

Abstract
Nipple pain is a common reason for premature cessation of breastfeeding. Despite the benefits of breastfeeding for both infant and mother, clinical support for problems such as maternal nipple pain remains a research frontier. Maternal pharmaceutical treatments, and infant surgery and bodywork interventions are commonly recommended for lactation-related nipple pain without evidence of benefit. The pain is frequently attributed to mammary dysbiosis, candidiasis, or infant anatomic anomaly (including to diagnoses of posterior or upper lip-tie, high palate, retrognathia, or subtle cranial nerve abnormalities). Although clinical protocols universally state that improved fit and hold is the mainstay of treatment of nipple pain and wounds, the biomechanical parameters of pain-free fit and hold remain an omitted variable bias in almost all clinical breastfeeding research. This article reviews the research literature concerning aetiology, classification, prevention, and management of lactation-related nipple–areolar complex (NAC) pain and damage. Evolutionary and complex systems perspectives are applied to develop a narrative synthesis of the heterogeneous and interdisciplinary evidence elucidating nipple pain in breastfeeding women. Lactation-related nipple pain is most commonly a symptom of inflammation due to repetitive application of excessive mechanical stretching and deformational forces to nipple epidermis, dermis and stroma during milk removal. Keratinocytes lock together when mechanical forces exceed desmosome yield points, but if mechanical loads continue to increase, desmosomes may rupture, resulting in inflammation and epithelial fracture. Mechanical stretching and deformation forces may cause stromal micro-haemorrhage and inflammation. Although the environment of the skin of the nipple–areolar complex is uniquely conducive to wound healing, it is also uniquely exposed to environmental risks. The two key factors that both prevent and treat nipple pain and inflammation are, first, elimination of conflicting vectors of force during suckling or mechanical milk removal, and second, elimination of overhydration of the epithelium which risks moisture-associated skin damage. There is urgent need for evaluation of evidence-based interventions for the elimination of conflicting intra-oral vectors of force during suckling.
Keywords: biomechanics, breastfeeding, infant suck, lactation, mechanobiological model, nipple damage, nipple pain, vasospasm, white spots
Introduction
Despite the known benefits of breastfeeding for both infant and mother, 1 interventions for clinical problems, such as breast inflammation and pain remain a research frontier.2,3 Overuse of pharmaceutical and surgical interventions is an increasingly serious international problem in health care.4,5 Both patients and clinicians typically overestimate the benefits of medical interventions and underestimate potential harms.6 –8 It is not surprising then, given the relative lack of research into clinical breastfeeding support, that overmedicalization and overtreatment is widespread in the care of breastfeeding women and their babies when inflammation, pain, and visible damage of the nipple–areolar complex emerge.9 –16
This is the third of three articles which consider aetiology, classification, and management of benign lactation-related inflammatory conditions of the breast. The first article focuses on breast alveoli, ducts, and stroma to propose a new mechanobiological model, in which excessive intra-luminal pressures trigger inter-lactocyte tight junction disruption and basement membrane rupture, which trigger inflammatory cascades and alveolar apoptosis. 17 The second article builds on this mechanobiological model to re-think classification, prevention, and management of the range of breast inflammations commonly known as engorgement, blocked ducts, phlegmon, subacute mastitis, mastitis, and abscess. 18
This third article addresses the common lactation-related problem of pain of the nipple–areolar complex, including of the nipple stroma (i.e. structural connective tissue of the mammary papilla in which vasculature, ducts, and nerve fibres are embedded). It does not aim to address all nipple–areolar complex pathology that may present during lactation. Clinicians should maintain a high index of suspicion for viral infection (in particular, herpes simplex and also herpes zoster viruses) in breastfeeding women with nipple pain (Box 1).
Box 1.
Viral infection of the nipple–areolar complex in the lactating breast: a rare but important condition.
| Herpes simplex virus (HSV) on the nipple or breast may present as a small or imperceptible vesicle on an erythematous base which ulcerates, associated with axillary lymph node enlargement. HSV may also present as a cluster of vesicles or ulcers on the nipple or breast, particularly during a primary outbreak.19–21 The lesions shed virus, and any contact with HSV during the first weeks and months of life may implicate the infant’s central nervous system, and prove fatal.
22
Clinicians should maintain a high index of suspicion for HSV in breastfeeding women with nipple pain. If a lactating woman or her family members have had a herpes outbreak, whether type 1 or 2, and she presents with unilateral nipple pain, a polymerase chain reaction (PCR) viral swab should be analysed, and the breast should be covered and kept away from the baby. Acyclovir or valacyclovir is prescribed, which is safe to use while breastfeeding, hastening resolution and decreasing viral shedding. Pumped milk should be discarded from that breast, and good hand-washing and pump-cleansing hygiene practised.23,24 Varicella zoster may present as a cluster of painful vesicles across the chest and breast. Herpes zoster infection can be fatal in a newborn. If lesions are not on the breast, breastfeeding should continue with lesions covered. If the lesions are on the breast, the infant should not be fed from that side and pumped milk discarded. If a mother experiences a herpes zoster outbreak within 48 h after birth, the infant should not breastfeed. Although antibodies pass through the milk, the infant also requires zoster immune globulin treatment. Antivirals are prescribed, as for HSV infection. |
The evolutionary and complex systems approach to lactation-related breast inflammation detailed in this three-part series forms part of the foundational breastfeeding domain of the programmes known as Neuroprotective Developmental Care (NDC or ‘the Possums programs’). 25 The NDC breastfeeding domain also includes the gestalt biomechanical model of infant suck and its clinical translation into the gestalt method of fit and hold (also referred to as ‘latch and positioning’).9,26,27 NDC has been developed and delivered in Australia since 2011. NDC synthesizes the latest evidence concerning early life care across the interrelated and interacting domains of breastfeeding, cry-fuss problems, infant sleep, and parental mood applying evolutionary and complex systems frames, and translates this synthesis into clinical practice. The breastfeeding domain is foundational, influencing each other domain.13,28 –35
Prevalence of lactation-related nipple pain and damage
Nipple pain is one of the most common reasons for introducing formula or ceasing breastfeeding.36,37 In Li et al.’s 38 study of 1323 mothers in the United States, more than a quarter stopped breastfeeding in the first month postpartum; 29.3% cited pain and 36.8% cited sore, cracked, or bleeding nipples as an important reason.
Nipple pain, with or without visible damage, occurs most often in the first-week post-birth. In 2014, Buck et al. 39 found that 79% of 317 first-time breastfeeding Australian mothers experienced nipple pain by the time they were discharged home after birth of their baby, despite being motivated to breastfeed, well-educated, and in a ‘Baby Friendly’ accredited institution with extensive postnatal support. A 2021 study of 58 Spanish women found that 97% experienced nipple soreness at 48 h postpartum, and a higher pain score was associated with skin-to-skin contact lasting more than two uninterrupted hours in the immediate postpartum. 40 A 2014 Cochrane review concluded that nipple pain reduced to mild levels 7–10 days after birth for a majority of breastfeeding women, regardless of treatment used. 41
Unfortunately, it is not possible to know which women will go on to develop persistent nipple pain and damage. In a 2020 online survey of 1084 women in the United Kingdom who had finished breastfeeding in the past 2 years, 76% reported having experienced latch-related nipple pain at some time. 42
Over half of women with nipple pain develop visible damage or wounds. Visible signs include blisters, bruises, erythema, oedema, cracks or fissures, ulcers, and exudate. These visible signs of damage are associated with increased pain. 43 Using the Numeric Rating Scale of 0–10, women with nipple damage reported a mean score of 6.2 in the first week and 5.8 after that period; women without visible damage reported a mean of 2.7. 44
Even at 8 weeks post-birth in Buck et al.’s 39 study, 20% of 340 respondents reported current nipple pain and 8% current nipple damage; 58% reported experiencing nipple pain at some time post-birth. In 2015, an audit of the Western Australia Breastfeeding Centre found that 36% of 1177 consultations by International Board Certified Lactation Consultants (IBCLCs) were for nipple pain. 45
Large studies suggest that nipple pain occurs more commonly in Australia, the United States, and the United Kingdom than in other parts of the world, such as Brazil, Denmark, South Africa, or Peru, emphasizing the importance of environmental factors.45 –50 To give an example of possible environmental variables, a popularly taught fit and hold strategy (shaping the breast with cross-cradle hold) is associated with a fourfold increase in nipple pain. 51 Method of fit and hold intervention remains an omitted variable bias in most nipple pain studies, typically alluded to without clarification under a statement that the participant received IBCLC support.
Lactation-related nipple pain predisposes to other conditions
Nipple pain is a distressing sensory and emotional experience which interferes with maternal mood, activity, and sleep, whether or not there is visible damage. Not surprisingly, it also predisposes to postnatal depression.43,52,53
Nipple pain is linked with an increased risk of breast inflammation (e.g. engorgement and mastitis). 54 Building on the mechanobiological model of breast inflammation detailed in the first article of this series, 17 this article hypothesizes that the conflicting intra-oral vectors of force which result in nipple pain and inflammation also compress lactiferous ducts, resulting in elevated intra-luminal backpressures and increased risk of breast inflammation. That is, the link between nipple pain and breast inflammation is associative, not causative.
Even without visible trauma, nipple pain is associated with low supply.45,55 Some hypothesize that this is because nipple pain disrupts sensory nerve signals from the nipple to the hypothalamus, impairing oxytocin release, and milk ejection. 56 However, there is no evidence that pain is causally linked to decreased oxytocin levels or less effective and less frequent milk ejections.
Instead, this article hypothesizes that two factors explain the association between low milk production and nipple pain. First, women experiencing pain with breastfeeds are more likely to restrict breastfeeding frequency, which downregulates milk production. Second, the same conflicting intra-oral vectors of force, which result in nipple inflammation and pain also compress lactiferous ducts and impair milk transfer, downregulating milk production.9,17,18,26,27 This is corroborated by the finding that infants whose mothers have nipple pain may transfer less milk (Box 2).57,58
Box 2.
Analysis of ultrasound and vacuum studies corroborates the mechanobiological model of nipple pain in breastfeeding.
| In 2008, Geddes et al. investigated 24 Australian infants diagnosed with ankyloglossia in the presence of breastfeeding problems, though definitions and assessment criteria for ankyloglossia were not stipulated. Some of their mothers were found by ultrasound to have a narrowing at the base of the intra-oral nipple and breast tissue during suckling; others to have narrowing of the tip of the nipple. These changes were not associated with difference in reports of maternal pain and resolved overall in both groups immediately post-scissors frenotomy, also associated with immediate decrease in self-reports of maternal pain. When interpreted through the lens of the mechanobiological model of nipple pain in breastfeeding, this study shows that infants with breastfeeding problems resulting in maternal nipple pain had difficulty achieving adequate intra-oral breast tissue volumes due to conflicting intra-oral vectors of force (or breast tissue drag) and positional instability. From the perspective of the mechanobiological model, the variable pattern of nipple and breast tissue expansion or narrowing is more likely to reflect differences in nipple and breast tissue elasticity as the intra-oral breast tissue responds to excessively high stretching mechanical loads, rather than differences in tongue movement. Pain scores may decrease immediately after scissors frenotomy due to the infant’s sympathetic nervous system reaction and the change in fit and hold which result when a mother and baby are exposed to an environmental stressor (e.g. frenotomy), though these factors remain an omitted variable bias in existing research.
59
In 2008, McClellan et al. compared intra-oral vacuums in the babies of 30 Australian women breastfeeding successfully without nipple pain, with 30 who had pain despite having received unspecified IBCLC interventions. Infants in the pain group applied significantly higher baseline and peak vacuums, and transferred less milk despite similar sucking times. Pausing at the breast occurred for about a quarter of the feed in both groups, but infants in the pain group applied significantly higher vacuums when pausing. 57 McClellan et al. (2015) compared 25 Australian breastfeeding women who had received IBCLC interventions without resolution of their persistent nipple pain, with 25 breastfeeding successfully without pain. 58 Infants with ankyloglossia were excluded, without clarification of assessment criteria. Baseline vacuums were almost twice as high in the pain group, with significantly higher peak vacuums. These findings corroborated the lead author’s 2008 study, above. The vacuum in the pain group was stronger than the maximum comfortable pumping vacuum measured for women who were successfully breastfeeding with no pain. 60 The study also found a (statistically insignificant) trend to slower milk transfer in the pain group, consistent with the decreased milk transfer identified in women with nipple pain in 2008. The authors conclude that higher vacuums are not associated with increased milk transfer. This is consistent with the mechanobiological hypothesis that conflicting intra-oral vectors of force cause nipple pain, excessively high vacuums, and ductal compression. 58 Pain group infants showed less expansion of the middle section of the intra-oral nipple and breast tissue, and no expansion at the base, consistent with increased mechanical stretching caused by an conflicting intra-oral vector of force which conflicts with the direction of vacuum application. The finding of decreased depth of intra-oral space when the mandible and tongue are down in the pain group is also consistent with increased stretching of intra-oral breast tissue resulting from conflicting intra-oral vectors of force (or breast tissue drag), and with decreased intra-oral breast tissue volume. 58 The average distance between the nipple tip and the junction of the hard and soft palate (NHSPJ) was about the same between the pain and control groups. A 2021 review proposed that this finding suggests increased breast tissue in the infant’s mouth may not be of benefit for breastfeeding-related pain. 55 However, because the NHSPJ is just one indicator of decreased intra-oral breast tissue surface area and volume; other indicators are the decreased diameter of the intra-oral nipple and breast tissue, and decreased depth of intra-oral space. In addition to the fundamental and dynamic impact of fit and hold on intra-oral biomechanics, factors such as nipple and breast tissue elasticity are likely to play a role in the infant’s capacity to optimize intra-oral breast tissue volume. Interpreted from the perspective of the mechanobiological model, these ultrasound and vacuum studies of breastfeeding pairs demonstrate the effect of conflicting intra-oral vectors of force as infants reflexly attempt to optimize intra-oral breast tissue volume. Infants generate higher baseline and peak vacuums to hold breast tissue in their mouths when the force of gravity drags the breast in a different direction, resulting in nipple pain and damage. 57 |
IBCLC: International Board Certified Lactation Consultant; NHSPJ: distance from the nipple tip to the junction of the hard and soft palate.
The lactating nipple–areolar complex is characterized by unique protective factors and unique exposure to risks relative to other human skin sites
The following key protective systems interact in the skin of the lactating nipple–areolar complex to maintain health and homeostasis (Appendix 1):
Host immune system.
Skin and milk microbiomes.
Adaptation to repeated mechanical loads (Box 3).
Wound-healing inflammation (Appendix 3).
Box 3.
Skin adapts to protect against mechanical forces.
| Skin deforms elastically in response to force or mechanical load, which occurs constantly in daily life, to protect against mechanical injury. Most human skin can be stretched to several times its initial size and yet return to its original genetically determined size and shape.
61
The weakest component of skin is the keratinocyte cell (Appendix 1). If there is a low level of mechanical stress, structures within the keratinocytes absorb the load, Desmosomes, which are the structural junctions linking keratinocytes, protect the integrity of keratinocytes by locking after a certain point of epithelial stretching, known as the ‘yield point’. That is, at the yield point, actomyosin contracts, activating catch bonds which help avoid epithelial fracture (Figure 1). 63 Skin has properties of plasticity which allow for progressive and permanent adaptation to mechanical forces applied over time. At first, mechanical stretching causes elongation of the skin in the direction of the acting forces, so that it thins. Then keratinocytes become more elongated and change their orientation to align along the direction of the load if it is applied repetitively, dissipating the load. 62 Skin has properties of plasticity which allow for progressive and permanent adaptation to mechanical forces applied over time. Mechanosensory processes respond to repeated or sustained external stress by strengthening desmosomes with more adhesion molecules. Mechanical stress also activates signal pathways which modulate gene expression, protein synthesis, and cellular growth. The skin develops a thickened epidermal layer as keratinocytes continue to elongate, divide, and proliferate in the direction of the force to alleviate stress within each cell, and stem cells migrate in, resulting in production of expanded skin tissue. More collagen is laid down in the dermal layer. When the surface area of skin increases, mechanical load is dissipated, strain applied at any one point decreases, and the risk of epithelial fracture is mitigated. Increased dermal collagen also protects against skin fracture.61,62,64 The inherent adaptivity of nipple–areolar complex skin in response to repetitive high mechanical loads may explain why women are particularly vulnerable to nipple pain and damage in the first week of breastfeeding, as their skin adapts. It also explains why women may report that their nipples visibly change over the course of lactation. |
The lactating nipple–areolar complex is characterized by unique protective factors and also exposed to unique risks, relative to other parts of human skin (Table 1). Applying this series’ mechanobiological model, prevention of and intervention for nipple pain and damage demand that innate protective factors are optimized, and risk factors minimized.
Table 1.
