

Abstract
BACKGROUND:
In Saudi Arabia, there is not much research on the risk of eating disorders and the influence of sociocultural factors on increasing the risk among university students. The objective of this study was to assess the prevalence of the risk of eating disorder (EDs) in King Abdulaziz University students, the influence of sociocultural factors, and any differences between males and females.
MATERIALS AND METHODS:
A cross-sectional study was conducted on 763 university students in Jeddah, Saudi Arabia. The data were collected in 3 months from February 2021 to April 2021. A self-administered Eating Attitude Test-26 scale was used to assess the risk of eating disorder among the students. The sociocultural attitude toward appearance questionnaire was used to measure the internalization of thinness, masculinity, and family, peer, and media attitude toward appearance. To test for statistical significance, t-test was used for continuous variables, whereas Ch-square test was performed for categorical variables. Logistic regression analysis were performed to determine factors associated with ED risk; all tests were performed at 0.05 significance level.
RESULTS:
The prevalence of the risk of eating disorder among the students was observed as 34%. The sociocultural attitude toward appearance was significantly higher among at risk of eating disorder students. The multiple logistic regression analysis showed that females are twice more likely to be at risk for eating disorder than males (2.25) with 95% confidence interval (1.50,3.39). Peer influence was significantly higher among males than females; however, females were significantly more influenced by the media than males.
CONCLUSION:
The prevalence of eating disorder risk in Saudi university students in Jeddah was observed as alarming and highly influenced by sociocultural factors; therefore, screening university students for eating disorder is very necessary. In addition, there should be media and health promotion campaigns on eating disorder and body image issues.
Keywords: Body mass index, eating disorder risk, Saudi Arabia, sociocultural factors, university students
Introduction
The prevalence of eating disorders (ED) as documented has continuously risen in recent years.[1] According to the American Psychiatric Association, ED can be defined as an interrupted eating pattern, which can be associated with an obsession with body image and weight resulting in serious health issues.[2] ED is a general term for several diseases such as anorexia nervosa, bulimia nervosa, and binge eating.[3] Individuals with ED have significantly lower health-related quality of life than individuals without ED. In the United States, it is estimated that 3.3 million healthy life years are lost yearly as a result of ED.[4,5] In Saudi Arabia, a study done in 2018 reported that 35% of female university students in Taif were at risk of ED.[6] This is considered extremely high compared with such western countries as the United States, where ED risk was reported as 11.6% and 5.7% among female and male university students, respectively.[7] Moreover, sociocultural factors, a determinant of health can be described as the environment surrounding individuals, such as the family, relatives, and friends, that is likely to influence one's way of thinking, from a very early age.[8,9] These sociocultural factors vary according to the society in which one lives. Factors such as family, peers, and media attitudes toward appearance could influence the risk of developing ED. These factors are more prevalent in societies where culture plays an important role.[10]
Compared with such western countries as the United States of America, Saudi Arabia is seen to have a high prevalence of ED risk among female university students. However, there is little research on the prevalence of ED risk in university students in Jeddah, especially among male students, and how the risk of ED is influenced by the sociocultural attitude toward appearance. Therefore, the objective of this study was to determine (i) the prevalence of the risk of ED risk in King Abdulaziz University students (Jeddah, Saudi Arabia), (ii) the influence of sociocultural factors on the ED risk, and (iii) the difference between the risk in males and females with regard to the influence of sociocultural factors.
Materials and Methods
A cross-sectional study was conducted on 763 university students in Jeddah, Saudi Arabia from February to April 2021. Ethical approval was obtained from the Institutional Review Board letter No. 86–21 dated 17/02/2021 and informed written consent was taken from all participants.
Sample size was calculated using the following formula  , with a confidence interval of 95% and precision of 4, the proportion of ED risk in university students was taken from a previous study conducted in Taif, Saudi Arabia (35.4%).[6] The final sample size was calculated as 549. As a control for low response and missing data, the sample size was increased by 30%, resulting in a total sample size of 713.
, with a confidence interval of 95% and precision of 4, the proportion of ED risk in university students was taken from a previous study conducted in Taif, Saudi Arabia (35.4%).[6] The final sample size was calculated as 549. As a control for low response and missing data, the sample size was increased by 30%, resulting in a total sample size of 713.
