

Abstract
In animal studies, the combination of in utero fluoride exposure and low iodine has greater negative effects on offspring learning and memory than either alone, but this has not been studied in children. We evaluated whether the maternal urinary iodine concentration (MUIC) modifies the association between maternal urinary fluoride (MUF) and boys’ and girls’ intelligence. We used data from 366 mother–child dyads in the Maternal–Infant Research on Environmental Chemicals Study. We corrected trimester-specific MUF and MUIC for creatinine, and averaged them to yield our exposure variables (MUFCRE, mg/g; MUICCRE, µg/g). We assessed children’s full-scale intelligence (FSIQ) at 3 to 4 years. Using multiple linear regression, we estimated a three-way interaction between MUFCRE, MUICCRE, and child sex on FSIQ, controlling for covariates. The MUICCRE by MUFCRE interaction was significant for boys (p = 0.042), but not girls (p = 0.190). For boys whose mothers had low iodine, a 0.5 mg/g increase in MUFCRE was associated with a 4.65-point lower FSIQ score (95% CI: −7.67, −1.62). For boys whose mothers had adequate iodine, a 0.5 mg/g increase in MUFCRE was associated with a 2.95-point lower FSIQ score (95% CI: −4.77, −1.13). These results suggest adequate iodine intake during pregnancy may minimize fluoride’s neurotoxicity in boys.
Keywords: fluoride, iodine, intelligence, neurodevelopment, pregnancy
1. Introduction
Fluoride exposure during early brain development has been associated with diminished intelligence quotient (IQ) scores among children living in areas with high levels of naturally occurring fluoride in drinking water (~3 mg/L) [1,2,3] and in areas where fluoride is added to public water supplies or salt for caries prevention [4,5,6]. The mechanism(s) underlying fluoride-associated cognitive deficits are not well understood, but changes to the thyroid function may be one such mechanism [7,8,9,10,11]. In 2006, the National Research Council (NRC) classified fluoride as an endocrine disruptor and recommended more research to understand fluoride’s effects on the thyroid gland, especially in iodine deficient pregnant women [12].
Iodine is an essential nutrient for thyroid hormone synthesis and normal thyroid function [13]. Sufficient iodine intake is critical for optimal maternal and fetal thyroid function and normal fetal neurodevelopment [14,15,16,17]. Even mild to moderate iodine deficiency in pregnancy has been linked to diminished cognitive abilities in children [14,18,19,20,21,22,23,24], though not in all studies [25,26]. The inconsistent results may reflect differences in the severity of maternal iodine deficiency, methodology, age at outcome assessment, or other biological co-factors.
Studies conducted in China examined whether fluoride exposure and iodine deficiency combine to impart adverse effects on children’s intelligence. Notably, school-aged children living in endemic fluoride and iodine-deficient areas had lower IQ scores than those living in endemic fluoride areas alone or iodine-deficient areas alone [27,28]. Fluoride in drinking water was reported to exacerbate the adverse effects of low iodine on child neurodevelopment and central nervous system function more broadly [28]. However, these studies were cross-sectional and did not account for potential confounders. In experimental studies, rat offspring exposed to both high fluoride and low iodine in utero showed greater deficits in learning and memory compared with those exposed to either high fluoride or low iodine [29,30].
Given the ubiquity of fluoride exposure, along with recent trends showing mild-to-moderate iodine deficiency in pregnant women [17,31,32], we evaluated whether the maternal iodine status modifies the association between prenatal fluoride exposure and children’s intelligence. We hypothesized that low urinary iodine concentrations in Canadian pregnant women would exacerbate the fluoride-associated intellectual deficits observed in their children. We further hypothesized that the effects would be stronger in boys than girls given previous findings of sex differences in the neurotoxicity of prenatal fluoride exposure [33].
2. Materials and Methods
2.1. Participants
Participants included mother–child dyads enrolled in the Canadian Maternal–Infant Research on Environmental Chemicals (MIREC) study. Between 2008 and 2011, 2001 pregnant women were recruited from 10 cities across Canada to participate in a longitudinal cohort study. The inclusion criteria were as follows: women who were 18 years of age or older who could provide consent, communicate in English or French, and were <14 weeks’ gestation. Participants were excluded if they had any medical complications, any known fetal abnormalities, or if there was illicit drug or alcohol abuse during pregnancy. Additional details of the MIREC study can be found in the cohort profile [34].
A subset of 808 women provided consent to participate with their child in the MIREC-Child Development Plus (CD Plus) follow-up study. Due to budgetary constraints, recruitment for MIREC CD Plus was limited to six of the ten cities from the original cohort, namely Vancouver, Toronto, Hamilton, Montreal, Kingston, and Halifax. The inclusion criteria for mother–child dyads in MIREC-CD Plus were as follows: mothers of singleton children born >28 weeks’ gestation who were between the ages of 3 and 4 at time of the study and had no congenital abnormalities, major neurological disorders, or history of convulsions. Among the 808 women who consented, 610 agreed to child IQ testing (76%), 601 of whom completed the neurodevelopmental testing. The latter subset of 601 mother–child dyads provided data for the current study.
Of the 601 children who completed IQ testing, 366 had complete data on maternal urinary fluoride (MUF), maternal urinary iodine concentration (MUIC), urinary creatinine (CRE), and covariates (See Figure 1); 235 were excluded for missing (i) creatinine data at all three trimesters (n = 175), (ii) a valid MUF measure available at all three trimesters (n = 9), (iii) MUICCRE < 600 μg/g data at trimesters 1 and 2 (n = 40), and (4) covariate data (n = 11). Women with MUICCRE values greater than or equal to 600 μg/g (n= 37) were excluded from the analyses because excess iodine levels have been linked to diminished intelligence [35], and we were specifically interested in comparing women with “low” levels of iodine with those with “adequate” levels of iodine, rather than “excess” levels of iodine. We considered MUICCRE values greater than or equal to 600 μg/g to be “higher than adequate” as opposed to the WHO cut-off of 500 μg/L for unadjusted MUIC [36], given that we used MUIC values corrected for creatinine, and MUICCRE values increase from trimester 1 to 2 [37].
Figure 1.
