

Abstract
Introduction
Metabolic syndrome (MetS) is a cluster of metabolic risk factors that include central obesity, hypertension, insulin resistance, and atherogenic dyslipidemia and is strongly associated with a greater risk for developing cardiovascular disease and type 2 diabetes mellitus.
Methods
A literature search was conducted using the words metabolic syndrome, definition and pathogenesis in Scopus, and PubMed. The search also extended to cover medicinal plants and their role as a potential treatment of the metabolic syndrome. The search based on studies published in the English language from 1st of January 2000 to 30th of May 2021. The abstracts and the articles were then screened. Articles were scanned and read; further relevant references in the reference lists are also included.
Results
Both lifestyle factors and genetic factors are involved in the pathogenesis of the metabolic syndrome. Recently, MetS have gained significant attention due to the high prevalence of obesity worldwide. Diagnosis of patients with MetS is important to improve the outcomes of the disease by employing lifestyle and risk factors modifications. Currently, there is a rising interest in medicinal plants and their extracts because the medicinal plants have minimal side effects. Here we review the history, definitions, pathogenesis, management of metabolic syndrome and summarize the beneficial effects of some medicinal plants and their extracts on MetS.
Conclusion
Further research and clinical studies are needed to establish whether medicinal plants can be safely given as potential therapy for metabolic syndrome and whether this can be beneficial in low resources setting countries.
Keywords: Metabolic Syndrome, Obesity, Insulin Resistance, Management, Medicinal plants
Introduction
Metabolic syndrome (MetS) is a group of metabolic risk factors that include central obesity, hypertension, insulin resistance, and atherogenic dyslipidemia and is strongly associated with a greater risk for developing cardiovascular disease and type 2 diabetes mellitus [1]. The elements that regulate MetS are central obesity, hypertension, insulin resistance, and atherogenic dyslipidemia [1]. Nonalcoholic fatty liver disease is considered the hepatic manifestation of MetS. Liver fat is increased in subjects with MetS [2]. Both lifestyle factors and genetic factors are also involved in the pathogenesis of MetS [3]. Recently, MetS have gained great attention due to the high prevalence of obesity worldwide [1]. Diagnosis of patients is important to improve the outcomes of the disease by employing lifestyle and risk factors modifications. The diagnosis of MetS depends on the presence of all or some of the components of MetS (central obesity, hypertension, insulin resistance, and dyslipidemia). The four main definitions for MetS are the World Health Organization definition (1999) [4], The international diabetes federation (IDF) consensus worldwide definition of the metabolic syndrome (2006) [5], The European Group for the Study of Insulin Resistance (1999) [6], The US National Cholesterol Education Program Adult Treatment Panel III (NCEP) (2001) [7]. The most important lifestyle modifications that the patients with metabolic syndrome should be employed are weight reduction, eating healthy food and exercise.
Moreover, patients with MetS should be advised to stop smoking [8, 9]. Some medicinal plants and dietary elements have been shown to improve the elements of metabolic MetS [10]. Importantly, some medicinal plants have the ability to improve insulin sensitivity, decrease blood glucose levels, plasma levels of cholesterol, triglycerides, low-density lipoprotein-cholesterol, body fat percentage, and blood pressure[10]. Medicinal plants can be defined as any plant contains substance that has therapeutic properties or exert beneficial pharmacological effect on humans or animals [11]. Medicinal plants include plants, herbs, food plants, spices, and microscopic plants [11]. Currently, there is a rising interest in medicinal plants and their extracts because the medicinal plants have minimal side effects [10]. These minimal side effects include nausea, vomiting, loss of appetite, diarrhea, constipation, pain, headache, dizziness, allergic reactions, muscle spasm, muscle weaknesses, and sleep disorders [12]. Moreover, medicinal plants are available, affordable and widely used [10]. Here we review the historical background, definitions, epidemiology, and pathogenesis of metabolic syndrome and summarize beneficial effects of some commonly used medicinal plants from Africa and the far east and their extracts on MetS.
Methods
This research project was conducted as a review article. The authors searched on the literature using the following databases: PubMed and Scopus. These databases were searched using the keywords: metabolic syndrome, definition, pathophysiology and treatment. The authors also searched using a combination of the following terms [(metabolic syndrome) AND (definition) AND (pathophysiology)] OR [(medicinal plants) AND (herb) AND (extract) AND (spices) AND (metabolic syndrome) AND (clinical trials)]. The search based on studies published in the English language from 1st of January 2000 to 30th of May 2021, the abstracts and the articles were then screened. Total number of publications found in the initial search was 11721 (6903 from PubMed and 4818 from Scopus). Total number of publications selected for the review was 85 (Fig. 1). The selected articles included 14 reviews, 24 animal studies and 47 randomized controlled trials. Articles were scanned and read; further relevant references in the reference lists are also included. The following criteria were used to select the articles:
Fig. 1.
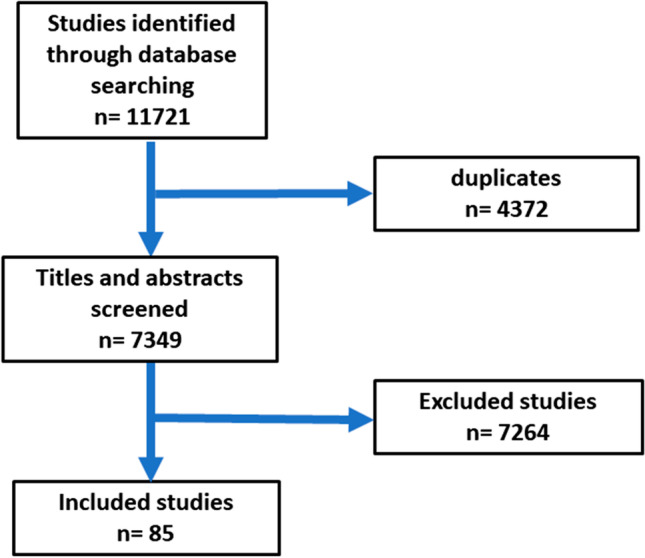
flow chart for selection of articles included in the review
Inclusion criteria
Only randomized controlled trials, animal research studies, and reviews were included in the study. Only English documents were eligible. Based on the topics, all studies about metabolic syndrome or medicinal plants were included
Exclusion criteria
Commentaries, letters to the editor, case reports, books, protocols, news, opinions, theses, note, short surveys, conference abstracts, repeated studies, randomized controlled trials with small sample size and papers written in other languages than English were removed.
All the retrieved manuscripts were imported into EndNote software to remove the duplicates. Then, the titles and abstracts of the studies were screened based on the eligibility criteria by two research team members. The flow chart for the selection of the publications is shown in Fig. 1.
Historical background of metabolic syndrome
The term "metabolic syndrome" was known in the late 1950s, but started to be commonly used in the late 1970s to describe the associations of risk factors with diabetes mellitus that had been observed in the 1920s [13]. In 1947, Jean Vague observed that obesity of the upper parts of the body is a predisposing factor to calculi, gout, diabetes mellitus, and atherosclerosis [14]. In 1977, the term "metabolic syndrome" was used by Haller for the group of obesity, diabetes mellitus, hyperlipoproteinemia, hyperuricemia, and hepatic steatosis to describe the effects of risk factors of atherosclerosis, the same observation was also reported in the same year [15, 16]. In 1977 and 1978, the concept that the risk factors for myocardial infarction form a cluster of abnormalities including glucose intolerance, hyperinsulinemia, hypercholesterolemia, hypertriglyceridemia and hypertension was developed by Gerald Phillips [17, 18]. In 1988, Gerald Reaven Suggested insulin resistance as the major causative factor of the disease and named the cluster of abnormalities, Syndrome X. He did not include central obesity, which was also proposed as the causative factor as part of the disease [19]. Currently, the terms "metabolic syndrome," "insulin resistance syndrome," and "syndrome X" are used to describe a group of metabolic abnormalities that increase the risk of developing type 2 diabetes and cardiovascular disease.
Components of metabolic syndrome
high blood pressure, atherogenic dyslipidemia (high triglycerides levels and reduced HDL levels and), high blood glucose and central obesity are the main components of MetS and are among the main criteria for diagnosing MetS that have been introduced by scientific societies such as World Health Organization (WHO), the International Diabetes Federation (IDF), the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATPIII) [20]. It has been shown that atherogenic dyslipidemia is the most prevalent component affecting MetS [21].
