

Abstract
China is in a critical air quality management stage. Rapid industrial development and urbanization has resulted in non‐ignorable air pollution, which seriously endangers human health. Assessment of the health impacts and economic losses of air pollution is essential for the prevention and control policy formulation. Based on ozone (O3) and fine particulate matter concentration (PM2.5) monitoring data in 331 Chinese cities from 2015 to 2020, this study evaluated the health effects and the corresponding economic losses of O3 and PM2.5 pollution on three health endpoints. The ratio of population exposed to O3 levels that exceeded the Chinese Ambient Air Quality Standards (CAAQS) increased from 13.35% in 2015 to 14.15% in 2020, which resulted in 133,415 (2015) ‐ 156,173 (2020) all‐cause deaths, 88,941 (2015) ‐ 104,051 (2020) cardiovascular deaths, and 28,614 (2015) ‐ 33,456 (2020) respiratory deaths. The ratio of population exposed to PM2.5 levels that exceeded the CAAQS decreased, but in many regions, especially in North China and the Yangtze River Delta, the PM2.5 concentration remained high. By 2020, nearly half of the population in China was still exposed to PM2.5 levels that exceeded the CAAQS, and the corresponding economic losses reached CNY 3.46 and 3.05 billion, respectively. These results improved the understanding of the spatial‐temporal variation trends of major air pollutants at city scale in China, and emphasize the continued coordination urgently needed for controlling O3 and PM2.5 following the implementation of the 2013 policy to mitigate air pollution to protect human health.
Keywords: air pollution, spatial‐temporal variation trends, population exposure, health risk, economic loss
Key Points
PM2.5 showed a significant decrease but still severe impacts on human health
Ozone (O3) is posing an increasingly serious threat to human health and economic loss in China
Coordinated control of PM2.5 and O3 is essential
1. Introduction
In recent years, air pollution problems have become increasingly severe worldwide, have a negative influence on human health, the climate, and economic development (Fang et al., 2013; Lelieveld et al., 2015; Shang et al., 2013). Among atmospheric pollutants, the most commonly reported include particulate matter with an aerodynamic diameter smaller than 2.5 microns (PM2.5) and 10 microns (PM10), nitric dioxide, sulfur dioxide, and ozone (O3; Shen et al., 2020). Notably, both long‐ and short‐term atmospheric pollutants are related to acute and chronic impacts on human health (Jerrett et al., 2009; Philip et al., 2014; Shang et al., 2013).
In recent decades, rapid urbanization has been closely related to air pollution and human health worldwide (Ferreri et al., 2018; Guan et al., 2019; Lim et al., 2012; Wang et al., 2018). In China, rapid development of cities has created various environmental pollution problems (Huang et al., 2014; Zhang et al., 2020), which pose a notable threat to human health and cause substantial economic losses. The Chinese government has implemented a range of measures to improve air quality, such as the 2012 National Ambient Air Quality Standard and the 2013 Air Pollution Prevention and Control Action Plan (APPCAP). These efforts have realized great achievements, particularly in the remarkable reduction in PM2.5 pollution in many cities in China, as reported in several previous studies (Gui et al., 2019; Zhao et al., 2021). However, O3 concentration exhibits an overall increasing trend, contrary to PM2.5 concentration. Zhao et al. (2021) demonstrated that the maximum daily 8‐hr average O3 concentration (MDA8 O3) increased 3.4 μg m−3 per year from 2015 to 2018 in China. Maji and Sarkar (2020) reported that, in the summertime, the mean MDA8 O3 value increased from 91.6 to 103.1 μg/m3 from 2015 to 2018 in China. Notably, studies have revealed that PM2.5 reduction promotes O3 enhancement (Li et al., 2019; Sicard et al., 2020).
O3 poses increasingly adverse effects on human health and can cause systemic oxidative stress and harm to the cardiovascular and respiratory systems (Gabehart et al., 2015; McDonnell et al., 1997; Salonen et al., 2018). Zhang et al. (2019) indicated that O3 pollution can also cause a variety of diseases and social phenomena, including asthma emergencies, hospitalization, and absenteeism from school. Previous studies have provided valuable insights into O3 risk assessment for protecting human health. On both regional and global scales, atmospheric chemistry models and remote sensing data have been adopted to estimate the potential health risks of O3 exposure. Based on an atmospheric chemistry‐general circulation model and satellite data, the global premature and cardiovascular mortality and lung cancer attributable to O3 and PM2.5 pollution in 2005 were estimated to reach approximately 773 thousand/year, 186 thousand/year, and 2000 thousand/year, respectively (Lelieveld et al., 2013). Anenberg et al. (2010) used a global atmospheric chemical transport model to calculate the global mortality associated with O3 in 2000, and found that the annual respiratory mortality attributable to O3 was estimated to be 0.7 ± 0.3 million. In addition to negative effects on human health, O3‐related economic losses are greatly increasing. Several previous studies have estimated these losses. Feng et al. (2019) found that the costs of morbidity regarding respiratory diseases and nonaccidental mortality reached US$ 690.9 billion and US$ 7.5 billion, respectively. Previously, Maji et al. (2019) calculated that the national economic loss in 2016 due to exposure to O3 was approximately US$ 7.6 billion.
Moreover, although the concentration of PM2.5 has declined in recent years, its impact on people's health and economic losses remains notable. Therefore, PM2.5 pollution and related issues still receive global attention. The mortality, cardiovascular and respiratory mortality related to PM2.5 in 2013 were estimated to be 763,595, 149,754, and 446,035, respectively, according to measured data (Song et al., 2016). Based on satellite data, Liu et al. (2017) examined the national deaths from stroke, lung cancer, and ischemic heart disease caused by PM2.5 pollution, and the number increased from approximately 800 thousand in 2004 to over 1,200 thousand in 2012. With a global atmospheric chemical transport model, Anenberg et al. (2010) found that the annual global mortality due to PM2.5 in 2000 was estimated to reach 3.5 ± 0.9 million cardiopulmonary deaths and 220 ± 80 thousand lung cancer deaths. Song et al. (2017) suggested that in 2015, PM2.5 accounted for more than 40.3% of the total stroke deaths and 33.1%, 26.8%, and 15.5% of all acute respiratory system, ischemic heart disease, and all‐cause deaths, respectively. With the use of monitoring data, the mortality related to PM2.5 in China in 2016 was calculated to reach 964 thousand deaths, which accounted for 9.98% of the total deaths. Specifically, the morbidity of respiratory and cardiovascular diseases was 605 thousand and 364 thousand, respectively (Maji et al., 2018). More importantly, the PM2.5‐related economic losses remain very high, as X. Lu et al. (2017) revealed that the highest economic loss caused by PM2.5 pollution in southern China occurred in 2012, at US$ 4.6 billion, which is approximately 6.1% of the local total gross domestic product. Xie et al. (2017) predicted that China will suffer economic losses of US$ 4.2 billion and equivalent life losses of US$ 285 billion due to PM2.5 pollution in 2030 without a control policy.
Since 2013, the air conditions in China have shown a combined pollution characterized by high concentrations of PM2.5 and O3, it is a top issue to understand their adverse effects on human health in the atmospheric environment field. Due to a lack of data, many previous studies were mostly conducted based on atmospheric chemistry models or satellite products (Anenberg et al., 2010; Lelieveld et al., 2013; Lin et al., 2018; Xie et al., 2016; Zhao et al., 2017). In recent years, with the establishment of air quality monitoring sites, it becomes possible to quantify the health risks of PM2.5 and O3 based on monitoring data. However, it must be point out that, although some studies have used monitoring data to investigate the link between PM2.5 and O3 and their associated diseases, most of these studies have focused on either a region (e.g., Beijing‐Tianjin‐Hebei, Yangtze River Delta (YRD)) or a single pollutant (e.g., PM2.5 or O3; Maji & Namdeo, 2021; Maji et al., 2018; Song et al., 2016). Moreover, a recent study revealed that the decline in PM2.5 in recent years has enhanced surface photochemical reactions, thereby exacerbated O3 pollution (Li et al., 2019). Notably, it remains unclear whether the reduction in health risk due to decreased PM2.5 is offset by the increase in health risk due to increased O3 concentrations. Therefore, it is valuable to analyze the human health effects of PM2.5 and O3 simultaneously.
The objectives of this study are to (a) identify the long‐term spatiotemporal variation trends and heterogeneity in O3 and PM2.5 pollution of 331 cities in China from 2015 to 2020 based on monitoring data, (b) quantify the impacts of O3 and PM2.5 pollution on human health, and (c) estimate the economic losses related to O3 and PM2.5 pollution in China.
2. Data and Methods
2.1. Data
There are notable climatic variations in the eastern, western, southern, and northern areas of China due to geographical effects. Given these differences, six representative regions were divided, as follows: (a) North China (Beijing, Tianjin, Hebei, Shanxi, Henan, and Shandong); (b) Northeast China (Heilongjiang, Jilin, and Liaoning); Northwest China (Inner Mongolia, Ningxia, Gansu, Shaanxi, and Xinjiang); Southeast China (Jiangsu, Anhui, Shanghai, Hubei, Hunan, Jiangxi, Guangdong, Fujian, Zhejiang, and Hainan); Southwest China (Guangxi, Chongqing, Sichuan, Yunnan and Guizhou); and the Tibetan Plateau (Qinghai and Tibet; Figure 1).
Figure 1.
