

Abstract
Background
Individual differences in the rate of aging and susceptibility to disease are not accounted for by chronological age alone. These individual differences are better explained by biological age, which may be estimated by biomarker prediction models. In the light of the aging demographics of the global population and the increase in lifestyle-related morbidities, it is interesting to invent a new biological age model to be used for health promotion.
Objective
This study aims to develop a model that estimates biological age based on physiological biomarkers of healthy aging.
Methods
Carefully selected physiological variables from a healthy study population of 100 women and men were used as biomarkers to establish an estimate of biological age. Principal component analysis was applied to the biomarkers and the first principal component was used to define the algorithm estimating biological age.
Results
The first principal component accounted for 31% in women and 25% in men of the total variance in the biological age model combining mean arterial pressure, glycated hemoglobin, waist circumference, forced expiratory volume in 1 second, maximal oxygen consumption, adiponectin, high-density lipoprotein, total cholesterol, and soluble urokinase-type plasminogen activator receptor. The correlation between the corrected biological age and chronological age was r=0.86 (P<.001) and r=0.81 (P<.001) for women and men, respectively, and the agreement was high and unbiased. No difference was found between mean chronological age and mean biological age, and the slope of the regression line was near 1 for both sexes.
Conclusions
Estimating biological age from these 9 biomarkers of aging can be used to assess general health compared with the healthy aging trajectory. This may be useful to evaluate health interventions and as an aid to enhance awareness of individual health risks and behavior when deviating from this trajectory.
Trial Registration
ClinicalTrials.gov NCT03680768; https://clinicaltrials.gov/ct2/show/NCT03680768
International Registered Report Identifier (IRRID)
RR2-10.2196/19209
Keywords: biological age, model development, principal component analysis, healthy aging, biomarkers, aging
Introduction
Biological age (BA) is a measure that quantifies where an individual is on the aging trajectory, assessed by the physiological profile, in comparison with the average person of that given chronological age (CA) within the population from which the equation was generated [1,2]. The predictive abilities of BA have been investigated in relation to age-related diseases such as cardiovascular disease (CVD) and type 2 diabetes (T2D) and some BA models have been found to predict mortality better than CA [3-5]. Parallels can be drawn between the changes that occur with aging and the changes that occur with an unhealthy lifestyle (especially related to physical inactivity and obesity) and the risk of developing CVD and T2D [6,7]. Therefore, the objective assessment of BA is an appealing approach for risk stratification and health literacy within public health promotion. However, truly measuring the current state of aging, and thereby objectively determining BA, would entail studies that follow people until they die and biomarkers representing all bodily functions. This is practically impossible and objectively unfeasible for use in a clinical setting. To circumvent this, BA models conceptualizing some mechanisms of aging are proposed as surrogate measures of BA. Despite a substantial research effort [8-10], there is still no agreement upon which panel of biomarkers to use when defining BA [11]. Targeting health promotion and management of lifestyle-related diseases, studies have developed several BA models that evaluate the degree of severity of the metabolic syndrome [12], the relation to waist circumference [13], the relation to physical fitness level [14,15], and the organ-specific health status [16], just to mention a few.
Increasing life expectancy and low fertility rates will have a profound impact on future resources and health care needs [17,18]. Forecasts anticipate that by 2050, people aged 65 years or above will constitute more than 20% of the population worldwide [19,20]. This is the decade in life where chronic diseases (eg, CVD, cancer, and T2D) frequently manifest [21], making healthy aging a key objective for research [22-24]. Healthy aging is defined as an extension of health span [25] also characterized by the “healthy aging phenotype” avoiding major chronic diseases as well as cognitive and physical impairments [22]. The important work from Lara and colleagues [26] has resulted in a panel of biomarkers of healthy aging. The purpose of our study was to apply a novel approach in order to incorporate biomarkers of healthy aging into a BA model. For this purpose, we used the first principal component (1PC) obtained from principal component analysis (PCA) as the method to assess individual BA. The goal was to create a BA model based on the healthy aging phenotype. In this way, the model can be used to identify those deviating from the healthy aging trajectory. Thus, no difference between average CA and estimated BA was expected in the study population of healthy individuals.
Methods
Participants
We included 100 healthy Danish individuals, 51 women and 49 men, between 18 and 65 years of age, to participate in an extensive health examination and the data collection of candidate biomarkers for the BA model. We recruited an equal number of women and men in each 5-year age category (Figure 1).
Figure 1.
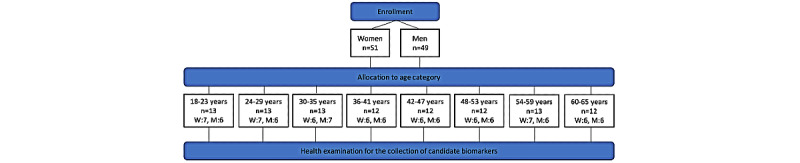
Flow chart of the allocation of enrolled participants in age categories. W: women; M: men.
Ethics Approval
The study was approved by the Regional Ethics Committee, Denmark (H-18031350), recorded as a Clinical Trial (Clinical Trial number: NCT03680768), and performed in accordance with the Helsinki declaration. Participants were informed orally and in writing about the study protocol and the potential risks before obtaining written consent.
Candidate Biomarkers
On the day of the health examination, participants came to the laboratory following an overnight fast and having avoided exercise activities and alcohol consumption for 24 hours and restrained from smoking for at least 4 hours. Information on the participants’ previous and current health status included weekly alcohol consumption, smoking habits, present medications, past medical history, and self-administered questionnaires on physical activity level (Physical Activity Scale 2.1) [27] and quality of life (12-item Short Form version 2 [SF-12v2]). We gathered data on the candidate biomarkers listed in Table 1. These 32 variables are all physiological components of healthy aging that are associated with aging, age-related diseases, and are affected by changes in lifestyle. In addition, this panel of biomarkers covers multiple areas of human function, and they are suitable to study in humans in vivo. For a more comprehensive description of the rationale for including these 32 variables as candidate biomarkers, we refer to our protocol paper (Clinical Trial number: NCT03680768) [28].
Table 1.
Candidate biomarkers measured in the study participants (n=100) showing means with SDs and outcome units per year increase (regression slope with 95% CI).
