

Abstract
Childhood adversity is a major risk factor for multiple forms of psychopathology, and recent efforts have focused on understanding the underlying psychological mechanisms. One outstanding candidate is emotion regulation, which has been associated with both childhood adversity, and psychopathology. Based on the available evidence, the present meta-analysis set out to investigate the mechanistic involvement of emotion regulation in the relation between childhood adversity and psychopathology. Systematic searches in three databases (PubMed; PsycINFO; Web of Science) identified 215 eligible studies. Using meta-analytic structural equation modeling, we fitted a partial mediation model to the available data across studies, in which childhood adversity was related to psychopathology both directly and through emotion regulation. Multiple emotion regulation dimensions were analyzed, including emotion regulation difficulties and the habitual use of rumination, distraction, reappraisal, and suppression. Measures of psychopathology included a wide range of internalizing and externalizing symptoms in both clinical and non-clinical samples. The results indicated that childhood adversity was positively associated with emotion regulation difficulties, as well as the habitual use of rumination and suppression. In turn, these measures of emotion regulation were positively associated with psychopathology. Habitual reappraisal use showed negative relations with both childhood adversity and psychopathology. All these emotion regulation measures were supported as mediators in the relation between childhood adversity and psychopathology. In contrast, distraction was not related to childhood adversity or psychopathology, and its mediator role was not supported. These results suggest that altered emotion regulation is a consistent marker of childhood adversity and contributes to risk of psychopathology.
Keywords: childhood, adversity, emotion, regulation, psychopathology
Extreme levels of childhood adversity have been consistently associated with lifelong and transdiagnostic risk of psychopathology (Green et al., 2010; Kessler et al., 2010). Recent efforts have focused on understanding the underlying psychological mechanisms, and progress in this area is crucial for increasing the specificity of psychological interventions (Dvir, Ford, Hill, & Frazier, 2014; Nanni, Uher, & Danese, 2012). Emotion regulation stands out among candidate mechanisms in light of its association with both childhood adversity (for review see Dvir et al., 2014; Hoppen & Chalder, 2018; Jaffee, 2017; McCrory, De Brito, & Viding, 2012; McLaughlin, 2016), and psychopathology (Aldao, Gee, De Los Reyes, & Seager, 2016; Beauchaine & Cicchetti, 2019; Gross & Jazaieri, 2014; Kring, 2008). However, relatively few studies have directly examined the mediator role of emotion regulation, and the integration of these results is not straightforward given the multiplicity of theoretical approaches to emotion regulation. We capitalized on recent advances in meta-analytic structural equation modeling to investigate the mechanistic involvement of emotion regulation in the relation between childhood adversity and psychopathology. To do so, we used extensive data on relevant pathways (i.e., childhood adversity to emotion regulation, and emotion regulation to psychopathology), as available in published studies.
Why emotion regulation?
Almost all forms of psychopathology involve a component of disrupted emotion regulation, making this concept a candidate mechanism in which to explore individual differences in the psychological consequences of stressful events (e.g., Lazarus & Folkman, 1984). In what is probably the first study on childhood adversity and coping, Leitenberg, Greenwald, and Cado (1992) examined the habitual use of multiple strategies in a sample of women who reported a history of childhood sexual abuse. Among the strategies assessed were rumination, cognitive reappraisal, and expressive suppression, and results indicated that, in this sample, suppression was used more frequently than other strategies, and it was negatively associated with psychological adjustment after controlling for multiple characteristics (e.g., age when abuse began, duration) of sexual abuse (Leitenberg et al., 1992). Another early study used a broader assessment “targeting processes central to emotionality and regulation, including affective lability, intensity, valence, flexibility, and situational appropriateness of emotional expressions” (Shields & Cicchetti, 1998 p. 385) and found that maltreated children (identified based on official social services records) showed higher emotional lability and negativity, and lower adaptive emotion regulation, as well as higher aggressive behavior compared to non-maltreated children. The effect of maltreatment on aggression became non-significant when controlling for emotional lability/negativity, which suggested that the latter may play a mediator role (Shields & Cicchetti, 1998). These studies have laid the groundwork for future investigations, which would incorporate other emotion regulation conceptualizations (e.g., Gratz & Roemer, 2004; Gross, 1998; Nolen-Hoeksema, 1991) that emerged in clinical psychology.
Studies on the development of emotion regulation have also suggested that this domain is likely to be vulnerable to childhood adversity. From a developmental perspective, emotion is a property that emerges in a cascading manner from abilities including attention, memory, theory of mind, and categorization—each of which may be influenced by childhood adversity (Ruba & Pollak, 2020). Similarly, emotion regulation subsumes many aspects and processes which undergo developmental changes throughout childhood and adolescence. For instance, emotion understanding improves in early childhood, the repertoire of emotion regulation strategies expands during adolescence, and the habitual use of certain emotion regulation strategies, particularly cognitive strategies (e.g., reappraisal), which allow individuals to regulate emotion while remaining engaged in the processing of emotional events, becomes consistent in adolescence and emerging adulthood (for review see Compas et al., 2017; R. A. Thompson & Goodman, 2010). These developmental changes are thought to be driven by an interplay between the maturation of neuroendocrine systems and social learning opportunities, both of which may be particularly sensitive to childhood adversity. On the one hand, the immature status of the hypothalamic-pituitary-adrenal axis and the prefrontal-amygdala circuits, for example, renders these stress systems susceptible to lifelong structural and functional alteration following childhood adversity (for review see Lupien, McEwen, Gunnar, & Heim, 2009; McCrory et al., 2012). On the other hand, youth learn how to regulate their emotions mostly from their parents, through modelling and feedback (Kiel & Kalomiris, 2015; Morris, Criss, Silk, & Houltberg, 2017). Maltreating parents consistently report poor emotion regulation (Lavi, Manor-Binyamini, et al., 2019; Lavi, Ozer, Katz, & Gross, 2021; Plate et al., 2019) and their influence may bias social learning of emotion regulation in children. Recent studies support this view: not only that parental emotion regulation difficulties are associated with children’s emotion regulation difficulties (Osborne, Duprey, O’Brien Caughy, & Oshri, 2021), but the former may fully account for the impact of childhood adversity on children’s emotion regulation (Milojevich, Machlin, & Sheridan, 2020). In summary, childhood adversity may negatively interfere with emotion regulation development through both premature activation of biological stress systems and maladaptive social learning.
Multiple conceptualizations of emotion regulation
One challenge to meta-analysis is related to the multiplicity of approaches to emotion regulation, which precludes the combination of all emotion regulation measures in a single global outcome. As illustrated in early studies (Leitenberg et al., 1992; Shields & Cicchetti, 1998), emotion regulation has been conceptualized along two main lines, which have developed relatively independently in different fields of psychology and are distinct at several levels (for review see John & Eng, 2014). One focuses on the functional effects of emotion regulation, as reflected by cognitive performance and goal-directed behavior in the presence of emotion (Cole, Michel, & Teti, 1994; Gratz & Tull, 2010; R. A. Thompson, 1994). From this perspective, emotion regulation, whether assessed as ability or difficulty, has been defined as the capacity to keep the balance between the urgency of emotion and competing goals (Cole et al., 1994), or modulating emotional arousal so as to foster an optimal level of engagement with environment (Shields & Cicchetti, 1998). The scope of emotion regulation assessments in this category is broad and includes: (a) effects of emotion on domains such as attentional control, goal pursuit, and social expression; (b) emotional awareness and the perception of emotional characteristics such as frequency, intensity, and lability; and (c) emotional acceptance, viewed as a fundamental condition of emotion regulation (opposite emotional control or the avoidance of emotion altogether) (for review see Gratz & Tull, 2010).
The second category includes process approaches to emotion regulation, focusing on strategies that are commonly employed in efforts to modulate emotional responses according to goals. These strategies (some of which have also been studied in the coping literature, see Compas et al., 2014) have been systematically characterized based on the stage of emotional processing in which they intervene (Gross, 1998, 2015), as well as their relation to psychopathology (Nolen-Hoeksema, 1991, 2004), and assessments have mostly focused on their habitual use (Gross & John, 2003; Treynor, Gonzalez, & Nolen-Hoeksema, 2003). Overall, both approaches (i.e., difficulties/ability, and strategies) have been used in research on childhood adversity, and provide complementary information that needs to be analyzed separately.
Previous meta-analyses
Two recent meta-analyses have examined the relation between childhood adversity and emotion regulation. One (Lavi, Katz, Ozer, & Gross, 2019) included only studies (k = 58) in children and adolescents aged up to 18, which met one of two criteria: maltreatment was substantiated based on official records, and longitudinal approach. Outcomes related to both emotion reactivity and emotion regulation were considered, and further coded separately depending on their focus on subjective experience, behavior, or physiology. The results supported increased negative affect in maltreated compared to non-maltreated youth, both at the level of experience and behavior, as well as decreased positive affect and increased aggression at the behavioral level. In which emotion regulation was concerned, maltreated youth showed increased difficulties, as indexed by a variety of outcomes related to both emotion regulation, and coping (Lavi, Katz, et al., 2019).
