

Overview
The coronavirus disease 2019 (COVID-19) pandemic is unprecedented and information about the severe acute respiratory syndrome coronavirus 2 is evolving rapidly. New York is one of the epicenters of the COVID-19 outbreak in the United States, reporting >1000 confirmed cases as of March 17, 2020, and cases are escalating exponentially. The majority of cases are in Westchester County (n=220) and New York City (NYC; n=463), which includes Bronx (1). The local index patient case was a Westchester man who became ill on February 22, was not associated with a recent travel exposure to a country on the watch list (China, Iran, South Korea, and Italy), or known to have had direct contact with a COVID-19–confirmed patient. At the present time it is estimated that community-wide transmission accounts for 87% of confirmed cases. Nephrologists in the Bronx have been handicapped in managing patients with ESKD during the early weeks of the COVID-19 pandemic due to the limitations of available rapid testing for severe acute respiratory syndrome coronavirus 2. Montefiore Medical Center, located in the north Bronx in close proximity to Westchester, has been one of the main tertiary care hospitals in NYC caring for persons under investigation (PUIs) and for COVID-19–confirmed patients. Our nephrology division’s clinical faculty care for approximately 850 patients with ESKD (approximately 800 on hemodialysis and approximately 50 on peritoneal dialysis) in 12 outpatient hemodialysis facilities (two Fresenius and 10 DaVita facilities) in the Bronx. We report our experience with caring for the ESKD population and patients who are hospitalized with AKI in the Bronx during the first 3 weeks of the local NYC COVID-19 pandemic.
Outpatient Dialysis Population
Strategies proposed for the prevention and management of COVID-19 transmission for patients with ESKD in the outpatient dialysis facilities have been dynamic. The American Society of Nephrology’s (ASN’s) Nephrologists Transforming Dialysis Safety (NTDS) website has been on the forefront of informing the nephrology community of the earliest and most updated guidance from the Centers for Disease Control and Prevention (CDC) about COVID-19 preparation and management of patients with ESKD in the outpatient dialysis setting (2,3). The NTDS’s initial release of frequently asked questions for outpatient dialysis facilities based on CDC guidelines was on March 4, and the ASN and CDC provided an informational webinar on March 11, which is still available on the website (4). The most updated policies from the large dialysis organizations (LDOs), including DaVita and Fresenius, were distributed to medical directors and staff for the Bronx facilities on March 16. Table 1 provides a timeline of the COVID-19 pandemic in Westchester and NYC and illustrates the necessary adaptations to CDC recommendations and the LDOs’ policies and procedures as the number of PUIs and confirmed COVID-19 cases increased in our region and as more information became available. Table 1 also illustrates the changing policies at Montefiore-affiliated outpatient hemodialysis facilities as guidelines and knowledge of the pandemic evolved.
Table 1.
Timeline and evolution of COVID-19 outpatient hemodialysis management recommendations (CDC) and policy changes (CDC and LDOs) for Montefiore-affiliated facilities
| Recommendation | March 3, 2020 | March 7, 2020 | March 17, 2020 |
| All patients with confirmed COVID-19 in Westchester and New York City | 2 | 82 | 1024 |
| Affected geographic areas | International travel to affected geographic areas within 14 d from | National geographic areas | Global spread |
| China | New Rochelle and New York City | Now largely community transmission without known exposure | |
| Iran | Washington State | ||
| Italy | |||
| Japan | |||
| South Korea | |||
| Sampling of specimens | Upper respiratory nasopharyngeal swab and oropharyngeal swab | Recommendation revised to a single upper respiratory nasopharyngeal swab | |
| Sputum if productive cough | |||
| BAL or tracheal aspirate | |||
| Laboratory testing locations | Ship overnight to CDC or New York State Department of Health | More local and commercial laboratories begin testing, but still very limited | |
| Restricted testing of patients who are hospitalized with severe symptoms only | |||
| After negative influenza and respiratory viral panel | |||
| Mask and isolation recommendations | N95 mask or respirator | Face masks are an acceptable alternative due to limited availability of N95 masks (unless aerosolized procedure planned) | |
| Airborne isolation | Droplet isolation | ||
