

Abstract
Objectives
While there have been some studies examining the post-traumatic growth (PTG) responses to the COVID-19 pandemic, few have been longitudinal studies exploring the changes over time or examining the underlying psychological PTG mechanisms. This study examined whether baseline perceived emotional intelligence (EI) predicted PTG through self-esteem and emotional regulation (ER) in a five-month follow-up study conducted on Chinese adolescents during the COVID-19 pandemic.
Methods
Validated measures were completed by 2090 participants, which assessed both the perceived EI and the PTG 1 month after a nationwide lockdown in China, with 1609 of these participating in the follow-up five months later. Structural equation models (SEM) were then used to explore the paths between the variables.
Results
As hypothesized, the follow-up survey found that the baseline perceived EI predicted PTG, ER, and self-esteem outcomes. The SEM analyses also revealed that self-esteem and ER significantly mediated the association between EI and PTG.
Limitations
Studies of three or more waves may be more suitable for longitudinal mediation analyses. Self-assessment reports may have subjective effects.
Conclusions
It was concluded that perceived EI might improve PTG in adolescents following the COVID-19 pandemic, and self-esteem and ER program training could be helpful in promoting PTG.
Keywords: PTG, Self-esteem, Emotional intelligence, Emotional regulation, COVID-19
1. Introduction
A few months after COVID-19 was first confirmed in Wuhan, China, in late 2019, it became a global pandemic, which increased the risk of mental health problems (Bourmistrova et al., 2022; Oosterhoff et al., 2020; Singh et al., 2020). For example, a recent review found that cases of anxiety, depression, and similar psychological issues began to appear in the general populations in eight countries (Xiong et al., 2020). Although the COVID-19 pandemic has been traumatogenic, posttraumatic growth (PTG) may also occur in general populations (Vazquez et al., 2021).
PTG was first proposed by Calhoun & Tedeschi, who defined it as the positive psychological change experienced from a struggle with challenging or traumatic life circumstances (Calhoun and Tedeschi, 1999). PTG has been found in many people who have faced traumatic circumstances, such as terror attacks (Eze et al., 2020), hurricanes (Shigemoto, 2021), and severe acute respiratory syndrome (SARS) (Cheng et al., 2006), with most being found to have experienced significant positive life changes. However, as most COVID-19 studies have tended to focus on the adverse psychological effects (Li et al., 2021; Magson et al., 2021), very few studies have comprehensively examined PTG (Hamam et al., 2021; Vazquez et al., 2021; Zhen and Zhou, 2022). Therefore, it is meaningful to explore the emergence of the PTG resulting from the impact of COVID-19 to explore the redefinition of people's lives, the positive changes in their relationships and personal strength, and their spiritual transformations.
The general model proposed by Tedeschi and Calhoun included several variables that could play a primary role in PTG (Tedeschi and Calhoun, 2004): positive personal characteristics, such as optimism, extraversion, openness to experience, and other factors; and individual social systems, such as the ability to cognitively process and manage the distressing emotions induced by challenging traumatic events. In this general model, certain pre-trauma personal characteristics were surmised to promote PTG when a person is confronted with challenging stressors. Emotional intelligence (EI), which is the ability to perceive and understand one's own and others' emotions, manage and direct one's own actions and thoughts (Davies, 2004; Salovey and Mayer, 1990), and positively refocus on planning a response to trauma, may predispose a person to PTG after trauma (Tuck and Patlamazoglou, 2019). As the EI examined in the current study was mainly based on a self-assessment survey, the term ‘perceived EI’ is used to distinguish it from the EI measured using performance-based tests. However, there have been few studies on the links between perceived EI and PTG in adolescents during the COVID-19 pandemic. Therefore, to go some way to filling this research gap, this longitudinal study explored the contribution of EI to PTG in adolescents and the underlying mechanism during the COIVD-19 pandemic.
1.1. Relationship between perceived EI and PTG
As previous research has found that perceived EI can decrease the effects of traumatic stress (Brackett et al., 2011), the relationship between perceived EI and PTG in the COVID-19 context is worth exploring. Individuals with high perceived EI are also thought to be better able to cope with stress and external environmental challenges, changes, and demands (Salovey et al., 2008).
Perceived EI has been found to be positively correlated with PTG in undergraduates experiencing adversity (Thomas et al., 2020), the results of which suggested that perceived EI could increase a person's ability to cope with traumatic stressors, manage emotional information, and experience personal growth. However, no studies have yet investigated this relationship in the COVID-19 pandemic context, and most studies on the relationship between perceived EI and PTG have been cross-sectional. Therefore, longitudinal studies on EI and PTG are needed to better determine the nature of this relationship.
1.2. Self-esteem as a potential mediator between EI and PTG
Self-esteem, which has been defined as a person's overall sense of worth (Rosenberg, 1965), has most commonly been measured using the Rosenberg Self-Esteem Scale (Robins et al., 2001; Rosenberg, 1979). Several empirical studies concluded that perceived EI was a strong determinant of high self-esteem (Pérez-Fuentes et al., 2019). For instance, Cheung et al. (2015) found that perceived EI could improve self-esteem through the positive effect of social competence in young adults. Perceived EI has also been found to contribute to self-esteem and self-pride (Mayer et al., 2000). Therefore, it is possible that perceived EI can predict self-esteem in adolescents who experienced the COVID-19 pandemic.
As PTG is related to positive psychological change (Calhoun and Tedeschi, 2006), it is also possible that self-esteem could be a PTG predictor. Self-esteem has been found to be a buffer and a protective factor against negative traumatic experiences (Walter et al., 2010). For example, Taku and McDiarmid (2015) found that self-esteem was a predictor for PTG in adolescents experiencing stressful life events. Therefore, taken together, these findings suggest that after a traumatic event, there may be a possible link between self-esteem and PTG.
