

Abstract
ADHD is a heterogeneous disorder that is highly impairing. Early, accurate diagnosis maximizes long-term positive outcomes for youth with ADHD. Tests of executive functioning (EF) are potential tools for screening and differential diagnosis of ADHD subtypes. However, previous research has been inconsistent regarding the specificity and magnitude of EF deficits across ADHD subtypes. Here, we advance knowledge of the EF-ADHD relationship by using: (1) dimensional latent factor models of ADHD that captures the heterogeneity of expression, and (2) a comprehensive, reliable battery of EF tasks and modeling relationships with a general factor of EF ability. We tested 1548 children and adolescents (ages 7–15 years) from the Texas Twin Project, a population-based cohort with a diverse socioeconomic and ethnic composition. We show that EF deficits were specific to the inattention domain of ADHD. Moreover, we found that the association between EF task performance and inattention was stable across sociodemographic groups. Our results demonstrate that failures of executive control are selectively manifested as covert inattentive symptoms, such as trouble with organization, forgetfulness, and distractedness, rather than overt symptoms, such as inappropriate talkativeness and interruption. Future research, utilizing a bifactor characterization of ADHD in clinical samples, is needed to further refine understanding of the nature of cognitive deficits in ADHD across the full range of symptom variation.
Keywords: ADHD, executive function, processing speed, inattention, hyperactivity, socioeconomic status
Introduction
Attention-Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder that increases an individual’s risk for negative life course outcomes, including poor academic performance, risky sexual behavior, substance use, and earlier mortality (Cuffe et al., 2015; Dalsgaard, Østergaard, Leckman, Mortensen, & Pedersen, 2015; Loe & Feldman, 2007; Usami, 2016). The public and private burdens of ADHD underscore the importance of understanding the disorder’s etiology and presentation. The present study investigates the role of cognitive deficits in ADHD, with a particular focus on executive function (EF) and processing speed. We aimed to advance this literature by improving EF measurement and examining the specificity of EF deficits across ADHD subtypes, clinical cut-offs, and sociodemographic groups.
Measurement of EF
ADHD is characterized by persistent difficulties in two domains of behavior: inattention and hyperactivity/impulsivity. Inattention involves difficulty sustaining focus during task performance, lack of persistence, and disorganization. Hyperactivity/impulsivity is characterized by difficulty remaining still or quiet, difficulty delaying gratification, and engaging in potentially harmful actions without considering consequences (National Institute of Mental Health, 2016). In line with the conceptualization of ADHD as a heterogeneous disorder characterized by multiple deficits, the dual-pathway model proposes two pathways to the development of ADHD (Sonuga-Barke, 2003). The motivational pathway involves hypersensitivity to delayed rewards resulting in difficulties with waiting, while the cognitive pathway involves deficits in EF (Sonuga-Barke, 2003; Barkley, 1997), defined as higher-order cognitive processes that enable goal-directed behaviors (Miyake et al., 2000).
EF domains typically include inhibition (the ability to control prepotent responses), working memory (the ability to maintain information in immediate memory simultaneous with cognitive processing), switching (the ability to efficiently shift attention to different stimuli or rules), and updating (the ability to monitor incoming stimuli and replace old information with new) (Diamond, 2013; Engle, 2002; Engelhardt, Briley, Mann, Harden, & Tucker-Drob, 2015). Additionally, processing speed, which is how quickly an individual can perceive information, process information and/or initiate a response (Shanahan et al., 2006), is sometimes treated by ADHD researchers as a component of EF (e.g., Brown, Reichel, & Quinlan, 2011). Other models of cognitive ability, however, conceptualize processing speed as a more basic ability that can affect the engagement of executive abilities. Individuals with slower processing speed may not process information fast enough for executive or decision-making processes to be engaged before other information or task demands are presented (Salthouse, 1996).
Consistent with the dual-pathway model, individuals with EF deficits are more likely to be diagnosed with ADHD (Seidman, 2006; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Individuals with a diagnosis of ADHD also show deficits on multiple measures of processing speed relative to controls (Shanahan et al., 2006; Willcutt, Pennington, Olson, Chhabildas, & Hulslander, 2005). But, the estimated magnitude of the association between ADHD and EF has varied depending on how EF is measured, as has the relative contribution of EF versus processing speed deficits.
The simplest measurement strategy uses single tasks to measure EFs (e.g., Willcutt et al., 2005; Boonstra et al., 2005; Biederman et al., 2004). For example, a backward digit span task is used to measure verbal working memory (WM). This approach can yield unreliable characterization of EF ability, as it is difficult to parse executive demands from other, more basic, task demands, such processing speed, when using single tasks (Miyake et al., 2000). The few studies that have considered the unique contributions of EF and processing speed to ADHD found that deficits in single-task EF performance among children with clinical ADHD were not significant after considering performance deficits on individual processing speed tasks (Rommelse et al., 2007).
Addressing this limitation, other studies have evaluated EF in ADHD using multiple measures of EF and processing speed, with each ability modeled as a single latent factor and multiple tasks tapping that ability as indicators. These studies found significant deficits in EF in individuals with ADHD, even after controlling for processing speed (Nigg et al., 2017), underscoring the need for further examination of these relations using dimensional measures that capture variance shared across tasks. These single factor models, however, diminish key understanding of how the “diversity” of EFs (Miyake et al., 2000) relate to ADHD. More recent studies of EF and ADHD have addressed this gap, using multiple regression factor models that estimated the unique contribution of different EF domains, and found contributions of specific domains, such as working memory and inhibition (McGrath et al., 2011; Brocki, Eninger, Thorell, & Bohlin, 2010).
Yet another statistical approach is to organize EF hierarchically to obtain a unifying EF factor that best captures common variance across different EF domains (Miyake et al., 2000; 2012). This general EF factor has been conceptualized as representing a cross-cutting ability to formulate and maintain goals (Friedman & Miyake, 2017) or as a general capacity for controlled attention (Engle, 2002). Our research group previously validated such a hierarchical model of EF in a middle childhood sample (Engelhardt et al., 2015). The existence of common variance shared across multiple EF domains and tasks raises the question of how a general factor of EF ability is related to ADHD. To our knowledge, no studies examining the effects of processing speed and EF on ADHD have been conducted in the context of a hierarchical model of EF, in which this unitary component is represented.
Measurement of ADHD
Studies of clinical populations suggest that EF might be differentially associated with ADHD subtypes (predominantly-inattentive [IA], predominantly-hyperactive/impulsive [HI], and combined [C]). Findings are inconsistent, however, with respect to which ADHD subtypes are associated with executive deficits and the relative magnitude of those associations (e.g. Geurts, Verté, Oosterlaan, Roeyers, & Sergeant, 2005; Saydam, Ayvaşik, & Alyanak, 2015; Wodka et al., 2008).
Previous research on the specificity of EF deficits in ADHD subtypes has heavily focused on clinical populations. Key meta-analytic research, that collated results of clinical and community-based studies, probed the validity of DSM-IV ADHD subtypes, and assessed their associations with external neuropsychological correlates (Willcutt et al., 2012). The results validated two distinct symptom dimensions of ADHD: inattention and hyperactivity/impulsivity, and demonstrated differential elevations in associations between external cognitive correlates, including working memory and processing speed, and the two symptom dimensions. Moreover, findings of the instability of the ADHD subtype classifications over the lifespan informed revisions of diagnostic terminology from ADHD ‘subtypes’ to ‘presentations’ to represent the fluidity of symptoms over time (DSM-5; American Psychological Association [APA], 2013). This is consistent with molecular genetic evidence that has shown that there is a strong correlation between genetic liability towards clinical diagnosis of ADHD and genetic liability toward continuously measured symptoms of hyperactivity/impulsivity and inattention in non-clinical populations (r > 0.9; Demontis et al., 2019). This further suggests that the cognitive processes characteristic of populations diagnosed with ADHD might also be relevant to populations with sub-clinical ADHD symptoms. Evaluating the specificity of EF deficits to ADHD presentations can be aided by examining the full range of symptom variation.
