

Abstract
Introduction:
Bartonella quintana is an anaerobic bacillus whose main target is the erythrocyte. This bacterium transmitted by the body louse notably infected the soldiers of the First World War from where the name of this disease: fever of the trenches. The 90s marked the return of this bacterial infection. B. quintana infection in the homeless was reported in the literature with a high incidence in these populations worldwide. This upsurge of cases justified this study for a better understanding of B. quintana infections.
Methods:
We conducted a systematic review to evaluate the seroprevalence of B. quintana infection by using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to collect scientific papers from PubMed and Google Scholar based on combining keywords.
Results:
The review included 45 articles published from April 1996 to March 2020 with 84 subpopulations of 21 countries from 4 continents; among them, 61 subpopulations had a positive rate from 0.2% to 65%. These subpopulations were divided into four main groups: homeless people, healthy people, blood donors, and symptoms/diseases. Homeless people were the main target of this infection, and three factors related to susceptibility were homeless period, age, and alcoholism. 6/11, 12/20, and 32/41 subpopulations of healthy people, blood donors, symptoms/diseases, respectively, had a positive percentage. However, factors of exposure in these three groups were not mentioned. Other reservoirs, vectors, and transmitted routes were identified to partially explain the worldwide spread of the infection, and it is important to have more further investigations to identify potential risk factors. This will help to limit contamination and prevent effectively.
Conclusions:
This serological overview indicated the importance of B. quintana infection that has emerged in multiple regions, touched worldwide populations.
Keywords: Bartonella quintana, infection, seroprevalence
INTRODUCTION
Bartonella quintana is a fastidious Gram-negative bacterium and the pathogen of trench fever, a disease that has the transmission from human to human through the body louse (Pediculus humanus corporis).[1] Trench fever caused epidemics worldwide and affected several million people during two World Wars, but the incidence decreased significantly after the end of each World War.[1,2] After the incubation period from 15 to 25 days, the most frequent symptoms are acute high fever, dizziness, headache, bone pain, and a relapsing febrile every 4–6 days, thus it was called “quintana fever.”[3] Although trench fever often caused a prolonged disability, the death was rare.[4] Other manifestations of B. quintana infection were reported, such as chronic bacteremia, endocarditis, bacillary angiomatosis, and lymphadenopathy.[2,5] Human is the natural reservoir host, in which the bacterium persists durably in erythrocytes, erythroblasts with the percentage of infected cells being very low.[6] Since the 1990s, B. quintana was recognized as a major re-emerging agent in urban homeless people due to poor living conditions and alcoholism. These factors promote high exposure to B. quintana by ectoparasites that are the vector of transmission.[3,7] Recently, there have been some scientific reports of B. quintana infection with a high rate of exposure from various subpopulations.[8,9,10]
There are many different tests for diagnosing B. quintana infection based on clinical characteristics, but to assess the incidence in the community for epidemiological studies, serologic test using immunoglobulin G (IgG) and IgM titers is the most widely used method.[2] We conducted this systematic review of seroprevalence to evaluate the rate of B. quintana infection over the past 25 years.
METHODS
Search strategy and selection criteria
The seroprevalence review was conducted according to guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The databases were searched and collected before March 2020 on PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) and Google Scholar (http://scholar.google.com/). The most recent article was published in Mars 2020. The keywords used for searching the databases were followed:
#1: “antibodies” OR “serology” OR “seroprevalence” OR “seroreactivity” OR “epidemiology” OR “prevalence”.
#2: “Bartonella spp.” OR “Bartonella quintana” OR “trench fever”.
Searched by: #1 AND #2.
Only articles published in English were referred and references from selected articles were also screened to avoid missing data. After evaluating the abstracts, the full texts were assessed for having the correct selection in this review. Exclusion criteria were as follows: (1) some studies used the same samples, and only one study was considered, and (2) not mentioned B. quintana.
To evaluate the percentage of B. quintana infection in population, we used both IgG and IgM titers. Depending on the manufacturer, serum threshold detected is different between articles.
Data collection
The data were collected from each article: year of publishing, countries, sample size, positive percentage, IgG titer, IgM titer, and P-value if compared with group control.
Data analysis
As a result of the heterogeneity of subpopulations and the nature of studies, we could not have a meta-analysis, hence described the main outcomes such as prevalence and related factors. Hence the main outcomes of this review were the prevalence and related factors of the bacterial infection
RESULTS
A total of 705 articles were selected through database searching and six additional articles were found through the references. After screening the titles and abstracts, 70 papers were analyzed full text; among them, 24 papers were excluded and 46 articles were qualified for this systematic review [Figure 1]. A total of 21 countries of 4 continents had the serological surveys, in detail: Africa has one article for each country (Algeria, Burundi, Congo, and Tunisia), Asia is the same (Japan, Thailand, Jordan, and Korea), America has 9 articles (5 in the US, 2 in Brazil, 1 in Peru, and 1 in Colombia), and Europe has 29 articles (10 in France, 6 in Sweden, 4 in Poland, 2 in Greece, 3 in Spain, and 1 for each country: Austria, Croatia, Denmark, and the UK). These studies were published from April 1996 to Mars 2020 and conducted on 84 subpopulations, and among them, 61 subpopulations had a positive proportion, equal 72.6% [Table 1]. We divided these subpopulations into four main groups: healthy people, blood donors, homeless people, and symptoms/diseases. In healthy people, 6/11 subpopulations had an infection with the rate from 1.4% to 25% and the highest was hunters [Figure 2]. Blood donors indicated 12/20 studies from 10 countries having positive sera between 0.2% and 50.5% [Figure 3]. In the homeless group with 12 subpopulations, only intravenous drug users were negative, but the number of participants in this study was only six. The rest had a positive rate from 1.8% to 65%, remarkably homeless patients cutaneous parasitic, homeless blood culture positive, Japanese homeless people had the positive rate over 50% [Figure 4]. In the symptoms/diseases group, 32/41 subpopulations had a positive prevalence between 0.5% and 64.5%, the highest in patients regional lymphadenopathy [Figure 5].
