

Abstract
Background and study aims Malignant disease accounts for up to 80 % of gastric outlet obstruction (GOO) cases, which may be treated with duodenal self-expanding metal stents (SEMS), surgical gastrojejunostomy (GJ), and more recently endoscopic-ultrasound-guided gastroenterostomy (EUS-GE). These three treatments have not been compared head-to-head in a randomized trial.
Methods We searched the Embase and MEDLINE databases for studies published January 2015−February 2021 assessing treatment of malignant GOO using duodenal SEMS, endoscopic (EUS-GE) or surgical (laparoscopic or open) GJ. Efficacy outcomes assessed included technical and clinical success rates, GOO recurrence and reintervention. Safety outcomes included procedure-related bleeding or perforation, and stent-related events for the duodenal SEMS and EUS-GE arms.
Results EUS-GE had a lower rate of technical success (95.3%) than duodenal SEMS (99.4 %) or surgical GJ (99.9%) ( P = 0.0048). For duodenal SEMS vs. EUS-GE vs. surgical GJ, rates of clinical success (88.9 % vs. 89.0 % vs. 92.3 % respectively, P = 0.49) were similar. EUS-GE had a lower rate of GOO recurrence based on limited data ( P = 0.0036), while duodenal SEMS had a higher rate of reintervention ( P = 0.041). Overall procedural complications were similar (duodenal SEMS 18.7 % vs. EUS-GE 21.9 % vs. surgical GJ 23.8 %, P = 0.32), but estimated bleeding rate was lowest ( P = 0.0048) and stent occlusion rate was highest ( P = 0.0002) for duodenal SEMS.
Conclusions Duodenal SEMS, EUS-GE, and surgical GJ showed similar clinical efficacy for the treatment of malignant GOO. Duodenal SEMS had a lower procedure-related bleeding rate but higher rate of reintervention.
Introduction
Malignant disease accounts for an estimated 50 % to 80 % of cases of gastric outlet obstruction (GOO), with pancreatic cancer being the most common associated malignancy (15 %–20 %) 1 . Patients with GOO may experience progressively worsening nausea, vomiting, weight loss, abdominal pain and severe dehydration 2 . Because patients with GOO secondary to an unresectable malignancy have limited life expectancy, palliative treatment prioritizes symptom resolution (especially relief of vomiting and return to oral intake) and minimization of hospital stays, complications and reinterventions 1 .
Palliative interventions for GOO include open or laparoscopic surgical gastrojejunostomy (GJ), duodenal stenting using self-expanding metal stents (SEMS), and endoscopic gastroenterostomy (EUS-GE). Surgical GJ and SEMS are the two most common palliative treatment options for patients with malignant GOO 2 . A 2019 meta-analysis of data from 27 studies including 2354 patients with malignant GOO found similar technical and clinical success rates for surgical GJ and duodenal stenting, with shorter mean time to resumption of oral intake for patients who received stenting 2 . However, because stenting was associated with shorter survival time (mean difference 43 days) and higher rates of stent‑related complications, reobstruction and reintervention compared to surgical GJ, the authors concluded that surgical GJ was preferable for patients with a long life expectancy and good performance status 2 . A 2018 meta-analysis of the same treatments analyzed only three randomized controlled trials (RCTs) including 84 patients after exclusion of many studies for low-quality data 1 . This analysis confirmed that compared to surgical GJ, patients receiving duodenal stenting had a faster return to oral intake, shorter mean hospital stay, increased recurrence of symptoms and increased reintervention rate, while quality of life and survival could not be analyzed due to insufficient adequate-quality data 1 .
Since 2015 3 , endoscopic ultrasound-guided gastroenterostomy (EUS-GE) has been studied for the management of GOO. A meta-analysis of 12 studies published through 2018 including 285 patients concluded that EUS-GE is effective and safe for patients with malignant GOO, estimating 92 % technical success, clinical success in 90 % of patients, symptom recurrence or unplanned reintervention in 9 % and adverse events (AEs) in 12 % 4 . Subsequently, a 2020 multicenter study of 45 patients showed lower technical (86.7 %) and clinical (73.3 %) success rates with AEs in 12 patients (26.7 %), including five fatal AEs that occurred at one center 5 .
The above treatments have been studied in observational studies and 2-arm randomized trials. No clinical trials have included all three treatments in a head-to-head comparison. To address this evidence gap, we conducted a systematic review and meta-analysis comparing the efficacy and safety of duodenal SEMS versus EUS-GJ versus surgical GJ in observational studies.
Methods
Search strategy
An expert librarian conducted searches of the Embase and MEDLINE databases (via Embase.com) to identify studies published in English between January 2015 and February 2021 ( eTable 1 ). January 2015 was chosen as the search start date because EUS-GE (newest of the three treatments) was first documented for the management of GOO in human patients in 2015 3 . RCTs, retrospective and prospective cohort studies, case-control studies, and case series that assessed endoscopic duodenal stenting or endoscopic or surgical GJ for malignant GOO were included. We excluded in vitro or animal studies, reviews or editorials, and publications that reported on < 10 patients, had article text in a non-English language, or had study populations that were clearly overlapping or had suspected overlap based on common authors and study sites with overlapping enrollment dates. In cases of overlap, we retained the study/studies with the most comprehensive data on the outcomes of interest that were mutually exclusive with all other included studies. If some but not all arms of a comparative study showed overlap with another publication, the arm(s) with overlap were excluded but the arm(s) without overlap were retained for the analysis.
Data extraction and assessment for risk of bias
For all manuscripts identified by the literature search, two authors (RK, SB) independently reviewed studies for eligibility and/or extracted data from selected publications for preidentified efficacy and safety endpoints. Discrepancies were resolved after review by a third author (PB) and consensus decision after discussion among the entire author group. Baseline information consisted of study characteristics (year published, country of origin, study design, sample size), patient characteristics (age, sex), treatment and treatment subgroup (e. g., type of stent, subcategory of surgery). Reasons for study exclusion were documented.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct this analysis 6 . The Newcastle-Ottawa Scale (NOS) was employed (author SB) to review the methodologic quality of non-randomized studies and assess for bias. An adapted NOS was used that assessed the selection and representativeness of the study population ( eTable 2 ) and the ascertainment of outcomes and exposures. Items from the NOS that made comparative assessments (e. g. exposed vs. non-exposed cohorts) were removed, as they did not apply to single-arm studies. This adaptation of the NOS has been used previously 7 8 9 , and for the purposes of this study, one question (“Were other important diagnoses excluded?”) was replaced by another question (“Was follow-up long enough for outcomes to occur? Reported adequate follow-up time”) to make it more appropriate for this systematic review. Yes/no responses were required for each of five questions, and the quality of each study was ranked as good (5 yes responses), moderate (4 yes responses), or poor ( ≤ 3 yes responses).
Endpoint assessment and definition
Efficacy outcomes assessed were “technical success” and “clinical success” as defined by the reporting authors, pre- and postprocedural Gastric Outlet Obstruction Scoring System (GOOSS) score 10 (no oral intake = 0, liquids only = 1, soft solids = 2, low-residue or full diet = 3), recurrence of GOO, and reintervention (for any reason) during the study period.
Safety outcomes assessed were overall adverse event rate, procedure-related bleeding and perforation, and for the duodenal stent and EUS-GE arms: stent migration, patency, occlusion, ingrowth and overgrowth. In many cases, procedure-related deaths were not distinguished from all-cause deaths, and some studies were designed to follow all patients until death. Therefore, as a surrogate of procedure-related deaths, we only extracted deaths described in the AEs section since this location in the paper suggested the authors thought the death could be procedure-related.
In some articles, some outcomes were only reported for technically successful cases. To avoid inflated estimates (e. g. clinical success only reported for technically successful cases) or exclusion of AEs in failed cases, all reported events were extracted, using denominators reflecting the entire study population.
Statistical methods
Efficacy and safety outcomes were assessed using a random-effects meta-analysis to estimate the proportion of patients with the measure or mean of the measure. Since the number of comparative studies was small and those studies were retrospective, both arms from all comparative studies were treated as independent studies and combined with non-comparative studies. The arcsine transformation was used to compute weighted pooled random-effects estimates for all endpoints. For endpoints with three treatment groups, pairwise comparisons between treatments were done with a Bonferroni adjustment. A sensitivity analysis was performed including only studies with “good” quality ratings. Heterogeneity was assessed across studies using the I 2 statistic 11 . Funnel plots were created to assess for publication bias across studies. The Begg and Mazumdar rank correlation test of funnel plot asymmetry and Egger’s linear regression test of funnel plot asymmetry were also used to assess publication bias 12 13 . All meta-analyses were performed using R (version 3.6.1); SAS (version 9.4, SAS Inc., Cary, North Carolina, United States) was used for plotting and all other analyses.
Results
Study selection and patient characteristics
Study and patient characteristics are summarized in Table 1 . The systematic literature search identified 451 unique articles, of which 61 studies representing 5772 subjects met the inclusion criteria ( Fig. 1 ). In total, 390 articles were excluded ( Fig. 1 ), most often for the wrong indication (including benign GOO) or being unrelated to the search objectives (n = 211), or because they were a review article or editorial (n = 65), case report or had < 10 patients (36), in vitro or animal study (32) or not available in English language (31). Fifty-two eligible studies were retrospective; and nine were prospective, including two randomized studies comparing covered SEMS to uncovered SEMS.
Table 1. Publications and extracted data.