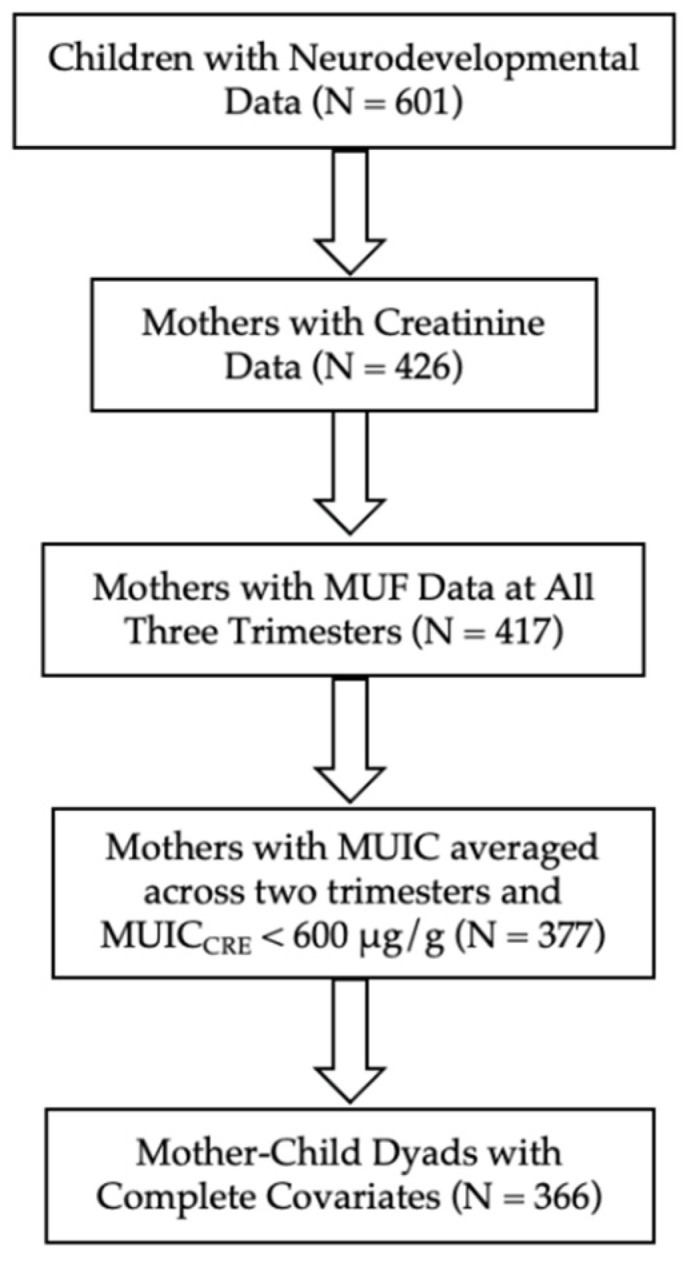
Sample flow chart.
The present study was approved by the research ethics boards at Health Canada and York University. The MIREC study was also approved by the research ethics boards at all participating recruitment sites and at Health Canada. All participants provided their informed consent.
2.2. Urine Collection
Urine was collected in Nalgene® containers, labeled with a unique identification, aliquoted into smaller Cryovials®, and stored at appropriate temperatures until they were shipped for fluoride or iodine analysis. Spot samples were collected in each trimester of pregnancy at a mean ± SD of 11.57 ± 1.57, 19.11 ± 2.39, and 33.11 ± 1.50 weeks’ gestation.
2.3. Maternal Urinary Fluoride Concentration
We derived maternal urinary fluoride (MUF, mg/L) concentrations by averaging fluoride concentrations across trimesters. We previously found a moderate correlation between the three samples, with intraclass correlation coefficients ranging from 0.37 to 0.40 [38]. Urine samples were analyzed at the Indiana University School of Dentistry through a modification of the hexamethyldisiloxane (HMDS; Sigma Chemical Co., St. Louis, MO, USA) micro-diffusion procedure described previously [38,39]. In neutral solutions, fluoride concentrations were measured down to 0.02 mg/L. Two of the spot urine samples (0.04%) were excluded from the first trimester as the readings surpassed the highest concentration standard of the instrument (5 mg/L).
2.4. Maternal Urinary Iodine Concentration
We derived the maternal urinary iodine concentration (MUIC, µg/L) by averaging iodine concentrations from two spot urine samples collected in the first and second trimester. MUIC is considered a reliable biomarker of recent iodine intake and reflects total iodine intake from all dietary sources [40]. MUIC was measured by the accredited Toxicology Laboratory at the Institut National de Santé Publique du Québec (INSPQ) using inductively coupled plasma mass spectrometry (ICP-MS). Values below the limit of detection (LOD, 38 µg/L) were replaced with the LOD divided by the square root of 2 (Hornung and Reed, 1990); 180 (9.74%) and 79 (4.56%) mothers had a MUIC below the LOD in trimesters 1 and 2, respectively.
2.5. Correcting for Variability in Urinary Dilution
To account for variability in urine dilution at time of measurement, MUF and MUIC were corrected for creatinine (CRE) measured in the same spot sample using the following equations:
where MUFT1 is the observed fluoride concentration, MUICT1 is the observed MUIC, and CRET1 is the observed creatinine concentration for that individual in trimester 1. MUFT2 is the observed fluoride concentration, MUICT2 is the observed MUIC, and CRET2 is the observed creatinine concentration for that individual in trimester 2. MUFT3 is the observed fluoride concentration, and CRET3 is the observed creatinine concentration for that individual in trimester 3. The measurement of urinary creatinine was previously described [38]. In pregnant women, the iodine to creatinine ratio (MUIC/CRE) is moderately correlated with 24 h urinary iodine excretion, the gold standard measure of iodine status relative to uncorrected urinary iodine concentration [14,41].
2.6. Children’s Full-Scale Intelligence Quotient
We assessed children’s intellectual abilities at 3 to 4 years of age using the Wechsler Preschool and Primary Scale of Intelligence-III with Canadian age-standardized norms (mean = 100, SD = 15). The test was administered in children’s homes in either English or French by qualified research professionals who were blinded to gestational iodine status or fluoride exposure in pregnancy. We used full-scale intelligence (FSIQ), a measure of global intellectual and cognitive functioning, as our primary outcome.