The lactating nipple–areolar complex is characterized by unique protective factors and unique exposure to risks relative to other human skin sites.
| Unique nipple–areolar complex risk | Unique nipple–areolar complex protective factor |
|---|---|
| Areolar sweat and mammary glands secrete more moisture than many other skin sites. | |
| Female nipple dermis has dense concentration of nociceptors (Appendix 1). | Female nipple dermis has dense concentration of nociceptors (Appendix 1). |
| Exposure to repetitive and frequent mechanical load from the negative pressure of suckling, applied perhaps 2–4 h in total during a 24-h period. | The nipple face has deep epithelial crevices and ridges, which enhance epithelial elasticity and distribute mechanical loads. Keratinocytes adapt to repetitive mechanical loads by: 1. Elongation 2. Changing orientation to align with direction of mechanical forces, and 3. Proliferation 64 (Box 3). |
| Exposure to excessively high stretching and deforming forces caused by conflicting intra-oral vectors of force during suckling or mechanical milk removal may result in epithelial and stromal inflammation, epithelial damage, and nociceptor stimulation.9,26,27 | Nipples are richly vascularized, resulting in unusually rapid transport of immune and wound-healing factors. A normal layer of nipple epidermis (not exposed to repeated micro-trauma and environmental humidity) may recover from damage in around 3 days, depending on depth of injury, compared to 7–10 days for damaged epidermis elsewhere on the skin. When there is exudate and necrotic eschar, cyclic mechanical stress under negative pressure exposes a nipple wound to repetitive debridement. |
| Lack of a subcutaneous layer exposes nipple stroma to the shearing and stretching effects of excessively high mechanical forces during suckling or mechanical milk removal, resulting in microvascular haemorrhages, an inflammatory cascade, and pain. | This article proposes that lack of subcutaneous layer has three evolutionary advantages: 1. Vacuum acts directly upon superficial lactiferous ducts without an added cushioning layer 2. Ductal dilation is optimized without the added intra-oral volume of subcutaneous tissue 3. The nipple achieves a firm and prominent shape with smooth muscle contraction. |
| Epithelial breaks due to exposure to excessively high mechanical forces are vulnerable to microbial overgrowth due to loss of the protective epithelial barrier. | Nipples are frequently bathed in human milk which contains myriad interacting immunoprotective factors, including the microbiome, metabolome, immune cells, and exosomes. Saliva, the infant oral microbiome, nipple skin, and breastmilk, including the milk microbiome interact to form the infant’s oral mucosal immune system (Box 4). 17 Infant saliva contains multiple interacting bactericidal, fungicidal, and immunoprotective factors. Bactericidal properities of infant saliva include pattern-recognition molecules that act as functional predecessors of antibodies, recruiting immune cells to defend against mucosal pathogens; antibacterial lysozyme; and histatins and polypeptide molecules that stimulate cell growth and kill bacteria and fungi, in particular Candida albicans. Histatins also stimulate keratinocyte and fibroblast migration, angiogenesis, and enhance the re-epithelialization of a wounded area.65–67 The growth of micro-organisms is inhibited by breastmilk alone and more so when infant saliva is mixed with breast milk, with synergistic bactericidal effects. |
| Bras and breast pads form an occlusive dressing (i.e. do not act as semi-permeable membranes). Occlusive dressings result in increased temperature, increased carbon dioxide and decreased oxygen levels, increased humidity, and increased acidity. These changes predispose to nipple epithelial overhydration and moisture-associated skin damage, which increases risk of epithelial fracture. Breast pads also absorb moisture (milk and sweat). This further predisposes to nipple epithelial overhydration and moisture-associated skin damage, which increases risk of epithelial fracture (Appendix 2). |
Aetiology: the mechanobiological model of lactation-related nipple pain and damage
Nipple pain in the absence of visible damage is caused by excessively high intra-oral mechanical loads
This article proposes a new mechanobiological model of lactation-related nipple pain and damage.
During suckling, the nipple epidermis, dermis, stromal core, and other intra-oral breast tissues stretch in response to the mechanical force of vacuum (Box 3). Vacuum is generated as the infant’s mandible drops in the context of the seal against the breast and the seal closing off the nasopharangeal space.9,26,27 Elasticity of breast tissue and nipple–areolar complex skin varies widely between women. But epithelium begins to tighten at high stretch loads, known as the ‘yield point’, as the desmosome locking mechanism is triggered (Figure 1).61,63
Figure 1.
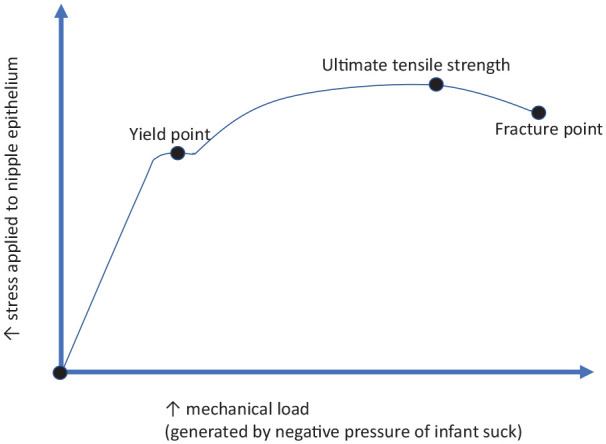
The mechanobiological model of nipple epithelium yield and fracture.
Graph adapted from Pawlaczyk et al. 61
This model proposes two mechanical causes of nipple pain which result from suckling and also from mechanical milk removal. First, nipple pain results when stretching forces are not evenly distributed over a large surface area of nipple, areolar and breast skin, so that desmosomes in the nipple epithelium are subject to repetitive and excessively high mechanical loads (Box 3). This causes the release of cytokines and histamines, triggering inflammatory cascades in the absence of visible tissue damage. If very high stretching or deformational forces are applied, a shearing load may also arise between the epidermis and dermis and the more stable interior collagen structure of the nipple, also causing release of cytokines and histamines and further inflammatory cascades.
Second, stromal micro-haemorrhage results from vascular micro-trauma when the nipple is exposed to repetitive stretching, bending, or deformational forces. Micro-haemorrhages trigger signalling pathways and an inflammatory cascade. Resultant increased stromal tension or swelling further perpetuates cascades of inflammatory responses. The collagen-rich, highly vascular core of the nipple is threaded through with nerve bundles, which may also be vulnerable to the effects of high stretching or deformational mechanical loads and the effects of local inflammation (Appendix 1).
Desmosome strain and inflammation in the nipple skin stimulate dermal nociceptors, triggering maternal nociception and perception of pain. Stromal microvascular haemorrhage and perhaps also neural irritation trigger stromal inflammation, maternal nociception and perception of pain. Persistent nipple pain results from persistent repetitive mechanical micro-trauma in the epithelium, dermis or stroma, which causes persistent inflammation. Inflammatory responses and associated nociceptor stimulation do not cease when an episode of suckling or mechanical milk removal ceases. Before the inflammation has had time to resolve the nipple is again exposed to the mechanical load of milk removal.
Nipple pain with visible damage results when excessively high intra-oral mechanical loads fracture the epithelium
If epithelium can no longer adapt to the mechanical strain of stretching, bending, and shearing forces (Box 3), and desmosomes have locked but the stretching force continues to increase, epithelium ruptures at the ‘fracture point’. 61 In the mechanobiological model of lactation-related nipple pain, the weakest part of the nipple–areolar complex epithelium, or the part placed under the most constant and severe elastic tension in the baby’s mouth, breaks apart (Figure 1). This results in visible trauma, including cracks, grazes, and ulcers, with associated pain and inflammation. Blisters result when horizontal shearing forces cause partial fracture and inflammatory serum collects in a pocket of fluid between layers of skin. Bruising results from vascular damage and haemorrhage.
Cracks are often located at the base of the nipple or in the epithelial crevices on the nipple face. Skin cracks nucleate (i.e. commence) in the stratum corneum along the plane of maximum shear stress, as desmosomes rupture. Fracture of the cells themselves is uncommon. Cracks then propagate along the topographical canyon features of the epithelium. 68
It may be on occasions possible to determine the direction of the intra-oral conflicting force from the location of a crack. For instance, if the crack is at 6 o’clock at the base of the nipple adjacent to the areola, the infant may be suckling from the breast at a height above the natural gravity-induced breast fall, causing the mechanical strain of upwards tension on the intra-oral nipple and breast tissue.9,26,27
The hypothesis that nipple pain and damage is caused by tongue friction or the tongue pinching or compressing the nipple against the palate or upper alveolar ridge is not supported by evidence
The hypothesis that maternal nipple pain and damage results from abnormal tongue movement which pinches or rubs the nipple against the palate or upper alveolar ridge has resulted in widespread overtreatment of breastfeeding infants with frenotomy and bodywork exercises.11,12,14–16,69 This hypothesis is not supported by ultrasound or magnetic resonance imaging of the biomechanics of infant suckling, nor anatomic dissection of the infant floor of mouth fascia.70–72 Studies of breastfeeding women with nipple pain have been interpreted as showing that nipple pain is due to either particular tongue contour and movement attributed to infant oral connective tissue tightness, or innately high vacuum generation.57,59 However, the gestalt biomechanical model, described elsewhere, proposes that these findings are more accurately interpreted as tongue contour changes in response to variable intra-oral breast tissue volumes, aligned with this article’s mechanobiological model (Box 2).9,26,27
Similarly, clinicians and researchers have hypothesized that pacifiers and bottle teats alter neural pathways coordinating tongue movement and sucking patterns, resulting in nipple pain. But this theory is based on misconceptions about the role of tongue in milk transfer. A 2015 systematic review of 14 articles found little evidence of a causal relationship between pacifier and bottle teat use, and nipple confusion.37,58,73
The tongue is a muscular hydrostat, which changes shape and contour without alteration in volume. 74 Applying the gestalt biomechanical model, the infant tongue is a supple adaptive organ, which does not compress the nipple and breast tissue to extract milk or drive milk transfer. Mandibular excursion generates peak intra-oral vacuum, as the anterior and mid-tongue track down en bloc with the mandible. Tongue shape and contour dynamically conform to available intra-oral breast tissue volume. The volume of nipple and breast able to be drawn up into the suckling infant’s mouth decreases in the presence of conflicting intra-oral vectors of force, also known as breast tissue drag.9,26,27
Clinicians and researchers have hypothesized that abnormal infant tongue contour and movement in breastfeeding due to restricted infant oral connective tissues causes a friction burn or graze of the nipple. But a burn or graze caused by friction would be expected to present differently to the cracks and ulcers which characterize lactation-related nipple damage (Box 4). A friction burn or graze is likely to cause a broad area of epithelial damage, on the aspect of the nipple which rests against the dorsum of the tongue during breastfeeding. But nipple cracks and ulcers are commonly located at the base of the nipple and on the nipple face, consistent with epithelial rupture due to tensile mechanical forces. Moreover, if the protective mucosal saliva and mucin layer were to disappear, the hypothesized friction burns would be as likely to occur on the surface of the infant tongue as on the maternal nipple–areolar complex, but maternal nipple damage in breastfeeding does not coincide with infant tongue mucosal damage (Box 4).
Box 4.
Infant saliva protects oral mucosa from friction burn.
| The mucosa of the infant’s tongue slides with minimal friction against mucosa lining other parts of the oral cavity because of the lubricating effects of saliva, saliva mucin, and breast milk. The infant’s parotid, submandibular, and sublingual salivary glands secrete saliva from birth, and as do the minor salivary glands which are widely distributed throughout the submucosa of the oral cavity, except on the gingiva and the anterior palate. All salivary glands secrete mucin, the predominant constituent of the oral mucous layer. Saliva mucin protects oral epithelial cells from dryness and contains synergistic proteins and peptides which promote cell mitosis and migration. Saliva mucin entraps microparticles, including micro-organisms, so that, they are suspended and unable to settle into biofilms, and some mucins interact with bacteria, dispersing, and selectively destroying them. Ultrasound and MRI confirm that there is no air in the oral cavity to exert a drying effect during suckling, even when the mother has nipple pain. 70 Tongue movement continuously redistributes saliva and saliva mucin over the surface of the nipple–areolar complex and intra-oral breast tissue |
MRI: magnetic resonance imaging.
Classification: signs and symptoms of excessively high stretching or deformational mechanical loads during milk removal
Lactation-related nipple pain, persistent nipple pain, and wounds of the nipple
Women describe symptoms of nipple and breast pain and discomfort along a spectrum of intensity with highly variable descriptors, including terms such as cutting, throbbing, pinching, burning, radiating, and stabbing. 43 Erythema and swelling are signs of nipple–areolar complex skin and nipple stromal inflammation. A fine white scale may result from a hyperkeratotic response of the stratum corneum, which occurs in the context of repetitive micro-trauma or moisture-associated skin damage (MSAD) (Appendix 2). Itchiness is hypothesized to result from histamine release, which stimulates nerve cells during the proliferative phase of wound healing (Appendix 3). 74
In a separate review of the research literature, this author has demonstrated that the symptoms of burning, radiating, stabbing, or itching pain which occur between breastfeeds, and which may be associated with signs of a shiny pink nipple and fine white skin flakes, are not indicative of mammary candidiasis. 13 These symptoms and signs are, however, consistent with inflammation, which results from excessively high stretching or deformational mechanical loads applied during suckling or mechanical milk removal. Effects of the inflammatory response continue between feeds.
Lactation-related vasospasm of the nipple
Breastfeeding women may describe shooting, stabbing, radiating, or burning nipple and breast pain at the same time as they notice visible blanching of the nipple face, referred to as vasospasm (Box 5). In 2014, Buck et al. 39 found that almost a quarter of 323 Australian breastfeeding women reported nipple vasospasm in the first 8 weeks after birth. Although these women had higher pain scores overall than women without nipple vasospasm, a majority also reported that their vasospasm was not problematic.
Box 5.
What is vasospasm?
| Vasospasm is a spasmodic contraction of the smooth muscle which lines the walls of the small arteries and arterioles, limiting blood flow. Vasospasm is the underlying mechanism which may lead to clinically evident blanching. After blanching, the colour of the skin may sometimes but not always change to purple, due to ischaemic deoxygenation, followed by a red flush once the arterioles relax again. White and then purple colouration are due to vasospasm; a red flush is due to subsequent hyperaemia. These colour changes are typically diagnosed as signs of primary Raynaud’s syndrome (also known as Raynaud’s disease or Raynaud’s phenomenon), of unknown cause. Primary Raynaud’s syndrome typically occurs between the ages of 15 and 30 years, most commonly in females, affecting the fingers, toes, or ears. A 1978 Scandinavian study found that Raynaud’s disease of the hands affects up to 20% of women of childbearing age.
75
Secondary Raynaud’s syndrome, that is, Raynaud’s with a known cause, can occur due to a connective tissue disorder (e.g. scleroderma, systemic lupus erythematosus, or rheumatoid arthritis), exposure to injury or prolonged vibration, cigarette smoking, thyroid dysfunction, and the oral contraceptive pill. There is no clear evidence linking caffeine intake to secondary Raynaud’s syndrome. Both primary and secondary Raynaud’s syndromes are more common in cold climates. The mechanisms of vasospasm remain poorly understood. In general, chronic hyperactivation of the sympathetic nervous system causes unstable vasoconstriction. This explains why chronic elevation of sympathetic nervous system activity (e.g. stress) is associated with high blood pressure and increased contraction or resistance of peripheral blood vessels. Inflammatory factors are known to destabilize the homeostasis of smooth muscle contraction and relaxation in arterioles, triggering contraction. |
All nipple pain guidelines acknowledge that mechanical breastfeeding trauma is a likely cause of vasospasm.76,77 Paradoxically, painful nipple vasospasm is nevertheless confused with the diagnosis of Raynaud’s syndrome and treated as a primary phenomenon which lacks a known underlying cause, requiring pharmaceutical intervention (Box 5).
In 2004, Anderson et al. studied 12 women who suffered from extremely painful breastfeeding. These women also experienced blanching of the nipple followed by cyanosis and/or erythema, precipitated by cold temperatures. Because 10 of these mothers were evaluated by IBCLCs who reported confidence that breastfeeding technique did not contribute, the authors concluded that poor positioning and poor attachment or latch were not responsible. Half of the women in this small case series were then diagnosed with Raynaud’s disease and prescribed nifedipine. All six reported prompt relief of pain. But this small methodologically weak study lacks a control for the placebo effect, and fit and hold remains an omitted variable bias. 78
The mechanobiological model proposes that nipple vasospasm in breastfeeding women results from repetitive mechanical micro-trauma, which causes inflammation. This inflammation impacts on the autonomic nervous system, destabilizing the homeostatic smooth muscle mechanisms in the walls of the rich vascular bed of the nipple stroma and dermis (Box 5). The subsequent tendency to vasospasm may occur either during breastfeeding or between feeds. That is, the distinction made between nipple vasospasm episodes which occur during or immediately after a feed, and nipple vasospasm episodes which occur between feeds, is not diagnostically helpful or relevant.
A history of autoimmune disease or diagnosis of Raynaud’s syndrome prior to lactation increases the likelihood of a vasospasm response to the inflammation of nipple dermis or stroma which results from excessive mechanical loads during breastfeeding or mechanical milk removal. Similarly, environmental factors, such as cold or touch are more likely to trigger a vasospasm response in nipple dermis or stroma which is inflamed due to intermittent experience of excessive mechanical loads during breastfeeding or pumping. Lactation-related nipple vasospasm is more accurately conceptualized as a secondary Raynaud’s syndrome, which occurs in response to inflammation from repetitive exposure to excessively high mechanical loads.
Lactation-related white spots
From the perspective of this article’s mechanobiological model of nipple pain and damage, there are three kinds of white spots. The first two are conceptualized as signs of localized epithelial inflammation.
Mitchell et al. hypothesize that white spots result from subacute mastitis and mammary dysbiosis, in which ductal biofilm formation extends to the nipple epithelium (Box 6).79,80 Their hypothesis builds on the 2017 Rodriguez and Fernandez hypothesis that breast inflammation results from biofilm blockages within lactiferous ducts. 81
Box 6.
The hypothesis that white spots are caused by mammary dysbiosis is not supported by evidence.
| In 2020, Mitchell et al. published a single case study of a 35-year-old lactating woman in the United States. In this analysis, the authors hypothesized that milk blebs are a surface extension of intra-ductal mammary dysbiosis and plugging caused by biofilm formation.
79
Mitchell et al. propose that dysbiosis extends superficially to dissect the duct at the nipple orifice, resulting in growth of epidermal tissue over the orifice. (See the second article in this series for a critique of the diagnosis of mammary dysbiosis.
