

Abstract
Background
The anti‐inflammatory effects of n‐3 (omega‐3 fatty acids, fish oil) have been suggested to be beneficial in chronic inflammatory disorders such as inflammatory bowel disease. This review is an update of a previously published Cochrane review.
Objectives
To systematically review the efficacy and safety of n‐3 for maintenance of remission in Crohn's disease (CD).
Search methods
The following databases were searched from inception to November 2013 without language restriction: CENTRAL, MEDLINE, EMBASE, HealthSTAR, PubMed, and ACP journal club.
Selection criteria
Randomized placebo‐controlled trials (RCT) of n‐3 for maintenance of remission in CD were included. Studies must have enrolled patients of any age group, who were in remission at the time of recruitment, and were followed for at least six months. The intervention must have been fish oil or n‐3 given in pre‐defined dosage. Co‐interventions were allowed only if they were balanced between the study groups.
Data collection and analysis
The primary outcome was the relapse rate and secondary outcomes included change in disease activity scores, time to first relapse and adverse events. Two independent investigators reviewed studies for eligibility, extracted the data and assessed study quality using the Cochrane risk of bias tool. The overall quality of the evidence supporting the primary and selected secondary outcomes was reassessed for the current update using the GRADE system. We used the RevMan software for analyses. We calculated the risk ratio (RR) and corresponding 95% confidence interval (CI) for dichotomous outcomes and the hazard ratio and 95% CI for time‐to‐event outcomes. Random‐effects or fixed‐effect models were used according to degree of heterogeneity and sensitivity analyses were performed in an attempt to explore possible sources of heterogeneity.
Main results
Six studies with a total of 1039 patients were eligible for inclusion. The two largest studies were rated as low risk of bias for all assessed items. Four studies were rated as unclear risk of bias for randomization and allocation concealment. Two studies were rated as high risk of bias for incomplete outcome data and selective reporting. There was a marginal significant benefit of n‐3 therapy for maintenance of remission. Thirty‐nine per cent of patients in the n‐3 group relapsed at 12 months compared to 47% of placebo patients (6 studies, 1039 patients; RR 0.77, 95% CI 0.61 to 0.98). A GRADE analysis rated the overall quality of the evidence for the primary outcome (i.e. relapse) as very low due to unexplained heterogeneity (I2 = 58%), publication bias, and a high or unknown risk of bias in four studies in the pooled analysis. When two large studies at low risk of bias were considered the benefit was no longer statistically significant. Thirty‐seven per cent of patients in the n‐3 group relapsed at 12 months compared to 42% of placebo patients (2 studies, 738 patients; RR 0.88, 95% CI 0.74 to 1.05). No significant heterogeneity was identified for this pooled analysis ( I2 = 0%). A GRADE analysis indicated that the overall quality of the evidence supporting this outcome was moderate due to sparse data (294 events). No serious adverse events were recorded in any of the studies but in a pooled analyses there was a significantly higher rate of diarrhea (4 studies, 862 patients; RR 1.36 95% CI 1.01 to 1.84) and upper gastrointestinal tract symptoms (5 studies, 999 patients; RR 1.65, 95% CI 1.25 to 2.18) in the n‐3 treatment group.
Authors' conclusions
Evidence from two large high quality studies suggests that omega 3 fatty acids are probably ineffective for maintenance of remission in CD. Omega 3 fatty acids appear to be safe although they may cause diarrhea and upper gastrointestinal tract symptoms.
Keywords: Adult; Child; Humans; Crohn Disease; Crohn Disease/diet therapy; Fatty Acids, Omega‐3; Fatty Acids, Omega‐3/therapeutic use; Fish Oils; Fish Oils/therapeutic use; Randomized Controlled Trials as Topic; Remission Induction; Secondary Prevention
Plain language summary
Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn's disease
Fish oil contains omega 3 fatty acids that may be beneficial in reducing inflammation, such as seen in the bowel of Crohn's disease patients. Randomized placebo‐controlled studies that evaluated the effect of daily intake of capsules containing omega‐3 fatty acids to maintain remission in Crohn's disease were reviewed. Six studies including 1039 patients were included in the review. A pooled analysis of six studies suggests a marginal benefit for omega 3 fatty acids over placebo (i.e. fake medicine) in preventing relapse of disease at one year. However, these results need to be interpreted with caution due to differences across the studies in terms of induction of remission regimens (e.g. surgical remission versus drug therapy) patients (e.g. adult versus pediatric patients) and medication regimens (e.g. some studies used different placebos), the possibility of publication bias (i.e. only studies with positive results are published) and low methodological quality in four studies in the pooled analysis. When the two largest and highest quality studies were pooled the results showed no benefit to omega‐3 treatment over placebo. There were no serious side effects in any of the studies. Common side effects included unpleasant taste, bad breath, heartburn, nausea and diarrhea. Evidence from two large high quality studies suggests that omega 3 fatty acids are probably ineffective for maintenance of remission in CD. Omega 3 fatty acids appear to be safe although they may cause diarrhea and upper gastrointestinal tract symptoms.
Summary of findings
for the main comparison.
| n‐3 therapy compared with placebo for maintaining remission in CD | ||||||
|
Patient or population: Crohn's disease patients in remission Settings: adult and pediatric outpatient gastroenterology and IBD centers, single‐center and multicenter; not stated in one study (Belluzzi 1997). Intervention: n‐3 or fish oil capsules Comparison: placebo capsules | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| placebo | n‐3 or fish oil capsules | |||||
| Relapse rate at one year (all studies) | Study population |
RR 0.77 (0.61 to 0.98) |
1039 (6 studies) | ⊕⊝⊝⊝ very low2,3,4 | ||
| 471 per 10001 | 363 per 1000 (287 to 462) | |||||
| Relapse rate at one year (sensitivity analysis of Belluzi 1996) | Study population | RR 0.77 (0.64 to 0.93) | 904 (5 studies) | ⊕⊝⊝⊝ very low3,4,5 | ||
| 459 per 1000 | 353 per 1000 (294 to 462) | |||||
| Relapse rate at one year (only EPIC studies) | Study population | RR 0.88 (0.74 to 1.05) | 738 (2 studies) | ⊕⊕⊕⊝ moderate6 | Well‐designed and implemented studies, larger than all other studies combined | |
| 424 per 1000 | 373 per 1000 (314 to 445) | |||||
| Adverse events rate‐Diarrhea | Study population | RR 1.36 (1.01 to 1.84) | 862 (4 studies) | ⊕⊕⊕⊝ moderate7 | ||
| 140 per 1000 | 190 per 1000 (141 to 258) | |||||
| Adverse events rate‐ Upper GI (nausea, vomiting, halitosis, heartburn, dyspepsia, dysgeusia and bloating) | Study population | RR 1.98 (1.38 to 2.85) | 999 (5 studies) | ⊕⊕⊕⊝ moderate8 | ||
| 123 per 1000 | 244 per 1000 (170 to 351) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk Ratio;RD: Risk Difference;OR: Odds Ratio; HR: Hazard Ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 The control group risk estimate comes from the control arm of the included studies. 2 Significant unexplained heterogeneity. 3 Likely publication bias is indicated by the absence of negative small studies. 4 Two of the studies in the analysis were at high risk of bias due to incomplete outcome data and selective reporting. 5 Sparse data (374 events). 6 Sparse data (294 events). 7 Sparse data (144 events). 8 Sparse data (167 events).
Background
Crohn's disease Crohn's disease (CD) is characterized by chronic intestinal inflammation causing a varying spectrum of clinical symptoms. Some patients have chronically active disease, while others have a pattern of clear exacerbations and remissions. It is currently hypothesized that chronic inflammation develops in genetically susceptible hosts in response to as yet unidentified environmental triggers, likely microbial in origin. No maintenance medication has been shown to be completely effective in preventing relapse, and thus prolonging remission intervals while minimizing adverse reactions has been the aim of treatment. Adherence to a low residue diet may reduce symptoms in patients with intestinal stenosis and administration of formulated food as the sole source of nutrition is efficacious in alleviating mucosal inflammation (Zachos 2007). Otherwise, no dietary restrictions or interventions have been convincingly shown to treat active CD or to prevent clinical exacerbation.
Omega‐3 poly‐unsaturated fatty acids (n‐3) Randomized controlled trials have suggested a positive effect of n‐3 in various disease states, including cardiovascular, inflammatory, immunological, psychological, and neurological disorders (Akabas 2006; Belluzzi 2002; Ergas 2002; Hooper 2004; Ruxton 2004; Simopoulos 2002). The beneficial effects of n‐3 are thought to be secondary to anti‐inflammatory, antithrombotic, antiarrhythmic, hypolipidemic and vasodilatory properties. Omega‐3 polyunsaturated fatty acids (n‐3) are incorporated into the wall of inflammatory cells and decrease the concentration of arachidonic acid (C20:4, n‐6). Arachidonic acid is the key substrate of cyclooxygenase and 5‐lipoxygenase enzymes which produce proinflammatory cytokines (Hillier 1991). In this way, n‐3 fatty acids reduce the production of leukotriene B4, thromboxane A2, prostaglandin E2, interleukin‐1, interleukin‐6 and tumor necrosis factor, and scavenge free radicals (Endres 1989; Fisher 1986; Kim 1996; Lee 1985; Simopoulos 2002).
Although n‐3 can be obtained from various vegetables, the major source of n‐3 is fish oil. The marine sources of n‐3 include eicosapentanoic acid (EPA or 20:5), docosahexanoic acid (DHA, 22:6) and docosapentanoic acid (DPA, 22:5), which are the longer chain n‐3 forms. Alpha linolenic acid (ALA, 18:3) is the shorter chain n‐3 obtained from nuts and vegetable oils. Although an endogenous process exists whereby ALA can be partially converted to the effective longer chain n‐3, there is debate about the effectiveness of this conversion (Arterburn 2006; Ruxton 2004).
n‐3 and Crohn's disease Studies on animal models and tissues of IBD patients have demonstrated the strong anti‐inflammatory properties of n‐3 (Nakazawa 2000; Vilaseca 1990). It has been proposed that a diet rich in fish oil protected the Japanese from IBD and now the rate of IBD is increasing due to dietary shift from n‐3 to n‐6 (Nakazawa 2000). Reports of n‐3 use for maintaining remission in CD have been conflicting (MacLean 2005). Although n‐3 has an excellent safety profile, when administered as raw fish oil it was shown to have troublesome adverse effects that reduced compliance. These adverse effects include unpleasant taste, halitosis, heartburn, nausea and diarrhea (Kim 1996; Lorenz 1989). Investigators have suggested the use of enteric coated capsules to improve compliance and absorption (Belluzzi 1994).
Importance of this review Narrative reviews of fish oil in CD have reported conflicting conclusions, based on the same published studies (Belluzzi 2002; Endres 1999; Kim 1996; Nakazawa 2000; Simopoulos 2002). Our previous systematic review published in 2009 concluded that omega‐3 fatty acids are probably ineffective for maintenance of remission in Crohn's disease (Turner 2009). In light of continued public interest in finding natural alternatives or adjuncts to current immunosuppressive therapies and the four years that have elapsed since the last literature search, we aimed to update our previous review.
Objectives
The primary objective of this study was to systematically review the effectiveness of fish oil or n‐3 for maintaining remission in CD. A secondary objective was to evaluate the adverse events associated with fish oil or n‐3 for maintaining remission in CD.
Methods
Criteria for considering studies for this review
Types of studies
Randomized placebo‐controlled trials of fish oil or n‐3 therapy administered for at least six months, reporting at least one of the primary or the secondary outcomes and published in any language, were included in this review. Studies published in an abstract form only were included if enough data were provided to assess the reported outcomes.
Types of participants
Crohn's disease patients (diagnosed using established criteria) who were in remission at the time of recruitment were included. We did not apply any age restrictions (both pediatric and adult patients were included). The following validated clinical indices could have been used to assess disease activity and remission: the Crohn's disease activity index (CDAI) (Best 1976), the pediatric Crohn's disease activity index (PCDAI) (Hyams 1991), the weighted pediatric Crohn's disease activity index (wPCDAI) and the other short versions (Turner 2012), and the Harvey‐Bradshaw index (Harvey 1980). In practice, only the first two indices were used in the eligible studies.
