

Key Points
Question
Is olfactory impairment associated with mortality?
Findings
In this multiadjusted observational systematic review and meta-analysis of 11 studies including 21 601 participants, with moderate-quality evidence overall, olfactory impairment was associated with a 52% higher risk of all-cause mortality.
Meaning
This study suggests that olfactory impairment may be an important risk marker of general health and aging; further research is required to uncover the potential underlying causal or confounding relationships.
Abstract
Importance
Olfactory impairment is highly prevalent and associated with multiple comorbidities, including neurodegenerative, cardiovascular, nutritional, and immune disorders. However, epidemiologic associations between olfactory impairment and mortality are discordant.
Objective
To systematically clarify the epidemiologic associations between olfactory impairment and mortality.
Data Sources
The PubMed, Embase, and Cochrane Library databases were searched from inception to August 13, 2021.
Study Selection
Two blinded reviewers selected observational studies published as full-length, English-language articles in peer-reviewed journals that reported the presence or severity of chronic olfactory impairment, whether objectively measured or self-reported, in association with any mortality estimate, among adults aged 18 years or older.
Data Extraction and Synthesis
Two reviewers independently extracted data, evaluated study bias using the Newcastle-Ottawa Scale, and appraised the quality of the evidence using the Grading of Recommendations Assessment, Development and Evaluation framework, following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines and a PROSPERO-registered protocol. Maximally adjusted estimates were pooled using mixed-effects models, heterogeneity was measured using I2 statistics, sources of heterogeneity were investigated using meta-regression and subgroup meta-analyses, and publication bias was qualitatively and quantitatively assessed.
Main Outcomes and Measures
Hazard ratios for all-cause mortality.
Results
One retrospective cohort study and 10 prospective cohort studies (with a total of 21 601 participants) from 1088 nonduplicated records were included. Ten studies had a low risk of bias, whereas 1 study had a moderate risk; exclusion of the latter did not alter conclusions. Nine studies were included in the meta-analysis. Olfactory loss was associated with a significantly higher pooled hazard of all-cause mortality (hazard ratio, 1.52; 95% CI, 1.28-1.80; I2 = 82%). Meta-regression sufficiently explained heterogeneity, with longer mean follow-up duration weakening the pooled association, accounting for 91.3% of heterogeneity. Self-reported and objective effect sizes were similar. Associations were robust to trim-and-fill adjustment and the Egger test for publication bias. The overall quality of evidence was moderate.
Conclusions and Relevance
The findings of this systematic review and meta-analysis suggest that olfactory impairment is associated with all-cause mortality and may be a marker of general health and biological aging. Further research is required to establish the underlying mechanisms and the scope for interventions.
This systematic review and meta-analysis investigates the epidemiologic associations between olfactory impairment and mortality.
Introduction
Population-based studies of olfactory impairment (OI) indicate an overall prevalence ranging from 19% to 24%,1,2,3 with a prevalence exceeding 50% for individuals aged 65 to 80 years, and reaching 80% among those older than 80 years.4 Olfactory impairment is also associated with multiple comorbidities: neurogenerative,5,6,7 cardiovascular,8 nutritional,9 and immune disorders.10,11 Although OI is common, it frequently goes unnoticed compared with other senses, such as hearing or vision.3,12 Because olfaction is used for a variety of purposes and is a critical component of human physiology,13 its impairment may result in appetite suppression and malnutrition,9 decreased safety14 owing to increased risk of hazardous events (eg, cooking-related incidents, ingestion of spoiled food, and accidental gas poisoning), and overall lower quality of life.15
Furthermore, there has been an increasing body of evidence suggesting that OI is an early sign of neurodegenerative disorders, such as Alzheimer disease,5,6,7 Parkinson disease,16,17,18 and cognitive decline,7,19,20 all of which are associated with greater mortality risk. Despite this evidence, 1 study suggests that only one-third of poor olfaction–associated mortality could be explained by dementia or Parkinson disease,21 which suggests that this impairment may be associated with a broader range of clinical diseases,22 diminishing cell regeneration,23 and age-related accumulation of environmental exposures.24 Olfactory impairment is also associated with other comorbidities, including diabetes,25 kidney disease,26 and epilepsy.27
Emerging evidence suggests that OI is independently associated with excess all-cause mortality among older adults.28,29,30,31 However, there is inconsistency in the literature, with at least 2 studies reporting no association between OI and all-cause mortality among older adults.32,33 Hence, we aim to systematically clarify this association and the role of potential confounders, such as demographic characteristics, socioeconomic status, and medical comorbidities. Given the growing burden of OI globally, we believe that this review is both timely and relevant and should yield public health implications and benefit patient care.
Methods
This study’s protocol is registered on PROSPERO (CRD42021279531) and reported in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guideline and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.34,35 The MOOSE checklist is included in eTable 1 in the Supplement.
Search Strategy
We searched PubMed, Embase, and the Cochrane Library databases from inception to August 13, 2021, using search terms for OI and mortality (eMethods in the Supplement). We also hand-searched the bibliographies of included articles and relevant reviews but identified no additional relevant records.
Study Selection, Data Extraction, and Risk-of-Bias Grading
Two of us (N.Y.-L.P. and A.S.R.C.) independently selected eligible studies (based on title and abstract, followed by full-text articles), extracted relevant data, and evaluated the risk of bias in a blinded manner, with conflicts resolved by a third author (J.X.T.). We included observational studies, published as full-length articles in peer-reviewed journals, that reported the associations between OI and mortality, with any estimate of mortality (eg, all-cause mortality, cardiovascular mortality, or mortality due to injury) among adults aged 18 years or older compared with participants without OI. We accepted objective (eg, the 12-item Brief Smell Identification Test [B-SIT]) and subjective self-reported measures of OI. To avoid duplication, the selected studies focused on the burden of chronic OI before the COVID-19 pandemic, instead of COVID-19–related OI, which occurs in a more acute setting.36 We excluded case reports, reviews, letters, conference abstracts, other non–full-length articles, and non–English-language publications. We extracted key data (eMethods in the Supplement) from each included article and assessed the risk of bias using the Newcastle-Ottawa Scale.37 Per the grading in the past, studies were assessed as having either a high (<5 stars), moderate (5-7 stars), or low (≥8 stars) risk of bias (eTable 2 in the Supplement).