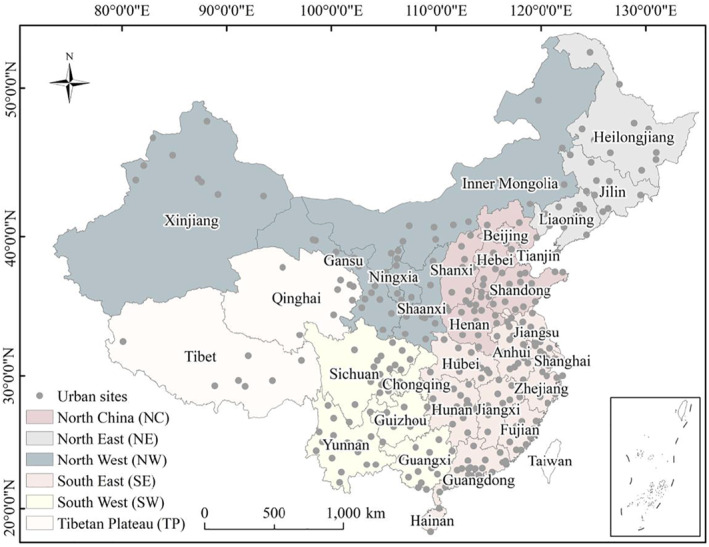
Geographic distribution of the 331 cities in China.
Monitoring data on the MDA8 O3 and PM2.5 from 1 January 2015, to 31 December 2020, that pertain to 367 cities were collected from the China National Environmental Monitoring Centre, 2020 (https://quotsoft.net/air/; Figure 1). Due to the acute lack of data in certain cities, 331 cities eventually participated in the following calculations. Moreover, considering the missing values and outliers in the data, a rigorous quality control of the data was performed using the method proposed by Barrero et al. (2015) to ensure the reliability of the study results. The annual mean values per city were calculated by averaging the daily data retrieved from all stations in this city.
Population data (>30 years for O3, all age groups for PM2.5) from the 6th Population Census in 2010 in each city were obtained from China’s economic and social big data research platform, 2020 https://data.cnki.net/yearbook/Single/N2021050059. In recent decades, the population of China has grown slowly. Therefore, in this study, no further adjustments were applied to the obtained population data.
2.2. The Univariate Linear Regression Model
The slope calculated by the univariate linear regression model in this study was used to explore and test the long‐term interannual variation rate of PM2.5 and O3 pollution. That indicates, how many units of PM2.5 and O3 are increasing or decreasing per year overall. The spatial patterns of the temporal variation trends (slope values) of the O3 and PM2.5 concentration were calculated for each city in China from 2015 to 2020 (Figure 2). The slope in the unitary linear regression model represents the annual rate of change, which has been analyzed by several previous studies (Hammer et al., 2020; Lu et al., 2020; Zhang et al., 2020). When the absolute value of the slope is larger, the increasing (positive slope values)/decreasing temporal trend (negative slope values) is stronger, which is a common method and the corresponding equation can be found in D. Lu et al. (2017).
Figure 2.
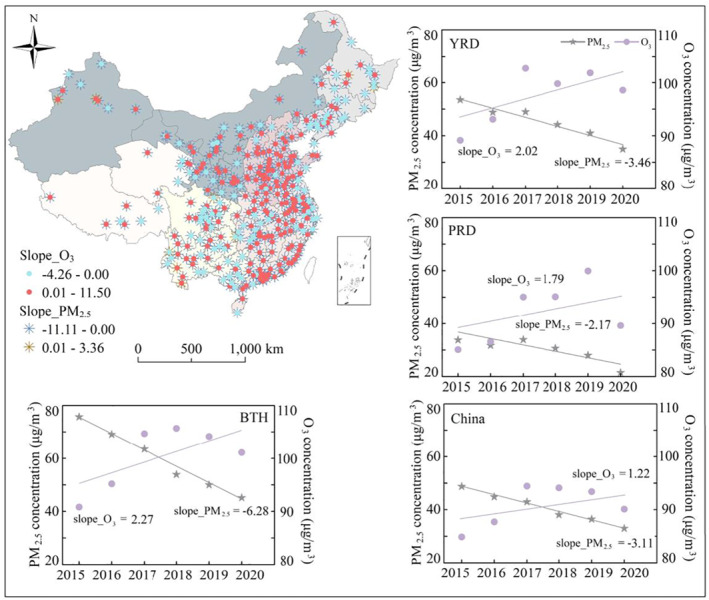
Spatiotemporal variation trends of the annual mean MDA8 O3 and PM2.5 concentrations from 2015 to 2020 in China. BTH represents Beijing‐Tianjin‐Hebei region, YRD represents Yangtze River Delta, PRD represents Pearl River Delta.
2.3. Health Impacts
Log‐linear (LL) exposure‐response functions were used in this study, which were drawn from Hubbell et al. (2009). If the level of air pollutants exceeds the safe threshold, then the exposure‐response coefficient can be used to calculate the change in health risk for one person with every 1 μg m−3 increase in concentration (Liao et al., 2017). Furthermore, if the population of each city is known, then we can estimate the health effects.
In this study, the LL method was adopted to evaluate the health impacts of O3 and PM2.5 pollution regarding three health endpoints, as:
| (1) |
| (2) |
where β is the exposure‐response coefficient indicating that, based on an increase of 1 μg m−3 per pollutant, the percentage increase in the health impact (Liao et al., 2017) is derived from the relative risks. In this study, exposure‐response coefficient (β) related O3 pollution was estimated from the long‐term epidemiological study by Turner et al. (2016) and cardiovascular and respiratory mortality from Lim et al. (2019), also a long‐term study (Table 1). Meanwhile, β related long‐term PM2.5 pollution was estimated from the previous studies (Aunan and Pan., 2004; Burnett et al., 2014; Kan and Chen., 2002; Xie et al., 2009, 2010) (Table 1). C is the annual average pollutant concentration, and C 0 represents the minimum risk exposure level, which is set to 26.7 ppb for O3 (Turner et al., 2016) and 10 μg/m3 for PM2.5 (WHO, 2006). The number of cases (E) that consider three endpoints related to O3 and PM2.5 is evaluated by using Equation 2. P is the exposed population, and f p is the baseline mortality rate, which was obtained from the China Health Statistical Yearbook (https://data.cnki.net/yearbook).
Table 1.
The Long‐Term Exposure‐Response Coefficient (β), RR, and Baseline Mortality for PM2.5 and Ozone (10 μg/m3)
| Parameter | All‐cause | Cardiovascular | Respiratory |
|---|---|---|---|
| β (PM2.5) | 0.00336 (0.00076, 0.00504) | 0.00068 (0.00043, 0.00093) | 0.00109 (0, 0.00221) |
| (Sources) | 1, 2, 3, 4, 5 | 1, 4, 5 | 1, 4, 5 |
| RR (PM2.5) | 1.0342 (1.0076, 1.0517) | 1.0068 (1.0043, 1.0093) | 1.0110 (1.0000, 1.0223) |
| (Sources) | 1, 2, 3, 4, 5 | 1, 5, 6 | 1, 5, 6 |
| C 0 | 10 μg/m3 | 10 μg/m3 | 10 μg/m3 |
| f p (PM2.5) | 0.00614 | 0.00546 | 0.01022 |
| β (O3) (Sources) | 0.00198 (0.001, 0.00392) | 0.00296 (0.001, 0.00583) | 0.00392 (0, 0.00862) |
| Turner et al., 2016 | Lim et al., 2019 | Lim et al., 2019 | |
| RR (O3) | 1.0200 (1.0100, 1.0400) | 1.0300 (1.0100–1.0600) | 1.0400 (1.0000–1.0900) |
| Turner et al., 2016 | Lim et al., 2019 | Lim et al., 2019 | |
| C 0 | 26.7 ppb | 26.7 ppb | 26.7 ppb |
| f p (O3) | 0.00654 | 0.00296 | 0.00072 |
2.4. Economic Impacts
The cost of illness (COI) model is applied to monetize the economic cost of each health endpoint, thereby estimating the socioeconomic loss caused by air pollution (Maji et al., 2018; Zhang et al., 2017).
The economic losses caused by O3 and PM2.5 pollution in this study are calculated with the COI method, which mainly refers to the additional health expenditures of residents attributed to air pollution, such as hospitalization and outpatient expenses. Based on the per capita medical expenses (MEs) in the China Health Statistics Yearbook (2015–2020), the economic loss in each city from 2015 to 2020 is estimated, as follows:
| (3) |
where i denotes the health endpoint, and RP i denotes the per capita MEs for the category i health endpoint, which was collected from the China Health Statistics Yearbook 2015–2020. The RP values for cardiovascular disease in 2015, 2016, 2017, 2018, 2019, and 2020 were CNY 23,997.56, 23,784.00, 24,949.80, 23,607.90, 27,579.12, and 27,579.12, respectively, and the RP values for respiratory disease were CNY 7,604.90, 7,663.60, 7,905.30, 7,975.60, 8,150.00, and 8,150.00, respectively.
3. Results
3.1. Annual Variations in the O3 and PM2.5
The slope values of the annual PM2.5 concentration for 2015–2020 shows higher values in the more industrial and populated areas, such as NC and the YRD (Figure 2). PM2.5 experienced a continuous and significant decrease across China, and decreased from 48.7 μg/m3 in 2015 to 33.0 μg/m3 in 2020 at a rate of 3.11 μg/m3 from 2015 to 2020. The BTH, YRD and PRD regions showed a decreased trend in the annual PM2.5 concentrations, which decreased at rates of 6.28, 3.46, and 2.17, respectively (Figure 2).
The spatial distribution of O3 concentration in China is similar to that of PM2.5. However, different from PM2.5, O3 concentration shows a sustained increase at an average annual rate of 1.22 μg/m3 from 84.9 μg/m3 in 2015 to 90.1 μg/m3 in 2020, which indicates that humans suffer from more severe health risks associated with O3 exposure. The increase was greater in BTH, YRD, and PRD regions (2.27 μg/m3, 2.02 μg/m3 and 1.79 μg/m3, respectively), than the national average of 1.22 μg/m3 (Figure 2).
