

Abstract
Social biases may influence providers’ judgments related to pre-exposure prophylaxis (PrEP) and patients’ consequent PrEP access. US primary and HIV care providers (n = 370) completed an experimental survey. Each provider reviewed one fictitious medical record of a patient seeking PrEP. Records varied by patient race (Black or White) and risk behavior (man who has sex with men [MSM], has sex with women [MSW], or injects drugs [MID]). Providers reported clinical judgments and completed measures of prejudice. Minimal evidence of racially biased judgments emerged. Providers expressing low-to-moderate sexual prejudice judged the MSM as more likely than the MSW to adhere to PrEP, which was associated with greater PrEP prescribing intention; sexual prejudice was negatively associated with anticipated MSM adherence. Providers judged the MID to be at higher risk, less likely to adhere, less safety-conscious, and less responsible than both the MSM and MSW; adverse adherence and responsibility judgments were associated with lower prescribing intention.
Keywords: HIV, Pre-exposure prophylaxis, Health personnel, Prejudice, Clinical decision-making
Resumen
Los sesgos sociales pueden influir sobre los juicios de proveedores de salud con respecto a la profilaxis pre-exposición (PrEP) y el consecuente acceso de los pacientes a PrEP. Proveedores de cuidados primarios y de VIH en los Estados Unidos (n = 370) respondieron una encuesta experimental. Cada proveedor leyó una historia médica de un paciente ficticio interesado en obtener PrEP. Las historias médicas variaron la raza (Negro o Blanco) y conducta de riesgo (hombre que tiene sexo con hombres [HSH], hombre que tiene sexo con mujeres [HSM], u hombre usuario de drogas inyectables [HDI]) del paciente. Los proveedores reportaron juicios clínicos y completaron medidas sobre prejuicio. La evidencia sobre sesgos raciales en los juicios clínicos fue mínima. Los proveedores que expresaron prejuicio sexual bajo a moderado, juzgaron que el paciente HSH tendría mayor adherencia a PrEP que el paciente HSM, lo cual se asoció con mayor intención de prescribir PrEP; el prejuicio sexual se asoció negativamente con la adherencia anticipada en HSH. El paciente HDI fue percibido como en mayor riesgo, con menor adherencia, menos preocupado por la seguridad, y menos responsable que los HSH y HSM; los juicios sobre baja adherencia y responsabilidad estuvieron asociados con menor intención de prescribir PrEP.
Introduction
Pre-exposure prophylaxis (PrEP) is a promising form of HIV prevention [1–4]. The US Centers for Disease Control and Prevention (CDC), US Preventive Services Task Force, and other health authorities recommend PrEP for people at risk for HIV due to sexual activity, injection drug use, or both [5–7]. However, disparities in PrEP implementation across risk groups have emerged. For example, US surveillance data suggests that 50% of men who have sex with men (MSM) recently discussed PrEP with their healthcare providers, compared with only 1% of heterosexuals and 5% of people who inject drugs (PWID) [8]. Other social disparities have also been documented with respect to patient-provider communication about PrEP and PrEP prescription, including racial disparities disadvantaging Black people relative to White people [9, 10]. Early research suggests that provider biases could contribute to these disparities by affecting clinical judgments related to PrEP prescription [11–13]. In the present study, we examined practicing US providers’ biases in PrEP clinical decision-making based on patient race, sexual orientation, and injection drug use by conducting an experimental survey in which we systematically varied key pieces of information in a fictitious medical record of a male patient seeking PrEP and asked providers to make judgments about the hypothetical patient. We also assessed the potential moderating effects of explicit and implicit prejudice.
Background
Providers play a fundamental role in determining PrEP access, operating as gatekeepers to this prescription-based medication. In many health settings, PrEP is not routinely discussed with or offered to patients [14–17]. Although federal recommendations for determining PrEP candidacy among MSM, heterosexually active men and women, and PWID have been issued [5, 6], PrEP discussion and prescription still relies heavily on providers’ discretion, allowing for social biases to manifest in clinical judgments [18, 19]. Social bias refers to an unfair response to a social group—generally delineated based on distinguishing social characteristics like race or sexual orientation—that devalues or disadvantages that group and its members [20]. In a healthcare context, social biases can involve unfair judgments or assumptions made about a patient or unfair treatment of a patient based on the patient’s social characteristics.
In the realm of PrEP service delivery, providers’ social biases sometimes manifest overtly, as demonstrated by providers demeaning patients and denying their request for PrEP because of their sexuality [21, 22]. Providers’ biases may also operate unconsciously and be subtle in nature but nonetheless impact assessment of a patient’s PrEP candidacy or intention to prescribe PrEP for a patient. For example, providers have frequently identified concerns about increased condomless sex as a barrier to prescribing PrEP [17], but this concern appears to be applied more commonly to MSM patients than heterosexual patients with reproductive goals, suggesting that sexual prejudice may underlie this differential judgment [23, 24].
Theory-guided, experimental research can help to enhance present understanding of the nature and scope of providers’ biases in PrEP-related clinical decision-making, including potential mechanisms via which patients’ race and other characteristics might lead to inequitable prescription practices. van Ryn et al. developed and later expanded a theoretical model explaining the social-cognitive processes through which, in the context of entrenched societal racism, patients’ race can activate providers’ racial biases and adversely affect clinical decision-making, ultimately contributing to treatment inequities [25, 26]. According to this model, the race of a patient influences a provider’s beliefs about the patient and interpretation of the patient’s presenting symptoms and concerns. These judgments inform the provider’s subsequent clinical decision-making, including their treatment recommendations [25, 26]. Individual provider characteristics, such as explicit and implicit racial prejudice, are theorized to moderate this indirect pathway between patient race and clinical decision-making [26].
Three previous studies have experimentally examined the impact of patient race and other characteristics on PrEP-related clinical decision-making [11–13], one of which also explored the moderating role of provider prejudice. All three were conducted with medical students and involved manipulating patient characteristics presented in a clinical vignette describing a patient inquiring about PrEP. The first two studies manipulated the race (Black or White) of an MSM patient, finding mixed evidence for patient race affecting PrEP-related clinical judgments [11, 12]. Specifically, the first study found that medical students judged a Black patient to be more likely than a White patient to engage in increased condomless sex if prescribed PrEP, which was associated with lower intention to prescribe [11]. The second study did not replicate this result and found minimal evidence for participant explicit or implicit racial prejudice playing a moderating role [12]. However, the second study did find that medical students expressing higher vs. lower explicit sexual prejudice (i.e., more negative attitudes toward gay men) judged the MSM patient to be more likely to engage in increased condomless sex and less likely to adhere to PrEP if prescribed PrEP. Additionally, the study found that anticipated condomless sex mediated the association between sexual prejudice and intention to prescribe PrEP [12]. The third study, which did not specify patient race, revealed significant differences in PrEP-related clinical judgments made about a gay male patient compared with patients of other sexual orientations and genders (e.g., lower perceived HIV risk and lower intention to prescribe PrEP for a heterosexual woman vs. gay man) [13]. Collectively, these three studies offer preliminary evidence of social biases in PrEP-related clinical decision-making, albeit inconsistent evidence with respect to racial bias.
The current experimental study extends this line of research in four important ways. First, given that the earlier studies were conducted with medical students, we sought to determine whether evidence of social biases affecting PrEP clinical decision-making emerged among licensed, practicing providers, who currently determine PrEP access. Similar to the second study and consistent with theory [12, 25, 26], we not only examined the impact of patient characteristics, but also the potential moderating role of explicit and implicit forms of participant prejudice.
Second, we sought to clarify whether the indirect effect of sexual prejudice on prescribing intention that was identified in the second study with respect to an MSM patient [12] translated to differential judgment of an MSM patient vs. a male patient with a female partner. This possibility could not be assessed in the second study because the vignette patient in both experimental conditions was an MSM.
Third, we sought to examine other mediating mechanisms through which patient characteristics may indirectly affect PrEP prescribing intention. According to van Ryn and colleagues’ social-cognitive theory of racial biases in clinical decision-making, patient race impacts clinical decision-making not only by affecting providers’ interpretation of a patient’s presenting symptoms and concerns but also by shaping their judgments about a patient’s deservingness of and appropriateness for care [25, 26]. Therefore, we examined multiple indicators of perceived deservingness of and appropriateness for care as mediating mechanisms. Additionally, consistent with past experimental studies [11–13] and provider-reported PrEP prescription barriers [27], we included anticipated patient risk behavior and PrEP adherence as other potential mechanisms. We also explored perceived patient HIV risk as a mechanism given early reports of PrEP prescribers differentiating PrEP service delivery based on perceived HIV risk of the patient (e.g., proactively educating all patients known to be MSM but not others due to HIV risk inferred from local epidemiology [28]). Since the time of data collection for the present study, perceived patient HIV risk has also been established as a mechanism linking patient gender/sexual orientation to medical students’ intention to prescribe PrEP [13].
Finally, we sought to expand the range of social biases investigated by including not only racial and sexual biases, but also biases related to injection drug use. Worldwide, there are over 15 million PWID, an estimated 18% of whom are living with HIV [29]. In the US, the opioid epidemic has fueled injection drug use [30] and led to rapid regional HIV outbreaks via syringe-sharing [31]. Offering PrEP to PWID could help to mitigate new HIV diagnoses attributed to injection drug use and represents an important area for future PrEP scale-up. Although PrEP is indicated for PWID and many PWID have expressed favorable attitudes toward PrEP [32–36], US surveillance data indicates that only about 26% are aware of PrEP and less than 1% have recently used PrEP [8].