Figure 1.
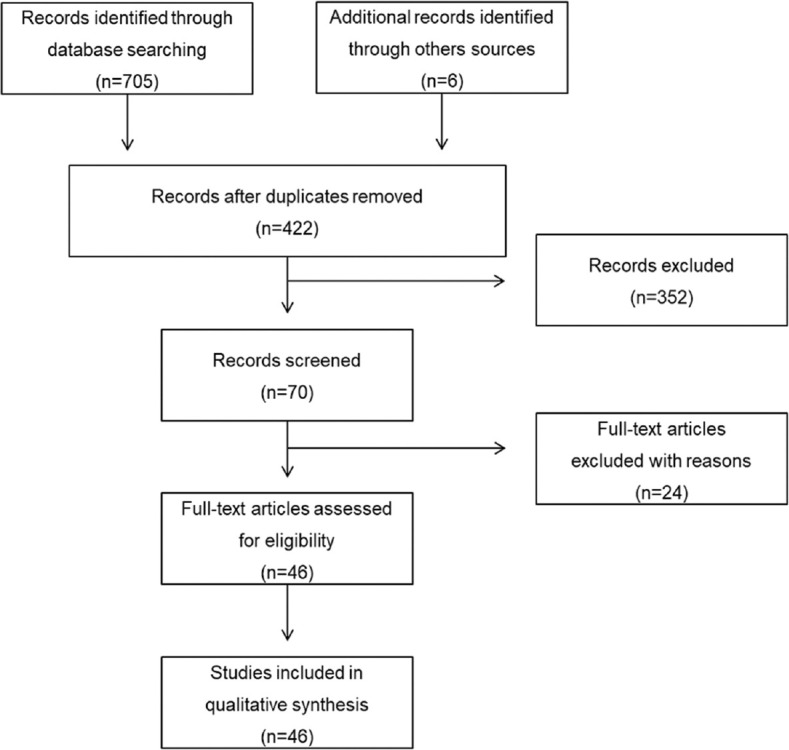
Flow diagram of the search strategy
Table 1.
Bartonella quintana seroprevalence among different subpopulations by chronological order of publication
| Year | References | Countries | Subpopulations | n | IgG (%) | IgM (%) | Percentage | P |
|---|---|---|---|---|---|---|---|---|
| 1996 | [14] | US | Patients | 192 | 20.3 | NA | 20.3 | <0.001 |
| Blood donors | 199 | 2 | NA | 2.0 | ||||
| 1996 | [13] | US | Intravenous drug users | 630 | 10 | NA | 10 | |
| 1996 | [12] | France | Homeless people | 221 | 1.8 | 0 | 1.8 | <0.05 |
| Blood donors | 250 | 0.0 | 0 | 0.0 | ||||
| Hospitalized homeless patients | 43 | 16.3 | 2.3 | 16.3 | <0.01 | |||
| Hospitalized patients | 57 | 0 | 0 | 0 | ||||
| 1996 | [30] | France | Patients suspected cat scratch disease | 64 | 9.4 | NA | 9.4 | |
| 1998 | [31] | Sweden | Chlamydophila pneumoniae IgG positive patients | 61 | 0 | NA | 0 | |
| 1998 | [32] | Burundi | Sutama patients | 102 | 12.7 | NA | 12.7 | NA |
| Febrile refugees | 232 | 8.2 | NA | 8.2 | ||||
| 1999 | [4] | France | Homeless patients | 71 | 29.6 | NA | 29.6 | <0.001 |
| Patients | 31 | 0.0 | NA | 0.0 | ||||
| Blood donors | 250 | 0.0 | NA | 0.0 | ||||
| 1999 | [33] | Sweden | Patients | 109 | 2.8 | NA | 2.8 | NA |
| Blood donors | 100 | 0.0 | NA | 0.0 | ||||
| 1999 | [16] | UK | Probable cat scratch disease | 565 | 13.1 | 1.4 | 13.8 | NA |
| Possible cat scratch disease | 48 | 8.3 | 2.1 | 10.4 | ||||
| Bacillary angiomatosis/peliosis | 37 | 5.4 | NA | 5.4 | ||||
| Blood culture-negative endocarditis | 66 | 15.2 | 7.6 | 16.7 | ||||
| Ophthalmic involvement | 17 | 17.6 | NA | 17.6 | ||||
| “Not appropriate” patients | 143 | 2.8 | NA | 2.8 | ||||
| “No details” patients | 124 | 9.7 | 1.6 | 10.5 | ||||
| Blood donors | 200 | 1.5 | 0 | 1.5 | ||||
| Healthy adult contact | 36 | 0 | 0 | 0 | ||||
| Toxoplasmosis | 16 | 0 | 0 | 0 | ||||
| Mumps virus | 13 | 0 | 7.7 | 7.7 | ||||
| Streptococcus pyogenes serology | 8 | 0 | 0 | 0 | ||||
| EBV | 11 | 0 | 9.1 | 9.1 | ||||
| Chlamydia spp. | 5 | 0 | 0 | 0 | ||||
| 1999 | [17] | Peru | Inhabitants | 194 | 12.4 | NA | 12.4 | <0.05 |
| Peasants | 84 | 0 | NA | 0.0 | ||||
| 2001 | [34] | US | Intravenous drug users | 204 | 2.0 | NA | 2.0 | |
| 2001 | [19] | France | Homeless patients cutaneous parasitic | 57 | 54.4 | 5.3 | 54.4 | <0.001 |
| Blood donors | 53 | 1.9 | 0 | 1.9 | ||||
| 2001 | [22] | Sweden | Elite orienteers | 1136 | 1.4 | NA | 1.4 | >0.05 |
| Blood donors | 322 | 0.3 | NA | 0.3 | ||||
| 2002 | [3] | France | Homeless blood culture positive | 40 | 65.0 | NA | 65.0 | <0.05 |
| Homeless blood culture negative | 82 | 19.5 | NA | 19.5 | ||||
| 2002 | [35] | Korea | Patients regional lymphadenopathy | 31 | 64.5 | NA | 64.5 | |
| 2002 | [36] | US | Patients | 200 | 9.5 | NA | 9.5 | |