1.3. Emotional regulation as a potential mediator between EI and PTG
The Gross ER process model (Gross, 1998; Peña-Sarrionandia et al., 2015) defines people with high perceived EI as good at shaping their emotions and having many emotional coping strategies. Therefore, perceived EI could predict ER in adolescents facing COVID-19 isolation.
As outlined, ER has also been found to play an essential role in PTG. For example, Foa et al. (2006) found that trauma recovery activated the emotional processing to avoid facing the trauma effects, Gross (2002) found that people who employed ER strategies changed their interpretation of the traumatic event by shifting their focus from negative to positive aspects, which in turn promoted PTG, and Thomas et al. (2020) found that ER was positively correlated with EI and PTG in a cross-sectional study. Therefore, these studies suggested that EI through ER could be the mechanism that facilitates PTG from the COVID-19 pandemic. Another proposed theoretical model with self-esteem as the central self-regulation aspect (Crocker et al., 2006; Rhodewalt and Tragakis, 2003) also suggested that ER could mediate self-esteem and PTG.
1.4. Present study
Recent research has indicated that PTG could develop from COVID-19 pandemic experiences (Pietrzak et al., 2021; Vazquez et al., 2021); however, there have been few studies on the possible COVID-19 PTG in adolescents, and no long-term longitudinal COVID-19 studies on the effects of EI on PTG. Although previous studies have shown that the PTG rate can fluctuate over time (Dekel et al., 2012), there have been few longitudinal studies conducted on the COVID-19 induced PTG changes over time in adolescents. This study, therefore, hypothesized that this PTG rate increased over time as the greater the perceived stress and the greater the need for re-evaluation during COVID-19 could be related to greater perceived growth (Danhauer et al., 2013; Feingold et al., 2022; Pietrzak et al., 2021).
This study assessed adolescent PTG in two waves during China's COVID-19 pandemic period using a mediation model constructed based on the general PTG model (Tedeschi and Calhoun, 2004) (see Fig. 1 ) to explore the relationships between perceived EI, ER, self-esteem, and PTG.
Fig. 1.
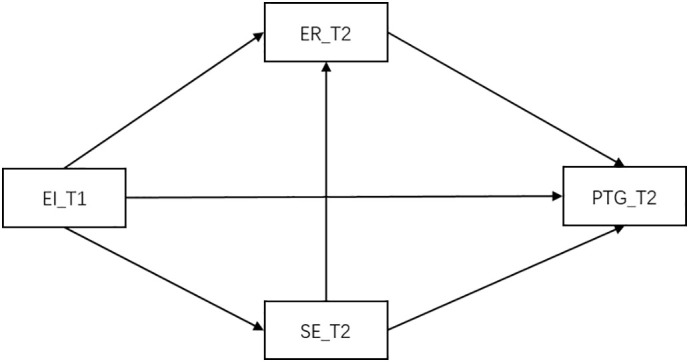
Longitudinal hypothesis mediation model framework
Abbreviations: T1 = Time 1 (baseline); T2 = Time 2 (follow-up); ER, emotional regulation; SE, self-esteem; PTG, posttraumatic growth; EI, emotional intelligence.
Based on the previous discussion, the following hypotheses were proposed.
Hypothesis 1
Between the two assessment periods (the baseline and follow-up), the adolescent PTG would increase.
Hypothesis 2
A perceived EI presence in the early lockdown stage would predict ER, self-esteem, and PTG after five months.
Hypothesis 3
ER and self-esteem play a mediating role in the relationship between perceived EI and PTG.
Hypothesis 4
ER plays a mediating role in the relationship between self-esteem and PTG.
2. Methods
2.1. Study design and settings
The adolescent samples were recruited from two senior high schools in Leshan and Jianyang counties, Sichuan Province, China. To investigate the predictive effects of EI on PTG, self-esteem, and ER and to explore the mechanism underlying these relationships to determine the PTG variations from exposure to the lengthy COVID-19 challenge, this study comprised a two-wave five-month prospective survey, with participants chosen using convenience sampling.
2.2. Sample
The baseline survey was completed by 2090 participants of the original 2399 recruited participants, with a response rate of 87.1%. Of these 2090 initial participants, 1609 (76.9%) completed both surveys, and of these 1609 participants, 1021 were female (63.5%), and the mean age was 16.54 years (SD, 0.98; range, 12–18 years).
2.3. Instruments and measures
2.3.1. Socio-demographics and exposure variables
At the baseline, participants provided information on their age, gender, grade, only child status, and COVID-19 exposure factors, such as “whether people in their community had been infected, whether family and friends had been infected, and whether family or friends had died from the infection,” with the binary responses being either “yes” or “no”.
2.3.2. Wong law emotional intelligence scale (WLEIS)
At the baseline, participants completed the 16-item Chinese language version of the Wong Law Emotional Intelligence Scale (WLEIS) (Wong and Law, 2002). All items had 5-point Likert scale response options From 1 = Strongly disagree to 5 = Strongly agree. The scale consists of four subscales: regulation of emotion, self-emotion appraisal, others' emotion appraisal, and use of emotion. The total WLEIS score ranges from 16 to 80, with higher scores indicating higher perceived EI levels. Although the perceived EI as measured by the WLEIS has been criticized because it is based on a self-report measurement, robust evidence has shown invariances between the self-rating in this questionnaire and other ratings (Libbrecht et al., 2010). Despite being conceived within a Chinese cultural framework, the WLEIS is considered a reliable tool for measuring emotional intelligence, has shown good reliability and validity across many cultures (Extremera Pacheco et al., 2019; Iliceto and Fino, 2017; LaPalme et al., 2016; Park and Yu, 2021) and good reliability and validity in Chinese youth (Kong, 2017; Shi and Wang, 2007). The Cronbach's α in the current study was 0.967.