Types of interventions
Trials were included if fish oil or n‐3 supplementation was given in any form (capsule, enteric coated or liquid) but with a defined dose. Co‐interventions were allowed only if they were balanced between the study groups. Studies in which the intervention group received diet enriched with fish products were excluded as the dose was not clear in these studies and other confounding variables could exist.
Types of outcome measures
Primary outcome The primary outcome was the relapse rate during the observation time. Definitions of relapse were guided by the validated indices specified above.
Secondary outcome The secondary outcomes were change in disease activity scores, time to first relapse and adverse events (diarrhea, nausea, vomiting, halitosis, heartburn, alterations in low density lipoproteins, alterations in glucose level, increase in bleeding time and abdominal pain). Withdrawal rate of participants among the intervention and control groups was also recorded. Other outcomes were recorded, if available: admission rate, use of steroids, disease activity at the end of follow‐up period and quality of life. However, most of these data were not available. Studies reporting only surrogate outcomes (e.g. serum or tissue levels of cytokines or inflammatory markers) were excluded.
Search methods for identification of studies
Search methods for identification of studies
Electronic databases
An on‐line database literature search from inception to November 2013 was performed for human studies, without language restrictions, using the following databases: MEDLINE (NLM, National Library of Medicine, Bethesda), EMBASE (Elsevier, NY) and HealthSTAR on OVID, as well as PubMed (NLM), the Cochrane Central Register of Controlled Trials (CENTRAL) and ACP journal club. On‐going trials were identified from the registry link: www.clinicaltrials.gov. The search strategies used for each database are documented in Appendix 1. All abstracts found by the above search strategy underwent individual screening for eligibility by DT.
Other sources Additional citations were identified by manually searching the references of articles retrieved from the computerized databases and relevant review articles. Unpublished studies were sought by contacting experts in the field, but none were identified.
Data collection and analysis
Selection of studies Abstracts of all articles meeting the above search strategy were screened for eligibility. Full text studies were retrieved if they were potentially eligible for inclusion. The retrieved full text articles were then independently reviewed by DT and AMG for eligibility. Disagreements were to be resolved by consensus between the remaining investigators.
Data extraction and management Two investigators (DT, AMG) independently completed a data extraction form for all eligible studies. The following data were retrieved:
1. General information: title, journal, year, published or unpublished. 2. Study information: design, ways used to ensure adequacy of randomization, concealment of allocation and blinding, power calculation (a priori and post hoc). 3. Intervention: form and dose of n‐3, type of comparison group, special diet used. 4. Eligibility: inclusion and exclusion criteria, total number screened and randomized. 5. Baseline characteristics (in each group): age, sex, race, disease severity (and how evaluated), concurrent medications used. 6. Follow‐up: length of follow‐up, assessment of compliance, withdrawals and loss to follow‐up. 7. Outcome: time to first relapse, disease activity at each evaluation time (and how was assessed) number of relapses during the follow‐up period, adverse events, use of steroid, number of hospital admissions and weight.
Assessment of methodological quality of included studies
Two authors (RL and OL) independently assessed the quality of included studies using the Cochrane risk of bias tool (Higgins 2011). Factors assessed included:
random sequence generation;
allocation concealment;
blinding;
incomplete outcome data;
selective outcome reporting; and
other potential sources of bias.
We rated each of these factors as ‘low risk’, ‘high risk’ or ‘unclear risk’. Disagreements were resolved by consensus.
We used the GRADE approach to assess the overall quality of evidence for the primary outcome and selected secondary outcomes of interest. Outcomes from pooling of randomized trials start as high quality evidence, but may be downgraded due to: (1) risk of bias, (2) indirectness of evidence, (3) inconsistency (unexplained heterogeneity), (4) imprecision (sparse data), and (5) reporting bias (publication bias). The overall quality of evidence for each outcome was determined after considering each of these elements, and categorized as high quality (i.e. further research is very unlikely to change our confidence in the estimate of effect); moderate quality (i.e. further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate); low quality (i.e. further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate); or very low quality (i.e. we are very uncertain about the estimate) (Guyatt 2008; Guyatt 2011; Schünemann 2011).
Missing data Primary authors were contacted for missing data, but none replied. A sensitivity analysis was planned in this case.
Statistical analysis Categorical data (as relapsed or not during the follow‐up period) for each study were transformed into two by two tables.
Measures of treatment effect We calculated the risk ratio (RR) and corresponding 95% confidence interval (95% CI) for dichotomous outcomes. For the primary analysis the actual relapse rate was used rather than the estimated rate (controlling for censored data), since most studies did not report the estimated relapse rate. The number needed to treat to benefit (NNTB) and the absolute risk reduction (risk difference) and corresponding 95% CI were also calculated where appropriate. For time‐to‐event data we calculated the hazard ratio (HR) and corresponding 95% CI. No continuous variables (i.e. number of relapses) were reported in the studies.
Meta‐analysis Random‐effects or fixed‐effect models were used to pool studies depending on clinical and statistical heterogeneity. Weighting was assigned according to the Mantel‐Haenszel method. For time‐to‐event analyses, the generic inverse variance function was used, inputting the lnHR (hazard ratio) with its lnSE (standard error) derived from the reported 95% CI of the HR. The lnSE was obtained using the formula: lnSE=(ln(lower 95% CI limit)‐ln(upper 95% CI limit))/3.92.
Assessment of Heterogeneity First, studies were independently reviewed for any clinical and methodological heterogeneity and possible reasons for heterogeneity were sought. The decision of whether to pool studies was aided by calculating the I2 measure, interpreted as 25% (low heterogeneity), 50% (moderate) and 75% (high) (Higgins 2003). Next, the Cochran Chi2 test for homogeneity (Q test) was calculated, and since the test has low sensitivity to detect heterogeneity, P < 0.1 was considered to be statistically significant.
Subgroup analysis A priori subgroup analyses were planned, governed by the number of identified studies: different dosing of eicosapentoic acid (EPA), follow‐up duration (< 9 months and > 9 months), pediatric versus adult population (< 18 years of age and > 18 years), different formulation of the fish oil (raw, encapsulated, or enteric coated).
Sensitivity analysis In order to assess the robustness of the eligibility criteria, planned sensitivity analyses included excluding poor quality studies, small studies (< 50 patients) and studies published in abstract form. A funnel plot was constructed to assess the possibility of publication bias.
Results
Description of studies
Results of the search The initial search yielded 142 non‐duplicated articles (See Figure 1). Based on abstract review, all potentially controlled trials and review articles for reference search were retrieved. Nineteen full text articles were assessed for eligibility. Two studies were excluded because they were not randomized controlled trials (Mate 1991; Tsujikawa 2000). Eight studies were excluded because they enrolled only active patients (i.e. focusing on whether n‐3 can induce remission (Bamba 2003; Eivindson 2005; Nielsen 2005; Sakurai 2002; Seidman 2003; Socha 2002; Trebble 2004; Trebble 2005). One study was excluded because it enrolled patients with active and inactive Crohn's disease (Lorenz 1989). Two studies were excluded because n‐3 treatment was for less than six months (Bjorkkjaer 2004; Geerling 2000). Six studies with a total of 1039 patients were included in this review (table of included studies). Two independent trials (EPIC‐1 and EPIC‐2) were reported in the same manuscript (Feagan 2008a) and were included in the last update (Turner 2009). No new studies were published since 2008, and thus no additional studies were included in the current review update. Agreement among reviewers regarding the eligibility of the included studies was 100%.
1.
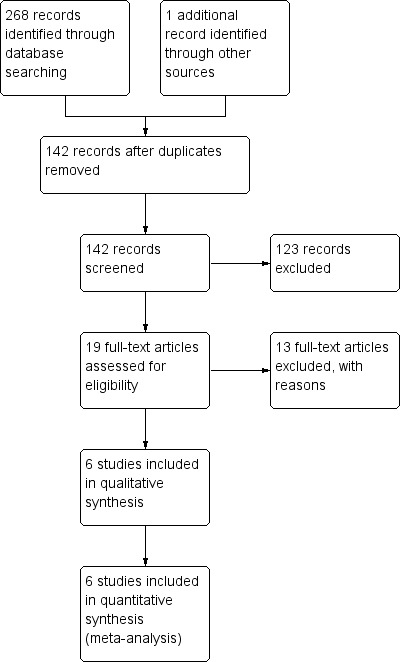
Study flow diagram.
Included studies: 1. Belluzzi 1996
Design: A double blind, placebo‐controlled trial of one year duration.
Sample size: A total of 78 adults (18 to 67 years of age, 50% men), 39 in each arm.
Setting: Outpatient clinics in Italy.
Participants: At baseline, participants were in remission (CDAI < 150 for at least 3 months, but less than 2 years) and high risk for relapse, judged by an increase in at least one of three serum inflammatory markers. No concurrent medications were allowed and there were no diet restrictions. Patients were followed every three months until one year.
Interventions: Enteric coated fish oil capsule with 60 minutes delay timed release (1.8 g/day of EPA and 0.9 g/day of DHA, as free fatty acids) versus identical placebo of 500 mg Miglyol 812 (a mixed‐acid triglyceride of fractionated medium chain fatty acids made up of caprylic and capric acid). The enteric coated time released capsules were used to avoid troubling adverse reactions such as nausea and halitosis thereby improving compliance.
Outcomes: Relapse rates over one year of follow‐up, as defined by CDAI > 150 or an increase of at least 100 points in CDAI from baseline for two weeks. Adverse events and time to first relapse were also monitored.
Design: A double blind, placebo‐controlled trial of one year duration with three groups: n‐3, placebo and reduced carbohydrate intake. The data and discussion regarding this study will refer only to the n‐3 intervention group in comparison with the placebo group (which was the primary aim of the trial).
Sample size: A total of 135 adults (17 to 65 years of age, 31% men), 70 in the n‐3 arm and 65 in the placebo arm.
Setting: Multicenter study in Germany.
Participants: At baseline, participants were in remission (CDAI < 150), induced with a course of corticosteroids. Steroids were still administered during the first two months of the study, but no other co‐interventions were allowed. Patients were instructed to consume a diet low in arachidonic acid and rich in fiber and were followed every three months until one year.
Interventions: Gelatin n‐3 capsules (3.3 g/day of EPA and 1.8 g/day of DHA, as ethyl Esther) versus identical placebo of corn oil. A second intervention group was treated with a low carbohydrate diet but was ignored for the purpose of this review.
Outcome: Primary outcome was the relapse free time period after randomization as defined by CDAI > 200 and a change from baseline CDAI by at least 60 points, plus an increase of C‐reactive protein serum level two standard deviations above normal mean. Relapse rate and adverse events were also monitored.
This study was published in abstract form only. Additional information was supplied by the author by personal communication.
Design: A double blind, placebo‐controlled trial of one year duration.
Sample size: A total of 50 adults (mean age 39 ± 13.8 years in the n‐3 group, and 35.2 ± 7.9 in the control group, 58% male), 26 in the n‐3 arm and 24 in the control arm.
Setting: Outpatients at a single IBD center in Italy.
Participants: Crohn's disease patients in remission (CDAI < 150) one month following ileal resection. No co‐interventions were administered and no specific diet was prescribed; participants were asked to continue their previous dietary habits.
Interventions: The n‐3 group received the same regimen as Belluzzi 1996 (enteric coated fish oil capsules with 60 minutes delay time release composed of 1.8 g/day of EPA and 0.9 g/day of DHA, as free fatty acids). Placebo capsules were Miglyol 812, as in Belluzzi 1996.
Outcome: Relapse rates during a one year follow‐up were recorded. Relapse was measured both clinically (CDAI > 150 with an increase of > 50 points from baseline) and by endoscopic or radiological appearance. For the meta‐analysis, only clinical relapse rates were included, similar to the other three included trials.
4. Romano 2005
Design: A double blind, placebo‐controlled trial of one year duration.
Sample size: A total of 38 children (5 to 16 years of age, 53% male), 18 in the n‐3 group and 20 in the comparison group.
Setting: Pediatric gastroenterology centers in Italy.