| First author | Year | Country | Study design | Treatment | Treatment subgroup | No. of Cases | Age [mean± SD] | Males (x/n) |
| Chiu 32 | 2015 | UK | Retrospective | SEMS | Uncovered | 18 | 70 median (range 46–85) | 8/18 |
| JW Kim 33 | 2015 | South Korea | Retrospective | SEMS | Uncovered | 38 | 68.9 ± 10.2 | 18/38 |
| SEMS | Covered | 29 | 68.5 ± 11.2 | 11/29 | ||||
| SH Kim 34 | 2015 | South Korea | Retrospective | SEMS | 27 Covered stents, 29 uncovered | 56 | 69 mean (range 52–91) | 36/56 |
| H Lee 35 | 2015 | South Korea | Prospective randomized; WAVE partially covered SEMS vs uncovered SEMS | SEMS | Partially covered | 51 | 57.9 ± 12.5 | 34/51 |
| SEMS | Uncovered | 51 | 58.7 ± 10.8 | 36/51 | ||||
| JE Lee 23 | 2015 | South Korea | Retrospective | SEMS | 60 Uncovered, 7 partially covered | 67 | 61.2 ± 12.7 | 41/67 |
| SEMS | 80 Uncovered; eight partially covered | 88 | 64.4 ± 12.8 | 61/88 | ||||
| D Oh 36 | 2015 | South Korea | Retrospective | SEMS | Partially covered | 20 | 64.5 median (range 39–85) | 11/20 |
| SY Oh 37 | 2015 | USA | Retrospective | SEMS | NS | 196 | 65.4 median (IQR 59.4–74.2) | 102/196 |
| SEMS | NS | 96 | 70.4 median (IQR 61.0–79.2) | 55/96 | ||||
| Park 24 | 2015 | South Korea | Retrospective | SEMS | Mixed (141 uncovered, 76 covered) | 217 | 60.7 ± 13.3 | 162/217 |
| Surgical | Mixed | 39 | 61.7 ± 13.3 | 34/39 | ||||
| Sato 38 | 2015 | Japan | Retrospective | SEMS | Uncovered | 61 | 64.0 ± 10.3 | 35/61 |
| Trotter 39 | 2015 | UK | Retrospective | SEMS | NS | 29 | ||
| Fiori 40 | 2016 | Italy | Prospective, not randomized | SEMS (arm excluded for overlap) 1 | Mixed covered and uncovered 1 | 72 1 | 71 1 | 46/70 1 |
| Surgical | Open | 30 | 70 | 19/30 | ||||
| Grunwald 41 | 2016 | USA | Retrospective | SEMS | NS | 100 | 69.7 | 43/100 |
| Itoi 42 | 2016 | Japan, India, USA | Prospective | EUS-GJ (EPASS) with LAMS | EUS-GJ | 20 | ||
| Jung 43 | 2016 | South Korea | Retrospective | SEMS | Fully covered | |||
| SEMS | Partially covered | |||||||
| SEMS | Uncovered | |||||||
| SEMS | Mixed | 220 | 63 median (IQR 15–90) | 125/220 | ||||
| Kato 44 | 2016 | Japan | Retrospective | SEMS | Uncovered | 46 | ||
| SEMS | Uncovered | 79 | ||||||
| SEMS | Uncovered | 125 | 70.2 mean (range 38–97) | 71/125 | ||||
| Khan 45 | 2016 | China | Prospective | SEMS | Uncovered | 30 | 65 mean (range 40–90) | 18/30 |
| Kobayashi 46 | 2016 | Japan | Retrospective | SEMS | Uncovered | 71 | 67.6 (range: 31–92) | 43/71 |
| Lye 47 | 2016 | Singapore | Retrospective | SEMS | Uncovered | 24 | 79.5 median (range 49–92) | 11/24 |
| Surgical | Open | 30 | ||||||
| Okuwaki 48 | 2016 | Japan | Retrospective | SEMS | Uncovered | 14 | 72 median (IQR 69–79) | 9/14 |
| SEMS | Uncovered | 17 | 71 median (IQR 66–75) | 8/17 | ||||
| J-H Park (1) 49 | 2016 | South Korea | Retrospective | SEMS | Partially covered | 125 | 61 mean (range 25–89) | 81/125 |
| SEMS | Partially covered | 68 | 62 mean (range 36–91) | 48/68 | ||||
| J-H Park (2) 50 | 2016 | South Korea | Retrospective propensity score-matched | SEMS | Dual stent consisting of outer partially covered stent and inner bare stent | 74 | 62.1 ± 13.8 | 57/74 |
| Surgical | Mixed | 74 | 61.1 ± 12.1 | 55/74 | ||||
| Rademacher 51 | 2016 | Germany | Retrospective | SEMS | NS | 62 | 70.5 median (range 63–81) | 35/62 |
| Sasaki 52 | 2016 | Japan | Prospective | SEMS | Uncovered | 39 | 69.2 ± 13.3 | 25/39 |
| Shin 53 | 2016 | South Korea | Retrospective | SEMS | Mixed | 124 | 71.8 median (range 42–97) | 70/122 |
| Tsauo 54 | 2016 | South Korea | Retrospective | SEMS | Partial | 75 | 61.7 ± 10.9 | 45/75 |
| Surgical | Mixed | 32 | 63.4 ± 9.6 | 21/32 | ||||
| Yamao 55 | 2016 | Japan | Retrospective | SEMS | Mixed covered and uncovered | 278 | 71.7 ± 11.4 | 163/278 |
| Bulut 56 | 2017 | Turkey | Retrospective | SEMS | Uncovered | 53 | 58.7 ± 15.07 | 33/53 |
| Chen 30 | 2017 | USA, Japan (EUS-GJ) USA (SEMS) | Retrospective | SEMS | NS | 52 | 64 ± 13.2 | 32/52 |
| EUS-GJ | EUS-GJ | 30 | 70 ± 13.3 | 17/30 | ||||
| Hori 57 | 2017 | Japan | Retrospective | SEMS | Uncovered | 126 | 74 median (range 39–101) | 160/252 |
| SEMS | Covered | 126 | ||||||
| Jang 58 | 2017 | South Korea | Retrospective | SEMS | NS | 99 | 58.8 ± 13.2 | 67/99 |
| Surgical | Mixed | 45 | 58.9 ± 11.4 | 36/45 | ||||
| Khashab 59 | 2017 | USA, Japan | Retrospective | EUS-GJ (arm excluded for overlap) 1 | 30 1 | 70 ± 13.3 1 | 17/30 1 | |
| Surgical | Open | 63 | 68 ± 9.6 | 32/63 | ||||
| Kim 60 | 2017 | South Korea | Retrospective | SEMS | Partially covered | 18 | 71.2 ± 10.0 | 9/18 |
| Ojima 61 | 2017 | Japan | Retrospective | Surgical | Open | 23 | 67 median (range 45–85) | 15/23 |
| Surgical | Lap | 30 | 71 median (range 52–85) | 20/30 | ||||
| Perez-Miranda 62 | 2017 | USA, Spain, France | Retrospective | EUS-GJ 1 | EUS-GJ 1 | 25 1 | 63.9 1 | 11/25 1 |
| Surgical | Lap, with conversion to open at surgeon's discretion | 29 | 75.8 | 22/29 | ||||
| Takahara 63 | 2017 | Japan | Retrospective | SEMS | Partially covered | 41 | 67 median (range 35–89) | 26/41 |
| Tanaka 64 | 2017 | Japan | Retrospective | Surgical | lap | 43 | 67 median (range 43–83) | 29/43 |
| Tsauo 65 | 2017 | South Korea | Retrospective | SEMS | Dual stent consisting of outer partially covered stent and inner bare stent | 40 | 56.8 ± 10.6 | 23/40 |
| Ye 66 | 2017 | Taiwan | Retrospective | SEMS | Uncovered | 87 | 71.1 ± 14.6 | 58/87 |
| Yoshida 67 | 2017 | Japan | Retrospective | SEMS | Uncovered | 23 | 70 (range 48–87) | 15/23 |
| Surgical | Mixed (28 open, 2 lap) | 30 | 63.5 (range 46–72) | 16/30 | ||||
| SEMS | Uncovered | 23 | 70 (range 48–87) | 15/23 | ||||
| Bekheet 68 | 2018 | South Korea | Retrospective | SEMS | Covered | 55 | 60.6 (range 38–89) | 35/55 |
| Choi 69 | 2018 | South Korea | Retrospective | SEMS (Bonastent Wing) | Partially covered | 63 | 65.0 (range 58.5–75.0) | 44/63 |
| Leiyuan 70 | 2018 | China | Retrospective | SEMS | NS | 29 | 64.6 ± 14.2 | 19/29 |
| Surgical | Lap | 34 | 59.8 ± 15.5 | 21/34 | ||||
| Uemura 71 | 2018 | Japan | Retrospective | SEMS | Uncovered | 64 | 72 (range 43–90) | 32/64 |
| Surgical | Open | 35 | 68 (range 47–87) | 12/35 | ||||
| Yukimoto 72 | 2018 | Japan | Retrospective | SEMS | Uncovered | 38 | 73.0 median (IQR 65.0–79.0) | 23/38 |
| Surgical | Open | 27 | 75.0 median (IQR 66.0–81.5) | 18/27 | ||||
| Ge 22 | 2019 | USA | Prospective | SEMS | Uncovered | 78 | 65.7 ± 12.6 | 47/78 |
| EUS-GJ | EUS-GJ | 22 | 66.4 ± 9.2 | 9/22 | ||||
| Jang 73 | 2019 | USA | Retrospective | SEMS | Uncovered | 183 | 66.2 ± 14.3 | 90/183 |
| Surgical | Mixed | 127 | 67.5 ± 11.1 | 80/127 | ||||
| Kerdsirichairat 74 | 2019 | USA | Retrospective | EUS-GJ | malignant | 48 | 65 median for all | 28/57 for all |
| EUS-GJ 1 | Benign 1 | 9 1 | ||||||
| Kumar 75 | 2019 | India | Retrospective | SEMS | NS | 90 | 56.4 ± 11.7 | 43/90 |
| SEMS | NS | 24 | 56.9 ± 11.6 | 12/24 | ||||
| Ramos 76 | 2019 | Brazil | Retrospective | Surgical | Gastric partitioning | 30 | 67.5 ± 13.4 | 22/30 |
| Surgical | Conventional GJ | 30 | 64.3 ± 12.7 | 19/30 | ||||
| Ratone 77 | 2019 | France | Retrospective | SEMS | Uncovered | 220 | 67.2 ± 13.9 | 123/220 |
| Sterpetti 78 | 2019 | Italy | Prospective | SEMS | 87 | 71 | 57/87 | |
| Alcala-Gonzalez 79 | 2020 | Spain | Retrospective | SEMS | Uncovered | 36 | 68 median (IQR 53–83) | 20/36 |
| Kastelijn 5 | 2020 | The Netherlands, Germany, Spain, Italy | Retrospective | EUS-GJ | EUS-GJ | 45 | 69.9 ± 12.3 | 22/45 |
| Miwa 80 | 2020 | Japan | Prospective | SEMS | Uncovered | 31 | 70 median (range 52–90) | 19/31 |
| Mo 81 | 2020 | South Korea | Retrospective | SEMS | 61 Uncovered, 29 covered initially | 90 | 72.1 (range 31–96) | 59/90 |
| Wu 82 | 2020 | Taiwan | Retrospective | SEMS | Uncovered | 71 | 63 ± 16 | 36/71 |
| SEMS | Uncovered | 32 | 62 ± 12 | 17/30 | ||||
| Xu 83 | 2020 | China | Retrospective | EUS-GJ | EUS-GE | 36 | 69.0 ± 12.8 | 17/36 |
| Yildirim 84 | 2020 | Turkey | Retrospective | Surgical | Open | 37 | 68.7 ± 14.4 | 25/37 |
| Surgical | Mixed (2 lap, 14 open) | 16 | 62.7 ± 10.2 | 11/16 | ||||
| Hindryckx 85 | 2021 | Belgium | Retrospective | EUS-GJ | EUS-GJ | 6 | ||
| Kouanda 86 | 2021 | USA | Retrospective | EUS-GJ | EUS-GJ | 36 | 70.4 ± 11.8 | 20/36 |
| Surgical | Open | 14 | 71.5 ± 15.6 | 8/14 | ||||
| Yamao 87 | 2021 | Japan | Prospective randomized | SEMS | Covered | 182 | 73.5 median (range 35–97) | 98/182 |
| SEMS | Uncovered | 184 | 72 median (range 43–96) | 107/184 |
SEMS, self-expanding metal stent; EUS-GJ, endoscopic ultrasound-guided gastrojejunostomy.
Trial arms were excluded due to overlap with one or more other studies.
Fig. 1.
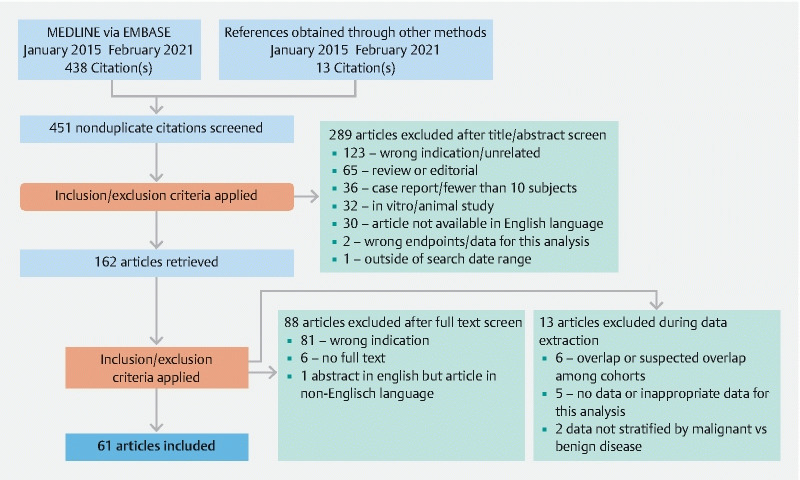
Flow diagram of literature search and study selection.
