

Key Points
Question
Does prone positioning reduce endotracheal intubation in adults who were awake and not intubated and who had hypoxemic respiratory failure from COVID-19?
Findings
In this randomized clinical trial that included 400 adults with acute hypoxemic respiratory failure from COVID-19, awake prone positioning compared with usual care resulted in endotracheal intubation at 30 days in 34.1% vs 40.5% of participants, respectively. Although the hazard ratio was 0.81, the result was not statistically significant.
Meaning
Although the findings do not support prone positioning in this setting, the effect size for the primary study outcome was imprecise and does not exclude a clinically important benefit.
Abstract
Importance
The efficacy and safety of prone positioning is unclear in nonintubated patients with acute hypoxemia and COVID-19.
Objective
To evaluate the efficacy and adverse events of prone positioning in nonintubated adult patients with acute hypoxemia and COVID-19.
Design, Setting, and Participants
Pragmatic, unblinded randomized clinical trial conducted at 21 hospitals in Canada, Kuwait, Saudi Arabia, and the US. Eligible adult patients with COVID-19 were not intubated and required oxygen (≥40%) or noninvasive ventilation. A total of 400 patients were enrolled between May 19, 2020, and May 18, 2021, and final follow-up was completed in July 2021.
Intervention
Patients were randomized to awake prone positioning (n = 205) or usual care without prone positioning (control; n = 195).
Main Outcomes and Measures
The primary outcome was endotracheal intubation within 30 days of randomization. The secondary outcomes included mortality at 60 days, days free from invasive mechanical ventilation or noninvasive ventilation at 30 days, days free from the intensive care unit or hospital at 60 days, adverse events, and serious adverse events.
Results
Among the 400 patients who were randomized (mean age, 57.6 years [SD, 12.83 years]; 117 [29.3%] were women), all (100%) completed the trial. In the first 4 days after randomization, the median duration of prone positioning was 4.8 h/d (IQR, 1.8 to 8.0 h/d) in the awake prone positioning group vs 0 h/d (IQR, 0 to 0 h/d) in the control group. By day 30, 70 of 205 patients (34.1%) in the prone positioning group were intubated vs 79 of 195 patients (40.5%) in the control group (hazard ratio, 0.81 [95% CI, 0.59 to 1.12], P = .20; absolute difference, −6.37% [95% CI, −15.83% to 3.10%]). Prone positioning did not significantly reduce mortality at 60 days (hazard ratio, 0.93 [95% CI, 0.62 to 1.40], P = .54; absolute difference, −1.15% [95% CI, −9.40% to 7.10%]) and had no significant effect on days free from invasive mechanical ventilation or noninvasive ventilation at 30 days or on days free from the intensive care unit or hospital at 60 days. There were no serious adverse events in either group. In the awake prone positioning group, 21 patients (10%) experienced adverse events and the most frequently reported were musculoskeletal pain or discomfort from prone positioning (13 of 205 patients [6.34%]) and desaturation (2 of 205 patients [0.98%]). There were no reported adverse events in the control group.
Conclusions and Relevance
In patients with acute hypoxemic respiratory failure from COVID-19, prone positioning, compared with usual care without prone positioning, did not significantly reduce endotracheal intubation at 30 days. However, the effect size for the primary study outcome was imprecise and does not exclude a clinically important benefit.
Trial Registration
ClinicalTrials.gov Identifier: NCT04350723
This pragmatic randomized clinical trial compares the efficacy and adverse events of prone positioning in adults not intubated with acute hypoxemia and COVID-19 vs patients receiving usual care without prone positioning.
Introduction
Hospitalizations due to COVID-19 strained critical care resources internationally.1,2,3 Surges limited the availability of resources for critically ill patients, emphasizing a need for practical, widely available, and affordable interventions. Awake prone positioning arose as a potentially useful intervention to investigate during the pandemic.
Prone positioning has been used since the 1970s in patients undergoing invasive mechanical ventilation for acute respiratory distress syndrome.4 Observational studies showed that prone positioning may result in increased lung volume,5 homogenized pleural pressure,6 and reduced shunting.7 Furthermore, randomized clinical trials found prone positioning to be associated with a lower risk of death in patients undergoing invasive mechanical ventilation for moderate to severe acute respiratory distress syndrome (relative risk, 0.74 [95% CI, 0.56-0.99]).8,9
Awake prone positioning has been used widely for patients with COVID-19. Prior to the pandemic, there were no randomized clinical trials examining the effects of prone positioning in patients who were awake and not intubated and who had hypoxemic respiratory failure.10 A meta-analysis of 2 randomized clinical trials and 12 observational studies found no association of awake prone positioning with the risk of endotracheal intubation in patients with COVID-19.11 In contrast, a meta-trial of 6 randomized clinical trials enrolling patients with COVID-19 found awake prone positioning to be safe and associated with a reduction in a composite outcome of endotracheal intubation or death within 28 days of enrollment.12 However, the most current practice guideline concluded that there is insufficient evidence to issue a clinical recommendation on this strategy.13
The COVI-PRONE (Awake Prone Position in Hypoxemic Patients with Coronavirus Disease 19) trial aimed to assess the efficacy and adverse events of awake prone positioning in patients who were not intubated and who had COVID-19 with hypoxemic respiratory failure.
