

Abstract
Objectives:
This study examined self-reported sleepiness as a pathway of effects underlying racial and socioeconomic disparities in children’s academic and cognitive performance.
Design:
The study design was longitudinal, and path modeling was used to test study hypotheses. Setting: Data were collected from participants residing in semirural communities and small towns surrounding Auburn, AL.
Participants:
Children (N = 282; 52% boys) participated in the study when they were 9 (M = 9.44, SD = .71) and 11 (M = 11.33, SD = .69) years old. The sample was 65% White/European American and 35% Black/African American. The majority of the children (63%) were living at or below the poverty line.
Measurements:
At age 9, children reported on their daytime sleepiness over the prior 2 weeks. At ages 9 and 11, children completed cognitive assessments in the laboratory, teachers reported on children’s academic functioning, and schools provided state (Alabama) standardized test scores.
Results:
African American children and children from lower socioeconomic status homes reported greater sleepiness. Greater sleepiness, in turn, predicted lower academic functioning, cognitive performance, and Alabama standardized test scores. Sleepiness was a significant intervening variable, but not a mediator, in these pathways. Race was a stronger predictor of sleepiness than socioeconomic status when both were entered in the same model.
Conclusions:
Results highlight sleepiness as a pathway of effects linking race and socioeconomic status to academic and cognitive outcomes. Psychoeducation targeting sleepiness for African American and lower–socioeconomic status children may be beneficial for boosting achievement.
Keywords: Race, Socioeconomic status, Sleepiness, Academic, Cognitive performance
Black/African American (AA) children and children from lower socioeconomic status (SES) families are at risk for insufficient and poor quality sleep, and elevated daytime sleepiness,1–3 which in turn are predictive of lower academic and cognitive performance.4–6 AA and lower-SES children are also at greater risk for lower academic and cognitive performance compared to white/European American (EA) and higher-SES children.7,8 It is plausible that sleep-wake behaviors contribute to these racial and socioeconomic disparities in children’s development. Recent work with adults has demonstrated that sleep duration and quality serve as intervening or mediating variables linking race/ethnicity and SES with poor physical and mental health.9,10 However, prior work has not examined sleepiness as a mediator or an intervening variable in associations between either race or SES and children’s adaptation. The present study assessed the role of self-reported sleepiness as a pathway of effects underlying racial and socioeconomic disparities in children’s academic and cognitive performance.
Children’s experience of daytime sleepiness, which results frequently from insufficient and poor sleep quality,11 has been linked with lower academic achievement and intellectual ability.5 Increases in daytime sleepiness have also been associated with slower trajectories of growth in cognitive performance across ages 8–10 years old.4 Following a 7-day protocol in which sleep was restricted to 5 hours per night, adolescents showed an increase in sleepiness that paralleled a decrease in attention, working memory, and executive functioning.12 A meta-analysis found that measures of sleepiness had stronger negative effects on children’s school performance, including grades and standardized test scores, than assessments of sleep quality or duration.6 This may be because individuals’ subjective experiences of alertness differ at equivalent levels of sleep quality or duration6 or that sleepiness results from a combination of both insufficient and poor quality sleep for some children.13 Sleepiness may be of particular relevance to academic and cognitive functioning because of its effects on attention and concentration in the school setting,14 as daytime fatigue may compromise children’s ability to engage with their environment.15
There are documented disparities in the duration and quality of sleep as well as daytime sleepiness between EA and AA individuals and between those living in higher- compared to lower-SES homes. Much of the literature pertains to adults,16–18 but there is emerging evidence that these differences in sleep begin in childhood.1–3 For example, in comparison to children from higher-SES backgrounds, those from lower-SES families report more sleep/wake problems2 and greater daytime sleepiness.1 Furthermore, children who felt their family’s socioeconomic position was lower relative to their school and society reported greater daytime sleepiness.3
In addition to racial and socioeconomic disparities in children’s sleep-wake behaviors, disparities have also been documented for academic and cognitive performance.7,8 Thus, it is possible that sleepiness acts as a mediating or intervening variable that underlies disparities detected in achievement outcomes. This idea is consistent with work with adults demonstrating the mediating role of poorer sleep quality in relations between SES, race, and physical and mental health outcomes.9,10 Among children, parent report of children’s greater difficulty initiating or maintaining sleep partially mediated the relation between parents’ perceptions of their family’s economic situation and children’s mental health, including greater symptoms of emotional and conduct problems.19
Current study
The current study examined sleepiness as a potential mechanism (mediator or intervening variable) in the associations among both race (EA and AA children) and SES and children’s academic and cognitive outcomes. To our knowledge, no published study has examined sleepiness in this context. We hypothesized that AA and lower-SES children would report greater daytime sleepiness, which in turn would predict lower academic and cognitive performance. We assessed these associations longitudinally through examination of sleepiness at age 9 and the outcome variables 2 years later at age 11. We controlled for autoregressive effects (ie, academic and cognitive performance at age 9), which allowed us to examine change in academic and cognitive performance over 2 years. Additionally, because there may be unique mechanisms of effects for race and SES, we examined models for each predictor separately as well as simultaneously.
Methods
Participants
Children were part of a longitudinal study of sleep, health, and adjustment across middle to late childhood (Auburn University Sleep Study). Data for the present investigation were drawn from 2 study waves 2 years apart. At the first wave, 282 children (52% boys) and their families were recruited from local elementary schools. Based on mothers’ report, children did not have a diagnosis of a clinical sleep disorder. Children’s mean age was 9.44 years (SD = .71) at the first assessment and 11.33 years (SD = .69) at the subsequent assessment. The sample was 65% EA and 35% AA, which reflect the racial/ethnic representation of the community. Family income-to-needs ratio (annual family income divided by the poverty threshold with respect to family size20) indicated that the majority of participants (63%) were living at or below the poverty line (ratio ≤2), 28% were lower middle class (ratio between 2 and 3), and 9% were middle class (ratio ≥3). Two years later, families partook in another study wave; 80% of the original sample was retained. There were no differences between those who remained vs dropped from the study with regard to family demographics or study variables.
