

Abstract
This study aimed to explore the structure of a modified version of the Girls Questionnaire for Autism Spectrum Condition (GQ-ASC; Attwood et al. 2011) to test its utility as an autism screening measure for adult women. We recruited 672 cisgender and trans women aged between 18 and 72 online. The sample contained 350 autistic women (M age = 36.21, standard deviation [SD] = 10.10) and 322 nonautistic women (M age = 34.83, SD = 9.93), screened using the Autism Quotient. A principal component analysis and parallel analysis revealed a five-component solution that accounted for 40.40% of the total variance. The extracted components appear to be consistent with what is known about the way girls and women display their autistic traits and interpreted as (1) Imagination and play: Describes interest in fantasy, fiction, and reflection on the quality and content of imaginative play in childhood. (2) Camouflaging: Describes effortful attempts to reduce the visibility of autistic traits. (3) Sensory sensitivities: Describes sensory processing hyper- and hyposensitivities across various modalities. (4) Socializing: Describes barriers to social understanding and participation. (5) Interests: Describes age-advanced and nonstereotypically feminine interests. We observed significant differences between autistic and nonautistic women across all extracted components, and the total score. A receiver operating characteristic analysis indicated an excellent level of discrimination. When applying a cutoff score of 57, the GQ-ASC correctly identified 80.0% of cases. The modified GQ-ASC is an effective and highly discriminant screening tool for use in adult autistic women. It provides valuable insight into the shared features and experiences of this underrecognized and underrepresented subset of the autistic community.
Lay summary
Why was this study done?
A lot of autistic women do not get an accurate or timely autism diagnosis. We know that when they do receive an autism diagnosis, they often feel stronger in their identity and feel more confident in advocating for their needs. We wanted to find a quick and easy way for professionals to work out which women should be referred for an autism assessment. We also wanted to help autistic women who do not want to have an assessment done feel confident in self-identifying as autistic.
What did the researchers do?
We changed the wording of an autism questionnaire that was designed for younger girls, and had 350 adult autistic cisgender and trans women aged between 18 and 71 years complete it. We looked at answers in a way that told us which questions were most useful for telling apart autistic women and nonautistic women.
What were the results of the study?
We found that a number of questions were grouped together into different areas that were common for autistic women. These areas were as follows:
-
(1)
Imagination and play: Questions about interest in fantasy, fiction, and imaginative play in childhood.
-
(2)
Camouflaging: Questions about acting in certain ways to try to hide autistic traits.
-
(3)
Sensory sensitivities: Questions about feeling undersensitive or oversensitive to things such as touch, small, taste, and noise.
-
(4)
Socializing: Questions about feeling confused in social situations, and finding it difficult to join in.
-
(5)
Interests: Questions about interests that are not common for children who are the same age, and interests that are not common for many girls.
What do these findings add to what was already known?
There are a lot of ideas about autism that do not always apply to autistic women. These findings will hopefully help professionals and nonexperts understand autistic women better.
What are potential weaknesses in the study?
We do not know if any of the 350 autistic women who completed the survey have an intellectual disability, and we do not know if having an intellectual disability will change the results of the study. This is something that will be interesting to look into in the future.
How will these findings help autistic adults now and in the future?
The findings of our study can help doctors and mental health professionals work out which women should be assessed for autism. Our findings may also help to change attitudes about who can be autistic, and what autism looks like.
Keywords: autistic, women, screening
Introduction
Autism Spectrum Disorder (ASD; henceforth, autism) is currently diagnosed at a rate of approximately three males to every one female,1 although some evidence suggests that the rate may be as low as 1.8:1.2 At present, there are a number of barriers that delay or prevent autistic girls and women from accessing assessment services. These include, although are not limited to, gendered assumptions about how autism presents and who it impacts1; an increased likelihood that female autistic traits will be attributed to other causes3,4; standardized assessment measures that may not be sensitive enough to capture autistic girls and women who experience and express their autism in unique and nuanced ways5–7; and active attempts by autistic girls and women to camouflage, or mask challenges related to their autistic traits to blend into social situations.8,9
The rate of identification and diagnosis in females, particularly girls, has improved over time,10 although they are still thought to be underrecognized and underrepresented.8 So, while the future for autistic girls continues to improve, it begs an important question: Where are all the autistic women?
It is the notion of a lost generation of autistic women11 that provides the impetus for the current line of enquiry. Formal diagnosis typically allows individuals access to support services, yet access to time and cost-effective screening measures may be as crucial. Screening tools can help clinicians identify those who should be referred for formal assessments, and assist those who do not wish to undergo formal assessments. For autistic women who do not feel the need to have their identity validated by the medical model of disability, access to sensitive and specific screening measures may be an empowering tool that allows them to assert and define their own autistic identity.11,12 When women do claim their autistic status, many report the process to be powerful and transformative.13 So much so that many feel the experience grants them a new sense of identity, purpose, and hope14 that allow them to be more assertive in their relationships, opinions, and in advocating for their needs.15
Aims
In this study, we aim to evaluate an autism screening measure, the Girls Questionnaire for Autism Spectrum Condition (GQ-ASC; Appendix Table A1),16 to establish its utility for identifying adult autistic cisgender and trans women. To do this, we conducted an exploratory investigation of GQ-ASC items to determine their appropriateness for use in autistic women older than 18 years. We also examined group differences between autistic and nonautistic women (N-ASD) on the extracted components of the GQ-ASC, and established an appropriate cutoff value that effectively discriminates between autistic and nonautistic women.
Method
Study design and participants
This study operated as an online, self-report questionnaire. We recruited n = 350 autistic cisgender and trans women, aged between 18 and 71 years, and n = 322 nonautistic cisgender and trans women, aged between 18 and 72 years (Table 1), through social media and online peer and support groups. Autistic participants reported that they had received a formal diagnosis, and we retained them for inclusion in this study if they also scored above 32 on the Autism Quotient (AQ).17,18 We retained nonautistic participants if they did not report a formal diagnosis and did not score above 32 on the AQ. It is worth noting that autistic traits, as displayed by girls and women, are not always effectively measured by the AQ due to inherent sensitivity issues.19 We made the methodological decision to use the AQ, as at present it is one of the most reliable screening tools for measuring the presence of autistic traits. Given the aforementioned issue of female underrepresentation in the autistic population, it was deemed appropriate to effectively distinguish between autistic and nonautistic (although potentially undiagnosed) participants in this community sample.
Table 1.