| Policies specific for outpatient hemodialysis location | Dialysis should not occur in an outpatient facility for a PUI unless an AIIR is available, preferably in an acute care hospital in an AIIR at this time | Dialysis for PUIs may occur in outpatient hemodialysis facilities | |
| Maintain at least 6 feet of separation between masked, symptomatic PUIs and other patients in waiting areas and during dialysis treatment. | |||
| Ideally, dialyze symptomatic PUIs in a separate room with the door closed. Hepatitis B isolation rooms should only be used if | |||
| The patient is hepatitis B surface antigen positive or | |||
| The facility has no patients on the census with hepatitis B infection who would require treatment in the isolation room | |||
| If a separate room is not available, the masked PUI should be treated at a corner or end-of-row station, away from the main flow of traffic, and separated by at least 6 feet from the nearest patient (in all directions) | |||
| Cohorting symptomatic PUIs, patients with confirmed COVID-19 requiring HD, and the HCP caring for them together | |||
| In the section of the unit and/or on the same shift (the last shift of the day), separating symptomatic PUIs from COVID-19–confirmed cases by day | |||
| Cohort into a designated COVID-19 facility | |||
| EMS transportation of PUIs or patients with COVID-19 to health care facilities | Recommendations are for EMS workers trained in infection control and use of PPE | ||
| No information exists for non-EMS staff | |||
| Use full PPE (N95 or face mask, eye protection, gowns, gloves) | |||
| Notify facility in advance so infection control measures may be taken before arrival | |||
| Patient should wear a face mask and be separated as much as possible | |||
| Family members and contacts should not ride if possible. If riding in the vehicle, they should wear a mask | |||
| When possible, isolate the driver from the patient compartment and close windows. Ventilation should be in nonrecirculated mode | |||
| If the vehicle is without an isolated driver compartment, outside air ventilation must be implemented | |||
| Patient screening and use of face masks | Before arrival | Patients call ahead to facility or physician to prepare and triage in the facility | |
| Patients with fever or respiratory symptoms advised to call ahead to facility or physician to prepare and triage (possibly to an acute hospital setting) | Infection prevention manager assists staff with patient screening | ||
| Goal is to keep patients out of the acute hospital setting if medically stable and can be dialyzed as an outpatient | |||
| Patients who have arrived to facility | All patients are required to wear a mask regardless of symptoms | ||
| Patients with symptoms should put on a face mask at check in | |||
| Essential visitors | Limit visitors to essential visitors | All essential visitors are now screened and must wear a mask while in facility (LDO policy) | |
| Face mask not required unless there are respiratory symptoms | |||
| Health care providers’ face mask use | HCPs required to wear a face mask | All HCPs are required to wear a face mask at all times while in facility (LDO policy)a | |
| During catheter connection and disconnection or | |||
| When caring for a PUI or patient positive for COVID-19a | |||
| PPE use (eye protection, disposable gown, and nonsterile gloves) | HCPs required to use full PPE | HCPs providing direct patient care are now required to use full PPE from the first patient interaction in the waiting room to the treatment floor | |
| During catheter connection and disconnection or | Remove PPE, except face mask, before entering medication room | ||
| When caring for a PUI or patient with confirmed COVID-19 and | Don new PPE upon leaving medication room | ||
| Change PPE between PUIs or patients with COVID-19 | (LDO policy) | ||
COVID-19, coronavirus disease 2019; CDC, Centers for Disease Control and Prevention; LDO, large dialysis organizations (DaVita Kidney Care and Fresenius Kidney Care); BAL, bronchoalveolar lavage; PUI, person under investigation; AIIR, airborne isolation room; HD, hemodialysis; HCP, health care provider; EMS, emergency medical services; PPE, personal protective equipment.
Until the supply of N95 masks is restored.
Early Actions Implemented in the First Week of March
Distribution of Information to Patients.
The NTDS poster on “COVID-19 awareness” and CDC posters on “cough etiquette” and “handwashing” were posted at the entrance of the facilities and in the lobby, both in Spanish and in English. Educational material was distributed to patients, families, and staff. More frequent antiseptic cleaning of chairs and door handles in the lobby was ordered and the provision of easy access to 60%–95% alcohol-based hand sanitizers was implemented in the waiting room.
Use of the CDC’s Patient Screening Questionnaire and Situation Guidelines.
