerry 1998
- Kerry SM, Bland JM. Analysis of a trial randomised in clusters. British Medical Journal 1998;316:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
King 2008
- King CA, Merchant CR. Social and interpersonal factors relating to adolescent suicidality: A review of the literature. Archives of Suicide Research 2008;12:181-196. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kreitman 1969
- Kreitman N, Philip AE, Greer S, Bagley CR. Parasuicide. British Journal of Psychiatry 1969;115:746-747. [DOI] [PubMed] [Google Scholar]
Lilley 2008
- Lilley R, Owens D, Horrocks J, House A, Noble R, Bergen H, Hawton K, Casey D, Simkin S, Murphy E, Cooper J, Kapur N. Hospital care and repetition following self-harm: Multicentre comparison of self-poisoning and self-injury. British Journal of Psychiatry 2008;192:440-445. [DOI] [PubMed] [Google Scholar]
Linehan 1991
- Linehan MM, Armstrong HE, Suarez A, Allmon D, Heard HL. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry 1991;48:1060-1064. [DOI] [PubMed] [Google Scholar]
Linehan 1993
- Linehan MM. Skills training manual for treating borderline personality disorder. New York, NY: Guildford Press, 1993. [Google Scholar]
Linehan 2007
- Linehan MM, Bohus M, Lynch TR. Dialectical behavior therapy for pervasive emotion dysregulation: Theoretical and practical underpinnings. In: Gross J, editors(s). Handbook of Emotion Regulation. New York, NY: Guilford Press, 2007:581-605. [Google Scholar]
Lu 2014
- Lu C, Zhang F, Lakoma MD, Madden JM, Rusinak D, Penford RB, Simon G, Ahmedani BK, Clarke G, Hunkeler EM, Waitzfelder B, Owen-Smith A, Raebel MA, Rossom R, Coleman KJ, Copeland LA, Soumerai SB. Changes in antidepressant use by young people and suicidal behavior after FDA warnings and media coverage: A quasi-experimental study. British Medical Journal 2014;348:g3596. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lynch 2006
- Lynch TR, Chapman AL, Rosenthal MZ, Kuo JR, Linehan MM. Mechanisms of change in dialectical behavior therapy: Theoretical and empirical observations. Journal of Clinical Psychology 2006;62:459-480. [DOI] [PubMed] [Google Scholar]
Madge 2008
- Madge N, Hewitt A, Hawton K, Wilde EJ, Corcoran P, Fekete S, Heeringen K, Leo A, Ystgaard M. Deliberate self-harm within an international community sample of young people: Comparative findings from the Child & Adolescent Self-harm in Europe (CASE) Study. The Journal of Child Psychology and Psychiatry 2008;49:667-677. [DOI] [PubMed] [Google Scholar]
Madge 2011
- Madge N, Hawton K, McMahon EM, Corcoran P, Leo D, Wilde EJ, Fekete S, Heeringen K, Ystgaard M, Arensman E. Psychological characteristics, stressful life events and deliberate self-harm: Findings from the Child and Adolescent Self-harm in Europe (CASE) study. European Child and Adolescent Psychiatry 2011;20:499-508. [DOI] [PubMed] [Google Scholar]
Mann 2013
- Mann JJ. The serotonergic system in mood disorders and suicidal behaviour. Philosophical Transactions ofThe Royal Society (B Biological Sciences) 2013;368:20120537. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marshall 2000
- Marshall M, Lockwood A, Bradley C, Adams C, Joy C, Fenton M. Unpublished rating scales: A major source of bias in randomised controlled trials of treatments for schizophrenia. British Journal of Psychiatry 2000;176:249-252. [DOI] [PubMed] [Google Scholar]
Maydeu‐Olivares 1996
- Maydeu-Olivares A, D'Zurilla TJ. A factor analytic study of the Social Problem-Solving Inventory: An integration of theory and data. Cognitive Therapy and Research 1996;20:115-133. [Google Scholar]
McMahon 2013
- McMahon EM, Corcoran P, Keeley H, Perry IJ, Arensman E. Adolescents exposed to suicidal behavior of others: Prevalence of self-harm and associated psychological, lifestyle, and life event factors. Suicide and Life-Threatening Behaviour 2013;43:634-645. [DOI] [PubMed] [Google Scholar]
McMahon 2014
- McMahon EM, Keeley H, Cannon M, Arensman E, Perry IJ, Clarke M, Chambers D, Corcoran P. The iceberg of suicide and self-harm in Irish adolescents: A population-based study. Social Psychiatry and Psychiatric Epidemiology 2014;49:1929-1935. [DOI] [PubMed] [Google Scholar]
MHRA 2003
- Medicines and Healthcare Products Regulatory Authority. Selective Serotonin Reuptake Inhibitors (SSRIs): Overview of regulatory status and CSM advice relating to major depressive disorder (MDD) in children and adolescents including a summary of available safety and efficacy data. http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertandrecalls/Safetywarningsandmessagesformedicines/CON019494 (Accessed 18 September 2014).
