

Abstract
Objectives
This work studied if and how current clinical practice agrees with European Viscosupplementation Consensus Group (EUROVISCO) recommendations and how this agreement might be different according to physician’s specialization. In addition, this work aimed to identify key decision factors that practitioners consider in their decision to retreat or not a patient with hyaluronic acid viscosupplementation.
Methods
Practitioners have been invited by e-mail to participate in an online exercise on viscosupplementation retreatment. They received a fictional patient case at random among a set of predefined fictional cases. The platform asked the practitioner if he/she would retreat the patient with viscosupplementation or not. To take a decision, the practitioner could select questions among a list of predefined questions. Among them, some were related to criteria used in the EUROVISCO decision tree and others served as confounding factors.
Results
A total of 506 practitioners participated to the exercise, of which 399 gave their decision about the case assigned to them by the platform. The observed agreement between practitioner decisions and EUROVISCO recommendations was 58.89 ± 4.95% (95% confidence interval [CI]). Overall, the decision to retreat was taken in 47.87% of the cases, while the EUROVISCO guidelines follow-up would have led to 55.89% retreatment for the same cases (P = 0.03).
Conclusions
In current practice, physicians tended to reinject their patients less than recommended, although EUROVISCO guidelines for viscosupplementation retreatment consider decision criteria that clearly correspond to those of practitioners in real life. These include the patients’ willingness to be treated or the patients’ perception of the effectiveness of the treatment.
Keywords: osteoarthritis, knee, hyaluronic acid, guidelines, viscosupplementation
Introduction
Viscosupplementation (VS) by intra-articular injection of hyaluronic acid (HA) is commonly used in the treatment of osteoarthritis (OA). This therapeutic modality is recommended by many scientific societies in patients with knee OA where pain is not adequately relieved with conventional therapy.1-3 The success rate of VS increases when the indication is correctly set and the injection is correctly performed. 4 With the aim of increasing this success rate, the European Viscosupplementation Consensus Group (EUROVISCO) expert group has published recommendations to help practitioners using VS.5-7 In September 2016, the EUROVISCO working group drew up a set of suggestions to help practitioners in the decision of retreatment with VS in patients with knee OA who have been previously treated with VS injections. 7 The task force built two separate decision algorithms based on the clinical result of the previous treatment. They have considered two scenarios: (1) the reinjection in patients successfully treated with VS, 6-12 months ago and (2) the reinjection in patients where previous VS failed or caused adverse reactions. The purpose of that recommendation was to consider all the factors that can influence, positively or negatively, a doctor’s decision to retreat patients with VS and also to build a decision-supporting algorithm. 4 In patients not satisfied with previous VS, several predictors of treatment failure have been identified. The unanimously identified factors were a wrong clinical analysis of pain, the extra-articular delivery of the HA, obesity, patellofemoral OA (isolated or severe), and very severe tibio-femoral joint space narrowing. Before taking the decision to retreat with VS in patients where VS failed, the first step in the decision tree was to confirm the appropriate indication. If indication was incorrect, one should not repeat VS injection and instead change to a more appropriate treatment by choosing one more adapted to the clinical situation. If the indication was correct but with concomitant one or several predictive factors of failure, the working group recommended to discuss other treatment options with the patient after explaining that the chances of success of a new or repeat VS are low. Another very frequent clinical scenario addressed by the EUROVISCO group was a patient, who significantly improved with VS, and returned to follow-up, 6-12 months later. Four different case scenarios were identified: (1) the patient remains “symptom free,” (2) the patient remains “minimally symptomatic” but with no increasing pain, (3) the patient is “minimally symptomatic” but with increasing pain, or (4) the patient is symptomatic again. In the first situation, the EUROVISCO working group did not recommend to retreat systematically. Consequently, it advised retreatment as soon as the pain recurs and if pain exceeds the Patient Acceptable Symptom State (PASS) threshold. In “minimally symptomatic” patients with no increase of pain, the EUROVISCO group proposed to retreat young patients, early stages of OA, patients with risk factors of progression, professional sportsmen, and patients with severe comorbidities. Those patients at high risk of disease progression could be retreated 12 months after the first injection even if they are asymptomatic.
