

Abstract
BACKGROUND
Evidence regarding the effectiveness of using orthotics in improving comfort, increasing running speed and helping to reduce injury rate during running is limited and mixed. Alongside the increasing popularity of running is the increasing rate of running-related injuries (RRIs). Further research into whether orthotics could be used to help reduce RRIs would be highly beneficial for those affected. Additionally, there is a need to clarify whether orthotics use increases comfort during running and helps improve running speed.
AIM
To investigate whether running with Aetrex Orthotics improves comfort and performance and reduces injury whilst running.
METHODS
Runners were recruited on a voluntary basis if they were 18 or older with no serious health conditions, ongoing foot pain or deformity, previous foot surgery in their lifetime or any surgery in the past 6 mo. Participants were randomly assigned to either an intervention group or a control group. All participants were asked to complete runs and provide quantitative data regarding comfort during running, running time and distance, and any RRIs over an 8-wk study period. Participants in the intervention group ran with Aetrex L700 Speed Orthotics, whilst participants in the control group ran without orthotics. Other than the addition of orthotics for participants in the intervention group, all participants were asked to run as they usually would. This report presents preliminary data from the first 47 participants recruited for this study. Running speed was calculated from running distance and time and given in miles per hour. For each outcome variable, the mean for each group, effect size and 95% confidence interval were calculated, and a t-test was performed to determine if between-group differences were statistically significant.
RESULTS
Data for all three primary outcomes was provided from a total of 254 runs by the 23 participants in the intervention group and a total of 289 runs by the 24 participants in the control group. Participants in the intervention group reported higher comfort scores (8.00 ± 1.41 vs 6.96 ± 2.03, P ≤ 0.0001), faster running speeds (6.27 ± 1.03 vs 6.00 ± 1.54, P = 0.013), and lower RRI rates (0.70 ± 1.01 vs 1.21 ± 1.53, P = 0.18) than those in the control group. These findings were statistically significant for comfort and running speed but not for RRI rate, with statistical significance considered if P < 0.05. No adjustments were made for group differences in age, gender, tendency for RRIs or usual running speed.
CONCLUSION
This preliminary report provides evidence for orthotics use in increasing comfort levels and running speed, but no significant difference in RRI rate.
Keywords: Running, Foot orthoses, Running related injuries, Pain, Patient comfort, Athletic performance
Core Tip: Running-related injuries are becoming increasingly prevalent due to the increasing popularity of this sport. Foot orthotics have been suggested to increase comfort and speed whilst running, as well as reduce injury rate. However, current evidence is limited and mixed. This article, presenting preliminary randomised control trial data, finds significant evidence that running with Aetrex L700 Speed Orthotics, compared to running with no orthotics, in 'participants' regular running shoes, improves comfort and running speed. Participants running with Aetrex L700 Speed Orthotics, on average, reported lower injury rates than those running without orthotics. However, this difference was not significant.
INTRODUCTION
Running is becoming an increasingly popular sport, likely due to it being easily accessible, low cost and having multiple physical and mental health benefits. However, alongside this, there is also an increase in running-related injuries (RRIs). These usually affect the lower limb, the most common site being the knee, with almost half of RRIs occurring here[1-5]. Other common areas include the lower leg, ankle and foot due to injuries such as Achilles Tendonitis, Plantar Fasciitis and Tibial Stress Syndrome[3]. RRIs result in pain and discomfort and often cause individuals to take time off running. Reported rates of RRIs vary between 19.4% to 79.3% - partly due to the variation in the definition for RRI used by different studies, and therefore, it is important that studies clarify which definition they use. The risk of RRIs when running, alongside the rising popularity of the sport, necessitates research to find ways to prevent injury.