18
) The patient had successfully breastfed two older children but her third infant received expressed breast milk exclusively from birth, due to persistent inability to latch, attributed to extremely large nipple size relative to the baby’s mouth. By the time this mother presented 6 months postpartum to a breast surgery clinic, she had received antibiotics for three previous episodes of mastitis, with the last episode occurring 2 weeks prior. She presented with persistent left breast pain, scattered areas of ‘plugging’ of her left breast and extensive left nipple blebs believed to be occluding multiple nipple orifices, with no erythema. Her milk grew multi-drug–resistant Staphylococcus aureus. The patient was treated with intravenous antibiotic therapy (daptomycin and dalbavancin). Two weeks later, her symptoms had improved but not resolved, and she received further intravenous dalbavancin. Eight weeks later, both bleb and pain were completely resolved.
79
This study does not report if the woman had been: 1. Self-treating her blocked ducts and mastitis with massage prior to presentation, which is commonly advised and likely to worsen breast inflammation;17,18 2. Applying breast compressions during mechanical milk removal, which is commonly advised but predisposes to breast inflammation; or 3. Attempting to ‘unroof’ or rub away the white spots, which is commonly advised but is likely to worsen pain and hyperkeratosis. Because this woman had successfully breastfed two infants prior, one for 10 and one for 16 months, it is unlikely that an abnormally large nipple relative to the infant’s mouth explains why she had been unable to latch this third infant over the previous 6 months. Unidentified and unmanaged problems of fit and hold are a more likely explanation. The report of early latch difficulty and brief nipple shield use for the second infant indicate previous emergence of fit and hold challenges. Applying a mechanobiological model, epithelial trauma from excessively high mechanical loads is the most likely cause of both breast inflammations and hyperkeratotic white spots on the nipple in this case. The authors assume that the white spots occluded nipple orifices but the case is more consistent with hyperkeratotic white spots rather than milk blisters. 79 In 2020, Mitchell and Johnson found that nipple ‘blebs’ represented 17% of all referrals to a US breastfeeding medicine practice. Thirty-four women were treated for blebs, at the same time as the clinicians addressed milk supply that was in excess of the infant’s needs, as deemed relevant. Patients were advised to apply mid-potency topic steroid cream ‘to thin the inflamed, fibrinous tissue obstructing the nipple orifice and to reduce pain with latch’ several times a day after breastfeeding, and prescribed 5–10 g organic powdered lecithin sunflower lecithin orally each day. Forty-four per cent were prescribed antibiotics for concurrent acute or subacute mastitis. Two blebs causing acute obstruction were unroofed with a sterile needle. One patient presented with an uncomplicated bleb at five months postpartum, was not compliant with lecithin or topical triamcinolone therapy, repeatedly unroofed her bleb at home, then re-presented months later with a hypertrophic, painful bleb. Triamcinolone injection was unsuccessful. Excision and pathology showed squamous hyperplasia, consistent with hyperkeratosis. Unfortunately, this methodologically weak retrospective audit does not corroborate mammary dysbiosis as an explanatory model for white spots of the nipple, nor demonstrate treatment efficacy. 80 |
The first two articles of this series on lactation-related breast inflammation argue that diagnoses of mammary dysbiosis and subacute or subclinical mastitis are not supported by the evidence, and that the hypothesis that breast inflammation is caused by intra-ductal biofilm is unconvincing. Pathogenic biofilm formation may be an occasional late stage development in a cascade of severe breast inflammation, not causative. Similarly, there is no convincing evidence-based rationale to suggest that white spots are an extension of intra-ductal biofilm to the face of the nipple (Box 6). These pathogenic bacterial models result in widespread prescription of short or prolonged courses of antibiotics for lactating women, with little evidence of benefit relative to the passage of time, and contribute to the global problem of antimicrobial resistance.17,18
Milk blister
A milk blister is an exquisitely painful white spot or lesion on the nipple face, usually with a clearly demarcated border. It is sometimes associated with a lump or cord-like area extending from the nipple blister into the breast.
This article proposes that microscopic epithelial inflammation in the region of a duct orifice, most likely due to mechanical trauma, may heal so that the stratified squamous epithelium which extends 2 mm inside the orifice fuses during the inflammatory process of wound healing (Appendix 1). There may be a build-up of milk in the main duct behind the resultant milk blister, resulting in elevated intra-luminal pressure in the glandular tissue drained by branches of that duct. The latter triggers inflammation and high white cell counts, 82 explaining the inspissated milk that is sometimes released or expressed when a milk blister is released.
Hyperkeratosis
This article hypothesizes that a hyperkeratotic spot of the nipple is an area of stratum corneum which has thickened in response to a focus of repetitive and excessively high mechanical trauma during breastfeeding or mechanical milk removal. A hyperkeratotic spot is often exquisitely painful in response to even mild pressure, perhaps because the thickened plaque of stratum corneum places pressure on the dermis, which is highly vascular and dense with sensory nerve endings.
A hyperkeratotic spot may appear pale white, cream, or yellowish, though colour alters during milk removal due to the effects of moisture and epithelial hydration. A hyperkeratotic spot may be larger with more diffuse borders than a milk blister. Multiple, irregular sized hyperkeratotic spots may form on the face of a nipple which is subject to repetitive micro-trauma. Attempts to unroof a hyperkeratotic spot, mistaking it for a milk blister, will worsen hyperkeratosis.
In 2012, a US medical practitioner Dr O’Hara published an abstract (only), which reported histological analysis of punch biopsies of painful white spots from five breastfeeding women. The tissue was characterized as rubbery and scar-like. Analysis found no bacteria or fungi, but leukocytes and fibrin were identified, signalling inflammation. The women reported that their symptoms resolved shortly after biopsy removal. These histological analyses are consistent with the diagnosis of hyperkeratosis. 83
O’Hara reported that patients with white spots who subsequently presented to that clinic (number not stated) were effectively treated with a short daily course of mid-potency steroid under occlusion. A moist wound dressing (plastic wrap) was applied to enhance penetration of steroid into inflamed and fibrotic tissue. The author concluded that ‘nipple blebs are an inflammatory response to nipple trauma. . . . Clinicians should check for and treat any underlying causes of the recurrent trauma’. 83
Milium
A milium is a painless, small white dermal cyst of keratin, lined by a layer of stratified squamous epithelium, which may appear in the crevices of the nipple face. A milium cyst may appear prominent and very white after a breastfeed or mechanical milk removal. It usually disappears in time, and no treatment is required.
The hypothesis that persistent nipple pain during lactation is nociplastic (due to central sensitization) conflicts with international criteria for nociplastic pain
Persistent nipple pain has been defined in the 2016 Academy of Breastfeeding Medicine Clinical Protocol #26: Persistent Pain with Breastfeeding as pain that persists for more than 2 weeks in a breastfeeding woman, and which has not responded to (undefined) interventions by IBCLCs. Clinical protocols for persistent lactation-related nipple pain list allodynia and hyperalgesia as differential diagnoses, requiring referral for psychological or pain clinic support, or medications, such as propranolol or selective serotonin reuptake inhibitors.76,84,85
The International Association for the Study of Pain defines nociplastic pain
The biomedical model conceptualizes pain as a direct consequence of tissue damage: the more severe an injury, with its associated inflammation, the more severe the pain. As tissue damage resolves, pain resolves. But this reductionist conception of pain is outdated.
An individual’s perception of pain emerges out of interactions between multiple factors. 86 During acute tissue damage, pain perception is predominantly affected by the extent and nature of the injury. Relatively unspecialized nerve cell endings known as nociceptors send a threat signal to the brain. The brain evaluates the extent of threat by drawing on information from current and past experiences, and this perception is moderated by the psychological state of the brain. Even in the case of acute injury, psychosocial and genetic factors, psychological state, and past experiences of pain interact to modulate pain perception. The International Association for the Study of Pain (IASP) states that pain is an experience of sensations and emotions and is always subjective. No pain, even acute pain in response to obvious tissue trauma, can be conceptualized as purely nociceptive.
The IASP defines chronic pain as pain which is present for at least 3 months and/or beyond normal healing time. 87 The experience of chronic pain emerges from:
Nociceptive stimulation (inflammation and tissue damage which stimulate nociceptors and initiate perception of pain),
Neuropathic stimulation (damage to peripheral nerves which initiates perception of pain), and
Nociplastic influences (central nervous system processing alteration or dysfunction, resulting in central sensitization or disruption of perception of pain signals). 88
The IASP defines nociplastic pain as ‘pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain’. 89 When pain is chronic, it no longer reflects the state of the tissues since most injuries heal within a few months. Central sensitization or nociplastic pain has been studied with cancer pain, rheumatoid arthritis, fibromyalgia, low back, and musculoskeletal pain, and increasingly with long COVID. Multifaceted care is required because social, psychological, and physical domains interact in pain perception. Pharmaceutical and non-pharmacological techniques including psychological support are required.88,90
Lactation-related nipple pain is acute even when persistent
This article argues that it is inappropriate to extrapolate management of functional chronic pain syndromes to the care of breastfeeding women with persistent nipple pain. Instead, this article proposes that the perception of nipple pain is triggered by acute tissue damage and inflammation, even when modulated by genetically moderated pain sensitivity, psychological state, and the impact of psychosocial factors. 91 It is important to note that although anxiety and depression modulate pain thresholds, anxiety and depression also result from the experience of pain with breastfeeding. 53
The nipple dermis is dense with nociceptors; nipple stroma is richly vascularized and threaded with nerve fibres (Appendix 1); both are vulnerable to inflammation caused by mechanical stretching and deformational forces. Inflammation caused by repetitive application of excessively high mechanical loads on the nipple skin or by stromal micro-haemorrhages, and perhaps also the effects of stretching deformational mechanical loads on stromal nerve fibres, send powerful nociceptive signals to the brain and should not be mistaken for nociplastic pain. Lactation-related nipple pain remains an acute pain according to the IASP definitions, even when nipple pain is persistent. The physical and psychological stress of breastfeeding in the presence of pain may exert effect by causing unconscious muscle tension, which results in elevation of shoulders and arms or difficulty making adjustments to fit and hold (micro-movements), worsening conflicting intra-oral vectors of force.9,26,27
In 2012, McClellan et al. noted that ‘lack of research describing the pain severity and characteristics for breastfeeding women may lead some clinicians to question the pain threshold of women experiencing persistent pain’, but suggested that the effects of excessively high intra-oral vacuums measured in women with nipple pain may be the predominant reason for ongoing pain perception, rather than central sensitization. 43 But ultrasound and vacuum studies of women experiencing nipple pain corroborate the mechanobiological model of lactation-related nipple pain (Box 2).
When application of mechanical forces cease altogether, in the absence of ongoing sucking or mechanical milk removal, inflammation of the nipple skin and stroma rapidly resolves and the experience of pain ceases. This explains why women with persistent nipple pain are more likely to prematurely cease lactation. 36
In a 2018 US case series of three lactating women with nipple and/or breast pain, Mudunna et al. assessed pain using a cotton-bud and pin-prick touch, which the authors proposed were non-painful stimuli, moving from the lateral edge of each breast quadrant in towards the nipple. The women demonstrated heightened breast skin sensitivity to the stimuli, and the authors stated that their pain resolved with oral antihistamines and beta-blockers. Mudunna et al. wrote:
Allodynia is perceiving a non-painful stimulus as painful. Other [breastfeeding] individuals experience increased pain from a normally painful stimulus (hyperalgesia). For a lactating woman with allodynia, an anatomically normal latch may be perceived as painful. Similarly, a woman with hyperalgesia may experience slight nipple compression during let down as excruciating. 85
But Mudunna et al. also hypothesize that persistent local inflammation due to repetitive exposure to micro-trauma is likely to sensitize the nociceptors and mechanoreceptors of nipple skin due to release of histamines and cytokines. Similarly, increased interstitial tension associated with the vasodilation and hypervascularity of breast inflammation triggers release of histamines and cytokines, sensitizing surrounding tissues. Mechanical pressure by a cotton bud or pin prick in the context of acute nipple or breast inflammation is likely to trigger nociceptive pain perception. This article argues that the local sensitivity effects of nipple and breast inflammation should not be confused with central sensitization.
Diagnoses of nociplastic pain, central sensitization, allodynia, and hyperalgesia may harm a lactating woman with nipple pain and damage. This is because these diagnoses may:
Invalidate her lived experience, which is that suckling or mechanical milk removal causes her pain and that if she were to cease this altogether, her pain would rapidly resolve;
Disempower her, since she is not helped to resolve the pain herself (as is the case, for example, with the gestalt method of fit and hold) but is advised that she requires pharmaceutical intervention and multi-disciplinary teams;
Re-traumatize her if she is a sexual abuse survivor by taking a sexual trauma history in a breastfeeding consultation, then proposing that persistent nipple pain is linked to sexual trauma and associated nociplastic effects;
Invite her to shift attention away from her experience of nipple pain. She may also feel pressured to divert her attention away from her nipple pain, so that she is not perceived as ‘exaggerating’ the pain in her brain. Not paying attention to nipple sensations and pain typically worsens conflicting intra-oral vectors of force during milk removal. From the perspective of the gestalt method, increased attention to nipple and breast sensation is required, drawing on psychological strategies which support contact with the present moment, as she applies micro-movements to eliminate breast tissue drag and resolve tissue damage and inflammation; 9,26,27
Place her at risk of side-effects of pharmaceutical interventions without evidence of benefit; and
Result in financial burden of treatments without evidence of benefit.
Prevention and management of lactation-related nipple pain
Evidence-based prevention and management of lactation-related nipple pain and persistent pain is detailed in Table 2. The mechanobiological approach to nipple pain translates into two key preventive or treatment strategies:
Table 2.
Evidence-based management of lactation-related nipple pain and wounds.
| Primary intervention: clinical translation of mechanobiological model | Primary intervention: mechanisms | Secondary or adjunct interventions | |
|---|---|---|---|
| Nipple pain and persistent pain | The gestalt method is currently the only fit and hold intervention which offers an evidence-based model for eliminating conflicting intra-oral vectors of force during milk removal.9,26,27 | Distribute mechanical load over a larger area of nipple and areola surface, by eliminating conflicting intra-oral vectors of force during suckling or mechanical milk removal. This eliminates repetitive mechanical micro-trauma. | Nipple shields are often used as compensation for failure to identify and address underlying problems of positional instability or conditioned dialling up at the breast, but remain an important adjunct intervention for nipple pain and damage. Both a 2015 systematic review and a 2021 review conclude that nipple shield use substantially benefits breastfeeding when problems emerge, both in measurable outcomes and in reports by mothers.55,92 In a study which randomized nipple shield use in a group of 20 mothers with nipple pain and 28 without breastfeeding problems, nipple shields improved maternal comfort and did not impact milk removal or sucking strength in the pain group.
