

Abstract
Background: Metabolic syndrome (MetS) is characterized by the cooccurrence of obesity, insulin resistance, dyslipidaemia, and hypertension. Red yeast rice (RYR) preparations might be beneficial for the prevention and treatment of MetS.
Objective: To implement a systematic review and meta−analysis to determine whether RYR preparations improve clinical endpoints and reduce risk factors for MetS.
Methods: The PubMed, Cochrane Library, EMBASE, Scopus, China National Knowledge Infrastructure, Chinese VIP Information, and WanFang databases were searched for randomized controlled trials (published up to September 2020), and a meta−analysis was performed using fixed− or random−effects models. The primary outcome measures were mortality and major adverse cardiovascular events (MACEs), and the secondary outcome measures were biochemical parameters of blood glucose, blood lipids, and blood pressure. The registration number is CRD42020209186.
Results: A total of 921 articles were identified, of which 30 articles were included in this article. RYR preparations group demonstrated significant improvements in MetS compared with control group. RYR preparations reduced the mortality and MACEs (RR = 0.62, 95% CI [0.49, 0.78]; RR = 0.54, 95% CI [0.43, 0.66]). In terms of blood glucose metabolism, fasting plasma glucose (FPG) (MD = −0.46 mmol/L, 95% CI [−0.71, −0.22]), haemoglobin A1c (HbA1c) (MD = −0.49, 95% CI [−0.71, −0.26]) and the homeostasis model assessment of insulin resistance (HOMA−IR) (MD = −0.93, 95% CI [−1.64, −0.21]) were decreased. Regarding the lipid metabolism, total cholesterol (TC) (MD = −0.74 mmol/L, 95% CI [−1.02, −0.46]), triglycerides (TG) (MD = −0.45 mmol/L, 95% CI [−0.70, −0.21]), and low−density lipoprotein cholesterol (LDL) (MD = −0.42 mmol/L, 95% CI [−0.78, −0.06]) were decreased, while high−density lipoprotein cholesterol (HDL) (MD = 0.14 mmol/L, 95% CI [0.09, 0.20]) was increased. Regarding blood pressure, the mean arterial pressure (MAP) (MD = −3.79 mmHg, 95% CI [−5.01, −2.57]) was decreased. In addition, RYR preparations did not increase the incidence of adverse reactions (RR = 1.00, 95% CI [0.69, 1.43]).
Conclusion: RYR preparations reduce mortality, MACEs, and multiple risk factors for MetS without compromising safety, which supports its application for the prevention and treatment of MetS. However, additional high−quality studies are needed to provide more evidence for the effect of RYR on MetS due to the heterogeneity in this study.
Systematic Review Registration: www.crd.york.ac.uk/PROSPERO, identifier CRD42020209186
Keywords: red yeast rice, metabolic syndrome, clinical endpoints, risk factors, dyslipidaemia, hypertension, diabetes
Introduction
Metabolic syndrome (MetS) comprises atherogenic dyslipidaemia, hypertension, obesity, and insulin resistance (Hu et al., 2020), and is associated with an increased risk of type 2 diabetes mellitus, nonalcoholic fatty liver disease, myocardial infarction, and stroke (Prasun, 2020). MetS has become increasingly prevalent with the improvement of people’s lives, and it is associated with an increased risk for cardiovascular disease (CVD) and all−cause mortality (Hirode and Wong, 2020). At present, MetS is an urgent global health problem that is unresolved, and there is no single drug that simultaneously treats the multiple diseases or regulates complex underlying mechanisms of MetS yet (Hu et al., 2020). Therefore, it is important to identify therapies that impede the development of metabolic diseases from a preventive perspective.
Red yeast rice (RYR), also known as Hong Qu, Hon−Chi, Anka and red Koji, is a functional food containing monacolin K (lovastatin), monacolin KA, citrinin (ppb), and so on (Halber et al., 2010), and active ingredient monacolin K is the first statin drug (lovastatin) to be approved for treatment of high cholesterol levels (Hunter and Hegele, 2017). RYR is made by fermenting steamed rice with an edible fungus, Monascus purpureus Went. RYR products included RYR powders, dietary supplements, and Chinese proprietary medicines (Xuezhikang and Zhibituo), and ingredients were controllable (Klingelhöfer, and Morlock, 2019). Substantial evidence suggests a strong biochemical effect of RYR on plasma lipid levels and it is frequently consumed to lower low−density lipoprotein (LDL) as an alternative to statins (Loubser et al., 2019).
Several meta−analyses have shown that RYR is an effective and relatively safe therapy for dyslipidaemia (Xiong et al., 2017; Sungthong et al., 2020). Increasing evidence also suggests that RYR has antidyslipidaemia, antidiabetic, antiatherosclerotic, antiobesity, and antihypertensive activities (Zhu et al., 2019), leading to a growing interest in the hypothesis that RYR has beneficial health effects on MetS and its adverse clinical outcomes. Thus, we aimed to evaluate the efficacy and safety of RYR preparations in MetS through a systematic review and meta−analysis of randomized controlled trials (RCTs).
Methods
This study was conducted and reported based on the guidelines of PRISMA and was registered in PROSPERO (the registration number is CRD42020209186).
Search Strategies
We identified articles by searching the following electronic databases from database inception until September 2020: PubMed, Cochrane Library, EMBASE, Scopus, China National Knowledge Infrastructure, Chinese VIP Information, and WanFang. The search strategy included population and intervention keywords (MetS and RYR preparations) as well as synonyms of these terms (Supplementary Material S1). We also manually searched the reference lists of the included articles. Authors of relevant studies were contacted to obtain additional and missing data. Two reviewers (RY, YY) independently identified relevant studies, and any disagreement was resolved through discussion or consultation with a third reviewer.
Selection of Studies
The inclusion criteria were as follows: a) Populations: participants meeting at least one of the international or domestic diagnostic criteria for MetS with no restrictions of age, sex, race, course; b) Interventions: patients in the treatment group were given RYR preparations alone or combined with conventional treatment (hypoglycemic drugs, lipid−lowering drugs, and antihypertensive drugs alone or the combination of these drugs), defining RYR preparations as involving Xuezhikang interventions or other relevant preparations; c) Comparators: patients in the control group were given conventional treatment or placebo; d) Outcomes: reported data for at least one of the interest outcomes: the primary outcomes of interest were mortality and MACEs, the secondary outcomes of interest included MetS risk factors, such as blood sugar parameters [fasting plasma glucose (FPG), haemoglobin A1c (HbA1c), homeostasis model assessment of insulin resistance (HOMA−IR), insulin sensitivity index (ISI)], blood lipid parameters [total cholesterol (TC), triglycerides (TG), LDL, high−density lipoprotein (HDL)], and blood pressure [mean arterial pressure (MAP), systolic blood pressure (SBP), and diastolic blood pressure (DBP)]. In addition, adverse reactions were also assessed; e) Study designs: RCTs.
The exclusion criteria were as follows: a) included patients with severe abnormal heart, liver and kidney function, severe infections, tumor or other serious primary disease; b) included patients with special populations such as lactating woman or pregnant women; c) patients in the treatment group were given nutraceuticals combination compound; d) no clinical data could be extracted; e) reviews, retrospective studies, observational studies, letters, case reports, and animal/cell experiments.
Data Extraction
The Cochrane Data Collection form was applied for the data extraction. Two independent investigators (RY and YY) reviewed the studies and extracted the data. The following data were extracted for each study: participant characteristics, such as the number of participants in each group, age, sex, drug and control treatment, intervention duration, outcomes (major adverse cardiovascular events (MACEs), mortality, and the biochemical parameters of blood glucose, blood lipids, and blood pressure), and adverse events.
Quality Assessment
Two reviewers (YR, YY) independently evaluated the quality of included studies according to the Physiotherapy Evidence Database (PEDro) scale (Moseley et al., 2020), which is exclusively applied to assess the risk of bias in RCTs. The PEDro criteria items include eligibility criteria, random allocation, concealed allocation, group similarity at baseline, participant/therapist/assessor blinding, dropout number, intention−to−treat analysis, between−group differences, and point estimate and variability. The PEDro scale awards 1 point per criterion (the first criterion is not scored): a score of less than 4 is considered “poor”, 4 to 5 is considered “fair”, 6 to 8 is considered “good” and 9 to 10 is considered ‘excellent’ (Cashin and Mcauley, 2020). In addition, we assessed the quality of included evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach, which classifies the evidence as high, moderate, low, or very low.
