

Abstract
Background
Clonidine is a presynaptic alpha‐2‐adrenergic receptor agonist that has been used for many years to treat hypertension and other conditions, including chronic pain. Adverse events associated with systemic use of the drug have limited its application. Topical use of drugs has been gaining interest since the beginning of the century, as it may limit adverse events without loss of analgesic efficacy. Topical clonidine (TC) formulations have been investigated for almost 20 years in clinical trials. This is an update of the original Cochrane Review published in Issue 8, 2015.
Objectives
The objective of this review was to assess the analgesic efficacy and safety of TC compared with placebo or other drugs in adults aged 18 years or above with chronic neuropathic pain.
Search methods
For this update we searched the Cochrane Register of Studies Online (CRSO), MEDLINE (Ovid), and Embase (Ovid) databases, and reference lists of retrieved papers and trial registries. We also contacted experts in the field. The most recent search was performed on 27 October 2021.
Selection criteria
We included randomised, double‐blind studies of at least two weeks' duration comparing TC versus placebo or other active treatment in adults with chronic neuropathic pain.
Data collection and analysis
Two review authors independently screened references for eligibility, extracted data, and assessed risk of bias. Any discrepancies were resolved by discussion or by consulting a third review author if necessary. Where required, we contacted trial authors to request additional information.
We presented pooled estimates for dichotomous outcomes as risk ratios (RRs) with 95% confidence intervals (CIs), and continuous outcomes as mean differences (MDs) with P values. We used Review Manager Web software to perform the meta‐analyses. We used a fixed‐effect model if we considered heterogeneity as not important; otherwise, we used a random‐effects model.
The review primary outcomes were: participant‐reported pain relief of 50% or greater; participant‐reported pain relief of 30% or greater; much or very much improved on Patient Global Impression of Change scale (PGIC); and very much improved on PGIC. Secondary outcomes included withdrawals due to adverse events; participants experiencing at least one adverse event; and withdrawals due to lack of efficacy. All outcomes were measured at the longest follow‐up period.
We assessed the certainty of evidence using GRADE and created two summary of findings tables.
Main results
We included four studies in the review (two new in this update), with a total of 743 participants with painful diabetic neuropathy (PDN). TC (0.1% or 0.2%) was applied in gel form to the painful area two to three times daily. The double‐blind treatment phase of three studies lasted 8 weeks to 85 days and compared TC versus placebo. In the fourth study, the double‐blind treatment phase lasted 12 weeks and compared TC versus topical capsaicin. We assessed the studies as at unclear or high risk of bias for most domains; all studies were at unclear risk of bias for allocation concealment and blinding of outcome assessment; one study was at high risk of bias for blinding of participants and personnel; two studies were at high risk of attrition bias; and three studies were at high risk of bias due to notable funding concerns. We judged the certainty of evidence (GRADE) to be moderate to very low, downgrading for study limitations, imprecision of results, and publication bias.
TC compared to placebo
There was no evidence of a difference in number of participants with participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks) between groups (risk ratio (RR) 1.21, 95% confidence interval (CI) 0.78 to 1.86; 179 participants; 1 study; low certainty evidence). However, the number of participants with participant‐reported pain relief of 30% or greater during longest follow‐up period (8 to 12 weeks) was higher in the TC group compared with placebo (RR 1.35, 95% CI 1.03 to 1.77; 344 participants; 2 studies, very low certainty evidence). The number needed to treat for an additional beneficial outcome (NNTB) for this comparison was 8.33 (95% CI 4.3 to 50.0). Also, there was no evidence of a difference between groups for the outcomes much or very much improved on the PGIC during longest follow‐up period (12 weeks) or very much improved on PGIC during the longest follow‐up period (12 weeks) (RR 1.06, 95% CI 0.76 to 1.49 and RR 1.82, 95% CI 0.89 to 3.72, respectively; 179 participants; 1 study; low certainty evidence). We observed no evidence of a difference between groups in withdrawals due to adverse events and withdrawals due to lack of efficacy during the longest follow‐up period (12 weeks) (RR 0.34, 95% CI 0.04 to 3.18 and RR 1.01, 95% CI 0.06 to 15.92, respectively; 179 participants; 1 study; low certainty evidence) and participants experiencing at least one adverse event during longest follow‐up period (12 weeks) (RR 0.65, 95% CI 0.14 to 3.05; 344 participants; 2 studies; low certainty evidence).
TC compared to active comparator
There was no evidence of a difference in the number of participants with participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks) between groups (RR 1.41, 95% CI 0.99 to 2.0; 139 participants; 1 study; low certainty evidence). Other outcomes were not reported.
Authors' conclusions
This is an update of a review published in 2015, for which our conclusions remain unchanged. Topical clonidine may provide some benefit to adults with painful diabetic neuropathy; however, the evidence is very uncertain. Additional trials are needed to assess TC in other neuropathic pain conditions and to determine whether it is possible to predict who or which groups of people will benefit from TC.
Keywords: Adult, Humans, Analgesics, Analgesics/therapeutic use, Chronic Pain, Chronic Pain/drug therapy, Clonidine, Clonidine/adverse effects, Diabetic Neuropathies, Diabetic Neuropathies/drug therapy, Neuralgia, Neuralgia/drug therapy, Randomized Controlled Trials as Topic
Plain language summary
Clonidine applied to the skin for adults with chronic neuropathic pain
Key message
We found no high certainty evidence to support the use of clonidine applied to the skin for painful diabetic neuropathy. We found no evidence for other chronic pain conditions.
What did we do?
To find out how clonidine applied to the skin (topical clonidine) works in people with neuropathic pain, we searched medical databases and references of retrieved papers and registries or clinical trials. We also contacted experts in the field. Two review authors independently screened references for eligibility, extracted data, and assessed risk of bias. When necessary, we contacted trial authors to request additional information.
What did we find?
We identified four studies for inclusion in the review. The studies lasted 8 weeks to 85 days and included a total of 743 participants with painful diabetic neuropathy. Clonidine (0.1% or 0.2%) was applied in gel form to the painful area two to three times daily, and was compared with placebo (dummy treatment) in three studies and with capsaicin applied to the skin in one study.
Limitations in how the studies were conducted and reported and the small amount of evidence available means that our confidence in the results is limited. The evidence suggests that in adults with painful diabetic neuropathy, topical clonidine may provide pain relief in some people. However, topical clonidine was not better than placebo for our other outcomes. We found no evidence of a difference between topical clonidine and capsaicin applied to the skin in painful diabetic neuropathy. The information from clinical trials is not enough to judge about possible long‐term side effects of clonidine applied to the skin; however, we found that during 8 to 12 weeks of treatment there was no evidence of a difference in number of side effects between study groups. We also do not know from the included trials how clonidine works in other chronic neuropathic pain conditions.
How up‐to‐date is this evidence?
The review is current to 27 October 2021.
Summary of findings
Summary of findings 1. Topical clonidine (TC) compared with placebo for chronic neuropathic pain in adults.
| Topical clonidine (TC) compared with placebo for chronic neuropathic pain in adults | |||||||
|
Participants or population: adults with painful diabetic neuropathy Settings: primary care, outpatient Intervention: 0.1% or 0.2% clonidine gel applied to both feet 2 to 3 times daily Comparison: placebo | |||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | NNTB (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | ||||||
| Placebo | TC | ||||||
| Participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks) |
29 per 100 | 35 per 100 (23 to 54) | RR 1.21 (0.78 to 1.86) | Not calculated | 179 (1 study) |
⊕⊕⊝⊝ Lowa |
No evidence of a difference |
| Participant‐reported pain relief of 30% or greater during longest follow‐up period (8 to 12 weeks) |
36 per 100 | 49 per 100 (37 to 64) |
RR 1.35 (1.03 to 1.77) | 8.3 (4.3 to 50.0) | 344 (2 studies) |
⊕⊝⊝⊝ Very lowb |
Evidence of a difference present |
| Much or very much improved on PGIC during longest follow‐up period (12 weeks) |
42 per 100 | 45 per 100 (32 to 63) |
RR 1.06 (0.76 to 1.49) | Not calculated | 179 (1 study) |
⊕⊕⊝⊝ Lowa |
No evidence of a difference |
| Very much improved on PGIC during longest follow‐up period (12 weeks) |
11 per 100 | 20 per 100 (10 to 41) | RR 1.82 (0.89 to 3.72) | Not calculated | 179 (1 study) | ⊕⊕⊝⊝ Lowa |
No evidence of a difference |
| Withdrawals due to adverse events during longest follow‐up period (12 weeks) |
3 per 100 | 1 per 100 (0 to 10) |
RR 0.34 (0.04 to 3.18) | Not calculated | 179 (1 study) |
⊕⊕⊝⊝ Lowc |
No evidence of a difference |
| Participants experiencing at least 1
adverse event during longest follow‐up period (12 weeks) |
13 per 100 | 10 per 100 (6 to 19) |
RR 0.65 (0.14 to 3.05) | Not calculated | 344 (2 studies) |
⊕⊕⊝⊝ Lowd |
No evidence of a difference |
| Withdrawal due to lack of efficacy (12 weeks) |
1 per 100 | 1 per 100 (0 to 16) | RR 1.01 (0.06 to 15.92) | Not calculated | 179 (1 study) |
⊕⊕⊝⊝ Lowc |
No evidence of a difference |
| *Mean baseline risk was chosen to determine the assumed risk in the control group. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; NNTB: number needed to treat for an additional beneficial outcome; PGIC: Patient Global Impression of Change scale; RR: risk ratio | |||||||
|
GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||||
aDowngraded one level for serious study limitations (the study was judged as at high risk of funding bias and unclear risk of bias for allocation concealment and blinding of outcome assessment) and one level for imprecision of results (optimal information size not met: fewer than 400 participants). bDowngraded one level for serious study limitations (the studies were judged as at high risk of funding bias and unclear risk of bias for allocation concealment and blinding of outcome assessment); one level for imprecision of results (optimal information size not met: fewer than 400 participants); and one level for publication bias (fewer than 200 participants in unpublished null effect studies required to make the result clinically irrelevant). cDowngraded one level for serious study limitations (the study was judged as at high risk of funding bias and unclear risk of bias for allocation concealment and blinding of outcome assessment) and one level for imprecision of results (optimal information size not met: fewer than 400 participants, wide confidence intervals, small number of events). dDowngraded one level for serious study limitations (the study was judged as at high risk of funding bias and unclear risk of bias for allocation concealment and blinding of outcome assessment) and one level for imprecision of results (optimal information size not met: fewer than 400 participants, wide confidence intervals).
Summary of findings 2. Topical clonidine (TC) compared with active comparator for chronic neuropathic pain in adults.
| Topical clonidine (TC) compared with active comparator for chronic neuropathic pain in adults | |||||||
|
Participants or population: adults with painful diabetic neuropathy Settings: tertiary care setting Intervention: 0.1% clonidine gel self administered 3 times daily on both feet Comparison: 0.75% capsaicin cream self administered 3 times daily on both feet | |||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | NNTB (95% CI) | Number of participants (studies) | Certainty of evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | ||||||
| Topical capsaicin | TC | ||||||
| Participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks) |
41 per 100 | 57 per 100 (41 to 82) |
RR 1.41 (0.99 to 2.0) |
Not calculated | 139 (1 study) | ⊕⊕⊝⊝ Lowa |
No evidence of a difference |
| Participant‐reported pain relief of 30% or greater during longest follow‐up period (12 weeks) |
Not reported | ||||||
| Much or very much improved on PGIC during longest follow‐up period (12 weeks) |
Not reported | ||||||
| Very much improved on PGIC during longest follow‐up period (12 weeks) |
Not reported | ||||||
| Withdrawals due to adverse events during longest follow‐up period (12 weeks) |
Not reported | ||||||
| Participants experiencing at least 1
adverse event during longest follow‐up period (12 weeks) |
Not reported | ||||||
| Withdrawal due to lack of efficacy (12 weeks) |
Not reported | ||||||
| *Mean baseline risk was chosen to determine the assumed risk in the control group. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; NNTB: number needed to treat for an additional beneficial outcome; PGIC: Patient Global Impression of Change scale; RR: risk ratio | |||||||
|
GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||||
aDowngraded one level for serious study limitations (the study was judged as at high risk of bias for blinding of participants and personnel and unclear risk of bias for allocation concealment, blinding of outcome assessment, and study size domains) and one level for imprecision of results (optimal information size not met: more than 50 and fewer than 199 participants per treatment arm).
Background
This review is based on a template for reviews of drugs used to relieve neuropathic pain. The aim is for all reviews to use the same methods, based on new criteria for what constitutes reliable evidence in chronic pain (Appendix 1) (Moore 2010a).
Description of the condition
Neuropathic pain comprises a wide range of pain conditions. It is defined by the International Association of the Study of Pain as "pain caused by lesion or disease of the somatosensory nervous system" (Jensen 2011; Macone 2018; Raja 2020), based on an earlier consensus meeting (Treede 2008). Neuropathic pain may be caused by nerve damage, but is often followed by changes in the central nervous system (Moisset 2007). It tends to be chronic and may be present for months or years. It is complex (Apkarian 2011; Tracey 2011), and neuropathic pain features can be found in patients with joint pain (Soni 2013). The pathomechanism of neuropathic pain differs significantly from that of nociceptive pain. Nociceptive pain is a consequence of tissue damage, whereas neuropathic pain results from maladaptive changes that can occur in injured sensory neurons and along the entire nociceptive pathway within the central nervous system, possibly leading to spontaneous pain or pain hypersensitivity. The most characteristic clinical symptoms of neuropathic pain are spontaneous pain, hyperalgesia, and allodynia; this has been easily demonstrated in various animal models (Hurley 2013; Macone 2018; Woolf 1999).
In primary care in the UK, the incidence per 100,000 person‐years of observation has been reported as 28 (95% confidence interval (CI) 27 to 30) for postherpetic neuralgia; 27 (95% CI 26 to 29) for trigeminal neuralgia; 0.8 (95% CI 0.6 to 1.1) for phantom limb pain; and 21 (95% CI 20 to 22) for painful diabetic neuropathy (PDN) (Hall 2008). Estimates vary between studies, which is often due to small sample sizes. The study of facial pain in the Netherlands found an incidence per 100,000 person‐years of 12.6 for trigeminal neuralgia and 3.9 for postherpetic neuralgia (Koopman 2009). A systematic review of chronic pain indicated that some neuropathic pain conditions, such as PDN, are more common than others, with prevalence rates up to 400 per 100,000 person‐years (McQuay 2007), illustrating how common the condition is as well as its chronicity. The prevalence of neuropathic pain was reported as 8.9% in England and 8.2% in Scotland (Fayaz 2016), 3.3% in Austria (Gustorff 2008), 6.9% in France (Bouhassira 2008), as high as 8% in the UK, and about 7% in a systematic review of studies published since 2000 (Andrew 2014; Torrance 2006). The incidence of some forms of neuropathic pain, such as diabetic neuropathy and postsurgical chronic pain (often neuropathic in origin), is increasing (Bouhassira 2019; Hall 2008).