High blood pressure is one of the commonest manifestations of the metabolic disturbances associated with hyperinsulinemia and insulin resistance, which is the key factor in the pathogenesis of MetS. Adipocytes release several factors including adiponectin, leptin, and resistin that play a role in controlling blood pressure [9]. Moreover, abnormal glucose tolerance is preceded by high blood pressure [22]. Hyperinsulinemia occurs in hypertension as a compensatory response to reduced insulin-stimulated glucose uptake by skeletal muscle [23]. It has been shown that 50% of patients with essential hypertension have insulin resistance [24].
Adiposity or abnormal fat accumulation is one of the causative factors of MetS because it affects insulin sensitivity [25]. It has been shown that central obesity is responsible for two-thirds of the factors that contribute to the development of adipose tissue-derived insulin resistance [26]. Insulin resistance leads to a progression from hyperinsulinemia to glucose intolerance and type 2 diabetes mellitus [27].
Definitions of Metabolic syndrome
The four main definitions for MetS are the World Health Organization definition (1999) [4], The International Diabetes Federation (IDF) consensus worldwide definition of the metabolic syndrome (2006) [5], The European Group for the Study of Insulin Resistance (1999) [6], The US National Cholesterol Education Program Adult Treatment Panel III (NCEP)(2001) [7]. The US National Cholesterol Education Program Adult Treatment Panel III (NCEP) was slightly updated by the American Heart Association [28]. In the same year, another definition for metabolic syndrome was set out by the International Diabetes Federation (IDF). These two definitions are very similar and identify individuals with a group of symptoms as patients of MetS. However, there are two differences between them; the IDF states that if BMI > 30 kg/m2, this indicates the individual has central obesity, and there is no need for measuring the waist circumference. However, this eliminates any individual without increased waist circumference if BMI < 30. On the other hand, the NCEP definition indicates that diagnosis of MetS can be based on other criteria. In addition, cut points for waist circumference based on geography is used in IDF while the cut points for waist circumference is not based on geography in NCEP.
WHO Criteria
The first internationally recognized definition of MetS was created by the diabetes consultation group of the World Health Organization (WHO). The World Health Organization criteria (1999) [4] requires presence of one of diabetes mellitus abnormalities: impaired glucose tolerance, impaired fasting glucose or insulin resistance, and two of the following: Blood pressure: ≥ 140/90 mmHg, dyslipidemia: triglycerides (TG): ≥ 1.695 mmol/L and high-density lipoprotein cholesterol (HDL-C) ≤ 0.9 mmol/L (male), ≤ 1.0 mmol/L (female), central obesity: waist:hip ratio > 0.90 (male); > 0.85 (female), or body mass index > 30 kg/m2, microalbuminuria: urinary albumin excretion ratio ≥ 20 μg/min or albumin:creatinine ratio ≥ 30 mg/g
International Diabetes Federation (IDF)
The IDF consensus worldwide definition of the metabolic syndrome (2006) [5] requires the presence of central obesity defined as waist circumference with ethnicity-specific values and any two of the following: Raised triglycerides: > 150 mg/dL (1.7 mmol/L) or specific treatment for this lipid abnormality, reduced HDL cholesterol: < 40 mg/dL (1.03 mmol/L) in males, < 50 mg/dL (1.29 mmol/L) in females, or specific treatment for this lipid abnormality, raised blood pressure: systolic BP > 130 or diastolic BP >85 mm Hg, or treatment of previously diagnosed hypertension, raised fasting plasma glucose :(FPG)>100 mg/dL (5.6 mmol/L), or previously diagnosed type 2 diabetes. If FPG >5.6 mmol/L or 100 mg/dL. Glucose tolerance test (GTT) is strongly recommended but is not necessary to define the presence of the syndrome. If BMI is >30 kg/m2, central obesity can be assumed and waist circumference is not measured.
The European Group for the Study of Insulin Resistance (1999) [6]
This definition requires insulin resistance defined as the top 25% of the fasting insulin values among non-diabetic individuals and two or more of the following: central obesity: waist circumference ≥ 94 cm (male), ≥ 80 cm (female), dyslipidemia: TG ≥ 2.0 mmol/L and/or HDL-C < 1.0 mmol/L or treated for dyslipidemia, hypertension: blood pressure ≥ 140/90 mmHg or antihypertensive medication, fasting plasma glucose ≥ 6.1 mmol/L
The US National Cholesterol Education Program Adult Treatment Panel III (NCEP)(2001) [7]
This requires at least three of the following: central obesity: waist circumference ≥ 102 cm or 40 inches (male), ≥ 88 cm or 36 inches(female), dyslipidemia: TG ≥ 1.7 mmol/L (150 mg/dl), dyslipidemia: HDL-C < 40 mg/dL (male), < 50 mg/dL (female), blood pressure ≥ 130/85 mmHg, fasting plasma glucose ≥ 6.1 mmol/L (110 mg/dl).
American Heart Association/ Updated NCEP [28]
According to Scott Grundy, this definition aimed to update the NCEP ATP III definition and not create a new definition. This definition requires elevated waist circumference: Men equal to or greater than 40 inches (102 cm), Women equal to or greater than 35 inches (88 cm), elevated triglycerides: Equal to or greater than 150 mg/dL (1.7 mmol/L), reduced HDL cholesterol: in men, less than 40 mg/dL (1.03 mmol/L), in women less than 50 mg/dL (1.29 mmol/L), elevated blood pressure: Equal to or greater than 130/85 mm Hg or use of medication for hypertension, elevated fasting glucose: Equal to or greater than 100 mg/dL (5.6 mmol/L) or use of medication for hyperglycemia.
Epidemiology of metabolic syndrome
MetS is a global problem. Abdominal obesity is associated with a greater risk for developing MetS. Prevalence of the disease varies between different countries and regions based on different factors, including gender, age, ethnic group, and the definition used for the diagnosis [29]. The risk for developing MetS is increasing with age. MetS affects less than 10% of young people in their twenties and 40% of the older people in their sixties [29]. School children can be affected by the disease, and even some children can have more than any two elements of the disease (central obesity, hypertension, insulin resistance and atherogenic dyslipidemia) [29]. It has been shown that there is a correlation between MetS in children and their probability of developing cardiovascular diseases in adulthood [29]. MetS affects more than a fifth of the population in the United States (More than 45 million adult individuals) [29].
With regard to gender and ethnic groups, the disease is prevalent in both Mexican Americans and African Americans. The disease affects women more than men in these two ethnic groups. Caucasian women and men are affected equally. The prevalence of the disease in the United States is highest among Mexican Americans, followed by African Americans and Caucasians [29]. Regarding the components of MetS, insulin resistance is commonest in Hispanics, hypertension is commonest in African-Americans, and atherogenic dyslipidemia is commonest in White people(29). MetS affects about 25% of the people in Europe. The prevalence of the disease is low in Southeast Asia, but it is rising towards the prevalence rates of Europe and the United States. The prevalence of MetS is high in the Middle East and sub-Saharan Africa [9].
Pathophysiology of metabolic syndrome
Although the exact mechanism for the pathogenesis of MetS is complex and not yet elucidated, it is well established that the predominant factor is an imbalance between caloric needs and intake [30]. A lack of physical exercise characterizes the lifestyle of patients with MetS, and their diet is high in fats [31]. Both lifestyle factors and genetic factors are involved in the pathogenesis of MetS [3]. Visceral adiposity has a significant contribution to the pathogenesis of MetS and its complications [32]. Insulin resistance is believed to be the leading cause of MetS and defines its clinical presentation [33]. Another proposed mechanism for the development of MetS is chronic inflammation.
Insulin resistance
Most individuals with multiple metabolic risk factors have insulin resistance. This observation led to the generation of the concept that insulin resistance is the principal causative agent of MetS. This concept generated a new term for MetS, namely the insulin resistance syndrome [34].
Insulin resistance is balanced by the rise in insulin secretion to preserve the blood glucose level within the normal levels. The proposed mediators responsible for the high secretion of insulin from the pancreas are autonomic nerves, glucose, the glucagon-like peptide-1, and free fatty acids. Failure of these mediators to raise insulin secretion to balance the insulin resistance would lead to type 2 diabetes [35].
