

Abstract
We employed longitudinal distributed lag modeling approach to systematically estimate how associations between built environment features and transport walking decayed with the increase of distance from home to built environment destinations. Data came from a cohort recruited from six U.S. cities (follow-up 2000–2010, N=3913, baseline mean age 60). Built environment features included all walkable destinations, consisting of common and popular destinations for daily life. We also included two subsets frequent social destinations and food stores to examine if the spatial scale effects differ by varying density for different types of built environment destinations. Adjusted results found that increases in transport walking diminished when built environment destinations were farther, although distance thresholds varied across different types of built environment destinations. Higher availability of walking destinations within 2-km and frequent social destinations within 1.6-km to be associated with transport walking. Food stores were not associated with transport walking. This new information will help policymakers and urban designers understand at what distances each type of built environment destinations influences transport walking, in turn informing the development of interventions and/or the placement of amenities within neighborhoods to promote transport walking. The findings that spatial scales depend on specific built environment features also highlight the need for methods that can more flexibly estimate associations between outcomes and different built environment features across varying contexts, in order to improve our understanding of the spatial mechanisms involved in said associations.
Keywords: Spatial Scale Effects, Distributed Lag Modeling, Transport Walking, Built Environments, Longitudinal
1. Introduction
Built environment features have drawn growing attention for their potential influence on health behaviors and health outcomes (Cummins et al., 2007; Diez Roux, 2001; Garin et al., 2014; Renalds et al., 2010; Roux, 2003). For example, empirical studies have found that built environment features such as mixed land use (Cao et al., 2007; Rodriguez et al., 2009), high accessibility to amenities (Cao, 2015; Cao et al., 2006; Frank et al., 2007; Heath et al., 2006; Kitamura et al., 1997; Li et al., 2020; Van Dyck et al., 2011), high residential density (Mooney et al., 2020; Braun et al., 2016; Khattak & Rodriguez, 2005), and greater road connectivity (Chatman, 2009) were associated with more transport walking. Some studies found the macro-scale neighborhood walkability was associated with more transport walking (Hirsch et al., 2013; McCormack et al., 2021; Steinmetz-Wood et al., 2020).
Despite growing evidence about built environment-health associations, the appropriate spatial scales for measuring built environment exposures in specific contexts remain largely unknown. Empirical studies show that associations between built environments and health behaviors vary depending on which spatial scales were used (Duncan et al., 2021; Kwan, 2012a; Li & Kim, 2020; Spielman & Yoo, 2009). Spatial scale in this study was measured through a set of continuous ring-shaped network buffers taken every 100-meter up to 5 km from a participant’s residence. Built environment exposures were measured by counting the number of walkable destinations within each ring-shaped network buffer. Until recently, studies employed pre-defined spatial scales such as buffers with arbitrary sizes (Jia et al., 2021; Rodriguez-Loureiro et al., 2021; Charreire et al., 2010; Forsyth et al., 2012) ranging from 100-meter to 4800-meter (Leal & Chaix, 2011) or various administrative units (Diez Roux, 2001, 2007; O’Campo, 2003) to delimit neighborhood boundaries within which built environment features were measured. However, pre-specified resiential buffers are susceptible to Modifiable Areal Unit Problem (MAUP) (Fotheringham & Wong, 1991)—the size and shape of a spatial unit within which built environment features are measured may influence the built environment-health associations. Further, while definitions of spatial scales using buffers or administrative boundaries are convenient to implement and easy to summarize, they may not appropriately represent individuals’ real geographic contexts (Kwan, 2012a; Kwan, 2012b). For example, research has shown that 1-mile circular and 1-mile network buffer, represents less than one-half of the neighborhood boundaries identified by residents of those neighborhoods (Smith et al., 2010). A recent study compared multiple buffers at 400 m, 800 m, 1000 m, 1600 m and 3000 m and found that traditional buffers captured, at best, two-thirds of individuals daily movement (Christensen et al., 2021). Besides, a residential buffer with a pre-specified radius for assessing built environment exposures is susceptiable to the residential effect fallacy (Chaix et al., 2017)—referring to the problem that the areas outside the pre-defined residential buffer along the course of daily activities may have built environment features that correlates with those in the residential buffer, thus overestimating the residential contextual effects. In addition, such pre-specified spatial scales do not capture individual-level differences in the relevant built environments, which are shaped by intra-personal differences in how physical and social environments are experienced (Chaix et al., 2009; de Almeida Célio et al., 2018; Lovasi et al., 2011; Macintyre et al., 2002). For instance, research has illustrated that individuals perceive relevant distances differently (Vallee et al., 2015), and experience different travel distances and activity spaces (Hirsch et al., 2014; Li & Kim, 2018; Mitchell et al., 2014). Third, typically used spatial scales may not be appropriate for different types of activities because empirical evidence shows that the walking distance varies depending on various activity purposes (Cerin et al., 2007; Gunn et al., 2017; Moudon et al., 2006; Yang & Diez-Roux, 2012). For instance, the walking distance for recreation was substantially longer than those for other activity purposes (Yang & Diez-Roux, 2012), and threhold distances varied for eating/drinking establishments (860 feet) and grocery stores (1445 feet) (Moudon et al., 2006). Some studies mitigated the potential bias by comparing the associations between walking/physical activities and built environment destinations using multiple concentric buffer rings (Gunn et al., 2017;Xie et al., 2021).
Crucially, pre-defined spatial scales may bias the relationships between built environments and health outcomes (Baek et al., 2016), and subsequently mislead the direction of policy interventions (Kwan, 2021) (Lovasi et al., 2011; Martin et al., 2014). Further, most built environment-health studies have primarily relied on cross-sectional designs, limiting the ability to draw causal inferences regarding the relationships between built environment features and health behaviors/outcomes due to both residential self-selection bias and temporal concerns of reverse causation. A few studies used longitudinal data, however, most used pre-specified spatial scales for built environment features (Hirsch et al., 2014; Knuiman et al., 2014; Schipperijn et al., 2015; Sun et al., 2014). Further, some were conducted outside of the U.S. with relatively small sample sizes (Knuiman et al., 2014; Schipperijn et al., 2015; Sun et al., 2014; Xie et al., 2021), and results may not be generalized to U.S. residents and their neighborhood contexts. Consequently, the field needs an easy to implement method of assessing appropriate spatial scales for different built environment features within different contexts so that it can inform future research to improve the assessment of health impacts of various built environment features and help policy makers make more effective interventions to promote health behaviors.
To bridge these gaps, we employed a longitudinal distributed lag modeling (DLM) approach (Baek et al., 2017; Baek et al., 2016) to examine spatial scale effects on associations between transport walking and built environment categories of all walking destinations, frequent social destinations, and food stores as a case study of built environment-health assocations using longitudinal data from the Multi-Ethnic Study of Atherosclerosis (MESA). Transport walking can contribute to physical activity (Cole et al., 2006) and subsequently improve health. Empirical evidence shows that higher levels of physical activities are associated with lower risk of obesity (Bassett et al., 2011) and other chronic diseases (Humphreys et al., 2013). This study primarily aimed to systematically estimate how the longitudinal associations between built environment features and transport walking vary with increasing distance between participants’ home and built environment destinations, and thus infer the spatial scale at which associations dissipate, which will inform policy interventions that where to place amenities to promote health related behaviors.
2. Methods
2.1. Sample and Data Sources
Data came from Multi-Ethnic Study of Atherosclerosis (MESA), a longitudinal study of 6814 adults aged 45–84 years without clinical cardiovascular disease at baseline (year 2000). Participants were recruited between July 2000 and August 2002 in six study sites (Los Angeles, CA; Chicago, IL; Saint Paul, MN; New York City, NY; Baltimore, MD; Forsyth County, NC). Data for this study came from baseline and three follow-up examinations of MESA: the second examination was between July 2002 and February 2004; examination 3 was between January 2004 and September 2005; and examination 5 was between April 2010 and May 2012. Examination 4 was not used because walking (our outcome variable) was not measured during that exam. MESA addresses were geocoded using TeleAtlas (Tele Atlas North America, Inc., Lebanon, New Hampshire).