For many years foot orthotics have been used by runners to correct the alignment of the lower leg, improve arch support and increase cushioning of the foot. Orthotics are inserts which fit into the shoe in place of the removable insole. There are many different types, including off-the-shelf and custom-made. Previous research into the use of orthotics has found that they can improve comfort, provide better arch support and decrease the incidence of certain lower limb injuries such as stress fractures[6-9]. However, some studies have found no statistically significant difference in the Incidence of certain RRIs, such as soft-tissue injuries, when comparing the use of orthotics to no orthotics[9,10]. One study suggested that orthotics were a risk factor for RRIs, although the runners using orthotics in this study may have been more prone to injury than those who were not[5].
Previous research into the impact that orthotics have on running performance is limited and gives no clear conclusion. Some studies have shown a small significant increase in running economy with cushioned shoes[11], whereas others have found orthotics to have a negative impact on running economy[12]. Whether or not an improvement in running economy leads to a subsequent increase in performance is also unclear[13].
Overall, previous research regarding the effect of orthotics on running comfort, RRI rate and running performance is not clear. There are conflicting issues creating a lack of guidance for both professional and amateur runners concerning whether orthotics should or should not be used. Further research is required to clarify the effectiveness of orthotics in increasing comfort during running, improving running performance and preventing RRIs. The aim of this study is to assess comfort during running, running performance and RRI rate for recreational runners using prefabricated Aetrex[14] Orthotics compared to recreational runners not using orthotics. The results from this study will add to the existing knowledge surrounding the effect of orthotics on running and may provide evidence of a useful tool to prevent RRIs.
This article presents preliminary data from this study, followed by a discussion of how this data confers, conflicts with, and expands the current evidence base.
MATERIALS AND METHODS
This is a randomised control trial. The primary objective is to investigate whether inserting prefabricated orthotics into running shoes will increase comfort and speed and help decrease injury during recreational running as compared to running shoes without orthotics.
Recruitment
Participants were recruited on a voluntary basis through local running clubs and social media advertisements. Posters were distributed containing contact details for the Principal Investigator. Participants who got in contact were provided with the participant information sheet via email or post by a member of the research team. Potential participants were asked to read the information sheet fully and given time for consideration. Subsequently, all participants had either a phone or Zoom call, depending on their preference, with the Principal Investigator to discuss any queries they had about the study. Once participants had understood all the information and were happy to proceed, written informed consent was obtained, either online via legalesign.com or by post.
To be eligible, participants had to be aged 18 or over and be used to completing runs of at least 5km distance during the last 1 year. Participants were excluded if they were using prescription orthotics, had any ongoing pain or deformity in the foot or any serious health condition which has led to a doctor advising them not to exercise. They were also excluded if they had undergone any surgery in the last 6 months or any surgery to the feet during their lifetime. Participants were informed of their ability to withdraw from the study at any time if they wished, without needing to give a reason.
Randomisation
Once recruited, participants were randomised into one of two groups: an intervention group, who ran with Aetrex[14] L700 Speed Orthotics in their usual running shoes (Group A), and a control group, who ran with no orthotics (Group B). The Aetrex[14] L700 Speed Orthotics are pictured in Figure 1. Group allocation occurred by the opening of pre-filled and sealed envelopes containing notes to assign them either to Group A or to Group B. These envelopes were shuffled, and an individual independent of the study picked an envelope at random to assign a participant to a group. There was no blinding of either participants or researchers to group allocations following randomisation.
Figure 1.

Image of Aetrex L700 Speed Orthotics.
Those in Group A received Aetrex[14] L700 Speed Orthotics via post, according to their shoe size, along with an instruction sheet on how to use the orthotics. Participants in Group B were asked to run as they usually would, with no adjustments made to their regular running shoes.
Data collection
Basic demographic information was collected from participants upon recruitment to the study. All participants were asked to complete runs and provide quantitative data over an 8-wk data collection period. Participants provided data remotely via an online or paper survey, depending on their preference. Other than the addition of orthotics for participants in Group A, all participants were asked to run without altering their regular running routine, thereby keeping confounding variables to a minimum.