Providers have reported significantly lower prescribing experience and intention with respect to PWID compared with people at sexual risk (e.g., MSM and heterosexuals) [37–40]. Additionally, despite evidence to the contrary [41, 42], providers have questioned the capacity of people who use drugs to adhere to PrEP [28, 43]. Negative attitudes toward people who use drugs are pervasive in medicine [44, 45], and individuals who use drugs commonly report having experienced unfair, dehumanizing treatment by providers during past medical encounters because of their drug use [46, 47]. Experiences of past mistreatment and anticipated provider judgment have led to reluctance to seek HIV and other health services or to disclose injection practices and risks to providers [36, 46, 48, 49]. However, it is unclear how injection drug use, if disclosed by a patient seeking a prescription for PrEP, would affect providers’ judgments about the patient and intention to prescribe PrEP.
Study Overview and Objectives
In the current online survey study, licensed US providers practicing in HIV or primary care settings, including physicians, nurses, physician assistants, and others, were randomly assigned to review a single fictitious medical record of a hypothetical male patient seeking a prescription for PrEP. Medical records varied by patient race (Black or White) and risk behavior (man who has sex with men [MSM], has sex with women [MSW], or injects drugs [MID])1 according to a 2 × 3 factorial design. Providers were asked to make a series of clinical judgments about the hypothetical patient whose record they reviewed (e.g., anticipated patient adherence, patient safety-consciousness, intention to prescribe PrEP for the patient). Providers completed attitudinal self-report measures of explicit racial prejudice, explicit sexual prejudice, and explicit prejudice against PWID. In addition, extending earlier research probing the possible role of implicit racial prejudice [12], providers completed a race implicit association test (IAT).
Our first objective was to evaluate whether and how biases based on patient race (Black vs. White), sexual orientation (as indicated by reported sex of sexual partner2; MSM vs. MSW), and injection drug use (MID vs. MSM and MID vs. MSW) manifested in providers’ PrEP-related clinical judgments. To do so, we tested for differences between experimental conditions. Specifically, we examined the effects of race, risk behavior, and—recognizing the potential for unique biases at the intersection of patient characteristics (e.g., race x sexual orientation [52, 53])––the interaction of race and risk behavior on the set of clinical judgments (see Fig. 1: Model A). We also assessed whether patient characteristics (race, risk behavior, and race x risk behavior) affected our primary outcome of interest, intention to prescribe PrEP, indirectly through their effect(s) on other PrEP-related clinical judgments (multiple mediation analyses; see Fig. 1: Model B).
Fig. 1.
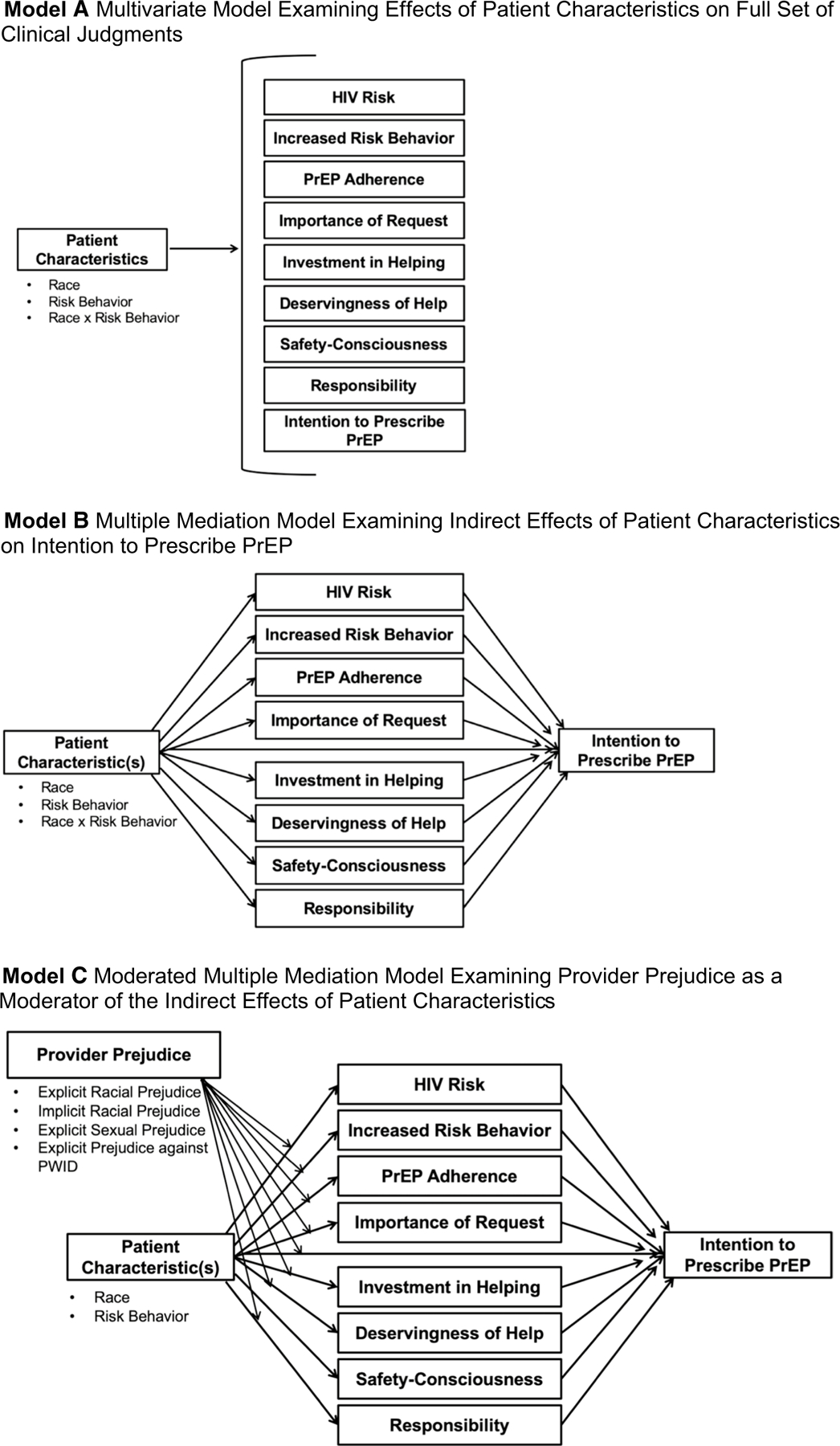
Conceptual models. Two patient characteristics were systematically manipulated in the 2 × 3 experimental design: race (Black or White) and risk behavior (man who has sex with men [MSM], man who has sex with women [MSW], and man who injects drugs [MID]). Patient race, patient risk behavior, and the interaction of patient race and risk behavior were examined relative to the set of clinical judgments reported by providers in a multivariate model (Model A). The indirect effects of patient characteristics on intention to prescribe PrEP for the patient were tested with all other clinical judgments of the patient considered as mediators in a parallel multiple mediator model (Model B). Finally, the moderating effect of provider prejudice on the indirect effects in the parallel multiple mediator model was examined for different patient characteristics and corresponding forms of prejudice (Model C)
Our second objective was to determine whether provider prejudice moderated any indirect effects of corresponding patient characteristics on intention to prescribe PrEP (moderated multiple mediation analyses; see Fig. 1: Model C). Specifically, we examined whether provider racial prejudice, explicit or implicit, moderated any indirect effects of patient race (Black vs. White); whether provider explicit sexual prejudice moderated any indirect effects of patient sexual orientation (MSM vs. MSW); and whether provider explicit prejudice against PWID moderated any indirect effects of patient injection drug use.
Hypotheses
Racial Bias
With respect to racial bias, we did not propose specific hypotheses about the effect of patient race on clinical judgments, indirect effects of patient race on prescribing intention, or moderating effects of provider racial prejudice given mixed evidence to date in experimental vignette-based studies examining patient race effects in the domain of PrEP clinical decision-making [11, 12]. Likewise, we did not propose specific hypotheses related to biases at the intersection of race and risk behavior.
Sexual Orientation Bias
With respect to sexual orientation bias, based on previous research suggesting that MSM have encountered sex-negative reactions and assumptions about condom nonuse and non-monogamy when seeking PrEP in a healthcare setting [54, 55] and that heterosexuals may not face the same level of scrutiny [23, 24], we hypothesized that the MSM patient would be judged as more likely to increase risk behavior, less safety-conscious, and less responsible than the MSW patient, and that these judgments would function as mechanisms via which MSM sexual orientation was indirectly associated with lower intention to prescribe PrEP. In light of previous research with medical students showing that explicit sexual prejudice was positively associated with anticipating increased condomless sex by an MSM patient and indirectly associated with lower intention to prescribe PrEP for him [12], we hypothesized that explicit sexual prejudice would moderate the indirect pathways between patient risk group (MSM vs. MSW) and prescribing intention. Specifically, we expected the hypothesized indirect effects via increased risk behavior, safety-consciousness, and responsibility to be stronger among providers expressing higher vs. lower levels of sexual prejudice.