Patients who were treated with EUS-GJ were significantly older than patients who were treated with duodenal SEMS or surgical GJ (mean age 69.1 for EUS-GJ, 64.2 for duodenal SEMS, 64.3 years for surgical GJ, P = 0.0004) The EUS-GJ treatment group had a lower proportion of males than the surgical GJ group (50.3 % vs. 65.6 %, P = 0.0042 for pairwise comparison). The preprocedural GOOSS scores were similar among groups (0.62 for duodenal SEMS vs. 0.60 for EUS-GJ vs. 0.68 for surgical GJ, P = 0.7783).
Study quality
All 61 publications were assessed for quality with the modified NOS. Thirty-eight studies were judged to have good quality, 17 moderate quality, and six poor quality ( eTable 2 ).
Assessment of heterogeneity
Heterogeneity was found in the analyses endpoints ( eTable 3 ). There was heterogeneity in the EUS-GE and SEMS groups for technical success, stent migration, and death reported in AE section, in the Surgical GJ and SEMS groups for clinical success, reintervention, procedure-related complications, and pre- and postprocedural GOOSS score, and for the SEMS group only for bleeding, recurrence of GOO, stent occlusion, ingrowth, and overgrowth. No heterogeneity was found in the analyses of perforation and patency for any group.
Efficacy outcomes
Technical success
Forty-four of 61 (72.1 %) studies reported rates of procedural technical success. Consistent with its more recent development, EUS-GE was reported to have a significantly lower rate of technical success than the other two treatments (pooled rates 95.3 % for EUS-GE vs. 99.4 % for duodenal SEMS [ P = 0.0495 for pairwise comparison] and 95.3 % for EUS-GE vs. 99.9 % for surgical GJ [ P = 0.0060 for pairwise comparison]) ( Table 2 ).
Table 2. Summary of efficacy and safety meta-analytic outcomes for three treatments for malignant gastric outlet obstruction.
| Duodenal SEMS | EUS-GJ | Surgical GJ | P value 1 | |||||||
| N studies | N patients | % (95 % CI) | N studies | N patients | % (95 % CI) | N studies | N patients | % (95 % CI) | ||
| Efficacy outcomes | ||||||||||
|
45 | 4413 | 99.4 % (98.9 % to 99.8 %) | 8 | 245 | 95.3 % (89.3 % to 98.9 %) | 13 | 564 | 99.9 % (99.5 % to 100.0 %) | 0.0048 |
|
45 | 4590 | 88.9 % (86.7 % to 90.9 %) | 8 | 245 | 89.0 % (82.3 % to 94.3 %) | 13 | 588 | 92.3 % (86.9 % to 96.3 %) | 0.49 |
|
27 | 2655 | 0.62 (0.50 to 0.73) | 2 | 65 | 0.60 (0.44 to 0.76) | 6 | 215 | 0.68 (0.52 to 0.83) | 0.78 |
|
19 | 2184 | 2.27 (2.12 to 2.41) | 2 | 59 | 2.57 (1.83 to 3.32) | 5 | 180 | 2.20 (1.48 to 2.92) | 0.71 |
|
11 | 573 | 28.7 % (19.7 % to 38.6 %) | 1 | 25 | 4.0 % (0.0 % to 15.0 %) | 8 | 342 | 16.9 % (11.6 % to 23.0 %) | 0.0036 |
|
33 | 2963 | 20.3 % (16.9 % to 23.9 %) | 4 | 129 | 11.2 % (4.9 % to 19.6 %) | 9 | 418 | 12.6 % (6.6 % to 20.1 %) | 0.041 |
| Safety outcomes | ||||||||||
|
43 | 4285 | 18.7 % (14.7 % to 23.1 %) | 6 | 189 | 21.9 % (16.3 % to 28.1 %) | 16 | 746 | 23.8 % (18.6 % to 29.5 %) | 0.32 |
|
25 | 2854 | 1.7 % (0.9 % to 2.7 %) | 4 | 141 | 2.9 % (0.2 % to 8.6 %) | 9 | 412 | 5.2 % (3.2 % to 7.5 %) | 0.0048 |
|
24 | 2823 | 1.6 % (1.1 % to 2.3 %) | 3 | 105 | 2.8 % (0.0 % to 10.7 %) | 3 | 170 | 2.0 % (0.0 % to 7.3 %) | 0.88 |
|
33 | 3451 | 4.8 % (3.6 % to 6.1 %) | 4 | 116 | 2.4 % (0.0 % to 10.1 %) | 0 | --- | --- | 0.45 |
|
22 | 1993 | 12.9 % (7.9 % to 18.8 %) | 3 | 69 | 0.5 % (0.0 % to 4.2 %) | 0 | --- | --- | 0.0002 |
|
22 | 2172 | 10.9 % (7.5 % to 14.8 %) | 1 | 24 | 4.2 % (0.0 % to 15.6 %) | 0 | --- | --- | 0.22 |
|
3 | 140 | 85.9 % (79.7 % to 91.2 %) | 0 | --- | --- | 0 | --- | --- | --- |
|
20 | 1962 | 5.5 % (4.1 % to 7.1 %) | 0 | --- | --- | 0 | --- | --- | --- |
|
0 | --- | --- | 0 | --- | --- | 5 | 196 | 16.1 % (6.8 % to 28.2 %) | --- |
|
26 | 2151 | 0.8 % (0.2 % to 1.7 %) | 4 | 151 | 1.7 % (0.0 % to 8.7 %) | 8 | 421 | 0.9 % (0.1 % to 2.9 %) | 0.89 |
|
47 | 4711 | --- | 8 | 243 | --- | 18 | 818 | --- | |
SEMS, self-expanding metal stent; EUS-GJ, endoscopic ultrasound-guided gastrojejunostomy; GOO, gastric outlet obstruction; GOOSS, Gastric Outlet Obstruction Scoring System; AE, adverse event.
P value for comparison of duodenal SEMS vs. EUS-GJ vs. surgical GJ.
Clinical success
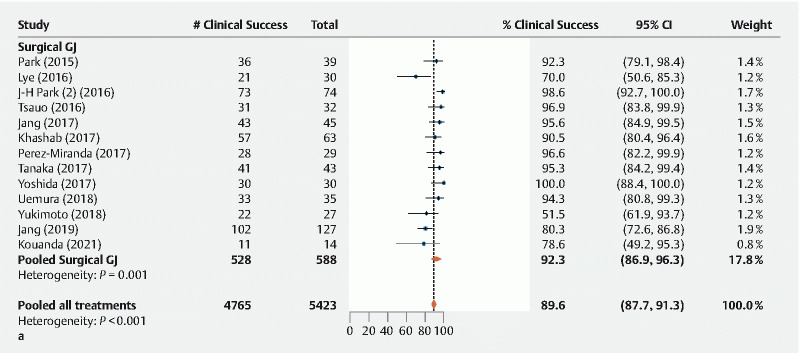
Five distinct definitions of “clinical success” were documented among 51 of 61 (83.6 %) studies that reported this endpoint. The most common definition was improved clinical symptoms (especially obstructive symptoms and vomiting) and/or improved oral intake or GOOSS score (19 studies), followed by change in GOOSS score (18), followed by improved oral intake (12), improved oral intake and hospital discharge (1), and resolution of GOO symptoms (intractable vomiting necessitating gastric drainage) the day after stent implantation (1). Pooled rates of “clinical success” were similar among the three treatments, with 88.9 % for duodenal SEMS, 89.0 % for EUS-GE, and 92.3 % for surgical GJ ( P = 0.49) ( Fig. 2a , Table 2 ). Among studies reporting outcomes for laparoscopic GJ alone, open surgical GJ alone, or mixed laparoscopic or surgical GJ, rates of clinical success were similar (96.6 % vs. 85.9 % vs. 93.8 % respectively, P = 0.2903).
Fig. 2a.
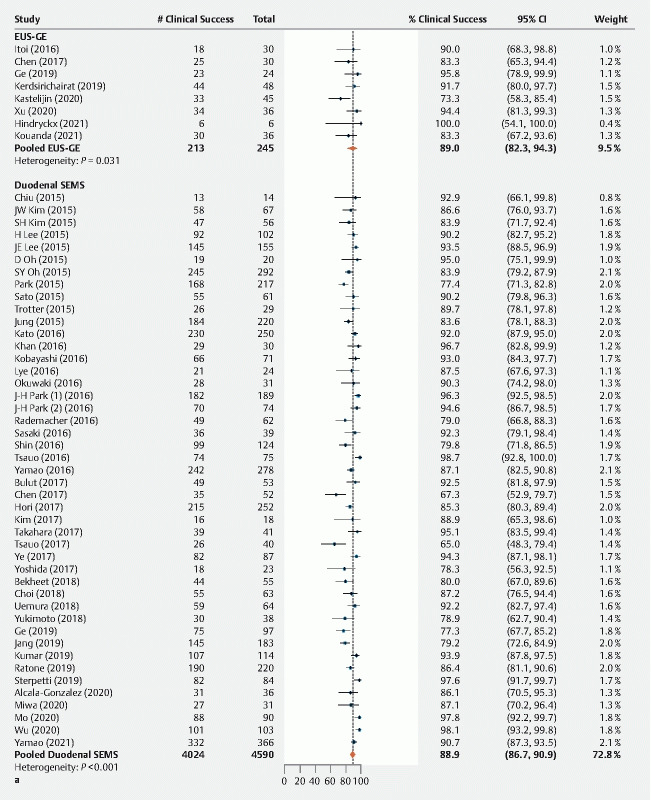
Analysis of efficacy outcomes. Outcomes for clinical success.
Fig. 2a.
Analysis of efficacy outcomes. Outcomes for clinical success.
Pre-procedure and post-procedure GOOSS score
Pooled estimates of mean preprocedural GOOSS score 0.62 for duodenal SEMS, 0.60 for EUS-GE, and 0.68 for surgical GJ, reflecting minimal oral intake before treatment ( Fig. 2b , Table 2 ). Estimated mean postprocedural GOOSS scores exceeded two for all three treatments (2.27 for duodenal SEMS, 2.57 for EUS-GE, and 2.20 for surgical GJ), suggesting that most patients were able to eat solid food after treatment ( Fig. 2c , Table 2 ).
Fig. 2b.
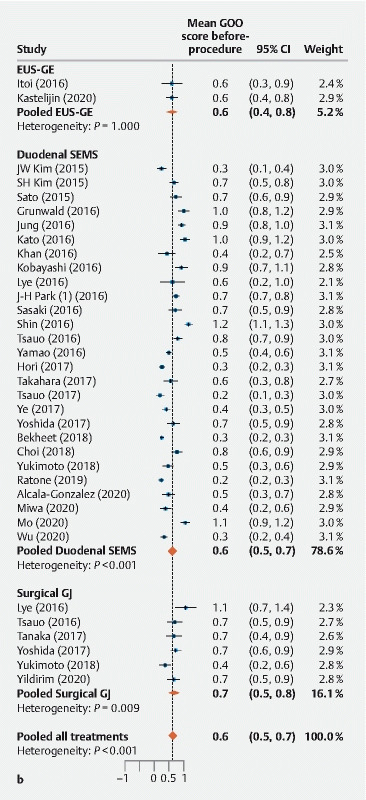
Analysis of efficacy outcomes. Outcomes for preprocedural GOOSS score.
Fig. 2c.