Data Analysis
RevMan 5.3.0 was utilized to analyse the results. Continuous variables were calculated by the mean difference (MD) and 95% confidence interval (CI). Dichotomous variables were expressed as relative risk (RR) with 95% CI. According to the Cochrane Handbook for Systematic Reviews of Interventions, once the multiple treatment groups were included from one study, the shared control group were split into two or more groups with smaller sample sizes, and two or more (reasonably independent) comparisons were included (Higgins et al., 2019). The heterogeneity of the results across the studies was evaluated using the I 2 statistic: I 2 < 50% were considered to have low heterogeneity and the results were estimated by a fixed−effects model, while I 2 ≥ 50% were considered to have moderate and high heterogeneity and the results were estimated by a random−effects model. In cases of heterogeneity, we investigated the potential causes by performing subgroup and meta−regression analyses. When there were high levels of heterogeneity, study characteristics and data−related factors (such as age, sex, intervention duration and intervention type) were explored to identify the cause of the heterogeneity. Stata 15.1 was utilized to draw funnel plots, and we conducted Egger’s test to detect publication bias when the number of studies for each outcome was above or equal to 10.
Results
Study Selection
A total of 921 articles were searched, and 805 articles were screened by the title and abstract after the removal of duplicates. A total of 139 articles were identified for review based on the full text, and 30 articles were eligible to be included in the review (Figure 1). Data were only included once in meta−analysis when participant data reported in more than one publication.
FIGURE 1.

Overview of the systematic review process.
Study Characteristics
In this meta−analysis, Li et al., 2017 contained two treatment groups and presented the results separately for Xuezhikang or Xuezhikang + Daixiefang compared with Daixiefang (a traditional Chinese medicine prescription). Two articles (Li et al., 2010) (Li et al., 2009) reported data from one trial. The clinical studies were published in English and Chinese from 1997 to 2019, and all of the studies were conducted in China except for one from Italy. A total of 5440 patients were included, and the mean age of the participants ranged from 41 to 76. Interventions included Xuezhikang and lovastatin, and trial duration ranged from 1 month to 4.5 years. The detailed characteristics of the included trials are shown in Table 1. The detailed information of RYR preparations in the included trials is described in Supplementary Table S1. The PEDro score ranged from 4 (Shen, 2011; Zhang and Wu, 2014) to 9 (Li et al., 2009; Li et al., 2010; Li et al., 2017) (Supplementary Table S2).
TABLE 1.
Study characteristics.
| Study (country) | Population | PEDro score | Participants (int:cont) | Male: Female (int/cont) | Age range | Trial intervention | Control intervention | Period of treatment | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Zhang, (2019) | Diabetes + hyperlipidaemia | 6 | 67:67 | 33:34/36:31 | int: 45.19 ± 3.84 | Lovastatin + metformin | Metformin | 8 weeks | TC, TG, FPG, HbA1c |
| cont: 45.18 ± 1.91 | |||||||||
| Xiao, (2019) | Hyperlipidaemia + prehypertension | 6 | 42:42 | 23:19/25:17 | int: 67.53 ± 5.76 | Xuezhikang | Atorvastatin calcium | 4 weeks | TC, TG, HDL−C, LDL−C SBP, DBP, MAP |
| cont: 68.24 ± 6.13 | |||||||||
| Li et al. (2017) | MetS | 9 | 20:21 | 5:15/11:10 | int: 68.25 ± 10.92/cont: 62.38 ± 9.90 | Xuezhikang | Daixiefang* | 12 weeks | TC, TG, HDL−C, LDL−C, FPG, HbA1c, HOMA−IR |
| 21:21 | 7:14/11:10 | int: 66.10 ± 8.85 | Xuezhikang + Daixiefang | ||||||
| cont: 62.38 ± 9.90 | |||||||||
| Wang and Wang, (2016) | Hyperlipidaemia + prehypertension | 6 | 62:62 | 48:14/46:16 | int: 66.7 ± 7.9 | Xuezhikang | Atorvastatin calcium | 8 weeks | TC, TG, HDL−C, LDL−C, SBP, DBP, MAP |
| cont: 67.6 ± 8.1 | |||||||||
| Zhao, (2015) | Diabetes + dyslipidaemia | 5 | 32:33 | 17:15/15:18 | int: 59.6 ± 4.7 | Xuezhikang | Placebo | 8 weeks | TC, TG, HDL−C, LDL−C |
| cont: 57.6 ± 5.3 | |||||||||
| Ke, (2015) | Diabetes + dyslipidaemia | 6 | 29:29 | 18:11/16:13 | int: 62.3 ± 6.6 | Xuezhikang | Simvastatin | 12 weeks | TC, TG, HDL−C, LDL−C, FPG |
| cont: 62.9 ± 7.1 | |||||||||
| Zhang and Wu, (2014) | MetS | 4 | 20:20 | 24:16 | 76 ± 10 | Xuezhikang + routine treatment | Routine treatment | 12 weeks | TG, HDL−C, SBP, DBP, FPG, HOMA−IR |
| Chen, (2013) | Diabetes + hyperlipidaemia | 7 | 45:44 | Not reported | 45–70 | Xuezhikang | Simvastatin | 12 weeks | TC, TG, HDL−C, LDL−C |
| Wang and Liu, (2013) | Diabetes + dyslipidaemia | 6 | 32:30 | 18:14/13:17 | int: 59 ± 7.6 | Xuezhikang | Simvastatin | 8 weeks | TG |
| cont: 61 ± 9.3 | |||||||||
| Wu and Wei, (2011) | Hypertension + dyslipidaemia | 5 | 75:75 | 48:27/49:26 | int: 54.8 ± 10.2 | Xuezhikang | Atorvastatin calcium | 8 weeks | TC, TG, HDL−C, LDL−C |
| cont: 55.26 ± 9.8 | |||||||||
| Ma and Qian, (2011) | Diabetes + dyslipidaemia | 6 | 37:37 | 22:15/24:13 | int: 42–66 | Xuezhikang | Simvastatin | 6 weeks | TC, TG, HDL−C |
| cont: 41–65 | |||||||||
| Shen, (2011) | Diabetes + dyslipidaemia | 4 | 40:25 | 35:30 | 45–65 | Xuezhikang + routine treatment | Routine treatment | 18 weeks | TG, HDL−C, LDL−C, MACEs |
| Li et al., 2010 | Hypertension + dyslipidaemia | 9 | 1363:1341 | 1093:270/1054:287 | int: 59.4 ± 9.2 | Xuezhikang | Placebo | 4.5 years | TC, TG, HDL−C, LDL−C, SBP, DBP, mortality, MACEs |
| cont: 59.2 ± 9.5 | |||||||||
| Zhai and Li, (2010) | Diabetes + hyperlipidaemia | 5 | 48:38 | 28:20/21:17 | int: 50.6 | Xuezhikang + routine treatment | Routine treatment | 12 weeks | TG, TC |
| cont: 51.8 | |||||||||
| Li et al, (2009) | Hypertension + dyslipidaemia | 9 | 772:758 | 1143/387 | int: 66 ± 4 | Xuezhikang | Placebo | 4.5 years | SBP, DBP, TG, TC, LDL−C, HDL−C |
| cont: 66 ± 4 | |||||||||
| He and Zhan, (2009) | Diabetic nephropathy | 6 | 72:72 | 56:16/58:14 | int: 53.3 ± 9.4 | Xuezhikang | Atorvastatin calcium | 48 weeks | TC, TG |
| cont: 51.3 ± 11.6 | |||||||||
| Zhang, (2009) | Diabetes + dyslipidaemia | 8 | 45:43 | 33:12/29:14 | int: 61.2 ± 4.6 | Xuezhikang + routine treatment | Routine treatment | 16 weeks | TC, TG, HDL−C |
| cont: 58.8 ± 6.2 | |||||||||
| Jin et al. (2007) | Diabetic nephropathy + dyslipidaemia | 6 | 30:30 | 21:9/19:11 | int: 52.81 ± 9.39 | Xuezhikang + routine treatment | Routine treatment | 12 weeks | TC, TG, HDL−C, FPG |
| cont: 54.96 ± 7.98 | |||||||||
| Zhao et al. (2007) | Diabetes + dyslipidaemia | 7 | 306:285 | 226:80/198:87 | int: 60.5 ± 8.7 | Xuezhikang | Placebo | 4 years | TC, TG, HDL−C, LDL−C, mortality, MACEs |
| cont: 61.6 ± 8.0 | |||||||||
| Wang et al. (2005) | Diabetes + hyperlipidaemia | 5 | 32:30 | 17:15/16:14 | int: 54.2 ± 10.4 | Xuezhikang | Pravastatin | 8 weeks | TC, TG, HDL−C, LDL−C |
| cont: 55.1 ± 9.5 | |||||||||
| Zhu and Yao, (2005) | Diabetes + hyperlipidaemia | 6 | 31:31 | 40:22 | 51–75 | Xuezhikang | Routine treatment | 4 weeks | TC, TG, FPG |
| Li et al. (2005) | Diabetes + hyperlipidaemia | 6 | 24:24 | Not reported | 40–50 | Xuezhikang + routine treatment | Routine treatment | 8 weeks | TC, TG, HDL−C, LDL−C, FPG, HbA1c |
| Yao et al. (2004) | Diabetes + hyperlipidaemia | 6 | 24:22 | 12:12/12:10 | int: 56.87 | Xuezhikang + routine treatment | Routine treatment | 8 weeks | TC, TG, HDL−C, LDL−C, FPG |
| cont: 57.37 | |||||||||
| Sui, (2003) | Diabetes + hyperlipidaemia | 5 | 48:32 | 24:24/22:10 | int: 45–73 | Xuezhikang | Amaranth capsules | 8 weeks | TC, TG, HDL−C, FPG, ISI, HbA1c |
| cont: 42–70 | |||||||||
| Deng et al. (2003) | Diabetes + hyperlipidaemia | 6 | 30:26 | 34:22 | 52.6 ± 7.3 | Xuezhikang + routine treatment | Routine treatment | weeks | TC, TG, HDL−C, LDL−C |
| Zeng et al. (2001) | Diabetes + hyperlipidaemia | 5 | 22:24 | 12:10/12:12 | int: 47–71 | Xuezhikang + routine treatment | Routine treatment | 8 weeks | TC, TG, HDL−C, LDL−C, FPG, HbA1c |
| cont: 52–74 | |||||||||
| Gentile et al. (2000) | Diabetes + hypercholesterolemia | 6 | 80:86 | 54:26/63:23 | int: 58 ± 5 | Lovastatin | Placebo | 24 weeks | TC, TG, HDL−C, LDL−C |
| cont: 61 ± 6 | |||||||||
| Peng et al. (2000) | Diabetes + hyperlipidaemia | 5 | 34:34 | 22:12/25:9 | int: 44.1 ± 9.0 | Xuezhikang + routine treatment | Routine treatment | 24 weeks | TC, TG, FPG, HbA1c |
| cont: 46.7 ± 9.6 | |||||||||
| Chang et al. (1998) | Hypertension + hyperlipidaemia | 6 | 32:30 | 30:32 | 56.7 ± 6.2 | Lovastatin | Inositol nicotinate | 2 months | TC, TG, HDL−C |
| Wang et al. (1997) | Diabetes + hyperlipidaemia | 5 | 17:17 | 9:25 | 60 ± 4 | Xuezhikang | Gemfibrozil | 4 weeks | TC, TG, HDL−C, ISI |
Note:*Daixiefang: a prescription of traditional Chinese medicine is used to improve the metabolism, including Prunus persica (L.) batsch, Rheum officinale Baill., Alisma plantago−aquatica Linn., trichosanthis radix, Dendranthema indicum(L) Des Moul., and Crataegus pinnatifida, Sargassum.