3.2. Population Exposure to O3 and PM2.5
PM2.5 is decreasing and O3 is increasing, which means China is currently experiencing complex and severe PM2.5 and O3 pollution. In this study, according to the annual average O3 and PM2.5 concentration and the population data of 331 cities in China and the above six representative regions, the cumulative population exposure level to O3 and PM2.5 is calculated (Figures 3 and 4).
Figure 3.
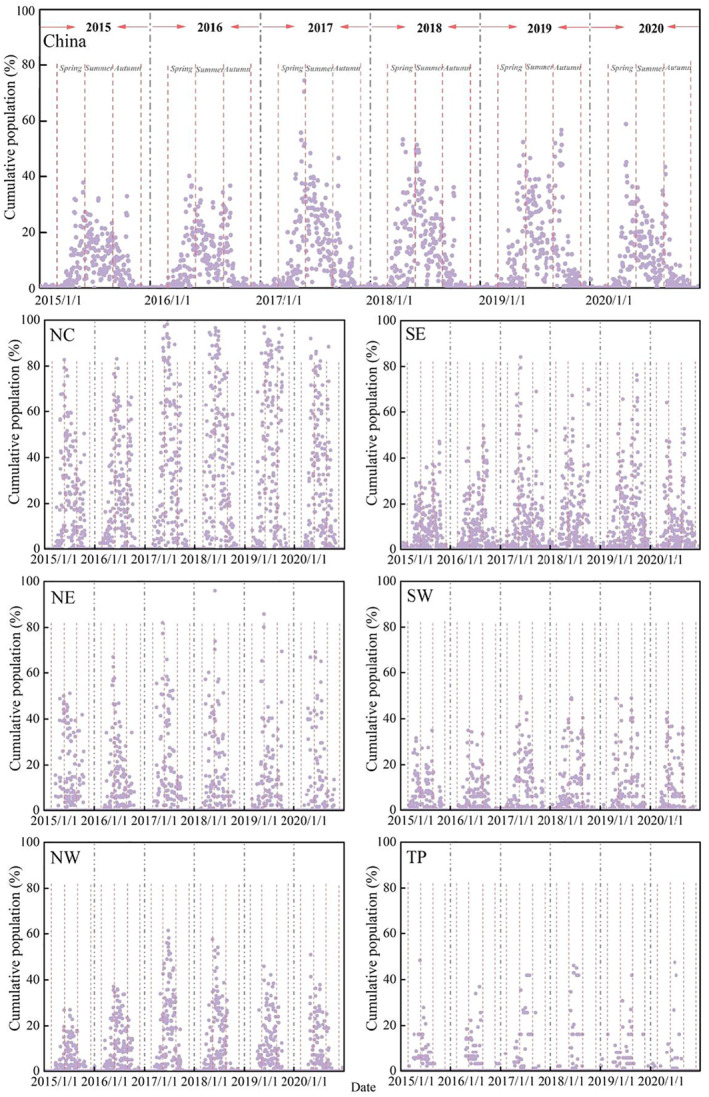
Population exposure to O3 in China and six representative regions.
Figure 4.
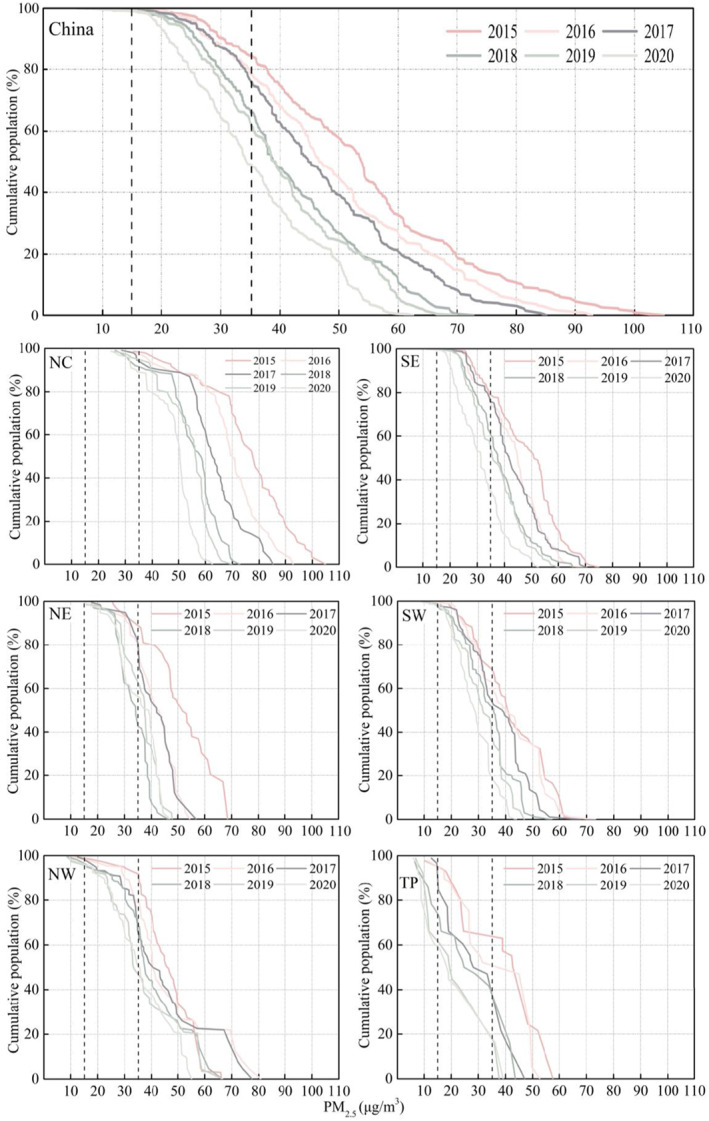
Population exposure to PM2.5 in six representative regions and China.
For O3, it is reported that at Level II of the CAAQS, the limits of MDA8 O3 and the daily maximum 1 hr O3 concentration are 160 μg/m3 (used in the study) and 200 μg/m3, respectively. In general, NC was the most severe region, followed by SE (including the YRD region), while the number of people exposed to excessive O3 concentration in the TP was low (Figure 3). The proportion of people exposed to O3 above the CAAQS in summer is higher than that in spring and autumn. In the summers of 2015, 2016, 2017, 2018, 2019 and 2020, 175.51 million (13.35%), 193.13 million (14.69%), 273.20 million (20.78%), 291.34 million (22.16%), 286.35 million (21.78%), and 186.03 million (14.15%) people in China were exposed to O3 pollution that exceeded the CAAQS. All of these results indicate that in recent years, especially in the summer, the risk of O3 exposure is high; therefore, it is necessary to analyze its impact on health.
For PM2.5, the cumulative population exposed to PM2.5 above the CAAQS (15 and 35 μg/m3) decreases along with the decrease in PM2.5 from 2015 to 2020 (Figure 4). In 2015, 2016, 2017, 2018, 2019 and 2020, the number of people in China living with PM2.5 levels higher than 35 μg/m3 was 1,111.39 million, 1,034.52 million, 1,008.96 million, 880.27 million, 837.23 million, and 647.71 million, respectively, which accounted for approximately 84.53%, 78.69%, 76.74%, 66.95%, 63.68%, and 49.27%, respectively, of the total population. Notably, overall, NC was the most severely affected region, where approximately 90% of people lived in areas where concentrations of PM2.5 greater than 35 μg/m3. However, notably, in 2020, nearly 50% of the population still experienced air problems. Therefore, although PM2.5 has exhibited a downward trend in recent years, there remains a need to further reduce PM2.5 pollution.
3.3. Health Impacts of O3 and PM2.5
In this study, the spatiotemporal distributions of three health endpoints mortality in adults (>30 years) attributed to O3 and PM2.5 exposure in 331 cities across China from 2015 to 2020 are shown in Figures S1‐S4 in Supporting Information S1. For O3, in China, the all‐cause mortality was 133,415 [95% confidence interval (CI): 67,927–259,873] in 2015 and 156,173 (95% CI: 79, 562–303,843) in 2020 at a threshold of 26.7 ppb (Table 2). In 2015, the estimated cardiovascular mortality was 88,941 (95% CI: 30,585–171,304), while respiratory mortality was 28,614 (95% CI: 0–60,511). These numbers increased to 104,051 (95% CI: 35,824–200,055) and 33,456 (95% CI: 0–70,548) in 2020. Cardiovascular and respiratory mortality accounted for 55.7% and 21.4% of all‐cause mortality, respectively. From 2015 to 2020, all‐cause, cardiovascular, and respiratory deaths attributable to O3 exposure increased by 17.1%, 17.0%, and 16.9%, respectively (Figures S1 and S2 in Supporting Information S1). The cities with the highest six‐year average all‐cause mortality due to O3 were Shanghai [4,101 (95% CI: 2,093–7,446)], Beijing [3,432 (95% CI: 1,750–6,668)], Linyi (Shandong) [1,887 (95% CI: 964–3,650)], Chengdu (Sichuan) [1,874 (95% CI: 954–3,648)], Chongqing [1,826 (95% CI: 926–3,587)] and Baoding (Hebei) [1,774 (95% CI:906–3,436)] (Figure S1 in Supporting Information S1). The provinces with high health impacts from 2015 to 2020 at the three health endpoints were Shandong, Jiangsu, Henan, Guangdong, and Hebei, and these results suggest that the relevant authorities should focus on O3 pollution control in these regions (Table 2). Overall, the health impacts‐related O3 exposure are strongly correlated with the level of O3 pollution and the size of the exposed population, such that several provinces, such as Shandong, Henan, Hebei, and Jiangsu, which have high O3 levels, experience high numbers of premature deaths due to their large population. Guangdong has relatively low levels of O3 pollution; however, it has the highest population in China, which caused the health effects attributed to long‐term O3 exposure to be higher than in other provinces (Figure S2 in Supporting Information S1).
Table 2.