Participants: At baseline, participants were in remission (PCDAI < 20 for at least two months). Exclusion criteria included previous intestinal resection, previous immunomodulator therapy, and corticosteroid therapy in the last three months. No diet restrictions are reported.
Interventions: Time dependent 5‐ASA (50 mg/kg/day) plus n‐3 in gastro‐resistant capsules (TRIOLIP‐SOFAR, Italy; 1.2 g/day of EPA and 0.6 g/day of DHA, as triglycerides) versus time dependent 5‐ASA (50 mg/kg/day) plus an olive oil placebo.
Outcome: Primary outcome was relapse rate within one year follow‐up as defined by PCDAI > 20. Time to first relapse was also recorded but not thoroughly presented.
5. Feagan 2008a (EPIC‐1)
Design: A double blind, placebo‐controlled trial of 52 weeks duration.
Sample size: A total of 383 adults randomized, but only 363 were eligible for the modified intention‐to‐treat (ITT) analysis, for which data were included only from patients who received at least 1 dose of the study drug and who provided any post randomization data (mean age 40.5 ± 15.2 years in the n‐3 group and 38.2 ± 13.1 in the control group, 45% male), 183 in the n‐3 group and 180 in the comparison group. Nine of the excluded patients were enrolled by a single site that violated the protocol in various cases.
Setting: Fifty‐one IBD sites in Canada, Europe, Israel, and United States between January 2003 and February 2007. Patients were evaluated one week before randomization, at the time of randomization and at 4, 16, 30, 44, and 52 weeks thereafter.
Participants: At baseline, eligible participants were in remission (CDAI < 150) for at least three months and had at least one exacerbation within the previous year. Exclusion criteria included allergy or intolerance to n‐3 or fish products; treatment with 5‐aminosalicylates, immunosuppressives, tumor necrosis factor‐α antagonists, or investigational drugs; existence of ostomy or short bowel syndrome; bowel resection or obstruction in the preceding 3 months; malignancy (with the exception of resected basal or squamous cell skin cancer or carcinoma of the cervix in situ); substance abuse; and severe medical diseases other than CD.
Interventions: Two time released 1 g gelatin capsules of n‐3 twice daily (Epanova; Tillotts Pharma AG, Ziefen, Switzerland) consisted of approximately 2.2 g/day of EPA and 0.8 g/day of DHA as free fatty acids versus identical placebo of four 1 g of medium‐chain triglyceride oil. To enhance tolerability, patients began with an initial dose of 1 g/day of the study drug for the first 7 days, increased to 2 g/day for 7 days and then further increased to the final dose. No new medications were allowed after randomization.
Outcome: Primary outcome was time to relapse, defined by either an increase of the CDAI score to 150 points or greater and an increase of more than 70 points from the score calculated at the randomization visit, or the initiation of prohibited medical therapy or surgery for symptomatic active CD. Secondary outcomes were the change in mean scores on the CDAI and SF‐36, the change in the mean serum triglyceride concentration, and the occurrence of adverse events.
6. Feagan 2008b (EPIC‐2)
Design: A double blind, placebo‐controlled trial of 58 weeks duration.
Sample size: A total of 379 adults randomized, but only 375 were eligible and received at least one dose of study medication and thus included in the analysis (mean age 38.5 ± 13.8 years in the n‐3 group and 40 ± 13.6 in the control group, 43% male), 187 in the n‐3 group and 188 in the comparison group.
Setting: Forty‐seven IBD sites in Canada, Europe, Israel, and United States between January 2003 and February 2007. Patients were evaluated at 8 weeks before randomization, at the time of randomization and at 2, 8, 16, 30, 44, and 58 weeks thereafter.
Participants: Patients with active disease were treated with a standardized 16‐week tapering course of either prednisone or budesonide at initial doses of 40 mg once daily and 9 mg once daily, respectively. If the CDAI score was < 150 points 8 weeks after the initiation of corticosteroid, than the patient was eligible for randomization. At this time, patients were receiving either 20 mg/day of prednisone or 6 mg/day of budesonide. Exclusion criteria were similar to those described in EPIC‐1.
Interventions: Similar to the EPIC‐1 trial. Corticosteroids were tapered off over 8 weeks.
Outcome: Primary and secondary outcome measures were similar to those used in EPIC‐1. In addition, an increase of the corticosteroid dose to control symptoms was considered a failure of treatment.
Risk of bias in included studies
None of the eligible articles were excluded based on poor quality. The results of the risk of bias analysis are summarized in Figure 2. Lorenz‐Meyer 1996 did not describe methods used for randomization or allocation concealment and was rated as unclear for these items. Follow‐up was adequate; however, the study had a drop‐out rate of 8/70 (11%) in the intervention arm and 7/65 (11%) in the control arm. Another 7 and 8 patients, respectively, violated the protocol but the results represent an ITT analysis. Belluzzi 1996 was a well designed study, but the report is lacking description on the methods used for randomization and allocation concealment. Blinding and follow‐up were well described. The drop‐out rate was 9%: 3% lost to follow‐up and 6% withdrew because of diarrhea. These patients were not included in the relapse rate calculation and, thus, we performed sensitivity analysis to account for this potential bias. Belluzzi 1997 was published as an abstract, with additional details supplied directly by the author. The drop‐out rate was high (16%), and only 16/26 in the n‐3 arm and 15/24 in the control arm were assessed for the primary outcome (endoscopic recurrence). Patients with clinical relapse were excluded from the analysis and this could be a source of attrition bias. Romano 2005 was a small but well designed study. The report lacked a description of the methods used for randomization and allocation concealment. A concern was raised from the unexpectedly high rate of relapse among the control group. Follow‐up was adequate and no patient dropped‐out. The results of laboratory testing were not reported and this item was rated as high risk of bias.
2.
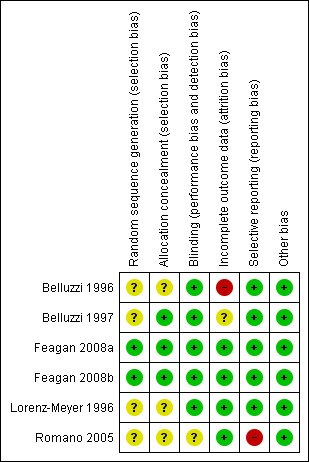
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Feagan 2008a reports the results of the EPIC‐1 and EPIC‐2 studies. In these well designed, performed and reported studies, eligible patients were randomized in a 1:1 ratio using a central randomization number generator stratified by the induction therapy received prior to randomization or the duration of remission. Neither the investigators nor the patients were aware of the treatment assignment. Adherence to the study drug as assigned was evaluated at each clinic visit by interviewing the patient and by capsule counts. Lost to follow‐up (not including patients that terminated the study early due to clinical relapse) was high but still in the acceptable range: 15.1% in EPIC‐1 and 12.8% in EPIC‐2. One critique of these studies is that the sample size calculation was performed for relapse rate while the primary outcome was based on survival analysis.
Effects of interventions
See: Table 1
Relapse rate All included studies reported the relapse rate at 1 year. Belluzzi 1996 found that significantly less patients from the intervention group relapsed (n = 11, 28%) compared to placebo (n = 27, 69%; P < 0.001) and concluded that enteric coated, timed release n‐3 is highly effective in maintaining remission in Crohn's disease. This was not an ITT analysis as the outcome of patients who dropped out due to relocation (n = 2, 3%) or adverse events (n = 5, 6%) was not recorded. However, extrapolating from the survival curve, the estimated 1‐year relapse rate was 39% in the intervention arm and 75% in the placebo arm. Lorenz‐Meyer 1996 found no difference in the relapse rate of the intervention group (n = 40, 57%) compared to placebo (n = 36, 55%; P = 0.84). Extrapolating from the survival curve, the estimated one year relapse rate was 69% in both groups. The authors concluded that gelatin capsules of ethyl ester fish oil capsules are not effective for maintenance of remission in Crohn's disease. Belluzzi 1997 found no benefit for n‐3 therapy for maintenance of remission after ileal resection. During the one year follow‐up, less patients from the intervention group experienced clinical relapse (n = 2, 8% versus n = 5, 21%; P = 0.24) or histological relapse compared to placebo (n = 9, 34% versus n = 15, 62%; P = 0.09). The authors concluded that enteric coated, timed release fish oil seems to be effective for maintenance of remission after ileal resection in Crohn's disease. A very high relapse rate was found in the placebo group of the Romano 2005 study (n = 19/20, 95% in the placebo group compared with n = 11/18, 61% in the intervention group; P < 0.001). Romano 2005 concluded that enteric coated n‐3 in addition to 5‐ASA are effective for maintenance of remission in pediatric Crohn's disease. In this study compliance was optimal, no patients were lost to follow‐up and all patients were analyzed.
In both EPIC‐1 and EPIC‐2 trials (Feagan 2008a), the largest of all existing studies, no significant difference in the relapse rate was found between the patients treated with n‐3 or placebo. In EPIC‐1, 54/183 (29.5%) treated with n‐3 relapsed compared to 62/180 (34.4%) in the placebo group (P = 0.31). To control for 55 patients who discontinued the intervention prematurely but did not experience a relapse (26 in the n‐3 group and 29 in the placebo group) a survival analysis was used, estimating the 1‐year relapse rate of the n‐3 group to be 31.6%, compared with 35.7% of the placebo group (P = 0.30). In EPIC‐2, the relapse rate was 84/187 (44.9%) and 94/188 (50%) in the n‐3 and placebo groups, respectively (P=0.38). The 1‐year relapse rate controlled for 48 patients who discontinued the intervention prematurely but did not experience a relapse (30 in the n‐3 group and 18 in the placebo group) was estimated at 47.8% and 48.8% in the n‐3 and placebo groups, respectively (P = 0.48).
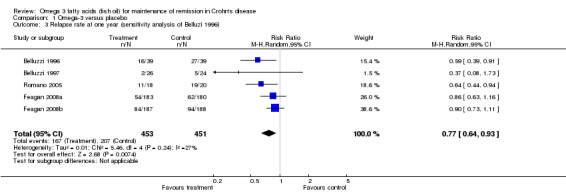
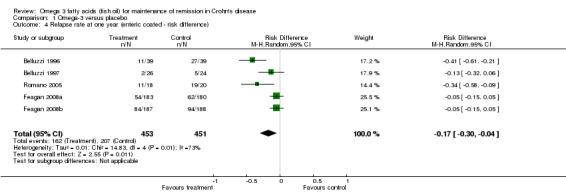
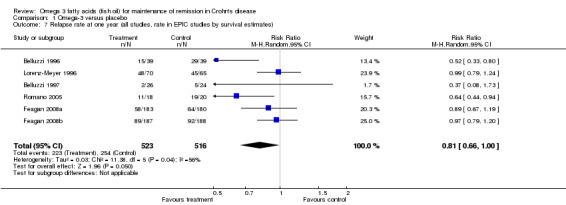
Since all studies shared the primary outcome (relapse rate over 1 year in quiescent CD patients) the data were pooled in a meta‐analysis (See Analysis 1.1). In the case of Belluzzi 1997, clinical relapse was included (in contrast with endoscopic or radiographic relapse) to make it comparable with the other studies. The pooled risk ratio was statistically significant in favor of omega‐3 fatty acids. Thirty‐nine per cent of patients in the n‐3 group relapsed at 12 months compared to 47% of placebo patients (6 studies, 1039 patients; RR 0.77, 95% CI 0.61 to 0.98). A GRADE analyses rated the overall quality of the evidence for the primary outcome (i.e. relapse) as very low due to unexplained heterogeneity (I2 = 58%), potential publication bias, and a high or unknown risk of bias in four studies in the pooled analysis. Although each study is somewhat different (i.e. one pediatric, one looked at post resection maintenance, one published in an abstract form, and some used a different placebo), the study by Lorenz‐Meyer 1996 differed the most having used a different formulation and dose of n‐3. Thus, a subgroup analysis of the five studies that used enteric coated capsules was performed (See Analysis 1.2). There was a reduction in the risk of relapse with the use of enteric coated n‐3 compared with placebo with statistically significant heterogeneity (P = 0.05, I2 = 58%). The pooled effect was statistically significant (RR 0.71, 95% CI 0.54 to 0.93). This analysis was repeated after considering all drop‐out patients in the intervention arm of Belluzzi 1996 as failures and all drop‐outs in the control arm as successes (See Analysis 1.3), but this did not alter the results (RR 0.77, 95% CI 0.64 to 0.93). As shown in Analysis 1.4, the absolute risk reduction was 17% (95% CI 4% to 30%), and the calculated NNTB to prevent one relapse over a one year period was 5 (95% CI 3 to 25).