Paralleling advances in the measurement of EF, latent factor models have emerged as a useful tool for advancing understanding of the structure of continuously measured ADHD symptoms in non-clinical populations. Results drawn from this approach support a distinction between inattentive and hyperactive/impulsive symptom dimensions (Willcutt et al., 2012; Kuntsi et al., 2014; Martel, Roberts, Gremillion, von Eye, & Nigg, 2011; Toplak et al., 2009), noting that impulsivity is not clearly separable from hyperactivity, and that a two-factor model is more parsimonious than a three-factor model in which impulsivity is represented as a separate dimension (Willcutt et al. 2012).
Extending beyond the two-correlated factor model, contemporary research has highlighted models that use a bifactor approach, in which variation common to inattention and hyperactive/impulsive symptoms is explained by a latent factor representing ‘general’ ADHD psychopathology, and residual non-shared variation is captured in two domain-specific factors, to represent variation in ADHD (Martel, von Eye, & Nigg, 2012; Ullebø, Breivik, Gillberg, Lundervold, & Posserud, 2012). Using a bifactor approach, it is still unclear, however, whether non-shared variance is best captured by two or three specific factors, as previous work suggests good fit indices for both models (Arias, Ponce, & Núñez, 2018; Rodenacker, Hautmann, Görtz-Dorten, & Döpfner, 2016; Wagner et al., 2016) Importantly, where early clinical subtyping led to distinctions between the two domains, studies validating this approach in child and adolescent samples (e.g. Arias et al., 2018; Rodenacker et al., 2016; Martel et al., 2011) highlight the strength of the association between inattention and hyperactivity/impulsivity, suggesting significant overlap and interactions among associated etiological pathways that require further investigation (Sonuga-Barke, Sergeant, Nigg, & Willcutt 2008).
Goals of the Current Paper
Here, we extend research which has previously used latent factor characterizations of EF and ADHD by combining state-of-the-art models of both phenotypes in a middle childhood sample. This provides a refinement to the literature that reflects both advances in statistical modeling and developments in clinical conceptualization of ADHD.
Beyond cognitive characteristics, another strand of research has considered the role of demographic factors in the development and manifestation of ADHD symptoms. Generally, symptoms of ADHD attenuate with age, potentially due to better self-regulatory ability (Raffaelli, Crockett, & Shen, 2005), and differences in EF between children with ADHD and controls are more pronounced in younger samples (Nikolas & Nigg, 2015). And, some studies have found sex differences in the EF-ADHD association (Nikolas & Nigg, 2015), although others have found no moderating effects of sex (Seidman et al., 2005; Brocki & Bohlin, 2004). We examined the extent to which EF-ADHD relationships were consistent across age and sex, as well as across race and socioeconomic status (SES). These analyses help to establish the extent to which the relationship between EF and ADHD is broadly generalizable across the population.
Method
Participants
Participants were 1548 children aged 7.80 to 15.25 (M=10.93, SD=1.79, 52.4% female), recruited as part of the Texas Twin Project, an ongoing study of child and adolescent multiples from the greater Austin and Houston areas (Harden, Tucker-Drob, & Tackett, 2013). This sample is ethnically and socioeconomically representative of the surrounding populations: 72.6% of participants identified as non-Hispanic Caucasian, 12.5% as Hispanic/Latino, 4.9% as African-American, 3.4% as Asian, 6.3% as multiple races or ethnicities, and 0.3% as other. Though participants were twins or other multiples, the current study treated them as unique observations; the non-independence of observations arising from individuals being nested within the same family was accounted for across all analyses (see Analyses). Children whose parents reported they would be unable to complete the written or verbal study tasks were not enrolled in the study. We did not exclude on the basis of any other conditions, including psychiatric diagnoses.
Measures
ADHD symptoms.
Symptoms of inattention and hyperactivity/impulsivity were assessed by participants’ parents using 20 items from the Conners-3 rating scales (Conners, 2008). Items were rated on a 4-point scale (from “not at all” to “very often”). Examples of items are ‘Doesn’t pay attention to details; makes careless mistakes’ for inattention, and ‘Acts as if driven by a motor’ for hyperactivity/impulsivity (see Table S5 in the Supplementary Materials for a list of all items). Parents rated each twin or multiple separately.
ADHD clinical categories.
For supplemental analyses, we followed the Conners-3 scoring guidelines to determine whether individuals met threshold clinical criteria for the following presentations of ADHD: predominantly inattentive [ADHD-IA], predominantly hyperactive-impulsive [ADHD-HI], and combined type [ADHD-C]. Per the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), individuals who had six or more symptoms counts in either or both domains met the clinical cut-off for ADHD. Within our sample, 13.7% of participants met the symptom count threshold for any form of ADHD (8.7% Inattentive, 8.4% Hyperactive, 3.4% Combined Type). While the prevalence in our sample is higher than clinical prevalence rates (5.9–7.1%; Willcutt, 2012), it is consistent with threshold ADHD symptom prevalence rates reported in several community-based child samples (11.2–15.5%; Rowland et al., 2015; Holbrook et al., 2016). These categorical variables representing ADHD, however, do not account for additional measures, including clinician interviews with caregivers, teacher rating forms, etc. that contribute to clinical assessment, and should not be regarded as diagnostic.
Executive functions.
The current study included 15 tasks assessing 4 EF domains: inhibition, switching, working memory, and updating (see Table S1 for detailed descriptions and reliability statistics of each task). Tasks were administered orally, on the computer, or on paper. Inhibition was assessed with four tasks: Animal Stroop (Wright, Waterman, Prescott, & Murdoch-Eaton, 2003), Mickey (Lee, Bull, & Ho, 2013), and Stop Signal. The study originally used an auditory Stop Signal task (Logan, Schachar, & Tannock, 1997), which was replaced with a visual Stop Signal task (Verbruggen, Logan, & Stevens, 2008) after the third year of data collection to accommodate the needs of administering EF tasks in the MRI scanner. Switching was assessed using four tasks: Trail Making (Salthouse, 2011), Local-Global (Miyake et al., 2000), Plus-Minus (Miyake et al., 2000), and a computerized Cognitive Flexibility task (Baym, Corbett, Wright, & Bunge, 2008). Cognitive Flexibility replaced the Plus-Minus task, again to accommodate MRI task administration after the third year of data collection. Working memory was assessed using three tasks: Symmetry Span (Kane et al., 2004), Digit Span Backward (Wechsler, 2003), and Listening Recall (Daneman & Carpenter, 1980). These tasks tap spatial, verbal, and auditory working memory, respectively. Updating was assessed with four tasks: Keeping Track (Miyake et al., 2000), Running Memory for Letters (Broadway & Engle, 2010), 2-Back task (Jaeggi, Buschkuehl, Perrig, & Meier, 2010), and, as a replacement to the 2-Back task after the third year of data collection, a 1- and 2-back task (Jaeggi et al., 2010). Data coverage across all tasks is provided in Table S3.
Our research group (Engelhardt et al., 2015; 2016) previously demonstrated that variation in EF is best captured by a hierarchical factor model, with individual EF tasks loading onto one of four latent factors representing each EF domain and each of these loading onto a common EF factor. This same hierarchical model (fit statistics: RMSEA=0.04, χ²(49)=169.97, p<0.001, SRMR=0.04; see Figure S1) was adopted in all the analyses presented in the current research.
Processing speed.