2.7. Covariates
We selected covariates a priori based on prior work with the same study cohort examining fluoride exposure and children’s intellectual abilities [6]. Covariates included maternal education (dichotomized as bachelor’s degree or higher), maternal race (White/non-White), study site, and a continuous measure of the quality of the home environment using the Home Observation for Measurement of the Environment (HOME)—Revised Edition [42] at the time of the home visit when children were aged 3 to 4 years old.
2.8. Statistical Analyses
We used chi-square tests for categorical covariates and t-tests for continuous covariates to test for sampling differences between those with complete data and those without complete data (i.e., without MUFCRE or MUICCRE but with FSIQ data). For descriptive purposes, MUICCRE was stratified into those with low (<200 μg/g) and adequate ≥200 and <600 μg/g urinary iodine. Independent sample t-tests were used to test for differences between boys and girls for exposure and outcome variables. Welch’s correction was applied for t-tests to account for unequal variance.
We used multiple linear regression to estimate a model with a three-way interaction between MUFCRE, MUICCRE, and child sex in predicting children’s FSIQ scores while controlling for maternal education, maternal race, study site, and the HOME score; this model included all constituent two-way interaction terms and first-order effects. To determine whether MUFCRE and MUICCRE interact as a function of sex without stratifying the sample, we then examined the model-implied MUFCRE by MUICCRE two-way interaction within each sex. To facilitate the interpretation of coefficients, we centered MUICCRE (i.e., subtracted a constant from every value of MUICCRE) around a “low” level (i.e., 147 μg/g which corresponds to the 10th percentile value for MUICCRE) and an “adequate” level (i.e., 294 μg/g which corresponds to the 50th percentile value for MUICCRE) [43,44]. We then re-ran the model using MUICCRE centered around the “low” and “adequate” levels of iodine, separately, with boys coded as the reference. The model was re-estimated with girls coded as the reference to interpret the association between MUFCRE and FSIQ for a girl whose mother had a low or adequate level of iodine during pregnancy. All models were evaluated for linearity, homoscedasticity, and normality and model assumptions were sufficiently met. No influential outliers were detected according to Cook’s distance.
We used STATA version 16.1 (STATA corporation) for data analysis. The level of significance was 0.05, and all statistical tests were two-tailed. All coefficients were reported for every 0.5 mg/g increase in MUFCRE (approximately the IQR).
3. Results
Most participants included in the present study were married or in a common-law relationship, had a bachelor’s degree or higher, and were White (Table 1). Mother–child dyads with complete data did not significantly differ from those without complete data on any of the demographic characteristics, except a greater proportion of mothers with complete data were White.
Table 1.
Demographic Characteristics of those with Complete Data (N = 366) and Incomplete Data (N = 211).
| Demographic Characteristic (Mean ± SD or N (%)) |
Complete Data (N = 366) | Incomplete Data (N = 211) | p |
|---|---|---|---|
| Mothers | |||
| Maternal Age (years) | 32.50 ± 4.51 | 32.55 ± 4.62 | 0.899 |
| Married or Common Law | 353 (96.54) | 205 (97.16) | 0.646 |
| White | 334 (91.26) | 181 (85.78) | 0.041 |
| Bachelor’s Degree or Higher | 243 (66.39) | 142 (67.30) | 0.824 |
| Taking a prenatal multivitamin | 319 (87.40) | 175 (82.94) | 0.140 |
| HOME Score | 47.23 ± 4.44 | 47.40 ± 4.10 | 0.649 |
| Children | |||
| Male | 186 (50.82) | 98 (46.44) | 0.311 |
| Age at Testing (years) | 3.44 ± 0.32 | 3.40 ± 0.31 | 0.144 |
Abbreviations: HOME = Home Observation Measurement of the environment.
The median (IQR) MUFCRE and MUICCRE were 0.61 (0.49) mg/g and 294 (181) μg/g, respectively. Boys and girls did not differ significantly in MUFCRE concentration or MUICCRE (Table 2). Children’s FSIQ scores were in the average range, with girls scoring significantly higher than boys (t(364) = −3.17, p = 0.002; Table 2).
Table 2.
MUFCRE, MUICCRE, and Full-Scale IQ by sex.
| Urinary Measurement |
All | Boys | Girls | ||||
|---|---|---|---|---|---|---|---|
| n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | p 1 | |
| MUFCRE (mg/g) | 366 | 0.61 (0.49) | 186 | 0.63 (0.52) | 180 | 0.61 (0.48) | 0.538 |
| MUICCRE (μg/g) | 366 | 294 (181) | 186 | 309 (181) | 180 | 287 (203) | 0.059 |
| Low | 86 | 148 (47) | 31 | 131 (73) | 55 | 152 (37) | 0.083 |
| Adequate | 280 | 341 (165) | 155 | 348 (187) | 125 | 336 (146) | 0.893 |
| Outcome | n | Mean ± SD | n | Mean ± SD | n | Mean ± SD | p 1 |
| FSIQ | 366 | 107.46 ± 13.75 | 186 | 105.25 ± 14.90 | 180 | 109.75 ± 12.09 | 0.002 |
Low MUICCRE < 200 μg/g, Adequate MUICCRE ≥ 200 & < 600 μg/g; Abbreviations: MUFCRE = Maternal urinary fluoride corrected for creatinine; MUICCRE = maternal urinary iodine concentration corrected for creatinine; FSIQ = Full-Scale IQ. 1 Comparing boys with girls.
Three-Way Interaction Model
We found a significant three-way interaction between MUFCRE, MUICCRE, and sex while controlling for relevant covariates (p = 0.019; see Table 3 and Figure 2). The two-way MUICCRE by MUFCRE interaction was significant for boys (p = 0.042), but not girls (p = 0.190). For boys whose mothers had a low MUICCRE, every 0.5 mg/g increase in MUFCRE was associated with a 4.65-point lower FSIQ score (95% CI: −7.67, −1.62; p = 0.003). For boys whose mothers had adequate MUICCRE, every 0.5 mg/g increase in MUFCRE was associated with a 2.95-point lower FSIQ score (95% CI: −4.77, −1.13; p = 0.002). In contrast, MUFCRE was marginally associated with FSIQ for girls whose mothers had low MUICCRE (B = 2.48; 95% CI: −0.31, 5.26; p = 0.081) and was not significantly associated with FSIQ for girls whose mothers had adequate MUICCRE (B = 1.31, 95%; CI: −0.41, 3.03; p = 0.135).