The other meta-analysis (Gruhn & Compas, 2020) included 35 studies in children and adolescents (age 5-18), which focused on childhood maltreatment, and emotion regulation and coping. Outcomes were categorized at three levels of generality, from broad domains (e.g., total emotion regulation/coping) to factors (e.g., emotion regulation/coping styles) and specific strategies. Childhood maltreatment was significantly associated with both domain measures, that is, negatively with emotion regulation/coping ability and positively with emotion regulation/coping difficulties. Significant associations were also found at the strategy level, including positive relations between maltreatment and emotional suppression (as well as expression), but not distraction (Gruhn & Compas, 2020). No relations were found at the factor level.
These meta-analyses have lent support to the relation between childhood adversity and emotion regulation in youth. However, both left out studies in adults, which are the largest part of the empirical literature, and excluded forms of childhood adversity other than maltreatment. Most forms of psychopathology start to emerge in adolescence and adulthood, so it is not surprising that studies investigating the involvement of childhood adversity and emotion regulation in risk of psychopathology have overly focused on adults. Some of these studies have supported the negative impact of a variety of adverse childhood experiences such as extreme poverty, natural disasters, war, or parental psychopathology on emotion regulation and risk of mental disorders, suggesting that these effects are not limited to maltreatment. In addition, and perhaps most importantly, previous meta-analyses have not addressed the mediator role of emotion regulation in the relation between childhood adversity and psychopathology, which holds the most clinical relevance.
The relations between emotion regulation and psychopathology have also been consistently supported in meta-analyses. For example, suppression and rumination have been positively associated (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Compas et al., 2017; Hu et al., 2014; Prefit, Candea, & Szentagotai-Tatar, 2019; Seligowski, Lee, Bardeen, & Orcutt, 2015), and reappraisal has been negatively associated (Aldao et al., 2010; Hu et al., 2014; Prefit et al., 2019; but see Seligowski et al., 2015) with psychopathology. It is noteworthy that some of these relations (e.g., suppression and psychopathology) were found to be larger in adults compared to children and adolescents (Aldao et al., 2010). Broader measures of emotion regulation, such as difficulties (Prefit et al., 2019; Seligowski et al., 2015) and abilities (Compas et al., 2017), have also shown consistent associations with internalizing and externalizing symptoms. These results support the mechanistic involvement of emotion regulation in psychopathology, and further underscore the hypothesis that emotion regulation may be one of the mediators underlying the impact of childhood adversity on mental health.
Mediation in meta-analysis
The main aim of the present study was to take a meta-analytic approach to the mediator role of emotion regulation in the pathway from childhood adversity to psychopathology. We used two-stage structural equation modeling (Cheung & Chan, 2005), in which a pooled correlation matrix is first created and then the mediation model is fitted to the data. This approach offers several advantages over other meta-analytic structural equation modeling methods: (a) it takes into account sample size differences across the elements of the pooled correlation matrix, and gives more weight to estimates with higher precision (i.e., smaller standard error based on higher N) (Cheung & Chan, 2009); (2) considers the potentially nested nature of correlations (Jak, 2015); and (3) uses the full information maximum likelihood estimation to handle missing data (studies missing one or more sets of correlations), a method which is robust against both data missing completely at random and missing at random (Enders, 2010). The latter potential bias (i.e., missing data) is indeed characteristic of the pool of studies that we meta-analyzed considering that some studies reported only one relation (i.e., either between childhood adversity and emotion regulation, or emotion regulation and psychopathology), while other studies reported both these relations.
Another limit of previous studies is that few have directly examined the mediating role of emotion regulation in the pathway between childhood adversity and psychopathology, and the results did not always support this hypothesis. In addition, in light of the effect size of the reported correlations, some of the previous studies may have been underpowered for mediation analysis (Fritz & Mackinnon, 2007). Therefore, a meta-analysis of this clinically outstanding issue has been warranted. Mindful of the distinct breadth and focus of emotion regulation measures employed in previous studies, multiple analyses were run in order to separately investigate the mediator role of emotion regulation difficulties, and of the habitual use of rumination, distraction, reappraisal, and suppression. We hypothesized that childhood adversity would positively correlate with emotion regulation difficulties, rumination, and suppression, and these emotion regulation measures would in turn correlate positively with symptoms of psychopathology. In the case of reappraisal, we expected negative correlations with both childhood adversity, and psychopathology. Given the mix of positive (e.g., higher relative efficiency in intense stress compared to reappraisal) and negative (i.e., poor memory of the stressor) consequences which have been associated with distraction (e.g., Sheppes & Meiran, 2007; Sheppes, Scheibe, Suri, & Gross, 2011), it was difficult to put forward a hypothesis on its relations with childhood adversity and psychopathology, and the analyses were, therefore, exploratory. We also examined partial mediation in light of the previous literature (e.g., McCrory & Viding, 2015; McLaughlin, 2016) which has suggested that multiple mechanisms are involved in the relation between childhood adversity and psychopathology. The present model thus included both the indirect (i.e., childhood adversity to psychopathology via emotion regulation) and direct pathways between childhood adversity and psychopathology.
Methods
Literature search
The literature search was conducted on PubMed, PsycINFO, and Web of Science bibliographic databases, from their inception to July 2021, using combinations of keywords related to childhood adversity and emotion regulation (see Supplementary Material for the full search string). In addition, we searched for articles on Google Scholar, and in the reference list of recent reviews. Only articles written in English and published in peer-reviewed journals were considered.
Selection of studies
All studies were independently evaluated by at least two authors. Studies were included if they met the following criteria: (1) they were conducted in humans; (2) empirical data was reported; (3) they included an assessment of childhood adversity (i.e., stressful events that occurred while growing up or before age 18) using self-report, other-report or official records; and (4) they included an assessment of emotion regulation using self- or other-report measures. Studies were excluded if they: (1) did not assess the occurrence of childhood adversity, but only related constructs such as parental characteristics (e.g., maternal abuse history; parental distress and rigidity; parental relational problems); (2) focused on outcomes which were only related to emotion regulation, pertaining either to executive processes not limited to emotion (e.g., self-regulatory abilities; thought suppression), and dispositional levels of affect (e.g., negative affect; alexithymia; shame proneness); (3) investigated general dimensions (i.e., factors) of coping (e.g., adaptive and maladaptive coping; engagement and disengagement coping; task- and emotion-focused coping; substance use coping; spiritual coping), rather than specific strategies that could be assimilated to emotion regulation; (4) inferred emotion regulation from autonomic activity or emotional behavior during social interactions, in light of the limited coherence between these measures and emotional experience (Mauss, Levenson, McCarter, Wilhelm, & Gross, 2005); (5) assessed emotion regulation using cognitive tasks which focus on the implementation stage of this process, rather than the strategy selection stage targeted by measures of habitual strategy use (Gross, 2015; McRae, Jacobs, Ray, John, & Gross, 2012); (6) included patients with psychosis; and (7) the same sample was used in another study included in the analysis.
Outcome measures
Emotion regulation.
Two categories of emotion regulation outcomes were considered, in line with constructs from mainstream developmental and clinical psychology. The first focused on emotion regulation difficulties, as indexed by perceived cognitive and behavioral efficiency during emotional states, as well as emotional awareness, and emotional acceptance. Based on preliminary analyses, which indicated that results do not differ when emotion regulation difficulties and emotion regulation ability are analyzed separately, they were combined by reversing the correlations on the latter outcome so that positive correlations indicated greater emotion regulation difficulties. The second category of outcomes focused on emotion regulation strategies, including (i) expressive suppression (i.e., reducing the behavioral expression of emotion); (ii) cognitive reappraisal (i.e., changing the appraisal of an emotional event); (iii) rumination (i.e., repetitive thinking about emotion, the situation that triggered it and its consequences); and (iv) distraction (i.e., moving attention away from an emotional event, through thinking about something else or engaging in another activity). In the initial stages of the literature search, we also considered situation-focused avoidance, and acceptance among the potential strategy-related outcomes, but eventually eliminated them from analysis. Avoidance is typically assessed using coping measures that do not distinguish between situational (e.g., efforts to avoid events that may trigger negative emotion) and cognitive avoidance (e.g., distraction, thought suppression, wishful thinking) (see Zimmer-Gembeck & Skinner, 2011). However, where multidimensional measures of avoidance included distraction and scores were available, the study was used in the analysis. In which acceptance was concerned, we found no measure that assessed its habitual use as an emotion regulation strategy. Instead, measures such as the Acceptance and Action Questionnaire (Hayes et al., 2004) assess broad emotional and behavioral problems, which are taken to indicate poor emotional acceptance. After careful review of each scale, some of these measures were coded as emotion regulation difficulties.
Psychopathology.
Measures of psychopathology included internalizing (e.g., anxiety, depression, eating) and externalizing (e.g., substance use, antisocial) symptoms.