1.1. Analysis.
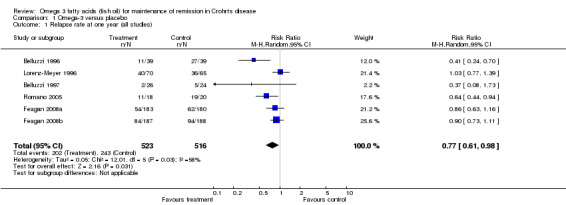
Comparison 1 Omega‐3 versus placebo, Outcome 1 Relapse rate at one year (all studies).
1.2. Analysis.
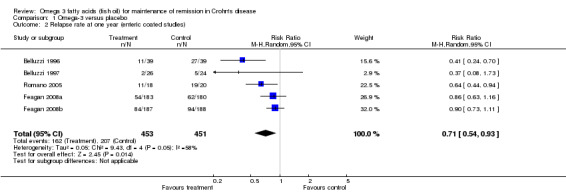
Comparison 1 Omega‐3 versus placebo, Outcome 2 Relapse rate at one year (enteric coated studies).
1.3. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 3 Relapse rate at one year (sensitivity analysis of Belluzi 1996).
1.4. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 4 Relapse rate at one year (enteric coated ‐ risk difference).
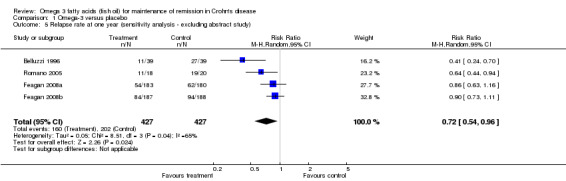
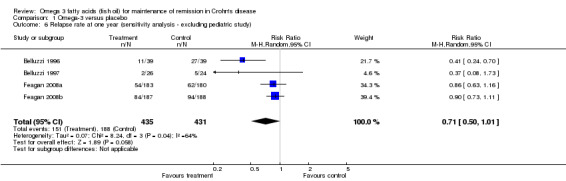
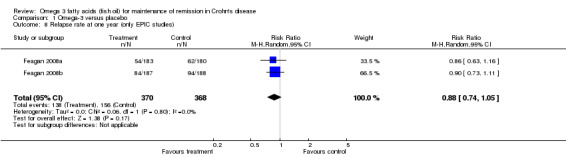
A sensitivity analysis excluding the abstract publication (See Analysis 1.5) did not change the results (RR 0.72; 95% CI 0.54 to 0.96). When the pediatric study by Romano 2005 was excluded (See Analysis 1.6) the risk ratio was no longer statistically significant (RR 0.71; 95% CI 0.50 to 1.01). When including the estimated one year relapse rate (Belluzzi 1996; Feagan 2008a; Lorenz‐Meyer 1996), rather than the actual relapse rate, the pooled risk ratio was no longer statistically significant (Analysis 1.7; RR 0.61, 95% CI 0.37 to 1.02; I2 = 56%). When combining only the two largest and most rigorously performed studies, EPIC‐1 and EPIC‐2, the risk ratio was not statistically significant (See Analysis 1.8). Thirty‐seven per cent of patients in the n‐3 group relapsed at 12 months compared to 42% of placebo patients (2 studies, 738 patients; RR 0.88, 95%CI 0.74 to 1.05). No heterogeneity was detected for this comparison (I2 = 0%). A GRADE analysis indicated that the overall quality of the evidence supporting this outcome was moderate due to sparse data (294 events).
1.5. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 5 Relapse rate at one year (sensitivity analysis ‐ excluding abstract study).
1.6. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 6 Relapse rate at one year (sensitivity analysis ‐ excluding pediatric study).
1.7. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 7 Relapse rate at one year (all studies, rate in EPIC studies by survival estimates).
1.8. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 8 Relapse rate at one year (only EPIC studies).
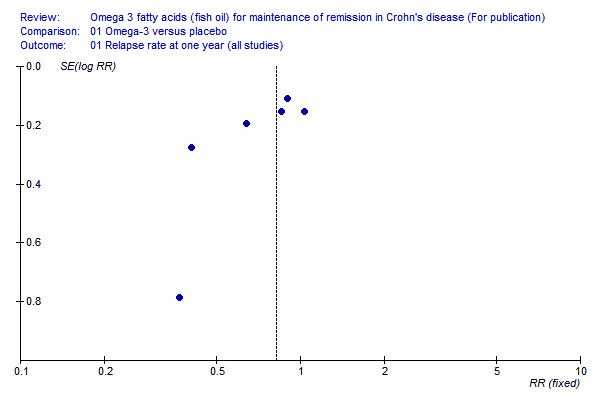
The small number of included studies limited the ability to construct a valid funnel plot. Nonetheless, the funnel plot (Figure 3) suggests the possibility of publication bias, with the representation of three positive but no negative low weighted studies. Time to first relapse Five studies reported on time to first relapse. Romano 2005 reported the median time to first relapse which was eight months in the intervention group compared to one month in the placebo group. No survival analysis or formal comparisons were presented. Belluzzi 1996 presented a survival curve; the median relapse free time was four months in the placebo group compared to greater than one year in the fish oil group (log rank test 0.006). At the end of the follow‐up period, 23 of the 39 patients in the intervention arm (59%) and 10 of the 39 patients in the placebo group (26%) were still in remission (P = 0.003). In EPIC‐1, EPIC‐2 (Feagan 2008a) and Lorenz‐Meyer 1996 a survival analysis was the primary aim. In Lorenz‐Meyer 1996, extrapolating from the Kaplan Meier curve, the median relapse free periods of the placebo and the intervention arms were 133 and 159 days, respectively. This difference was not significant in both the ITT and per protocol analyses. Similarly, the proportion of relapse free patients after one year of follow‐up was 31% in both groups.
3.
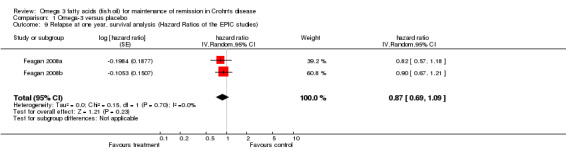
Only EPIC‐1 and EPIC‐2 reported the Hazard Ratio (HR) with 95% CI (HR 0.82, 95% CI 0.57 to 1.18 for EPIC‐1, and HR 0.90, 95% CI 0.67 to 1.21 for EPIC‐2). The pooled log HR did not show any superiority for n‐3 treatment relative to placebo (Analysis 1.9; HR 0.87, 95% CI 0.69 to 1.09). No heterogeneity was detected for this comparison (I2 = 0%). Disease activity at the end of the year Belluzzi 1996 reported on change of disease activity at the end of the follow‐up period. The reduction in three inflammatory markers (erythrocytes sedimentation rate, serum alpha 2 globulins and alpha 1‐acid glycoprotein) was significantly larger in the fish oil group compared to placebo. The EPIC‐1 and EPIC‐2 studies reported no significant differences between the study groups in CDAI scores, but data were not shown (Feagan 2008a).
1.9. Analysis.
Comparison 1 Omega‐3 versus placebo, Outcome 9 Relapse at one year, survival analysis (Hazard Ratios of the EPIC studies).
Biological effect of n‐3 Five studies reported the biological effect of treatment. Two studies evaluated the incorporation of n‐3 into red blood cells (RBC) membranes and three studies evaluated the change in serum triglycerides. Belluzzi 1996 presented data on patients who remained in remission at the end of the follow‐up period. Omega 3 fatty acids replaced 50% of the RBC arachidonic acid in the intervention arm and remained unchanged in the placebo arm. Romano 2005 showed that all subjects in the intervention arm had a statistically significant increase in the RBC concentration of EPA and DHA, and a decrease in arachidonic acid. Lorenz‐Meyer 1996, and Feagan 2008a (EPIC‐1 and EPIC‐2) reported a significant decrease in serum triglycerides among n‐3 treated patients compared to placebo. Quality of life No significant difference in SF‐36 scores was found between the study groups in the EPIC‐1 and EPIC‐2 studies (Feagan 2008a). These data were not shown.
Adverse events Overall, no serious adverse events were reported in any of the trials. Belluzzi 1997 did not report on adverse events, but reported by personal communication that no serious adverse events occurred in either arm. Adverse events that were different between the treatment arms in at least one of the remaining five studies are summarized in Additional Table 2. Romano 2005 reported that there were no adverse events in either group, but no explicit list of items are presented. Belluzzi 1996 reported that 4/39 patients in the intervention arm withdrew due to adverse events compared to 1/39 patients in the placebo arm (due to diarrhea). Discontinuation rates secondary to adverse events in EPIC‐1 and EPIC‐2 (Feagan 2008a) were 9/183 versus 7/180 and 9/187 versus 5/188 in the n‐3 and the placebo groups, respectively. In EPIC‐1, 79.2% of patients who received n‐3 had adhered to the study drug, compared with 75.6% of those who received placebo (P=0.40). The corresponding adherence rates for EPIC‐2 were 75.4% and 81.4%, respectively (P=0.16).
1. Adverse events that were different between the intervention and control arms.
| Study | Belluzzi 1996 | Lorenz‐Meyer 1996 | Romano 2005 | Feagan 2008; EPIC 1 | Feagan 2008; EPIC 2 |
| Diarrhea ‐intervention vs control | 4/39 (10%) vs. 1/39 (3%) | 1/70 (1%) vs. 1/65 (2%) | 0/18 (0%) vs. 0/20 (0%) | 35/187 (19%) vs. 21/184 (11%) | 44/189 (23%) vs 37/188 (20%) |
| Halitosis, or heartburn ‐intervention vs control | 0/39 (0%) vs. 0/39 (0%) | 10/70 (14%) vs. 2/65 (3%) | 0/18 (0%) vs. 0/20 (0%) | not reported but dysgeusia: 2/187 (1%) vs 1/184 (0.5%) | not reported but dysgeusia: 10/189 (5%) vs. 2/188 (1%) |
| Nausea ‐intervention vs control | 0/39 (0%) vs. 0/39 (0%) | 0/70 (0%) vs. 0/65 (0%) | 0/18 (0%) vs. 0/20 (0%) | 17/187 (9%) vs. 4/184 (2%) | 30/189 (16%) vs. 19/188 (10%) |
| All upper GI symptoms ‐intervention vs. controls (halitosis, nausea, vomiting, dyspepsia, dysgeusia and bloating) | 0/39 (0%) vs. 0/39 (0%) | 10/70 (14%) vs. 2/65 (3%) | 0/18 (0%) vs. 0/20 (0%) | 27/187 (14%) vs..12/184 (6.5%) | 67/189 (35.5%) vs. 45/188 (24%) |
Lorenz‐Meyer 1996 was excluded from the meta‐analysis of adverse events because the pathophysiology of the adverse events in that study was very different than the others (upper gastrointestinal symptoms with regular gelatin capsules compared to more lower gastrointestinal symptoms with the timed release capsules used in all the other studies). In the pooled analyses, there was significantly more diarrhea and upper gastrointestinal symptoms with n‐3 treatment compared to placebo. Nineteen per cent of n‐3 patients had diarrhea compared to 14% of placebo patients (Analysis 1.10, 4 studies, 862 patients; RR 1.36, 95% CI 1.01 to 1.84). Twenty‐one per cent of n‐3 patients had upper gastrointestinal symptoms compared to 12% of the placebo group (Analysis 1.11, 5 studies, 999 patients; RR 1.65, 95% CI 1.25 to 2.18). No heterogeneity was detected for these comparisons (I2 = 0% for both comparisons).
1.10. Analysis.
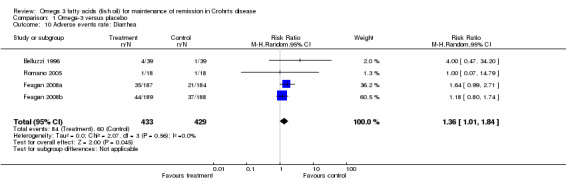
Comparison 1 Omega‐3 versus placebo, Outcome 10 Adverse events rate: Diarrhea.