The Estimated Three Premature Deaths Related to Long‐Term Exposure to O3 in China and Provinces With High Premature Deaths From 2015 to 2020
| Region | Year | All‐cause | Cardiovascular | Respiratory |
|---|---|---|---|---|
| China | 2015 | 133,415 (67,927–259,873) | 88,941 (30,585–171,304) | 28,614 (0–60,511) |
| 2016 | 145,188 (73,933–282,711) | 96,773 (33,290–186,295) | 31,116 (0–65,774) | |
| 2017 | 175,735 (89,315–340,091) | 116,570 (40,215–223,500) | 37,445 (0–78,603) | |
| 2018 | 172,845 (88,132–335,707) | 115,060 (39,683–220,670) | 36,964 (0–77,633) | |
| 2019 | 171,249 (87,316–332,630) | 114,002 (39,315–218,661) | 36,625 (0–76,934) | |
| 2020 | 156,173 (79,562–303,843) | 104,051 (35,824–200,055) | 33,456 (0–70,548) | |
| Shandong | 2015 | 14,887 (7,598–28,859) | 9,901 (3,421–18,934) | 3,178 (0–6,643) |
| 2016 | 15,308 (7,814–29,663) | 10,178 (3,519–19,455) | 3,266 (0–6,822) | |
| 2017 | 17,964 (9,184–34,707) | 11,927 (4,135–22,697) | 3,821 (0–7,926) | |
| 2018 | 17,072 (8,732–32,955) | 11,329 (3,932–21,533) | 3,629 (0–7,510) | |
| 2019 | 18,533 (9,479–35,776) | 12,299 (4,268–23,376) | 3,939 (0–8,153) | |
| 2020 | 17,460 (8,924–33,754) | 11,596 (4,018–22,087) | 3,717 (0–7,720) | |
| Jiangsu | 2015 | 11,358 (5,797–22,017) | 7,553 (2,610–14,445) | 2,424 (0–5,068) |
| 2016 | 11,053 (5,639–21,442) | 7,353 (2,539–14,078) | 2,361 (0–4,944) | |
| 2017 | 12,324 (6,297–23,838) | 8,187 (2,835–15,607) | 2,625 (0–5,459) | |
| 2018 | 11,146 (5,688–21,613) | 7,414 (2,561–14,184) | 2,380 (0–4,978) | |
| 2019 | 12,085 (6,172–23,403) | 8,033 (2,779–15,338) | 2,577 (0–5,373) | |
| 2020 | 11,347 (5,791–22,004) | 7,548 (2,607–14,441) | 2,423 (0–5,069) | |
| Henan | 2015 | 10,502 (5,348–20,451) | 7,000 (2,408–13,477) | 2,252 (0–4,758) |
| 2016 | 13,259 (6,763–25,737) | 8,824 (3,045–16,907) | 2,834 (0–5,942) | |
| 2017 | 15,674 (8,009–30,319) | 10,413 (3,606–19,849) | 3,338 (0–6,943) | |
| 2018 | 16,093 (8,226–31,109) | 10,687 (3,704–20,354) | 3,425 (0–7,113) | |
| 2019 | 15,976 (8,165–30,889) | 10,611 (3,676–20,214) | 3,401 (0–7,066) | |
| 2020 | 14,185 (7,240–27,498) | 9,434 (3,260–18,041) | 3,028 (0–6,330) | |
| Guangdong | 2015 | 9,561 (4,865–18,647) | 6,378 (2,190–12,307) | 2,053 (0–4,355) |
| 2016 | 8,957 (4,553–17,498) | 5,980 (2,050–11,568) | 1,927 (0–4,103) | |
| 2017 | 11,709 (5,963–22,792) | 7,803 (2,685–15,015) | 2,510 (0–5,298) | |
| 2018 | 11,888 (6,056–23,132) | 7,921 (2,727–15,232) | 2,547 (0–5,372) | |
| 2019 | 12,852 (6,552–24,971) | 8,557 (2,950–16,420) | 2,749 (0–5,779) | |
| 2020 | 10,276 (5,229–20,037) | 6,854 (2,355–13,220) | 2,206 (0–4,676) | |
| Hebei | 2015 | 8,164 (4,157–15,897) | 5,442 (1,872–10,475) | 1,750 (0–3,698) |
| 2016 | 9,074 (4,623–17,655) | 6,046 (2,082–11,624) | 1,944 (0–4,099) | |
| 2017 | 12,015 (6,137–23,258) | 7,985 (2,763–15,237) | 2,561 (0–5,335) | |
| 2018 | 12,544 (6,411–24,253) | 8,331 (2,887–15,872) | 2,670 (0–5,549) | |
| 2019 | 11,718 (5,984–22,693) | 7,789 (2,694–14,874) | 2,499 (0–5,211) | |
| 2020 | 10,813 (5,517–20,978) | 7,194 (2,484–13,774) | 2,310 (0–4,837) |
It is estimated that approximately 920 million people (70% of the total population) are living in areas with a six‐year average PM2.5 greater than 35 μg/m3. The cause‐specific premature deaths and differences between 2016 and 2020 and 2015 due to long‐term PM2.5 exposure in each city were therefore examined (Figures S3 and S4 in Supporting Information S1). Table 3 reports the details on three health endpoints in China and the five provinces with high premature deaths from 2015 to 2020. In China, all‐cause deaths decreased by 39.4%, from 1,105,089 (95% CI: 267,049–1,590,192) in 2015 to 669,555 (95% CI: 157,576–979,324) in 2020, and the highest value was found in 2015 (Figure S4 in Supporting Information S1). During the study period, cardiovascular and respiratory mortality decreased by 41.0%, from 212,917 (95% CI: 135,515–289,319) in 2015 to 125,529 (95% CI: 79,686–171,020) in 2020, and by 40.8%, from 632,101 (95% CI: 0–1,245,414) in 2015 to 374,265 (95% CI: 0–745,934) in 2020. From the provincial perspective, the number of all‐cause premature deaths during the study period was higher in Henan (11.0%) [2015: 121,506; 2020: 76,673], Shandong (9.9%) [2015: 116,004; 2020: 69,265], and Hebei (8.4%) [2015: 94,543; 2020: 53,726] (Table 3). A larger decreasing trend in premature deaths was identified for the provinces of Zhejiang (55.9%), Hubei (46.4%), Guangdong (46.8%), Guizhou (44.9%), Hebei (43.2%), Shandong, Jiangsu, Fujian, Guangxi, and Yunnan (40.0%–45.0%). In 2015, five cities had the highest all‐cause mortality, that is, Beijing [28,997 (95% CI: 7,154–41,180)], Chongqing [25,607 (95% CI: 6,130–37,050)], Shanghai [19,385 (95% CI: 4,638–28,056)], Baoding [18,770 (95% CI (4,784–26,135)], and Tianjin [14,475 (95% CI: 3,533–20,691)]. By 2020, the all‐cause mortality in Chongqing [14,212 (95% CI: 3,315–20,904)], Beijing [12,730 (95% CI: 2,985–18,658)], Shanghai [9,784 (95% CI: 2,275–14,419)], and Tianjin [9,710 (95% CI: 2,308–14,110)] remained the highest.
Table 3.