93
Nipple shields may have a role at the same time as primary interventions are applied in the following three presentations: 1. Severe pain and/or damage 2. Conditioned sympathetic nervous system hyperarousal at the breast in association with nipple pain, commonly due to unidentified positional instability 3. Very low-height nipple, contributing to difficulties bringing the baby on to the breast despite ongoing intervention to eliminate conflicting intra-oral vectors of force |
| Avoid unnecessary and ineffective topical applications (Table 3). Optimize time without bra, wearing soft garment. Nocturnal sleep is an important opportunity to allow air to circulate around the breast, even in the context of milk leakage. A towel on or under the sheets may be used for milk containment. | Avoid epithelial overhydration and moisture-associated skin damage. This is necessary to prevent worsened pain and damage, and to support wound healing. | Intermittent maternal ibuprofen use between feeds. Analgesic use when directly breastfeeding may interfere with a woman’s capacity to attend to nipple sensation and eliminate repetitive mechanical micro-trauma. If pain is so significant that a woman cannot imagine breastfeeding without analgesia, her nipples need to rest from direct breastfeeding. | |
| Vasospasm | The gestalt method is currently the only fit and hold intervention that offers an evidence-based model for eliminating conflicting intra-oral vectors of force during milk removal.9,26,27 | Distribute mechanical load over a larger area of nipple and areola surface, by eliminating conflicting intra-oral vectors of force during suckling or mechanical milk removal. This eliminates repetitive mechanical micro-trauma. | Keep nipples warm in between feeds. Avoid triggers, for example, cold. Avoid stimulants, beta-blocker, or vasoconstrictor medications (e.g. propranolol, pseudoephedrine). |
| Hyperkeratotic spot of nipple | The gestalt method is currently the only fit and hold intervention which offers an evidence-based model for eliminating conflicting intra-oral vectors of force during milk removal.9,26,27 | Distribute mechanical load over a larger area of nipple and areola surface, by eliminating conflicting intra-oral vectors of force during suckling or mechanical milk removal. This eliminates repetitive mechanical micro-trauma. | Application of steroid cream (e.g. mometasone twice daily for the first day, then daily for a week) may have a temporary role in suppressing the inflammation, at the same time as repetitive micro-trauma of breast tissue drag is addressed. Occlusive dressing or ointment should be avoided, as moisture-associated skin damage increases the vulnerability of the nipple epithelium to micro-trauma. |
| Milk blister | A bevelled needle may be used to lift the epithelial roof. Often, there is immediate leakage of milk once the blister is unroofed. Feed the infant as frequently as possible from that breast for the next few days. | Short frequent episodes of milk flow through the orifice, once breast tissue drag is eliminated, may prevent the epithelial roof re-sealing over the duct orifice. | Advise women not to rub the nipple with a cloth or fingernail or attempt to deroof the blister themselves, as hyperkeratosis can result from self-treatment. If a milk blister persists, a steroid cream may suppress the inflammatory response which causes the roof to form. Laser is successfully used for treatment of sublingual salivary gland mucoceles, which are retention cysts similarly caused by an epithelial roof at the duct orifice. Research is required to investigate whether laser has a role in the case of recurrent milk blisters. |
| Classic tongue-tie | Simple scissors frenotomy. Laser frenotomy is only indicated for ankyloglossia associated with complex congenital syndromes.94–96 | No requirement for wound stretching or bodywork exercises post-frenotomy, which are not supported by the evidence.69,97,98 | |
| Nipple–areolar complex wounds | The gestalt method is currently the only fit and hold intervention which offers an evidence-based model for eliminating conflicting intra-oral vectors of force during milk removal.9,26,27 | Distribute mechanical load over a larger area of nipple and areola surface, by eliminating conflicting intra-oral vectors of force during suckling or mechanical milk removal. This eliminates repetitive mechanical micro-trauma. | Adjunct interventions as for nipple pain and persistent pain, above. |
| Cleanse wound exudate gently with clean water in shower or cotton wool soaked with clean water. Do not intentionally remove the scab. | Wound exudate is protective. Scab formation is part of the healing process (Appendix 3). The infant mouth is an ideal cleansing and debriding application due to antimicrobial and immunoprotective effects of infant saliva, human milk, and milk and oral microbiomes. | Do not attempt to debride and do not rub the nipple. If there is extensive ulceration, a scab may be too large for a woman to feel comfortable allowing her infant onto the breast, due to concerns about swallowing the scab. In this case, if a nipple shield is not appropriate, her nipple needs to rest from direct breastfeeding until the scab is naturally shed. Saline water stings and is unnecessary. | |
| If necessary, cease direct breastfeeding until nipple wounds are well healed (about 5–7 days depending on extent of wound). | When adequately healed, commence fit and hold intervention to eliminate underlying causes. | Hand expression is best protection of nipple wounds. Ensure no rubbing of nipple on flange if removing milk mechanically and minimize amount of areola that is drawn into tunnel. Olive oil may help eliminate friction during mechanical milk removal (lanolin may become adherent). Minimize pumping if it seems to perpetuate damage and use stored expressed breast milk, donor milk, or formula as temporary measure; hand express for comfort and to avoid breast inflammation. If the baby is older and supply is established, production will quickly build again if a woman needs to minimize mechanical milk removal or hand expression until wound is healed. Regardless, ceasing any milk removal other than to avoid breast inflammation in the short term may best promote healing and protect breastfeeding long term. | |
| Short frequent flexible feeds or milk removals are more effective for milk transfer and maintenance of supply than long less frequent breastfeeds. 18 | Limit duration of breastfeeds after initial milk ejections, using judgement and experimentation. The Neuroprotective Developmental Care concept of frequent flexible feeds is defined in second article in this three-part series. 18 | Application of expressed breast milk to nipple wound. Expressed breast milk may be more effective than all other applications used for lactation-related nipple pain. 41 A systematic review showed significant reduction in time to umbilical cord separation with topical application of human breast milk, without increased risk of infection. 99 | |
| Remove breast pads carefully or soak off if adherent. Apply lanolin or hydrogel sheet when wearing a bra to prevent adherence of exudate to breast pad, which may worsen damage when bra is required to be worn. | Lanolin and hydrogel sheet applications have not been shown to improve healing, and may delay healing (Table 2). 41 This is because moist wound care risks moisture-associated skin damage. Lanolin and hydrogel do not help heal nipple pain or damage but may prevent exudate and eschar adhering to breast pad and perpetuating damage when pad is removed. Lanolin does not need to be washed from nipple–areolar complex prior to breastfeeding; hydrogel does need to be washed off. | Photobiomodulation or light therapy has the potential to downregulate inflammation and promote more rapid resolution of stromal micro-haemorrhages and wound healing, in the context of ongoing primary interventions. Requires further research (Box 7). | |
| Secondary infection | Topical or oral antibiotics | Recommended if cellulitis occurs, or if there is heavy purulent malodorous discharge of nipple wound, when primary interventions do not immediately help. | |
| Topical or oral anti-fungals | Standard course of treatment may occasionally have a role for nipples which have been kept moist, humid, and warm for long periods, and particularly in the context of oral antibiotic use. No reason to treat infant oral cavity unless clinically obvious candida plaques. Prolonged maternal antifungal treatment is never required. 13 |
Elimination of repetitive mechanical micro-trauma due to excessively high stretching or bending mechanical loads during milk removal and
Avoidance of epithelial overhydration and MASD.
Box 7.
Does photobiomodulation therapy help resolve breastfeeding-related nipple pain and damage?
| Photobiomodulation therapy has been utilized to accelerate wound healing since its introduction in the 1960s. Laser application activates cellular photoreceptors, which modulate molecular, cellular, and tissue process, increasing protein synthesis and cell proliferation and modulating inflammatory mediators, cytokine production and growth factors, to reduce pain and swelling, and promote wound healing. In 2000, Pietschnig et al. first evaluated the effects of light therapy for the management of nipple pain in a small study, demonstrating a reduction in nipple pain. However, as participants also used lanolin cream concurrently, and as there was no control, the effect could not be attributed to light therapy. 100 In 2007, Posso et al. compared one application of light therapy to placebo in 40 postnatal women. The results demonstrated a significant reduction in nipple pain at 1 and 10 min after light therapy. 101 Further pilot and case studies have since been conducted, offering preliminary evidence that light therapy reduces nipple pain.102–104 In 2016, Coca et al. conducted a triple-blinded RCT of 59 participants randomized to receive either placebo or light therapy for three sessions at 0, 24, and 48 h after group allocation, in addition to standard care. Results demonstrated a significant reduction in nipple pain for the light therapy group after the first and second applications. The third application was not analysed due to a significant drop out rate as participants were discharged from hospital. 105 A follow-up study in 2019 by Camargo et al. performed just one session of light therapy compared to placebo using higher energy settings than in their previous study and showed no changes in reported nipple pain. The authors reflected that more applications of light therapy with lower energy settings may have been more effective and emphasized the need for further studies investigating different parameters, particularly low-fluence settings. 106 In 2016, Buck, Eckereder & Amir published an Australian case study of two postnatal women with nipple pain who were provided with a novel application of three sessions of light therapy within a 24-h period, providing early findings of a significant reduction in nipple pain and improved healing. 103 |
RCT: randomized controlled trial.
Key strategy 1: eliminate repetitive mechanical micro-trauma
A. Optimize fit and hold to eliminate conflicting intra-oral vectors of force during breastfeeding
Studies examining the causes of lactation-related nipple pain and clinical management and clinical protocols universally agree that poor infant positioning or latch is the most common cause of nipple pain. Guidelines advise that suboptimal fit and hold should be addressed before any other treatment is instituted.37,41,45,48,76,77
Yet the way an infant fits into the maternal breast and body, which has direct impact upon the biomechanics of suckling, remains an omitted variable bias in almost all nipple pain research. Commonly taught approaches to fit and hold when problems emerge rely upon outdated biomechanical models of infant suck (Box 8). 107 Much of what is offered women with breastfeeding difficulty, including interventions for fit and hold, is based upon experience or opinion (Box 8).2,108 –111 In 2016, Thompson et al. demonstrated in a retrospective analysis of the medical records of 635 mother–baby pairs that symmetrical apposition of the infant’s chin, cheeks and nose against the breast decreased nipple pain fourfold, compared with cross-cradle hold in which the mother used one hand to shape her breast as she brought the baby on. Although this study elucidated one aspect of fit and hold required to optimize intra-oral breast tissue volume, it does not offer explanatory biomechanical models or develop an evidence-base for a fit and hold intervention. 51
Box 8.
Commonly applied fit and hold strategies lack an evidence base.
| A popularly applied fit and hold technique teaches women to shape their breast with their hand and apply a cross-cradle hold as they bring the infant on. In 2002, a prospective cohort study of 1171 new mothers in Bristol, UK, found that when hospital midwives were taught and applied this technique, the rate of breastfeeding increased at 6 weeks post-birth.
112
But a 2016 Australian study of 653 pairs showed that this same technique worsened the incidence of nipple pain fourfold.
51
A 2003 Latvian study of 95 breastfeeding women found no difference between a mother’s level of reported pain and infant head or body position, or breastfeeding dynamic attributes of the baby. But clinical indicators used to signify optimal breastfeeding were not based on a model of suckling biomechanics. 113 A 2004 observational study in the US, which lacked a control group, found that damaged nipples healed after helping the mother attach her baby with visible and everted lips. 114 Similarly, a 2017 Brazilian systematic review of factors associated with nipple trauma in lactation concluded that incorrect handling during breastfeeds contributed. 37 This latter study used the UNICEF Baby-Friendly Hospital breastfeeding management strategies of visible, everted lips and more areola visible above the baby’s mouth than below as ‘gold standard’ for fit and hold. Most guidelines on nipple pain advise the clinician to look for wide-open mouth with lips turned out, assuming this helps the baby take a wide mouthful of breast and rest close to the mother’s body without biting or clenching the jaw at the breast.76,115 But in 2020 Mills et al. conducted magnetic resonance imaging analysis of eight successfully breastfeeding babies, whose mothers were pain free. Their findings corroborated the gestalt biomechanical model, showing that infant lips are usually neutral successful during breastfeeding, not everted or in a ‘special k’ shape. 70 In the gestalt model, women experiencing pain apply strategies developed to address the mechanical effects of conflicting intra-oral vectors of force, so that the infant’s lips are no longer visible. More breast tissue is then drawn up into the baby’s mouth to distribute the mechanical load and protect the nipple epithelium and stroma from high stretching forces.9,26,51 |
UNICEF: United Nations Children’s Fund.
The failure of current approaches to fit and hold to effectively resolve repetitive biomechanical micro-trauma during breastfeeding leads to widespread overmedicalization and overtreatment of both breastfeeding women and their babies, risking unintended outcomes. Examples include inappropriate diagnosis of mammary candidiasis resulting in unnecessary treatment with anti-fungals; overtreatment with infant frenotomy for inappropriate diagnoses of oral connective tissue restrictions; inappropriate diagnoses of cranial nerve dysfunctions and pathologizing of palate shape, tongue length, and shape of mandible resulting in unnecessary treatment with bodywork exercises;69,97,98 diagnoses of idiopathic vasospasm or Raynaud’s syndrome resulting in overtreatment with calcium channel blockers; inappropriate diagnoses of nipple white spots as subacute mastitis or mammary candidiasis resulting in unnecessary treatment with antibiotics and anti-fungals; and inappropriate diagnoses of functional pain or central sensitization, resulting in use of medications without evidence of efficacy.11–13,14,16
In 2015, Kent et al. reported that 42% of cases presenting to the Breastfeeding Centre of Western Australia showed lack of improvement with fit and hold and other interventions offered by IBCLCs, noting that though some studies claim to show that certain fit and hold interventions improved nipple pain outcomes,114,116,117 other studies could not replicate these findings.118 –120 They observed: ‘Nipple pain is often attributed to suboptimal positioning and attachment of the infant although conclusive evidence is yet to be provided regarding which aspect(s) of positioning may be most important’. The IBCLCs went on to diagnose ankyloglossia and palatal anomaly in 36% of the infants of women presenting with nipple pain. 45
Given the international evidence demonstrating overdiagnosis of ankyloglossia, and the normality of a wide variety of palatal contours, this article proposes another explanation: that scientific investigation of the elements of fit and hold which impact on maternal pain remains a research frontier.
The foundational importance of laid-back or baby-led breastfeeding
The physiologic or mammalian approach to breastfeeding initiation, including skin-to-skin contact postpartum, has been a major advance in the field of clinical breastfeeding support over the past two decades, with positive impacts on breastfeeding outcomes.121 –124
A 2020 systematic review of 11 Chinese randomized controlled trials (RCTs) and one Italian RCT investigating ‘biological nurturing’ or ‘laid-back breastfeeding’ approaches found that when women are taught baby-led or laid-back breastfeeding in hospital immediately after the birth, the incidence of nipple pain and damage decreases for up to 8 weeks. 125 The Italian RCT randomized 180 women to either biological nurturing at birth or a control group, and showed decreased nipple pain and damage, engorgement, and mastitis during the hospital stay, and 58% decrease in cracked nipples at discharge in the intervention group. But biological nurturing made no difference to the rates of nipple shield use, breast problems at 30 days post-birth, or to rates of exclusive breastfeeding at 4 months. 126
A 2021 Chinese RCT of 504 pairs demonstrated that implementing baby-led self-attachment from birth results in a 12% increase in exclusive breastfeeding at day 3, and an 8% and 5% decrease in the number who reported nipple pain at 3 days and 3 months postpartum, respectively. 127
While biological nurturing or baby-led approaches are demonstrated in these studies to be foundationally important for prevention of breastfeeding difficulties from birth, baby-led approaches have not been demonstrated to be effective therapeutic interventions for emergent breastfeeding problems. A 2013 Swedish RCT of 103 mothers with infants up to 16 weeks of age with severe latch-on difficulties found that a baby-led or skin-to-skin intervention did not increase the likelihood that the infant would latch on. 128
Applying the mechanobiological model, this article proposes that although laid-back or baby-led breastfeeding methods are essential from birth, they do not integrate new knowledge about the biomechanics of infant suck to address the mechanical forces that cause nipple pain and damage. That is, the biological nurturing approaches are not enough to prevent breastfeeding problems including nipple pain and damage for many women.
The gestalt method is the only available clinical approach to fit and hold which integrates the principles of laid-back or baby-led breastfeeding with an evidence-based model of the biomechanics of infant suckling, translated into a reproducible, flexibly applied clinical intervention.9,26,27
Normal maternal and infant anatomies are highly variable
Human anatomy, including infant tongue length, mandibular shape, and palate contour and height, and maternal breast, nipple, areola, upper and forearm length, and abdominal contour are highly variable. Labelling, that is, medicalizing or pathologizing, the wide range of normal maternal and infant anatomy disempowers and discourages breastfeeding women, and unnecessarily exacerbates parental anxiety. In the gestalt model, it is understood that certain normal anatomic variations may increase vulnerability to the emergence of problems in the complex adaptive system of the breastfeeding mother–baby pair. This emphasizes the importance of preventive and management approaches to fit and hold which optimize intra-oral breast tissue volume and eliminate breast tissue drag.9,26,27
Infant oral connective tissues, including the lingual and labial frenula, also display wide anatomic variability which are currently pathologized and inappropriately treated with either surgery or courses of bodywork therapy. The normal spectrum of labial frenula anatomy is not linked with breastfeeding problems, and should not be pathologized as restricted or ‘tied’.129–131 There is no anatomic or functional basis for the diagnosis of posterior tongue-tie.72,94,95,132 The latter two diagnoses are examples of overmedicalization of breastfeeding problems, resulting in exponential increase in unnecessary infant oral surgery and bodywork exercises.11,12,14–16,97,98,133 Studies that claim to show benefits of frenotomy for diagnoses of posterior or upper lip-ties are methodologically flawed, demonstrating bias.134,135 Unintended consequences of frenotomy include infant pain, haemorrhage, worsened feeding, oral aversion, damage to lingual nerve branches altering tongue sensation, sublingual mucocele, and weight loss.72,136 –139 The gestalt model proposes that behaviours during breastfeeding of fussing, back-arching, pulling off the breast, and ‘shallow latch’ are all signs of suboptimal fit and hold and are not attributable to infant oral connective tissue restrictions, neurological weakness or motor dyscoordination.9,25 –27
Certain poorly defined anatomic variations have been shown in preliminary studies to have links with breastfeeding problems, including nipple pain. A 2009 Iranian study showed that 50 newborns of mothers with flat nipple, inverted nipple, large breasts and/or large nipples had a mean decrease in weight by day 7 compared to 50 newborns whose mothers did not have these breast variations. 140 A 2013 Thai study of 449 women showed that nipple lengths of less than 7 mm were associated with less success in bringing baby to the breast and initiating breastfeeding in the first 24 h, but no conclusions about breastfeeding success or capacity to latch after the first day could be drawn. 46 In 2020, Ventura et al. 141 studied 119 women in a US breastfeeding centre, showing that various combinations of wider, longer nipples and denser areolas were associated with difficulty latching, sore nipples, low milk supply, and slow infant weight gain. But there is no reliably established link between nipple shape and breastfeeding failure.
This article proposes that multiple morphological factors interact with multiple modifiable biomechanical factors to determine an infant’s capacity to transfer milk efficiently from his or her mother’s breast, without causing her pain. The gestalt model applies a complexity science perspective to clinical breastfeeding support, which aims to optimize intra-oral breast tissue volume across the wide diversity of maternal and infant anatomies. In this way, anatomic and other vulnerabilities within the complex adaptive system of the mother–baby pair are compensated for, because the protective effect of multiple other factors is optimized.9,25–27
Impact of anatomic abnormality
Ankyloglossia is a congenital abnormality of the lingual frenulum, which significantly restricts movement of the infant’s tongue and has been linked with maternal nipple pain. Prevalence estimates vary between 3% and 10%, in the absence of agreed definitions and demonstrated overdiagnosis. 96 Although many infants have a prominent and membranous frenulum, which may attach anywhere along the ventral surface of the tongue, a tongue-tie is a variation of frenulum which may attach close to the tip of tongue, often to the alveolar ridge instead of the floor of the mouth, and is assessed clinically as impacting on the infant’s capacity to suckle without causing maternal nipple pain. Lack of consensus definition of ankyloglossia is a methodological flaw in all investigations into this condition, and there are no studies comparing the effects of optimal fit and hold intervention with frenotomy. A small case series of breastfeeding pairs showed that the effects of a brief gestalt intervention on tongue contour, measured by ultrasound imaging, was the same as had been measured elsewhere post-frenotomy. 27 A classic tongue-tie typically requires a simple scissors frenotomy.94,142
B. Eliminate conflicting vectors of force during mechanical milk removal
Conflicting vectors of force (breast tissue drag) applied to the nipple during pumping may cause persistent nipple pain and damage. Hands-free mechanical milk removal, with pump flanges supported in an elastic band, may increase the risk of breast tissue drag and epithelial damage. Mechanical milk removal may also result in an erythematous, slightly swollen ring rash on the areola, a sign that the areola is repetitively drawn into the flange and exposed to friction. Pain-free, thickened discoloration, and hyperkeratosis of the nipple face, caused by repetitive ischaemia, may result from exclusive pumping.