Participant Characteristics
| ASD |
N-ASD |
|
|---|---|---|
|
n = 350 |
n = 322 |
|
| n (%) | n (%) | |
| Age | M = 36.21 years, SD = 10.10 | M = 34.88 years, SD = 9.93 |
| Ethnicity | ||
| Caucasian | 283 (80.90) | 272 (84.50) |
| Country of residence | ||
| Australia | 112 (32.20) | 246 (76.66) |
| The United Kingdom | 64 (18.30) | 17 (5.30) |
| The United States | 124 (33.60) | 41 (12.80) |
| Canada | 14 (4.00) | 2 (0.60) |
| Sex at birth | ||
| Female | 345 (98.60) | 322 (100.00) |
| Male | 4 (1.10) | — |
| Other | 1 (0.30) | — |
| Gender identity | ||
| Female | 280 (80.20) | 309 (96.30) |
| Male | 3 (0.90) | 1 (0.30) |
| Other | 66 (18.90) | 11 (3.40) |
ASD, autistic participants; N-ASD, nonautistic participants; SD, standard deviation.
Furthermore, we made this methodological decision to include both cisgender and trans women in an attempt to retain a more inclusive and representative cohort.
Ethical considerations
We received ethical approval from the governing university Human Research Ethics Committee. This was in accordance with the ethical standards of the national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. We obtained informed consent from all participants. No monetary or other incentives were offered to participants.
Materials
Girls Questionnaire for Autism Spectrum Condition
We used a version of the GQ-ASC,16 modified for use with adult women. The GQ-ASC is a 58-item screening assessment, relating to four areas: Play between ages 5 and 12 years, Friendship and Social Situations, Abilities and Interests, and Sensory Profile and Medical History. Fifty-four of the 58 GQ-ASC questions are scored on a 4-point agree/disagree scale (definitely agree, slightly agree, slightly disagree, and definitely disagree), while four items yield a yes/no response for the presence of mental health symptomology. The GQ-ASC was initially designed for self-report use in ages 13–19, with an extension of age found to be appropriate (typically up to 25 years).16 We modified the GQ-ASC language to again expand the age criteria in the present study, by presenting age limiting questions in the past tense (e.g., “I was well behaved at school,” instead of “I am well behaved school”).
Autism Spectrum Quotient
The AQ17 is a frequently used, self-administered instrument that is designed to measure the degree to which an individual, without a co-occurring intellectual disability, has traits associated with autism. The AQ is designed for use in adults aged 16 years and older. It comprised 50 questions, assessing five different areas related to autism: Social Skills, Attention Switching, Attention to Detail, Communication, and Imagination. The AQ is scored on a 4-point agree/disagree scale (definitely agree, slightly agree, slightly disagree, and definitely disagree). Baron-Cohen et al.17 established that a cutoff score of 32 identified 80% of autistic individuals, while only 2% of controls exceeded the cutoff. This cutoff score was subsequently confirmed as appropriate in a more recent Australian study, where test/retest reliability was also high.18
Procedure
We placed advertisements on social media and online women's autism community and support groups. Advertising materials targeted women older than 18 years, who had either received an autism diagnosis or were nonautistic. We asked participants to complete an online, self-report questionnaire. We presented participants with a plain language statement explaining the nature of the study and asked them to give their informed consent to participate. We collected nonidentifiable demographic information, followed by the measures listed above.
Statistical analysis
We used IBM SPSS version 25 (IBM Corp, Armonk, NY) to analyze data. We used the AQ to cross-reference autism diagnoses and give an approximation of autism trait severity. We performed a principal component analysis (PCA) with orthogonal varimax rotation on GQ-ASC items, using data from autistic participants only. We used Monte Carlo testing to conduct a parallel analysis of 1000 raw data permutations to determine the number of eigenvalues to be extracted, and a Mann–Whitney U test o examine group differences between autistic and nonautistic women when responding to the extracted components of the GQ-ASC. We used Fisher's z to understand differences in correlations between the GQ-ASC and the AQ, and finally, we used a receiver operating characteristic (ROC) curve to define a scoring cutoff value that demonstrated good sensitivity and specificity in discriminating between autistic and nonautistic cases.
Results
Data screening and preliminary analyses
Preliminary analyses revealed 5.10% of missing data across GQ-ASC items. Little's MCAR test determined these values to be missing completely at random (χ2(839) = 850.58, p = 0.38), and they were replaced using an expectation maximization technique. Kolmogorov–Smirnov tests indicated that all GQ-ASC items were non-normally distributed (p < 0.001), which was expected, as we included only autistic cases. Skew on individual GQ-ASC items ranged from −3.68 (standard error [SE] = 1.31), with a kurtosis of 15.34 (SE = 0.26), to 1.69 (SE = 0.13), with a kurtosis of 2.42 (SE = 0.26).
Principal component analysis
We assessed the suitability of PCA before analysis by manually inspecting the item correlation matrix. It revealed that all variables had at least one correlation coefficient >0.30. The overall Kaiser–Meyer–Olkin (KMO) was 0.71, while individual KMO values ranged between 0.51 and 0.82. Variables with a KMO below 0.50 were removed from subsequent PCA iterations (n = 1, KMO = 0.45; Kaiser, 1974). Bartlett's test of sphericity was significant (p > 0.001), indicating that data were factorizable.
We conducted an initial PCA on 54 items of the 58 GQ-ASC items. Four items were excluded from the analysis as they produced a binary yes/no outcome. The initial PCA revealed 19 components with eigenvalues greater than one. Visual inspection of the scree plot indicated that six components should be retained for further analyses.20 We removed 19 items from subsequent PCA iterations as they did not meet the minimum inclusion criteria (Table 2). Namely, the retained components load onto individual variables at a level higher than 0.40 (component loading >0.40); the proportion of each variable's variance accounted for by the PCA be >0.30 (communalities >0.30); and the resultant solution does not display a “complex structure” (i.e., no cross-loading variables).
Table 2.