Neuropathic pain is known to be difficult to treat effectively; only a minority of individuals experience clinically relevant benefit from any one intervention. A multidisciplinary approach is now advocated, with pharmacological interventions combined with physical or cognitive interventions, or both. Conventional analgesics are usually not effective. Some patients may benefit from a topical lidocaine patch or low‐concentration topical capsaicin, although evidence showing benefits is uncertain (Anitescu 2013; Derry 2012; Khaliq 2007). High‐concentration topical capsaicin may be helpful for some patients with postherpetic neuralgia (Derry 2013). Treatment more usually consists of so‐called unconventional analgesics such as antidepressants (e.g. duloxetine, amitriptyline) or antiepileptics (e.g. gabapentin, pregabalin) (Lunn 2009; Moore 2009; Moore 2011a; Moore 2012; Sultan 2008). An overview of treatment guidelines points out general similarities, as well as differences, in treatment approaches (Bates 2019; Hurley 2013; O'Connor 2009; Smith 2013). The proportion of patients who achieve worthwhile pain relief (typically ≥ 50% reduction in pain intensity) is small, generally 10% to 25% greater than with placebo, and numbers needed to treat for additional beneficial outcome (NNTBs) are usually between four and 10 (Moore 2013; Xu 2016).
Chronic painful conditions constantly account for top‐ranking conditions for years lived with disability (Vos 2020), and are responsible for considerable loss of quality of life and employment, as well as increased healthcare costs (Andrew 2014).
Description of the intervention
Clonidine is a presynaptic alpha‐2‐adrenergic receptor agonist and an agonist of imidazoline receptors (Eisenach 1996; Yasaei 2021). It has been in clinical use for over 40 years. It was first registered for treatment of hypertension, but was later shown to be effective for treatment of acute and chronic pain (Neil 2011). Clonidine is an extremely potent antinociceptive agent with potency equal to or greater than that reported for morphine (Gentili 1997; Samso 1996). Clonidine has been used to treat acute and chronic pain and may be effective when applied intravenously, epidurally, and intrathecally (Asano 2000; Crespo 2017; Eisenach 1995; Hassenbusch 2002; Sierralta 1996). However, systemic and central use of clonidine is limited by undesirable adverse events including sedation, dry mouth, hypotension, and rebound hypertension (Dias 1999; Puskas 2003). Since the beginning of the century, topical forms of administration have been developed with the intention of limiting centrally mediated adverse events without reduction in analgesic efficacy (Sawynok 2003). Clonidine is lipophilic and easily penetrates the skin to reach the local antinociceptive pathways. The half‐life of clonidine is about eight hours, thus it should be applied three times daily. Clonidine can be prepared in various concentrations by compounding pharmacies (Derry 2017; Flores 2012; Paganoni 2018).
Several animal studies have shown that topical clonidine (TC) may be an effective analgesic. Dogrul and colleagues demonstrated that topical administration of clonidine increased the pain threshold to radiant heat stimuli (measured by tail‐flick test) in mice. Antinociceptive activity was limited to the portion of the tail exposed to drug solution. Systemic administration of the alpha‐2‐receptor antagonist yohimbine before immersion of the tail blocked the antinociceptive activity of TC (Dogrul 2004). Chi and colleagues studied the efficacy of topically applied clonidine in an animal model of neuropathic, postoperative, and inflammatory pain. Clonidine was effective in neuropathic pain, only partially effective in postoperative pain, and not effective in inflammatory pain. The analgesic efficacy of clonidine in postoperative pain manifested on the sixth day of application, and reduction in thermal hyperalgesia ‐ not mechanical allodynia ‐ was observed (Chi 2007).
How the intervention might work
Target receptors for clonidine ‐ alpha‐2 receptors ‐ are located in the brain, spinal cord, and dorsal root ganglia and on sensory neurons (Kawaski 2003; Ongioco 2000; Riedl 2009). Activation of alpha‐2 receptors leads to release of an inhibitory G‐protein, which down‐regulates adenylate cyclase and other second messengers responsible for initiating and maintaining the abnormal excitability of nociceptors (Lavand'homme 2002). Antinociceptive effects of clonidine are mediated via spinal and supraspinal sites of action (Asano 2000; Bernard 1994; Buerkle 1998). However, investigators in previous studies showed that peripheral administration of alpha‐2‐receptor agonists also induces antinociception (Aley 1997; Buerkle 1998; Buerkle 2000; Gentili 1996). The mechanism of action of clonidine is similar to that of opioids. Antinociceptive effects of topically administered opioids have been previously reported (Kolesnikov 1999; Kolesnikov 2000); however, tolerance to antinociceptive action was observed after repeated administration (Kolesnikov 1999). Tolerance to the antinociceptive action of clonidine was observed in animal studies and was not attenuated by N‐Methyl‐D‐aspartate (NMDA)‐receptor antagonists such as ketamine (Dogrul 2004).
Clonidine is also an imidazoline‐receptor agonist. Stimulation of the I2‐imidazoline subclass of receptors causes analgesia. I2‐imidazoline receptors are located centrally in the brain and spinal cord and peripherally on peripheral nerve endings. Activation of peripheral imidazoline receptors may be responsible for additional mechanisms of analgesic activity of TC (Khan 1999).
Why it is important to do this review
Practitioners have for many years attempted to use TC to treat neuropathic pain; however, no clear evidence is available to support this clinical practice. In the last 20 years, new randomised clinical trials investigating this topic have been published. The aim of this review was to determine whether TC is effective in neuropathic pain, and to specify in which neuropathic pain conditions in particular it is effective. This topic has not been examined in another Cochrane Review.
Standards used to assess evidence in chronic pain trials have changed substantially, with particular attention paid to trial duration, withdrawals, and statistical imputation following withdrawal ‐ all of which can substantially alter estimates of efficacy. The most important change is the move from use of average pain scores, or average change in pain scores, to the numbers of study participants who report a large decrease in pain (≥ 50%); this level of pain relief has been shown to correlate with improvement in comorbid symptoms, function, and quality of life (Gewandter 2015).
This Cochrane Review was designed to assess evidence in ways that make both statistical and clinical sense, and to use developing criteria for what constitutes reliable evidence in chronic pain (Moore 2010a). Trials included and analysed had to meet minimum criteria for reporting quality (blinding, randomisation), validity (duration, dose and timing, diagnosis, outcomes, etc.), and size (ideally ≥ 500 participants in a comparison in which the NNTB is ≥ 4) (Moore 1998). This approach imposes high standards and marks a departure from the way previous reviews were conducted.
Objectives
The objective of this review was to assess the analgesic efficacy and safety of TC compared with placebo or other drugs in adults aged 18 years or above with chronic neuropathic pain.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials with double‐blind assessment of outcomes following two weeks of treatment or longer. Randomised trials are the optimal design for minimising bias when evaluating the effectiveness of an intervention, and a two‐week treatment period is considered a minimum treatment time to assess the efficacy of drugs in chronic pain conditions. Cross‐over studies were also eligible for inclusion, provided results for the first phase were reported clearly. We required full journal publications, with the exception of online clinical trial results summaries of otherwise unpublished clinical trials and abstracts with sufficient data for analysis. We did not include short abstracts (usually meeting reports). We excluded studies that were non‐randomised, experimental studies using pain induction, case reports, and clinical observations. We applied no language restrictions.
Types of participants
We included adults aged 18 years or above. Participants had to have one or more of a wide range of chronic (lasting over three months) neuropathic pain conditions, including the following.
Painful diabetic neuropathy
Postherpetic neuralgia
Trigeminal neuralgia
Phantom limb pain
Postoperative or traumatic neuropathic pain
Complex regional pain syndrome
Cancer‐related neuropathy
HIV neuropathy
Spinal cord injury
Types of interventions
Topical clonidine had to be administered to a painful area for relief of neuropathic pain in a form of cream, ointment, gel, patch, or plaster and compared with placebo or any active comparator. We included studies in which placebo or the comparator was administered via any route: topically, orally, intravenously, subcutaneously, etc. We did not include studies where clonidine was applied transdermally with the intention of producing a systemic effect, not a local effect.
Types of outcome measures
We anticipated that studies would use a variety of outcome measures, with most studies employing standard subjective scales (numerical rating scale (NRS) or visual analogue scale (VAS)) for pain intensity or pain relief, or both. We were particularly interested in Initiative on Methods, Measurement and Pain Assessment in Clinical Trials (IMMPACT) definitions of moderate and substantial benefit in chronic pain studies (Gewandter 2015). Benefit is defined as at least 30% pain relief over baseline (moderate), at least 50% pain relief over baseline (substantial), much or very much improved on the Patient Global Impression of Change scale (PGIC) (moderate), and very much improved on the PGIC (substantial). These outcomes differ from those used in some other reviews, concentrating as they do on continuous outcomes, when pain responses do not follow a normal (Gaussian) distribution. People with chronic pain desire high levels of pain relief, ideally more than 50%, and pain not worse than mild (O'Brien 2010).
Primary outcomes
Participant‐reported pain relief of 50% or greater during longest follow‐up period
Participant‐reported pain relief of 30% or greater during longest follow‐up period
Much or very much improved on PGIC during longest follow‐up period
Very much improved on PGIC during longest follow‐up period
Secondary outcomes
Withdrawals due to adverse events during longest follow‐up period
Participants experiencing at least one adverse event during longest follow‐up period
Withdrawals due to lack of efficacy during longest follow‐up period
Participants experiencing at least one serious adverse event during longest follow‐up period. Serious adverse events typically include any untoward medical occurrence or effect that at any dose results in death, is life‐threatening, requires hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, is a congenital anomaly or birth defect, or is an ‘important medical event’ that may jeopardise the participant or may require an intervention to prevent one of the above characteristics/consequences.
Specific adverse events, in particular somnolence and dizziness during longest follow‐up period
Any pain‐related outcome indicating some improvement during longest follow‐up period (including physical and emotional functioning)
Skin biopsy results
Change in average pain intensity during longest follow‐up period
Search methods for identification of studies
Electronic searches
We searched the following databases for this update.
Cochrane Register of Studies Online (CRSO), 17 September 2014 to 27 October 2021
MEDLINE and MEDLINE in Process (Ovid), September 2014 to 27 October 2021
Embase (Ovid), September 2014 to 2021 week 43
We used medical subject headings (MeSH) or equivalent and text word terms and applied no language restrictions. We tailored searches to individual databases; our search strategies are provided in Appendix 2, Appendix 3, and Appendix 4. The most recent search was performed on 27 October 2021. The search strategy wad developed by the Pain, Palliative and Supportive Care Group (PaPaS) Review Group’s Information Specialist and was independently peer reviewed. The PaPaS Information Specialist performed the searches.
Searching other resources
We searched the following trial registers on 27 October 2021 for ongoing trials.
metaRegister of controlled trials (mRCT) (www.controlled-trials.com/mrct/)
ClinicalTrials.gov (clinicaltrials.gov/)
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (apps.who.int/trialsearch/)
In addition, we searched the grey literature, checked the reference lists of reviews and retrieved articles for additional studies, and searched citations on key articles. We contacted experts in the field to ask about unpublished and ongoing trials, and contacted investigators or study sponsors when necessary.
Data collection and analysis
Selection of studies
We determined study eligibility by reading the abstract of each study identified by the search. We eliminated studies that clearly did not satisfy our inclusion criteria; these decisions were made by five review authors (WS, RZ, AW, JJ, J Woron). We obtained the full texts of studies identified as potentially relevant by at least one review author. Two review authors (AW, WS) independently read the full texts of these studies and decided whether or not they met the inclusion criteria. In cases of disagreement, review authors reached conclusions by discussion or by seeking the opinion of a third review author (J Wordliczek or JD, JJ) if necessary. We did not anonymise the studies in any way before assessment. We created a PRISMA flow diagram to document the screening process (Liberati 2009), as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2021a). We included studies in the review irrespective of whether measured outcome data were reported in a 'useable' way.
Data extraction and management
Two review authors (WS, AW) independently extracted data from the studies using a standard, piloted data extraction form (Appendix 5). Any disagreements were resolved by consultation and discussion with a third review author (J Wordliczek). One review author (WS) entered data into Cochrane statistical software Review Manager Web (RevMan Web 2020), and another review author (AW) checked the data for accuracy. We collated multiple reports of the same study so that each study, rather than each report, was the unit of interest in the review. We collected characteristics of the included studies in sufficient detail to populate a 'Characteristics of included studies' table. We included the following data when available.
Study design (including methods, location, funding sources, study author declarations of interest)
Setting
Participants (including inclusion criteria, exclusion criteria, number of participants screened/enrolled/randomly assigned to each treatment arm, age, number of males, duration of pain condition, mean baseline pain intensity)
Intervention (including form of application, place of application, concentration, dose, dosing regimen)
Comparator (including form of application, place of application, concentration, dose, dosing regimen)
Outcomes (including measures and time points)
Numerical data for outcomes of interest
Other important information
Assessment of risk of bias in included studies
We used the Oxford Quality Score as the basis for inclusion (Jadad 1996), limiting inclusion to studies that were at a minimum randomised and double‐blind.
Two review authors (WS, AW) independently assessed risk of bias for each study, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2021a). Any disagreements were resolved by discussion. We completed a risk of bias table for each included study using the risk of bias tool in Review Manager Web (RevMan Web 2020).
We assessed the following biases for each included study.
-
Random sequence generation (checking for possible selection bias). We assessed the method used to generate the allocation sequence as follows.
Low risk of bias (any truly random process, e.g. random number table, computer random number generator)
Unclear risk of bias (insufficient detail about the method of randomisation to permit a judgement of 'low' or 'high' risk of bias)
We excluded studies using a non‐random process (e.g. odd or even date of birth; hospital or clinic record number)
-
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions before assignment determines whether intervention allocation could have been foreseen in advance of, or during, recruitment, or changed after assignment. We assessed methods as follows.