The following data was collected by participants immediately after each run: (1) Comfort - collected on a self-report visual analogue scale (VAS) of 0 to 10, where 0 is "No comfort" and 10 is "Maximum comfort"[15]; and (2) Running duration (measured in hours and minutes) and running distance (measured in miles) – used to calculate running speed.
Once per week, participants were asked to provide data relating to any RRIs experienced in the previous seven days via a self-report 'fill me in' section of the survey. The consensus definition for an RRI presented by Yamato and co-workers[16] was used in this study which is: "Running-related musculoskeletal pain in the lower limbs that causes a restriction or stoppage of running (distance, speed, duration, or training) for at least 7 d or 3 consecutive scheduled training sessions, or that which requires the runner to consult a physician or other health professional." Participants were provided with an RRI information sheet to inform them of this definition, and the common sites, symptoms and causes of RRIs, to help them provide accurate, consistent data relating to the injury.
Weeks 1 and 2 of data collection were an 'acclimatisation period', and weeks 7 and 8 were a 'de-acclimatisation period'; during these weeks, only injury data was collected. Comfort during running, running time and running distance data was collected during weeks 3, 4, 5 and 6.
The preliminary data presented in this article relates to the first 47 participants recruited for the study. However, recruitment is still ongoing in order to obtain a larger study cohort of 106 participants to maximise the reliability and reproducibility of results. This number is based on a sample size calculation performed using a target significance level of 5%, target power of 80% and allowing for a 20% dropout rate.
Statistical analysis
Once collected, data was stored appropriately, and statistical testing was performed[17]. The standard deviations, effect size (mean difference) and 95% confidence interval for each outcome variable were calculated to determine the direction and strength of any correlations in the results. An unpaired two-tailed t-test was performed from the data for each outcome variable to determine if between-group differences were statistically significant. Standard deviations differed between the two groups, and so all t-tests used Welch's correction to adjust for this.
The statistical methods of this study were reviewed by Steven Lane from the Department of Biostatistics, University of Liverpool.
The full trial protocol can be accessed at: https://clinicaltrials.gov/ct2/show/NCT04901442?term=orthotic%2C+running+related+injury%2C+comfort&cntry=GB&draw=2&rank=1.
RESULTS
This article presents preliminary data from the first 47 participants recruited to this randomised control trial (intervention group = 23, control group = 24). The details of participant flow, including numbers of participants recruited, randomly allocated to a group, and included in analysis, as well as withdrawals, are provided in Figure 2.
Figure 2.

Participant flow, including randomised group assignment and any withdrawals.
Recruitment began in July 2021 and is planned to finish in October 2022. Participants ranged in age from 19 to 67 years old (mean age = 39.9 years old). Participants in the intervention group were, on average, older than participants in the control group, with a mean age of 42.2 and 37.8 years old, respectively. 61.7% of study participants were male, and both groups contained more males than females. Basic demographic data and clinical characteristics for the 47 participants included in the preliminary analysis are provided in Table 1.
Table 1.
Basic demographic information for participants included in preliminary analysis
|
|
Orthotic group (%)
|
Control (no orthotic) group (%)
|
Total (%)
|
| Sex | |||
| Male | 13 (56.5) | 16 (66.7) | 29 (61.7) |
| Female | 10 (43.5) | 8 (33.4) | 18 (38.3) |
| Age (years) | |||
| < 20 | 1 (4.3) | 0 (0) | 1 (2.1) |
| 20-29 | 1 (4.3) | 3 (12.5) | 4 (8.5) |
| 30-39 | 6 (26) | 9 (37.5) | 15 (31.9) |
| 40-49 | 10 (43.5) | 10 (41.7) | 20 (42.6) |
| 50-59 | 3 (13) | 1 (4.2) | 4 (8.5) |
| 60-69 | 2 (8.7) | 1 (4.2) | 3 (6.4) |
| Total | 23 | 24 | 47 |
All participants were analysed within their original assigned groups, and all participants in the intervention group ran with the orthotics for the entire study period. Data for all three primary outcomes were provided from a total of 254 runs by the 23 participants in the intervention group (an average of 11 runs per participant) and a total of 289 runs by the 24 participants in the control group (an average of 12 runs per participant). Results for each primary outcome in each group are provided in Table 2, along with the mean difference and its precision. Results show positive effects between the use of Aetrex[14] Orthotics and comfort and running speed compared with using no orthotic. The effect size for the use of the orthotics on comfort was 1.10 (95%CI 0.81-1.40), larger than for running speed, which showed an effect size of 0.28 (95%CI 0.06–0.50). These differences in comfort and running speed are statistically significant, with P values of < 0.0001 and 0.013, respectively.