2.3.3. Posttraumatic growth inventory(PTGI)
The participants completed the PTGI (Tedeschi and Calhoun, 1996), which has been found to be reliable and valid in Chinese adolescent samples (Gao et al., 2010; Tang et al., 2021), at the baseline and the five-month follow-up. PTGI consists of five subscales, including relating to others (RTO), new possibilities (NP), personal strength (PS), appreciation of life (AOL), and spiritual change (SC). The PTGI items are responded to on a 6-point Likert scale from 0 = no change to 5 = complete change, with the cut-off value being 61; that is, a score higher than 61 indicates significant PTG (moderate or high growth) (Rodríguez-Rey et al., 2017). At Time 1 (T1), the PTG was measured based on the previous month, and at Time 2 (T2), the PTG was measured based on the last five months between T1 and T2. The internal scale consistency was excellent, with the Cronbach's α at T1 = 0.968 and at T2 = 0.972.
2.3.4. Rosenberg self-esteem scale (RSES)
In the five-month follow-up survey, the participants also completed the 10-item Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1986) to assess their global self-esteem, each item for which was rated on a 4-point scale from 1 = strongly disagree to 4 = strongly agree. The total scores ranged from 10 to 40, with higher scores indicating higher self-esteem. The RSES has been found to have good reliability and validity in Chinese adolescent samples (Chen et al., 2017), with the RSES Cronbach's α in this study being 0.818.
2.3.5. Emotion regulation scale
In the five-month follow-up survey, the ER was measured using a revised Chinese version of the Emotion Regulation Scale (Gross and John, 2003; Li et al., 2007), which comprises ten items, each of which is rated on a 7-point Likert scale ranging from 1 = strongly disagree to 7 = strongly agree. The scale comprises cognitive reappraisal and emotional suppression subscales, with cognitive reappraisal having six items and emotional suppression four items. In this study, this scale had strong internal consistency for the cognitive reappraisal subscale (Cronbach's α = 0.943), the emotional suppression subscale (Cronbach's α = 0.871), and the total scale (Cronbach's α = 0.934).
2.4. Procedure
After the institution's ethics committee approved the study, the local education board, and the school administrations, as well as consent from the parents, online survey links were then pushed to the parents using an established WeChat group along with the questionnaire completion instructions. The survey was completed by the students, who were free to choose whether to answer the questionnaire or not. They were also told that they could leave at any time. Phone and email contacts were also given so that the participants and parents could contact the researchers if they had any questions.
China was in a nationwide COVID-19 lockdown from January 21 to April 11. Therefore, the baseline survey (T1) was conducted between February 24 and February 28, 2020, and the follow-up survey (T2) was conducted between July 11 and July 23, 2020, which was after the students had returned to school on April 1st and before the summer holidays start on July 25th.
2.5. Data analysis
Of the initial 2090 participants, 1609 adolescents completed the follow-up assessment at T2, and there were no missing data as all options were mandatory. A chi-square test or t-test was used to compare the differences in the baseline variables between the participants who had completed both surveys and those who had not.
A chi-square test was used for the PTG comparison of the demographic and pandemic exposure variables; a paired t-test was conducted to assess the PTG variance between the two assessment periods; Pearson's correlation analysis was conducted to examine the relationships between the main variables.
Confirmatory Factor Analyses (CFAs) were used to assess the psychometric properties of the EI. ER and PTG scales. More specifically, for each scale, we explored the fit of models to evaluate factor structure by its subscales. Then, structural equation modeling (SEM) was used to verify the path hypotheses. A range of indicators was used to assess the model fit; the chi-square test, the comparative fit index (CFI), the Tucker-Lewis index (TLI), the Goodness of Fit Index (GFI), the standardized root mean squared residual (SRMR), and the root mean square error of approximation (RMSEA). The CFI, GFI, and TLI were all greater than 0.90, the SRMR<0.060, and the RMSEA was less than 0.08, which indicated a good model fit. AMOS 23.0 was then employed to test the hypothesized model.
2.6. Ethical issues
This study was approved by the Sichuan University Ethics Committee and was in accordance with the Helsinki declaration. Permission was also obtained from the local education department and the respective school administrations, after which the parents and the student participants gave authorization and informed consent. To ensure that the participant data from the two waves were matched, the last four digits of the parents' mobile phone numbers and the students' IDs were required as part of the survey completion. All data are encrypted and kept by the appointed researcher of this project. Nobody is allowed to disclose students' personal information to other people or mass media unless requested by a parent or a guardian. All procedures comply with the requirements of the Mental Health Law of China and the Law of the Protection of Juveniles of China.
3. Results
The baseline study sample characteristics are shown in Table 1 . As hypothesized, there was a slight increase in the PTG, which was 22.4% (n = 361) at the baseline and 25.0% (n = 402) at the follow-up. While significant differences were found between the PTG rates for the male and female participants (T1, 29.9% vs. 18.1%; T2, 30.4% vs. 21.8%), no differences were found for the COVID-19 related and the other variables. The paired t-test indicated that the PTG had significantly increased at the follow-up compared to the baseline (42.38 ± 26.06 vs. 39.46 ± 26.71, t = 5.85, p < 0.001).