Free fatty acids are key player in the pathogenesis of MetS. Adipose tissue insulin resistance causes mobilization of free fatty acids. Free fatty acids inhibit the effect of insulin on lipid, causing lipolysis leading to further increase in the levels of free fatty acids. Free fatty acids decrease the uptake of glucose in the muscle through inhibition of protein kinase and induce gluconeogenesis and lipogenesis in the liver by increasing the activity of the enzyme protein kinase. Furthermore, after reaching the pancreas, free fatty acids inhibit the release of insulin. Insulin resistance causes high blood pressure through inhibition of insulin and fatty acids mediated vasoconstriction. Insulin resistance induces the release of pro-inflammatory cytokines from the adipose tissue and prothrombotic state, contributing to the risk of developing cardiovascular disease [8].
Visceral adipose tissue has high insulin resistance and causes diversion of free fatty acids to the liver through the portal circulation [36]. Visceral adipose tissue produces metabolites and biologically active substances, including glycerol, free fatty acids(FFA), the pro-inflammatory cytokines, including tumor necrosis factor-alpha and interleukin-6, C-reactive protein, adiponectin, leptin, and resistin. The secretion of adiponectin is reduced in patients with abdominal obesity [37]. The pro-inflammatory cytokines are elevated in patients with metabolic syndrome [38, 39], thus suggesting a role for chronic inflammation as a possible mechanism for the progression of metabolic syndrome.
Role of Glucagon-like- pepetide-1 in MetS
Glucagon-like peptide-1 (GLP-1) is an incretin hormone that plays a significant role in regulating glucose homeostasis [40]. Following ingestion of food, the proglucagon molecules in the intestinal enterocytes (named L-cells) are cleaved to form peptides composed of 30 amino acids, named GLP-1, and is then secreted into the blood [41]. When GLP-1 reaches the pancreatic cells, it binds to the GLP-1 receptor (GLP-1R) on the cell surface to induce insulin secretion. This action is facilitated by increased intracellular Calcium levels. This process becomes inactivated when the blood glucose level drops below 5 mmol/L.
Furthermore, GLP-1 signaling decreases the expression of pro-inflammatory cytokines and proapoptotic factors and enhances the viability of the pancreatic cells [42, 43]. When the blood glucose levels become higher than normal fasting levels, GLP-1 inhibits the secretion of glucagon secretion from the pancreas to enhance the postprandial effect of insulin in mediating the anabolism of the consumed nutrients [41, 44]. Furthermore, a study conducted by Toft-Nielsen et al. showed that fasting plasma levels of plasma GLP-1 were significantly higher in patients with Type 2 diabetes than individuals with normal glucose tolerance. This means that the effect of glucagon-like peptide-1 decreases in patients type 2 diabetes, which may contribute to the decreased incretin activity in patients type 2 diabetes [45]. Bodnaruc et al. suggested that stimulation of GLP-1 can be a good strategy for treating type 2 diabetes and obesity [46]. A study conducted by Seonet al. found that GLP-1 plasma Levels can be a potential Indicator of MetS [47].
Role of chronic inflammation
Chronic inflammation contributes to the pathogenesis of both insulin resistance and MetS. Pro-inflammatory cytokines inhibit the signal transduction of insulin, therefore, can cause insulin resistance in skeletal muscle, liver and adipose tissue. In insulin resistance, the pro-inflammatory cytokines are released by tissue macrophages, adipose tissue, liver, and skeletal muscles [48]. TNF-α induces lipolysis, increases free fatty acids, inhibits adiponectin release, and inactivates insulin receptors in smooth muscle cells and adipocytes [49]. High plasma TNF-α levels are correlated with obesity and insulin resistance [50]. Insulin resistance and high body fat increase the release of IL-6. IL-6 raises the levels of fibrinogen, leading to a prothrombotic state. IL-6 increases production of C-reactive protein (CRP). IL-1 is an important cytokine-stimulated by metabolic stress. Chronic activation of this cytokine results in elevation of CRP levels in metabolic syndrome [51]. Moreover, IL-1 plays a major role in developing type 2 diabetes mellitus and cardiovascular disease by inducing chronic low-grade inflammation [52]. It has been shown that antagonists of the IL-1 pathway improve the blood glucose levels and reduce the plasma level of the IL-6 and CRP in diabetic patients [52].
Role of CRP
All the components of metabolic syndrome are associated with high plasma levels of C-reactive protein (CRP) [53]. High CRP levels indicate chronic inflammatory state, which play a significant role in the development of type 2 diabetes and cardiovascular disease [54]. There is a correlation between the high levels of C-reactive protein and the development of MetS [55].
Fatty liver as part of metabolic syndrome
Studies demonstrated that Non-Alcoholic Fatty Liver Disease (NAFLD) might be a feature of MetS [56]. Laboratory investigations, pathophysiologic considerations, and clinical associations support that insulin resistance has a major contribution to the pathogenesis of both MetS and Non-Alcoholic Fatty Liver. Liver fat is significantly increased in subjects with MetS. 99% of individuals with NAFLD have at least one risk factor of MetS and 33% have all the features of MetS [56].
Management of metabolic syndrome
MetS is a worldwide problem affecting millions of people worldwide. The aim of managing MetS is to control the risk factors and reduce cardiovascular morbidity and mortality. Management of MetS involves lifestyle modifications and the use of medications.
Lifestyle modifications
MetS results from an imbalance between caloric intake and caloric needs. Reduction of body weight is a vital lifestyle modification. The aim of body weight reduction is to lose about 7-10% in baseline body weight over 6-12 months and reduce caloric intake by 500-1000 calories per day [8]. Eating healthy food is important for a healthy lifestyle. Low intake of fats, cholesterol, and sugars is highly recommended for metabolic syndrome patients [8]. Exercise increases the consumption of calories and reduces the risk of cardiovascular mortality and morbidity. Around 30-60 min of moderate-intensity exercise every day is beneficial to patients with metabolic syndrome [8]. Smoking increases the risk of ischemic heart disease and can worsen all the consequences of metabolic syndrome. Patients with MetS should consult their doctors to help them to stop smoking [9].
Drug therapy
Along with lifestyle modification, drug therapy is another option for management. The drug therapy aims to control the metabolic risk factors of MetS. Diuretics or angiotensin-converting enzyme inhibitors are used to control the high blood pressure. Statins reduce high blood cholesterol. Insulin sanitizers reduce high blood glucose level. Aspirin is used to decrease the risk of blood clots [9]. There is no single drug therapy for treating metabolic syndrome. Prolonged multiple medications are used in the current pharmacotherapy. Therefore, it is challenging for the patients to consume multiple medications leading to compliance reduction. Thus there is growing interest in using medicinal plants and their extracts in reducing the risk of MetS since the medicinal plants have minimal side effects [10]. Some medicinal plants with their extracts have been shown to be beneficial for MetS.
Medicinal plants in management of the metabolic syndrome
Medicinal plants are affordable, available, and commonly used [10]. Medicinal plants and their extracts have proven benefits in managing patients with MetS with minimal side effects [10]. Importantly, some medicinal plants have the ability to improve insulin sensitivity, decrease blood glucose levels, plasma levels of cholesterol, triglycerides, low-density lipoprotein-cholesterol, body fat percentage, and blood pressure[10]. Medicinal plants and their extracts can be taken orally. As the benefits of these medicinal plants and their extracts are still studied, these medicinal plants are not recommended as a substitute for the current drug therapy used for treating metabolic syndrome. Here, we review some medicinal plants that are commonly used in developing countries that have been studied and have shown some benefits in MetS (Table 1). These medicinal plants target all the components of MetS (Fig. 2).