Table 2.
Data on all primary outcomes for both groups
|
|
Intervention group
|
Control group
|
Mean difference (95%CI)
|
P
value
|
| Comfort | 8.06 ± 1.41 | 6.96 ± 2.03 | 1.10 (0.81 to 1.40) | < 0.0001 |
| Injury rate | 0.70 ± 1.01 | 1.21 ± 1.53 | -0.51 (-1.28 to 0.25) | 0.18 |
| Running speed (miles per hour) | 6.27 ± 1.03 | 6.00 ± 1.54 | 0.28 (0.06 to 0.50) | 0.013 |
Values for the intervention group and control group are expressed as mean ± standard deviation. Statistical analysis used P values from unpaired two-tailed t-tests with Welch's correction. Significant difference was considered if P < 0.05. CI: Confidence interval. Injury rate: Number of injuries reported per participant over the 8-wk study period.
Participants in the intervention group reported a lower RRI rate than the control group, with an average of 0.70 injuries per participant running with the orthotics during the study period, compared to 1.21 injuries per participant running with no orthotics. This corresponds to a negative effect of -0.51 (95%CI -1.28 to 0.25) for RRI rate with the orthotics compared with no orthotics. This difference, however, is not statistically significant (P = 0.18).
Table 2 also shows standard deviations for each mean value. These are generally large relative to mean values, demonstrating widespread data. As a result, 95% confidence intervals for effect sizes are also wide. Interestingly, standard deviations and confidence intervals for all outcome measures data were larger for the control group, indicating that the intervention group generally produced more consistent data.
Despite injury being measured in the study, it was ensured that no participants experienced any additional harm or injury as a result of taking part by asking all participants to run as they normally would, without changing their running frequency, duration or speed. The only intervention was the addition of orthotics in the running shoes of participants in the intervention group, which demonstrated a lower RRI rate than the control group. One participant withdrew from the study due to injury. However, they were assigned to the control group meaning their injury was not due to the study intervention. This participant did not require any medical intervention other than cessation of running.
DISCUSSION
This article presents preliminary results from a randomised control trial study investigating the impact of running with Aetrex[14] Orthotics inserted into normal running shoes on comfort, running speed and RRI rate compared with running in normal running shoes with no orthotics. It finds that participants who ran with Aetrex[14] Orthotics reported higher comfort scores and running speeds and lower RRI rates than those who ran with no orthotics. This confers with other studies that have tested prefabricated orthotics[8,9] and adds to the current evidence for orthotics improving these parameters. The working principle of orthotics in benefitting comfort and reducing injury relates to their function in distributing pressure across the soles of the feet and decreasing overpronation. This subsequently reduces the internal rotation of the lower limb joints, which in turn reduces the risk of pressure- and overpronation-associated lower limb injuries[18-20]. This working principle is illustrated in Figures 3 and 4.
Figure 3.