Methods
Trial Design and Oversight
We conducted a pragmatic, unblinded randomized clinical trial at 21 hospitals in Canada, Kuwait, Saudi Arabia, and the US. Investigators obtained approval from their local research ethics review boards. The trial protocol (Supplement 1) and statistical analysis plan (Supplement 2) were published prior to trial completion.14 An independent data and safety monitoring committee reviewed the interim analysis at 50% recruitment of the original sample size and provided recommendations to the trial steering committee. Study research coordinators obtained a priori or deferred consent for all enrolled patients. Screening and enrollment occurred between May 19, 2020, and May 18, 2021 (eTable 1 and eFigure 1 in Supplement 3).
Patients
The trial included patients aged 18 years or older who were not intubated, who had suspected or confirmed COVID-19, and who required at least 40% oxygen (via low- or high-flow oxygen devices) or noninvasive positive pressure ventilation and were being treated in an intensive care unit (ICU) or a monitored acute care unit. Patients were excluded from the trial if they (1) had received invasive mechanical ventilation, (2) had contraindications to prone positioning, (3) were at risk of complications from prone positioning, or (4) had been self-prone positioning prior to enrollment. Details of the eligibility criteria appear in the eMethods in Supplement 3. Racial and ethnic categorization was used to reflect international enrollment and provide a description of racial and ethnic diversity in this study. Research coordinators abstracted race and ethnicity using prespecified fixed categories from medical records when available.
Randomization
Using a web-based randomization system with undisclosed variable block sizes of 2, 4, and 6, allocation was 1:1 and stratified by hospital and by ratio of oxygen saturation as measured by pulse oximetry (Spo2) to fraction of inspired oxygen (Fio2) of greater than 150 or of 150 or less. The nature of the intervention precluded blinding of participating patients, families, the health care team, or research staff.
Study Intervention
Patients randomized to the intervention group underwent awake prone positioning. The target duration of prone positioning was 8 h/d to 10 h/d with 2 to 3 breaks (1-2 hours each), if needed (Figure 1). Daily prone positioning sessions were protocolized to continue until 1 of the following stopping criteria was met: a relative improvement in the Fio2 requirement by 40% from the baseline value that was sustained for 24 hours; endotracheal intubation; or discharge from the ICU or acute care unit. The treating team supervised patients who could move themselves during the prone positioning process and assisted the patients with positioning as required.
Figure 1. Screening, Enrollment, Randomization, and Inclusion in Analysis in the COVI-PRONE Trial.

COVI-PRONE, Awake Prone Position in Hypoxemic Patients with Coronavirus Disease 19.
aNo data were collected on screened patients found to be ineligible.
bCentral web-based randomization stratified by hospital and by ratio of oxygen saturation as measured by pulse oximetry to fraction of inspired oxygen of greater than 150 or of 150 or less.
Patients randomized to the control group, and their treating team, were informed of their group assignment. Nurses instructed patients not to position themselves in the prone position.
Patients in the intervention and control groups received usual care at the discretion of the treating team. Daily data collection on co-interventions continued until the intervention stopping criteria were met. In both groups, nurses used prone positioning logs to document the number of prone positioning hours every day. Daily documentation of prone positioning hours continued until the day of meeting stopping criteria.
Study Outcomes
The primary outcome was endotracheal intubation within 30 days of randomization. The secondary outcomes included mortality at 60 days, days free from invasive mechanical ventilation or noninvasive ventilation at 30 days, days free from the ICU or hospital at 60 days, and adverse events. In this study, adverse events included both adverse events and serious adverse events. Further details appear in eTable 2 in Supplement 3.
Sample Size Calculation
The original target sample size was 350 participants based on an assumption for an estimated absolute risk reduction of 15%, an endotracheal intubation rate of 60% in the control group, a power of 80%, and a 2-sided α level of 5% (α = .05). Due to lack of preexisting studies to inform the sample size calculation, these assumptions were based on discussion and consensus among steering committee members.
As the management of COVID-19 evolved, the threshold for endotracheal intubation of COVID-19 patients changed, and guidelines suggested a trial of other respiratory support modalities prior to endotracheal intubation.13 Therefore, the steering committee decided to increase the study sample size to 400 participants. This sample size increase allowed 80% power to detect an absolute reduction of 13.5% for endotracheal intubation, assuming an endotracheal intubation risk of 45% in the control group.
Due to the lack of evidence to inform the study sample size calculation, the decision to increase the sample size from 350 to 400 participants was based on discussion and consensus among the steering committee members; all members were blinded to the study outcomes and interim analysis results. In addition, this change was approved by the independent data and safety monitoring committee and by the local research ethics review boards.
Statistical Analysis
Patient baseline characteristics are reported as percentages for categorical variables and as means (SDs) or medians (IQRs) for continuous variables as appropriate. The primary analyses were conducted with patients analyzed according to their randomization group; the full analysis set included all randomized patients. There were no missing outcome data. The main analysis for the primary outcome (ie, endotracheal intubation within 30 days of randomization), mortality at 60 days, and a post hoc composite outcome of endotracheal intubation or death at 30 days was an unadjusted Cox proportional hazards regression analysis with the results reported as hazard ratios (HRs) with 95% CIs. Graphical diagnostics based on the scaled Schoenfeld residuals showed that the proportionality assumption was met. In addition, we constructed Kaplan-Meier survival curves, including log-rank tests. To assess the effect of competing risk of death, we used the Fine and Gray subdistribution hazard model for the primary outcome.15
We conducted preplanned secondary analyses for binary outcomes (ie, endotracheal intubation at 30 days and mortality at 60 days) comparing the proportion of patients in the 2 groups using the χ2 test or the Fisher exact test as appropriate and presented the results as relative risks and 95% CIs. We also conducted a preplanned secondary per-protocol analysis excluding patients with protocol deviations (ie, patients who did not participate in prone positioning in the intervention group and patients who participated in any prone positioning in the control group). To assess hospital site effect, we conducted a post hoc mixed-effects modeling analysis using hospital site as a random effect.