Injection Drug Use Bias
With respect to injection drug use bias, based on research with providers documenting lower anticipated PrEP adherence among PWID and negative character judgments about PWID [30, 45, 56, 57], we hypothesized that the MID patient would be perceived as less likely to adhere to PrEP, less safety-conscious, and less responsible than the MSM and MSW patients, and that these judgments would function as mechanisms via which patient injection drug use was indirectly associated with lower intention to prescribe PrEP. We hypothesized that explicit prejudice against PWID would moderate these indirect effects, such that the hypothesized indirect effects would be stronger among providers expressing higher vs. lower levels of prejudice against PWID. Although we proposed parallel hypotheses for comparisons of the MID vs. MSM patient and the MID vs. MSW patient, we deliberately conducted separate comparisons rather than combining the MSM and MSW patients into a single sexual risk comparison group because of the difference in HIV risk conferred by the MSM and MSW patients’ sexual behaviors and the hypothesized differences in providers’ clinical judgments about the MSM and MSW patients.
Methods
Participants and Procedures
All study procedures were reviewed and approved by the Yale University Human Subjects Committee (IRB #HSC-1308012487) and the George Washington University Office of Human Research (IRB #061636). An online survey was developed by the principal investigator (SKC) based on earlier studies [11, 12]. To verify understanding by the target population and enhance validity, the experimental manipulation (described below) and survey measures were revised based on feedback from physician co-authors, including individuals with expertise in HIV treatment, HIV prevention with PrEP, and addiction medicine. The survey was distributed to US providers via professional email distribution lists (e.g., American Academy of HIV Medicine, Society for General Internal Medicine) in 2016–2017. Participants were eligible to participate if they were providers who were licensed to prescribe medicine in the US and were practicing in an outpatient primary care or HIV care setting in the US. They were instructed to complete the survey using a computer rather than an alternative electronic device, which was necessary for valid administration of the IAT used to assess implicit racial prejudice.
Following initial online screening and consent, participants were asked about their familiarity and experience with PrEP. Subsequently, they were provided background information about HIV and PrEP. Background information included modes of HIV transmission; populations for whom PrEP had been indicated by the CDC (MSM, heterosexual men and women, and PWID); efficacy estimates; side effects; approval by the US Food and Drug Administration; and basic CDC guidelines for follow-up care. At the time of survey administration, once-daily dosing of tenofovir disoproxil fumarate with emtricitabine (TDF/FTC;Truvada®) was the only form of PrEP that was approved by the US Food and Drug Administration and available in the US, so only this form of PrEP was referenced in the survey. Participants were also asked to review a table specifying the estimated per-act probability of HIV transmission for different HIV risk behaviors ordered according to risk, which included the three behaviors experimentally manipulated in the fictitious medical record: sharing needles with a person with HIV during injection drug use (63 per 10,000 exposures)—the behavior reported by the MID patient; insertive penile-anal sex, described as penetrating a partner with HIV during anal sex (11 per 10,000 exposures)—the behavior reported by the MSM patient; and insertive penile-vaginal sex, described as a man having vaginal sex with a woman with HIV (4 per 10,000 exposures)—the behavior reported by the MSW patient [58, 59].
Participants were then asked to carefully review the medical record of a hypothetical patient, whom they were told to assume was new to their practice (Fig. 2). Each participant was randomly assigned to review one version of the medical record. Two key pieces of information were systematically manipulated across versions: patient race and risk behavior. All medical records were otherwise identical and described a 31-year-old man seeking a prescription for PrEP with no medical contraindications or significant medical history. These background details were selected to align with past vignette studies [11, 12]. The medical record also indicated that the patient tested HIV-negative via a 4th-generation HIV antigen/antibody test, had normal creatinine clearance, had been vaccinated against Hepatitis B, and possessed medical insurance.
Fig. 2.
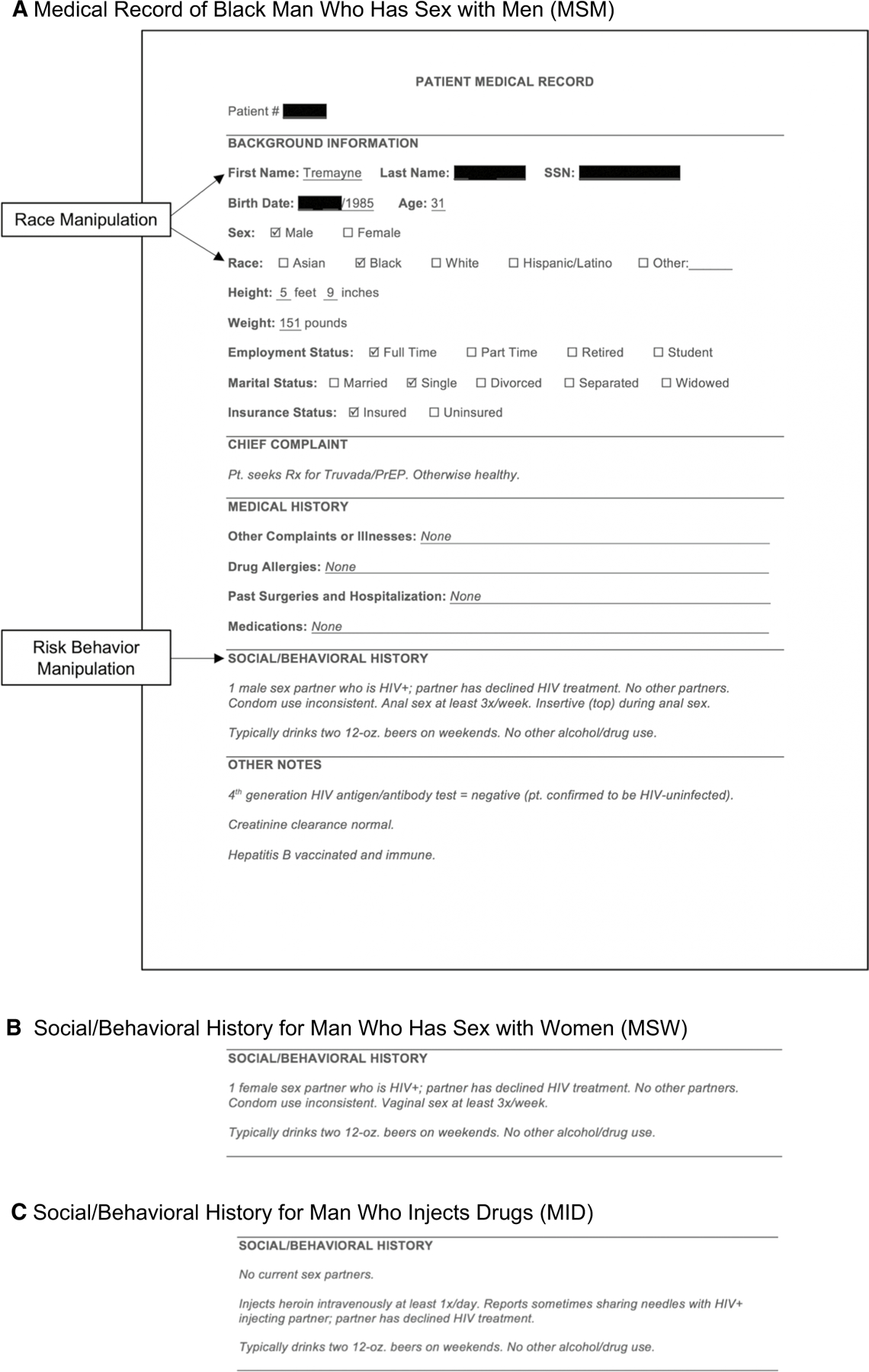
Experimental Stimulus. A Example of the full experimental stimulus (fictitious medical record) reviewed by providers randomized to a Black MSM patient condition. Patient race was manipulated through the first name of the patient and the race checkbox endorsed. Patient names for the Black condition (Tremayne, Tyrone, Jermaine) and White condition (Neil, Greg, Brad) were selected from a list of pre-tested names commonly associated with Black and White men. Patient risk behavior was manipulated through the Social/ Behavioral History of the patient. B and C The Social/Behavioral History in the MSW and MID patient conditions, respectively.
Race was indicated as Black or White based on the patient’s first name and the race checkbox endorsed. Patient names for the Black condition (Tremayne, Tyrone, Jermaine) and White condition (Neil, Greg, Brad) were randomly selected from a list of pre-tested names commonly associated with Black and White men [60, 61]. Risk behavior was indicated in the Social/Behavioral History as insertive male-male condomless anal sex (representing the MSM condition), male–female condomless vaginal sex (representing the MSW condition), or sharing needles during heroin injection (representing the MID condition). Thus, each participant was randomized to read about one of 18 different patients: A Black MSM named Tremayne, Tyrone, or Jermaine; a White MSM named Neil, Greg, or Brad; a Black MSW named Tremayne, Tyrone, or Jermaine; a White MSW named Neil, Greg, or Brad; a Black MID named Tremayne, Tyrone, or Jermaine; or a White MID named Neil, Greg, or Brad. All hypothetical patients were described as having one partner—whether a sexual or injecting partner—who was living with HIV and had declined HIV treatment (to suggest viral load detectability/viral transmissibility). All three risk behaviors were mutually exclusive (e.g., a patient who injected drugs was described as having no current sexual partners).
After reviewing the medical record, participants were asked to make a series of judgments about the patient (e.g., anticipated patient adherence, patient safety-consciousness, intention to prescribe PrEP for the patient). Additionally, they completed measures of explicit racial, sexual, and injection drug use prejudice and implicit racial prejudice. At the conclusion of the survey, participants received compensation (a $25.00 gift card or entry into a lottery to win an Apple iPad mini) and were provided with a link to the CDC website for more information about PrEP.