Statistical Analysis
We used mixed-effects models (eMethods in the Supplement) to pool maximally covariate-adjusted hazard ratios (HRs) from each study. Given that HRs, odds ratios, and risk ratios numerically approximate one another when follow-up duration, mean rate of event, and magnitude of risk are low,38 we pooled these maximally adjusted ratios as an overall HR if the aforementioned conditions were met. We assessed and considered between-study heterogeneity as significant if the P value of the Q test was less than .10 or if the I2 statistic was 50% or greater. If a study used an analytical method that is incompatible for synthesis, we converted the effect estimate to an appropriate ratio for synthesis or excluded the study from meta-analysis.
To investigate potential sources of heterogeneity, we performed subgroup, sensitivity, and meta-regression analyses of the following prespecified study-level characteristics: method of measuring OI (eg, objective vs subjective or self-reported, or by the specific smell test), mortality types (eg, all cause and cardiovascular), age, sex, duration of follow-up, prevalence of OI, and adjustment for covariates (eg, presence of cognitive impairment). To investigate small-study effects, we assessed funnel plot asymmetry both visually and using the Egger bias test, imputing potentially missing studies using the trim-and-fill method (eMethods in the Supplement) if publication bias was suspected.
We conducted all analyses using R studio, version 1.3 (R Group for Statistical Computing) (eMethods in the Supplement). Unless otherwise specified, we considered a 2-sided P < .05 as statistically significant.
Certainty of Evidence
We evaluated the quality of pooled evidence at the outcome level (eTable 3 in the Supplement) using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.39
Results
The study selection is summarized in Figure 1. We included 11 articles from 1088 nonduplicated records after initial selection based on title and abstract and subsequent selection based on full texts.21,22,28,29,30,31,32,33,40,41,42
Figure 1. PRISMA Flow Diagram of Study Selection Process.

CVD indicates cardiovascular disease; IHD, ischemic heart disease; and TBI, traumatic brain injury.
Study Characteristics
Of the 11 included studies (Table),21,22,28,29,30,31,32,33,40,41,42 all were observational studies, with 1 retrospective cohort study and 10 prospective cohort studies. Risk of bias when assessed using the Newcastle-Ottawa Scale ranged from low (10 studies)21,22,28,29,30,31,32,33,40,42 to moderate (1 study).41 Sensitivity analyses (excluding the moderate risk-of-bias study) did not substantially alter our results. A total of 7 studies were conducted in North America,21,22,28,30,31,33,41 2 in Europe,29,40 1 in Australia,32 and 1 in China.42 The mean age of participants ranged from 59 to 81 years. We included 9 studies in our meta-analyses.21,22,28,29,30,32,33,40,42
Table. Summary of Included Studies.
| Study | Country | Study design | Sample size, No. | Mean age, y | Male patients, % | Median follow-up duration, y | Impairment definition | Impairment prevalence, % | Covariates | NOS (maximum 9) |
|---|---|---|---|---|---|---|---|---|---|---|
|
US | Retrospective cohort study | 3503 | 59.0 | 47.7 | 5 |
|
17.9 | Age, sex, race and ethnicity, income, educational level, hypertension, cardiovascular diseases, diabetes, stroke, smoking, recent cold symptoms, previous sinus infection, previous head injury, nasal or facial fracture, cognition, major depressive disorder | 9 |
|
US | Prospective cohort study | 1169 | 81.0 | 30.7 | 4.1 |
|
NA | Age, education, race and ethnicity, sex, language, comorbidity index, dementia, depression, head injury, alcohol abuse, BMI, smoking, hearing impairment, vision impairment | 9 |
|
Sweden | Prospective cohort study | 1774 | 63.5 | 45.3 | 9.4 |
|
NA | Age, sex, years of education, history of heart disease, stroke, high blood pressure, diabetes, depression, cognitive performance, dementia, apolipoprotein E4 gene | 9 |
|
US | Prospective cohort study | 2264 | 69.1 | NA | 5 |
|
NA | NA | 6 |
|
Australia | Prospective cohort study | 1636 | 73.5 | 41.9 | 5 |
|
27 | Age, sex, BMI, systolic blood pressure, current smoking status, alcohol consumption, poor self-rated health, visual impairment, presence of hypertension and/or diabetes, history of cancer, angina, stroke, and/or acute myocardial infarction, serum total cholesterol, cognitive impairment | 8 |
|
Italy | Prospective cohort study | 1035 | 74.7 | 44.3 | 9 |
|
57 | Age, sex, educational level, glomerular filtration rate, hemoglobin level, CES-D, Mini-Mental State Examination, ADL, diagnosis of malignant neoplasm, peripheral arterial disease, use of ACE inhibitors and benzodiazepines, frailty | 8 |
|
US | Prospective cohort study | 2289 | 75.6 | 48.1 | 13 |
|
66.1 | Age, sex, race and ethnicity, educational level, BMI, alcohol drinking, physical activity, smoking, self-reported health status, coronary heart disease, CHF, cerebrovascular disease, peripheral vascular disease, cancer, diabetes, hypertension, depressive symptoms, chronic kidney disease | 9 |
|
US | Prospective cohort study | 2918 | 68.0 | 48.4 | 5 |
|
26.5 | Age, anosmia, hyposmia, sex, race and ethnicity, educational level, comorbidity index, myocardial infarction, heart failure, stroke, diabetes, hypertension, emphysema or COPD, liver damage, cancer | 9 |
|
US | Prospective cohort study | 2418 | 68.9 | 42.2 | 12.8 |
|
23.8 | Age, sex, educational level, hypertension, diabetes, cardiovascular disease, cancer, cognitive impairment, frailty, smoking, exercise, BMI, alcohol, intima-media thickness, C-reactive protein, interleukin 6 | 9 |
|
US | Prospective cohort study | 1162 | 79.7 | 25.5 | 4.2 |
|
NA | Age, educational level, sex, Boston Naming Test (visual confrontation naming), Katz Scale for ADL, vascular risk factors (smoking, hypertension and diabetes), vascular conditions (myocardial infarction, CHF, stroke, and claudication), BMI, cognitive activity, social activity, physical activity, depressive symptoms, apolipoprotein E gene | 8 |
|
China | Prospective cohort study | 1443 | 68.9 | 45.8 | 8.6 | Sniffin’ Sticks Screening Test | 53.6 | Age, sex, failure to identify rose odor, ADL score, chronic kidney disease, serum LDL cholesterol, failure to identify fish odor, anemia, failure to identify coffee odor | 9 |
Abbreviations: ACE, angiotensin-converting enzyme; ADL, activities of daily living; BMI, body mass index; CES-D, Center for Epidemiologic Studies–Depression; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disorder; LDL, low-density lipoprotein; NA, not applicable; NHANES, National Health and Nutrition Examination Survey; NOS, Newcastle-Ottawa Scale; NSHAP, National Social Life, Health, and Aging Project; OI, olfactory impairment.