Sample selection began with MESA cohort members recruited from the six sites who agreed to participate in the MESA Neighborhood Study (N=6191). We retained participants who were retained in the follow-up exams and that had accurate residential addresses geocoded at street level or Zip code +4 level at both Exam 1 and Exam 5 (yielding a sample of 4503 participants). We further excluded 186 participants missing transport walking at Exam 1, 2, 3, and Exam 5, and 204 participants with missing sociodemographic information at Exam 1, 2, 3 and Exam 5, and 200 participants who we did not calculate built environment exposures due to missing historic residential data. The final sample for analysis consisted of 3913 participants. The excluded participants were roughly similar to the participants in the final analytical sample, except that the participants in the analytical sample were slightly more advantaged (larger proportion with a college degree, employed, and higher income-wealth index) and had slightly higher proportion of White (data not shown).
Built environment data came from National Establishment Time Series (NETS) database (Hoehner & Schootman, 2010; Walls & Associates, 2013), obtained through the MESA Neighborhoods study and Retail Environments for Cardiovascular Disease (RECVD) project (https://sites.google.com/view/recvd-team-project-site/home). These data are available for the years 2000–2014 which overlaps with MESA Exams 1–5. Census block population data came from Census 2000 and Census 2010 SF1 data. Road network data were obtained from Census 2010 TIGER Roads data.
2.2. Variables
2.2.1. Health outcome—transport walking minutes per week
The health outcome variable was transport walking minutes per week. A MESA survey asked participants whether they had walked to get to places (bus, car, work, store) in a typical week in the past month. If yes, they were asked to report how many days per week and how much time per day they walked to get to places. We calculated transport walking minutes per week by multiplying number of days for transport walking per week by number of minutes for transport walking per day.
2.2.2. Built environment exposures
Built environment features included a broad category of all walkable destinations, consisting of common and popular destinations for daily life (e.g., food stores, restaurants, drug stores and pharmacies, department stores, post offices, banks/credit unions, libraries, beauty shops and barbers, social/entertainment destinations, museums, schools). We further included two subsets of the broad category of all walkable destinations (frequent social destinations and food stores) to examine if the spatial scale effects differ by varying density for different types of built environment destinations. Frequent social destinations consisted of destinations that facilitate social interaction and promote social engagement (e.g., beauty shop/barber, libraries, non-physical activity recreation clubs, religion). Food stores consisted of a variety of food outlet destinations (e.g. supermarkets, convenience stores, small grocers/bodegas, fish market, fruit and vegetable markets, bakery, candy, ice cream, and coffee shops). The detailed list of all the destinations is shown in Supplement Table 1 (ST1). Built environment exposures were calculated using ArcGIS [GIS software] (Version 10.5. Redlands, CA: Environmental Systems Research Institute, Inc., 2016).
2.2.3. Covariates
Covariates were selected based on a prior MESA study which examined longitudinal associations between walking and built environment features (Hirsch et al., 2014). Time-invariant person-level covariates included age at baseline, sex, race/ethnicity, and education. Time-varying covariates included income-wealth index, employment status, household car ownership, body mass index (BMI), self-rated health compared with others of the same age, and arthritis flare-up in the past 2 weeks. The income-wealth index was specified as a 9-point scale (0 being the lowest level of income and no assets and 8 being the highest level of income and all 4 assets). Details about the index are shown in the note of Table 1 and the index was described previously in depth (Hajat et al., 2010). Area-level covariates included population density in a 1-mile residential buffer, street network ratio in a 1-mile residential buffer, and region (from census categories: Northeast, Midwest, South, West). To calculate population density in a 1-mile Euclidean buffer around residence, first we used the ‘intersect’ geoprocessing tool in ArcGIS [GIS software] (Version 10.5. Redlands, CA: Environmental Systems Research Institute, Inc., 2016) to calculate the total population for block groups/pieces of block groups within a 1-mile Euclidean buffer of each participant and then we divided the total population by the area of the buffer. Street network ratio in a 1-mile residential buffer was calculated as the ratio of the area of a 1-mile network buffer to the area of a 1-mile Euclidean buffer around each participant’s residence. The ratio varies between 0 and 1, with 0 meaning none of the area can be reached through the road network and 1 meaning the entire area can be reached through the street network (i.e., the highest level of network ratio).
Table 1.
Longitudinal sociodemographic and neighborhood characteristics among participants in the Multi-Ethnic Study of Atherosclerosis (MESA), 2000–2010
| Exam 1 | Exam 2 | Exam 3 | Exam 5 | |
|---|---|---|---|---|
| Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | |
| Total transport walking minutes/week (minute) | 180 (60–420) | 120 (35–315) | 120 (35–325) | 150 (30–420) |
| Time-varying covariates | Mean (STD) | Mean (STD) | Mean (STD) | Mean (STD) |
| Age | 60 (9.5) | 62 (9.5) | 63 (9.5) | 70 (9.5) |
| Income-wealth indexa (ranges from 0 to 8) | 5.02 (2.24) | 5.00 (2.25) | 5.01 (2.23) | 5.01 (2.19) |
| Body mass index (kg/m2) | 28.30 (5.40) | 28.40 (5.52) | 28.38 (5.56) | 28.47 (5.67) |
| Population density per square mile | 15508.14 (19487.05) | 15296.48 (19505.22) | 15015.29 (19342.31) | 14581.92 (19254.95) |
| Street network ratio | 0.42 (0.15) | 0.41 (0.15) | 0.41 (0.15) | 0.41 (0.16) |
| % | % | % | % | |
| Currently employed | 61.41 | 58.57 | 56.4 | 44.21 |
| Own at least one car | 84.82 | 84.82 | 84.59 | 85.87 |
| Arthritis flare-up in past 2 weeks | 10.94 | 10.32 | 11.99 | 19.37 |
| Self-rated health compared with others | % | % | % | % |
| Better | 60.59 | 60.59 | 60.26 | 58.63 |
| Same | 34.86 | 34.86 | 35.5 | 36.08 |
| Worse | 4.55 | 4.55 | 4.24 | 5.29 |
| Regionb | % | % | % | % |
| Northeast | 16.87 | 16.87 | 16.76 | 16.66 |
| Midwest | 36.93 | 36.44 | 36.21 | 35.91 |
| South | 30 | 30.36 | 30.46 | 30.87 |
| West | 16.2 | 16.33 | 16.56 | 16.56 |
| Time-invariant covariates | % | |||
| Female sex | 52.95 | |||
| Race/ethnicity | ||||
| White | 42.42 | |||
| Black/African American | 25.45 | |||
| Chinese | 11.96 | |||
| Hispanic | 20.16 | |||
| Education level | ||||
| High school/GED or less | 30.49 | |||
| Some college | 29.16 | |||
| BA or above | 40.35 | |||
Note:
An income-wealth index was created by adding together two 5-categorey variables, inflation adjusted per capita income (ranges from 0 to 4) and wealth index (ranges from 0 to 4). Inflation adjusted per capita income was created by the following formula ([annual household income * inflation factor at the year of exam] / number of people in the household)/ $10000. Next, in order to combine it with wealth, income per capita was subsequently categorized into quintiles. Wealth index was calculated as the sum of home ownership (0 or 1), car ownership (0 or 1), land ownership (0 or 1), and investments (0 or 1). After summing the 5 categories of income and 5-categories of wealth, this yielded a 9-point scale (0 being the lowest level of income and no assets and 8 being the highest level of income and all 4 assets). The MESA income-wealth index has been previously described in depth (Hajat et al., 2010).