Table 1:
Summary for all these medicinal plants and their possible potential benefits as treatment for metabolic syndrome
| Plant | Possible benefits as therapy for metabolic syndrome | References |
|---|---|---|
|
Cinnamon (Cinnamomum verum) |
improve insulin sensitivity, lipid lowering and reduce systolic blood pressure | 57, 58 |
|
Colocynth (Citrullus colocynthis) |
anti-inflammatory, hypoglycemic, lipid-lowering, antihypertensive and antidiabetic | 59,60,61,62,63,64 |
| Curcumin (Curcuma longa) | blood glucose lowering, improve insulin sensitivity, reduce body weight and antihyperlipidemic | 10, 65 |
|
Date palm (Phoenix dactylifera L.) |
blood glucose lowering and improve insulin sensitivity | 66, 67, 68, 69 |
|
Doum (Hyphaene thebaica) |
blood glucose lowering and improve insulin sensitivity | 70,71 |
|
Garlic (Allium sativum) |
Improve all the components of metabolic syndrome | 72, 73, 74, 75 |
|
Green tea ( Camellia sinensis) |
body weight reduction, reduce blood glucose and insulin, lipid lowering and antihypertensive | 76, 77, 78, 79 |
|
Gum Arabic (Acacia Senegal) |
reduce plasma cholesterol concentrations, blood pressure, anti-inflammatory, reduce insulin levels, decrease body mass index and visceral adiposity | 80, 81, 82 |
| Hibiscus sabdariffa | anti-inflammatory effect, improve insulin sensitivity and lipid lowering | 83, 84, 85, 86 |
|
Mangosteen (Garcinia mangostana Linn) |
Anti-inflammatory effect, decrease serum glucose, improved lipid profile, improve insulin sensitivity and body weight lowering | 87, 88, 89, 90, 91 |
|
Neem (Azadirachta indica) |
Improve glucose tolerance, increased the regeneration of B cells increasing insulin secretion | 92 |
| Nigella Sativa | Anti-inflammatory, lipid lowering, blood glucose lowering and body weight lowering | 93, 94, 95 |
Fig. 2.

components of metabolic syndrome targeted by medicinal plants. Medicinal plants target all the components of metabolic syndrome. 1, abdominal obesity; 2, blood pressure; 3, insulin resistance; 4 and 5: dyslipidemia; FFA, free fatty acids; BP, blood pressure; FBS, fasting blood glucose; TG, triglycerides; HDL, high-density lipoprotein Ci, Cinnamon; Co, Colocynth; Cu, Curcumin; Da, Date palm; Do, Doum; G, Garlic; GT, Green tea; GA, Gum Arabic; Hs, Hibiscus sabdariffa; Ma, Mangosteen; N, Neem; NS, Nigella Sativa
Cinnamon
Cinnamon (Cinnamomum Verum) from tree bark is grown in the Mediterranean region and Asia and has been used as a spice. The elements present in cinnamon include coumarin, polyphenol compounds, cinnamaldehyde, cinnamic acid, eugenol, and methyl chalcone polymer. Polyphenol compounds have insulin-sensitizing, antioxidant, and anti-inflammatory effects. Moreover, methyl chalcone polymer in cinnamon induces hydrolysis of fat molecules, increases glycogen synthesis in the liver, enhances entry of glucose, and increases phosphorylation of insulin receptors in adipose tissues and skeletal muscles. Animal studies conducted reported that cinnamon and its components improve insulin sensitivity, decrease blood glucose levels, glycosylated hemoglobin, plasma levels of cholesterol, triglycerides, low-density lipoprotein-cholesterol, body fat percentage, and blood pressure. In a randomized, double blind control trial, Jain et al. found that daily administration of 3 grams of cinnamon for 16 weeks caused an improvement of the elements of MetS and reduction in the prevalence of defined MetS by 34.5% [57]. The mechanism of action of cinnamon is not yet elucidated; however, some experimental studies indicated that cinnamon could improve the transport of glucose through the regulation of adipocyte gene expression [58].
Colocynth
Colocynth (Citrullus colocynthis) or Handal belongs to the Cucurbitaceae family. It is grown in Africa and Europe. The aromatic seeds of Colocynth contain active substances such as glycosides, alkaloids, saponins, flavonoids, and tannins [59]. Colocynth exerts an anti-inflammatory effect by decreasing the release of the pro-inflammatory cytokines and down-regulating the expression of COX-2 [60]. In addition, Colocynth has hypoglycemic, lipid-lowering, antihypertensive effects, and antioxidant activity through eliminating reactive oxygen species (ROS). Furthermore, Colocynth have antidiabetic effect by increasing insulin and decreasing blood glucose level by 10% [61, 62]. The antidiabetic activity of Citrullus colocynthis is mainly due to the restoration of insulin secretion and the inhibition of intestinal glucose uptake [63]. A recent study done by Tabani et al to investigate the effect of Citrullus colocynthis extracts on the liver injury associated with MetS in experimental animals showed that Citrullus colocynthis has hypoglycemic, lipid-lowering, and hepatoprotective effects [64].
Curcumin
Curcumin is an extract from the curcuma longa of the ginger family. It is used as a spice in Southeast Asian countries. Clinical studies demonstrated the ability of curcumin in improving metabolic disorders. evidence from experimental studies in animals demonstrated that curcumin has antioxidant, anti-cancer, antihyperglycemic, and anti-inflammatory activities [10].
Studies have demonstrated that curcumin intake can have the ability to prevent weight loss, decrease plasma glucose levels, enhance the sensitivity of insulin, and increase levels of adiponectin. Moreover, curcumin is antihyperlipidemic [65]. The proposed mechanisms of action of curcumin in decreasing plasma glucose levels in diabetic experimental animals are reduction in the levels of free fatty acids, tumor necrosis factor-α (TNF-α), suppression of the activity of nuclear factor-kappa B (NF-κB). In addition, curcumin increases the activity of the enzyme glucokinase in the liver and decreases the activity of glucose-6-phosphatase and phosphoenolpyruvate carboxykinase. The lipid-lowering effect of curcumin is because curcumin increases the levels of Peroxisome Proliferator-Activated Receptor gamma (PPAR-γ) and reduces the expression of the low-density lipoprotein cholesterol (LDL-C) receptor [65].
Date palm
Date palm (Phoenix dactylifera L.) is one of the most popular fruit crops. It is grown in Africa, Middle East, and South Asia. It is used in traditional medicine for years. Date palm fruit contains protein, vitamins, minerals, flavonoids, dietary fibers, sugar, and phenolic compounds and has high therapeutic value with significant antioxidant, antibacterial, anti-cancer, antidiabetic, cardio-protective and anti-inflammatory properties [66, 67]. Administration of date palm extract daily for 30 days has been shown to decrease the plasma cholesterol level by 47% and have a protective effect against hyperglycemia after a high-fat diet [68] and prevent the depletion of antioxidants and myocyte injury marker enzymes. Furthermore, Date palm downregulates the pro-inflammatory cytokines' expressions and reduces myonecrosis, edema, and infiltration of inflammatory cells [69] in experimental animals.
Doum
Hyphaene thebaica or doum is a palm tree with edible oval fruit. It is popular in Africa. It is produced in sandy and dry areas. Doum contains carbohydrates, minerals, vitamins, flavonoids, and polyphenol compounds and antioxidants [70]. Salib et al. demonstrated that daily administration of compounds from Hyphaene thebaica epicarp for 30 days decreased the blood glucose by 50% and glycosylated hemoglobin levels and improved insulin tolerance in diabetic experimental animals [71].
Garlic
Garlic (Allium sativum) has an important therapeutic value. Because of the antioxidant properties of garlic, garlic can reduce the cardiovascular risk of MetS [72]. A study conducted by Padiya et al. showed that raw garlic reduced serum glucose by 45%, insulin by 25%, and triglycerides by 45%, improve insulin sensitivity in experimental animals, and might have the same effects in humans [73]. Another study was carried out by Choudhary et al. to investigate the effect of raw crushed garlic on the elements of metabolic syndrome in humans found that raw crushed garlic improved the elements of MetS, including central obesity, blood pressure, blood levels of glucose and triglycerides and increased the plasma level of high-density lipoprotein cholesterol [74]. Moreover, Gomez-Arbelaez et al. in study to evaluate the effects of the administration of aged garlic extract on MetS found that administration of aged garlic extract for twelve weeks was followed by improved blood levels adiponectin in patients with MetS [75].
Green tea
Tea is one of the most consumable beverages. It is generally consumed in forms of black and green tea. Green tea is obtained from Camellia sinensis leaves [76]. Camellia sinensis is grown in East Asia and tropical and subtropical areas. A randomized clinical trial conducted by Mousavi et al. found that the daily intake of four cups of green tea for two months resulted in a reduction in body mass index (27.4 to 26.9) (P < 0.001), waist circumference (95.8 to 91.5) (P < 0.001), body weight (73.2 to 71.9) (P < 0.001), and systolic blood pressure (126.2 to 118.6) (P < 0.05) in patients with Type 2 diabetes [77]. In another study conducted by Rasavi et al. to explore the effects of green tea on the elements of MetS in experimental animals, administration green tea for 11 days reduced body weight by 35%, improved hyperlipidemia (increased HDL by 22% and reduced triglycerides by 26%), plasma blood glucose level by 47%, and reduced the leptin level by 50% and blood pressure by 25% [78]. Moreover, Zhang et al. in an experimental study, demonstrated the effect of Yunkang 10 green tea on metabolic syndrome. Administration of Yunkang 10 green tea for 8 weeks reduced the blood level of glucose by 26.3%, cholesterol by 23.7%, triglycerides by 21.3%, insulin by 46.8%, and alanine aminotransferase activity and relieved the fatty liver and hepatic inflammation [79].