Initially, patients were advised to call ahead to the outpatient hemodialysis facility or call their nephrologist to report fever or respiratory symptoms so that they could be advised on whether to proceed to the hospital or be safely evaluated in the hemodialysis facility. The provider could then call the hospital staff to prepare for their arrival or the hemodialysis facility could prepare to screen them. For patients arriving at the outpatient facility, only those outpatients who were symptomatic were being formally screened and given a mask. Patients who met criteria for being a PUI were sent to the hospital and the provider called the hospital staff in advance. At this time, the recommendations were that it would be advisable to refer symptomatic PUIs to an acute hospital setting where hemodialysis could be performed in an airborne isolation room and where staff would use personal protective equipment (PPE), including an N95 mask. Those PUIs sent to the hospital would have a respiratory viral panel performed to test for both influenza A and B and for respiratory syncytial viral. Due to severe limitations on COVID-19 testing—where tests were initially sent to the CDC and were then performed by the New York State Department of Health with a 1–2 day time to result, this testing was reserved only for the moderate to severely ill PUIs.
Revisions to Hemodialysis Situation Guidelines and Screening: Mid-March
The revised CDC recommendations in this period were such that droplet isolation and use of face masks were acceptable, due to shortage of N95 masks, unless an aerosolized procedure was planned. This facilitated performing hemodialysis in the outpatient facility under the specific conditions outlined in Table 1. Hospitalization was reserved for the patients with ESKD who were the most ill and who required an acute level of care. A triage plan—coordinated by centralized infection prevention managers working with the dialysis staff and physician—was instrumental to determine the most appropriate setting to provide hemodialysis for PUIs who were asymptomatic, symptomatic, and COVID-19 confirmed, with the goal of avoiding unnecessary emergency department visits and hospitalizations.
As the number of PUIs and confirmed patients with COVID-19 has grown, so has the need to expand outpatient screening to everyone. The revised screening policy at the two major LDOs now mandate that all patients, visitors, staff, physicians, and physician extenders entering the dialysis clinic must be screened for signs and symptoms of COVID-19 before admittance to the dialysis treatment floor.
Policy for Use of PPE.
Initially, only patients who arrived at the dialysis facility with fever or respiratory symptoms were asked to put on a mask before entering. Health care workers were only required to wear masks during catheter connection procedures or if they had a cough. Due to the rapid rise in COVID-19 cases, the LDOs soon intensified their PPE policy beyond that recommended by the CDC. The current revised policy is that all patients are required to wear a mask upon entry to the facility and throughout their treatment, regardless of risk or symptoms. All other essential visitors must wear a mask while in the facility. All health care providers are required to wear a face mask at all times, both on and off the treatment floor.
All staff members providing direct patient care are now required to wear full PPE, including gowns, gloves, face shields or goggles, and surgical face masks, from the first patient interaction in the facility lobby to the treatment floor. In the medication preparation area, staff are required to only wear a surgical face mask and are expected to remove PPE (except face masks) before entry to the medication preparation area and then don new PPE (including gown, gloves, and face shield) upon leaving the medication preparation area and returning to the treatment floor. The obvious potential downside to these extreme measures is the risk of potentially competing with acute hospitals for the limited and rapidly shrinking supply of PPE.
Plans for Outpatient Hemodialysis Provision for Patients with COVID-19.
In the third week of March, the first patient requiring hemodialysis with confirmed COVID-19 presented at one of our Montefiore-affiliated outpatient LDO facilities for dialysis. The patient was dialyzed at the outpatient facility 2 days before when the patient was asymptomatic, screened negative, and denied fever, respiratory symptoms, recent travel, or other known exposure. The outpatient hemodialysis staff, patients, and visitors who may have been exposed to the virus are being evaluated to ascertain the level of exposure to determine if they meet criteria for a PUI, and are being closely monitored for fever (temperature taken twice daily, monitor for respiratory symptoms) for 14 days.
One of the LDOs reported that six patients on hemodialysis in their United States facilities have been confirmed COVID-19 positive as of March 17 and were receiving hemodialysis in the acute hospital setting. Because we anticipate more patients on hemodialysis testing COVID-19 positive, Montefiore-affiliated LDO facilities plan to cohort patients with confirmed COVID-19 who are medically stable into designated COVID-19 units in the Bronx. The proposed plan is for symptomatic PUIs to be dialyzed on the last shift, separated from other patients, so as to allow for a proper environmental disinfection period. Ideally, PUIs should undergo rapid testing; however, local testing sites and laboratories were severely limited and, as of March 20, have been closed by the New York State Department of Health due to a severe shortage of test kits and PPE for the staff manning these testing sites. These patients may also dialyze at an allocated “COVID-19 facility,” providing the symptomatic PUIs and those with confirmed COVID-19 dialyze on different days. The CDC has provided recommended guidelines for transport of a PUI or patient with documented COVID-19 to an acute hospital or outpatient hemodialysis facility, but this pertains to trained emergency medical services using appropriate PPE and environmental disinfection (5). The local department of health must closely monitor every patient with confirmed COVID-19, perform an evaluation of residence, and provide PPE for cohabitants.