1.11. Analysis.
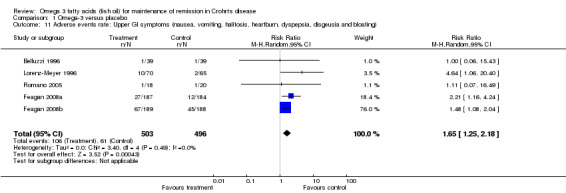
Comparison 1 Omega‐3 versus placebo, Outcome 11 Adverse events rate: Upper GI symptoms (nausea, vomiting, halitosis, heartburn, dyspepsia, disgeusia and bloating).
Other outcomes Other planned outcomes (i.e. steroid use, admission rate, and number of exacerbations) were not reported in any of the studies.
Discussion
Despite the fact that the EPIC studies did not show a clinical benefit to n‐3, the pooled effect of the six included studies was marginally significant (RR 0.77, 95% CI 0.61 to 0.98). However, this presumed benefit is probably misleading for several reasons:
1) There was a large degree of heterogeneity in the pooled analysis that could not be explained on the basis of different methodology of the studies; 2) The statistically significant benefit did not hold when including the estimated, rather than the actual,one year relapse rate (calculated using survival estimates to account for censored data), nor did it hold when the small pediatric study (Romano 2005) was excluded; and 3) A funnel plot suggested publication bias, wherein small negative trials were under‐represented.
Taken together, it is likely that the rigorously performed EPIC studies produced more precise estimates of the true treatment effect than the pooled analysis. It is important to emphasize that the sample size of each EPIC study was approximately double the sample size of all other included studies combined.
This conclusion is disappointing in view of indirect evidence that supports the effectiveness of n‐3 in modulating inflammation of IBD. Orally administered n‐3 is readily incorporated in IBD affected bowel mucosa (Hillier 1991), thereby reducing the production of local proinflammatory cytokines (Hillier 1991; Meister 2005). Fish oil also alters signaling pathways and has a direct effect on the expression of many genes (Bassaganya‐Riera 2006; Deckelbaum 2006; Roy 2007). Fish oil proved to be protective in animal models with experimental IBD (Nieto 2002; Socha 2005; Vilaseca 1990). In a recent study, n‐3 did not protect pigs from dextran sodium sulfate (DSS) induced IBD, but accelerated clinical remission (Bassaganya‐Riera 2006). Finally, some reports indicated depleted serum n‐3 in IBD patients (Kuroki 1997; Siguel 1996), but this was not replicated by others (Figler 2007; Socha 2005). An initial uncontrolled human study of fish oil supplementation, showed promising results for maintenance of remission in CD (Mate 1991).
It is difficult to explain the limited or absent clinical benefit of n‐3 in Crohn's disease in view of the strong biologic rationale and the extensive supportive evidence from tissue samples and animal models. One explanation may lie in the delivery system of the drug. However, the n‐3 fatty acids were being consumed and absorbed in all studies, as reflected by decreased serum triglycerides and altered fatty acid composition of RBC. The dose might have been inadequate or the formulation not optimal. In a scientific study aimed to find the optimal chemical formulation in IBD, n‐3 as enteric coated fatty acids with 60 minutes timed release had the highest serum and RBC incorporation rate and the lowest rate of adverse events, in comparison to different timed release and triglyceride compounds (Belluzzi 1994). The chemical formulation, thus, also seems to be important. It had been shown that the intestinal absorption of n‐3 is higher with free fatty acids (e.g. EpanovaTM) compared with triacylglycerol (e.g. Max‐EPA) or ester formulations (el Boustani 1987; Lawson 1988), probably due to enhanced absorption. Accordingly, the smaller effect size found in Romano 2005 could be attributed to the ethyl ester formulation that was used compared to the free fatty acids used in the other studies. In contrast, the EPIC studies failed to show benefit with EpanovaTM tablets that contain timed release free fatty acids (albeit in a soft gelatin capsules; the authors claim that its bioavailability is similar to the hard capsules used by Belluzzi 1996). Notwithstanding the abovementioned data, it does appear that the biological effect of n‐3 is more complex than once believed, and likely includes both anti‐inflammatory and pro‐inflammatory actions (Hokari 2013). This is also supported by a few animal studies that actually demonstrated a worsening of experimental colitis in mice receiving n‐3 supplementation (Matsunaga 2008; Woodworth 2010). It has also been suggested that the administration of n‐3 to established patients, as in the human interventional studies reviewed here, is fundamentally different from the animal studies in which n‐3 was generally administered before the onset of disease (Marion‐Letellier 2013).
Fish oil is considered very safe, but in the pooled analyses troublesome adverse events such as diarrhea and upper gastrointestinal symptoms were more frequent than in controls. Findings that n‐3 may alter LDL level, bleeding time and glucose level have not been consistently reproduced (Oh 2005), and did not come up in any of the included studies. The non‐serious but bothersome adverse events include unpleasant taste, halitosis, heartburn, nausea and diarrhea (Kim 1996; Lorenz 1989). It has been shown, that unlike raw fish, various over‐the‐counter n‐3 preparations have at the most negligible amounts of mercury and organochlorines (Melanson 2005). Another concern relates to infants whose growth rate may be altered with high intake ratios of EPA to DHA (Akabas 2006).
A limitation of this review is the clinical heterogeneity among the included studies. The studies used different preparations of omega‐3 fatty acids, with different compositions and different delivery systems. The placebo also varied among the trials, and it is possible that these placebos were not inert, with potentially either positive or negative effects. One of the studies was in the post‐operative setting and another examined only pediatric patients. On the other hand, the studies were very similar in other aspects: all included only CD patients in remission, and used a similar end point of relapse rate over an identical follow‐up period of one year. The use of any drug during a quiescent period is a tradeoff between the efficacy for maintaining remission and the associated adverse events. The current effective maintenance therapies for Crohn's disease, immunomodulators and infliximab, possess potentially concerning adverse reactions. Besides serious short term adverse events (e.g. infections, infusion reactions, pancreatitis, hepatitis and severe cytopenia), it has been shown that 6‐mercaptopurine and azathioprine (Kandiel 2005), and recently also infliximab (Thayu 2005), may increase the risk of developing lymphoma. The search for an effective yet safe drug to maintain remission in Crohn's disease continues.
Authors' conclusions
Implications for practice.
Evidence from two large high quality studies suggests that omega 3 fatty acids are probably ineffective for maintenance of remission in CD. Omega 3 fatty acids appear to be safe although they may cause diarrhea and upper gastrointestinal tract symptoms.
Implications for research.
Further adequate sample‐sized clinical trials are needed utilizing effective delivery methods of omega 3 fatty acids. Future studies should use different formulations of n‐3 in the intervention arm, inert placebo oil, and include long‐term outcome data. However, before more large scale RCTs evaluating omega 3 products are conducted further basic research regarding the putative mechanism of action and the role of local drug delivery is needed.
What's new
| Date | Event | Description |
|---|---|---|
| 18 June 2014 | Amended | Contains new information provided by author of included study |
History
Protocol first published: Issue 1, 2007 Review first published: Issue 2, 2007
| Date | Event | Description |
|---|---|---|
| 30 May 2014 | Amended | Correction regarding correspondence with author of included study |
| 22 November 2013 | New search has been performed | New search, no new studies identified |
| 22 November 2013 | New citation required but conclusions have not changed | Updated review with two new authors |
Acknowledgements
Funding for the IBD/FBD Review Group (September 1, 2010 ‐ August 31, 2015) has been provided by the Canadian Institutes of Health Research (CIHR) Knowledge Translation Branch (CON ‐ 105529) and the CIHR Institutes of Nutrition, Metabolism and Diabetes (INMD); and Infection and Immunity (III) and the Ontario Ministry of Health and Long Term Care (HLTC3968FL‐2010‐2235).
Miss Ila Stewart has provided support for the IBD/FBD Review Group through the Olive Stewart Fund.
The authors would like to thank Professor Andrea Belluzzi for providing additional information on his study.
Appendices
Appendix 1. Electronic Search Strategies
Appendix I – Electronic Search Strategies
| Database | Search | Query | Results |
|
PUBMED run Nov. 22, 2013 |
1 | (singl* OR doubl* OR tripl* OR trebl* OR blind* OR mask* OR placebo* OR single‐blind* OR double‐blind* OR triple‐blind* OR random* OR (controlled clinical)) | 2,478,073 |
| 2 | (crohn* OR enteritis OR ileitis) | 53,319 | |
| 3 | (#1 AND #2) | 6,478 | |
| 4 | ((fish oil) OR efamed OR (fish oils) OR promega OR (super epa) OR superepa OR (tuna oil) OR (tuna oils)) | 22,213 | |
| 5 | (omega‐3 OR (omega 3) OR (n‐3 fatty acid) OR (n3 fatty acid) OR (n‐3 PUFA) OR (n3 PUFA) OR (n‐3 polyunsaturated) OR (n3 polyunsaturated) OR (n3 poly unsaturated) OR (n‐3 poly unsaturated) OR (seal oil) OR (krill oil)) | 21,926 | |
| 6 | (icosapentaenoic OR docosahexaenoic OR linolenic OR eicosapentaenoic OR alpha‐linolenic OR EPA OR DHA) | 30,125 | |
| 7 | (#4 OR #5 OR #6) | 45,886 | |
| 8 | (#3 AND #7) | 57 | |
| EMBASE + EMBASE Classic (1947 – 2013) run Nov. 22, 2013 | 1 | random$.tw. | 882,607 |
| 2 | factorial$.tw. | 22,991 | |
| 3 | (crossover$ or cross over$ or cross‐over$).tw. | 72,085 | |
| 4 | placebo$.tw. | 207,389 | |
| 5 | single blind.mp. | 24,794 | |
| 6 | double blind.mp. | 186,064 | |
| 7 | triple blind.mp. | 338 | |
| 8 | (singl$ adj blind$).tw. | 14,471 | |
| 9 | (double$ adj blind$).tw. | 151,927 | |
| 10 | (tripl$ adj blind$).tw. | 383 | |
| 11 | assign$.tw. | 242,174 | |
| 12 | allocat$.tw. | 83,271 | |
| 13 | crossover procedure/ | 39,339 | |
| 14 | double blind procedure/ | 123,454 | |
| 15 | single blind procedure/ | 18,566 | |
| 16 | triple blind procedure/ | 60 | |
| 17 | randomized controlled trial/ | 362,954 | |
| 18 | or/1‐17 | 1,298,268 | |
| 19 | (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.) | 5,891,223 | |
| 20 | 18 not 19 | 1,115,668 | |
| 21 | exp Crohn disease/ or crohn*.mp. or exp colon Crohn disease/ | 66,863 | |
| 22 | (enteritis or ileitis).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 63,073 | |
| 23 | 21 or 22 | 108,448 | |
| 24 | 20 and 23 | 4,950 | |
| 25 | fish oil.mp. or exp fish oil/ | 14,247 | |
| 26 | (efamed or fish oils or promega or "super epa" or superepa or "tuna oil" or "tuna oils").mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 3,778 | |
| 27 | omega‐3.mp. or exp omega 3 fatty acid/ | 21,010 | |
| 28 | ("omega 3" or "n‐3 fatty acid" or "n3 fatty acid" or "n‐3 PUFA" or "n3 PUFA" or "n‐3 polyunsaturated" or "n3 polyunsaturated" or "n3 poly unsaturated" or "n‐3 poly unsaturated" or "seal oil" or "krill oil").mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 23,487 | |
| 29 | icosapentaenoic acid.mp. or exp icosapentaenoic acid/ | 10,769 | |
| 30 | docosahexaenoic acid.mp. or exp docosahexaenoic acid/ | 14,509 | |
| 31 | linolenic acid.mp. or exp linolenic acid/ | 11,370 | |