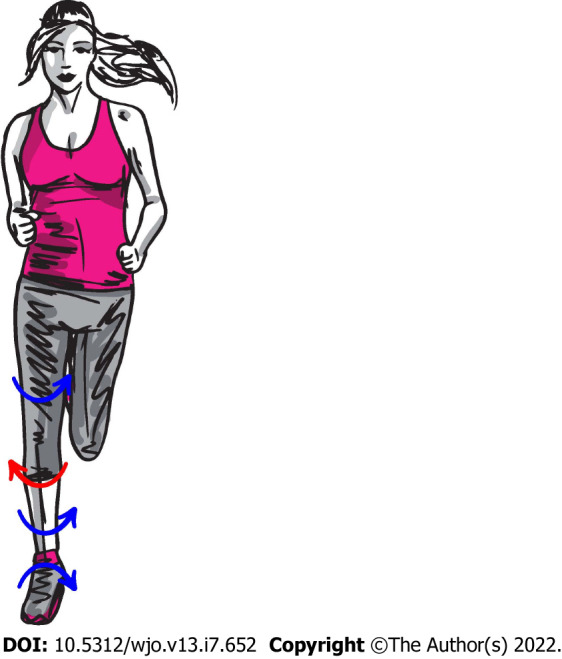
Internal rotation of lower limb joints and opposing external rotation of the patella caused by overpronation during running, which can lead to injuries.
Figure 4.
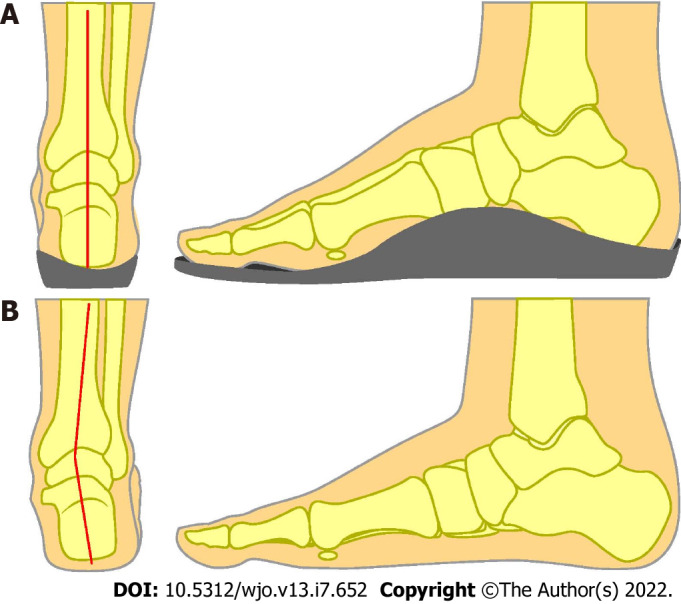
Working principle of orthotics. A: The correction of lower limb alignment by orthotics, by reducing overpronation; B: Compared to the lower limb misalignment present without orthotics, due to overpronation.
In this preliminary report, the relationship between improved comfort during running with Aetrex[14] Orthotics showed the largest effect size, whereas improvements in running speed and reductions in RRI rate showed smaller effects. Improvements in comfort and running speed when running with the orthotics were statistically significant in this study. This is relevant and advances current evidence for orthotics in improving these parameters, as many previous studies have been unable to find significant improvements[9,10]. In contrast, the reduction in RRI rate with orthotics in this study was not significant. These findings suggest that orthotics may be a cost-benefit. However, a full cost analysis will be provided in the final study report.
The spread of data was high for all outcome measures; this may be partly due to the nature of the variables, as running speed varies greatly between different runners, likewise tendency for injury. This may partly explain why many previous studies have found benefits in comfort, running performance and injury reduction with orthotics use[17,21], but that was not statistically significant, and additionally why the reduction in RRI rate with orthotics in this study was not significant.
Strengths and limitations
A limitation of the data in this preliminary report is the small number of participants. Further analysis, once the study has recruited its target sample size (106 participants), will provide more reliable and reproducible results. Another limitation is the lack of blinding of participants following group assignment due to the nature of the study. Some improvements in comfort and performance reported by participants who were provided with an orthotic may have been due to the placebo effect if participants had expectations that the orthotic would improve these parameters. VAS was selected for comfort scoring as it has been shown to have high inter-session reliability when used for a comfort rating of footwear[15], but it is still a subjective measurement, creating the potential for bias.