Mikolajczak 2009
- Mikolajczak M, Petrides KV, Hurry J. Adolescents choosing self-harm as an emotion regulation strategy: The protective role of trait emotional intelligence. British Journal of Clinical Psychology 2009;48:181-93. [DOI] [PubMed] [Google Scholar]
Miller 2007
- Miller AL, Rathus JH, Linehan MM. Dialectical Behavior Therapy with Suicidal Adolescents. New York, NY: Guilford Press, 2007. [Google Scholar]
Miller 2014
- Miller M, Swanson SA, Azrael D, Pate V, Stürmer T. Antidepressant dose, age, and the risk of deliberate self-harm. JAMA Internal Medicine 2014;174:899-909. [DOI] [PubMed] [Google Scholar]
Moher 1998
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 1998;352:609-13. [DOI] [PubMed] [Google Scholar]
Montgomery 1979
- Montgomery SA, Åsberg M. A new depression scale designed to be sensitive to change. British Journal of Psychiatry 1979;134:382-9. [DOI] [PubMed] [Google Scholar]
NCCMH 2004
- National Collaborating Centre for Mental Health. Clinical Guideline 16. Self-harm: the short-term physical and psychological management and secondary prevention of self-harm in primary and secondary care. London: National Institute for Clinical Excellence, 2004. [Google Scholar]
Newton 2010
- Newton AS, Hamm MP, Bethell J, Rhodes AE, Bryan CJ, Tjosvold L, et al. Pediatric suicide-related presentations: A systematic review of mental health care in the emergency department. Annals of Emergency Medicine 2010;56:649-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nezu 2010
- Nezu AM, Nezu CM, D'Zurilla TJ. Problem-solving therapy. In: Kazantzis N, Reinecke MA, Freeman A, editors(s). Cognitive and behavioral theories in clinical practice. New York, NY: Guilford Press, 2010:76-114. [Google Scholar]
NICE 2004
- National Institute of Clinical Excellence (NICE). Self-Harm: The Short Term Physical and Psychological Management and Secondary Prevention of Self-Harm in Primary and Secondary Care [National Clinical Practice Guideline 160]. London: Gaskell and British Psychological Society, 2004. [PubMed] [Google Scholar]
NICE 2005
- National Institute of Clinical Excellence. Depression in Children and Young People: Identification and management in primary, community and secondary care [National Clinical Practice Guideline Number 28]. London: The British Psychological Society, 2005. [PubMed] [Google Scholar]
Nock 2007
- Nock MK, Teper R, Hollander M. Psychological treatment of self-injury among adolescents. Journal of Clinical Psychology 2007;63:1081-9. [DOI] [PubMed] [Google Scholar]
O'Connor 2012
- O'Connor RC, Rasmussen S, Hawton K. Distinguishing adolescents who think about self-harm from those who engage in self-harm. British Journal of Psychiatry 2012;200:330-5. [DOI] [PubMed] [Google Scholar]
O'Connor 2014
- O'Connor RC, Rasmussen S, Hawton K. Adolescent self-harm: A school-based study in Northern Ireland. Journal of Affective Disorders 2014;159:46-52. [DOI] [PubMed] [Google Scholar]
Office of the Surgeon General (US) 2012
- Office of the Surgeon General (US)/National Action Alliance for Suicide Prevention (US) 2012. 2012 National Strategy for Suicide Prevention: Goals and Objects for Action. A report of the U.S. Surgeon General and of the National Action Alliance for Suicide Prevention. Washington, DC: US Department of Health and Human Services, 2012. [PubMed] [Google Scholar]
Osman 1998
- Osman A, Downs WR, Kopper BA, Barrios FX, Baker MT, Osman JR, et al. The Reasons for Living Inventory for Adolescents (RFL-A): Development and psychometric properties. Journal of Clinical Psychology 1998;54:1063-78. [DOI] [PubMed] [Google Scholar]
Ougrin 2011b
- Ougrin D, Latif S. Specific psychological treatment versus treatment as usual in adolescents with self-harm: Systematic review and meta-analysis. Crisis 2011;32:74-80. [DOI] [PubMed] [Google Scholar]
Ougrin 2012
- Ougrin D, Tranah T, Leigh E, Taylor L, Asarnow JR. Practitioner review: Self-harm in adolescents. Journal of Child Psychology and Psychiatry 2012;53:337-50. [DOI] [PubMed] [Google Scholar]
Ougrin 2013