The goal of this survey was to assess whether the current clinical practice followed the recommendations of the EUROVISCO in terms of retreatment with VS in patients suffering from knee OA. This study followed three objectives: The primary objective was to measure the agreement rate of the current clinical practice with the EUROVISCO decision algorithms for the retreatment with VS in patients suffering from knee OA over a broad range of physicians from several specialization, the secondary objective was to assess whether there were different agreement rates with EUROVISCO algorithm for re-VS between physicians’ specialization, and finally, the exploratory objective was to identify the most common causes of discrepancies in VS decisions.
Materials and Methods
Study Design
Fictional study cases were sent to doctors asking for their decision in terms of VS retreatment or not. These cases contained a short medical history and a list of all necessary and several useless criteria to make a decision about VS retreatment. These questionnaires were implemented as online forms. The value of each criterion was hidden by default. The physician has the possibility to display the criteria that he/she thought to be relevant to make the decision, in which case, the fact that the physician required this information was stored for future analysis. Several fictional cases (29) were designed such that recommendations could be followed from every possible path in the decision algorithm. Each physician received and answered to one fictional case allocated in a circular way for each specialization. Physicians were chosen among the following specializations: physical therapist/physiatrist, rheumatologist, orthopedic surgeon, or general practitioners. The EUROVISCO retreatment decision-support algorithm has not been reminded to the participant or even mentioned until after he or she fulfilled on a voluntary basis the study.
Endpoints
The primary endpoint was the proportion of agreement between physician’s decision and EUROVISCO recommendation to retreat or not with VS and the 95% confidence interval (CI) around this proportion. The secondary endpoint tested the differences of agreement rates between all pairs of doctor specializations. The exploratory endpoints were (1) for each fictional study case, the proportion of agreement between physician’s decisions and EUROVISCO recommendations to retreat or not with VS, (2) for each criterion, the proportion of displays when relevant or not in the EUROVISCO decision algorithm, (3) the discrepancies in decisions between different specializations, and (4) the discrepancies in decisions between different practice environment.
Statistical Methods
Primary analysis
n was the total number of answered study cases and agree the number of answered questionnaires for which the physician’s response was identical to the EUROVISCO recommendation. The proportion of agreement p was estimated as nagree/n. The 95% CI was given by the following R code binom.test (n_agree,n,conf.level = .95)$conf.int.
Secondary analysis
na1 and nd1 were the numbers of agreement and disagreement with the EUROVISCO recommendations in physicians of group 1, and na2 and nd2 were the numbers of agreement and disagreement in physicians of group 2. The P value that the proportions of agreement differ between the two groups was given by the following R code: prop.test(matrix(c(n_a1,n_d1,n_a2,n_d2),nrow=2,byrow=T))$p.value. These tests were performed for each pair of doctor specializations. P values have been corrected for multiple testing.
Exploratory endpoints
Similarly to secondary analyses, proportion tests have been conducted for comparing agreement and disagreement numbers between countries, environmental practices, stories, recommendation knowledge, age groups, career education, and experience with VS.
Impact of question position (on the list of available questions) has been investigated. Questions at the beginning of the list were clicked much more often than the others. This artifact due to the user interface was removed by fitting a log-linear regression which estimates the number of clicks from the question’s position in the list. After correction, the most popular questions have been classified according to the residual amount of clicks.
Sample Size
Primary analysis
The sample size was chosen such that the margin error of the agreement rate was below 10% for all possible agreement rates, according to a binomial test with a 95% confidence level (Suppl. File A). This approach determined that having a population of n = 200 ensured that the margin error was inferior to 10% for all values of p. Therefore, the required sample size was at least 200 doctors to measure the global agreement rate.