The study sample demonstrates a wide range of ages (19 to 67 years old), adding to the generalisability of the results. It also reflects the 2017 Sport England Active Lives Survey[22] estimate of the characteristics of the UK running population, in that it contains a greater number of men than women, adding to the validity of the results. However, the voluntary nature of recruitment in this study means that its sample cannot be said to be representative of the general population.
No adjustments were made for group differences in certain variables, such as tendency to become injured and usual running speed, and these may have had confounding effects on the results. One way to improve reliability in this study could be to collect quantitative data from participants for normal injury tendency (e.g. number of weeks spent injured, or number of RRIs in the past one year) and running speed (e.g., average running speed overall runs in the past six months) and adjust for group differences in these parameters.
CONCLUSION
This preliminary report of randomised control trial data provides evidence that using Aetrex[14] Orthotics in normal running shoes increases comfort levels and speed during running and decreases RRI rates, with the relationship between orthotics use and improved comfort showing the largest effect size. However, only improvements in comfort and running performance were significant. The sample size included in this preliminary analysis is small (n = 47). Further analysis, once recruitment and data collection in this study is complete, will expand on the findings given in this report and provide a full analysis of the cost-benefit.
ARTICLE HIGHLIGHTS
Research background
There is currently mixed and limited evidence regarding the effectiveness of orthotics use in increasing comfort and speed and reducing injury rate during running.
Research motivation
Further research into the effect of orthotics use on running-related injury (RRI) rates would be helpful for the ever-growing population of runners, who frequently suffer from RRIs. Additionally, there is a need to clarify whether orthotics use increases comfort during running and helps improve running speed.
Research objectives
To investigate whether running with Aetrex Orthotics improves comfort and performance and reduces injury whilst running.
Research methods
A randomised control trial study design was used. Participants were regular runners over 18 with no serious health conditions, ongoing foot pain or deformity, previous foot surgery in their lifetime or any surgery in the past 6 months, recruited on a voluntary basis through local running clubs and social media advertisements. Participants were randomly assigned to either an intervention group or a control group. Participants in the intervention group ran with Aetrex orthotics inserted into their normal running shoes, whilst participants in the control group ran in their normal running shoes with no orthotics. All participants were asked to complete runs as they usually would and provide data regarding comfort during running, running time and distance, and any RRIs over an 8-wk study period. For each outcome variable, the mean for each group, effect size and 95% confidence interval were calculated, and a t-test was performed to determine if between-group differences were statistically significant.
Research results
This article presents the interim results from the first 47 participants recruited to this study (intervention group = 23, control group = 24), who provided data for all three primary outcomes from a total of 543 runs. Participants in the intervention group reported higher comfort scores (8.00 ± 1.41 vs 6.96 ± 2.03, P ≤ 0.0001), faster running speeds (6.27 ± 1.03 vs 6.00 ± 1.54, P = 0.013), and lower RRI rates (0.70 ± 1.01 vs 1.21 ± 1.53, P = 0.18) than participants in the control group. Statistical significance was considered if P < 0.05. The findings were statistically significant for comfort and running speed but not for RRI rate.
Research conclusions
This interim report finds that using Aetrex Orthotics whilst running significantly increases comfort and speed. Using Aetrex Orthotics also reduces the rate of RRIs. However, this was not significant.
Research perspectives
Further analysis, once recruitment and data collection in this study is complete, is needed to expand on the findings given in this report and provide a full analysis of the cost-benefit of using orthotics for running.
ACKNOWLEDGEMENTS
We would like to thank all participants who took part in this study.
Footnotes
Institutional review board statement: This study was reviewed and approved by Wales Research Committee 5 (reference number: 21/WA/0098).
Clinical trial registration statement: This study is registered at https://clinicaltrials.gov/ct2/show/NCT04901442. The registration identification number is: NCT04901442.
Informed consent statement: All study participants gave their informed, written consent (via an online e-form) prior to study inclusion.