Data extraction
Data from each study were independently extracted by three authors, and disagreements were resolved by discussion (97.2% interrater reliability). We extracted information that allowed us to calculate the effect size from each study, that is, correlations between adversity and emotion regulation (as well as symptoms of psychopathology), and mean differences in emotion regulation between groups selected for childhood adversity (or psychopathology). Standardized regression coefficients were also used to estimate correlations based on the formula of Peterson and Brown (2005). Descriptive information about each study was extracted, including sample size, participants’ age, sample sex distribution, study design (i.e., cross-sectional or longitudinal), and the country where the study was conducted.
Meta-analysis
In Stage 1, the random effects model was used to obtain a pooled correlation matrix among all coded variables (Boker et al., 2011). Given its statistical efficiency and capacity to handle missing data, the full information maximum likelihood estimation was used to pool correlation matrices (Cheung, 2015). Gignac and Szodorai (2016) guidelines were used to interpret estimated mean effect sizes as: small (r = 0.10), moderate (r = 0.20), and high (r = 0.30). To evaluate the degree of homogeneity of effect sizes, the total heterogeneity of weighted mean effects (Cochran’s Q) and the total variation across studies attributable to heterogeneity (I2) were calculated (Higgins & Thompson, 2002). Statistically significant Q indices (p < .01) across the pooled correlation matrices were interpreted as indicators of systematic variance that cannot be explained by sampling error. The I2 was interpreted as the percentage of total variance that can be attributed to between-studies variability (Huedo-Medina, Sanchez-Meca, Marin-Martinez, & Botella, 2006). Values above 75% were interpreted as considerable heterogeneity (Higgins & Green, 2008). Heterogeneity in each correlation set (i.e., childhood adversity – emotion regulation; emotion regulation – psychopathology; childhood adversity - psychopathology) was also examined, based on τ2 coefficients.
In Stage 2, weighted least squares estimation was used to fit the hypothesized mediation models to the resultant pooled correlation matrix from Stage 1. Considering that the mediation model was saturated (and fit indices always indicate perfect fit to the data in these cases, i.e., χ2[0] = 0.00, p = 1; CFI = 1.00; RMSEA = 0.00), mediation was tested by evaluating the significance of the direct and indirect effects (computed as the product of the direct effects). The significance of the estimated parameters was evaluated based on 95% likelihood-based confidence intervals (Neale & Miller, 1997). The parameter estimate was considered statistically significant if the 95% confidence interval around the estimated parameter did not include zero (Shrout & Bolger, 2002).
Study quality
We used a set of previously devised (Madigan et al., 2019; Thornberry, Knight, & Lovegrove, 2012) criteria: (1) representativeness of the sample; (2) inclusion of participants with no history of childhood adversity; (3) assessment of childhood adversity based on multiple informant reports; (4) use of validated measures of childhood adversity ; and (5) use of validated measures of emotion regulation. In addition, we assessed study quality based on the inclusion of non-clinical controls in studies that included clinical samples (i.e., meeting established criteria for mental disorders in a clinical interview) considering that the exclusive focus on the latter category is likely to give a skewed perspective on the correlation between childhood adversity and psychopathology (e.g., up to 80-90% of psychiatric patients report childhood adversity; see Saunders & Adams, 2014).
Results
Data overview
Across emotion regulation dimensions, a total of 215 articles (217 datasets) met the inclusion criteria (see Fig. 1 and Supplementary Table 1), most of which were on emotion regulation difficulties (k = 149; N = 60473) followed by reappraisal (k = 44; N = 14223), rumination (k = 40; N = 13888), suppression (k = 33; N = 9936), and distraction (k = 19; N = 6610). Most studies (k = 170) reported a single effect size, but there were studies in which two (k = 31), three (k = 13) or four (k = 3) effect sizes related to distinct emotion regulation outcomes were reported. The majority of studies (65.44%) focused on childhood maltreatment, while the rest (34.56%) examined a wider array of childhood adverse experiences. Studies in adults predominated (63.59%) relative to studies in children and adolescents (30.88%; participant age not reported in 5.53%).
Fig. 1.
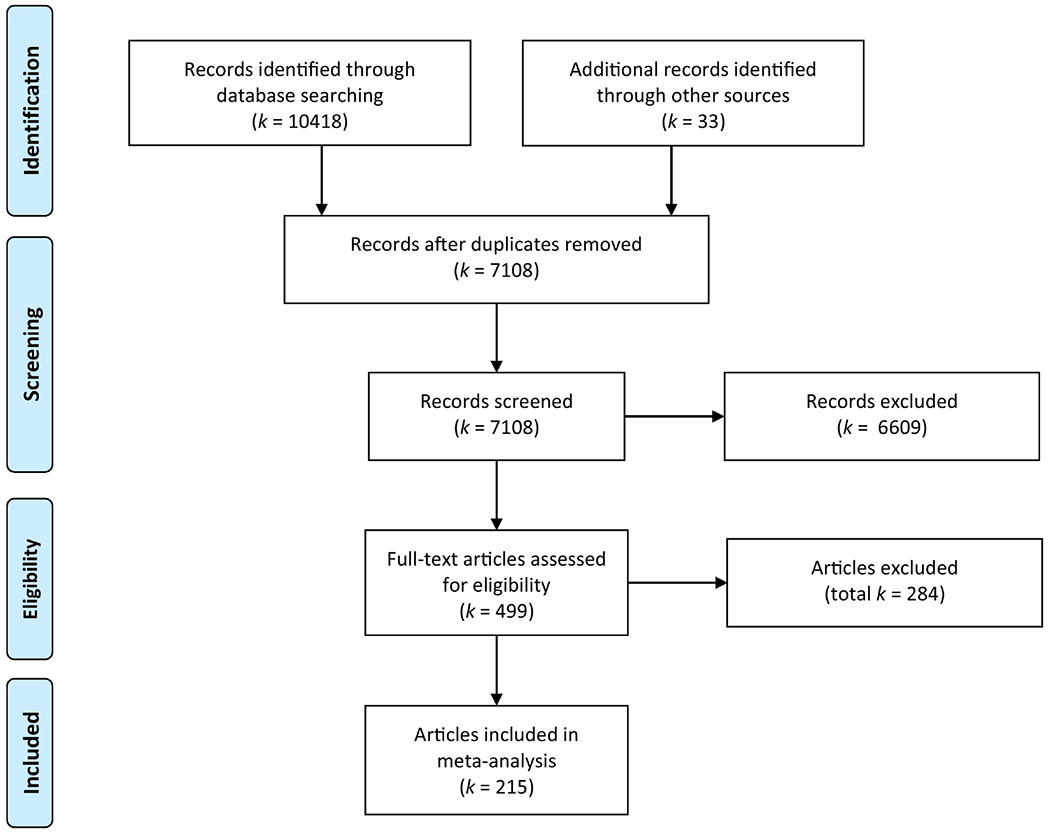
Flow diagram describing the process of study selection.
Stage 1: Pooled correlations
Table 1 shows the pooled correlations and between study heterogeneity coefficients, based on the random-effect analyses in each data set.
Table 1.
Pooled correlations (below the diagonal) and proportion of between-study heterogeneity I2 (above the diagonal) based on Stage 1 random-effect analyses
| Emotion regulation difficulties | |||
|---|---|---|---|
| V1. CA | V2. ER | V3. Psychopathology | |
| V1. CA | 1 | 0.69*** | 0.73** |
| V2. ER | 0.26*** | 1 | 0.83*** |
| V3. Psychopathology | 0.26*** | 0.45*** | 1 |
| Distraction | |||
| V1. CA | 1 | 0.79 | 0.26 |
| V2. ER | 0.01 | 1 | 0.89 |
| V3. Psychopathology | 0.33*** | −0.01 | 1 |
| Rumination | |||
| V1. CA | 1 | 0.80* | 0.79* |
| V2. ER | 0.21*** | 1 | 0.94*** |
| V3. Psychopathology | 0.34*** | 0.39*** | 1 |
| Reappraisal | |||
| V1. CA | 1 | 0.71* | 0.83* |
| V2. ER | −0.06** | 1 | 0.80* |
| V3. Psychopathology | 0.35*** | −0.13*** | 1 |
| Suppression | |||
| V1. CA | 1 | 0.65 | 0.82 |
| V2. ER | 0.17*** | 1 | 0.60 |
| V3. Psychopathology | 0.31*** | 0.23*** | 1 |
Note. Abbreviations: CA, childhood adversity; ER, emotion regulation. Significance of between-study proportions is based on τ2 coefficients.
p < 0.05;
p < 0.01;
p < 0.001
Correlations between childhood adversity and emotion regulation.
Childhood adversity was significantly associated with all emotion regulation dimensions except distraction. Specifically, childhood adversity was positively associated with emotion regulation difficulties, habitual rumination use, and habitual suppression use. In contrast, childhood adversity was negatively associated with habitual reappraisal use.
Correlations between emotion regulation and psychopathology.
The pooled correlations between all emotion regulation measures (except distraction) and psychopathology were significant. Emotion regulation difficulties, habitual rumination use, and habitual suppression use were positively associated with psychopathology. Habitual reappraisal use was negatively associated with psychopathology.
Correlations between childhood adversity and psychopathology.
All analyses indicated a significant positive association between childhood adversity and psychopathology.