| Biomarkersa | Mean (SD) | Slope (CI) | |||
| Body composition |
|
|
|||
|
|
Weight (kg) | 75.7 (13.1) | 0.03 (–0.2 to 0.2) | ||
|
|
Waist circumference (cm) | 83.4 (9.8) | 0.2 (0.05 to 0.3) | ||
|
|
Hip circumference (cm) | 101.4 (7.1) | –0.001 (–0.1 to 0.1) | ||
|
|
Waist/hip ratio | 0.8 (0.07) | 0.002 (0.001 to 0.003) | ||
|
|
Fat mass (%) | 26.8 (8.3) | 0.09 (–0.03 to 0.2) | ||
|
|
Muscle mass (kg) | 52.8 (10.9) | –0.05 (–0.2 to 0.1) | ||
| Metabolic health |
|
|
|||
|
|
Fasting blood glucose (mmol/l) | 5.1 (0.4) | 0.01 (0.004 to 0.015) | ||
|
|
HbA1cb (mmol/mol) | 32.8 (3.2) | 0.12 (0.08 to 0.16) | ||
|
|
AGEsc (AU) | 1.8 (0.5) | 0.027 (0.022 to 0.031) | ||
|
|
Insulin (pmol/l) | 44.4 (25.3) | 0.05 (–0.32 to 0.42) | ||
|
|
Triglycerides (mmol/l) | 0.9 (0.4) | 0.002 (–0.004 to 0.008) | ||
|
|
Free fatty acids (μmol/l) | 440 (212) | 2.36 (–0.72 to 5.46) | ||
|
|
Leptin (pg/ml) | 8411 (9472) | –60.0 (–199.8 to 79.9) | ||
|
|
Adiponectin (mg/ml) | 11515 (6490) | 106.6 (13.4 to 199.8) | ||
|
|
HDLd (mmol/l) | 1.5 (0.4) | 0.01 (0.006 to 0.017) | ||
|
|
LDLe (mmol/l) | 2.8 (0.8) | 0.02 (0.01 to 0.03) | ||
|
|
TCf (mmol/l) | 4.5 (0.9) | 0.03 (0.02 to 0.04) | ||
|
|
TC/HDL ratio | 3.1 (0.9) | 0.003 (–0.01 to 0.02) | ||
| Immune function |
|
|
|||
|
|
CRPg (mg/l) | 1.6 (3.4) | –0.04 (–0.09 to 0.01) | ||
|
|
suPARh (ng/ml) | 2.09 (0.5) | 0.01 (0.003 to 0.017) | ||
| Cell blood count |
|
|
|||
|
|
Hemoglobin (mmol/l) | 8.7 (0.8) | 0.004 (–0.01 to 0.02) | ||
|
|
Hematocrit (%) | 41.6 (3.8) | 0.03 (–0.03 to 0.09) | ||
| Cardiorespiratory function |
|
|
|||
|
|
Diastolic BPi (mmHg) | 78.0 (10.1) | 0.4 (0.3 to 0.5) | ||
|
|
Systolic BP (mmHg) | 124.2 (16.7) | 0.6 (0.3 to 0.8) | ||
|
|
FEV1j (L) | 3.9 (0.9) | –0.02 (–0.04 to –0.01) | ||
|
|
FVCk (L) | 4.9 (1.0) | –0.02 (–0.04 to –0.01) | ||
|
|
FEV1/FVC ratio (%) | 77.8 (11.6) | –0.13 (–0.20 to –0.05) | ||
| Physical capacity |
|
|
|||
|
|
VO2maxl (ml/minute/kg) | 39.3 (8.11) | –0.18 (–0.28 to –0.06) | ||
|
|
STSm (stands) | 23.4 (5.2) | –0.07 (–0.14 to 0.01) | ||
|
|
Handgrip strength (kg) | 36.0 (9.4) | –0.8 (–0.2 to 0.1) | ||
|
|
Biceps strength (kg) | 35.0 (11.5) | –0.1 (–0.3 to 0.03) | ||
|
|
Quadriceps strength (Nm) | 152.4 (51.3) | –0.7 (–1.4 to 0.1) | ||
aMissing values were present in leptin (n=99), CRP (n=87), hematocrit (n=97), hemoglobin (n=99) and bicep’s strength (n=98).
bHbA1c: glycated hemoglobin type A1c.
cAGE: advanced glycation end product.
dHDL: high-density lipoprotein.
eLDL: low-density lipoprotein.
fTC: total cholesterol.
gCRP: C-reactive protein.
hsuPAR: soluble urokinase plasminogen activator receptor.
iBP: blood pressure.
jFEV1: forced expiratory volume in 1 second.
kFVC: forced vital capacity.
lVO2max: maximal oxygen consumption.
mSTS: 30-second sit-to-stand chair rise.
Procedures
Variables of body composition were measured by dual-energy X-ray absorptiometry scanning (Lunar Prodigy Advance; Lunar). Waist and hip circumference were measured twice using a standard measuring tape. Variables of metabolic health and immune function were measured from venous blood samples. We extracted plasma and stored it at –80°C before analysis. Plasma concentrations of C-reactive protein, total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, free fatty acids, and glycerol were measured separately by spectrophotometry (Cobas 6000 c501; Roche). Plasma fasting blood glucose (FBG) concentration was measured on an automated analyzer (Hitachi 912; Roche). Plasma insulin, adiponectin, and leptin concentrations were measured by RIA kits (HADP-61HK; Millipore). Plasma concentrations of soluble urokinase plasminogen activator receptor (suPAR) were measured using the commercially available suPARnostic ELISA kit, according to the manufacturer’s instructions (ViroGates). Advanced glycation end products (AGEs) were measured noninvasively using an AGE reader (Diagnoptics Technologies). We measured glycated hemoglobin type A1c (HbA1c) on whole blood using DCA Vantage Analyser (Siemens Healthcare) for the analysis. Resting arterial blood pressure (BP) was measured in triplicate (with 1-minute intervals) using an automatic monitor (Boso-medicus control). Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were assessed by spirometer measurements (Vyntus SPIRO spirometer) with participants sitting on a chair and wearing a nose clip and mouthpiece. Initially, participants breathed normally before conducting a rapid maximal inspiration immediately followed by an expiration with a maximal effort that continued until no more air could be expelled while maintaining an upright posture. The procedure was repeated a minimum of 3 times and a maximum of 7. The trial with the highest reading was used and the Vyntus SPIRO software (SentrySuite) automatically assessed the repeatability, acceptability, and usability criteria defined by the American Thoracic Society and the European Respiratory Society [29]. The handgrip, biceps, and quadriceps strength were measured by a handheld dynamometer (Takei, A5401; Physical Company), a digital back strength dynamometer (Takei TKK 5402; Takei Scientific Instruments Co. Ltd.), and a handheld dynamometer (microFET2; Hoggan Health Industries, Inc.), respectively. At least three attempts were made until no rise in strength occurred. Each test was interspersed with 1-minute rest. Maximal oxygen consumption (VO2max) was measured by a graded exercise test, performed on a bicycle ergometer (Lode Corival) using breath-by-breath (Quark PFT Ergo; Cosmed) oxygen consumption measurements. After 5 minutes of warm-up at 50 and 100 W for women and men, respectively, the load increased by 25 W every minute until voluntary exhaustion. VO2max was determined as the highest 30-second rolling average of VO2.
Exclusion and Inclusion of Candidate Biomarkers
To observe the trajectory of normal healthy aging, we excluded participants diagnosed with or having a previous history of T2D, CVD, cancer, and thyroid dysfunction and who were free of the use of medication to lower cholesterol levels, glucose concentration, and BP [16,30-32]. In addition, a 99% reference interval (mean ±2.96×SD) was applied to examine any potential outliers [30]. To acknowledge age-related decrements within the healthy aging spectrum, however, extreme values below or above the reference interval were individually assessed [33]. We excluded the candidate biomarker AGE from the study due to technical problems affecting the reliability of the measurements.
The actual selection between the remaining 31 candidate biomarkers followed a systematic stepwise method in alignment with previous studies [3,30,34]. To begin with, all candidate biomarkers were submitted to Pearson correlation analysis to assess the strength and direction of association between CA and the candidate biomarkers. All biomarkers that were significantly correlated with CA (|r|>0.15; P≤.05) were included. To minimize redundancy arising in the analysis, we assessed intercorrelation between the included biomarkers. If the correlation between biomarkers was high (|r|≥0.7) and they have a similar clinical function, they are likely to be dependent on the same biological factor and one is excluded depending on the strength of the relationship with CA and the clinical relevance.
Principal Component Analysis
PCA is a factor analysis that reduces dimensions but preserves most of the information in the original data set. PCA is a linear transformation that applies orthogonal rotation to find factors/principal components that capture the largest amount of information in the data [35]. As the PCA produces uncorrelated principal components disclosing which variables are most valuable for clustering the data, it can be used to elucidate the minimum numbers of candidate biomarkers necessary for estimating BA [36]. Traditionally, all principal components with an eigenvalue above 1 are included, or alternatively the number of principal components that together contain 80% of the variation in the data set. However, we will follow the approach first applied by Nakamura et al in 1988 [37] and applied by others since [12,30,31,38], and use the 1PC from the PCA to estimate individual BA.