Multistage sampling was used to recruit participants. First, the university colleges were grouped into two strata: females and males, with an equal allocation of colleges in each stratum. Thereafter, cluster sampling was used in which five colleges were chosen from each stratum randomly. Finally, an academic year was randomly selected from each college, and all students in the selected year were included in the study. For the male strata, the following disciplines were included randomly: medicine, dentistry, Islamic law and studies, information technology, and science track of the preparatory year. For the female strata, the following disciplines were randomly included: medicine, nursing, computer science, psychology, and preparatory year of the administrative track.
Data collection was done using a self-administered questionnaire consisting of three sections as follows: first section had sociodemographic factors as age, marital status, gender, university year and college, height (m) and weight (kg), smoking, household income, mothers' and fathers' education level, any chronic condition, and type of diet followed. The Body Mass Index (BMI) was calculated through the self-reported height and weight, which was measured by weight (kg)/height (m2). The BMI classification was categorized as underweight (BMI <18.5), normal (18.5 ≤25), overweight (25 ≤30), and obese (BMI of 30 or more).
The second section consisted of the Eating Attitudes Test (EAT)-26 self-assessment scale that assessed persons who are at risk for ED. This questionnaire was developed first by Garner and Garfinkel in 1979 and has since been used in multiple studies to determine the risk for ED, where it shows a high validity and reliability. The questionnaire measured two variables: ED risk and risky eating behavior. The questionnaire had a scoring system for the ED risk part which can be calculated as follows: for questions 1–25, “always” count as 3, “usually,” count as 2, and “often” count as 1. For “rarely,” “sometimes,” or “never,” it counts as 0. For question 26, “always,” “usually,” or “often,” count as 0, “sometimes,” count as 1, “rarely,” count as 2, and “never” count as 3. The participant is considered at risk of ED if their score is more than 20, the second part of the questionnaire is risky behavior in the past 6 months, behavior is considered binge risky behavior if the participants reports binge eating 2-3 times a week or more, inducing vomiting and laxative risky behavior if reported once a month or less, and for excessive exercise if it is reported as more than 60 minutes a day.[11]
The third section included the sociocultural attitudes toward appearance questionnaire (SATAQ-4). The first form of the questionnaire was developed in 1995 by Heinberg and Thompson. In 2015, the last version of this questionnaire updated and validated by Schaefer, showed a high convergent validity and reliability, with a Cronbach's alpha of 0.8. The questionnaire had five subscales: (i) self-pressure to internalization of thinness, (ii) internalization to masculinity, (iii) family pressure, (iv) peer pressure, and (v) media pressure. Furthermore, with 22 items, each item had a 5-point Likert scale, from strongly disagree to strongly agree, the higher the score, the higher the sociocultural influence. The highest possible score was 110 for the overall scale, while for each subscale, the highest score for internalized thinness was 25, internalized masculinity 25, family pressure 20, peer pressure 20, and media pressure 20.[12,13]
The Arabic version of the EAT-26 and SATAQ-4 of this questionnaire was used here, as it had been used in a previous study and been translated from English to Arabic and vice versa by two certified translators.[14]
The self-administered questionnaire was sent to the students in the study by phone on the number obtained from the students' leaders of each batch.
Continuous data such as sociodemographic factors were presented as mean, standard deviation (±SD), while categorical variables were represented as frequency and percentages. Furthermore, the unadjusted analysis for categorical variables was performed using Pearson's Chi-squared two-way analysis. Student's t-test was used to assess the unadjusted significant difference between the SATAQ-4 subscale and ED risk. For the adjusted analysis, the multiple logistic regression model was built to predict the factors associated with ED risk as its dependent binary variable. To check the logistic regression assumption, data were checked for multicollinearity to make sure that the data were not correlated. All data were tested for normality before the conduct of the t-test and found to be normally distributed. The data were considered statistically significant at a P < 0.05 and a confidence interval of 95%. The statistical analysis was done using the STATA 13.0 software program.
Results
After excluding incomplete questionnaires, the total number of participants was 763, with a mean age of 21 (1.82). Table 1 represents the sociodemographic and the characteristics of the sample. As shown in Table 1, approximately 34% of the students scored more than 20 on the EAT-26 scale and were considered at risk for ED.
Table 1.