Items Excluded from Principal Component Analyses
| GQ-ASC items | Reason for exclusion |
|---|---|
| 8. When I was 5–12 years old, I role played the teacher or other adults in my solitary games | 1, 2 |
| 10. I have many friends | 1, 2 |
| 11. I preferred to play with younger children | 1, 2 |
| 12. I prefer single, close friendships | 1, 2 |
| 26. My facial expression sometimes does not match my mood or the situation | 1, 2 |
| 30. I am talented in art | 1, 2 |
| 31. I am talented in mathematics | 3 |
| 33. I like to express myself in writing (journaling in pen or pencil, or in emails, or I write fiction) | 1, 2 |
| 34. I am talented in languages | 1, 2 |
| 37. I stand out as different from my peers in terms of clothing | 1, 2 |
| 40. I am interested in nature | 1, 2 |
| 42. I have a special interest related to food | 2 |
| 47. I am bothered by bright lights or certain kind of lights (e.g., fluorescent light) | 1, 2 |
| 49. I have poor endurance and tire easily | 1, 2 |
| 50. I seek certain sensations (e.g., I jump, swing, spin, can't sit still, fidget, masturbate intensively, twist blanket around my body tightly) | 2 |
| 51. I avoid certain sensations (e.g., I am distressed when my feet leave the ground, I fear heights, dislike activities where my head is upside down) | 1, 2 |
| 52. I am distracted during any task or conversation when there is a lot of noise around | 1, 2 |
| 54. I am confused about my sexual orientation | 1, 2 |
| 35R. I am interested in looking feminine | 1, 2 |
1, component loading <0.40; 2, communality <0.30; 3, KMO <0.50.
GQ-ASC, Girls Questionnaire for Autism Spectrum Condition; KMO, Kaiser–Meyer–Olkin.
We applied a varimax orthogonal rotation to aid interpretability, with the resulting rotated solution exhibiting a “simple structure,”21 containing six components that explained 46.82% of the total variance. We then used a Monte Carlo simulation to conduct a parallel analysis19 of 1000 raw data permutations to robustly determine the number of eigenvalues to be retained.22 It revealed a five-component solution that accounted for 40.40% of the total variance, with the sixth component plotting marginally below the simulated data mean and 95th percentile (Fig. 1).
FIG. 1.

Factor analysis scree plots for data and for modeled parallel analysis based on 1000 permutations. Both curves show 95% confidence intervals.
We interpreted the extracted components as follows: (1) Imagination and play: Describes interest in fantasy, fiction, and reflection on the quality and content of imaginative play in childhood; (2) Camouflaging: Describes effortful attempts to reduce the visibility of autistic traits; (3) Sensory sensitivities: Describes sensory processing hyper- and hyposensitivities across various modalities; (4) Socializing: Describes barriers to social understanding and participation; (5) Interests: Describes age-advanced and nonstereotypically feminine interests; and the subsequently excluded component (6) Compliant behavior: Describes behavior that is compliant with authority and peers. All extracted components were considered to be consistent with girls' and women's autistic trait presentation (Table 3). We assessed the reliability of the five retained components by calculating McDonald's omega, which were all low or approaching adequate levels (Table 3).
Table 3.
Summary of Six Extracted Components with Varimax Rotation for 22 Items
| GQ-ASC components and items | Component loading | Communalities | ω |
|---|---|---|---|
| Component 1: Imagination and play | 0.64 | ||
| 28R. I enjoy fantasy worlds | 0.74 | 0.60 | |
| 29R. I am interested in fiction | 0.64 | 0.44 | |
| 5R. When I was 5–12 years old, I played as imaginatively as other girls | 0.63 | 0.48 | |
| 4R. When I was 5–12 years old, I had imaginary friends or imaginary animals | 0.59 | 0.41 | |
| 6R. When I was 5–12 years old, I created my own complex “setups” with toys | 0.53 | 0.36 | |
| Component 2: Camouflaging | 0.67 | ||
| 17. I copy or “clone” myself on other females | 0.76 | 0.65 | |
| 16. I avidly observe other females socializing | 0.70 | 0.51 | |
| 15. I am attracted to females with strong personalities who tell me what to do | 0.65 | 0.55 | |
| 18. I adopt a different persona in different situations | 0.59 | 0.46 | |
| Component 3: Sensory sensitivities | 0.58 | ||
| 53. I am attached to certain objects or toys (e.g., favorite toy, pillow, piece of cloth) which I carry, touch, or rub to calm myself | 0.66 | 0.51 | |
| 46. I expressed distress during grooming (e.g., I fight or cry during fingernail cutting, haircutting, combing) or when I am touched (e.g., someone touches my feet) | 0.63 | 0.49 | |
| 24. Some social situations make me mute | 0.55 | 0.34 | |
| 48. I am distressed by certain smells or I avoid certain tastes that are a typical part of a diet | 0.51 | 0.33 | |
| Component 4: Socializing | 0.58 | ||
| 25. I socialize quite well for a while, but subsequently feel exhausted | 0.73 | 0.59 | |
| 23. I often have a facial “mask” that hides my social confusion | 0.57 | 0.49 | |
| 45. I have intense emotions | 0.54 | 0.38 | |
| 21. I apologize when I make a social error | 0.48 | 0.38 | |
| Component 5: Interests | 0.56 | ||
| 1R. When I was 5–12 years old, I preferred to play with girls' toys | 0.75 | 0.61 | |
| 2. When I was 5–12 years old, I preferred to play with boys' toys | 0.70 | 0.51 | |
| 38. My interests were advanced for my age (e.g., opera) | 0.55 | 0.35 | |
| 32. I am talented in music | 0.51 | 0.33 |
R, reverse scored item; ω, McDonald's omega.
Weak to moderate bivariate correlations between each of the resultant GQ-ASC components indicated no evidence of multicollinearity. Correlation coefficients ranged between 0.08 and 0.74 (Table 4).
Table 4.
Subscale Correlation Matrix
| GQ-ASC subscales | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Imagination and play | 1.00 | ||||
| 2. Camouflaging | 0.52 | 1.00 | |||
| 3. Sensory | 0.08* | 0.48** | 1.00 | ||
| 4. Socializing | 0.12** | 0.46** | 0.53** | 1.00 | |
| 5. Interests | 0.05 | 0.16** | 0.37** | 0.28** | 1.00 |
Pearson's r; **p < 0.01, *p < 0.05.
Group differences on GQ-ASC components
We performed a Mann–Whitney U test to compare GQ-ASC component scores for autistic and nonautistic women, where higher scores indicate great endorsement of the items in each component. We applied reverse scoring to some items, indicating that a higher score on these questions equals a lower endorsement of the item (denoted by R, Table 3). We found significant differences in all components, and the total score (Table 5).
Table 5.