Measures
Prior to receiving background information about HIV and PrEP or reviewing the patient medical record, participants reported their familiarity with PrEP, with response options ranging from (1) Not at all familiar (this is my first time hearing about PrEP) to (5) Extremely familiar (I have expert knowledge of PrEP). They also indicated their experience with PrEP, including prior discussion of PrEP with HIV-negative patients (irrespective of whether it led to PrEP prescription) and prior prescription of PrEP.
Main measures are summarized in Table 1. Clinical judgments about the hypothetical patient who was described in the fictitious medical record included: the patient’s HIV risk without PrEP, likelihood of the patient increasing his risk behavior if prescribed PrEP, anticipated patient adherence if prescribed PrEP, importance of the patient’s request, investment in helping the patient, the patient’s deservingness of help, perceived safety-consciousness of the patient, perceived level of responsibility of the patient, and intention to prescribe PrEP for the patient. Participants were able to see the medical record while reporting clinical judgments. After all clinical judgments had been completed, self-report measures of explicit racial prejudice, explicit sexual prejudice, explicit prejudice against PWID, sociodemographic characteristics, and clinical background characteristics were administered.
Table 1.
Summary of main survey measures
| Clinical judgments | Item(s) | Response options | # Items | Cronbach’s alpha |
|---|---|---|---|---|
|
| ||||
| HIV Risk | How high do you think this patient’s risk of getting HIV is WITHOUT PrEP? | 5-point scale ranging from (1) Extremely Low to (5) Extremely High | 1 | – |
| Increased Risk Behavior | How likely would this patient be to increase his risk behavior if he started taking Truvada as PrEP? | 5-point scale ranging from (1) Not At All Likely to (5) Extremely Likely | 1 | – |
| PrEP Adherence | If you were to prescribe Truvada to this patient as PrEP, how ADHERENT do you think he would be? | 5-point scale ranging from (1) Not At All Adherent to (5) Extremely Adherent | 1 | – |
| Importance of Request | How IMPORTANT would this patient’s request be to you? | 5-point scale ranging from (1) Not At All Important to (5) Extremely Important | 1 | – |
| Investment in Helping | How INVESTED would you be in helping this patient compared to most of the other patients that you see? | 5-point scale ranging from (1) Much Less Invested to (5) Much More Invested | 1 | – |
| Deservingness of Help | This patient deserves help protecting himself from HIV. | 5-point scale ranging from (1) Strongly Disagree to (5) Strongly Agree | 1 | – |
| Safety-Consciousness | Based on the information provided, how would you rate this patient’s SAFETY-CON- SCIOUSNESS? | 5-point scale ranging from (1) Not At All Safety-Conscious to (5) Extremely Safey-Conscious | 1 | – |
| Responsibility | Based on the information provided, how would you rate this patient’s level of RESPONSI-BILITY? | 5-point scale ranging from (1) Extremely Irresponsible to (5) Extremely Responsible | 1 | – |
| Intention to Prescribe PrEP | Would you prescribe Truvada as PrEP to this patient? | 5-point scale ranging from (1) Definitely Not to (5) Definitely Yes | 1 | – |
|
| ||||
| Prejudice | Sample items | Response options | # Items | Cronbach’s alpha |
|
| ||||
| Explicit Racial Prejudicea | Blacks are getting too demanding in their push for equal rights. It is easy to understand the anger of Black people in America. [reverse-scored] |
5-point scale ranging from (1) Strongly Disagree to (5) Strongly Agree | 7 | 0.87 |
| Explicit Sexual Prejudiceb | Many gay men use their sexual orientation so that they can obtain special privileges. Gay men do not have all the rights they need. [reverse-scored] |
5-point scale ranging from (1) Strongly Disagree to (5) Strongly Agree | 12 | 0.91 |
| Explicit Prejudice Against People Who Inject Drugsc | Injecting drugs is morally wrong. Injection drug users are weak minded. | 5-point scale ranging from (1) Strongly Disagree to (5) Strongly Agree | 6 | 0.84 |
| Implicit Racial Prejudiced | – | – | – | – |
Modern Racism Scale [62]
Modern Homonegativity Scale—Gay Men (MHS-G) [63]
Adapted from Drug Use Stigmatization Scale [64]; drug type was specified as “injection drug”; one original scale item omitted
Based on a race implicit association test (IAT), which is a computerized response-latency task. Scores can range from − 2 to 2, with higher scores suggesting greater prejudice (a more negative implicit attitude toward Black vs. White men)
In addition, three attention/manipulation check items were included to confirm that participants had appropriately attended to the characteristics of the patient described in the medical record. Specifically, participants were considered to have “passed” the attention/manipulation check if they correctly identified the sex of the patient as male, correctly identified the race/ethnicity of the patient as Black or White according to their assigned experimental condition, and—for MSM and MSW conditions only—correctly identified the sex of the patient’s sexual partner according to their assigned condition. For the MID condition, all responses pertaining to the sex of the patient’s sexual partner were accepted (“female,” “male,” “the patient did not have any current sexual partners,” and “I don’t know”) even though “the patient did not have any current sexual partners” was the correct response. Whereas misidentifying sexual partner sex in the MSM and MSW conditions indicated that participants were unaware of the patient’s primary risk, in the MID condition, misidentifying sexual partner sex did not necessarily negate their awareness of the patient’s primary risk (shared injection equipment). The attention/manipulation check items were purposely presented later in the survey, separated from exposure to the medical record by multiple other measures.
Finally, consistent with the second of the medical student studies upon which the current study builds [12], we administered an IAT [65, 66] as an indicator of implicit racial prejudice. We use the term “prejudice” when referring to IAT performance throughout this work rather than “preference” or “bias”—terms preferred by some researchers—for clarity (to keep the valence of participant social attitude measures consistent and distinguish this measure from biases inferred from differences between experimental conditions; see Greenwald et al. 2021 [67] for discussion on terminology). The IAT is a computerized response-latency task that was administered via Inquisit by Millisecond (https://www.millisecond.com/). Over a series of trials, participants were asked to quickly categorize stimuli that appeared on their computer screen. Stimuli included images of Black and White male faces drawn from a standard database and words with positive or negative connotations (e.g., “marvelous,” “superb,” “tragic,” “horrible”). We restricted the facial images to male faces (rather than male and female) because the hypothetical patient in the experimental manipulation was a man. IATs determine participants’ automatic cognitive associations based on their relative response times during categorization trials. For example, a participant with a more negative implicit attitude toward Black vs. White people would more quickly categorize Black faces as bad and White faces as good than categorize Black faces as good and White faces as bad. The IAT generated a numerical score ranging from – 2 to 2, referred to as a D score. Higher D scores suggested greater implicit racial prejudice (a more negative implicit attitude toward Black vs. White men).
Analyses
The full analytic sample was restricted to participants who completed all self-report survey measures preceding the IAT. Analyses examining the effect(s) of one or both experimentally manipulated patient characteristics (race and/or risk) were initially restricted to participants who passed the attention/manipulation check to ensure that all participants had adequately attended to the race and risk behavior of the patient presented to them and were aware of those characteristics when making clinical judgments about the patient. Analyses including implicit racial prejudice as a variable were restricted to participants who completed the IAT; did not have an excessively high IAT completion time, defined as greater than three standard deviations above the mean; and responded correctly (i.e., accurately categorized IAT stimuli according to instructions at first attempt) at least 80% of the time in a subset of trials. Because there were three outlying IAT completion times that were heavily skewing the mean and standard deviation (12.6, 24.8, and 342.3 min), we excluded those response records before applying these criteria. Both the attention/manipulation check and IAT restrictions were imposed for analyses examining the effect(s) of one or both experimentally manipulated patient characteristics and also including implicit racial prejudice as a variable.
Although analyses examining the effect(s) of one or both experimentally manipulated patient characteristics were initially restricted to participants who passed the attention/manipulation check, analyses were subsequently repeated with the full analytic sample to determine whether the same pattern of results emerged. Analyses with the larger sample (including participants who failed the attention/manipulation check) were conducted to account for the possibility that participants’ attention to the patient’s race and/or risk behavior was systematically associated with prejudice (e.g., participants who were especially high in prejudice or especially conscious of prejudice would be more likely to attend to corresponding patient characteristics) and, thus, exclusion based on attention/manipulation check items could reduce the representativeness of our sample. We also directly tested associations between passing the attention/manipulation check and each form of prejudice using independent samples t-tests.
Multivariate analysis of variance (MANOVA) and multivariate analysis of covariance (MANCOVA) adjusting for relevant background characteristics (detailed below) were performed to examine the effects of the experimental manipulation, including the partial, conditional, and interaction effects of patient race (Black or White) and patient risk behavior (MSM, MSW, or MID) on the full set of nine clinical judgments. Wilks’ Lambda was used as the omnibus test statistic, with post-hoc pairwise comparisons performed using Tukey’s Honestly Significant Difference (HSD) Test.