Association of OI With Mortality
Definition of OI
Ten of the included studies21,22,28,29,30,31,32,33,41,42 (Table) measured olfaction objectively via standardized tests, and 1 study40 assessed olfaction via self-report. Of the 10 studies that assessed olfaction objectively, OI was defined as the inability to recognize 2 of 3 odors (mint, coffee, and air),40 the inability to correctly identify more than 2 of 8 odors (2 studies),30,32 the inability to correctly identify 9 or more of 13 odors (1 study),29 and the inability to correctly identify 2 of 12 odors (2 studies).21,31 Three studies further stratified their population based on the severity of the impairment.22,28,42
Meta-analysis for All-Cause Mortality
Meta-analysis included 9 studies (Figure 2).21,22,28,29,30,32,33,40,42 Participants with OI had a significantly higher pooled hazard of all-cause mortality (HR, 1.52; 95% CI, 1.28-1.80) compared with participants without OI. Between-study heterogeneity was considerable (I2 = 82%) and statistically significant. Many of the studies adjusted for covariates: namely, age and sex (9 of 9), body mass index (2 of 9), educational level (7 of 9), smoking (5 of 9), alcohol use (4 of 9), hypertension (4 of 9), diabetes (6 of 9), cardiovascular disease (7 of 9), cognitive impairment (5 of 9), and head injury (2 of 9). Two studies were excluded from meta-analysis; Leschak and Eisenberger41 used mediation analysis and had no compatible effect size to pool, and Wilson et al31 calculated the HR with olfactory function as a continuous variable (B-SIT score) instead of dichotomizing participants into those with OI and those without OI. Wilson et al31 found that, for each additional accurate choice on an odor identification test, the risk of death within a mean time span of 5 years decreased by approximately 6%. Leschak and Eisenberger41 examined whether social deficits mediated the association between OI and mortality and found that physical intimacy significantly mediated the association between OI and mortality in women even after correcting for social network size, whereas this association was not mediated by emotional intimacy.
Figure 2. Forest Plot Showing the Longitudinal Association Between Olfactory Impairment and All-Cause Mortality.

HR indicates hazard ratio; seTE, standard error treatment effect; and TE, treatment effect.
Meta-regression and Subgroup Meta-analyses (by OI Measurement)
The meta-analysis of OI and all-cause mortality contained sufficient studies for further analyses. Meta-regression (eTable 4 in the Supplement) identified mean follow-up duration as a significant effect moderator (β [SE], –0.0504 [0.0120]; P = .02), accounting for 91.3% of heterogeneity. The pooled HR decreased by a factor of 0.95 for every additional yearly increase in follow-up. All other characteristics (sample size, country [non-US vs US], mean age, method of OI measurement [self-report vs objective], percentage of male participants, number of covariates, and prevalence of OI) were not significant effect moderators.
The pooled association remained significant and similar when subgroup meta-analyses were conducted (eTable 5 in the Supplement). When stratified by the method of OI measurement, heterogeneity for objective OI measurement subgroup analysis remained significant (I2 = 86%), whereas that for self-reported OI measurement was eliminated (I2 = 0%) (eFigure 1 in the Supplement). Further subgroup analyses including studies that used the same olfactory tests eliminated between-study statistical heterogeneity (I2 = 0%). When stratified by country, heterogeneity in non-US countries was eliminated, whereas that for US studies remained high (I2 = 90%) (eFigure 2 in the Supplement).
Sensitivity Analysis
Sensitivity analysis was performed, and 4 studies were excluded.21,22,28,42 Because Devanand et al28 and Liu et al21 stratified their population based on severity of OI and did not report an overall study estimate, we computed an overall study estimate using a fixed-effects model for our overall meta-analysis (Figure 2). Xiao et al42 used a single-smell test, unlike the other studies in which olfactory function was determined by a score derived from the identification of multiple odors. Pinto et al22 used odds ratios instead of HRs as reported by the other studies. Hence, owing to the differences in methods and statistical analyses of these 4 studies, we excluded them in a sensitivity analysis. The pooled HR remained statistically significant, and its 95% CI became narrower (HR, 1.35; 95% CI, 1.20-1.50). Heterogeneity was also eliminated (I2 = 0%).
Publication Bias
Publication bias was assessed qualitatively by visual inspection for funnel plot asymmetry (Figure 3), as well as quantitatively using the Egger test and trim-and-fill imputation. The funnel plot suggested possible asymmetry about the midpoint. However, results of the Egger test suggest that funnel plot asymmetry was not statistically significant.
Figure 3. Contour-Enhanced Funnel Plot for the Longitudinal Association of Olfactory Impairment With All-Cause Mortality.

The shaded circles indicate the original study estimates, and the unshaded circles indicate the missing estimate imputed via the trim-and-fill method. Dark gray, gray, and light gray contour lines indicate conventional milestones in levels of statistical significance (P < .10, P < .05, and P < .01, respectively).