Low risk of bias (e.g. telephone or central randomisation; consecutively numbered, sealed, opaque envelopes)
Unclear risk of bias (insufficient detail about the method of randomisation to permit a judgement of 'low' or 'high' risk of bias)
We excluded studies that did not conceal allocation (e.g. open list)
-
Blinding of participants and personnel (checking for possible performance bias). We assessed methods used to blind study participants and personnel from the knowledge of which intervention a participant received. We assessed these methods as follows.
Low risk of bias (study states that it was blinded and describes the method used to achieve blinding, e.g. identical form of cream or gel; matched in appearance and smell, or a double‐dummy technique)
Unclear risk of bias (study states that it was blinded but does not provide an adequate description of how this was achieved)
We considered studies that were not double‐blind to have high risk of bias
-
Blinding of outcome assessment (checking for possible detection bias). We assessed methods used to blind outcome assessors from the knowledge of which intervention a participant received. We assessed these methods as follows.
Low risk of bias (study states clearly that outcome assessors were unaware of treatment allocation, ideally describing how this was achieved)
Unclear risk of bias (study states that outcome assessors were blind to treatment allocation, but a clear statement on how this was achieved is lacking)
High risk of bias (outcome assessment was not blinded)
-
Incomplete outcome data (checking for possible attrition bias due to the amount, nature, and handling of incomplete outcome data). We assessed methods used to deal with incomplete data as follows.
Low risk (no missing outcome data; reasons for missing outcome data are unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias); missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; missing data have been imputed using 'baseline observation carried forward’ analysis)
Unclear risk of bias (insufficient reporting of attrition/exclusions to permit a judgement of 'low' or 'high' risk of bias (e.g. number randomised not stated, no reasons for missing data provided, or the study does not address this outcome)
High risk of bias (reason for missing outcome data is likely to have been related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups; ‘as‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation; potentially inappropriate application of simple imputation)
-
Selective reporting (checking for reporting bias). We assessed reporting biases due to selective outcome reporting. We judged studies as follows.
Low risk of bias (the study protocol is available, and all of the study’s prespecified (primary and secondary) outcomes that are of interest in the review have been reported in the prespecified way)
Unclear risk of bias (insufficient information available to permit a judgement of 'low' or 'high' risk of bias)
High risk of bias (not all the study’s prespecified primary outcomes have been reported; one or more primary outcomes have been reported using measurements, analysis methods, or subsets of the data (e.g. subscales) that were not prespecified; one or more reported primary outcomes were not prespecified (unless clear justification for their reporting is provided, such as an unexpected adverse effect); one or more outcomes of interest in the review have been reported incompletely so that they cannot be entered in a meta‐analysis; the study report fails to include results for a key outcome that would be expected to have been reported for such a study)
-
Study size (checking for possible biases confounded by small size). Based on methodology proposed by the ACTINPAIN Cochrane Special Interest Group (Moore 2011a), we judged studies as follows.
Low risk of bias (≥ 200 participants per treatment arm)
Unclear risk of bias (50 to 199 participants per treatment arm)
High risk of bias (< 50 participants per treatment arm)
-
Funding bias. We judged studies as follows.
Low risk of bias (no notable concerns, e.g. funding by governmental institution)
High risk of bias (notable concerns, e.g. funding by pharmaceutical company)
Unclear risk of bias (funding source not disclosed)
Measures of treatment effect
We used dichotomous data to calculate risk ratio (RR) and number needed to treat for an additional beneficial outcome (NNTB) with 95% confidence intervals (CIs) to establish statistical differences. We calculated NNTBs as the reciprocal of absolute risk reduction (ARR). For unwanted effects, the NNTB becomes the number needed to treat for an additional harmful outcome (NNTH), which is calculated in the same manner. We used a fixed‐effect model, unless we found significant statistical heterogeneity (see Data synthesis). Given that the amount of evidence was small, we decided to include a continuous outcome for illustrative purposes only, and presented data as mean difference (MD) with P value. We considered P values equal to or less than 0.05 (two‐sided alpha) as statistically significant.
Unit of analysis issues
We accepted randomisation by individual participant only.
We accepted cross‐over studies only if clear reporting for the first cross‐over phase was available.
We planned to split the control treatment arm between active treatment arms in a single study in which active treatment arms were not combined for analysis; however, this was not the case in this review.
Dealing with missing data
We used intention‐to‐treat (ITT) analysis when the ITT population consisted of participants who were randomly assigned, took at least one dose of assigned study medication, and provided at least one postbaseline assessment. We assigned missing participants zero improvement.
Assessment of heterogeneity
As a first step, we determined whether clinical heterogeneity was significant between studies. We assessed clinical heterogeneity by comparing participants, interventions, and outcomes amongst studies. If we found significant discrepancies between studies, we did not report the pooled effect.
If we found no clear evidence of clinical heterogeneity, we assessed quantified statistical heterogeneity between trials by calculating the I2 statistic, which describes the percentage of total variation across studies due to heterogeneity rather than to chance, per Chapter 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2021b). We regarded statistical heterogeneity as low if the I2 statistic was less than 30%, moderate if between 30% and 50%, substantial if between 50% and 75%, and considerable if above 75%, per Chapter 10 of the Cochrane Handbook (Higgins 2021b). We planned that if we found evidence of heterogeneity, we would investigate and report possible reasons for it. In the case of considerable heterogeneity, we would not report the pooled effect.
Assessment of reporting biases
We assessed publication bias using a method designed to detect the quantity of unpublished data with a null effect required to make any result clinically irrelevant (usually taken to mean an NNTB of 10 or higher in this condition) (Moore 2008). We considered that fewer than 200 participants in unpublished null effect studies could give rise to doubts about the impact of efficacy results.
The aim of this review was to use dichotomous data of known utility (Moore 2010b). The review does not depend on what authors of the original studies chose to report, although clearly difficulties could arise in studies that failed to report dichotomous results. For illustrative purposes, we added a continuous outcome, that is change in average pain intensity as reported by participants using the numerical rating scale (NRS), which, however, poorly reflects efficacy and utility.
Data synthesis
When at least two studies performed similar comparisons and reported the same outcome measures, and heterogeneity indicated that reporting the pooled effect was appropriate, we performed meta‐analyses using Review Manager Web (RevMan Web 2020). We used a fixed‐effect model for meta‐analysis when we considered that heterogeneity was not important or low. If we found moderate or greater heterogeneity amongst studies, we used a random‐effects model (Higgins 2021a). We calculated 95% CIs, and considered corresponding P values equal to or less than 0.05 (two‐sided alpha) as statistically significant.
Subgroup analysis and investigation of heterogeneity
We planned all analyses according to individual painful conditions because placebo response rates with the same outcome can vary between conditions, as can drug‐specific effects (Moore 2009). However, insufficient data precluded the performance of any meaningful subgroup analysis.
Sensitivity analysis
We did not plan and did not conduct sensitivity analysis because we expected the evidence to be too limited to allow reliable analysis. Also, sensitivity analyses based on different concentrations of drug were not possible.
Summary of findings and assessment of the certainty of the evidence
Three review authors (WS, AW, JJ) independently rated the certainty of the body of evidence for the outcomes. We used the GRADE system to rank the certainty of the evidence, employing GRADEpro GDT software and the guidelines provided in the Cochrane Handbook for Systematic Reviews of Interventions and GRADE Handbook (GRADEpro GDT; Higgins 2021c; Schünemann 2013).
The GRADE approach uses five considerations (study limitations (risk of bias), unexplained heterogeneity and inconsistency of effect, imprecision, indirectness, and publication bias) to assess the certainty of the body of evidence for each outcome. The GRADE system uses the following criteria for assigning grade of evidence.
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
The GRADE system considers study design as a marker of quality. Randomised controlled trials are considered to be high certainty evidence, and can be downgraded for important limitations. The following are factors that can decrease the certainty level of a body of evidence.
Serious or very serious study limitations (risk of bias)
Important or serious inconsistency of results
Some or major indirectness of evidence
Serious or very serious imprecision
Probability of publication bias
We included summary of findings tables to present the main findings for the comparisons topical clonidine (TC) versus placebo and TC versus active comparator in a transparent and simple tabular format. In particular, we included key information concerning the certainty of evidence, the magnitude of effect of the interventions examined, and the sum of available data on the following outcomes.
Participant‐reported pain relief of 50% or greater
Participant‐reported pain relief of 30% or greater
Much or very much improved on PGIC
Very much improved on PGIC
Withdrawals due to adverse events
Participants experiencing at least one adverse event
Withdrawals due to lack of efficacy
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies tables.
Results of the search
Our updated search period extended from September 2014 to 27 October 2021. We identified 478 records from the database searches and 11 additional records through other sources. After de‐duplication, we screened 390 records, of which 4 full‐text articles were assessed for eligibility. Four studies (two new at this update: Kiani 2015; NCT02068027) involving a total of 743 participants were eligible for inclusion in the review (see Characteristics of included studies). We excluded six (two from the most recent search) ineligible studies (see Characteristics of excluded studies). We identified one ongoing study (see Characteristics of ongoing studies). A flow diagram outlining the trial screening and selection process is presented in Figure 1.
1.
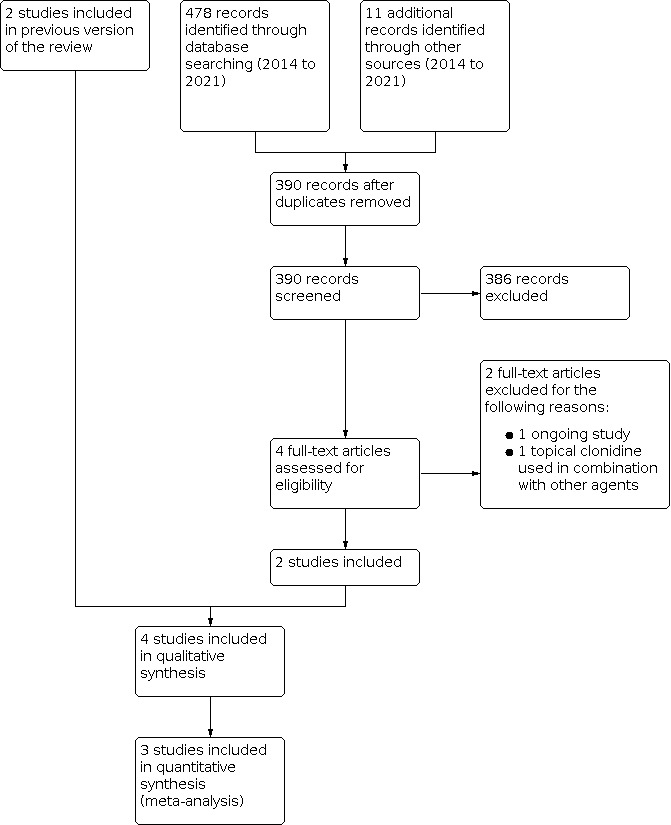
Study flow diagram.
Included studies
All of the included studies were published in English. Three studies were conducted in the USA and one in Iran. Two studies were conducted by the same first author. All four studies assessed the efficacy and safety of topically applied clonidine gel in adult participants with painful diabetic neuropathy (PDN). Three studies compared TC with placebo, and one study compared TC with topical capsaicin. The total number of participants in all four studies was 743.
The study of Campbell 2009 was reported only in abstract form. We contacted the study authors and obtained additional unpublished information. In this study, investigators applied gel to both feet twice daily for two weeks, then three times daily for eight weeks total. A total of 54 participants received 650 µL of 0.1% TC per foot, and another 54 participants received 500 µL of 0.2% clonidine per foot. The control group (57 participants) was given matching placebo.
In Campbell 2012, 91 participants were allocated to the clonidine group and received 650 µg of 0.1% clonidine gel three times daily for 12 weeks. The control group (91 participants) received matching placebo. One participant in each group did not receive the allocated intervention because these participants were found to be ineligible after randomisation. One participant in the clonidine group was excluded from the ITT population because no baseline NRS score was obtained. During the screening phase of the study, researchers assessed nociceptor function by determining pain response to 0.1% topical capsaicin applied to the pretibial area for 30 minutes. Capsaicin responders were defined as participants with pain intensity of 2 or more points on the NRS during capsaicin stimulation; investigators identified 33 such individuals in the clonidine group and 30 in the placebo group.
In NCT02068027, 130 participants were allocated to the clonidine group and received 0.1% clonidine gel, two times daily to both feet for 85 days. The control group (130 participants) received matching placebo. Thirteen participants in the TC group and 16 in the placebo group did not complete the study. The study was reported only as unpublished data.
In Kiani 2015, 70 participants were allocated to the TC group and received 0.1% clonidine gel administered three times daily for 12 weeks on both feet. The control group (69 participants) received 0.75% capsaicin cream administered three times daily on both feet. Sixteen participants in the TC group and 30 in the topical capsaicin group did not complete the study.
Baseline participant characteristics did not differ significantly between groups in all studies. More than 80% of participants had type 2 diabetes. In Campbell 2012, mean duration of diabetes was approximately 10 years, and mean duration of pain was approximately three years; mean baseline pain intensity was about 6.5 points on the NRS. In Kiani 2015, mean duration of diabetes was approximately 10.5 years in the TC group and 8.5 years in the topical capsaicin group, and mean duration of pain was approximately 21 months in the TC group and 18 months in the topical capsaicin group; mean baseline pain intensity was about 7.5 points on the visual analogue scale (VAS). Campbell 2009 and NCT02068027 did not provide this information.
A biotechnology company, Arcion Therapeutics, supported two of the included studies (Campbell 2009; Campbell 2012), and a pharmaceutical company, BioDelivery Sciences International, supported one study (NCT02068027). Kiani 2015 was funded by a grant from Hamedan University of Medical Sciences. In one study authors declared conflicts of interest (Campbell 2012). The authors of Kiani 2015 declared no conflicts of interest. The authors of the other two included studies did not provide information on conflict of interest (Campbell 2009; NCT02068027).
Excluded studies
We excluded six potentially relevant studies from the analysis. Reasons for exclusion included lack of a control group in two studies (Davis 1991; Meno 2001); transdermal (not topical) drug delivery in three studies (Byas‐Smith 1995; Lauretti 2009; Zeigler 1992); and TC used in combination with other drugs in one study (Brutcher 2019). Transdermal application is intended to exert predominantly systemic effects, with skin only a vehicle for administration. This form of application allows slow and gradual release of medication into the bloodstream with relatively constant blood levels. Topical administration exerts mainly peripheral effects at the site of application.