Procedure
The study was approved by the institution’s review board. Parents provided consent to participate, and children provided assent. At age 9, children participated in a laboratory visit during which they reported on their sleepiness and completed cognitive assessments. The same cognitive assessments were repeated at age 11. Teachers reported on children’s classroom performance, and schools provided scores on standardized tests at both study waves.
Measures
Sleep parameters
The main sleep variable of interest in the present study was children’s sleepiness. Although not the focus of the study, sleep duration and quality at age 9 were also assessed and statistically controlled in all analyses to examine the unique effects of sleepiness separate from these sleep parameters.
Sleepiness.
Children completed the Sleep Habits Survey21 via interview. This questionnaire is well established in samples of school-age children.5 The Sleepiness scale (9 items; 1 item regarding driving was deleted) assesses whether the child has fallen asleep, struggled to stay awake, or both during a variety of daily life situations in the past 2 weeks, such as traveling or attending a class at school (α = .70).
Sleep quality.
The sleep/wake problems scale (10 items) of the Sleep Habits Survey was used to measure sleep quality, which was entered as a covariate in all analyses. Example items include whether the child has slept in past noon or had an extremely hard time falling asleep. Children answer on a 5-point scale ranging from “Everyday” to “Never” (α = .63).
Sleep duration.
Children’s nighttime sleep duration was measured using Motionlogger Octagonal Basic actigraphs (Ambulatory Monitoring, Inc, Ardsley, NY). An actigraph assesses sleep via an accelerometer that indicates when there is movement. Intervals when the child was awake or sleeping were then calculated in 1-minute epochs. Sleep duration was defined as the number of epochs scored as sleep between sleep onset and final morning awakening. Children were instructed to wear the actigraph on their nondominant wrist for 7 nights. Actigrahy data were only analyzed for participants with 5 or more nights of actigraphy information (87% of the sample). If the child took medicine for an acute illness on a particular night (eg, cough syrup), the data for that night were not included in analyses. There was good night-to-night stability in sleep duration (α = .85).
Academic and cognitive performance
Towards a more comprehensive examination of these constructs, we used 3 different assessments including teacher reports, individually-administered cognitive measures, and school records of performance on standardized tests.
Academic functioning.
Teachers’ report of children’s academic functioning was obtained from the Student Behavior Survey.22 This questionnaire has established reliability and validity22 and includes questions regarding children’s academic performance (8 items) and habits (13 items). Academic performance items concern children’s abilities in domains such as reading skills and comprehension, spelling, and math. Teachers provide ratings on a 5-point scale ranging from 1 (“Deficient”) to 5 (“Superior”). For the academic habits items, teachers report the frequency with which children show skills such as completing homework assignments and following directions. Ratings are on a 4-point scale from 1 (“Never”) to 4 (“Usually”). The 2 scales were correlated at both time points (rs = .55 and .58). Consistent with prior work,23 we standardized and summed the 2 scales to create 1 academic functioning scale. Internal consistency for this overall scale was good at both time points (αs = .70 and .72).
Cognitive performance.
The well-validated Woodcock Johnson Tests of Cognitive Abilities24,25 were administered individually to children in our research laboratory. Children’s overall performance score, labeled Brief Intellectual Ability (BIA), was used in analyses. This score is a composite reflecting children’s abilities on tests of Verbal Comprehension (analogies, synonyms and antonyms, vocabulary), Concept Formation (fluid and categorical reasoning), and Visual Matching (perceptual processing). BIA scores generally show rank-order stability when assessed in the same group of individuals over time. Per established procedures, vertically equated item response theory–scaled scores (ie, W scores) are produced by the Woodcock Johnson Tests of Cognitive Abilities scoring program and were used in analyses. W scores are calibrated on a Rasch model26 and as such indicate an individual’s deviation from a criterion score. W scores, as contrasted with peer-comparison scores, are ideally suited for measuring change over time.27 The mean score for each age, standardized using very large samples of children, is 500.
Achievement tests.
Children’s performance on the Alabama Reading and Math Tests (ARMT; Montgomery, AL, USA: Alabama State Department of Education) was obtained from schools. The ARMT is an annually administered, criterion-referenced test that is based on Alabama’s reading and mathematics standards. It includes items derived from the nationally-administered Stanford Achievement Test (Stanford 10; Pearson). There is not a normed mean score for the ARMT, and scores do not fall along a particular scale but rather indicate student performance compared to state standards. Children’s scores on the reading and math sections of the test were correlated (r = .71) and were summed to create a total ARMT score.
Demographics
Mothers reported on children’s race and sex as well as family income and number of household members for calculating income-to-needs ratio, which were used to derive SES. Mothers also reported on whether the child had been diagnosed with ADHD or with a chronic illness such as asthma. Children’s weight and height were measured during the laboratory visit, from which standardized BMI (zBMI) was derived based on the Centers for Disease Control criteria.28
Analytic approach
Path modeling analyses were conducted to examine whether sleepiness at age 9 served as a mediating or intervening variable linking race or SES with academic/cognitive outcomes (mostly referred to as academic outcomes for brevity thereafter) at age 11. First, mediation was tested by estimating paths between race and sleepiness (path a), sleepiness and the academic outcome variables (b), and race and the academic outcome variables (c’). The direct relationships between race and the academic outcomes without sleepiness in the model (c) were tested by fixing the paths to and from the sleepiness variable to 0. To fulfill the requirements of full mediation, paths a, b, and c must be significant and path c’ (the direct relationship between race and academic performance with sleepiness in the model) nonsignificant.29 If path c’ remains significant with sleepiness in the model, then partial mediation is supported. If neither full nor partial mediation emerges, the possibility still exists for an intervening relationship, in which the association between 2 variables is contingent on a third.30 In such cases, path c (the direct relationship between race and academic performance without sleepiness in the model) is nonsignificant, but both a and b are significant. In the absence of evidence of full or partial mediation but significant a and b paths, we tested whether sleepiness acted as an intervening variable. The well-established Monte Carlo simulation method31 was used to test the strength of the intervening effects via an online calculation tool32 that produced confidence intervals such that a significant indirect effect was indicated when the confidence interval did not include 0.