Region categories came from Census catogories.
2.3. Distributed lag models
Distributed lag models (DLMs) have been widely used in economics (Almon, 1965) and air pollution studies (Dominici et al., 2004; Pope III et al., 1991; Welty et al., 2009). Most recently, DLMs have been used to estimate associations between spatially-lagged food environment exposures and body mass index(Baek et al., 2017; Baek et al., 2016). DLM is advantageous in exploring how effects of built environment on health outcomes vary across distance without pre-specifying a geographic scale; and identifying spatial scales at which the effects peak and the distance at which the effects vanish.
2.3.1. DLMs for the MESA longitudinal data
In all models, the outcome Yij is transport walking minutes per week for participant i at Exam j, which is log-transformed as it is skewed to the right. In order to estimate how the association between walking destinations and transport walking vary with network distance between participants and destinations, the DLM uses a set of “distributed lag covariates”, instead of a single count of destinations within a network buffer of pre-determined radius. The distributed lag covariates are the count of built environment destinations for participant i at Exam j measured within a ring-shaped network buffer area with inner and outer radii of rl−1 and rl , respectively, and are denoted as Xij(rl−1; rl) for l = 1,2, … ,50. The diagram of the ring-shaped network buffers within which the built environment destinations were assessed was displayed in Supplement Figure 1. We set the width of the ring as rl-rl−1= 100-meter, which is a typical width for city blocks in U.S. cities and thus a reasonable increment for walking distance. In a hypothetical city with 100 × 100 meter blocks, the distributed lag covariates would thus represent the number of destinations available within consecutive groups of blocks incrementally further away from each participant’s residence. We set the largest ring-shaped network buffer area to have outer radius of 5-km (3.11 miles), since most people walk less than 3 miles per day (Yang & Diez-Roux, 2012). Hence, the inner and outer radii of the first ring-shaped network area were 0 and 0.1-km; the inner and outer radii of the 50th ring-shaped network area were 4.9-km and 5-km. Distributed lagged covariates were constructed in this way for all walking destinations, frequent social destinations and food stores. The longitudinal distributed lag models estimated were then:
| (1) |
where: β0i is a random intercept for person i; Zij denotes a set of time varying and time invariant covariates. The model also included a random time slope (year 2000 to year 2010), β2i, that enables the longitudinal change in transport walking to vary between individuals.
The DLM estimates associations β(rl−1;rl) between transport walking and destinations at every100-meter, which represent the average difference in transport walking minutes associated with one additional walkable destination within the ring-shaped network area within rl−1 and rl distance from the subject. Because of the large number of associations estimated, the model could be prone to overfitting and collinearity problems. Additionally, it is desirable to have coefficients from adjacent rings be similar to each other, since, for example, one would not expect the association between walking and availability of walking destinations in one block to be drastically different from the association in the next block. Thus, to resolve potential overfitting and collinearity problems and encourage similarity of coefficients among adjacent rings, the distributed lag coefficients β(rl−1;rl) are constrained to follow a smooth, continuous pattern across distance using smoothing splines (Baek et al., 2017; Baek et al., 2016; Zanobetti et al., 2000). Three separate DLMs were estimated for each of the built environment exposures (all walkable destinations, frequent social destinations, and food stores). Estimation of distributed lag model parameters were carried out using a restricted maximum likelihood estimation in the software R.
2.3.2. Sensitivity analyses for DLMs
We conducted cross-sectional DLMs for transport walking and all walkable destinations and the two subdomains at Exam 5. The purpose of this was to use a simplified model to check the performance of the model (absent time). Using this simplified model, we stratified the cross-sectional DLM for transport walking and all walkable destinations at Exam 5 by population density (below median versus median or above) and by region, separately. The purpose of the stratification was to assess whether results were similar across different contexts.
2.3.3. Results presentation and interpretation
First, we used figures to display the estimated distributed lag coefficients quantifying associations between transport walking and built environment exposures up to 5-km from home locations. These figures visualize whether and how the associations between transport walking and built environment destinations diminish with increasing distance between residential locations and these destinations, and help identify the distances or spatial scales within which the health effects of built environment exist. The DLM coefficients β(rl−1;rl) in the figures are shown in the log scale since the outcome variable is log-transformed. Second, we presented aggregated values of these coefficients, representing associations within ring-shaped network area associations that have wider width (e.g., 0.5 km). These aggregated values may be more policy-relevant compared to the associations at 100-meter resolution shown in the figures. For a given ring-shaped network area with inner and outer radii of rm and rk, these aggregated associations were derived by summing the coefficients within the range, i.e., . We presented seven of these with respective ranges of 0 – 0.5km, 0.5 – 1km, 1 – 1.5km, 1.5 – 2km, 2 – 3km, 3 – 4km, 4 – 5km. Additionally, to facilitate comparison to prior studies, we calculated the average buffer area association for seven network buffer areas with a radius of rk of 0.5km, 1km, 1.5km, 2km, 3km, 4km, and 5km. We back-transformed the average ring-shaped network area association and the average buffer area association by (Exp()) and (Exp()) to aid interpretation, respectively. Note that we pre-multiplied these aggregated associations by 10 for better interpretation. Namely, the transformed associations represent the average percent increase in transport walking minutes per week associated with 10 additional walkable destinations in the two aforementioned aggregated spatial scales, respectively.
3. Results
3.1. Descriptive results
Table 1 displays characteristics of the analytical sample of MESA participants at Exam 1, 2, 3, and 5. The sample was 53% female, 42% of white, and had average of 14 years of education (standard deviation [SD] = 3.7). Mean participant age was 60 years (SD = 9.5) at Exam 1. At Exam 1, 61% were employed and that dropped to 44% at Exam 5. About 85% of participants owned at least one car. Participant BMI was approximately 28.3 kg/m2. The percent of participants with arthritis flare-up in past 2-weeks increased from 11% at Exam 1 to 19% at Exam 5. Average length of living in the current neighborhood was 19 years at Exam 1 and about 71% of participants remained at the same residence over follow-up. Median minutes of self-reported weekly transport walking at Exam 1 was 180 (Q1–Q3: 60 – 420) and was 150 (Q1–Q3: 30 – 420) at Exam 5 (see Table 1). The difference in transport walking minutes per week between Exam 5 and Exam 1 was as follows: median change was 0 (Q1: −175, Q3: 180, 10th percentile: −420, 90th percentile: 450), mean change was −5.57 (SD: 540.07).The population density of participants’ 1-mile neighborhood decreased over time, with mean of 15508.14 (SD: 19487.05) at Exam 1 and 14581.92 (SD: 19254.95) at Exam 5. Mean street network ratio did not change much over time (Exam 1 to Exam 5: 0.42 to 0.41).
Descriptive statistics for built environment exposures at Exam 1, 2, 3, and 5 in a series of ring-shaped network areas is displayed in Supplement Table 2 (ST2). The median count of all walkable destinations and subdomains (frequent social destinations and food stores) increased with increasing distance from participants’ home. For example, at Exam 1, in the ring-shaped network area closest to participants’ home locations (inner and outer radii of 0km and 0.5km) the median count of all walkable destinations at Exam 1 was 9 (Q1–Q3: 2–30) and increased to 369 (Q1–Q3: 196–779) in the ring-shaped network area farthest from participants’ home locations (inner and outer radii of 4-km and 5-km, ST2). The counts of frequent social destinations and food stores in different geographic scales showed similar patterns, increasing from smaller scales to larger scales. In addition, the counts of all walkable destinations and subdomains increased slightly from Exam 1 to Exam 5. For example, in the ring-shaped network area closest to participants’ home (0 – 0.5 km) the median count of walkable destinations increased from 9 to 11 from Exam 1 to Exam 5.