The Estimated Three Premature Deaths Related to Long‐Term Exposure to PM2.5 in China and Provinces With High Premature Deaths From 2015 to 2020
| Region | Time | All‐cause | Cardiovascular | Respiratory |
|---|---|---|---|---|
| China | 2015 | 1,105,089 (267,049–1,590,192) | 212,917 (135,515–289,319) | 632,101 (0–1,245,414) |
| 2016 | 999,538 (239,961–1,444,093) | 191,280 (121,664–260,087) | 568,472 (0–1,123,254) | |
| 2017 | 939,871 (224,650–1,361,527) | 179,050 (113,835–243,563) | 532,504 (0–1,054,194) | |
| 2018 | 810,276 (192,155–1,179,521) | 153,112 (97,269–208,443) | 455,945 (0–905,723) | |
| 2019 | 774,314 (183,241–1,128,637) | 146,001 (92,731–198,802) | 434,914 (0–864,733) | |
| 2020 | 669,555 (157,576–979,324) | 125,529 (79,686–171,020) | 374,265 (0–745,934) | |
| Shandong | 2015 | 116,004 (28,681–164,567) | 22,884 (14,598–31,026) | 67,687 (0–132,047) |
| 2016 | 100,613 (24,551–143,880) | 19,580 (12,474–26,581) | 58,039 (0–113,876) | |
| 2017 | 85,792 (20,692–123,568) | 16,496 (10,497–22,420) | 48,991 (0–96,610) | |
| 2018 | 72,971 (17,419–105,774) | 13,883 (8,825–18,887) | 41,297 (0–81,804) | |
| 2019 | 78,912 (18,894–114,169) | 15,059 (9,576–20,482) | 44,776 (0–88,580) | |
| 2020 | 69,265 (16,479–100,614) | 13,132 (8,345–17,872) | 39,085 (0–77,535) | |
| Jiangsu | 2015 | 71,576 (17,216–164,567) | 13,724 (8,730–31,026) | 40,776 (0–132,047) |
| 2016 | 60,361 (14,379–143,880) | 11,459 (7,283–26,581) | 34,100 (0–113,876) | |
| 2017 | 57,377 (13,658–123,568) | 10,884 (6,917–22,420) | 32,392 (0–96,610) | |
| 2018 | 55,884 (13,278–105,774) | 10,580 (6,723–18,887) | 31,498 (0–81,804) | |
| 2019 | 51,300 (12,127–114,169) | 9,662 (6,136–20,482) | 28,788 (0–88,580) | |
| 2020 | 42,424 (9,956–100,614) | 7,931 (5,033–17,872) | 23,656 (0–77,535) | |
| Henan | 2015 | 121,506 (30,059–172,276) | 23,984 (15,300–32,516) | 70,936 (0–138,352) |
| 2016 | 108,689 (26,618–155,063) | 21,231 (13,531–28,813) | 62,899 (0–123,216) | |
| 2017 | 98,023 (23,805–140,574) | 18,982 (12,087–25,782) | 56,311 (0–110,717) | |
| 2018 | 92,623 (22,385–133,223) | 17,847 (11,359–24,252) | 52,986 (0–104,398) | |
| 2019 | 87,560 (21,084–126,227) | 16,808 (10,694–22,848) | 49,931 (0–98,534) | |
| 2020 | 76,673 (18,314–111,091) | 14,596 (9,279–19,857) | 43,417 (0–85,979) | |
| Guangdong | 2015 | 48,942 (11,423–71,954) | 9,097 (5,770–12,404) | 27,160 (0–54,327) |
| 2016 | 44,751 (10,420–65,894) | 8,298 (5,262–11,317) | 24,783 (0–49,624) | |
| 2017 | 46,860 (10,923–68,949) | 8,699 (5,517–11,863) | 25,977 (0–51,989) | |
| 2018 | 41,678 (9,685–61,445) | 7,713 (4,890–10,521) | 23,042 (0–46,176) | |
| 2019 | 36,898 (8,544–54,518) | 6,803 (4,312–9,283) | 20,337 (0–40,817) | |
| 2020 | 26,056 (5,993–38,666) | 4,771 (3,022–6,515) | 14,277 (0–28,738) | |
| Hebei | 2015 | 94,543 (11,423–133,319) | 18,841 (5,770–25,520) | 55,641 (0–108,080) |
| 2016 | 86,279 (10,420–122,381) | 17,023 (5,262–23,079) | 50,351 (0–98,219) | |
| 2017 | 80,695 (10,923–114,925) | 15,812 (5,517–21,452) | 46,820 (0–91,597) | |
| 2018 | 67,270 (9,685–96,720) | 12,972 (4,890–17,626) | 38,508 (0–75,846) | |
| 2019 | 61,021 (8,544–88,082) | 11,691 (4,312–15,895) | 34,739 (0–68,610) | |
| 2020 | 53,726 (5,993–77,933) | 10,209 (3,022–13,891) | 30,376 (0–60,199) |
3.4. Economic Loss Attributable to O3 and PM2.5 Pollution
For the convenience of calculation, we assume that the population incurs no per capita MEs related to premature deaths. This study estimates only the economic losses associated with cardiovascular and respiratory diseases caused by O3 and PM2.5. Figure S5 in Supporting Information S1 shows city‐specific economic loss associated with cardiovascular and respiratory diseases attributable to O3 and PM2.5 pollution in China by using the COI method with different C 0 values (for O3: 26.7 ppb; for PM2.5: 10 μg/m3). Economic losses attributable to the O3 increased from 2015 to 2020 and reached a maximum at different times in different cities. There was an increasing trend of economic losses from cardiovascular and respiratory mortality, which increased from 2.13 billion CNY (95% CI: 0.73–4.11 billion) in 2015 to 2.87 billion CNY (95% CI:0.99–5.52 billion) in 2020 and from 0.22 billion CNY (95% CI: 0–0.46 billion) in 2015 to 0.27 billion CNY (95% CI: 0–0.57 billion) in 2020 (Table 4 and Figure S5 in Supporting Information S1). In 2020, the cities with the highest economic losses from cardiovascular diseases due to long‐term O3 exposure were Shanghai [66.52 (95% CI: 22.93–127.64) million], Beijing [57.52 (95% CI: 19.80–110.63) billion], Tianjin [37.19 (95% CI: 12.83–71.27) million], Linyi (Shandong) [36.49 (95% CI: 12.66–69.42) million], and Chengdu (Sichuan) [30.63 (95% CI: 10.52–59.14) million]. In contrast, Nujiang (Yunnan) [161,471 (95% CI: 54,751–317,418)] and Linzhi (Tibet) [205,143 (95% CI: 70,068–398,992)] had the lowest economic losses, which were approximately 0.28% and 0.36% of those in Beijing, respectively. Economic losses in 2020 due to cardiovascular mortality accounted for approximately 91.3% of the total economic losses attributable to O3 exposure, which is much higher than those due to respiratory mortality.
Table 4.
The Economic Loss Related to Long‐Term Exposure to O3 and PM2.5 in China and Provinces With High Premature Deaths From 2015 to 2020
| Pollutants | Time | Cardiovascular (billion) | Respiratory (billion) |
|---|---|---|---|
| O3 | 2015 | 2.13 (0.73–4.11) | 0.22 (0–0.46) |
| 2016 | 2.30 (0.79–4.43) | 0.24 (0–0.50) | |
| 2017 | 2.91 (1.00–5.58) | 0.30 (0–0.62) | |
| 2018 | 2.72 (0.94–5.21) | 0.29 (0–0.62) | |
| 2019 | 3.14 (1.08–6.03) | 0.30 (0–0.63) | |
| 2020 | 2.87 (0.99–5.52) | 0.27 (0–0.57) | |
| PM2.5 | 2015 | 5.11 (3.25–6.94) | 4.81 (0–9.47) |
| 2016 | 4.55 (2.89–6.18) | 4.35 (0–8.61) | |
| 2017 | 4.47 (2.84–6.07) | 4.21 (0–8.33) | |
| 2018 | 3.61 (2.30–4.92) | 3.64 (0–7.22) | |
| 2019 | 4.03 (2.56–5.48) | 3.54 (0–7.05) | |
| 2020 | 3.46 (2.20–4.71) | 3.05 (0–6.08) |
The economic losses of cardiovascular and respiratory mortality related to long‐term PM2.5 exposure decreased from 5.11 billion CNY (95% CI: 3.25–6.94) in 2015 to 3.46 billion (95% CI: 2.20–4.71) in 2020 and from 4.81 billion CNY (95% CI: 0–9.47) in 2015 to 3.05 billion CNY (95% CI: 0–6.08) in 2020 (Table 4 and Figure S5 in Supporting Information S1). In 2015, the cities with the highest economic loss of cardiovascular diseases‐‐ related to long‐term PM2.5 exposure were Beijing [136.96 (95% CI: 87.34–185.74) million], Chongqing [117.24 (95% CI: 74.55–159.47) million], Shanghai [88.71 (95% CI: 56.41–120.67) million], Baoding (Hebei) [91.68 (95% CI (58.66–123.93) million], and Tianjin [67.63 (95% CI: 43.08–91.80) million]. By 2020, the economic losses in Chongqing [72.80 (95% CI: 46.17–99.28) million], Beijing [65.58 (95% CI: 41.62–89.38) million], Shanghai [49.96 (95% CI: 31.68–68.14) million], and Tianjin [50.73 (95% CI: 32.24–69.05) million] remained the highest. From the provincial perspective, economic losses during the study period were higher in Henan (11.62%) [2015: 1.12; 2020: 0.76 billion], Shandong (10.45% of total economic loss in 2020) [2015: 1.06; 2020: 0.68 billion], and Hebei (8.13%) [2015: 0.88; 2020: 0.53 billion] (Figure S6 in Supporting Information S1).
4. Discussion
This study assessed the health impacts and economic loss‐related long‐term exposure to MDA8 O3 and PM2.5 in China during the study period of 2015–2020. This study showed that the O3 concentration and the deaths of three health endpoints and economic loss cause by long‐term O3 exposure increased significantly in China, which is similar to the results of other studies (Lu et al., 2020; Maji & Namdeo, 2021). At the same time, the PM2.5 concentration and corresponding premature mortality decreased significantly in most cities; however, they still exceed the CAAQS in many regions. China is facing new challenges from the complex and increasing mix of O3 and PM2.5 pollution.
Some prior studies examined the health effects attributed to O3 exposure from a national perspective predominantly based on atmospheric chemistry models or satellite data (Lelieveld et al., 2013; Lin et al., 2018). Because the accuracy of health impact assessments attributable to O3 can be greatly influenced by the O3 data source, the monitoring data can help to obtain a more accurate result. Maji and Namdeo. (2021) reported the impact of long‐term O3 exposure on human health by using a model consistent with this study (LL model) in which data from 2015 to 2019 were examined. Their results showed that in 2019, when 26.7 ppb was used as the threshold (C 0 ) for MDA8 O3, the mortality for the all‐cause, cardiovascular, and respiratory was 181 thousand (95% CI: 91.5–352 thousand), 112 thousand (95% CI: 38.1–214 thousand) and 33.8 (95% CI: 0–71.4 thousand), respectively, which is generally consistent with the results of this study; however, when the (C 0 ) for MDA8 O3 was set to 0 ppb, the mortality was 487 thousand (95% CI: 249–922 thousand), 298 thousand (95% CI: 104–552 thousand), and 89,000 (95% CI: 0–178,000), respectively, which is much larger than the results of this study; these differences suggest that the selection of the O3 threshold results in widely varying estimates of long‐term premature mortality. Recently, Guan et al. (2021) conducted a nationwide study of 338 cities in China which generated much higher estimated health risks from O3 than did our study. The difference between the results of these two studies may be that this study used exposure‐response coefficient (β) from Lim et al. (2019) and Turner et al. (2016), whereas the study by Guan et al. (2021) used β from Jerrett et al. (2009). Notably, the selection of β also has a significant impact on the assessment of health impacts. Malley et al. (2017) used different RR values, from Jerrett et al. (2009) and Turner et al. (2016) to estimate mortality caused by O3 pollution in China, with large differences in the results. The differences among these studies indicate that the health impact assessment‐related O3 is primarily related to the O3 threshold (C 0 ), exposure‐response coefficient (β), and the data source of O3. Additionally, the selection of the O3 indicator has a great impact on the health assessment‐related to O3 exposure (Feng et al., 2019).