- Ougrin D, Boege I, Stahl D, Banarsee R, Taylor E. Randomised controlled trial of therapeutic assessment versus usual assessment in adolescents with self-harm: 2-year follow-up. Archives of Diseases in Childhood 2013;98:772-6. [DOI] [PubMed] [Google Scholar]
Ougrin 2015
- Ougrin D, Tranah T, Stahl D, Moran P, Asarnow JR. Therapeutic interventions for suicide attempts and self-harm in adolescents: Systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry 2015;54:97-107. [DOI] [PubMed] [Google Scholar]
Patton 2007
- Patton GC, Hemphill SA, Beyers JM, Bond L, Toumbourou JW, McMorris BJ, et al. Pubertal stage and deliberate self-harm in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 2007;46:508-14. [DOI] [PubMed] [Google Scholar]
Platt 1971
- Platt JJ, Spivak G, Bloom M. Means-Ends Problem Solving Procedure (MEPS): Manual and Tentative Norms. Philadelphia, PA: Department of Health Services and Hahnemann Medical College and Hospital, 1971. [Google Scholar]
Radloff 1991
- Radloff LS. The use of the Center for Epidemiologic Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence 1991;20:149-66. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Review Manager (RevMan), Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Reynolds 1985
- Reynolds WM. Suicidal Ideation Questionnaire: Professional Manual. Odessa, FL: Psychological Assessment Resources, 1985. [Google Scholar]
Reynolds 1988
- Reynolds WM. Suicidal Ideation Questionnaire: Professional Manual. Odessa, FL: Psychological Assessment Resources, 1988. [Google Scholar]
Reynolds 1999
- Reynolds WM, Mazza JJ. Assessment of suicidal ideation in inner-city children and young adolescents: Reliability and validity of the Suicidal Ideation Questionnaire-JR. School Psychology Review 1999;28:17-30. [Google Scholar]
Robinson 2011
- Robinson J, Hetrick SE, Martin C. Preventing suicide in young people: Systematic review. Australian and New Zeland Journal of Psychiatry 2011;45:3-26. [DOI] [PubMed] [Google Scholar]
Rossouw 2013
- Rossouw TI. Mentalization-based treatment: Can it be translated into practice in clinical settings and teams? Journal of the American Academy of Child and Adolescent Psychiatry 2013;52:220-2. [DOI] [PubMed] [Google Scholar]
Royal College of Psychiatrists 2014
- Royal College of Psychiatrists. Managing Self-harm in Young People. Guideline number CR192. London, UK: Royal College of Psychiatrists, 2014. [Google Scholar]
Sackett 1997
- Sackett D. The Cochrane Collaboration Handbook. Oxford: Update Software, 1997. [Google Scholar]
Schulz 1995
- Schulz KF. Subverting randomization in controlled trials. Journal of the American Medical Association 1995;274:1456-8. [PubMed] [Google Scholar]
Schünemann 2008a
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Presenting results and 'summary of findings’ tables. In: Higgins JPT, Green S, editors(s). Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, 2008. [Google Scholar]
Scoliers 2009
- Scoliers G, Portzky G, Madge N, Hewitt A, Hawton K, Wilde EJ, et al. Reasons for adolescent deliberate self-harm: A cry of pain and/or a cry for help? Findings from the child and adolescent self-harm in Europe (CASE) study. Social Psychiatry and Psychiatric Epidemiology 2009;44:601-7. [DOI] [PubMed] [Google Scholar]
Sheen 2002
- Sheen CL, Dillon JF, Bateman DN, Simpson KJ, MacDonald TM. Paracetamol toxicity: Epidemiology, prevention and costs to the health‐care system. QJM: An International Journal of Medicine 2002;95:609-19. [DOI] [PubMed] [Google Scholar]
Sinclair 2011
- Sinclair JMA, Gray A, Rivero-Arias O, Saunders KEA, Hawton K. Healthcare and social services resource use and costs of self-harm patients. Social Psychiatry and Psychiatric Epidemiology 2011;46:263-71. [DOI] [PubMed] [Google Scholar]
Speckens 2005
- Speckens AE, Hawton K. Social problem solving in adolescents with suicidal behavior: A systematic review. Suicide and Life Threatening Behavior 2005;35:365-87. [DOI] [PubMed] [Google Scholar]
Stallard 2013