3.2. Spatial scale effects in the longitudinal associations between transport walking and built environment destinations
Figure 1 shows estimated distributed lag coefficients (log) for longitudinal associations between transport walking and built environment categories within 5-km from residential locations, adjusted for sociodemographic characteristics. The thresholds at which a higher number of walkable destinations was associated with more transport walking varied by destination types. For all walkable destinations and for frequent social destinations, transport walking declined with distance to destinations and the thresholds for the effects were approximately 2-km and 1.6-km, respectively. Further, the decline in walking minutes with distance from destinations was steeper for frequent social destinations compared to all walkable destinations. For food stores, there was little evidence of an association (confidence intervals include 0) or a decline in the association with distance.
Figure 1.
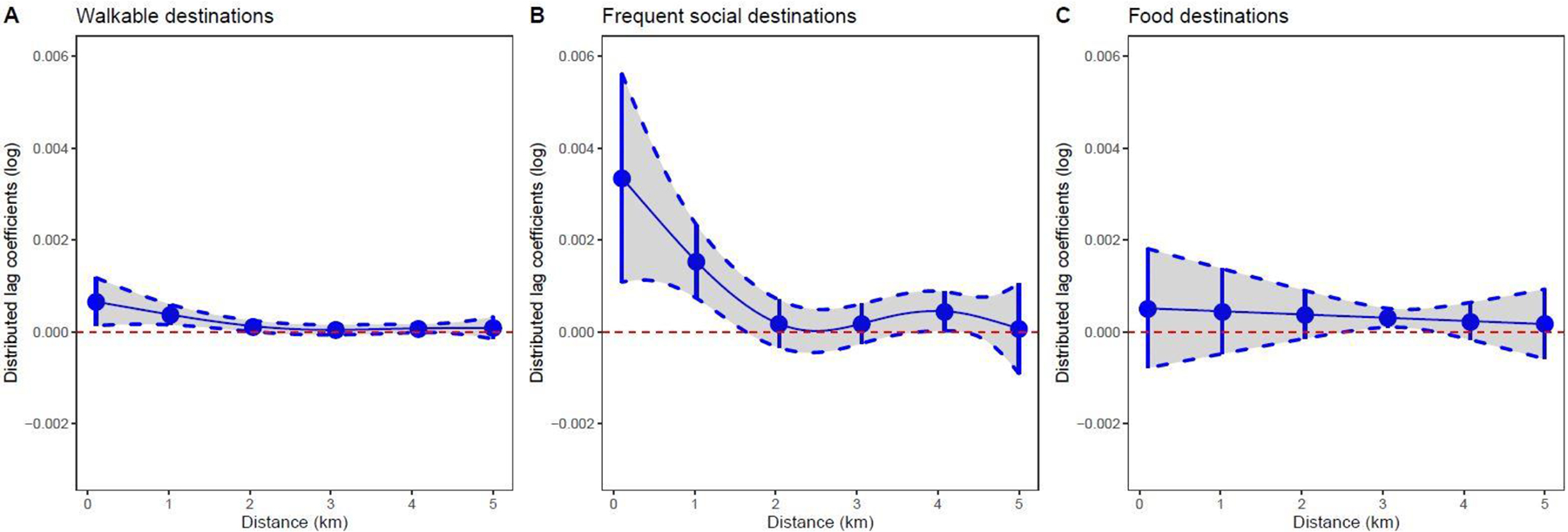
Distributed lag modeling results for longitudinal data on transport walking (log scale) and built environment destinations in the ring-shaped network areas up to 5-km from residence. Panel A: all walkable destinations; Panel B: frequent social destinations; Panel C: food stores. Dashed lines represent 95% confidence intervals. Each model adjusted age, gender, race, education, per capita income and wealth index, BMI, self; rated health, arthritis last 2 weeks, car ownership, marital status, employment status, population density in 1-mile residential buffer, street network ratio in 1-mile residential buffer.
Table 2 shows estimated average ring-shaped network area associations between transport walking and built environment categories in the seven aggregated ring-shaped network areas with various inner and outer radii derived from the DLM coefficients in the 50 ring-shaped network areas. The average transport walking minutes per week increased by 3.0% (this was equivalent to 4.5 minutes at Exam 5) per 10 additional walkable destinations in the ring-shaped network area with inner and outer radii of 0 and 0.5 km. The average transport walking minutes per week increased by 2.2%, 1.5%, and 0.8% per 10 additional walkable destinations in the ring-shaped network areas with ranges of 0.5 – 1 km, 1 – 1.5 km, and 1.5 – 2 km, respectively. For frequent social destinations, the average transport walking minutes per week increased by 15.8% (this is equivalent to 24 minutes at Exam 5), 10.1%, 5.3% per 10 additional frequent social destinations in the ring-shaped network areas with ranges of 0 – 0.5 km, 0.5 – 1 km, and 1 – 1.5 km, respectively. In addition, Table 2 also displays the average buffer area associations between transport walking and built environment categories in the seven network buffer areas with various radii derived from the DLM coefficients in the 50 ring-shaped network areas. In general, the estimated average buffer area associations existed between transport walking minutes per week and walkable destinations and frequent social destinations in the buffer areas up to 0.5 km, 1 km, 1.5 km, 2 km, 3 km, 4 km, and 5 km, respectively. For example, the average transport walking minutes per week increased by 5.3% per 10 additional walkable destinations in the 1-km buffer and by 27.5% per 10 additional frequent social destinations in the 1-km buffer. Food stores were not associated with transport walking within the buffer areas with various ranges.
Table 2.
Estimated associations between transport walking and built environment exposures within specific ring-shaped areas and buffer areas, based on longitudinal data from MESA, 2000–2010.