Three tasks were used to construct a latent measure of processing speed: Symbol Search (Wechsler, 2003), Pattern Comparison, and Letter Comparison (Salthouse & Babcock, 1991). Each task assessed how quickly and accurately participants identified similarities between symbols, patterns, or letters. See Table S2 for detailed description of the tasks and Figure S2 for model parameters (fit statistics: RMSEA= 0.00, CFI=1.00, SRMR=0.00).
Sociodemographic characteristics.
Parents completed a demographic survey regarding the age, sex, and race of their children, as well as their own sex, race, educational attainment, and household income. A composite index consisting of parent-reported household income and parental education (years of completed education averaged across both parents) was used to represent SES.
Analyses
All analyses were conducted using structural equation modelling implemented with Mplus version 8 software (Muthén and Muthén, 2017). The ‘TYPE=COMPLEX’ command was used for all analyses to account for non-independence of observations (twins nested within families). The first set of analyses used ordinal item-level data, so weighted least squares estimation was employed in MPlus. Subsequent models used full information maximum likelihood to account for missing data by design. For models using binary-coded diagnostic categories of ADHD, a Bayesian estimator was specified to allow convergence (Muthén, Muthén, & Asparouhov, 2015).
Analyses were conducted in four steps. First, we conducted confirmatory factor analytic models of item-level symptom data in order to determine the best-fitting model for the ADHD symptoms. Five confirmatory factor models of ADHD were fit and evaluated based on model fit indices (see Tables S4 and S6). Model fit was evaluated using the chi-squared test (χ2), root mean square error of approximation (RMSEA), comparative-fit index (CFI), and Tucker-Lewis index (TLI). Model fit comparisons were conducted using χ2difference tests, and were adjusted for with the scaling correction factor provided by Mplus (Satorra & Bentler, 2010).
Second, we parcelled item-level symptom data to avoid estimation issues in subsequent models of ADHD symptoms (Rhemtulla, Brosseau-Liard, & Savalei, 2012). Specifically, symptom parcels were constructed by summing the scores of two Conners-3 items, resulting in 10 parcels (5 parcels for each domain; see Table S5) that could be treated as continuous variables. The selection of items for each parcel was based on whether the items had similar loadings on the latent ADHD factors in the best-fitting model from the first step. For example, ‘Has trouble organizing tasks or activities’ and ‘Fails to complete schoolwork, chores or tasks’ showed similar loadings on a inattention factor (λ = .698 and λ = .692, respectively) and were consequently incorporated into the same parcel. The parcels ranged in value from 0 to 6 and were not normally distributed due to inflation of zero responses (Figure S3). However, previous work has found that treating categorical variables as continuous using robust maximum likelihood estimation (MLR) produces unbiased estimates of factor correlations, even when the category thresholds are asymmetric, as long as there are five or more categories (Rhemtulla et al., 2012).
Third, we conducted multivariate regressions that estimated associations between general EF, processing speed, and ADHD outcomes using a stepwise approach. We first accounted for all the variance in ADHD by processing speed, and then estimated the unique contribution of EF. Previous work in this sample found that both factor loadings and intercepts of the individual EF measures are measurement invariant across age groups (Engelhardt et al., 2015) and that general EF accounted for age-related differences in WM and updating, but not inhibition and switching (Hartung et al., 2020), suggesting the need to account for individual differences at the first-order domain-specific level for EF. For ADHD, individual symptoms have been shown to vary based on age (Harvey, Lugo-Candelas & Breaux, 2015) and sex (Mowlem, Agnew-Blais, Taylor, & Asherson, 2019). Taken together, and to maintain consistency with previous analyses of these variables in this dataset (Engelhardt et al., 2015; 2016; Malanchini et al., 2019), the main effects of age and sex were controlled for at the level of the first-order EF factors, at the level of the parcels for ADHD, and at the factor-level for processing speed. We estimate separate models that included and excluded processing speed.
We also conducted post-hoc analyses to assess the specificity of processing speed and EF relations. In this model, rather than the general EF factor, each domain-specific factor was regressed on processing speed, and we re-estimated the unique variance in the ADHD factors associated with Common EF (Figure S4).
Fourth, latent variable interaction models (Figure S5) were conducted using the XWITH syntax in Mplus to test whether the associations between Common EF and ADHD outcomes were moderated by key sociodemographic variables (age, race, sex, and family SES). In consideration of the large age range of our sample, and the known differences in EF ability and ADHD symptoms across this developmental range (Huizinga, Dolan, & van der Molen, 2006; Ramtekkar, Reiersen, Todorov, & Todd, 2010), we assessed both linear (i.e. chronological) and non-linear (i.e. age2) main and interactive effects of age. Given the number of interactions needed to examine the moderating effects at all levels of each sociodemographic variable (7 moderators across each of 3 ADHD domains), we used the Benjamini-Hochberg false discovery rate method (Benjamini & Hochberg, 1995) to correct for effects of multiple testing. FDR-adjusted thresholds for significance were calculated using the p.adjust function in R.
Results
A Bifactor Model is the Best-Fitting Model of ADHD Symptoms
We compared the fit of the following confirmatory factor models of ADHD: (1) a one-factor model, in which all items were regressed onto a single latent ADHD factor; (2) a correlated two-factor model comprised of latent inattention and hyperactivity/impulsivity factors; (3) a correlated three-factor model in which items within the hyperactivity-impulsivity factor were further divided into independent hyperactivity and impulsivity latent factors; (4) a two-dimension bifactor model in which individual items simultaneously loaded onto a general ADHD factor and specific inattention and hyperactivity/impulsivity factors; and (5) a three-dimension bifactor model which further split the hyperactivity-impulsivity residual variance into two distinct factors. Table S6 includes the model fit statistics.
The two-dimension a model provided the best fit for the data (χ2(25) = 75.18, p < 0.001; RMSEA = 0.05, CFI = 0.99; Figure 1). This result is consistent with previous studies (Toplak et al., 2009; Martel et al., 2011).
Figure 1. Bifactor model of parent-rated ADHD symptoms.