New Outpatient Hemodialysis Placement.
Testing for COVID-19 would be invaluable for placing new patients requiring hemodialysis for admission into the appropriate outpatient facility, similarly to what is done for hepatitis B and tuberculosis screening. No such policy exists at this time.
Patients Who Are Hospitalized
Established Patients on Hemodialysis Presenting to the Acute Hospital
Figure 1 is a flow diagram that illustrates the proposed plan for the management of patients on hemodialysis sent to the Montefiore emergency department with fever, respiratory symptoms, known travel, or known COVID-19 exposure as of the morning of March 20. This has been a dynamic decision process and adjustments have been made on an almost daily basis. As the number of patients with COVID-19 who require hospitalization has increased, it has been decided to now cohort all patients with COVID-19 (from three Montefiore-affiliated hospitals) to the Moses Campus hospital to conserve PPE and streamline protocols.
Figure 1.
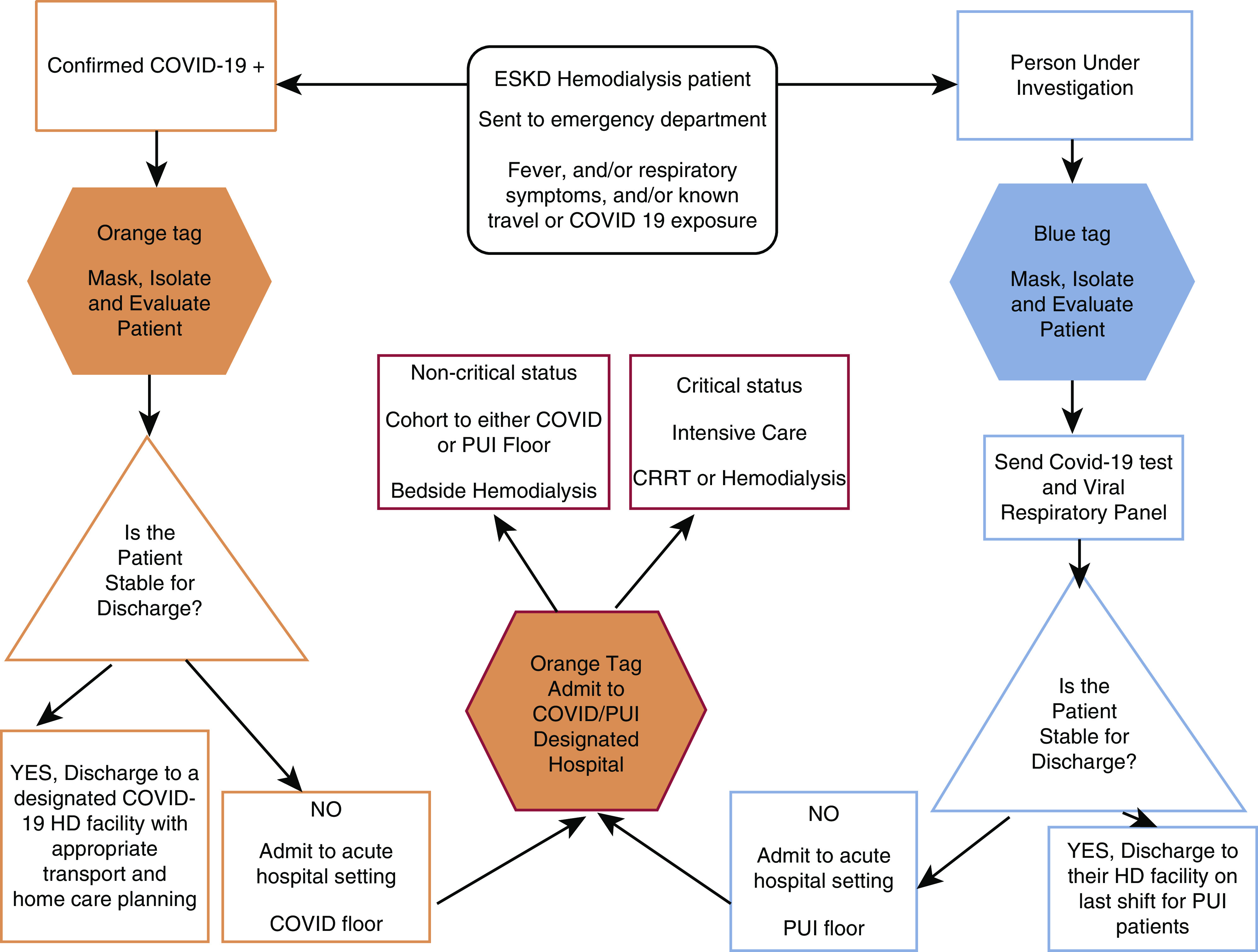
Management of ESKD for patients with coronavirus disease 2019 and persons under investigation in the emergency department. Early identification of suspect or confirmed COVID-19 patients and their risk level is determined immediatly upon screening prior to entering the emergency department. COVID-19 suspected or confirmed patients are then evaluated by the emergency department staff to further determine their clinical stability. Patients who require acute hospitalization are admitted to a COVID-19 or PUI floor, or to an intensive care unit. Stable patients are discharge with appropriate travel precautions and self-isolation. COVID-19, coronavirus disease 2019; CRRT, continuous RRT; HD, hemodialysis; PUI, person under investigation.