| N = 3913 | Outcome: transport walking minutes per week | |||||||
|---|---|---|---|---|---|---|---|---|
| Ring-shaped areas (Rm - Rk) | Buffer areas (0 - Rk) | |||||||
| Exposure | buffer ranges (km): Rm - Rk | 95% C.I. | buffer ranges (km): 0 - Rk | 95% C.I. | ||||
| 1. Walkable destinations | 0 – 0.5 | 0.030 | 0.008 | 0.053 | 0 – 0.5 | 0.030 | 0.008 | 0.053 |
| 0.5 – 1 | 0.022 | 0.008 | 0.036 | 0 – 1 | 0.053 | 0.016 | 0.091 | |
| 1 – 1.5 | 0.015 | 0.006 | 0.023 | 0 – 1.5 | 0.068 | 0.022 | 0.117 | |
| 1.5 – 2 | 0.008 | 0.002 | 0.015 | 0 – 2 | 0.077 | 0.024 | 0.133 | |
| 2 – 3 | 0.007 | −0.005 | 0.018 | 0 – 3 | 0.084 | 0.019 | 0.154 | |
| 3 – 4 | 0.006 | −0.004 | 0.016 | 0 – 4 | 0.091 | 0.015 | 0.172 | |
| 4 – 5 | 0.008 | −0.006 | 0.021 | 0 – 5 | 0.099 | 0.010 | 0.197 | |
| 1.1. Frequent social destinations | 0 – 0.5 | 0.158 | 0.057 | 0.269 | 0 – 0.5 | 0.158 | 0.057 | 0.269 |
| 0.5 – 1 | 0.101 | 0.047 | 0.157 | 0 – 1 | 0.275 | 0.107 | 0.469 | |
| 1 – 1.5 | 0.053 | 0.018 | 0.088 | 0 – 1.5 | 0.342 | 0.127 | 0.598 | |
| 1.5 – 2 | 0.018 | −0.009 | 0.047 | 0 – 2 | 0.367 | 0.117 | 0.672 | |
| 2 – 3 | 0.008 | −0.038 | 0.055 | 0 – 3 | 0.377 | 0.075 | 0.765 | |
| 3 – 4 | 0.039 | −0.005 | 0.084 | 0 – 4 | 0.430 | 0.069 | 0.914 | |
| 4 – 5 | 0.025 | −0.026 | 0.079 | 0 – 5 | 0.466 | 0.041 | 1.065 | |
| 1.2. Food stores | 0 – 0.5 | 0.025 | −0.035 | 0.089 | 0 – 0.5 | 0.025 | −0.035 | 0.089 |
| 0.5 – 1 | 0.023 | −0.027 | 0.076 | 0 – 1 | 0.049 | −0.061 | 0.173 | |
| 1 – 1.5 | 0.022 | −0.019 | 0.063 | 0 – 1.5 | 0.072 | −0.078 | 0.247 | |
| 1.5 – 2 | 0.020 | −0.010 | 0.051 | 0 – 2 | 0.093 | −0.088 | 0.310 | |
| 2 – 3 | 0.034 | 0.001 | 0.069 | 0 – 3 | 0.131 | −0.087 | 0.401 | |
| 3 – 4 | 0.027 | −0.001 | 0.056 | 0 – 4 | 0.161 | −0.088 | 0.479 | |
| 4 – 5 | 0.018 | −0.035 | 0.074 | 0 – 5 | 0.182 | −0.120 | 0.589 | |
Note: the coefficient 0.022 means a 2.2% change (over the 10 years of follow-up) in walking minutes per week for an additional 10 destinations within a 0.5 to 1 kilometer distance from the residence. Each model adjusts covariates: age, gender, race, education, per capita income, BMI, self; rated health, arthritis last 2 weeks, car ownership, marital status, employment status, population density in 1-mile residential buffer, street connectivity at 1-mile residential buffer. Bold fonts indicate p < 0.05.
3.3. Sensitivity analysis results
Supplement Figure 2 shows cross-sectional associations between transport walking and the three built environment categories. In cross-sectional analyses (exam 5 only), the plots of the distributed lag coefficients showed a similar pattern to the longitudinal results. Further, the DLM coefficients estimated from stratified cross-sectional analysis by population density (below median vs. median or above) also showed a similar pattern (magnitude of association decreased with increasing distance), although the associations for less dense areas (population density < median) were not significant at the 0.05 level. Stratified cross-sectional results by region also showed a similar pattern.
4. Discussion
This study employed a longitudinal distributed lag modeling approach to explore the associations between transport walking and various built environment destinations in a set of continuous ring-shaped network buffers up to 5-km from a participant’s home to the built environment destinations. This method enables us to measure and illustrate how the associations decay with the increasing distance from home to built environment destinations and allows us to infer the spatial scales at which these built environment exposures impact transport walking. Further, the longitudinal data used in the DLM help produce more robust results on the associations between transport walking and built environment destinations. We found that the magnitude of the association between transport walking and walkable destinations decreases with increases in distance from home to walkable destinations; this result also held for the subdomain of frequent social destinations. These associations were positive, as expected, when destinations were close to residential locations, and were negligible and not significant by approximately 2 km (all walkable destinations) and 1.6 km for frequent social destinations. There was little evidence for an association between food stores and transport walking at any distance.
The specificity in our DLM approach is a step forward to addressing the Modifiable Areal Unit Problem (MAUP) (Fotheringham & Wong, 1991) because it jointly estimates the associations between transport walking and built environments in various spatial units with small distance intervals to circumvent a pre-defined residential buffer with a fixed radius. Our DLM method also helps visualize how associations diminish with distance and identify at what scale the associations vanish. Furthermore, unlike traditional pre-defined residential buffers, our DLM method mitigates the residential effect fallacy (Chaix et al 2017) since it accounts for spatial autocorrelation of built environment features in closer and faraway distance up to 5-km from residence by estimating associations between transport walking and built environment features in a series of continuous ring-shaped network areas. Additionally, our DLM method broadens the spatial scale from the immediate residential neighborhood to a larger area to better approximate the true geographic contexts, which partially mitigates the Uncertain Geographic Context Problem. Further, our findings illustrate the thresholds at what scale the spatial associations become negligible vary across different types of built environment features, enriching the nuanced understanding on the associations between transport walking and various built environment features.
The associations we found are stronger in closer distance and weaker in farther distance, which support the long standing (though not often tested) hypothesis that health-related behaviors are more related with built environment features at closer distance (Baek et al., 2016; Spielman et al., 2009). The model results provide information about the distance at which walkable destinations may no longer influence transport walking. The spatial scales inferred from the model were somewhat different for different built environment features (smaller scales for frequent social destinations compared to all walkable destinations), which highlights that spatial scales are dependent on which feature of the built environment is being measured. The spatial scales for all walkable destinations and for frequent social destinations were approximately at 2 km and 1.6 km, respectively. Stronger associations for all walkable destinations and frequent social destinations might be because these amenities are more prevalent in the environment and thus encouraging all sorts of errands, and trip-chaining (going from one place to another). These findings are aligned with results in previous literature that indicated that the threshold walking distance varies depending on different types of destinations (Cerin et al., 2007; Gunn et al., 2017; Moudon et al., 2006; Yang & Diez-Roux, 2012). Meanwhile, we did not find evidence that food stores are associated with transport walking. One potential explanation might be because food stores are rarer and people may need to travel farther to get to food stores. Indeed, empirical evidence from a U.S. city Atlanta shows that the mean travel distance for food ranges from 4.5 miles (7.24 km) for coffee shops to 6.3 miles (10 km) for superstores and only 7% of all trips to a food outlet were by walking (Kerr et al., 2012). Nevertheless, more studies are needed to investigate the food environment and its assocations with transport walking.
We found that transport walking was associated with walkable destinations within 2-km from home and was associated with frequent social destinations within 1.6-km from home. These findings are generally consistent with previous findings in another MESA study which finds that transport walking is associated with popular walkable destinations and social destinations measured in a 1-mile (1.6 km) buffer (Hirsch et al., 2014), and results in another community survey study which finds transport walking is associated with neighborhood walkability assessed in a 1-mile (1.6 km) buffer (Li et al., 2020). The alignment of our findings with prior results verifies the prior results. Nevertheless, we note that our analyses are more robust than the traditional pre-defined buffer-based methods used in the previous study. Our method is able to systematically estimate associations between transport walking and built environment features decayed with the increase of distance from home locations. Further, our results highlight that the spatial scales within which built environments have health impacts vary across different types of built environment destinations.
Our DLM results about the spatial scales across distances have important implications. First, the DLM results enable us to identify the most relevant distance for detecting associations between transport walking and built environment features. This can be used to guide policymakers regarding where to place amenities or how to design spaces to encourage transport walking, which could ultimately increase physical activity levels and reduce motorized trips. Further, the DLM results suggest that the spatial scales within which the associations between transport walking and built environment features exist vary among different types of built environment features, shedding new light on identifying relevant spatial scales for different built environment features. It also highlights the need for methods that can more flexibly estimate associations between outcomes and different built environment features across varying contexts, in order to improve our understanding of the spatial mechanisms involved in said associations. This finding will inform future research to choose appropriate spatial scales to assess different built environment features and develop more robust associations with health outcomes. It will also help policymakers understand where to place different types of amenities to promote transport walking.