Recently, Burnett et al. (2018) and Yin et al. (2020) estimated that there were 1.11 million in 2015 and 850,000 in 2017 deaths from all‐cause deaths due to long‐term PM2.5 exposure, respectively, and our results were slightly lower than that reported in Burnett et al. (2018), but higher than that reported in Yin et al. (2020). Notably, the factors which influenced O3‐related health risk assessment can also affect that of PM2.5. For example, Song et al. (2016) reported that there were 763,595 all‐cause, 149,754 cardiovascular, and 446,035 respiratory deaths caused by PM2.5 pollution in 2013, which were slightly lower than that in this study. One possible reason is that their study region contains only 190 cities, which is far less than this study. Furthermore, there is a significant decrease in PM2.5 concentration in recent years. According to the study of Kuerban et al. (2020), in 2015, PM2.5 pollution caused 436,260, 149,755, and 94,397 deaths from all‐cause, respiratory, and cardiovascular diseases, and the three health endpoints death numbers in 2018 are 344,177, 109,326, and 70,982, respectively using LL model with much lower estimated health risks than our results. The differences may because the selection of the exposed population, this study used the all population as the exposed population, but Kuerban et al. (2020) considered only the population of cities with monitoring stations, which resulted in a lower value. Based on LL model, Maji et al. (2018) showed that the total all‐cause deaths attributed to PM2.5 in China was 1.258 (95% CI: 1.053, 1.420) million in 2016, which were slightly higher than our results. The reason for the difference may lie in the different selection of coefficients: this study used β and f p from the previous studies (Aunan and Pan., 2004; Burnett et al., 2014; Kan and Chen., 2002; Xie et al., 2009, 2010), whereas the study by Maji et al. (2018) used β and f p from Li et al. (2013), Qiu et al. (2013) and NBSC. (2016). Although these studies used the same LL model, the number of deaths related to PM2.5 were different, indicating that the PM2.5‐related health impact assessment is also influenced by the exposed population, coefficients (f p and β), and number of cities.
According to previous studies (Burnett et al., 2015; Yin et al., 2017), the estimated RRs with LL and IER models are relatively consistent. Maji et al. (2018) demonstrated that the number of all‐cause deaths attributed to PM2.5 in China was 0.964 (95% CI: 0.447, 1.355) million using IER model (the sum of four type of mortality: cerebrovascular, chronic obstructive pulmonary, ischemic heart disease, and lung cancer), whereas the all‐cause deaths was 1.258 (95% CI: 1.053, 1.420) million based on LL model (the sum of five health endpoints: hospital admission due to cardiovascular disease, hospital admission due to respiratory disease, asthma attack, chronic bronchitis and emergency room visits for respiratory disease). It indicates that the LL model results have a slightly higher value of PM2.5‐related deaths due to the different coefficients and selection of health endpoints. Moreover, IER were employed to estimate limited health endpoints during PM2.5 related exposure‐response assessment (Yin et al., 2017), which is not suitable for our aims to directly obtain the mortality corresponding to the three health endpoints (all‐cause, cardiovascular, and respiratory diseases) caused by PM2.5 and O3 pollution. Furthermore, there are no robust cohort studies to suggest which risk model is more appropriate for China (Maji et al., 2018). A recent cohort study showed that the RR values estimated in areas of high PM2.5 concentration in China were not consistent with those specified in the IER model. The China‐specific cohort studies contribute to narrow the gap in RR values in the high concentration areas, but are not appropriate for IER, suggesting that IER may underestimate the effect of high PM2.5 levels in China (Pope et al., 2018). Therefore, considering reasons mentioned above, this study applied the LL model to estimate the number of deaths from the three health endpoints, which has been widely adopted by many other studies (Kuerban et al., 2020; Maji & Namdeo, 2021; Yin et al., 2017).
We applied the COI method to quantify the medical expenditure of each city by considering each health endpoint attributable to O3 and PM2.5 pollution from 2015 to 2020. High O3‐ and PM2.5 related economic losses were found in Beijing, Tianjin, Hebei, Anhui, Henan, Shandong, Jiangsu, Sichuan, Guangdong and Zhejiang Provinces. Some studies have shown that the adverse health effects of air pollution can cause significant economic losses (Nansai et al., 2020; World Bank, 2016). Maji et al. (2019) used the value of a statistical life (VSL) model to assess the economic loss caused by O3 pollution in 338 cities in China, and the results showed that there was an economic loss of US$7.6 billion in 2016. Wang et al. (2021) estimated the MEs and the VSL caused by the health burden of PM2.5 and O3 in 31 Chinese provinces from 2010 to 2050, and their results indicated that the MEs due to PM2.5 and O3 was approximately US$ 6.3 billion and that the VSL was approximately US$ 112.1 billion in 2010. The results of these two studies are higher than those of this study, and the differences may lie in the selection of the models and the sources of pollutant data, which may lead to dramatic differences in the results. Moreover, Lanzi et al. (2018) predicted that PM2.5 pollution will cause US$ 2.26 trillion economic loss in 2030 without any control. Xie et al. (2017) showed that if there is no control policy, China will suffer US$ 4.2 billion in economic losses and US$ 285 billion in human loss in 2030. Therefore, we should continue to give more attention to air quality improvement, especially coordinated control for O3 and PM2.5 pollution.
Several uncertainties are involved in this study. First, we assumed that the total population of each city is exposed to the same average O3 and PM2.5 concentrations, although the exposure environment of each person varies greatly in space and time (Maji et al., 2018). Second, the air quality monitoring stations are mainly distributed in urban areas, but the population of each city is not located only across these areas, which can introduce some uncertainty. Studies have revealed that the O3 is significantly higher in suburban areas than in urban areas (Sicard et al., 2016). Therefore, in this study, the health effects estimated using the average concentration over all areas in each city may smaller than the actual effects.
5. Conclusions
This study analyzed the temporal and spatial heterogeneity of long‐term O3 and PM2.5 pollution in 331 cities across China from 2015 to 2020. It was found that PM2.5 concentrations continued to decrease in almost all Chinese cities, especially in cities located in NC and the YRD; conversely, O3 showed an overall increasing trend. The population exposed to high PM2.5 decreased from 2015 to 2020, but notably, although there was a substantial reduction in PM2.5 due to the implementation of the APPCAP in recent years, it was still high in many cities. By 2020, approximately half of the population lived in areas where PM2.5 exceeded the CAAQS; therefore, further control of PM2.5 pollution will still be necessary in the future. Meanwhile, the ratio of the population exposed to O3 continued to increase from 13.35% in 2015% to 14.15% in 2020; it peaked at 22.16% in 2018 and caused all‐cause, cardiovascular, and respiratory mortality of 156,173 [95% CI: 79,562–303,843], 104,051 (95% CI: 35,824–200,055), and 33,456 (95% CI: 0–70,548) in 2020, respectively. According to these increases and the results of this study, it is imperative to urgently propose and adopt strict measures to control the continued rise of O3 pollution in the future.
Conflict of Interest
The authors declare no conflicts of interest relevant to this study.
Supporting information
Supporting Information S1
Acknowledgments
This work was supported by the National Key Research and Development Plan of China (2019YFA0606901); the Visiting Fellowship from China Scholarship Council (No. 202106040072); China Postdoctoral Science Foundation (2020M681157).
Zhang, X. , Cheng, C. , & Zhao, H. (2022). A health impact and economic loss assessment of O3 and PM2.5 exposure in China from 2015 to 2020. GeoHealth, 6, e2021GH000531. 10.1029/2021GH000531
Contributor Information
Changxiu Cheng, Email: chengcx@bnu.edu.cn.
Hui Zhao, Email: zhaohui_nuist@163.com.
Data Availability Statement
Data sets for this study are publicly available. Data on ozone concentration are available via the China National Environmental Monitoring Centre (https://quotsoft.net/air/), and Population data (>30 years and all age group) obtained from the 6th Population Census (https://data.cnki.net/yearbook/Single/N2021050059).