Table 3.
Results of the three-way interaction model.
| Variable | B | SE(B) | p |
|---|---|---|---|
| MUFCRE (mg/g) | −5.89 | 1.85 | 0.002 |
| MUICCRE (μg/g) | −0.03 | 0.01 | 0.023 |
| Sex | −3.09 | 2.17 | 0.155 |
| MUFCRE × MUICCRE | 0.02 | 0.01 | 0.042 |
| MUFCRE × Sex | 8.51 | 2.40 | <0.001 |
| MUICCRE × Sex | 0.03 | 0.02 | 0.042 |
| MUFCRE × MUICCRE × Sex | −0.04 | 0.02 | 0.019 |
Note. SE: Standard Error, R2 = 0.28, F (15, 350) = 8.97, p < 0.001; Abbreviations: MUFCRE = maternal urinary fluoride corrected for creatinine; MUICCRE = maternal urinary iodine concentration corrected for creatinine. Model adjusted for maternal level of education, maternal ethnicity, HOME score, and study site. MUICCRE is centered around the “adequate” level of iodine, and boys are coded as the reference. The coefficient for MUFCRE represents the association between MUFCRE and FSIQ for a boy whose mother had an adequate level of MUICCRE during pregnancy.
Figure 2.

Model—implied three-way interaction between maternal urinary fluoride (MUFCRE), maternal urinary iodine concentration (MUICCRE) and child sex. Every 0.5 mg/g increase in MUFCRE was significantly associated with a 4.65- and −2.95-point lower FSIQ score for boys whose mothers had low MUICCRE or adequate MUICCRE, respectively. MUFCRE was marginally associated with FSIQ for girls whose mothers had low MUICCRE and not significantly associated with FSIQ for girls whose mothers had adequate MUICCRE.
4. Discussion
We examined whether gestational iodine status modifies the association between prenatal fluoride exposure and preschool boys’ and girls’ intelligence in the Maternal Infant Research on Environmental Chemicals (MIREC) Study. To do so, we estimated the three-way interaction between prenatal fluoride exposure, gestational iodine status, and sex on children’s FSIQ. We found that the association between prenatal fluoride exposure and FSIQ was stronger among boys whose mothers had low urinary iodine concentrations in pregnancy compared to boys whose mothers had adequate iodine concentrations in pregnancy. These findings are consistent with previous experimental and human epidemiological studies [27,28,29,30,45] and indicate that even mildly reduced iodine levels may have biological significance when interacting with fluoride. Importantly, our findings were observed in a Canadian pregnancy sample with, on average, sufficient iodine intake (median iodine = 294 μg/g) and with 88% of women taking prenatal multi-vitamins.
Regarding potential mechanisms, experimental evidence demonstrates that prenatal exposure to both high fluoride and low iodine can induce neurochemical changes in offspring. For example, Ge et al., (2011) found that brains of rat offspring exposed to both high fluoride and low iodine in utero had different protein profiles compared with controls; proteins involved in cellular signaling and metabolism were most affected [46]. Other studies with similar experimental designs found higher levels of superoxide dismutase and malondialdehyde (biomarkers of oxidative stress), apoptosis, and histopathological changes (e.g., elongation of neural dendrites and missing nuclei) in the brains of rat offspring exposed to high fluoride and low iodine compared with those exposed to either alone [29,47,48].
The combination of low iodine and high fluoride may also adversely impact thyroid function. A prior study conducted in Canada showed that higher urinary fluoride levels in adults were associated with higher thyroid stimulating hormone levels, but only among adults who had low urinary iodine concentrations (≤0.38 µmol/L) [49]. One potential mechanism by which fluoride may interact with iodine to affect thyroid function is by inhibiting one or more enzymes involved in normal thyroid function, such as deiodinases [50]. This would increase the iodine requirement, such that the effect would be more severe in the presence of iodine deficiency. Another common hypothesis is that fluoride displaces thyroidal iodine uptake since it is more electronegative and has a lighter atomic weight than iodine [51].
Experimental studies have also shown that the effects of fluoride may be exacerbated by deficient or excess iodine [52]. For instance, Guan et al. (1988) observed decreases in T3 and T4 among adult Wistar rats with sufficient iodine intake who were exposed to fluoride at a concentration of 30 mg/L [53]. These same changes were observed among iodine-deficient rats who were exposed to fluoride at a lower concentration of only 10 mg/L. Another study with adult mice observed lower levels of triiodothyronine (T3) and thyroxine (T4) among mice with a deficient iodine intake coupled with low fluoride intake when compared with mice with a moderate iodine intake [52]. Thus, the relationship between fluoride exposure and thyroid function may differ as a function of iodine intake.
The impact of fluoride and iodine on thyroid hormones during pregnancy is especially relevant to cognitive abilities in offspring. The fetus is entirely dependent on maternal thyroid hormones until mid-gestation and continues to be partially dependent until birth [54]. Even subtle changes in maternal thyroid hormone levels in pregnancy can have adverse effects on brain structure [55,56,57] and neurodevelopment [55,56,58]. Low iodine and exposure to higher levels of fluoride in drinking water during pregnancy are both independently associated with a greater risk of developing hypothyroidism [59,60]. Our results are consistent with the combination of low iodine and high fluoride compounding thyroid disruption during fetal development, the most vulnerable period of brain development.
In our study, the interaction between fluoride and iodine was only evident in boys. This finding is consistent with a recent cross-sectional study conducted in China showing that iodine modified the susceptibility of the thyroid gland to fluoride exposure in school-aged boys, but not girls [45]. For boys with lower urinary levels of iodine, higher urinary fluoride was associated with larger thyroid volumes, whereas higher levels of iodine reduced the effects of fluoride on the thyroid. To our knowledge, no study has examined sex-specific effects of the interaction between prenatal fluoride and iodine on neurodevelopmental outcomes, but some epidemiological and animal studies of fluoride neurotoxicity found that boys are more vulnerable to prenatal fluoride exposure than girls [33]. Sex-specific effects in the interaction between fluoride and iodine, particularly among mothers with insufficient iodine intake, may disrupt in utero thyroid hormones. Given that the thyroid gland expresses estrogen and androgen receptors, boys and girls may respond differently to thyroid hormone insufficiency [61,62,63]. One study, for example, found that maternal trajectories of thyroid hormones were associated with preschool boys’ behavioural development but not girls’ [64]. Taken together, these findings indicate that future investigations of fluoride’s neurotoxicity should examine the roles of iodine intake and child sex, and whether thyroid hormones mediate the pathway for fluoride and iodine’s effects on boys’ IQ.