- Stallard P, Spears M, Montgomery AA, Phillips R, Sayal K. Self-harm in young adolescents (12-16 years): Onset and short term continuation in a community sample. BMC Psychaitry 2013;13:328. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sublette 2006
- Sublette ME, Hibbeln JR, Galfalvy H, Oquendo MA, Mann JJ. Omega-3 polyunsaturated essential fatty acid status as a predictor of future suicide risk. American Journal of Psychiatry 2006;163:1100-2. [DOI] [PubMed] [Google Scholar]
Tanskanen 2001
- Tanskanen A, Hibbeln JR, Hintikka J, Haatainen K, Honkalampi K, Viinamäki H. Fish consumption,depression, and suicidality in a general population. Archives of General Psychiatry 2001;58:512-3. [DOI] [PubMed] [Google Scholar]
Taylor 1984
- Taylor EA, Stansfeld SA. Children who poison themselves. II. Prediction of attendance for treatment. British Journal of Psychiatry 1984;145:132-5. [DOI] [PubMed] [Google Scholar]
Torgerson 2004
- Torgerson D. The use of Zelen's design in randomised trials. British Journal of Obstetrics and Gynaecology: An International Journal of Obstetrics and Gynaecology 2004;111:2. [DOI] [PubMed] [Google Scholar]
Townsend 2001
- Townsend E, Hawton K, Altman D, Arensman E, Gunnell D, Hazell P, et al. The efficacy of problem-solving treatments after deliberate self-harm: Meta-analysis of randomized controlled trials with respect to depression, hopelessness and improvement in problems. Psychological Medicine 2001;31:979-88. [DOI] [PubMed] [Google Scholar]
Townsend 2014
- Townsend E. Self-harm in young people. Clinical review. Evidence-Based Mental Health 2014;17:97-9. [DOI] [PubMed] [Google Scholar]
Tyrer 2012
- Tyrer P. Why benzodiazepines are not going away. Commentary on benzodiazepines for anxiety disorders. Advances in Psychiatic Treatment 2012;18:259-62. [Google Scholar]
van Heeringen 2014
- Heeringen K, Mann JJ. The neurobiology of suicide. The Lancet Psychiatry 2014;1:63-72. [DOI] [PubMed] [Google Scholar]
Washburn 2012
- Washburn JJ, Richardt SL, Styer DM, Gebhardt M, Juzwin KR, Yourek A, et al. Psychotherapeutic approaches to non-suicidal self-injury in adolescents. Child and Adolescent Psychiatry and Mental Health 2012;6:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Westbrook 2011
- Westbrook D, Kennerley H, Kirk J. An introduction to cognitive behaviour therapy: Skills and applications. 2nd edition. London, UK: SAGE Publications Ltd, 2011. [Google Scholar]
Wood 2001b
- Wood A, Trainor G. Developmental group psychotherapy for adolescents: A manual for mental health professionals. Manchester, UK: University of Manchester, 2001. [Google Scholar]
World Health Organization 2014
- World Health Organization. Preventing suicide: A global imperative. Geneva, Switzerland: World Health Organization, 2014. [Google Scholar]
Ystgaard 2009
- Ystgaard M, Arensman E, Hawton K, Madge N, Heeringen K, Hewitt A, et al. Deliberate self-harm in adolescents: Comparison between those who receive help following self-harm and those who do not. Journal of Adolescence 2009;32:875-91. [DOI] [PubMed] [Google Scholar]
Zigmond 1983
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica 1983;67:361-70. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Hawton 1998
- Hawton K, Arensman E, Townsend E, Bremner S, Feldman E, Goldney R, et al. Deliberate self harm: Systematic review of efficacy of psychosocial and pharmacological treatments in preventing repetition. British Medical Journal 1998;317:441-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hawton 1999
- Hawton K, Townsend E, Arensman E, Gunnell D, Hazell P, House A, et al. Psychosocial and pharmacological treatments for deliberate self harm. The Cochrane Database of Systematic Reviews 1999, Issue 4. Art. No: CD004577. [DOI: 10.1002/14651858.CD004577.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2011
- National Institute for Health and Clinical Excellence. Self-harm: Longer-term Management [National Clinical Practice Guideline Number 133]. London: National Institute for Health and Clinical Excellence, 2011. [PubMed] [Google Scholar]