Risk of Bias
The median score on the PEDro (on a scale of 0–10) for the included trials was 6. Among the 30 original trials, ten (33.3%) trials were considered “fair” quality and had a medium risk of bias (PEDro score ranging from 4 to 5). Seventeen (56.7%) trials were considered “good” quality and had a low risk of bias (PEDro score ranging from 6 to 8). Three (10.0%) trials were considered “excellent” quality and had a low risk of bias (PEDro score of 9) (Table 1). The main reasons for the risk of bias were nonblinded therapists (24 trials [80.0%]), nonblinded assessors (30 trials [100.0%]), not performing concealed allocation (27 trials [90.0%]), and withdrawal rates higher than 15% (8 trials [26.7%]) ( Supplementary Table S2).
Effects of RYR Preparations on Mortality and MACEs
Two trials (Zhao et al., 2007; Li et al., 2010) including 3297 participants reported therapeutic effects of RYR on mortality, and three trials (Zhao et al., 2007; Li et al., 2010; Shen, 2011) including 3360 participants reported its therapeutic effects on MACEs. RYR preparations significantly reduced the mortality (RR = 0.62, 95% CI [0.49, 0.78]), and MACEs (RR = 0.54, 95% CI [0.43, 0.66]) compared with control group. Furthermore, there was no heterogeneity among the studies (Figure 2).
FIGURE 2.

Forest plots of the risk of (A) mortality and (B) MACEs.
Effects of RYR Preparations on MetS Risk Factors
Blood Glucose Parameters (FPG, HbA1c, HOMA-IR, and ISI)
Ten trials including 646 participants reported therapeutic effects of RYR on FPG, and RYR preparations significantly reduced FPG level (−0.46 mmol/L, 95% CI [−0.71, −0.22]) compared with control group ( Figure 3A). There was high heterogeneity among the studies of FPG and subgroup analysis was performed. RYR preparations significantly reduced FPG level (−0.92 mmol/L, 95% CI [−1.26, −0.58], p < 0.00001, I 2 = 41%) in 40- to 50-year-old patients with more notable effects and low heterogeneity, while other subgroups had high heterogeneity. Besides, compared with conventional therapy, RYR plus conventional therapy reduced FPG level (−0.53 mmol/L, 95% CI [−0.93, −0.12], p = 0.01, I 2 = 67%) with medium heterogeneity, while other subgroups had high heterogeneity ( Supplementary Figure S1 ). Five trials including 392 participants reported its therapeutic effects on HbA1c, and RYR preparations reduced HbA1c level (−0.49, 95% CI [−0.71, −0.26]) compared with control group ( Figure 3B). There was high heterogeneity among the studies of HbA1c, hence subgroup analysis was performed. However, compared with conventional therapy, RYR plus conventional therapy reduced HbA1c level (−1.48 mmol/L, 95% CI [−2.13, −0.84], p < 0.00001, I 2 = 94%) with high heterogeneity, and the heterogeneity remains unexplained in other subgroups ( Supplementary Figure S2 ). Two trials including 102 participants reported therapeutic effects on HOMA−IR, and two trials including 114 participants reported therapeutic effects on ISI. RYR preparations lowered HOMA−IR (−0.93, 95% CI [−1.64, −0.21]) while did not increase ISI (2.02, 95% CI [−1.09, 5.12]) compared with control group ( Figures 3C,D−). There was high heterogeneity among the studies of HOMA-IR and ISI, yet subgroup analysis could not be performed and the heterogeneity could not be fully investigated due to the limited number of studies and the small sample sizes. Therefore, further validation on existing results is required.
FIGURE 3.

Forest plots of (A) FPG, (B) HbA1c, (C) HOMA−IR, and (D) ISI.
Lipid Profile Parameters (TC, TG, LDL-C, and HDL-C)
Twenty−three trials including 5084 participants reported therapeutic effects of RYR on TC, 26 trials including 5234 participants on TG, 16 trials including 4391 participants on LDL, and 19 trials including 4653 participants on HDL. RYR preparations reduced the levels of TC (−0.74 mmol/L, 95% CI [−1.02, −0.46]), TG (−0.45 mmol/L, 95% CI [−0.70, −0.21]) and LDL−C (−0.42 mmol/L, 95% CI [−0.78, −0.06]), while increased HDL−C level (0.14 mmol/L, 95% CI [0.09, 0.20]) compared with control group ( Figure 4). There was high heterogeneity among the studies of TC, TG, LDL−C and HDL−C, hence subgroup analysis was performed. RYR preparations significantly reduced the levels of TC (−1.55 mmol/L, 95% CI [−1.85, −1.25], p < 0.00001, I 2 = 0%) and TG (−0.70 mmol/L, 95% CI [−0.90, −0.50], p < 0.00001, I 2 = 24%) in 40− to 50−year−old patients with more notable effects and low heterogeneity, while other subgroups had high heterogeneity. It also significantly reduced TG level (−0.59 mmol/L, 95% CI [−0.66, −0.52], p < 0.00001, I 2 = 0%) in a higher proportion of women (male: female = 1:1.5) with more notable effects and low heterogeneity, while other subgroups had high heterogeneity. Moreover, RYR preparations significantly reduced the levels of TC (−0.19 mmol/L, 95% CI [−0.23, −0.15], p < 0.00001, I 2 = 26%), TG (−0.12 mmol/L, 95% CI [−0.18, −0.05], p = 0.0005, I 2 = 0%), LDL (−0.20 mmol/L, 95% CI [−0.23, −0.17], p < 0.00001, I 2 = 0%), and increased the level of HDL (0.01 mmol/L, 95% CI [0.00, 0.02], p = 0.02, I 2 = 0%) in the intervention duration of >12 months with mild effects and low heterogeneity, while other subgroups had high heterogeneity. However, compared with conventional therapy, RYR plus conventional therapy reduced the levels of TC (−1.48 mmol/L, 95% CI [−2.13, −0.84], p < 0.00001, I 2 = 94%), TG (−0.53 mmol/L, 95% CI [−0.78, −0.28], p < 0.0001, I 2 = 75%) and LDL (−0.70 mmol/L, 95% CI [−1.12, −0.28], p < 0.001, I 2 = 91%), while increased HDL level (0.40 mmol/L, 95% CI [0.03, 0.78], p = 0.03, I 2 = 96%) with high heterogeneity; compared with lipid−lowing drugs, RYR preparations increased HDL level (0.07 mmol/L, 95% CI [0.01, 0.12], p = 0.01, I 2 = 67%) with medium heterogeneity; compared with placebo, RYR preparations reduced the levels TC (−0.83 mmol/L, 95% CI [−1.58, −0.09], p = 0.03, I 2 = 100%) and LDL (−0.83 mmol/L, 95% CI [−1.64, −0.03], p = 0.04, I 2 = 100%) with high heterogeneity ( Supplementary Figures S3–S6 ). In addition, meta−regression analysis revealed that age was a significant moderator of TC (p = 0.017) ( Supplementary Table S3 ).