The primary analysis method for the continuous outcomes (ie, days free from invasive mechanical ventilation or noninvasive ventilation and days free from the ICU or hospital) was an unadjusted linear regression analysis in which the main independent variable was group allocation. In addition, for all study outcomes, we conducted secondary analyses adjusting for stratification variables (ie, recruiting hospital site and severity of hypoxemia). All primary and secondary analyses of the study outcomes used 2-sided testing and an α = .05.
We compared the primary outcome in prespecified subgroups with prespecified hypotheses and reported the corresponding P value for the interaction. In addition, we reported the false discovery rate to account for multiplicity by calculating the expected proportion of tests with false-positive results at a specified rank for a set of tests.16 Predefined subgroup analyses focused on the severity of hypoxemia (Spo2:Fio2 ≤ 150 vs Spo2:Fio2 > 150) and the threshold used was based on the median Spo2:Fio2 in a case series that was available during the trial design,17 the mode of respiratory support at baseline (low-flow oxygen [ie, oxygen delivery other than via high-flow nasal cannula or noninvasive ventilation regardless of the fraction of oxygen delivered to the patient], high-flow oxygen, or noninvasive positive pressure ventilation); age (<70 years vs ≥70 years); and sex (male or female). All analyses were conducted using SAS version 9.4 (SAS Institute Inc).
Results
During the study period, a total of 4229 patients were screened and, of these, 595 met the eligibility criteria and 400 were randomized (205 to the awake prone positioning group and 195 to the control group; Figure 1). Final follow-up was completed in July 2021. Patient characteristics at randomization were similar between groups. The mean age was 56.8 years (SD, 12.5 years) in the prone positioning group and 58.3 years (SD, 13.2 years) in the control group and the mean body mass index (calculated as weight in kilograms divided by height in meters squared) was 29.7 (SD, 4.7) and 29.5 (SD, 4.9), respectively (Table 1 and eTable 3 in Supplement 3).
Table 1. Baseline Characteristics of the Patients.
| Prone positioning (n = 205) | Control (n = 195) | |
|---|---|---|
| Age, mean (SD), y | 56.8 (12.5) | 58.3 (13.2) |
| Sex, No. (%) | ||
| Male | 149 (73) | 134 (69) |
| Female | 56 (27) | 61 (31) |
| Body mass index, mean (SD)a | 29.7 (4.7) | 29.5 (4.9) |
| Glasgow Coma Scale score ≥14, No. (%)b | 205 (100) | 193 (99) |
| Race, No. (%)c | (n = 181) | (n = 180) |
| Alaska Native/American Indian | 1 (<1) | 2 (1) |
| Asian | 40 (22) | 36 (20) |
| Black | 3 (2) | 3 (2) |
| Middle Eastern | 86 (48) | 94 (52) |
| White | 51 (28) | 45 (25) |
| Country of enrollment, No. (%) | ||
| Canada | 84 (41) | 77 (40) |
| Kuwait | 26 (13) | 23 (12) |
| Saudi Arabia | 80 (39) | 82 (42) |
| US | 15 (7) | 13 (7) |
| Confirmed COVID-19, No. (%)d | 199 (97) | 189 (97) |
| Time from hospital admission to randomization, median (IQR), d | 1.6 (0.9-3.2) | 1.5 (0.8-3.7) |
| Severity of hypoxemia measured by Spo2:Fio2, No. (%)e | ||
| ≤150 | 121 (59) | 117 (60) |
| >150 | 84 (41) | 78 (40) |
| Spo2:Fio2, median (IQR) | 132 (103-174) | 136 (110-181) |
| Fio2, median (IQR), % | 70 (55-90) | 70 (52-90) |
| Oxygenation mode, No. (%) | ||
| High flow | 148 (72) | 132 (68) |
| Low flowf | 45 (22) | 43 (22) |
| Noninvasive positive pressure ventilation | 12 (6) | 20 (10) |
| Preexisting condition, No. (%)g | ||
| Chronic cardiovascular disease | 101 (49) | 102 (52) |
| Hypertension | 94 (46) | 96 (49) |
| Diabetes | 83 (40) | 76 (39) |
| Chronic pulmonary disease | 23 (11) | 25 (13) |
| Chronic kidney disease | 15 (7) | 12 (6) |
| No comorbidities, No. (%) | 47 (23) | 41 (21) |
| Pharmacological intervention, No. (%) | ||
| Corticosteroids | 194 (95) | 186 (95) |
| Prophylactic-dose anticoagulantsh | 158 (77) | 155 (79) |
| Antibiotics | 163 (80) | 154 (79) |
| Tocilizumab | 36 (18) | 33 (17) |
| Therapeutic-dose anticoagulantsi | 23 (11) | 24 (12) |
Abbreviations: Fio2, fraction of inspired oxygen; Spo2, oxygen saturation as measured by pulse oximetry.
Calculated as weight in kilograms divided by height in meters squared.
Measures consciousness by using eye, verbal, and motor responsiveness. Scores range from 3 to 15; higher scores reflect better levels of consciousness.
Race and ethnicity were not documented in the patient’s medical record for 16 patients in the prone positioning group and 12 patients in the control group. The documented race or ethnicity was not captured by the prespecified race and ethnicity categories in the study’s baseline case report form for 8 patients in the prone positioning group and 3 patients in the control group.
