

Abstract
Purpose
To evaluate the effect of COVID-19 on retinal tissues by conducting a systematic review and meta-analysis of the current literature.
Background
The novel coronavirus disease is not yet well understood. The orbit provides a window into the body's microvasculature, and as such, it is a non-invasive opportunity to analyse the systemic circulation in vivo. By analysing the current literature, we test the hypothesis that non-invasive imaging of the retina could provide insight into the effect of COVID-19 on the retinal microvasculature.
Methods
For this systematic review and meta-analysis, we screened PubMed databases and LitCOVID19 using the search criteria: (OCTA or Optical Coherence Tomography Angiography) AND (COVID-19 or corona or SARS-CoV-2) AND (retina or fundus). Databases were searched on 11 January 2022. The primary study outcomes were studies that utilised OCTA to analyse the retina; secondary outcomes involved studies that involved other imaging modalities such as OCT, fundus photography, and fundus autofluorescence.
Findings
The total number of studies included in this review was 32. Optical coherence tomography angiography scans show reduced central retinal vascular density, a thinner ganglion cell layer, a thicker retinal nerve fibre layer, and an enlarged foveal avascular zone. Optical coherence tomography scans demonstrate a thicker central macular thickness and other changes to the macula, ganglion cell, and inner nuclear layers. Many fundus photographs depicted cotton wool spots, microhaemorrhages, and vascular occlusions. Non-invasive imaging technology has demonstrated that COVID-19 can profoundly affect the retina. Therefore, there is a requirement for long-term follow-up of COVID-19 patients to assess whether the retinal damage caused by COVID-19 is reversible.
Supplementary Information
The online version contains supplementary material available at 10.1007/s40123-022-00509-8.
Keywords: COVID-19, Imaging, OCT, OCTA, Retina
Key Summary Points
| COVID-19 causes a microvascular disorder that affects the retina in many ways. |
| Understanding the long-term effects of COVID-19 remains an unmet need. |
| Understanding how the body's microvasculature can be affected by COVID-19 could affect future treatment. |
| Optical coherence tomography angiography scans show reduced central retinal vascular density, a thinner ganglion cell layer, a thicker retinal nerve fibre layer, and an enlarged foveal avascular zone. Optical coherence tomography scans demonstrate thicker central macular thickness and changes to the macula, ganglion cell, and inner nuclear layers. Many fundus photographs depicted cotton wool spots as well as vascular occlusions. |
Introduction
COVID-19 is a systemic disease that involves multiple organs through direct viral invasion and immune-mediated inflammation. Widespread endotheliitis may cause microvascular dysfunction and tissue ischaemia. The primary mechanism behind vascular damage caused by COVID-19 appears to be a disseminated intravascular coagulation (DIC)-like hypercoagulable state [1]. This process is driven by the direct viral infection of the endothelial cells, leading to endothelial inflammation [2]. Elevated D-dimers, prothrombin time, activated partial thromboplastin time (aPTT), fibrinogen, and cytokines evidence this, even when conditions such as hypertension, diabetes, or dyslipidaemia are absent [3].
The angiotensin-converting enzyme-related carboxypeptidase (ACE2) receptor is the entry site of COVID-19 to heart venule pericytes and capillaries [4]. The ACE2 receptor is also involved in retinopathy secondary to diabetes and hypertension [5]. SARS-CoV-2 uses the angiotensin-converting enzyme-related carboxypeptidase (ACE2) receptor to enter cells [6]. In a study by Casagrande et al. [7], 3 out of 14 (21%) COVID-19 positive subjects had retinal biopsies taken where SARS-CoV-2 viral RNA was detected. In addition, there is a strong affinity of COVID-19 for the ACE-2 receptor expressed on the surface of Muller cells, the retinal pigment epithelium, and pericytes of endothelial cells in the retina and choroid [8]. The ACE2 receptor provides a critical role in retinal neurovascular function, which could also justify direct non-ischaemic damage to the retina [9]. The immune cells in the vessel walls recruited by SARS-CoV-2 could produce endothelial cellular oedema [3]. In addition, the viral infection can provoke an immune response with endothelial dysfunction and associated apoptosis, leading to micro-thrombotic events.
Literature discussing the long-term effects of COVID-19 is limited [9, 10]. The infections can be relapsing and remitting and have a wide range of symptoms [11, 12]. However, the severity of the patient's initial COVID-19 illness does not predict the development of long-term effects. There are likely several distinct post-COVID-19 syndromes, including post-intensive care syndrome and post-viral fatigue syndrome. Central vessel density (VD) is deemed a biomarker for diseases such as diabetes [13], inflammatory bowel disease [14], chronic kidney disease [15], and Alzheimer's disease [16]. Central VD shows the potential to become a biomarker for microvascular damage in COVID-19 patients too. COVID-19 retinal changes do not appear specific to COVID-19 as they are vascular, inflammatory, and neuronal changes triggered by the viral infection. It is too early to say whether changes persist or if they are reversible.
In COVID-19-infected patients, the prevalence of ocular manifestations ranges from 2 to 32% [17]. Ocular complications include a wide range of pathologies. For example, anterior segment conditions such as conjunctivitis and anterior uveitis are common, but there are several reports of vision-threatening conditions such as retinitis, optic neuritis, choroiditis, and retinal vasculitis [18–21]. The literature regarding the ocular manifestations of COVID-19 mainly describes anterior segment disorders, such as pyogranulomatous anterior uveitis [22], chemosis, and conjunctivitis [20]. Conjunctivitis is the most common sign and can develop at any stage of the disease [3]. Immune-mediated tissue damage, activation of the coagulation cascade and the prothrombotic state induced by COVID-19, the associated comorbidities, and drugs used in the disease management are all responsible for the findings in the eye [3].
Optical coherence tomography angiography (OCTA) could represent a valid, non-invasive biomarker of microvascular dysfunction following COVID-19 infection [23]. It provides depth-resolved imaging of blood flow in the retina with microvascular detail that exceeds the capability of other forms of imaging [24]. In addition, OCTA provides accessible, fast, and economic vascular analysis without dye injection. Studies suggest that OCTA parameters may reflect the microvascular changes occurring elsewhere in less-accessible organs such as the lungs or the kidneys [25]. In addition, associations made between ocular and systemic disease status may directly impact patient management. For example, a study by Garcia-Vidal et al. [26] described three different disease profiles (inflammatory, co-infection, and thrombotic) in blood patterns of COVID-19 patients using artificial intelligence that aids physicians in personalising treatment, thus significantly reducing the mortality rate of these patients. This review aims to evaluate the effect of COVID-19 on retinal tissues by conducting a systematic review and meta-analysis of the current literature.