Mann–Whitney U Test for Girls Questionnaire for Autism Spectrum Condition Subscales Between Autistic and Nonautistic Women
| ASD |
N-ASD |
U | z | p | |
|---|---|---|---|---|---|
|
n = 350 |
n = 322 |
||||
| Mean rank | Mean rank | ||||
| Imagination and play | 365.70 | 310.36 | 47,956.00 | −3.13 | 0.002 |
| Camouflaging | 407.49 | 295.34 | 31,504.00 | −9.93 | <0.001 |
| Sensory | 455.61 | 207.03 | 14,660.00 | −16.62 | <0.001 |
| Socializing | 412.32 | 254.09 | 29,813.50 | −10.69 | <0.001 |
| Interests | 413.14 | 253.19 | 29,524.00 | −10.72 | <0.001 |
| Total score | 438.54 | 225.60 | 20,639.50 | −14.21 | <0.001 |
ASD, autistic women; N-ASD, nonautistic women.
The results demonstrate that while there are significant differences between the groups, autistic women do not display more traits associated with the extracted components overall. Autistic women had greater sensory sensitivities and engaged in higher levels of camouflaging behavior, but they engaged less with imagination and play, and were less interested in stereotypically feminine toys and age-typical interests in childhood (Table 5).
Group differences between the GQ-ASC and AQ
We used Spearman's rank-order correlation to examine the relationship between the GQ-ASC and AQ at both total score and component levels. We found that while many of the subscales displayed a moderate degree of correlation, others displayed weak or no association at all (Table 6). To assess the significance of the difference between correlation coefficients from the GQ-ASC and the AQ in autistic and nonautistic participants, we first collapsed Spearman's ρ to Pearson's r,23 to apply Fisher's r-to-z transformation. We found significant differences in many of the correlations, indicating that while both scales measure autistic traits, they appear to be measuring different constructs associated with autism (Table 6).
Table 6.
Correlations Between Girls Questionnaire for Autism Spectrum Condition and Autism Quotient Subscales Between Autistic and Nonautistic Women
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. GQ-ASC total score | — | −0.53** | 0.64** | 0.75** | 0.71** | 0.55** | 0.58** | 0.58** | 0.42** | 0.53** | 0.05 | 0.33** |
| 2. GQ-ASC imagination and play | −0.60** | — | −0.10 | −0.17** | −0.18** | −0.24** | −0.01 | −0.06 | −0.04 | −0.15* | 0.34** | 0.00 |
| 3. GQ-ASC camouflaging | 0.52** | −0.08 | — | 0.47** | 0.44** | 0.18** | 0.41** | 0.44** | 0.31** | 0.36** | 0.12* | 0.14* |
| 4. GQ-ASC sensory sensitivities | 0.59** | −0.24** | 0.25** | — | 0.54** | 0.22** | 0.62** | 0.59** | 0.44** | 0.46** | 0.25** | 0.36** |
| 5. GQ-ASC socializing | 0.49** | −0.16** | 0.19** | 0.18** | — | 0.25** | 0.54** | 0.49** | 0.38** | 0.47** | 0.15** | 0.33** |
| 6. GQ-ASC interests | 0.35** | −0.01 | −0.15** | 0.08 | 0.06 | — | 0.32** | 0.29** | 0.16** | 0.28** | 0.01 | 0.26** |
| 7. AQ total score | 0.05 | 0.29** | 0.09 | 0.22** | −0.06 | 0.13* | — | 0.82** | 0.81** | 0.72** | 0.49** | 0.49** |
| 8. AQ communication | 0.20** | −0.08 | 0.13* | 0.23** | 0.00 | 0.08 | 0.44** | — | 0.65** | 0.51** | 0.30** | 0.23** |
| 9. AQ social skills | 0.01 | 0.04 | 0.04 | 0.18** | −0.13* | −0.04 | 0.61** | 0.23** | — | 0.53** | 0.32** | 0.16** |
| 10. AQ attention switching | 0.10 | −0.03 | 0.06 | 0.18** | 0.07 | −0.02 | 0.33** | 0.02 | 0.26** | — | 0.22** | 0.23** |
| 11. AQ imagination | −0.20** | 0.56** | 0.03 | 0.06 | −0.12* | 0.09 | 0.65** | 0.05 | 0.21** | 0.09 | — | 0.25 |
| 12. AQ attention to detail | 0.12* | 0.05 | −0.03 | 0.03 | 0.11* | 0.18** | 0.51** | 0.07 | 0.13* | −0.10 | 0.09 | — |
Lower diagonal portion of matrix: autistic cases, upper diagonal portion of matrix: nonautistic cases; Spearman's ρ, **p < 0.01, *p < 0.05., shaded cells: significant differences between autistic and nonautistic groups using Fisher's z.
AQ, Autism Quotient.
Cutoff score for total GQ-ASC
We assessed the ability of the GQ-ASC to discriminate between autistic and nonautistic cases by interpreting an ROC curve. The area under the ROC curve was 0.89 (95% confidence interval 0.89–0.92), indicating an excellent level of discrimination (Fig. 2).24
FIG. 2.
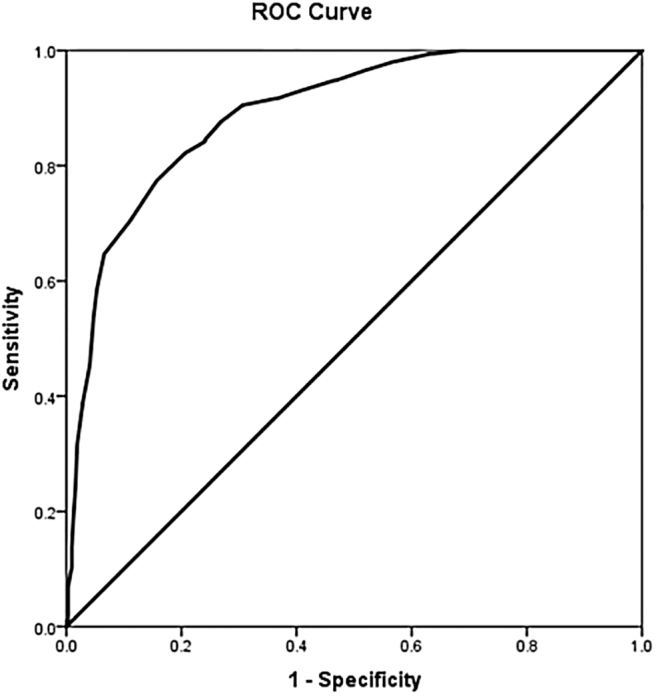
ROC curve for the overall score of the Girls Questionnaire for Autism Spectrum Condition as modified. ROC, receiver operating characteristic.
The results indicate that when applying a cutoff score of 57, the GQ-ASC correctly identified 80.0% of cases (Table 7) and displayed a high level of both sensitivity—the proportion of autistic women who are correctly identified, and specificity—the proportion of nonautistic women who are correctly identified.