To err on the side of caution, trim-and-fill adjustement was performed, which imputed 5 additional studies. The recomputed overall HR did not change substantially (HR, 1.21; 95% CI, 1.04-1.40).
Quality of Evidence
Using the GRADE framework (eTable 3 in the Supplement), the certainty of evidence for all-cause mortality was determined to be moderate. The certainty was upgraded by 1 level for studies reporting a dose-response relationship. Downgrading was not necessary because the initial detected heterogeneity was sufficiently explained by meta-regression (follow-up duration), with mean follow-up duration accounting for 91.3% of heterogeneity. The Egger test also demonstrated that bias was not significant, and trim-and-fill analysis showed that the pooled association remained significant.
Discussion
In this systematic review and meta-analysis of 11 observational studies comprising a combined cohort of 21 601 participants, we found that participants with OI had 52% increased hazards of all-cause mortality (HR, 1.52; 95% CI, 1.28-1.80) compared with participants with normal olfaction. This association was adjusted for potential confounders, such as age, sex, cognitive impairment, smoking, and alcohol use, and remained robust to quantitative and qualitative assessments of publication bias. Heterogeneity was sufficiently explained via subgroup analyses, sensitivity analyses, and meta-regression.
To our knowledge, this is the first systematic review and meta-analysis of the epidemiologic association between OI and mortality. Although we have shown the existence of this association, our study is unable to definitively deduce a causal relationship between OI and mortality. This evidence represents the burden of OI that is not due to COVID-19. Although COVID-19–related anosmia is associated with lower mortality, based on an observational study of 576 patients,36 it is unknown whether patients with COVID-19 and long-term anosmia are at higher subsequent risk of mortality compared with patients with COVID-19 who regain their sense of smell.
To date, the exact pathophysiologic characteristics linking OI and mortality are yet to be fully understood. Confounding is likely (Figure 4) and may include factors such as neurodegenerative disorders, systemic diseases, depression, advanced biological aging, and environmental pollution, among others. First, OI is a known early biomarker prior to full emergence of various neurodegenerative diseases, including Alzheimer disease and Parkinson disease.43,44,45,46,47 Neurodegenerative markers such as α-synuclein, β-amyloid, and tau have been implicated in the olfactory tract based on previous pathologic studies.45,46,48,49 Second, systemic diseases such as diabetes, autoimmune diseases, or iron deficiency may cause central and peripheral olfactory dysfunction10,11 and may be associated with mortality. Third, depression can generate endogenous inflammatory cytokines and glucocorticoids, which may impair olfactory neurogenesis and may also increase the risk of mortality.50,51,52 Fourth, OI may reflect underlying advanced physiological aging that predisposes an individual to mortality because cellular regeneration is an essential process in maintaining olfaction.23,53,54,55 Fifth, the olfactory nerve is the only cranial nerve in direct contact with the environment. Airborne toxicants may injure olfactory neurons55 as well as other organs, including the central nervous, pulmonary, and cardiovascular systems, which may be associated with increased mortality.33 Although not all these factors can be adjusted for in epidemiologic studies, many of the included studies had accounted for some of these factors as covariates. For instance, dementia or Parkinson disease explained only part of the association between OI and mortality,21 whereas adjustment for diabetes and depression did not weaken the association.29,30 Hence, mechanisms other than confounding should be considered.
Figure 4. Schematic Representation of Some Possible but Unconfirmed Confounders and Causal Pathways Between Olfactory Impairment and Mortality.
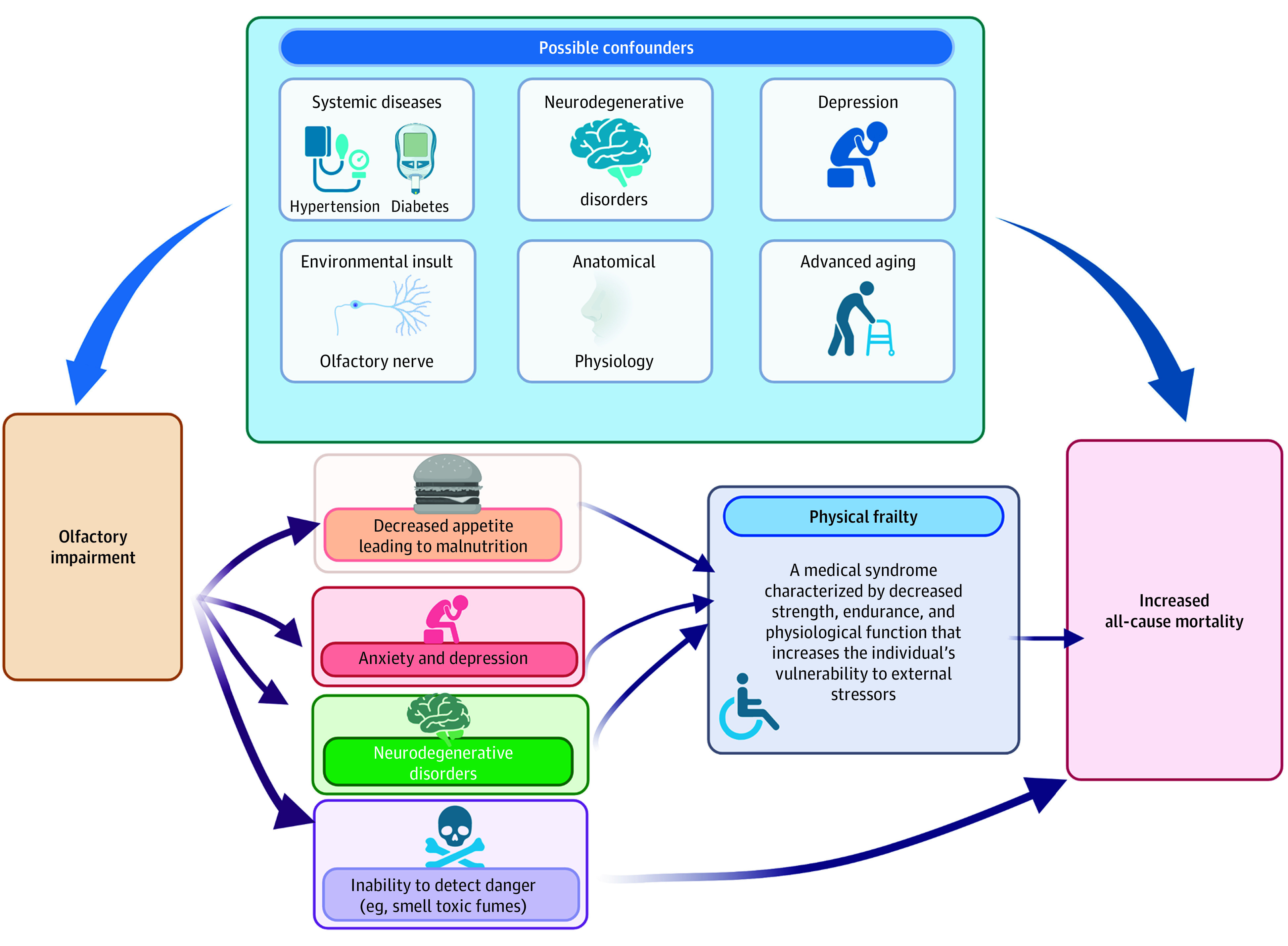
One potential mediator on the pathway between OI and mortality is physical frailty (Figure 4).56 Frailty is a medical syndrome characterized by decreased strength, endurance, and physiological function, increasing an individual’s vulnerability to external stressors,57,58 which may lead to increased mortality. There is some evidence that OI may be associated with frailty, and thus mortality, by means of malnutrition, depression, and cognitive decline. First, because taste is largely a function of retronasal olfaction, OI may impair the enjoyment of food, thus causing a loss of appetite, loss of weight, and malnutrition,47 which are factors associated with frailty. Second, OI may reduce food satisfaction, create concerns about personal hygiene, lessen social participation, and thus increase the