Methods
Following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, we completed our systematic review. The review protocol was not previously registered. This article is based on previously conducted studies and does not contain any new studies with humans or animals performed by either author. A systematic literature review was performed (for screening, eligibility and inclusion) from the electronic databases PubMed and LitCOVID19 for English language articles and English translated abstracts of non-English articles. The literature search was performed on 11 January 2022. We used the search criteria: (OCTA or Optical Coherence Tomography Angiography) AND (COVID-19 or corona or SARS-CoV-2) AND (retina or fundus). The studies were not restricted to a time point of assessment. Please refer to the supplementary material to view each study’s follow-up period. Primary outcomes included those studies which used OCTA to analyse the effect of COVID-19 on retinal tissues, and secondary outcomes included studies involving any other forms of imaging such as optical coherence tomography (OCT), fundus photography, and fundus autofluorescence.
Study titles and abstracts were screened to ensure they met the eligibility criteria by the first author. The full texts of all titles which appeared to meet the inclusion criteria were downloaded and screened. References of relevant articles identified through the search were also scanned. Inclusion criteria included papers that outline the effect of COVID-19 on the retina, and exclusion criteria included papers researching the effect of COVID-19 vaccination on the retina. In addition, we included any prospective and retrospective studies, case series, case reports, and correspondence reporting retinal manifestations in confirmed COVID-19 patients of any age, gender, and race in this study. Patients were confirmed as COVID-19 positive cases based on clinical criteria (recommended by their National Health agencies) or positive reverse transcription polymerase chain reaction (RT-PCR) for viral RNA from nasopharyngeal swabs [27]. Studies with only suspected cases of COVID-19 were excluded from analysis. A Microsoft Excel spreadsheet was used to obtain data from the eligible studies related to study design and setting, clinical details, including disease severity, and reported ocular signs and symptoms.
Results
This study identified 126 articles from the initial search (Fig. 1). The total number of included studies in this review was 32. Please refer to the supplementary material for a summary of these studies. OCTA scans show reduced central retinal VD, a thinner ganglion cell layer, a thicker retinal nerve fibre layer, and an enlarged foveal avascular zone (FAZ). OCT demonstrated scotomas, thicker central macular thickness, and changes to the macula, ganglion cell, and inner nuclear layers. Fundus photography depicted cotton wool spots (CWS), retinal haemorrhages, and vascular occlusions. The risk of bias assessment has been summarised in Table 1. The results are broken down and explained further below.
Fig. 1.
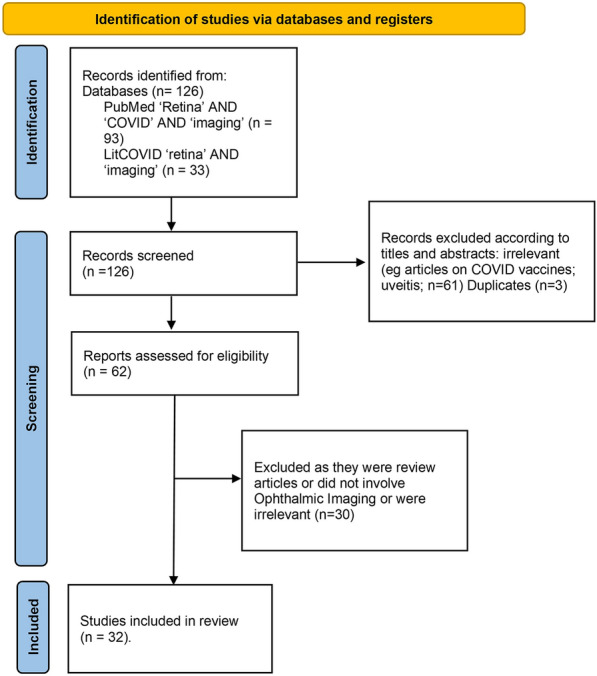
PRISMA flow diagram of studies included in this review
Table 1.
Risk of bias assessment (evaluated using Newcastle-Ottawa Quality Assessment Scale, adapted for Case-Control Studies and Case Series)
| Risk of bias | Selection | Comparability | Exposure/outcome |
|---|---|---|---|
| Abrishami et al. | Moderate | Moderate | Low |
| Beni et al. | Moderate | Low | Low |
| Burgos-Blasco et al. | Low | Low | Low |
| Cennamo et al. | Low | Low | Low |
| Banderas García et al. | Low | Moderate | Low |
| Gonzalez Zamora et al. | High | Low | Low |
| Guemes Villahoz et al. | High | Low | Low |
| Hazar et al. | Low | Low | Low |
| Invernizzi et al. | Moderate | Low | Low |
| Oren et al. | Low | Low | Low |
| Savastano et al. | Low | Moderate to high | Low |
| Szkodny et al. | Low | Low | Low |
| Turker et al. | Moderate | Low | Low |
| Zapata et al. | Low | Low | Low |
| Brantl et al. | Moderate | Moderate | Low |
| Bypareddy et al. | Low | Low | Low |
| Costa et al. | Moderate | Moderate | Low |
| Landecho et al. | Moderate | Moderate | Low |
| Lani Louzada et al. | Moderate | Moderate | Low |
| Marinho et al. | High | Moderate | High |
| Pereira et al. | Moderate | Moderate | Low |
| Pirraglia et al. | Low | Low | Low |
| Sim et al. | High | Low | Low |
How does SARS-CoV-2 Affect the Retina?
The retina has the most significant metabolic demand of any body tissue [25, 28]. The retina's blood flow is constant, even when blood pressure and blood gas tension change, which is often the case in patients with severe COVID-19 infection [25]. The retinal vasculature is resistant to autonomic innervation influences and hormonal mediators [29]. Therefore, the retina is an ideal organ to study local microcirculation [30]. The boundary that delimits the FAZ is particularly susceptible to ischaemic changes as it is composed of retinal plexi, which are end arteries with no anastomotic connections [25]. In addition, FAZ area enlargement correlates with capillary loss in different retinal vascular diseases, such as diabetic retinopathy and retinal vascular occlusions [9]. Occlusive phenomena of intravascular coagulation are more evident in small-scale vascular plexi, such as in the retinal vessels [31].
Retinal foveal flow impairment may occur because of an obstructive event in the vessel lumen, mainly thrombotic phenomena. A delicate capillary network categorises the vascular structure of the deep capillary plexus (DCP). These narrow capillaries make the DCP more vulnerable to thrombotic events than the superficial capillary plexus (SCP), which has a larger vascular calibre. Capillary dropout could result from increased apoptosis of the endothelial cells in a proinflammatory endothelium dysfunctional environment. COVID-19 infection is likely also to affect retinal vessels through an immune-mediated reaction. The endothelial injury could be the underlying mechanism that might link inflammation and thrombosis in severe cases [25].