References
- Anenberg, S. C. , Horowitz, L. W. , Tong, D. Q. , & West, J. J. (2010). An estimate of the global burden of anthropogenic ozone and fine particulate matter on premature human mortality using atmospheric modeling. Environmental Health Perspectives, 118(9), 1189–1195. 10.1289/ehp.0901220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aunan, K. , & Pan, X. C. (2004). Exposure‐response functions for health effects of ambient air pollution applicable for China e a meta‐analysis. The Science of the Total Environment, 329(1–3), 3–16. 10.1016/j.scitotenv.2004.03.008 [DOI] [PubMed] [Google Scholar]
- Barrero, M. A. , Orza, J. A. G. , Cabello, M. , & Canton, L. (2015). Categorisation of air quality monitoring stations by evaluation of PM10 variability. The Science of the Total Environment, 524–525, 225–236. 10.1016/j.scitotenv.2015.03.138 [DOI] [PubMed] [Google Scholar]
- Burnett, R. , Chen, H. , Szyszkowicz, M. , Fann, N. , Hubbell, B. , Pope, C. A. , et al. (2018). Global estimates of mortality associated with long‐term exposure to outdoor fine particulate matter. Proceedings of the National Academy of Sciences of the United States of America, 115(38), 9592–9597. 10.1073/pnas.1803222115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnett, R. T. , Pope, C. A. , Ezzati, M. , Olives, C. , Lim, S. S. , Mehta, S. , et al. (2014). An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environmental Health Perspectives, 122(4), 397–403. 10.1289/ehp.1307049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnett, R. T. , Pope, C. A., III . Ezzati, M. , Olives, C. , Lim, S. S. , Mehta, S. , et al. (2015). An integrated risk function for estimating the Global Burden of Disease attributable to ambient fine particulate matter exposure. University of British Columbia. [DOI] [PMC free article] [PubMed] [Google Scholar]
- China National Environmental Monitoring Centre . (2020). National Air Quality Forecast Information Dissemination System [Dataset]. Monitoring Data. Retrieved from https://quotsoft.net/air/
- China’s economic and social big data research platform . (2020). The 6th Population Census [Dataset]. Retrieved from https://data.cnki.net/yearbook/Single/N2021050059
- Fang, Y. , Naik, V. , Horowitz, L. W. , & Mauzerall, D. L. (2013). Air pollution and associated human mortality: The role of air pollutant emissions, climate change and methane concentration increases from the preindustrial period to present. Atmospheric Chemistry and Physics, 13(3), 1377–1394. 10.5194/acp-13-1377-2013 [DOI] [Google Scholar]
- Feng, Z. , De Marco, A. , Anav, A. , Gualtieri, M. , Sicard, P. , Tian, H. , et al. (2019). Economic losses due to ozone impacts on human health, forest productivity and crop yield across China. Environmental International, 131, 104966. 10.1016/j.envint.2019.104966 [DOI] [PubMed] [Google Scholar]
- Ferreri, J. M. , Peng, R. D. , Bell, M. L. , Ya, L. , Li, T. , & Anderson, G. B. (2018). The January 2013 Beijing "Airpocalypse" and its acute effects on emergency and outpatient visits at a Beijing hospital. Air Quality Atmosphere & Health, 11(3), 301–309. 10.1007/s11869-017-0538-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabehart, K. , Correll, K. A. , Loader, J. E. , White, C. W. , & Dakhama, A. (2015). The lung response to ozone is determined by age and is partially dependent on toll‐Like receptor 4. Respiratory Research, 16(1), 117. 10.1186/s12931-015-0279-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guan, Y. , Kang, L. , Wang, Y. , Zhang, N. N. , & Ju, M. T. (2019). Health loss attributed to PM2.5 pollution in China’s cities: Economic impact, annual change and reduction potential. Journal of Cleaner Production, 217, 284–294. 10.1016/j.jclepro.2019.01.284 [DOI] [Google Scholar]
- Guan, Y. , Xiao, Y. , Wang, Y. , Zhang, N. , & Chu, C. (2021). Assessing the health impacts attributable to PM2.5 and ozone pollution in 338 Chinese cities from 2015 to 2020. Environmental Pollution, 287, 117623. 10.1016/j.envpol.2021.117623 [DOI] [PubMed] [Google Scholar]
- Gui, K. , Che, H. , Wang, Y. , Wang, H. , Zhang, L. , Zhao, H. , et al. (2019). Satellite‐derived PM2.5 concentration trends over Eastern China from 1998 to 2016: Relationships to emissions and meteorological parameters. Environmental Pollution, 247, 1125–1133. 10.1016/j.envpol.2019.01.056 [DOI] [PubMed] [Google Scholar]
- Hammer, M. S. , Donkerlaar, A. V. , Li, C. , Lyapustin, A. , Sayer, A. M. , Hsu, N. C. , et al. (2020). Global estimates and long‐term trends of fine particulate matter concentrations (1998–2018). Environmental Science & Technology, 54(13), 7879–7890. 10.1021/acs.est.0c01764 [DOI] [PubMed] [Google Scholar]
- Huang, R. J. , Zhang, Y. , Bozzetti, C. , Ho, K. F. , Cao, J. J. , Han, Y. , et al. (2014). High secondary aerosol contribution to particulate pollution during haze events in China. Nature, 514(7521), 218–222. 10.1038/nature13774 [DOI] [PubMed] [Google Scholar]
- Hubbell, B. , Fann, N. , & Levy, J. I. (2009). Methodological considerations in developing local‐scale health impact assessments: Balancing national, regional, and local data. Air Quality Atmosphere & Health, 2, 99–110. 10.1007/s11869-009-0037-z [DOI] [Google Scholar]
- Jerrett, M. , Burnett, R. T. , Pope, C. A., II. , Ito, K. , Thurston, G. , Krewski, D. , et al. (2009). Long‐term ozone exposure and mortality. New England Journal of Medicine, 360(11), 1085–1095. 10.1056/nejmoa0803894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kan, H. D. , & Chen, B. H. (2002). Analysis of exposure response relationships of air particulate matter and adverse health outcomes in China. Journal of Environment and Health, 19, 422–424. [Google Scholar]
- Kuerban, M. , Waili, Y. , Fan, F. , Liu, Y. , Qin, W. , Dore, A. J. , et al. (2020). Spatio‐temporal patterns of air pollution in China from 2015 to 2018 and implications for health risks. Environmental Pollution, 258, 113659. 10.1016/j.envpol.2019.113659 [DOI] [PubMed] [Google Scholar]
- Lanzi, E. , Dellink, R. , & Chateau, J. (2018). The sectoral and regional economic consequences of outdoor air pollution to 2060. Energy Economics, 71, 89–113. 10.1016/j.eneco.2018.01.014 [DOI] [Google Scholar]
- Lelieveld, J. , Barlas, C. , Giannadaki, D. , & Pozzer, A. (2013). Model calculated global, regional and megacity premature mortality due to air pollution. Atmospheric Chemistry and Physics, 13(14), 7023–7037. 10.5194/acp-13-7023-2013 [DOI] [Google Scholar]
- Lelieveld, J. , Evans, J. S. , Fnais, M. , Giannadaki, D. , & Pozzer, A. (2015). The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature, 525(7569), 367–+. 10.1038/nature15371 [DOI] [PubMed] [Google Scholar]
- Li, K. , Jacob, D. J. , Liao, H. , Shen, L. , Zhang, Q. , & Bates, K. H. (2019). Anthropogenic drivers of 2013‐2017 trends in summer surface ozone in China. Proceedings of the National Academy of Sciences of the United States of America, 116(2), 422–427. 10.1073/pnas.1812168116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, P. , Xin, J. , Wang, Y. , Wang, S. , Li, G. , Pan, X. , et al. (2013). The acute effects of fine particles on respiratory mortality and morbidity in Beijing, 2004–2009. Environmental Science & Pollution Research, 20(9), 6433–6444. 10.1007/s11356-013-1688-8 [DOI] [PubMed] [Google Scholar]
- Liao, Z. , Gao, M. , Sun, J. , & Fan, S. (2017). The impact of synoptic circulation on air quality and pollution‐related human health in the Yangtze River Delta region. The Science of the Total Environment, 607, 838–846. 10.1016/j.scitotenv.2017.07.031 [DOI] [PubMed] [Google Scholar]
- Lim, C. C. , Hayes, R. B. , Ahn, J. , Shao, Y. , Silverman, D. T. , Jones, R. R. , et al. (2019). Long‐term exposure to ozone and cause‐specific mortality risk in the United States. American Journal of Respiratory and Critical Care Medicine, 200(8), 1022–1031. 10.1164/rccm.201806-1161oc [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim, S. S. , Vos, T. , Flaxman, A. D. , Danaei, G. , Shibuya, K. , Adair Rohani, H. , et al. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990‐2010: A systematic analysis for the global burden of disease study 2010. Lancet, 380(9859), 2224–2260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin, Y. , Jiang, F. , Zhao, J. , Zhu, G. , He, X. , Ma, X. , et al. (2018). Impacts of O3 on premature mortality and crop yield loss across China. Atmospheric Environment, 194, 41–47. 10.1016/j.atmosenv.2018.09.024 [DOI] [Google Scholar]
- Liu, M. , Huang, Y. , Ma, Z. , Jin, Z. , Liu, X. , Wang, H. , et al. (2017). Spatial and temporal trends in the mortality burden of air pollution in China: 2004‐2012. Environment International, 98, 75–81. 10.1016/j.envint.2016.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu, D. , Xu, J. , Yang, D. , & Zhao, J. (2017). Spatio‐temporal variation and influence factors of PM2.5 concentrations in China from 1998 to 2014. Atmospheric Pollution Research, 8(6), 1151–1159. 10.1016/j.apr.2017.05.005 [DOI] [Google Scholar]
- Lu, X. , Lin, C. , Li, Y. , Yao, T. , Fung, J. C. H. , & Lau, A. K. H. (2017). Assessment of health burden caused by particulate matter in southern China using high‐resolution satellite observation. Environment International, 98, 160–170. 10.1016/j.envint.2016.11.002 [DOI] [PubMed] [Google Scholar]
- Lu, X. , Zhang, L. , Wang, X. , Gao, M. , Li, K. , Zhang, Y. , et al. (2020). Rapid increases in warm‐Season surface ozone and resulting health impact in China since 2013. Environmental Science and Technology Letters, 7(4), 240–247. 10.1021/acs.estlett.0c00171 [DOI] [Google Scholar]
- Maji, K. J. , & Namdeo, A. (2021). Continuous increases of surface ozone and associated premature mortality growth in China during 2015‐2019. Environmental Pollution, 269, 116183. 10.1016/j.envpol.2020.116183 [DOI] [PubMed] [Google Scholar]