Strengths and Limitations
Our study has several strengths, including a modest-sized pregnancy cohort, prospective design, state-of-the-art biomarkers of fluoride exposure and iodine status, available information on a wide array of potential maternal and child confounders, and use of standardized and valid measures of child intelligence. Our study also has limitations. Compared with the general Canadian population, women in the MIREC cohort were more educated, older, predominantly Caucasian, and more likely to be married or in common law relationships [34], which may limit the generalizability of our findings. The high use of prenatal multivitamins in our sample likely reduced the risk of moderate-to-severe iodine deficiency which may be observed in other populations. Even though we used state-of-the-art biomarkers, fluoride and iodine both have short half-lives and could therefore be impacted by recent fluoride or iodine ingestion. Further, we measured iodine and fluoride in urine spot samples instead of 24 h urine samples. We attempted to minimize this limitation by averaging urine fluoride across all three trimesters of pregnancy, and urine iodine across two trimesters of pregnancy. Nonetheless, we acknowledge that up to ten repeat spot urine samples may be needed to accurately reflect individual iodine status [65].
5. Conclusions
This is the first prospective epidemiological study to estimate the interplay between prenatal fluoride exposure and maternal iodine status in relation to child IQ in boys and girls. Our findings indicate that the association between prenatal fluoride exposure and full-scale intelligence previously identified in this cohort [6] was exacerbated by low maternal iodine in pregnancy among boys. These results, which were found among mother-child pairs living in fluoridated and non-fluoridated communities in Canada, underscore the importance of sufficient iodine intake in pregnancy to minimize the neurotoxicity of fluoride in boys.
Acknowledgments
We thank Nicole Lupien, Stéphanie Bastien, and Romy-Leigh McMaster (Centre de Recherche, CHU Sainte-Justine), and the MIREC Study Coordinating Staff for their administrative support, the MIREC study group of investigators and site investigators, as well as the MIREC Biobank; Jillian Ashely-Martin for her review of our manuscript as the Knowledge Translation representative for the MIREC study; Christine Buckley, Frank Lippert, and Prithvi Chandrappa, (Indiana University School of Dentistry), for their analysis of urinary fluoride at the Indiana University School of Dentistry. Ciprian Mihai Cirtiu, Insitut National de Santé Publique du Québec, for measuring the urinary creatinine and iodine.
Author Contributions
Conceptualization, C.V.G., M.H., R.G. and C.T.; methodology, C.V.G., M.H., D.F., R.H. and C.T.; software, C.V.G.; validation, D.F. and R.H.; formal analysis, C.V.G.; investigation, B.L. and E.A.M.-M.; resources, E.A.M.-M.; data curation, C.V.G.; writing—original draft preparation, C.V.G. and M.H.; writing—review and editing, C.V.G., M.H., R.G., J.C., P.A., E.A.M.-M., T.M., J.K., D.F., R.H., B.L. and C.T.; visualization, C.V.G.; supervision, C.T.; project administration, C.T.; funding acquisition, B.L., P.A. and C.T. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at Health Canada (2019-023H) and York University (12 December 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Anonymized data described in the manuscript are available to qualified investigators with IRB approval.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Funding Statement
This research was funded by National Institute of Environmental Health Science, grant numbers R21ES027044, 2016–2019; R01ES030365, 2020–2025 and the Maternal-Infant Research on Environmental Chemicals Study was funded by the Chemicals Management Plan at Health Canada, the Ontario Ministry of the Environment, and the Canadian Institute for Health Research, grant number MOP-81285, 2006).
Footnotes
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Lu Y., Sun Z.R., Wu L.N., Wang X., Lu W., Liu S.S. Effect of High-Fluoride Water on Intelligence in Children. Fluoride. 2000;33:74–78. [Google Scholar]
- 2.Xiang Q., Liang Y., Chen L., Wang C., Chen B., Chen X., Zhou M. Effect of Fluoride in Drinking Water on Children’s Intelligence. Fluoride. 2003;36:84–94. [Google Scholar]
- 3.Zhao L.B., Liang G.H., Zhang D.N., Wu X.R. Effect of a High Fluoride Water Supply on Children’s Intelligence. Fluoride. 1996;29:190–192. [Google Scholar]
- 4.Bashash M., Thomas D., Hu H., Martinez-Mier E.A., Sanchez B.N., Basu N., Peterson K.E., Ettinger A.S., Wright R., Zhang Z., et al. Prenatal Fluoride Exposure and Cognitive Outcomes in Children at 4 and 6–12 Years of Age in Mexico. Environ. Health Perspect. 2017;125:97017. doi: 10.1289/EHP655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Till C., Green R., Flora D., Hornung R., Martinez-Mier E.A., Blazer M., Farmus L., Ayotte P., Muckle G., Lanphear B. Fluoride Exposure from Infant Formula and Child IQ in a Canadian Birth Cohort. Environ. Int. 2020;134:105315. doi: 10.1016/j.envint.2019.105315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Green R., Lanphear B., Hornung R., Flora D., Martinez-Mier E.A., Neufeld R., Ayotte P., Muckle G., Till C. Association between Maternal Fluoride Exposure during Pregnancy and IQ Scores in Offspring in Canada. JAMA Pediatr. 2019;173:940–948. doi: 10.1001/jamapediatrics.2019.1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chaitanya N., Karunakar P., Allam N., Priya M., Alekhya B., Nauseen S. A Systematic Analysis on Possibility of Water Fluoridation Causing Hypothyroidism. Indian J. Dent. Res. 2018;29:358–363. doi: 10.4103/ijdr.IJDR_505_16. [DOI] [PubMed] [Google Scholar]