risk of depression.15 Biologically, OI likely has an association with brain function, particularly emotional control,15 because olfactory bulb ablation elicits chemical and behavioral changes similar to those of depression.59 Third, smell may be involved in cognition because endoscopic sinus surgery that is associated with improved olfaction has been shown to enhance cognition.60 Together, malnutrition, depression, and cognitive impairment may be associated with frailty and mortality. Alternatively, OI may be directly associated with all-cause mortality owing to the inability to detect fires, gas leaks, spoiled food, and toxic substances.14 Nonetheless, our study cannot draw causal conclusions owing to the observational nature of the included studies.
Strengths and Limitations
There are several strengths of this review. The adequate number of systematically included studies from a varied range of situations enhances the generalizability of our findings. A strict prespecified method of systematically searching for bias and evaluating the quality of grading according to international criteria was followed. No studies were excluded based on high risk of bias. Of 11 included studies, only 1 had moderate risk of bias, whereas the rest had low risk of bias. To effectively account for relevant confounders in the extant literature, we extracted and pooled the maximally adjusted effect estimates. Meta-regression could effectively explain heterogeneity, with extended follow-up periods diminishing the association between OI and all-cause mortality. In addition, most of the included studies (8 of 9) used objective methods to quantify OI. These objective methods are frequently undertaken in controlled environments with defined processes that better measure OI and rely on genuine perception of stimulus when offered, reducing response and measurement bias.61
Nevertheless, several limitations must be considered. First, within the objective categories, different measurement methods were used by different studies, which may have resulted in measurement bias and may have reduced accuracy in quantifying OI. One of the 9 included studies in the meta-analysis used self-report, which may have resulted in inaccuracy becaused subjective measurements are prone to variation, inconsistency, and recall bias. Second, owing to the observational nature of the included studies, causal conclusions could not be made because residual confounding could not be ruled out, although the longitudinal nature of the studies showed a clear temporal sequence. It is possible that some unmeasured demographic characteristics, environmental factors, or preexisting comorbidities were not included as covariates. Third, the wide variation in the quantity and types of covariates among the included studies could have resulted in biased findings. Despite this, meta-regression failed to identify the number of covariates as a major effect moderator because most studies controlled for sociodemographic factors, lifestyle factors, and critical comorbidities, such as cardiovascular and neurodegenerative disease. Some studies may have established a negative bias by overadjusting their statistical models by incorporating variables that are mediators of the association between OI and mortality. Fourth, the considerable statistical heterogeneity of the included studies (I2 = 82%) may have limited the generalizability of our meta-analysis. This statistical heterogeneity may be due to clinical (eg, self-report and objective measurements) or methodological differences, or both. Fifth, the exclusion of articles not written in English may have restricted the external validity of our study and introduced a selection bias in the population. Sixth, given that vision and hearing impairments are also associated with mortality,62 further work should explore whether the excess mortality associated with OI may be compounded by the presence of concomitant sensory impairments.
Conclusions
In this multiadjusted observational systematic review and meta-analysis of 21 601 participants in 11 studies with moderate-quality evidence overall, OI was associated with a 52% higher risk of all-cause mortality. Olfactory impairment is a prevalent problem, especially among elderly individuals. Hence, physicians should consider the relevance of OI to general health and aging. Patients should be educated on the importance of OI and how to manage it and its underlying medical comorbidities. Moving forward, more research is required to determine the exact mechanism underlying the association between OI and mortality and the scope for interventions. These results will aid in understanding the causal relationship between OI and mortality and will be of great utility in deciding whether interventions (eg, medication or olfactory training) and testing for OI should be offered to reduce mortality and improve patients’ quality of life.
eMethods.
eReferences.