| 2003 | [20] | France | Patients pericardial effusion | 204 | 0.5 | NA | 0.5 | >0.05 |
| Blood donors | 260 | 0.0 | NA | 0.0 | ||||
| 2003 | [37] | Sweden | Autopsy of heroin addicts | 59 | 3.4 | NA | 3.4 | NA |
| Forensic autopsy | 44 | 0.0 | NA | 0.0 | ||||
| 2003 | [10] | Greece | Blood donors | 500 | 15.0 | 0 | 15.0 | |
| 2003 | [38] | Poland | Bartonellosis patients | 265 | 1.5 | 0.4 | 1.9 | |
| 2004 | [39] | Denmark | Elite orienteers | 43 | 0.0 | 0 | 0 | NA |
| Blood donors | 159 | 0.0 | 0 | 0 | ||||
| Elite indoor sportsmen | 63 | 0.0 | 0 | 0 | ||||
| 2004 | [40] | Jordan | Children patients | 482 | 4.1 | NA | 4.1 | |
| 2005 | [8] | Brazil | Healthy individuals | 437 | 12.8 | NA | 12.8 | |
| 2005 | [41] | Algeria | Suspected endocarditis | 61 | 11.5 | NA | 11.5 | |
| 2005 | [42] | France | Blood culture-negative endocarditis | 346 | 15.3 | NA | 15.3 | |
| 2005 | [7] | France | Homeless people | 930 | 7.5 | NA | 7.5 | <0.001 |
| Blood donors | 467 | 0.6 | NA | 0.6 | ||||
| 2005 | [43] | Tunisia | Blood culture-negative endocarditis | 40 | 30.0 | NA | 30.0 | |
| 2005 | [44] | Sweden | Blood donors | 498 | 0.2 | NA | 0.2 | |
| 2005 | [45] | Greece | HIV patients | 253 | 5.9 | 0 | 5.9 | |
| 2006 | [18] | Japan | Homeless people | 151 | 57.0 | 0 | 57.0 | <0.05 |
| Blood donors | 200 | 50.5 | 0 | 50.5 | ||||
| 2007 | [46] | Poland | Homeless alcoholic | 29 | 6.9 | 3.4 | 6.9 | NA |
| Homeless intravenous drug users | 6 | 0.0 | 0 | 0.0 | ||||
| Blood donors | 50 | 0.0 | 0 | 0.0 | ||||
| 2008 | [47] | Sweden | Homeless people | 48 | 4.2 | NA | 4.2 | NA |
| Blood donors | 61 | 1.6 | NA | 1.6 | ||||
| 2008 | [48] | France | Uveitis | 1321 | 0.5 | NA | 0.5 | NA |
| Blood donors | 260 | 0.0 | NA | 0.0 | ||||
| 2008 | [49] | Spain | HIV patients | 340 | 12.9 | NA | 12.9 | |
| 2011 | [50] | Thailand | Febrile patients | 423 | 3.3 | NA | 3.3 | NA |
| Nonfebrile patients | 98 | 3.1 | NA | 3.1 | ||||
| 2011 | [51] | Congo | Patients | 155 | 0.6 | NA | 0.6 | |
| 2012 | [52] | Croatia | Lymphadenopathy patients | 268 | 8.6 | NA | 8.6 | |
| 2013 | [53] | Poland | Patients suggesting Bartonella spp. infection | 663 | 0.0 | 0 | 0.0 | |
| 2014 | [54] | France | Blood donors | 472 | 0.0 | NA | 0.0 | |
| 2015 | [55] | Brazil | Blood donors | 500 | 32.0 | NA | 32.0 | |
| 2016 | [56] | US | Adults | 197 | 0.0 | NA | 0.0 | |
| 2016 | [9] | Austria | Hunters | 100 | 25.0 | NA | 25.0 | >0.05 |
| Blood donors | 100 | 27.0 | NA | 27.0 | ||||
| 2017 | [57] | Colombia | Homeless people | 153 | 12.4 | NA | 12.4 | |
| 2017 | [58] | Spain | Veterinarians | 89 | 11.2 | NA | 11.2 | |
| 2019 | [21] | Poland | Musculoskeletal patients | 40 | 0.0 | 0 | 0 | >0.05 |
| Blood donors | 65 | 4.6 | 1.5 | 4.6 | ||||
| 2020 | [59] | Spain | Sanitary workers | 97 | 16.5 | NA | 16.5 |
NA: Not applicated
Figure 2.