Table 1.
f PTG_T1 and PTG_T2 prevalence stratified by the demographic and exposure variables (N = 1609).
| Variables | PTG_T1 (n) |
Prevalence (%) |
χ2 | PTG_T2 (n) |
Prevalence (%) |
χ2 |
|---|---|---|---|---|---|---|
| Total | (n = 361) | 22.4 | (n = 402) | 25.0 | ||
| Gender | 29.92⁎⁎⁎ | 14.73⁎⁎⁎ | ||||
| Male(n = 588) | 176 | 29.9 | 179 | 30.4 | ||
| Female(n = 1021) | 185 | 18.1 | 223 | 21.8 | ||
| Age(yr) | 3.33⁎ | 6.05⁎⁎ | ||||
| ≤15(n = 243) | 51 | 21.0 | 53 | 27.6 | ||
| 16(n = 526) | 128 | 24.3 | 144 | 32.2 | ||
| 17(n = 552) | 127 | 23.0 | 145 | 34.1 | ||
| 18(n = 288) | 55 | 19.1 | 60 | 25.8 | ||
| Grade | 5.23 | 4.17 | ||||
| 10(n = 485) | 101 | 20.8 | 120 | 24.7 | ||
| 11(n = 692) | 174 | 25.1 | 188 | 27.2 | ||
| 12(n = 432) | 86 | 19.9 | 94 | 21.8 | ||
| Only-child status | 0.08 | 0.44 | ||||
| Yes(n = 397) | 87 | 21.9 | 105 | 26.4 | ||
| No(n = 1212) | 274 | 22.6 | 297 | 24.5 | ||
| Someone in the community is infected | 0.87 | 0.99 | ||||
| Yes(n = 92) | 20 | 21.7 | 23 | 25.0 | ||
| No(n = 1517) | 341 | 22.5 | 379 | 25.0 | ||
| A relative or friend is infected | 0.54 | 0.63 | ||||
| Yes(n = 13) | 2 | 15.4 | 4 | 30.9 | ||
| No(n = 1596) | 359 | 22.5 | 398 | 24.9 | ||
| A relative or friend died from the infection | 0.35 | 0.74 | ||||
| Yes(n = 3) | 0 | 0 | 1 | 33.3 | ||
| No(n = 1606) | 361 | 22.5 | 401 | 25.0 |
Abbreviations: PTG, post-traumatic growth; T1, time 1; T2, time 2.
p < 0.05.
p < 0.01.
p < 0.001.
The means, standard deviations (SD), and correlations between the T1 and T2 continuous variables are shown in Table 2 . The PTG at the baseline was highly correlated with the PTG in the follow-up (r = 0.712), and the perceived EI at the baseline was significantly correlated with the ER at the follow up (r = 0.647) and moderately correlated with the T1 PTG (r = 0.477), the T2 PTG (r = 0.392), and the T2 self-esteem (r = 0.471).
Table 2.
Correlations for the main study variables (N = 1609).
| Variable | M | S | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|---|
| 1.PTG_T1 | 39.46 | 26.71 | 1 | ||||
| 2. PTG_T2 | 42.38 | 26.06 | 0.712⁎⁎ | 1 | |||
| 3. Emotional intelligence_T1 | 72.83 | 20.26 | 0.477⁎⁎ | 0.392⁎⁎ | 1 | ||
| 4. Emotional regulation_T2 | 43.87 | 12.82 | 0.402⁎⁎ | 0.311⁎⁎ | 0.647⁎⁎ | 1 | |
| 5. Self-esteem_T2 | 26.85 | 3.92 | 0.349⁎⁎ | 0.363⁎⁎ | 0.471⁎⁎ | 0.259⁎⁎ | 1 |
Abbreviations: PTG, post-traumatic growth.
p < 0.01.
The results of the CFA indicated that the factor structure of three scales all fitted well with the data, including the EI scale (RMSEA = 0.055, 95% CI: 0.050–0.059; GFI = 0.961; CFI = 0.986; and SRMR = 0.058), ER scale (RMSEA = 0.049, 95% CI: 0.040–0.058; GFI = 0.986; CFI = 0.993; and SRMR = 0.051) and PTG_T2 scale (RMSEA = 0.059, 95% CI: 0.055–0.063; GFI = 0.956; CFI = 0.981; and SRMR = 0.052).
The SEM model (Fig. 2 ) also revealed a good fit to the data: (DF = 61, chi-square = 692.95, p < 0.001; RMSEA = 0.080, 95% CI: 0.075–0.086; GFI = 0.935; CFI = 0.962; and SRMR = 0.045). The results indicated that the T1 perceived EI significantly predicted the T2 PTG (b = 0.23, p < 0.001), the T2 ER (b = 0.70, p < 0.001) and the T2 self-esteem (b = 0.51, p < 0.001). ER partly mediated the association between perceived EI and PTG (b = 0.08, 95%CI 0.02–0.14, p < 0.001), and self-esteem partly mediated the association between perceived EI and PTG (b = 0.11, 95%CI 0.08–0.13, p < 0.001).
Fig. 2.

Longitudinal mediation model for EI on PTG
**p < 0.01;***p < 0.001; Beta values standardized.
Abbreviations: T1 = Time 1 (baseline); T2 = Time 2 (follow-up); ER, emotional regulation; CR, cognitive reappraisal; ES, emotional repression; SE, self-esteem; PTG, posttraumatic growth; EI, emotional intelligence; EI1, regulation of emotion; EI2, self-emotion appraisal; EI3, others' emotion appraisal; EI4, use of emotion; RTO, relating to others; NP, new possibilities; PS, personal strength; AOL, appreciation of life; SC, spiritual change.
4. Discussion
This was the first longitudinal study to assess PTG prevalence over time during the COVID-19 pandemic, prospectively determine the role of perceived EI in predicting PTG over five months, and examine the mediating role of ER and self-esteem in this relationship. The PTG rates for the participant adolescents were found to slightly increase during the worst phase of the COVID-19 pandemic. Therefore, as hypothesized, the SEM models demonstrated that EI predicted subsequent PTG and that ER and self-esteem mediated this relationship.