To do so, included biomarkers were normalized to a mean of 0 and unit SD, which gives them equal weight in the PCA. The subsequent estimation of BA was performed in 3 steps. First, based on the PCA loading scores, a standardized individual BA score (BAS) was modeled:
| BAS = w0 + (w1x1) + (w2x2) +...+ (wNxN) (1) |
where x represents the original value of each of the N biomarkers (without units). The coefficient wn is defined as
| wn = loading scoren/σn (2) |
and the constant w0 as
where wn represents each of the N biomarkers and  and σ represent the original mean and SD for each biomarker, respectively. The loading scores represent the contribution of each biomarker to 1 unit vector of the principal component.
and σ represent the original mean and SD for each biomarker, respectively. The loading scores represent the contribution of each biomarker to 1 unit vector of the principal component.
Second, we transform the BA score into BA in units of years by application of the T-scale method [37]:
where σCA and  are the SD and mean of CA, respectively, of the sample size. However, this introduces a regression toward the mean effect (overestimation of younger individuals’ BA and underestimation of older individuals’ BA) [39], which is why the correction model proposed by Dubina et al [40] is applied:
are the SD and mean of CA, respectively, of the sample size. However, this introduces a regression toward the mean effect (overestimation of younger individuals’ BA and underestimation of older individuals’ BA) [39], which is why the correction model proposed by Dubina et al [40] is applied:
where BAc is the corrected biological age, yi represents individual CA,  is the mean CA of the study sample, and represents the slope in the linear regression assessing the relationship between BA and CA.
is the mean CA of the study sample, and represents the slope in the linear regression assessing the relationship between BA and CA.
Statistics
We present candidate biomarkers as means with SDs and by linear regression to describe the direction and change of the candidate biomarkers per year. We assessed normal distribution using q-q plots and histograms, and checked variance of homogeneity and assessment of linearity by plotting residuals versus predicted values. Paired t test was used to assess differences within sex and the difference between BAc and CA (age difference) was calculated as CA – BAc. The statistical analyses were performed in SAS Enterprise Guide 7.1 and MATLAB R2018b. Statistical significance was considered at P≤.05 in all statistical tests.
Results
Systematic Stepwise Selection of Biomarkers
Correlation Analysis
Pearson correlation coefficient was calculated for each of the 31 candidate biomarkers as a function of CA (Multimedia Appendix 1). Overall, 15 biomarkers substantially correlated with CA covering 5 domains. Body composition (waist circumference and waist/hip ratio), metabolic health (FBG, HbA1c, adiponectin, HDL, LDL, and TC), immune function (suPAR), cardiorespiratory function (diastolic and systolic BP, FEV1, FVC, FEV1/FVC ratio), and physical capacity (VO2max). We observed positive correlations in waist circumference, waist/hip ratio, FBG, adiponectin, HbA1c, HDL, LDL, TC, suPAR, diastolic BP (DBP), and systolic BP (SBP) and negative correlations for FEV1, FVC, FEV1/FVC ratio, and VO2max (Figure 2).
Figure 2.
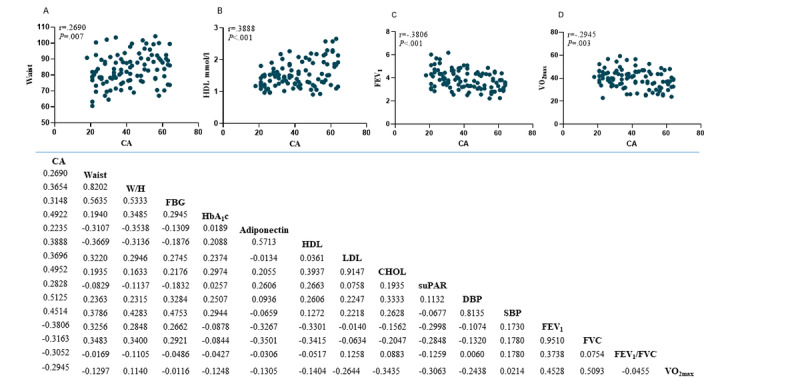
Top: Scatterplots and Pearson’s correlations of: waist circumference (A), high density lipoprotein (B), forced expiratory volume in 1. sec (C), maximal oxygen uptake (D). Bottom: Pearson’s correlation coefficients of the 15 biomarkers significantly correlated with age and their inter-correlations. CA: chronological age; W/H: waist to hip ratio; FBG: fasting blood glucose; HbA1c: glycated hemoglobin type A1c; HDL: High density lipoprotein; LDL: Low density lipoprotein; CHOL: total cholesterol; suPAR: soluble urokinase plasminogen activator receptor; DBP: Diastolic blood pressure; SBP: Systolic blood pressure; FEV1: Forced expiratory volume in 1. sec; VO2max: maximal oxygen uptake.
Assessment of Redundancy
We observed high intercorrelations for some of the variables (Figure 2, bottom) and selected those with the strongest correlation with age or with the highest clinical significance within each cluster. Therefore, as FEV1, FVC, and FEV1/FVC ratio all represent pulmonary function and FEV1 has the highest correlation with age (r=–0.3806; P<.001) compared with FVC (r=–0.3163; P=.001) and FEV1/FVC (r=–0.3052; P=.002), FEV1 was selected. In the same manner we selected TC (r=0.4952; P<.001) over LDL (r=0.3696; P<.001). HbA1c and FBG concentration are both markers of glycemic control, and a high correlation between HbA1c and FBG has been shown in people with and without T2D [41,42]. We suggest that the moderate intercorrelation (r=0.2945; P=.003) found in this study is due to the sample size. HbA1c, which shows a higher correlation with age, has previously been used in the literature in BA models [31] and is generally preferred over FBG due to its higher applicability in a clinical setting. Thus, to reduce redundancy, we only include HbA1c as a marker of glycemic control despite an intercorrelation less than 0.7.
We observed a high intercorrelation between waist circumference and waist/hip ratio, the latter having the highest correlation with CA. Despite this, waist circumference was selected due to its strong association with visceral adipose tissue [43], its clinical importance as the best single anthropometric measure able to identify individuals at high risk of CVD and T2D, and its simplicity [44-46]. In addition, the inherent problem of the equation that an individual who is morbidly obese could have the same waist/height ratio as a normal-weight individual made us select waist circumference. Finally, DBP and SBP had an intercorrelation of r=0.8135 (P<.001), and a very similar correlation with age (r=0.5125; P<.001 and r=0.4514; P<.001, respectively). Instead, we calculated mean arterial pressure (MAP = 1/3SBP + 2/3DBP) to capture both parameters. MAP had a correlation with age of r=0.510 (P<.001) and an intercorrelation with SBP and DBP of r=0.943 (P<.001) and r=0.961 (P<.001), respectively. Thus, a total of 9 biomarkers were submitted to the PCA: waist circumference, FEV1, HbA1c, adiponectin, HDL, TC, suPAR, MAP, and VO2max (scatterplots and Pearson correlation with age for all 9 biomarkers are available in Multimedia Appendix 2).
Applying PCA
Following the normalization of the data set comprising the 9 biomarkers, we applied PCA for women and men separately, with and without the inclusion of CA. By including and excluding CA, we could assess if the direction of the 1PC was similar in both cases, thus assuming that the 1PC can be seen as a general aging factor. The analysis showed high loading scores for CA on the 1PC for both women and men (0.473 and 0.515, respectively), confirming the close relationship between age and 1PC (Table 2). In the second PCA, we excluded CA and found that the relationship between the 9 biomarkers and the 1PC persisted. The 1PC had eigenvalues above 1.0 and accounts for 30.96% (females) and 25.04% (males) of the total variance in the battery of 9 biomarkers (Table 3). These results indicate that the 9 biomarkers reflect underlying measures of a healthy aging trajectory.