Secondary analysis
The number of doctors required in each group (specialization) to show statistical differences with a significance level of 95% and a power of 80% was 200 physicians per specialization, that is, 800 physicians in total, for differences in agreement rates of at least 15%.
This sample size computation did not take correction for multiple testing into account (Suppl. File B).
Results
A total of 506 practitioners participated to the exercise, of which 399 gave their decision about the case assigned to them by the platform. Demographic and professional characteristics of participants are presented in Table 1 .
Table 1.
Demographic and Professional Characteristics of the 506 (399) Participants.
| Characteristics | Values |
|---|---|
| Age range, years | % |
| 20-29 | 4.7 (6.4) |
| 30-39 | 26.2 (33.3) |
| 40-49 | 13.6 (18.2) |
| 50-59 | 14.6 (18.9) |
| 60-69 | 14 (17.8) |
| 70-79 | 1.1 (0.1) |
| 90-99 | 0.1 (0.1) |
| Unknown | 25.2 (5.2) |
| Specialization | % |
| Rheumatologist | 30.2 (32.3) |
| Physical therapist | 38.5 (40.1) |
| Orthopedic surgeon | 25.3 (22.8) |
| General practitioner | 5.93 (4.76) |
| Country of activity | % |
| Belgium | 2.37 (3.01) |
| France | 21.3 (27.1) |
| Germany | 14.2 (18.0) |
| Italy | 3.16 (4.01) |
| Portugal | 1.38 (1.75) |
| Turkey | 28.9 (36.6) |
| Other | 3.39 (4.27) |
| Unknown | 25.3 (5.26) |
| Type of medical activity | % |
| Hospital | 19.4 (24.6) |
| Mixed practice (private + hospital) | 14.6 (18.5) |
| Private practice (several) | 13.4 (17.0) |
| Private practice (single) | 9.49 (12.0) |
| University hospital | 17.8 (22.6) |
| Unknown | 25.3 (5.26) |
| Knowledge about recommendations | % |
| Yes | 20.9 (26.6) |
| No | 53.8 (68.2) |
| Unknown | 25.3 (5.26) |
| Years of practice | % |
| 0-4 | 10.1 (12.8) |
| 5-9 | 15.4 (19.5) |
| 10-14 | 11.3 (14.3) |
| 15-19 | 4.94 (6.27) |
| 20-24 | 9.68 (12.3) |
| 25-29 | 7.91 (10.0) |
| >30 | 13.0 (16.5) |
| Unknown | 27.7 (8.27) |
| Frequency of viscosupplementation injection | % |
| Never | 0.99 (1.25) |
| <1×/year | 1.78 (2.26) |
| 1×/year | 5.93 (7.52) |
| 1×/month | 16.4 (20.8) |
| 1×/week | 15.6 (19.8) |
| >1×/week | 34.0 (43.1) |
| Unknown | 25.3 (5.26) |
Among them, 235 (59%) agreed with the EUROVISCO recommendations and 164 (41%) disagreed ( Fig. 1 ). The probability to be agreed with the recommendations was significant with a value of P < 0.001. Only 16% of physicians were retreating patients who should not have been retreated as recommended. Inversely, 24.5% of the physician did not reinjected patients who should be retreated according to the guidelines.
Figure 1.