Consistent with the study hypotheses, the model found that higher perceived EI levels significantly predicted higher PTG levels in the adolescent sample during COVID-19. This finding aligned with previous longitudinal research that found that EI at the baseline predicted subsequent PTG in adults a few years after a trauma event (Tuck and Patlamazoglou, 2019). The study results also accorded with a cross-sectional study that found that higher perceived EI levels correlated with higher PTG in patients after the confirmation of a severe disease (Rider Mundey et al., 2019). The possible explanation for these results is that people with high EI may tend to employ more adaptive (rational, intuitive) than maladaptive (dependent, avoidant) cognitive styles to cope with stress (Avsec, 2012). Other possible explanations are that perceived EI contributes to resilience (McCarthy et al., 2020), which in turn could enhance personal strength, which is a subcomponent of PTG; that is, people's perceptions of the COVID-19 stress may have helped them reevaluate their life purpose and values.
The current findings add to the field by suggesting that perceived EI predicts adolescent self-esteem and promotes PTG, which expands the findings in Senol-Durak (2014), which suggested that stress-related growth and self-esteem were correlated. As also suggested in (Schutte et al., 2002), people with higher perceived EI may use this ability to understand and regulate others and their own emotions to cope with environmental threats, which may enable them to maintain higher levels of self-esteem and perceptions of self-worth or value. Therefore, adolescents with high self-esteem may experience positive change when faced with stressful life circumstances because their inner resources provide them with a better ability to cope with adversity (Taku and Britton, 2017). As the study results were also in line with previous studies that found positive associations between self-esteem and PTG (Taku and McDiarmid, 2015), this study complements earlier findings that higher perceived EI levels promote adolescent self-esteem and lead to PTG when needing to deal with COVID-19 measures.
The current study revealed the ER mechanism underlying the relationship between perceived EI and PTG in adolescents, which in part corresponded to Zysberg and Raz's (2019) findings that participants with higher EI were better able to regulate their emotions during the COVID-19 pandemic and may have helped them evaluate the associated restrictions in a more positive light. This study's results were also partly in line with Orejuela-Dávila et al.'s (2019) experimental study that found people who chose ER reappraisal strategies frequently reported greater growth. Based on the adaptive emotional functioning model, it has been proposed that emotionally intelligent people construct their own ER rules (Mayer and Salovey, 1995). Two previous studies also provided robust evidence that EI could predict ER in high-pressure situations, which also supports the results in the current study (Laborde et al., 2014; Zysberg and Raz, 2019). Given these confirmations, effective ER strategies could assist people in redefining the meaning of trauma, life, and self, establishing greater trust in their own strength, and discovering new possibilities that would, in turn, facilitate PTG. However, ER was not found to be a mediating factor between self-esteem and PTG, although self-esteem is more likely to have better emotion regulation ability (Adiyanti et al., 2020) which could, in turn, affect PTG, possibly because the effect was not strong enough to cause the relationship to disappear when the other variables were added; therefore, this needs further exploration.
Around 22%–25% of the sample had significant PTG during the COVID-19 lockdown period, about half that of a previous Chinese college student COVID-19 pandemic study (Chi et al., 2020). This discrepancy could have been because of sample differences, different cut-off values, or differences in age and education levels. However, in the absence of similar studies on PTG in a pandemic context, it is difficult to make comparisons; therefore, more COVID-19 research is needed on different samples and at different time intervals. It was found that males were more likely to have higher PTG than females, which was in contrast to several previous trauma studies that reported higher PTG in females (Hafstad et al., 2011; Meyerson et al., 2011); therefore, further research on these mechanisms is also needed.
Although this study adds to an understanding of the PTG processes and mechanisms, there were several limitations. First, survey credibility was partly affected because it involved self-assessment; therefore, more objective future investigations are needed to verify these relationships. Second, due to the limited sample size and the cultural differences, the applicability of these results to other regions in China or other countries also needs to be further verified. Third, although there is no evidence that online assessments affect measurement validity, further research based on paper and pencil surveys should be conducted to confirm these data. Fourth, as valid mediation tests require at least three-time points (Maxwell and Cole, 2007), the two mediation waves may have limited the results to some extent. Fifth, the majority of the sample was female, which may have affected the sample representativeness. Sixth, as the Wong and Law emotional intelligence scale was used to measure the perceived EI, the self-assessment and the possibility that the scale may be more sensitive to certain traits (Karim, 2010) could limit the applicability of the results; therefore, performance-based EI tests could be conducted to confirm the actual performance. Finally, there was only a 5-month interval between the two measures; therefore, more waves and longer intervals are needed to fully justify the findings.
5. Conclusion
In sum, in this longitudinal design, we found adolescent EI could predict current and later COVID-19 related PTG. Moreover, it also gives some preliminary findings on the underlying mechanism in this relationship. Emotional adjustment strategies and self-esteem may act as mediators of the association between EI and PTG. As life for most teenagers has been significantly disrupted and mental health concerns have increased due to pandemic measures (Bourmistrova et al., 2022), promoting adolescent growth and reducing any negative impacts is important. As the predictive role of EI in the PTG process was highlighted, these results have important implications for the promotion of PTG during and after the COVID-19 pandemic in the general adolescent populations. Firstly, this short-term longitudinal study provides some reliable evidence that high perceived EI can promote growth, which suggests that perceived EI training programs for adolescents could assist them in overcoming the adverse effects of the pandemic and promote growth. Moreover, it is also suggested that parents pay attention to the cultivation of their children's EI as well as their academic performances. Finally, this research also provided a greater understanding of the underlying perceived EI mechanisms related to PTG and highlighted that training in self-esteem and emotional adjustment skills could promote PTG in teenagers during and following the COVID-19 pandemic.
Funding
This research was supported by grants from China's National Planning Office of Philosophy and Social Science (18BSH121).
Compliance with ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
CRediT authorship contribution statement
Wanjie Tang: Writing - original draft, Visualization, Resources, Software, Writing - review & editing; Zhouxingyu Yan: Writing - original draft, Writing - review & editing, Funding acquisition; Yi Lu: Writing – revised version, statistics, Writing - review & editing; Jiuping Xu: Investigation, Data curation, Funding acquisition, Writing – original draft, Supervision, Writing - review & editing.