Sociodemographic characteristics of participants and eating disorders risk (2021)
| Characteristics | Frequency N (%) | Total |
|---|---|---|
| ED risk | ||
| At risk | 260 (34.1) | 763 |
| Not at risk | 503 (65.9) | |
| Gender | ||
| Female | 443 (58.1) | 763 |
| Male | 320 (41.9) | |
| Status | ||
| Single | 737 (97.1) | 759 |
| Married | 22 (2.9) | |
| Year in university | ||
| First year | 181 (23.7) | 762 |
| Second year | 127 (16.7) | |
| Third year | 220 (28.9) | |
| Fourth year | 151 (19.8) | |
| <4 years | 83 (10.9) | |
| Mother’s education | ||
| Illiterate | 40 (5.2) | 759 |
| Primary | 71 (9.3) | |
| Middle | 101 (13.3) | |
| High school | 175 (23.1) | |
| University and postgraduate | 372 (49.0) | |
| Father’s education | ||
| Illiterate | 15 (1.9) | 760 |
| Primary | 43 (5.7) | |
| Middle | 95 (12. 5) | |
| High school | 206 (27.1) | |
| University and postgraduate | 401 (52.8) | |
| Family income (SAR) | ||
| <5000 | 88 (11.6) | 758 |
| 5000-10,000 | 194 (25.6) | |
| 10,001-15,000 | 176 (23.2) | |
| >15,000 | 300 (39.6) | |
| Smoke | ||
| No | 620 (81.3) | 763 |
| Yes | 143 (18.7) | |
| History | ||
| Asthma | 32 (4.2) | 763 |
| Mental disease | 5 (0.7) | |
| Diabetes | 4 (0.5) | |
| Other | 30 (3.9) | |
| None | 692 (90.7) | |
| Diet followed | ||
| Vegetarian or vegan | 24 (3.1) | 771 |
| Intermittent fasting | 72 (9.3) | |
| Calorie’s deficit | 24 (3.1) | |
| Other (ex: Cutting sugar, one meal a day) | 47 (6.1) | |
| Not specific diet | 604 (78.3) | |
| BMI | ||
| Underweight | 130 (19.2) | 676 |
| Normal weight | 303 (44.8) | |
| Overweight | 148 (21.9) | |
| Obese | 95 (14.0) |
BMI=Body mass index, ED=Eating disorders
Figure 1 illustrates the ED risk of students' years attended in the university, students in their 2nd year of university showed the highest prevalence of ED risk, as around 39% of the students were at risk of ED. In addition, 34.2% of students in their 1st year of university were at risk of ED. Students who had spent more than 4 years in the university had the least prevalence of ED risk (30.1%).
Figure 1.
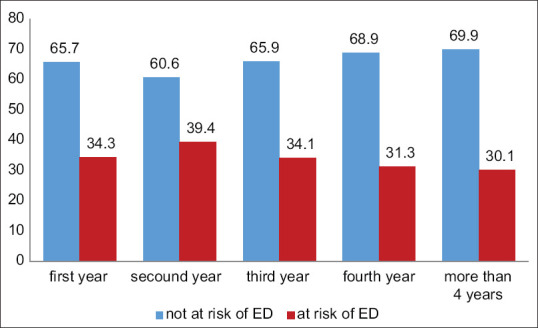
Eating disorder risk in different college years (2021)
Table 2 shows the mean difference of ED risk in relation to SATAQ-4. As shown in the table, internalization to thinness, internalization to masculinity, family pressure, peer pressure, and media pressure were all significantly higher among at risk of ED students (P < 0.05). Moreover, internalization of thinness showed a higher magnitude difference between students at risk (M = 19.38, SD ± 4.04) and students who were not (M = 16.12 SD ± 3.82). Furthermore, internalization of masculinity showed a high difference between students at risk (M = 18.96 ± 4.05) and those who were not (M = 16.51, ±3.93). On the other hand, the influence of peer attitude toward appearance on ED risk had the least magnitude of difference.
Table 2.