Table 7.
Receiver Operating Characteristic Curve Discriminant Ability of the Girls Questionnaire for Autism Spectrum Condition
| Cutoff score | Sensitivity % | Specificity % | Correctly predicteda | False alarm casesa | Missesa | Correct rejectionsa | Odds of an errora |
|---|---|---|---|---|---|---|---|
| >31 | 100.0 | 0.0 | 10.00 | 990.00 | — | — | 99.00 |
| >33 | 100.0 | 0.6 | 10.00 | 984.00 | — | 6.00 | 61.50 |
| >35 | 100.0 | 1.2 | 10.00 | 978.00 | — | 12.00 | 44.45 |
| >37 | 100.0 | 1.9 | 10.00 | 971.00 | — | 19.00 | 33.48 |
| >39 | 100.0 | 2.2 | 10.00 | 968.00 | — | 22.00 | 30.25 |
| >40 | 100.0 | 3.4 | 10.00 | 956.00 | — | 34.00 | 21.73 |
| >41 | 100.0 | 4.7 | 10.00 | 943.00 | — | 47.00 | 16.54 |
| >42 | 100.0 | 5.6 | 10.00 | 935.00 | — | 55.00 | 14.38 |
| >43 | 100.0 | 6.8 | 10.00 | 923.00 | — | 67.00 | 11.99 |
| >44 | 99.7 | 7.8 | 10.00 | 913.00 | — | 77.00 | 10.49 |
| >45 | 99.7 | 9.6 | 10.00 | 895.00 | — | 95.00 | 8.52 |
| >46 | 99.4 | 11.8 | 10.00 | 873.00 | — | 117.00 | 6.87 |
| >47 | 99.4 | 13.0 | 10.00 | 861.00 | — | 129.00 | 6.19 |
| >48 | 99.1 | 14.9 | 10.00 | 842.00 | — | 148.00 | 5.33 |
| >49 | 99.1 | 17.7 | 10.00 | 815.00 | — | 175.00 | 4.41 |
| >50 | 99.1 | 20.5 | 10.00 | 787.00 | — | 203.00 | 3.69 |
| >51 | 98.9 | 23.6 | 10.00 | 756.00 | — | 234.00 | 3.10 |
| >52 | 98.6 | 27.0 | 10.00 | 723.00 | — | 267.00 | 2.61 |
| >53 | 98.0 | 29.5 | 10.00 | 698.00 | — | 292.00 | 2.31 |
| >54 | 97.4 | 33.5 | 10.00 | 658.00 | — | 332.00 | 1.92 |
| >55 | 96.0 | 37.0 | 10.00 | 624.00 | — | 366.00 | 1.66 |
| >56 | 95.1 | 42.2 | 10.00 | 572.00 | — | 418.00 | 1.34 |
| >57 | 94.0 | 46.3 | 9.00 | 532.00 | 1.00 | 458.00 | 1.14 |
| >58 | 92.0 | 50.3 | 9.00 | 492.00 | 1.00 | 498.00 | 0.97 |
| >59 | 91.1 | 52.5 | 9.00 | 470.00 | 1.00 | 520.00 | 0.89 |
| >60 | 88.9 | 56.2 | 9.00 | 434.00 | 1.00 | 556.00 | 0.77 |
| >61 | 87.4 | 58.7 | 9.00 | 409.00 | 1.00 | 581.00 | 0.69 |
| >62 | 82.9 | 61.2 | 8.00 | 384.00 | 2.00 | 606.00 | 0.63 |
| >63 | 79.1 | 66.1 | 8.00 | 336.00 | 2.00 | 654.00 | 0.51 |
| >64 | 76.6 | 69.6 | 8.00 | 301.00 | 2.00 | 689.00 | 0.43 |
| >65 | 71.4 | 73.0 | 7.00 | 267.00 | 3.00 | 723.00 | 0.37 |
| >66 | 67.7 | 76.4 | 7.00 | 234.00 | 3.00 | 756.00 | 0.31 |
| >67 | 64.0 | 80.1 | 6.00 | 197.00 | 4.00 | 793.00 | 0.25 |
| >68 | 60.0 | 84.2 | 6.00 | 156.00 | 4.00 | 834.00 | 0.19 |
| >69 | 56.3 | 86.0 | 6.00 | 139.00 | 4.00 | 851.00 | 0.17 |
| >70 | 50.3 | 89.1 | 5.00 | 108.00 | 5.00 | 882.00 | 0.13 |
| >71 | 44.0 | 91.6 | 4.00 | 83.00 | 6.00 | 907.00 | 0.10 |
| >72 | 35.4 | 94.1 | 4.00 | 58.00 | 6.00 | 932.00 | 0.07 |
| >73 | 30.0 | 96.6 | 3.00 | 34.00 | 7.00 | 956.00 | 0.04 |
| >74 | 24.3 | 96.9 | 2.00 | 31.00 | 8.00 | 959.00 | 0.04 |
| >75 | 18.9 | 98.8 | 2.00 | 12.00 | 8.00 | 978.00 | 0.02 |
| >75 | 15.7 | 99.1 | 2.00 | 9.00 | 8.00 | 981.00 | 0.02 |
| >76 | 15.4 | 99.1 | 2.00 | 9.00 | 8.00 | 981.00 | 0.02 |
| >77 | 13.1 | 99.7 | 1.00 | 3.00 | 9.00 | 987.00 | 0.01 |
| >78 | 10.3 | 99.7 | 1.00 | 3.00 | 9.00 | 987.00 | 0.01 |
| >79 | 8.3 | 99.7 | 1.00 | 3.00 | 9.00 | 987.00 | 0.01 |
| >80 | 5.7 | 99.7 | 1.00 | 3.00 | 9.00 | 987.00 | 0.01 |
| >80 | 3.7 | 99.7 | — | 3.00 | 10.00 | 987.00 | 0.01 |
| >81 | 3.4 | 99.7 | — | 3.00 | 10.00 | 987.00 | 0.01 |
| >82 | 2.6 | 100.0 | — | — | 10.00 | 990.00 | 0.01 |
| >83 | 1.4 | 100.0 | — | — | 10.00 | 990.00 | 0.01 |
| >84 | 0.0 | 100.0 | — | — | 10.00 | 990.00 | 0.01 |
Correctly predicted and false alarms from 1000 presentations assuming 1.0% of all cases have autism.