FIGURE 4.
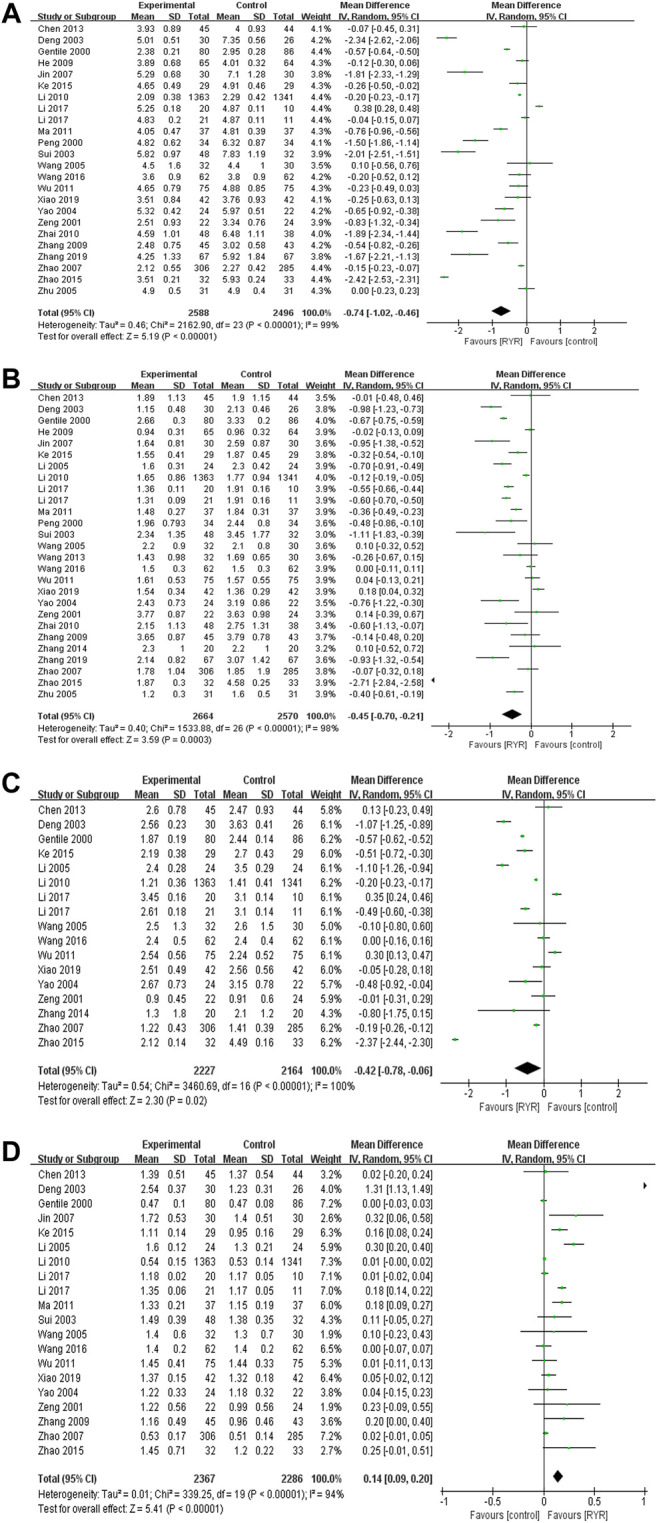
Forest plots of (A) TC, (B) TG, (C) LDL−C, and (D) HDL−C.
Blood Pressure Parameters (MAP, SBP, and DBP)
Two trials (Wang and Wang, 2016; Xiao 2019) including 208 participants reported therapeutic effects of RYR on MAP, and RYR preparations reduced MAP level (−3.79 mmHg, 95% CI [−5.01, −2.57]) compared with control group ( Figure 5A). There was high heterogeneity among the studies of MAP, while subgroup analysis could not be performed and the heterogeneity could not be fully investigated due to the limited number of studies and the small sample sizes. Therefore, further validation on existing results is required. Four trials including 2952 participants reported its therapeutic effects on SBP and DBP, while RYR preparations did not reduce SBP or DBP levels compared with control group ( Figures 5B,C−). There was high heterogeneity among the studies of SBP and DBP and subgroup analysis was performed. RYR preparations significantly reduced SBP level (−8.59 mmHg, 95% CI [−12.28, −4.91], p < 0.00001, I 2 = 62%) and DBP level (−7.02 mmHg, 95% CI [−8.82, −5.22], p < 0.00001, I 2 = 0%) in 60 to 70-year-old patients with more notable effects and low to medium heterogeneity, while other subgroups had high heterogeneity. RYR preparations significantly reduced SBP level (−6.72 mmHg, 95% CI [−11.31, −2.14], p = 0.004, I 2 = 74%) and DBP level (−6.36 mmHg, 95% CI [−8.93, −3.79], p < 0.00001, I 2 = 39%) in the intervention duration of ≤3 months with more notable effects and low to medium heterogeneity, while other subgroups had high heterogeneity. Furthermore, compared with lipid−lowing drugs, RYR preparations significantly reduced SBP level (−8.59 mmHg, 95% CI [−12.28, −4.91], p < 0.00001, I 2 = 62%) and DBP level (−7.02 mmHg, 95% CI [−8.82, −5.22], p < 0.00001, I 2 = 0%) with more notable effects and low to medium heterogeneity, while other subgroups had high heterogeneity ( Supplementary Figures S7–S8 ).
FIGURE 5.

Forest plots of (A) MAP, (B) SBP, and (C) DBP.
Effects of RYR Preparations on Adverse Reactions
Twelve trials including 4164 participants reported adverse reactions, including gastrointestinal disorders (nausea, abdominal pain, diarrhoea, flatulence, etc.), mental−neurological symptoms (depression, etc.), oedema, myalgia, dizziness, and allergic reactions. RYR preparations did not increase the incidence of adverse reactions compared with control group (1.00, 95% CI [0.69, 1.43]) and there was low heterogeneity (I 2 = 22%) among the studies ( Figure 6).
FIGURE 6.

Forest plot of the adverse reactions.
Sensitivity Analysis
Sensitivity analysis demonstrated the pooled effect estimates of mortality, MACEs, FPG, HbA1c, TC, TG, LDL-C, HDL-C, MAP, and adverse reactions did not substantially modify, and these results are robust. However, the pooled effect estimates showed no significant differences for HOMA−IR after excluding the study by Zhang and Wu, 2014, which indicated that this result was not robust. The reason might be related to low methodological quality of Zhang and Wu, 2014 (PEDro score = 4) with no concealed allocation and blinding, and the high risk of selection bias might exaggerate the effect of RYR preparations in lowering HOMA−IR. Furthermore, the pooled effect estimates showed significant differences in SBP and DBP after excluding the study by Li et al., 2010a, which also indicated that this result was not robust. The reason might be related to long duration of treatment in Li et al., 2010b (4.5 years), and the effects of RYR preparations on SBP and DBP might not be significant in the long follow−up time.
Publication Bias
Both visual inspection of the funnel plot and Egger’s test demonstrated no evidence of publication bias in FPG (p = 0.265), LDL-C (p = 0.241) and adverse reactions (p = 0.573). However, there was publication bias for TC (p = 0.040), TG (p = 0.001) and HDL−C (p = 0.002) (Figure 7 and Supplementary Table S4).
FIGURE 7.

Funnel plots of (A) FPG, (B) TC, (C) TG, (D) HDL−C, (E) LDL−C, and (F) adverse reactions.
Quality of the Evidence
All of the outcomes of interest were assessed with GRADE and evidence profiles are shown in Table 2. There was high-quality evidence on mortality, MACEs and adverse reactions; medium−quality evidence on FPG, HbA1c, HOMA-IR, TC, LDL-C, MAP and DBP; low-quality evidence on TG, HDL-C and SBP; and very low−quality evidence on ISI. The certainty of the evidence ranged from very low to high, which might be attributed to the risk of bias, reporting bias, inconsistency, and imprecision, indicating that these estimates are uncertain and that future studies are likely to influence our confidence in the results.
TABLE 2.