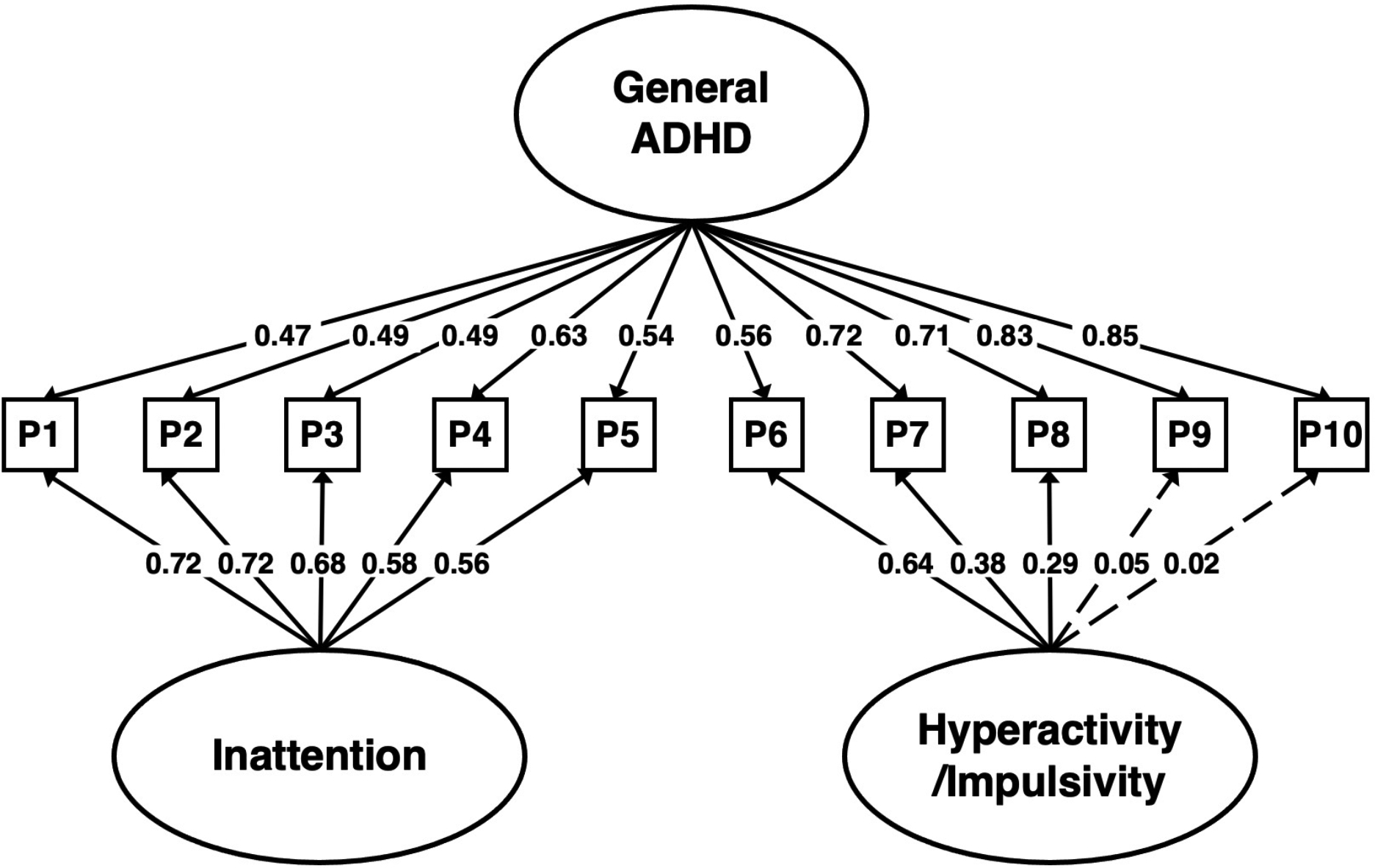
Solid paths are significantly different from zero at p < .01. All point estimates are standardized. Non-significant loadings were dropped in subsequent models. Fit statistics: RMSEA=0.04, χ2(25)=75.18, p<0.001, CFI=0.99, TLI=0.98, SRMR=0.02.
Inattention, but Not Hyperactivity/Impulsivity, is Uniquely Associated with EF Deficits
The bifactor model of ADHD, with two specific factors, was employed to partition variance common across all symptom parcels from variance unique to the inattention and hyperactivity/impulsivity domains. All factors were regressed on EF. EF was most strongly associated with the inattention factor (β = −0.24, p < 0.01; Figures 2–3a). A weaker but significant association also emerged between EF and general ADHD (β = −0.12, p < 0.05). EF was not significantly associated with hyperactivity/impulsivity.
Figure 2. Standardized regression coefficients of ADHD symptom factors on EF, before and after adjusting for processing speed differences.
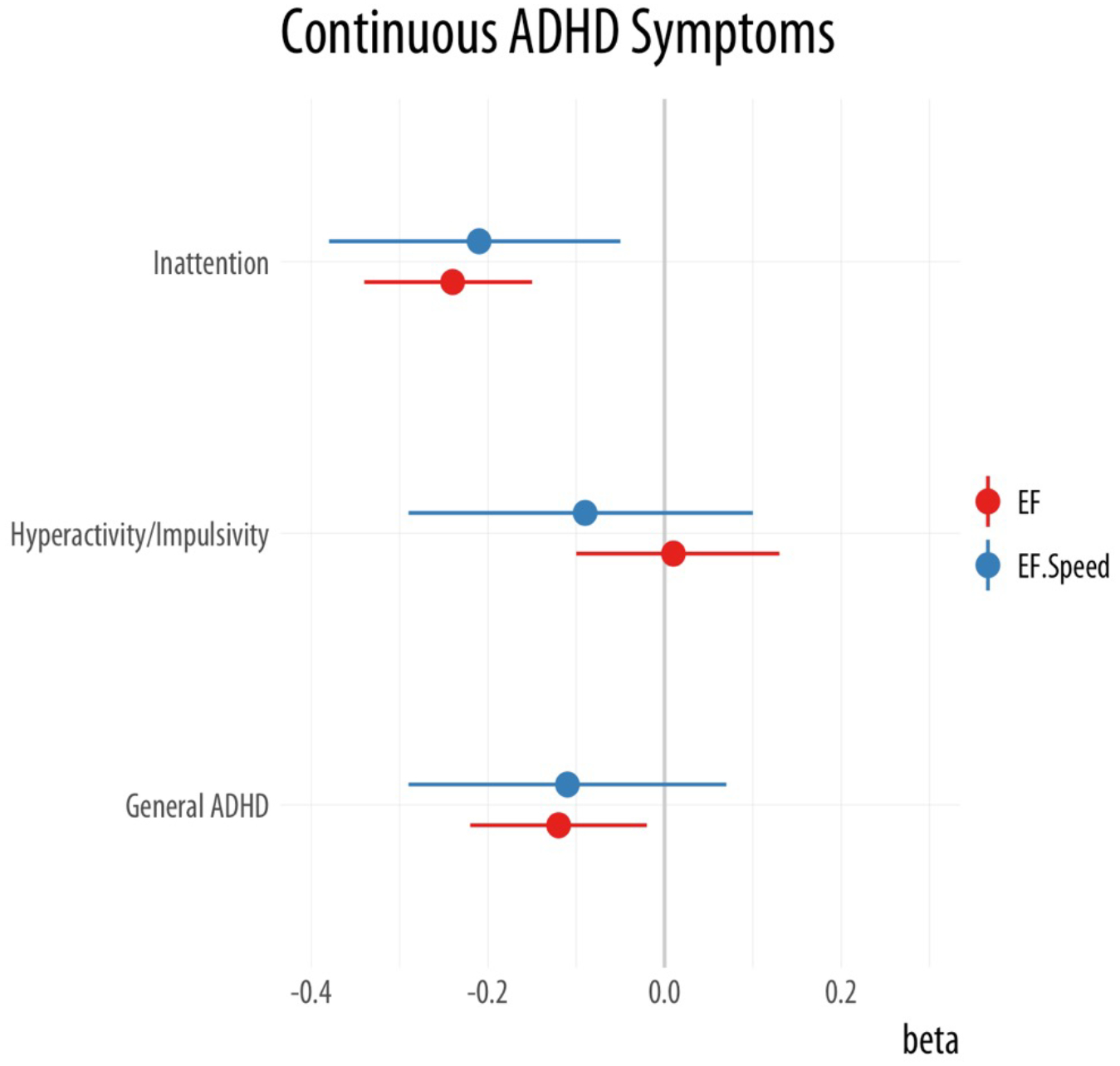
Bars represent the 95% confidence intervals. Note. EF.Speed represents EF controlling for effects of processing speed.
Figure 3. Bifactor ADHD regressed onto executive functioning (EF): (a) before and (b) after accounting for the effects of processing speed.