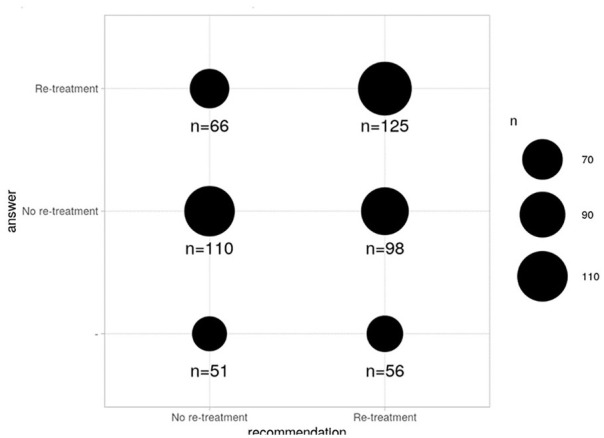
The confusion matrix. Columns correspond to the European Viscosupplementation Consensus Group algorithm recommendations. Rows represent individual decisions by the participants. The bottom row corresponds to missing answers.
“Over-treatment” was defined as a decision by the physician to retreat with VS, while EUROVISCO recommendation would be not to retreat. “Under-treatment” was then defined as the decision not to retreat with VS, while EUROVISCO recommendation would be to retreat. Comparing medical disciplines in terms of overtreatment or undertreatment showed that orthopedic surgeons tended to be those that overtreat the most (44%), while rheumatologists were the least overtreating (29%). In-between, physiotherapists overtreated in 40% of the cases. In contrast, rheumatologists were those that tended to undertreat their patients the most (53%), while orthopedic surgeons were those who undertreated the less (31%). In-between, physiotherapists undertreated in 42% of the cases. Despite this, no significant difference between specialization was observed.
No significant difference between countries was observed in terms of agreement with the recommendation. Belgian, French, and Italian physicians tended to under retreat patients comparing with other countries, but the difference between countries was not significant (Belgium 70%, France 58%, Italy 57%, Turkey 42%, and Germany 28%). Of note, there was an important correlation between the country of each participant and the distribution of the discipline. It might thus be possible that different terms cover overlapping realities in practice, just named differently depending on the country.
Further, no clear difference was observed between doctors practicing in private or in the hospital in terms of agreement to retreat. There was no difference between physicians working at university hospitals and those working in nonuniversity hospitals.
There was also no significant difference between physicians that knew the EUROVISCO recommendations and those that did not know these recommendations.
The age of the physician and the number of years of practice were not factors that influence decision to retreat with VS.
When the number of questions asked by the doctor about the story (n of clicks) was higher, a tendency for less overtreatment, but no strong tendency about undertreatment, was observed.
After corrections, the five questions the most asked by the physicians were (1) does the patient have previous injection of corticosteroids? (2) according the patient, what is the efficacy level of the treatment after 6 months? (3) does the patient wish to be or not retreated? (4) does patient have current consumption of nonsteroidal anti-inflammatory drugs (NSAIDs)? and finally, (5) is there another cause of knee pain than OA (e.g. meniscal tear, trauma, tendinitis, and osteonecrosis)?
Discussion
In general, evidence-based recommendations are established on the basis of a systematic review of the literature and/or meta-analyses and the opinion of expert researchers or clinicians. Too often, these recommendations are the object of criticism because they are too far removed from medical practice. It is for this reason that the EUROVISCO group investigated whether its recommendations were in line with medical practice. To this end, we asked European physicians to choose whether or not to retreat fictitious cases of patients suffering from OA of the knee and to compare their choice with that of the decision-making algorithm established by the EUROVISCO experts group. This approach was original and according to our knowledge had never been carried out in the field of OA.
By this way, we have demonstrated that a majority of physicians followed in their practice the EUROVISCO recommendations. However, 25% did not reinjected patient, while EUROVISCO group was recommended to do that. We can make several hypotheses to explain this difference: (1) ignorance of the EUROVISCO recommendations. Indeed, only 28% of the participants said they knew about these recommendations. Those who knew the guidelines tended to retreat more frequently that those who did not know the EUROVISCO guidelines; (2) the definition of treatment failure was often subjective in the current medical practice, while EUROVISCO algorithm impose objective criteria. To define the failure of treatment, the EUROVISCO group used the PASS defined as the value beyond which patients consider themselves well (i.e., strictly < at 4 on a 10-point rating scale); (3) in real life, recurrence or increase in pain if often the criteria used to decide for a reinjection while the EUROVISCO algorithm also consider retreatment in asymptomatic or minimally symptomatic patients with early stage of OA, young age, risks factors of progression, and professional sportsperson. Severe comorbidities that contraindicate NSAIDs and surgery were also considered as arguments in favor of an earlier retreatment.