GRADE quality assessment.
| Bias | Inconsistency | Indirectness | Imprecision | Publication bias | Rating | ||
|---|---|---|---|---|---|---|---|
| Mortality, 2 RCTs (n = 3297) | RR 0.62, 95%CI 0.49 to 0.78, I2 0% | 0 | 0 | 0 | 0 | 0 d | 4: high |
| MACEs, 3 RCTs (n = 3360) | RR 0.54, 95%CI 0.43 to 0.66, I2 0% | 0 | 0 | 0 | 0 | 0 d | 4: high |
| FPG, 10 RCTs (n = 646) | MD −0.46, 95% CI −0.71to −0.22, I2 86% | 0 | −1 b | 0 | 0 | 0 | 3: medium |
| HbAc1, 5 RCTs (n = 392) | MD −0.49, 95%CI −0.71 to −0.26, I2 95% | 0 | −1 b | 0 | 0 | 0 d | 3: medium |
| HOMA−IR, 2 RCTs (n = 102) | MD −0.93, 95%CI −1.64 to −0.21, I2 95% | 0 | −1 b | 0 | 0 | 0 d | 3: medium |
| ISI, 2 RCTs (n = 114) | MD 2.02, 95%CI −1.09 to 5.12, I2 61% | −1 a | −1 b | 0 | −1 c | 0 d | 1: very low |
| TC, 23 RCTs (n = 5114) | MD −0.74, 95%CI −1.02 to −0.46, I2 99% | 0 | 0 | 0 | 0 | −1 e | 3: medium |
| TG, 26 RCTs (n = 5264) | MD −0.45, 95%CI −0.70 to −0.21, I2 98% | 0 | −1 b | 0 | 0 | −1 e | 2: low |
| LDL, 16 RCTs (n = 4421) | MD −0.42, 95%CI −0.78 to −0.06, I2 100% | 0 | −1 b | 0 | 0 | 0 | 3: medium |
| HDL, 19 RCTs (n = 4683) | MD 0.14, 95%CI 0.09 to 0.20, I2 94% | 0 | −1 b | 0 | 0 | −1 e | 2: low |
| MAP, 2 RCTs (n = 208) | MD −3.79, 95%CI −5.01 to −2.57, I2 79% | 0 | −1 b | 0 | 0 | 0 d | 3: medium |
| SBP, 4 RCTs (n = 2952) | MD −4.80, 95%CI −9.94 to 0.35, I2 93% | 0 | −1 b | 0 | −1 c | 0 d | 2: low |
| DBP, 4 RCTs (n = 2952) | MD −3.79, 95%CI −8.55 to 0.96, I2 94% | 0 | 0 | 0 | −1 c | 0 d | 3: medium |
| Adverse reactions, 12 RCTs (n = 4194) | RR 1.00, 95%CI 0.69 to 1.43, I2 22% | 0 | 0 | 0 | 0 | 0 | 4: high |
Downgraded one place due to the majority of trials scoring <6 on the PEDro scale.
Downgraded one place due to unexplained heterogeneity.
Downgraded one place due to the small sample size or the combined effect size passing the invalid line.
Funnel plots not completed due to <10 studies in the meta−analysis.
Downgraded one place due to publication bias.
Discussion
Summary of Main Results
This systematic review and meta-analysis showed robust and consistent findings that RYR preparations reduce mortality, MACEs, and risk factors of MetS. Therefore, RYR preparations might be an effective treatment to improve health outcomes and might assist in decreasing the MetS risk factors and preventing progression to CVD. Taken together, the results of these studies support the beneficial effects of RYR preparations across different clinical settings.
Clinical Benefits and Mechanism of Improving MetS Biochemical Parameter
Blood glucose parameters are related to diabetes. A recent nationwide epidemiological data demonstrated that elevated FPG increase the risk of CVD (Kaneko et al., 2021); each 1% higher HbA1c, independent of diabetes status, is associated with an 18% greater risk of myocardial infarction (de Jong et al., 2020); HOMA−IR is positive correlation with CVD risk (Lu et al., 2020). This meta−analysis observed that RYR preparations significantly reduced the levels of FPG, HbA1c and HOMA−IR, indicating its promising application in improving diabetes and CVD. Previous studies indicated that RYR could stimulate muscarinic M3 receptors in pancreatic cells and augment insulin release to lower plasma glucose (Chen and Liu, 2006); and inhibit high glucose−induced proangiogenic cells senescence and oxidative stress, thereby decreasing the vascular complications of diabetes (Liu et al., 2017), which might partly account for the improved blood glucose parameters after RYR preparations treatment.
Blood lipid profiles play a critical role in arteriosclerotic CVD. A cross−sectional study in T2 diabetes found that a lower TG was associated with a reduced CVD risk in the short term (Ren et al., 2018); Mortality and morbidity from CVD were reduced via primary and secondary prevention through lipid−lowering therapy targeting LDL−C (Collins et al., 2016, Serban et al., 2016); HDL has antidiabetic functions by increasing insulin sensitivity and β−cell function (Cochran et al., 2021). As the results of the present study, the reductions of TC, TG, LDL−C and the increase of HDL−C are likely to be clinically significant in improving glucose and lipid metabolism and then reducing CAD risk. Previous studies indicated that RYR could lower lipid by inhibiting HMG−CoA reductase (Banach et al., 2018), which might partly account for the improved blood lipid profiles after RYR preparations treatment.
High blood pressure can result in heart failure, heart attack, stroke, and kidney disease (Desai, 2020), and MAP is a predictor of all−cause and CVD mortality in the middle−aged and elderly populations (Sun et al., 2020). In the present study, RYR preparations significantly reduced MAP level of 3.79 mmHg, it also significantly reduced SBP and DBP level in 60−70 years old patients and in the intervention duration of ≤3 months. In addition, previous studies indicated that RYR could improve artery stiffness, endothelial dysfunction and inflammation by promoting and stabilizing the expression of endothelial nitric oxide synthase (eNOS) (Hu et al., 2020; Cicero et al., 2021). Therefore, the mechanism of RYR on lowering blood pressure might be due to improving endothelial dysfunction and inflammation.
Consistency and Disagreement With Other Studies
Up to now, used as assistance for CVD prevention, nutraceuticals has mainly been focusing on lipid-lowering, as referred in the documents produced by the International Lipid Expert Panel (ILEP). As lipid-lowering nutraceuticals, RYR plays an important role in the reduction of inflammation-related residual CVD risk (Ruscica et al., 2021). Recent studies suggested that RYR could be used in patients at cardiovascular risk who had not reached the LDL-C target, but not eligible for statins or unable to tolerate statins (Banach et al., 2019). RYR has been validated to decrease blood sugar, lower cholesterol, control high blood pressure, and inhibit inflammation (Patel, 2016). Therefore, these findings indicated that RYR could treat MetS and improve the prognosis of CVD, which is consistent with our findings. Recent reports identified a low prevalence of suspected adverse effects associated with RYR (Banach et al., 2021), confirmed its safety in hypercholesterolemic patients, even in patients with statin intolerance (Fogacci et al., 2019; Cicero et al., 2021), and our findings also supported the safety of RYR.
Previous study indicated that the lipid−lowering effect of RYR was not influenced by age or gender in physicians (Verhoeven et al., 2013). However, in the subgroup analysis of the present study, RYR preparations significantly reduced the levels of FPG, TC and TG in 40−50 years old patients, SBP and DBP in 60−70 years old patients, and TG in women with more notable effects and low to medium heterogeneity, which suggested that RYR preparations might have better therapeutic advantages in these populations. The different results on age and gender might be related to the basal metabolic rate, vascular dysfunction, and sex differences in TG metabolism: previous studies indicated that basal metabolic rate was significantly higher in middle age (40−50 years old) compared with old age (60−70 years old) (St−Onge and Gallagher, 2010); blood pressure has an increasingly positive association with vascular dysfunction and vascular stiffness as age increases (Wen et al., 2015); women have better clearance of meal−related TG and estrogen is acting directly in the liver to reduce TG level (Palmisano et al., 2018). Therefore, RYR preparations might have better effects on blood glucose and blood lipid in middle−aged people by regulating basal metabolic rate, have better effect on SBP and DBP in old−aged people by improving vascular dysfunction and artery stiffness, and have better effect on TG in women by virtue of better TG clearance. Previous clinical trials showed that MAP, SBP, or DBP were not significantly different between Xuezhikang and placebo at 6, 12, 24, and 48 months (Li et al., 2010). While the present study found that RYR preparations could reduce MAP level, it also reduced SBP and DBP levels in the intervention duration of ≤3 months, which indicated that short duration of RYR preparations intervention might be beneficial to reducing blood pressure. Previous studies indicated that nutraceuticals (berberine, RYR, policosanol) significantly reduced the levels of TC, LDL and HOMA−IR after a 12-months treatment (Marazzi et al., 2011). Nevertheless, in the subgroup analysis of the present study, RYR preparations had a small but significant improvement on TC, TG, LDL and HDL in the intervention duration of >12 months with low heterogeneity, which provided more evidence on long−term use of RYR preparations on reducing blood lipid. Previous systematic review showed that RYR plus conventional therapy lowered the levels of TC, LDL, and SBP compared with conventional therapy, and the levels of TC and LDL compared with placebo plus conventional therapy, while RYR plus statins lowered the levels of TC, TG, LDL, SBP, and DBP compared with statins (Xiong et al., 2017). However, the I 2 ranged from 47 to 98%, suggesting the medium to high heterogeneity among the included studies. In the present study, RYR preparations reduced the levels of SBP and DBP, while increased HDL level compared with lipid−lowing drugs (I 2 ranged from 0 to −95%); RYR preparations plus conventional therapy reduced the levels of FPG, HbA1c, TC, TG and LDL, while increased HDL level compared with conventional therapy (I 2 ranged from 58 to −96%); RYR preparations reduced TC and LDL levels compared with placebo (I 2 = 100%), which was partly consistent with the previous study. Additionally, the present study further indicated that RYR preparations showed positive effect on DBP with low heterogeneity (I2 = 0%), and it also beneficially regulate FPG, HbA1c and HDL levels, which have not been reported in the systematic review of Xiong et al., 2017.