An identical set of analyses was run next, replacing race with SES. Finally, a third set of analyses included both race and SES predicting sleepiness in the same model to assess the unique influences of each predictor variable on sleepiness and academic outcomes, controlling for the other.1 The autoregressive paths from the age 9 academic variables to age 11 academic variables were entered in all models to facilitate interpretation of change in the outcome variable and to provide information about the direction of effects.33 Additionally, the 3 academic outcome variables were covaried at both time points to assess unique effects. Toward stringent tests of the models, child sex, zBMI, a diagnosis of chronic illness (n = 53, predominantly asthma) or ADHD (n = 37), and sleep duration and quality at age 9 were covaried in all models. Model fit was considered good if it satis-fied 2 of 3 criteria: χ2/df ≤ 3, comparative fit index (CFI) ≥ .90, and root mean square error of approximation (RMSEA) ≤ .08.34
Analyses were conducted using the Amos Graphics add-on for SPSS 21, which uses full information maximum likelihood estimation to account for missing data. Rates of missingness were generally low (6%−35%) with the exception of teacher-reported academic functioning at age 11, for which only 40% of teachers provided data. Reasons for missing data included parents not giving consent for contacting teachers and teachers choosing not to complete the measures. Using Bonferroni correction to account for multiple t tests, children with missing data for teacher-reported academic functioning at age 11 did not differ from those with complete data with regard to demographics or any study variable. Full information maximum likelihood estimation is considered to be the best statistical method for accounting for missing data due to less bias in estimation and fewer type I errors, and can handle missing data rates up to 90%.35,36
Results
Preliminary analyses
Bivariate correlations, means, and standard deviations for main study variables and covariates are provided in Table 1. Values for all variables were within 4 SDs of the mean, and skewness statistics were all b±1.0. t tests revealed that, compared to EA children, AA children reported greater sleepiness and received lower academic functioning, BIA, and ARMT scores at age 9, in addition to lower BIA and ARMT scores at age 11. AA children were more likely than EA children to live at or below the poverty line, χ2 = 25.60, P b .01. There were no significant differences between boys and girls on main study variables. Means and standard deviations for AA and EA children for the sleepiness and academic variables are presented in Table 2.
Table 1.
Bivariate correlations, means, and standard deviations for main study variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Race | |||||||||||||||
| 2. Family income-to-needs ratio | −.40*** | ||||||||||||||
| 3. Sex | −.02 | .06 | |||||||||||||
| 4. zBMI | .12 | .02 | .03 | ||||||||||||
| 5. Illness/asthma | .07 | −.09 | .10 | −.04 | |||||||||||
| 6. ADHD | −.04 | −.03 | .06 | −.17** | .08 | ||||||||||
| 7. Sleep duration: age 9 | −.12 | .14* | −.11 | −.22** | −.11 | .04 | |||||||||
| 8. Sleep/wake problems: age 9 | .30** | −.21** | .01 | .06 | −.02 | .05 | −.06 | ||||||||
| 9. Sleepiness: age 9 | .25*** | −.15* | −.06 | −.01 | −.04 | −.01 | .01 | .44** | |||||||
| 10. Academic functioning: age 9 | −.25*** | .30*** | −.08 | .05 | −.06 | −.25*** | .15* | −.18* | −.21** | ||||||
| 11. BIA: age 9 | −.25*** | .25*** | −.01 | .05 | −.11 | −.16* | .01 | −.11 | −.24*** | .51*** | |||||
| 12. Alabama test total: age 9 | −.22** | .22** | −.02 | .07 | −.03 | −.21** | .01 | −.18* | −.35*** | .62*** | .76*** | ||||
| 13. Academic functioning: age 11 | −.06 | .27* | −.14 | .07 | −.05 | −.33** | .07 | −.20 | −.41*** | .70*** | .57*** | .57*** | |||
| 14. BIA: age 11 | −.27*** | .29*** | .01 | .11 | −.07 | −.17* | .00 | −.15* | −.30*** | .55*** | .81*** | .79*** | .63*** | ||
| 15. Alabama test total: age 11 | −.20* | .24** | .07 | .14 | .01 | −.25** | .04 | −.16* | −.27** | .68*** | .72*** | .80*** | .72*** | .76 | |
| M | - | 1.71 | - | 0.61 | - | - | 458.31 | 18.97 | 14.68 | 0.00 | 494.57 | 1277.30 | 0.00 | 507.27 | 1353.16 |
| SD | - | 1.04 | - | 1.15 | - | - | 56.16 | 5.23 | 4.61 | 1.78 | 10.34 | 73.01 | 1.77 | 11.20 | 65.47 |
Race was coded as 0 = EA, 1 = AA. Sex was coded as 0 = female, 1 = male. Illness/asthma and ADHD were coded as 0 = absent, 1 = present. Academic functioning was the sum of standardized academic performance and academic habits variables. Prior to standardization, academic performance M (SD) = 28.28 (6.16) and 26.53 (6.78) at ages 9 and 11, respectively. Academic habits M = 45.84 (7.95) and 46.01 (6.65) at ages 9 and 11.
P ≤ .05,
P < .01,
P < .001.
Table 2.
Descriptive sleepiness and academics information by race variable
| AA (N = 99) | EA (N = 183) | t test | |
|---|---|---|---|
| Variable | M (SD) | M (SD) | |
| Sleepiness: age 9 | 16.25 (4.73) | 13.84 (4.33) | −4.19*** |
| Academic functioning: age 9 | −.60 (1.94) | .32 (1.61) | 3.62*** |
| BIA: age 9 | 491.02 (10.17) | 496.43 (9.96) | 4.17*** |
| Alabama test total: age 9 | 1254.71 (62.82) | 1288.68 (75.31) | 3.25** |
| Academic functioning: age 11 | −.12 (1.83) | .17 (1.66) | .78 |
| BIA: age 11 | 503.38 (11.41) | 509.64 (10.43) | 3.98*** |
| Alabama test total: age 11 | 1335.56 (61.63) | 1362.32 (65.82) | 2.43* |
P ≤ .05,
P < .01,
P < .001.