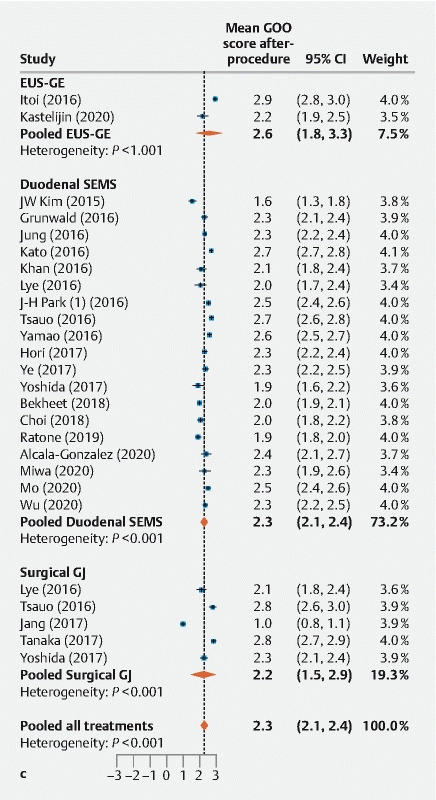
Analysis of efficacy outcomes. Outcomes for postprocedural GOOSS score.
Recurrence of GOO
Recurrence of GOO in the EUS-GE group (4.0 %, 95 % CI 0.0 % to 15.0 %) was significantly lower than for duodenal SEMS (28.7 %, 95 % CI 19.7 % to 38.6 %; P = 0.0040 for pairwise comparison) and similar to surgical GJ (16.9 %, 95 % CI 11.6 % to 23.0 %; P = 0.11 for pairwise comparison) ( Fig. 2d , Table 2 ). Only one EUS-GE study (N = 25 patients) was included in this comparison, while 11 studies of duodenal SEMS (573 patients) and eight studies of surgical GJ (342 patients) were represented.
Fig. 2d.
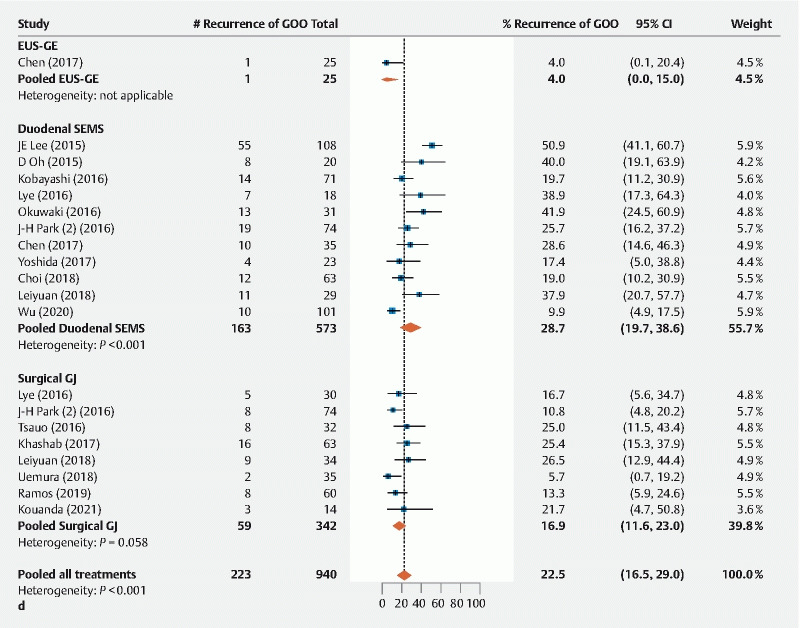
Analysis of efficacy outcomes. Outcomes for recurrence of GOO.
Reintervention
Rates of reintervention (for any reason) during the study period were lower for EUS-GE (11.2 % among 129 patients in four studies) and surgical GJ (12.6 % among 418 patients in nine studies) than for duodenal SEMS (20.3 % among 2963 patients in 33 studies) ( P = 0.041 for comparison of all three treatments, pairwise comparisons did not show significant differences) ( Fig. 2e , Table 2 ).
Fig. 2e.
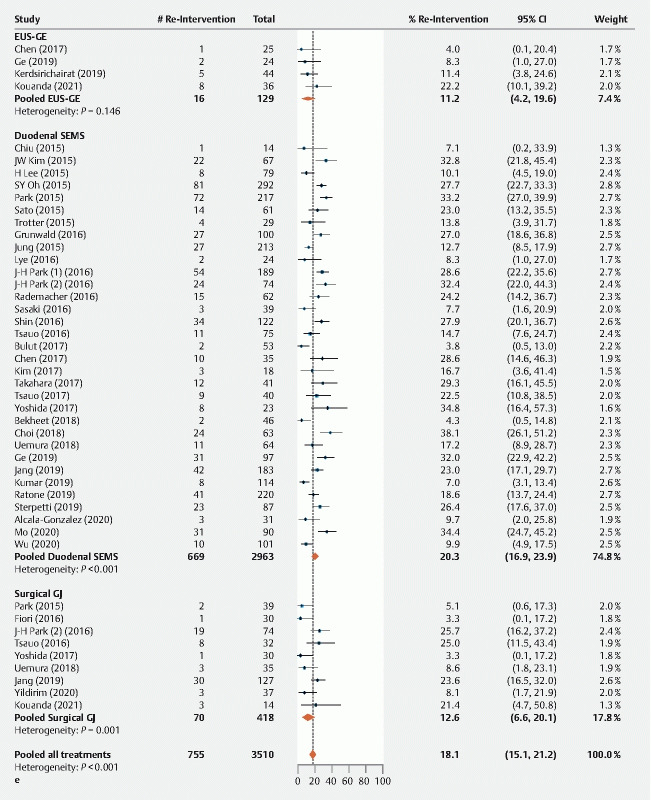
Analysis of efficacy outcomes. Outcomes for reintervention.
Safety outcomes
Any procedure-related serious adverse event
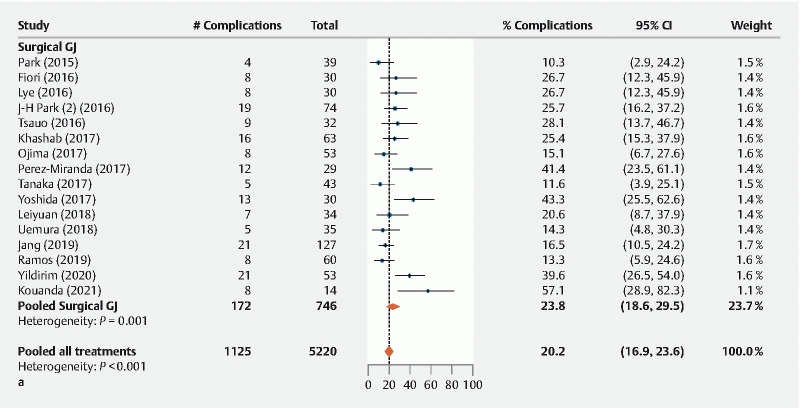
The pooled rate of any procedure-related serious adverse event was similar among the three treatments, i. e. 18.7 %, 95 % CI 14.7 % to 23.1 % for SEMS vs. 21.9 %, 95 % CI 16.3 % to 28.1 % for EUS-GE vs. 23.8 %, 95 % CI 18.6 % to 29.5 % for surgical GJ ( P = 0.32) ( Fig. 3a , Table 2 ). Among studies reporting outcomes for laparoscopic GJ alone, open surgical GJ alone, or mixed laparoscopic or open surgical GJ, rates of procedure-related complications were similar (17.6 % vs. 26.9 % vs. 19.3 % respectively, P = 0.1340).
Fig. 3a.
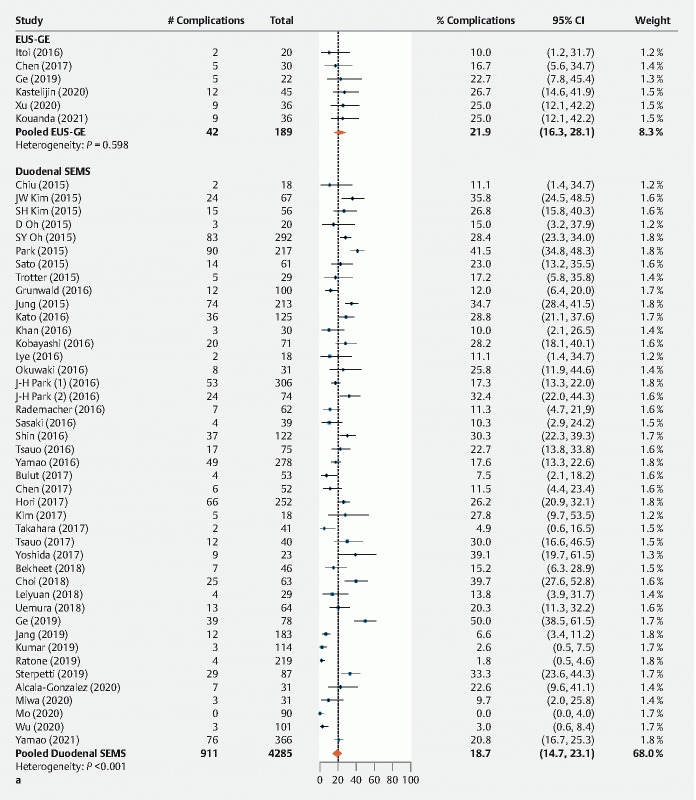
Analysis of safety outcomes. Outcomes for any procedure-related adverse event.
Fig. 3a.
Analysis of safety outcomes. Outcomes for any procedure-related adverse event.
Bleeding
The bleeding rate associated with duodenal SEMS (1.7 %, 95 % CI 0.9 % to 2.7 %) was similar to the rate for EUS-GE (2.9 %, 95 % CI 0.2 % to 8.6 %; P = 0.999 for pairwise comparison) and lower than the rate for surgical GJ (5.2 %, 95 % CI 3.2 % to 7.5 %; P = 0.0033 for pairwise comparison) ( Fig. 3b , Table 2 ).
Fig. 3b.
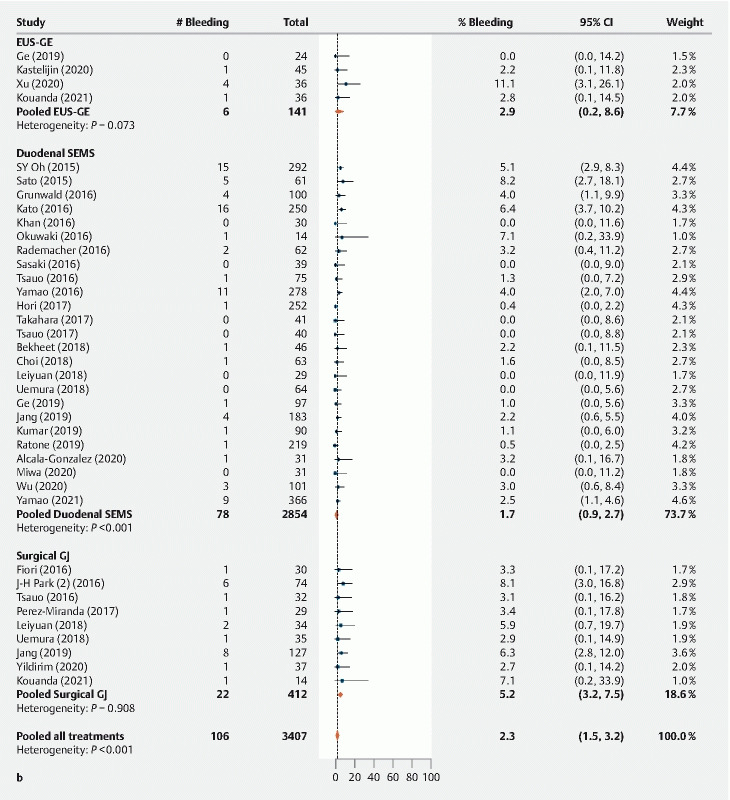
Analysis of safety outcomes. Outcomes for bleeding.