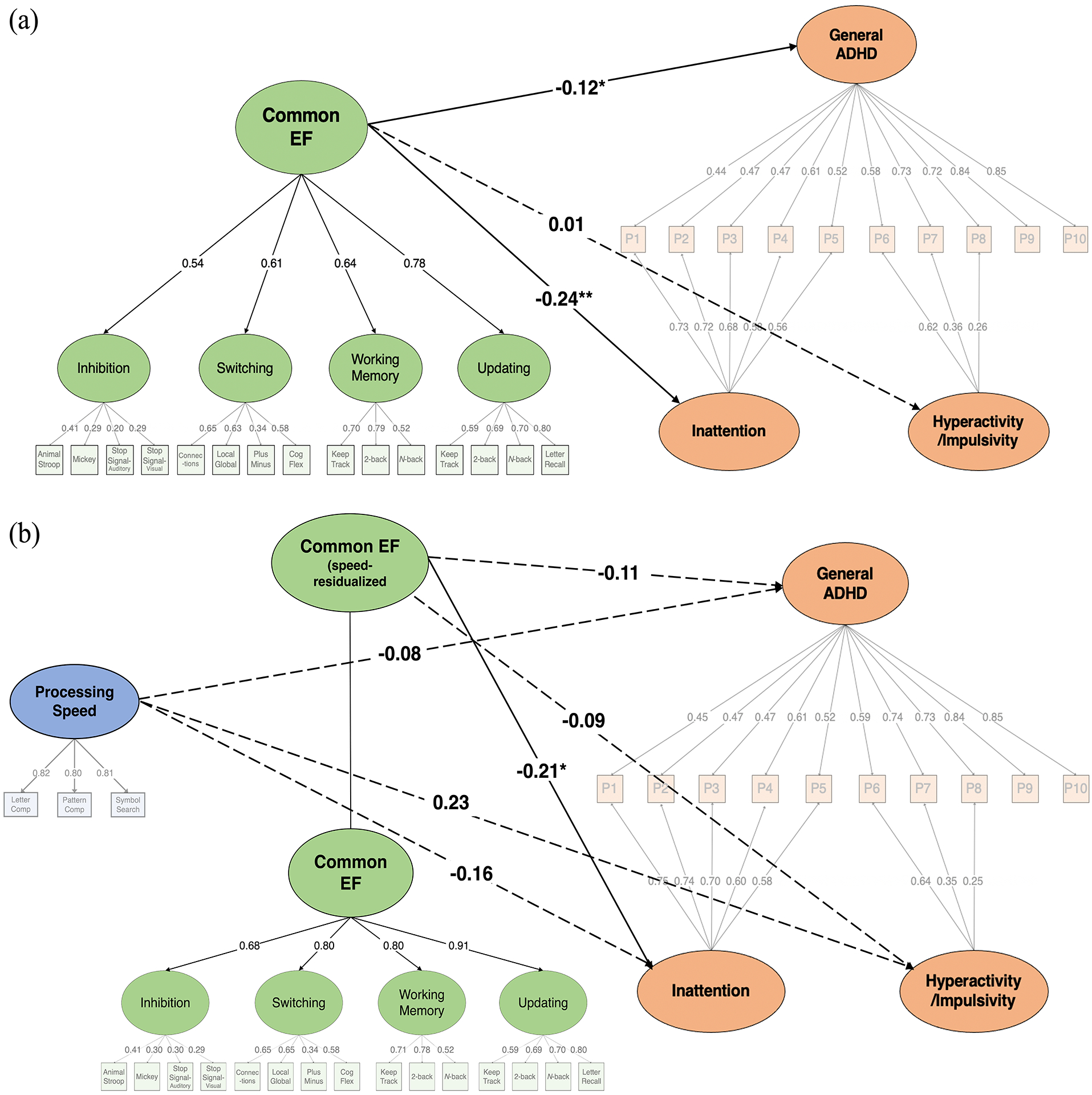
All point estimates are standardized regression coefficients. Age and sex were included as covariates in these models. The effects of age and sex were controlled for at the factor level for processing speed, the level of first-order factor for EF, and at the indicator-level for ADHD. Fit statistics: (a) RMSEA=0.07, χ2(358)=2985.32, p<0.001, CFI=0.80, TLI=0.77, SRMR=0.14; (b) RMSEA=0.02, χ2(349)=646.57, p<0.001, CFI=0.98, TLI=0.97, SRMR=0.04.
Note. Solid paths indicate significance (*p<0.05; **p<0.01).
Relationship between EF and Inattentive Symptoms is Not Entirely Reducible to Processing Speed Differences
After including processing speed in the model, we next examined whether the EF-ADHD association was attenuated. A negative association between EF and inattention remained after accounting for variance explained by processing speed (β = −0.21, p < 0.05). However, the link between EF and general ADHD was attenuated and no longer significant (Figures 2 and 3b, Table S7). The contribution of processing speed to inattention was not significant (β = −0.16, p = 0.10). Together, EF and processing speed accounted for 12.3% of the variance in inattention (R2 = 0.123, p < 0.01).
Post-hoc analyses, considering an alternate model in the processing speed – EF relationship was modeled at the level of the domain-specific EF factors, revealed consistent results: EF continued to be predictive of inattention (β = −0.12, p < 0.05), but not general ADHD or hyperactivity/impulsivity (Table S11). Additionally, significant associations between processing speed and inattention (β = −0.33, p < 0.01), and general ADHD (β = −0.17, p < 0.05), emerged. Of note, while our full model demonstrate very good fit (χ2(349)=646.57, p<0.0001; RMSEA=0.02, CFI=0.98, TLI=0.97), the alternate model demonstrated better model fit when compared to the original model (χ2(346)=613.44, p<0.0001; RMSEA=0.02, CFI=0.98, TLI=0.98; SRMR=0.04; χdiff2(3)=34.28, p<0.001). These post-hoc analyses suggest that the specificity of the observed association with inattention is robust to how we characterize the EF-processing speed relation, but the extent to which all the cognitive deficits in ADHD domains can be attributed to EF versus processing speed depends on how the relationships between cognitive abilities are modeled.
Finally, we conducted supplementary analyses examining the relation between speed, EF, and individuals who met threshold symptom counts for each ADHD presentation. Across threshold presentation categories (combined-, inattentive-, and hyperactive-impulsive presentation), the association between EF and ADHD was not significant beyond processing speed. Refer to supplementary materials for full model results (see Figures S6a–c, Table S7).
Association between EF and Inattentive Symptoms is Stable across Sociodemographic Characteristics
Socioeconomic status and demographic factors did not significantly moderate the relation between speed-residualized EF and general or domain-specific ADHD (Tables S8 and S9).
While there were no main effects of sex on PS, speed-residualized EF, or ADHD domains (p > 0.05), there were small effects of race on EF (βhispanic = −0.16, p < 0.01; βblack = −0.14, p < 0.05, reflecting lower mean EF performance compared to White children), and SES on PS (r = 0.12, p < 0.01) and EF (r = 0.17, p < 0.05, Table S10), and substantial effects of age on PS (r = 0.77, p < 0.01), Common EF (r = 0.73, p < 0.001, Table S10), and general ADHD (β = −0.25, p < 0.001, Table S8).
Discussion
The functional and psychosocial burden associated with a diagnosis of ADHD is profound (Caci et al., 2014). Beyond clinical populations, a substantial proportion of children present with subclinical, yet often debilitating, ADHD symptoms (6.6% in the United States; Fayyad et al., 2017), which are similarly associated with adverse scholastic and functional outcomes (Currie & Stabile, 2006). The cognitive profile of ADHD across the full range of symptom presentation has not been the subject of detailed investigation. The present study examined the association between variation in EF and ADHD, in a sample of the general population, considering the continuous range of symptom variation.
Findings from the present study are consistent with the proposition that executive deficits characterize the cognitive profile of individuals with ADHD, and that EF deficits specifically relate to the inattention domain (Brocki et al., 2010). This is consistent with neurocognitive theories of ADHD, particularly the dual-pathway model, that identify deficits in executive function as a major pathway to the development of ADHD (Sonuga-Barke, 2003; Barkley, 1997). The specificity of the association between EF and the inattention domain further corroborates the conceptualization of ADHD as an etiologically heterogeneous disorder.