Discussion
This study aimed to explore the structure of the GQ-ASC to establish its most salient features as they apply to adult cisgender and trans autistic women. It also aimed to examine differences in responding between autistic and nonautistic women on the extracted components of the GQ-ASC, and to identify the most appropriate cutoff score for differentiating between autistic and nonautistic cases. The resulting reduced item structure aligned well with current understandings of how autistic women display their autistic traits. It demonstrated moderately low, to approaching-adequate levels of internal consistency within each extracted component; a high degree of sensitivity, as it produced significantly different outcomes between autistic and nonautistic respondents across all extracted components; and a very robust capacity to discriminate between autistic and nonautistic women.
The GQ-ASC was originally developed as a parental report for younger girls or as a self-report screening measure for older girls and teens. It includes four subscales: Play (between 5 and 12 years old), Friendships and Social Situations, Abilities and Interests, and Sensory Profile. These key constructs are transposed well onto the components extracted through the present analysis, although with some notable differences and extensions of the original themes that may be accounted for by the adult age of this cohort.
GQ-ASC extracted components
Imagination and play
The five items in this component relate to an interest in fiction and fantasy worlds, and the individuals' perspective on the quality and content of their imaginary play when compared with their nonautistic peers in childhood. All five items displayed high component loading values, and with the exception of item number six (When I was 5–12 years old, I created my own complex ‘set ups’ with toys), each recorded relatively high communalities. We examined the internal consistency of this component with item number six excluded, and found it was not improved. Reduced or delayed imaginative play is consistently documented in autistic children,25,26 although what is noteworthy about these findings is the self-awareness of autistic women when rating the quality of their imaginative play in relation to nonautistic peers, which is perhaps unique to the older age of this cohort. We found imagination and play to be negatively correlated with camouflaging (Table 6), which perhaps reflects a refined ability to observe the imaginative play of others throughout childhood, and reflect on the quality and content of one's own. This is an area that warrants further investigation.
Camouflaging
We identified four items in this component, each relating to the active process of developing and displaying strategies that minimize the impact of social challenges.8 Each item reported high component loading values, and high communalities, with this component recording the highest degree of internal consistency (ω = 0.67). This aligns well with the report that over 90% of autistic women have attempted to camouflage their autism.9 The nature of social interactions are inherently more complex in adult years than in childhood, with demands that may otherwise fall on parents or carers and the buffer that presents no longer being an option for many. As such, it is expected that the demand for camouflaging behaviors increases as women find themselves in various settings (e.g., education, workplace, and varying degrees of intimate relationships).
Sensory sensitivities
We included four items in this component, most of which describe either hypo- or hypersensitivity to various sensory processing modalities. Item number 24 (Some social situations make me mute) does not appear to be reflective of the same latent construct, although it may be that sensory overload due to social situations impairs the individuals' ability to process and respond to information, that leads to shut down (feeling situationally mute) or meltdown. Sensory processing hyper- and hyposensitivities are considerably more common in autistic individuals than in nonautistic individuals,27 and reported to be more prominent in autistic girls than boys.28 The autistic experience of the sensory world is complex, as it is often described as a source of pain and distress, and also as a source of pleasure and safety.29 This paradoxical relationship is reflected in the retained items that describe both sensory overload and the soothing quality sensory input can have. Autistic women displayed significantly more sensory sensitivities than nonautistic women in the present study, with the effect size being greater than 1.6 standard deviations (Table 5).
Socializing
This component contained four items, each relating to challenges experienced in social interactions. The items all recorded high component loading values, and communalities, with no notable changes to internal consistency with the exclusion of any individual item. Difficulties in social skills are a core feature of autism,30 and are shared across both male and female autistic presentations. These questions appear to explain adult autistic social challenges well, although they may not accurately reflect the experiences of autistic women with higher support needs, or a co-occurring intellectual disability, as they describe a high degree of insight and active responding to social missteps.
Interests
Two of the four items of this component discuss gendered childhood interests, with the third eliciting information about age-typical interests in childhood. It has been reported that many autistic girls do not show a strong preference for female-typical toys,31,32 and that autistic women frequently identified as “tomboys” in childhood.33 Item number 32 (I am talented in music) appears to be qualitatively different from the other items in this component, with internal consistency improving for the component overall if this item is removed. It is likely that this question relates more specifically to the experiences of children, and that unique talents may be explored in a more adult-centric way through further item development exploring interests and abilities in arts, languages, sport, and studying psychology.
Utility of the GQ-ASC and AQ as screening measures
In exploring the relationship between the GQ-ASC and AQ, we found a number of significant relationships and differences between the scales. Some subscales that would appear to be measuring similar constructs showed moderately strong correlations, such as “GQ-ASC Imagination and Play” and “AQ Imagination,” while others displayed a negative relationship (“GQ-ASC Socializing” and “AQ Social skills”) or no relationship at all (“GQ-ASC Socializing” and “AQ Communication”). These results suggest that while both scales measure features of autistic presentation, they appear to be measuring different constructs associated with autism. This may be attributable to differential trait presentation between men and women, or gendered understandings of autism inherent in the development of each scale, or both. This is an area that requires future research with carefully controlled groups, although the results of the ROC indicate that the modified format of GQ-ASC presented here is highly valuable in identifying autistic women.
Strengths and limitations
This study benefited from a large sample size that enabled us to robustly detect small effects, although we acknowledge the impact of several limitations. The mode of data collection (online, self-report) presents a barrier to our ability to understand autistic trait presentation beyond what is self-reported and measured by the AQ. In addition, as previously discussed, the AQ itself is known to have inherent sensitivity issues when measuring the autistic traits of women.18 This may be compounded by our decision to include cisgender and trans autistic women, and warrants further investigation with both participants who are discreetly classified as either cisgender or trans women, and with a clinical cohort whose autistic traits can be assessed using gold standard tools.
Our recruitment strategy may challenge the interpretability of our findings in a number of ways. Namely, in an effort to be reflective of the high number of trans and gender-diverse autistic people in the community,33 we opened this study to cisgender and trans women, excluding only cisgender men. However, it is currently unclear whether autistic presentation differs between cisgender women and gender-diverse people. This is an important area for future investigation as we work toward understanding the nuanced differences within autistic presentations. Similarly, our convenience sampling from multiple countries and a very broad age range does not allow us to understand any cultural or age-based differences between participants, and their ability to access diagnostic services or supports. Finally, we did not collect any information about the presence or absence of co-occurring intellectual disability, which presents a challenge to the generalizability of the findings. It is currently unclear whether autistic women with a co-occurring intellectual disability share the same autistic presentation, as measured by the GQ-ASC, as those without a co-occurring intellectual disability. This is an area that will be important to consider in future research.