Primary analyses
Relations between race and academic/cognitive outcomes: sleepiness as a pathway of effects
The first model examined the role of sleepiness as a mediator or intervening variable linking race to academic and cognitive performance (Fig. 1). There were several significant effects for the covariates, which are not depicted in the figure for enhanced clarity of primary effects. ADHD status was associated with lower scores on all 3 academic variables at age 9, rs = −.15 to −.24, Ps < .01, and with lower teacher-reported academic functioning, B = −.22, P < .001, and ARMT scores, B = −.10, P = .06, at age 11. Children diagnosed with chronic illnesses had lower BIA scores at age 9, r = −.10, P < .05. Greater sleepiness was related to lower scores on the 3 academic variables at age 9, rs = −.16 to −.21, Ps < .05. AA children had lower scores for the 3 academic variables at age 9, rs = −.26 to −.29, Ps < .001, and more sleep/wake problems, r = .30, p < .001). These paths, in addition to the covariances between the academic variables at age 9, the covariances between sleepiness and each of the other sleep variables, and the residual variances for the academic variables at age 11, were statistically controlled in all models.
Fig. 1.
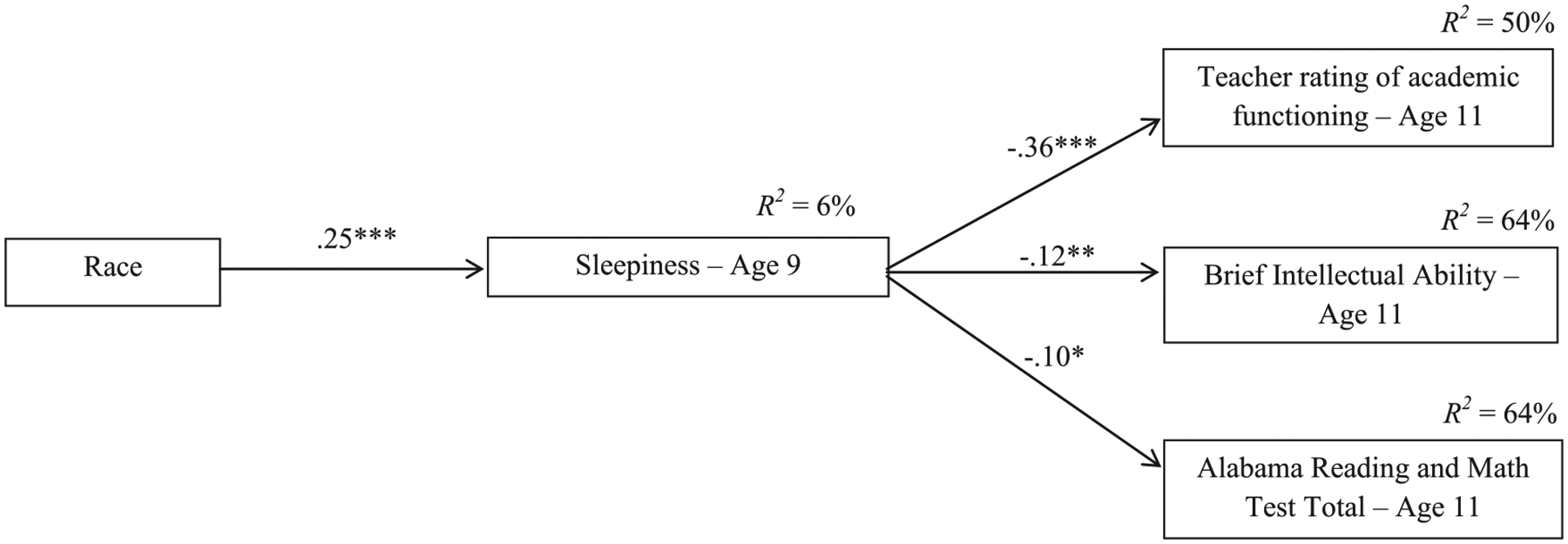
Path model of age 9 sleepiness as an intervening variable linking child race to age 11 academic/cognitive performance. Child sex, zBMI, illness/asthma, ADHD status, sleep duration and quality, and age 9 academic/cognitive performance variables were covaried and allowed to predict the outcome variables. All academic/cognitive outcome variables were entered in the same model and were covaried. R2 values represent the variance accounted for by all predictors and covariates. Covariates and covariances between the outcome variables are not depicted for simplicity. Race was coded as 0 = EA, 1 = AA. Model fit: χ2/df = 3.14, CFI = .91, RMSEA = .08. *P ≤ .05, **P < .01, ***P < .001.
Path modeling analyses testing study hypotheses demonstrated that race was associated with sleepiness such that AAs had higher levels of sleepiness at age 9, P < .001 (Fig. 1). Greater sleepiness was associated with decreases in teacher-reported academic functioning, BIA scores, and ARMT scores from ages 9 to 11, Ps < .05. However, there were no direct relationships between race and the academic variables with or without sleepiness entered into the model (Table 3). Therefore, mediation effects could not exist. To examine the role of sleepiness as an intervening variable, the significance of each of the indirect effects from race to the academic variables via sleepiness was tested using Monte Carlo simulations. Findings indicated significant indirect effects for academic functioning (95% CI −.54 to −.12), BIA scores (95% CI −1.26 to −.13), and ARMT scores (95% CI −7.71 to −.02). The nonsignificant direct associations, but significant indirect effects, suggest that greater sleepiness was an intervening variable connecting lower levels of academic performance to AA children.
Table 3.