- Maji, K. J. , & Sarkar, C. (2020). Spatio‐temporal variations and trends of major air pollutants in China during 2015‐2018. Environmental Science & Pollution Research, 27(27), 33792–33808. 10.1007/s11356-020-09646-8 [DOI] [PubMed] [Google Scholar]
- Maji, K. J. , Ye, W. F. , Arora, M. , & Nagendra, S. M. S. (2018). PM2.5‐related health and economic loss assessment for 338 Chinese cities. Environment International, 121, 392–403. 10.1016/j.envint.2018.09.024 [DOI] [PubMed] [Google Scholar]
- Maji, K. J. , Ye, W. F. , Arora, M. , & Nagendra, S. M. S. (2019). Ozone pollution in Chinese cities: Assessment of seasonal variation, health effects and economic burden. Environmental Pollution, 247, 792–801. 10.1016/j.envpol.2019.01.049 [DOI] [PubMed] [Google Scholar]
- Malley, C. S. , Henze, D. K. , Kuylenstierna, J. C. I. , Vallack, H. W. , Davila, Y. , Anenberg, S. C. , et al. (2017). Updated global estimates of respiratory mortality in adults 30 Years of age attributable to long‐term ozone exposure. Environmental Health Perspectives, 125(8), 087021. 10.1289/ehp1390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonnell, W. F. , Stewart, P. W. , Andreoni, S. , Seal, E. , Kehrl, H. R. , Horstman, D. H. , et al. (1997). Prediction of ozone‐induced FEV1 changes: Effects of concentration, duration, and ventilation. American Journal of Respiratory and Critical Care Medicine, 156(3), 715–722. 10.1164/ajrccm.156.3.9611044 [DOI] [PubMed] [Google Scholar]
- Nansai, K. , Tohno, S. , Chatani, S. , Kanemoto, K. , Kurogi, M. , Fujii, Y. , et al. (2020). Affluent countries inflict inequitable mortality and economic loss on ASIA via PM2.5 emissions. Environment International, 134, 105238. 10.1016/j.envint.2019.105238 [DOI] [PubMed] [Google Scholar]
- NBSC . (2016). China statistical Yearbook 2016. National Bureau of Statistical of China. [Dataset]. Retrieved from http://www.stats.gov.cn/tjsj/ndsj/2016/indexeh.htm
- Philip, S. , Martin, R. V. , van Donkelaar, A. , Lo, J. W. H. , Wang, Y. , Chen, D. , et al. (2014). Global chemical composition of ambient fine particulate matter for exposure assessment. Environmental Science & Technology, 48(22), 13060–13068. 10.1021/es502965b [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope, C. A. , Cohen, A. J. , & Burnett, R. T. (2018). Cardiovascular disease and fine particulate matter. Circulation Research, 122(12), 1645–1647. 10.1161/circresaha.118.312956 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qiu, H. , Yu, I. T. , Wang, X. , Tian, L. , Tse, L. A. , & Wong, T. W. (2013). Differential effects of fine and coarse particles on daily emergency cardiovascular hospitalizations in Hong Kong. Atmospheric Environment, 64, 296–302. 10.1016/j.atmosenv.2012.09.060 [DOI] [Google Scholar]
- Salonen, H. , Salthammer, T. , & Morawska, L. (2018). Human exposure to ozone in school and office indoor environments. Environment International, 119, 503–514. 10.1016/j.envint.2018.07.012 [DOI] [PubMed] [Google Scholar]
- Shang, Y. , Sun, Z. , Cao, J. , Wang, X. , Zhong, L. , Bi, X. , et al. (2013). Systematic review of Chinese studies of short‐term exposure to air pollution and daily mortality. Environment International, 54, 100–111. 10.1016/j.envint.2013.01.010 [DOI] [PubMed] [Google Scholar]
- Shen, F. , Zhang, L. , Jiang, L. , Tang, M. , Gai, X. , Chen, M. , & Ge, X. (2020). Temporal variations of six ambient criteria air pollutants from 2015 to 2018, their spatial distributions, health risks and relationships with socioeconomic factors during 2018 in China. Environment International, 137, 105556. 10.1016/j.envint.2020.105556 [DOI] [PubMed] [Google Scholar]
- Sicard, P. , De Marco, A. , Agathokleous, E. , Feng, Z. , Xu, X. , Paoletti, E. , et al. (2020). Amplified ozone pollution in cities during the COVID‐19 lockdown. The Science of the Total Environment, 735, 139542. 10.1016/j.scitotenv.2020.139542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sicard, P. , Serra, R. , & Rossello, P. (2016). Spatiotemporal trends in ground‐level ozone concentrations and metrics in France over the time period 1999–2012. Environmental Research, 149, 122–144. 10.1016/j.envres.2016.05.014 [DOI] [PubMed] [Google Scholar]
- Song, C. , He, J. , Wu, L. , Jin, T. , Chen, X. , Li, R. , et al. (2017). Health burden attributable to ambient PM2.5 in China. Environmental Pollution, 223, 575–586. 10.1016/j.envpol.2017.01.060 [DOI] [PubMed] [Google Scholar]
- Song, Y. , Wang, X. , Maher, B. A. , Li, F. , Xu, C. , Liu, X. , et al. (2016). The spatial‐temporal characteristics and health impacts of ambient fine particulate matter in China. Journal of Cleaner Production, 112, 1312–1318. 10.1016/j.jclepro.2015.05.006 [DOI] [Google Scholar]
- Turner, M. C. , Jerrett, M. , Pope, C. A. , Krewski, D. , Gapstur, S. M. , Diver, W. R. , et al. (2016). Long‐term ozone exposure and mortality in a large prospective study. American Journal of Respiratory and Critical Care Medicine, 193(10), 1134–1142. 10.1164/rccm.201508-1633oc [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, Q. , Wang, J. , He, M. Z. , Kinney, P. L. , & Li, T. (2018). A county‐level estimate of PM2.5 related chronic mortality risk in China based on multi‐model exposure data. Environment International, 110, 105–112. 10.1016/j.envint.2017.10.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, Y. Y. , Hu, J. L. , Zhu, J. , Li, J. Y. , Qin, M. M. , Liao, H. , et al. (2021). Health Burden and economic impacts attributed to PM2.5 and O3 in China from 2010 to 2050 under different representative concentration pathway scenarios. Resources, Conservation and Recycling, 173, 105731. 10.1016/j.resconrec.2021.105731 [DOI] [Google Scholar]
- WHO . (2006). WHO air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide. Retrieved from http://apps.who.int/iris/bitstream/10665/69477/1/WHO_SDE_PHE_OEH_06.02_eng.pdf [PubMed] [Google Scholar]
- World Bank . (2016). The cost of air pollution: Strengthening the economic case for action. World Bank Group. [Google Scholar]
- Xie, P. , Liu, X. Y. , Liu, Z. R. , Li, T. T. , & Bai, Y. H. (2009). Study of exposure‐response relationship of air particulate pollution in China. China Environmental Science, 29, 1034–1040. [Google Scholar]
- Xie, P. , Liu, X. Y. , Liu, Z. R. , Li, T. T. , Zhong, L. J. , & Xiang, Y. R. (2010). Impact of exposure to air pollutants on human health effects in Pearl River Delta. China Environmental Science, 30(7), 997–1003. [Google Scholar]
- Xie, Y. , Dai, H. , Dong, H. , Hanaoka, T. , & Masui, T. (2016). Economic impacts from PM2.5 pollution‐related health effects in China: A provincial‐level analysis. Environmental Science & Technology, 50(9), 4836–4843. 10.1021/acs.est.5b05576 [DOI] [PubMed] [Google Scholar]
- Xie, Y. , Dai, H. , Zhang, Y. , Tatsuya, H. , & Toshihiko, M. (2017). Health and economic impacts of ozone pollution in China: A provincial level analysis. Atmospheric Chemistry and Physics, 1–63. [Google Scholar]
- Yin, H. , Pizzol, M. , & Xu, L. (2017). External costs of PM2.5 pollution in Beijing, China: Uncertainty analysis of multiple health impacts and costs. Environmental Pollution, 226, 356–369. 10.1016/j.envpol.2017.02.029 [DOI] [PubMed] [Google Scholar]
- Yin, P. , Brauer, M. , Cohen, A. J. , Wang, H. D. , Li, J. , Burnett, R. T. , et al. (2020). The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990‐2017: An analysis for the global burden of disease study 2017. Lancet planetary health, 4(9), E386–E398. 10.1016/s2542-5196(20)30161-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, D. , Bai, K. , Zhou, Y. , Shi, R. , & Ren, H. (2019). Estimating ground‐level concentrations of multiple air pollutants and their health impacts in the Huaihe River Basin in China. International Journal of Environmental Research and Public Health, 16(4), 579. 10.3390/ijerph16040579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, X. , Ou, X. , Yang, X. , Qi, T. , Nam, K. M. , Zhang, D. , et al. (2017). Socioeconomic burden of air pollution in China: Province‐level analysis based on energy economic model. Energy Economics, 68, 478–489. 10.1016/j.eneco.2017.10.013 [DOI] [Google Scholar]
- Zhang, X. X. , Gu, X. C. , Cheng, C. X. , & Yang, D. Y. (2020). Spatiotemporal heterogeneity of PM2.5 and its relationship with urbanization in North China from 2000 to 2017. The Science of the Total Environment, 744, 140925. 10.1016/j.scitotenv.2020.140925 [DOI] [PubMed] [Google Scholar]
- Zhao, H. , Chen, K. , Liu, Z. , Zhang, Y. , Shao, T. , & Zhang, H. (2021). Coordinated control of PM2.5 and O3 is urgently needed in China after implementation of the “Air pollution prevention and control action plan”. Chemosphere, 270, 129441. 10.1016/j.chemosphere.2020.129441 [DOI] [PubMed] [Google Scholar]
- Zhao, L. , Liang, H. R. , Chen, F. Y. , Chen, Z. , Guan, W. J. , & Li, J. H. (2017). Association between air pollution and cardiovascular mortality in China: A systematic review and meta‐analysis. Oncotarget, 8(39), 66438–66448. 10.18632/oncotarget.20090 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- China National Environmental Monitoring Centre . (2020). National Air Quality Forecast Information Dissemination System [Dataset]. Monitoring Data. Retrieved from https://quotsoft.net/air/
- China’s economic and social big data research platform . (2020). The 6th Population Census [Dataset]. Retrieved from https://data.cnki.net/yearbook/Single/N2021050059
- NBSC . (2016). China statistical Yearbook 2016. National Bureau of Statistical of China. [Dataset]. Retrieved from http://www.stats.gov.cn/tjsj/ndsj/2016/indexeh.htm
Supplementary Materials
Supporting Information S1
Data Availability Statement
Data sets for this study are publicly available. Data on ozone concentration are available via the China National Environmental Monitoring Centre (https://quotsoft.net/air/), and Population data (>30 years and all age group) obtained from the 6th Population Census (https://data.cnki.net/yearbook/Single/N2021050059).