In the current study, executive deficits were not linked to individual differences in hyperactive-impulsive symptoms. Previous research has demonstrated that no impairment in EF measures was observed in children with ADHD-HI, once symptoms of inattention were controlled for (Chhabildas et al., 2001). In additional support, after controlling for hyperactivity-impulsivity, symptoms of inattention-disorganization were found to be uniquely associated with EF deficits (Nigg et al., 2005). A further possibility is that the hyperactivity/impulsivity domain is characterized by a different neuropsychological profile than that of the inattentive domain. Motivational difficulties have been proposed as a potential pathway to the development of hyperactive/impulsive symptoms (Sonuga-Barke, 2003), supported by research demonstrating differential relations between EF and delay aversion, a mediator of motivation, and ADHD symptom domains (Thorell, 2007). Notably, the lack of association observed between the general ADHD factor, which accounts for variance shared between inattentive and hyperactive-impulsive symptoms, and EF, after controlling for the effects of processing speed, further substantiates distinct etiological pathways driving domain-specific ADHD symptoms (Kuntsi et al., 2014). Extending this, future research that jointly considers cognitive and motivational constructs, in the context of a bifactor conceptualization of ADHD, would allow one to test the purported uniqueness of the pathways leading to the development of inattention and hyperactivity/impulsivity.
Our results were consistent across all levels of the sociodemographic distribution. Age, sex, socioeconomic status, and race were not found to moderate the EF-ADHD association. Given the broad age range of participants in the study, and strong evidence for the individual effect of age on EF performance (Huizinga et al., 2006) and ADHD (Ramtekkar et al., 2010) in our sample and previous research, the lack of age moderation might be surprising. But we note that, whereas hyperactivity/impulsivity symptoms decline with age (Raffaelli et al., 2005), predominantly inattentive presentation ADHD tends to be a more stable diagnosis over time, and combined-presentation diagnoses often convert to an predominantly inattentive diagnosis as hyperactive-impulsive symptoms diminish with age (Hurtig et al., 2007). The specificity of the EF-inattention link might contribute to its consistency across ages. Overall, the present results suggest that the relation between EF and ADHD, and specifically EF and inattention, is stable across sociodemographic groups, and provides a useful sensitivity check of the main effects, bolstering our characterization of the cognitive model of ADHD.
Our findings should be considered in light of a few limitations. First, the current investigation employed a cross-sectional design, which limits our ability to interpret the direction of effects in the association between EF and ADHD. Second, the wide age range of our participants may have prevented us from identifying differential patterns of associations over development (Happé, Booth, Charlton, & Hughes, 2006). However, the lack of an observed moderating effect of age, when modeled both linearly and quadratically, appears to contradict this proposition. Third, although our decisions on how to model item-level data on ADHD symptoms were guided by previous work (Little et al., 2013; Rhemtulla et al., 2012), alternative approaches to modeling could have been implemented. Finally, though we tested multiple competing factor models of ADHD, we were unable to evaluate all possible variations of these factor structures. For example, recent research suggests that an S-1 bifactor model (Eid et al., 2017) – an alternative to the symmetric bifactor approach employed in this paper – may be advantageous for representing specific ADHD subtypes (Burns, Geiser, Servera, Becker, & Beauchaine, 2020), though may be less equipped to capture a general propensity toward ADHD (Willoughby, 2020). Future research would benefit from continuing to refine the latent architecture of ADHD and to examine whether variation in factor structure influences associations with external cognitive correlates.
Employing the bifactor characterization of ADHD symptom structure, in a general population sample, the current study found that a specific link between a superordinate ‘Common EF’ factor and the inattention, but not hyperactive-impulsivity or shared, dimension of ADHD symptoms, an effect observed to be independent of processing speed. Utilizing updated latent modeling approaches, the study widens the scope of ADHD research beyond clinical cut-offs and provides further refinement of modeling approaches to existing neurocognitive models of ADHD likely to inform future research in clinical and community samples.
Supplementary Material
Research Highlights.
Variation in ADHD in population-based samples includes domain-general (common ADHD) and domain-specific (Inattention and Hyperactivity/Impulsivity) variance.
We examined how executive function modeled as variance shared across (Common EF), versus variance specific to individual EF domains and tasks, relates to ADHD.
Common EF was uniquely associated with the ADHD Inattention domain, even after accounting for the effects of processing speed.
Acknowledgements.
We are grateful to the families within the Texas Twin Study cohort that participated in this study. This research was supported a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant, R01HD083613 (KPH, EMTD), a University of Texas at Austin Population Research Center NIH grant, R24HD042849 (KPH, EMTD), and Jacobs Foundation Research Fellowships (KPH, EMTD).
Footnotes
Conflicts of Interest. The authors have declared no conflicts of interest.
Ethical Considerations. Informed consent was obtained from parents of all children who participated in this study. The University of Texas Institutional Review Board granted ethical approval.
Data availability.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
- American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revision). Washington, DC: Author. [Google Scholar]
- Arias VB, Ponce FP, & Núñez DE (2018). Bifactor models of attention-deficit/hyperactivity disorder (ADHD): An evaluation of three necessary but underused psychometric indexes. Assessment, 25(7), 885–897. [DOI] [PubMed] [Google Scholar]
- Barkley RA (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychological bulletin, 121(1), 65. [DOI] [PubMed] [Google Scholar]
- Baym CL, Corbett BA, Wright SB, & Bunge SA (2008). Neural correlates of tic severity and cognitive control in children with Tourette syndrome. Brain, 131(1), 165–179. [DOI] [PubMed] [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal statistical society: series B (Methodological), 57(1), 289–300. [Google Scholar]
- Biederman J, Monuteaux MC, Doyle AE, Seidman LJ, Wilens TE, Ferrero F, … & Faraone SV (2004). Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. Journal of consulting and clinical psychology, 72(5), 757. [DOI] [PubMed] [Google Scholar]
- Boonstra M, Oosterlaan J, Sergeant J, & Buitelaar J (2005). Executive functioning in adult ADHD: a meta-analytic review. Psychological medicine. [DOI] [PubMed] [Google Scholar]
- Broadway JM, & Engle RW (2010). Validating running memory span: Measurement of working memory capacity and links with fluid intelligence. Behavior Research Methods, 42(2), 563–570. [DOI] [PubMed] [Google Scholar]
- Brocki KC, & Bohlin G (2004). Executive functions in children aged 6 to 13: A dimensional and developmental study. Developmental neuropsychology, 26(2), 571–593. [DOI] [PubMed] [Google Scholar]
- Brocki KC, Eninger L, Thorell LB, & Bohlin G (2010). Interrelations between executive function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: A two year longitudinal study. Journal of abnormal child psychology, 38(2), 163–171. [DOI] [PubMed] [Google Scholar]
- Brown TE, Reichel PC, & Quinlan DM (2011). Executive function impairments in high IQ children and adolescents with ADHD. Open Journal of Psychiatry, 1(02), 56. [Google Scholar]