Heterogeneity.
Overall heterogeneity was significant in all analyses (all Cochran’s Q ps < 0.001; see Table 1 for the proportion of between-study variability or I2). However, analyses in each correlation set (i.e., based on τ2 coefficients) suggested that only the correlations between childhood adversity and emotion regulation difficulties, habitual rumination and habitual reappraisal showed significant levels of heterogeneity. In contrast, the correlations between childhood adversity and the habitual use of distraction and suppression tended to be homogenous between studies. Similarly, there was significant between-study heterogeneity in the correlations between, on the one hand, emotion regulation difficulties, habitual rumination use, and habitual reappraisal use, and psychopathology, on the other hand. Correlations between habitual suppression use and psychopathology, as well as those between habitual distraction use and psychopathology tended to be homogenous. In which the correlations between childhood adversity and psychopathology was concerned, heterogeneity was significant only in the analyses on emotion regulation difficulties, and habitual rumination use.
Stage 2: Mediation model
We fitted a path model to the pooled Stage 1 correlation matrices, in which childhood adversity predicted psychopathology both through each of the emotion regulation dimensions (separately), and directly. Table 2 describes all parameter estimates and 95% CIs. The paths from both childhood adversity to emotion regulation, and emotion regulation to psychopathology were significant in the analyses on all emotion regulation outcomes except distraction. Childhood adversity was positively associated with emotion regulation difficulties, habitual rumination use, and habitual suppression use, and negatively with habitual reappraisal use. In turn, emotion regulation difficulties, habitual rumination use, and habitual suppression use were all positively associated with psychopathology. Habitual reappraisal use was negatively associated with psychopathology. As expected considering the significant paths described above, all emotion regulation dimensions except distraction were significant mediators in the relation between childhood adversity and psychopathology. Furthermore, the direct path from childhood adversity to psychopathology was also significant in all analyses.
Table 2.
Parameter estimates and 95% confidence intervals of Stage 2 model paths
| Emotion regulation difficulties | |||
|---|---|---|---|
| Estimate | LLCI | ULCI | |
| β CA→ER | 0.26 | 0.24 | 0.27 |
| β ER→psychopathology | 0.41 | 0.38 | 0.45 |
| B CA→psychopathology | 0.15 | 0.11 | 0.18 |
| βCA→ER * βER→psychopathology (indirect effect) | 0.10 | 0.09 | 0.12 |
| Distraction | |||
| β CA→ER | 0.01 | −0.06 | 0.08 |
| β ER→psychopathology | −0.01 | −0.12 | 0.09 |
| B CA→psychopathology | 0.33 | 0.27 | 0.39 |
| βCA→ER * βER→psychopathology (indirect effect) | −0.00 | −0.00 | 0.00 |
| Rumination | |||
| β CA→ER | 0.21 | 0.16 | 0.26 |
| β ER→psychopathology | 0.33 | 0.24 | 0.41 |
| B CA→psychopathology | 0.27 | 0.21 | 0.33 |
| βCA→ER * βER→psychopathology (indirect effect) | 0.07 | 0.04 | 0.09 |
| Reappraisal | |||
| β CA→ER | −0.06 | −0.10 | −0.02 |
| β ER→psychopathology | −0.10 | −0.16 | −0.05 |
| B CA→psychopathology | 0.34 | 0.28 | 0.40 |
| βCA→ER * βER→psychopathology (indirect effect) | 0.01 | 0.00 | 0.01 |
| Suppression | |||
| β CA→ER | 0.17 | 0.12 | 0.21 |
| β ER→psychopathology | 0.18 | 0.12 | 0.24 |
| B CA→psychopathology | 0.28 | 0.19 | 0.36 |
| βCA→ER * βER→psychopathology (indirect effect) | 0.03 | 0.02 | 0.04 |
Note. Abbreviations: CA, childhood adversity; ER, emotion regulation; LLCI, lower level confidence interval; ULCI, upper level confidence interval.
Study quality
The majority of studies were categorized as high-quality on most criteria (see Supplementary Table 2): non-clinical participants included in the sample (78.44%); participants with and without childhood adversity included in the sample (91.28%); confirmed absence of childhood adversity in the comparison group (88.07%); valid childhood adversity measures (87.16%); and valid emotion regulation measures (99.08%). However, the putative absence of psychopathology in the non-clinical group was substantiated in few (14.22%) studies. Furthermore, very few studies employed a representative sample (3.21%), and multiple informants in the assessment of childhood adversity (3.67%).
In order to check whether the results were biased by study quality, we categorized studies based on all but the latter three criteria, for which there were too few high-quality studies. Specifically, studies that met all these criteria were considered high-quality, and those failing to meet any of these criteria were considered low-quality. We followed up the mediation models (Stage 2) separately in the high- and low-quality subgroups, and compared between these models (Supplementary Table 3). In which emotion regulation difficulties and rumination were concerned, we replicated the original results in both subgroups and the difference between models was not significant. Similarly, all paths and the indirect effect were replicated in both high- and low-quality studies on suppression, but there was a significant difference between models. In studies on reappraisal, all paths and the indirect effect were replicated only in the high-quality studies subgroup, and the difference between models in the high- and low-quality subgroups was significant. The path from reappraisal to psychopathology, and the indirect effect of childhood adversity on psychopathology through reappraisal were not significant in the low-quality subgroup. In the distraction sample, all paths (except that from childhood adversity to psychopathology) and the indirect effect were not significant in the low-quality subgroup, replicating the original analysis. In the high-quality subgroup, however, the path from distraction to psychopathology became significant, while the path from childhood adversity to distraction and the indirect effect remained non-significant. As expected, the difference between models was significant.
Discussion
The present meta-analysis found consistent evidence for a mediating role of emotion regulation in the relation between childhood adversity and psychopathology. This view was supported in multiple analyses focused on several distinct emotion regulation measures, and across a wide range of symptoms of psychopathology. The data reported in this paper complement and extend previous meta-analyses on childhood adversity and emotion regulation (Gruhn & Compas, 2020; Lavi, Katz, et al., 2019). First, the present study extends the analysis to symptoms of psychopathology using a two-stage structural equation modeling approach to examine both direct and indirect pathways between childhood adversity, emotion regulation, and psychopathology. This has allowed us to test the hypothesis that emotion regulation is a mechanism underlying enhanced vulnerability to psychopathology. Second, the present analyses also include studies of adults, which comprise the largest part of the literature, as well as clinically relevant emotion regulation strategies that have not been previously analyzed (e.g., rumination, reappraisal). Finally, studies included in the present analysis investigated a wide array of childhood negative event exposures, including maltreatment, peer victimization, extreme poverty, severe illness, parental psychopathology, and natural disasters. Together, these studies suggest that the negative consequences of childhood adversity on emotion regulation and psychopathology are not limited to childhood maltreatment and warrant a broader perspective on the dimensions of adversity.
Adaptive and maladaptive aspects of emotion regulation
The hypothesized indirect effect of childhood adversity on psychopathology was supported by both broad measures of emotion regulation (i.e., difficulties), and measures of the habitual use of specific emotion regulation strategies. Furthermore, among process measures, both higher habitual use of typically maladaptive strategies (i.e., rumination, suppression) and lower habitual use of typically adaptive strategies (i.e., reappraisal) played a mediator role in the relation between childhood adversity and psychopathology. In terms of effect sizes, emotion regulation difficulties, rumination and suppression showed medium and large associations, whereas reappraisal showed small associations with both childhood adversity and psychopathology. In the case of emotion regulation difficulties, the larger effect sizes may be explained by the broader conceptual approach underlying these measures, which includes both emotionality and regulation, compared to the more focused domain of process measures. The larger relations showed by rumination and suppression relative to reappraisal, however, could suggest that the emotion regulation mechanisms that intervene between childhood adversity and psychopathology involve mostly an enhanced use of maladaptive strategies, and to a lesser extent, a reduced use of adaptive strategies. This is in line with previous evidence in psychopathology (e.g., Aldao & Nolen-Hoeksema, 2010; D’Avanzato, Joormann, Siemer, & Gotlib, 2013; Hilt & Pollak, 2013), but should be interpreted with caution considering that we could not compare between models involving different strategies. Moreover, recent evidence suggests that the costs and benefits of emotion regulation strategies largely depends on context, and the adaptive vs. maladaptive distinction should be reconsidered (Sheppes, 2020).
The association between childhood adversity and the habitual use of distraction was not significant in the present analyses (see also Gruhn & Compas, 2020), and neither was the indirect effect of childhood adversity on psychopathology through distraction. One explanation may be the failure to distinguish between cognitive and behavioral means of distraction in previous studies (Zimmer-Gembeck & Skinner, 2011). While both involve moving attention away from emotional events, cognitive distraction also requires the generation of a neutral thought or image on which to refocus attention, which may make it relatively more effortful than behavioral distraction and more susceptible to individual differences (e.g., Hilt, Leitzke, & Pollak, 2017; Shaw, Hilt, & Starr, 2019). It is also noteworthy that the association between distraction and psychopathology was significant when the analysis focused on high-quality studies. Therefore, future studies should be mindful of the distinctions between multiple forms of distraction, and avoid biases in research design such as failing to include controls for groups selected for childhood adversity or psychopathology, and using instruments with unknown validity.