Defined as a positive polymerase chain reaction for SARS-CoV-2.
A small case series showed a median level of 150 for Spo2:Fio2 in patients undergoing prone positioning. Spo2:Fio2 was used instead of the more commonly used Pao2:Fio2 to avoid mandating arterial blood gases in every patient during the pandemic.
Included oxygen delivery via any device other than high-flow nasal cannula or noninvasive ventilation regardless of the fraction of oxygen delivered to the patient.
Abstracted from the patient’s chart whenever available. The most commonly reported comorbidities in patients with COVID-19 were selected based on the available literature at the time of the trial design.
Low-molecular-weight heparin or unfractionated heparin. Additional details appear in eTable 2 in Supplement 3.
Low-molecular-weight heparin, unfractionated heparin, warfarin, or direct oral anticoagulants. Additional details appear in eTable 2 in Supplement 3.
Most enrolled patients had confirmed COVID-19 at the time of randomization (97.0%). The median percentage of Fio2 at randomization was 70% (IQR, 55%-90%) in the awake prone positioning group and 70% (IQR, 52%-90%) in the control group and the median Spo2:Fio2 was 132 (IQR, 103-174) and 136 (IQR, 110-181), respectively. Approximately 60% of enrolled patients had an Spo2:Fio2 of 150 or less. The most prevalent comorbidities at baseline were chronic hypertension (48%) and diabetes (40%). Most patients received corticosteroids (95%) and prophylactic-dose anticoagulants (78%) at the time of enrollment.
Prone Positioning Intervention
In the awake prone positioning group, the median duration of prone positioning was 5.0 hours (IQR, 2.0-8.0 hours) on day 1. In the first 4 days after randomization, the median duration of prone positioning was 4.8 h/d (IQR, 1.8-8.0 h/d) in the awake prone positioning group vs 0 h/d (IQR, 0-0 h/d) in the control group (Figure 2 and eTable 4 in Supplement 3) and the mean between-group difference was 4.48 h/d (95% CI, 3.90-5.06 h/d; P < .001).
Figure 2. Duration of Awake Prone Positioning by Study Group.

The box plots display the median duration of prone positioning. The line represents the median, the box edges represent the first and third quartiles, the whiskers represent the most extreme values up to 1.5 × IQR, and the dots represent the more extreme values.
In the awake prone positioning group, the median number of prone positioning days was 3 (IQR, 1-5 days). Of the 205 patients in the prone positioning group, 21 (10.2%) did not undergo any prone positioning after randomization, mostly due to patient preference. Additional details appear in eTable 5 in Supplement 3. In the control group, 38 patients (19.5%) underwent prone positioning after randomization, mainly at the request of the care treating team or patient preference (eTable 5 in Supplement 3). The median duration of prone positioning for the 38 patients who underwent prone positioning in the control group was 0.9 h/d (IQR, 0.3-3.5 h/d). The duration of daily prone positioning and patient adherence appear in eFigures 2-4 in Supplement 3.
During the study intervention period, the use of pharmacological agents such as corticosteroids, immunomodulators, anticoagulants, vasoactive agents, and antivirals was similar between groups (eTables 3-4 and eTable 6 in Supplement 3). After randomization, 143 patients (69.8%) in the prone positioning group and 122 patients (62.6%) in the control group received low-flow oxygen and 176 patients (85.5%) vs 165 patients (84.6%), respectively, received high-flow oxygen. In contrast, 53 patients (25.9%) in the prone positioning group and 60 patients (30.8%) in the control group received noninvasive positive pressure ventilation after randomization (eTable 4 in Supplement 3). Details on the duration of each oxygenation mode used per group appear in eTable 7 in Supplement 3. Awake prone positioning was associated with modest improvement in both Spo2:Fio2 and Fio2 compared with the values collected prior to prone positioning (eFigure 5 in Supplement 3). Changes in oxygenation parameters appear in eFigures 6-7 in Supplement 3.
Primary Outcome
By day 30, 70 of 205 patients (34.1%) were intubated in the prone positioning group vs 79 of 195 patients (40.5%) in the control group (HR, 0.81 [95% CI, 0.59 to 1.12], P = .20; absolute difference, −6.37% [95% CI, −15.83% to 3.10%]; Table 2 and Figure 3A). The preplanned per-protocol analysis was consistent with the primary analysis in that 62 of 184 patients (33.7%) were intubated in the prone positioning group vs 57 of 157 patients (36.3%) in the control group (HR, 0.89 [95% CI, 0.62 to 1.28], P = .54; Table 2). A competing risk analysis yielded an HR of 0.81 (95% CI, 0.59 to 1.10; P = .19).
Table 2. Primary and Secondary Outcomes.