Mediation, moderated mediation, and supplemental moderation analyses were conducted using Hayes’ PROCESS macro (Version 3.5, Templates 4, 8, and 1, respectively; www.process.org) [68]. For the mediation analyses, we used the PROCESS macro to generate 5000 bootstrapped samples, from which 95% confidence intervals were established to estimate indirect effects. Bootstrapping is a preferred strategy for testing mediation because it directly quantifies indirect effects rather than inferring them from constituent paths and does not require the testing of multiple hypotheses as in traditional causal steps approaches such as the Baron and Kenny method. Bootstrapping also avoids assumptions about the shape of the sampling distribution of the indirect effect (as in the Sobel test) [68, 69]. We first constructed two multiple mediator models to examine the indirect effects of patient characteristics on prescribing intention, including the 8 other clinical judgments as parallel mediators. In one model, patient race was tested as a dichotomous focal predictor (Black vs. White). In the other, patient risk behavior was tested as a multicategorical focal predictor (MID vs. MSM vs. MSW), which allowed for pairwise comparisons of patient sexual orientation (MSM vs. MSW) and patient injection drug use (MID vs. MSM and MID vs. MSW). Contrast effects were examined to compare the magnitude of significant specific indirect effects. Because the PROCESS macro could not generate contrast effects for a multiple mediation model with a multicategorical focal predictor, we constructed three models with dichotomous focal predictors corresponding to the three behavior-based pairwise comparison (i.e., MSM vs. MSW, MID vs. MSM, and MID vs. MSW) for the purpose of reporting contrast effects.
Moderated mediation occurs when one or more indirect effects systematically varies based on the level of one or more other variables. To examine potential indirect effects of intersecting patient characteristics (race x sexual orientation and race x injection drug use) on intention to prescribe PrEP, we tested a moderated mediation model in which patient race moderated the indirect effect of patient risk behavior (multicategorical focal predictor) on intention to prescribe PrEP through the eight other clinical judgments (mediators). We subsequently tested each of the four forms of prejudice as moderators of the indirect effects of the corresponding patient characteristic on intention to prescribe PrEP. Indices of Moderated Mediation were used to determine whether each moderated mediation model was significant, as indicated by a 95% confidence interval that did not straddle zero [68, 70]. Significant moderated mediation models were probed using the PROCESS macro; indirect effects are reported at the 16th, 50th, and 84th percentiles for continous moderators [68].
Supplemental moderation analyses were performed to determine whether any unmediated effects of the experimentally manipulated patient characteristics on intention to prescribe PrEP were moderated by provider prejudice. For these moderation models, the Johnson-Neyman technique was applied when probing significant interactions using the PROCESS macro [68].
Relevant background characteristics that were adjusted for in multivariable models included sociodemographic and clinical background characteristics that were conceptually and/or empirically related to one or more clinical judgments. The following relevant background characteristics were adjusted for in MANCOVA, mediation, moderated mediation, and supplemental moderation analyses: age, race, gender, sexual orientation, provider type, HIV specialization, practice setting, PrEP familiarity, and PrEP experience. Models examining the indirect or moderated effects of patient race but not patient risk behavior were adjusted for patient risk behavior. Models examining the indirect or moderated effects of patient risk behavior but not patient race were adjusted for patient race. MANCOVA and moderated mediation models involving the interaction of patient race x patient risk behavior also included explicit racial prejudice as a covariate given that explicit racial prejudice varied across patient risk behavior conditions (but not patient race conditions) despite randomization.
Results
Participant Characteristics
There were 701 unique survey records. Most respondents (n = 452; 64.5%) met eligibility criteria and consented to participate and 391 (55.8%) completed the self-report survey preceding the IAT. Four were excluded due to suspected repetition/fraudulent responding and an additional 17 were excluded because their reported medical degree(s) suggested ineligibility to prescribe PrEP (e.g., participants with PharmDs would not have been eligible to prescribe PrEP in any state at the time of data collection). Thus, 370 participants qualified for inclusion in our full analytic sample. Of these, 56.2% were recruited via the American Academy of HIV Medicine email distribution list (6.9% of the 3015 members emailed), 22.7% were recruited via the Society of General Internal Medicine email distribution list (2.5% of the 3346 members emailed), 12.2% were recruited via other professional email distribution lists, 7.0% reported being referred by a friend or colleague (e.g., via a forwarded email), and 1.9% did not remember or otherwise did not indicate their recruitment source.
Of the 370 participants in the full analytic sample, 276 (74.6%) passed all required attention/manipulation check items to be included in analyses examining the effects of experimental condition (patient race and/or risk behavior). Specifically, 95.1% of participants correctly identified the patient as male, 77.3% correctly identified the patient’s race, and—considering the MSM and MSW conditions only—93.9% correctly identified the sex of the patient’s sexual partner. Of the 370 participants in the full analytic sample, 193 (52.2%) completed the IAT and 190 met IAT duration and accuracy criteria to be included in analyses involving implicit racial prejudice (three were excluded because of excessively high completion times). When both attention/manipulation check and IAT restrictions were imposed for analyses examining the effect(s) of one or both experimentally manipulated patient characteristics and implicit racial prejudice, the sample included 149 participants.
Independent samples t-tests examining the association between passing the attention/manipulation check and prejudice revealed that explicit prejudice was generally lower among participants who passed. Specifically, explicit racial prejudice was significantly lower among participants who passed (M [SD] = 1.43 [0.52]) vs. those who did not (M [SD] = 1.69 [0.67]), t (133) = 3.45, p = 0.001; explicit sexual prejudice was marginally lower among participants who passed (M [SD] = 1.70 [0.62]) vs. those who did not (M [SD] = 1.85 [0.71]), t (145) = 1.87, p = 0.064; and explicit prejudice against PWID was significantly lower among participants who passed (M [SD] = 1.90 [0.70]) vs. those who did not (M [SD] = 2.09 [0.74]), t (368) = 2.22, p = 0.027. There was no significant difference in implicit racial prejudice among participants who passed (M [SD] = 0.20 [0.50]) vs. those who did not (M [SD] = 0.26 [0.53]), t (188) = 0.63, p = 0.529.
Sample characteristics are presented in Table 2. Participants ranged in age from 25 to 71 years (M[SD] = 45.7[11.4]). The sample was predominantly White (72.1%) and heterosexual (74.9%). Most participants practiced in an urban setting (77.0%), were trained as physicians (67.3%), and identified as HIV specialists (66.5%). The vast majority reported having previously cared for one or more MSM (98.9%), MSW (97.6%), and MID (96.8%) patients. Most reported that they were either very familiar with PrEP, defined as knowing a lot of information about PrEP, including details such as recent clinical trial results (38.9%); or extremely familiar with PrEP, defined as having expert knowledge of PrEP (31.4%). The vast majority had discussed PrEP with one or more patients (92.2%), and many had prescribed PrEP (78.9%).