| 32 | ("eicosapentaenoic acid" or "eicosapentaenoic acid*" or "icosapentaenoic acid*" or "docohexaenoic acid*" or "alpha‐linolenic acid" or "linolenic acid*" or "alpha‐linolenic acid*" or EPA or DHA).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] | 36,564 | |
| 33 | 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 | 60,990 | |
| 34 | 24 and 33 | 94 | |
|
All OVID Medline (1946 – present) run Nov. 22, 2013 |
1 | random$.tw. | 73,9513 |
| 2 | factorial$.tw. | 18,494 | |
| 3 | (crossover$ or cross over$ or cross‐over$).tw. | 64,433 | |
| 4 | placebo$.tw. | 169,408 | |
| 5 | single blind.mp. | 24,116 | |
| 6 | double blind.mp. | 160,664 | |
| 7 | triple blind.mp. | 260 | |
| 8 | (singl$ adj blind$).tw. | 11,808 | |
| 9 | (double$ adj blind$).tw. | 121,299 | |
| 10 | (tripl$ adj blind$).tw. | 320 | |
| 11 | assign$.tw. | 213,631 | |
| 12 | allocat$.tw. | 71,382 | |
| 13 | crossover procedure/ | 0 | |
| 14 | double blind procedure/ | 0 | |
| 15 | single blind procedure/ | 0 | |
| 16 | triple blind procedure/ | 0 | |
| 17 | randomized controlled trial/ | 390,954 | |
| 18 | or/1‐17 | 1,106,670 | |
| 19 | (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.) | 4,056,651 | |
| 20 | 18 not 19 | 981,666 | |
| 21 | exp Crohn disease/ or crohn*.mp. or exp colon Crohn disease/ | 41,252 | |
| 22 | (enteritis or ileitis).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept, rare disease supplementary concept, unique identifier] | 16,138 | |
| 23 | 21 or 22 | 54,204 | |
| 24 | 20 and 23 | 2,323 | |
| 25 | fish oil.mp. or exp fish oil/ | 20,955 | |
| 26 | (efamed or fish oils or promega or "super epa" or superepa or "tuna oil" or "tuna oils").mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept, rare disease supplementary concept, unique identifier] | 6,963 | |
| 27 | omega‐3.mp. or exp omega 3 fatty acid/ | 19,961 | |
| 28 | ("omega 3" or "n‐3 fatty acid" or "n3 fatty acid" or "n‐3 PUFA" or "n3 PUFA" or "n‐3 polyunsaturated" or "n3 polyunsaturated" or "n3 poly unsaturated" or "n‐3 poly unsaturated" or "seal oil" or "krill oil").mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept, rare disease supplementary concept, unique identifier] | 15,620 | |
| 29 | icosapentaenoic acid.mp. or exp icosapentaenoic acid/ | 30 | |
| 30 | docosahexaenoic acid.mp. or exp docosahexaenoic acid/ | 7,754 | |
| 31 | linolenic acid.mp. or exp linolenic acid/ | 6,995 | |
| 32 | ("eicosapentaenoic acid" or "eicosapentaenoic acid*" or "icosapentaenoic acid*" or "docohexaenoic acid*" or "alpha‐linolenic acid" or "linolenic acid*" or "alpha‐linolenic acid*" or EPA or DHA).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept, rare disease supplementary concept, unique identifier] | 25,252 | |
| 33 | 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 | 40,767 | |
| 34 | 24 and 33 | 38 | |
|
OVID HealthSTAR (1966 – Oct. 2013) run Nov. 22, 2013 |
1 | random$.tw. | 506,378 |
| 2 | factorial$.tw. | 9,199 | |
| 3 | (crossover$ or cross over$ or cross‐over$).tw. | 46,972 | |
| 4 | placebo$.tw. | 137,186 | |
| 5 | single blind.mp. | 23,308 | |
| 6 | double blind.mp. | 160,326 | |
| 7 | triple blind.mp. | 199 | |
| 8 | (singl$ adj blind$).tw. | 9,666 | |
| 9 | (double$ adj blind$).tw. | 110,768 | |
| 10 | (tripl$ adj blind$).tw. | 246 | |
| 11 | assign$.tw. | 108,502 | |
| 12 | allocat$.tw. | 46,302 | |
| 13 | crossover procedure/ | 0 | |
| 14 | double blind procedure/ | 0 | |
| 15 | single blind procedure/ | 0 | |
| 16 | triple blind procedure/ | 0 | |
| 17 | randomized controlled trial/ | 174,967 | |
| 18 | or/1‐17 | 742,216 | |
| 19 | (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.) | 84,390 | |
| 20 | 18 not 19 | 741,219 | |
| 21 | exp Crohn disease/ or crohn*.mp. or exp colon Crohn disease/ | 19,397 | |
| 22 | (enteritis or ileitis).mp. [mp=title, original title, abstract, name of substance word, subject heading word] | 4,406 | |
| 23 | 21 or 22 | 23,010 | |
| 24 | 20 and 23 | 1,651 | |
| 25 | fish oil.mp. or exp fish oil/ | 8,731 | |
| 26 | (efamed or fish oils or promega or "super epa" or superepa or "tuna oil" or "tuna oils").mp. [mp=title, original title, abstract, name of substance word, subject heading word] | 2,663 | |
| 27 | omega‐3.mp. or exp omega 3 fatty acid/ | 8,565 | |
| 28 | ("omega 3" or "n‐3 fatty acid" or "n3 fatty acid" or "n‐3 PUFA" or "n3 PUFA" or "n‐3 polyunsaturated" or "n3 polyunsaturated" or "n3 poly unsaturated" or "n‐3 poly unsaturated" or "seal oil" or "krill oil").mp. [mp=title, original title, abstract, name of substance word, subject heading word] | 7,187 | |
| 29 | icosapentaenoic acid.mp. or exp icosapentaenoic acid/ | 6 | |
| 30 | docosahexaenoic acid.mp. or exp docosahexaenoic acid/ | 2,341 | |
| 31 | linolenic acid.mp. or exp linolenic acid/ | 1,890 | |
| 32 | ("eicosapentaenoic acid" or "eicosapentaenoic acid*" or "icosapentaenoic acid*" or "docohexaenoic acid*" or "alpha‐linolenic acid" or "linolenic acid*" or "alpha‐linolenic acid*" or EPA or DHA).mp. [mp=title, original title, abstract, name of substance word, subject heading word] | 9,522 | |
| 33 | 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 | 16,205 | |
| 34 | 24 and 33 | 28 | |
| Cochrane Library (CENTRAL) run Nov. 22, 2013 | 1 | crohn* or enteritis or ileitis | 1,797 |
| 2 | (fish oil) or efamed or (fish oils) or promega or (super epa) or superepa or (tuna oil) or (tuna oils) | 1,535 | |
| 3 | omega‐3 or (omega 3) or (n‐3 fatty acid) or (n3 fatty acid) or (n‐3 PUFA) or (n3 PUFA) or (n‐3 polyunsaturated) or (n3 polyunsaturated) or (n3 poly unsaturated) or (n‐3 poly unsaturated) or (seal oil) or (krill oil) |
2,930 | |
| 4 | icosapentaenoic or docosahexaenoic or linolenic or eicosapentaenoic or alpha‐linolenic or EPA or DHA |
2,168 | |
| 5 | #2 or #3 or #4 | 4,549 | |
| 6 | #1 and #5 | 49* | |
|
ACP Journal Club run Nov. 22, 2013 |
“crohn*” OR “ileitis” OR “enteritis” | 7 hits, none of which were related to fish oils | |
| DDW abstracts (1981‐2010; later abstracts are found in EMBASE) | (crohn* OR ileitis OR enteritis) AND (omega OR fish OR tuna OR seal OR krill OR polyunsaturated OR icosapentaenoic OR docosahexaenoic OR linolenic OR eicosapentaenoic OR PUFA OR DHA OR EPA OR fatty OR promega OR efamed) | 24 |
* Of those 49 hits, only 27 were references to clinical trials and thus only those 27 hits were exported to Endnote.
Data and analyses
Comparison 1. Omega‐3 versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Relapse rate at one year (all studies) | 6 | 1039 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.61, 0.98] |
| 2 Relapse rate at one year (enteric coated studies) | 5 | 904 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.54, 0.93] |
| 3 Relapse rate at one year (sensitivity analysis of Belluzi 1996) | 5 | 904 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.64, 0.93] |
| 4 Relapse rate at one year (enteric coated ‐ risk difference) | 5 | 904 | Risk Difference (M‐H, Random, 95% CI) | ‐0.17 [‐0.30, ‐0.04] |
| 5 Relapse rate at one year (sensitivity analysis ‐ excluding abstract study) | 4 | 854 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.54, 0.96] |
| 6 Relapse rate at one year (sensitivity analysis ‐ excluding pediatric study) | 4 | 866 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.50, 1.01] |
| 7 Relapse rate at one year (all studies, rate in EPIC studies by survival estimates) | 6 | 1039 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.66, 1.00] |
| 8 Relapse rate at one year (only EPIC studies) | 2 | 738 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.74, 1.05] |
| 9 Relapse at one year, survival analysis (Hazard Ratios of the EPIC studies) | 2 | hazard ratio (Random, 95% CI) | 0.87 [0.69, 1.09] | |
| 10 Adverse events rate: Diarrhea | 4 | 862 | Risk Ratio (M‐H, Random, 95% CI) | 1.36 [1.01, 1.84] |
| 11 Adverse events rate: Upper GI symptoms (nausea, vomiting, halitosis, heartburn, dyspepsia, disgeusia and bloating) | 5 | 999 | Risk Ratio (M‐H, Random, 95% CI) | 1.65 [1.25, 2.18] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Belluzzi 1996.
| Methods | Double blind, placebo‐controlled trial | |
| Participants | N = 39 in each arm All patients had CDAI < 150 at baseline with an increase in inflammatory markers |
|
| Interventions | Enteric coated, n‐3 as timed release fatty acids (1.8 g/day of EPA, 0.9 g/day of DHA) versus identical placebo of 500 mg Miglyol 812 | |
| Outcomes | Relapse rates over 1 year Adverse events Time to first relapse |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Balanced block randomization scheme The method of randomization was not described |
| Allocation concealment (selection bias) | Unclear risk | The method of allocation concealment was not described |
| Blinding (performance bias and detection bias) All outcomes | Low risk | The study medications were packed identically and labelled with each patient’s code number There was no difference in odor between the fish‐oil and placebo preparations, provided the capsules were not broken |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Participants who withdrew due to diarrrhea were not included in the relapse rate calculation and it is unclear whether they were included in lab results at the end of the study |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Belluzzi 1997.
| Methods | Double blind, placebo‐ controlled trial | |
| Participants | N = 26 in the intervention arm and 24 in the control arm Patients in remission one month following ileal resection |
|
| Interventions | Enteric coated, n‐3 as timed release fatty acids (1.8 g/day of EPA, 0.9 g/day of DHA) versus identical placebo of 500 mg Miglyol 812 | |
| Outcomes | Clinical and endoscopic relapse rates over 1 year | |
| Notes | Published in abstract form | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The random list was prepared by the pharmacist of the company producing the product using a balanced block randomization scheme The method of randomization was not described |
| Allocation concealment (selection bias) | Low risk | Centrallized pharmacy randomization |
| Blinding (performance bias and detection bias) All outcomes | Low risk | The study medications were packed identically and labelled with each patient’s code number |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Only 16/26 in the n‐3 arm and 15/24 in the control arm were assessed for the primary outcome (endoscopic recurrence) This might be due to exclusion of patients with clinical relapse but no explanation was given |
| Selective reporting (reporting bias) | Low risk | Expected outcomes were reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Feagan 2008a.
| Methods | Double blind, placebo‐controlled trial (EPIC‐1) | |
| Participants | n = 183 in the intervention arm and 180 in the control arm CDAI < 150 for at least three months and at least one exacerbation within the previous year |
|
| Interventions | Enteric coated, n‐3 as timed release fatty acids (2.2 g/day of EPA, 0.8 g/day of DHA) versus identical placebo of 4 g/day medium‐chain triglyceride oil No new medications were allowed after randomization |
|
| Outcomes | Time to relapse 1 year relapse rate Adverse events Change in CDAI Change in SF‐36 |
|
| Notes | Both EPIC‐1 and EPIC‐2 were reported in one manuscript of Feagan 2008 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Eligible patients were randomly assigned, in a 1:1 ratio using a random number generator |
| Allocation concealment (selection bias) | Low risk | Both studies used a central randomization procedure |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Identical placebo Neither the investigators nor the patients were aware of the treatment assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Drop‐outs balanced across intervention groups with similar reasons for withdrawal |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Feagan 2008b.