eFigure 1. Forest Plot Showing the Longitudinal Association Between Olfactory Impairment and All-Cause Mortality, Stratified by Method of Measurement of Olfactory Impairment
eFigure 2. Forest Plot Showing the Longitudinal Association Between Olfactory Impairment and All-Cause Mortality, Stratified by Country
eTable 1. Meta-analysis of Observational Studies in Epidemiology (MOOSE) Checklist
eTable 2. Evaluation of Risk of Bias Using the Newcastle-Ottawa Scale (NOS) for Cohort Studies
eTable 3. Evaluation of Quality of Pooled Evidence Using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Framework
eTable 4. Random-Effects Meta-Regression of Log(HRs) Against Potential Effect Moderators (Continuous and Categorical Study-Level Characteristics) for the Longitudinal Association of Olfactory Loss With All-Cause Mortality
eTable 5. Meta-Analyses in Subgroups, Stratified by Categorical Study-Level Characteristics for the Longitudinal Associations of Olfactory Impairment With All-Cause Mortality
References
- 1.Vennemann MM, Hummel T, Berger K. The association between smoking and smell and taste impairment in the general population. J Neurol. 2008;255(8):1121-1126. doi: 10.1007/s00415-008-0807-9 [DOI] [PubMed] [Google Scholar]
- 2.Brämerson A, Johansson L, Ek L, Nordin S, Bende M. Prevalence of olfactory dysfunction: the Skövde population-based study. Laryngoscope. 2004;114(4):733-737. doi: 10.1097/00005537-200404000-00026 [DOI] [PubMed] [Google Scholar]
- 3.Murphy C, Schubert CR, Cruickshanks KJ, Klein BE, Klein R, Nondahl DM. Prevalence of olfactory impairment in older adults. JAMA. 2002;288(18):2307-2312. doi: 10.1001/jama.288.18.2307 [DOI] [PubMed] [Google Scholar]
- 4.Godoy MD, Voegels RL, Pinna FdeR, Imamura R, Farfel JM. Olfaction in neurologic and neurodegenerative diseases: a literature review. Int Arch Otorhinolaryngol. 2015;19(2):176-179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Devanand DP, Lee S, Manly J, et al. Olfactory deficits predict cognitive decline and Alzheimer dementia in an urban community. Neurology. 2015;84(2):182-189. doi: 10.1212/WNL.0000000000001132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lafaille-Magnan ME, Poirier J, Etienne P, et al. ; PREVENT-AD Research Group . Odor identification as a biomarker of preclinical AD in older adults at risk. Neurology. 2017;89(4):327-335. doi: 10.1212/WNL.0000000000004159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Roberts RO, Christianson TJ, Kremers WK, et al. Association between olfactory dysfunction and amnestic mild cognitive impairment and Alzheimer disease dementia. JAMA Neurol. 2016;73(1):93-101. doi: 10.1001/jamaneurol.2015.2952 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Siegel JK, Wroblewski KE, McClintock MK, Pinto JM. Olfactory dysfunction persists after smoking cessation and signals increased cardiovascular risk. Int Forum Allergy Rhinol. 2019;9(9):977-985. doi: 10.1002/alr.22357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gopinath B, Russell J, Sue CM, Flood VM, Burlutsky G, Mitchell P. Olfactory impairment in older adults is associated with poorer diet quality over 5 years. Eur J Nutr. 2016;55(3):1081-1087. doi: 10.1007/s00394-015-0921-2 [DOI] [PubMed] [Google Scholar]
- 10.Dinc ME, Dalgic A, Ulusoy S, Dizdar D, Develioglu O, Topak M. Does iron deficiency anemia affect olfactory function? Acta Otolaryngol. 2016;136(7):754-757. doi: 10.3109/00016489.2016.1146410 [DOI] [PubMed] [Google Scholar]
- 11.Aydın E, Tekeli H, Karabacak E, et al. Olfactory functions in patients with psoriasis vulgaris: correlations with the severity of the disease. Arch Dermatol Res. 2016;308(6):409-414. doi: 10.1007/s00403-016-1662-7 [DOI] [PubMed] [Google Scholar]
- 12.Dong J, Pinto JM, Guo X, et al. The prevalence of anosmia and associated factors among U.S. Black and White older adults. J Gerontol A Biol Sci Med Sci. 2017;72(8):1080-1086. doi: 10.1093/gerona/glx081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Seo HS, Jeon KJ, Hummel T, Min BC. Influences of olfactory impairment on depression, cognitive performance, and quality of life in Korean elderly. Eur Arch Otorhinolaryngol. 2009;266(11):1739-1745. doi: 10.1007/s00405-009-1001-0 [DOI] [PubMed] [Google Scholar]
- 14.Santos DV, Reiter ER, DiNardo LJ, Costanzo RM. Hazardous events associated with impaired olfactory function. Arch Otolaryngol Head Neck Surg. 2004;130(3):317-319. doi: 10.1001/archotol.130.3.317 [DOI] [PubMed] [Google Scholar]
- 15.Croy I, Nordin S, Hummel T. Olfactory disorders and quality of life—an updated review. Chem Senses. 2014;39(3):185-194. doi: 10.1093/chemse/bjt072 [DOI] [PubMed] [Google Scholar]
- 16.Berg D, Godau J, Seppi K, et al. ; PRIPS Study Group . The PRIPS Study: screening battery for subjects at risk for Parkinson’s disease. Eur J Neurol. 2013;20(1):102-108. doi: 10.1111/j.1468-1331.2012.03798.x [DOI] [PubMed] [Google Scholar]
- 17.Chen H, Shrestha S, Huang X, et al. ; Health ABC Study . Olfaction and incident Parkinson disease in US White and Black older adults. Neurology. 2017;89(14):1441-1447. doi: 10.1212/WNL.0000000000004382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ross GW, Petrovitch H, Abbott RD, et al. Association of olfactory dysfunction with risk for future Parkinson’s disease. Ann Neurol. 2008;63(2):167-173. doi: 10.1002/ana.21291 [DOI] [PubMed] [Google Scholar]