Intermittent hypoxia in patients with pneumonia can induce the endothelial cells to release tissue factors and trigger the extrinsic coagulation cascade [32]. A recent paper by Zhang et al. [33] suggests that the leading factor in the pathogenesis of microcirculatory damage in COVID-19 patients is complement-mediated thrombotic microangiopathy [34]. Complement system activation is directly responsible for ocular vascular damage, with rare atypical haemolytic uraemic syndrome cases leading to retinal artery and vein occlusions [35].
OCTA Findings in Patients with COVID-19
OCTA can be invaluable in detecting retinal vascular disease in systemic disorders like diabetes before clinically apparent retinopathy [34]. OCTA may detect microvascular abnormalities such as microaneurysms, venous beading, enlargement of the FAZ, and capillary nonperfusion in diabetic eyes before any clinical signs of retinopathy. OCTA could provide similar benefits in patients with COVID-19 as the VD reductions reported in studies, such as in Abrishami's study, are comparable to those in patients with diabetes [36].
OCTA Findings in Patients 2 Weeks Post COVID-19
All studies analysing patients around 2 weeks post-hospital discharge found retinal microvascular changes such as CWS, retinal nerve fibre layer (RNFL) thickening, enlarged FAZ, or reduced VD. Turker et al. [37] used OCTA to study 27 patients' eyes 1 week post-discharge for COVID-19. There was an age-matched control cohort of 27 patients. The study group VD proved considerably lower compared with the control group. The study group also had higher choriocapillaris flow area values than the control group. Gonzalez-Zamora et al. [25] also studied COVID-19 patients 14 days after hospital discharge. They observed a significantly thinner ganglion cell layer and thicker RNFL on the OCTA of 25 severe bilateral COVID-19 patients than in 25 controls. RNFL thickening was more significant in the COVID-19 cases with CWS than in those without CWS. They also observed an enlarged FAZ area with a lowered foveal VD compared with controls. Abrishami et al. [36] performed OCTA on 31 patients who were at least 2 weeks symptom-free post-COVID-19. Compared with age-matched controls, the COVID-19 cohort had significantly reduced mean VD. In addition, there was evidence of decreased blood flow in the capillary networks.
OCTA Findings in Patients Up to Four Months Post COVID-19
Hazar et al. [38] studied 50 patients without comorbidities 1-month post-discharge for moderate COVID-19 using 3 × 3-mm macula OCTA scans. The results were compared with 55 healthy patients who were of similar age. Lower VDs were significantly correlated with the baseline white blood cell and neutrophil values of the COVID-19 patients. The FAZ was not significantly different from the control group. Savastano et al. [39] also studied COVID-19 patients 1 month after COVID-19 infection via OCTA. They identified a reduced perfusion density and perfusion flow index of the radial peripapillary capillary (RPC) plexus in 80 COVID-19 patients. Their findings suggest an impairment in the blood supply to the peripapillary RNFL in patients following SARS-CoV-2 infection.
Guemes Villahoz et al. [40] performed OCTA in patients 12 weeks after COVID-19 diagnosis. Ninety patients were included, 19 (20%) COVID-19 patients with associated thrombotic events, 47 (49.5%) COVID-19 patients without thrombotic events, and 29 (30.5%) healthy controls. COVID-19 patients presented significantly lower VD than healthy controls. Perfusion density was also significantly decreased. No differences in OCTA parameters were found between COVID-19 patients with and without thrombotic events. Beni et al. [41] compared 51 COVID-19 recovered Iranian patients 40–95 days post-diagnosis with 37 controls. They found that patients with moderate-intensity SARS-CoV-2 pneumonia had altered peripapillary and macular VD compared to healthy subjects. Recovered COVID-19 eyes showed a significant increase in peripapillary retinal nerve fibre (RNFL) thickness and superficial and deep macular VDs in parafoveal and perifoveal regions compared with healthy controls. This study contradicts the studies reporting a reduction in VD in COVID-19 eyes [37, 40, 42].
It is vital to highlight Brantl’s [43] study, which did not find any retinal signs in patients 3 months post COVID-19 recovery. Twenty-one patients were examined 3 months after their initial presentation to the emergency department (14 had been hospitalised and 7 discharged home). They attended an ophthalmological examination 3 months after their COVID-19 illness. They had no ocular involvement at any stage of the disease, and their retinae remained unaffected at follow-up. Szkodny et al. [44] found nothing significant on OCTA in a cohort of 156 COVID patients (the most extensive study population in this review) compared with 98 controls. Patients were 1–4 months post mild to severe diagnoses of COVID-19.
OCTA Findings in Patients Up to Eight Months Post COVID-19
A pilot study by Cennamo et al. [23] found that OCTA showed retinal vascular changes in 40 eyes of 40 subjects 6 months post-discharge for COVID-19 pneumonia. Compared with 40 eyes of age-matched healthy subjects, the study group showed a significant reduction in the SCP, DCP, and RPC VD. OCTA depicted a more significant impairment of the DCP than the SCP in COVID-19 patients compared to controls, as also occurs in diabetic retinopathy [45] and other systemic vasculopathy. The authors hypothesise that COVID-19-related thrombotic microangiopathy could cause vascular perfusion damage to the SCP and RPC, resulting in restriction in axoplasmic flow and subsequent retinal structural loss. Zapata et al.'s [46] study demonstrated that a decreased central retinal VD was related to COVID-19 infection severity. They classified patients discharged home post-COVID-19 into mild (n = 24), moderate (n = 24), and severe (n = 21) disease categories. Their control cohort consisted of 27 age- and sex-matched patients. Garcia et al. [47] re-imaged the same cohort of patients imaged in Zapata et al.'s study 8 months after the baseline visit. This study provides evidence of lower central retinal VD persistence in patients with moderate and severe COVID-19 pneumonia.
Rare Retinal Conditions Reported in Patients with COVID-19
A case report by Gonzalez-Lopez et al. [48] reported a 50-year-old man with bilateral COVID-19 pneumonitis who developed an arcuate visual field defect in his left eye. OCTA revealed multiple focal areas of retinal microvascular ischaemia in the SCP, the largest of which corresponded to the arcuate scotoma observed on visual fields testing. Visual field defects due to retinal microangiopathy may occur during the late phase of COVID-19. Another case report by Ortiz-Seller et al. [49] describes a case of inflammatory chorioretinopathy and Adie's syndrome possibly associated with COVID-19. A 51-year-old woman tested positive for symptomatic COVID-19 infection. Two days later, she complained of retro-orbital pain and difficulty reading. OCT-A revealed bilateral areas of nonperfusion at the choriocapillaris. Spectral-domain OCT demonstrated bilateral inner retinal thinning coupled with focal disturbances of the outer retinal layers. Ultra-wide-field fundus autofluorescence revealed weak hyper-autofluorescence of lesions. The diagnosis of inflammatory chorioretinal disease and Adie's syndrome possibly associated with COVID-19 was established. Some suggest that after viral infection, denervation of the postganglionic supply to the pupil sphincter and the ciliary muscle may occur.