Ongoing studies
We found one registered, randomised study on the efficacy and safety of TC 1% gel compared with placebo or ketamine (NCT00661063). Planned study duration was 12 weeks. The study was to start in 2008, but we have found no study results. We tried to contact study authors by phone and email (as provided in the study description on ClinicalTrials.gov), but have received no response. For details, see Characteristics of ongoing studies.
Risk of bias in included studies
We used Cochrane's domain‐based evaluation table, which is provided in Review Manager Web (RevMan Web 2020), to assess the validity and quality of included trials. Details of the assessment are specified in the Characteristics of included studies table, and summaries of assessments are provided in Figure 2 and Figure 3. None of the studies was at low risk of bias in all domains. We judged one study as having high risk of bias for blinding of participants and personnel (Kiani 2015); two studies as having high risk of bias for incomplete outcome data (Campbell 2009; NCT02068027); one study as having high risk of bias for selective reporting (Campbell 2009); and three studies as having high risk of bias for funding bias (Campbell 2009; Campbell 2012; NCT02068027). We assessed all of the included studies as having unclear risk of bias for allocation concealment, blinding of outcome assessment, and study size. Two studies were at unclear risk of bias for random sequence generation and blinding of participants and personnel (Campbell 2009; NCT02068027).
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Random sequence generation
We assessed two studies as at low risk of bias for random sequence generation (Campbell 2012; Kiani 2015). We judged two studies as having unclear risk of bias for this domain, as the study authors only stated that the study was randomised, providing no information on method of randomisation; however, there was also no information provided suggesting that randomisation was done improperly (Campbell 2009; NCT02068027).
Allocation concealment
We assessed all studies as at unclear risk of bias for allocation concealment. The study authors did not provide information on allocation concealment, although there was also no information provided suggesting that allocation concealment was absent or done improperly.
Blinding
Blinding of participants and personnel
We assessed one study as at low risk of bias for blinding of participants and personnel (Campbell 2012). The study authors stated that the placebo formulation was identical in appearance, consistency, packaging, and labelling as the intervention drug. We judged two studies as having unclear risk of bias for this domain, as study authors provided no information on blinding method, although there was also no information provided suggesting that blinding was done improperly or was not performed (Campbell 2009; NCT02068027). We judged one study as having high risk of bias for this domain, as even though the drugs were packed in no‐label laminated tubes, clonidine was provided in gel form and capsaicin in cream form (Kiani 2015).
Blinding of outcome assessment
We assessed all studies as at unclear risk of bias for blinding of outcome assessment. Study authors did not provide information on whether outcome assessment was blinded or not, although there was also no information provided suggesting that blinding of outcome assessment was done improperly or was not performed.
Incomplete outcome data
We assessed two studies as having low risk of attrition bias, as baseline observation carried forward or multiple imputations by the regression method was used as an imputation method, and clear information about the number of participants lost from observation was provided (Campbell 2012; Kiani 2015). We judged Campbell 2009 as having high risk of attrition bias because the number of participants randomly assigned was not equal to the number described in the demographics table (one participant is missing). Some results are missing, and researchers provide no information about how they dealt with missing data in this study. We judged NCT02068027 as having high risk of attrition bias because 13 participants in the TC group and 16 participants in the placebo group did not complete the study, and no information about how missing data were dealt with is provided by study authors.
Selective reporting
Study protocols were available for three studies, which we assessed as having low risk of reporting bias. Results for all outcomes listed in the protocols were reported and presented clearly. The results were also consistent with the methods section of the studies (Campbell 2012; Kiani 2015; NCT02068027). We judged Campbell 2009 as having high risk of reporting bias because a study protocol was not available, and presentation of results was unclear.
Other potential sources of bias
Study size
All studies included between 50 and 199 participants per treatment arm, and were therefore assessed as at unclear risk of bias for study size.
Funding bias
We assessed one study as at low risk of funding bias, because the study was supported by a grant from Hamedan University of Medical Sciences. Three studies were supported by industry funding and were judged as at high risk of funding bias. A biotechnology company, Arcion Therapeutics, supported two of these studies (Campbell 2009; Campbell 2012), and a pharmaceutical company, BioDelivery Sciences International, supported one study (NCT02068027).
Effects of interventions
Topical clonidine (TC) versus placebo
Three studies (604 participants) evaluated this comparison (Campbell 2009; Campbell 2012; NCT02068027).
Primary outcome measures
Participant‐reported pain relief of 50% or greater during longest follow‐up period
One study (Campbell 2012; 179 participants) in adults with PDN reported on participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks). Thirty‐five per cent of participants in the TC group and 29% of participants in the placebo group achieved this outcome. There was no evidence of a difference between groups (risk ratio (RR) 1.21, 95% confidence interval (CI) 0.78 to 1.86). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Participant‐reported pain relief of 30% or greater during longest follow‐up period
Two studies (Campbell 2009; Campbell 2012; 344 participants) in adults with PDN reported on participant‐reported pain relief of 30% or greater during longest follow‐up period (8 to 12 weeks). Meta‐analysis of the results shows that more participants in the TC group experienced at least 30% pain reduction (48% of participants) compared with those given placebo (36% of participants) during an 8‐ to 12‐week treatment period (RR 1.35, 95% CI 1.03 to 1.77) (Analysis 1.1; Figure 4). The number needed to treat for an additional beneficial outcome (NNTB) to achieve this endpoint was 8.33 (95% CI 4.3 to 50). We judged the certainty of evidence to be very low for this outcome, downgraded for serious study limitations due to risk of bias, imprecision (optimal information size not met), and publication bias (fewer than 200 participants in unpublished null effect studies required to make the result clinically irrelevant).
1.1. Analysis.

Comparison 1: Topical clonidine versus placebo in painful diabetic neuropathy, Outcome 1: Participant‐reported pain relief of 30% or greater during longest follow‐up period
4.

Forest plot of comparison: 1 Topical clonidine versus placebo in painful diabetic neuropathy, outcome: 1.1 Pain relief ≥ 30%.
Much or very much improved on Patient Global Impression of Change scale (PGIC) during longest follow‐up period
One study (Campbell 2012; 179 participants) in adults with PDN reported an outcome defined as much or very much improved on PGIC during longest follow‐up period (12 weeks). There was no evidence of a difference between groups (RR 1.06, 95% CI 0.76 to 1.49). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Very much improved on PGIC during longest follow‐up period
One study (Campbell 2012; 179 participants) in adults with PDN reported an outcome defined as very much improved on PGIC during longest follow‐up period (12 weeks). There was no evidence of a difference between groups (RR 1.82, 95% CI 0.89 to 3.72). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Secondary outcome measures
Withdrawals due to adverse events during longest follow‐up period
One study (Campbell 2012; 179 participants) in adults with PDN reported on withdrawals due to adverse events during longest follow‐up period (12 weeks). There was no evidence of a difference between groups (RR 0.34, 95% CI 0.04 to 3.18). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Participants experiencing at least one adverse event during longest follow‐up period
Two studies (Campbell 2009; Campbell 2012; 344 participants) in adults with PDN reported on participants experiencing at least one adverse event during longest follow‐up period (12 weeks). Meta‐analysis of the results showed no evidence of a difference between groups (11.7% versus 12.9% in TC and placebo groups, respectively; RR 0.65, 95% CI 0.14 to 3.05; Analysis 1.2; Figure 5). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
1.2. Analysis.

Comparison 1: Topical clonidine versus placebo in painful diabetic neuropathy, Outcome 2: Participants experiencing at least 1 adverse event during longest follow‐up period
5.

Forest plot of comparison: 1 Topical clonidine versus placebo in painful diabetic neuropathy, outcome: 1.2 Participants with ≥ 1 adverse event.
Withdrawals due to lack of efficacy during longest follow‐up period
One study (Campbell 2012; 179 participants) in adults with PDN reported on withdrawals due to lack of efficacy during longest follow‐up period (12 weeks). There was no evidence of a difference between groups (RR 1.01, 95% CI 0.06 to 15.92). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Participants experiencing at least one serious adverse event during longest follow‐up period
Two studies (Campbell 2012; NCT02068027; 439 participants) in adults with PDN reported on participants experiencing at least one serious adverse event during longest follow‐up period. Meta‐analysis of the results shows no evidence of a difference between TC and placebo for this outcome (RR 1.71, 95% CI 0.70 to 4.22; Analysis 1.3). We judged the certainty of evidence to be moderate for this outcome, downgraded for serious study limitations due to risk of bias.
1.3. Analysis.

Comparison 1: Topical clonidine versus placebo in painful diabetic neuropathy, Outcome 3: Participants experiencing at least 1 serious adverse event during longest follow‐up period
Campbell 2009 reported one severe adverse event in the placebo group. However, the study did not specify the adverse event and whether it met the criteria for serious adverse events as indicated in this review, thus we did not include the study in the meta‐analysis.
Specific adverse events, in particular somnolence and dizziness during longest follow‐up period
Two studies (Campbell 2009; Campbell 2012; 344 participants) in adults with PDN reported on participants with specific adverse events. Campbell 2012 reported the same number of participants with adverse events associated with the nervous system (two participants per group), which included burning sensation, dizziness, and headache. Campbell 2009 described 11 adverse events associated with the nervous system in the TC group, and eight in the placebo group. The study authors did not specify these adverse events. Meta‐analysis of the results shows no evidence of a difference between TC and placebo for this outcome (RR 0.77, 95% CI 0.35 to 1.68 Analysis 1.4). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
1.4. Analysis.

Comparison 1: Topical clonidine versus placebo in painful diabetic neuropathy, Outcome 4: Participants experiencing at least 1 adverse event associated with the nervous system
Any pain‐related outcome indicating some improvement during longest follow‐up period (including physical and emotional functioning)
One study (Campbell 2012; 179 participants) in adults with PDN reported on pain relief quantified in scales assessing quality of life. Study investigators did not report evidence of a difference between groups for the Brief Pain Inventory, Chronic Pain Sleep Inventory, or Hospital Anxiety and Depression Scale. We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Skin biopsy results
None of the included studies assessed skin biopsy results.
Change in average pain intensity during longest follow‐up period
Pain intensity was reported by participants in their diaries using the NRS.
One study (Campbell 2012; 179 participants) in adults with PDN reported on change in average pain intensity during longest follow‐up period. There was evidence of a difference between groups (2.3‐point reduction in TC group compared with a 1.7‐point reduction in placebo group; mean difference 0.6; P = 0.07). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
TC versus active comparator
One study (139 participants) evaluated topical clonidine versus topical capsaicin (Kiani 2015).
Primary outcome measures
Participant‐reported pain relief of 50% or greater during longest follow‐up period
One study (Kiani 2015; 139 participants) in adults with PDN reported on participant‐reported pain relief of 50% or greater during longest follow‐up period (12 weeks). This outcome was achieved by 57.1% of participants in the TC group and 40.6% of participants in the topical capsaicin group. There was no evidence of a difference between groups (RR 1.41, 95% CI 0.99 to 2.0). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Participant‐reported pain relief of 30% or greater during longest follow‐up period
The included study did not report on participant‐reported pain relief of 30% or greater during longest follow‐up period.
Much or very much improved on PGIC during longest follow‐up period
The included study did not report on much or very much improved on PGIC during longest follow‐up period.
Very much improved on PGIC during longest follow‐up period
The included study did not report on very much improved on PGIC during longest follow‐up period.
Secondary outcome measures
Withdrawals due to adverse events during longest follow‐up period
The included study did not report on withdrawals due to adverse events during longest follow‐up period.
Participants experiencing at least one adverse event during longest follow‐up period
The included study did not report on participants experiencing at least one adverse event during longest follow‐up period.
Withdrawals due to lack of efficacy during longest follow‐up period
The included study did not report on withdrawals due to lack of efficacy during longest follow‐up period.
Participants experiencing at least one serious adverse event during longest follow‐up period
The included study did not report on participants experiencing at least one serious adverse event during longest follow‐up period.
Specific adverse events, in particular somnolence and dizziness during longest follow‐up period
One study (Kiani 2015; 139 participants) in adults with PDN reported on dermatologic complications. More participants (58%) in the topical capsaicin group had dermatologic complications compared with the TC group (5.7%) (RR 0.10, 95% CI 0.04 to 0.26). We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Any pain‐related outcome indicating some improvement during longest follow‐up period (including physical and emotional functioning)
The included study did not report on any pain‐related outcome indicating some improvement during longest follow‐up period (including physical and emotional functioning).
Skin biopsy results
The included study did not report on skin biopsy results.
Change in average pain intensity during longest follow‐up period
One study (Kiani 2015; 139 participants) in adults with PDN reported on change in average pain intensity during longest follow‐up period. Participants reported the reduction in the median pain score from baseline, as assessed by the VAS during follow‐up visits. Study authors reported no evidence of a difference between the TC and topical capsaicin groups. We judged the certainty of evidence to be low for this outcome, downgraded for serious study limitations due to risk of bias, and imprecision (optimal information size not met).
Discussion
Summary of main results
This updated review includes four trials with a total of 743 participants; two of these studies were newly included in this update, and the conclusions have not changed. All studies were conducted in adults with painful diabetic neuropathy (PDN). Studies lasted 8 or 12 weeks and compared topical clonidine (TC) versus placebo (Campbell 2009; Campbell 2012; NCT02068027), or TC versus topical capsaicin (Kiani 2015). 0.1% or 0.2% TC in gel form was applied to the painful area two to three times daily.
There was no evidence of a difference in number of participants with participant‐reported pain relief of 50% or greater during longest follow‐up period; however, the number of participants with participant‐reported pain relief of 30% or greater during longest follow‐up period (8 to 12 weeks) was higher in the TC group compared with the placebo group. Nevertheless, the number needed to treat for an additional beneficial outcome (NNTB) for this outcome was relatively high. Also, one study (179 participants) showed no difference in improvement classified by participants as much or very much improved on Patient Global Impression of Change scale (PGIC) or very much improved on PGIC during longest follow‐up period (12 weeks), based on low certainty evidence. Furthermore, we observed no evidence of a difference in rate of withdrawals due to adverse events, rate of withdrawals due to lack of efficacy, and number of participants experiencing at least one serious adverse event during longest follow‐up period (12 weeks), based on low certainty evidence.