Table 2.
Sample characteristics
| Total analytic sample (N = 370)a |
Experimental condition analytic subsamples |
||||||
|---|---|---|---|---|---|---|---|
| Black MSM patient (n = 61)a |
White MSM patient (n = 65)a |
Black MSW patient (n = 63)a |
White MSW patient (n = 56)a |
Black MID patient (n = 64)a |
White MID patient (n = 61)a |
||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
|
| |||||||
| Years of age | |||||||
| < 30 | 13 (3.5) | 2 (3.3) | 2 (3.1) | 3 (4.8) | 2 (3.6) | 3 (4.7) | 1 (1.6) |
| 30–39 | 122 (33.2) | 11 (18.0) | 24 (37.5) | 24 (38.1) | 21 (38.2) | 18 (28.1) | 24 (39.3) |
| 40–49 | 93 (25.3) | 18 (29.5) | 14 (21.9) | 12 (19.0) | 19 (34.5) | 17 (26.6) | 13 (21.3) |
| 50–59 | 77 (20.9) | 19 (31.1) | 10 (15.6) | 17 (27.0) | 6 (10.9) | 15 (23.4) | 10 (16.4) |
| 60+ | 63 (17.1) | 11 (18.0) | 14 (21.9) | 7 (11.1) | 7 (12.7) | 11 (17.2) | 13 (21.3) |
| Race/ethnicity | |||||||
| White | 266 (72.1) | 40 (65.6) | 47 (72.3) | 46 (73.0) | 39 (70.9) | 48 (75.0) | 46 (75.4) |
| Asian | 43 (11.7) | 9 (14.8) | 7 (10.8) | 9 (14.3) | 5 (9.1) | 9 (14.1) | 4 (6.6) |
| Latino/x/a or Hispanic | 26 (7.0) | 5 (8.2) | 5 (7.7) | 3 (4.8) | 6 (10.9) | 5 (7.8) | 2 (3.3) |
| Black/African American | 22 (6.0) | 2 (3.3) | 5 (7.7) | 4 (6.3) | 3 (5.5) | 2 (3.1) | 6 (9.8) |
| Other | 12 (3.3) | 5 (8.2) | 1 (1.5) | 1 (1.6) | 2 (3.6) | 0 (0.0) | 3 (4.9) |
| Gender | |||||||
| Female | 189 (51.2) | 26 (42.6) | 31 (47.7) | 28 (44.4) | 24 (43.6) | 40 (62.5) | 40 (65.6) |
| Male | 177 (48.0) | 35 (57.4) | 31 (47.7) | 35 (55.6) | 31 (56.4) | 24 (37.5) | 21 (34.4) |
| Other | 3 (0.8) | 0 (0.0) | 3 (4.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Sexual orientationb | |||||||
| Heterosexual | 268 (74.9) | 43 (74.1) | 52 (80.0) | 51 (81.0) | 34 (63.0) | 43 (72.9) | 45 (76.3) |
| Gay/lesbian | 73 (20.4) | 13 (22.4) | 10 (15.4) | 12 (19.0) | 17 (31.5) | 14 (23.7) | 7 (11.9) |
| Bisexual | 13 (3.6) | 1 (1.7) | 2 (3.1) | 0 (0.0) | 2 (3.7) | 2 (3.4) | 6 (10.2) |
| Other | 4 (1.1) | 1 (1.7) | 1 (1.5) | 0 (0.0) | 1 (1.9) | 0 (0.0) | 1 (1.7) |
| Region of US | |||||||
| Northeast | 148 (40.0) | 18 (29.5) | 30 (46.2) | 24 (38.1) | 18 (32.1) | 31 (48.4) | 27 (44.3) |
| West | 90 (24.3) | 19 (31.1) | 11 (16.9) | 14 (22.2) | 13 (23.2) | 18 (28.1) | 15 (24.6) |
| South | 89 (24.1) | 14 (23.0) | 15 (23.1) | 18 (28.6) | 19 (33.9) | 10 (15.6) | 13 (21.3) |
| Midwest | 43 (11.6) | 10 (16.4) | 9 (13.8) | 7 (11.1) | 6 (10.7) | 5 (7.8) | 6 (9.8) |
| Geographic setting | |||||||
| Urban | 285 (77.0) | 44 (72.1) | 51 (78.5) | 46 (73.0) | 41 (73.2) | 56 (87.5) | 47 (77.0) |
| Suburban | 68 (18.4) | 13 (21.3) | 12 (18.5) | 15 (23.8) | 12 (21.4) | 8 (12.5) | 8 (13.1) |
| Rural | 17 (4.6) | 4 (6.6) | 2 (3.1) | 2 (3.2) | 3 (5.4) | 0 (0.0) | 6 (9.8) |
| Provider typec | |||||||
| Physician | 249 (67.3) | 44 (72.1) | 40 (61.5) | 43 (68.3) | 40 (71.4) | 36 (56.3) | 46 (75.4) |
| Nursing | 86 (23.2) | 11 (18.0) | 17 (26.2) | 18 (28.6) | 9 (16.1) | 19 (29.7) | 12 (19.7) |
| Physician’s assistant | 38 (10.3) | 6 (9.8) | 8 (12.3) | 5 (7.9) | 7 (12.5) | 9 (14.1) | 3 (4.9) |
| Other | 6 (1.6) | 1 (1.6) | 2 (3.1) | 1 (1.6) | 1 (1.8) | 0 (0.0) | 1 (1.6) |
| HIV specialization | |||||||
| HIV specialist | 246 (66.5) | 42 (68.9) | 40 (61.5) | 41 (65.1) | 40 (71.4) | 47 (73.4) | 36 (59.0) |
| Non-specialist | 124 (33.5) | 19 (31.1) | 25 (38.5) | 22 (34.9) | 16 (28.6) | 17 (26.6) | 25 (41.0) |
| Years of clinical practice | |||||||
| 0–5 | 75 (20.3) | 6 (9.8) | 16 (24.6) | 14 (22.2) | 14 (25.0) | 10 (15.6) | 15 (24.6) |
| 6–10 | 78 (21.1) | 12 (19.7) | 9 (13.8) | 15 (23.8) | 12 (21.4) | 13 (20.3) | 17 (27.9) |
| 11–20 | 107 (28.9) | 24 (39.3) | 20 (30.8) | 12 (19.0) | 17 (30.4) | 22 (34.4) | 12 (19.7) |
| 21–45 | 110 (29.7) | 19 (31.1) | 20 (30.8) | 22 (34.9) | 13 (23.2) | 19 (29.7) | 17 (27.9) |
| Most common practice settingsc | |||||||
| University/academic | 143 (38.6) | 22 (36.1) | 28 (43.1) | 25 (39.7) | 22 (39.3) | 23 (35.9) | 23 (37.7) |
| Community health center | 139 (37.6) | 26 (42.6) | 22 (33.8) | 26 (41.3) | 17 (30.4) | 24 (37.6) | 24 (39.3) |
| Hospital | 98 (26.5) | 16 (26.2) | 11 (16.9) | 17 (27.0) | 18 (32.1) | 17 (26.6) | 19 (31.1) |
| Experience providing care for patient types of interestc | |||||||
| 1+ MSM | 366 (98.9) | 61 (100.0) | 65 (100.0) | 61 (96.8) | 56 (100.0) | 63 (98.4) | 60 (98.4) |
| 1+ MSW | 361 (97.6) | 60 (98.4) | 64 (98.5) | 60 (95.2) | 56 (100.0) | 62 (96.9) | 59 (96.7) |
| 1+ MID | 358 (96.8) | 59 (96.7) | 61 (93.8) | 62 (98.4) | 54 (96.4) | 64 (100.0) | 58 (95.1) |
| PrEP familiarity | |||||||
| Not at all (first time hearing about PrEP) | 1 (0.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.8) | 0 (0.0) | 0 (0.0) |
| A little (heard of PrEP but don’t really know what it is) | 8 (2.2) | 2 (3.3) | 1 (1.5) | 2 (3.2) | 2 (3.6) | 1 (1.6) | 0 (0.0) |
| Somewhat (know what PrEP is and basic information about it) | 101 (27.3) | 15 (24.6) | 23 (35.4) | 17 (27.0) | 13 (23.2) | 14 (21.9) | 19 (31.1) |
| Very (know a lot of information about PrEP, including details such as recent clinical trial results) | 144 (38.9) | 25 (41.0) | 22 (33.8) | 27 (42.9) | 20 (35.7) | 23 (35.9) | 27 (44.3) |
| Extremely (have expert knowledge of PrEP) | 116 (31.4) | 19 (31.1) | 19 (29.2) | 17 (27.0) | 20 (35.7) | 26 (40.6) | 15 (24.6) |
| Experience discussing PrEP with patientsc,d | |||||||
| 1+ patient (any type) | 341 (92.2) | 53 (86.9) | 57 (87.7) | 59 (93.7) | 53 (94.6) | 61 (95.3) | 58 (95.1) |
| 1+ MSM | 329 (88.9) | 51 (83.6) | 56 (86.2) | 54 (85.7) | 52 (92.9) | 60 (93.8) | 56 (91.8) |
| 1+ MSW | 228 (61.6) | 33 (54.1) | 37 (56.9) | 41 (65.1) | 33 (58.9) | 47 (73.4) | 37 (60.7) |
| 1+ MID | 206 (55.7) | 32 (52.5) | 36 (55.4) | 34 (54.0) | 27 (48.2) | 39 (60.9) | 38 (62.3) |
| Experience prescribing PrEP for patientsd | |||||||
| 1+ patient (any type) | 292 (78.9) | 47 (77.0) | 46 (70.8) | 49 (77.8) | 43 (76.8) | 54 (84.4) | 53 (86.9) |
Due to missing data, n = 358–370 across characteristics for the total analytic sample. For experimental condition analytic subsamples: n = 58–61 for Black MSM, n = 64–65 for White MSM, n = 63 for Black MSW (no missing data), n = 54–56 for White MSW, n = 59–64 for Black MID, and n = 59–61 for White MID
Participants who endorsed “I prefer not to say” were coded as missing
Categories were not mutually exclusive
“Any type” includes all patients, irrespective of gender, sexual orientation, drug use, or other characteristics
MSM man who has sex with men, MSW man who has sex with women, MID man who injects drugs
Bivariate Correlations Among Prejudice and Clinical Judgment Measures
Correlations, means, and standard deviations of prejudice and clinical judgment measures for the restricted analytic sample are presented in Table 3. Correlations, means, and standard deviations for the unrestricted analytic sample (including participants who failed the attention/manipulation check) and for each of the six race x risk subsamples are available in Online Appendix 1 (see supplementary materials). On average, participants expressed fairly low levels of prejudice. All three measures of explicit prejudice (explicit racial prejudice, sexual prejudice, and prejudice against PWID) were positively correlated with one another but not with implicit racial prejudice. Intention to prescribe PrEP was significantly correlated with seven of the eight other clinical judgments: negatively with increased risk behavior, and positively with PrEP adherence, importance of the patient’s request, investment in helping, deservingness of help, safety-consciousness, and responsibility (all p < 0.050). Intention to prescribe PrEP was marginally positively correlated with the eighth clinical judgment, perceived HIV risk of the patient (p = 0.063).
Table 3.