Acute macular neuroretinopathy (AMN) is a rare condition with unknown aetiology, but about 50% of cases are associated with respiratory or influenza-like illness [50]. OCTA in paracentral acute middle maculopathy (PAMM) shows reduced flow in intermediate, deep, and superficial capillary plexus. In AMN, there is a reduction in DCP blood flow. Virgo and Mohamed et al. [51] reported that two patients with SARS-CoV-2 disease presented with a new paracentral scotoma and were found to have PAMM and AMN lesions, indicating that COVID-19 can also cause ischaemic events in the DCP.
OCT Findings in Patients with COVID-19
Several studies evaluated the fundus using OCT. One of the first communications regarding COVID-19 and the retina was a publication by Marinho et al. [52] in the Lancet in May 2020; they reported the presence of CWS, retinal haemorrhages, and hyperreflective plaques in the ganglion cell-inner plexiform layer (GC-IPL) of patients with acute COVID-19 infection. However, subsequent communications from several authors indicated that the hyperreflective plaques were a misinterpretation and could be explained by variation in normal retinal vasculature [53, 54]. Nonetheless, the literature shows that the COVID-19 retina has an 8.86-fold microvasculopathy prevalence [55].
The most common retinal features described include CWS, microhaemorrhages, and venous tortuosity. These signs indicate acute vascular events and retinal ischaemia. Burgos-Blasco et al. [56] studied 29 children who recovered from COVID-19 compared with 61 controls. They reported increased peripapillary retinal nerve fibre layer (RNFL) thickness in the recovered COVID-19 patients. Sim et al. [57] studied 108 patients 16 days post COVID-19 diagnosis. They found that one in nine COVID-19 eyes had retinal microvascular signs on ocular imaging. These retinal microvascular lesions are commonly found in diabetes, hypertension, and cardiovascular disease patients and may reflect the heightened cardiovascular and thrombotic alterations seen in COVID-19. Eleven eyes (5.1%) had hyper-reflective plaques in the GC-IPL layer on OCT. Marinho et al. [52] described four patients who presented with CWS and microhaemorrhages along the retinal arcade, with no symptoms or signs of intraocular inflammation. Oren et al.’s [58] study included 35 COVID-19 patients and 25 age- and sex-matched controls. The thickness of each retinal layer was measured using spectral-domain OCT 14–30 days after COVID-19 symptom onset. The mean central macular thickness was significantly higher in the COVID-19 group than in the control group. The mean values of the ganglion cell layer and inner nuclear layer thickness were significantly less than in the control group. These results could represent COVID-19 retinal involvement.
Individual Case Reports
COVID-19 has also been associated with less common ocular conditions such as inflammatory chorioretinopathy, central retinal artery occlusion (CRAO), optic neuritis, and impending central retinal vein occlusion (CRVO). It is important to note that these disorders have been reported as individual cases, and they have not been observed on a larger scale. Whether or not these findings signify coincidental relationships remains ambivalent. Vascular occlusions are more likely to occur because of the hypercoagulable state associated with COVID-19 and the thrombo-inflammatory immune response [59–61]. In a case reported by Dumitrascu et al. [59], a 48-year-old obese male with severe COVID-19 developed incomplete ophthalmic artery occlusion despite being on apixaban following enoxaparin treatment for deep vein thrombosis. Ortiz-Egea et al. [62] report a case of a 42-year-old male who presented with a left temporal relative scotoma. OCT showed a hyperreflective, placoid band at the GCL and IPL, which spared the outer retina at diagnosis and 1 month later. A COVID-19 diagnosis was made because of a systemic investigation for an ocular abnormality.
Gascon et al. reported a 53-year-old man who presented with acute left eye visual loss, a negative scotoma, and dyschromatopsia. He had COVID-19 contact 8 days prior to symptom onset. Funduscopic examination revealed several retinal haemorrhages. Spectral-domain optical coherence tomography showed lesions consistent with AMN and PAMM. After his presentation, SARS-CoV-2 was confirmed [63]. Olguín-Manríquez et al. evaluated a 35-year-old Hispanic female who presented with monocular vision loss. She tested positive for COVID-19 2 weeks before her presentation. Cross-sectional OCT scans in extrafoveal lesions demonstrated hyper-reflective material in the outer retina. They observed interdigitation zone disruption and hyperreflective material at the foveal depression. Colour fundus photographs showed multiple yellow-white placoid lesions involving the fovea in the right eye. Investigations were consistent with acute posterior multifocal placoid pigment epitheliopathy (APMPPE) in a convalescent COVID-19 patient [64].
Fundus Photography and Fundus Autofluorescence Findings in Patients with COVID-19
There are numerous reports of CWS in patients with COVID-19 [21, 52, 65–67]. Their presence in the eyes of COVID-19 patients could be due to occlusive vasculopathy (as seen in diabetic or hypertensive vascular disease), ACE2 down-regulation by SARS-CoV-2, hyper-coagulopathy, or immune-complex deposition in the vessel walls [68]. Landecho et al. [65] evaluated 27 asymptomatic subjects with multi-modal imaging 14 days after hospital discharge due to COVID-19 bilateral pneumonia. They found CWS in 6 of 27 eyes (22%). Invernizzi et al. [67] screened 54 patients with COVID-19 with fundus photography. They found CWS in 7.4% and retinal haemorrhages in 9.25%. In addition, 27.7% had dilated fundus veins. Retinal vein diameter was significantly larger in patients with COVID-19, and it correlated directly with disease severity and decreased with time. Mean artery and mean vein diameter was higher in the study group. Lani-Louzada et al. [69] found retinal haemorrhages in 3/25 patients (12%) via fundus photography in COVID-19 inpatients. Retinal lesions such as these are not uncommon in severely ill or septic patients, and so they are likely related to the immune response or clinical interventions such as ventilation rather than from SARS-CoV-2 itself.
Pereira et al. [66] reported retinal findings in patients admitted with severe COVID-19. Ten patients (55.6%) showed retinal changes, including macular hyperpigmentation, hard exudates, CWS, retinal sectoral pallor, peripheral retinal haemorrhages, and peripapillary flame-shaped haemorrhages. All patients were on anticoagulants to prevent the prothrombotic condition in severe cases of COVID-19. However, the study team acknowledges the lack of consideration of pre-existing comorbidities, intensive care unit admission, and vasoactive pharmacological support. Therefore, it is equivocal whether these findings might directly result from SARS-CoV-2 infection. However, the study lacked imaging with OCT or OCTA. A cohort of 138 hospitalised patients was imaged 6 days post-COVID-19. Nothing was found on fundus photographs except for one streak haemorrhage found in one eye of a patient, which was likely incidental [70].