Declaration of competing interest
The authors declare that they have no conflicts of interest.
Acknowledgment
The authors wish to thank all study participants and all research collaborators. This study also thanks the editors and reviewers for helping us to improve this manuscript.
References
- Adiyanti M.G., Nugraheni A.A., Yuliawanti R., Ragasukmasuci L.B., Maharani M. Emotion regulation and empathy as mediators of self-esteem and friendship quality in predicting cyberbullying tendency in javanese-indonesian adolescents. Int. J. Adolesc. Youth. 2020;25(1):251–263. [Google Scholar]
- Avsec A. Do emotionally intelligent individuals use more adaptive decision-making styles? Stud. Psychol. 2012;54(3):209. [Google Scholar]
- Bourmistrova N.W., Solomon T., Braude P., Strawbridge R., Carter B. Long-term effects of COVID-19 on mental health: a systematic review. J. Affect. Disord. 2022;299:118–125. doi: 10.1016/j.jad.2021.11.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brackett M.A., Rivers S.E., Salovey P. Emotional intelligence: implications for personal, social, academic, and workplace success. Soc. Personal. Psychol. Compass. 2011;5(1):88–103. [Google Scholar]
- Calhoun L.G., Tedeschi R.G. Routledge; 1999. Facilitating Posttraumatic Growth: A Clinician's Guide. [Google Scholar]
- Calhoun L.G., Tedeschi R.G. 2006. The Foundations of Posttraumatic Growth: An Expanded Framework. [Google Scholar]
- Chen W., Zhang D., Pan Y., Hu T., Liu G., Luo S. Perceived social support and self-esteem as mediators of the relationship between parental attachment and life satisfaction among Chinese adolescents. Personal. Individ. Differ. 2017;108:98–102. [Google Scholar]
- Cheng S.K., Chong G.H., Chang S.S., Wong C.W., Wong C.S., Wong M.T., Wong K.C. Adjustment to severe acute respiratory syndrome (SARS): roles of appraisal and post-traumatic growth. Psychol. Health. 2006;21(3):301–317. [Google Scholar]
- Cheung C.K., Cheung H.Y., Hue M.T. Emotional intelligence as a basis for self-esteem in young adults. J. Psychol. 2015;149(1):63–84. doi: 10.1080/00223980.2013.838540. [DOI] [PubMed] [Google Scholar]
- Chi X., Becker B., Yu Q., Willeit P., Jiao C., Huang L., Hossain M.M., Grabovac I., Yeung A., Lin J. Prevalence and psychosocial correlates of mental health outcomes among Chinese college students during the coronavirus disease (covid-19) pandemic. Front. Psychiatry. 2020;11:803. doi: 10.3389/fpsyt.2020.00803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crocker J., Brook A.T., Niiya Y., Villacorta M. The pursuit of self-esteem: contingencies of self-worth and self-regulation. J. Pers. 2006;74(6):1749–1772. doi: 10.1111/j.1467-6494.2006.00427.x. [DOI] [PubMed] [Google Scholar]
- Danhauer S.C., Case L.D., Tedeschi R., Russell G., Vishnevsky T., Triplett K., Ip E.H., Avis N.E. Predictors of posttraumatic growth in women with breast cancer. Psycho-Oncology. 2013;22(12):2676–2683. doi: 10.1002/pon.3298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davies S. The wisdom in feeling: psychological processes in emotional intelligence. Pers. Psychol. 2004;57(2):511. [Google Scholar]
- Dekel S., Ein-Dor T., Solomon Z. Posttraumatic growth and posttraumatic distress: a longitudinal study. Psychol. Trauma Theory Res. Pract. Policy. 2012;4(1):94. [Google Scholar]
- Extremera Pacheco N., Rey Peña L., Sánchez Álvarez N. Validation of the Spanish version of the Wong law emotional intelligence scale (WLEIS-S) Psicothema. 2019;31(1):94–100. doi: 10.7334/psicothema2018.147. [DOI] [PubMed] [Google Scholar]
- Eze J.E., Ifeagwazi C.M., Chukwuorji J.C. Core beliefs challenge and posttraumatic growth: mediating role of rumination among internally displaced survivors of terror attacks. J. Happiness Stud. 2020;21(2):659–676. [Google Scholar]
- Feingold J.H., Hurtado A., Feder A., Peccoralo L., Southwick S.M., Ripp J., Pietrzak R.H. Posttraumatic growth among health care workers on the frontlines of the COVID-19 pandemic. J. Affect. Disord. 2022;296:35–40. doi: 10.1016/j.jad.2021.09.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foa E.B., Huppert J.D., Cahill S.P. In: Pathological Anxiety: Emotional Processing in Etiology and Treatment. Rothbaum B.O., editor. Guilford; New York, NY: 2006. Emotional processing theory: an update; pp. 3–24. [Google Scholar]
- Gao J., Wang M., Deng J., Qian M., Liu X., <check>HE Q.</check>. Revision and preliminary application of Chinese version of post-traumatic growth inventory in adolescents experienced the Wenchuan earthquake. Chin. Mental Health J. 2010;126–130 [Google Scholar]
- Gross J.J. The emerging field of emotion regulation: an integrative review. Rev. Gen. Psychol. 1998;2(3):271–299. [Google Scholar]
- Gross J.J. Emotion regulation: affective, cognitive, and social consequences. Psychophysiology. 2002;39:281–291. doi: 10.1017/s0048577201393198. [DOI] [PubMed] [Google Scholar]
- Gross J.J., John O.P. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 2003;85(2):348. doi: 10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- Hafstad G.S., Kilmer R.P., Gil-Rivas V. Posttraumatic growth among Norwegian children and adolescents exposed to the 2004 tsunami. Psychol. Trauma Theory Res. Pract. Policy. 2011;3(2):130. [Google Scholar]