Patients are immediately masked (if this has not already been done) and isolated. The evaluating emergency room providers wear full PPE during the screening process. Patients who are confirmed for COVID-19 are issued an orange tag (high risk) and clinical stability for discharge is determined. If stable, they are reassigned to a designated COVID-19 outpatient hemodialysis facility. A PUI receives a blue tag (intermediate risk) and undergoes further testing for COVID-19 and a respiratory viral pathogen panel. If a PUI is stable for discharge, they may be assigned to a PUI-designated last shift or isolation room at an outpatient hemodialysis facility until COVID-19 testing results become available. COVID-19 tests were initially sent to the CDC for processing, and then to the New York State Department of Health. As of now, Montefiore Laboratory has the capability to perform on-site, rapid COVID-19 testing in a limited quantity. Patients on hemodialysis who have either COVID-19 or PUI status that require urgent dialysis in the emergency department are treated in the isolation room, which is then disinfected and requires a down period of 207 minutes before the room can be used.
Hemodialysis Procedure for Patients with COVID-19 or PUIs Assigned to the Hospital Floor
For patients with confirmed COVID-19 or PUIs who require hospitalization, the level of patient acuity dictates whether they require a critical care setting or may be closely monitored on the dedicated COVID-19–positive floor. Patients with COVID-19 and PUIs receive bedside hemodialysis in their room using a portable hemodialysis machine with portable reverse osmosis, which is hooked up to the walled hemodialysis plumbing unit. The efflux goes directly into the designated drain to prevent excess splash. Droplet precautions are maintained. The dialysis staff uses full PPE, including isolation gowns, masks (preferably N95 if available), appropriate eye protection, and gloves. The staff has been trained to don and doff their protective gear according to CDC protocols. The dialysis machine is cleaned and disinfected with 1:100 bleach wipes. The machines are not dedicated to any individual patient. The tubing and dialyzers are discarded in the red hazardous waste bins.
Patients with COVID-19 or PUIs Assigned to the Critical Care Setting
The nephrology team assesses the need for RRT and which modality is most appropriate. When in the patient room, full PPE is required. Limited medical staff exposure is advised and physical exam is performed only when necessary. Patients who receive continuous venovenous hemodialysis (CVVHD) require a dialysis catheter (untunneled or tunneled) for vascular access. The CVVHD effluent is directed into a dedicated drain to minimize splash and does not require any additional disinfection. CVVHD is performed by the critical care nursing staff wearing full PPE. Critical patients who receive intermittent hemodialysis are treated by the dialysis nursing staff in full PPE, as described previously. The dialysis nursing staff minimizes time in the patient room by sitting outside the glass partition as is possible. Intubation procedures are performed by the critical care team using the appropriate PPE including N95 masks.