Strengths and Limitations
There have been many previous meta-analyses and reviews about RYR preparations, while these analyses mainly focused on lipid profiles and safety (Dujovne, 2017; Banach et al., 2019). The present meta-analysis mainly focused on the efficacy and safety of RYR preparations on MetS, showed the association between biochemical parameters and clinical benefits, all of which might provide the evidence base for clinical practice. Moreover, the results showed promising effects of RYR preparations on improving glucose and lipid metabolism, modifying cardiovascular risk, effectively reducing the occurrence of mortality and MACEs, which have not been evaluated in the previous meta−analysis. Furthermore, the results demonstrated that RYR preparations were well tolerated with a favourable safety profile.
There are some limitations of our study. First, most of the studies included were of low and moderate methodological quality, which might increase the risk of bias, and therefore, only low- and medium-level evidence can be established. Second, most of the included studies focused on the Chinese population, except for one study conducted in Italy, thus, it is not clear whether the effect of RYR preparations could be extended to other populations. Third, although some of the outcomes in subgroup analysis showed more notable effects and low heterogeneity, sample sizes of these studies were small, thus the efficacy needs further investigation. Finally, regarding the high heterogeneity, different patient ages and sexes, different intervention durations and intervention types were taken into account; however, although subgroup analysis and meta−regression analyses were conducted, the heterogeneities were not eliminated for HbA1c, HOMA−IR, ISI and MAP, and differences remained among the studies in terms of the limited number of studies, sample sizes, race, religious beliefs, and concern regarding the disease; thus, these results should be interpreted with caution. Therefore, more large−sample and high−quality RCTs in broader populations are needed to provide additional data support for the efficacy of RYR on MetS.
Conclusion
The evidence of the current review suggests that RYR preparations significantly reduce the occurrence of mortality and MACEs in MetS and improve blood glucose, lipid profiles, and blood pressure. Taken over the long term, RYR preparations could improve clinical endpoints, prevent metabolic diseases, and reduce the risk of CAD. However, due to the low− and moderate−quality evidence of the included studies and the heterogeneity among the different studies, the results of our study should be evaluated with prudence, and more high−quality clinical studies are required to provide stronger evidence for RYR in the treatment of MetS. These findings suggest that RYR preparations should be taken into consideration for the prevention and treatment of MetS due to its favourable effects on multiple risk factors for hyperglycaemia, dyslipidaemia, and hypertension and its acceptable safety profile.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author Contributions
RY and YY contributed equally to this work. RY and WC contributed to the concept and design of the systematic review. RY and YY performed the literature search, data collection, and data analysis. RY, YY, LW, QX, YW, WS, and YM performed data interpretation. RY, YY, LW contributed to the manuscript preparation. SL, WC, and KC critically revised the systematic review. All authors contributed to the article and approved the submitted version.
Funding
This work was partially supported by the CACMS Innovation Fund (CI 2021A00914), the Opening Project of the Key Laboratory of Integrative Chinese and Western Medicine for the Diagnosis and Treatment of Circulatory Diseases of Zhejiang Province (2C32001), the National Natural Science Foundation of China (82004193) and the Fundamental Research Funds for the Central public welfare research institutes (ZZ14−YQ−007).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.744928/full#supplementary-material
References
- Banach M., Bruckert E., Descamps O. S., Ellegård L., Ezhov M., Föger B., et al. (2019). The Role of Red Yeast rice (RYR) Supplementation in Plasma Cholesterol Control: A Review and Expert Opinion. Atheroscler. Suppl. 39, e1–e8. 10.1016/j.atherosclerosissup.2019.08.023 [DOI] [PubMed] [Google Scholar]
- Banach M., Katsiki N., Latkovskis G., Rizzo M., Pella D., Penson P. E., et al. (2021). Postmarketing Nutrivigilance Safety Profile: a Line of Dietary Food Supplements Containing Red Yeast rice for Dyslipidemia. Arch. Med. Sci. 17 (4), 856–863. 10.5114/aoms/133716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Banach M., Patti A. M., Giglio R. V., Cicero A. F. G., Atanasov A. G., Bajraktari G., et al. (2018). The Role of Nutraceuticals in Statin Intolerant Patients. J. Am. Coll. Cardiol. 72 (1), 96–118. 10.1016/j.jacc.2018.04.040 [DOI] [PubMed] [Google Scholar]
- Cashin A. G., Mcauley J. H. (2020). Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 66 (1), 59. 10.1016/j.jphys.2019.08.005 [DOI] [PubMed] [Google Scholar]
- Chang Y. H., Wang M., Li S. J., Yang Q. Z., Zhang Y. M., Zhao H. L. (1998). Clinical Observation of Lipid−Lowering Effect of Lovastatin on Essential Hypertension with Hyperlipidemia. Chin. J. Intern. Med. 37 (4), 277–280. 10.3760/j.issn:0578-1426.1998.04.025 [DOI] [Google Scholar]
- Chen C. C., Liu I. M. (2006). Release of Acetylcholine by Hon−Chi to Raise Insulin Secretion in Wistar Rats. Neurosci. Lett. 404 (1−2), 117–121. 10.1016/j.neulet.2006.05.024 [DOI] [PubMed] [Google Scholar]
- Chen G. J. (2013). Clinical Observation of Xuezhikang and Simvastatin in the Treatment of Type 2 Diabetes Mellitus with Hyperlipidemia. Chin. J. Mod. Drug Appl. 7 (19), 142–144. 10.3969/j.issn.1673-9523.2013.19.118 [DOI] [Google Scholar]
- Cicero A. F. G., Fogacci F., Zambon A. (2021). Red Yeast Rice for Hypercholesterolemia: JACC Focus Seminar. J. Am. Coll. Cardiol. 77 (5), 620–628. 10.1016/j.jacc.2020.11.056 [DOI] [PubMed] [Google Scholar]
- Cochran B. J., Ong K.−L., Manandhar B., Rye K.−A. (2021). High Density Lipoproteins and Diabetes. Cells 10 (4), 850. 10.3390/cells10040850 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins R., Reith C., Emberson J., Armitage J., Baigent C., Blackwell L., et al. (2016). Interpretation of the Evidence for the Efficacy and Safety of Statin Therapy. Lancet 388 (10059), 2532–2561. 10.1016/S0140-6736(16)31357-5 [DOI] [PubMed] [Google Scholar]
- de Jong M., Woodward M., Peters S. A. E. (2020). Diabetes, Glycated Hemoglobin, and the Risk of Myocardial Infarction in Women and Men: A Prospective Cohort Study of the UK Biobank. Diabetes Care 43 (9), 2050–2059. 10.2337/dc19-2363 [DOI] [PubMed] [Google Scholar]
- Deng Y. X., Zhang J., Dong Y. G., Duan Q. L. (2003). Therapeutic Effect of Xuezhikang on 56 Cases of Type 2 Diabetes Mellitus. Mod. J Integr Tradit Chin West. Med 12 (13), 1376–1377. 10.3969/j.issn.1008-8849.2003.13.016 [DOI] [Google Scholar]
- Desai A. N. (2020). High Blood Pressure. JAMA 324 (12), 1254–1255. 10.1001/jama.2020.11289 [DOI] [PubMed] [Google Scholar]