Perforation
Perforation rates were similar among the three treatments, with 1.6 % for duodenal SEMS, 2.8 % for EUS-GE, and 2.0 % for surgical GJ ( P = 0.88) ( Fig. 3c , Table 2 ).
Fig. 3c.
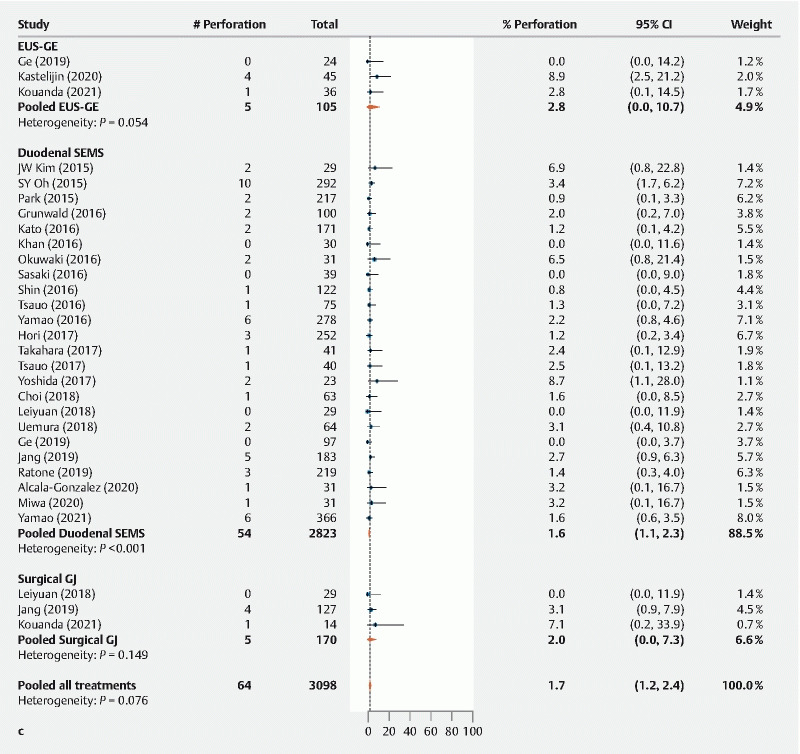
Analysis of safety outcomes. Outcomes for perforation.
Stent-related outcomes
Duodenal SEMS and EUS-GE were reported to have similar rates of stent migration (4.8 % vs. 2.4 % respectively, P = 0.45) ( Fig. 3d , Table 2 ) and tissue ingrowth (10.9 % vs. 4.2 % [based on one study of EUS-GE], P = 0.22) ( Fig. 3e , Table 2 ), while stent occlusion was significantly higher for duodenal SEMS (12.9 % vs. 0.5 % respectively, P = 0.0002) ( Fig. 3f , Table 2 ).
Fig. 3d.
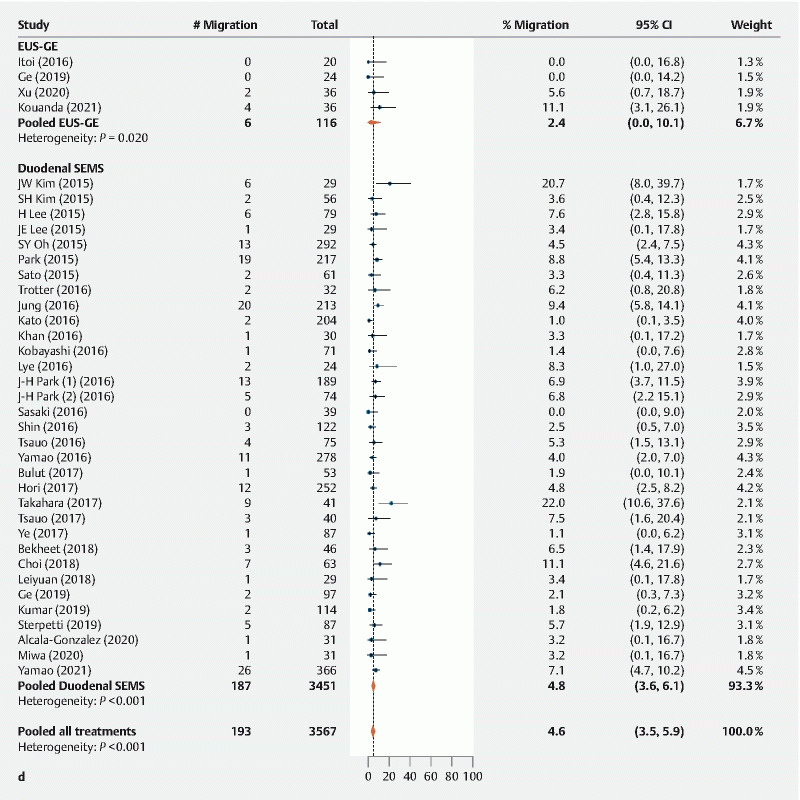
Analysis of safety outcomes. Outcomes for stent migration.
Fig. 3e.
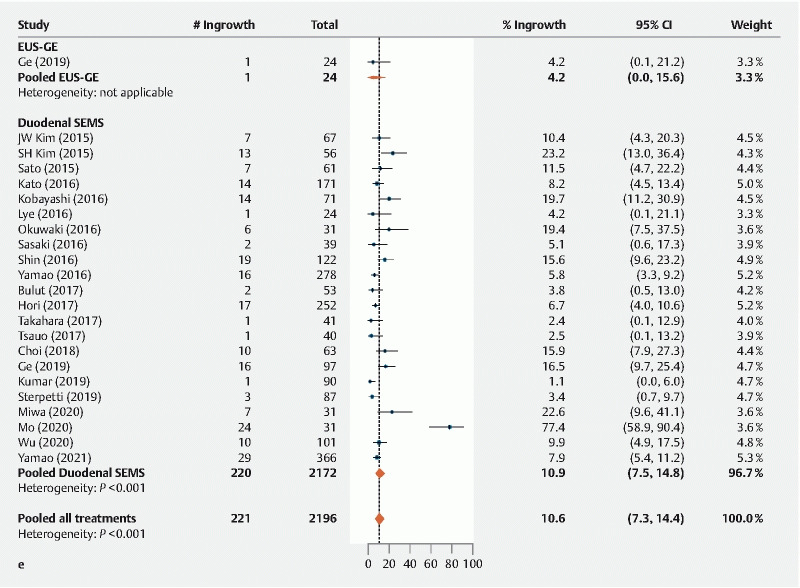
Analysis of safety outcomes. Outcomes for e tissue ingrowth.
Fig. 3f.
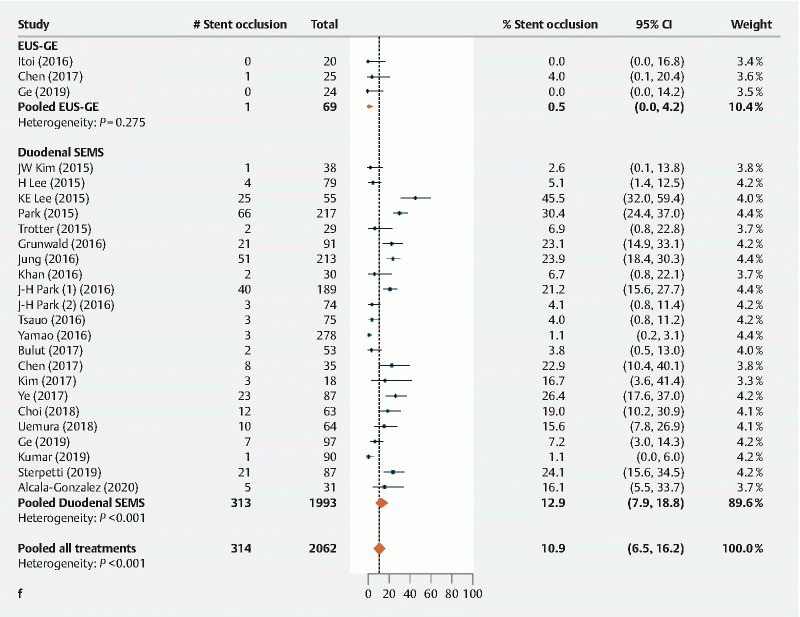
Analysis of safety outcomes. Outcomes for stent occlusion.
Stent patency (85.9 %) ( Fig. 3g , Table 2 ) and tissue overgrowth (5.5 %) ( Fig. 3h , Table 2 ) were adequately reported for duodenal SEMS but not for EUS-GE.
Fig. 3g.
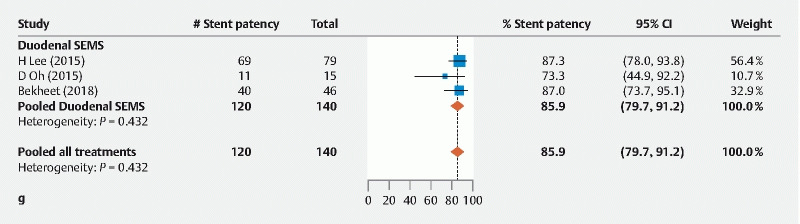
Analysis of safety outcomes. Outcomes for stent patency.
Fig. 3h.
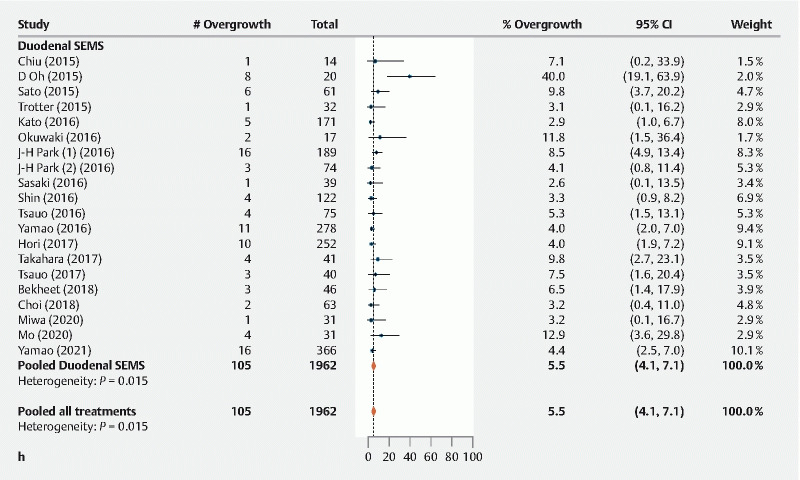
Analysis of safety outcomes. Outcomes for tissue overgrowth.
Deaths reported in adverse events section
Using deaths reported in the AEs section of the articles as a surrogate of procedure-related deaths, all three interventions were associated with a similar risk (EUS-GE [1.7 %], vs. duodenal SEMS [0.8 %], and surgical GJ [0.9 %] [ P = 0.89]) ( Fig. 3i , Table 2 ).
Fig. 3i.