Results from direct effects models predicting academic and cognitive performance variables
| Academic functioning: age 11 | BIA: age 11 | Alabama test total: age 11 | |||||
|---|---|---|---|---|---|---|---|
| Variable | B (SE) | β | B (SE) | β | B (SE) | β | |
| Model 1 | |||||||
| Academic functioning: age 9 | .52 (.08) | .58*** | - | - | - | - | |
| BIA: age 9 | - | - | .78 (.05) | .78*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | .65 (.05) | .75*** | |
| ADHD: age 9 | −.96 (.38) | −.20* | - | - | −16.51 (9.69) | −.09ϯ | |
| Race | .03 (.27) | .01 | −1.17 (.99) | −.05 | −6.74 (7.05) | −.05 | |
| R 2 | .42 | .63 | .63 | ||||
| Model 2 | |||||||
| Academic functioning: age 9 | .48 (.08) | .53*** | - | - | - | - | |
| BIA: age 9 | - | - | .78 (.04) | .77*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | .64 (.04) | .74*** | |
| ADHD: age 9 | −.99 (.39) | −.21* | - | - | −16.52 (9.47) | −.09ϯ | |
| SES: age 9 | .18 (.14) | .11 | .80 (.47) | .08ϯ | 4.66 (3.34) | .08 | |
| R 2 | .41 | .63 | .63 | ||||
| Model 3 | |||||||
| Academic functioning: age 9 | .49 (.08) | .55*** | - | - | - | - | |
| BIA: age 9 | - | - | .77 (.05) | .76*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | .64 (.05) | .74*** | |
| ADHD: age 9 | −.99 (.38) | −.21** | - | - | −17.03 (9.64) | −.09ϯ | |
| Race | .23 (.29) | .07 | −.58 (1.06) | −.03 | −4.34 (7.55) | −.03 | |
| SES: age 9 | .22 (.14) | .14 | .76 (.51) | .08 | 4.20 (3.62) | .07 | |
| R 2 | .43 | .63 | .63 | ||||
P < .10,
P ≤ .05,
P < .01,
P < .001.
Relations between SES and academic/cognitive outcomes: sleepiness as pathway of effects
The second model assessed sleepiness as a process variable in the association between SES and academic and cognitive performance (Fig. 2). The same paths involving the covariates in the first model were significant and therefore statistically controlled, in addition to significant paths between lower SES and lower scores for all 3 academic variables at age 9, rs = .25–.30, Ps < .001; lower sleep duration, r = .12, P = .05; and more sleep/wake problems, r = −.20, P < .01.
Fig. 2.
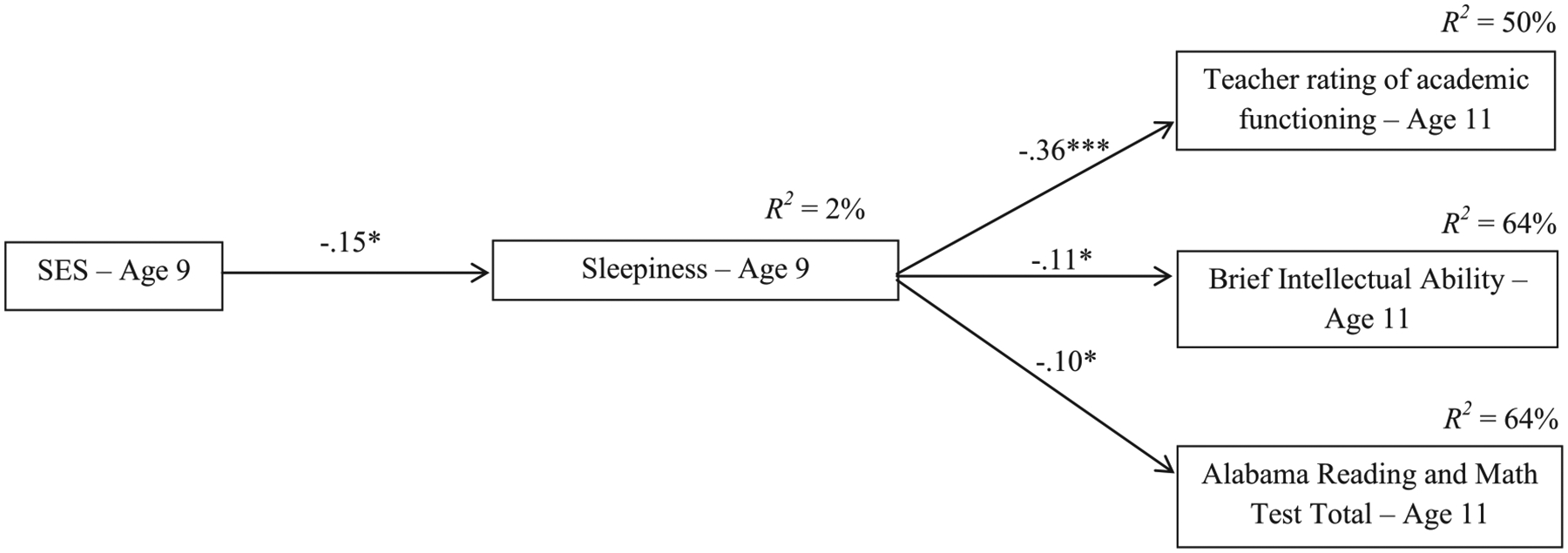
Path model of age 9 sleepiness as an intervening variable linking child SES to age 11 academic/cognitive performance. Child sex, zBMI, illness/asthma, ADHD status, sleep duration and quality, and age 9 academic/cognitive performance variables were covaried and allowed to predict the outcome variables. All academic/cognitive outcome variables were entered in the same model and were covaried. R2 values represent the variance accounted for by all predictors and covariates. Covariates and covariances between the outcome variables are not depicted for simplicity. Of note, although the association between sleepiness and ARMT scores was significant, the indirect effect linking SES to ARMT scores via sleepiness was not. Model fit: χ2/df = 3.00, CFI = .91, RMSEA = .08. *P ≤ .05, ***P < .001.
Regarding study hypotheses, lower SES was associated with greater sleepiness at age 9, P < .05 (Fig. 2). Greater sleepiness in turn predicted decreases in all 3 academic outcomes between ages 9 and 11, Ps ≤ .05. There were no significant direct associations between SES and age 11 academic outcomes regardless of whether sleepiness was entered into the models (Table 3). Thus, mediation effects could not exist. Monte Carlo simulations yielded significant indirect effects for teacher-reported academic functioning (95% CI .01 to .18) and BIA scores (95% CI .01 to .40), but not for ARMT scores. Results indicated that sleepiness was an intervening variable linking lower SES to lower academic functioning and lower cognitive performance.