Moving toward multiple mechanisms
The direct pathway between childhood adversity and psychopathology was also significant in models that included the indirect effect, suggesting that emotion regulation can only partially account for the association between childhood adversity and psychopathology. This is in line with the view that multiple mechanisms are needed to account for how childhood adversity is associated with a wide range of mental disorders. For instance, alterations of reward processing at the neural and behavioral level have been found in childhood adversity (e.g., Birn, Roeber, & Pollak, 2017; Dennison et al., 2019; Dillon et al., 2009) and a recent meta-analysis has supported these associations (Oltean, Miu, & Szentágotai-Tătar, 2022). Executive functioning is another domain that may be affected by childhood adversity (e.g., den Kelder, Van den Akker, Geurts, Lindauer, & Overbeek, 2018; Harms, Bowen, Hanson, & Pollak, 2018). One of the challenges for future studies is to assess multiple mechanisms concurrently and characterize their specific contributions.
Clinical implications
Having supported the mediator role of emotion regulation has important implications for mental health interventions in childhood adversity. On the one hand, emotion regulation could be targeted in prevention programs for reducing the risk of psychopathology in individuals with childhood adversity. A variety of emotion regulation training approaches are available and have shown promising results in reducing rumination (e.g., Hilt & Pollak, 2012; Yasinski, Hayes, & Laurenceau, 2016) and enhancing reappraisal (e.g., LeBlanc, Uzun, Aydemir, & Mohiyeddini, 2020; Liu, Ein, Gervasio, & Vickers, 2019), resulting in decreased stress reactivity and symptoms of psychopathology in healthy samples. On the other hand, psychotherapy could increasingly focus on emotion regulation, especially considering that individuals with childhood adversity show reduced response to generic clinical interventions (Nanni et al., 2012). While cognitive restructuring (i.e., reappraisal) has long been an important component of cognitive-behavioral psychotherapy, and third-wave psychotherapies have focused on emotional acceptance (which is included in assessments of emotion regulation difficulties), new approaches (e.g., Renna, Quintero, Fresco, & Mennin, 2017) have been recently developed, which harness a wider range of emotion regulation processes in psychotherapy and target individuals with high levels of chronic distress.
Limitations
One of the limitations of the present study is that we examined a saturated model (i.e., including all possible pathways between variables), which has perfect fit to the data, and we could not compare alternative models. More comprehensive models would allow us to investigate the relative contribution of multiple forms of emotion regulation such as, for example, maladaptive (e.g., rumination, suppression) compared to adaptive (e.g., reappraisal) strategies. To date, these analyses are not possible given that the large majority of studies have assessed only one emotion regulation dimension.
Another limitation is related to heterogeneity in study quality, which may have biased the present results. While our findings on emotion regulation difficulties, habitual rumination and habitual suppression held in both high- and low-quality studies, the mediator role of reappraisal was replicated only in high-quality studies. Furthermore, these follow-up analyses focused only on a subset of quality criteria. The remaining criteria were met by a small number of studies and using them would have resulted in too few high-quality studies to run the analyses. Specifically, most studies failed to substantiate clinical status in putatively non-clinical samples, to use representative samples, and to use multiple informants in childhood adversity assessments.
File drawer effects may have also influenced our findings considering that, in the absence of an established method in two-stage structural equation modeling, we could not investigate publication bias. Finally, we acknowledge the failure to preregister the meta-analysis as a potential limitation.
Future directions and conclusions
Most studies that were included in the present meta-analysis assessed multiple types of childhood adversity and either examined their cumulative effect or tried to isolate their specific effects on emotion regulation and psychopathology. The former approach has been criticized for making the assumption that all types of childhood adversity weigh equally, and the latter is critically limited by the high co-occurrence of childhood adversity types. Smith and Pollak (2020) have recently argued that childhood adversity types are socio-legal categories, and may not map well onto developmental and neural processes. In contrast, childhood adversity characteristics such as developmental age at first exposure, chronicity, and severity may account for significant heterogeneity in long-term neuropsychiatric effects (Smith & Pollak, 2020). An early illustration was provided by the first study on childhood adversity and emotion regulation (Leitenberg et al., 1992), which assessed multiple characteristics of adversity and found that age at first exposure and chronicity were associated with emotion regulation. However, to date, this approach has been used in only a handful of studies on emotion regulation, uncovering more negative effects related to the earlier onset (Dunn, Nishimi, Gomez, Powers, & Bradley, 2018; Kim & Cicchetti, 2010) and the chronicity of childhood adversity (Ehring & Quack, 2010; K. L. Thompson, Hannan, & Miron, 2014). More extensive investigations of childhood adversity characteristics could shed light on important regularities (e.g., sensitive periods, dose-response effects) in the impact on emotion regulation and psychopathology.
One of the major challenges that lie ahead is related to defining severity of childhood adversity. The present sample of studies illustrates the multitude of ways in which childhood adversity severity has been assessed until now, either in terms of greater number of adverse events, affective relation to the perpetrator, lower age at exposure, score above threshold sensitive to concordance with a parallel measure (e.g., interview) or to risk of psychopathology, and stressful impact of the adverse experience. The heterogeneity of severity approaches makes it difficult to integrate findings across studies, and underscore the need to develop and use consensus measures. The next generation of studies should also capitalize on current evidence that a wide range of adverse events have similar negative effects (Cronholm et al., 2015; Finkelhor,Shattuck, Turner, & Hamby, 2015; Smith & Pollak, 2021), and adverse events tend to co-occur (Green et al., 2010; Kessler et al., 2010; Smith & Pollak, 2020). This will involve the development of more comprehensive instruments and analytic approaches that account for multicollinearity.
Future studies could also investigate the relation between childhood adversity and individual differences in multiple stages of emotion regulation. While the present results speak of differences in the strategy selection stage, little is known about the impact of childhood adversity on strategy implementation and monitoring (Sheppes, Suri, & Gross, 2015). Limited evidence indicates that childhood adversity is not associated with altered implementation of reappraisal (e.g., Bilc et al., 2018; Miu et al., 2016), although differences at the neural level have shown a moderator role in the relation between childhood adversity and psychopathology (Rodman, Jenness, Weissman, Pine, & McLaughlin, 2019). In contrast, childhood adversity may be associated with enhanced expressive suppression ability (Luterek, Orsillo, & Marx, 2005), blunted expression ability (Pitur & Miu, 2020), and reduced expressive flexibility (i.e., the capacity to switch between expression of emotion and expressive suppression according to context demands) (Pitur & Miu, 2020).
In conclusion, the present meta-analytic results support the hypothesis that emotion regulation is one of the mechanisms underlying the association between childhood adversity and risk of psychopathology, and provide compelling grounds for focusing on emotion regulation in prevention and intervention efforts.
Supplementary Material
Highlights.
Childhood adversity is associated with emotion regulation difficulties.
Other associations included increased habitual rumination and suppression, and reduced habitual reappraisal.
No evidence for the relation between childhood adversity and habitual distraction.
All the above, but not distraction are associated with psychopathology.
Difficulties, rumination, suppression, and reappraisal were mediators between childhood adversity and psychopathology.
Role of Funding Sources
Andrei C. Miu was supported by a grant of the Romanian Ministry of Education and Research, CNCS - UEFISCDI, project numbers PN-III-P4-ID-PCE-2020-2609 and PN-III-P1-1.1-TE-2019-1243. CNCS - UEFISCDI had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Aurora Szentágotai-Tătar was supported by a grant of the Romanian Ministry of Education and Research, CNCS - UEFISCDI, project numbers PN-III-P4-ID-PCE-2020-2894. CNCS - UEFISCDI had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Diana Nechita was supported by a grant of the Romanian Ministry of Education and Research, CNCS - UEFISCDI, project number PN-III-P1-1.1-PD-2019-0706 CNCS - UEFISCDI had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Seth Pollak was supported by the National Institute of Mental Health (R01MH61285) and the National Institute of Child Health and Human Development (U54 HD090256). These funders had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Biographies
Author biographies
Andrei C. Miu Ph.D. is Professor of Cognitive Neuroscience and Behavioral Genetics, and Director of the Cognitive Neuroscience Laboratory at the Department of Psychology, Babeş-Bolyai University, Cluj-Napoca, Romania. He has a B.A. in Psychology, a M.Sc. in Neuroscience and Molecular Medicine, and a Ph.D. in Psychology, with an interdisciplinary thesis on emotion and cognition. His research has approached individual differences in emotion, their biological and genetic underpinnings, and their role in cognitive performance and risk of psychopathology. His recent work has focused on the involvement of emotion regulation as a mechanism in the association between childhood maltreatment and psychopathology, using behavioral, neurophysiological, neuroendocrine and genetic methods. Dr. Miu has received research fellowships and awards from Fulbright, Go8 Future Research Leaders in Australia, SEMPRE UK, among others, and has been PI of multiple grants. He served as Vice-President of the National Neuroscience Society of Romania, and national representative in the Governing Council of the International Brain Research Organization, and has been in the editorial boards of several international journals including Emotion, Translational Neuroscience, Frontiers in Aging Neuroscience, and Scientific Reports. He has also initiated the Romanian Twin Registry. His latest book is Genes, Brain and Emotions: Interdisciplinary and Translational Perspectives, co-edited with K.-P. Lesch and J. R. Homberg, and published by Oxford University Press in 2019.