| Methods | Double blind, placebo‐ controlled trial (EPIC‐2) | |
| Participants | n = 187 in the intervention arm and 188 in the control arm Steroid induced remission with CDAI < 150 after 8 weeks of treatment |
|
| Interventions | Similar to the EPIC‐1 trial; corticosteroids were tapered off over 8 weeks from randomization | |
| Outcomes | Same as for EPIC‐1 above | |
| Notes | Both EPIC‐1 and EPIC‐2 were reported in one manuscript (Feagan 2008) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Eligible patients were randomly assigned, in a 1:1 ratio using a random number generator |
| Allocation concealment (selection bias) | Low risk | Both studies used a central randomization procedure |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Identical placebo Neither the investigators nor the patients were aware of the treatment assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Drop‐outs balanced across intervention groups with similar reasons for withdrawal |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Lorenz‐Meyer 1996.
| Methods | Double blind, placebo‐controlled trial | |
| Participants | N = 70 in the intervention arm and 65 in the control arm CDAI < 150 at baseline Patients on a diet low in arachidonic acid and rich in fiber |
|
| Interventions | Non‐enteric coated, n‐3 as ethylesther (3.3 g/day of EPA and 1.8 g/day of DHA) versus identical placebo of corn oil | |
| Outcomes | Relapse rates over 1 year Adverse events |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Identical placebo of corn oil |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The study had a high drop‐out rate, but the drop‐out appeared to be balanced: 8/70 (11%) in the intervention arm and 7/65 (11%) in the control arm |
| Selective reporting (reporting bias) | Low risk | All expected outcomes were reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Romano 2005.
| Methods | Double blind, placebo‐controlled trial | |
| Participants | N = 18 in the intervention arm and 20 in the control arm PCDAI < 20 at baseline |
|
| Interventions | Enteric coated n‐3 as triglycerides (1.2 g/day of EPA and 0.6 g/day of DHA) versus placebo of olive oil Both groups received 5‐ASA (50 mg/kg/day) |
|
| Outcomes | Relapse rates over 1 year Time to first relapse |
|
| Notes | Pediatric study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Drop‐out rate not specifically reported, but there appear to have been no drop‐outs |
| Selective reporting (reporting bias) | High risk | Laboratory testing was performed as specified in the methods section, but no results are reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
Abbreviations: CDAI = Crohn's disease activity index; PCDAI = pediatric Crohn's disease activity index; 5‐ASA = 5‐amino salicylic acid; EPA = eicosapentanoic acid; DHA = docosahexanoic acid
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bamba 2003 | Study enrolled patients with active Crohn's disease |
| Bjorkkjaer 2004 | N‐3 treatment was for less than 6 months |
| Eivindson 2005 | Study enrolled patients with active Crohn's disease |
| Geerling 2000 | N‐3 treatment was for less than 6 months |
| Lorenz 1989 | Study enrolled both patients with active and non‐active Crohn's disease Attempts to obtain data from the authors on the inactive patients only were unsuccessful |
| Mate 1991 | Non‐randomized study |
| Nielsen 2005 | Study enrolled patients with active Crohn's disease |
| Sakurai 2002 | Study enrolled patients with active Crohn's disease |
| Seidman 2003 | Study enrolled patients with active Crohn's disease |
| Socha 2002 | Study enrolled patients with active Crohn's disease |
| Trebble 2004 | Study enrolled patients with active Crohn's disease |
| Trebble 2005 | Study enrolled patients with active Crohn's disease |
| Tsujikawa 2000 | Non‐randomized study |
Contributions of authors
RL Responsible for search for new literature published since the previous review, reviewed and edited the updated manuscript.
OL Participated in review and editing of the updated manuscript.
AMG Formulated the research question, provided IBD expert opinion, selected and reviewed the eligible studies, involved in the analyses, and reviewed the manuscript.
DT Responsible for the literature search, selecting and reviewing the eligible studies, performing the analyses; wrote the previous versions of the manuscript and reviewed the current manuscript.
Sources of support
Internal sources
Mount Sinai Hospital, University of Toronto, Toronto, Canada.
Department of Health Policy, Management and Evaluation, U of T, Canada.
Hospital for Sick Children, Toronto, Canada.
External sources
No sources of support supplied
Declarations of interest
None known.
Edited (no change to conclusions)
References
References to studies included in this review
Belluzzi 1996 {published data only}
- Belluzzi A, Brignola C, Campieri M, Pera A, Boschi S, Miglioli M. Effect of an enteric‐coated fish‐oil preparation on relapses in Crohn's disease. New England Journal of Medicine 1996;334(24):1557‐60. [DOI] [PubMed] [Google Scholar]
Belluzzi 1997 {published data only}
- Belluzzi A, Campieri M, Belloli C, Boschi S, Cottone M, Rizzello F, et al. A new enteric coated preparation of omega‐3 fatty acids for preventing post‐surgical recurrence in Crohn's disease. Gastroenterology 1997;112(4):A494. [Google Scholar]
Feagan 2008a {published data only}
- Feagan BG, Sandborn WJ, Mittmann U, Bar‐Meir S, D'Haens G, Bradette M, et al. Omega‐3 free fatty acids for the maintenance of remission in Crohn disease: the EPIC Randomized Controlled Trials. JAMA 2008;299(14):1690‐7. [DOI] [PubMed] [Google Scholar]
Feagan 2008b {published data only}
- Feagan BG, Sandborn WJ, Mittmann U, Bar‐Meir S, D'Haens G, Bradette M, et al. Omega‐3 free fatty acids for the maintenance of remission in Crohn disease: the EPIC Randomized Controlled Trials. JAMA 2008;299(14):1690‐7. [DOI] [PubMed] [Google Scholar]
Lorenz‐Meyer 1996 {published data only}
- Lorenz‐Meyer H, Bauer P, Nicolay C, Schulz B, Purrmann J, Fleig WE, et al. Omega‐3 fatty acids and low carbohydrate diet for maintenance of remission in Crohn's disease. A randomized controlled multicenter trial. Study Group Members (German Crohn's Disease Study Group). Scandinavian Journal of Gastroenterology 1996;31(8):778‐85. [DOI] [PubMed] [Google Scholar]
Romano 2005 {published data only}
- Romano C, Cucchiara S, Barabino A, Annese V, Sferlazzas C. Usefulness of omega‐3 fatty acid supplementation in addition to mesalazine in maintaining remission in pediatric Crohn's disease: a double‐blind, randomized, placebo‐controlled study. World Journal of Gastroenterology 2005;11(45):7118‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Bamba 2003 {published data only}
- Bamba T, Shimoyama T, Sasaki M, Tsujikawa T, Fukuda Y, Koganei K, et al. Dietary fat attenuates the benefits of an elemental diet in active Crohn's disease: a randomized, controlled trial. European Journal of Gastroenterology and Hepatology 2003;15(2):151‐7. [DOI] [PubMed] [Google Scholar]
Bjorkkjaer 2004 {published data only}
- Bjorkkjaer T, Brunborg LA, Arslan G, Lind RA, Brun JG, Valen M, et al. Reduced joint pain after short‐term duodenal administration of seal oil in patients with inflammatory bowel disease: comparison with soy oil. Scandinavian Journal of Gastroenterology 2004;39(11):1088‐94. [DOI] [PubMed] [Google Scholar]
Eivindson 2005 {published data only}
- Eivindson M, Gronbaek H, Nielsen JN, Frystyk J, Flyvbjerg A, Jorgensen L, et al. Insulin‐like growth factors (IGFs) and IGF binding proteins in active Crohn's disease treated with omega‐3 or omega‐6 fatty acids and corticosteroids. Scandinavian Journal of Gastroenterology 2005;40(10):1214‐21. [DOI] [PubMed] [Google Scholar]
Geerling 2000 {published data only}
- Geerling BJ, Badart‐Smook A, Deursen C, Houwelingen AC, Russel MG, Stockbrugger RW, et al. Nutritional supplementation with N‐3 fatty acids and antioxidants in patients with Crohn's disease in remission: effects on antioxidant status and fatty acid profile. Inflammatory Bowel Diseases 2000;6(2):77‐84. [DOI] [PubMed] [Google Scholar]
Lorenz 1989 {published data only}
- Lorenz R, Weber PC, Szimnau P, Heldwein W, Strasser T, Loeschke K. Supplementation with n‐3 fatty acids from fish oil in chronic inflammatory bowel disease‐‐a randomized, placebo‐controlled, double‐blind cross‐over trial. Journal of Internal Medicine. Supplement 1989;731:225‐32. [DOI] [PubMed] [Google Scholar]
Mate 1991 {published data only}
- Mate J, Castanos R, Garcia‐Samaniego J, Pajares JM. Does dietary fish oil maintain the remission of Crohn's disease (CD): A case control study. Gastroenterology 1991;100(5):A228. [Google Scholar]
Nielsen 2005 {published data only}
- Nielsen AA, Jorgensen LG, Nielsen JN, Eivindson M, Gronbaek H, Vind I, et al. Omega‐3 fatty acids inhibit an increase of proinflammatory cytokines in patients with active Crohn's disease compared with omega‐6 fatty acids. Alimentary Pharmacology and Therapeutics 2005;22(11‐12):1121‐8. [DOI] [PubMed] [Google Scholar]
Sakurai 2002 {published data only}
- Sakurai T, Matsui T, Yao T, Takagi Y, Hirai F, Aoyagi K, et al. Short‐term efficacy of enteral nutrition in the treatment of active Crohn's disease: a randomized, controlled trial comparing nutrient formulas. JPEN. Journal of Parenteral and Enteral Nutrition 2002;26(2):98‐103. [DOI] [PubMed] [Google Scholar]
Seidman 2003 {published data only}
- Seidman E, Bouthillier L, Thibault L, Lepage G, Chartre M, Deslandres C, et al. Clinical and nutritional parameters in Crohn's disease patients treated with either an n‐3 PUFA‐enriched semi‐elemental or a polymeric diet. Results of a randomized controlled trial. Journal of Pediatric Gastroenterology and Nutrition 2003;37(3):393. [Google Scholar]
Socha 2002 {published data only}
- Socha P, Ryzko J, Koletzko B, Czubkowski P, Korszynska D, Celinska‐Cedro D, et al. The influence of fish oil therapy in children with inflammatory bowel disease on the fatty acid status. Pediatria Wspolczesna 2002;4(3):413‐6. [Google Scholar]
Trebble 2004 {published data only}
- Trebble TM, Arden NK, Wootton SA, Calder PC, Mullee MA, Fine DR, et al. Fish oil and antioxidants alter the composition and function of circulating mononuclear cells in Crohn disease. American Journal of Clinical Nutrition 2004;80(5):1137‐44. [DOI] [PubMed] [Google Scholar]
Trebble 2005 {published data only}
- Trebble TM. Bone turnover and nutritional status in Crohn's disease: relationship to circulating mononuclear cell function and response to fish oil and antioxidants. Proceedings of the Nutrition Society 2005;64(2):183‐91. [DOI] [PubMed] [Google Scholar]
Tsujikawa 2000 {published data only}
- Tsujikawa T, Satoh J, Uda K, Ihara T, Okamoto T, Araki Y, et al. Clinical importance of n‐3 fatty acid‐rich diet and nutritional education for the maintenance of remission in Crohn's disease. Journal of Gastroenterology 2000;35(2):99‐104. [DOI] [PubMed] [Google Scholar]
Additional references
Akabas 2006