4.1. Strengths and limitations
This study has some strengths. First, this is the first study to use a longitudinal DLM approach to provide systematic evidence on how the associations between transport walking and walkable destinations vary across distances between participant’s residential locations and walkable destinations. The method helps identify appropriate spatial scales for walkable destinations and frequent social destinations. The DLM approach provides a way to circumvent pre-specifying a spatial scale to measure built environment destinations by estimating associations between transport walking and built environments in a set of consecutive ring-shaped network areas. Further, the DLM results are more flexible than pre-defined buffer methods as they can be easily aggregated to various buffer areas with varying radii, thus enabling comparison with prior studies. Second, the method can be flexibly applied to various built environment features and contexts. Third, this study used systematically coded business data (Hirsch et al., 2021) consistent with several other cohorts (enhancing reproducibility). Fourth, the longitudinal data came from a diverse sample of race, gender, and region which provided more robust associations between transport walking and walkable destinations.
This study also has some limitations. First, although the MESA study was longitudinal, we were unable to estimate whether within-person changes in built environment exposures were associated with within-person changes in transport walking. Although estimating such associations using the DLM approach is possible, there is relatively little change in transport walking and in walkable destinations during the study period. Second, this study focused on examining the spatial scale effects for built environment destinations in areas up to 5-km from residence, which may not cover potential activity spaces for daily movement. Future studies can extend the DLM method to broader activity spaces that account for built environment exposures over the course of daily activities using GPS tracking data. Third, we focused on a specific subset of environment features, namely all walkable destinations and the two subdomains (frequent social destinations, and food stores). Further research can extend to examine other built environment features and their impacts on both transport walking and other health outcomes. Fourth, the participants in our study sample were mostly middle-age and older adults residing in urbanized areas. Our results might not be generalizable to all adults or children or people in suburban or rural areas who may have different travel patterns and time demands. Addtionally, our transport walking minutes were self-reported data, which may not be as accurate as those measured using pedometers or accelerometers.
5. Conclusions
The longitudinal DLM approach enabled us to infer the spatial scales at which associations between availability of walking destinations and transport walking occur, thus allowing us to understand how far built environment destinations are associated with transport walking. We found higher availability of walking destinations within 2-km and frequent social destinations within 1.6-km to be associated with walking for transport. This new information will help policymakers and urban designers understand at what distances each type of built environment destinations influences transport walking, in turn informing the development of interventions and/or the placement of amenities within neighborhoods to promote transport walking. The findings that spatial scales depend on specific built environment features also highlight the need for methods that can more flexibly estimate associations between outcomes and different built environment features across varying contexts, in order to improve our understanding of the spatial mechanisms involved in said associations.
Supplementary Material
Highlights.
We used longitudinal distributed lag models to estimate associations between walkable destinations and transport walking decayed with the increase of distance from home.
Higher availability of walking destinations within 2-km and frequent social destinations within 1.6-km to be associated with walking for transport.
The spatial scales within which built environments have health impacts vary across different types of built environment destinations.
Our findings inform policymakers where to place amenities within neighborhood to promote health behaviors.
References:
- Almon S (1965). The distributed lag between capital appropriations and expenditures. Econometrica: Journal of the Econometric Society, 33(1), 178–196. doi: 10.2307/1911894 [DOI] [Google Scholar]
- Baek J, Hirsch JA, Moore K, Tabb LP, Barrientos-Gutierrez T, Lisabeth LD, Diez-Roux AV & Sánchez BN (2017). Statistical Methods to Study Variation in Associations Between Food Store Availability and Body Mass in the Multi-Ethnic Study of Atherosclerosis. Epidemiology (Cambridge, Mass.), 28(3), 403–411. doi: 10.1097/EDE.0000000000000631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baek J, Sanchez BN, Berrocal VJ, & Sanchez-Vaznaugh EV (2016). Distributed Lag Models Examining Associations Between the Built Environment and Health. Epidemiology, 27(1), 116–124. doi: 10.1097/ede.0000000000000396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bassett DR Jr, Wyatt HR, Thompson H, Peters JC & Hill JO (2010). Pedometer-measured physical activity and health behaviors in United States adults. Medicine and science in sports and exercise, 42(10), 1819–1825. doi: 10.1249/MSS.0b013e3181dc2e54 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braun LM, Rodriguez DA, Song Y, Meyer KA, Lewis CE, Reis JP, & Gordon-Larsen P (2016). Changes in walking, body mass index, and cardiometabolic risk factors following residential relocation: Longitudinal results from the CARDIA study. Journal of Transport & Health, 3(4), 426–439. doi: 10.1016/j.jth.2016.08.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cao XY (2015). Examining the impacts of neighborhood design and residential self-selection on active travel: a methodological assessment. Urban Geography, 36(2), 236–255. doi: 10.1080/02723638.2014.956420 [DOI] [Google Scholar]
- Cao XY, Handy SL, & Mokhtarian PL (2006). The influences of the built environment and residential self-selection on pedestrian behavior: Evidence from Austin, TX. Transportation, 33(1), 1–20. doi: 10.1007/s11116-005-7027-2 [DOI] [Google Scholar]
- Cao XY, Mokhtarian PL, & Handy SL (2007). Cross-sectional and quasi-panel explorations of the connection between the built environment and auto ownership. Environment and Planning A, 39(4), 830–847. doi: 10.1068/a37437 [DOI] [Google Scholar]
- Cerin E, Leslie E, du Toit L, Owen N, & Frank LD (2007). Destinations that matter: associations with walking for transport. Health & Place, 13(3), 713–724. doi: 10.1016/j.healthplace.2006.11.002 [DOI] [PubMed] [Google Scholar]
- Chaix B, Duncan D, Vallée J, Vernez-Moudon A, Benmarhnia T & Kestens Y (2017). The “residential” effect fallacy in neighborhood and health studies. Epidemiology, 28(6), 789–797. doi: 10.1097/EDE.0000000000000726 [DOI] [PubMed] [Google Scholar]
- Chaix B, Merlo J, Evans D, Leal C, & Havard S (2009). Neighbourhoods in eco-epidemiologic research: Delimiting personal exposure areas. A response to Riva, Gauvin, Apparicio and Brodeur. Social Science & Medicine, 69(9), 1306–1310. doi: 10.1016/j.socscimed.2009.07.018 [DOI] [PubMed] [Google Scholar]
- Charreire H, Casey R, Salze P, Simon C, Chaix B, Banos A, Badariotti D, Weber C and Oppert JM (2010). Measuring the food environment using geographical information systems: a methodological review. Public Health Nutrition, 13(11), 1773–1785. doi: 10.1017/s1368980010000753 [DOI] [PubMed] [Google Scholar]