Bivariate correlations, means, and standard deviations of main measures (n = 276)
| Measurea | Pearson correlation coefficient (r) |
M (SD) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |||
|
| |||||||||||||||
| 1 | Explicit racial prejudice | – | 1.43 (0.52) | ||||||||||||
| 2 | Implicit racial prejudiceb | 0.13 | – | 0.20 (0.50) | |||||||||||
| 3 | Explicit sexual prejudice | 0.62** | 0.16 | – | 1.70 (0.62) | ||||||||||
| 4 | Explicit prejudice against people who inject drugs | 0.48** | 0.04 | 0.49** | – | 1.90 (0.70) | |||||||||
| 5 | HIV risk | 0.01 | 0.10 | − 0.02 | − 0.11 | – | 4.16 (0.89) | ||||||||
| 6 | Increased risk behavior | 0.06 | 0.09 | 0.21** | 0.09 | 0.05 | – | 1.67 (0.90) | |||||||
| 7 | PrEP adherence | − 0.11 | 0.04 | − 0.17** | − 0.19** | − 0.05 | − 0.19** | – | 3.79 (0.69) | ||||||
| 8 | Importance of request | − 0.08 | 0.00 | − 0.24** | − 0.18** | 0.16** | − 0.08 | 0.33** | – | 4.65 (0.55) | |||||
| 9 | Investment in helping | − 0.02 | 0.07 | − 0.15* | − 0.13* | 0.16** | − 0.08 | 0.08 | 0.24** | – | 3.70 (0.86) | ||||
| 10 | Deservingness of help | − 0.22** | − 0.14 | − 0.37** | − 0.34** | 0.10 | − 0.11 | 0.15* | 0.32** | 0.13* | – | 4.82 (0.47) | |||
| 11 | Safety-consciousness | 0.04 | − 0.07 | − 0.07 | − 0.11 | − 0.21** | − 0.12* | 0.33** | 0.18** | 0.08 | 0.08 | – | 2.99 (0.97) | ||
| 12 | Responsibility | − 0.05 | − 0.06 | − 0.13* | − 0.15* | − 0.14* | − 0.23** | 0.40** | 0.18** | 0.07 | 0.11 | 0.68** | – | 3.39 (1.01) | |
| 13 | Intention to prescribe PrEP | − 0.04 | − 0.03 | − 0.22** | − 0.20** | 0.11 | − 0.16** | 0.41** | 0.47** | 0.18** | 0.31** | 0.15* | 0.31** | – | 4.62 (0.64) |
(1) Explicit racial prejudice represents a mean score based on 7 items assessing attitudes toward Black Americans (Modern Racism Scale). Scores can range from 1 to 5, with higher values indicating stronger prejudice (more negative attitudes toward Black Americans). (2) Implicit racial prejudice represents a D score generated by an implicit association test (IAT), which is a computerized response-latency task. Scores can range from − 2 to 2, with higher scores suggesting greater prejudice (a more negative implicit attitude toward Black vs. White men). (3) Explicit sexual prejudice represents a mean score based on 12 items assessing attitudes toward gay men (Modern Homonegativity Scale-Gay Men (MHS-G)). Scores can range from 1 to 5, with higher values indicating stronger prejudice (more negative attitudes toward gay men). (4) Explicit prejudice against people who inject drugs represents a mean score based on 6 items assessing attitudes toward people who inject drugs (Drug Use Stigmatization Scale). Scores can range from 1 to 5, with higher values indicating stronger prejudice (more negative attitudes toward people who inject drugs). (5–13) All clinical judgments represent single-item measures. Scores can range from 1 to 5, with higher values indicating stronger endorsement
For the implicit racial prejudice measure only, the analytic sample was restricted to those participants who passed the manipulation check, completed the IAT, and met duration and accuracy criteria (n = 149 vs. 276)
p < 0.05
p < 0.01
Effects of Patient Race and Risk Behavior on Clinical Judgments
The MANOVA was conducted to examine the effects of the experimental manipulation of patient characteristics (race and risk behavior) on clinical judgments as depicted in Fig. 1: Model A. Omnibus tests indicated a significant effect of patient risk behavior on the full set of clinical judgments (Wilks’ Λ = 0.67, F [18, 522] = 6.38, p < 0.001, partial η2 = 0.18) but no significant race effect (Wilks’ Λ = 0.98, F [9, 261] = 0.66, p = 0.744, partial η2 = 0.02) or risk x race interaction effect (Wilks’ Λ = 0.93, F [18, 522] = 1.01, p = 0.449, partial η2 = 0.03). The analysis was repeated adjusting for relevant background characteristics (MANCOVA) and elicited the same pattern of findings (risk behavior effect: Wilks’ Λ = 0.65, F [18, 482] = 6.37, p < 0.001, partial η2 = 0.19; race effect: Wilks’ Λ = 0.98, F [9, 241] = 0.59, p = 0.805, partial η2 = 0.02; risk x race interaction effect: Wilks’ Λ = 0.91, F [18, 482] = 1.33, p = 0.166, partial η2 = 0.05).
Figure 3 displays differences in clinical judgments by patient risk behavior. MANOVA post-hoc pairwise comparisons conducted using Tukey’s HSD Test revealed significant differences by patient risk condition for multiple clinical judgments. Specifically, compared with the MSM patient, participants perceived the MSW patient to be at lower HIV risk (MMSW-MSM = − 0.56, SE = 0.12, p < 0.001) and less likely to adhere to PrEP (MMSW-MSM = − 0.25, SE = 0.10, p = 0.027). There was no significant difference in their intention to prescribe PrEP for the MSW vs. the MSM patient (MMSW-MSM = − 0.08, SE = 0.09, p = 0.669). Compared with both the MSM and MSW patients, participants perceived the MID patient to be at higher HIV risk (MMID-MSM = 0.30, SE = 0.12, p = 0.035; MMID-MSW = 0.86, SE = 0.12, p < 0.001); less likely to adhere to PrEP (MMID-MSM = −0.53, SE = 0.10, p < 0.001; MMID-MSW = − 0.28, SE = 0.10, p = 0.012); less safety-conscious (MMID-MSM = − 0.54, SE = 0.14, p < 0.001; MMID-MSW = − 0.53, SE = 0.14, p < 0.001); and less responsible (MMID-MSM = − 0.52, SE = 0.15, p = 0.001; MMID-MSW = − 0.47, SE = 0.14, p = 0.004). Participants reported marginally lower intention to prescribe PrEP for the MID vs. the MSM patient (MMID-MSM = − 0.22, SE = 0.09, p = 0.058) but no difference in intention to prescribe for the MID vs. the MSW patient (MMID-MSW = − 0.14, SE = 0.09, p = 0.318).
Fig. 3.
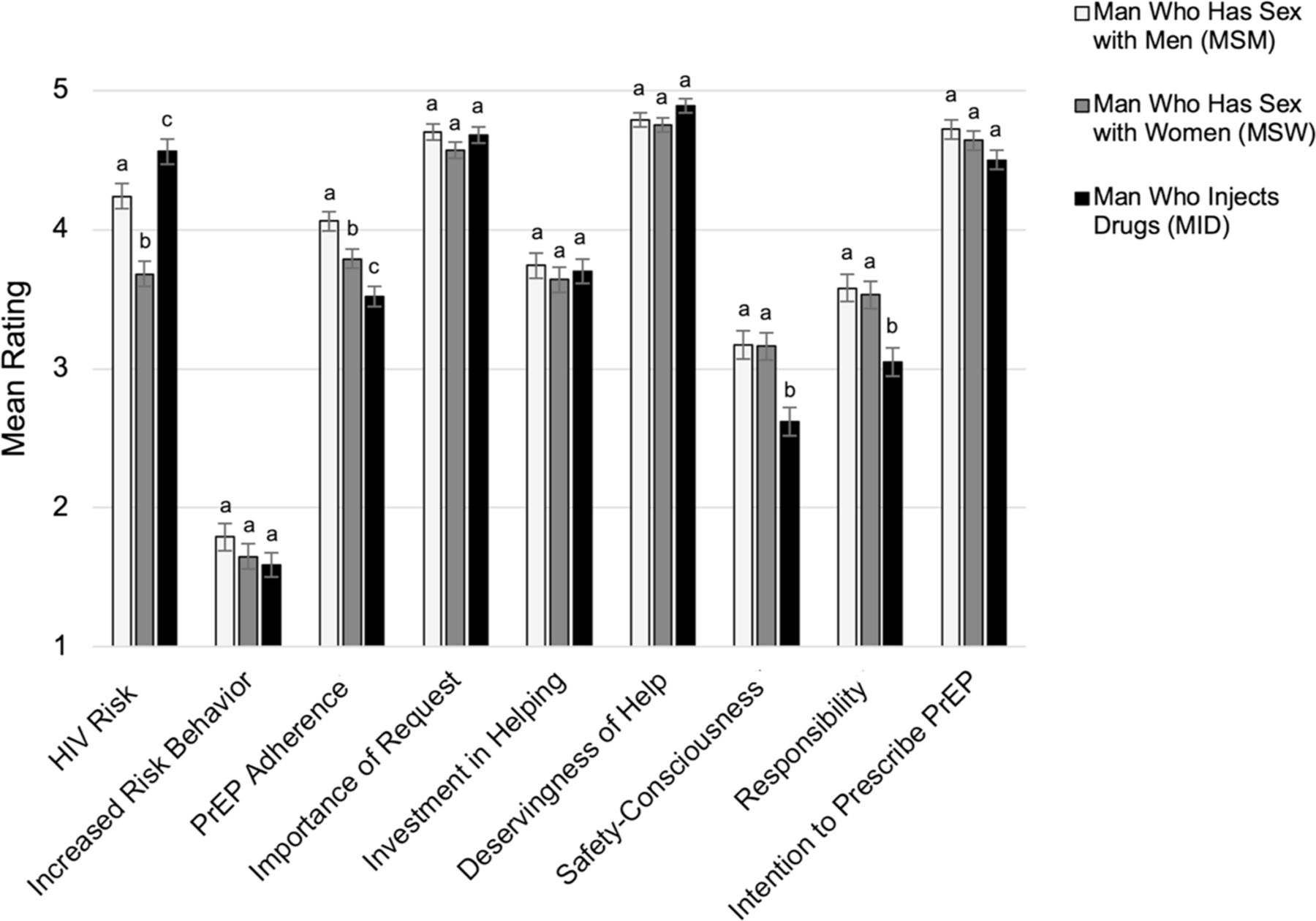
Differences in clinical judgment by patient risk behavior. Mean ratings and error bars represent estimated marginal means and standard errors. For each clinical judgment, different letters indicate statistically significant mean differences between two groups according to post-hoc pairwise comparisons (p < 0.050). For example, as indicated by differing letters (a–c), the MSM was judged to be at significantly higher HIV risk than the MSW, and the MID was judged to be at significantly higher HIV risk than both the MSM and the MSW
Indirect Effects of Patient Race and Risk Behavior on Intention to Prescribe PrEP
Mediation analyses were conducted to test the indirect effects of the experimentally manipulated patient characteristics on intention to prescribe, with the eight other clinical judgments positioned as parallel mediators as depicted in Fig. 1: Model B. Results of the parallel multiple mediator analyses are summarized in Tables 4 and 5 and Fig. 4. No indirect effects of patient race on prescribing intention were detected via any of the proposed mediating pathways. An indirect effect of patient sexual orientation on PrEP prescribing intention was found through anticipated PrEP adherence, with providers anticipating greater PrEP adherence by the MSM vs. the MSW patient, which was associated with greater intention to prescribe PrEP for the MSM patient.