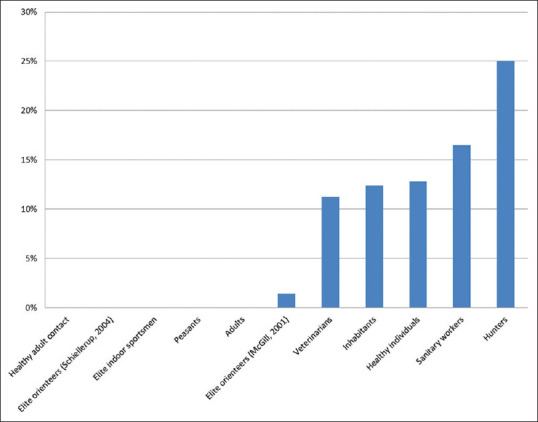
Seroprevalence diagram of healthy people
Figure 3.
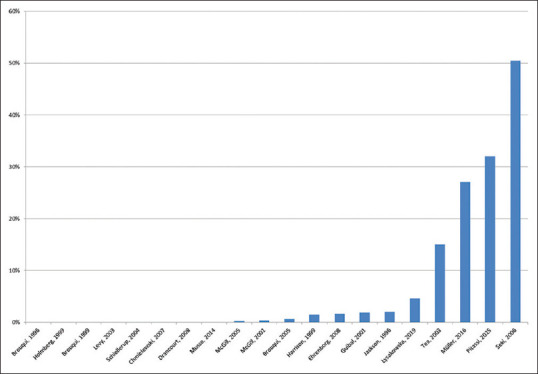
Seroprevalence diagram of blood donors
Figure 4.
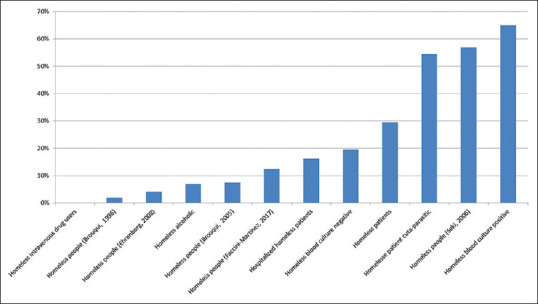
Seroprevalence diagram of homeless people
Figure 5.

Seroprevalence diagram of symptoms/diseases
DISCUSSION
In the 1st years of the 90s, several studies on some patient cases reported that B. quintana caused bacillary angiomatosis, endocarditis, and chronic lymphadenopathy, but in 1993, an outbreak of bacteremia occurred in 10 homeless alcoholics.[11] Three years later, several serosurveys on a large number of indigent population in France and the US suggested a significant proportion of B. quintana infection.[12,13,14]
The return of the common disease in World War required an easy-to-apply approach to diagnose the disease. The isolation of B. quintana has been a difficult challenge; the detection of antibodies remains the most practical test for diagnosis of Bartonella infection in the case of inaccessible tissue.[15] While IgG reflects the evidence of past infection at an undetermined time, IgM shows the recent or current infection,[16] hence all articles used IgG and only 11 articles added IgM. 60/84 subpopulations detected IgG for diagnostic threshold and 11/31 subpopulations had IgM positive with some cases, only having two subpopulations with two patients positive with IgM without IgG. Apparently, IgM assisted IgG in diagnosing infection related to epidemiological research of B. quintana.
As the large scale of geographic human subpopulations were exposed to B. quintana around the world, the majority of homeless subpopulations had a positive percentage higher in comparison with group controls that was elucidated by the proof of the body louse being the suitable vector for transmission and highly prevalent in this group.[7,17] For homeless people, independent factors that influenced to significant serological levels were the length of homeless period with more than 1 year[18] or 3 years and the age of homeless people above 40 years,[19] alcohol abuse.[14] In other groups, only one investigation showed that B. quintana antibodies in villagers having a factor of “louse infected” were significantly higher in peasants and ectoparasitic infestation had a meaningful correlation with highest altitude village and women;[19] four studies had the comparison between two subpopulations but no difference of seroprevalence.[9,20,21,22] Not mentioned to homeless people, we noticed that 12/20 subpopulations of blood donor group, 6/11 subpopulations of healthy group, and 32/41 subpopulations of symptoms/diseases group with a totoal of 50/72 subpopulations surveyed from four continents had positive proportion; remarkably, 28 subpopulations had an exposure rate at least 10%. These positive subpopulations had no evidence of having risk factors such as unsanitary living conditions, contact with infected lice; thus this infection could be a result of some non-identified under-estimated factors. Fleas could also be involved in this disease because they are responsible for zoonoses on the one hand and B. quintana has already been detected in cat fleas from different sites in France[23] and monkey fleas in Gabon on the other hand.[24] Fleas could be a potential vector of B. quintana alongside the recognized role of human body. Human is not the only reservoir of this Gram-negative bacterium, various studies showed animals were others reservoirs and this bacterium can cause diseases, such as bacteremia in a domestic cat,[25] in wild Japanese macaques,[26] in rhesus macaques,[27] endocarditis in dogs.[28] Following a serological study, the positive percentage with B. quintana was 36.4% in healthy rhesus macaque.[27] An experimental study showed a similar mechanism of transmission in human that B. quintana located in the gastrointestinal tract of cat fleas and released into feces.[29] Rhesus macaques are susceptible to B. quintana and Polyptychoides obtusus lice acted as the vector of transmission among this primate.[60] From feces of infected lice, B. quintana penetrates into human body through altered skin. However, other evidence revealed that cat bites or insect bites can transmit B. quintana to human, as known that cat is pet closing to human and insects present worldwide.[61,62] Thus, various reservoirs, vectors, and transmitted ways were detected to help understand more about B. quintana infection, but there are still many issues that have not been clarified yet to explain how B. quintana exposure on over the world.