| Prone positioning (n = 205) |
Control (n = 195) |
Difference (95% CI) | Effect (95% CI) | P value | |
|---|---|---|---|---|---|
| Primary outcome | |||||
| Endotracheal intubation within 30 d of randomization, No. (%) | 70 (34) | 79 (41) | Absolute, −6.37 (−15.83 to 3.10)a | HR, 0.81 (0.59 to 1.12)b | .20 |
| RR, 0.87 (0.71 to 1.07)c | .19 | ||||
| Per-protocol analysis, No./total No. (%) | 62/184 (34) | 57/157 (36) | Absolute, −2.61 (−12.77 to 7.55)a | HR, 0.89 (0.62 to 1.28)b | .54 |
| Secondary outcomes | |||||
| Mortality at 60 d, No. (%) | 46 (22) | 46 (24) | Absolute, −1.15 (−9.40 to 7.10)a | HR, 0.93 (0.62 to 1.40)b | .72 |
| Days free from invasive mechanical ventilation or noninvasive ventilation at 30 d, mean (SD) | 21.4 (12.7) | 19.4 (13.2) | Mean, 2.04 (−0.50 to 4.59)d | .12 | |
| Days free from invasive mechanical ventilation at 30 d, mean (SD) | 21.6 (12.4) | 19.6 (13.1) | Mean, 2.03 (−0.47 to 4.54)d | .11 | |
| ICU-free days at 60 d, mean (SD) | 38.6 (23.6) | 34.5 (24.6) | Mean, 4.07 (−0.67 to 8.81)d | .09 | |
| Hospital-free days at 60 d, mean (SD) | 34.4 (22.9) | 30.8 (23.5) | Mean, 3.52 (−1.05 to 8.08)d | .13 | |
Abbreviations: HR, hazard ratio; ICU, intensive care unit; RR, relative risk.
Expressed as percentages.
Generated using an unadjusted Cox proportional hazards regression model for the primary analysis.
Generated using the χ2 test.
Generated using an unadjusted linear regression analysis.
Figure 3. Kaplan-Meier Survival Curves for Endotracheal Intubation Within 30 Days of Randomization and Mortality at 60 Days.
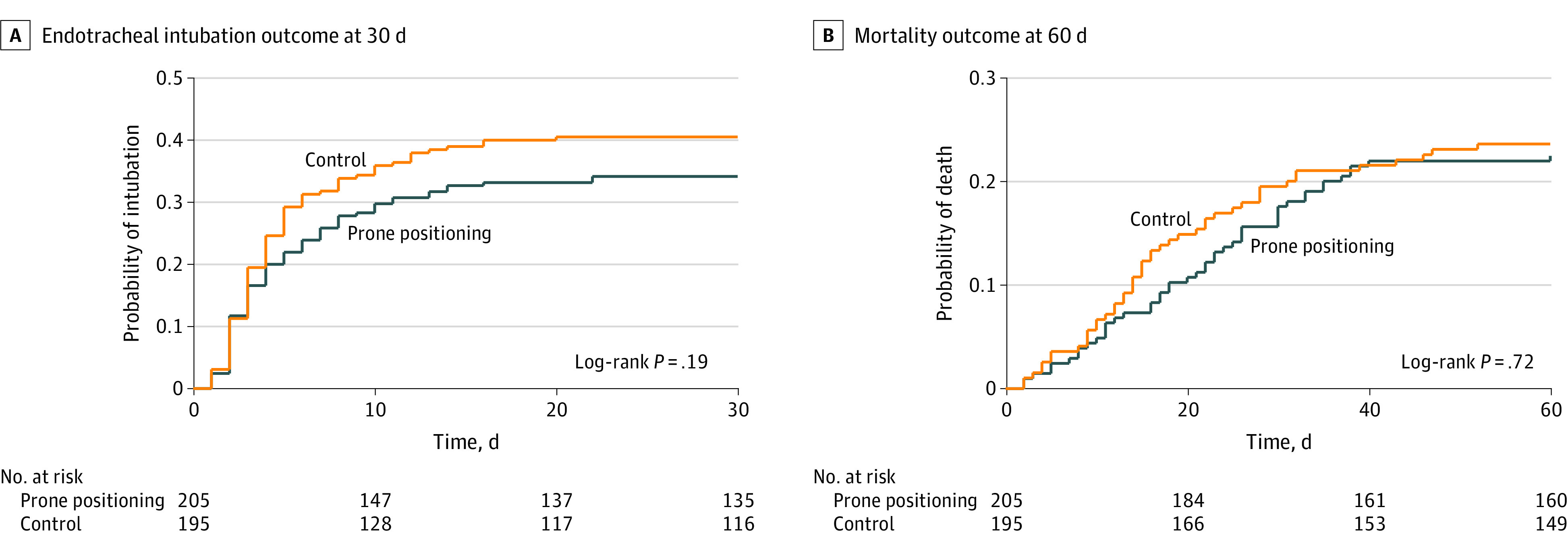
A, The log-rank test did not demonstrate a significant between-group difference (P = .19). The median time of observation was 30 days (IQR, 7-30 days) in the awake prone positioning group and 30 days (IQR, 5-30 days) in the control group.
B, The log-rank test did not demonstrate a significant between-group difference (P = .72). In both groups, the median time of observation was 60 days (IQR, 60-60 days).
Secondary Outcomes
At 60 days, 46 of 205 patients (22.4%) died in the prone positioning group and 46 of 195 patients (23.6%) died in the control group (HR, 0.93 [95% CI, 0.62 to 1.40], P = .72; absolute difference, −1.15% [95% CI, −9.40% to 7.10%]; Figure 3B). At 30 days, patients in the prone positioning group had a mean of 21.6 days (SD, 12.4 days) free from invasive mechanical ventilation compared with a mean of 19.6 days (SD, 13.1 days) in the control group (mean difference, 2.03 days [95% CI, −0.47 to 4.54 days], P = .11). The between-group differences were not statistically significant for ventilation-free days (invasive mechanical or noninvasive) at 30 days (mean difference, 2.04 days [95% CI, −0.50 to 4.59 days], P = .12), ICU-free days at 60 days (mean difference, 4.07 days [95% CI, −0.67 to 8.81 days], P = .09), and hospital-free days at 60 days (mean difference, 3.52 days [95% CI, −1.05 to 8.08 days], P = .13; Table 2). The adjusted linear regression analysis for secondary continuous outcomes yielded consistent results that were not statistically significant (eTable 8 in Supplement 3).