Conflict-of-interest statement: George Ampat, Jonathan M G Sims and Samantha J Rhodes are Directors/employees of Talita Cumi Ltd. Talita Cumi Ltd has a commercial relationship with Aetrex, Inc. 414 Alfred Avenue Teaneck, NJ 07666, USA. Alice E Fortune has no conflict of interest.
CONSORT 2010 statement: The authors have read the CONSORT 2010 Statement, and the manuscript was prepared and revised according to the CONSORT 2010 Statement.
Provenance and peer review: Unsolicited article; Externally peer reviewed.
Peer-review model: Single blind
Corresponding Author's Membership in Professional Societies: British Orthopaedic Association, No. 15546.
Peer-review started: March 6, 2022
First decision: April 28, 2022
Article in press: June 24, 2022
Specialty type: Orthopedics
Country/Territory of origin: United Kingdom
Peer-review report’s scientific quality classification
Grade A (Excellent): 0
Grade B (Very good): B, B, B
Grade C (Good): 0
Grade D (Fair): D
Grade E (Poor): 0
P-Reviewer: Ghannam WM, Egypt; Liang P, China; Peng BG, China; Velázquez-Saornil J, Spain S-Editor: Liu JH L-Editor: A P-Editor: Liu JH
Contributor Information
Alice E Fortune, School of Medicine, University of Liverpool, Liverpool L69 3GE, United Kingdom.
Jonathan M G Sims, Research Unit, Talita Cumi Ltd, Southport PR8 3NS, United Kingdom.
Samantha J Rhodes, Research Unit, Talita Cumi Ltd, Southport PR8 3NS, United Kingdom.
George Ampat, School of Medicine, University of Liverpool, Liverpool L69 3GE, United Kingdom. geampat@liverpool.ac.uk.
Data sharing statement
The anonymised dataset is available from the corresponding author at g.ampat@liverpool.ac.uk. Participants gave informed consent for sharing of anonymised data.
References
- 1.Koplan JP, Rothenberg RB, Jones EL. The natural history of exercise: a 10-yr follow-up of a cohort of runners. Med Sci Sports Exerc. 1995;27:1180–1184. [PubMed] [Google Scholar]
- 2.van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007;41:469–480; discussion 480. doi: 10.1136/bjsm.2006.033548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36:95–101. doi: 10.1136/bjsm.36.2.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kemler E, Blokland D, Backx F, Huisstede B. Differences in injury risk and characteristics of injuries between novice and experienced runners over a 4-year period. Phys Sportsmed. 2018;46:485–491. doi: 10.1080/00913847.2018.1507410. [DOI] [PubMed] [Google Scholar]
- 5.van der Worp MP, ten Haaf DS, van Cingel R, de Wijer A, Nijhuis-van der Sanden MW, Staal JB. Injuries in runners; a systematic review on risk factors and sex differences. PLoS One. 2015;10:e0114937. doi: 10.1371/journal.pone.0114937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Finestone A, Giladi M, Elad H, Salmon A, Mendelson S, Eldad A, Milgrom C. Prevention of stress fractures using custom biomechanical shoe orthoses. Clin Orthop Relat Res. 1999:182–190. doi: 10.1097/00003086-199903000-00022. [DOI] [PubMed] [Google Scholar]
- 7.Gerych D, Tvrznik A, Prokesova E, Nemeckova Z, Jelen K. Analysis of peak pressure, maximal force, and contact area changes during walking and running with conventional and shock-absorbing insoles in the combat boots of the Czech army. J Mech Med Biol. 2013;13 [Google Scholar]
- 8.Mündermann A, Stefanyshyn DJ, Nigg BM. Relationship between footwear comfort of shoe inserts and anthropometric and sensory factors. Med Sci Sports Exerc. 2001;33:1939–1945. doi: 10.1097/00005768-200111000-00021. [DOI] [PubMed] [Google Scholar]