This study also showed that only two thirds of the participants followed recommendations in terms of retreatment. This point could be taken into consideration in the interpretation of real-life postmarketing clinical trials and could affect the long-term potential chondroprotective effects of VS. Indeed, as mentioned before, 25% of the physicians did not retreated while they should retreated if they followed the recommendation limiting the potential beneficial effect of multiple injection on cartilage metabolism.
The more the doctor asked questions about the fictitious case, the less they tended to retreat patients with VS. One explanation is that a high number of questions allow them to identify risk factors of VS failure. The five most often questions were (1) does the patient have previous injection of corticosteroids? (2) according the patient, what is the efficacy level of the treatment after 6 months? (3) does the patient wish to be or not retreated? 4) does the patient have current consumption of NSAIDs? and finally, (5) is there another cause of knee pain than OA (e.g. meniscal tear, trauma, tendinitis, and osteonecrosis)? Interestingly, these questions allowed the physician to identify criteria that were included in the EUROVISCO algorithm. In contrast, the less selected questions were those related to confounding factors (i.e. Does patient have vascular pathology in lower limb? Does patient have edema in lower limb?). This confirms that criteria used in the EUROVISCO are in line with the current clinical practice.
Another important observation of this study is that the type of practice (private or hospital), specialization, number of years of practice, age, or even geographical location did not significantly influence the decision to retreat with VS. This suggests that the decision to retreat is influenced more by medical criteria than by socioeconomic considerations. However, these exploratory data have to be interpreted with caution since the sample size was too small. Indeed, having 200 physicians per specialization, that is, 800 physicians in total, was required to show significant results for differences in agreement rates of at least 15%.
This work has some other limitations. A written survey always exposes to the risk of looking for the “best” response and might artificially increase the gap between written answers and the real life. The survey was conducted in different countries with several differences in terms of patients’ profile and social insurance. Furthermore, the recruitment was not homogenous and some countries (France and Turkey) recruited far more than others and this may influence the final results.
Conclusions
The EUROVISCO recommendations for VS retreatment for knee OA and clinical practice significantly agree in a majority of cases. EUROVISCO recommendations consider decision criteria that are clearly matching those of practitioners in real life. These include patients’ willingness to be treated or patients’ perception about treatment efficacy.
Supplemental Material
Supplemental material, sj-docx-1-car-10.1177_19476035211053827 for Retreatment with Hyaluronic Acid Viscosupplementation in Knee Osteoarthritis: Agreement between EUROVISCO Guidelines and Current Medical Practice by Yves Henrotin, Cedric Tits, Jérôme Paul, Pierre Gramme, Thibault Helleputte, Alberto Migliore, Pascal Richette, Xavier Chevalier, Jordi Monfort, Demirhan Diracoglu, Hervé Bard, Jörg Jerosch, Dominique Baron, Raman Raghu and Thierry Conrozier in CARTILAGE
Supplemental material, sj-docx-2-car-10.1177_19476035211053827 for Retreatment with Hyaluronic Acid Viscosupplementation in Knee Osteoarthritis: Agreement between EUROVISCO Guidelines and Current Medical Practice by Yves Henrotin, Cedric Tits, Jérôme Paul, Pierre Gramme, Thibault Helleputte, Alberto Migliore, Pascal Richette, Xavier Chevalier, Jordi Monfort, Demirhan Diracoglu, Hervé Bard, Jörg Jerosch, Dominique Baron, Raman Raghu and Thierry Conrozier in CARTILAGE
Footnotes
Supplementary material for this article is available on the Cartilage website at http://cart.sagepub.com/supplemental.