- 19.Finkel D, Reynolds CA, Larsson M, Gatz M, Pedersen NL. Both odor identification and ApoE-ε4 contribute to normative cognitive aging. Psychol Aging. 2011;26(4):872-883. doi: 10.1037/a0023371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Olofsson JK, Rönnlund M, Nordin S, Nyberg L, Nilsson LG, Larsson M. Odor identification deficit as a predictor of five-year global cognitive change: interactive effects with age and ApoE-epsilon4. Behav Genet. 2009;39(5):496-503. doi: 10.1007/s10519-009-9289-5 [DOI] [PubMed] [Google Scholar]
- 21.Liu B, Luo Z, Pinto JM, et al. Relationship between poor olfaction and mortality among community-dwelling older adults: a cohort study. Ann Intern Med. 2019;170(10):673-681. doi: 10.7326/M18-0775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pinto JM, Wroblewski KE, Kern DW, Schumm LP, McClintock MK. Olfactory dysfunction predicts 5-year mortality in older adults. PLoS One. 2014;9(10):e107541. doi: 10.1371/journal.pone.0107541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Watabe-Rudolph M, Begus-Nahrmann Y, Lechel A, et al. Telomere shortening impairs regeneration of the olfactory epithelium in response to injury but not under homeostatic conditions. PLoS One. 2011;6(11):e27801. doi: 10.1371/journal.pone.0027801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Prediger RD, Aguiar AS Jr, Matheus FC, et al. Intranasal administration of neurotoxicants in animals: support for the olfactory vector hypothesis of Parkinson’s disease. Neurotox Res. 2012;21(1):90-116. doi: 10.1007/s12640-011-9281-8 [DOI] [PubMed] [Google Scholar]
- 25.Weinstock RS, Wright HN, Smith DU. Olfactory dysfunction in diabetes mellitus. Physiol Behav. 1993;53(1):17-21. doi: 10.1016/0031-9384(93)90005-Z [DOI] [PubMed] [Google Scholar]
- 26.Tung TH, Chen SJ, Liu JH, et al. A community-based follow-up study on diabetic retinopathy among type 2 diabetics in Kinmen. Eur J Epidemiol. 2005;20(4):317-323. doi: 10.1007/s10654-004-6651-z [DOI] [PubMed] [Google Scholar]
- 27.Kohler CG, Moberg PJ, Gur RE, O’Connor MJ, Sperling MR, Doty RL. Olfactory dysfunction in schizophrenia and temporal lobe epilepsy. Neuropsychiatry Neuropsychol Behav Neurol. 2001;14(2):83-88. [PubMed] [Google Scholar]
- 28.Devanand DP, Lee S, Manly J, et al. Olfactory identification deficits and increased mortality in the community. Ann Neurol. 2015;78(3):401-411. doi: 10.1002/ana.24447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ekström I, Sjölund S, Nordin S, et al. Smell loss predicts mortality risk regardless of dementia conversion. J Am Geriatr Soc. 2017;65(6):1238-1243. doi: 10.1111/jgs.14770 [DOI] [PubMed] [Google Scholar]
- 30.Schubert CR, Fischer ME, Pinto AA, et al. Sensory impairments and risk of mortality in older adults. J Gerontol A Biol Sci Med Sci. 2017;72(5):710-715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wilson RS, Yu L, Bennett DA. Odor identification and mortality in old age. Chem Senses. 2011;36(1):63-67. doi: 10.1093/chemse/bjq098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gopinath B, Sue CM, Kifley A, Mitchell P. The association between olfactory impairment and total mortality in older adults. J Gerontol A Biol Sci Med Sci. 2012;67(2):204-209. doi: 10.1093/gerona/glr165 [DOI] [PubMed] [Google Scholar]
- 33.Choi JS, Jang SS, Kim J, Hur K, Ference E, Wrobel B. Association between olfactory dysfunction and mortality in US adults. JAMA Otolaryngol Head Neck Surg. 2021;147(1):49-55. doi: 10.1001/jamaoto.2020.3502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71):n71. doi: 10.1136/bmj.n71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting: Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 36.Talavera B, García-Azorín D, Martínez-Pías E, et al. Anosmia is associated with lower in-hospital mortality in COVID-19. J Neurol Sci. 2020;419:117163. doi: 10.1016/j.jns.2020.117163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute. Accessed October 24, 2021. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 38.Symons MJ, Moore DT. Hazard rate ratio and prospective epidemiological studies. J Clin Epidemiol. 2002;55(9):893-899. doi: 10.1016/S0895-4356(02)00443-2 [DOI] [PubMed] [Google Scholar]
- 39.Guyatt GH, Oxman AD, Vist GE, et al. ; GRADE Working Group . GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926. doi: 10.1136/bmj.39489.470347.AD [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Laudisio A, Navarini L, Margiotta DPE, et al. The association of olfactory dysfunction, frailty, and mortality is mediated by inflammation: results from the InCHIANTI Study. J Immunol Res. 2019;2019:3128231. doi: 10.1155/2019/3128231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Leschak CJ, Eisenberger NI. The role of social relationships in the link between olfactory dysfunction and mortality. PLoS One. 2018;13(5):e0196708. doi: 10.1371/journal.pone.0196708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Xiao Z, Zhao Q, Liang X, Wu W, Cao Y, Ding D. Poor odor identification predicts mortality risk in older adults without neurodegenerative diseases: the Shanghai Aging Study. J Am Med Dir Assoc. 2021;22(10):2218-2219. doi: 10.1016/j.jamda.2021.05.026 [DOI] [PubMed] [Google Scholar]
- 43.Djordjevic J, Jones-Gotman M, De Sousa K, Chertkow H. Olfaction in patients with mild cognitive impairment and Alzheimer’s disease. Neurobiol Aging. 2008;29(5):693-706. doi: 10.1016/j.neurobiolaging.2006.11.014 [DOI] [PubMed] [Google Scholar]
- 44.Attems J, Walker L, Jellinger KA. Olfactory bulb involvement in neurodegenerative diseases. Acta Neuropathol. 2014;127(4):459-475. doi: 10.1007/s00401-014-1261-7 [DOI] [PubMed] [Google Scholar]