The association between sociocultural attitude toward appearance subscales with eating disorder risk (2021)
| SATA subscales | ED risk | N | Subscale score Mean±SD | t | P-value |
|---|---|---|---|---|---|
| Internalization of thinness | Not at risk | 503 | 16.12±3.82 | −10.96 | < 0.001 |
| At risk | 260 | 19.38±4.04 | |||
| Internalization of masculinity | Not at risk | 503 | 16.51±3.93 | −8.07 | < 0.001 |
| At risk | 260 | 18.96±4.05 | |||
| Family attitude toward appearance | Not at risk | 503 | 11.17±4.01 | −5.46 | < 0.001 |
| At risk | 260 | 12.87±4.16 | |||
| Peer attitude toward appearance | Not at risk | 503 | 9.48±4.12 | −4.87 | < 0.001 |
| At risk | 260 | 11.09±4.67 | |||
| Media attitude toward appearance | Not at risk | 503 | 9.90±5.06 | −6.8 | < 0.001 |
| At risk | 260 | 12.70±5.85 | |||
| Total SATAQ-4 | Not risk | 503 | 63.20±14.03 | −10.77 | < 0.001 |
| At risk | 260 | 75.02±14.96 |
Data are significant at P-level<0.05. Student’s independent t-test as a measure of association. ED=Eating disorders, SATA=Sociocultural attitude toward appearance, SATAQ-4=SATA questionnaire, SD=Standard deviation
Table 3 shows the significant difference between male and female students regarding risk for ED. Female students had a higher prevalence of ED risk than male students, with 38.8% of females compared to 27.5% of male students (P < 0.05, χ2 : 10.60). Even though male students had a higher prevalence of binge eating behavior than females (37% and 32%, respectively), no significant difference was observed (P = 0.159). There was a significant difference in induced vomiting behavior between male and female students (P < 0.05, χ2 : 12.80), with a higher prevalence of 11.3% in female students compared to 4% in male students. Furthermore, a significant difference (P < 0.05, χ2 : 4.71) was also observed in the use of laxatives between male and female students, with a higher prevalence in females than males.
Table 3.
The difference between male and female students regarding eating disorders risk and risky behavior (2021)
| Male (n=320) N (%) | Female (n=443) N (%)a | χ 2 | P-value | |
|---|---|---|---|---|
| ED risk | ||||
| At risk | 88 (27.5) | 172 (38.8) | 10.60 | 0.001 |
| Not at risk | 232 (72.5) | 271 (61.1) | ||
| Binge eating behavior | ||||
| Risky | 119 (37.2) | 143 (32.3) | 1.98 | 0.159 |
| Not risky | 201 (62.8) | 300 (67.7) | ||
| Induced vomiting behavior | ||||
| Risky | 13 (4.0) | 50 (11.3) | 12.80 | < 0.001 |
| Not risky | 307 (95.9) | 393 (88.7) | ||
| Laxative use | ||||
| Risky | 19 (5.9) | 46 (10.4) | 4.71 | 0.030 |
| Not risky | 301 (94.0) | 397 (89.6) | ||
| Risky exercise behavior | ||||
| Risky | 16 (5.0) | 26 (5.9) | 0.26 | 0.603 |
| Not risky | 304 (95.0) | 417 (94.1) |
Data are significant at P-level<0.05. Pearson’s Chi-square as a measure of association. ED=Eating disorders
Table 4 displays the difference between male and female students regarding the risk for ED at the subscales of SATAQ-4. The internalized thinness showed that female students at risk were significantly (P < 0.05) more internalized than male students at risk ([females: M = 19.80, SD ± 3.85]; [males: M = 18.56, SD ± 4.28; t-value = −2.34]).
Table 4.
The difference between male and female students at risk of eating disorder on sociocultural attitude toward appearance subscales (2021)
| SATAQ-4 subscales | Gender at risk for ED | n | Mean±SD | t | P-value |
|---|---|---|---|---|---|
| Internalization of thinness | Male at risk | 88 | 18.56±4.28 | −2.34 | 0.019 |
| Female at risk | 172 | 19.80±3.85 | |||
| Internalization of masculinity | Male at risk | 88 | 19.48±4.06 | 1.50 | 0.133 |
| Female at risk | 172 | 18.69±4.02 | |||
| Family attitude toward appearance | Male at risk | 88 | 13.34±4.08 | 1.28 | 0.199 |
| Female at risk | 172 | 12.63±4.19 | |||
| Peer attitude toward appearance | Male at risk | 88 | 12.19±4.33 | 2.74 | 0.006 |
| Female at risk | 172 | 10.53±4.74 | |||
| Media attitude toward appearance | Male at risk | 88 | 11.27±5.73 | −2.95 | 0.003 |
| Female at risk | 172 | 13.45±5.78 | |||
| Total SATAQ-4 | Male at risk | 88 | 74.81±14.67 | −0.15 | 0.870 |
| Female at risk | 172 | 75.12±15.15 |
Data are significant at P-level<0.05. Student’s independent t-test as a measure of association. SD=Standard deviation, SATAQ-4=Sociocultural attitudes toward appearance questionnaire, ED=Eating disorders
On the other hand, internalization of masculinity among males showed a higher mean than female students (M = 19.48 SD ± 4.06 and M = 18.69 SD ± 4.02, respectively), with a t-value of 1.50; yet no significant difference was observed.