Based on low certainty evidence from one study (139 participants), there was no evidence of a difference between TC and topical capsaicin in participant‐reported pain relief of 50% or greater or change in average pain intensity during longest follow‐up period (12 weeks); however, a lower rate of dermatologic complications was observed in the TC group.
Overall completeness and applicability of evidence
One of the crucial limitations of the available evidence is that all of the studies included in the review were performed in adults with PDN. We found no studies in other neuropathic pain conditions such as trigeminal neuralgia, postherpetic neuralgia, phantom limb pain, and others, hence the evidence does not fully address the review question, and conclusions cannot be generalised to the whole population of adults with neuropathic pain.
It should be noted that in NCT02068027, the study exclusion criteria were very strict; for example, patients with symptomatic or severe coronary insufficiency, clinically significant cardiac conduction disturbances, myocardial infarction (within last 12 months), or moderate to severe cerebrovascular disease were excluded. Yet, many people with diabetes have these cardiovascular diseases. It is therefore uncertain if the study findings are valid for many adults with painful diabetic peripheral neuropathy in clinical practice.
Moreover, in Campbell 2012, participants experienced stimulation with 0.1% capsaicin during the screening phase. Even though topical capsaicin in a concentration of 8% may produce long‐lasting pain relief (Derry 2013), we believe that 0.1% capsaicin should not influence response to clonidine; however, such a situation cannot be ruled out completely. Even though the study authors claim better results amongst capsaicin responders, there is no clear evidence of a difference between TC and placebo in this subgroup of participants in change in PGIC, and results for at least 50% and 30% pain relief are not presented.
Quality of the evidence
Overall, we judged the evidence to be of moderate to very low certainty.
There were three potential problems for which we downgraded the certainty of the evidence, as follows.
Study limitations. The studies were at unclear or high risk for most risk of bias domains: all were at unclear risk of bias for allocation concealment and blinding of outcome assessment; one study was at high risk of bias for blinding of participants and personnel; two studies were at high risk of attrition bias; and three studies were at high risk of bias due to notable funding concerns.
Imprecision of results. For all outcomes except participants experiencing at least one serious adverse event during longest follow‐up period, the optimal information size was not met. Most of the results, excluding participant‐reported pain relief of 30% or greater during longest follow‐up period, had wide confidence intervals crossing the line of no effect and including both benefit and harm.
High probability of publication bias. We assessed publication bias using a method designed to detect the quantity of unpublished data with a null effect required to make any result clinically irrelevant (usually taken to mean an NNTB ≥ 10 in this condition; Moore 2008). In our review, fewer than 200 participants in unpublished null effect studies would rise NNTB to over 10, which indicates a high probability of publication bias.
Potential biases in the review process
We followed the guidelines provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2021a), and took measures to reduce bias in the review process. We used a comprehensive search strategy based on previous Cochrane Reviews for randomised controlled trials on neuropathic pain. We did not restrict our search to topical application of the drug, so that we could identify all relevant studies. Additionally, we searched reference lists of potentially relevant studies and reviews and trial registries and contacted experts in the field. Two review authors independently read abstracts identified by the search. The probability that any important studies were omitted in the search process is low, as is the possibility of bias in this review process.
Two review authors worked independently to assess bias and extract data from the included studies, consulting a third review author when necessary. We contacted study authors whenever we encountered missing information; however, this information was only obtainable in the case of Campbell 2009, and in many cases this lack of information precluded comprehensive data extraction or bias assessment. Moreover, it should be noted that Campbell 2009 was based on the published abstract and on unpublished data provided by study authors, and the assessment of NCT02068027 was based only on unpublished data, so the studies are at high risk of reporting bias.
Whilst we tried to minimise the influence of publication bias in the review process, the review may nevertheless be subject to it. There is one study with no published results (NCT00661063). It is possible that this study has negative results and might, if included into the analysis, have resulted in an NNTB ≥ 10, which would make the results clinically irrelevant.
Moreover, it should be noted that long‐term studies, which are relevant to chronic pain conditions, are missing. This could have serious impact on the conclusions drawn from this review, as long‐term studies might have not confirmed our findings.
Agreements and disagreements with other studies or reviews
In 2019, Yang and colleagues published a review summarising the evidence on the available agents for topical use in people with PDN (without age restriction), including lidocaine plasters or patches, capsaicin cream, gel or patches, amitriptyline cream, clonidine gel, ketamine cream, and other agents (Yang 2019). For topical clonidine (TC), the review included Campbell 2009 and Campbell 2012 studies and referred to a previous version of our review (Wrzosek 2015). The conclusions of that review are consistent with the results of our work.
The Neuropathic Pain Special Interest Group conducted a comprehensive systematic review with meta‐analysis published in 2015 focusing on pharmacotherapy for neuropathic pain in patients of any age (Finnerup 2015). For TC, the review included the Campbell 2012 study, but not the other studies included in our review. Additionally, Finnerup and colleagues included two studies that were excluded from our review due to transdermal, not topical, drug delivery (Byas‐Smith 1995; Zeigler 1992). Both of these studies assessed the efficacy and safety of TC in PDN. The review authors state that GRADE recommendations for TC for neuropathic pain are inconclusive because of discrepant findings; however, they based this conclusion on evidence from different clinical trials than those included in our review.
Authors' conclusions
Implications for practice.
For adults with chronic neuropathic pain
The major implication of this review for people with chronic neuropathic pain is that a higher percentage of adults with painful diabetic neuropathy (PDN) may achieve pain relief of 30% or greater when treated with topical clonidine (TC) compared with placebo (48% versus 36%); however, the evidence for this outcome is very uncertain. Eight more people would have to be treated with TC compared to placebo for one more person to achieve moderate benefit. We found no evidence on how TC works in people with other neuropathic pain conditions.
For clinicians
The major implication of this review for clinicians is that TC may provide some benefit to adults with PDN; however, the available evidence is very uncertain. The percentage of participants who achieved pain relief of 50% or greater was comparable to that in placebo group, although the percentage of participants who achieved pain relief of 30% or greater was higher in the TC group compared with the placebo group (48% versus 36%). The number needed to treat for an additional beneficial outcome (NNTB) for this comparison was over 8, which means that eight more people would have to be treated with TC compared to placebo for one more person to achieve moderate benefit. Other drugs are available for treatment of individuals with PDN with lower NNTB; however, there may be circumstances when an experienced clinician may choose to use it, because the evidence does not exclude beneficial effects in a small percentage of people, especially in situations where other available therapies have failed or as part of multimodal approach to refractive pain syndromes. We found no evidence on how TC works in people with other neuropathic pain conditions.
Some clinicians may be concerned about long‐term safety of the drug and would prefer to see more safety data. There were no differences in numbers of participants with adverse events, numbers of withdrawals due to adverse events or lack of efficacy, and overall withdrawal rate between TC and placebo; however, it is possible that differences may not have been detected due to the relatively low number of included participants and relatively short duration of the trials. As only a very small concentration of clonidine is reached in plasma during topical application (Campbell 2012), it can be assumed that topical use will be associated with rather few important adverse events, although this is not certain.
Another difficulty is that a ready‐to‐use preparation of TC is not currently available, and the drug for topical use has to be prepared by a compounding pharmacy. Moreover, TC does not have US Food and Drug Administration or European Medicines Agency approval for neuropathic pain and thus must be prescribed 'off‐label'.
For policymakers and funders of the intervention
TC may provide some benefit to adults with PDN; however, the available evidence is of very low certainty. The circumstances in which this therapy would be tried are likely only when other available treatment options have failed, or as part of a multimodal approach to refractive pain syndromes. Lack of data precludes any conclusions on the effectiveness of TC in other neuropathic pain conditions.
Implications for research.
General implications
This review has highlighted the lack of good evidence for TC for neuropathic pain treatment. We found very low quality evidence suggesting that TC may provide some benefit to adults with PDN, although only about one out of eight people treated with the drug may achieve pain relief of 30% or greater when compared with placebo. Chronic neuropathic pain is difficult to treat, and even effective pharmaceuticals provide relief to only a minority of people. Future research might thus explore whether it is possible to predict who or which groups of people with PDN will benefit from TC.
Additionally, good‐quality clinical trials are needed to establish the role of TC in other neuropathic pain conditions such as postherpetic neuralgia, trigeminal neuralgia, phantom limb pain, complex regional pain syndrome, and others.
The treatment period of the studies included in this review was 8 to 12 weeks. Longer duration trials would be more appropriate to establish the efficacy of TC in chronic pain conditions. Moreover, trials of longer duration are needed to assess the safety of TC. Extension studies from randomised controlled trials could provide some additional evidence.
Design
The optimal future clinical trial to answer the review question should last 3 months or longer, include a minimum of 400 participants, and have a randomised, double‐blind, placebo‐controlled or parallel‐group design. Proper randomisation method, allocation concealment, and blinding of participants and personnel should be guaranteed. Detection bias should be minimised by the blinding of outcome assessment. Missing data should be managed with last observation carried forward or another reliable imputation method. Presentation of results should be clear. Non‐pharmaceutical industry‐sponsored trials would be preferred whenever possible.
Measurement (endpoints)
Future research should include outcome measures that are relevant to clinical practice. The gold standard for now is the 'responder' analysis, although this has recently been questioned (Mbowe 2020). It might thus be reasonable to present additional 'mean values' analysis to better reflect the real‐life situation.
What's new
| Date | Event | Description |
|---|---|---|
| 27 October 2021 | New search has been performed | Review updated to include the results of a new search on 27 October 2021. |
| 27 October 2021 | New citation required but conclusions have not changed | Two new studies (399 participants) included; GRADE assessment of certainty of evidence added; tiers of evidence removed; conclusions remain unchanged. |
History
Protocol first published: Issue 2, 2014 Review first published: Issue 8, 2015
Acknowledgements
We would like to thank Managing Editor Anna Erskine for her help with the writing of this review and the previous version. We would like to thank Information Specialist Joanne Abbott for helping with the searches.
Cochrane Review Group funding acknowledgement: this project was funded by the National Institute for Health Research (NIHR) via Cochrane Infrastructure funding to the Cochrane Pain, Palliative and Supportive Care Review Group (PaPaS). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Editorial and peer‐reviewer contributions
The Cochrane Pain, Palliative and Supportive Care Review Group (PaPaS) supported the authors in the development of this review.
The following people conducted the editorial process for this article.
Sign‐off Editor (final editorial decision): Dr Neil O'Connell, PaPaS Co‐ordinating Editor, and Reader at Brunel University London.
Managing Editor (selected peer reviewers, collated peer‐reviewer comments, provided editorial guidance to authors, edited the article): Anna Erskine, Oxford University Hospitals (OUH) NHS Foundation Trust, Oxford, UK.
Contact Editor (editorial and methods input): Alessandro Chiarotto, Department of General Practice, Erasmus MC, University Medical Center, Rotterdam, the Netherlands, and Hopin Lee, Centre for Statistics in Medicine, Nuffield Department of Orthopaedics Rheumatology and Musculoskeletal Sciences (NDORMS), University of Oxford, UK.
Information Specialist (preparing search strategy and running searches): Joanne Abbott, Oxford University Hospitals (OUH) NHS Foundation Trust, Oxford, UK.
Copy‐editing: Lisa Winer, Cochrane Copy Edit Support
Peer reviewers (provided comments and made editorial suggestions): Hollie Birkinshaw, Royal Holloway, University of London (clinical/content review), Brian Duncan (consumer review), Juliana Ester Martin Lopez, PhD and Senior Researcher. Health Technology Assessment (clinical/content review), Jennifer Hilgart, Cochrane Editorial and Methods Department (methods review), Thomas PH Shelton, Mid Yorkshire NHS Trust (clinical/content review).
Appendices
Appendix 1. Methodological considerations for chronic pain
There have been several recent changes in how efficacy of conventional and unconventional treatments is assessed in chronic painful conditions. The outcomes are now better defined, particularly with new criteria of what constitutes moderate or substantial benefit (Gewandter 2015); older trials may only report participants with 'any improvement'. Newer trials tend to be larger, thereby avoiding problems from the random play of chance. Newer trials also tend to be longer, up to 12 weeks; longer trials provide a more rigorous and valid assessment of efficacy in chronic conditions. As new standards have evolved for assessing efficacy in neuropathic pain, we are now applying stricter criteria for the inclusion of trials and assessment of outcomes, and are more aware of problems that may affect our overall assessment. The following is a summary of some of the recent insights that must be considered in this new review.
Pain results tend to have a U‐shaped distribution rather than a bell‐shaped distribution. This is true in acute pain (Moore 2011b), back pain (Moore 2010b), and arthritis, as well as in fibromyalgia (Straube 2010); in all cases average results usually describe the experience of almost no one in the trial. Data expressed as averages are potentially misleading, unless they can be proven to be suitable. As a consequence, we have to depend on dichotomous results (the individual either has or does not have the outcome) usually from pain changes or patient global assessments. The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) group has helped with their definitions of minimal, moderate, and substantial improvement (Gewandter 2015). In arthritis, trials shorter than 12 weeks ‐ especially those shorter than eight weeks ‐ overestimate the effect of treatment (Moore 2009); the effect is particularly strong for less effective analgesics, and this may also be relevant in neuropathic‐type pain. The proportion of patients with at least moderate benefit can be small, even with an effective medicine, falling from 60% with an effective medicine in arthritis, to 30% in fibromyalgia (Moore 2009; Straube 2008; Sultan 2008). A Cochrane Review of pregabalin in neuropathic pain and fibromyalgia demonstrated different response rates for different types of chronic pain (higher in diabetic neuropathy and postherpetic neuralgia and lower in central pain and fibromyalgia) (Moore 2009). This indicates that different neuropathic pain conditions should be treated separately from one another, and that pooling should not be done unless there are good grounds for doing so. Finally, currently unpublished individual patient analyses indicate that patients who get good pain relief (moderate or better) have major benefits in many other outcomes, affecting quality of life in a significant way (Moore 2010c).