- 8.Wang M., Liu L., Li H., Li Y., Liu H., Hou C., Zeng Q., Li P., Zhao Q., Dong L., et al. Thyroid Function, Intelligence, and Low-Moderate Fluoride Exposure among Chinese School-Age Children. Environ. Int. 2020;134:105229. doi: 10.1016/j.envint.2019.105229. [DOI] [PubMed] [Google Scholar]
- 9.Khandare A.L., Validandi V., Gourineni S.R., Gopalan V., Nagalla B. Dose-Dependent Effect of Fluoride on Clinical and Subclinical Indices of Fluorosis in School Going Children and Its Mitigation by Supply of Safe Drinking Water for 5 Years: An Indian Study. Environ. Monit. Assess. 2018;190:1–8. doi: 10.1007/s10661-018-6501-1. [DOI] [PubMed] [Google Scholar]
- 10.KheradPisheh Z., Mirzaei M., Mahvi A.H., Mokhtari M., Azizi R., Fallahzadeh H., Ehrampoush M.H. Impact of Drinking Water Fluoride on Human Thyroid Hormones: A Case-Control Study. Sci. Rep. 2018;8:2674. doi: 10.1038/s41598-018-20696-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Peckham S., Lowery D., Spencer S. Are Fluoride Levels in Drinking Water Associated with Hypothyroidism Prevalence in England? A Large Observational Study of GP Practice Data and Fluoride Levels in Drinking Water. J. Epidemiol. Community Health. 2015;69:619–624. doi: 10.1136/jech-2014-204971. [DOI] [PubMed] [Google Scholar]
- 12.National Research Council . Fluoride in Drinking Water; A Scientific Review of EPA’s Standards. National Academies Press; Washington, DC, USA: 2006. [Google Scholar]
- 13.Institute of Medicine . Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc: A Report of the Panel on Micronutrients… [et al.], Standing Committee on the Scientific Eva. National Academies Press; Cambridge, MA, USA: 2001. [PubMed] [Google Scholar]
- 14.Murcia M., Espada M., Julvez J., Llop S., Lopez-Espinosa M.J., Vioque J., Basterrechea M., Rianõ I., González L., Alvarez-Pedrerol M., et al. Iodine Intake from Supplements and Diet during Pregnancy and Child Cognitive and Motor Development: The INMA Mother and Child Cohort Study. J. Epidemiol. Community Health. 2018;72:216–222. doi: 10.1136/jech-2017-209830. [DOI] [PubMed] [Google Scholar]
- 15.de Escobar G.M., Obregón M.J., Escobar del Rey F. Maternal Thyroid Hormones Early in Prenancy and Fetal Brain Development. Best Pract. Res. Clin. Endocrinol. Metab. 2004;18:225–248. doi: 10.1016/j.beem.2004.03.012. [DOI] [PubMed] [Google Scholar]
- 16.Glinoer D. The Regulation of Thyroid Function during Normal Pregnancy: Importance of the Iodine Nutrition Status. Best Pract. Res. Clin. Endocrinol. Metab. 2004;18:133–152. doi: 10.1016/j.beem.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 17.Katz P.M., Leung A.M., Braverman L.E., Pearce E.N., Tomlinson G., He X., Vertes J., Okun N., Walfish P.G., Feig D.S. Iodine Nutrition during Pregnancy in Toronto, Canada. Endocr. Pract. 2013;19:206–211. doi: 10.4158/EP12193.OR. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.De Escobar G.M., Obregón M.J., Del Rey F.E. Iodine Deficiency and Brain Development in the First Half of Pregnancy. Public Health Nutr. 2007;10:1554–1570. doi: 10.1017/S1368980007360928. [DOI] [PubMed] [Google Scholar]
- 19.Zimmermann M.B. Iodine Deficiency in Pregnancy and the Effects of Maternal Iodine Supplementation on the Offspring: A Review. Am. J. Clin. Nutr. 2009;89:668–672. doi: 10.3945/ajcn.2008.26811C. [DOI] [PubMed] [Google Scholar]
- 20.Melse-Boonstra A., Jaiswal N. Iodine Deficiency in Pregnancy, infancy, and childhood and its consequences for brain development. Best Pract. Res. Clin. Endocrinol. Metab. 2010;24:29–38. doi: 10.1016/j.beem.2009.09.002. [DOI] [PubMed] [Google Scholar]
- 21.Bath S.C. The Effect of Iodine Deficiency during Pregnancy on Child Development. Proc. Nutr. Soc. 2019;78:150–160. doi: 10.1017/S0029665118002835. [DOI] [PubMed] [Google Scholar]
- 22.Pearce E.N. Effects of Iodine Deficiency in Pregnancy. J. Trace Elem. Med. Biol. 2012;26:131–133. doi: 10.1016/j.jtemb.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 23.Bath S.C., Steer C.D., Golding J., Emmett P., Rayman M.P. Effect of Inadequate Iodine Status in UK Pregnant Women on Cognitive Outcomes in Their Children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC) Lancet. 2013;382:331–337. doi: 10.1016/S0140-6736(13)60436-5. [DOI] [PubMed] [Google Scholar]
- 24.Levie D., Korevaar T.I.M., Bath S.C., Murcia M., Dineva M., Llop S., Espada M., Van Herwaarden A.E., De Rijke Y.B., Ibarluzea J.M., et al. Association of Maternal Iodine Status with Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019;104:5957–5967. doi: 10.1210/jc.2018-02559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ghassabian A., Steenweg-de Graaff J., Peeters R.P., Ross H.A., Jaddoe V.W., Hofman A., Verhulst F.C., White T., Tiemeier H. Maternal Urinary Iodine Concentration in Pregnancy and Children’s Cognition: Results from a Population-Based Birth Cohort in an Iodine-Sufficient Area. BMJ Open. 2014;4:e005520. doi: 10.1136/bmjopen-2014-005520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rebagliato M., Murcia M., Álvarez-Pedrerol M., Espada M., Fernández-Somoano A., Lertxundi N., Navarrete-Muñoz E.M., Forns J., Aranbarri A., Llop S., et al. Iodine Supplementation during Pregnancy and Infant Neuropsychological Development. Am. J. Epidemiol. 2013;177:944–953. doi: 10.1093/aje/kws333. [DOI] [PubMed] [Google Scholar]