Finally, the ROC curve assessing the total score of the GQ-ASC and stated cutoff value must be interpreted with caution. While there is currently a lack of evidence of higher order unidimensionality within the GQ-ASC, we encourage future research to evaluate the plausibility of this hypothesis.
Clinical implications
A succinct and effective screening measure that accurately captures the presentation of autistic adult women has the capacity to drastically change referral pathways. In much the same way as the short-form AQ34 and Quantitative Checklist for Autism in Toddlers35 are reported to act as rapid screeners that guide assessment referral,36 the GQ-ASC may also be of use to practitioners. It is proposed that the use of GQ-ASC as a screening tool would be particularly pertinent for women who present with mental health conditions such as anxiety, depression, or eating disorders, given their high rates of co-occurrance.36–39
In lieu of a formal autism assessment, this screening measure may also be of benefit to undiagnosed autistic women. For many who do not feel disabled by their autistic status or do not feel it necessary to have their experiences legitimized by the medical model of disability, access to a brief and cost-effective screening tool can be empowering for autistic women who wish to define and claim their own autistic identity.11,12
Conclusion and Future Directions
This investigation presents the GQ-ASC as an effective and highly discriminant screening tool for use in adult autistic women. It provides valuable insight into the shared features and experiences of this underrecognized and underrepresented subset of the autistic community, and may serve to empower undiagnosed women to pursue formal assessment or define their own autistic identity. Further research and refinement of this tool are necessary to capture other meaningful and nuanced components of autistic women's presentation. This will be particularly important in a clinical cohort, with clear understanding of the impact of co-occurring intellectual disability and more varied sex and gender presentations.
Appendix
Appendix Table A1.
Modified Girls Questionnaire for Autism Spectrum Condition Scale
| Modified GQ-ASC | Definitely disagree | Slightly disagree | Slightly agree | Definitely agree |
|---|---|---|---|---|
| Imagination and play | ||||
| 1. (R) I enjoy fantasy worlds | 1 | 2 | 3 | 4 |
| 2. (R) I am interested in fiction | 1 | 2 | 3 | 4 |
| 3. (R) When I was 5 –12 years old, I played as imaginatively as other girls | 1 | 2 | 3 | 4 |
| 4. (R) When I was 5–12 years old, I had imaginary friends or imaginary animals | 1 | 2 | 3 | 4 |
| 5. (R) When I was 5–12 years old, I created my own complex “setups” with toys | 1 | 2 | 3 | 4 |
| Camouflaging | ||||
| 6. I copy or “clone” myself on other females | 1 | 2 | 3 | 4 |
| 7. I avidly observe other females socializing | 1 | 2 | 3 | 4 |
| 8. I am attracted to females with strong personalities who tell me what to do | 1 | 2 | 3 | 4 |
| 9. I adopt a different persona in different situations | 1 | 2 | 3 | 4 |
| Sensory sensitivities | ||||
| 10. I am attached to certain objects or toys (e.g., favorite toy, pillow, piece of cloth) which I carry, touch, or rub to calm myself | 1 | 2 | 3 | 4 |
| 11. I expressed distress during grooming (e.g., I fought or cried during fingernail cutting, haircutting, combing) or when I am touched (e.g., someone touches my feet) | 1 | 2 | 3 | 4 |
| 12. Some social situations make me mute | 1 | 2 | 3 | 4 |
| 13. I am distressed by certain smells or I avoid certain tastes that are a typical part of a diet | 1 | 2 | 3 | 4 |
| Socializing | ||||
| 14. I socialize quite well for a while, but subsequently feel exhausted | 1 | 2 | 3 | 4 |
| 15. I often have a facial “mask” that hides my social confusion | 1 | 2 | 3 | 4 |
| 16. I have intense emotions | 1 | 2 | 3 | 4 |
| 17. I apologize when I make a social error | 1 | 2 | 3 | 4 |
| Interests | ||||
| 18. (R) When I was 5–12 years old, I preferred to play with girls' toys | 1 | 2 | 3 | 4 |
| 19. When I was 5–12 years old, I preferred to play with boys' toys | 1 | 2 | 3 | 4 |
| 20. My interests were advanced for my age (e.g., opera) | 1 | 2 | 3 | 4 |
| 21. I am talented in music | 1 | 2 | 3 | 4 |
Items 1,2,3,4,5,18 to be reverse scored. A total score of >56 sensitive to 80% of cases.
GQ-ASC, Girls Questionnaire for Autism Spectrum Condition.
Authorship Confirmation Statement
C.M.B. conducted statistical analyses, interpreted findings, and reported results. M.A.S. provided supervision and guidance for all components of analysis, interpretation of findings, and reporting of results. T.A. and M.G. provided guidance and input on the interpretation and reporting of results. All coauthors have reviewed and approved this article before its submission. We confirm that this article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this research.