Gum Arabic
Gum Arabic (GA) is a soluble fiber obtained from exudates of Acacia senegal in sub-Saharan Africa. Gum Arabic is a very safe dietary fiber. Gum Arabic is used in the Middle East for the treatment of chronic kidney disease. Gum Arabic has been shown to blunt the increase in body weight, plasma levels of glucose and insulin following a high-fat diet, reduce blood pressure, plasma levels of cholesterol, tumor necrosis factor-α, enhance the plasma levels of interleukin 10 (IL-10), reduce insulin levels in type II diabetes and prevent metabolic syndrome in experimental animals [80]. In a randomized controlled clinical trial conducted by Babiker et al., daily administration of 30 grams of Gum Arabic for 3 months decreased body mass index, visceral adiposity and systolic blood pressure by 2%, 23.7% and 7.6% respectively in hypertensive diabetic patients [81]. All the mechanisms of action of Gum Arabic have not yet been elucidated; however, some experimental studies found that Gum Arabic has the ability to reduce intestinal expression and activity of Sodium-Glucose Transporter (SGLT1) [82].
Hibiscus sabdariffa
Hibiscus sabdariffa or karakade is grown in Africa. It is used for treatment of hypertension, hyperlipidemia, and diseases of the gastrointestinal tract [83]. Hibiscus sabdariffa extract has an anti-inflammatory ability through modulation of cyclooxygenase 2 and inducible nitric oxide synthase [84]. Treatment with Hibiscus sabdariffa extract for 8 weeks reduced lipid peroxidation, and plasma levels of triglyceride by 57% [85]. Administration of Hibiscus sabdariffa extract for 42 days blunted the increase in body weight, enhanced glucose tolerance, sensitivity of insulin, improved the levels of low-density lipoprotein cholesterol and high-density lipoprotein cholesterol, decreased the plasma levels of the pro-inflammatory cytokine after a high-fat diet [86].
Mangosteen
Mangosteen (Garcinia mangostana Linn) is grown in Southeast Asia. It used to treat diarrhea, fever, and wound infection. Most components in mangosteen are isoprenylated xanthones, alpha gamma mangostins. Mangosteen and its active compounds have anti-cancer, antibacterial, and antimalarial effects [87]. Mangosteen has been shown to have an anti-inflammatory effect by inhibiting the release of prostaglandin E2 and nitric oxide release and by inhibiting the production of the pro-inflammatory cytokines [88, 89]. Treatment with mangosteen extract was followed by loss of weight, decreased plasma glucose level, and improved lipid profile through sirtuin 1-AMP-activated protein kinase pathway after high-fat diet induced MetS in experimental animals [90]. Results obtained from several studies conducted on human subjects for 26 weeks to evaluate the efficacy of mangosteen extracts on metabolic syndrome were similar to the results of experimental studies [91].
Neem
Azadirachta indica or neem is well known to have medicinal value. It is grown in the Middle East and Africa. Treatment with neem extracts for 21 days improved glucose tolerance, reduces intestinal glucosidase activity, and increased the activity of the enzyme glucose-6-phosphate dehydrogenase, which increased glucose utilization. Moreover, treatment with neem extracts increased the regeneration of insulin-producing cells, increasing insulin secretion and insulin plasma level [92].
Nigella Sativa
Nigella Sativa (N. Sativa) or black seed is used in traditional medicine for many years due to its curing properties. The therapeutic characteristics originate from some of the elements of Nigella Sativa, including alkaloids, volatile oil, flavonoids, amino acids, proteins, carbohydrates, fibers, fatty acids, and volatile oil. A randomized clinical trial conducted by Mohtashami found that consumption of bread with Nigella Sativa improved fasting blood glucose and reduced body weight, waist circumference, and body mass index in patients with MetS [93]. Another randomized controlled clinical trial done by Shirazi et al showed that administration of 500 mg Nigella Sativa once daily for 8 weeks significantly reduced the plasma levels of blood glucose (90.8 ± 16.9 vs. 113.7 ± 12.1), triglyceride (158.3 ± 14.0 vs. 166.7 ± 16.0), cholesterol (115.1 ± 17.6 vs. 127.7 ± 12.6), and low-density lipoprotein cholesterol (115.1 ± 17.6 vs. 127.7 ± 12.6) in postmenopausal women with MetS [94]. Moreover, Nigella sativa oil is very efficient in the control of pro-inflammatory cytokines [95].
Table 1 summarizes all these medicinal plants and their possible potential benefits as a treatment for metabolic syndrome. This is particularly important in low resources setting countries in Africa and the Far East.
Conclusion
MetS is a worldwide problem affecting millions of people. There are different definitions for MetS. The exact mechanism for the pathogenesis of MetS is complex and not yet elucidated. Prolonged multiple medications are used in the current pharmacotherapy. Therefore, it is challenging for the patients to use these medications. Cinnamon (Cinnamomum verum), Colocynth (Citrullus colocynthis), Curcumin (Curcuma longa), Date palm (Phoenix dactylifera L.), Doum (Hyphaene thebaica), Garlic (Allium sativum), Green tea (Camellia sinensis), Gum Arabic (Acacia Senegal), Hibiscus sabdariffa, Mangosteen (Garcinia mangostana Linn), Neem (Azadirachta indica) and Nigella Sativa showed potential benefits as treatment for MetS.
Recommendation
Further research and clinical studies are needed to evaluate medicinal plants' efficacy and establish whether medicinal plants can be safely given as a potential therapy for MetS, and whether this can be beneficial in low resources setting countries.
Author contributions
Ahmed M and Almobarak AO designed the manuscript. Ahmed M wrote the manuscript. Kumari N, Mirgani Z, Saeed A, Ramadan A, Ahmed MH edited the manuscript. All authors contributed to the article and approved the submitted version.
Declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
The original online version of this article was revised: The Abstract was omitted from the original article
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Change history
5/3/2022
A Correction to this paper has been published: 10.1007/s40200-022-01035-x
References
- 1.Grundy SM, Hansen B, Smith SC, Jr, Cleeman JI, Kahn RA, American Heart A, et al. Clinical management of metabolic syndrome: report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Arterioscler Thromb Vasc Biol. 2004;24(2):e19–e24. doi: 10.1161/01.ATV.0000112379.88385.67. [DOI] [PubMed] [Google Scholar]
- 2.Ahmed M, Ahmed MH. Nonalcoholic fatty liver disease and COVID-19: An epidemic that begets pandemic. World J Clin Cases. 2021;9(17):4133–4142. doi: 10.12998/wjcc.v9.i17.4133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ussar S, Griffin NW, Bezy O, Fujisaka S, Vienberg S, Softic S, et al. Interactions between Gut Microbiota, Host Genetics and Diet Modulate the Predisposition to Obesity and Metabolic Syndrome. Cell Metab. 2015;22(3):516–530. doi: 10.1016/j.cmet.2015.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.WHO. Definition, diagnosis and classification of diabetes mellitus and its complications. 1999.