Furthermore, even though male students had a higher mean of family influence on the risk of ED with a t-value of 1.28, no significant difference was observed.
Peer attitude appeared to be significantly different between male and female students at risk (P < 0.05), as males showed a higher mean value (M = 12.19, SD ± 4.33) than females (M = 10.53, SD ± 4.74) with a t-value of 2.74. In contrast, the influence of media attitude was higher in females than males with a t-value of −2.95, and significant difference (P < 0.05), the overall score of SATAQ-4 showed no significant difference.
To identify independent factors that predict ED risk, multiple logistic regressions were conducted. BMI, excessive exercise, and gender variables were presented as categorical variables, while SATAQ-4 total was presented as a continuous variable. As shown in Table 5, female students were significantly twice more likely to have ED risk than male students (odds ratio [OR] = 2.25, 95% confidence interval [CI] = 1.50,3.39) after the adjustment for other variables. “Excessive exercise for more than 60 min” showed a significant trend in its categories (P < 0.05) compared to the reference group that never exercised (P < 0.05). For the BMI, students who were obese were significantly more likely to have ED risk (OR = 2.25, 95% CI = 1.28, 3.95) than the reference group (normal weight students).
Table 5.
Multiple logistic regression analysis for association between eating disorder risk and various risk factors (2021)
| Risk factor | Coefficient | Odds ratio (OR) | SE† | 95% CI for OR | P-value |
|---|---|---|---|---|---|
| Exercise >60 min§ | |||||
| Never | - | 1.00 | - | - | - |
| From once a week to 2-3 times a month | 0.73 | 2.09 | 0.46 | 1.34-3.24 | 0.001 |
| 2-6 times a week | 1.28 | 3.62 | 0.92 | 2.20-5.96 | < 0.001 |
| Once a day or more | 1.95 | 7.03 | 2.86 | 3.17-15.62 | < 0.001 |
| Gender | |||||
| Male | - | 1.00 | - | - | - |
| Female | 0.81 | 2.25 | 0.46 | 1.50-3.39 | < 0.001 |
| BMI | |||||
| Normal weight | - | 1.00 | - | - | - |
| Underweight | 0.23 | 1.26 | 0.34 | 0.73-2.16 | 0.400 |
| Overweight | 0.38 | 1.46 | 0.35 | 0.91-2.35 | 0.115 |
| Obese | 0.81 | 2.25 | 0.64 | 1.28-3.95 | 0.004 |
| SATAQ-4 total** | 0.048 | 1.05 | 0.007 | 1.03-1.06 | < 0.001 |
*Adjusted odds ratio, **Continuous variable, †SE of coefficient, ‡95% CI of the OR, §Trend test shows a significant P of<0.001. Logistic regression analysis. Hosmer–Lemeshow goodness of fit=0.5481, ROC=0.7751, R2=0.1911. SATAQ-4=Sociocultural attitudes toward appearance questionnaire, OR=Odds ratio, CI=Confidence interval, OR=Odds ratio, SE=Standard error, BMI=Body mass index, ED=Eating disorders, ROC=Receiver operating characteristic curve
Moreover, when the SATAQ-4 total score increased by one score, the odd of students to be at risk of ED will increase by 5% (OR = 1.05, 95% CI = 1.03, 1.06).
Discussion
This study aimed at assessing the prevalence of ED risk of King Abdulaziz University students, in addition to the relationship between ED risk and sociocultural attitude toward appearance, as well as the difference between male and female students at risk.