- Dujovne C. A. (2017). Red Yeast Rice Preparations: Are They Suitable Substitutions for Statins. Am. J. Med. 130 (10), 1148–1150. 10.1016/j.amjmed.2017.05.013 [DOI] [PubMed] [Google Scholar]
- Fogacci F., Banach M., Mikhailidis D. P., Bruckert E., Toth P. P., Watts G. F., et al. (2019). Safety of Red Yeast rice Supplementation: A Systematic Review and Meta−Analysis of Randomized Controlled Trials. Pharmacol. Res. 143, 1–16. 10.1016/j.phrs.2019.02.028 [DOI] [PubMed] [Google Scholar]
- Gentile S., Turco S., Guarino G., Sasso C. F., Amodio M., Magliano P., et al. (2000). Comparative Efficacy Study of Atorvastatin vs Simvastatin, Pravastatin, Lovastatin and Placebo in Type 2 Diabetic Patients with Hypercholesterolaemia. Diabetes Obes. Metab. 2 (6), 355–362. 10.1046/j.1463-1326.2000.00106.x [DOI] [PubMed] [Google Scholar]
- Halbert S. C., French B., Gordon R. Y., Farrar J. T., Schmitz K., Morris P. B., et al. (2010). Tolerability of Red Yeast rice (2,400 Mg Twice Daily) versus Pravastatin (20 Mg Twice Daily) in Patients with Previous Statin Intolerance. Am. J. Cardiol. 105 (2), 198–204. 10.1016/j.amjcard.2009.08.672 [DOI] [PubMed] [Google Scholar]
- He L., Zhan J. F. (2009). The Early Intervention and Clinic Effect of Xuezhikang on Diabetic Nephropathy Patients. J. Kunming Med. Univ. 30 (12), 78–82. 10.3969/j.issn.1003-4706.2009.12.021 [DOI] [Google Scholar]
- Higgins J., Thomas J., Chandler J., Cumpston M., Li T., Page M., et al. (Editors) (2019). Cochrane Handbook for Systematic Reviews of Interventions Version 6. Cochrane part 4 section 23-3-4. Available at: www.training.cochrane.org/handbook/archive/v6 . [Google Scholar]
- Hirode G., Wong R. J. (2020). Trends in the Prevalence of Metabolic Syndrome in the United States, 2011−2016. JAMA 323 (24), 2526–2528. 10.1001/jama.2020.4501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu J., Wang J., Gan Q. X., Ran Q., Lou G. H., Xiong H. J., et al. (2020). Impact of Red Yeast Rice on Metabolic Diseases: A Review of Possible Mechanisms of Action. J. Agric. Food Chem. 68 (39), 10441–10455. 10.1021/acs.jafc.0c01893 [DOI] [PubMed] [Google Scholar]
- Hunter P. M., Hegele R. A. (2017). Functional Foods and Dietary Supplements for the Management of Dyslipidaemia. Nat. Rev. Endocrinol. 13 (5), 278–288. 10.1038/nrendo.2016.210 [DOI] [PubMed] [Google Scholar]
- Jin J., Zhang W. W., He Y, J., Peng Z., Yu M. (2007). 60 Cases Clinical Observation of Xuezhikang on Diabetic Nephropathy with Abnormal Blood Lipid. Zhejiang Med. J. 29 (9), 973–974. 10.3969/j.issn.1006-2785.2007.09.034 [DOI] [Google Scholar]
- Kaneko H., Itoh H., Kiriyama H., Kamon T., Fujiu K., Morita K., et al. (2021). Fasting Plasma Glucose and Subsequent Cardiovascular Disease Among Young Adults: Analysis of a Nationwide Epidemiological Database. Atherosclerosis 319, 35–41. 10.1016/j.atherosclerosis.2020.12.024 [DOI] [PubMed] [Google Scholar]
- Ke M. J. (2015). A Clinical Observation of the Efficacy of Xuezhikang in the Treatment of Type 2 Diabetes with Dyslipidemia. China Med. Pharm. 5 (21), 98–100. 10.34038/jpp.2019.01.003 [DOI] [Google Scholar]
- Klingelhöfer I., Morlock G. E. (2019). Lovastatin in Lactone and Hydroxy Acid Forms and Citrinin in Red Yeast rice Powders Analyzed by HPTLC−UV/FLD. Anal. Bioanal. Chem. 411 (25), 6655–6665. 10.1007/s00216-019-02039-y [DOI] [PubMed] [Google Scholar]
- Li C. Y., Chen Z. S., Hu J. W., Yu J., Luo Y. (2017). The Intervention Effect of Daixiefang on the Patients of Metabolic Syndrome with Dyslipidemia, Insulin Resistance. J. Tianjin Univ. Tradit Chin. Med. 36 (4), 258–262. 10.11656/j.issn.1673-9043.2017.04.06 [DOI] [Google Scholar]
- Li H., Zheng Q. G., Lv S. G. (2005). Observation of Therapeutic Effect of Xuezhikang on Hyperlipidemia of Type 2 Diabetes Mellitus with Microalbuminuria. Fujian Med. J. 27 (5), 60–61. 10.3969/j.issn.1001-7585.2003.08.077 [DOI] [Google Scholar]
- Li J. J., Lu Z. L., Kou W. R., Chen Z., Wu Y. F., Yu X. H., et al. (2009). Beneficial Impact of Xuezhikang on Cardiovascular Events and Mortality in Elderly Hypertensive Patients with Previous Myocardial Infarction from the China Coronary Secondary Prevention Study (CCSPS). J. Clin. Pharmacol. 49 (8), 947–956. 10.1177/0091270009337509 [DOI] [PubMed] [Google Scholar]
- Li J. J., Lu Z. L., Kou W. R., Chen Z., Wu Y. F., Yu X. H., et al. (2010). Long−term Effects of Xuezhikang on Blood Pressure in Hypertensive Patients with Previous Myocardial Infarction: Data from the Chinese Coronary Secondary Prevention Study (CCSPS). Clin. Exp. Hypertens. 32 (8), 491–498. 10.3109/10641961003686427 [DOI] [PubMed] [Google Scholar]
- Li J. J., Lu Z. L., Kou W. R., Chen Z., Wu Y. F., Yu X. H., et al. (2010a). Impact of Xuezhikang on Coronary Events in Hypertensive Patients with Previous Myocardial Infarction from the China Coronary Secondary Prevention Study (CCSPS). Ann. Med. 42 (3), 231–240. 10.3109/07853891003652534 [DOI] [PubMed] [Google Scholar]
- Li J. J., Lu Z. L., Kou W. R., Wu Z. Y. F., Yu X. H., Zhao Y. C. (2010b). Impact of Xuezhikang on Coronary Events in Hypertensive Patients with Previous Myocardial Infarction from the China Coronary Secondary Prevention Study (CCSPS). Ann. Med. 42 (3), 231–240. 10.3109/07853891003652534 [DOI] [PubMed] [Google Scholar]
- Liu J. T., Chen H. Y., Chen W. C., Man K. M., Chen Y. H. (2017). Red Yeast Rice Protects Circulating Bone Marrow−Derived Proangiogenic Cells against High−Glucose−Induced Senescence and Oxidative Stress: The Role of Heme Oxygenase−1. Oxid. Med. Cel. Longev. 2017, 3831750. 10.1155/2017/3831750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loubser L., Weider K. I., Drake S. M. (2019). Acute Liver Injury Induced by Red Yeast rice Supplement. BMJ Case Rep. 12 (3), e227961. 10.1136/bcr-2018-227961 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu M. C., Fang W. C., Li W. C., Yeh W. C., Shieh Y. H., Chen J. Y. (2020). The Association between Insulin Resistance and Cardiovascular Disease Risk: A Community−Based Cross−Sectional Study Among Taiwanese People Aged over 50 Years. Int. J. Environ. Res. Public Health 17 (19), 7195. 10.3390/ijerph17197195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma X, L., Qian Z. (2011). Clinical Observation on the Effect of Xuezhikang and Simvastatin on Dyslipidemia in Type 2 Diabetes Mellitus. J. Qiqihaer Univ. Med. 32 (18), 2979–2980. 10.3969/j.issn.1002-1256.2011.18.045 [DOI] [Google Scholar]
- Marazzi G., Cacciotti L., Pelliccia F., Iaia L., Volterrani M., Caminiti G., et al. (2011). Long−term Effects of Nutraceuticals (Berberine, Red Yeast rice, Policosanol) in Elderly Hypercholesterolemic Patients. Adv. Ther. 28 (12), 1105–1113. 10.1007/s12325-011-0082-5 [DOI] [PubMed] [Google Scholar]
- Moseley A. M., Elkins M. R., Van der Wees P. J., Pinheiro M. B. (2020). Using Research to Guide Practice: The Physiotherapy Evidence Database (PEDro). Braz. J. Phys. Ther. 24 (5), 384–391. 10.1016/j.bjpt.2019.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmisano B. T., Zhu L., Eckel R. H., Stafford J. M. (2018). Sex Differences in Lipid and Lipoprotein Metabolism. Mol. Metab. 15, 45–55. 10.1016/j.molmet.2018.05.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel S. (2016). Functional Food Red Yeast rice (RYR) for Metabolic Syndrome Amelioration: a Review on Pros and Cons. World J. Microbiol. Biotechnol. 32 (5), 87. 10.1007/s11274-016-2035-2 [DOI] [PubMed] [Google Scholar]