Appendix 2. CRS Online (CENTRAL) search strategy (2021 update)
#1 MESH DESCRIPTOR PAIN EXPLODE ALL TREES
#2 MESH DESCRIPTOR PERIPHERAL NERVOUS SYSTEM DISEASES EXPLODE ALL TREES
#3 MESH DESCRIPTOR SOMATOSENSORY DISORDERS
#4 MESH DESCRIPTOR MYOFASCIAL PAIN SYNDROMES EXPLODE ALL TREES
#5 MESH DESCRIPTOR POLYMYALGIA RHEUMATICA
#6 ((pain* or discomfort*) near10 (central or complex or rheumat* or muscl* or muscul* or myofasci* or nerv* or neuralg* or neuropath*)):TI,AB,KY
#7 ((fibromyalgi* or fibrost* or FM or FMS)):TI,AB,KY
#8 ((neur* or nerv*) near6 (compress* or damag*)):TI,AB,KY
#9 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8
#10 MESH DESCRIPTOR Clonidine EXPLODE ALL TREES
#11 ((Clonidin* or clofelin or klofelin or m5041t or catapres* or clopheline or m‐5041t or st‐155 or klofenil or isoglaucon or clofenil or hemiton or st155 or catapresan or chlophazolin or gemiton or dixarit)):TI,AB,KY
#12 #10 OR #11
#13 #9 AND #12
Appendix 3. MEDLINE and MEDLINE In‐Process (via Ovid) search strategy (2021 update)
1. exp PAIN/
2. exp PERIPHERAL NERVOUS SYSTEM DISEASES/
3. SOMATOSENSORY DISORDERS/
4. FIBROMYALGIA/ or exp MYOFASCIAL PAIN SYNDROMES/ or POLYMYALGIA RHEUMATICA/
5. ((pain* or discomfort*) adj10 (central or complex or rheumat* or muscl* or muscul* or myofasci* or nerv* or neuralg* or neuropath*)).mp.
6. (fibromyalgi* or fibrost* or FM or FMS).mp.
7. ((neur* or nerv*) adj6 (compress* or damag*)).mp.
8. or/1‐7
9. Clonidine/
10. (Clonidin* or clofelin or klofelin or m5041t or catapres* or clopheline or m‐5041t or st‐155 or klofenil or isoglaucon or clofenil or hemiton or st155 or catapresan or chlophazolin or gemiton or dixarit).mp.
11. or/9‐10
12. 8 and 11
13. randomized controlled trial.pt.
14. controlled clinical trial.pt.
15. randomized.ab.
16. placebo.ab.
17. drug therapy.fs.
18. randomly.ab.
19. trial.ab.
20. or/13‐19
21. exp animals/ not humans.sh.
22. 20 not 21
23. 12 and 22
Appendix 4. Embase search strategy (via Ovid) (2021 update)
1. exp PAIN/
2. exp PERIPHERAL NERVOUS SYSTEM DISEASES/
3. SOMATOSENSORY DISORDERS/
4. FIBROMYALGIA/ or exp MYOFASCIAL PAIN SYNDROMES/ or POLYMYALGIA RHEUMATICA/
5. ((pain* or discomfort*) adj10 (central or complex or rheumat* or muscl* or muscul* or myofasci* or nerv* or neuralg* or neuropath*)).mp.
6. (fibromyalgi* or fibrost* or FM or FMS).mp.
7. ((neur* or nerv*) adj6 (compress* or damag*)).mp.
8. or/1‐7
9. Clonidine/
10. (Clonidin* or clofelin or klofelin or m5041t or catapres* or clopheline or m‐5041t or st‐155 or klofenil or isoglaucon or clofenil or hemiton or st155 or catapresan or chlophazolin or gemiton or dixarit).mp.
11. or/9‐10
12. 8 and 11
13. random$.tw.
14. factorial$.tw.
15. crossover$.tw.
16. cross over$.tw.
17. cross‐over$.tw.
18. placebo$.tw.
19. (doubl$ adj blind$).tw.
20. (singl$ adj blind$).tw.
21. assign$.tw.
22. allocat$.tw.
23. volunteer$.tw.
24. Crossover Procedure/
25. double‐blind procedure.tw.
26. Randomized Controlled Trial/
27. Single Blind Procedure/
28. or/13‐27
29. (animal/ or nonhuman/) not human/
30. 28 not 29
31. 12 and 30
Appendix 5. Data extraction form
Study ID
| Methods | |
| Participants | Inclusion criteria: Exclusion criteria: Number of participants screened/enrolled: Number of randomly assigned participants (C/P): Number of participants who received allocated intervention (C/P): Mean age (C/P): Number of males (C/P): Duration of pain condition (years ± SD; C/P): Mean baseline pain intensity (NRS; mean ± SD; C/P): |
| Interventions | Intervention group: Control group: |
| Outcomes | |
| Notes | |
C: clonidine group; P: placebo group.
Risk of bias assessment
| Domain | Risk of bias | Support for judgement | ||
| Low risk | High risk | Unclear | ||
|
Random sequence generation (selection bias) |
||||
|
Allocation concealment (selection bias) |
||||
|
Blinding of participants and personnel (performance bias) |
|
|||
|
Blinding of outcome assessment (detection bias) |
|
|||
|
Incomplete outcome data (attrition bias) |
||||
|
Selective outcome reporting (reporting bias) |
||||
| Size of study | ||||
| Notes: | ||||
Data and analyses
Comparison 1. Topical clonidine versus placebo in painful diabetic neuropathy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Participant‐reported pain relief of 30% or greater during longest follow‐up period | 2 | 344 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [1.03, 1.77] |
| 1.2 Participants experiencing at least 1 adverse event during longest follow‐up period | 2 | 344 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.14, 3.05] |
| 1.3 Participants experiencing at least 1 serious adverse event during longest follow‐up period | 2 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.71 [0.70, 4.22] |
| 1.4 Participants experiencing at least 1 adverse event associated with the nervous system | 2 | 344 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.35, 1.68] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Campbell 2009.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled study with 8‐week treatment period | |
| Participants | Adults with PDN Number of randomly assigned participants (C 0.1%/C 0.2%/P): 166 (54/54/57) Study authors declare that 166 participants were randomly assigned; however, only 165 are described in the demographics table. |
|
| Interventions | Intervention groups: 0.1% clonidine gel, 2 times daily, 650 µL per foot for the first 2 weeks and 3 times daily thereafter (n = 54) 0.2% clonidine gel, 2 times daily, 500 µL per foot for the first 2 weeks and 3 times daily thereafter (n = 54) Control group: placebo applied in the same way (n = 57) |
|
| Outcomes | Numerical pain rating scale (NRS) Participants with > 30% pain reduction Adverse events |
|
| Notes | Unpublished data acquired from study authors. Conducted in the USA, multiple locations; no information on type of hospitals (primary, secondary, or tertiary care) No information on how participants were recruited Participants were allowed to remain on concomitant medications. Duration of pain: information not provided Funding: the study was supported by biotechnology company, Arcion Therapeutics Conflict of interest of study authors: no information provided |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Process of randomisation is not described in detail in the study, although the authors state that the study is randomised, and there is no information suggesting that randomisation was done improperly. |
| Allocation concealment (selection bias) | Unclear risk | There is no information about allocation concealment in the study, although there is also no information suggesting that allocation concealment was absent or done improperly. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No detailed information on method of blinding participants and personnel provided in the study, although there is also no information suggesting that blinding of participants and personnel was done improperly or not performed |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No detailed information on method of blinding of outcome assessment provided in the study, although there is also no information suggesting that blinding of outcome assessment was done improperly or not performed |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Number of randomly assigned participants not equal to the number described in the demographics table (1 participant missing). Some results are missing. |
| Selective reporting (reporting bias) | High risk | Study protocol not available. Presentation of results not clear. |
| Study size | Unclear risk | Size of study: more than 50 and fewer than 199 participants per treatment arm |
| Funding bias | High risk | A biotechnology company, Arcion Therapeutics, supported the study. |
Campbell 2012.
| Study characteristics | ||
| Methods | Randomised, double‐blind, multicentre (USA), parallel‐group study, 12‐week treatment period Study consists of a screening phase (28 ± 7 days), baseline phase (7 days), treatment phase, and follow‐up period. During screening phase, nociceptor function was tested by determining pain response to 0.1% topical capsaicin applied to the pretibial area of each participant for 30 minutes. |
|
| Participants | Inclusion criteria:
Exclusion criteria:
Number of patients screened: 464 Number of randomly assigned patients (C/P): 182 (91/91) Number of participants who received allocated intervention (C/P): 180 (90/90) Mean age (C/P): 59.4/57.6 years Number of males (C/P): 44/42 Duration of foot pain (years ± SD; C/P): 3.0 ± 1.3/2.9 ± 1.3 Mean baseline pain (0‐to‐10 NRS ± SD; C/P): 6.4 ± 1.4/6.5 ± 1.5 |
|
| Interventions | Intervention group: clonidine gel 650 µg per foot, 3 times daily, concentration 0.1% self administered on both feet (n = 91) Control group: matching placebo (n = 91) 464 participants were screened, 182 were randomly assigned (91/91), 90 participants in both groups received allocated intervention (1 participant in each group was found to be ineligible after randomisation), 1 participant in the clonidine group was excluded from analysis because no baseline NRS score was available. Intention‐to‐treat population: clonidine 89/placebo 90 Discontinuation: participants lost to follow‐up: C: 3/P: 4; withdrawal of participant consent: C: 1/P: 1; protocol violation: C: 2/P: 4; adverse events: C: 1/P: 3; lack of efficacy: C: 1/P: 1 |
|
| Outcomes | Participants with > 30% pain reduction Participants with > 50% pain reduction Avarage pain severity Brief Pain Inventory: severity scale, average pain, functional interference scale Chronic Pain Sleep Inventory: overall seep quality Clinician and Patient Global Impressions of Change: overall change in pain status Hospital Anxiety and Depression Scale: anxiety scale, depression scale Adverse events |
|
| Notes | Conducted in the USA, tertiary care setting (university hospital) No information on how the patients were recruited Participants discontinued use of "as needed" pain medications other than paracetamol, daily pain medications were continued on stable daily dosing. 97 participants underwent a 3‐millimetre skin punch biopsy performed to quantify intraepidermal nerve fibre density. Duration of pain (years): TC 3.0/capsaicin 2.9 Funding: the study was supported by biotechnology company, Arcion Therapeutics Conflict of interest of study authors: CMC was awarded a travel grant from Arcion to present and attend the Neuropathic Pain Conference in 2008. BS, MK, and WKS consult for Arcion. KB and JNC are employed by Arcion. The other authors have no conflicts of interest. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation in blocks with stratifications with regard to baseline pain severity |
| Allocation concealment (selection bias) | Unclear risk | There is no information about allocation concealment in the study, although there is also no information suggesting that allocation concealment was absent or done improperly. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Placebo formulation was identical in appearance, consistency, packaging, and labelling. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No detailed information on method of blinding of outcome assessment provided in the study, although there is also no information suggesting that blinding of outcome assessment was done improperly or not performed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Baseline observation carried forward in cases of missing results |
| Selective reporting (reporting bias) | Low risk | Study protocol available, results for all outcomes listed in the protocol presented in a clear way. |
| Study size | Unclear risk | Size of study: more than 50 and fewer than 199 participants per treatment arm |
| Funding bias | High risk | The study was supported by biotechnology company, Arcion Therapeutics. |
Kiani 2015.
| Study characteristics | ||
| Methods | Randomised, double‐blind, parallel‐group study with 12‐week treatment period | |
| Participants | Adults with type 2 diabetes, aged 30 to 70 years, who had PDN Inclusion criteria:
Exclusion criteria:
Number of patients screened: 278 Number of randomly assigned patients (TC/capsaicin): 139 (70/69) Number of participants who received allocated intervention (TC/capsaicin): 139 (70/69) Mean age (TC/capsaicin): 56.9/56.5 years Number of males (TC/capsaicin): 18/20 Duration of foot pain (months ± SD; TC/capsaicin): 21.2 ± 30.0/18.0 ± 16.57 Mean baseline pain (0‐to‐10 VAS ± SD; TC/capsaicin): 7.8 ± 1.7/7.5 ± 1.5 |
|
| Interventions | Intervention group: 0.1% clonidine gel self administered 3 times daily on both feet, below the ankles (n = 70) Control group: 0.75% capsaicin cream self administered 3 times daily on both feet, below the ankles (n = 69) 278 participants were screened, 157 were eligible, 139 were randomly assigned (70/69), 139 participants (70 TC/69 capsaicin) received allocated intervention. Intention‐to‐treat population: TC 70/capsaicin 69 Discontinuation: TC 16/capsaicin 30; reasons for discontinuation not provided |
|
| Outcomes | Participants with ≥ 50% pain reduction Reduction in median pain score from baseline, as assessed by VAS Adverse events |
|
| Notes | Conducted in Iran, tertiary care setting (university hospital) No information on how the patients were recruited Duration of pain (months): TC 21.2/capsaicin 18.0 Funding: the study was supported by a grant from Hamedan University of Medical Sciences (project number: D/P/16/35/2666). Unichem Laboratories (India) via the Kimiara Company in Iran provided clonidine as free sample, and capsaicin was provided by Kish Medipharm Pharmaceutical Company (Iran) Conflict of interest of study authors: study authors declared no conflict of interest |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation done by permuted‐block design. |
| Allocation concealment (selection bias) | Unclear risk | There is no information about allocation concealment in the study, although there is also no information suggesting that allocation concealment was absent or done improperly. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Although drugs were packed in no‐label laminated tubes, clonidine was provided in gel form and capsaicin in cream form. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No detailed information on method of blinding of outcome assessment provided in the study, although there is also no information suggesting that blinding of outcome assessment was done improperly or not performed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Multiple imputations by the regression method was used in case of missing data. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. Results for all outcomes listed in the protocol available and presented clearly. |
| Study size | Unclear risk | Size of study: more than 50 and fewer than 199 participants per treatment arm |
| Funding bias | Low risk | The study was supported by a grant from Hamedan University of Medical Sciences. |
NCT02068027.