Adverse Events
No serious adverse events were reported in either group; however, 26 adverse events were reported in 21 patients in the prone positioning group and no events were reported in the control group. Most reported adverse events were musculoskeletal pain or discomfort from prone positioning (13 of 205 patients [6.34%]) and desaturation (2 of 205 patients [0.98%]). Unintentional removal of intravenous access occurred in 1 patient (Table 3 and eTable 2 in Supplement 3).
Table 3. Adverse Events.
| Prone positioning (n = 205) | Control (n = 195) | |
|---|---|---|
| Serious adverse events, No. of patientsa | 0 | 0 |
| Adverse events, No. (%) of patients | 21 (10) | 0 |
| Total reported adverse events, No. | 26 | 0 |
| Type of adverse event, No. (%) | ||
| Pain or discomfortb | 16 (62) | 0 |
| Desaturation | 4 (15) | 0 |
| Unintentional removal of intravenous access | 1 (4) | 0 |
| Hypotension | 1 (4) | 0 |
| Nausea | 1 (4) | 0 |
| Shortness of breath | 1 (4) | 0 |
| Dizziness | 1 (4) | 0 |
| Coughing | 1 (4) | 0 |
Any occurring after study-mandated procedures that were directly related to the treatment or intervention and resulted in any of the following outcomes: death, life-threatening adverse event, disability, or incapacity.
Musculoskeletal pain in the back, abdomen, chest, or neck. Additional details appear in eTable 9 in Supplement 3.
Subgroup Analyses
A prespecified subgroup analysis by severity of hypoxemia yielded an HR of 0.44 (95% CI, 0.23 to 0.87; absolute difference, −16.58% [95% CI, −29.50% to −3.65%]) for endotracheal intubation in patients with Spo2:Fio2 greater than 150 at baseline and an HR of 1.02 (95% CI, 0.70 to 1.48; absolute difference, 0.95% [95% CI, −11.72% to 13.63%]) in patients with Spo2:Fio2 of 150 or less at baseline (P = .03 for interaction and P = .12 for false discovery rate). The subgroup analysis by oxygen delivery modality yielded an HR of 0.61 (95% CI, 0.42 to 0.88; absolute difference, −16.13% [95% CI, −27.55% to −4.72%]) for endotracheal intubation in patients who received high-flow oxygen at baseline, an HR of 3.69 (95% CI, 1.07 to 12.70; absolute difference, 38.33% [95% CI, 5.39% to 71.28%]) in patients who received noninvasive positive pressure ventilation at baseline, and an HR of 1.35 (95% CI, 0.60 to 3.05; absolute difference, 7.86% [95% CI, −10.65% to 26.36%]) in patients who received low-flow oxygen at baseline (P = .54 for interaction and P = .73 for false discovery rate). Similarly, there was no evidence of heterogeneity of treatment effect in other subgroups (eTable 9 in Supplement 3). We were unable to conduct a prespecified subgroup analysis by COVID-19 status because almost all enrolled patients had confirmed COVID-19 at baseline.
Post Hoc Analyses
A post hoc analysis showed that 74 of 205 patients (36.1%) in the prone positioning group and 89 of 195 patients (45.6%) in the control group were intubated or died within days 30 after randomization (HR, 0.75 [95% CI, 0.55 to 1.02], P = .07; absolute difference, −9.54% [95 CI, −19.14% to 0.05%]). For the primary outcome, a post hoc mixed-effects modeling analysis, using hospital site as a random effect, yielded an HR of 0.80 (95% CI, 0.58 to 1.11, P = .18; eTable 8 in Supplement 3).
Discussion
In this international, pragmatic, unblinded randomized clinical trial enrolling 400 patients who were not intubated and who had confirmed or suspected COVID-19, awake prone positioning compared with usual care did not show a statistically significant difference in endotracheal intubation within 30 days after randomization or for the secondary outcomes.
Several small trials have assessed awake prone positioning in patients with COVID-19; however, none of which individually showed a reduction in endotracheal intubation or death.18,19,20,21,22,23 Another 6 randomized clinical trials were prospectively analyzed and published collectively as a meta-trial12 and showed a reduced risk of endotracheal intubation at 28 days with awake prone positioning. However, these trials differed by the inclusion criteria and the prone positioning protocols used, and most achieved short durations (<3 h/d) of prone positioning. In addition, the effect sizes of the individual studies were inconsistent, and the pooled estimate seemed to be primarily driven by the results from 1 trial (NCT04477655).
The preplanned subgroup analysis showed a possible reduction in endotracheal intubation risk with prone positioning in patients with Spo2:Fio2 greater than 150 and in those receiving high-flow oxygen. It is possible that patients with more severe disease do not benefit from awake prone positioning. However, the false discovery rate did not reach statistical significance for any of the preplanned subgroups, therefore, these findings should be interpreted with great caution and considered hypothesis generating.24
In this trial, 26 adverse events were reported, the majority (62%) of which were related to pain and discomfort from prone positioning (Table 3). These findings are congruent with other trials.12 Long hours of awake prone positioning are challenging and highly influenced by patient comfort and preference in contrast to prone positioning of sedated (and often pharmacologically paralyzed) patients requiring invasive mechanical ventillation.8
In the current trial, the median duration of prone positioning per day (in the first 4 days after randomization) was approximately 5 hours for a median of 3 days. Although the median duration of prone positioning in our study was longer than in most published trials, the target of 8 h/d to 10 h/d was not universally achieved. The most common reason for interruption of prone positioning was patient request, which might have been related to overall subjective improvement or related to discomfort from prone positioning (eTable 10 in Supplement 3). Given the pragmatic design of this trial, these findings reflect the challenges with implementing prone positioning in awake patients with severe illness. Studying strategies to enhance prone positioning adherence is worthy of future investigation (eg, verbal support, anxiolytics, pain control, mechanical support devices).