Table 2.
The linear combination of normalized variables for the 1PC by gender (chronological age included).
| Principal component analysis variables | Loading scores for 1PCa | ||
|
|
Women | Men | |
| Chronological age | 0.473 | 0.515 | |
| Mean arterial blood pressureb | 0.392 | 0.294 | |
| Glycated hemoglobin | 0.348 | 0.352 | |
| Waist circumference | 0.144 | 0.378 | |
| Forced expiratory volume in 1 second | –0.164 | –0.340 | |
| Maximal oxygen consumption | –0.287 | –0.321 | |
| Adiponectin | 0.199 | 0.078 | |
| High-density lipoprotein | 0.346 | 0.127 | |
| Total cholesterol | 0.405 | 0.337 | |
| suPARc | 0.220 | 0.167 | |
| Eigenvalued | 3.50 | 2.90 | |
| Explained variance %e | 35.04 | 28.96 | |
a1PC: first principal component comprising the best fit line with the largest sum of squares distances.
bMean arterial blood pressure = (1/3SBP + 2/3DBP), where SBP is systolic blood pressure and DBP is diastolic blood pressure.
csuPAR: soluble urokinase plasminogen activator receptor.
dEigenvalue: the sum of squared distances for 1PC.
eExplained variance %: how many percent does the 1PC explain of the total variance in the data set.
Table 3.
The linear combination of normalized variables for the 1PCa by gender (chronological age excluded) and the relative contribution of each physiological variable to BAb estimation.
|
|
Women | Men | |||
|
|
Loading scores | Contribution (%) | Loading scores | Contribution (%) | |
| Mean arterial blood pressurec | 0.435 | 18.9 | 0.349 | 12.2 | |
| Glycated hemoglobin | 0.408 | 16.7 | 0.324 | 10.5 | |
| Waist circumference | 0.173 | 3.0 | 0.491 | 24.1 | |
| Forced expiratory volume in 1 second | –0.138 | 1.9 | –0.309 | 9.5 | |
| Maximal oxygen consumption | –0.341 | 11.6 | –0.475 | 22.6 | |
| Adiponectin | 0.228 | 5.2 | –0.046 | 0.2 | |
| High-density lipoprotein | 0.390 | 15.2 | –0.020 | 0.04 | |
| Total cholesterol | 0.467 | 21.8 | 0.3804 | 14.5 | |
| suPARd | 0.238 | 5.7 | 0.254 | 6.4 | |
| Eigenvaluee | 2.79 | N/Af | 2.25 | N/A | |
| Explained variance %g | 30.96 | N/A | 25.04 | N/A | |
a1PC: first principal component comprising the best fit line with the largest sum of squares distances.
bBA: biological age.
cMean arterial blood pressure = (1/3SBP + 2/3DBP), where SBP is systolic blood pressure and DBP is diastolic blood pressure.
dsuPAR: soluble urokinase plasminogen activator receptor.
eEigenvalue: the sum of squared distances for 1PC.
fN/A: Not applicable.
gExplained variance %: how many percent does the 1PC explain of the total variance in the data set.
To clarify how the variables contribute to the estimation of the BA model, we calculated the percentage contribution of each variable using the following equation:
 |
where a2n is the given loading score and N is the number of variables (Table 3). In women, TC concentration contributed the most (21.8%) followed by MAP (18.9%) and HbA1c (16.7%). For men, waist circumference contributed the most (24.1%) closely followed by VO2max (22.6%) and TC concentration (14.5%).
Biological Age Model
By applying Equation 1, the loading scores from the PCA were used to construct individual standardized BAS as a function of the 9 biomarkers as shown in the following equations:
| BASfemale = –11.04 + (0.03MAP) + (0.126HbA1c) + (0.018Waist) – (0.018FEV1) – (0.053VO2max) + (3.205·10–5·Adiponectin) + (0.909HDL) + (0.500TC) + (0.400suPAR) |
| BASmale = –11.23 + (0.037MAP) + (0.103HbA1c) + (0.066Waist) – (0.431FEV1) – (0.067VO2max) – (1.058·10–5·Adiponectin) – (0.062HDL) + (0.442TC) + (0.828suPAR) |
Subsequently, the BAS was scaled by applying Equation 4.
| BAfemale = (BAS × 13.6) + 41.3 |
| BAmale = (BAS × 13.8) + 41.1 |
Scaling the score into units of years makes it more feasible to use when applying it to health promotion in the general population. Introducing this relationship between CA and BA has been shown to create some bias at the regression ends. Thus, following the previously mentioned correction model of Dubina et al [40] (Equation 5), the final BA models are expressed as
| BAcfemale = –56.67 + (0.27MAP) + (1.02HbA1c) + (0.1453Waist) – (2.03FEV1) – (0.43VO2max) + (0.0003·Adiponectin) + (7.39HDL) + (4.06TC) + (3.24suPAR) + (0.20CA) |
| BAcmale = –70.37 + (0.34MAP) + (0.95HbA1c) + (0.60Waist) – (3.96FEV1) – (0.62VO2max) – (9.73·10–5·Adiponectin) – (0.57HDL) + (4.06TC) + (7.61suPAR) + (0.32CA) |
The corrections are visualized in Figure 3, showing how the overestimation of BA in younger adults and underestimation of older adults are attenuated. In addition, Figure 4 visualizes the regression of BAc on CA (R2=0.73; P<.001 and R2=0.65; P<.001). BAc is scattered relatively close and symmetrically above and below the regression line with a standard error of the estimate of 8.2 years (women) and 10.2 years (men). We found no statistical difference between mean CA and mean BAc in women (P=.99) or men (P=.99). To assess the agreement between CA and BAc, we made a Bland-Altman plot and found a mean difference of 0.002 in women and – 0.006 in men, respectively (Figure 5).
Figure 3.
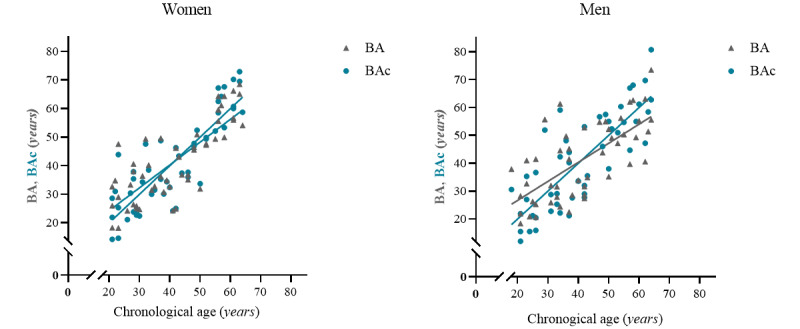
Regression lines before (BA) and after (BAc) correction for women and men, respectively.
Figure 4.
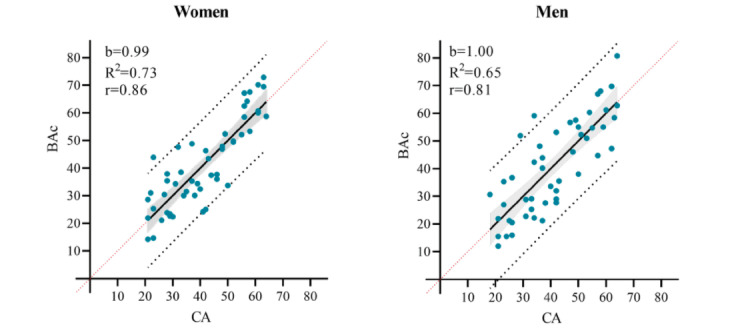
The BAc regression lines for women and men, respectively with 95% Confidence interval (shaded area), 95% Prediction intervals (black dotted lines) and line of identity (red dotted line). Slope (b), correlation coefficient (r) and coefficient of determination (R2).