Fundus autofluorescence (FAF) imaging provides a topographic mapping of lipofuscin distribution in the retinal pigment epithelium (RPE) cell layer and other fluorophores in the outer retina and sub-neurosensory space. A study by Marinho et al. [71] aimed to investigate FAF findings in COVID-19 patients. Of a cohort of 106 patients, 18 had FAF findings. Hyper-autofluorescence findings were present in 6 patients and hypo-autofluorescence in 14 patients, and 6 patients had mixed pattern lesions. Costa et al. [72] studied 64 hospitalised patients: mild to moderate (n = 7), severe (n = 33), critical (n = 24); N = 2 from the severe cohort showed discrete white-yellowish dots in the posterior pole, leading to hypo-reflective changes at the RPE level, outer segment, and ellipsoid layers. A retrospective case report by Conrady et al. [73] described a 40-year-old female who experienced significant monocular visual loss shortly after contracting COVID-19. Ophthalmic imaging was consistent with white-dot-like outer retinopathy. Her vision, symptoms, and outer retinal changes improved within 10 days of starting steroids. While rare, COVID-19 can cause inflammatory-associated changes in the outer retina and significant vision loss.
Discussion
Ocular involvement is a side effect of SARS-CoV-2 infection. However, retinal involvement has been inconsistently reported, and some study results appear to contradict each other. Studies involving OCTA suggest sub-clinical microvascular effects, but it is not definite whether the effects result from COVID-19 or whether patient demographics and concomitant conditions could influence findings.
Several studies found higher rates of retinal abnormalities in those who suffered severe COVID-19. Patients tend to be older and often have comorbidities such as increased BMI, diabetes, and cardiovascular risk factors. Systemic comorbidities could heighten the retinal microvascular damage caused by COVID-19 [74]. Patients with severe COVID-19 are more likely to have received treatment such as corticosteroids and ventilation, and they are also more likely to suffer from blood gas and pressure changes, increasing the risk of thrombotic events and hypertension [75]. However, microvascular changes in the retina could be a side effect of COVID-19 treatments rather than a direct effect. Notably, CWS and microhaemorrhages are triggered by inflammation, and they are often seen in septic patients. Nonetheless, retinal changes have also been reported in studies involving asymptomatic patients without comorbidities [57].
Many studies report on decreased retinal VD in COVID-19 patients. However, decreased VD could represent standard age-related alterations [76]. Nevertheless, studies involving age- and sex-matched controls have helped add to the validity of retinal microvascular disease as a feature of COVID-19.
The wide range in the time post-COVID-19 when retinal imaging took place could rationalise the inconsistencies in the frequency of abnormal findings between studies. It ranged from 2 weeks post COVID to 8 months of follow-up. In hospitalised patients, OCTA was often carried out after discharge when patients were recovered. Longitudinal studies over time from the acute phase will be necessary to assess vascular outcomes in COVID-19 patients.
It is important to note that this systematic review protocol was not pre-registered in any of the publicly available registries (e.g., PROSPERO). This might have caused a level of bias in the conduct and reporting of the systematic review. Despite our best efforts to manage them, sampling bias and patient demographics such as age, diabetes, and hyperlipidaemia may still be present. OCT-A’s limitations must also be considered. The images and data analysing techniques might lead to different results and must be considered when comparing the results of different studies. Studies also do not have information on retinal status before COVID-19 infection.
Conclusion
This systematic review presents an extensive overview of the various possible retinal features of COVID-19 published to date from around the world. Findings suggest that thrombotic and inflammatory phenomena are occurring in the retina of COVID-19 patients. In addition, OCTA imaging findings in patients with COVID-19 support the hypothesis that the pathophysiology of COVID-19 has a microvascular component. COVID-19 retinal micro-vasculopathy appears to be significant, and the long-term vascular effects are still unknown. Further research is required to analyse the longitudinal evolution of retinal changes over time and their correlation with COVID-19 severity.
Supplementary Information
Below is the link to the electronic supplementary material.
Acknowledgements
We thank the researchers who posted the studies in the public domain.
Funding
No funding or sponsorship was received for this study or the publication of this article.
Authorship
Both authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Author Contributions
Both authors contributed to the study's conception and design. Dr Orlaith McGrath performed the literature search and data analysis. Dr Orlaith McGrath wrote the first draft, and Professor Tariq Aslam critically revised the manuscript. Both authors were involved in the revising, critically appraising and final approval of the manuscript.
Disclosures
Dr Orlaith McGrath declares that they have no personal, financial, commercial, or academic conflict of interest. Tariq M. Aslam has received funding and educational grants from Bayer, Novartis, Roche, Allergan, Laboratoires Thea, Oraya, and Bausch and Lomb, Topcon, Heidelberg, Canon.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any authors.
Data Availability
Data sharing does not apply to this article as no datasets were generated or analysed during the current study.