- 9.Bonanno DR, Landorf KB, Munteanu SE, Murley GS, Menz HB. Effectiveness of foot orthoses and shock-absorbing insoles for the prevention of injury: a systematic review and meta-analysis. Br J Sports Med. 2017;51:86–96. doi: 10.1136/bjsports-2016-096671. [DOI] [PubMed] [Google Scholar]
- 10.Larsen K, Weidich F, Leboeuf-Yde C. Can custom-made biomechanic shoe orthoses prevent problems in the back and lower extremities? J Manipulative Physiol Ther. 2002;25:326–331. doi: 10.1067/mmt.2002.124419. [DOI] [PubMed] [Google Scholar]
- 11.Fuller JT, Bellenger CR, Thewlis D, Tsiros MD, Buckley JD. The effect of footwear on running performance and running economy in distance runners. Sports Med. 2015;45:411–422. doi: 10.1007/s40279-014-0283-6. [DOI] [PubMed] [Google Scholar]
- 12.Crago D, Bishop C, Arnold JB. The effect of foot orthoses and insoles on running economy and performance in distance runners: A systematic review and meta-analysis. J Sports Sci. 2019;37:2613–2624. doi: 10.1080/02640414.2019.1651582. [DOI] [PubMed] [Google Scholar]
- 13.O Sullivan IJ, Johnson MI, Hind K, Breen S, Francis P. Are changes in running economy associated with changes in performance in runners? J Sports Sci. 2019;37:1521–1533. doi: 10.1080/02640414.2019.1575177. [DOI] [PubMed] [Google Scholar]
- 14.Aetrex . Aetrex.com [Internet]. Aetrex.com: Aetrex Worldwide, Inc.; 2022. [Google Scholar]
- 15.Lindorfer J, Kröll J, Schwameder H. Comfort assessment of running footwear: Does assessment type affect inter-session reliability? Eur J Sport Sci. 2019;19:177–185. doi: 10.1080/17461391.2018.1502358. [DOI] [PubMed] [Google Scholar]
- 16.Yamato TP, Saragiotto BT, Lopes AD. A consensus definition of running-related injury in recreational runners: a modified Delphi approach. J Orthop Sports Phys Ther. 2015;45:375–380. doi: 10.2519/jospt.2015.5741. [DOI] [PubMed] [Google Scholar]
- 17.Richter RR, Austin TM, Reinking MF. Foot orthoses in lower limb overuse conditions: a systematic review and meta-analysis--critical appraisal and commentary. J Athl Train. 2011;46:103–106. doi: 10.4085/1062-6050-46.1.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bonanno DR, Landorf KB, Menz HB. Pressure-relieving properties of various shoe inserts in older people with plantar heel pain. Gait Posture. 2011;33:385–389. doi: 10.1016/j.gaitpost.2010.12.009. [DOI] [PubMed] [Google Scholar]
- 19.Albert S, Rinoie C. Effect of custom orthotics on plantar pressure distribution in the pronated diabetic foot. J Foot Ankle Surg. 1994;33:598–604. [PubMed] [Google Scholar]
- 20.Desmyttere G, Hajizadeh M, Bleau J, Begon M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: A systematic review and meta-analysis. Clin Biomech (Bristol, Avon) 2018;59:117–129. doi: 10.1016/j.clinbiomech.2018.09.018. [DOI] [PubMed] [Google Scholar]
- 21.Hume P, Hopkins W, Rome K, Maulder P, Coyle G, Nigg B. Effectiveness of foot orthoses for treatment and prevention of lower limb injuries : a review. Sports Med. 2008;38:759–779. doi: 10.2165/00007256-200838090-00005. [DOI] [PubMed] [Google Scholar]
- 22.SportEngland . Active Lives Adult Survey: May 16/17 Report [Internet]. England: Sport England; 2017. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The anonymised dataset is available from the corresponding author at g.ampat@liverpool.ac.uk. Participants gave informed consent for sharing of anonymised data.