Figure 5.
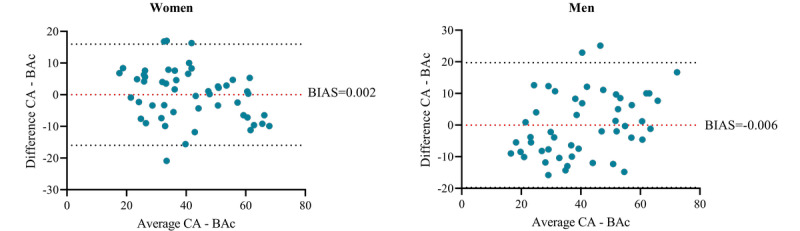
Bland Altman plot for women and men, respectively with BIAS (red dotted line), upper and lower limits of agreement (black dotted lines).
Discussion
Principal Findings
In this study, we aimed to develop a BA model, able to measure healthy aging trajectory, using simple, clinically relevant biomarkers that would respond to changes in health behavior. We selected 9 biomarkers listed in Table 3 and applied PCA to estimate individual BA. The 9 biomarkers represent metabolic health (HDL, TC, and adiponectin) and bodily functions (FEV1, MAP, and suPAR), and include very important clinical age–related variables (VO2max, HbA1c, and waist circumference) [28]. We found no difference between BAc and CA in the healthy reference group of women and men, and the BA model for both women and men showed a high linear relationship with CA. The disagreement between CA and BAc was low and unbiased. A higher variation in the BA model for men resulted in a lower coefficient of determination (R2=0.65; P<.001) compared with the BA model for women (R2=0.73; P<.001).
Sex differences were also observed in the relative contribution of each biomarker to the BA estimate. This indicates that some biomarkers of aging are influenced by sexual dimorphism [47]. HDL, for example, contributes 15.2% ([0.392/0.999] × 100) in women and a negligible 0.04% in men ([–0.022/1.001] × 100). HDL levels are higher in women than in men of the same age [48]. However, during menopause HDL levels decrease (and LDL increase), thereby increasing the cumulative risk of CVD [49]. In general, the multifaceted effects of menopause on metabolism may imply that further development of the model should evaluate if separate models for pre- and postmenopausal women are required. Waist circumference contributed the most (24.1%) in the estimation of BA for men but only 3.0% in the estimation of BA for women. This agrees well with the sex difference in fat distribution—men have a relatively more central distribution of fat with aging even in the absence of weight gain [50]. By contrast, a similar deterioration of VO2max and FEV1 between sexes is expected [47]. This was not the case in our study, as VO2max and FEV1 contributed more to the BA model for men. This difference may be balanced by normalizing VO2max and FEV1 to lean mass and height, respectively. In addition, the small sample size should be mentioned as a limitation in these observations.
The BA model is based on a healthy reference adult subsample of the population. However, in 8% (4/51) of the women and 16% (n=8/49) of the men, the age difference (CA – BAc) was more than +10 years (Figure 5). One of these women and 7 of these men stand out by having a BMI between 25 and 36 kg/m2. Because BMI is causally related to morbidity and mortality [51], it could be argued that individuals with a BMI over 24.9 kg/m2 are not suitable to be included in this study representing a healthy aging reference group. However, cardiorespiratory fitness (VO2max) may be an even better predictor for CVD and premature all-cause mortality [52]. Further, a better VO2max was found to attenuate the risks related to overweight and obesity [53,54]. The majority (41/51, 80%, and 46/49, 94%, of women and men, respectively) of the study participants adhered to the recommendations of a minimum of 150 minutes/week of moderate to vigorous physical activity and had a moderate to high cardiorespiratory fitness level [28]. Therefore, we did not use high BMI as exclusion criteria. Within this consideration, there also lies an effort to recruit a subsample of the population representing normal healthy aging instead of an extremely healthy and active subsample often more prone to participate.
Comparison With Previous Work
In our data set, the highest correlated biomarker with CA was MAP (r=0.51; P<.001). MAP reflects vascular resistance and BP measurements are the commonly used biomarkers in BA studies [1,4,32,37,55]. However, in contrast to our study, pulmonary function (FEV1 and FVC) consistently appears as the most significant parameter related to CA in these former studies [1,4,32,37,55]. In our study, FEV1 only appears as the third most correlated biomarker (r=–0.38; P<.001). A possible explanation is that the biomarkers used for BA estimations rely on register-based data collected in the mid- and late 20th century, primarily representing individuals from Asia and the United States. Thus, it reflects a certain time era and population behavior, for example, regarding smoking prevalence, which has decreased since then [56]. Finally, it is important also to take into account the difference in health behavior seen between ethnic groups.
To estimate BA, we used the 1PC as a general aging factor. In the field of BA prediction models, PCA is considered an improvement compared with multiple linear regression [31]. Even so, PCA is still a linear model, thereby assuming that biomarkers change linearly throughout the age span [57]. While many biomarkers are assumed to decline with a slope of 1% per year [58], some biomarkers may deviate from this linearity, especially toward the higher end of the age span. The proportions of total variance explained by the PCA in our study (31% and 25% women and men, respectively) were similar to those found in other studies using the 1PC, varying from 23% to 42% [3,12,30,32] in women and from 20% to 37% in men [3,12,30,31,37,55]. These studies found that using PCA was valid and clinically useful. However, recent studies [5,34,36] comparing different models found that the Klemera and Doubal model (KDM) [59] was superior at predicting mortality outcomes [60]. Keeping in mind that these results also depend on the specific set of biomarkers included, the algorithm from the KDM should be included in future research on the present BA estimation.
Future Research
This is a first-generation model which is why this work should be used to initiate further research to understand the interpretation of the model fully. Larger sample size is necessary to do a proper sensitivity analysis on how changes in each biomarker affect the BA estimate. In addition, a larger sample size would improve the validity of the selected biomarkers. In this study, the biomarkers were selected based on their significant correlation with CA in a cross-sectional analysis. Using cross-sectional data provides information on the age difference in the biomarkers at a specific point in time. To improve the statistical validity of the measures selected as biomarkers, a significant longitudinal correlation with CA should be investigated. This way the age difference in the biomarkers can be assessed over time [9].
Applying the BA model to longitudinal data is an important future investigation, to see if a relatively high BA is a predictor of poor health outcomes such as T2D, CVD, and mortality. Furthermore, investigating the BA model in health-related interventions will provide evidence as to whether the model can be used as a valid clinical tool for measuring disease risks. Our study has strength in its reproducibility—a key element for BA applicability. The majority of the 9 biomarkers are common measurements in the clinic and in science, where standard quantitative techniques are used. Thus, quantifying BA by the combination of these 9 biomarkers has the advantage of being less susceptible to artifactual variations related to the method of measurement and being accessible from stored plasma samples and databases in national health registers. That being said, the feasibility of measuring suPAR and adiponectin in regular clinical routine is low. Thus, future studies should investigate how the exclusion of suPAR and adiponectin affects the ability of the BA model to identify high-risk individuals and to assess the effect of health-enhancing interventions.