- Peng W. H., Qu Q., Chen J. (2000). The Effects of Xuezhikang on Microalbuminuria in Non−dependent Diabetes Mellitus with hyperlipidemiaCNKI:SUN:FZZY. J. Fuzhou Gen. Hosp. 7 (4), 17–19. 10.1177/000456329303000504 [DOI] [Google Scholar]
- Prasun P. (2020). Mitochondrial Dysfunction in Metabolic Syndrome. Biochim. Biophys. Acta Mol. Basis Dis. 1866 (10), 165838. 10.1016/j.bbadis.2020.165838 [DOI] [PubMed] [Google Scholar]
- Ren Y., Ren Q., Lu J., Guo X., Huo X., Ji L., et al. (2018). Low Triglyceride as a Marker for Increased Risk of Cardiovascular Diseases in Patients with Long−Term Type 2 Diabetes: A Cross−Sectional Survey in China. Diabetes Metab. Res. Rev. 34 (2), e2960. 10.1002/dmrr.2960 [DOI] [PubMed] [Google Scholar]
- Ruscica M., Penson P. E., Ferri N., Sirtori C. R., Pirro M., Mancini G. B. J., et al. (2021−). Impact of Nutraceuticals on Markers of Systemic Inflammation: Potential Relevance to Cardiovascular Diseases − A Position Paper from the International Lipid Expert Panel (ILEP). Prog. Cardiovasc. Dis. 67, 40–52. 10.1016/j.pcad.2021.06.010 [DOI] [PubMed] [Google Scholar]
- Shen H. X. (2011). Clinical Observation of Xuezhikang in Treating Diabetic Patients with Dyslipidemia. Contemp. Med. 17 (6), 66–67. 10.3969/j.issn.1009-4393.2011.6.048 [DOI] [Google Scholar]
- St−Onge M. P., Gallagher D. (2010). Body Composition Changes with Aging: the Cause or the Result of Alterations in Metabolic Rate and Macronutrient Oxidation. Nutrition 26 (2), 152–155. 10.1016/j.nut.2009.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sui L. (2003). Clinical Effect of Xuezhikang on Type 2 Diabetes Mellitus Complicated with Hyperlipidemia. Liaoning Pharm. Clin. 6 (2), 73–74. 10.3969/j.issn.1673-0070.2003.02.009 [DOI] [Google Scholar]
- Sun S., Lo K., Liu L., Huang J., Feng Y. Q., Zhou Y. L., et al. (2020). Association of Mean Arterial Pressure with All−Cause and Cardiovascular Mortality in Young Adults. Postgrad. Med. J. 96 (1138), 455–460. 10.1136/postgradmedj-2019-137354 [DOI] [PubMed] [Google Scholar]
- Sungthong B., Yoothaekool C., Promphamorn S., Phimarn W. (2020). Efficacy of Red Yeast rice Extract on Myocardial Infarction Patients with Borderline Hypercholesterolemia: A Meta−Analysis of Randomized Controlled Trials. Sci. Rep. 10 (1), 2769. 10.1038/s41598-020-59796-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verhoeven V., Lopez Hartmann M., Remmen R., Wens J., Apers S., Van Royen P. (2013). Red Yeast rice Lowers Cholesterol in Physicians − a Double Blind, Placebo Controlled Randomized Trial. BMC Complement. Altern. Med. 13, 178. 10.1186/1472-6882-13-178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang G. H., Luo Y., Ren H, Q. (2005). Clinical Observation of Xuezhikang in the Treatment of Type 2 Diabetes Mellitus Complicated with Hyperlipidemia. Chin. Hosp. Pharm. J. 25 (12), 1160–1161. 10.3321/j.issn:1001-5213.2005.12.030 [DOI] [Google Scholar]
- Wang X. J., Wang J. (2016). Comparative Study for Clinical Effect in Treating Elderly Lacunar Infarction Patients Complicated with Hyperlipidaemia and Prehypertension between Xuezhikang Capsule and Atorvastatin Calcium Tablets. Pract. J. Card. Cereb. Pneu Vasc. Dis. 24 (6), 67–71. 10.3969/j.issn.1008-5971.2016.06.017 [DOI] [Google Scholar]
- Wang Y. F., Yang C. K., Xu W. J., Sun L., Liu B., Wang G. G. (1997). Regulation of Xuezhikang and Jiferozil on Hyperlipidemia and Insulin Sensitivity in Senile Patients. Chin. Med. News 12 (19), 22–23. [Google Scholar]
- Wang Y. X., Liu X, W. (2013). Clinical Effect Analysis of Xuezhikang in the Treatment of Type 2 Diabetes Mellitus with Dyslipidemia. Med. J. Chin. Peopl Health 25 (18), 2–3. 10.3969/j.issn.1672-0369.2013.18.016 [DOI] [Google Scholar]
- Wu W. X., Wei R, Q. (2011). Clinical Observation of Xuezhikang and Atorvastatin on Hypertensive Patients with Dyslipidemia. J. Youjiang Med. Univ. Natl. 33 (6), 760–762. 10.3969/j.issn.1001-5817.2011.06.0091 [DOI] [Google Scholar]
- Xiao J. (2019). Comparison of Clinical Efficacy of Xuezhikang Capsule and Atorvastatin Calcium Tablets in the Treatment of Senile Lacunar Cerebral Infarction with Hyperlipidemia and Prehypertension. Yao Pin Ping Jia 16 (10), 41–43. 10.3969/j.issn.1672-2809.2019.10.013 [DOI] [Google Scholar]
- Xiong X., Wang P., Li X., Zhang Y., Li S. (2017). The Effects of Red Yeast rice Dietary Supplement on Blood Pressure, Lipid Profile, and C−Reactive Protein in Hypertension: A Systematic Review. Crit. Rev. Food Sci. Nutr. 57 (9), 1831–1851. 10.1080/10408398.2015.1018987 [DOI] [PubMed] [Google Scholar]
- Yao Z., Yu F. H., Ding X. P. (2004). Clinical Observation of Jiangzhi Decoction on Type 2 Diabetes Mellitus with Hyperlipemia. Shanghai J. Tradit Chin. Med. 38 (11), 11–12. 10.16305/j.1007-1334.2004.11.005 [DOI] [Google Scholar]
- Zeng X. Y., Pan J., Zhao Z. G. (2001). Endothelial protection of Xuezhikang in Type 2 Diabetes Mellitus Complicated with Hyperlipemia. J. Third Mil. Med. 23 (6), 726–728. 10.3321/j.issn:1000-5404.2001.06.034 [DOI] [Google Scholar]
- Zhai W. J., Li A. Q. (2010). Effect of Xuezhikang on the Serum High − Sensitivity C − Reactive Protein and Blood Lipid in Patients with Type 2 Diabetes Mellitus and Hyperlipidemia. Xuzhou Acta Academ Med. 30 (2), 102–103. 10.3969/j.issn.1000-2065.2010.02.012 [DOI] [Google Scholar]
- Zhang L. L. (2009). Observation of Therapeutic Effect of Xuezhikang on Type 2 Diabetes Mellitus with Dyslipidemia. J. China Tradit Chin. Med. Inform. 1 (3), 10–11. [Google Scholar]
- Zhang X. L. (2019). Study on Combination of Two Drugs in Treating Diabetes Mellitus with Hyperlipidemia. China Contin. Med. Educ. 11 (25), 138–140. 10.3969/j.issn.1674-9308.2019.25.056 [DOI] [Google Scholar]
- Zhang Z. H., Wu Ping. S. (2014). Effect of Xuezhikang on Metabolic Syndrome in the Elderly. Chin. J. Gerontol. 34 (13), 3597–3599. 10.3969/j.issn.1005-9202.2014.13.040 [DOI] [Google Scholar]
- Zhao J. X. (2015). Clinical Observation of Xuezhikang on Type 2 Diabetes with Dyslipidemia. Continuing Med Educ 29 (1), 115–116. 10.3969/j.issn.1004-6763.2015.01.075 [DOI] [Google Scholar]
- Zhao S. P., Lu Z. L., Du B. M., Chen Z., Wu Y. F., Yu X. H., et al. (2007). Xuezhikang, an Extract of Cholestin, Reduces Cardiovascular Events in Type 2 Diabetes Patients with Coronary Heart Disease: Subgroup Analysis of Patients with Type 2 Diabetes from China Coronary Secondary Prevention Study (CCSPS). J. Cardiovasc. Pharmacol. 49 (2), 81–84. 10.1097/FJC.0b013e31802d3a58 [DOI] [PubMed] [Google Scholar]
- Zhu B., Qi F., Wu J., Yin G., Hua J., Zhang Q., et al. (2019). Red Yeast Rice: A Systematic Review of the Traditional Uses, Chemistry, Pharmacology, and Quality Control of an Important Chinese Folk Medicine. Front. Pharmacol. 10, 1449. 10.3389/fphar.2019.01449 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu C. C., Yao Z. L. (2005). The Clinical Research of XuezhiKang in Treatment of the Geriatric Patients Who Had Hyperlipidemia and Type 2 Diabetes Mellitus. Chin. J. Pract. Chin. Mod. Med. 18 (15), 521–522. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.