- Hamam A.A., Milo S., Mor I., Shaked E., Eliav A.S., Lahav Y. Peritraumatic reactions during the COVID-19 pandemic–The contribution of posttraumatic growth attributed to prior trauma. J. Psychiatr. Res. 2021;132:23–31. doi: 10.1016/j.jpsychires.2020.09.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iliceto P., Fino E. The italian version of the Wong-law emotional intelligence scale (WLEIS-I): a second-order factor analysis. Personal. Individ. Differ. 2017;116:274–280. [Google Scholar]
- Karim J. An item response theory analysis of Wong and law emotional intelligence scale. Procedia Soc. Behav. Sci. 2010;2(2):4038–4047. [Google Scholar]
- Kong F. The validity of the Wong and law emotional intelligence scale in a Chinese sample: tests of measurement invariance and latent mean differences across gender and age. Personal. Individ. Differ. 2017;116:29–31. [Google Scholar]
- Laborde S., Lautenbach F., Allen M.S., Herbert C., Achtzehn S. The role of trait emotional intelligence in emotion regulation and performance under pressure. Personal. Individ. Differ. 2014;57:43–47. [Google Scholar]
- LaPalme M.L., Wang W., Joseph D.L., Saklofske D.H., Yan G. Measurement equivalence of the Wong and law emotional intelligence scale across cultures: an item response theory approach. Personal. Individ. Differ. 2016;90:190–198. [Google Scholar]
- Li W., Hengchao L., Zhongquan L. Reliability and validity of emotion regulation questionnaire Chinese revised version. Chin. J. Health Psychol. 2007;6:013. [Google Scholar]
- Li Y., Zhao J., Ma Z., McReynolds L.S., Lin D., Chen Z., Wang T., Wang D., Zhang Y., Zhang J. Mental health among college students during the COVID-19 pandemic in China: a 2-wave longitudinal survey. J. Affect. Disord. 2021;281:597–604. doi: 10.1016/j.jad.2020.11.109. [DOI] [PubMed] [Google Scholar]
- Libbrecht N., Lievens F., Schollaert E. Measurement equivalence of the Wong and law emotional intelligence scale across self and other ratings. Educ. Psychol. Meas. 2010;70(6):1007–1020. [Google Scholar]
- Magson N.R., Freeman J.Y., Rapee R.M., Richardson C.E., Oar E.L., Fardouly J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J. Youth Adolesc. 2021;50(1):44–57. doi: 10.1007/s10964-020-01332-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maxwell S.E., Cole D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Methods. 2007;12(1):23. doi: 10.1037/1082-989X.12.1.23. [DOI] [PubMed] [Google Scholar]
- Mayer J.D., Salovey P. Emotional intelligence and the construction and regulation of feelings. Appl. Prev. Psychol. 1995;4(3):197–208. [Google Scholar]
- Mayer J.D., Salovey P., Caruso D.R., Sternberg R. In: Models of Emotional Intelligence. Mayer J.D., editor. 2000. [Google Scholar]
- McCarthy S.A., Ford T.C., Lomas J.E., Stough C. Subclinical autistic traits mediate the relationship between emotional intelligence and resiliency in adolescents. Personal. Individ. Differ. 2020;158 [Google Scholar]
- Meyerson D.A., Grant K.E., Carter J.S., Kilmer R.P. Posttraumatic growth among children and adolescents: a systematic review. Clin. Psychol. Rev. 2011;31(6):949–964. doi: 10.1016/j.cpr.2011.06.003. [DOI] [PubMed] [Google Scholar]
- Oosterhoff B., Palmer C.A., Wilson J., Shook N. Adolescents' motivations to engage in social distancing during the COVID-19 pandemic: associations with mental and social health. J. Adolesc. Health. 2020;67(2):179–185. doi: 10.1016/j.jadohealth.2020.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orejuela-Dávila A.I., Levens S.M., Sagui-Henson S.J., Tedeschi R.G., Sheppes G. The relation between emotion regulation choice and posttraumatic growth. Cognit. Emot. 2019 doi: 10.1080/02699931.2019.1592117. [DOI] [PubMed] [Google Scholar]
- Park H.-J., Yu S. Validity and Reliability of the Korean version of the Wong and Law Emotional Intelligence Scale for Nurses. SAGE Open. 2021;11(2) 21582440211023202. [Google Scholar]
- Peña-Sarrionandia A., Mikolajczak M., Gross J.J. Integrating emotion regulation and emotional intelligence traditions: a meta-analysis. Front. Psychol. 2015;6:160. doi: 10.3389/fpsyg.2015.00160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Fuentes, Molero Jurado M.d.M., Del Pino R.M., Gázquez Linares J.J. Emotional intelligence, self-efficacy and empathy as predictors of overall self-esteem in nursing by years of experience. Front. Psychol. 2019;10:2035. doi: 10.3389/fpsyg.2019.02035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pietrzak R.H., Tsai J., Southwick S.M. Association of Symptoms of posttraumatic stress disorder with posttraumatic psychological growth among US veterans during the COVID-19 pandemic. JAMA Netw. Open. 2021;4(4):e214972. doi: 10.1001/jamanetworkopen.2021.4972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhodewalt F., Tragakis M.W. Self-esteem and self-regulation: toward optimal studies of self-esteem. Psychol. Inq. 2003;14(1):66–70. [Google Scholar]
- Rider Mundey K., Nicholas D., Kruczek T., Tschopp M., Bolin J. Posttraumatic growth following cancer: the influence of emotional intelligence, management of intrusive rumination, and goal disengagement as mediated by deliberate rumination. J. Psychosoc. Oncol. 2019;37(4):456–477. doi: 10.1080/07347332.2018.1514449. [DOI] [PubMed] [Google Scholar]