Conclusions
The 9 physiological variables identified in this study as aging biomarkers are highly relevant to assess age-related changes affecting the risk of disease and physical capacity. The BA model has potential for clinical use, due to low technical difficulty and minimally invasive techniques. Estimation of BA has potential as an outcome measure in health-promoting interventions and as a pedagogical aid. Future research is required to investigate how the model will work in populations deviating from the healthy aging spectrum (eg, in individuals with T2D, CVD, or low cardiorespiratory fitness). We expect that the indicator of being biologically old is easy to understand, as a risk of disease and premature mortality, which explains why this indicator might drive individual motivation toward a healthier lifestyle. However, work remains to be performed to improve the model’s validity as a clinical tool and its predictive abilities including, but not restricted to, its reanalysis in a much larger sample size, test-retest reliability, and assessment of the longitudinal stability of the biomarkers.
Acknowledgments
This work was supported by the Copenhagen Center for Health Technology, the Center for Healthy Aging, and the University College Copenhagen. The sponsors had no involvement in the study design, writing of the manuscript, or choice of publication.
Abbreviations
- 1PC
first principal component
- BA
biological age
- BAc
corrected biological age
- BAS
biological age score
- BP
blood pressure
- CA
chronological age
- DBP
diastolic blood pressure
- FBG
fasting blood glucose
- FEV1
forced expiratory volume in 1 second
- FVC
forced vital capacity
- HbA1c
glycated hemoglobin
- HDL
high-density lipoprotein
- KDM
Klemera and Doubal model
- LDL
low-density lipoprotein.
- MAP
mean arterial pressure
- PCA
principal component analysis
- SBP
systolic blood pressure
- SF-12
12-item Short Form
- suPAR
soluble urokinase plasminogen activator receptor
- T2D
type 2 diabetes mellitus
- TC
total cholesterol
- VO2max
maximal oxygen consumption
Correlation coefficient with chronological age for the nine measurements included as biomarkers in the BA model. (A) Waist circumference (cm), (B) High Density Lipoprotein (HDL) (mmol/L), (C) Forced Expiratory Volume in the first second (FEV1) (L), (D) Maximal oxygen consumption (VO2max) (ml/min/kg), (E) Total cholesterol concentration (mmol/L), (F) Mean Arterial Pressure (MAP) (mmHg), (G) Glycated hemoglobin (HbA1c) (mmol/mol), (H) Adiponectin (mg/ml), (I) soluble urokinase plasminogen activator receptor (suPAR) (ng/ml).
{kind=link}
Candidate biomarkers measured in the study participants (n=100) and their correlation with age.
Footnotes
Authors' Contributions: KLSH and JWH conceptualized the study and in collaboration with AB-K, K-ÅH, HBDS, and JCBJ designed the study. KLSH, MF, PH, and AB performed the data collection. K-ÅH and AB-K did the formal analysis. KH wrote the first draft, and AB-K, K-ÅH, JCBJ, HBDS, FD, and JWH revised and edited the manuscript.
Conflicts of Interest: None declared.
References
- 1.Borkan G, Norris A. Assessment of biological age using a profile of physical parameters. J Gerontol. 1980 Mar;35(2):177–84. doi: 10.1093/geronj/35.2.177. doi: 10.1093/geronj/35.2.177. [DOI] [PubMed] [Google Scholar]
- 2.Levine ME, Crimmins EM. A comparison of methods for assessing mortality risk. Am J Hum Biol. 2014 Aug 04;26(6):768–76. doi: 10.1002/ajhb.22595. http://europepmc.org/abstract/MED/25088793 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kang YG, Suh E, Lee J, Kim DW, Cho KH, Bae C. Biological age as a health index for mortality and major age-related disease incidence in Koreans: National Health Insurance Service - Health screening 11-year follow-up study. Clin Interv Aging. 2018;13:429–436. doi: 10.2147/CIA.S157014. doi: 10.2147/CIA.S157014.cia-13-429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Waziry R, Gras L, Sedaghat S, Tiemeier H, Weverling GJ, Ghanbari M, Klap J, de Wolf F, Hofman A, Ikram MA, Goudsmit J. Quantification of biological age as a determinant of age-related diseases in the Rotterdam Study: a structural equation modeling approach. Eur J Epidemiol. 2019 Aug 13;34(8):793–799. doi: 10.1007/s10654-019-00497-3.10.1007/s10654-019-00497-3 [DOI] [PubMed] [Google Scholar]
- 5.Levine ME. Modeling the rate of senescence: can estimated biological age predict mortality more accurately than chronological age? J Gerontol A Biol Sci Med Sci. 2013 Jun;68(6):667–74. doi: 10.1093/gerona/gls233. http://europepmc.org/abstract/MED/23213031 .gls233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Stratton JR, Levy WC, Cerqueira MD, Schwartz RS, Abrass IB. Cardiovascular responses to exercise. Effects of aging and exercise training in healthy men. Circulation. 1994 Apr;89(4):1648–55. doi: 10.1161/01.cir.89.4.1648. [DOI] [PubMed] [Google Scholar]
- 7.Kalyani RR, Corriere M, Ferrucci L. Age-related and disease-related muscle loss: the effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014 Oct;2(10):819–29. doi: 10.1016/S2213-8587(14)70034-8.S2213-8587(14)70034-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baker GT, Sprott RL. Biomarkers of aging. Exp Gerontol. 1988;23(4-5):223–39. doi: 10.1016/0531-5565(88)90025-3. [DOI] [PubMed] [Google Scholar]
- 9.Ingram DK, Nakamura E, Smucny D, Roth GS, Lane MA. Strategy for identifying biomarkers of aging in long-lived species. Exp Gerontol. 2001 Jul;36(7):1025–34. doi: 10.1016/s0531-5565(01)00110-3.S0531-5565(01)00110-3 [DOI] [PubMed] [Google Scholar]
- 10.Sprott RL. Biomarkers of aging and disease: introduction and definitions. Exp Gerontol. 2010 Jan;45(1):2–4. doi: 10.1016/j.exger.2009.07.008.S0531-5565(09)00145-4 [DOI] [PubMed] [Google Scholar]
- 11.Crimmins E, Vasunilashorn S, Kim JK, Alley D. Biomarkers related to aging in human populations. Adv Clin Chem. 2008;46:161–216. doi: 10.1016/s0065-2423(08)00405-8. http://europepmc.org/abstract/MED/19004190 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kang YG, Suh E, Chun H, Kim S, Kim DK, Bae C. Models for estimating the metabolic syndrome biological age as the new index for evaluation and management of metabolic syndrome. CIA. 2017 Feb;Volume 12:253–261. doi: 10.2147/cia.s123316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhao X, Zhu S, Jia X, Yu L, Liu H. Constructing a waist circumference density index to predict biological age and evaluating the clinical significance of waist circumference density age. Exp Gerontol. 2013 Apr;48(4):422–6. doi: 10.1016/j.exger.2013.02.007.S0531-5565(13)00038-7 [DOI] [PubMed] [Google Scholar]
- 14.Hamza SM, Kaufman S. Role of spleen in integrated control of splanchnic vascular tone: physiology and pathophysiology. Can J Physiol Pharmacol. 2009 Jan;87(1):1–7. doi: 10.1139/Y08-103.y08-103 [DOI] [PubMed] [Google Scholar]
- 15.Gołąb S, Woronkowicz A, Kryst Biological aging and physical fitness in men aged 20-70 years from Kraków, Poland. Am J Hum Biol. 2016 Jul;28(4):503–9. doi: 10.1002/ajhb.22820. [DOI] [PubMed] [Google Scholar]
- 16.Bae C, Kang YG, Kim S, Cho C, Kang HC, Yu BY, Lee S, Cho KH, Lee DC, Lee K, Kim JS, Shin KK. Development of models for predicting biological age (BA) with physical, biochemical, and hormonal parameters. Arch Gerontol Geriatr. 2008 Sep;47(2):253–65. doi: 10.1016/j.archger.2007.08.009.S0167-4943(07)00180-X [DOI] [PubMed] [Google Scholar]