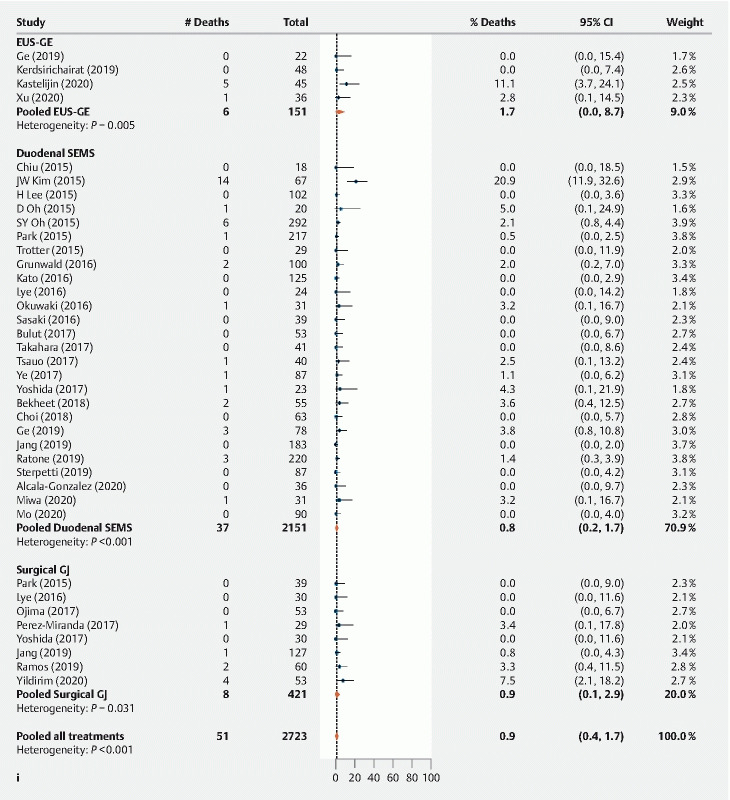
Analysis of safety outcomes. Outcomes for deaths reported in AE section.
Sensitivity analysis
In a sensitivity analysis including 43 studies (33 SEMS, 6 EUS-GE, four surgical GJ) rated as good quality, statistically significant differences from the main analysis included: no significant difference in technical success (99.4 % vs. 95.2 % vs. 99.6 %, P = 0.097) and reintervention (18.9 % vs. 11.2 % vs. 23.4 %, P = 0.082), and a significant difference in preprocedural GOOSS score (0.59 vs. 0.60 vs. 1.07, P = 0.037) among the SEMS, EUS-GJ and surgical GJ arms respectively.
Publication bias
Publication bias was suggested by a significant Begg and Mazumdar test (p ≤ 0.10) with continuity correction for technical success in duodenal SEMS and surgical GJ, procedure-related complications for EUS-GE and surgical GJ, and overgrowth for duodenal SEMS ( eTable 4 ). The Egger test showed a lack of symmetry of the funnel plots ( eFigures 1A–1M ) for technical success (surgical GJ), reintervention (surgical GJ), procedure-related complications (EUS-GE and surgical GJ), bleeding (duodenal SEMS), perforation (EUS-GE), migration (EUS-GJ), overgrowth (duodenal SEMS), and preprocedural and postprocedural GOOSS score (duodenal SEMS for both measures).
Discussion
In this systematic review and meta-analysis of 61 studies including 5772 patients with malignant GOO, duodenal SEMS, EUS-GE and surgical GJ were found to achieve similar rates of clinical success and similar improvement in dietary intake. EUS-GE was reported to have the lowest rate of technical success and (based on one study) lowest recurrence of GOO, while duodenal SEMS had the highest rate of reintervention. Overall procedure-related AEs were similar among the treatments, but duodenal SEMS had a lower bleeding rate than the other two treatments and a higher rate of stent occlusion than EUS-GE.
Surgical GJ for GOO evolved from an open procedure performed for a patient with a duodenal ulcer in 1884 14 , to the introduction of laparoscopic GJ in 1992 15 . Laparoscopic GJ has shown improved morbidity and mortality rates compared with the open surgical approach 16 , for which delayed gastric emptying rates of 20 % or more and overall complication rates of 25 % to 35 % have been reported 1 . Endoscopic duodenal stenting using SEMS was described in the early 1990 s as a minimally invasive treatment for malignant GOO 17 . While periprocedural outcomes for duodenal stenting are favorable, high reocclusion rates increase the risk of obstruction and need for reintervention over time 18 . A 2020 multicenter prospective study of EUS-GE reported a high rate of AEs including five fatalities 5 . However, because the deaths were reported at one center, these results might be more reflective of an early phase of procedural training than of long-term expected outcomes at centers with endoscopists who are familiar with the technique 19 .
Our findings are consistent with the 2021 American Gastroenterology Association Clinical Practice Update on the Optimal Management of the Malignant Alimentary Tract Obstruction 20 . This expert review advised that for surgical candidates with GOO having life expectancy greater than 2 months and good functional status, surgical GJ should be considered, preferably using a laparoscopic approach 20 . EUS-GE was considered an acceptable alternative to surgical GJ depending on the endoscopist’s experience, while patients who are not candidates for surgical or endoscopic GE should be considered for an enteral stent 20 . Similarly, the European Society of Gastrointestinal Endoscopy (ESGE) currently recommends EUS-GE performed in an expert setting for malignant GOO, as an alternative to enteral stenting or surgery 21 . EUS-GE is a newer procedure requiring advanced endoscopist expertise; therefore should currently be limited to specialized endoscopy centers with high procedural volume and endoscopists trained in this advanced therapeutic EUS approach. Our results reflect the early stage of EUS-GE procedural development, including its significantly lower reported rate of technical success and higher (but not significantly) rate of deaths reported in the AEs sections of eligible articles. After wider dissemination and increasing familiarity among endoscopists, EUS-GE could potentially be used more frequently as a less invasive approach compared to surgery.
There are several considerations that go into selection of what treatment approach is chosen for an individual patient with malignant GOO. Reviewing the cross-sectional imaging (ideally a CT scan) to evaluate for proximity of the small bowel to the stomach, and quantity of intervening ascites (which, should give pause at least with early use of EUS-GE) 22 . Carcinomatosis with ascites predicts unfavorable long-term clinical outcomes in patients undergoing SEMS placement for malignant GOO 23 24 , and a large amount of ascites is currently considered by some to be an absolute contraindication to EUS-GE 25 . Both covered and uncovered enteral SEMS have been utilized in the management of malignant GOO, although, covered SEMS are not universally available worldwide (unavailable in the US, while available in Asia and Europe). Compared to covered SEMS, uncovered duodenal SEMS are generally thought to have lower risk of migration and lower risk of impacting biliary and pancreatic drainage when it covers the papilla, but have higher risk of reobstruction from tumor ingrowth 26 27 . Hence, the following factors could be considered in the choice of covered vs uncovered SEMS: 1) anticipated life expectancy and aggressiveness of the tumor; 2) extraluminal vs intraluminal tumors (tumor ingrowth is less of a problem in extrinsic tumors); 3) location of the tumor relative to the papilla; and 4) availability by region/country.
Life expectancy greater than 2 to 3 months should encourage the selection of an EUS-GE, due to its lower rates of reintervention, and although not borne out in this meta-analysis, a likely higher rate of initial clinical success as reported in some previous studies and based on our experience 22 28 . For patients with combined obstruction of the bile duct and duodenum (common occurrence in periampullary malignancies) at centers with adequate endoscopic expertise, EUS-GE may have an advantage over endoscopic stenting because the site of intervention is away from the tumor site 29 . Therefore, the problem of reocclusion of the stent as a result of tumor overgrowth or ingrowth is unlikely compared to endoscopic enteral stenting 30 . In summary, when expertise is available, EUS-GE can be used in most cases for the treatment of malignant GOO as a less invasive alternative to surgery. However, patients with anticipated short survival, widespread metastasis, diffuse malignant infiltration of the gastric wall, or uncontrolled ascites are better approached with SEMS. Surgery can be reserved for patients with expected prolonged survival in whom less invasive procedures are not feasible or have failed.
Our study has strengths and limitations. In the absence of a 3-arm RCT, this meta-analysis compares the two most common palliative treatments for malignant GOO (duodenal stenting using SEMS and surgical GJ), as well as the newer EUS-GE procedure. Our eligibility criteria were relatively generous to include sufficient data to compare all three treatments. While this allowed an informative review, the quality of some studies included may be lower than reviews with stricter inclusion criteria 1 . Baseline characteristics among the three treatment arms were not equal for age and proportion of males; however, similarity of preprocedural GOOSS scores suggested that patients in all three treatment arms had similarly low levels of oral intake at baseline. Our analysis focused on palliative treatment of symptoms associated with malignant GOO, not on the treatment of associated conditions such as biliary obstruction, which is estimated to occur in 40 % to 92 % of patients with malignant GOO 31 . EUS-GE can be performed using at least three different techniques including direct EUS-GE, device-assisted EUS-GE, and EPASS double balloon-occluded gastrojejunostomy bypass 25 . Outcomes for specific techniques might vary compared to findings for our combined “EUS-GE” category. Time to postprocedure return to oral intake and resumption of chemotherapy, and SEMS migration rates by postprocedure chemotherapy status could not be analyzed because they were incompletely reported or not reported among studies. Because it is a newer technique, limited data on EUS-GE were available for some estimates, e. g. only one EUS-GE study was represented in the analysis of GOO recurrence. Although available in some studies, data on mortality and survival rates was usually missing or of very low quality as has been reported previously 1 . Therefore, our estimated mortality rates may have low generalizability. Incomplete reporting (e. g. outcomes reported only in technically successful cases or other patient subgroup) was also a barrier to comprehensive data on all outcomes.
Conclusions
Duodenal SEMS, EUS-GE and surgical GJ achieve similar rates of clinical success and improved dietary intake. Safety profiles were similar except that bleeding was less common and reintervention was more common for duodenal SEMS. Based on less data than the other two treatments, EUS-GE appears to be a promising treatment for patients with malignant GOO for whom surgery is contraindicated or less desirable.
Acknowledgements
The authors acknowledge Boston Scientific employees Margaret Gourlay, MD, MPH, and Jennifer Olson, PhD, for assistance in preparation of the manuscript. The data, analytic methods, and study materials for this study may be made available to other researchers in accordance with the Boston Scientific Data Sharing Policy (http://www.bostonscientific.com/en-US/data-sharing-requests.html).
Footnotes
Competing interests Dr. Benias is a consultant for Boston Scientific and Fujifilm. Dr. Kozarek receives research support from Boston Scientific and the National Institutes of Health. Dr. Peetermans, Mr. McMullen and Ms. Gjata are full-time employees of Boston Scientific Corporation. Dr. Irani is a consultant for Boston Scientific and Gore.