References
- 1. Loomes R, Hull L, Mandy WPL. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(6):466–474. [DOI] [PubMed] [Google Scholar]
- 2. Rutherford M, McKenzie K, Johnson T, et al. Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism. 2016;20(5):628–634. [DOI] [PubMed] [Google Scholar]
- 3. Duvekot J, van der Ende J, Verhulst FC, et al. Factors influencing the probability of a diagnosis of autism spectrum disorder in girls versus boys. Autism. 2017;21(6):646–658. [DOI] [PubMed] [Google Scholar]
- 4. Young H, Oreve MJ, Speranza M. Clinical characteristics and problems diagnosing autism spectrum disorder in girls. Arch Pédiatr. 2018;25(6):399–403. [DOI] [PubMed] [Google Scholar]
- 5. Halladay AK, Bishop S, Constantino JN, et al. Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Mol Autism. 2015;6(1):36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lai MC, Lombardo MV, Auyeung B, Chakrabarti B, Baron-Cohen S. Sex/gender differences and autism: Setting the scene for future research. J Am Acad Child Adolesc Psychiatry. 2015;54(1):11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Dworzynski K, Ronald A, Bolton P, Happé F. How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders?. J Am Acad Child Adolesc Psychiatry. 2012;51(8):788–797. [DOI] [PubMed] [Google Scholar]
- 8. Lai MC, Lombardo MV, Ruigrok AN, et al. Quantifying and exploring camouflaging in men and women with autism. Autism. 2017;21(6):690–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Mol Autism. 2018;9(1):42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Fombonne E. The changing epidemiology of autism. J Appl Res Intellect Disabil. 2005;18(4):281–294. [Google Scholar]
- 11. Lai MC, Baron-Cohen S. Identifying the lost generation of adults with autism spectrum conditions. Lancet Psychiatry. 2015;2(11):1013–1027. [DOI] [PubMed] [Google Scholar]
- 12. Kapp SK, Gillespie-Lynch K, Sherman LE, Hutman T. Deficit, difference, or both? Autism and neurodiversity. Dev Psychol. 2013;49(1):59. [DOI] [PubMed] [Google Scholar]
- 13. Brownlow C, O'Dell L. Constructing an autistic identity: AS voices online. Ment Retard. 2006;44(5):315–321. [DOI] [PubMed] [Google Scholar]
- 14. Ormond S, Brownlow C, Garnett MS, Rynkiewicz, A, Attwood, T. (2018). Profiling autism symptomatology: An exploration of the Q-ASC parental report scale in capturing sex differences in autism. J Autism Dev Disord. 48(2):389–403. [DOI] [PubMed] [Google Scholar]
- 15. Webster AA, Garvis S. The importance of critical life moments: An explorative study of successful women with autism spectrum disorder. Autism. 2017;21(6):670–677. [DOI] [PubMed] [Google Scholar]
- 16. Bargiela S, Steward R, Mandy W. The experiences of late-diagnosed women with autism spectrum conditions: An investigation of the female autism phenotype. J Autism Dev Disord. 2016;46(10):3281–3294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, malesand females, scientists and mathematicians. J Autism Dev Disord. 2001;31(1):5–17. [DOI] [PubMed] [Google Scholar]
- 18. Broadbent J, Galic I, Stokes MA. Validation of autism spectrum quotient adult version in an Australian sample. Autism Res Treat. 2013; DOI: 10.1155/2013/984205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Baron-Cohen S, Cassidy S, Auyeung B, et al. Attenuation of typical sex differences in 800 adults with autism vs. 3,900 controls. PLoS One. 2014;9(7):e102251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Cattell RB. The screen test for the number of factors. Multivar Behav Res. 1966;1(2):245–276. [DOI] [PubMed] [Google Scholar]
- 21. Thurstone LL. Multiple Factor Analysis. Chicago, IL: University of Chicago Press; 1947. [Google Scholar]
- 22. O'Connor BP. SPSS and SAS programs for determining the number of components using parallel analysis and Velicer's MAP test. Behav Res Methods Instrum Comput. 2000;32:396–402. [DOI] [PubMed] [Google Scholar]
- 23. Howell DC. Statistical Methods for Psychology, 8th ed.. Belmont, CA: Wadsworth; 2013. [Google Scholar]
- 24. Hosmer DW Jr, Lemeshow S, Sturdivant RX. Applied Logistic Regression, Vol. 398. NY, NY: John Wiley & Sons; 2013. [Google Scholar]
- 25. Wing L, Gould J. Severe impairments of social interaction and associated abnormalities in children: Epidemiology and classification. J Autism Dev Disord. 1979;9(1):11–29. [DOI] [PubMed] [Google Scholar]
- 26. Wolfberg P, Bottema-Beutel K, DeWitt M. Including children with autism in social and imaginary play with typical peers: Integrated play groups model. Am J Play. 2012;5(1):55–80. [Google Scholar]
- 27. Tomchek SD, Dunn W. Sensory processing in children with and without autism: A comparative study using the short sensory profile. Am J Occup Ther. 2007;61(2):190–200. [DOI] [PubMed] [Google Scholar]
- 28. Ormond S, Brownlow C, Garnett MS, Rynkiewicz A, Attwood T. Profiling autism symptomatology: An exploration of the Q-ASC parental report scale in capturing sex differences in autism. J Autism Dev Disord. 2018;48(2):389–403. [DOI] [PubMed] [Google Scholar]
- 29. O'Neill M, Jones RS. Sensory-perceptual abnormalities in autism: A case for more research? J Autism Dev Disord. 1997;27(3):283–293. [DOI] [PubMed] [Google Scholar]
- 30. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Arlington, VA: American Psychiatric Pub; 2013. [Google Scholar]
- 31. Knickmeyer RC, Wheelwright S, Baron-Cohen SB. Sex-typical play: Masculinization/defeminization in girls with an autism spectrum condition. J Autism Dev Disord. 2008;38(6):1028–1035. [DOI] [PubMed] [Google Scholar]
- 32. Harrop C, Green J, Hudry K, PACT Consortium. Play complexity and toy engagement in preschoolers with autism spectrum disorder: Do girls and boys differ? Autism. 2017;21(1):37–50. [DOI] [PubMed] [Google Scholar]
- 33. Dewinter J, De Graaf H, Begeer S. Sexual orientation, gender identity, and romantic relationships in adolescents and adults with autism spectrum disorder. J Autism Dev Disord. 2017;47(9):2927–2934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Ingudomnukul E, Baron-Cohen S, Wheelwright S, Knickmeyer R. Elevated rates of testosterone-related disorders in women with autism spectrum conditions. Horm Behav. 2007;51(5):597–604. [DOI] [PubMed] [Google Scholar]
- 35. Allison C, Auyeung B, Baron-Cohen S. Toward brief “red flags” for autism screening: The short autism spectrum quotient and the short quantitative checklist in 1,000 cases and 3,000 controls. J Am Acad Child Adolesc Psychiatry. 2012;51(2):202–212. [DOI] [PubMed] [Google Scholar]
- 36. Allison C, Baron-Cohen S, Wheelwright S, et al. The Q-CHAT (Quantitative CHecklist for Autism in Toddlers): A normally distributed quantitative measure of autistic traits at 18–24 months of age: Preliminary report. J Autism Dev Disord. 2008;38(8):1414–1425. [DOI] [PubMed] [Google Scholar]
- 37. Tint A, Weiss JA, Lunsky Y. Identifying the clinical needs and patterns of health service use of adolescent girls and women with autism spectrum disorder. Autism Res. 2017;10(9):1558–1566. [DOI] [PubMed] [Google Scholar]
- 38. Mandy W, Chilvers R, Chowdhury U, et al. Sex differences in autism spectrum disorder: Evidence from a large sample of children and adolescents. J Autism Dev Disord. 2012;42(7):1304–1313. [DOI] [PubMed] [Google Scholar]
- 39. Huke V, Turk J, Saeidi S, Kent A, Morgan JF. Autism spectrum disorders in eating disorder populations: A systematic review. Eur Eating Disord Rev. 2013;21(5):345–351. [DOI] [PubMed] [Google Scholar]