CONCLUSIONS
In the last 25 years, 46 serological investigations with 84 subpopulations on over the world indicated the re-emergence of B. quintana infection. Other reservoirs, vectors, and transmission were mentioned to more understanding of this disease but not enough to explain the worldwide spread. This study showed a serological overview of a common infection that has become a considerable problem of global public health.
Research quality and ethics statement
The authors of this manuscript declare that this scientific work complies with reporting quality, formatting and reproducibility guidelines set forth by the EQUATOR Network (http://www.equator-network.org/).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank Pr. Michel Drancourt and Dr. Gerard Aboudharam (Aix-Marseille University, France) for advices and corrections.
REFERENCES
- 1.Maurin M, Raoult D. Bartonella (Rochalimaea) quintana infections. Clin Microbiol Rev. 1996;9:273–92. doi: 10.1128/cmr.9.3.273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Foucault C, Brouqui P, Raoult D. Bartonella quintana characteristics and clinical management. Emerg Infect Dis. 2006;12:217–23. doi: 10.3201/eid1202.050874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Foucault C, Barrau K, Brouqui P, Raoult D. Bartonella quintana bacteremia among homeless people. Clin Infect Dis. 2002;35:684–9. doi: 10.1086/342065. [DOI] [PubMed] [Google Scholar]
- 4.Brouqui P, Lascola B, Roux V, Raoult D. Chronic Bartonella quintana bacteremia in homeless patients. N Engl J Med. 1999;340:184–9. doi: 10.1056/NEJM199901213400303. [DOI] [PubMed] [Google Scholar]
- 5.Drancourt M, Mainardi JL, Brouqui P, Vandenesch F, Carta A, Lehnert F, et al. Bartonella (Rochalimaea) quintana endocarditis in three homeless men. N Engl J Med. 1995;332:419–23. doi: 10.1056/NEJM199502163320702. [DOI] [PubMed] [Google Scholar]
- 6.Rolain JM, Foucault C, Guieu R, La Scola B, Brouqui P, Raoult D. Bartonella quintana in human erythrocytes. Lancet. 2002;360:226–8. doi: 10.1016/s0140-6736(02)09462-x. [DOI] [PubMed] [Google Scholar]
- 7.Brouqui P, Stein A, Dupont HT, Gallian P, Badiaga S, Rolain JM, et al. Ectoparasitism and vector-borne diseases in 930 homeless people from Marseilles. Medicine (Baltimore) 2005;84:61–8. doi: 10.1097/01.md.0000152373.07500.6e. [DOI] [PubMed] [Google Scholar]
- 8.da Costa PS, Brigatte ME, Greco DB. Antibodies to Rickettsia rickettsii, Rickettsia typhi, Coxiella burnetii, Bartonella henselae, Bartonella quintana, and Ehrlichia chaffeensis among healthy population in Minas Gerais, Brazil. Mem Inst Oswaldo Cruz. 2005;100:853–9. doi: 10.1590/s0074-02762005000800006. [DOI] [PubMed] [Google Scholar]
- 9.Müller A, Reiter M, Schötta AM, Stockinger H, Stanek G. Detection of Bartonella spp.in Ixodes ricinus ticks and Bartonella seroprevalence in human populations. Ticks Tick Borne Dis. 2016;7:763–7. doi: 10.1016/j.ttbdis.2016.03.009. [DOI] [PubMed] [Google Scholar]
- 10.Tea A, Alexiou-Daniel S, Arvanitidou M, Diza E, Antoniadis A. Occurrence of Bartonella henselae and Bartonella quintana in a healthy Greek population. Am J Trop Med Hyg. 2003;68:554–6. doi: 10.4269/ajtmh.2003.68.554. [DOI] [PubMed] [Google Scholar]
- 11.Spach DH, Kanter AS, Dougherty MJ, Larson AM, Coyle MB, Brenner DJ, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995;332:424–8. doi: 10.1056/NEJM199502163320703. [DOI] [PubMed] [Google Scholar]
- 12.Brouqui P, Houpikian P, Dupont HT, Toubiana P, Obadia Y, Lafay V, et al. Survey of the seroprevalence of Bartonella quintana in homeless people. Clin Infect Dis. 1996;23:756–9. doi: 10.1093/clinids/23.4.756. [DOI] [PubMed] [Google Scholar]
- 13.Comer JA, Flynn C, Regnery RL, Vlahov D, Childs JE. Antibodies to Bartonella species in inner-city intravenous drug users in Baltimore, Md. Arch Intern Med. 1996;156:2491–5. [PubMed] [Google Scholar]
- 14.Jackson LA, Spach DH, Kippen DA, Sugg NK, Regnery RL, Sayers MH, et al. Seroprevalence to Bartonella quintana among patients at a community clinic in downtown Seattle. J Infect Dis. 1996;173:1023–6. doi: 10.1093/infdis/173.4.1023. [DOI] [PubMed] [Google Scholar]