Race and SES in the same model
In the final model, variables representing race and SES were simultaneously entered as predictors to assess their relative effects on sleepiness and academic outcomes accounting for the other (Fig. 3). All significant paths involving the covariates from the prior models were retained. Findings indicated that the association between SES and sleepiness was no longer significant when race was entered in the model. However, the significant association between race and sleepiness remained, P < .001, as did the relations between greater sleepiness and lower performance on the 3 academic measures, Ps < .05. As in the prior models, neither race nor SES was directly associated with academic outcomes at age 11 (Table 3), and thus, mediation effects were not operative. Monte Carlo simulations showed that the indirect effects linking race to the academic variables were all significant (95% CI −.52 to −.10 for academic functioning, −1.19 to −.11 for BIA scores, and −7.43 to −.02 for ARMT scores). Thus, greater sleepiness operated as an intervening variable in examined associations. Results for all path models are included in Table 4.
Fig. 3.
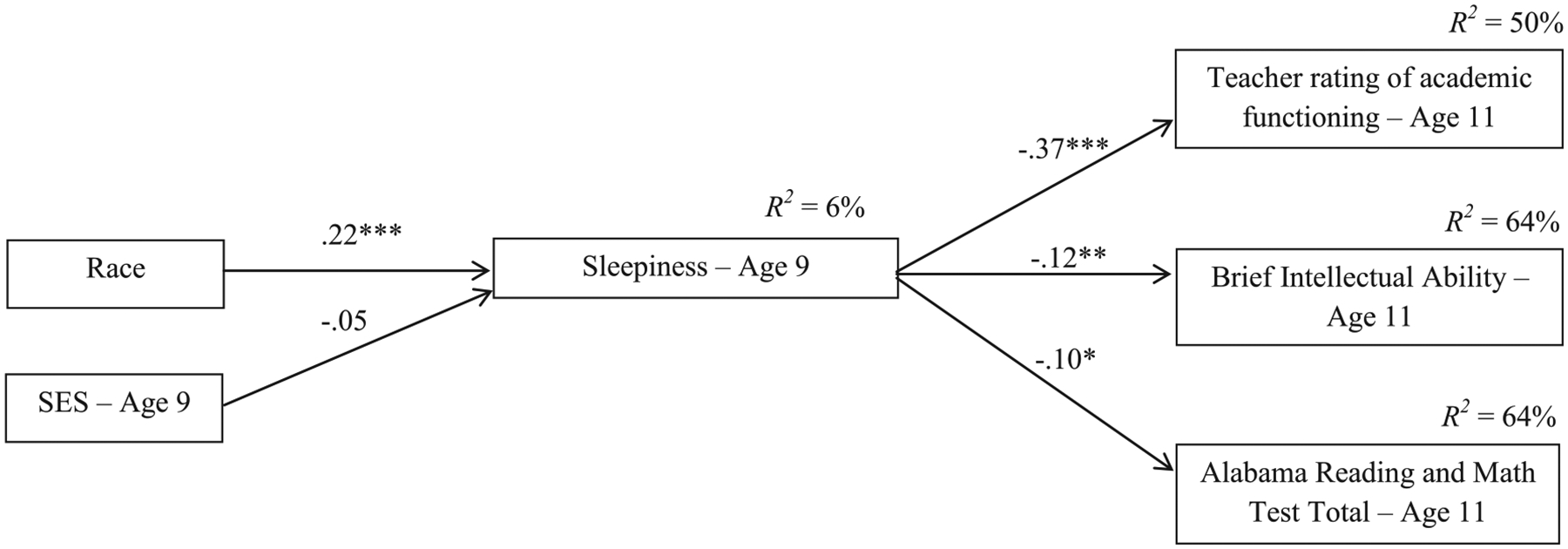
Path model of age 9 sleepiness as an intervening variable linking child race and SES to age 11 academic/cognitive performance. Child sex, zBMI, illness/asthma, ADHD status, sleep duration and quality, and age 9 academic/cognitive performance variables were covaried and allowed to predict the outcome variables. All academic/cognitive outcome variables were entered in the same model and were covaried. R2 values represent the variance accounted for by all predictors and covariates. Covariates and covariances between the outcome variables are not depicted for simplicity. Race was coded as 0 = EA, 1 = AA. Model fit: χ2/df = 2.77, CFI = .91, RMSEA = .07. *P ≤ .05, **P < .01, ***P < .001.
Table 4.
Results from indirect effects models examining sleepiness as an intervening variable linking race/SES to academic and cognitive performance variables
| Sleepiness: age 9 | Academic functioning: age 11 | BIA: age 11 | Alabama test total: age 11 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | B (SE) | β | B (SE) | β | B (SE) | β | B (SE) | β | |
| Model 1 | |||||||||
| Academic functioning: age 9 | - | - | .41 (.07) | .45*** | - | - | - | - | |
| BIA: age 9 | - | - | - | - | .77 (.04) | .76*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | - | - | .64 (.05) | .74*** | |
| ADHD: age 9 | - | - | −1.16 (.36) | −.24** | - | - | −18.20 (9.64) | −.10ϯ | |
| Race | 2.39 (.57) | .25*** | - | - | - | - | - | - | |
| Sleepiness: age 9 | - | - | −.13 (.03) | −.36*** | −.26 (.10) | −.12** | −1.44 (.73) | −.10* | |
| R 2 | .06 | .50 | .64 | .64 | |||||
| Model 2 | |||||||||
| Academic functioning: age 9 | - | - | .41 (.07) | .45*** | - | - | - | - | |
| BIA: age 9 | - | - | - | - | .77 (.05) | .76*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | - | - | .64 (.05) | .74*** | |
| ADHD: age 9 | - | - | −1.15 (.36) | −.24** | - | - | −17.93 (9.58) | −.09ϯ | |
| SES: age 9 | −.65 (.28) | −.15* | - | - | - | - | - | - | |
| Sleepiness: age 9 | - | - | −.13 (.03) | −.36*** | −.26 (.10) | −.11* | −1.43 (.73) | −.10* | |
| R 2 | .02 | .50 | .64 | .64 | |||||
| Model 3 | |||||||||
| Academic functioning: age 9 | - | - | .41 (.07) | .45*** | - | - | - | - | |
| BIA: age 9 | - | - | - | - | .77 (.05) | .76*** | - | - | |
| Alabama test total: age 9 | - | - | - | - | - | - | .64 (.05) | .74*** | |
| ADHD: age 9 | - | - | −1.15 (.36) | −.24** | - | - | −18.08 (9.60) | −.10ϯ | |
| Race | 2.19 (.63) | .23*** | - | - | - | - | - | - | |
| SES: age 9 | −.24 (.30) | −.05 | - | - | - | - | - | - | |
| Sleepiness: age 9 | - | - | −.13 (.03) | −.36*** | −.26 (.10) | −.12* | −1.44 (.73) | −.10* | |
| R 2 | .06 | .50 | .64 | .64 | |||||
P < .10,
P ≤ .05,
P < .01,
P < .001.