- Burns GL, Geiser C, Servera M, Becker SP, & Beauchaine TP (2020). Application of the bifactor S–1 model to multisource ratings of ADHD/ODD symptoms: An appropriate bifactor model for symptom ratings. Journal of Abnormal Child Psychology, 48(7), 881–894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caci H, Doepfner M, Asherson P, Donfrancesco R, Faraone SV, Hervas A, & Fitzgerald M (2014). Daily life impairments associated with self-reported childhood/adolescent attention-deficit/hyperactivity disorder and experiences of diagnosis and treatment: Results from the European Lifetime Impairment Survey. European Psychiatry, 29(5), 316–323. [DOI] [PubMed] [Google Scholar]
- Chhabildas N, Pennington BF, & Willcutt EG (2001). A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. Journal of abnormal child psychology, 29(6), 529–540. [DOI] [PubMed] [Google Scholar]
- Conners CK (2008). Conners 3rd edition manual. Toronto, Ontario, Canada: Multi-Health Systems. [Google Scholar]
- Cuffe SP, Visser SN, Holbrook JR, Danielson ML, Geryk LL, Wolraich ML, & McKeown RE (2015). ADHD and Psychiatric Comorbidity: Functional Outcomes in a School-Based Sample of Children. Journal of Attention Disorders. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Currie J, & Stabile M (2006). Child mental health and human capital accumulation: the case of ADHD. Journal of health economics, 25(6), 1094–1118. [DOI] [PubMed] [Google Scholar]
- Dalsgaard S, Østergaard SD, Leckman JF, Mortensen PB, & Pedersen MG (2015). Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: a nationwide cohort study. The Lancet, 385(9983), 2190–2196. [DOI] [PubMed] [Google Scholar]
- Daneman M, & Carpenter PA (1980). Individual differences in working memory and reading. Journal of verbal learning and verbal behavior, 19(4), 450–466. [Google Scholar]
- Demontis D, Walters RK, Martin J, Mattheisen M, Als TD, Agerbo E, … & Cerrato F (2019). Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nature genetics, 51(1), 63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond A (2013). Executive functions. Annual review of psychology, 64, 135–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eid M, Geiser C, Koch T, & Heene M (2017). Anomalous results in G-factor models: Explanations and alternatives. Psychological methods, 22(3), 541. [DOI] [PubMed] [Google Scholar]
- Engelhardt LE, Briley DA, Mann FD, Harden KP, & Tucker-Drob EM (2015). Genes unite executive functions in childhood. Psychological science, 26(8), 1151–1163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engelhardt LE, Mann FD, Briley DA, Church JA, Harden KP, & Tucker-Drob EM (2016). Strong genetic overlap between executive functions and intelligence. Journal of Experimental Psychology: General, 145(9), 1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engle RW (2002). Working memory capacity as executive attention. Current directions in psychological science, 11(1), 19–23. [Google Scholar]
- Fayyad J, Sampson NA, Hwang I, Adamowski T, Aguilar-Gaxiola S, Al-Hamzawi A, … Kessler RC (2017). The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Attention Deficit and Hyperactivity Disorders, 9(1), 47–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman NP, & Miyake A (2017). Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex, 86, 186–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geurts HM, Verté S, Oosterlaan J, Roeyers H, & Sergeant JA (2005). ADHD subtypes: do they differ in their executive functioning profile?. Archives of Clinical Neuropsychology, 20(4), 457–477. [DOI] [PubMed] [Google Scholar]
- Happé F, Booth R, Charlton R, & Hughes C (2006). Executive function deficits in autism spectrum disorders and attention-deficit/hyperactivity disorder: examining profiles across domains and ages. Brain and cognition, 61(1), 25–39. [DOI] [PubMed] [Google Scholar]
- Harden KP, Tucker-Drob EM, & Tackett JL (2013). The Texas twin project. Twin Research and Human Genetics, 16(1), 385–390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartung J, Engelhardt LE, Thibodeaux ML, Harden KP, & Tucker-Drob EM (2020). Developmental transformations in the structure of executive functions. Journal of experimental child psychology, 189, 104681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harvey EA, Lugo-Candelas CI, & Breaux RP (2015). Longitudinal changes in individual symptoms across the preschool years in children with ADHD. Journal of Clinical Child & Adolescent Psychology, 44(4), 580–594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holbrook JR, Cuffe SP, Cai B, Visser SN, Forthofer MS, Bottai M, … & McKeown RE (2016). Persistence of parent-reported ADHD symptoms from childhood through adolescence in a community sample. Journal of Attention Disorders, 20(1), 11–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huizinga M, Dolan CV, & van der Molen MW (2006). Age-related change in executive function: Developmental trends and a latent variable analysis. Neuropsychologia, 44(11), 2017–2036. [DOI] [PubMed] [Google Scholar]
- Hurtig T, Ebeling H, Taanila A, Miettunen J, Smalley SL, McGough JJ, … & Moilanen IK (2007). ADHD symptoms and subtypes: relationship between childhood and adolescent symptoms. Journal of the American Academy of Child & Adolescent Psychiatry, 46(12), 1605–1613. [DOI] [PubMed] [Google Scholar]
- Jaeggi SM, Buschkuehl M, Perrig WJ, & Meier B (2010). The concurrent validity of the N-back task as a working memory measure. Memory, 18(4), 394–412. [DOI] [PubMed] [Google Scholar]
- Kane MJ, Hambrick DZ, Tuholski SW, Wilhelm O, Payne TW, & Engle RW (2004). The generality of working memory capacity: a latent-variable approach to verbal and visuospatial memory span and reasoning. Journal of Experimental Psychology: General, 133(2), 189. [DOI] [PubMed] [Google Scholar]
- Kuntsi J, Pinto R, Price TS, van der Meere JJ, Frazier-Wood AC, & Asherson P (2014). The separation of ADHD inattention and hyperactivity-impulsivity symptoms: pathways from genetic effects to cognitive impairments and symptoms. Journal of abnormal child psychology, 42(1), 127–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee K, Bull R, & Ho RM (2013). Developmental changes in executive functioning. Child development, 84(6), 1933–1953. [DOI] [PubMed] [Google Scholar]
- Little TD, Rhemtulla M, Gibson K, & Schoemann AM (2013). Why the items versus parcels controversy needn’t be one. Psychological methods, 18(3), 285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loe IM, & Feldman HM (2007). Academic and educational outcomes of children with ADHD. Journal of pediatric psychology, 32(6), 643–654. [DOI] [PubMed] [Google Scholar]
- Logan GD, Schachar RJ, & Tannock R (1997). Impulsivity and inhibitory control. Psychological science, 8(1), 60–64. [Google Scholar]
- Malanchini M, Engelhardt LE, Grotzinger AD, Harden KP, & Tucker-Drob EM (2019). “Same but different”: Associations between multiple aspects of self-regulation, cognition, and academic abilities. Journal of Personality and Social Psychology, 117(6), 1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martel MM, Roberts B, Gremillion M, Von Eye A, & Nigg JT (2011). External validation of bifactor model of ADHD: Explaining heterogeneity in psychiatric comorbidity, cognitive control, and personality trait profiles within DSM-IV ADHD. Journal of abnormal child psychology, 39(8), 1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martel MM, Von Eye A, & Nigg J (2012). Developmental differences in structure of attention-deficit/hyperactivity disorder (ADHD) between childhood and adulthood. International journal of behavioral development, 36(4), 279–292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGrath LM, Pennington BF, Shanahan MA, Santerre‐Lemmon LE, Barnard HD, Willcutt EG, … & Olson RK (2011). A multiple deficit model of reading disability and attention‐deficit/hyperactivity disorder: Searching for shared cognitive deficits. Journal of Child Psychology and Psychiatry, 52(5), 547–557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miyake A, & Friedman NP (2012). The nature and organization of individual differences in executive functions: Four general conclusions. Current directions in psychological science, 21(1), 8–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, & Wager TD (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive psychology, 41(1), 49–100. [DOI] [PubMed] [Google Scholar]