Supplementary material :
References
- 1.Upchurch E, Ragusa M, Cirocchi R. Stent placement versus surgical palliation for adults with malignant gastric outlet obstruction. Cochrane Database Syst Rev. 2018;5:CD012506. doi: 10.1002/14651858.CD012506.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mintziras I, Miligkos M, Wachter S et al. Palliative surgical bypass is superior to palliative endoscopic stenting in patients with malignant gastric outlet obstruction: systematic review and meta-analysis. Surg Endosc. 2019;33:3153–3164. doi: 10.1007/s00464-019-06955-z. [DOI] [PubMed] [Google Scholar]
- 3.Barthet M, Binmoeller K F, Vanbiervliet G et al. Natural orifice transluminal endoscopic surgery gastroenterostomy with a biflanged lumen-apposing stent: first clinical experience (with videos) Gastrointest Endosc. 2015;81:215–218. doi: 10.1016/j.gie.2014.09.039. [DOI] [PubMed] [Google Scholar]
- 4.Iqbal U, Khara H S, Hu Y et al. EUS-guided gastroenterostomy for the management of gastric outlet obstruction: A systematic review and meta-analysis. Endosc Ultrasound. 2020;9:16–23. doi: 10.4103/eus.eus_70_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kastelijn J B, Moons L MG, Garcia-Alonso F J et al. Patency of endoscopic ultrasound-guided gastroenterostomy in the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2020;8:E1194–E1201. doi: 10.1055/a-1214-5659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Haffar S, Bazerbachi F, Prokop L et al. Frequency and prognosis of acute pancreatitis associated with fulminant or non-fulminant acute hepatitis A: A systematic review. Pancreatology. 2017;17:166–175. doi: 10.1016/j.pan.2017.02.008. [DOI] [PubMed] [Google Scholar]
- 8.Bazerbachi F, Leise M D, Watt K D et al. Systematic review of mixed cryoglobulinemia associated with hepatitis E virus infection: association or causation? Gastroenterol Rep (Oxf) 2017;5:178–184. doi: 10.1093/gastro/gox021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Murad M H, Sultan S, Haffar S et al. Methodological quality and synthesis of case series and case reports. BMJ evidence-based medicine. 2018;23:60–63. doi: 10.1136/bmjebm-2017-110853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Adler D G, Baron T H. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol. 2002;97:72–78. doi: 10.1111/j.1572-0241.2002.05423.x. [DOI] [PubMed] [Google Scholar]
- 11.Higgins J P, Thompson S G, Deeks J J et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Begg C B, Mazumdar M. Biometrics; 1994. Operating characteristics of a rank correlation test for publication bias. [PubMed]
- 13.Egger M, Smith G D, Schneider M et al. Bias in meta-analysis detected by a simple, graphical test. Bmj. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pach R, Orzel-Nowak A, Scully T. Ludwik Rydygier--contributor to modern surgery. Gastric Cancer. 2008;11:187–191. doi: 10.1007/s10120-008-0482-7. [DOI] [PubMed] [Google Scholar]
- 15.Wilson R G, Varma J S. Laparoscopic gastroenterostomy for malignant duodenal obstruction. Br J Surg. 1992;79:1348. doi: 10.1002/bjs.1800791235. [DOI] [PubMed] [Google Scholar]
- 16.Manuel-Vazquez A, Latorre-Fragua R, Ramiro-Perez C et al. Laparoscopic gastrojejunostomy for gastric outlet obstruction in patients with unresectable hepatopancreatobiliary cancers: A personal series and systematic review of the literature. World J Gastroenterol. 2018;24:1978–1988. doi: 10.3748/wjg.v24.i18.1978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Keymling M, Wagner H J, Vakil N et al. Relief of malignant duodenal obstruction by percutaneous insertion of a metal stent. Gastrointest Endosc. 1993;39:439–441. doi: 10.1016/s0016-5107(93)70125-x. [DOI] [PubMed] [Google Scholar]
- 18.Mosler P, Mergener K D, Brandabur J J et al. Palliation of gastric outlet obstruction and proximal small bowel obstruction with self-expandable metal stents: a single center series. J Clin Gastroenterol. 2005;39:124–128. [PubMed] [Google Scholar]
- 19.Keane M G, Khashab M A. Malignant GOO: Are duodenal stenting and surgical gastrojejunostomy obsolete? Endosc Int Open. 2020;8:E1455–E1457. doi: 10.1055/a-1231-5011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ahmed O, Lee J H, Thompson C C et al. AGA Clinical Practice Update on The Optimal Management of the Malignant Alimentary Tract Obstruction: Expert Review. Clin Gastroenterol Hepatol. 2021 doi: 10.1016/j.cgh.2021.03.046. [DOI] [PubMed] [Google Scholar]
- 21.van der Merwe S W, van Wanrooij R LJ, Bronswijk M et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2022;54:185–205. doi: 10.1055/a-1717-1391. [DOI] [PubMed] [Google Scholar]
- 22.Ge P S, Young J Y, Dong W et al. EUS-guided gastroenterostomy versus enteral stent placement for palliation of malignant gastric outlet obstruction. Surg Endosc. 2019;33:3404–3411. doi: 10.1007/s00464-018-06636-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lee J E, Lee K, Hong Y S et al. Impact of carcinomatosis on clinical outcomes after self-expandable metallic stent placement for malignant gastric outlet obstruction. PLoS One. 2015;10:e0140648. doi: 10.1371/journal.pone.0140648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Park C H, Park J C, Kim E H et al. Impact of carcinomatosis and ascites status on long-term outcomes of palliative treatment for patients with gastric outlet obstruction caused by unresectable gastric cancer: stent placement versus palliative gastrojejunostomy. Gastrointest Endosc. 2015;81:321–332. doi: 10.1016/j.gie.2014.06.024. [DOI] [PubMed] [Google Scholar]
- 25.Tonozuka R, Tsuchiya T, Mukai S et al. Endoscopic ultrasonography-guided gastroenterostomy techniques for treatment of malignant gastric outlet obstruction. Clin Endosc. 2020;53:510–518. doi: 10.5946/ce.2020.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tringali A, Costa D, Anderloni A et al. Covered versus uncovered metal stents for malignant gastric outlet obstruction: a systematic review and meta-analysis. Gastrointest Endosc. 2020;92:1153–1163 e1159. doi: 10.1016/j.gie.2020.06.033. [DOI] [PubMed] [Google Scholar]
- 27.Shi-Yi L, Ai-Wu M, Yi-Ping J et al. Placement of duodenal stents across the duodenal papilla may predispose to acute pancreatitis: a retrospective analysis. Diagn Interv Radiol. 2012;18:360–364. doi: 10.4261/1305-3825.DIR.5045-11.1. [DOI] [PubMed] [Google Scholar]
- 28.Boghossian M B, Funari M P, De Moura D TH et al. EUS-guided gastroenterostomy versus duodenal stent placement and surgical gastrojejunostomy for the palliation of malignant gastric outlet obstruction: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021;406:1803–1817. doi: 10.1007/s00423-021-02215-8. [DOI] [PubMed] [Google Scholar]
- 29.Nabi Z, Reddy D N. Endoscopic management of combined biliary and duodenal obstruction. Clin Endosc. 2019;52:40–46. doi: 10.5946/ce.2018.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chen Y I, Itoi T, Baron T H et al. EUS-guided gastroenterostomy is comparable to enteral stenting with fewer re-interventions in malignant gastric outlet obstruction. Surg Endosc. 2017;31:2946–2952. doi: 10.1007/s00464-016-5311-1. [DOI] [PubMed] [Google Scholar]
- 31.Zhang H C, Tamil M, Kukreja K et al. Review of simultaneous double stenting using endoscopic ultrasound-guided biliary drainage techniques in combined gastric outlet and biliary obstructions. Clin Endosc. 2020;53:167–175. doi: 10.5946/ce.2019.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chiu K W, Razack A, Maraveyas A. Self-expandable metal stent placement for malignant duodenal obstruction distal to the bulb. Eur J Gastroenterol Hepatol. 2015;27:1466–1472. doi: 10.1097/MEG.0000000000000479. [DOI] [PubMed] [Google Scholar]
- 33.Kim J W, Jeong J B, Lee K L et al. Comparison between uncovered and covered self-expandable metal stent placement in malignant duodenal obstruction. World J Gastroenterol. 2015;21:1580–1587. doi: 10.3748/wjg.v21.i5.1580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kim S H, Chun H J, Yoo I K et al. Predictors of the patency of self-expandable metallic stents in malignant gastroduodenal obstruction. World J Gastroenterol. 2015;21:9134–9141. doi: 10.3748/wjg.v21.i30.9134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lee H, Min B H, Lee J H et al. Covered metallic stents with an anti-migration design vs. uncovered stents for the palliation of malignant gastric outlet obstruction: a multicenter, randomized trial. Am J Gastroenterol. 2015;110:1440–1449. doi: 10.1038/ajg.2015.286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Oh D, Lee S S, Song T J et al. Efficacy and safety of a partially covered duodenal stent for malignant gastroduodenal obstruction: a pilot study. Gastrointest Endosc. 2015;82:32–36 e31. doi: 10.1016/j.gie.2014.11.039. [DOI] [PubMed] [Google Scholar]
- 37.Oh S Y, Edwards A, Mandelson M et al. Survival and clinical outcome after endoscopic duodenal stent placement for malignant gastric outlet obstruction: comparison of pancreatic cancer and nonpancreatic cancer. Gastrointest Endosc. 2015;82:460–468 e462. doi: 10.1016/j.gie.2015.01.026. [DOI] [PubMed] [Google Scholar]
- 38.Sato T, Hara K, Mizuno N et al. Gastroduodenal stenting with Niti-S stent: long-term benefits and additional stent intervention. Dig Endosc. 2015;27:121–129. doi: 10.1111/den.12300. [DOI] [PubMed] [Google Scholar]
- 39.Trotter J M, Balamurugan R, Dear K L et al. Non-centralised service for palliative stenting of malignant gastric outlet obstruction. Ann R Coll Surg Engl. 2015;97:32–34. doi: 10.1308/003588414X14055925058995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Fiori E, Sterpetti A V, De Cesare A et al. Factors leading to improved results for endoscopic stenting for metastatic antropyloric adenocarcinoma. a comparison with gastrojejunostomy. J Gastrointest Surg. 2016;20:1802–1806. doi: 10.1007/s11605-016-3236-6. [DOI] [PubMed] [Google Scholar]
- 41.Grunwald D, Cohen J, Bartley A et al. The location of obstruction predicts stent occlusion in malignant gastric outlet obstruction. Therap Adv Gastroenterol. 2016;9:815–822. doi: 10.1177/1756283X16667893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Itoi T, Ishii K, Ikeuchi N et al. Prospective evaluation of endoscopic ultrasonography-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) for malignant gastric outlet obstruction. Gut. 2016;65:193–195. doi: 10.1136/gutjnl-2015-310348. [DOI] [PubMed] [Google Scholar]
- 43.Jung K, Ahn J Y, Jung H Y et al. Outcomes of endoscopically inserted self-expandable metal stents in malignancy according to the type of stent and the site of obstruction. Surg Endosc. 2016;30:4001–4010. doi: 10.1007/s00464-015-4712-x. [DOI] [PubMed] [Google Scholar]
- 44.Kato H, Kawamoto H, Matsumoto K et al. Outcome of self-expandable metallic stent deployment in patients with malignant gastroduodenal outlet obstruction and Niti-S and WallFlex comparison: a multicenter retrospective clinical study. J Dig Dis. 2016;17:518–525. doi: 10.1111/1751-2980.12377. [DOI] [PubMed] [Google Scholar]
- 45.Khan H, Zhining F, Ghafoor A et al. Palliative treatment of malignant gastric outlet obstruction with self expandable metal stents. J Postgrad Med Instit. 2016;30:213–217. [Google Scholar]
- 46.Kobayashi K, Kobara H, Masaki T. Splenic arterial injury caused by use of a lumen-apposing metal stent for walled-off pancreatic necrosis drainage. Dig Endosc. 2019;31:331. doi: 10.1111/den.13376. [DOI] [PubMed] [Google Scholar]