Contributor Information
Orlaith E. McGrath, Email: orlaith.mcgrath@mft.nhs.uk
Tariq M. Aslam, Email: tariq.aslam@mft.nhs.uk
References
- 1.Asakura H, Ogawa H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int J Hematol. 2021;113(1):45–57. doi: 10.1007/s12185-020-03029-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lowenstein CJ, Solomon SD. Severe COVID-19 is a microvascular disease. Circulation. 2020;142(17):1609–1611. doi: 10.1161/CIRCULATIONAHA.120.050354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sen M, Honavar SG, Sharma N, Sachdev MS. COVID-19 and eye: a review of ophthalmic manifestations of COVID-19. Indian J Ophthalmol. 2021;69(3):488. doi: 10.4103/ijo.IJO_297_21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen L, Li X, Chen M, Feng Y, Xiong C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc Res. 2020;116(6):1097–1100. doi: 10.1093/cvr/cvaa078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Senanayake P, Drazba J, Shadrach K, Milsted A, Rungger-Brandle E, Nishiyama K, et al. Angiotensin II and its receptor subtypes in the human retina. Invest Ophthalmol Vis Sci. 2007;48(7):3301–3311. doi: 10.1167/iovs.06-1024. [DOI] [PubMed] [Google Scholar]
- 6.Ni W, Yang X, Yang D, Bao J, Li R, Xiao Y, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care. 2020;24(1):422. doi: 10.1186/s13054-020-03120-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Casagrande M, Fitzek A, Püschel K, Aleshcheva G, Schultheiss HP, Berneking L, et al. Detection of SARS-CoV-2 in human retinal biopsies of deceased COVID-19 patients. Ocul Immunol Inflamm. 2020;28(5):721–725. doi: 10.1080/09273948.2020.1770301. [DOI] [PubMed] [Google Scholar]
- 8.Gheblawi M, Wang K, Viveiros A, Nguyen Q, Zhong JC, Turner AJ, et al. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: celebrating the 20th anniversary of the discovery of ACE2. Circ Res. 2020;126(10):1456–1474. doi: 10.1161/CIRCRESAHA.120.317015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carvalho-Schneider C, Laurent E, Lemaignen A, Beaufils E, Bourbao-Tournois C, Laribi S, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect. 2021;27(2):258–263. doi: 10.1016/j.cmi.2020.09.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Garrigues E, Janvier P, Kherabi Y, Le Bot A, Hamon A, Gouze H, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. 2020;81(6):e4–e6. doi: 10.1016/j.jinf.2020.08.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–140. doi: 10.1016/S2215-0366(20)30462-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Paterson RW, Brown RL, Benjamin L, Nortley R, Wiethoff S, Bharucha T, et al. The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain. 2020;143(10):3104–3120. doi: 10.1093/brain/awaa240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ting DSW, Tan GSW, Agrawal R, Yanagi Y, Sie NM, Wong CW, et al. Optical coherence tomographic angiography in type 2 diabetes and diabetic retinopathy. JAMA Ophthalmol. 2017;135(4):306–312. doi: 10.1001/jamaophthalmol.2016.5877. [DOI] [PubMed] [Google Scholar]
- 14.Nakayama LF, Bergamo VC, Conti ML, Fares NT, Costa LA, Ambrogini O, et al. The retinal foveal avascular zone as a systemic biomarker to evaluate inflammatory bowel disease control. Int J Retina Vitreous. 2019;5:16. doi: 10.1186/s40942-019-0168-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vadalà M, Castellucci M, Guarrasi G, Terrasi M, La Blasca T, Mulè G. Retinal and choroidal vasculature changes associated with chronic kidney disease. Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1687–1698. doi: 10.1007/s00417-019-04358-3. [DOI] [PubMed] [Google Scholar]
- 16.Zhang YS, Zhou N, Knoll BM, Samra S, Ward MR, Weintraub S, et al. Parafoveal vessel loss and correlation between peripapillary vessel density and cognitive performance in amnestic mild cognitive impairment and early Alzheimer's Disease on optical coherence tomography angiography. PLoS ONE. 2019;14(4):e0214685. doi: 10.1371/journal.pone.0214685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ulhaq ZS, Soraya GV. The prevalence of ophthalmic manifestations in COVID-19 and the diagnostic value of ocular tissue/fluid. Graefes Arch Clin Exp Ophthalmol. 2020;258(6):1351–1352. doi: 10.1007/s00417-020-04695-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Seah I, Agrawal R. Can the coronavirus disease 2019 (COVID-19) affect the eyes? A review of coronaviruses and ocular implications in humans and animals. Ocul Immunol Inflamm. 2020;28(3):391–395. doi: 10.1080/09273948.2020.1738501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sindhuja K, Lomi N, Asif MI, Tandon R. Clinical profile and prevalence of conjunctivitis in mild COVID-19 patients in a tertiary care COVID-19 hospital: a retrospective cross-sectional study. Indian J Ophthalmol. 2020;68(8):1546–1550. doi: 10.4103/ijo.IJO_1319_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wu P, Duan F, Luo C, Liu Q, Qu X, Liang L, et al. Characteristics of ocular findings of patients with coronavirus disease 2019 (COVID-19) in Hubei Province. China JAMA Ophthalmol. 2020;138(5):575–578. doi: 10.1001/jamaophthalmol.2020.1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pirraglia MP, Ceccarelli G, Cerini A, Visioli G, d'Ettorre G, Mastroianni CM, et al. Retinal involvement and ocular findings in COVID-19 pneumonia patients. Sci Rep. 2020;10(1):17419. doi: 10.1038/s41598-020-74446-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mazzotta C, Giancipoli E. Anterior acute uveitis report in a SARS-CoV-2 patient managed with adjunctive topical antiseptic prophylaxis preventing 2019-nCoV spread through the ocular surface route. Int Med Case Rep J. 2020;13:513–520. doi: 10.2147/IMCRJ.S260252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cennamo G, Reibaldi M, Montorio D, D'Andrea L, Fallico M, Triassi M. Optical coherence tomography angiography features in post-COVID-19 pneumonia patients: a pilot study. Am J Ophthalmol. 2021;227:182–190. doi: 10.1016/j.ajo.2021.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Spaide RF, Fujimoto JG, Waheed NK, Sadda SR, Staurenghi G. Optical coherence tomography angiography. Prog Retin Eye Res. 2018;64:1–55. doi: 10.1016/j.preteyeres.2017.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.González-Zamora J, Bilbao-Malavé V, Gándara E, Casablanca-Piñera A, Boquera-Ventosa C, Landecho MF, et al. Retinal microvascular impairment in COVID-19 bilateral pneumonia assessed by optical coherence tomography angiography. Biomedicines. 2021;9(3):247. doi: 10.3390/biomedicines9030247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Garcia-Vidal C, Moreno-García E, Hernández-Meneses M, Puerta-Alcalde P, Chumbita M, Garcia-Pouton N, et al. Personalized therapy approach for hospitalized patients with COVID-19. Clin Infect Dis. 2020;74:127–132. doi: 10.1093/cid/ciaa964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sen S, Kannan NB, Kumar J, Rajan RP, Kumar K, Baliga G, et al. Retinal manifestations in patients with SARS-CoV-2 infection and pathogenetic implications: a systematic review. Int Ophthalmol. 2022;42(1):323–336. doi: 10.1007/s10792-021-01996-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Patton N, Aslam T, Macgillivray T, Pattie A, Deary IJ, Dhillon B. Retinal vascular image analysis as a potential screening tool for cerebrovascular disease: a rationale based on homology between cerebral and retinal microvasculatures. J Anat. 2005;206(4):319–348. doi: 10.1111/j.1469-7580.2005.00395.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fruttiger M. Development of the retinal vasculature. Angiogenesis. 2007;10(2):77–88. doi: 10.1007/s10456-007-9065-1. [DOI] [PubMed] [Google Scholar]