Patients with COVID-19 or PUIs with AKI
Patients with AKI requiring RRT are triaged in the same manner as to whether they require intensive care or can be treated on the medical floor. An untunneled dialysis catheter is placed by either critical care, interventional radiology, or the nephrology team. If hemodynamically unstable, the patient is transferred to the intensive care unit (ICU) for either intermittent hemodialysis or CVVHD. If hemodynamically stable, the patient can be cohorted on a dedicated COVID-19 medical floor and receive bedside hemodialysis in their room. Hemodialysis nurses wear full PPE and minimize exposure time by sitting immediately outside of the doorway during the hemodialysis treatment. Planning meetings by the hospital and nephrology leadership have been ongoing to adapt to the rise in the number of patients with COVID-19. We have been able to increase our dialysis capacity on several dedicated COVID-19 floors by installing additional walled hemodialysis plumbing in the patient rooms. The goal is to try to further increase capacity by purchasing more hemodialysis machines and CVVHD machines; however, these supplies are in high demand. The major limiting factor is the number of rooms with hemodialysis plumbing on the COVID-19 cohort floors and the number of hemodialysis nursing staff available, because these individualized treatments in the patient’s room require one-to-one nursing. A potential future option for the patients with AKI is to provide acute peritoneal dialysis; however, we have not implemented this yet.
Montefiore Nephrology Service Census for COVID-19–Confirmed Cases
As of March 20, the Montefiore Medical Center inpatient nephrology services have cared for 20 patients with confirmed COVID-19: seven were patients with ESKD on hemodialysis (five receiving bedside hemodialysis in their room and two receiving CVVHD in the ICU) and 13 were patients with AKI (six not requiring RRT, five receiving CVVHD in the ICU, and two receiving hemodialysis in the ICU). One of the patients in the ICU died after withdrawal of care, and one patient with AKI died.
Discharge Planning for Patients with COVID-19 or PUIs
Discharge planning for hospitalized patients with confirmed COVID-19 or PUIs on hemodialysis requires appropriate planning and allocation to the outpatient facility, as described above. As described previously, the CDC has provided recommended guidelines for transport of a PUI or patient with documented COVID-19 to an outpatient hemodialysis (5). The local department of health must monitor every patient with confirmed COVID-19, perform an evaluation of residence, and provide PPE for cohabitants before discharge. The NYC Department of Health does not require a negative COVID-19 test to discharge a patient from a health care facility. As per the NYC Department of Health, after discharge, a patient with confirmed COVID-19 or PUIs should self-isolate and remind their household contacts to self-monitor (6). Self-isolation for persons who are not hospitalized and have COVID-19 or are PUIs is recommended for 7 days after onset of illness and 72 hours after being consistently afebrile (without antipyretics) with resolving respiratory symptoms, as per the NYC Department of Health (6). If discharge occurs before this self-isolation period, it is recommended that patients with confirmed COVID-19 and PUIs dialyze at an allocated COVID-19 facility or PUI designated last shift. The duration required for placing a discharged PUI on a PUI designated last shift, or patient with confirmed COVID-19 at a COVID-19 outpatient hemodialysis facility may need to be for a longer period. Future guidelines are needed regarding the timing of patient discharge from a COVID-19 hemodialysis facility to their home facility, and should consider the utility of requiring a negative COVID-19 viral test result when testing becomes more widely available.
Disclosures
M. Coco and M. Mokrzycki have nothing to disclose.
Funding
None.
Author Contributions
M. Coco was responsible for data curation; M. Mokrzycki conceptualized the article; and M. Mokrzycki and M. Coco wrote the original draft.
References
- 1.Department of Health, New York State : Novel coronavirus (COVID-19), 2020. Available at: https://coronavirus.health.ny.gov/home. Accessed March 17, 2020
- 2.American Society of Nephrology : Nephrologists Transforming Dialysis Safety, 2020. Available at: https://www.asn-online.org/ntds/. Accessed April 1, 2020
- 3.Centers for Disease Control and Prevention : Interim additional guidance for infection prevention and control recommendations for patients with suspected or confirmed COVID-19 in outpatient hemodialysis facilities, 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/healthcare-facilities/dialysis.html. Accessed April 1, 2020
- 4.American Society of Nephrology : COVID-19 information for providers of dialysis services, 2020. Available at: https://www.asn-online.org/ntds/resources/Webcast_2020_03_11_COVID-19.mp4. Accessed April 1, 2020
- 5.Centers for Disease Control and Prevention : Interim guidance for emergency medical services (EMS) systems and 911 public safety answering points (PSAPs) for COVID-19 in the United States, 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-for-ems.html. Accessed April 1, 2020
- 6.Health Department, New York City : Health alert #6: COVID-19 updates for New York City, 2020. Available at: https://www1.nyc.gov/assets/doh/downloads/pdf/han/alert/2020/covid-19-03152020.pdf. Accessed April 1, 2020