This study indicates that around 34% of the students scored more than 20 on the EAT-26 scale and were at risk of ED. Similarly, a study conducted in Taif, Saudi Arabia, using the EAT-26 scale found that around 35.4% of female university students were at risk of ED.[6] This might be because Taif and Jeddah are in the same region of Saudi Arabia, unlike another study in Dammam, which showed a slightly lower ED risk prevalence of 30% in female university students.[14] This might indicate that university students in the western region of Saudi Arabia may have a higher prevalence of ED risk than those in the eastern region. This can be explained by the fact that the cultures of the two regions differ and therefore contribute uniquely to the increased prevalence of ED risk.
Furthermore, when compared with other countries using the same EAT-26 scale, a study conducted in the United States (2018) showed that 10.5% of university students were at risk of ED.[15] Another study in China conducted in 2015 showed that 4.5% of the students were at risk,[16] which is surprising, since for years western countries have had a much higher prevalence than nonwestern countries. However, in the last few years, Saudi Arabia has faced rapid economic and cultural changes which might have had an impact on the emerging issue of EDs risk in the Saudi society.
For the relationship between SATAQ-4 and ED risk, internalized thinness and masculinity, family pressure, peer pressure, and media pressure scores were all highly significantly higher among at risk students. When compared with other studies conducted in the United States (2018) between at-risk students and students not at risk, Internalization for ideal body, family and peer pressures were considered risk factors among male students. In addition, they reported a significant difference between at risk female and male in the pressure scale, with at risk female having a higher score in family and peer pressure compared to at risk male.[15] This result shows that Saudi university students are under a great deal of pressure to look a particular way by family, peers, and media, thus resulting in the high prevalence of ED risk. Moreover, females were significantly more influenced by the media than male students. This shows that the media such as magazines and TV are either mainly focused on the female image or that male students do not feel influenced by the media. In contrast, males at risk were highly more pressured by their peers than females.
In this study, it was found that excessive exercise was associated with increased risk of ED, as the logistic regression showed a significant trend in the exercise categories. Moreover, it had been previously reported that excessive exercise was associated with an increased risk of ED, as shown in a study conducted in 2018 of 335 females, in which 226 females were diagnosed with anorexia or bulimic nervosa as against 109 healthy females. It found that even though both groups reported that they exercised, a significant difference was observed in all the groups regarding self-reported exercising, as anorexia and bulimic patients reported a higher number of hours per week of exercising with mean hours ranging from 5.95 for anorexic patients and 6.24 for bulimic patients, while healthy females had mean hours of 3.60 of exercise per week.[17]
This study has several strengths. To the best of our knowledge, it is the first such study conducted in Jeddah of university students to assess the risk of ED and the risk of male students. Furthermore, the sample size was considerably good, as more than 700 university students were included in this study. This study also has several limitations. First, the questionnaires were sent to the students by means of messages, making it more likely to be filled out several times. However, to counteract this, any repeated answers were removed to eliminate errors in the result.
Owing to the considerable number of students in the preparatory year, it was challenging to choose the classes randomly, so the choice of the preparatory year classes using convenience sampling. Finally, the results cannot be generalized as this study was conducted in only one university in Jeddah.
Conclusion
The prevalence of ED risk among King Abdulaziz University students is 34%, with a higher prevalence in females than males. Besides, sociocultural attitudes toward appearance were highly significant with the risk of ED.