- 45.Vasavada MM, Wang J, Eslinger PJ, et al. Olfactory cortex degeneration in Alzheimer’s disease and mild cognitive impairment. J Alzheimers Dis. 2015;45(3):947-958. doi: 10.3233/JAD-141947 [DOI] [PubMed] [Google Scholar]
- 46.Wilson RS, Schneider JA, Arnold SE, Tang Y, Boyle PA, Bennett DA. Olfactory identification and incidence of mild cognitive impairment in older age. Arch Gen Psychiatry. 2007;64(7):802-808. doi: 10.1001/archpsyc.64.7.802 [DOI] [PubMed] [Google Scholar]
- 47.Van Regemorter V, Hummel T, Rosenzweig F, Mouraux A, Rombaux P, Huart C. Mechanisms linking olfactory impairment and risk of mortality. Front Neurosci. 2020;14:140. doi: 10.3389/fnins.2020.00140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Attems J, Jellinger KA. Olfactory tau pathology in Alzheimer disease and mild cognitive impairment. Clin Neuropathol. 2006;25(6):265-271. [PubMed] [Google Scholar]
- 49.Jellinger KA, Attems J. Alzheimer pathology in the olfactory bulb. Neuropathol Appl Neurobiol. 2005;31(2):203. doi: 10.1111/j.1365-2990.2004.00619.x [DOI] [PubMed] [Google Scholar]
- 50.Kohli P, Soler ZM, Nguyen SA, Muus JS, Schlosser RJ. The association between olfaction and depression: a systematic review. Chem Senses. 2016;41(6):479-486. doi: 10.1093/chemse/bjw061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Furtado M, Katzman MA. Examining the role of neuroinflammation in major depression. Psychiatry Res. 2015;229(1-2):27-36. doi: 10.1016/j.psychres.2015.06.009 [DOI] [PubMed] [Google Scholar]
- 52.Yuan TF, Hou G, Arias-Carrion O. Chronic stress impacts on olfactory system. CNS Neurol Disord Drug Targets. 2015;14(4):486-491. doi: 10.2174/1871527314666150429111356 [DOI] [PubMed] [Google Scholar]
- 53.Pagano SF, Impagnatiello F, Girelli M, et al. Isolation and characterization of neural stem cells from the adult human olfactory bulb. Stem Cells. 2000;18(4):295-300. doi: 10.1634/stemcells.18-4-295 [DOI] [PubMed] [Google Scholar]
- 54.Prediger RDS, Aguiar AS Jr, Matheus FC, et al. Intranasal administration of neurotoxicants in animals: support for the olfactory vector hypothesis of Parkinson’s disease. Neurotox Res. 2012;21(1):90-116. [DOI] [PubMed] [Google Scholar]
- 55.Doty RL. The olfactory vector hypothesis of neurodegenerative disease: is it viable? Ann Neurol. 2008;63(1):7-15. doi: 10.1002/ana.21327 [DOI] [PubMed] [Google Scholar]
- 56.Tan BKJ, Man REK, Gan ATL, et al. Is sensory loss an understudied risk factor for frailty? a systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. 2020;75(12):2461-2470. Published correction appears in J Gerontol A Biol Sci Med Sci. 2022;77(2):e109. doi: 10.1093/gerona/glaa171 [DOI] [PubMed] [Google Scholar]
- 57.Somekawa S, Mine T, Ono K, et al. Relationship between sensory perception and frailty in a community-dwelling elderly population. J Nutr Health Aging. 2017;21(6):710-714. doi: 10.1007/s12603-016-0836-5 [DOI] [PubMed] [Google Scholar]
- 58.Harita M, Miwa T, Shiga H, et al. Association of olfactory impairment with indexes of sarcopenia and frailty in community-dwelling older adults. Geriatr Gerontol Int. 2019;19(5):384-391. doi: 10.1111/ggi.13621 [DOI] [PubMed] [Google Scholar]
- 59.Lumia AR, Teicher MH, Salchli F, Ayers E, Possidente B. Olfactory bulbectomy as a model for agitated hyposerotonergic depression. Brain Res. 1992;587(2):181-185. doi: 10.1016/0006-8993(92)90995-L [DOI] [PubMed] [Google Scholar]
- 60.Alt JA, Mace JC, Smith TL, Soler ZM. Endoscopic sinus surgery improves cognitive dysfunction in patients with chronic rhinosinusitis. Int Forum Allergy Rhinol. 2016;6(12):1264-1272. doi: 10.1002/alr.21820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Hannum ME, Ramirez VA, Lipson SJ, et al. Objective sensory testing methods reveal a higher prevalence of olfactory loss in COVID-19 positive patients compared to subjective methods: a systematic review and meta-analysis. medRxiv. Preprint published July 6, 2020. doi: 10.1101/2020.07.04.20145870 [DOI] [PMC free article] [PubMed]
- 62.Tan BKJ, Ng FYC, Song HJJMD, Tan NKW, Ng LS, Loh WS. Associations of hearing loss and dual sensory loss with mortality: a systematic review, meta-analysis, and meta-regression of 26 observational studies with 1 213 756 participants. JAMA Otolaryngol Head Neck Surg. Published online December 30, 2021. doi: 10.1001/jamaoto.2021.3767 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods.
eReferences.
eFigure 1. Forest Plot Showing the Longitudinal Association Between Olfactory Impairment and All-Cause Mortality, Stratified by Method of Measurement of Olfactory Impairment
eFigure 2. Forest Plot Showing the Longitudinal Association Between Olfactory Impairment and All-Cause Mortality, Stratified by Country
eTable 1. Meta-analysis of Observational Studies in Epidemiology (MOOSE) Checklist
eTable 2. Evaluation of Risk of Bias Using the Newcastle-Ottawa Scale (NOS) for Cohort Studies
eTable 3. Evaluation of Quality of Pooled Evidence Using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Framework
eTable 4. Random-Effects Meta-Regression of Log(HRs) Against Potential Effect Moderators (Continuous and Categorical Study-Level Characteristics) for the Longitudinal Association of Olfactory Loss With All-Cause Mortality
eTable 5. Meta-Analyses in Subgroups, Stratified by Categorical Study-Level Characteristics for the Longitudinal Associations of Olfactory Impairment With All-Cause Mortality