- 15.Koehler JE, Sanchez MA, Tye S, Garrido-Rowland CS, Chen FM, Maurer T, et al. Prevalence of Bartonella infection among human immunodeficiency virus-infected patients with fever. Clin Infect Dis. 2003;37:559–66. doi: 10.1086/375586. [DOI] [PubMed] [Google Scholar]
- 16.Harrison TG, Doshi N. Serological evidence of Bartonella spp. infection in the UK. Epidemiol Infect. 1999;123:233–40. doi: 10.1017/s0950268899002927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Raoult D, Birtles RJ, Montoya M, Perez E, Tissot-Dupont H, Roux V, et al. Survey of three bacterial louse-associated diseases among rural Andean communities in Peru: Prevalence of epidemic typhus, trench fever, and relapsing fever. Clin Infect Dis. 1999;29:434–6. doi: 10.1086/520229. [DOI] [PubMed] [Google Scholar]
- 18.Seki N, Sasaki T, Sawabe K, Sasaki T, Matsuoka M, Arakawa Y, et al. Epidemiological studies on Bartonella quintana infections among homeless people in Tokyo, Japan. Jpn J Infect Dis. 2006;59:31–5. [PubMed] [Google Scholar]
- 19.Guibal F, de La Salmonière P, Rybojad M, Hadjrabia S, Dehen L, Arlet G. High seroprevalence to Bartonella quintana in homeless patients with cutaneous parasitic infestations in downtown Paris. J Am Acad Dermatol. 2001;44:219–23. doi: 10.1067/mjd.2001.110062. [DOI] [PubMed] [Google Scholar]
- 20.Levy PY, Corey R, Berger P, Habib G, Bonnet JL, Levy S, et al. Etiologic diagnosis of 204 pericardial effusions. Medicine (Baltimore) 2003;82:385–91. doi: 10.1097/01.md.0000101574.54295.73. [DOI] [PubMed] [Google Scholar]
- 21.Łysakowska ME, Brzezińska O, Szybka M, Konieczka M, Moskwa S, Moskwa S, et al. The seroprevalence of Bartonella spp. in the blood of patients with musculoskeletal complaints and blood donors, Poland: A pilot study. Clin Rheumatol. 2019;38:2691–8. doi: 10.1007/s10067-019-04591-5. [DOI] [PubMed] [Google Scholar]
- 22.McGill S, Wesslen L, Hjelm E, Holmberg M, Rolf C, Friman G. Serological and epidemiological analysis of the prevalence of Bartonella spp. antibodies in Swedish elite orienteers 1992-93. Scand J Infect Dis. 2001;33:423–8. doi: 10.1080/00365540152029882. [DOI] [PubMed] [Google Scholar]
- 23.Rolain JM, Franc M, Davoust B, Raoult D. Molecular detection of Bartonella quintana, B. koehlerae, B. henselae, B. clarridgeiae, Rickettsia felis, and Wolbachia pipientis in cat fleas, France. Emerg Infect Dis. 2003;9:338–42. doi: 10.3201/eid0903.020278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rolain JM, Bourry O, Davoust B, Raoult D. Bartonella quintana and Rickettsia felis in Gabon. Emerg Infect Dis. 2005;11:1742–4. doi: 10.3201/eid1111.050861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.La VD, Tran-Hung L, Aboudharam G, Raoult D, Drancourt M. Bartonella quintana in domestic cat. Emerg Infect Dis. 2005;11:1287–9. doi: 10.3201/eid1108.050101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sato S, Kabeya H, Yoshino A, Sekine W, Suzuki K, Tamate HB, et al. Japanese macaques (Macaca fuscata) as natural reservoir of Bartonella quintana. Emerg Infect Dis. 2015;21:2168–70. doi: 10.3201/eid2112.150632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Huang R, Liu Q, Li G, Li D, Song X, Birtles RJ, et al. Bartonella quintana infections in captive monkeys, China. Emerg Infect Dis. 2011;17:1707–9. doi: 10.3201/eid1709.110133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kelly P, Rolain JM, Maggi R, Sontakke S, Keene B, Hunter S, et al. Bartonella quintana endocarditis in dogs. Emerg Infect Dis. 2006;12:1869–72. doi: 10.3201/eid1212.060724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kernif T, Leulmi H, Socolovschi C, Berenger JM, Lepidi H, Bitam I, et al. Acquisition and excretion of Bartonella quintana by the cat flea, Ctenocephalides felis felis. Mol Ecol. 2014;23:1204–12. doi: 10.1111/mec.12663. [DOI] [PubMed] [Google Scholar]
- 30.Dupon M, Savin De Larclause AM, Brouqui P, Drancourt M, Raoult D, De Mascarel A, et al. Evaluation of serological response to Bartonella henselae, Bartonella quintana and Afipia felis antigens in 64 patients with suspected cat-scratch disease. Scand J Infect Dis. 1996;28:361–6. doi: 10.3109/00365549609037920. [DOI] [PubMed] [Google Scholar]