| Study characteristics | ||
| Methods | Multicentre, randomised, double‐blind, placebo‐controlled study The study included 5 phases: Screening Phase (up to 21 days duration), Baseline Phase (Day 14 to Day 8), Placebo Lead in Phase (Day −7 to Day 1), Double blind Treatment Phase (85 days), and a Post‐treatment Follow up Phase (7 days, only for participants not enrolling in the open‐label long‐term safety study, CLO 311). |
|
| Participants | Adults with PDN Number of randomly assigned patients (C/P): 260 (130/130) Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Intervention group: 0.1% clonidine gel, 2 times daily to both feet (n = 130) Control group: placebo applied in the same way (n = 130) |
|
| Outcomes | Change From Baseline to Day 84 (Week 12) assessed by participants using numeric pain rating scale score Mean Daily Worst Pain Intensity ‐ numeric pain rating scale scores Serious adverse events |
|
| Notes | Conducted in the USA, multiple locations, no information on type of hospitals (primary, secondary, or tertiary care) No information on how participants were recruited Duration of pain: information not provided Funding: the study was supported by pharmaceutical company, BioDelivery Sciences International Conflicts of interest of study authors: no information provided |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Process of randomisation not described in detail in the study, although the authors state that the study is randomised, and there is no information suggesting that randomisation was done improperly. |
| Allocation concealment (selection bias) | Unclear risk | There is no information about allocation concealment in the study, although there is also no information suggesting that allocation concealment was absent or done improperly. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No detailed information on method of blinding of participants and personnel provided in the study, although there is also no information suggesting that blinding of participants and personnel was done improperly or not performed |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No detailed information on method of blinding of outcome assessment provided in the study, although there is also no information suggesting that blinding of outcome assessment was done improperly or not performed |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 13 participants in TC group and 16 in placebo group did not complete the study. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. Results for all outcomes listed in the protocol available and presented clearly. |
| Study size | Unclear risk | Size of study: more than 50 and fewer than 199 participants per treatment arm |
| Funding bias | High risk | The study was supported by pharmaceutical company BioDelivery Sciences International. |
C: clonidine ECG: electrocardiogram NRS: numerical pain rating scale P: placebo PDN: painful diabetic neuropathy SD: standard deviation TC: topical clonidine VAS: visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Brutcher 2019 | Topical clonidine used in combination with topical ketamine, gabapentin, and lidocaine in a compounded cream |
| Byas‐Smith 1995 | Transdermal, not topical, drug delivery |
| Davis 1991 | Lack of a control group |
| Lauretti 2009 | Transdermal, not topical, drug delivery |
| Meno 2001 | Lack of a control group |
| Zeigler 1992 | Transdermal, not topical, drug delivery |
Characteristics of ongoing studies [ordered by study ID]
NCT00661063.
| Study name | Diabetic neuropathy topical treatment |
| Methods | Randomised, double‐blind, placebo‐controlled, parallel‐group study Study duration: 12 weeks |
| Participants | Patients with a diagnosis of diabetes mellitus type 1 or 2 and mononeuropathy or polyneuropathy. Patients had to be treated with tricyclic antidepressants or carbamazepine ≥ 3 weeks. Age ≥ 18 years |
| Interventions | Participants were to receive clonidine 1% gel or ketamine 150 μg/g twice a day or both, or placebo. |
| Outcomes | Pain evaluation by visual analogue scale Pain evaluation by amount of rescue medication required |
| Starting date | Study should have started in 2008; however, no results were available until now. We tried to contact the study author but without success. |
| Contact information | Judymara L Gozzani; gozzani@osite.com.br |
| Notes |
Differences between protocol and review
There were several differences between the protocol and the review, as follows.
In the protocol, we planned to analyse evidence in two tiers. The Cochrane Pain, Palliative and Supportive Care (PaPaS) Group recommendations have changed since that time and advise GRADE assessment of the evidence, therefore we have assessed certainty of evidence according to GRADE guidelines in this version of the review.
In their recent work, Mbowe and colleagues demonstrated that "responder" analyses based on pain reduction thresholds may not always reflect the real‐life effectiveness of drugs (Mbowe 2020), therefore as the evidence in our review was limited, for illustrative purposes we decided to include an additional secondary (continuous) outcome: change in average pain intensity during longest follow‐up period.
In the protocol, we planned to investigate possible reasons of heterogeneity when I2 was greater then 50%. In the final review we regarded statistical heterogeneity as low if the I2 statistic was less than 30%; moderate if between 30% and 50%; substantial if between 50% and 75%; and considerable if above 75%.
Contributions of authors
Conceiving of the review: WS, AW
Co‐ordinating the review: WS, AW
Undertaking manual searches: WS, AW, RZ, JJ, J Woron, J Wordliczek, JG
Screening search results: WS, AW, RZ, JJ, J Woron, JG
Organising retrieval of papers: AW, WS
Screening retrieved papers against inclusion criteria: WS, AW, RZ, JJ, J Woron, J Wordliczek
Appraising quality of papers: WS, AW, RZ, JJ, JD, J Wordliczek
Extracting data from papers: WS, AW, JJ, J Wordliczek
Writing to authors of papers for additional information: AW
Obtaining and screening data on unpublished studies: WS, AW, JJ, J Woron, J Wordliczek
Managing data for the review: WS, AW
Entering data into Review Manager Web: AW
Analysing Review Manager Web statistical data: AW
Performing other statistical analysis not using Review Manager Web: none
Double‐checking data entered by person one: WS
Writing the review: WS, AW, JJ, J Woron, JD, J Wordliczek, JG
Providing general advice on the conduct of this review: J Wordliczek, JD
Taking responsibility for reading and checking the review before submission: WS, AW
All authors will be responsible for future updates.
Sources of support
Internal sources
New Source of support, Other
External sources
-
National Institute for Health Research (NIHR), UK
Cochrane Infrastructure funding to the Cochrane Pain, Palliative and Supportive Care Review Group (PaPaS)
Declarations of interest
Wojciech Serednicki has no relevant conflicts of interest to declare. Dr Serednicki is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
Anna Wrzosek has no relevant conflicts of interest to declare. Dr Wrzosek is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
Jaroslaw Woron has no relevant conflicts of interest to declare.
Jaroslaw Garlicki has no relevant conflicts of interest to declare. Dr Garlicki is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
Jan Dobrogowski has no relevant conflicts of interest to declare.
Joanna Jakowicka‐Wordliczek has no relevant conflicts of interest to declare. Dr Jakowicka‐Wordliczek is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
Jerzy Wordliczek has no relevant conflicts of interest to declare. Dr Wordliczek is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
Renata Zajaczkowska has no relevant conflicts of interest to declare. Dr Zajaczkowska is a specialist in Anaesthesiology and Intensive Therapy and deals with patients with chronic pain conditions and patients hospitalised in the intensive care unit.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Campbell 2009 {published and unpublished data}
- Campbell C, Campbell J, Schmidt W, Brady K, Stouch B.Topical clonidine gel reduces pain caused by diabetic neuropathy: results of a multicenter, placebo-controlled clinical trial. Journal of Pain 2009;4:S55. [Google Scholar]
Campbell 2012 {published data only}
- Campbell CM, Kipnes MS, Stouch BC, Brady KL, Kelly M, Schmidt WK, et al.Randomized control trial of topical clonidine for treatment of painful diabetic neuropathy. Pain 2012;153(9):1815-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kiani 2015 {published data only}
- Kiani J, Sajedi F, Nasrollahi SA, Esna-Ashari F.A randomized clinical trial of efficacy and safety of the topical clonidine and capsaicin in the treatment of painful diabetic neuropathy. Journal of Research in Medical Sciences 2015;20(4):359-63. [PMC free article] [PubMed] [Google Scholar]
NCT02068027 {unpublished data only}
- NCT02068027.Safety and efficacy study of clonidine hydrochloride topical gel, 0.1%, in the treatment of pain associated with diabetic neuropathy. www.clinicaltrials.gov/ct2/show/NCT02068027 (first received 20 February 2014).
References to studies excluded from this review
Brutcher 2019 {published data only}
- Brutcher R, Kurihara C, Bicket M, Moussavian-Yousefi P, Reece D, Solomon L, et al.Compounded topical pain creams to treat localized chronic pain: a randomized controlled trial. Annals of Internal Medicine 2019;170(5):309-18. [DOI] [PubMed] [Google Scholar]
Byas‐Smith 1995 {published data only}
- Byas-Smith MG, Max MB, Muir J, Kingman ACN.Transdermal clonidine compared to placebo in painful diabetic neuropathy using a two-stage 'enriched enrollment' design. Pain 1995;60(3):267-74. [DOI] [PubMed] [Google Scholar]
Davis 1991 {published data only}
- Davis KD, Treede RD, Raja SN, Meyer RA, Campbell JN.Topical application of clonidine relieves hyperalgesia in patients with sympathetically maintained pain. Pain 1991;47(3):309-17. [DOI] [PubMed] [Google Scholar]
Lauretti 2009 {published data only}
- Lauretti GR, Mattos AL, Lima ICPR, Matsumoto M, Resende CS.The clinical and laboratorial evaluation of transdermal ketamine, fentanyl, clonidine or their combination in chronic low back pain. European Journal of Pain 2009;13:S126. [Google Scholar]
Meno 2001 {published data only}
- Meno A, Arita H, Hanaoka K.Preliminary report: the efficacy of clonidine hydrochloride ointment for postherpetic neuralgia. Masui - Japanese Journal of Anesthesiology 2001;50(2):160-3. [PubMed] [Google Scholar]
Zeigler 1992 {published data only}
- Zeigler D, Lynch SA, Muir J, Benjamin J, Max MBCN.Transdermal clonidine versus placebo in painful diabetic neuropathy. Pain 1992;48(3):403-8. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
NCT00661063 {published data only}
- NCT00661063.Diabetic neuropathy topical treatment. www.clinicaltrials.gov/ct2/show/NCT00661063 (first received 18 April 2008).
Additional references
Aley 1997
- Aley KO, Levine JD.Multiple receptors involved in peripheral alpha 2, mu, and A1 antinociception, tolerance, and withdrawal. Journal of Neuroscience 1997;17(2):735–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Andrew 2014
- Andrew R, Derry S, Taylor RS, Straube S, Phillips CJ.The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Practice 2014;14(1):79-94. [DOI] [PubMed] [Google Scholar]
Anitescu 2013
- Anitescu M, Benzon HT, Argoff CE.Advances in topical analgesics. Current Opinion in Anaesthesiology 2013;25(5):551-61. [DOI] [PubMed] [Google Scholar]
Apkarian 2011
- Apkarian AV, Hashmi JA, Baliki MN.Pain and the brain: specificity and plasticity of the brain in clinical chronic pain. Pain 2011;152(3 Suppl):S49-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Asano 2000
- Asano T, Dohi S, Ohta S, Shimonaka H, Lida H.Antinociception by epidural and systemic alpha(2)-adrenoceptor agonists and their binding affinity in rat spinal cord and brain. Anesthesia & Analgesia 2000;90(2):400–7. [DOI] [PubMed] [Google Scholar]
Bates 2019
- Bates D, Carsten SB, Hanes MC, Jolly SM, Chakravarthy KV, Deer TR, et al.A comprehensive algorithm for management of neuropathic pain. Pain Medicine (United States) 2019;20(Suppl 1):S2-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bernard 1994
- Bernard JM, Kick O, Bonnet F.Which way for the administration of alpha2-adrenergic agents to obtain the best analgesia? Cahiers d Anesthésiologie 1994;42(2):223–8. [PubMed] [Google Scholar]
Bouhassira 2008
- Bouhassira D, Lanteri-Minet M, Attal N, Laurent B, Touboul C.Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008;136:380–7. [DOI] [PubMed] [Google Scholar]
Bouhassira 2019
- Bouhassira D.Neuropathic pain: definition, assessment and epidemiology. Revue Neurologique 2019;175(1-2):16-25. [PMID: ] [DOI] [PubMed] [Google Scholar]
Buerkle 1998
- Buerkle H, Yaksh TL.Pharmacological evidence for different alpha2-adrenergic receptor sites mediating analgesia and sedation in the rat. British Journal of Anaesthesia 1998;81(2):208–15. [DOI] [PubMed] [Google Scholar]
Buerkle 2000
- Buerkle H.Peripheral antinociceptive action of alpha2-adrenoceptoragonist. Baillière's Clinical Anaesthesiology 2000;2:411–8. [Google Scholar]
Chi 2007
- Chi L, Sekiyama H, Hayashida M, Takeda K, Sumida T, Sawamura S, et al.Effects of topical application of clonidine cream on pain behaviors and spinal Fos protein expression in rat models of neuropathic pain, postoperative pain, and inflammatory pain. Anesthesiology 2007;107(3):486-94. [DOI] [PubMed] [Google Scholar]
Crespo 2017
- Crespo S, Dangelser G, Haller G.Intrathecal clonidine as an adjuvant for neuraxial anaesthesia during caesarean delivery: a systematic review and meta-analysis of randomised trials. International Journal of Obstetric Anesthesia 2017;32:64-76. [DOI] [PubMed] [Google Scholar]
Derry 2012
- Derry S, Moore RA.Topical capsaicin (low concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2012, Issue 9. Art. No: CD010111. [DOI: 10.1002/14651858.CD010111] [DOI] [PMC free article] [PubMed] [Google Scholar]
Derry 2013
- Derry S, Sven-Rice A, Cole P, Tan T, Moore RA.Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No: CD007393. [DOI: 10.1002/14651858.CD007393.pub3] [DOI] [PubMed] [Google Scholar]
Derry 2017
- Derry S, Wiffen PJ, Kalso EA, Bell RF, Aldington D, Phillips T, et al.Topical analgesics for acute and chronic pain in adults - an overview of Cochrane Reviews. Cochrane Database of Systematic Reviews 2017, Issue 5. Art. No: CD008609. [DOI: 10.1002/14651858.CD008609.pub2] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dias 1999