Strengths of this study include enrollment of patients with severe COVID-19 in acute care settings, commensurate with a high median Fio2 requirement of 70% at randomization; in this trial, 60% of patients had an Spo2:Fio2 of 150 or less. In addition, the international collaboration led to including patients with racial and ethnic diversity, enhancing the generalizability of the results.
Limitations
This study has several limitations. First, although the study sample size was increased from 350 to 400 patients and a total of 149 endotracheal intubation events occurred, the effect size for the primary outcome was imprecise. The 95% CI included a 15.8% absolute reduction in endotracheal intubation but could not exclude a 3.1% absolute increase. It is also possible that the effect of prone positioning is heterogenous as suggested by subgroup analyses, further contributing to imprecision.
Second, patient preference and health care team request led to 19% of patients in the control group undergoing some prone positioning. However, the median duration of daily prone positioning in these patients was less than 1 hour, and the per-protocol analysis was consistent with the primary intention-to-treat analysis. Furthermore, 58% of these patients were intubated despite prone positioning, suggesting that the prone positioning was prompted by severe disease.
Third, the inability to keep the health care teams blinded to the study intervention and the lack of structured criteria for endotracheal intubation may have introduced bias. However, pharmacological and nonpharmacological interventions after randomization were similar in both groups (eTables 4 and 6 in Supplement 3).
Conclusions
In patients with acute hypoxemic respiratory failure from COVID-19, prone positioning, compared with usual care without prone positioning, did not significantly reduce endotracheal intubation at 30 days. However, the effect size for the primary study outcome was imprecise and does not exclude a clinically important benefit.
Section Editor: Christopher Seymour, MD, Associate Editor, JAMA (christopher.seymour@jamanetwork.org).
Trial protocol
Statistical analysis plan
eMethods. Inclusion and exclusion criteria and list of trial outcomes and definitions
eTable 1. Screening and enrollment by site
eTable 2. Adverse events and serious adverse events (SAEs)
eTable 3. Additional characteristics of patients at baseline
eTable 4. Interventions and co-interventions after randomization
eTable 5. Protocol deviations
eTable 6. Additional co-interventions after randomization
eTable 7. Duration of oxygenation modality use after randomization
eTable 8. Additional analysis for study outcomes
eTable 9. Subgroup analyses for endotracheal intubation outcome
eTable 10. Reasons for incomplete daily proning (less than 8 hours) in the proning group
eFigure 1. Monthly and cumulative enrollment
eFigure 2. Duration of proning over time
eFigure 3. Duration of proning in the per protocol population on days 1-4
eFigure 4. Adherence to any prone positioning in the prone positioning group and control group
eFigure 5. Mean SpO2:FiO2 and standard deviations (error bars) pre and post proning (on day 1)
eFigure 6. SpO2:FiO2 over time
eFigure 7. Fraction of inspired oxygen in study groups over time
Nonauthor collaborators
Data sharing statement
References
- 1.Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA. 2020;323(16):1545-1546. doi: 10.1001/jama.2020.4031 [DOI] [PubMed] [Google Scholar]
- 2.Pal R, Yadav U. COVID-19 pandemic in India: present scenario and a steep climb ahead. J Prim Care Community Health. 2020;11:2150132720939402. doi: 10.1177/2150132720939402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aziz S, Arabi YM, Alhazzani W, et al. Managing ICU surge during the COVID-19 crisis: rapid guidelines. Intensive Care Med. 2020;46(7):1303-1325. doi: 10.1007/s00134-020-06092-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Piehl MA, Brown RS. Use of extreme position changes in acute respiratory failure. Crit Care Med. 1976;4(1):13-14. doi: 10.1097/00003246-197601000-00003 [DOI] [PubMed] [Google Scholar]
- 5.Malbouisson LM, Busch CJ, Puybasset L, Lu Q, Cluzel P, Rouby JJ; CT Scan ARDS Study Group . Role of the heart in the loss of aeration characterizing lower lobes in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2000;161(6):2005-2012. doi: 10.1164/ajrccm.161.6.9907067 [DOI] [PubMed] [Google Scholar]
- 6.Mutoh T, Guest RJ, Lamm WJ, Albert RK. Prone position alters the effect of volume overload on regional pleural pressures and improves hypoxemia in pigs in vivo. Am Rev Respir Dis. 1992;146(2):300-306. doi: 10.1164/ajrccm/146.2.300 [DOI] [PubMed] [Google Scholar]
- 7.Gattinoni L, Vagginelli F, Chiumello D, Taccone P, Carlesso E. Physiologic rationale for ventilator setting in acute lung injury/acute respiratory distress syndrome patients. Crit Care Med. 2003;31(4)(suppl):S300-S304. doi: 10.1097/01.CCM.0000057907.46502.7B [DOI] [PubMed] [Google Scholar]
- 8.Guérin C, Reignier J, Richard JC, et al. ; PROSEVA Study Group . Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-2168. doi: 10.1056/NEJMoa1214103 [DOI] [PubMed] [Google Scholar]
- 9.Munshi L, Del Sorbo L, Adhikari NKJ, et al. Prone position for acute respiratory distress syndrome: a systematic review and meta-analysis. Ann Am Thorac Soc. 2017;14(suppl 4):S280-S288. doi: 10.1513/AnnalsATS.201704-343OT [DOI] [PubMed] [Google Scholar]