- 31.Boman J, Söderberg S, Forsberg J, Birgander LS, Allard A, Persson K, et al. High prevalence of Chlamydia pneumoniae DNA in peripheral blood mononuclear cells in patients with cardiovascular disease and in middle-aged blood donors. J Infect Dis. 1998;178:274–7. doi: 10.1086/517452. [DOI] [PubMed] [Google Scholar]
- 32.Raoult D, Ndihokubwayo JB, Tissot-Dupont H, Roux V, Faugere B, Abegbinni R, et al. Outbreak of epidemic typhus associated with trench fever in Burundi. Lancet. 1998;352:353–8. doi: 10.1016/s0140-6736(97)12433-3. [DOI] [PubMed] [Google Scholar]
- 33.Holmberg M, McGill S, Ehrenborg C, Wesslén L, Hjelm E, Darelid J, et al. Evaluation of human seroreactivity to Bartonella species in Sweden. J Clin Microbiol. 1999;37:1381–4. doi: 10.1128/jcm.37.5.1381-1384.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Comer JA, Diaz T, Vlahov D, Monterroso E, Childs JE. Evidence of rodent-associated Bartonella and Rickettsia infections among intravenous drug users from Central and East Harlem, New York City. Am J Trop Med Hyg. 2001;65:855–60. doi: 10.4269/ajtmh.2001.65.855. [DOI] [PubMed] [Google Scholar]
- 35.Chae MB, Lee JY, Kwak YG, Park SH, Lim HJ, Park SW, et al. Prevalence of antibodies to Bartonella henselae and Bartonella quintana in Korean patients with lymphadenopathy. Korean J Infect Dis. 2002;34:305–10. [Google Scholar]
- 36.Smith HM, Reporter R, Rood MP, Linscott AJ, Mascola LM, Hogrefe W, et al. Prevalence study of antibody to ratborne pathogens and other agents among patients using a free clinic in downtown Los Angeles. J Infect Dis. 2002;186:1673–6. doi: 10.1086/345377. [DOI] [PubMed] [Google Scholar]
- 37.McGill S, Rajs J, Hjelm E, Lindquist O, Friman G. A study on forensic samples of Bartonella spp antibodies in Swedish intravenous heroin addicts. APMIS. 2003;111:507–13. doi: 10.1034/j.1600-0463.2003.1110409.x. [DOI] [PubMed] [Google Scholar]
- 38.Podsiadły E, Sokolowska E, Tylewska-Wierzbanowska S. Seroprevalence of Bartonella henselae and Bartonella quintana infections in Poland in 1998-2001. Ann N Y Acad Sci. 2003;990:407–8. doi: 10.1111/j.1749-6632.2003.tb07401.x. [DOI] [PubMed] [Google Scholar]
- 39.Schiellerup P, Dyhr T, Rolain JM, Christensen M, Damsgaard R, Ethelberg S, et al. Low seroprevalence of Bartonella species in Danish elite orienteers. Scand J Infect Dis. 2004;36:604–6. doi: 10.1080/00365540410017617. [DOI] [PubMed] [Google Scholar]
- 40.Al-Majali AM, Al-Qudah KM. Seroprevalence of Bartonella henselae and Bartonella quintana infections in children from Central and Northern Jordan. Saudi Med J. 2004;25:1664–9. [PubMed] [Google Scholar]
- 41.Benslimani A, Fenollar F, Lepidi H, Raoult D. Bacterial zoonoses and infective endocarditis, Algeria. Emerg Infect Dis. 2005;11:216–24. doi: 10.3201/eid1102.040668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Houpikian P, Raoult D. Blood culture-negative endocarditis in a reference center: Etiologic diagnosis of 348 cases. Medicine (Baltimore) 2005;84:162–73. doi: 10.1097/01.md.0000165658.82869.17. [DOI] [PubMed] [Google Scholar]
- 43.Znazen A, Rolain JM, Hammami N, Kammoun S, Hammami A, Raoult D. High prevalence of Bartonella quintana endocarditis in Sfax, Tunisia. Am J Trop Med Hyg. 2005;72:503–7. [PubMed] [Google Scholar]
- 44.McGill S, Wesslén L, Hjelm E, Holmberg M, Auvinen MK, Berggren K, et al. Bartonella spp. seroprevalence in healthy Swedish blood donors. Scand J Infect Dis. 2005;37:723–30. doi: 10.1080/00365540510012152. [DOI] [PubMed] [Google Scholar]
- 45.Pape M, Kollaras P, Mandraveli K, Tsona A, Metallidis S, Nikolaidis P, et al. Occurrence of Bartonella henselae and Bartonella quintana among human immunodeficiency virus-infected patients. Ann N Y Acad Sci. 2005;1063:299–301. doi: 10.1196/annals.1355.047. [DOI] [PubMed] [Google Scholar]
- 46.Chmielewski T, Podsiadły E, Tylewska-Wierzbanowska S. Presence of Bartonella spp. in various human populations. Pol J Microbiol. 2007;56:33–8. [PubMed] [Google Scholar]
- 47.Ehrenborg C, Byström R, Hjelm E, Friman G, Holmberg M. High Bartonella spp. seroprevalence in a Swedish homeless population but no evidence of trench fever. Scand J Infect Dis. 2008;40:208–15. doi: 10.1080/00365540701632972. [DOI] [PubMed] [Google Scholar]