- 5.Alberti KG, Zimmet P, Shaw J. Metabolic syndrome--a new worldwide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23(5):469–480. doi: 10.1111/j.1464-5491.2006.01858.x. [DOI] [PubMed] [Google Scholar]
- 6.Balkau B, Charles MA. Comment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistance (EGIR) Diabet Med. 1999;16(5):442–443. doi: 10.1046/j.1464-5491.1999.00059.x. [DOI] [PubMed] [Google Scholar]
- 7.Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486-97. [DOI] [PubMed]
- 8.Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL. Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Ther Adv Cardiovasc Dis. 2017;11(8):215–225. doi: 10.1177/1753944717711379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gupta A, Gupta V. Metabolic syndrome: what are the risks for humans? Biosci Trends. 2010;4(5):204–212. [PubMed] [Google Scholar]
- 10.Arozal W, Louisa M, Soetikno V. Selected Indonesian Medicinal Plants for the Management of Metabolic Syndrome: Molecular Basis and Recent Studies. Front Cardiovasc Med. 2020;7:82. doi: 10.3389/fcvm.2020.00082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sofowora A, Ogunbodede E, Onayade A. The role and place of medicinal plants in the strategies for disease prevention. African journal of traditional, complementary, and alternative medicines : AJTCAM. 2013;10(5):210–229. doi: 10.4314/ajtcam.v10i5.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Posadzki P, Watson LK, Ernst E. Adverse effects of herbal medicines: an overview of systematic reviews. Clin Med (Lond). 2013;13(1):7–12. doi: 10.7861/clinmedicine.13-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Joslin EP. The Outlook for the Diabetic. Cal West Med. 1927;26(2):177–182. [PMC free article] [PubMed] [Google Scholar]
- 14.La VJ. differenciation sexuelle; facteur determinant des formes de l'obesite. Presse Med. 1947;55(30):339. [PubMed] [Google Scholar]
- 15.Haller H. Epidermiology and associated risk factors of hyperlipoproteinemia. Z Gesamte Inn Med. 1977;32(8):124–128. [PubMed] [Google Scholar]
- 16.Singer P. [Diagnosis of primary hyperlipoproteinemias]. Z Gesamte Inn Med. 1977;32(9):129-33 concl. [PubMed]
- 17.Phillips GB. Sex hormones, risk factors and cardiovascular disease. Am J Med. 1978;65(1):7–11. doi: 10.1016/0002-9343(78)90685-X. [DOI] [PubMed] [Google Scholar]
- 18.Phillips GB. Relationship between serum sex hormones and glucose, insulin and lipid abnormalities in men with myocardial infarction. Proc Natl Acad Sci U S A. 1977;74(4):1729–1733. doi: 10.1073/pnas.74.4.1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595–1607. doi: 10.2337/diab.37.12.1595. [DOI] [PubMed] [Google Scholar]
- 20.Pouragha H, Amiri M, Saraei M, Pouryaghoub G, Mehrdad R. Body impedance analyzer and anthropometric indicators; predictors of metabolic syndrome. J Diabetes Metab Disord. 2021:1–10. [DOI] [PMC free article] [PubMed]
- 21.Nolan PB, Carrick-Ranson G, Stinear JW, Reading SA, Dalleck LC. Prevalence of metabolic syndrome and metabolic syndrome components in young adults: A pooled analysis. Prev Med Rep. 2017;7:211–215. doi: 10.1016/j.pmedr.2017.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Feskens EJ, Tuomilehto J, Stengard JH, Pekkanen J, Nissinen A, Kromhout D. Hypertension and overweight associated with hyperinsulinaemia and glucose tolerance: a longitudinal study of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetologia. 1995;38(7):839–847. doi: 10.1007/s001250050361. [DOI] [PubMed] [Google Scholar]
- 23.Lind L, Berne C, Lithell H. Prevalence of insulin resistance in essential hypertension. J Hypertens. 1995;13(12 Pt 1):1457–1462. [PubMed] [Google Scholar]
- 24.Lima NK, Abbasi F, Lamendola C, Reaven GM. Prevalence of insulin resistance and related risk factors for cardiovascular disease in patients with essential hypertension. Am J Hypertens. 2009;22(1):106–111. doi: 10.1038/ajh.2008.263. [DOI] [PubMed] [Google Scholar]
- 25.Utzschneider KM, Carr DB, Hull RL, Kodama K, Shofer JB, Retzlaff BM, et al. Impact of intra-abdominal fat and age on insulin sensitivity and beta-cell function. Diabetes. 2004;53(11):2867–2872. doi: 10.2337/diabetes.53.11.2867. [DOI] [PubMed] [Google Scholar]
- 26.Jiang J, Cai X, Pan Y, Du X, Zhu H, Yang X, et al. Relationship of obesity to adipose tissue insulin resistance. BMJ Open Diabetes Res Care. 2020;8(1). [DOI] [PMC free article] [PubMed]
- 27.Despres JP, Lemieux I. Abdominal obesity and metabolic syndrome. Nature. 2006;444(7121):881–887. doi: 10.1038/nature05488. [DOI] [PubMed] [Google Scholar]
- 28.Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 29.Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28(4):629–636. doi: 10.1161/ATVBAHA.107.151092. [DOI] [PubMed] [Google Scholar]
- 30.Glosse P, Fajol A, Hirche F, Feger M, Voelkl J, Lang F, et al. A high-fat diet stimulates fibroblast growth factor 23 formation in mice through TNFalpha upregulation. Nutr Diabetes. 2018;8(1):36. doi: 10.1038/s41387-018-0037-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Edwardson CL, Gorely T, Davies MJ, Gray LJ, Khunti K, Wilmot EG, et al. Association of sedentary behaviour with metabolic syndrome: a meta-analysis. PLoS One. 2012;7(4):e34916. doi: 10.1371/journal.pone.0034916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Espinola-Klein C, Gori T, Blankenberg S, Munzel T. Inflammatory markers and cardiovascular risk in the metabolic syndrome. Front Biosci (Landmark Ed). 2011;16:1663–1674. doi: 10.2741/3812. [DOI] [PubMed] [Google Scholar]
- 33.Lann D, LeRoith D. Insulin resistance as the underlying cause for the metabolic syndrome. Med Clin North Am. 2007;91(6):1063–1077. doi: 10.1016/j.mcna.2007.06.012. [DOI] [PubMed] [Google Scholar]
- 34.Einhorn D, Reaven GM, Cobin RH, Ford E, Ganda OP, Handelsman Y, et al. American College of Endocrinology position statement on the insulin resistance syndrome. Endocr Pract. 2003;9(3):237–252. [PubMed] [Google Scholar]
- 35.Ahren B, Pacini G. Islet adaptation to insulin resistance: mechanisms and implications for intervention. Diabetes Obes Metab. 2005;7(1):2–8. doi: 10.1111/j.1463-1326.2004.00361.x. [DOI] [PubMed] [Google Scholar]
- 36.Despres JP, Lemieux I, Bergeron J, Pibarot P, Mathieu P, Larose E, et al. Abdominal obesity and the metabolic syndrome: contribution to global cardiometabolic risk. Arterioscler Thromb Vasc Biol. 2008;28(6):1039–1049. doi: 10.1161/ATVBAHA.107.159228. [DOI] [PubMed] [Google Scholar]
- 37.Kobayashi K. Adipokines: therapeutic targets for metabolic syndrome. Curr Drug Targets. 2005;6(4):525–529. doi: 10.2174/1389450054021972. [DOI] [PubMed] [Google Scholar]
- 38.Fernandez-Real JM, Ricart W. Insulin resistance and chronic cardiovascular inflammatory syndrome. Endocr Rev. 2003;24(3):278–301. doi: 10.1210/er.2002-0010. [DOI] [PubMed] [Google Scholar]
- 39.Wisse BE. The inflammatory syndrome: the role of adipose tissue cytokines in metabolic disorders linked to obesity. J Am Soc Nephrol. 2004;15(11):2792–2800. doi: 10.1097/01.ASN.0000141966.69934.21. [DOI] [PubMed] [Google Scholar]
- 40.Faerch K, Torekov SS, Vistisen D, Johansen NB, Witte DR, Jonsson A, et al. GLP-1 Response to Oral Glucose Is Reduced in Prediabetes, Screen-Detected Type 2 Diabetes, and Obesity and Influenced by Sex: The ADDITION-PRO Study. Diabetes. 2015;64(7):2513–2525. doi: 10.2337/db14-1751. [DOI] [PubMed] [Google Scholar]