- 27.Ren D., Li K., Liu D. A Study of the Intellectual Ability of 8–14 Year-Old Children in High Fluoride, Low Iodine Areas. Fluoride. 2008;41:319–320. [Google Scholar]
- 28.Fa-Fu L., Aihaiti H.X.Z., Jin U., Ji-Yong J., Maimaiti A. The Relationship of a Low-Iodine and High- Fluoride Environment to Subclinical Cretinism in Xinjiang. Iodine Defic. Disord. Newsl. 1991;7:24–25. [Google Scholar]
- 29.Wang J., Ge Y., Ning H., Wang S. Effects of High Fluoride and Low Iodine on Biochemical Indexes of the Brain and Learning-Memory of Offspring Rats. Fluoride. 2004;37:201–208. [Google Scholar]
- 30.Hong J.H., Ge Y.M., Ning H.M. Effects of High Fluoride and Low Iodine on Learning-Memory and TchE of Brain in Offspring Rats. China Prev. Med. 2005;6:489–491. [Google Scholar]
- 31.Mioto V.C.B., de Castro Nassif Gomes Monteiro A.C., De Camargo R.Y.A., Borel A.R., Catarino R.M., Kobayashi S., Chammas M.C., Marui S. High Prevalence of Iodine Deficiency in Pregnant Women Living in Adequate Iodine Area. Endocr. Connect. 2018;7:762–767. doi: 10.1530/EC-18-0131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Perrine C.G., Herrick K.A., Gupta P.M., Caldwell K.L., Activity P., Surveys N.E. Iodine Status of Pregnant Women and Women of Reproductive Age in the United States. Thyroid. 2019;29:153–154. doi: 10.1089/thy.2018.0345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Green R., Rubenstein J., Popoli R., Capulong R., Till C. Sex-Specific Neurotoxic Effects of Early-Life Exposure to Fluoride: A Review of the Epidemiologic and Animal Literature. Curr. Epidemiol. Rep. 2020;7:263–273. doi: 10.1007/s40471-020-00246-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Arbuckle T.E., Fraser W.D., Fisher M., Davis K., Liang C.L., Lupien N., Bastien S., Velez M.P., Von Dadelszen P., Hemmings D.G., et al. Cohort Profile: The Maternal-Infant Research on Environmental Chemicals Research Platform. Paediatr. Perinat. Epidemiol. 2013;27:415–425. doi: 10.1111/ppe.12061. [DOI] [PubMed] [Google Scholar]
- 35.Li F., Wan S., Zhang L., Li B., He Y., Shen H., Liu L. A Meta-Analysis of the Effect of Iodine Excess on the Intellectual Development of Children in Areas with High Iodine Levels in Their Drinking Water. Biol. Trace Elem. Res. 2022;200:1580–1590. doi: 10.1007/s12011-021-02801-3. [DOI] [PubMed] [Google Scholar]
- 36.World Health Organization . WHO Global Database on Iodine Deficiency. Department of Nutrition for Health and Development World Health Organization; Geneva, Switzerland: 2004. Worldwide Iodine Status. [Google Scholar]
- 37.Luo J., Li C., Zhang X., Shan Z., Teng W. Reference Intervals of the Ratio of Urine Iodine to Creatinine in Pregnant Women in an Iodine-Replete Area of China. Biol. Trace Elem. Res. 2020;199:62–69. doi: 10.1007/s12011-020-02133-8. [DOI] [PubMed] [Google Scholar]
- 38.Till C., Green R., Grundy J.G., Hornung R., Neufeld R., Martinez-Mier E.A., Ayotte P., Muckle G., Lanphear B. Community Water Fluoridation and Urinary Fluoride Concentrations in a National Sample of Pregnant Women in Canada. Environ. Health Perspect. 2018;126:107001. doi: 10.1289/EHP3546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Martínez-Mier E.A., Cury J.A., Heilman J.R., Katz B.P., Levy S.M., Li Y., Maguire A., Margineda J., O’Mullane D., Phantumvanit P., et al. Development of Gold Standard Ion-Selective Electrode-Based Methods for Fluoride Analysis. Caries Res. 2011;45:3–12. doi: 10.1159/000321657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Zimmermann M.B., Andersson M. Assessment of Iodine Nutrition in Populations: Past, Present, and Future. Nutr. Rev. 2012;70:553–570. doi: 10.1111/j.1753-4887.2012.00528.x. [DOI] [PubMed] [Google Scholar]
- 41.Li C., Peng S., Zhang X., Xie X., Wang D., Mao J., Teng X., Shan Z., Teng W. The Urine Iodine to Creatinine as an Optimal Index of Iodine during Pregnancy in an Iodine Adequate Area in China. J. Clin. Endocrinol. Metab. 2016;101:1290–1298. doi: 10.1210/jc.2015-3519. [DOI] [PubMed] [Google Scholar]
- 42.Caldwell B.M., Bradley R.H. Home Observation for Measurement of the Environment. University of Arkansas; Little Rock, AR, USA: 1979. [Google Scholar]
- 43.Bauer D.J., Curran P.J., Thurstone L.L. Probing Interactions in Fixed and Multilevel Regression: Inferential and Graphical Techniques. Multivariate Behav. Res. 2005;40:373–400. doi: 10.1207/s15327906mbr4003_5. [DOI] [PubMed] [Google Scholar]
- 44.Van Mil N.H., Tiemeier H., Bongers-Schokking J.J., Ghassabian A., Hofman A., Hooijkaas H., Jaddoe V.W.V., de Muinck Keizer-Schrama S.M., Steegers E.A.P., Visser T.J., et al. Low Urinary Iodine Excretion during Early Pregnancy Is Associated with Alterations in Executive Functioning in Children. J. Nutr. 2012;142:2167–2174. doi: 10.3945/jn.112.161950. [DOI] [PubMed] [Google Scholar]