- Mowlem F, Agnew-Blais J, Taylor E, & Asherson P (2019). Do different factors influence whether girls versus boys meet ADHD diagnostic criteria? Sex differences among children with high ADHD symptoms. Psychiatry research, 272, 765–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK and Muthén BO (1998–2017). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén [Google Scholar]
- Muthén BO, Muthén LK, & Asparouhov T (2015). Estimator choices with categorical outcomes. Mplus. [Google Scholar]
- National Institute of Mental Health (2016, March). Attention Deficit Hyperactivity Disorder. Retrieved from https://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml
- Nigg JT, Jester JM, Stavro GM, Ip KI, Puttler LI, & Zucker RA (2017). Specificity of executive functioning and processing speed problems in common psychopathology. Neuropsychology, 31(4), 448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nigg JT, Stavro G, Ettenhofer M, Hambrick DZ, Miller T, & Henderson JM (2005). Executive functions and adhd in adults: Evidence for selective effects on ADHD symptom domains. Journal of Abnormal Psychology, 114(4), 706. [DOI] [PubMed] [Google Scholar]
- Nikolas MA, & Nigg JT (2015). Moderators of neuropsychological mechanism in attention-deficit hyperactivity disorder. Journal of abnormal child psychology, 43(2), 271–281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raffaelli M, Crockett LJ, & Shen YL (2005). Developmental stability and change in self-regulation from childhood to adolescence. The Journal of Genetic Psychology, 166(1), 54–76. [DOI] [PubMed] [Google Scholar]
- Ramtekkar UP, Reiersen AM, Todorov AA, & Todd RD (2010). Sex and age differences in attention-deficit/hyperactivity disorder symptoms and diagnoses: implications for DSM-V and ICD-11. Journal of the American Academy of Child & Adolescent Psychiatry, 49(3), 217–228. [PMC free article] [PubMed] [Google Scholar]
- Rhemtulla M, Brosseau-Liard PÉ, & Savalei V (2012). When can categorical variables be treated as continuous? A comparison of robust continuous and categorical SEM estimation methods under suboptimal conditions. Psychological methods, 17(3), 354. [DOI] [PubMed] [Google Scholar]
- Rodenacker K, Hautmann C, Görtz-Dorten A, & Döpfner M (2016). Bifactor models show a superior model fit: Examination of the factorial validity of parent-reported and self-reported symptoms of attention-deficit/hyperactivity disorders in children and adolescents. Psychopathology, 49(1), 31–39. [DOI] [PubMed] [Google Scholar]
- Rommelse NN, Altink ME, De Sonneville LM, Buschgens CJ, Buitelaar J, Oosterlaan J, & Sergeant JA (2007). Are motor inhibition and cognitive flexibility dead ends in ADHD?. Journal of Abnormal Child Psychology, 35(6), 957–967. [DOI] [PubMed] [Google Scholar]
- Rowland AS, Skipper BJ, Umbach DM, Rabiner DL, Campbell RA, Naftel AJ, & Sandler DP (2015). The prevalence of ADHD in a population-based sample. Journal of attention disorders, 19(9), 741–754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salthouse TA (1996). The processing-speed theory of adult age differences in cognition. Psychological review, 103(3), 403. [DOI] [PubMed] [Google Scholar]
- Salthouse TA (2011). What cognitive abilities are involved in trail-making performance?. Intelligence, 39(4), 222–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salthouse TA, & Babcock RL (1991). Decomposing adult age differences in working memory. Developmental psychology, 27(5), 763. [Google Scholar]
- Satorra A, & Bentler PM (2010). Ensuring positiveness of the scaled difference chi-square test statistic. Psychometrika, 75(2), 243–248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saydam RB, Ayvaşik HB, & Alyanak B (2015). Executive functioning in subtypes of attention deficit hyperactivity disorder. Nöro Psikiyatri Arşivi, 52(4), 386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seidman LJ (2006). Neuropsychological functioning in people with ADHD across the lifespan. Clinical psychology review, 26(4), 466–485. [DOI] [PubMed] [Google Scholar]
- Seidman LJ, Biederman J, Monuteaux MC, Valera E, Doyle AE, & Faraone SV (2005). Impact of gender and age on executive functioning: do girls and boys with and without attention deficit hyperactivity disorder differ neuropsychologically in preteen and teenage years?. Developmental neuropsychology, 27(1), 79–105. [DOI] [PubMed] [Google Scholar]
- Shanahan MA, Pennington BF, Yerys BE, Scott A, Boada R, Willcutt EG, … & DeFries JC (2006). Processing speed deficits in attention deficit/hyperactivity disorder and reading disability. Journal of abnormal child psychology, 34(5), 584. [DOI] [PubMed] [Google Scholar]
- Sonuga-Barke EJ (2003). The dual pathway model of AD/HD: an elaboration of neurodevelopmental characteristics. Neuroscience & Biobehavioral Reviews, 27(7), 593–604. [DOI] [PubMed] [Google Scholar]
- Sonuga-Barke EJ, Sergeant JA, Nigg J, & Willcutt E (2008). Executive dysfunction and delay aversion in attention deficit hyperactivity disorder: nosologic and diagnostic implications. Child and adolescent psychiatric clinics of North America, 17(2), 367–384. [DOI] [PubMed] [Google Scholar]
- Thorell LB (2007). Do delay aversion and executive function deficits make distinct contributions to the functional impact of ADHD symptoms? A study of early academic skill deficits. Journal of Child Psychology and Psychiatry, 48(11), 1061–1070. [DOI] [PubMed] [Google Scholar]
- Toplak ME, Pitch A, Flora DB, Iwenofu L, Ghelani K, Jain U, & Tannock R (2009). The unity and diversity of inattention and hyperactivity/impulsivity in ADHD: evidence for a general factor with separable dimensions. Journal of Abnormal Child Psychology, 37(8), 1137–1150. [DOI] [PubMed] [Google Scholar]
- Ullebø AK, Breivik K, Gillberg C, Lundervold AJ, & Posserud MB (2012). The factor structure of ADHD in a general population of primary school children. Journal of Child Psychology and Psychiatry, 53(9), 927–936. [DOI] [PubMed] [Google Scholar]
- Usami M (2016). Functional consequences of attention‐deficit hyperactivity disorder on children and their families. Psychiatry and clinical neurosciences, 70(8), 303–317. [DOI] [PubMed] [Google Scholar]
- Verbruggen F, Logan GD, & Stevens MA (2008). STOP-IT: Windows executable software for the stop-signal paradigm. Behavior research methods, 40(2), 479–483. [DOI] [PubMed] [Google Scholar]
- Wagner F, Martel MM, Cogo-Moreira H, Maia CRM, Pan PM, Rohde LA, & Salum GA (2016). Attention-deficit/hyperactivity disorder dimensionality: the reliable ‘g’and the elusive ‘s’ dimensions. European Child & Adolescent Psychiatry, 25(1), 83–90. [DOI] [PubMed] [Google Scholar]
- Wechsler D (2003). Wechsler intelligence scale for children-WISC-IV. Psychological Corporation. [Google Scholar]
- Willcutt EG (2012). The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics, 9(3), 490–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcutt EG, Doyle AE, Nigg JT, Faraone SV, & Pennington BF (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biological psychiatry, 57(11), 1336–1346. [DOI] [PubMed] [Google Scholar]
- Willcutt EG, Nigg JT, Pennington BF, Solanto MV, Rohde LA, Tannock R, … & Lahey BB (2012). Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. Journal of abnormal psychology, 121(4), 991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcutt EG, Pennington BF, Olson RK, Chhabildas N, & Hulslander J (2005). Neuropsychological analyses of comorbidity between reading disability and attention deficit hyperactivity disorder: In search of the common deficit. Developmental neuropsychology, 27(1), 35–78. [DOI] [PubMed] [Google Scholar]
- Willoughby MT (2020). Commentary on Application of the Bifactor S-1 Model to Multisource Ratings of ADHD/ODD Symptoms: An Appropriate Bifactor Model for Symptom Ratings. Journal of abnormal child psychology, 48(7), 901–904. [DOI] [PubMed] [Google Scholar]
- Wodka EL, Mostofsky SH, Prahme C, Gidley Larson JC, Loftis C, Denckla MB, & Mark Mahone E (2008). Process examination of executive function in ADHD: Sex and subtype effects. The Clinical Neuropsychologist, 22(5), 826–841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright I, Waterman M, Prescott H, & Murdoch‐Eaton D (2003). A new Stroop‐like measure of inhibitory function development: Typical developmental trends. Journal of Child Psychology and Psychiatry, 44(4), 561–575. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.