- Chatman DG (2009). Residential choice, the built environment, and nonwork travel: evidence using new data and methods. Environment and Planning A, 41(5), 1072–1089. doi: 10.1068/a4114 [DOI] [Google Scholar]
- Christensen A, Griffiths C, Hobbs M, Gorse C, & Radley D (2021). Accuracy of buffers and self-drawn neighbourhoods in representing adolescent GPS measured activity spaces: An exploratory study. Health & Place, 69, 102569. doi: 10.1016/j.healthplace.2021.102569 [DOI] [PubMed] [Google Scholar]
- Cole R, Leslie E, Bauman A, Donald M, & Owen N (2006). Socio-demographic variations in walking for transport and for recreation or exercise among adult Australians. Journal of physical activity and health, 3(2), 164–178. doi: 10.1123/jpah.3.2.164 [DOI] [PubMed] [Google Scholar]
- Cummins S, Curtis S, Diez-Roux AV, & Macintyre S (2007). Understanding and representing ‘place’in health research: a relational approach. Social Science & Medicine, 65(9), 1825–1838. doi: 10.1016/j.socscimed.2007.05.036 [DOI] [PubMed] [Google Scholar]
- de Almeida Célio F, de Lima Friche AA, Jennings MZ, de Souza Andrade AC, Xavier CC, Proietti F, Coulton CJ and Caiaffa WT (2018). Contextual characteristics associated with the perceived neighbourhood scale in a cross-sectional study in a large urban centre in Brazil. Bmj Open, 8(8), e021445. doi: 10.1136/bmjopen-2017-021445 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diez Roux AV (2001). Investigating neighborhood and area effects on health. American Journal of Public Health, 91(11), 1783–1789. doi: 10.2105/ajph.91.11.1783 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diez Roux AV (2007). Neighborhoods and health: where are we and were do we go from here? Revue d’epidemiologie et de sante publique, 55(1), 13–21. doi: 10.1016/j.respe.2006.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dominici F, McDermott A, & Hastie TJ (2004). Improved semiparametric time series models of air pollution and mortality. Journal of the American Statistical Association, 99(468), 938–948. doi: 10.1198/016214504000000656 [DOI] [Google Scholar]
- Duncan GE, Hurvitz PM, Moudon AV, Avery AR, & Tsang S (2021). Measurement of neighborhood-based physical activity bouts. Health & Place, 70, 102595. doi: / 10.1016/j.healthplace.2021.102595 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forsyth A, Van Riper D, Larson N, Wall M, & Neumark-Sztainer D (2012). Creating a replicable, valid cross-platform buffering technique: The sausage network buffer for measuring food and physical activity built environments. International Journal of Health Geographics, 11, 9. doi: 10.1186/1476-072x-11-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fotheringham AS, & Wong DW (1991). The modifiable areal unit problem in multivariate statistical analysis. Environment and Planning A, 23(7), 1025–1044. doi: 10.1068/a231025 [DOI] [Google Scholar]
- Frank LD, Saelens BE, Powell KE, & Chapman JE (2007). Stepping towards causation: Do built environments or neighborhood and travel preferences explain physical activity, driving, and obesity? Social Science & Medicine, 65(9), 1898–1914. doi: 10.1016/j.soescimed.2007.05.053 [DOI] [PubMed] [Google Scholar]
- Garin N, Olaya B, Miret M, Ayuso-Mateos JL, Power M, Bucciarelli P, & Haro JM (2014). Built environment and elderly population health: a comprehensive literature review. Clinical practice and epidemiology in mental health: CP & EMH, 10, 103. doi: 10.2174/1745017901410010103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gunn LD, King TL, Mavoa S, Lamb KE, Giles-Corti B, & Kavanagh A (2017). Identifying destination distances that support walking trips in local neighborhoods. Journal of Transport & Health, 5, 133–141. doi: 10.1016/j.jth.2016.08.009 [DOI] [Google Scholar]
- Hajat A, Diez-Roux A, Franklin TG, Seeman T, Shrager S, Ranjit N, Castro C, Watson K, Sanchez B & Kirschbaum C (2010). Socioeconomic and race/ethnic differences in daily salivary cortisol profiles: the multi-ethnic study of atherosclerosis. Psychoneuroendocrinology, 35(6), 932–943. doi: 10.1016/j.psyneuen.2009.12.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heath GW, Brownson RC, Kruger J, Miles R, Powell KE, & Ramsey LT (2006). The effectiveness of urban design and land use and transport policies and practices to increase physical activity: a systematic review. Journal of physical activity and health, 3(s1), S55–S76. doi: 10.1123/jpah.3.s1.s55 [DOI] [PubMed] [Google Scholar]
- Hirsch JA, Moore KA, Cahill J, Quinn J, Zhao Y, Bayer FJ, Rundle A & Lovasi GS (2021). Business data categorization and refinement for application in longitudinal neighborhood health research: a methodology. Journal of urban health, 98(2), 271–284. doi: 10.1007/s11524-020-00482-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch JA, Moore KA, Clarke PJ, Rodriguez DA, Evenson KR, Brines SJ, Zagorski MA & Diez Roux AV (2014). Changes in the Built Environment and Changes in the Amount of Walking Over Time: Longitudinal Results From the Multi-Ethnic Study of Atherosclerosis. American Journal of Epidemiology, 180(8), 799–809. doi: 10.1093/aje/kwu218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch JA, Winters M, Clarke P, & McKay H (2014). Generating GPS activity spaces that shed light upon the mobility habits of older adults: a descriptive analysis. International Journal of Health Geographics, 13, 14. doi: 10.1186/1476-072x-13-51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch JA, Moore KA, Evenson KR, Rodriguez DA, & Roux AVD (2013). Walk Score® and Transit Score® and Walking in the Multi-Ethnic Study of Atherosclerosis. American Journal of Preventive Medicine, 45(2), 158–166. doi: 10.1016/j.amepre.2013.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoehner CM, & Schootman M (2010). Concordance of commercial data sources for neighborhood-effects studies. Journal of urban health, 87(4), 713–725. doi: 10.1007/s11524-010-9458-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphreys BR, McLeod L & Ruseski JE (2014). Physical activity and health outcomes: evidence from Canada. Health economics, 23(1), 33–54. doi: 10.1002/hec.2900 [DOI] [PubMed] [Google Scholar]
- Jia P, Pan X, Liu F, He P, Zhang W, Liu L, Zou Y & Chen L (2021). Land use mix in the neighbourhood and childhood obesity. Obesity Reviews, 22, e13098. doi: 10.1111/obr.13098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr J, Frank L, Sallis JF, Saelens B, Glanz K, & Chapman J (2012). Predictors of trips to food destinations. International Journal of Behavioral Nutrition and Physical Activity, 9(1), 58. doi: 10.1186/1479-5868-9-58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khattak AJ, & Rodriguez D (2005). Travel behavior in neo-traditional neighborhood developments: A case study in USA. Transportation Research Part a-Policy and Practice, 39(6), 481–500. doi: 10.1016/j.tra.2005.02.009 [DOI] [Google Scholar]
- Kitamura R, Mokhtarian PL, & Laidet L (1997). A micro-analysis of land use and travel in five neighborhoods in the San Francisco Bay Area. Transportation, 24(2), 125–158. doi: 10.1023/a:1017959825565 [DOI] [Google Scholar]
- Knuiman MW, Christian HE, Divitini ML, Foster SA, Bull FC, Badland HM, & Giles-Corti B (2014). A Longitudinal Analysis of the Influence of the Neighborhood Built Environment on Walking for Transportation. American Journal of Epidemiology, 180(5), 453–461. doi: 10.1093/aje/kwu171 [DOI] [PubMed] [Google Scholar]
- Kwan M-P (2012a). How GIS can help address the uncertain geographic context problem in social science research. Annals of GIS, 18(4), 245–255. doi: 10.1080/19475683.2012.727867 [DOI] [Google Scholar]
- Kwan M-P (2012b). The Uncertain Geographic Context Problem. Annals of the Association of American Geographers, 102(5), 958–968. doi: 10.1080/00045608.2012.687349 [DOI] [Google Scholar]
- Leal C & Chaix B (2011). The influence of geographic life environments on cardiometabolic risk factors: a systematic review, a methodological assessment and a research agenda. Obesity reviews, 12(3), 217–230. doi: 10.1111/j.1467-789X.2010.00726.x [DOI] [PubMed] [Google Scholar]