The following strategies aim to minimize damage to nipple–areolar complex skin and nipple stroma during mechanical milk removal.
Ensure nipple moves freely without rubbing on inside of the flange tunnel, and that minimal areola is drawn up into the tunnel;
Invite a woman to experiment between different sized flanges;
Invite her to experiment with different flange options, for example, Pumpin’ Pals or Milkdrop cushions;
Hand expression of one breast while pumping the other, then swap the next time;
Pump on lowest effective vacuum setting and for short periods of time, for example, 10 min, because frequent short pumping is more effective in milk removal and milk generation than less often, longer periods; 18
Do not use hands-free pumping (because hands-free pumping, curtails a woman’s capacity to eliminate breast tissue drag which conflicts with the direction of the vacuum;
Consider applying olive oil as lubricant.
Key strategy 2: avoid epithelial overhydration and moisture associated skin damage
Topical applications to nipples during lactation, including anti-fungal treatments, mupirocin antibiotic cream, hydrogel discs, lanolin, vitamins A and E, Vaseline, sundry emollients, and ‘All Purpose Nipple Ointment’ have been shown to be ineffective for nipple pain and damage, and risk epithelial overhydration and MASD (Table 3; Appendix 2). MASD results in an erythematous rash with clearly defined edges visible on the areola, corresponding with topical application. Overhydration and MASD may be confused with an irritant contact dermatitis or an allergic contact dermatitis. 22 Overhydration and MASD place the nipple–areolar complex at risk of damage or delayed healing (Appendix 2).
Table 3.
Interventions which do not help lactation-related nipple pain and wounds.
| Intervention | Commonly applied rationale | Why intervention is not recommended |
|---|---|---|
| Debridement of wound | Classic wound care requires removal of necrotic and non-viable tissue. Exudate and eschar are dirty or infected, needing to be cleansed. | Wound exudate is protective. Do not attempt to debride, do not rub. Scab formation is part of the healing process. The infant mouth is an ideal cleansing and debriding application due to antimicrobial and immunoprotective effects of infant saliva, human milk, and milk and oral microbiome (Box 4). |
| Anti-fungals (maternal topical or systemic; infant oral topical) | Mammary candidiasis presents with radiating, burning, stabbing pain either during or between feeds, pink shiny epithelium and hyperkeratotic flakes. | The evidence does not support treatment of maternal nipple pain with anti-fungals except in rare situations; prolonged courses and gentian violet are never indicated. Infants only need oral anti-fungal treatment in the presence of visible candidal plaques. 13 |
| Sunlight | Dries out and heals wounds. | Irritating and dehydrating effect on skin if too much sunlight exposure. Do not aim for direct sunlight exposure on nipples, though modest incidental exposure unlikely to harm. |
| Hairdryer | Dries out and heals wounds. | Irritating and dehydrating effect of warm air on skin if too much exposure. |
| Honey | Antimicrobial, anti-inflammatory, and antioxidant activities. Stimulates lymphocytic and phagocytic activities. | Manuka honey contains the chemical methylglyoxal, which is toxic to human cells, and may delay healing. 143 |
| Gentian violet | Recommended if topical miconazole and oral fluconazole do not improve nipple pain. | Cytotoxic; risks nipple epithelial erosions; and prolonged courses of antifungals and gentian violet are never indicated. 13 |
| Petroleum-based products, for example, Vaseline | Protects wound by keeping it moist. | Risks moisture associated skin damage (MASD; Appendix 2). |
| Salt water | Kills bacteria. | Causes pain and stinging without benefit. |
| Steroid cream or ointment, for example, betamethasone, mometasone, or triamcinolone | Reduces inflammation. | Fails to address repetitive mechanical micro-trauma which results in inflammation; disrupts inflammatory processes and may disrupt skin microbiome homeostasis; may overhydrate and risk MASD (Appendix 2) |
| Topical antiseptic | Kills bacteria. | Cytotoxic properties that kill human cells, including newly formed tissue generated on periphery of and within wound, impeding wound healing. |
| Silver cap | Silver ions believed to be effective against common wound pathogens, including methicillin-resistant S. aureus, by adhering to bacterial cell membrane, penetrating cell wall, and disabling enzymes. Cap believed to prevent entrance of micro-organisms to wound site and protect against trauma, by creating an hypoxic, moist, protected microenvironment. | Silver has cytotoxic effects on both keratinocytes and fibroblasts, and results in significant delay in epithelialization in vitro.
144
Silver-containing dressings or topical agents have not been shown to improve skin wound healing or prevent infection. In 2015, an Italian RCT randomized 40 women with nipple fissures to silver cap use or standard care. The latter included an unspecified fit and hold intervention by an IBCLC and topical application of expressed breast milk. No changes between groups were detected at day 2, but more rapid resolution of symptoms was reported with silver cap at days 7 and 15. 145 This study is methodologically weak because one popularly applied fit and hold intervention has been demonstrated to worsen nipple pain fourfold and it is not clear which approach the IBCLCs used; also, application of expressed breast milk only without advice concerning prevention of adherence of the nipple wound to breast pad risks exacerbation of epithelial damage. |
| Zinc oxide, for example, desitin, sudacrem, sometimes mixed with cod liver oil | Debridement, epithelial protection. | Must be removed from nipple prior to breastfeed which may exacerbate nipple damage; safety has not been established if ingested by infant. Risks MASD. |
| ‘Natural’ nipple care products: calendula, kamillosan, juba, aloe vera, guaiazulene ointment, P. oleracea | Healing properties claimed. | Risk epidermal overhydration and MASD; no evidence of benefit |
| Tea bag or hot water compress | Heat increases blood flow, oxygen and nutrients. | Niazi et al.’s systematic review claimed benefit of warm water compresses for nipple pain but the analysis is methodologically weak. 146 |
| All-purpose nipple ointment (APNO) contains: 1. Mupirocin ointment 2%: 15 g 2. Betamethasone ointment 0.1%: 15 g 3. Miconazole powder to a concentration of 2% miconazole. |
Heals nipples, destroys bacteria and candida. | Risks MASD. Suppressing bacteria with mupirocin destabilizes normal microbiome and may worsen infection; studies show no benefit.17,41 Betamethasone suppresses inflammation, which is necessary for wound healing and for resolution of any microbial overgrowth. Miconazole treats Candida which has not been shown to cause nipple pain. 13 A total of 1151 breastfeeding Canadian women with damage to one or both nipples were randomized into APNO and lanolin application groups. No significant difference found in pain scores after 1 week. Women in lanolin group reported greater satisfaction with their infant feeding method. 147 |
| Breast shell | Protects painful or damaged nipples and promotes healing. | A 2004 study of 94 Latvian women with sore nipples, randomized into using breast shells combined with lanolin compared to usual care, showed no benefit. 114 Risks MASD. Pressure on lactiferous ducts by breast shells may predispose to breast inflammation, cause nipple–areolar oedema, and delay healing. |
| Infant bodywork | Cranial nerve dysfunctions, fascial restrictions, musculoskeletal misalignments, and dysfunctional neural habits impact on tongue function, causing maternal nipple pain. Neural and motoric dysfunctions are interconnected when a holistic perspective is applied to fascial and postural dysfunctions. | Intra-oral or other bodywork exercises do not address the biomechanical problems whicht result in lactation-related nipple pain. From a holistic and complexity science perspective, these dysfunctions arise dynamically out of interactions between the maternal and infant bodies. The effects of repeated intra-oral bodywork exercises on the infant oral mucosal immune system and microbiome are unknown, but may introduce a range of environmental micro-organisms in abnormal volume loads due to repeated digital insertion, also intermittently drying out protective mucosa. Ninety-seven mother–baby pairs with infants younger than 6 weeks with biomechanical sucking dysfunctions were randomized to 30-min sham or real osteopathic treatment by an osteopath treatment combined with unspecified 1-h intervention by an IBCLC. No improvement in nipple pain with osteopathic treatment relative to IBCLC intervention was found. 98 Bodywork is ineffective in reduction of nipple pain. 97 |
| Lidocaine or topical analgesics | Anesthetizes skin during milk removal. | Suppression of pain sensation allows infant to continue to feed with breast tissue drag which risks worsened nipple damage. |
| Vasospasm treatment with medication (for example, nifedipine 30 mg slow release daily, increased to 60 mg daily; amlodipine 5–10 mg daily or twice daily in warmer months; diltiazem; verapamil 120–360 mg/day; antibiotics) | Nifedipine increases nitric oxide levels that induce vasodilation, resulting in decreased oxygen demand and increased oxygenation. Amlodipine causes less peripheral oedema. Antibiotics may be prescribed because vasospasm is believed to be caused by mammary dysbiosis. | There is no evidence or evidence-based physiological rationale to suggest that vasospasm is caused by mammary dysbiosis. Medications for vasospasm have not been studied in breastfeeding women, and there is no evidence to suggest they make any difference compared to the passage of time or placebo. Side-effects of nifedipine include headaches due to cerebral vasodilation, ankle oedema, flushing, dizziness, fatigue, and myalgias. |
| Vasospasm treatment with complementary therapies (for example, vitamin B6; magnesium 300 mg twice daily; fish oil; calcium supplmentation; evening primrose oil or gamma linoleic acid) | Help relieve vasospasm. Magnesium relaxes blood vessels walls. Fish oil capsules which contain essential fatty acids relax blood vessels walls. Calcium and evening primrose oil relax blood vessel walls. |
No evidence or evidence-based physiological rationale to suggest benefit. Vitamin B6 in high doses may cause neurological side-effects. |
| Treatment for persistent pain which has not resolved with IBCLC intervention (for example, non-steroidal anti-inflammatories; antihistamine such as cetirizine; serotonin reuptake inhibitor such as sertraline; beta-blocker such as propranolol; neuralgia medication such as gabapentin) | Central sensitization (breastfeeding pain reasoning model); diagnoses of allodynia, hyperalgesia, functional pain, and neuropathic pain.84,85 | No evidence of benefit for pharmaceutical, psychological, or multi-disciplinary pain clinic treatments. Risks of unintended outcomes, including patient disempowerment and medication side-effects. Serotonin reuptake inhibitors may elicit withdrawal syndrome. 148 Gabapentin may cause a low-grade headache. |
RCT: randomized controlled trial; APNO: all-purpose nipple ointment; IBCLC: International Board Certified Lactation Consultants.
Environmental humidity from occlusion, including from a bra and breastpad, alters skin pH and microbiome, and hydrates the epithelium. This interferes with the cohesive strength of the desmosomes, resulting in worsened epithelial deformation in response to mechanical load, increased length of crack propagation pathways, secondary crack formation, and oblique crack interfaces in the stratum corneum (Appendix 2). A study of skin (from a woman’s breast but not during lactation) found that at 7% relative humidity, the sheer crack plane was aligned with the direction of the stress, but with 100% relative humidity, the cracks were longer, with increased area of crack interface, and an increased energy cost of tissue rupture. 68
Prevention and management of lactation-related nipple–areolar complex wounds
The two key strategies of (1) elimination of repetitive mechanical micro-trauma and (2) avoidance of epithelial overhydration and MASD, above, are fundamental to both the prevention and management of nipple–areolar complex wounds.
There is currently no international consensus on optimal skin wound care even after common skin procedures and excision, with patients receiving a wide variety of recommendations. 149 It is not surprising, then, given the frontier status of clinical breastfeeding support, that there is little research elucidating breastfeeding-related nipple wound healing.
The NDC evolutionary and complex systems approach to prevention and management of inflammatory nipple pain and damage in breastfeeding mirrors a paradigm shift occurring in the treatment of skin wounds. In wound care, the pathogenic micro-organism model which results in antibiotic treatment is increasingly replaced by multi-lateral interventions which aim to optimize the healthy function of the interacting biological systems of host immunity, including the skin microbiome.
Current clinical protocols for the management of breastfeeding-related nipple damage confuse the pathophysiology of acute wounds with that of chronic wounds. A chronic wound regardless of initial insult fails to heal due to endogenous dysregulation of the immune response. 144 A chronic wound is characterized by excessive levels of pro-inflammatory macrophages and an overabundance of inflammatory mediators, as the inflammatory phase of wound healing fails to resolve. This becomes difficult to control clinically due to formation of pathogenic bacterial biofilms, perpetuated by a dysregulated immune environment. The chronic wounds of diabetic foot ulcers, vascular ulcers, and pressure ulcers feature pathogenic biofilm formation, chronic exudation, tissue necrosis, defective re-epithelization, and decreased angiogenesis. 150 In contrast, acute wounds occur in response to external insult and undergo a series of molecular events which result in restoration of structural integrity (Appendix 3). This article argues that although lactation-related nipple pain and damage may be persistent, the injury remains acute. Once the source of repeated mechanical insult ceases, damaged epithelium heals rapidly due to the unique features of the nipple–areolar complex (Table 1).
Table 2 details evidence-based management of lactation-related nipple pain and nipple–areolar complex wounds. Table 3 lists commonly applied strategies which are not effective.
The role of antibiotics
The pathogenic model of wound management assumes that a reduction in microbial load reduces wound infection, and that more or longer antibiotic or anti-fungal treatment is necessary if a wound does not heal. But the pathogenic microbiota paradigm of skin wounds is vigorously contested, including by this article, in the context of the global crisis of antimicrobial resistance and the urgent need for responsible antimicrobial use.151 –154 As the Director General of the World Health Organization stated in 2020: ‘Antimicrobial resistance is a slow tsunami that threatens to undo a century of medical progress’. 151
Research elucidating biofilm development in chronic wounds (such as burns, diabetic, or vascular ulcers) has been erroneously extrapolated to inform clinical protocols for management of nipple skin showing signs of lactation-related inflammation and damage.144,150 Clinical protocols advise that when a purulent exudate is visible on an area of nipple damage, bacterial infection is likely and topical mupirocin or oral antibiotics should be prescribed, citing research which shows that Staphylococcus aureus has been isolated from the nipple of about one-third of women with persistent nipple pain.41,115
But skin microbiomes commonly include S. aureus in the absence of pain or damage. Healthy skin biofilms are strong and dynamic ecological structures created by dense network associations of bacteria and fungi, and integral to the host’s immune defence (Appendix 1). 13 Antibiotics have been shown to destabilize the skin microbiome without altering the diversity or relative abundance of specific targeted species. This may explain why antimicrobial approaches which have proven so effective for internal infections have minimal efficacy against skin wound infections. Several topical formulations of antibiotics have been shown to be ineffective in chronic skin wounds, yet risk bacterial resistance, contact dermatitis, and MASD. 144 A number of studies conclude that most existing approaches to skin wound care are ineffective, and some interfere with healing. 155
Lactation-related nipple damage only rarely requires topical or oral antibiotic application. Wound exudate is mostly protective. A severely purulent exudate which is thick, grey green or yellow, and has a strongly unpleasant odour may warrant topical antibiotic treatment. Oral antibiotics may be required if cellulitis develops beyond the wound border, presenting as erythematous, spreading peri-wound inflammation and swelling, or for impetiginous changes of the nipple–areolar complex with weeping, yellow crusting blisters that do not respond to topical antibiotics.
Conclusion
Nipple pain and damage is common in breastfeeding women. It is associated with low supply and mood disruption and substantially increases the risk of premature cessation of breastfeeding. Nipple pain and damage is a common reason for women to engage in mechanical milk removal rather than direct breastfeeding. However, mechanical milk removal to predominantly feed an infant with expressed breast milk is a work-intensive practice that increases occupational fatigue.
All current clinical protocols for lactation-related nipple pain and damage emphasize the importance of fit and hold (‘latch and positioning’) problems as the primary cause of nipple pain and damage. But clinical breastfeeding support remains a research frontier; commonly applied fit and hold interventions for nipple pain and damage are experience-based only. Fit and hold continues to be an omitted variable bias in clinical breastfeeding research. Given this context and the worldwide trend to overdiagnosis and overtreatment, it is not surprising that management of lactation-related nipple pain and damage is overmedicalized. A wide range of diagnoses and interventions are applied which have been demonstrated to be ineffective, lack an evidence base, and place mothers and babies at risk of unintended outcomes.
This article builds on two previous articles concerning lactation-related breast inflammation, to propose a mechanobiological model of lactation-related nipple pain and wounds. New research concerning skin responses to mechanical stress and the impacts of MASD is translated into clinical approaches. Interventions which avoid inappropriate medicalization but address the underlying mechanical causes of nipple pain and damage in breastfeeding are explicated. These strategies have been delivered over the past decade in clinical contexts in Australia, as part of the foundational breastfeeding domain of NDC (or ‘the Possums programs’).
Evaluation of the clinical implications of the mechanobiological model of lactation-related nipple pain and damage is urgently required, if breastfeeding rates are to increase.