- 41.Kieffer TJ, Habener JF. The glucagon-like peptides. Endocr Rev. 1999;20(6):876–913. doi: 10.1210/edrv.20.6.0385. [DOI] [PubMed] [Google Scholar]
- 42.Brubaker PL, Drucker DJ. Minireview: Glucagon-like peptides regulate cell proliferation and apoptosis in the pancreas, gut, and central nervous system. Endocrinology. 2004;145(6):2653–2659. doi: 10.1210/en.2004-0015. [DOI] [PubMed] [Google Scholar]
- 43.Yusta B, Baggio LL, Estall JL, Koehler JA, Holland DP, Li H, et al. GLP-1 receptor activation improves beta cell function and survival following induction of endoplasmic reticulum stress. Cell Metab. 2006;4(5):391–406. doi: 10.1016/j.cmet.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 44.Graaf C, Donnelly D, Wootten D, Lau J, Sexton PM, Miller LJ, et al. Glucagon-Like Peptide-1 and Its Class B G Protein-Coupled Receptors: A Long March to Therapeutic Successes. Pharmacol Rev. 2016;68(4):954–1013. doi: 10.1124/pr.115.011395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Toft-Nielsen MB, Damholt MB, Madsbad S, Hilsted LM, Hughes TE, Michelsen BK, et al. Determinants of the impaired secretion of glucagon-like peptide-1 in type 2 diabetic patients. J Clin Endocrinol Metab. 2001;86(8):3717–3723. doi: 10.1210/jcem.86.8.7750. [DOI] [PubMed] [Google Scholar]
- 46.Bodnaruc AM, Prud'homme D, Blanchet R, Giroux I. Nutritional modulation of endogenous glucagon-like peptide-1 secretion: a review. Nutr Metab (Lond). 2016;13:92. doi: 10.1186/s12986-016-0153-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Seon MJ, Hwang SY, Son Y, Song J, Kim OY. Circulating GLP-1 Levels as a Potential Indicator of Metabolic Syndrome Risk in Adult Women. Nutrients. 2021;13(3). [DOI] [PMC free article] [PubMed]
- 48.de Luca C, Olefsky JM. Inflammation and insulin resistance. FEBS Lett. 2008;582(1):97–105. doi: 10.1016/j.febslet.2007.11.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hotamisligil GS, Murray DL, Choy LN, Spiegelman BM. Tumor necrosis factor alpha inhibits signaling from the insulin receptor. Proc Natl Acad Sci U S A. 1994;91(11):4854–4858. doi: 10.1073/pnas.91.11.4854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tsigos C, Kyrou I, Chala E, Tsapogas P, Stavridis JC, Raptis SA, et al. Circulating tumor necrosis factor alpha concentrations are higher in abdominal versus peripheral obesity. Metabolism. 1999;48(10):1332–1335. doi: 10.1016/S0026-0495(99)90277-9. [DOI] [PubMed] [Google Scholar]
- 51.Ridker PM, Howard CP, Walter V, Everett B, Libby P, Hensen J, et al. Effects of interleukin-1beta inhibition with canakinumab on hemoglobin A1c, lipids, C-reactive protein, interleukin-6, and fibrinogen: a phase IIb randomized, placebo-controlled trial. Circulation. 2012;126(23):2739–2748. doi: 10.1161/CIRCULATIONAHA.112.122556. [DOI] [PubMed] [Google Scholar]
- 52.Larsen CM, Faulenbach M, Vaag A, Volund A, Ehses JA, Seifert B, et al. Interleukin-1-receptor antagonist in type 2 diabetes mellitus. N Engl J Med. 2007;356(15):1517–1526. doi: 10.1056/NEJMoa065213. [DOI] [PubMed] [Google Scholar]
- 53.Ridker PM, Buring JE, Cook NR, Rifai N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14 719 initially healthy American women. Circulation. 2003;107(3):391–397. doi: 10.1161/01.CIR.0000055014.62083.05. [DOI] [PubMed] [Google Scholar]
- 54.Popovic M, Ebrahimi F, Urwyler SA, Donath MY, Christ-Crain M. The role of IL-1 in the regulation of copeptin in patients with metabolic syndrome. Endocr Connect. 2020;9(7):715–723. doi: 10.1530/EC-20-0197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Florez H, Castillo-Florez S, Mendez A, Casanova-Romero P, Larreal-Urdaneta C, Lee D, et al. C-reactive protein is elevated in obese patients with the metabolic syndrome. Diabetes Res Clin Pract. 2006;71(1):92–100. doi: 10.1016/j.diabres.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 56.Paschos P, Paletas K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia. 2009;13(1):9–19. [PMC free article] [PubMed] [Google Scholar]
- 57.Gupta Jain S, Puri S, Misra A, Gulati S, Mani K. Effect of oral cinnamon intervention on metabolic profile and body composition of Asian Indians with metabolic syndrome: a randomized double -blind control trial. Lipids Health Dis. 2017;16(1):113. doi: 10.1186/s12944-017-0504-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Cao H, Graves DJ, Anderson RA. Cinnamon extract regulates glucose transporter and insulin-signaling gene expression in mouse adipocytes. Phytomedicine. 2010;17(13):1027–1032. doi: 10.1016/j.phymed.2010.03.023. [DOI] [PubMed] [Google Scholar]
- 59.Birem Z, Tabani K, Lahfa F, Djaziri R, Hadjbekkouche F, Koceir EA, et al. Effects of colocynth alkaloids and glycosides on Wistar rats fed high-fat diet. A biochemical and morphological study. Folia Histochem Cytobiol. 2017;55(2):74–85. doi: 10.5603/FHC.a2017.0011. [DOI] [PubMed] [Google Scholar]
- 60.Marzouk B, Marzouk Z, Fenina N, Bouraoui A, Aouni M. Anti-inflammatory and analgesic activities of Tunisian Citrullus colocynthis Schrad. immature fruit and seed organic extracts. Eur Rev Med Pharmacol Sci. 2011;15(6):665–672. [PubMed] [Google Scholar]
- 61.Abdel-Hassan IA, Abdel-Barry JA, Tariq MS. The hypoglycaemic and antihyperglycaemic effect of citrullus colocynthis fruit aqueous extract in normal and alloxan diabetic rabbits. J Ethnopharmacol. 2000;71(1-2):325–330. doi: 10.1016/S0378-8741(99)00215-9. [DOI] [PubMed] [Google Scholar]
- 62.Rahbar AR, Nabipour I. The hypolipidemic effect of Citrullus colocynthis on patients with hyperlipidemia. Pak J Biol Sci. 2010;13(24):1202–1207. doi: 10.3923/pjbs.2010.1202.1207. [DOI] [PubMed] [Google Scholar]
- 63.Patel DK, Prasad SK, Kumar R, Hemalatha S. An overview on antidiabetic medicinal plants having insulin mimetic property. Asian Pac J Trop Biomed. 2012;2(4):320–330. doi: 10.1016/S2221-1691(12)60032-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tabani K, Birem Z, Halzoune H, Saiah W, Lahfa F, Koceir EA, et al. Therapeutic effect of alkaloids and glycosides of colocynth seeds on liver injury, associated with metabolic syndrome in wistar rats, subject to nutritional stress. Pak J Pharm Sci. 2018;31(1(Suppl.)):277-90. [PubMed]
- 65.Nishiyama T, Mae T, Kishida H, Tsukagawa M, Mimaki Y, Kuroda M, et al. Curcuminoids and sesquiterpenoids in turmeric (Curcuma longa L.) suppress an increase in blood glucose level in type 2 diabetic KK-Ay mice. J Agric Food Chem. 2005;53(4):959–963. doi: 10.1021/jf0483873. [DOI] [PubMed] [Google Scholar]
- 66.Younas A, Naqvi SA, Khan MR, Shabbir MA, Jatoi MA, Anwar F, et al. Functional food and nutra-pharmaceutical perspectives of date (Phoenix dactylifera L.) fruit. J Food Biochem. 2020:e13332. [DOI] [PubMed]
- 67.Al-Alawi RA, Al-Mashiqri JH, Al-Nadabi JSM, Al-Shihi BI, Baqi Y. Date Palm Tree (Phoenix dactylifera L.): Natural Products and Therapeutic Options. Front. Plant Sci. 2017;8:845. doi: 10.3389/fpls.2017.00845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Khan TJ, Kuerban A, Razvi SS, Mehanna MG, Khan KA, Almulaiky YQ, et al. In vivo evaluation of hypolipidemic and antioxidative effect of 'Ajwa' (Phoenix dactylifera L.) date seed-extract in high-fat diet-induced hyperlipidemic rat model. Biomed Pharmacother. 2018;107:675–680. doi: 10.1016/j.biopha.2018.07.134. [DOI] [PubMed] [Google Scholar]