- 30.Kur J, Newman EA, Chan-Ling T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog Retin Eye Res. 2012;31(5):377–406. doi: 10.1016/j.preteyeres.2012.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Martin VA. Disseminated intravascular coagulopathy. Trans Ophthalmol Soc U K. 1978;98(4):506–507. [PubMed] [Google Scholar]
- 32.Al-Ani F, Chehade S, Lazo-Langner A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb Res. 2020;192:152–160. doi: 10.1016/j.thromres.2020.05.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Zhang Y, Xiao M, Zhang S, Xia P, Cao W, Jiang W, et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. N Engl J Med. 2020;382(17):e38. doi: 10.1056/NEJMc2007575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cao D, Yang D, Huang Z, Zeng Y, Wang J, Hu Y, et al. Optical coherence tomography angiography discerns preclinical diabetic retinopathy in eyes of patients with type 2 diabetes without clinical diabetic retinopathy. Acta Diabetol. 2018;55:469–477. doi: 10.1007/s00592-018-1115-1. [DOI] [PubMed] [Google Scholar]
- 35.Bertoli F, Veritti D, Danese C, Samassa F, Sarao V, Rassu N, et al. Ocular findings in COVID-19 patients: a review of direct manifestations and indirect effects on the eye. J Ophthalmol. 2020;2020:4827304. doi: 10.1155/2020/4827304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Abrishami M, Emamverdian Z, Shoeibi N, Omidtabrizi A, Daneshvar R, Saeidi Rezvani T, et al. Optical coherence tomography angiography analysis of the retina in patients recovered from COVID-19: a case-control study. Can J Ophthalmol. 2021;56(1):24–30. doi: 10.1016/j.jcjo.2020.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Turker IC, Dogan CU, Guven D, Kutucu OK, Gul C. Optical coherence tomography angiography findings in patients with COVID-19. Can J Ophthalmol. 2021;56(2):83–87. doi: 10.1016/j.jcjo.2020.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hazar L, Karahan M, Vural E, Ava S, Erdem S, Dursun ME, et al. Macular vessel density in patients recovered from COVID 19. Photodiagnosis Photodyn Ther. 2021;34:1267. doi: 10.1016/j.pdpdt.2021.102267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Savastano A, Crincoli E, Savastano MC, Younis S, Gambini G, De Vico U, et al. Peripapillary retinal vascular involvement in early post-COVID-19 patients. J Clin Med. 2020;9(9):2895. doi: 10.3390/jcm9092895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Guemes-Villahoz N, Burgos-Blasco B, Vidal-Villegas B, Donate-López J, de la Muela MH, López-Guajardo L, et al. Reduced macular vessel density in COVID-19 patients with and without associated thrombotic events using optical coherence tomography angiography. Graefes Arch Clin Exp Ophthalmol. 2021;259(8):2243–2249. doi: 10.1007/s00417-021-05186-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Beni AN, Dehghani A, Kianersi F, Ghanbari H, Habibi Z, Memarzadeh E, et al. Retinal findings of COVID-19 patients using ocular coherence tomography angiography two to three months after infection: ocular appearance recovered COVID-19 patient. Photodiagnosis Photodyn Ther. 2022;38:102726. doi: 10.1016/j.pdpdt.2022.102726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cennamo G, Reibaldi M, Montorio D, D'Andrea L, Fallico M, Triassi M. Optical coherence tomography angiography features in post COVID-19 pneumonia patients: a pilot study. Am J Ophthalmol. 2021;227:182–190. doi: 10.1016/j.ajo.2021.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Brantl V, Schworm B, Weber G, Schiefelbein J, Kreutzer TC, Michalakis S, et al. Long-term ocular damage after recovery from COVID-19: lack of evidence at three months. BMC Ophthalmol. 2021;21(1):421. doi: 10.1186/s12886-021-02179-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Szkodny D, Wylęgała E, Sujka-Franczak P, Chlasta-Twardzik E, Fiolka R, Tomczyk T, et al. Retinal OCT findings in patients after COVID infection. J Clin Med. 2021;10(15):3233. doi: 10.3390/jcm10153233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Scarinci F, Picconi F, Virgili G, Varano M, Giorno P, Frontoni S, et al. Microvascular impairment as a biomarker of diabetic retinopathy progression in the long-term follow up in type 1 diabetes. Sci Rep. 2020;10(1):18266. doi: 10.1038/s41598-020-75416-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Zapata M, Banderas García S, Sánchez-Moltalvá A, Falcó A, Otero-Romero S, Arcos G, et al. Retinal microvascular abnormalities in patients after COVID-19 depending on disease severity. Br J Ophthalmol. 2020;106:559–563. doi: 10.1136/bjophthalmol-2020-317953. [DOI] [PubMed] [Google Scholar]
- 47.Banderas García S, Aragón D, Azarfane B, Trejo F, Garrell-Salat X, Sánchez-Montalvá A, et al. Persistent reduction of retinal microvascular vessel density in patients with moderate and severe COVID-19 disease. BMJ Open Ophthalmol. 2022;7(1):e000867. doi: 10.1136/bmjophth-2021-000867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gonzalez-Lopez JJ, Felix Espinar B, Ye-Zhu C. Symptomatic retinal microangiophaty in a patient with coronavirus disease 2019 (COVID-19): single case report. Ocul Immunol Inflamm. 2020;29:642–644. doi: 10.1080/09273948.2020.1852260. [DOI] [PubMed] [Google Scholar]
- 49.Ortiz-Seller A, Martínez Costa L, Hernández-Pons A, Valls Pascual E, Solves Alemany A, Albert-Fort M. Ophthalmic and neuro-ophthalmic manifestations of coronavirus disease 2019 (COVID-19) Ocul Immunol Inflamm. 2020;28(8):1285–1289. doi: 10.1080/09273948.2020.1817497. [DOI] [PubMed] [Google Scholar]
- 50.Bhavsar KV, Lin S, Rahimy E, Joseph A, Freund KB, Sarraf D, et al. Acute macular neuroretinopathy: a comprehensive review of the literature. Surv Ophthalmol. 2016;61:538–565. doi: 10.1016/j.survophthal.2016.03.003. [DOI] [PubMed] [Google Scholar]