Appendix 1
Key aspects of functional anatomy of the nipple and areolar complex in lactation
Anatomic variability
Human nipple and areolar size, shape, and colour in lactation are remarkably diverse. In a group of 300 Japanese women, 60% had nipples that were cylindrical in shape. In 25%, the nipple was narrower at the base than at the tip. The other 15% were oval. Nipples measured between 6 and 23 mm wide at the nipple base, and could be level with the areola, measured at 0 mm or up to 20 mm high. 156 In a study of 119 Californian women, who were 69% white and 23% Hispanic/Latino, nipple base width ranged between 15 and 34 mm, and height between 5 and 20 mm high (with right nipples significantly longer than left nipples). 141
Nipple–areolar complex skin
Human skin is a layered and composite tissue which acts as a physical and chemical barrier to the external environment. The skin of the lactating nipple–areolar complex is characterized by both unique protective factors and unique exposure to risk (Table 1).
The top surface or face of a woman’s nipple is covered with convoluted epidermal ridges. This article proposes that from an evolutionary perspective, these corrugations have evolved to enhance epidermal elasticity and resilience during breastfeeding. The epidermis of the nipple lacks sensory nerves or blood vessels.
At the base of the epidermis, in the stratum basale, keratinocytes differentiate from epidermal stem cells. These columnar epithelial keratinocytes rest on a basement membrane and are structurally welded together by specialized junctions known as desmosomes. Desmosomes behave like a spring and transmit physical forces throughout the cells. Keratinocytes then differentiate and migrate up through two other layers (the stratum spinosum and the stratum granulosum) towards the surface of the epidermis, producing pro- and anti-inflammatory cytokines. By the time keratinocytes reach the outermost layer, the stratum corneum, they have lost their nucleus and organelles. The stratum corneum comprised about 15 layers of flattened dead keratinocytes, referred to as corneocytes. Each corneocyte is surrounded by a lipid rich matrix and contains a tough, complex network of keratin filaments. The stratum corneum constantly sheds corneocytes, and is impermeable, preventing water loss.
The dermis lies underneath the epidermis, and is a thick fibrous elastic structure, dense in collagen, which gives skin its mechanical strength. The dermis is highly vascular and densely innervated with sensory nerve endings, including nociceptors and mechanoreceptors. 61
Subcutaneous tissue
Most human skin has a subcutaneous base under the dermis, a soft layer of loose connective tissue and fat which contains larger blood vessels and nerves. This subcutaneous layer helps regulate body temperature and acts as a shock-absorber. 63 However, the nipple–areolar complex lacks subcutaneous tissue. Below the areolar muscle, there is just a thin layer of fat with blood vessels, which disappears as it approaches the nipple papilla.
This article proposes that the nipple–areolar complex lack of subcutaneous tissue has three evolutionary advantages.
The vacuum of milk removal acts directly upon superficial lactiferous ducts without the interference of an added cushioning layer.
Ductal dilation is optimized without the added intra-oral volume of subcutaneous tissue.
The nipple is able to achieve a firm shape and definition, in the absence of softening subcutaneous tissue.
Nipple stroma
The nipple core is composed of irregular, very dense fibrous or collagen tissue, which supports the lactiferous ducts, and upon which the dermis rests. Circular and radial smooth muscle fibres run under the dermis of the nipple, and contract upon tactile, mechanical or temperature stimulation. 157 Contractile radial and circular smooth muscle fibres are also found beneath the dermis of the areola, continuous with nipple smooth muscle fibres. Contraction of the nipple and areolar smooth muscle is moderated through the sympathetic adrenergic nerves, and occurs in tandem. Elevation of the nipple papilla has both a visual and tactile effect, orienting the infant for suckling. The nipple warms during breastfeeding due to both vasodilation and the warmth of the infant’s mouth. Nipple duct diameters decrease with cold applications. 158
The face of the lactating nipple has on average nine lactiferous duct orifices (range 4–18). 159 The circular and radial smooth muscle fibres form a mesh-like structure in the connective tissue around the ducts at the tip of the nipple, with larger fibres found along the ducts as they extend into the nipple stroma. Nipple stroma is threaded through with densely interlaced ducts and ductules, small blood vessels, nerves that run to the sensory nerve endings of the dermis, and bundles of smooth muscle tissue. Lactiferous ducts are lined with cuboidal epithelium, but squamous epithelium lines the last one of 2 mm of the duct leading up to the orifice.
Nipple–areolar complex microbiome
The microbiome is part of the skin’s immunoregulatory mechanism and extends deep into the dermis. The host immune system controls the composition of skin microbiomes, although skin microbiomes are also shaped by age, diet, hormonal state, and geographic location. 155 Surface lipids and antimicrobial peptides of intact skin also help to prevent entry of potentially harmful environmental substances and micro-organisms.
The healthy NAC epidermis is therefore a structural scaffold for the NAC microbiome. Nipple microbiome includes biofilm, since microbes immobilize into biofilms when they attach to a surface. A biofilm may be just a few dozen bacteria, or hundreds of thousands of bacteria, and is necessary for skin health. For example, hidradenitis suppurativa is a chronic inflammatory skin disease in which patients have a low numbers of skin bacteria and lack biofilm.
Appendix 2
Moist wound healing worsens nipple pain and damage during lactation
Overhydration and moisture-associated skin damage predispose to epithelial damage and delay healing of skin wounds
Water content is as high as 70% in a healthy epidermis. Continuous exposure of human skin to water for 72–144 h resulted in a mild, transient dermatitis or eczema in half of test sites. 160
Extended hydration alters permeability and flexibility of the stratum corneum, weakens desmosomes, and changes electrical impedance properties. Corneocytes swell with prolonged exposure to water, though the network of keratin filaments limits how much can be absorbed. Hyper-hydration causes desmosome rupture, microstructural changes in lipid self-assembly, and penetration of biomacromolecules through the barrier of the stratum corneum. Extended hydration and swelling of the corneocytes results in increased epidermal thickness, dilation of intracellular spaces, enhanced mitotic rate, and reduced cytokine levels. The temperature of wet skin is lower, and vascular perfusion is higher. Hyper-hydration also penetrates into the dermis.
The term macerated has been used to describe the condition of skin subject to extended hydration. The term maceration lacks a clear definition, though researchers agree that macerated skin is pale and soft, with connective tissue fibres that separate easily, causing skin breakdown. Macerated skin is more alkaline than healthy skin, and a macerated epidermis is more vulnerable to mechanical pressure. In chronic exudative wounds, high levels of peri-wound maceration delay healing.160–162 Maceration is just one component of what is most recently referred to as moisture-associated skin damage (MASD), though there is also no agreed definition for MASD. MASD presents as erythema, maceration, or skin erosion caused by prolonged exposure to a source of moisture. Mechanical forces, such as shearing or stretching pressures, microbial or chemical irritants, wound exudate, or overhydration are required for MASD to occur. 144
A bio-occlusive dressing or membrane allows oxygen in yet retains a moisture balance, so that, the wound is neither too dry nor too moist. In 1962, Dr George Winter found that the superficial skin wounds of young domestic pigs kept humid with vapour-permeable film dressing healed twice as quickly as wounds exposed to the porcine environment. 163 Moist wound healing with bio-occlusive dressings quickly became the accepted practice for the treatment of acute wounds, and soon extended to chronic wounds. Moist wound healing has been extensively studied for burns and skin grafts, and for chronic wounds due to blood circulation insufficiencies, such as pressure sores or diabetic ulcers. Moist wound healing orthodoxy claims that a scab impairs wound healing because it impairs spread of keratinocytes through the exudative layer across the base of the wound. This hypothesis mentions little regarding the role of granulation in the management of exuding wounds. 161
Moist wound healing has been shown to result in patient reports of increased skin pain or discomfort. 160 Recently, researchers have begun to question the orthodoxy of moist wound healing, arguing that semi-permeable moist wound healing may be beneficial in certain contexts, such as chronic wounds, burns and grafts, but that this is not always the case. Scab formation is part of the normal healing of an acute wound, and results in healing without infection even though epithelialization may be slower relative to moist wound healing (Appendix 3). A 2016 study of 10 rabbits’ ears showed that desiccation of acutely generated wounds improved wound healing, with decreased bacterial burden in the wound bed, increased granulation tissue formation, and less upregulation of inflammatory markers compared to saline-treated wounds. 164
The benefits of the hyperosmolar environment which develops during desiccation and scab formation are acknowledged to outweigh the benefits of rapid epithelialization in certain settings. This article argues that this is the case in lactation-related nipple pain and damage, due to the high risk of overhydration and MASD of the lactating nipple–areolar complex.
The evidence does not support moist wound healing for nipple pain and damage
Hydrogel or glycerin dressings are comprised of cross-linked hydrophilic polymers and up to 96% water. As well as providing a moist wound healing environment, they are thought to reduce pain by creating a cold surface on the wound. Lanolin for lactating nipples is treated with hydroxypropyl acrylate (HPA lanolin), which removes pesticide and detergent residues. From at least 1997, clinical protocols have recommended hydrogel breast pads or highly purified lanolin for nipple damage during lactation.
In 1997, Cable et al. from the United States, proposed that moist wound healing in the form of hydrogel dressings should be applied to all breastfeeding-damaged nipples, stating (without data) that several hundred women with nipple damage in the authors’ practice reported pain relief with hydrogel sheets. 165 In 1998, a small US trial in which 42 women with bleeding and cracked nipples were randomized for treatment either with lanolin and breast shells or hydrogel was discontinued early, because a third in the hydrogel group developed infection. Women in the lanolin group reported less pain. 166
A 2003 US study randomized 106 mothers to hydrogel dressings or lanolin ointment between feeds with the aim of preventing nipple pain and damage from the first 24 h after birth. The study was funded by the manufacturer of the hydrogel dressings, and the researchers were not blinded. Women reported a lower pain score on days 10 and 12 in the hydrogel group, and the lanolin group developed more breast infections. But there was no comparison of the amount of nipple damage women experienced, and no report on breastfeeding outcomes. 167
A 2005 Iranian study randomized 63 women with nipple fissures to either lanolin three times daily, breastmilk after each feed, or no treatment. There was no difference in healing time between the breast milk and no-treatment groups, and the nipples of women using lanolin took significantly longer to heal. 168
A 2014 systematic review by Dennis et al. investigating interventions for nipple pain concluded that use of hydrogel, lanolin, or all-purpose nipple ointment did not improve maternal perceptions of pain, and that application of expressed breast milk or no treatment may be equally or more beneficial than application of an ointment, such as lanolin. 41
In 2014, Sasaki et al. retrospectively analysed 131 records from an IBCLC’s practice. Substantially more women in the group who used lanolin developed nipple and areolar erythema with severe pain (burning, stabbing, and between feedings), and/or severe breast pain with a fever and malaise. 169 In 2017, Jackson et al. published a Canadian study that randomized 186 breastfeeding women with nipple pain to lanolin or usual care. Lanoline did not alter the levels of pain experienced by day 7 or breastfeeding duration. 170
In 2018, Neto et al. randomized 180 Brazilian women with pain associated with nipple trauma to use of either lanolin or expressed breast milk. Lanolin was associated with less nipple pain and damage at 49 h after treatment commenced, with the effect persisting for up to 7 days. 171 This corroborated the findings of a 2010 German RCT of 84 lactating mothers with painful and damaged nipples, who had significantly reduced pain with breastfeeding and significantly higher healing rates of nipple trauma within 3 days of commencing lanolin treatment, with effects still evident at 14 days. 172
In 2020, 1084 women in the United Kingdom who had given birth to their youngest child within the last 24 months and had recently completed their breastfeeding journey were surveyed online by a manufacturer of purified lanolin. Seven hundred thirty-nine women (68%) reported that they had experienced physical problems relating to breastfeeding. Of these, 554 (75%) experienced general nipple tenderness or soreness. One hundred seventy-one used lanolin as their primary intervention, and were able to breastfeed an additional 7.3 weeks on average compared to those who did not (33.5 weeks compared to 26.2 weeks). However, this study had multiple methodological weaknesses, including that factors other than lanolin may have increased the duration of breastfeeding. 42
In summary, the research does not support manufacturer’s claims of healing benefits of lanolin or hydrogel sheets for nipple damage. There may be a role for judicious use of these applications when there is a risk that broken nipple epithelium will adhere to breast pads (Table 1).
The nipple–areolar complex in the lactating breast is at increased risk of delayed healing due tomoisture associated skin damage
This article proposes that moist wound healing does not help, and may worsen, nipple blisters, grazes, cracks, and ulcers, because the lactating nipple–areolar complex (NAC) skin is uniquely at risk of MASD (Table 1).
Prevention of skin maceration and overhydration is vital for nipple protection during breastfeeding. Often women present with nipple and areola erythema after applying lanolin, hydrogel sheets, miconazole gel or other topical applications. This is commonly attributed to an allergic reaction, but is more likely to be MASD. Any topical application which hydrates the nipple epithelium risks MASD. The tissue disruption of overhydration makes nipple skin, which is repetitively exposed to vacuum pressure whether from suckling or pumping, more vulnerable to pain and damage, and should be avoided wherever possible. The occlusive conditions of bras and breast pads increase the risk of MASD, placing the damaged nipple epithelium at risk of delayed healing. 160
This article proposes that because of the unique context of the painful or damaged lactating NAC (Table 1), prevention of overhydration and as much opportunity for dry wound healing as possible is necessary to optimize outcomes.
Appendix 3
Mechanisms of nipple–areolar complex wound healing during lactation
Acute wound healing is characterized by four overlapping phases: haemostasis, inflammation, proliferation, and remodelling. 74
Haemeostasis
Once excessive stretching forces result in rupture of nipple epithelial desmosomes, the dermis too may tear, accompanied by microscopic or visible bleeding. Epithelial rupture with or without dermal injury triggers a cascade of inflammatory signals, as an efficient and evolutionary process of wound healing begins. Platelets are carried by the blood stream to the site of damage, combining with blood cells and fibrin to create a clot, which provides a scaffold for incoming inflammatory cells. Neutrophils are immediately recruited as a first line of defence against unfriendly bacteria.
Inflammation
A cascade of signals from broken desmosomes, microvascular trauma, and platelets continue to trigger the inflammatory response, which dilates vasculature and increases endothelial permeability, resulting in exudate. This thin, clear or cloudy moisture is remarkable for its healing properties.
Exudate contains proteins, such as fibrinogen and fibrin and is rich in electrolytes, leukocytes, and proteases, and also protective bioactive molecules, including various growth factors, cytokines, and hormones. Exudate promotes keratinocyte proliferation and fibroblast growth. Exudate neutrophils and later, macrophages, clean the wound of dead or dying tissue. The moisture of the exudate allows cells in the wound area to communicate with each other, ensuring coordinated healing. (Acute wound exudate is very different to the exudate of chronic wounds like diabetic or vascular wounds, which are not equivalent to nipple damage, even when a nipple wound is persistent. Chronic wounds have high levels of proteases.) 74
The moisture, warmth, and nutrients of the wound area alter the microbiome, creating opportunities for colonization by new micro-organisms or for expansion of existing micro-organisms. To heal, diverse populations of bacteria, fungi, and other micro-organisms dynamically interact, modulating each other’s growth, and regulated by the homeostatic control of the host’s immune system. 144
As the clot hardens and dehydrates, an eschar scab forms. The scab may be yellowish, orange, or brown. It is dehydrated and composed of dead cells in a fibrin mesh which seals the breach in the epidermis and acts as a carapace. An epithelial blister similarly acts like bubble wrap, protecting the wound. Both keep micro-organisms out, and allow keratinocytes and broken blood vessels underneath to heal.
Proliferation
Synthesis of collagen by fibrocytes generates a new granulation tissue matrix. Angiogenesis (or blood vessel proliferation) facilitates rich vascularization of the granulation tissue and extracellular matrix deposition, and provides oxygen and nutrients necessary for tissue synthesis. Oxygen also kills harmful anaerobic bacteria.
Remodelling
Stem cells continuously renew keratinocytes, which proliferate and migrate upwards from the basal layer to fill the wound defect. In all phases of wound healing, keratinocytes interact with fibroblasts, endothelial cells, immune cells, growth factors, and cytokines in a coordinated manner. Epidermal cells from sweat glands and the wound periphery also migrate to re-epithelialize the wound. Tissue remodelling and re-epithelization of the wound leads to reconstitution of the physical barrier of the nipple skin. 74
Footnotes
Author contribution(s): Pamela Douglas: Conceptualization; Data curation; Formal analysis; Methodology; and Project administration.
Declaration of conflicting interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author is Medical Director of Possums & Co. www.possumsonline.com, a charity which educates health professionals in Neuroprotective Developmental Care (NDC or ‘the Possums programs’), including in the gestalt approach to clinical breastfeeding support. Possums & Co. offers many free resources but also sells access to the Milk & Moon programmes www.milkandmoonbabies.com which provide parents with breastfeeding information and peer support, and to education resources for providers at ndceducationhub.com. The charity invests all revenue raised back into education and research which supports the well-being of mothers and babies.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The charity Possums & Co. funded the open-access publication fee.
Ethical approval: No ethics approval was required for this paper.