- 17.Vollset SE, Goren E, Yuan C, Cao J, Smith AE, Hsiao T, Bisignano C, Azhar GS, Castro E, Chalek J, Dolgert AJ, Frank T, Fukutaki K, Hay SI, Lozano R, Mokdad AH, Nandakumar V, Pierce M, Pletcher M, Robalik T, Steuben KM, Wunrow HY, Zlavog BS, Murray CJL. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020 Oct 17;396(10258):1285–1306. doi: 10.1016/S0140-6736(20)30677-2. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(20)30677-2 .S0140-6736(20)30677-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vaupel JW. Biodemography of human ageing. Nature. 2010 Mar 25;464(7288):536–42. doi: 10.1038/nature08984. http://europepmc.org/abstract/MED/20336136 .nature08984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Harper S. Economic and social implications of aging societies. Science. 2014 Oct 31;346(6209):587–91. doi: 10.1126/science.1254405.346/6209/587 [DOI] [PubMed] [Google Scholar]
- 20.Petsko GA. A seat at the table. Genome Biol. 2008;9(12):113. doi: 10.1186/gb-2008-9-12-113. https://genomebiology.biomedcentral.com/articles/10.1186/gb-2008-9-12-113 .gb-2008-9-12-113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.MacNee W, Rabinovich RA, Choudhury G. Ageing and the border between health and disease. Eur Respir J. 2014 Nov;44(5):1332–52. doi: 10.1183/09031936.00134014. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=25323246 .09031936.00134014 [DOI] [PubMed] [Google Scholar]
- 22.Franco OH, Karnik K, Osborne G, Ordovas JM, Catt M, van der Ouderaa F. Changing course in ageing research: The healthy ageing phenotype. Maturitas. 2009 May 20;63(1):13–9. doi: 10.1016/j.maturitas.2009.02.006.S0378-5122(09)00063-2 [DOI] [PubMed] [Google Scholar]
- 23.Lara J, Godfrey A, Evans E, Heaven B, Brown LJE, Barron E, Rochester L, Meyer TD, Mathers JC. Towards measurement of the Healthy Ageing Phenotype in lifestyle-based intervention studies. Maturitas. 2013 Oct;76(2):189–99. doi: 10.1016/j.maturitas.2013.07.007. https://linkinghub.elsevier.com/retrieve/pii/S0378-5122(13)00225-9 .S0378-5122(13)00225-9 [DOI] [PubMed] [Google Scholar]
- 24.Seals DR, Justice JN, LaRocca TJ. Physiological geroscience: targeting function to increase healthspan and achieve optimal longevity. J Physiol. 2016 Apr 15;594(8):2001–24. doi: 10.1113/jphysiol.2014.282665. doi: 10.1113/jphysiol.2014.282665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kuh D, New Dynamics of Ageing (NDA) Preparatory Network A life course approach to healthy aging, frailty, and capability. J Gerontol A Biol Sci Med Sci. 2007 Jul;62(7):717–21. doi: 10.1093/gerona/62.7.717.62/7/717 [DOI] [PubMed] [Google Scholar]
- 26.Lara J, Cooper R, Nissan J, Ginty AT, Khaw K, Deary IJ, Lord JM, Kuh D, Mathers JC. A proposed panel of biomarkers of healthy ageing. BMC Med. 2015 Sep 15;13:222. doi: 10.1186/s12916-015-0470-9. https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-015-0470-9 .10.1186/s12916-015-0470-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Aadahl M, Jørgensen Torben. Validation of a new self-report instrument for measuring physical activity. Med Sci Sports Exerc. 2003 Jul;35(7):1196–202. doi: 10.1249/01.MSS.0000074446.02192.14. [DOI] [PubMed] [Google Scholar]
- 28.Husted KLS, Fogelstrøm Mathilde, Hulst P, Brink-Kjær Andreas, Henneberg K, Sorensen HBD, Dela F, Helge JW. A Biological Age Model Designed for Health Promotion Interventions: Protocol for an Interdisciplinary Study for Model Development. JMIR Res Protoc. 2020 Oct 26;9(10):e19209. doi: 10.2196/19209. https://www.researchprotocols.org/2020/10/e19209/ v9i10e19209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, Hallstrand TS, Kaminsky DA, McCarthy K, McCormack MC, Oropez CE, Rosenfeld M, Stanojevic S, Swanney MP, Thompson BR. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019 Oct 15;200(8):e70–e88. doi: 10.1164/rccm.201908-1590ST. http://europepmc.org/abstract/MED/31613151 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jee H, Jeon BH, Kim YH, Kim H, Choe J, Park J, Jin Y. Development and application of biological age prediction models with physical fitness and physiological components in Korean adults. Gerontology. 2012;58(4):344–53. doi: 10.1159/000335738.000335738 [DOI] [PubMed] [Google Scholar]
- 31.Park J, Cho B, Kwon H, Lee C. Developing a biological age assessment equation using principal component analysis and clinical biomarkers of aging in Korean men. Arch Gerontol Geriatr. 2009;49(1):7–12. doi: 10.1016/j.archger.2008.04.003.S0167-4943(08)00082-4 [DOI] [PubMed] [Google Scholar]
- 32.Ueno LM, Yamashita Y, Moritani T, Nakamura E. Biomarkers of aging in women and the rate of longitudinal changes. J Physiol Anthropol Appl Human Sci. 2003 Jan;22(1):37–46. doi: 10.2114/jpa.22.37. http://joi.jlc.jst.go.jp/JST.JSTAGE/jpa/22.37?from=PubMed . [DOI] [PubMed] [Google Scholar]
- 33.Altman DG. Preparing to analyse data. Practical statistics for medical research. London, UK: Chapman & Hall; 1991. pp. 126–130. [Google Scholar]
- 34.Jee H, Park J. Selection of an optimal set of biomarkers and comparative analyses of biological age estimation models in Korean females. Arch Gerontol Geriatr. 2017 May;70:84–91. doi: 10.1016/j.archger.2017.01.005.S0167-4943(17)30021-3 [DOI] [PubMed] [Google Scholar]
- 35.Jackson E. A User's Guide to Principal Components. Hoboken, NJ: John Wiley & Sons, Inc; 1991. [Google Scholar]
- 36.Cho IH, Park KS, Lim CJ. An empirical comparative study on biological age estimation algorithms with an application of Work Ability Index (WAI) Mech Ageing Dev. 2010 Feb;131(2):69–78. doi: 10.1016/j.mad.2009.12.001.S0047-6374(09)00167-5 [DOI] [PubMed] [Google Scholar]
- 37.Compher CW, Kinosian BP, Rubesin SE, Ratcliffe SJ, Metz DC. Energy absorption is reduced with oleic acid supplements in human short bowel syndrome. JPEN J Parenter Enteral Nutr. 2009;33(1):102–8. doi: 10.1177/0148607108325074.0148607108325074 [DOI] [PubMed] [Google Scholar]
- 38.Iwasaki Y, Kazama JJ, Yamato H, Matsugaki A, Nakano T, Fukagawa M. Altered material properties are responsible for bone fragility in rats with chronic kidney injury. Bone. 2015 Dec;81:247–254. doi: 10.1016/j.bone.2015.07.015.S8756-3282(15)00289-6 [DOI] [PubMed] [Google Scholar]
- 39.Jee H. Selection of a set of biomarkers and comparisons of biological age estimation models for Korean men. J Exerc Rehabil. 2019 Feb;15(1):31–36. doi: 10.12965/jer.1836644.322. https://www.e-jer.org/journal/view.php?year=2019&vol=15&page=31 .jer-15-1-31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dubina TL, Mints AYa. Zhuk EV. Biological age and its estimation. III. Introduction of a correction to the multiple regression model of biological age in cross-sectional and longitudinal studies. Exp Gerontol. 1984;19(2):133–43. doi: 10.1016/0531-5565(84)90016-0. [DOI] [PubMed] [Google Scholar]
- 41.Rohlfing CL, Wiedmeyer H, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care. 2002 Feb;25(2):275–8. doi: 10.2337/diacare.25.2.275. [DOI] [PubMed] [Google Scholar]
- 42.Ghazanfari Z, Haghdoost AA, Alizadeh SM, Atapour J, Zolala F. A Comparison of HbA1c and Fasting Blood Sugar Tests in General Population. Int J Prev Med. 2010;1(3):187–94. http://europepmc.org/abstract/MED/21566790 . [PMC free article] [PubMed] [Google Scholar]
- 43.Pouliot MC, Després J P, Lemieux S, Moorjani S, Bouchard C, Tremblay A, Nadeau A, Lupien PJ. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol. 1994 Mar 01;73(7):460–8. doi: 10.1016/0002-9149(94)90676-9.0002-9149(94)90676-9 [DOI] [PubMed] [Google Scholar]
- 44.Alberti, G. Zimmet, P. Shaw, J. Grundy, S. The IDF consensus worldwide definition of the metabolic syndrome. Metabolic Syndrome. 2006. [2022-04-28]. https://sites.pitt.edu/~super1/Metabolic/IDF1.pdf?msclkid=10a866e4c6ff11ec94d75d182f473628 .