- 51.Virgo J, Mohamed M. Paracentral acute middle maculopathy and acute macular neuroretinopathy following SARS-CoV-2 infection. Eye (London) 2020;34(12):2352–2353. doi: 10.1038/s41433-020-1069-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Marinho PM, Marcos AAA, Romano AC, Nascimento H, Belfort R. Retinal findings in patients with COVID-19. Lancet. 2020;395(10237):1610. doi: 10.1016/S0140-6736(20)31014-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Vavvas DG, Sarraf D, Sadda SR, Eliott D, Ehlers JP, Waheed NK, et al. Concerns about the interpretation of OCT and fundus findings in COVID-19 patients in recent Lancet publication. Eye (Lond) 2020;34(12):2153–2154. doi: 10.1038/s41433-020-1084-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ouyang P, Zhang X, Peng Y, Jiang B. Seeking clarity on retinal findings in patients with COVID-19. Lancet. 2020;396(10254):e35. doi: 10.1016/S0140-6736(20)31921-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Teo KY, Invernizzi A, Staurenghi G, Cheung CMG. COVID-19-related retinal micro-vasculopathy: a review of current evidence. Am J Ophthalmol. 2022;235:98–110. doi: 10.1016/j.ajo.2021.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Burgos-Blasco B, Güemes-Villahoz N, Morales-Fernandez L, Callejas-Caballero I, Perez-Garcia P, Donate-Lopez J, et al. Retinal nerve fibre layer and ganglion cell layer changes in children who recovered from COVID-19: a cohort study. Arch Dis Child. 2022;107(2):175–179. doi: 10.1136/archdischild-2021-321803. [DOI] [PubMed] [Google Scholar]
- 57.Sim R, Cheung G, Ting D, Wong E, Wong TY, Yeo I, et al. Retinal microvascular signs in COVID-19. Br J Ophthalmol. 2021 doi: 10.1136/bjophthalmol-2020-318236. [DOI] [PubMed] [Google Scholar]
- 58.Oren B, Aksoy Aydemır G, Aydemır E, Atesoglu HI, Goker YS, Kızıltoprak H, et al. Quantitative assessment of retinal changes in COVID-19 patients. Clin Exp Optom. 2021;104:717–722. doi: 10.1080/08164622.2021.1916389. [DOI] [PubMed] [Google Scholar]
- 59.Dumitrascu OM, Volod O, Bose S, Wang Y, Biousse V, Lyden PD. Acute ophthalmic artery occlusion in a COVID-19 patient on apixaban. J Stroke Cerebrovasc Dis. 2020;29(8):1049. doi: 10.1016/j.jstrokecerebrovasdis.2020.104982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Acharya S, Diamond M, Anwar S, Glaser A, Tyagi P. Unique case of central retinal artery occlusion secondary to COVID-19 disease. IDCases. 2020;21:e00867. doi: 10.1016/j.idcr.2020.e00867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Sheth JU, Narayanan R, Goyal J, Goyal V. Retinal vein occlusion in COVID-19: a novel entity. Indian J Ophthalmol. 2020;68(10):2291–2293. doi: 10.4103/ijo.IJO_2380_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ortiz-Egea JM, Ruiz-Medrano J, Ruiz-Moreno JM. Retinal imaging study diagnoses in COVID-19: a case report. J Med Case Rep. 2021;15(1):15. doi: 10.1186/s13256-020-02620-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Gascon P, Briantais A, Bertrand E, Ramtohul P, Comet A, Beylerian M, et al. Covid-19-associated retinopathy: a case report. Ocul Immunol Inflamm. 2020;28(8):1293–1297. doi: 10.1080/09273948.2020.1825751. [DOI] [PubMed] [Google Scholar]
- 64.Olguín-Manríquez F, Cernichiaro-Espinosa L, Olguín-Manríquez A, Manríquez-Arias R, Flores-Villalobos EO, Kawakami-Campos PA. Unilateral acute posterior multifocal placoid pigment epitheliopathy in a convalescent COVID-19 patient. Int J Retina Vitreous. 2021;7(1):41. doi: 10.1186/s40942-021-00312-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Landecho MF, Yuste JR, Gándara E, Sunsundegui P, Quiroga J, Alcaide AB, et al. COVID-19 retinal microangiopathy as an in vivo biomarker of systemic vascular disease? J Intern Med. 2021;289(1):116–120. doi: 10.1111/joim.13156. [DOI] [PubMed] [Google Scholar]
- 66.Pereira LA, Soares LCM, Nascimento PA, Cirillo LRN, Sakuma HT, Veiga GLD, et al. Retinal findings in hospitalised patients with severe COVID-19. Br J Ophthalmol. 2022;106(1):102–105. doi: 10.1136/bjophthalmol-2020-317576. [DOI] [PubMed] [Google Scholar]
- 67.Invernizzi A, Torre A, Parrulli S, Zicarelli F, Schiuma M, Colombo V, et al. Retinal findings in patients with COVID-19: Results from the SERPICO-19 study. EClinicalMedicine. 2020;27:100550. doi: 10.1016/j.eclinm.2020.100550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Markan A, Bansal R, Gautam N, Ahuja C, Agarwal A, Katoch D, et al. Longitudinal analysis of cotton wool spots in COVID-19 with high-resolution spectral domain optical coherence tomography and optical coherence tomography angiography. Clin Experiment Ophthalmol. 2021;49(4):392–395. doi: 10.1111/ceo.13919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Lani-Louzada R, Ramos C, Cordeiro RM, Sadun AA. Retinal changes in COVID-19 hospitalized cases. PLoS ONE. 2020;15(12):e0243346. doi: 10.1371/journal.pone.0243346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Bypareddy R, Rathod BLS, Shilpa YD, Hithashree HR, Nagaraj KB, Hemalatha BC, et al. Fundus evaluation in COVID-19 positives with non-severe disease. Indian J Ophthalmol. 2021;69(5):1271–1274. doi: 10.4103/ijo.IJO_3227_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Marinho PM, Marcos AAA, Branco AMC, Mourad WM, Sakamoto V, Romano AC, et al. Retinal autofluorescence findings after COVID-19. Int J Retina Vitreous. 2021;7(1):71. doi: 10.1186/s40942-021-00341-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Costa Í, Bonifácio LP, Bellissimo-Rodrigues F, Rocha EM, Jorge R, Bollela VR, et al. Ocular findings among patients surviving COVID-19. Sci Rep. 2021;11(1):11085. doi: 10.1038/s41598-021-90482-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Conrady CD, Faia LJ, Gregg KS, Rao RC. Coronavirus-19-associated retinopathy. Ocul Immunol Inflamm. 2021;29:675–676. doi: 10.1080/09273948.2021.1894456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Guemes-Villahoz N, Burgos-Blasco B, Donate-Lopez J, Garcia-Feijoo J. Retinal findings in COVID-19 patients with diabetes mellitus. Diabetes Res Clin Pract. 2020;168:108395. doi: 10.1016/j.diabres.2020.108395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Malas MB, Naazie IN, Elsayed N, Mathlouthi A, Marmor R, Clary B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: a systematic review and meta-analysis. EClinicalMedicine. 2020;29:100639. doi: 10.1016/j.eclinm.2020.100639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Lin Y, Jiang H, Liu Y, Rosa Gameiro G, Gregori G, Dong C, et al. Age-related alterations in retinal tissue perfusion and volumetric vessel density. Invest Ophthalmol Vis Sci. 2019;60(2):685–693. doi: 10.1167/iovs.18-25864. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data sharing does not apply to this article as no datasets were generated or analysed during the current study.