- 48.Drancourt M, Berger P, Terrada C, Bodaghi B, Conrath J, Raoult D, et al. High prevalence of fastidious bacteria in 1520 cases of uveitis of unknown etiology. Medicine (Baltimore) 2008;87:167–76. doi: 10.1097/MD.0b013e31817b0747. [DOI] [PubMed] [Google Scholar]
- 49.Pons I, Sanfeliu I, Nogueras MM, Sala M, Cervantes M, Amengual MJ, et al. Seroprevalence of Bartonella spp. infection in HIV patients in Catalonia, Spain. BMC Infect Dis. 2008;8:58. doi: 10.1186/1471-2334-8-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Bhengsri S, Baggett HC, Peruski LF, Morway C, Bai Y, Fisk TL, et al. Bartonella seroprevalence in rural Thailand. Southeast Asian J Trop Med Public Health. 2011;42:687–92. [PubMed] [Google Scholar]
- 51.Laudisoit A, Iverson J, Neerinckx S, Shako JC, Nsabimana JM, Kersh G, et al. Human seroreactivity against Bartonella species in the democratic republic of Congo. Asian Pac J Trop Med. 2011;4:320–2. doi: 10.1016/S1995-7645(11)60094-1. [DOI] [PubMed] [Google Scholar]
- 52.Vilibic-Cavlek T, Karlovic-Martinkovic D, Ljubin-Sternak S, Tabain I, Persic Z, Mlinaric-Galinovic G. High prevalence of Bartonella henselae and Bartonella quintana antibodies in Croatian patients presenting with lymphadenopathy. Pol J Microbiol. 2012;61:315–7. [PubMed] [Google Scholar]
- 53.Fiecek B, Chmielewski T, Lewandowska G, Tylewska-Wierzbanowska S. Characteristics of Bartonella spp. infections in Poland in the years 2009-2012 identified in the laboratory of National Institute of Public Health – National Institute of Hygiene. Przegl Epidemiol. 2013;67:637–40. 725-7. [PubMed] [Google Scholar]
- 54.Musso D, Broult J, Parola P, Raoult D, Fournier PE. Absence of antibodies to Rickettsia spp., Bartonella spp., Ehrlichia spp. and Coxiella burnetii in Tahiti, French Polynesia. BMC Infect Dis. 2014;14:255. doi: 10.1186/1471-2334-14-255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Pitassi LH, de Paiva Diniz PP, Scorpio DG, Drummond MR, Lania BG, Barjas-Castro ML, et al. Bartonella spp. bacteremia in blood donors from Campinas, Brazil. PLoS Negl Trop Dis. 2015;9:e0003467. doi: 10.1371/journal.pntd.0003467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Lau C, Musso D, Fournier PE, Parola P, Raoult D, Weinstein P. Absence of serological evidence of Rickettsia spp., Bartonella spp., Ehrlichia spp. and Coxiella burnetii infections in American Samoa. Ticks Tick Borne Dis. 2016;7:703–5. doi: 10.1016/j.ttbdis.2016.02.019. [DOI] [PubMed] [Google Scholar]
- 57.Faccini-Martínez ÁA, Márquez AC, Bravo-Estupiñan DM, Calixto OJ, López-Castillo CA, Botero-García CA, et al. Bartonella quintana and typhus group Rickettsiae exposure among homeless persons, Bogotá, Colombia. Emerg Infect Dis. 2017;23:1876–9. doi: 10.3201/eid2311.170341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Oteo JA, Maggi R, Portillo A, Bradley J, García-Álvarez L, San-Martín M, et al. Prevalence of Bartonella spp. by culture, PCR and serology, in veterinary personnel from Spain. Parasit Vectors. 2017;10:553. doi: 10.1186/s13071-017-2483-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Portillo A, Maggi R, Oteo JA, Bradley J, García-Álvarez L, San-Martín M, et al. Bartonella spp.prevalence (serology, culture, and PCR) in sanitary workers in La Rioja Spain. Pathogens. 2020;9:189. doi: 10.3390/pathogens9030189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Li H, Liu W, Zhang GZ, Sun ZZ, Bai JY, Jiang BG, et al. Transmission and maintenance cycle of Bartonella quintana among rhesus macaques, China. Emerg Infect Dis. 2013;19:297–300. doi: 10.3201/eid1902.120816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Bergmans AM, Coenen JL, Bakhuizen R, Mooi BW, Ramdat Misier AR, Wilbrink B, et al. Endocarditis in a Dutch patient caused by Bartonella quintana. Clin Microbiol Infect. 1997;3:692–5. doi: 10.1111/j.1469-0691.1997.tb00480.x. [DOI] [PubMed] [Google Scholar]
- 62.Breitschwerdt EB, Maggi RG, Sigmon B, Nicholson WL. Isolation of Bartonella quintana from a woman and a cat following putative bite transmission. J Clin Microbiol. 2007;45:270–2. doi: 10.1128/JCM.01451-06. [DOI] [PMC free article] [PubMed] [Google Scholar]