Aurora Szentágotai-Tătar Ph.D. is Professor of Clinical Psychology and Psychotherapy and Director of the Applied Clinical Psychology Laboratory at the Department of Clinical Psychology and Psychotherapy, Babeş-Bolyai University, Cluj-Napoca, Romania. She has an MA in Counselling and Psychotherapy, and a Ph.D. in Clinical Psychology. Her research is focused on the relation between emotion regulation and psychopathology, the impact of early life stress on mental health and well-being, and the efficacy of cognitive behavioral therapy. She is past editor-in-chief of the Journal of Cognitive and Behavioral Psychotherapies and serves on the editorial board of the Journal of Rational-Emotive & Cognitive-Behavior Therapy. She is Vice-president of the Romanian Association of Cognitive Behavioral Psychotherapies, fellow of the Albert Ellis Institute, and member of the International Institute for the Advanced Studies of Psychotherapy and Applied Mental Health. She is the recipient of the In Hoc Signo Vinces Award from the Romanian National Council for Research in Higher Education.
Róbert S. Balázsi Ph.D. is Associate Professor at the Babeş-Bolyai University, Department of Psychology, Cluj-Napoca, Romania. His research interests focus on applications of second-generation multivariate data analysis in psychological research, particularly on applications of structural equation modeling (SEM) in the analysis of factorial structures and the invariance of psychological measurement instruments with numerical and non-numerical indicators. He is also interested in the applications of advanced SEM models which extend the limits of statistical modeling, replacing traditional multivariate methods, such as MLSEM (multilevel structural equation modeling), MASEM (meta-analytic structural equation modeling), LCA (latent class analysis), or LSTM (latent state-trait modeling). In 2019 he was awarded the National Outstanding Educator Award for teaching behavioral research methods and data analysis at undergraduate and graduate levels. He also co-authored several textbooks on the topic.
Diana Nechita Ph.D. is Assistant Professor at the Department of Clinical Psychology and Psychotherapy, Babes-Bolyai University, Romania. Dr. Nechita’s research interests include emotion regulation, self-conscious emotions, evidence-based psychotherapies. Her primary research interests are in examining self-conscious emotions and their regulation in relation with psychopathology. She is particularly interested in how shame can be more effectively regulated. She examined shame as a shared vulnerability factor for eating and anxiety disorders, while also looking at the effect of self-compassion strategies on shame. Her current research involves the use of ecological momentary assessment and interventions in understanding the role of shame and its regulation in relation with disturbed eating behaviors.
Ioana Bunea M. A. is a Doctoral Candidate in the Cognitive Neuroscience Laboratory, Department of Psychology, Babeş-Bolyai University, Cluj-Napoca, CJ, Romania. Her work has focused on the long-term psychological impact of childhood adversity, particularly in the domains of emotion regulation and sensitivity to social rejection.
Seth David Pollak is the Vaughan Bascom Distinguished Professor of Psychology at the University of Wisconsin-Madison. He holds dual Ph.D.s in Brain & Cognitive Sciences and Child Clinical Psychology. His research has deepened our understanding of children’s emotional development — not only in terms of how the developing brain makes emotional behavior possible, but also how emotional experiences in childhood, such as adversity and stress, influences development of the brain. Dr. Pollak has been the recipient of the Boyd-McCandless Award for Distinguished Contributions to Child Development, the American Psychological Association’s Distinguished Early Career Award, the APS James McKeen Cattell Sabbatical Award, as well as the Chancellor’s Distinguished Teaching Award from the University of Wisconsin. He is a Fellow of the American Association for the Advancement of Science, the Association for Psychological Science, the American Academy of Arts and Sciences, and a Guggenheim Fellow.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest
All authors declare that they have no conflicts of interest.
References
Studies included in the meta-analysis are indicated in the Supplementary Materials.
- Aldao A, Gee DG, De Los Reyes A, & Seager I (2016). Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Development and Psychopathology, 28(4), 927–946. doi: 10.1017/s0954579416000638 [DOI] [PubMed] [Google Scholar]
- Aldao A, & Nolen-Hoeksema S (2010). Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behaviour Research and Therapy, 48(10), 974–983. doi: 10.1016/j.brat.2010.06.002 [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S, & Schweizer S (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. doi: 10.1016/j.cpr.2009.11.004 [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, & Cicchetti D (2019). Emotion dysregulation and emerging psychopathology: A transdiagnostic, transdisciplinary perspective. Development and Psychopathology, 31(3), 799–804. doi: 10.1017/s0954579419000671 [DOI] [PubMed] [Google Scholar]
- Bilc MI, Vulturar R, Chis A, Buciuman M, Nutu D, Bunea I, … Miu AC (2018). Childhood trauma and emotion regulation: The moderator role of BDNF Val66Met. Neuroscience Letters, 685, 7–11. doi: 10.1016/j.neulet.2018.07.018 [DOI] [PubMed] [Google Scholar]
- Birn RM, Roeber BJ, & Pollak SD (2017). Early childhood stress exposure, reward pathways, and adult decision making. Proceedings of the National Academy of Sciences of the United States of America, 114(51), 13549–13554. doi: 10.1073/pnas.1708791114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boker S, Neale M, Maes H, Wilde M, Spiegel M, Brick T, … Fox J (2011). OpenMx: An open source extended structural equation modeling framework. Psychometrika, 76(2), 306–317. doi: 10.1007/s11336-010-9200-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheung MWL (2015). Meta-analysis: A structural equation modeling approach. Chichester, UK: John Wiley & Sons. [Google Scholar]
- Cheung MWL, & Chan W (2005). Meta-analytic structural equation modeling: A two-stage approach. Psychological Methods, 10(1), 40–64. doi: 10.1037/1082-989x.10.1.40 [DOI] [PubMed] [Google Scholar]
- Cheung MWL, & Chan W (2009). A two-stage approach to synthesizing covariance matrices in meta-analytic structural equation modeling. Structural Equation Modeling-a Multidisciplinary Journal, 16(1), 28–53. doi: 10.1080/10705510802561295 [DOI] [Google Scholar]
- Cole PM, Michel MK, & Teti LO (1994). The development of emotion regulation and dysregulation: A clinical perspective. Monographs of the Society for Research in Child Development, 59(2-3), 73–100. [PubMed] [Google Scholar]
- Compas BE, Jaser SS, Bettis AH, Watson KH, Gruhn MA, Dunbar JP, …Thigpen JC (2017). Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological Bulletin, 143(9), 939–991. doi: 10.1037/bul0000110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Jaser SS, Dunbar JP, Watson KH, Bettis AH, Gruhn MA, & Williams EK (2014). Coping and emotion regulation from childhood to early adulthood: Points of convergence and divergence. Australian Journal of Psychology, 66(2), 71–81. doi: 10.1111/ajpy.12043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, …Fein JA (2015). Adverse childhood experiences: Expanding the concept adversity. American Journal of Preventive Medicine, 49(3), 354–361. doi: 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- D’Avanzato C, Joormann J, Siemer M, & Gotlib IH (2013). Emotion regulation in depression and anxiety: Examining diagnostic specificity and stability of strategy use. Cognitive Therapy and Research, 37(5), 968–980. doi: 10.1007/s10608-013-9537-0 [DOI] [Google Scholar]
- den Kelder RO, Van den Akker AL, Geurts HM, Lindauer RJL, & Overbeek G (2018). Executive functions in trauma-exposed youth: a meta-analysis. European Journal of Psychotraumatology, 9(1). doi: 10.1080/20008198.2018.1450595 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennison MJ, Rosen ML, Sambrook KA, Jenness JL, Sheridan MA, & McLaughlin KA (2019). Differential associations of distinct forms of childhood adversity with neurobehavioral measures of reward processing: A developmental pathway to depression. Child Development, 90(1), e96–e113. doi: 10.1111/cdev.13011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dillon DG, Holmes AJ, Birk JL, Brooks N, Lyons-Ruth K, & Pizzagalli DA (2009). Childhood adversity is associated with left basal ganglia dysfunction during reward anticipation in adulthood. Biological Psychiatry, 66(3), 206–213. doi: 10.1016/j.biopsych.2009.02.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn EC, Nishimi K, Gomez SH, Powers A, & Bradley B (2018). Developmental timing of trauma exposure and emotion dysregulation in adulthood: Are there sensitive periods when trauma is most harmful? Journal of Affective Disorders, 227, 869–877. doi: 10.1016/j.jad.2017.10.045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dvir Y, Ford JD, Hill M, & Frazier JA (2014). Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harvard Review of Psychiatry, 22(3), 149–161. doi: 10.1097/Hrp.0000000000000014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehring T, & Quack D (2010). Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Behavior Therapy, 41(4), 587–598. doi: 10.1016/j.beth.2010.04.004 [DOI] [PubMed] [Google Scholar]