- Dias VC, Tendler B, Oparil S, Reilly PA, Snar P, White WB.Clinical experience with transdermal clonidine in African-American and Hispanic-American patients with hypertension: evaluation from a 12-week prospective, open-label clinical trial in community-based clinics. American Journal of Therapeutics 1999;6(1):19–24. [DOI] [PubMed] [Google Scholar]
Dogrul 2004
- Dogrul A, Uzbay IT.Topical clonidine antinociception. Pain 2004;111(3):385-91. [DOI] [PubMed] [Google Scholar]
Eisenach 1995
- Eisenach JC, DuPen S, Dubois M, Miguel R, Allin D, Epidural Clonidine Study Group 2.Epidural clonidine analgesia for intractable cancer pain. Pain 1995;61(3):391–9. [DOI] [PubMed] [Google Scholar]
Eisenach 1996
- Eisenach JC, De Kock M, Klimscha W.Alpha2-adrenergic agonists for regional anesthesia: a clinical review of clonidine (1984–1995). Anesthesiology 1996;85:655–74. [DOI] [PubMed] [Google Scholar]
Fayaz 2016
- Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT.Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open 2016;6:e010364. [DOI] [PMC free article] [PubMed] [Google Scholar]
Finnerup 2015
- Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, et al.Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurology 2015;14(2):162-73. [PMID: 25575710] [DOI] [PMC free article] [PubMed] [Google Scholar]
Flores 2012
- Flores MP, Castro AP, Nascimento Jdos S.Topical analgesics. Revista Brasileira de Anestesiologia 2012;62(2):244-52. [DOI] [PubMed] [Google Scholar]
Gentili 1996
- Gentili M, Juhel A, Bonnet F.Peripheral analgesic effect of intra-articular clonidine. Pain 1996;64(3):593–6. [DOI] [PubMed] [Google Scholar]
Gentili 1997
- Gentili M, Houssel P, Osman M, Henel D, Juhel A, Bonnet F.Intra-articular morphine and clonidine produce comparable analgesia but the combination is not more effective. British Journal of Anaesthesia 1997;79(5):660–1. [DOI] [PubMed] [Google Scholar]
Gewandter 2015
- Gewandter JS, Dworkin RH, Turk DC, Farrar JT, Fillingim RB, Gilron I, et al.Research design considerations for chronic pain prevention clinical trials: IMMPACT recommendations. Pain 2015;156(7):1184-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT.Version accessed 5 March 2022. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Gustorff 2008
- Gustorff B, Dorner T, Likar R, Grisold W, Lawrence K, Schwarz F, et al.Prevalence of self-reported neuropathic pain and impact on quality of life: a prospective representative survey. Acta Anaesthesiologica Scandinavica 2008;52(1):132-6. [DOI] [PubMed] [Google Scholar]
Hall 2008
- Hall GC, Carroll D, McQuay HJ.Primary care incidence and treatment of four neuropathic pain conditions: a descriptive study, 2002-2005. BMC Family Practice 2008;9:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hassenbusch 2002
- Hassenbusch SJ, Gunes S, Wachsman S, Willis KD.Intrathecal clonidine in the treatment of intractable pain: a phase I/II study. Pain Medicine 2002;3:85–91. [DOI] [PubMed] [Google Scholar]
Higgins 2021a
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s).Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Higgins 2021b
- Deeks JJ, Higgins JPT, Altman DG, Schünemann HJ, Vist GE, Glasziou P, et al.Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Higgins 2021c
- Schünemann HJ, Higgins JPT, Vist GE, Glasziou P, Akl EA, Skoetz N, et al.Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Hurley 2013
- Hurley RW, Adams MC, Benzon HT.Neuropathic pain: treatment guidelines and updates. Current Opinion in Anaesthesiology 2013;26(5):580-7. [DOI] [PubMed] [Google Scholar]
Jadad 1996
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al.Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clinical Trials 1996;17(1):1-12. [DOI] [PubMed] [Google Scholar]
Jensen 2011
- Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, et al.A new definition of neuropathic pain. Pain 2011;152(10):2204-5. [DOI] [PubMed] [Google Scholar]
Kawaski 2003
- Kawasaki Y, Kumamoto E, Furue H, Yoshimura M.Alpha 2 adrenoceptor mediated presynaptic inhibition of primary afferent glutamatergic transmission in rat substantia gelatinosa neurons. Anesthesiology 2003;98(3):682–9. [DOI] [PubMed] [Google Scholar]
Khaliq 2007
- Khaliq W, Alam S, Puri N.Topical lidocaine for the treatment of postherpetic neuralgia. Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No: CD004846. [DOI: 10.1002/14651858.CD004846.pub2] [DOI] [PubMed] [Google Scholar]
Khan 1999
- Khan ZP, Ferguson CN, Jones RM.Alpha-2 and imidazoline receptor agonists. Their pharmacology and therapeutic role. Anaesthesia 1999;54(2):146-65. [DOI] [PubMed] [Google Scholar]
Kolesnikov 1999
- Kolesnikov YA, Pasternak GW.Topical opioid in mice: analgesia and reversal of tolerance by a topical N-methyl-D-aspartate antagonist. Journal of Pharmacology and Experimental Therapeutics 1999;290:247–52. [PubMed] [Google Scholar]
Kolesnikov 2000
- Kolesnikov YA, Chereshnev I, Pasternak GW.Analgesic synergy between topical lidocaine and topical opioids. Journal of Pharmacology and Experimental Therapeutics 2000;295:546-51. [PubMed] [Google Scholar]
Koopman 2009
- Koopman JS, Dieleman JP, Huygen FJ, Mos M, Martin CG, Sturkenboom MC.Incidence of facial pain in the general population. Pain 2009;147(1-3):122-7. [DOI] [PubMed] [Google Scholar]
Lavand'homme 2002
- Lavand‘homme PM, Ma W, De KM, Eisenach JC.Perineural alpha(2A)-adrenoceptor activation inhibits spinal cord neuroplasticity and tactile allodynia after nerve injury. Anesthesiology 2002;97:972–80. [DOI] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al.The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339:b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lunn 2009
- Lunn MP, Hughes RA, Wiffen PJ.Duloxetine for treating painful neuropathy or chronic pain. Cochrane Database of Systematic Reviews 2009, Issue 4. Art. No: CD007115. [DOI: 10.1002/14651858.CD007115.pub2] [DOI] [PubMed] [Google Scholar]
Macone 2018
- Macone A, Otis JAD.Neuropathic pain. Seminars in Neurology 2018;38(6):644-53. [PMID: ] [DOI] [PubMed] [Google Scholar]
Mbowe 2020
- Mbowe O, Gewandter J, Turk D, Dworkin R, McDermott M.Are there really only 2 kinds of people in the world? Evaluating the distribution of change from baseline in pain clinical trials. Pain 2020;161(1):195-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
McQuay 2007
- McQuay HJ, Smith LA, Moore RA.Chronic pain. In: Stevens A, Raftery J, Mant J, Simpson S, editors(s). Health Care Needs Assessment. 3rd series edition. Oxford: Radcliffe Publishing, 2007. [Google Scholar]
Moisset 2007
- Moisset X, Bouhassira D.Brain imaging of neuropathic pain. Neuroimaging 2007;37(Suppl 1):S80-8. [DOI] [PubMed] [Google Scholar]
Moore 1998
- Moore RA, Gavaghan D, Tramèr MR, Collins SL, McQuay HJ.Size is everything - large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209-16. [DOI] [PubMed] [Google Scholar]
Moore 2008
- Moore RA, Barden J, Derry S, McQuay HJ.Managing potential publication bias. In: McQuay HJ, Kalso E, Moore RA, editors(s). Systematic Reviews in Pain Research: Methodology Refined. Seattle: IASP Press, 2008:15-24. [ 978–0–931092–69–5] [Google Scholar]
Moore 2009
- Moore RA, Straube S, Wiffen PJ, Derry S, McQuay HJ.Pregabalin for acute and chronic pain in adults. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No: CD007076. [DOI: 10.1002/14651858.CD007076.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2010a
- Moore RA, Eccleston C, Derry S, Wiffen P, Bell RF, Straube S, et al."Evidence" in chronic pain - establishing best practice in the reporting of systematic reviews. Pain 2010;150:386-9. [DOI] [PubMed] [Google Scholar]
Moore 2010b
- Moore RA, Straube S, Paine J, Phillips CJ, Derry S, McQuay HJ.Fibromyalgia: moderate and substantial pain intensity reduction predicts improvement in other outcomes and substantial quality of life gain. Pain 2010;149(2):360-4. [DOI] [PubMed] [Google Scholar]
Moore 2010c
- Moore RA, Smugar SS, Wang H, Peloso PM, Gammaitoni A.Numbers-needed-to-treat analyses - do timing, dropouts, and outcome matter? Pooled analysis of two randomized, placebo-controlled chronic low back pain trials. Pain 2010;151(3):592-7. [DOI] [PubMed] [Google Scholar]
Moore 2011a
- Moore RA, Wiffen PJ, Derry S, McQuay HJ.Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2011, Issue 3. Art. No: CD007938. [DOI: 10.1002/14651858.CD007938.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2011b
- Moore RA, Mhuircheartaigh RJ, Derry S, McQuay HJ.Mean analgesic consumption is inappropriate for testing analgesic efficacy in post-operative pain: analysis and alternative suggestion. European Journal of Anaesthesiology 2011;28(6):427-32. [DOI] [PubMed] [Google Scholar]
Moore 2012
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ.Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2012, Issue 12. Art. No: CD008242. [DOI: 10.1002/14651858.CD008242.pub2] [DOI] [PubMed] [Google Scholar]
Moore 2013
- Moore RA, Straube S, Aldington D.Pain measures and cut-offs - 'no worse than mild pain' as a simple, universal outcome. Anaesthesia 2013;68(4):400-12. [DOI] [PubMed] [Google Scholar]
Neil 2011
- Neil MJ.Clonidine: clinical pharmacology and therapeutic use in pain management. Current Clinical Pharmacology 2011;6:280-7. [DOI] [PubMed] [Google Scholar]
O'Brien 2010
- O'Brien EM, Staud RM, Hassinger AD, McCulloch RC, Craggs JG, Atchison JW, et al.Patient-centered perspective on treatment outcomes in chronic pain. Pain Medicine 2010;11(1):6-15. [DOI] [PubMed] [Google Scholar]
O'Connor 2009
- O'Connor AB, Dworkin RH.Treatment of neuropathic pain: an overview of recent guidelines. American Journal of Medicine 2009;122(10 Suppl):S22-32. [DOI] [PubMed] [Google Scholar]
Ongioco 2000
- Ongioco RR, Richardson CD, Rudner XL, Stafford-Smith M, Schwinn DA.Alpha2-adrenergic receptors in human dorsal root ganglia: predominance of alpha2b and alpha2c subtype mRNSs. Anesthesiology 2000;92(4):968–76. [DOI] [PubMed] [Google Scholar]
Paganoni 2018
- Paganoni S.Evidence-based physiatry: topical analgesics for acute and chronic pain in adults - an overview of Cochrane Reviews. American Journal of Physical Medicine & Rehabilitation 2018;97(7):531-2. [PMID: ] [DOI] [PubMed] [Google Scholar]
Puskas 2003
- Puskas F, Camporesi EM, O'Leary CE, Hauser M, Nasrallah FV.Intrathecal clonidine and severe hypotension after cardiopulmonary bypass. Anesthesia & Analgesia 2003;97(5):1251–3. [DOI] [PubMed] [Google Scholar]
Raja 2020
- Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al.The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain 2020;161(9):1976-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan Web 2020 [Computer program]
- Review Manager Web (RevMan Web).Version 3.0.1. The Cochrane Collaboration, 2020. Available at revman.cochrane.org.
Riedl 2009
- Riedl MS, Schnell SA, Overland AC, Chabot-Doré AJ, Taylor AM, Ribeiro-da-Silva A, et al.Coexpression of alpha 2A-adrenergic and delta-opioid receptors in substance P-containing terminals in rat dorsal horn. Journal of Comparative Neurology 2009;513:385–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
Samso 1996
- Samso E, Valles J, Pol O, Gallart L, Puig MM.Comparative assessment of the anaesthetic and analgesic effects of intramuscular and epidural clonidine in humans. Canadian Journal of Anesthesia 1996;43(12):1195–202. [DOI] [PubMed] [Google Scholar]
Sawynok 2003
- Sawynok J.Topical and peripherally acting analgesics. Pharmacological Reviews 2003;55(1):1–20. [DOI] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s).Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Sierralta 1996
- Sierralta F, Naquira D, Pinardi G, Miranda HF.Alpha-adrenoceptor and opioid receptor modulation of clonidine-induced antinociception. British Journal of Pharmacology 1996;119(3):551–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2013
- Smith BH, Lee J, Price C, Baranowski AP.Neuropathic pain: a pathway for care developed by the British Pain Society. British Journal of Anaesthesia 2013;111:73-9. [DOI] [PubMed] [Google Scholar]
Soni 2013
- Soni A, Batra R, Gwilym S, Spector T, Hart D, Arden N, et al.Neuropathic features of joint pain: a community-based study. Arthritis & Rheumatism 2013;65(7):1942-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2008
- Straube S, Derry S, McQuay HJ, Moore RA.Enriched enrolment: definition and effects of enrichment and dose in trials of pregabalin and gabapentin in neuropathic pain. A systematic review. British Journal of Clinical Pharmacology 2008;66(2):266-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2010
- Straube S, Derry S, Moore RA, Paine J, McQuay HJ.Pregabalin in fibromyalgia - responder analysis from individual patient data. BMC Musculoskeletal Disorders 2010;11:150. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sultan 2008
- Sultan A, Gaskell H, Derry S, Moore RA.Duloxetine for painful diabetic neuropathy and fibromyalgia pain: systematic review of randomised trials. BMC Neurology 2008;8:29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Torrance 2006
- Torrance N, Smith BH, Bennett MI, Lee AJ.The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. Journal of Pain 2006;7(4):281–9. [DOI] [PubMed] [Google Scholar]
Tracey 2011
- Tracey I.Can neuroimaging studies identify pain endophenotypes in humans? Nature Reviews Neurology 2011;7(3):173-81. [DOI] [PubMed] [Google Scholar]
Treede 2008
- Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al.Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology 2008;70(18):1630-5. [DOI] [PubMed] [Google Scholar]
Vos 2020
- GBD 2019 Diseases and Injuries Collaborators: Vos T , Lim SS, Abbafati C, Abbas K, Abbasi M, Abbasifard M, et al.Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396(10258):1204-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Woolf 1999
- Woolf CJ, Mannion RJ.Neuropathic pain: aetiology, symptoms, mechanisms, and management. Lancet 1999;353(9168):1959-64. [DOI] [PubMed] [Google Scholar]
Xu 2016
- Xu L, Zhang Y, Huang Y.Advances in the treatment of neuropathic pain. Advances in Experimental Medicine and Biology 2016;904:117-29. [PMID: ] [DOI] [PubMed] [Google Scholar]
Yang 2019
- Yang X, Fang P, Xiang D, Yang Y.Topical treatments for diabetic neuropathic pain (Review). Experimental and Therapeutic Medicine 2019;17(3):1963-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yasaei 2021
- Yasaei R, Saadabadi A.Clonidine. Treasure Island (FL): StatPearls Publishing, 2021. [PubMed] [Google Scholar]
References to other published versions of this review
Wrzosek 2015
- Wrzosek A, Woron J, Dobrogowski J, Jakowicka-Wordliczek J, Wordliczek J.Topical clonidine for neuropathic pain. Cochrane Database of Systematic Reviews 2015, Issue 8. Art. No: CD010967. [DOI: 10.1002/14651858.CD010967.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]