Acknowledgments and Funding: The authors are grateful to the Walloon region who funded the present research (grant number 7360 entitled PROUESSE) implemented by the BIOWIN competitiveness cluster. The authors want to thank the physicians for their participation in the study.
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cedric Tits, Jérôme Paul, and Pierre Gramme are employees of DNAlytics; Thibault Helleputte is a shareholder of DNAlytics; Thierry Conrozier is a consultant of LABRHA, SANOFI, and MEDAC; and Alberto Migliore, Pascal Richette, Xavier Chevalier, Jordi Monfort, Demirhan Diracoglu, Hervé Bard, Jörg Jerosch, Dominique Baron, Raman Raghu, and Yves Henrotin declared no conflict of interests.
ORCID iD: Yves Henrotin  https://orcid.org/0000-0003-1073-449X
https://orcid.org/0000-0003-1073-449X
References
- 1. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil. 2019. Nov;27(11):1578-89. [DOI] [PubMed] [Google Scholar]
- 2. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, et al. Standing Committee for International Clinical Studies Including Therapeutic Trials ESCISIT. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis. 2003. Dec;62(12):1145-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Sellam J, Courties A, Eymard F, Ferrero S, Latourte A, Ornetti P, et al. French Society of Rheumatology. Recommendations of the French Society of Rheumatology on pharmacological treatment of knee osteoarthritis. Joint Bone Spine. 2020. Dec;87(6):548-55. [DOI] [PubMed] [Google Scholar]
- 4. Conrozier T, Eymard F, Chouk M, Chevalier X. Impact of obesity, structural severity and their combination on the efficacy of viscosupplementation in patients with knee osteoarthritis. BMC Musculoskelet Disord. 2019. Aug 17;20(1_suppl):376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Conrozier T, Monfort J, Chevalier X, Raman R, Richette P, Diraçoglù D, et al. EUROVISCO recommendations for optimizing the clinical results of viscosupplementation in osteoarthritis. Cartilage. 2020. Jan;11(1_suppl):47-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Henrotin Y, Chevalier X, Raman R, Richette P, Montfort J, Jerosch J, et al. EUROVISCO guidelines for the design and conduct of clinical trials assessing the disease-modifying effect of knee viscosupplementation. Cartilage. 2020. Jan;11(1_suppl):60-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Raman R, Henrotin Y, Chevalier X, Migliore A, Jerosch J, Montfort J, et al. Decision algorithms for the retreatment with viscosupplementation in patients suffering from knee osteoarthritis: recommendations from the EUROpean VIScosupplementation COnsensus Group (EUROVISCO). Cartilage. 2018. Jul;9(3):263-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-car-10.1177_19476035211053827 for Retreatment with Hyaluronic Acid Viscosupplementation in Knee Osteoarthritis: Agreement between EUROVISCO Guidelines and Current Medical Practice by Yves Henrotin, Cedric Tits, Jérôme Paul, Pierre Gramme, Thibault Helleputte, Alberto Migliore, Pascal Richette, Xavier Chevalier, Jordi Monfort, Demirhan Diracoglu, Hervé Bard, Jörg Jerosch, Dominique Baron, Raman Raghu and Thierry Conrozier in CARTILAGE
Supplemental material, sj-docx-2-car-10.1177_19476035211053827 for Retreatment with Hyaluronic Acid Viscosupplementation in Knee Osteoarthritis: Agreement between EUROVISCO Guidelines and Current Medical Practice by Yves Henrotin, Cedric Tits, Jérôme Paul, Pierre Gramme, Thibault Helleputte, Alberto Migliore, Pascal Richette, Xavier Chevalier, Jordi Monfort, Demirhan Diracoglu, Hervé Bard, Jörg Jerosch, Dominique Baron, Raman Raghu and Thierry Conrozier in CARTILAGE