- Enders CK (2010). Applied missing data analysis. New York: Guilford Press. [Google Scholar]
- Finkelhor D, Shattuck A, Turner H, & Hamby S (2015). A revised inventory of Adverse Childhood Experiences. Child Abuse & Neglect, 48, 13–21. doi: 10.1016/j.chiabu.2015.07.011 [DOI] [PubMed] [Google Scholar]
- Fritz MS, & Mackinnon DP (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. doi: 10.1111/j.1467-9280.2007.01882.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gignac GE, & Szodorai ET (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. doi: 10.1016/j.paid.2016.06.069 [DOI] [Google Scholar]
- Gratz KL, & Roemer L (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. doi: 10.1023/B:Joba.0000007455.08539.94 [DOI] [Google Scholar]
- Gratz KL, & Tull MT (2010). Emotion regulation as a mechanism of change in acceptance- and mindfulness-based treatments. In Baer RA (Ed.), Assessing mindfulness and acceptance processes in clients: Illuminating the theory and practice of change (pp. 107–133). Oakland, CA, US: New Harbinger Publications. [Google Scholar]
- Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: Associations with first onset of DSM-IV disorders. Archives of General1 Psychiatry, 67(2), 113–123. doi: 10.1001/archgenpsychiatry.2009.186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross JJ (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271–299. doi: 10.1037/1089-2680.2.3.271 [DOI] [Google Scholar]
- Gross JJ (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. doi: 10.1080/1047840x.2014.940781 [DOI] [Google Scholar]
- Gross JJ, & Jazaieri H (2014). Emotion, emotion regulation, and psychopathology: An affective science perspective. Clinical Psychological Science 2(4), 387–401. doi: 10.1177/2167702614536164 [DOI] [Google Scholar]
- Gross JJ, & John OP (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. doi: 10.1037/0022-3514.85.2.348 [DOI] [PubMed] [Google Scholar]
- Gruhn MA, & Compas BE (2020). Effects of maltreatment on coping and emotion regulation in childhood and adolescence: A meta-analytic review. Child Abuse & Neglect, 103. doi: 10.1016/j.chiabu.2020.104446 [DOI] [PubMed] [Google Scholar]
- Harms MB, Bowen KES, Hanson JL, & Pollak SD (2018). Instrumental learning and cognitive flexibility processes are impaired in children exposed to early life stress. Developmental Science, 21(4). doi: 10.1111/desc.12596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes SC, Strosahl K, Wilson KG, Bissett RT, Pistorello J, Toarmino D, … McCurry SM (2004). Measuring experiential avoidance: A preliminary test of a working model. Psychological Record, 54(4), 553–578. doi: 10.1007/Bf03395492 [DOI] [Google Scholar]
- Higgins JP, & Green S (2008). Cochrane handbook for systematic reviews of interventions:. The Cochrane Collaboration [Google Scholar]
- Higgins JP, & Thompson SG (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21(11), 1539–1558. doi: 10.1002/sim.1186 [DOI] [PubMed] [Google Scholar]
- Hilt LM, Leitzke BT, & Pollak SD (2017). Can’t take my eyes off of you: Eye tracking reveals how ruminating young adolescents get stuck. Journal of Clinical Child and Adolescent Psychology, 46(6), 858–867. doi: 10.1080/15374416.2015.1121824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilt LM, & Pollak SD (2012). Getting out of rumination: Comparison of three brief interventions in a sample of youth. Journal of Abnormal Child Psychology, 40(7), 1157–1165. doi: 10.1007/s10802-012-9638-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilt LM, & Pollak SD (2013). Characterizing the ruminative process in young adolescents. Journal of Clinical Child and Adolescent Psychology, 42(4), 519–530. doi: 10.1080/15374416.2013.764825 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoppen TH, & Chalder T (2018). Childhood adversity as a transdiagnostic risk factor for affective disorders in adulthood: A systematic review focusing on biopsychosocial moderating and mediating variables. Clinical Psychology Review, 65, 81–151. doi: 10.1016/j.cpr.2018.08.002 [DOI] [PubMed] [Google Scholar]
- Hu T, Zhang D, Wang J, Mistry R, Ran G, & Wang X (2014). Relation between emotion regulation and mental health: A meta-analysis review. Psychological Reports, 114(2), 341–362. doi: 10.2466/03.20.PR0.114k22w4 [DOI] [PubMed] [Google Scholar]
- Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F, & Botella J (2006). Assessing heterogeneity in meta-analysis: Q statistic or I-2 index? Psychological Methods, 11(2), 193–206. doi: 10.1037/1082-989x.11.2.193 [DOI] [PubMed] [Google Scholar]
- Jaffee SR (2017). Child maltreatment and risk for psychopathology in childhood and adulthood. Annual Review of Clinical Psychology, 13, 525–551. doi: 10.1146/annurev-clinpsy-032816-045005 [DOI] [PubMed] [Google Scholar]
- Jak S (2015). Meta-analytic structural equation modelling. Dordrecht, Netherlands: Springer. [Google Scholar]
- John OP, & Eng J (2014). Three approaches to individual differences in affect regulation: Conceptualizations, measures, and findings. In Gross JJ (Ed.), Handbook of emotion regulation (pp. 321–345). New York, NY, US: Guilford Press. [Google Scholar]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, … Williams DR (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. British Journal of Psychiatry, 197(5), 378–385. doi: 10.1192/bjp.bp.110.080499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiel EJ, & Kalomiris AE (2015). Current themes in understanding children’s emotion regulation as developing from within the parent–child relationship. Current Opinion in Psychology, 3, 11–16. doi: 10.1016/j.copsyc.2015.01.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim J, & Cicchetti D (2010). Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. Journal of Child Psychology and Psychiatry, 51(6), 706–717. doi: 10.1111/j.l469-7610.2009.02202.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kring AM (2008). Emotion disturbances as transdiagnostic processes in psychopathology. In Lewis M, Haviland-Jones JM, & Feldman-Barrett L (Eds.), Handbook of emotion (3rd ed., pp. 691–705). New York, NY, US: Guilford Press. [Google Scholar]
- Lavi L, Katz LF, Ozer EJ, & Gross JJ (2019). Emotion reactivity and regulation in maltreated children: A meta-analysis. Child Development, 90(5), 1503–1524. doi: 10.1111/cdev.13272 [DOI] [PubMed] [Google Scholar]
- Lavi I, Manor-Binyamini I, Seibert E, Katz LF, Ozer EJ, & Gross JJ (2019). Broken bonds: A meta-analysis of emotion reactivity and regulation in emotionally maltreating parents. Child Abuse & Neglect, 88, 376–388. doi: 10.1016/j.chiabu.2018.11.016 [DOI] [PubMed] [Google Scholar]
- Lavi I, Ozer EJ, Katz LF, & Gross JJ (2021). The role of parental emotion reactivity and regulation in child maltreatment and maltreatment risk: A meta-analytic review. Clinical Psychology Review, 90, 102099. doi: 10.1016/j.cpr.2021.102099 [DOI] [PubMed] [Google Scholar]
- Lazarus RS, & Folkman S (1984). Stress, appraisal, and coping. New York: Springer. [Google Scholar]
- LeBlanc S, Uzun B, Aydemir A, & Mohiyeddini C (2020). Validation of an emotion regulation training program on mental well-being. Psychological Reports, 123(5), 1518–1536. doi: 10.1177/0033294119878399 [DOI] [PubMed] [Google Scholar]
- Leitenberg H, Greenwald E, & Cado S (1992). A retrospective study of long-term methods of coping with having been sexually abused during childhood. Child Abuse & Neglect, 16(3), 399–407. doi: 10.1016/0145-2134(92)90049-w [DOI] [PubMed] [Google Scholar]
- Liu JJW, Ein N, Gervasio J, & Vickers K (2019). The efficacy of stress reappraisal interventions on stress responsivity: A meta-analysis and systematic review of existing evidence. Plos One, 14(2). doi: 10.1371/journal.pone.0212854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lupien SJ, McEwen BS, Gunnar MR, & Heim C (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, 10(6), 434–445. doi: 10.1038/nrn2639 [DOI] [PubMed] [Google Scholar]
- Luterek JA, Orsillo SM, & Marx BP (2005). An experimental examination of emotional experience, expression, and disclosure in women reporting a history of childhood sexual abuse. Journal of Traumatic Stress, 18(3), 237–244. doi: 10.1002/jts.20027 [DOI] [PubMed] [Google Scholar]
- Madigan S, Cyr C, Eirich R, Fearon RMP, Ly A, Rash C, … Alink LRA (2019). Testing the cycle of maltreatment hypothesis: Meta-analytic evidence of the intergenerational transmission of child maltreatment. Development and Psychopathology, 31(1), 23–51. doi: 10.1017/S0954579418001700 [DOI] [PubMed] [Google Scholar]