- 69.Al-Yahya M, Raish M, AlSaid MS, Ahmad A, Mothana RA, Al-Sohaibani M, et al. 'Ajwa' dates (Phoenix dactylifera L.) extract ameliorates isoproterenol-induced cardiomyopathy through downregulation of oxidative, inflammatory and apoptotic molecules in rodent model. Phytomedicine. 2016;23(11):1240–1248. doi: 10.1016/j.phymed.2015.10.019. [DOI] [PubMed] [Google Scholar]
- 70.Aboshora W, Yu J, Omar KA, Li Y, Hassanin HAM, Navicha WB, et al. Preparation of Doum fruit (Hyphaene thebaica) dietary fiber supplemented biscuits: influence on dough characteristics, biscuits quality, nutritional profile and antioxidant properties. J Food Sci Technol. 2019;56(3):1328–1336. doi: 10.1007/s13197-019-03605-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Salib JY, Michael HN, Eskande EF. Antidiabetic properties of flavonoid compounds isolated from Hyphaene thebaica epicarp on alloxan induced diabetic rats. Pharmacognosy Res. 2013;5(1):22–29. doi: 10.4103/0974-8490.105644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Perez-Torres I, Torres-Narvaez JC, Pedraza-Chaverri J, Rubio-Ruiz ME, Diaz-Diaz E, Del Valle-Mondragon L, et al. Effect of the Aged Garlic Extract on Cardiovascular Function in Metabolic Syndrome Rats. Molecules. 2016;21(11). [DOI] [PMC free article] [PubMed]
- 73.Padiya R, Khatua TN, Bagul PK, Kuncha M, Banerjee SK. Garlic improves insulin sensitivity and associated metabolic syndromes in fructose fed rats. Nutr Metab (Lond). 2011;8:53. doi: 10.1186/1743-7075-8-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Choudhary PR, Jani RD, Sharma MS. Effect of Raw Crushed Garlic (Allium sativum L.) on Components of Metabolic Syndrome. J Diet Suppl. 2018;15(4):499–506. doi: 10.1080/19390211.2017.1358233. [DOI] [PubMed] [Google Scholar]
- 75.Gomez-Arbelaez D, Lahera V, Oubina P, Valero-Munoz M, de Las HN, Rodriguez Y, et al. Aged garlic extract improves adiponectin levels in subjects with metabolic syndrome: a double-blind, placebo-controlled, randomized, crossover study. Mediators Inflamm. 2013;2013:285795. doi: 10.1155/2013/285795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y, et al. Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study. JAMA. 2006;296(10):1255–1265. doi: 10.1001/jama.296.10.1255. [DOI] [PubMed] [Google Scholar]
- 77.Mousavi A, Vafa M, Neyestani T, Khamseh M, Hoseini F. The effects of green tea consumption on metabolic and anthropometric indices in patients with Type 2 diabetes. J Res Med Sci. 2013;18(12):1080–1086. [PMC free article] [PubMed] [Google Scholar]
- 78.Razavi BM, Lookian F, Hosseinzadeh H. Protective effects of green tea on olanzapine-induced-metabolic syndrome in rats. Biomed Pharmacother. 2017;92:726–731. doi: 10.1016/j.biopha.2017.05.113. [DOI] [PubMed] [Google Scholar]
- 79.Zhang Y, Gu M, Wang R, Li M, Li D, Xie Z. Dietary supplement of Yunkang 10 green tea and treadmill exercise ameliorate high fat diet induced metabolic syndrome of C57BL/6 J mice. Nutr Metab (Lond). 2020;17:14. doi: 10.1186/s12986-020-0433-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Nasir O. Renal and extrarenal effects of gum arabic ( Acacia senegal )--what can be learned from animal experiments? Kidney Blood Press Res. 2013;37(4-5):269–279. doi: 10.1159/000350152. [DOI] [PubMed] [Google Scholar]
- 81.Babiker R, Elmusharaf K, Keogh MB, Saeed AM. Effect of Gum Arabic (Acacia Senegal) supplementation on visceral adiposity index (VAI) and blood pressure in patients with type 2 diabetes mellitus as indicators of cardiovascular disease (CVD): a randomized and placebo-controlled clinical trial. Lipids Health Dis. 2018;17(1):56. doi: 10.1186/s12944-018-0711-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Nasir O, Artunc F, Wang K, Rexhepaj R, Foller M, Ebrahim A, et al. Downregulation of mouse intestinal Na(+)-coupled glucose transporter SGLT1 by gum arabic (Acacia Senegal) Cell Physiol Biochem. 2010;25(2-3):203–210. doi: 10.1159/000276554. [DOI] [PubMed] [Google Scholar]
- 83.Sayago-Ayerdi SG, Arranz S, Serrano J, Goni I. Dietary fiber content and associated antioxidant compounds in Roselle flower (Hibiscus sabdariffa L.) beverage. J Agric Food Chem. 2007;55(19):7886–7890. doi: 10.1021/jf070485b. [DOI] [PubMed] [Google Scholar]
- 84.Chen CC, Hsu JD, Wang SF, Chiang HC, Yang MY, Kao ES, et al. Hibiscus sabdariffa extract inhibits the development of atherosclerosis in cholesterol-fed rabbits. J Agric Food Chem. 2003;51(18):5472–5477. doi: 10.1021/jf030065w. [DOI] [PubMed] [Google Scholar]
- 85.Wang SC, Lee SF, Wang CJ, Lee CH, Lee WC, Lee HJ. Aqueous Extract from Hibiscus sabdariffa Linnaeus Ameliorate Diabetic Nephropathy via Regulating Oxidative Status and Akt/Bad/14-3-3gamma in an Experimental Animal Model. Evid Based Complement Alternat Med. 2011;2011:938126. doi: 10.1093/ecam/nep181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Diez-Echave P, Vezza T, Rodriguez-Nogales A, Ruiz-Malagon AJ, Hidalgo-Garcia L, Garrido-Mesa J, et al. The prebiotic properties of Hibiscus sabdariffa extract contribute to the beneficial effects in diet-induced obesity in mice. Food Res Int. 2020;127:108722. doi: 10.1016/j.foodres.2019.108722. [DOI] [PubMed] [Google Scholar]
- 87.Aizat WM, Jamil IN, Ahmad-Hashim FH, Noor NM. Recent updates on metabolite composition and medicinal benefits of mangosteen plant. PeerJ. 2019;7:e6324. doi: 10.7717/peerj.6324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Chen LG, Yang LL, Wang CC. Anti-inflammatory activity of mangostins from Garcinia mangostana. Food Chem Toxicol. 2008;46(2):688–693. doi: 10.1016/j.fct.2007.09.096. [DOI] [PubMed] [Google Scholar]
- 89.Cho BO, Ryu HW, So Y, Lee CW, Jin CH, Yook HS, et al. Anti-Inflammatory Effect of Mangostenone F in Lipopolysaccharide-Stimulated RAW264.7 Macrophages by Suppressing NF-kappaB and MAPK Activation. Biomol Ther (Seoul). 2014;22(4):288–294. doi: 10.4062/biomolther.2014.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Chae HS, Kim YM, Bae JK, Sorchhann S, Yim S, Han L, et al. Mangosteen Extract Attenuates the Metabolic Disorders of High-Fat-Fed Mice by Activating AMPK. J Med Food. 2016;19(2):148–154. doi: 10.1089/jmf.2015.3496. [DOI] [PubMed] [Google Scholar]
- 91.Watanabe M, Gangitano E, Francomano D, Addessi E, Toscano R, Costantini D, et al. Mangosteen Extract Shows a Potent Insulin Sensitizing Effect in Obese Female Patients: A Prospective Randomized Controlled Pilot Study. Nutrients. 2018;10(5). [DOI] [PMC free article] [PubMed]
- 92.Bhat M, Kothiwale SK, Tirmale AR, Bhargava SY, Joshi BN. Antidiabetic Properties of Azardiracta indica and Bougainvillea spectabilis: In Vivo Studies in Murine Diabetes Model. Evid Based Complement Alternat Med. 2011;2011:561625. doi: 10.1093/ecam/nep033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Mohtashami A. Effects of Bread with Nigella Sativa on Blood Glucose, Blood Pressure and Anthropometric Indices in Patients with Metabolic Syndrome. Clin Nutr Res. 2019;8(2):138–147. doi: 10.7762/cnr.2019.8.2.138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Shirazi M, Khodakarami F, Feizabad E, Ghaemi M. The effects of nigella sativa on anthropometric and biochemical indices in postmenopausal women with metabolic syndrome. Endocrine. 2020;69(1):49–52. doi: 10.1007/s12020-020-02265-w. [DOI] [PubMed] [Google Scholar]
- 95.Bordoni L, Fedeli D, Fiorini D, Gabbianelli R. Extra Virgin Olive Oil and Nigella sativa Oil Produced in Central Italy: A Comparison of the Nutrigenomic Effects of Two Mediterranean Oils in a Low-Grade Inflammation Model. Antioxidants (Basel). 2019;9(1). [DOI] [PMC free article] [PubMed]