ORCID iD: Pamela Douglas  https://orcid.org/0000-0002-3394-9816
https://orcid.org/0000-0002-3394-9816
References
- 1. Victora CG, Bahl R, Barros AJD, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016; 387: 475–490. [DOI] [PubMed] [Google Scholar]
- 2. Stuebe AM. We need patient-centered research in breastfeeding medicine. Breastfeed Med 2021; 16(4): 349–350. [DOI] [PubMed] [Google Scholar]
- 3. Rey J. Frontier research: bringing the future closer. In: Lychnos: Notebooks of the Fundacion General CSIC (No. 5), June 2011, https://fgcsic.es/lychnos/en_en/forum/frontier_research_bringing_the_future_closer
- 4. Brownlee S, Chalkidou K, Doust J, et al. Evidence for overuse of medical services around the world. Lancet 2017; 390: 156–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Saini V, Brownlee S, Elshaug AG, et al. Addressing overuse and underuse around the world. Lancet 2017; 390: 105–107. [DOI] [PubMed] [Google Scholar]
- 6. Hoffmann TC, Del Mar C. Patients’ expectations of the benefits and harms of treatments, screening and tests – a systematic review. JAMA Intern Med 2015; 175(2): 274–286. [DOI] [PubMed] [Google Scholar]
- 7. Hoffman T, Del Mar C. Clinicians’ expectations of the benefits and harms of treatments, screening, and tests – a systematic review. JAMA Intern Med 2017; 177(3): 407–419. [DOI] [PubMed] [Google Scholar]
- 8. Hanoch Y, Rolison J, Freund AM. Reaping the benefits and avoiding the risks: unrealistic optimism in the health domain. Risk Anal 2018; 39(4): 792–804. [DOI] [PubMed] [Google Scholar]
- 9. Douglas PS, Geddes DB. Practice-based interpretation of ultrasound studies leads the way to less pharmaceutical and surgical intervention for breastfeeding babies and more effective clinical support. Midwifery 2018; 58: 145–155. [DOI] [PubMed] [Google Scholar]
- 10. Douglas P. Diagnosing gastro-oesophageal reflux disease or lactose intolerance in babies who cry a lot in the first few months overlooks feeding problems. J Paediatr Child Health 2013; 49(4): e252–e256. [DOI] [PubMed] [Google Scholar]
- 11. Kapoor V, Douglas PS, Hill PS, et al. Frenotomy for tongue-tie in Australian children (2006-2016): an increasing problem. Med J Aust 2018; 208: 88–89. [DOI] [PubMed] [Google Scholar]
- 12. Wei E, Tunkel D, Boss E, et al. Ankyloglossia: update on trends in diagnosis and management in the United States, 2012-2016. Otolaryngol Head Neck Surg 2020; 163: 1029–1031. [DOI] [PubMed] [Google Scholar]
- 13. Douglas PS. Overdiagnosis and overtreatment of nipple and breast candidiasis: a review of the relationship between the diagnosis of mammary candidiasis and Candida albicans in breastfeeding women. Womens Health 2021; 17: 17455065211031480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ellehauge E, Schmidt Jensen J, Gronhoj C, et al. Trends of ankyloglossia and lingual frenotomy in hospital settings among children in Denmark. Dan Med J 2020; 67(5): A01200051. [PubMed] [Google Scholar]
- 15. Joseph KS, Kinniburgh B, Metcalfe A, et al. Temporal trends in ankyloglossia and frenotomy in British Columbia, Canada, 2004-2013: a population-based study. CMAJ Open 2016; 4(1): E33–E40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dixon B, Gray J, Elliot N, et al. A multifaceted programme to reduce the rate of tongue-tie release surgery in newborn infants: observational study. Int J Pediatr Otorhinolaryngol 2018; 113: 156–163. [DOI] [PubMed] [Google Scholar]
- 17. Douglas PS. Re-thinking benign inflammation of the lactating breast: a mechanobioloon of the nipple: a treatable cause of painful breasgical model. Womens Health 2022; 18: 17455065221075907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Douglas PS. Re-thinking benign inflammation of the lactating breast: classification, prevention, and management. Womens Health 2022. [in press]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust 1978; 2(9): 411–412. [PubMed] [Google Scholar]
- 20. Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol 2008; 22(7): 878–879. [DOI] [PubMed] [Google Scholar]
- 21. James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther 2010; 88(5): 720–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Barrett ME, Heller MM, Fullerton Stone H, et al. Dermatoses of the breast in lactation. Dermatol Ther 2013; 26(4): 331–336. [DOI] [PubMed] [Google Scholar]
- 23. Barrett ME, Heller MM, Fullerton H, et al. Primary herpes simplex virus infection of the nipple in a breastfeeding woman, Cutis 2016; 87(6): E10–11. [PubMed] [Google Scholar]
- 24. Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol 1986; 11(6): 664–666. [DOI] [PubMed] [Google Scholar]
- 25. Crawford E, Whittingham K, Pallett E, et al. An evaluation of Neuroprotective Developmental Care (NDC/Possums Programs) in the first 12 months of life. Matern Child Health J 2022; 26(1): 110–123. [DOI] [PubMed] [Google Scholar]
- 26. Douglas PS, Keogh R. Gestalt breastfeeding: helping mothers and infants optimise positional stability and intra-oral breast tissue volume for effective, pain-free milk transfer. J Hum Lact 2017; 33(3): 509–518. [DOI] [PubMed] [Google Scholar]
- 27. Douglas PS, Perrella SL, Geddes DT. A brief gestalt intervention changes ultrasound measures of tongue movement during breastfeeding: case series. BMC Pregnancy Childbirth 2022; 22: 94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Douglas P, Hill P. Managing infants who cry excessively in the first few months of life. BMJ 2011; 343: d7772. [DOI] [PubMed] [Google Scholar]
- 29. Douglas PS. Excessive crying and gastro-oesophageal reflux disease in infants: misalignment of biology and culture. Med Hypotheses 2005; 64(5): 887–898. [DOI] [PubMed] [Google Scholar]
- 30. Douglas PS, Hill PS. A neurobiological model for cry-fuss problems in the first three to four months of life. Med Hypotheses 2013; 81(5): 816–822. [DOI] [PubMed] [Google Scholar]
- 31. Douglas P, Miller Y, Bucetti A, et al. Preliminary evaluation of a primary care intervention for cry-fuss behaviours in the first three to four months of life (‘The Possums Approach’): effects on cry-fuss behaviours and maternal mood. Aust J Prim Health 2013; 21: 38–45. [DOI] [PubMed] [Google Scholar]
- 32. Whittingham K, Douglas PS. Optimising parent-infant sleep from birth to 6 months: a new paradigm. Infant Ment Health J 2014; 35: 614–623. [DOI] [PubMed] [Google Scholar]
- 33. Douglas PS. Pre-emptive intervention for autism spectrum disorder: theoretical foundations and clinical translation. Front Integr Neurosci 2019; 13: 66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Ball H, Douglas PS, Kulasinghe K, et al. The Possums Infant Sleep Program: parents’ perspectives on a novel parent-infant sleep intervention in Australia. Sleep Health 2018; 4(6): 519–526. [DOI] [PubMed] [Google Scholar]
- 35. Ball H, Taylor CE, Thomas V, et al. Development and evaluation of ‘Sleep, Baby & You’ – an approach to supporting parental well-being and responsive infant caregiving. PLoS ONE 2020; 15(8): e0237240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Odom E, Li R, Scanlon KS, et al. Reasons for earlier than desired cessation of breastfeeding. Pediatrics 2013; 131(3): e726–e732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Dias JS, Vieira TDO, Vierira GO. Factors associated to nipple trauma in lactation period: a systematic review. Rev Bras Saude Materno Infant 2017; 17(1): 27–42. [Google Scholar]
- 38. Li R, Fein SB, Chen J, et al. Why mothers stop breastfeeding: mothers’ self-reported reasons for stopping during the first year. Pediatrics 2008; 122(Suppl. 2): S69–S76. [DOI] [PubMed] [Google Scholar]
- 39. Buck ML, Amir LH, Cullinane M, et al. Nipple pain, damage and vasospasm in the first eight weeks postpartum. Breastfeed Med 2014; 9: 56–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Jiminez Gomez MI, Meneses Monroy A, Corrillero Martín J, et al. Prevalence of nipple soreness at 48 hours postpartum. Breastfeed Med 2021; 16(4): 325–331. [DOI] [PubMed] [Google Scholar]
- 41. Dennis C, Jackson K, Watson J. Interventions for treating painful nipples among breastfeeding women. Cochrane Database Syst Rev 2014; 12: CD007366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Bourdillon K, McCausland T, Jones S. Latch-related nipple pain in breastfeeding women: the impact on breastfeeding outcomes. Br J Midwifery 2020; 28(7): 406–414. [Google Scholar]
- 43. McClellan HL, Hepworth AR, Garbin CP, et al. Nipple pain during breastfeeding with or without visible trauma. J Hum Lact 2012; 28(4): 511–521. [DOI] [PubMed] [Google Scholar]
- 44. Coca KP, Amir LH, Da Silva Alves MDR, et al. Measurement tools and intensity of nipple pain among women with or without damaged nipples: a quantitative systematic review. J Adv Nurs 2018; 75: 1162–1172. [DOI] [PubMed] [Google Scholar]
- 45. Kent JC, Ashton E, Hardwick C, et al. Nipple pain in breastfeeding mothers: incidence, causes and treatments. Int J Environ Res Public Health 2015; 12: 12247–12263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Puapornpong P, Paritakul P, Suksamarnwong M, et al. Nipple pain incidence, the predisposing factors, the recovery period after care management, and the exclusive breastfeeding outcome. Breastfeed Med 2017; 12: 169–173. [DOI] [PubMed] [Google Scholar]
- 47. Feenstra MM, Jørgine Kirkeby M, Thygesen M, et al. Early breastfeeding problems: a mixed method study of mothers’ experiences. Sex Reprod Healthc 2018; 16: 167–174. [DOI] [PubMed] [Google Scholar]
- 48. Santos KJ, Santana GS, Vieira TDO, et al. Prevalence and factors associated with cracked nipples in the first month postpartum. BMC Pregnancy Childbirth 2016; 16: 209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Doherty T, Sanders D, Jackson D. Early cessation of breastfeeding amongst women in South Africa: an area needing urgent attention to improve child health. BMC Pregnancy Childbirth 2012; 12: 105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Strong GD. Provider management and support for breastfeeding pain. J Obstet Gynecol Neonatal Nurs 2011; 40(6): 753–764. [DOI] [PubMed] [Google Scholar]
- 51. Thompson RE, Kruske S, Barclay L, et al. Potential predictors of nipple trauma from an in-home breastfeeding programme: a cross-sectional study. Women Birth 2016; 29(4): 336–344. [DOI] [PubMed] [Google Scholar]
- 52. Watkins S, Meltzer-Brody S, Zolnoun D. Early breastfeeding experiences and postpartum depression. Obstet Gynecol 2011; 118(2, Pt 1): 214–221. [DOI] [PubMed] [Google Scholar]
- 53. Brown A, Rance J, Bennett P. Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. J Adv Nurs 2016; 72(2): 273–282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Cullinane M, Amir LH, Donath SM, et al. Determinants of mastitis in women in the CASTLE study: a cohort study. BMC Fam Pract 2015; 16: 181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Geddes DT, Gridneva Z, Perrella SL, et al. 25 years of research in human lactation: from discovery to translation. Nutrients 2021; 13: 1307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Newton M, Newton NR. The let-down reflex in human lactation. J Pediatr 1948; 33(6): 698–704. [DOI] [PubMed] [Google Scholar]
- 57. McClellan HI, Geddes DT, Kent JC, et al. Infants of mothers with persistent nipple pain exert strong sucking vacuums. Acta Paediatr 2008; 97(9): 1205–1209. [DOI] [PubMed] [Google Scholar]
- 58. McClellan HL, Kent JC, Hepworth AR, et al. Persistent nipple pain in breastfeeding mothers associated with abnormal infant tongue movement. Int J Environ Res Public Health 2015; 12: 10833–10845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Geddes DT, Langton DB, Gollow I, et al. Frenulotomy for breastfeeding infants with ankyloglossia: effect on milk removal and sucking mechanism as imaged by ultrasound. Pediatrics 2008; 122(1): e188–e194. [DOI] [PubMed] [Google Scholar]
- 60. Kent JC, Mitoulas LR, Cregan MD, et al. Importance of vacuum for breastmilk expression. Breastfeed Med 2008; 3(1): 11–19. [DOI] [PubMed] [Google Scholar]
- 61. Pawlaczyk M, Lelonkiewicz M, Wieczorowski M. Age-dependent biomechanical properties of the skin. Postepy Dermatol Alergol 2013; 5: 302–306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Tokuyama E, Nagai Y, Takahashi K. Mechanical stretch on human skin equivalents increases the epidermal thickness and develops the basement membrane. PLoS ONE 2015; 10(11): e0141989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Tepole AB, Gosain AK, Kuhl E. Stretching skin: the physiological limit and beyond. Int J Non Linear Mech 2012; 47(8): 938–949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Monemian Esfahani A, Rosenbohm J, Reddy K, et al. Tissue regeneration from mechanical stretching of cell-cell adhesion. Tissue Eng Part C Methods 2019; 25(11): 631–640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Sweeney EL, Al-Shehri SS, Cowley DM, et al. The effect of breastmilk and saliva combinations on the in vitro growth of oral pathogenic and commensal microorganisms. Sci Rep 2018; 8: 15112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Pan L, Zhang X, Gao Q. Effects and mechanisms of histatins as novel skin wound-healing agents. J Tissue Viability 2021; 30(2): 190–195. [DOI] [PubMed] [Google Scholar]
- 67. Hajishengallis G, Russell MW. Innate humoral defense factors. Mucosal Immunol 2015; 1: 251–270. [Google Scholar]
- 68. Liu X, Cleary J, German GK. The global mechanical properties and multi-scale failure mechanics of heterogeneous human stratum corneum. Acta Biomater 2016; 43: 78–87. [DOI] [PubMed] [Google Scholar]
- 69. Schwerla F, Daake B, Moeckel E, et al. Osteopathic treatment of infants in their first year of life: a prospective multicenter observational study (OSTINF study). Complement Med Res 2021; 28(5): 395–406. [DOI] [PubMed] [Google Scholar]
- 70. Mills N, Lydon A-M, Davies-Payne D, et al. Imaging the breastfeeding swallow: pilot study utilizing real-time MRI. Laryngoscope Investig Otolaryngol 2020; 5(3): 572–579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Geddes DT, Sakalidis VS. Ultrasound imaging of breastfeeding – a window to the inside: methodology, normal appearances, and application. J Hum Lact 2016; 32(2): 340–349. [DOI] [PubMed] [Google Scholar]
- 72. Mills N, Keough N, Geddes DT, et al. Defining the anatomy of the neonatal lingual frenulum. Clin Anat 2019; 32(6): 824–835. [DOI] [PubMed] [Google Scholar]
- 73. Zimmerman E, Thompson K. Clarifying nipple confusion. J Perinatol 2015; 35(11): 895–899. [DOI] [PubMed] [Google Scholar]
- 74. Rodrigues M, Kosaric N, Bonham CA, et al. Wound healing: a cellular perspective. Physiol Rev 2019; 99(1): 665–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Olsen N, Nielson SL. Prevalence of primary Raynaud’s phenomenon in young females. Scand J Clin Lab Invest 1978; 37: 761–776. [DOI] [PubMed] [Google Scholar]
- 76. Berens P, Eglash A, Malloy M, et al. Persistent pain with breastfeeding: ABM clinical protocol #26. Breastfeed Med 2016; 11: 46–56. [DOI] [PubMed] [Google Scholar]
- 77. Amir LH, Beaza C, Charlamb JR, et al. Identifying the cause of breast and nipple pain during lactation. BMJ 2021; 374: n1628. [DOI] [PubMed] [Google Scholar]
- 78. Anderson JE, Held N, Wright K. Raynaud’s phenomenon of the nipple: a treatable cause of painful breastfeeding. Pediatrics 2004; 113(4): e360–e364. [DOI] [PubMed] [Google Scholar]
- 79. Mitchell K, Eglash A, Bamberger E. Mammary dysbiosis and nipple blebs treated with intravenous daptomycin and dalbavancin. J Hum Lact 2020; 36(2): 365–368. [DOI] [PubMed] [Google Scholar]
- 80. Mitchell K, Johnson HM. Breast pathology that contributes to dysfunction of human lactation: a spotlight on nipple blebs. J Mammary Gland Biol Neoplasia 2020; 25(2): 79–83. [DOI] [PubMed] [Google Scholar]
- 81. Rodriguez JM, Fernandez L. Infectious mastitis during lactation: a mammary dysbiosis model. In: McGuire M, Bode L. (eds) Prebiotics and probiotics in human milk. New York: Academic Press, 2017, pp. 401–428. [Google Scholar]
- 82. Witkowska-Zimny M, Kaminska-El-Hassan E. Cells of human breast milk. Cell Mol Biol Lett 2017; 22: 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. O’Hara M. Bleb histology reveals inflammatory infiltrate that regresses with topic steroids: a case series. Breastfeed Med 2012; 7(Suppl. 1): S2. [Google Scholar]
- 84. Amir LH, Jones LE, Buck ML. Nipple pain associated with breastfeeding: incorporating current neurophysiology into clinical reasoning. Aust Fam Physician 2015; 44(3): 127–132. [PubMed] [Google Scholar]
- 85. Muddana A, Asbill DT, Jerath MR, et al. Quantitative sensory testing, antihistamines, and beta-blockers for management of persistent breast pain: a case series. Breastfeed Med 2018; 13(4): 275–280. [DOI] [PubMed] [Google Scholar]
- 86. Mosely L. Reconceptualising pain according to modern pain science. Phys Ther Rev 2007; 12(3): 169–178. [Google Scholar]