- 10.Telias I, Katira BH, Brochard L. Is the prone position helpful during spontaneous breathing in patients with COVID-19? JAMA. 2020;323(22):2265-2267. doi: 10.1001/jama.2020.8539 [DOI] [PubMed] [Google Scholar]
- 11.Fazzini B, Page A, Pearse R, Puthucheary Z. Prone positioning for non-intubated spontaneously breathing patients with acute hypoxaemic respiratory failure: a systematic review and meta-analysis. Br J Anaesth. 2022;128(2):352-362. doi: 10.1016/j.bja.2021.09.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ehrmann S, Li J, Ibarra-Estrada M, et al. ; Awake Prone Positioning Meta-Trial Group . Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. Lancet Respir Med. 2021;9(12):1387-1395. doi: 10.1016/S2213-2600(21)00356-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alhazzani W, Evans L, Alshamsi F, et al. Surviving Sepsis Campaign guidelines on the management of adults with coronavirus disease 2019 (COVID-19) in the ICU: first update. Crit Care Med. 2021;49(3):e219-e234. doi: 10.1097/CCM.0000000000004899 [DOI] [PubMed] [Google Scholar]
- 14.Duhailib ZA, Arabi YM, Culgin S, et al. Awake prone position in hypoxemic patients with coronavirus disease 19 (COVI-PRONE): a study protocol and statistical analysis plan for randomized clinical trial. medRxiv. Posted online August 8, 2021. doi: 10.1101/2021.08.06.21261531 [DOI]
- 15.Wolbers M, Koller MT, Stel VS, et al. Competing risks analyses: objectives and approaches. Eur Heart J. 2014;35(42):2936-2941. doi: 10.1093/eurheartj/ehu131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Glickman ME, Rao SR, Schultz MR. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J Clin Epidemiol. 2014;67(8):850-857. doi: 10.1016/j.jclinepi.2014.03.012 [DOI] [PubMed] [Google Scholar]
- 17.Solverson K, Weatherald J, Parhar KKS. Tolerability and safety of awake prone positioning COVID-19 patients with severe hypoxemic respiratory failure. Can J Anaesth. 2021;68(1):64-70. doi: 10.1007/s12630-020-01787-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gad GS. Awake prone positioning versus non invasive ventilation for COVID-19 patients with acute hypoxemic respiratory failure. Egypt J Anesth. 2021;37(1):85-90. doi: 10.1080/11101849.2021.1889944 [DOI] [Google Scholar]
- 19.Jayakumar D, Ramachandran P, Rabindrarajan E, Vijayaraghavan BKT, Ramakrishnan N, Venkataraman R. Standard care versus awake prone position in adult nonintubated patients with acute hypoxemic respiratory failure secondary to COVID-19 infection—a multicenter feasibility randomized controlled trial. J Intensive Care Med. 2021;36(8):918-924. doi: 10.1177/08850666211014480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Johnson SA, Horton DJ, Fuller MJ, et al. Patient-directed prone positioning in awake patients with COVID-19 requiring hospitalization (PAPR). Ann Am Thorac Soc. 2021;18(8):1424-1426. doi: 10.1513/AnnalsATS.202011-1466RL [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kharat A, Dupuis-Lozeron E, Cantero C, et al. Self-proning in COVID-19 patients on low-flow oxygen therapy: a cluster randomised controlled trial. ERJ Open Res. 2021;7(1):00692-2020. doi: 10.1183/23120541.00692-2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rosén J, von Oelreich E, Fors D, et al. ; PROFLO Study Group . Awake prone positioning in patients with hypoxemic respiratory failure due to COVID-19: the PROFLO multicenter randomized clinical trial. Crit Care. 2021;25(1):209. doi: 10.1186/s13054-021-03602-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Taylor SP, Bundy H, Smith WM, Skavroneck S, Taylor B, Kowalkowski MA. Awake prone positioning strategy for nonintubated hypoxic patients with COVID-19: a pilot trial with embedded implementation evaluation. Ann Am Thorac Soc. 2021;18(8):1360-1368. doi: 10.1513/AnnalsATS.202009-1164OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? updating criteria to evaluate the credibility of subgroup analyses. BMJ. 2010;340:c117. doi: 10.1136/bmj.c117 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial protocol
Statistical analysis plan
eMethods. Inclusion and exclusion criteria and list of trial outcomes and definitions
eTable 1. Screening and enrollment by site
eTable 2. Adverse events and serious adverse events (SAEs)
eTable 3. Additional characteristics of patients at baseline
eTable 4. Interventions and co-interventions after randomization
eTable 5. Protocol deviations
eTable 6. Additional co-interventions after randomization
eTable 7. Duration of oxygenation modality use after randomization
eTable 8. Additional analysis for study outcomes
eTable 9. Subgroup analyses for endotracheal intubation outcome
eTable 10. Reasons for incomplete daily proning (less than 8 hours) in the proning group
eFigure 1. Monthly and cumulative enrollment
eFigure 2. Duration of proning over time
eFigure 3. Duration of proning in the per protocol population on days 1-4
eFigure 4. Adherence to any prone positioning in the prone positioning group and control group
eFigure 5. Mean SpO2:FiO2 and standard deviations (error bars) pre and post proning (on day 1)
eFigure 6. SpO2:FiO2 over time
eFigure 7. Fraction of inspired oxygen in study groups over time
Nonauthor collaborators
Data sharing statement