Discussion
The present study examined child sleepiness as a pathway of effects contributing to racial and socioeconomic disparities in academic and cognitive performance. AA and lower-SES children reported greater sleepiness at age 9, which predicted decreases in teacher-reported academic functioning, cognitive performance, and state standardized test scores from ages 9 to 11. Sleepiness functioned as a significant intervening variable but not a mediator in these pathways. When both race and SES were entered into the same model, race but not SES remained as a significant predictor of sleepiness. These novel longitudinal findings contribute to a growing literature implicating sleepiness as a pathway of effects in associations between race and SES and developmental outcomes.
Findings are consistent with prior work showing that AA and lower-SES children are at greater risk for insufficient sleep, poor sleep quality, and greater sleepiness1–3 compared to their EA and higher-SES peers, and with research demonstrating a link between sleepiness and lower academic and cognitive performance.4–6 Indicative of the robustness of effects, the covariances between the academic variables were statistically controlled, and therefore, the findings indicate that unique associations exist between greater sleepiness and each of the outcome variables tested. The results were supportive of intervening but not mediating effects. Therefore, sleepiness cannot be conceptualized as an explanatory variable in the relationship between race/SES and change in the outcomes over time. Intervening effects support an unfolding developmental process, however, in which sleepiness connects race/SES and change in academic outcomes.37 Furthermore, initial analyses were supportive of bivariate correlations between lower SES and lower academic and cognitive outcomes, and of differences between AA and EA children on these outcome variables. Thus, it is highly plausible that absence of mediation effects is due to the high stability in the outcome measures over 2 years and the fact that autoregressive effects were included in the models.
Sleepiness significantly predicted the outcomes while statistically controlling for sleep duration and quality, which may suggest that there are individual differences in subjective experiences of sleepiness, even at equivalent levels of sleep duration or quality, that have important implications for academic and cognitive performance. This finding advocates for the assessment of sleepiness, which is scarce in the child development, public health, and pediatric sleep fields.
There are several study limitations and strengths. First, the study was not able to address potential mechanisms linking race and SES to greater sleepiness, which could shed more light on causes of the sleep disparity detected. In prior work with children, more presleep worries and disruptive sleep conditions were intervening variables linking lower SES to poorer quality sleep.1 Race-based stress, such as experiences of discrimination and stereotype threat, may also contribute to poor sleep quality for AA children.38,39 Identifying pathways of effects in observed relations remain open questions for future studies.
Additionally, there was a substantial percentage of missing data for teacher-reported academic functioning at age 11. Our sample was also largely semirural or from small towns with generally low SES. These 2 factors may limit the generalizability of the findings. Furthermore, although the study was longitudinal, the most rigorous testing of indirect effects requires 3 rather than the 2 time points in the current study. The study was strengthened by use of multiple assessments of academic and cognitive outcomes and by discerning unique effects for each outcome while controlling for the others. Other strengths include analyses that controlled for autoregressive effects, which allow for assessing change in cognitive and academic outcomes even in the context of the high stability of child functioning over 2 years. We were also able to examine the unique effects associated with race and SES that are frequently confounded in the literature. Of note, however, the distribution of SES was not equivalent across EA and AA families, which makes comparisons between them more tenuous.
Findings contribute to a growing literature implicating sleep-wake processes as potential mechanisms of risk that impair children’s academic and cognitive performance. The effects were particularly pronounced for AA children, who confront unique stressors that may compromise the duration and quality of their sleep and increase daytime sleepiness. For some children and families, psychoeducation targeting the sleep environment and sleep hygiene may be a useful approach.40
Acknowledgments
We wish to thank our research laboratory staff, particularly Bridget Wingo, for data collection and preparation, as well as the children and parents who participated.
This study was supported by grant R01HL093246 from the National Heart, Lung, and Blood Institute awarded to Mona El-Sheikh. The content is solely the responsibility of the authors and does not necessarily reflect the official views of the National Institutes of Health.
Footnotes
Disclosures
The authors have no conflicts of interest to declare.
In preliminary analyses not reported in the article, we also examined interactions between race and SES as predictors of outcomes, and no significant effects emerged.