- Robins R.W., Hendin H.M., Trzesniewski K.H. Measuring global self-esteem: construct validation of a single-item measure and the Rosenberg self-esteem scale. Personal. Soc. Psychol. Bull. 2001;27(2):151–161. [Google Scholar]
- Rodríguez-Rey R., Palacios A., Alonso-Tapia J., Pérez E., Álvarez E., Coca A., Mencía S., Marcos A.M., Mayordomo-Colunga J., Fernández F. Posttraumatic growth in pediatric intensive care personnel: dependence on resilience and coping strategies. Psychol. Trauma Theory Res. Pract. Policy. 2017;9(4):407. doi: 10.1037/tra0000211. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. Rosenberg self-esteem scale (RSE). Acceptance and commitment therapy. Measures package. 1965;61(52):18. [Google Scholar]
- Rosenberg M. Conceiving the Self. Basic Books; New York: 1979. Conceiving the self; p. 318. [Google Scholar]
- Rosenberg M. In: Conceiving the Self. Krieger R.E., editor. 1986. [Google Scholar]
- Salovey P., Mayer J.D. Emotional intelligence. Imagin. Cogn. Pers. 1990;9(3):185–211. [Google Scholar]
- Salovey P., Detweiler-Bedell B., Detweiler-Bedell J., Mayer J. Handbook of Emotions. 2008. Emotional intelligence, coping, and self-regulation; pp. 533–547. [Google Scholar]
- Schutte N.S., Malouff J.M., Simunek M., McKenley J., Hollander S. Characteristic emotional intelligence and emotional well-being. Cognit. Emot. 2002;16(6):769–785. [Google Scholar]
- Senol-Durak E. Stress related growth among diabetic outpatients: role of social support, self-esteem, and cognitive processing. Soc. Indic. Res. 2014;118(2):729–739. [Google Scholar]
- Shi J., Wang L. Validation of emotional intelligence scale in Chinese university students. Personal. Individ. Differ. 2007;43(2):377–387. [Google Scholar]
- Shigemoto Y. Association between trajectories of personal growth initiative and post‐traumatic stress after Hurricane Harvey: a latent growth mixture modeling approach. Stress. Health. 2021;37(2):285–296. doi: 10.1002/smi.2995. [DOI] [PubMed] [Google Scholar]
- Singh S., Roy M.D., Sinha C.P.T.M.K., Parveen C.P.T.M.S., Sharma C.P.T.G., Joshi C.P.T.G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. 2020;113429 doi: 10.1016/j.psychres.2020.113429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taku K., Britton M. 2017. Relationships Between Self-esteem and Posttraumatic Growth Among Adolescents in the US. [Google Scholar]
- Taku K., McDiarmid L. Personally important posttraumatic growth in adolescents: the effect on self-esteem beyond commonly defined posttraumatic growth. J. Adolesc. 2015;44:224–231. doi: 10.1016/j.adolescence.2015.08.001. [DOI] [PubMed] [Google Scholar]
- Tang W., Wang Y., Lu L., Lu Y., Xu J. Post-traumatic growth among 5195 adolescents at 8.5 years after exposure to the Wenchuan earthquake: roles of post-traumatic stress disorder and self-esteem. J. Health Psychol. 2021;26(13):2450–2459. doi: 10.1177/1359105320913947. [DOI] [PubMed] [Google Scholar]
- Tedeschi R.G., Calhoun L.G. The posttraumatic growth inventory: measuring the positive legacy of trauma. J. Trauma. Stress. 1996;9(3):455–471. doi: 10.1007/BF02103658. [DOI] [PubMed] [Google Scholar]
- Tedeschi R.G., Calhoun L.G. Posttraumatic growth: conceptual foundations and empirical evidence. Psychol. Inq. 2004;15(1):1–18. [Google Scholar]
- Thomas E.A., Hamrick L.A., Owens G.P., Tekie Y.T. Posttraumatic growth among undergraduates: contributions from adaptive cognitive emotion regulation and emotional intelligence. Traumatology. 2020;26(1):68. [Google Scholar]
- Tuck D., Patlamazoglou L. The relationship between traumatic stress, emotional intelligence, and posttraumatic growth. J. Loss Trauma. 2019;24(8):721–735. [Google Scholar]
- Vazquez C., Valiente C., García F.E., Contreras A., Peinado V., Trucharte A., Bentall R.P. Post-traumatic growth and stress-related responses during the COVID-19 pandemic in a national representative sample: the role of positive core beliefs about the world and others. J. Happiness Stud. 2021:1–21. doi: 10.1007/s10902-020-00352-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walter K.H., Horsey K.J., Palmieri P.A., Hobfoll S.E. The role of protective self-cognitions in the relationship between childhood trauma and later resource loss. J. Trauma. Stress. 2010;23(2):264–273. doi: 10.1002/jts.20504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong C.-S., Law K.S. The effects of leader and follower emotional intelligence on performance and attitude: an exploratory study. Leadersh. Q. 2002;13(3):243–274. [Google Scholar]
- Xiong J., Lipsitz O., Nasri F., Lui L.M., Gill H., Phan L., McIntyre R.S. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J. Affect. Disord. 2020;277:55–64. doi: 10.1016/j.jad.2020.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhen R., Zhou X. Latent patterns of posttraumatic stress symptoms, depression, and posttraumatic growth among adolescents during the COVID‐19 pandemic. J. Trauma. Stress. 2022;35(1):197–209. doi: 10.1002/jts.22720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zysberg L., Raz S. Emotional intelligence and emotion regulation in self-induced emotional states: physiological evidence. Personal. Individ. Differ. 2019;139:202–207. [Google Scholar]