- 47.Lye T J, Goh Y C, Eng A K et al. Endoscopic self-expandable metallic stenting for palliation of malignant gastric outlet obstruction in Southeast Asia. ANZ J Surg. 2016;86:464–468. doi: 10.1111/ans.12866. [DOI] [PubMed] [Google Scholar]
- 48.Okuwaki K, Kida M, Yamauchi H et al. Randomized controlled exploratory study comparing the usefulness of two types of metallic stents with different axial forces for the management of duodenal obstruction caused by pancreatobiliary cancer. J Hepatobiliary Pancreat Sci. 2016;23:289–297. doi: 10.1002/jhbp.341. [DOI] [PubMed] [Google Scholar]
- 49.Park J H, Lee J H, Song H Y et al. Over-the-wire versus through-the-scope stents for the palliation of malignant gastric outlet obstruction: A retrospective comparison study. Eur Radiol. 2016;26:4249–4258. doi: 10.1007/s00330-016-4289-3. [DOI] [PubMed] [Google Scholar]
- 50.Park J H, Song H Y, Yun S C et al. Gastroduodenal stent placement versus surgical gastrojejunostomy for the palliation of gastric outlet obstructions in patients with unresectable gastric cancer: a propensity score-matched analysis. Eur Radiol. 2016;26:2436–2445. doi: 10.1007/s00330-015-4106-4. [DOI] [PubMed] [Google Scholar]
- 51.Rademacher C, Bechtler M, Schneider S et al. Self-expanding metal stents for the palliation of malignant gastric outlet obstruction in patients with peritoneal carcinomatosis. World J Gastroenterol. 2016;22:9554–9561. doi: 10.3748/wjg.v22.i43.9554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sasaki R, Sakai Y, Tsuyuguchi T et al. Endoscopic management of unresectable malignant gastroduodenal obstruction with a nitinol uncovered metal stent: A prospective Japanese multicenter study. World J Gastroenterol. 2016;22:3837–3844. doi: 10.3748/wjg.v22.i14.3837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Shin Y S, Choi C W, Kang D H et al. Factors associated with clinical failure of self-expandable metal stent for malignant gastroduodenal obstruction. Scand J Gastroenterol. 2016;51:103–110. doi: 10.3109/00365521.2015.1064992. [DOI] [PubMed] [Google Scholar]
- 54.Tsauo J, Yoo M W, Song H Y et al. Partially-covered stent placement versus surgical gastrojejunostomy for the palliation of malignant gastroduodenal obstruction secondary to pancreatic cancer. Abdom Radiol (NY) 2016;41:2233–2240. doi: 10.1007/s00261-016-0810-z. [DOI] [PubMed] [Google Scholar]
- 55.Yamao K, Kitano M, Kayahara T et al. Factors predicting through-the-scope gastroduodenal stenting outcomes in patients with gastric outlet obstruction: a large multicenter retrospective study in West Japan. Gastrointest Endosc. 2016;84:757–763 e756. doi: 10.1016/j.gie.2016.03.1498. [DOI] [PubMed] [Google Scholar]
- 56.Bulut E, Ciftci T, Akhan O et al. Palliation of malignant gastroduodenal obstruction: fluoroscopic metallic stent placement with different approaches. Diagn Interv Radiol. 2017;23:211–216. doi: 10.5152/dir.2016.16165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hori Y, Naitoh I, Hayashi K et al. Predictors of stent dysfunction after self-expandable metal stent placement for malignant gastric outlet obstruction: tumor ingrowth in uncovered stents and migration of covered stents. Surg Endosc. 2017;31:4165–4173. doi: 10.1007/s00464-017-5471-7. [DOI] [PubMed] [Google Scholar]
- 58.Jang S H, Lee H, Min B H et al. Palliative gastrojejunostomy versus endoscopic stent placement for gastric outlet obstruction in patients with unresectable gastric cancer: a propensity score-matched analysis. Surg Endosc. 2017;31:4217–4223. doi: 10.1007/s00464-017-5480-6. [DOI] [PubMed] [Google Scholar]
- 59.Khashab M A, Bukhari M, Baron T H et al. International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2017;5:E275–E281. doi: 10.1055/s-0043-101695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Kim H J. Clinical outcomes of biliary and duodenal self-expandable metal stent placements for palliative treatment in patients with periampullary cancer. Gastrointestinal Intervention. 2017;6:171–175. [Google Scholar]
- 61.Ojima T, Nakamori M, Nakamura M et al. Laparoscopic gastrojejunostomy for patients with unresectable gastric cancer with gastric outlet obstruction. J Gastrointest Surg. 2017;21:1220–1225. doi: 10.1007/s11605-017-3387-0. [DOI] [PubMed] [Google Scholar]
- 62.Perez-Miranda M, Tyberg A, Poletto D et al. EUS-guided gastrojejunostomy versus laparoscopic gastrojejunostomy: an international collaborative study. J Clin Gastroenterol. 2017;51:896–899. doi: 10.1097/MCG.0000000000000887. [DOI] [PubMed] [Google Scholar]
- 63.Takahara N, Isayama H, Nakai Y et al. A novel partially covered self-expandable metallic stent with proximal flare in patients with malignant gastric outlet obstruction. Gut Liver. 2017;11:481–488. doi: 10.5009/gnl16259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tanaka T, Suda K, Satoh S et al. Effectiveness of laparoscopic stomach-partitioning gastrojejunostomy for patients with gastric outlet obstruction caused by advanced gastric cancer. Surg Endosc. 2017;31:359–367. doi: 10.1007/s00464-016-4980-0. [DOI] [PubMed] [Google Scholar]
- 65.Tsauo J, Yoo M W, Park J H et al. Overlapping self-expandable metallic stent for palliation of a long (>10 cm) malignant gastroduodenal obstruction. Acta Radiol. 2017;58:565–572. doi: 10.1177/0284185116664228. [DOI] [PubMed] [Google Scholar]
- 66.Ye B W, Chou C K, Hsieh Y C et al. Metallic stent expansion rate at day one predicts stent patency in patients with gastric outlet obstruction. Dig Dis Sci. 2017;62:1286–1294. doi: 10.1007/s10620-017-4534-x. [DOI] [PubMed] [Google Scholar]
- 67.Yoshida Y, Fukutomi A, Tanaka M et al. Gastrojejunostomy versus duodenal stent placement for gastric outlet obstruction in patients with unresectable pancreatic cancer. Pancreatology. 2017;17:983–989. doi: 10.1016/j.pan.2017.09.011. [DOI] [PubMed] [Google Scholar]
- 68.Bekheet N, Kim M T, Park J H et al. Fluoroscopic gastroduodenal stent placement in 55 patients with endoscopic stent placement failure. Cardiovasc Intervent Radiol. 2018;41:1233–1240. doi: 10.1007/s00270-018-1933-0. [DOI] [PubMed] [Google Scholar]
- 69.Choi Y K, Ahn J Y, Na H K et al. Winged partially covered self-expandable metal stent to prevent distal migration in malignant gastric outlet obstruction. Dig Dis Sci. 2018;63:3409–3416. doi: 10.1007/s10620-018-5284-0. [DOI] [PubMed] [Google Scholar]
- 70.Leiyuan S, Jianli X, Zhengzhong Z et al. Comparison of treatment outcomes of endoscopic stenting and laparoscopic gastrojejunostomy for malignant gastric outlet obstruction. Am Surg. 2018;84:991–995. [PubMed] [Google Scholar]
- 71.Uemura S, Iwashita T, Iwata K et al. Endoscopic duodenal stent versus surgical gastrojejunostomy for gastric outlet obstruction in patients with advanced pancreatic cancer. Pancreatology. 2018;18:601–607. doi: 10.1016/j.pan.2018.04.015. [DOI] [PubMed] [Google Scholar]
- 72.Yukimoto T, Morisaki T, Komukai S et al. The palliative effect of endoscopic uncovered self-expandable metallic stent placement versus gastrojejunostomy on malignant gastric outlet obstruction: a pilot study with a retrospective chart review in Saga, Japan. Intern Med. 2018;57:1517–1521. doi: 10.2169/internalmedicine.0171-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Jang S, Stevens T, Lopez R et al. Superiority of gastrojejunostomy over endoscopic stenting for palliation of malignant gastric outlet obstruction. Clin Gastroenterol Hepatol. 2019;17:1295–1302 e1291. doi: 10.1016/j.cgh.2018.10.042. [DOI] [PubMed] [Google Scholar]
- 74.Kerdsirichairat T, Irani S, Yang J et al. Durability and long-term outcomes of direct EUS-guided gastroenterostomy using lumen-apposing metal stents for gastric outlet obstruction. Endosc Int Open. 2019;7:E144–E150. doi: 10.1055/a-0799-9939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kumar V, Ghoshal U C, Mohindra S et al. Palliation of malignant gastroduodenal obstruction with self-expandable metal stent using side- and forward-viewing endoscope: Feasibility and outcome. JGH Open. 2019;3:65–70. doi: 10.1002/jgh3.12110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Ramos M, Barchi L C, de Oliveira R J et al. Gastric partitioning for the treatment of malignant gastric outlet obstruction. World J Gastrointest Oncol. 2019;11:1161–1171. doi: 10.4251/wjgo.v11.i12.1161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Ratone J P, Caillol F, Zemmour C et al. Outcomes of duodenal stenting: Experience in a French tertiary center with 220 cases. Dig Liver Dis. 2020;52:51–56. doi: 10.1016/j.dld.2019.06.025. [DOI] [PubMed] [Google Scholar]
- 78.Sterpetti A V, Fiori E, Sapienza P et al. Complications after endoscopic stenting for malignant gastric outlet obstruction: a cohort study. Surg Laparosc Endosc Percutan Tech. 2019;29:169–172. doi: 10.1097/SLE.0000000000000656. [DOI] [PubMed] [Google Scholar]
- 79.Alcala-Gonzalez L, Masachs Perecaula M, Dot Bach J et al. Endoscopic stenting for gastroduodenal outlet obstruction of a malignant origin, real life experience in a single center. Rev Esp Enferm Dig. 2020;112:712–715. doi: 10.17235/reed.2020.6600/2019. [DOI] [PubMed] [Google Scholar]
- 80.Miwa H, Sugimori K, Kaneko T et al. Clinical outcome of a highly flexible duodenal stent for gastric outlet obstruction: A multicenter prospective study. JGH Open. 2020;4:729–735. doi: 10.1002/jgh3.12326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Mo J W, Kim Y M, Kim J H et al. Clinical outcomes after multiple self-expandable metallic stent placement using stent-in-stent technique for malignant gastric outlet obstruction. Medicine (Baltimore) 2020;99:e19432. doi: 10.1097/MD.0000000000019432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Wu C H, Lee M H, Tsou Y K et al. Efficacy and adverse effects of self-expandable metal stent placement for malignant duodenal obstruction: the papilla of Vater as a landmark. Cancer Manag Res. 2020;12:10261–10269. doi: 10.2147/CMAR.S273084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Xu G, Shen Y, Lv Y et al. Safety and efficacy of endoscopic ultrasound-guided gastroenterostomy using double balloon occlusion methods: a clinical retrospective study in 36 patients with malignant gastric outlet obstruction. Endosc Int Open. 2020;8:E1690–E1697. doi: 10.1055/a-1221-9656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Yildirim R, Candas B, Usta A A et al. Efficacy of stomach-partitioning on gastric emptying in patients undergoing palliative gastrojejunostomy for malign gastric outlet obstruction. Ulus Travma Acil Cerrahi Derg. 2020;26:678–684. doi: 10.14744/tjtes.2020.14668. [DOI] [PubMed] [Google Scholar]
- 85.Hindryckx P, Degroote H. Lumen-apposing metal stents for approved and off-label indications: a single-centre experience. Surg Endosc. 2021;35:6013–6020. doi: 10.1007/s00464-020-08090-6. [DOI] [PubMed] [Google Scholar]
- 86.Kouanda A, Binmoeller K, Hamerski C et al. Endoscopic ultrasound-guided gastroenterostomy versus open surgical gastrojejunostomy: clinical outcomes and cost effectiveness analysis. Surg Endosc. 2021;35:7058–7067. doi: 10.1007/s00464-020-08221-z. [DOI] [PubMed] [Google Scholar]
- 87.Yamao K, Kitano M, Chiba Y et al. Endoscopic placement of covered versus uncovered self-expandable metal stents for palliation of malignant gastric outlet obstruction. Gut. 2021;70:1244–1252. doi: 10.1136/gutjnl-2020-320775. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.