References
- 1.Bagley EJ, Kelly RJ, Buckhalt JA, El-Sheikh M. What keeps low-SES children from sleeping well: the role of presleep worries and sleep environment. Sleep Med. 2015;16(4):496–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.El-Sheikh M, Bagley EJ, Keiley M, Elmore-Staton L, Chen E, Buckhalt JA. Economic adversity and children’s sleep problems: multiple indicators and moderation of effects. Health Psychol. 2013;32(8):849–859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jarrin DC, McGrath JJ, Quon EC. Objective and subjective socioeconomic gradients exist for sleep in children and adolescents. Health Psychol. 2014;33(3):301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bub KL, Buckhalt JA, El-Sheikh M. Children’s sleep and cognitive performance: a cross-domain analysis of change over time. Dev Psychol. 2011;47(6):1504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Buckhalt JA, El-Sheikh M, Keller PS, Kelly RJ. Concurrent and longitudinal relations between children’s sleep and cognitive functioning: the moderating role of parent education. Child Dev. 2009;80(3):875–892. [DOI] [PubMed] [Google Scholar]
- 6.Dewald JF, Meijer AM, Oort FJ, Kerkhof GA, Bögels SM. The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: a meta-analytic review. Sleep Med Rev. 2010;14(3):179–189. [DOI] [PubMed] [Google Scholar]
- 7.Lawson GM, Farah MJ. Executive function as a mediator between SES and academic achievement throughout childhood. Int J Behav Dev. 2017;41(1): 94–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Little M Racial and socioeconomic gaps in executive function skills in early elementary school: nationally representative evidence from the ECLS-K: 2011. Educ Res. 2017;46(2):103–109. [Google Scholar]
- 9.Moore PJ, Adler NE, Williams DR, Jackson JS. Socioeconomic status and health: the role of sleep. Psychosom Med. 2002;64(2):337–344. [DOI] [PubMed] [Google Scholar]
- 10.Tomfohr LM, Pung MA, Dimsdale JE. Mediators of the relationship between race and allostatic load in African and white Americans. Health Psychol. 2016;35(4): 322. [DOI] [PubMed] [Google Scholar]
- 11.Moore M, Meltzer LJ. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9(2):114–121. [DOI] [PubMed] [Google Scholar]
- 12.Lo JC, Ong JL, Leong RL, Gooley JJ, Chee MW. Cognitive performance, sleepiness, and mood in partially sleep deprived adolescents: the need for sleep study. Sleep. 2016;39(3):687–698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Roehrs T Daytime sleepiness and alertness. Principles and Practice of Sleep Medicine; 2005. p. 39–50. [Google Scholar]
- 14.Heijden KB, Vermeulen M, Donjacour CE, Gordijn M, Hamburger HL, Meijer AM, et al. Chronic sleep reduction is associated with academic achievement and study concentration in higher education students. J Sleep Res. 2018;27: 165–174. [DOI] [PubMed] [Google Scholar]
- 15.Sadeh A Consequences of sleep loss or sleep disruption in children. Sleep Med Clin. 2007;2(3):513–520. [Google Scholar]
- 16.Hale L, Do DP. Racial differences in self-reports of sleep duration in a populationbased study. Sleep. 2007;30(9):1096–1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Petrov ME, Lichstein KL. Differences in sleep between black and white adults: an update and future directions. Sleep Med. 2016;18:74–81. [DOI] [PubMed] [Google Scholar]
- 18.Chen X, Wang R, Zee P, Lutsey PL, Javaheri S, Alcántara C, et al. Racial/ethnic differences in sleep disturbances: the Multi-Ethnic Study of Atherosclerosis (MESA). Sleep. 2015;38(6):877–888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bøe T, Hysing M, Stormark KM, Lundervold AJ, Sivertsen B. Sleep problems as a mediator of the association between parental education levels, perceived family economy and poor mental health in children. J Psychosom Res. 2012;73(6): 430–436. [DOI] [PubMed] [Google Scholar]
- 20.Commerce USDo. How the Census Bureau measures poverty. Available from: https://www.census.gov/topics/income-poverty/poverty/guidance/povertymeasures.html; 2016.
- 21.Wolfson AR, Carskadon MA. Sleep schedules and daytime functioning in adolescents. Child Dev. 1998;69(4):875–887. [PubMed] [Google Scholar]
- 22.Lachar D, Wingenfeld S, Kline R, Gruber C. Student Behavior Survey (SBS) Manual. Los Angeles: Western Psychological Services; 2000. [Google Scholar]
- 23.El-Sheikh M, Buckhalt JA, Cummings EM, Keller PS. Sleep disruptions and emotional insecurity are pathways of risk for children. J Child Psychol Psychiatry. 2007;48(1):88–96. [DOI] [PubMed] [Google Scholar]
- 24.McGrew KS, Woodcock RW. Woodcock Johnson III Technical Manual. Itasca, IL: Riverside Publishing Company; 2001. [Google Scholar]
- 25.Woodcock RW, McGrew KS, Mather M. Woodcock-Johnson III Tests of Cognitive Abilities. New York, NY: Riverside; 2001. [Google Scholar]
- 26.Rasch G Studies in Mathematical Psychology: I. Probabilistic Models for Some Intelligence and Attainment Tests. Oxford, England: Nielsen & Lydiche; 1960. [Google Scholar]
- 27.Jaffe LE. Development, Interpretation, and Application of the W Score and the Relative Proficiency Index (Woodcock-Johnson III Assessment Service Bulletin No.11). Rolling Meadows, IL: Riverside; 2009. [Google Scholar]
- 28.Prevention CfDCa. Body mass index (BMI) percentile calculator for child and teen. Available from: http://nccd.cdc.gov/dnpabmi/Calculator.aspx; 2014.
- 29.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173. [DOI] [PubMed] [Google Scholar]
- 30.MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Preacher KJ, Selig JP. Advantages of Monte Carlo confidence intervals for indirect effects. Commun Methods Measures. 2012;6(2):77–98. [Google Scholar]
- 32.Selig JP, Preacher KJ. Monte Carlo Method for Assessing Mediation: An Interactive Tool for Creating Confidence Intervals for Indirect Effects [Computer Software]; 2008. [Google Scholar]
- 33.Cole DA, Maxwell SE. Testing mediational models with longitudinal data: questions and tips in the use of structural equation modeling. J Abnorm Psychol. 2003;112(4):558. [DOI] [PubMed] [Google Scholar]
- 34.Browne MW, Cudeck R. Alternative ways of assessing model fit. Sage focus; editions, 154.; 1993. (136-). [Google Scholar]
- 35.Enders CK, Bandalos DL. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Struct Equ Model. 2001;8(3):430–457. [Google Scholar]
- 36.Muthén LK, Muthén BO. Mplus Version 7 User’s Guide. Los Angeles, CA: Muthén & Muthén; 2012. [Google Scholar]
- 37.Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7(4):422. [PubMed] [Google Scholar]
- 38.Heissel JA, Levy DJ, Adam EK. Stress, sleep, and performance on standardized tests: understudied pathways to the achievement gap. AERA Open. 2017;3(3) (2332858417713488). [Google Scholar]
- 39.Levy DJ, Heissel JA, Richeson JA, Adam EK. Psychological and biological responses to race-based social stress as pathways to disparities in educational outcomes. Am Psychol. 2016;71(6):455–473. [DOI] [PubMed] [Google Scholar]
- 40.Mindell JA, Kuhn B, Lewin DS, Meltzer LJ, Sadeh A. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep. 2006;29(10):1263–1276. [PubMed] [Google Scholar]