Therefore, young adults should be taught from an early age the habits of eating healthy rather than focusing on being skinny. In addition, the society should be educated on EDs, especially in university students. The Saudi Ministry of Health has a great presence on social media, so developing a campaign to reach a wide range of people in the media is needed. Risky behaviors such as the use of laxatives and induced vomiting were found to be high among the students. This warrants a need for mandatory supervision of students who engage in such a behavior and screening for risky behavior and EDs in vulnerable students. A university clinic to support students in need of help should also be provided. Furthermore, ED which for years had been considered a nonexistent health issue is still a relatively new topic in the Saudi population. The Saudi society and healthcare officials need to focus more on ED. More research on ED risk in other parts of Saudi Arabia, as well as among obese people and those who exercise excessively is recommended since this study shows that excessive exercise increases the risk. Studies in settings such as gyms are also much needed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Galmiche M, Déchelotte P, Lambert G, Tavolacci MP. Prevalence of eating disorders over the 2000-2018 period: A systematic literature review. Am J Clin Nutr. 2019;109:1402–13. doi: 10.1093/ajcn/nqy342. [DOI] [PubMed] [Google Scholar]
- 2.Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013. American Psychiatric Association. [Google Scholar]
- 3.Zam W, Saijari R, Sijari Z. Overview on eating disorders. Prog Nutr. 2018;20:29–35. [Google Scholar]
- 4.van Hoeken D, Hoek HW. Review of the burden of eating disorders: Mortality, disability, costs, quality of life, and family burden. Curr Opin Psychiatry. 2020;33:521–7. doi: 10.1097/YCO.0000000000000641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Winkler LA, Christiansen E, Lichtenstein MB, Hansen NB, Bilenberg N, Støving RK. Quality of life in eating disorders: A meta-analysis. Psychiatry Res. 2014;219:1–9. doi: 10.1016/j.psychres.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 6.Taha AA, Abu-Zaid HA, Desouky DE. Eating disorders among female students of Taif University, Saudi Arabia, Arch Iran Med. 2018;21:111–7. [PubMed] [Google Scholar]
- 7.Yu Z, Indelicato NA, Fuglestad P, Tan M, Bane L, Stice C. Sex differences in disordered eating and food addiction among college students. Appetite. 2018;129:12–8. doi: 10.1016/j.appet.2018.06.028. [DOI] [PubMed] [Google Scholar]
- 8.Chin V, Noor NM. Sociocultural determinants of health and illness: A theoretical inquiry. Geogr Malays J Soc Spece. 2014;10:49–59. [Google Scholar]
- 9.Marginson S, Dang TK. Vygotsky's sociocultural theory in the context of globalization. Asia Pac J Educ. 2017;37:116–29. [Google Scholar]
- 10.Ata RN, Schaefer LM, Thompson JK. Sociocultural theories of eating disorders. In: The Wiley Handbook of Eating Disorders, Assessment, Prevention, Treatment, Policy, and Future Directions. United states: John Wiley & Sons, Ltd; 2015. pp. 269–82. [Google Scholar]
- 11.Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes test: Psychometric features and clinical correlates. Psychol Med. 1982;12:871–8. doi: 10.1017/s0033291700049163. [DOI] [PubMed] [Google Scholar]
- 12.Schaefer LM, Harriger JA, Heinberg LJ, Soderberg T, Kevin Thompson J. Development and validation of the sociocultural attitudes towards appearance questionnaire-4-revised (SATAQ-4R) Int J Eat Disord. 2017;50:104–17. doi: 10.1002/eat.22590. [DOI] [PubMed] [Google Scholar]
- 13.Heinberg LJ, Thompson JK, Stormer S. Development and validation of the Sociocultural Attitudes Towards Appearance Questionnaire. Int J Eat Disord. 1995;17:81–9. doi: 10.1002/1098-108x(199501)17:1<81::aid-eat2260170111>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 14.Alwosaifer AM, Alawadh SA, Abdel Wahab MM, Boubshait LA, Almutairi BA. Eating disorders and associated risk factors among Imam Abdulrahman Bin Faisal university preparatory year female students in Kingdom of Saudi Arabia. Saudi Med J. 2018;39:910–21. doi: 10.15537/smj.2018.9.23314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Turel T, Jameson M, Gitimu P, Rowlands Z, Mincher J, Pohle-Krauza R. Disordered eating: Influence of body image, sociocultural attitudes, appearance anxiety and depression – A focus on college males and a gender comparison. Cogent Psychol. 2018;5:1–22. [Google Scholar]
- 16.Yu J, Lu M, Tian L, Lu W, Meng F, Chen C, et al. Prevalence of disordered eating attitudes among university students in Wuhu, China. Nutr Hosp. 2015;32:1752–7. doi: 10.3305/nh.2015.32.4.9187. [DOI] [PubMed] [Google Scholar]
- 17.Schlegl S, Dittmer N, Hoffmann S, Voderholzer U. Self-reported quantity, compulsiveness and motives of exercise in patients with eating disorders and healthy controls: Differences and similarities. J Eat Disord. 2018;6:17. doi: 10.1186/s40337-018-0202-6. [DOI] [PMC free article] [PubMed] [Google Scholar]