- Mauss IB, Levenson RW, McCarter L, Wilhelm FH, & Gross JJ (2005). The tie that binds? Coherence among emotion experience, behavior, and physiology. Emotion, 5(2), 175–190. doi: 10.1037/1528-3542.5.2.175 [DOI] [PubMed] [Google Scholar]
- McCrory EJ, De Brito SA, & Viding E (2012). The link between child abuse and psychopathology: A review of neurobiological and genetic research. Journal of the Royal Society of Medicine, 105(4), 151–156. doi: 10.1258/jrsm.2011.110222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrory EJ, & Viding E (2015). The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder. Development and Psychopathology, 27(2), 493–505. doi: 10.1017/s0954579415000115 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA (2016). Future directions in childhood adversity and youth psychopathology. Journal of Clinical Child and Adolescent Psychology, 45(3), 361–382. doi: 10.1080/15374416.2015.1110823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRae K, Jacobs SE, Ray RD, John OP, & Gross JJ (2012). Individual differences in reappraisal ability: Links to reappraisal frequency, well-being, and cognitive control. Journal of Research in Personality, 46(1), 2–7. doi: 10.1016/j.jrp.2011.10.003 [DOI] [Google Scholar]
- Milojevich HM, Machlin L, & Sheridan MA (2020). Early adversity and children’s emotion regulation: Differential roles of parent emotion regulation and adversity exposure. Development and Psychopathology, 32(5), 1788–1798. doi: 10.1017/S0954579420001273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miu AC, Carnuta M, Bilc M, Szekely RD, Vulturar R, Chis A, … Gross JJ (2016). Differential susceptibility in emotion regulation: BDNF Val66Met moderates the effects of childhood adversity on reappraisal. Genes, Brain and Behavior, 16(4), 419–426. [DOI] [PubMed] [Google Scholar]
- Morris AS, Criss MM, Silk JS, & Houltberg BJ (2017). The impact of parenting on emotion regulation during childhood and adolescence. Child Development Perspectives, 11(4), 233–238. doi: 10.1111/cdep.12238 [DOI] [Google Scholar]
- Nanni V, Uher R, & Danese A (2012). Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: A meta-analysis. American Journal of Psychiatry, 169(2), 141–151. doi: 10.1176/appi.ajp.2011.11020335 [DOI] [PubMed] [Google Scholar]
- Neale MC, & Miller MB (1997). The use of likelihood-based confidence intervals in genetic models. Behavior Genetics, 27(2), 113–120. doi: 10.1023/a:1025681223921 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100(4). doi: 10.1037/0021-843X.100.4.569 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S (2004). The response styles theory. In Papageorgiou C & Wells A (Eds.), Depressive Rumination: Nature, Theory and Treatment (Vol. 107, pp. 107–124). Chichester, UK: John Wiley & Sons. [Google Scholar]
- Oltean LE, Miu AC, & Szentágotai-Tătar A (2022). Childhood adversity and impaired reward processing: A meta-analysis. Child Abuse & Neglect. [DOI] [PubMed] [Google Scholar]
- Osborne KR, Duprey EB, O’Brien Caughy M, & Oshri A (2021). Parents’ maltreatment histories, dimensions of emotion regulation, and connections to offspring self-regulation A sex-specific transmission pathway. Journal of Psychopathology and Behavioral Assessment, doi: 10.1007/s10862-021-09881-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson RA, & Brown SP (2005). On the use of beta coefficients in meta-analysis. Journal of Applied Psychology, 90(1), 175–181. doi: 10.1037/0021-9010.90.1.175 [DOI] [PubMed] [Google Scholar]
- Pitur S, & Miu AC (2020). Childhood maltreatment and expressive flexibility: Specific effects of threat and deprivation? Cognition & Emotion, 1–8. doi: 10.1080/02699931.2020.1795625 [DOI] [PubMed] [Google Scholar]
- Plate RC, Bloomberg Z, Bolt DM, Bechner AM, Roeber BJ, & Pollak SD (2019). Abused children experience high anger exposure. Frontiers in Psychology, 10, 440. doi: 10.3389/fpsyg.2019.00440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prefit AB, Candea DM, & Szentagotai-Tatar A (2019). Emotion regulation across eating pathology: A meta-analysis. Appetite, 143, 104438. doi: 10.1016/j.appet.2019.104438 [DOI] [PubMed] [Google Scholar]
- Renna ME, Quintero JM, Fresco DM, & Mennin DS (2017). Emotion regulation therapy: A mechanism-targeted treatment for disorders of distress. Frontiers in Psychology, 8. doi: 10.3389/fpsyg.2017.00098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodman AM, Jenness JL, Weissman DG, Pine DS, & McLaughlin KA (2019). Neurobiological markers of resilience to depression following childhood maltreatment: The role of neural circuits supporting the cognitive control of emotion. Biological Psychiatry, 86(6), 464–473. doi: 10.1016/j.biopsych.2019.04.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruba AL, & Pollak SD (2020). Children’s emotion inferences from masked faces: Implications for social interactions during COVID-19. Plos One, 15(12). doi: 10.1371/journal.pone.0243708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saunders BE, & Adams ZW (2014). Epidemiology of traumatic experiences in childhood. Child and Adolescent Psychiatric Clinics of North America, 23(2), 167–184. doi: 10.1016/j.chc.2013.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seligowski AV, Lee DJ, Bardeen JR, & Orcutt HK (2015). Emotion regulation and posttraumatic stress symptoms: a meta-analysis. Cognitive Behavior Therapy, 44(2), 87–102. doi: 10.1080/16506073.2014.980753 [DOI] [PubMed] [Google Scholar]
- Shaw ZA, Hilt LM, & Starr LR (2019). The developmental origins of ruminative response style: An integrative review. Clinical Psychology Review, 74. doi: 10.1016/j.cpr.2019.101780 [DOI] [PubMed] [Google Scholar]
- Sheppes G (2020). Transcending the “good & bad” and “here & now” in emotion regulation: Costs and benefits of strategies across regulatory stages. Advances in Experimental Social Psychology, 61, 185–236. doi: 10.1016/bs.aesp.2019.09.003 [DOI] [Google Scholar]
- Sheppes G, & Meiran N (2007). Better late than never? On the dynamics of online regulation of sadness using distraction and cognitive reappraisal. Personality and Social Psychology Bulletin, 33(11), 1518–1532. doi: 10.1177/0146167207305537 [DOI] [PubMed] [Google Scholar]
- Sheppes G, Scheibe S, Suri G, & Gross JJ (2011). Emotion-regulation choice. Psychological Science, 22(11), 1391–1396. doi: 10.1177/0956797611418350 [DOI] [PubMed] [Google Scholar]
- Sheppes G, Suri G, & Gross JJ (2015). Emotion regulation and psychopathology. Annual Review of Clinical Psychology, Vol 11, 11, 379–405. doi: 10.1146/annurev-clinpsy-032814-112739 [DOI] [PubMed] [Google Scholar]
- Shields AM, & Cicchetti D (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27(4), 381–395. doi: 10.1207/s15374424jccp2704_2 [DOI] [PubMed] [Google Scholar]
- Shrout PE, & Bolger N (2002). Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods, 7(4), 422–445. [PubMed] [Google Scholar]
- Smith KE, & Pollak SD (2020). Rethinking concepts and categories for understanding the neurodevelopmental effects of childhood adversity. Perspectives on Psychological Science. doi: 10.1177/1745691620920725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith KE, & Pollak SD (2021). Early life stress and neural development: Implications for understanding the developmental effects of COVID-19. Cognitive Affective and Behavioral Neuroscience. doi: 10.3758/s13415-021-00901-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson KL, Hannan SM, & Miron LR (2014). Fight, flight, and freeze: Threat sensitivity and emotion dysregulation in survivors of chronic childhood maltreatment. Personality and Individual Differences, 69, 28–32. doi: 10.1016/j.paid.2014.05.005 [DOI] [Google Scholar]
- Thompson RA (1994). Emotion regulation: A theme in search of definition. Monographs of the Society for Research in Child Development, 59(2-3), 25–52. [PubMed] [Google Scholar]
- Thompson RA, & Goodman M (2010). Development of emotion regulation: More than meets the eye. In Kring AM & Sloan DM (Eds.), Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment (pp. 38–58). New York, NY: The Guilford Press. [Google Scholar]
- Thornberry TP, Knight KE, & Lovegrove PJ (2012). Does maltreatment beget maltreatment? A systematic review of the intergenerational literature. Trauma Violence & Abuse, 13(3), 135–152. doi: 10.1177/1524838012447697 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treynor W, Gonzalez R, & Nolen-Hoeksema S (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27(3), 247–259. doi: 10.1023/A:1023910315561 [DOI] [Google Scholar]
- Yasinski C, Hayes AM, & Laurenceau JP (2016). Rumination in everyday life: The influence of distancing, immersion, and distraction. Journal of Experimental Psychopathology, 7(2), 225–245. doi: 10.5127/jep.042714 [DOI] [Google Scholar]
- Zimmer-Gembeck MJ, & Skinner EA (2011). The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development, 35(1), 1–17. doi: 10.1177/0165025410384923 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.