- 45.Du Y., Zhou G., Gong B., Ma J., An N., Gao M., Yang M., Ma Q., Huang H., Zuo Q., et al. Iodine Modifies the Susceptibility of Thyroid to Fluoride Exposure in School-Age Children: A Cross-Sectional Study in Yellow River Basin, Henan, China. Biol. Trace Elem. Res. 2021;199:3658–3666. doi: 10.1007/s12011-020-02519-8. [DOI] [PubMed] [Google Scholar]
- 46.Ge Y., Niu R., Zhang J., Wang J. Proteomic Analysis of Brain Proteins of Rats Exposed to High Fluoride and Low Iodine. Arch. Toxicol. 2011;85:27–33. doi: 10.1007/s00204-010-0537-5. [DOI] [PubMed] [Google Scholar]
- 47.Ge Y., Ning H., Wang S., Wang J. Effects of High Fluoride and Low Iodine on Brain Histopathology in Offspring Rats. Fluoride. 2005;38:127–132. [Google Scholar]
- 48.Ge Y., Ning H., Feng C., Wang H., Yan X., Wang S., Wang J. Apoptosis in Brain Cells of Offspring Rats Exposed to High Fluoride and Low Iodine. Fluoride. 2006;39:173–178. [Google Scholar]
- 49.Malin A.J., Riddell J., McCague H., Till C. Fluoride Exposure and Thyroid Function among Adults Living in Canada: Effect Modification by Iodine Status. Environ. Int. 2018;121:667–674. doi: 10.1016/j.envint.2018.09.026. [DOI] [PubMed] [Google Scholar]
- 50.Waugh D.T. Fluoride exposure induces inhibition of sodium/iodide symporter (NIS) contributing to impaired iodine absorption and iodine deficiency: Molecular mechanisms of inhibition and implications for public health. Int. J. Environ. Res. Public Health. 2019;16:1086. doi: 10.3390/ijerph16061086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Singh N., Verma K.G., Verma P., Sidhu G.K., Sachdeva S. A comparative study of fluoride ingestion levels, serum thyroid hormone & TSH level derangements, dental fluorosis status among school children from endemic and non-endemic fluorosis areas. Springerplus. 2014;3:7. doi: 10.1186/2193-1801-3-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Zhao W., Zhu H., Yu Z., Aoki K., Misumi J., Zhang X. Long-Term Effects of Various Iodine and Fluorine Doses on the Thyroid and Fluorosis in Mice. Endocr. Regul. 1998;32:63–70. [PubMed] [Google Scholar]
- 53.Guan Z.Z., Zhuang Z.-J., Yang P.-S., Pan S. Synergistic Action of Iodine-Deficiency and Fluorine-Intoxication of Rat Thyroid. Chin. Med. J. 1988;101:679–684. [PubMed] [Google Scholar]
- 54.Rovet J.F. The Role of Thyroid Hormones for Brain Development and Cognitive Function. Endocr. Dev. 2014;26:26–43. doi: 10.1159/000363153. [DOI] [PubMed] [Google Scholar]
- 55.Moog N.K., Entringer S., Heim C., Wadhwa P.D., Kathmann N., Buss C. Influence of Maternal Thyroid Hormones during Gestation on Fetal Brain Development. Neuroscience. 2017;342:68–100. doi: 10.1016/j.neuroscience.2015.09.070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Prezioso G., Giannini C., Chiarelli F. Effect of Thyroid Hormones on Neurons and Neurodevelopment. Horm. Res. Paediatr. 2018;90:73–81. doi: 10.1159/000492129. [DOI] [PubMed] [Google Scholar]
- 57.Jansen T.A., Korevaar T.I.M., Mulder T.A., White T., Muetzel R.L., Peeters R.P., Tiemeier H. Maternal Thyroid Function during Pregnancy and Child Brain Morphology: A Time Window-Specific Analysis of a Prospective Cohort. Lancet Diabetes Endocrinol. 2019;7:629–637. doi: 10.1016/S2213-8587(19)30153-6. [DOI] [PubMed] [Google Scholar]
- 58.Miranda A., Sousa N. Maternal Hormonal Milieu Influence on Fetal Brain Development. Brain Behav. 2018;8:e00920. doi: 10.1002/brb3.920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Zimmermann M.B. The Effects of Iodine Deficiency in Pregnancy and Infancy. Paediatr. Perinat. Epidemiol. 2012;26:108–117. doi: 10.1111/j.1365-3016.2012.01275.x. [DOI] [PubMed] [Google Scholar]
- 60.Hall M., Green R., Goodman C.V., Farmus L., Lanphear B., Martinez-Mier A., Hornung R., Ayotte P., Till C. Fluoride Exposure and Hypothyroidism in a Canadian Pregnancy Cohort. Birth Defects Res. 2021;113:804. [Google Scholar]
- 61.Batista G., Hensch T.K. Critical Period Regulation by Thyroid Hormones: Potential Mechanisms and Sex-Specific Aspects. Front. Mol. Neurosci. 2019;12:77. doi: 10.3389/fnmol.2019.00077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Duarte-Guterman P., Navarro-Martín L., Trudeau V.L. Mechanisms of Crosstalk between Endocrine Systems: Regulation of Sex Steroid Hormone Synthesis and Action by Thyroid Hormones. Gen. Comp. Endocrinol. 2014;203:69–85. doi: 10.1016/j.ygcen.2014.03.015. [DOI] [PubMed] [Google Scholar]
- 63.Baksi S., Pradhan A. Thyroid Hormone: Sex-Dependent Role in Nervous System Regulation and Disease. Biol. Sex Differ. 2021;12:25. doi: 10.1186/s13293-021-00367-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Li P., Teng Y., Ru X., Liu Z., Han Y., Tao F., Huang K. Sex-Specific Effect of Maternal Thyroid Hormone Trajectories on Preschoolers’ Behavioral Development: A Birth Cohort Study. J. Clin. Endocrinol. Metab. 2022;107:e2037–e2046. doi: 10.1210/clinem/dgab887. [DOI] [PubMed] [Google Scholar]
- 65.König F., Andersson M., Hotz K., Aeberli I., Zimmermann M.B. Ten Repeat Collections for Urinary Iodine from Spot Samples or 24-Hour Samples Are Needed to Reliably Estimate Individual Iodine Status in Women. J. Nutr. 2011;141:2049–2054. doi: 10.3945/jn.111.144071. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Anonymized data described in the manuscript are available to qualified investigators with IRB approval.