- Akabas SR, Deckelbaum RJ. Summary of a workshop on n‐3 fatty acids: current status of recommendations and future directions. American Journal of Clinical Nutrition 2006;83(6 Suppl):1536S‐8S. [DOI] [PubMed] [Google Scholar]
Arterburn 2006
- Arterburn LM, Hall EB, Oken H. Distribution, interconversion, and dose response of n‐3 fatty acids in humans. American Journal of Clinical Nutrition 2006;83(6 Suppl):1467S‐76S. [DOI] [PubMed] [Google Scholar]
Bassaganya‐Riera 2006
- Bassaganya‐Riera J, Hontecillas R. CLA and n‐3 PUFA differentially modulate clinical activity and colonic PPAR‐responsive gene expression in a pig model of experimental IBD. Clinical Nutrition 2006;25(3):454‐65. [DOI] [PubMed] [Google Scholar]
Belluzzi 1994
- Belluzzi A, Brignola C, Campieri M, Camporesi EP, Gionchetti P, Rizzello F, et al. Effects of new fish oil derivative on fatty acid phospholipid‐membrane pattern in a group of Crohn's disease patients. Digestive Diseases and Sciences 1994;39(12):2589‐94. [DOI] [PubMed] [Google Scholar]
Belluzzi 2002
- Belluzzi A. N‐3 fatty acids for the treatment of inflammatory bowel diseases. Proceedings of the Nutrition Society 2002;61(3):391‐5. [DOI] [PubMed] [Google Scholar]
Best 1976
- Best WR, Becktel JM, Singleton JW, Kern F Jr. Development of a Crohn's disease activity index. National Cooperative Crohn's Disease Study. Gastroenterology 1976;70(3):439‐44. [PubMed] [Google Scholar]
Deckelbaum 2006
- Deckelbaum RJ, Worgall TS, Seo T. N‐3 fatty acids and gene expression. American Journal of Clinical Nutrition 2006;83(6 Suppl):1520S‐5S. [DOI] [PubMed] [Google Scholar]
el Boustani 1987
- Boustani S, Colette C, Monnier L, Descomps B, Crastes de Paulet A, Mendy F. Enteral absorption in man of eicosapentaenoic acid in different chemical forms. Lipids 1987;22(10):711‐4. [DOI] [PubMed] [Google Scholar]
Endres 1989
- Endres S, Ghorbani R, Kelley VE, Georgilis K, Lonnemann G, Meer JW, et al. The effect of dietary supplementation with n‐3 polyunsaturated fatty acids on the synthesis of interleukin‐1 and tumor necrosis factor by mononuclear cells. New England Journal of Medicine 1989;320(5):265‐71. [DOI] [PubMed] [Google Scholar]
Endres 1999
- Endres S, Lorenz R, Loeschke K. Lipid treatment of inflammatory bowel disease. Current Opinion in Clinical Nutrition and Metabolic Care 1999;2(2):117‐20. [DOI] [PubMed] [Google Scholar]
Ergas 2002
- Ergas D, Eilat E, Mendlovic S, Sthoeger ZM. N‐3 fatty acids and the immune system in autoimmunity. Israel Medical Association Journal 2002;4(1):34‐8. [PubMed] [Google Scholar]
Figler 2007
- Figler M, Gasztonyi B, Cseh J, Horvath G, Kisbenedek AG, Bokor S, et al. Association of n‐3 and n‐6 long chain polyunsaturated fatty acids in plasma lipid classes with inflammatory bowel diseases. British Journal of Nutrition 2007;97(6):1154‐61. [DOI] [PubMed] [Google Scholar]
Fisher 1986
- Fisher M, Upchurch KS, Levine PH, Johnson MH, Vaudreuil CH, Natale A, et al. Effects of dietary fish oil supplementation on polymorphonuclear leukocyte inflammatory potential. Inflammation 1986;10(4):387‐92. [DOI] [PubMed] [Google Scholar]
Guyatt 2008
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck‐Ytter Y, Alonso‐Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2011
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction ‐ GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [DOI] [PubMed] [Google Scholar]
Harvey 1980
- Harvey RF, Bradshaw JM. A simple index of Crohn's‐disease activity. Lancet 1980;1(8167):514. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org. [Google Scholar]
Hillier 1991
- Hillier K, Jewell R, Dorrell L, Smith CL. Incorporation of fatty acids from fish oil and olive oil into colonic mucosal lipids and effects upon eicosanoid synthesis in inflammatory bowel disease. Gut 1991;32(10):1151‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hokari 2013
- Hokari R, Matsunaga H, Miura S. Effect of dietary fat on intestinal inflammatory diseases. Journal of Gastroenterology and Hepatology 2013;28 Suppl 4:33‐6. [DOI] [PubMed] [Google Scholar]
Hooper 2004
- Hooper L, Thompson RL, Harrison RA, Summerbell CD, Moore H, Worthington HV, et al. Omega 3 fatty acids for prevention and treatment of cardiovascular disease. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD003177.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hyams 1991
- Hyams JS, Ferry GD, Mandel FS, Gryboski JD, Kibort PM, Kirschner BS, et al. Development and validation of a pediatric Crohn's disease activity index. Journal of Pediatric Gastroenterology and Nutrition 1991;14(4):439‐47. [PubMed] [Google Scholar]
Kandiel 2005
- Kandiel A, Fraser AG, Korelitz BI, Brensinger C, Lewis JD. Increased risk of lymphoma among inflammatory bowel disease patients treated with azathioprine and 6‐mercaptopurine. Gut 2005;54(8):1121‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 1996
- Kim YI. Can fish oil maintain Crohn's disease in remission?. Nutrition Reviews 1996;54(8):248‐52. [DOI] [PubMed] [Google Scholar]
Kuroki 1997
- Kuroki F, Iida M, Matsumoto T, Aoyagi K, Kanamoto K, Fujishima M. Serum n3 polyunsaturated fatty acids are depleted in Crohn's disease. Digestive Diseases and Sciences 1997;42(6):1137‐41. [DOI] [PubMed] [Google Scholar]
Lawson 1988
- Lawson LD, Hughes BG. Human absorption of fish oil fatty acids as triacylglycerols, free acids, or ethyl esters. Biochemical and Biophysical Research Communications 1988;152(1):328‐35. [DOI] [PubMed] [Google Scholar]
Lee 1985
- Lee TH, Hoover RL, Williams JD, Sperling RI, Ravalese J 3rd, Spur BW, et al. Effect of dietary enrichment with eicosapentaenoic and docosahexaenoic acids on in vitro neutrophil and monocyte leukotriene generation and neutrophil function. New England Journal of Medicine 1985;312(19):1217‐24. [DOI] [PubMed] [Google Scholar]
MacLean 2005
- MacLean CH, Mojica WA, Newberry SJ, Pencharz J, Garland RH, Tu W, et al. Systematic review of the effects of n‐3 fatty acids in inflammatory bowel disease. American Journal of Clinical Nutrition 2005;82(3):611‐9. [DOI] [PubMed] [Google Scholar]
Marion‐Letellier 2013
- Marion‐Letellier R, Savoye G, Beck PL, Panaccione R, Ghosh S. Polyunsaturated fatty acids in inflammatory bowel diseases: a reappraisal of effects and therapeutic approaches. Inflammatory Bowel Diseases 2013;19(3):650‐61. [DOI] [PubMed] [Google Scholar]
Matsunaga 2008
- Matsunaga H, Hokari R, Kurihara C, Okada Y, Takebayashi K, Okudaira K, et al. Omega‐3 fatty acids exacerbate DSS‐induced colitis through decreased adiponectin in colonic subepithelial myofibroblasts. Inflammatory Bowel Diseases 2008;14(10):1348‐57. [DOI] [PubMed] [Google Scholar]
Meister 2005
- Meister D, Ghosh S. Effect of fish oil enriched enteral diet on inflammatory bowel disease tissues in organ culture: differential effects on ulcerative colitis and Crohn's disease. World Journal of Gastroenterology 2005;11(47):7466‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Melanson 2005
- Melanson SF, Lewandrowski EL, Flood JG, Lewandrowski KB. Measurement of organochlorines in commercial over‐the‐counter fish oil preparations: implications for dietary and therapeutic recommendations for omega‐3 fatty acids and a review of the literature. Archives of Pathology and Laboratory Medicine 2005;129(1):74‐7. [DOI] [PubMed] [Google Scholar]
Nakazawa 2000
- Nakazawa A, Hibi T. Is fish oil (n‐3 fatty acids) effective for the maintenance of remission in Crohn's disease?. Journal of Gastroenterology 2000;35(2):173‐5. [DOI] [PubMed] [Google Scholar]
Nieto 2002
- Nieto N, Torres MI, Rios A, Gil A. Dietary polyunsaturated fatty acids improve histological and biochemical alterations in rats with experimental ulcerative colitis. Journal of Nutrition 2002;132(1):11‐9. [DOI] [PubMed] [Google Scholar]
Oh 2005
- Oh R. Practical applications of fish oil (Omega‐3 fatty acids) in primary care. Journal of the American Board of Family Practice 2005;18(1):28‐36. [DOI] [PubMed] [Google Scholar]
Roy 2007
- Roy N, Barnett M, Knoch B, Dommels Y, McNabb W. Nutrigenomics applied to an animal model of Inflammatory Bowel Diseases: Transcriptomic analysis of the effects of eicosapentaenoic acid‐and arachidonic acid‐enriched diets. Mutation Research 2007;622(1‐2):103‐16. [DOI] [PubMed] [Google Scholar]
Ruxton 2004
- Ruxton CH, Reed SC, Simpson MJ, Millington KJ. The health benefits of omega‐3 polyunsaturated fatty acids: a review of the evidence. Journal of Human Nutrition and Dietetics 2004;17(5):449‐59. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org. [Google Scholar]
Siguel 1996
- Siguel EN, Lerman RH. Prevalence of essential fatty acid deficiency in patients with chronic gastrointestinal disorders. Metabolism 1996;45(1):12‐23. [DOI] [PubMed] [Google Scholar]
Simopoulos 2002
- Simopoulos AP. Omega‐3 fatty acids in inflammation and autoimmune diseases. Journal of the American College of Nutrition 2002;21(6):495‐505. [DOI] [PubMed] [Google Scholar]
Socha 2005
- Socha P, Ryzko J, Koletzko B, Celinska‐Cedro D, Woynarowski M, Czubkowski P, et al. Essential fatty acid depletion in children with inflammatory bowel disease. Scandinavian Journal of Gastroenterology 2005;40(5):573‐7. [DOI] [PubMed] [Google Scholar]
Thayu 2005
- Thayu M, Markowitz JE, Mamula P, Russo PA, Muinos WI, Baldassano RN. Hepatosplenic T‐cell lymphoma in an adolescent patient after immunomodulator and biologic therapy for Crohn disease. Journal of Pediatric Gastroenterology and Nutrition 2005;40(2):220‐2. [DOI] [PubMed] [Google Scholar]
Turner 2012
- Turner D, Griffiths AM, Walters TD, Seah T, Markowitz J, Pfefferkorn M, et al. Mathematical weighting of the pediatric Crohn's disease activity index (PCDAI) and comparison with its other short versions. Inflammatory Bowel Diseases 2012;18(1):55‐62. [DOI] [PubMed] [Google Scholar]
Vilaseca 1990
- Vilaseca J, Salas A, Guarner F, Rodriguez R, Martinez M, Malagelada JR. Dietary fish oil reduces progression of chronic inflammatory lesions in a rat model of granulomatous colitis. Gut 1990;31(5):539‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Woodworth 2010
- Woodworth HL, McCaskey SJ, Duriancik DM, Clinthorne JF, Langohr IM, Gardner EM, et al. Dietary fish oil alters T lymphocyte cell populations and exacerbates disease in a mouse model of inflammatory colitis. Cancer Research 2010;70(20):7690‐9. [DOI] [PubMed] [Google Scholar]
Zachos 2007
- Zachos M, Tondeur M, Griffiths AM. Enteral nutritional therapy for induction of remission in Crohn's disease. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/14651858.CD000542.pub2] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Turner 2007
- Turner D, Zlotkin SH, Shah PS, Griffiths AM. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn's disease. Cochrane Database of Systematic Reviews 2007, Issue 2. [DOI: 10.1002/14651858.CD006320.pub2] [DOI] [PubMed] [Google Scholar]
Turner 2009
- Turner D, Zlotkin SH, Shah PS, Griffiths AM. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn's disease.. Cochrane Database of Systematic Reviews 2009, Issue 1. [DOI: 10.1002/14651858.CD006320.pub3] [DOI] [PubMed] [Google Scholar]