- 87. International Association for the Study of Pain. Definitions of chronic pain syndromes, 2022, https://www.iasp-pain.org/advocacy/definitions-of-chronic-pain-syndromes/
- 88. Fitzcharles M-A, Cohen SP, Clauw DJ, et al. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet 2021; 397: 2098–2110. [DOI] [PubMed] [Google Scholar]
- 89. International Association for the Study of Pain. Terminology, 2022, https://www.iasp-pain.org/resources/terminology/#pain
- 90. Moseley LG, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain 2015; 16(9): 807–813. [DOI] [PubMed] [Google Scholar]
- 91. Lucas R, Zhang Y, Walsh SJ, et al. OXTR rs53576 variation with breast and nipple pain in breastfeeding women. Pain Manag Nurs 2021; 22(3): 369–376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Chow S, Chow R, Popovic M, et al. The use of nipple shields: a review. Front Public Health 2015; 3: 236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Coentro VS, Perrella SL, Lai CT, et al. Nipple shield use does not impact sucking dynamics in breastfeeding infants of mothers with nipple pain. Eur J Pediatr 2021; 180: 1537–1543. [DOI] [PubMed] [Google Scholar]
- 94. LeFort Y, Evans A, Livingstone V, et al. Academy of Breastfeeding Medicine Position Statement on ankyloglossia in breastfeeding dyads. Breastfeed Med 2021; 16(4): 278–281. [DOI] [PubMed] [Google Scholar]
- 95. Fraser L, Benzie S, Montgomery J. Posterior tongue tie and lip tie: a lucrative private industry where the evidence is uncertain. BMJ 2020; 371: m3928. [DOI] [PubMed] [Google Scholar]
- 96. Douglas PS. Special edition: tongue-tie expert roundtable. Clin Lact 2017; 8(3): 87–131. [Google Scholar]
- 97. Prevost P, Gleberzon B, Carleo B, et al. Manual therapy for the pediatric population: a systematic review. BMC Complement Altern Med 2019; 19: 60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Herzhaft-Le Roy J, Xhignesse M, Gaboury I. Efficacy of an osteopathic treatment coupled with lactation consultations for infants’ biomechanical sucking difficulties: a randomized controlled trial. J Hum Lact 2017; 33(1): 165–172. [DOI] [PubMed] [Google Scholar]
- 99. Kirk AHP, Yang J, Sim WC, et al. Systematic review of the effect of topical application of human breast milk on early umbilical cord separation. J Obstet Gynecol Neonatal Nurs 2019; 48(2): 121–130. [DOI] [PubMed] [Google Scholar]
- 100. Pietschnig B, Pani M, Kafer A, et al. Use of soft laser in the therapy of sore nipples in breastfeeding women. Adv Exp Med Biol 2000; 478: 437–438. [PubMed] [Google Scholar]
- 101. Posso I, Goncalves S, Posso M, et al. Control of nipple pain during breastfeeding using low level laser therapy. Reg Anesth Pain Med 2007; 32(5): 185. [Google Scholar]
- 102. Araujo AR, Nascimento ALV, Camargos JM, et al. Photobiomodulation as a new approach for the treatment of nipple traumas: a pilot study, randomized and controlled. Fisioter Bras 2013; 14(1): 20–26. [Google Scholar]
- 103. Buck ML, Eckereder G, Amir LH. Low level laser therapy for breastfeeding problems. Breastfeed Rev 2016; 24(2): 27–31. [PubMed] [Google Scholar]
- 104. Chaves MEDA, Araujo AR, Santos SF, et al. LED phototherapy improves healing of nipple trauma: a pilot study. Photomed Laser Surg 2012; 30(3): 172–178. [DOI] [PubMed] [Google Scholar]
- 105. Coca KP, Marcacine KO, Gamba MA, et al. Efficacy of low-level laser therapy in relieving nipple pain in breastfeeding women: a triple-blind, randomized, controlled trial. Pain Manag Nurs 2016; 17(4): 281–289. [DOI] [PubMed] [Google Scholar]
- 106. Camargo BTS, Coca KP, Amir LH, et al. The effect of a single irradiation of low-level laser on nipple pain in breastfeeding women: a randomized controlled trial. Lasers Med Sci 2020; 35: 63–69. [DOI] [PubMed] [Google Scholar]
- 107. Watson Genna C. (ed.). Supporting sucking skills in breastfeeding infants. Burlington, MA: Jones and Bartlett Learning, 2016. [Google Scholar]
- 108. Gavine A, MacGillivray S, Renfew MJ, et al. Education and training of healthcare staff in the knowledge, attitudes and skills needed to work effectively with breastfeeding women: a systematic review. Int Breastfeed J 2017; 12: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Wood NK, Woods NF, Blackburn ST, et al. Interventions that enhance breastfeeding initiation, duration, and exclusivity: a systematic review. MCN Am J Matern Child Nurs 2016; 41(5): 299–307. [DOI] [PubMed] [Google Scholar]
- 110. Boss M, Saxby N, Pritchard D, et al. Interventions supporting medical practitioners in the provision of lactation care: a systematic review and narrative analysis. Matern Child Nutr 2021; 17(3): e13160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Boss E. Normal human lactation: closing the gap. F1000Res 2018; 7: F1000 Faculty Rev-801. [Google Scholar]
- 112. Ingram J, Johnson D, Greenwood R. Breastfeeding in Bristol: teaching good positioning, and support from fathers and families. Midwifery 2002; 18(2): 87–101. [DOI] [PubMed] [Google Scholar]
- 113. Blair A, Cadwell K, Turner-Maffei C, et al. The relationship between positioning, the breastfeeding dynamic, the latching process and pain in breastfeeding mothers with sore nipples. Breastfeed Rev 2003; 11(2): 5–10. [PubMed] [Google Scholar]
- 114. Cadwell K, Turner-Maffei C, Blair A, et al. Pain reduction and treatment of sore nipples in nursing mothers. J Perinat Educ 2004; 13(1): 29–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Amir LH, Bearzatto A. Overcoming challenges faced by breastfeeding mothers. Aust Fam Physician 2016; 45(8): 552–556. [PubMed] [Google Scholar]
- 116. Darmangeat V. The frequency and resolution of nipple pain when latch is improved in a private practice. Clin Lact 2011; 2(3): 22–24. [Google Scholar]
- 117. Righard L, Alade MO. Suckling technique and its effect on success of breastfeeding. Birth 1992; 19(4): 185–189. [DOI] [PubMed] [Google Scholar]
- 118. Henderson A, Stamp G, Pincombe J. Postpartum positioning and attachment education for increasing breastfeeding: a randomized trial. Birth 2001; 28(4): 236–242. [DOI] [PubMed] [Google Scholar]
- 119. de Oliveira LD, Giugliani ER, do Espirito, Santo LC, et al. Effect of intervention to improve breastfeeding technique on the frequency of exclusive breastfeeding and lactation-related problems. J Hum Lact 2006; 22(3): 315–321. [DOI] [PubMed] [Google Scholar]
- 120. Labarere J, Bellin V, Fourny M, et al. Assessment of a structured in-hospital educational intervention addressing breastfeeding: a prospective randomised open trial. BJOG 2003; 110(9): 847–852. [PubMed] [Google Scholar]
- 121. Schafer R, Genna CW. Physiologic breastfeeding: a contemporary approach to breastfeeding initiation. J Midwifery Women’s Health 2015; 60(5): 546–553. [DOI] [PubMed] [Google Scholar]
- 122. Colson SD, Meek JH, Hawdon JM. Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Hum Dev 2008; 84(7): 441–449. [DOI] [PubMed] [Google Scholar]
- 123. Smillie CM. How infants learn to feed: a neurobehavioral model. In: Watson CG. (ed.). Supporting sucking skills in breastfeeding infants. New York: Jones and Bartlett Learning, 2016, pp. 89–111. [Google Scholar]
- 124. Moore ER, Berman N, Anderson GC, et al. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev 2016; 11: CD003519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Wang Z, Liu Q, Min L, et al. The effectiveness of laid-back position on lactation related nipple problems and comfort: a meta-analysis. BMC Pregnancy Childbirth 2021; 21: 248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Milinco J, Travan L, Cattaneo A, et al. Effectiveness of biological nurturing on early breastfeeding problems: a randomized controlled trial. Int Breastfeed J 2020; 15(1): 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Yin C, Su X, Liang Q, et al. Effect of baby-led self-attachment breastfeeding technique in the postpartum period on breastfeeding rates: a randomized study. Breastfeed Med 2021; 16: 734–740. [DOI] [PubMed] [Google Scholar]
- 128. Svensson KE, Velandia M, Matthiesen A-ST, et al. Effects of mother-infant skin-to-skin contact on severe latch-on problems in older infants: a randomized trial. Int Breastfeed J 2013; 8: 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Nakhash R, Wasserteil N, Mimouni FB, et al. Upper lip tie and breastfeeding: a systematic review. Breastfeed Med 2019; 14(2): 83–87. [DOI] [PubMed] [Google Scholar]
- 130. Shah S, Allen P, Walker R, et al. Upper lip tie: anatomy, effect on breastfeeding, and correlation with ankyloglossia. Laryngoscope 2021; 131(5): E1701–E1706. [DOI] [PubMed] [Google Scholar]
- 131. Douglas PS, Cameron A, Cichero J, et al. Australian Collaboration for Infant Oral Research (ACIOR) Position Statement 1. Upper lip-tie, buccal ties, and the role of frenotomy in infants. Australas Dent Pract 2018: 144–146, https://pameladouglas.com.au/sites/default/files/Upperlip-tiebuccaltiesandtheroleoffrenotomy2018ADP.pdf
- 132. Van Biervliet S, Van Winckel M, Velde SV, et al. Primum non nocere: lingual frenotomy for breastfeeding problems, not as innocent as generally accepted. Eur J Pediatr 2020; 179: 1191–1195. [DOI] [PubMed] [Google Scholar]
- 133. Walsh J, Links A, Boss E, et al. Ankyloglossia and lingual frenotomy: national trends in inpatient diagnosis and management in the United States, 1997-2012. Otolaryngol Head Neck Surg 2017; 156(4): 735–740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Ghaheri B, Lincoln D, Mai TNT, et al. Objective improvement after frenotomy for posterior tongue-tie: a prospective randomized trial. Otolaryngol Head Neck Surg. Epub ahead of print 7 September 2021. DOI: 10.1177/01945998211039784. [DOI] [PubMed] [Google Scholar]
- 135. Douglas PS. Making sense of studies which claim benefits of frenotomy in the absence of classic tongue-tie. J Hum Lact 2017; 33(3): 519–523. [DOI] [PubMed] [Google Scholar]
- 136. Heaton PJ. Posterior tongue tie and lip tie – division of tongue-tie: surgical complications. BMJ 2021; 372: n8. [DOI] [PubMed] [Google Scholar]
- 137. Kim DH, Dickie A, Shih ACH, et al. Delayed hemorrhage following laser frenotomy leading to hypovolemic shock. Breastfeed Med 2021; 16(4): 346–348. [DOI] [PubMed] [Google Scholar]
- 138. Hale M, Mills N, Edmonds L, et al. Complications following frenotomy for ankyloglossia: a 24-month prospective New Zealand Paediatric Surveillance Unit study. J Paediatr Child Health 2019; 56(4): 557–562. [DOI] [PubMed] [Google Scholar]
- 139. Solis-Pazmino P, Kim GS, Lincango-Naranjo E. Major complications after tongue-tie release: a case report and systematic review. Int J Pediatr Otorhinolaryngol 2021; 1(138): 110356. [DOI] [PubMed] [Google Scholar]
- 140. Vazirinejad R, Darakhshan S, Esmaeili A, et al. The effect of maternal breast variations on neonatal weight gain in the first seven days of life. Int Breastfeed J 2009; 4: 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Ventura AK, Lore B, Mireles O. Associations between variations in breast anatomy and early breastfeeding challenges. J Hum Lact 2021; 37(2): 403–413. [DOI] [PubMed] [Google Scholar]
- 142. O’Shea JE, Foster JP, O’Donnell CPF, et al. Frenotomy for tongue-tie in newborn infants (review). Cochrane Database Syst Rev 2017; 3: CD011065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Yabes JM, White BK, Murray CK. In vitro activity of manuka honey and polyhexamethylene biguanide on filamentous fungi and toxicity to human cell lines. Med Mycobiol 2017; 1(55): 3343–3343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Drago F, Gariazzo L, Cioni M. The microbiome and its relevance in complex wounds. Eur J Dermatol 2019; 29(1): 6–13. [DOI] [PubMed] [Google Scholar]
- 145. Marrazzu A, Sanna MG, Dessole F. Evaluation of the effectiveness of a silver-impregnated medical cap for topical treatment of nipple fissure of breastfeeding mothers. Breastfeed Med 2015; 10(5): 232–238. [DOI] [PubMed] [Google Scholar]
- 146. Niazi A, Rahimi VB, Soheili-Far S, et al. A systematic review on prevention and treatment of nipple pain and fissure: are they curable? J Pharmacopuncture 2018; 21(3): 139–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Dennis C-L, Schottle N, Hodnett E, et al. An all-purpose nipple ointment versus lanolin in treating painful damaged nipples in breastfeeding women: a randomized controlled trial. Breastfeed Med 2012; 7(6): 473–479. [DOI] [PubMed] [Google Scholar]
- 148. Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: are guidelines evidence-based? Addict Behav 2019; 97: 111–121. [DOI] [PubMed] [Google Scholar]
- 149. Nguyen JK, Huang A, Siegel DM, et al. Variability in wound care recommendations following dermatologic procedures. Dermatol Surg 2020; 46(2): 186–191. [DOI] [PubMed] [Google Scholar]
- 150. Raziyeva K, Kim Y, Zharkinbekov Z. Immunology of acute and chronic wound healing. Biomolecules 2021; 11(5): 700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. World Health Organization. Addressing the crisis in antibiotic development, 2020, https://www.who.int/news/item/09-07-2020-addressing-the-crisis-in-antibiotic-development
- 152. Editorial. The antimicrobial crisis: enough advocacy, more action. Lancet 2020; 395(10220): 247. [DOI] [PubMed] [Google Scholar]
- 153. Durham P. Why antibiotic resistance really is a tragedy. The Medical Republic, 29 May 2019, https://medicalrepublic.com.au/antibiotic-resistance-really-tragedy/21127
- 154. Lesho EP, Laguio-Vila M. The slow-motion catastrophe of antimicrobial resistance and practical interventions for all prescribers. Mayo Clin Proc 2019; 94(6): 1040–1047. [DOI] [PubMed] [Google Scholar]
- 155. Sams-Dodd J, Sams-Dodd F. Time to abandon antimicrobial approaches in wound healing: a paradigm shift. Wounds 2018; 30(11): 345–352. [PubMed] [Google Scholar]
- 156. Sanuki J-i, Fukuma E, Uchida Y. Morphologic study of nipple-areola complex in 600 breasts. Aesthetic Plast Surg 2008; 33(3): 295–297. [DOI] [PubMed] [Google Scholar]
- 157. Geddes DT. Ultrasound imaging of the lactating breast: methodology and application. Int Breastfeed J 2009; 4: 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158. Gardner H, Lai CT, Ward LC, et al. Thermal physiology of the lactating nipple influences the removal of human milk. Sci Rep 2019; 9: 11854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159. Ramsay DT, Kent JC, Hartmann RA, et al. Anatomy of the lactating human breast redefined with ultrasound imaging. J Anat 2005; 206(6): 525–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160. Whitehead F, Giampieri S, Graham T, et al. Identifying, managing and preventing skin maceration: a rapid review of the clinical evidence. J Wound Care 2017; 26(4): 159–165. [DOI] [PubMed] [Google Scholar]
- 161. Rippon MG, Ousey K, Cutting KF. Wound healing and hyper-hydration: a counterintuitive model. J Wound Care 2016; 25(2): 68, 70–75. [DOI] [PubMed] [Google Scholar]
- 162. Ousey K, Cutting KF, Rogers AA, et al. The importance of hydration in wound healing: reinvigorating the clinical perspective. J Wound Care 2016; 25(3): 122, 124–130. [DOI] [PubMed] [Google Scholar]
- 163. Winter G. Formation of the scab and the rate of epithelization of superficial wounds in the skin of the young domestic pig. Nature 1962; 193: 293–294. [DOI] [PubMed] [Google Scholar]
- 164. Park E, Long SA, Seth AK, et al. The use of desiccation to treat Staphylococcus aureus biofilm-infected wounds. Wound Repair Regen 2016; 24(2): 394–401. [DOI] [PubMed] [Google Scholar]
- 165. Cable B, Stewart M, Davis J. Nipple wound care: a new approach to an old problem. J Hum Lact 1997; 13(4): 313–318. [DOI] [PubMed] [Google Scholar]
- 166. Brent N, Rudy SR, Redd B, et al. Sore nipples in breast-feeding women: a clinical trial of wound dressings vs conventional care. Arch Pediatr Adolesc Med 1998; 152(11): 1077–1082. [DOI] [PubMed] [Google Scholar]
- 167. Dodd V, Chalmers C. Comparing the use of hydrogel dressings to lanolin ointment with lactating mothers. J Obstet Gynecol Neonatal Nurs 2003; 32(4): 486–494. [DOI] [PubMed] [Google Scholar]
- 168. Mohammadzadeh A, Farhat A, Esmaeily H. The effect of breast milk and lanolin on sore nipples. Saudi Med J 2005; 26(8): 1231–1234. [PubMed] [Google Scholar]
- 169. Sasaki BC, Pinkerton K, Leipelt A. Does lanolin use increase the risk of infection in breastfeeding women? Clin Lact 2014; 5(1): 28–32. [Google Scholar]
- 170. Jackson KT, Dennis C-L. Lanolin for the treatment of nipple pain in breastfeeding women: a randomized controlled trial. Matern Child Nutr 2017; 13(3): e12357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171. Neto CM, de Albuquerque RS, de Souza SC, et al. Comparative study of the use of HPA lanolin and breast milk for treating pain associated with nipple trauma. Rev Bras Ginecol Obstet 2018; 40(11): 664–672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172. Abou-Dakn M, Fluhr JW, Gensch M, et al. Positive effect of HPA lanolin versus expressed breastmilk on painful and damaged nipples during lactation. Skin Pharmacol Physiol 2010; 2011(24): 27–35. [DOI] [PubMed] [Google Scholar]