- 45.Wei M, Gaskill SP, Haffner SM, Stern MP. Waist circumference as the best predictor of noninsulin dependent diabetes mellitus (NIDDM) compared to body mass index, waist/hip ratio and other anthropometric measurements in Mexican Americans--a 7-year prospective study. Obes Res. 1997 Jan;5(1):16–23. doi: 10.1002/j.1550-8528.1997.tb00278.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1071-7323&date=1997&volume=5&issue=1&spage=16 . [DOI] [PubMed] [Google Scholar]
- 46.Dobbelsteyn CJ, Joffres MR, MacLean DR, Flowerdew G. A comparative evaluation of waist circumference, waist-to-hip ratio and body mass index as indicators of cardiovascular risk factors. The Canadian Heart Health Surveys. Int J Obes Relat Metab Disord. 2001 May;25(5):652–61. doi: 10.1038/sj.ijo.0801582. [DOI] [PubMed] [Google Scholar]
- 47.Karasik D, Demissie S, Cupples LA, Kiel DP. Disentangling the genetic determinants of human aging: biological age as an alternative to the use of survival measures. J Gerontol A Biol Sci Med Sci. 2005 May;60(5):574–87. doi: 10.1093/gerona/60.5.574. http://europepmc.org/abstract/MED/15972604 .60/5/574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Giribela AH, Melo NR, Latrilha MC, Baracat EC, Maranhão Raul C. HDL concentration, lipid transfer to HDL, and HDL size in normolipidemic nonobese menopausal women. Int J Gynaecol Obstet. 2009 Feb;104(2):117–20. doi: 10.1016/j.ijgo.2008.10.001.S0020-7292(08)00449-9 [DOI] [PubMed] [Google Scholar]
- 49.Matthews KA, Meilahn E, Kuller LH, Kelsey SF, Caggiula AW, Wing RR. Menopause and risk factors for coronary heart disease. N Engl J Med. 1989 Sep 07;321(10):641–6. doi: 10.1056/NEJM198909073211004. [DOI] [PubMed] [Google Scholar]
- 50.Stevens J, Katz EG, Huxley RR. Associations between gender, age and waist circumference. Eur J Clin Nutr. 2010 Jan;64(1):6–15. doi: 10.1038/ejcn.2009.101. http://europepmc.org/abstract/MED/19738633 .ejcn2009101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Prospective Studies Collaboration. Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J, Halsey J, Qizilbash N, Collins R, Peto R. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009 Mar 28;373(9669):1083–96. doi: 10.1016/S0140-6736(09)60318-4. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(09)60318-4 .S0140-6736(09)60318-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kodama S, Saito Kazumi, Tanaka Shiro, Maki Miho, Yachi Yoko, Asumi Mihoko, Sugawara Ayumi, Totsuka Kumiko, Shimano Hitoshi, Ohashi Yasuo, Yamada Nobuhiro, Sone Hirohito. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009 May 20;301(19):2024–35. doi: 10.1001/jama.2009.681.301/19/2024 [DOI] [PubMed] [Google Scholar]
- 53.Wei M, Kampert JB, Barlow CE, Nichaman MZ, Gibbons LW, Paffenbarger RS, Blair SN. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA. 1999 Oct 27;282(16):1547–53. doi: 10.1001/jama.282.16.1547.joc90699 [DOI] [PubMed] [Google Scholar]
- 54.Gaesser Glenn A, Angadi Siddhartha S. Obesity treatment: Weight loss versus increasing fitness and physical activity for reducing health risks. iScience. 2021 Oct 22;24(10):102995. doi: 10.1016/j.isci.2021.102995. https://linkinghub.elsevier.com/retrieve/pii/S2589-0042(21)00963-9 .S2589-0042(21)00963-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Nakamura E, Miyao K. A method for identifying biomarkers of aging and constructing an index of biological age in humans. J Gerontol A Biol Sci Med Sci. 2007 Oct 01;62(10):1096–105. doi: 10.1093/gerona/62.10.1096.62/10/1096 [DOI] [PubMed] [Google Scholar]
- 56.GBD 2015 Tobacco Collaborators Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017 May 13;389(10082):1885–1906. doi: 10.1016/S0140-6736(17)30819-X. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(17)30819-X .S0140-6736(17)30819-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hollingsworth JW, Hashizume A, Jablon S. Correlations between tests of aging in Hiroshima subjects--an attempt to define "physiologic age". Yale J Biol Med. 1965 Aug;38(1):11–26. http://europepmc.org/abstract/MED/5841151 . [PMC free article] [PubMed] [Google Scholar]
- 58.Jackson SHD, Weale MR, Weale RA. Biological age--what is it and can it be measured? Arch Gerontol Geriatr. 2003;36(2):103–15. doi: 10.1016/s0167-4943(02)00060-2.S0167494302000602 [DOI] [PubMed] [Google Scholar]
- 59.Klemera P, Doubal S. A new approach to the concept and computation of biological age. Mech Ageing Dev. 2006 Mar;127(3):240–8. doi: 10.1016/j.mad.2005.10.004.S0047-6374(05)00265-4 [DOI] [PubMed] [Google Scholar]
- 60.Jia L, Zhang W, Chen X. Common methods of biological age estimation. Clin Interv Aging. 2017;12:759–772. doi: 10.2147/CIA.S134921. doi: 10.2147/CIA.S134921.cia-12-759 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Correlation coefficient with chronological age for the nine measurements included as biomarkers in the BA model. (A) Waist circumference (cm), (B) High Density Lipoprotein (HDL) (mmol/L), (C) Forced Expiratory Volume in the first second (FEV1) (L), (D) Maximal oxygen consumption (VO2max) (ml/min/kg), (E) Total cholesterol concentration (mmol/L), (F) Mean Arterial Pressure (MAP) (mmHg), (G) Glycated hemoglobin (HbA1c) (mmol/mol), (H) Adiponectin (mg/ml), (I) soluble urokinase plasminogen activator receptor (suPAR) (ng/ml).
Candidate biomarkers measured in the study participants (n=100) and their correlation with age.