- Li J, Auchincloss AH, Yang Y, Rodriguez DA, & Sánchez BN (2020). Neighborhood characteristics and transport walking: Exploring multiple pathways of influence using a structural equation modeling approach. Journal of Transport Geography, 85, 102703. doi: 10.1016/j.jtrangeo.2020.102703 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li J, & Kim C (2018). Measuring Individuals’ Spatial Access to Healthy Foods by Incorporating Mobility, Time, and Mode: Activity Space Measures. The Professional Geographer, 70(2), 198–208. doi: 10.1080/00330124.2017.1338591 [DOI] [Google Scholar]
- Li J, & Kim C (2020). Exploring relationships of grocery shopping patterns and healthy food accessibility in residential neighborhoods and activity space. Applied Geography, 116, 102169. doi: 10.1016/j.apgeog.2020.102169 [DOI] [Google Scholar]
- Lovasi GS, Grady S, & Rundle A (2011). Steps Forward: Review and Recommendations for Research on Walkability, Physical Activity and Cardiovascular Health. Public Health Reviews, 33(2), 484–506. doi: 10.1007/BF03391647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macintyre S, Ellaway A, & Cummins S (2002). Place effects on health: how can we conceptualise, operationalise and measure them? Social Science & Medicine, 55(1), 125–139. doi: 10.1016/s0277-9536(01)00214-3 [DOI] [PubMed] [Google Scholar]
- Martin A, Ogilvie D, & Suhrcke M (2014). Evaluating causal relationships between urban built environment characteristics and obesity: a methodological review of observational studies. International Journal of Behavioral Nutrition and Physical Activity, 11, 15. doi: 10.1186/s12966-014-0142-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCormack GR, Koohsari MJ, Turley L, Nakaya T, Shibata A, Ishii K, Yasunaga A & Oka K (2021). Evidence for urban design and public health policy and practice: Space syntax metrics and neighborhood walking. Health & Place, 67, 102277. doi: 10.1016/j.healthplace.2019.102277 [DOI] [PubMed] [Google Scholar]
- Mitchell JT, Schick RS, Hallyburton M, Dennis MF, Kollins SH, Beckham JC, & McClernon FJ (2014). Combined Ecological Momentary Assessment and Global Positioning System Tracking to Assess Smoking Behavior: A Proof of Concept Study. Journal of Dual Diagnosis, 10(1), 19–29. doi: 10.1080/15504263.2013.866841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mooney SJ, Hurvitz PM, Moudon AV, Zhou C, Dalmat R, & Saelens BE (2020). Residential neighborhood features associated with objectively measured walking near home: Revisiting walkability using the Automatic Context Measurement Tool (ACMT). Health & Place, 63, 102332. doi: 10.1016/j.healthplace.2020.102332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moudon AV, Lee C, Cheadle AD, Garvin C, Johnson D, Schmid TL, Weathers RD and Lin L (2006). Operational definitions of walkable neighborhood: theoretical and empirical insights. Journal of physical activity and health, 3(s1), S99–S117. doi: 10.1123/jpah.3.s1.s99 [DOI] [PubMed] [Google Scholar]
- O’Campo P (2003). Invited Commentary: Advancing Theory and Methods for Multilevel Models of Residential Neighborhoods and Health. American Journal of Epidemiology, 157(1), 9–13. doi: 10.1093/aje/kwf171 [DOI] [PubMed] [Google Scholar]
- Pope CA III, Dockery DW, Spengler JD, & Raizenne ME (1991). Respiratory health and PM10 pollution: a daily time series analysis. American Review of Respiratory Disease, 144(3_pt_1), 668–674. doi: 10.1164/ajrccm/144.3_Pt_1.668 [DOI] [PubMed] [Google Scholar]
- Renalds A, Smith TH, & Hale PJ (2010). A systematic review of built environment and health. Family & community health, 33(1), 68–78. doi: 10.1097/FCH.0b013e3181c4e2e5 [DOI] [PubMed] [Google Scholar]
- Rodriguez DA, Evenson KR, Roux AVD, & Brines SJ (2009). Land Use, Residential Density, and Walking The Multi-Ethnic Study of Atherosclerosis. American Journal of Preventive Medicine, 37(5), 397–404. doi: 10.1016/j.amepre.2009.07.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodriguez-Loureiro L, Casas L, Bauwelinck M, Lefebvre W, Vanpoucke C, Vanroelen C, & Gadeyne S (2021). Social inequalities in the associations between urban green spaces, self-perceived health and mortality in Brussels: Results from a census-based cohort study. Health & Place, 70, 102603. doi: 10.1016/j.healthplace.2021.102603 [DOI] [PubMed] [Google Scholar]
- Roux AVD (2003). Residential environments and cardiovascular risk. Journal of urban health, 80(4), 569–589. doi: 10.1093/jurban/jtg065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schipperijn J, Ried-Larsen M, Nielsen MS, Holdt AF, Grontved A, Ersboll AK, & Kristensen PL (2015). A Longitudinal Study of Objectively Measured Built Environment as Determinant of Physical Activity in Young Adults: The European Youth Heart Study. J Phys Act Health, 12(7), 909–914. doi: 10.1123/jpah.2014-0039 [DOI] [PubMed] [Google Scholar]
- Smith G, Gidlow C, Davey R, & Foster C (2010). What is my walking neighbourhood? A pilot study of English adults’ definitions of their local walking neighbourhoods. International Journal of Behavioral Nutrition and Physical Activity, 7, 8. doi: 10.1186/1479-5868-7-34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielman SE, & Yoo EH (2009). The spatial dimensions of neighborhood effects. Soc Sci Med, 68(6), 1098–1105. doi: 10.1016/j.socscimed.2008.12.048 [DOI] [PubMed] [Google Scholar]
- Steinmetz-Wood M, El-Geneidy A, & Ross NA (2020). Moving to policy-amenable options for built environment research: The role of micro-scale neighborhood environment in promoting walking. Health & Place, 66, 102462. doi: 10.1016/j.healthplace.2020.102462 [DOI] [PubMed] [Google Scholar]
- Sun GB, Oreskovic NM, & Lin H (2014). How do changes to the built environment influence walking behaviors? a longitudinal study within a university campus in Hong Kong. International Journal of Health Geographics, 13, 10. doi: 10.1186/1476-072x-13-28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vallee J, Le Roux G, Chaix B, Kestens Y, & Chauvin P (2015). The ‘constant size neighbourhood trap’ in accessibility and health studies. Urban Studies, 52(2), 338–357. doi: 10.1177/0042098014528393 [DOI] [Google Scholar]
- Van Dyck D, Cardon G, Deforche B, Owen N, & De Bourdeaudhuij I (2011). Relationships between neighborhood walkability and adults’ physical activity: How important is residential self-selection? Health & Place, 17(4), 1011–1014. doi: 10.1016/j.healthplace.2011.05.005 [DOI] [PubMed] [Google Scholar]
- Walls, & Associates. (2013). National Establishment Time-Series (NETS) Database: 2012 Database Description.
- Wan N, Zou B, & Sternberg T (2012). A three-step floating catchment area method for analyzing spatial access to health services. International Journal of Geographical Information Science, 26(6), 1073–1089. doi: 10.1080/13658816.2011.624987 [DOI] [Google Scholar]
- Welty LJ, Peng R, Zeger S, & Dominici F (2009). Bayesian distributed lag models: estimating effects of particulate matter air pollution on daily mortality. Biometrics, 65(1), 282–291. doi: 10.1111/j.1541-0420.2007.01039.x [DOI] [PubMed] [Google Scholar]
- Xie B, Lu Y, Wu L, & An Z (2021). Dose-response effect of a large-scale greenway intervention on physical activities: The first natural experimental study in China. Health & Place, 67, 102502. doi: 10.1016/j.healthplace.2020.102502 [DOI] [PubMed] [Google Scholar]
- Yang Y, & Diez-Roux AV (2012). Walking Distance by Trip Purpose and Population Subgroups. American Journal of Preventive Medicine, 43(1), 11–19. doi: 10.1016/j.amepre.2012.03.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanobetti A, Wand M, Schwartz J, & Ryan L (2000). Generalized additive distributed lag models: quantifying mortality displacement. Biostatistics, 1(3), 279–292. doi: / 10.1093/biostatistics/1.3.279 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.