Table 4.
Indirect effects of patient characteristics on prescribing intention: race and sexual orientation indirect effects
| Mediator | Patient race effectsa |
Patient sexual orientation effectsb |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Black (1) vs. White (0) |
MSM (1) vs. MSW (0) |
|||||||||||
| Indirect effect | SE | 95% CI | Partially standardized indirect effect | SE | 95% CI | Relative indirect effect | SE | 95% CI | Partially standardized relative indirect effect | SE | 95% CI | |
|
| ||||||||||||
| HIV risk | 0.00 | 0.01 | [− 0.01, 0.01] | 0.00 | 0.01 | [− 0.02, 0.02] | 0.02 | 0.03 | [− 0.03, 0.08] | 0.03 | 0.05 | [− 0.05, 0.13] |
| Increased risk behavior | 0.00 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.01 | [− 0.01, 0.04] | 0.00 | 0.01 | [− 0.02, 0.02] | 0.00 | 0.01 | [− 0.03, 0.03] |
| PrEP adherence | 0.02 | 0.01 | [− 0.01, 0.05] | 0.03 | 0.02 | [− 0.01, 0.07] | 0.04 | 0.02 | [0.01, 0.10]* | 0.07 | 0.04 | [0.01, 0.16]* |
| Importance of request | 0.04 | 0.03 | [− 0.01, 0.10] | 0.06 | 0.04 | [− 0.01, 0.15] | 0.05 | 0.04 | [− 0.01, 0.13] | 0.08 | 0.06 | [− 0.02, 0.20] |
| Investment in helping | 0.00 | 0.01 | [− 0.01, 0.02] | 0.01 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.01 | [− 0.01, 0.04] |
| Deservingness of help | 0.00 | 0.01 | [− 0.02, 0.04] | 0.01 | 0.02 | [− 0.03, 0.06] | 0.02 | 0.02 | [− 0.01, 0.08] | 0.03 | 0.04 | [− 0.01, 0.13] |
| Safety-consciousness | − 0.02 | 0.02 | [− 0.06, 0.01] | − 0.03 | 0.03 | [− 0.10, 0.02] | − 0.01 | 0.02 | [− 0.05, 0.03] | − 0.01 | 0.03 | [− 0.08, 0.04] |
| Responsibility | 0.03 | 0.02 | [0.00, 0.08]c | 0.04 | 0.03 | [− 0.01, 0.12] | 0.02 | 0.02 | [− 0.02, 0.07] | 0.03 | 0.04 | [− 0.04, 0.11] |
|
| ||||||||||||
| Direct effect | SE | 95% CI | Partially Standardized direct effect | Relative direct effect | SE | 95% CI | Partially standardized relative direct effect | |||||
|
| ||||||||||||
| 0.00 | 0.06 | [− 0.13, 0.13] | 0.00 | 0.01 | 0.08 | [− 0.16, 0.17] | 0.01 | |||||
|
| ||||||||||||
| Total effect | SE | 95% CI | Partially standardized total effect | Relative total effect | SE | 95% CI | Partially standardized relative total effect | |||||
|
| ||||||||||||
| 0.08 | 0.08 | [− 0.07, 0.22] | 0.12 | 0.15 | 0.09 | [− 0.03, 0.33] | 0.23 | |||||
No contrast effects are shown because there were no significant specific indirect effects
MSM man who has sex with men, MSW man who has sex with women
Based on bootstrapped analysis of parallel multiple mediator model with dichotomous predictor (patient race) adjusting for age, gender, race, sexual orientation, provider type, HIV specialization, practice setting, PrEP familiarity, PrEP experience, and patient risk behavior (MID, MSM, or MSW)
Based on bootstrapped analysis of parallel multiple mediator model with multicategorical predictor (patient risk behavior) adjusting for age, gender, race, sexual orientation, provider type, HIV specialization, practice setting, PrEP familiarity, PrEP experience, and patient race (Black or White). Indirect, direct, and total effects reported are relative effects because patient risk behavior is multicategorical
c95% CI [− 0.0045, 0.0829] without rounding and therefore statistically non-significant
p < 0.05
Table 5.
Indirect effects of patient characteristics on prescribing intention: injection drug use indirect effects
| Mediator | Patient injection drug use effectsa |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MID (1) vs. MSM (0) |
MID (1) vs. MSW (0) |
|||||||||||
| Relative indirect effect | SE | 95% CI | Partially standardized relative indirect effect | SE | 95% CI | Relative indirect effect | SE | 95% CI | Partially standardized relative indirect effect | SE | 95% CI | |
|
| ||||||||||||
| HIV risk | 0.01 | 0.02 | [− 0.02, 0.05] | 0.02 | 0.03 | [− 0.03, 0.08] | 0.03 | 0.04 | [− 0.05, 0.12] | 0.04 | 0.07 | [− 0.08, 0.20] |
| Increased risk behavior | 0.00 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.02 | [− 0.02, 0.05] | 0.00 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.02 | [− 0.02, 0.05] |
| PrEP adherence | − 0.09 | 0.04 | [− 0.17, − 0.02]* | − 0.14 | 0.06 | [− 0.27, − 0.03]* | − 0.04 | 0.02 | [− 0.10, − 0.01]* | − 0.07 | 0.04 | [− 0.15, − 0.01]* |
| Importance of request | − 0.02 | 0.03 | [− 0.09, 0.04] | − 0.03 | 0.05 | [− 0.14, 0.05] | 0.03 | 0.03 | [− 0.03, 0.09] | 0.04 | 0.05 | [− 0.05, 0.14] |
| Investment in helping | 0.00 | 0.01 | [− 0.02, 0.01] | 0.00 | 0.01 | [− 0.03, 0.02] | 0.00 | 0.01 | [− 0.01, 0.03] | 0.01 | 0.01 | [− 0.02, 0.04] |
| Deservingness of help | 0.01 | 0.01 | [− 0.03, 0.03] | 0.01 | 0.02 | [− 0.05, 0.05] | 0.03 | 0.02 | [0.00, 0.07]*b | 0.04 | 0.03 | [0.00, 0.12]*c |
| Safety-consciousness | 0.06 | 0.04 | [− 0.01, 0.15] | 0.09 | 0.06 | [− 0.02, 0.23] | 0.05 | 0.04 | [− 0.01, 0.13] | 0.08 | 0.06 | [− 0.02, 0.20] |
| Responsibility | − 0.08 | 0.04 | [− 0.17, − 0.01]* | − 0.12 | 0.06 | [− 0.26, − 0.01]* | − 0.06 | 0.03 | [− 0.14, − 0.01]* | − 0.09 | 0.05 | [− 0.21, − 0.01]* |
|
| ||||||||||||
| Relative direct effect | SE | 95% CI | Partially standardized relative direct effect | Relative direct effect | SE | 95% CI | Partially standardized relative direct effect | |||||
|
| ||||||||||||
| − 0.18 | 0.09 | [− 0.35, − 0.01]* | − 0.28 | − 0.17 | 0.09 | [− 0.35, 0.01] | − 0.27 | |||||
|
| ||||||||||||
| Relative total effect | SE | 95% CI | Partially standardized relative total effect | Relative total effect | SE | 95% CI | Partially standardized relative total effect | |||||
|
| ||||||||||||
| − 0.28 | 0.09 | [− 0.47, − 0.10]* | − 0.45 | − 0.13 | 0.09 | [− 0.32, 0.05] | − 0.21 | |||||
|
| ||||||||||||
| Significant specific indirect effects contrasted | Contrast effectd | SE | 95% CI | Partially standardized contrast effect | SE | 95% CI | Contrast effectd | SE | 95% CI | Partially standardized contrast effect | SE | 95% CI |
|
| ||||||||||||
| PrEP adherence vs. deservingness of help | – | – | – | – | – | – | 0.00 | 0.03 | [− 0.06, 0.08] | 0.00 | 0.05 | [− 0.09, 0.12] |
| PrEP adherence vs. responsibility | 0.04 | 0.07 | [− 0.10, 0.18] | 0.07 | 0.11 | [− 0.16, 0.28] | − 0.05 | 0.05 | [− 0.16, 0.05] | − 0.08 | 0.08 | [− 0.25, 0.08] |
| Deservingness of help vs. responsibility | – | – | – | – | – | – | − 0.05 | 0.05 | [− 0.16, 0.04] | − 0.08 | 0.08 | [− 0.12, 0.10] |
MSM man who has sex with men, MSW man who has sex with women, MID man who injects drugs
Based on bootstrapped analysis of parallel multiple mediator model with multicategorical predictor (patient risk behavior) adjusting for age, gender, race, sexual orientation, provider type, HIV specialization, practice setting, PrEP familiarity, PrEP experience, and patient race (Black or White). Indirect, direct, and total effects reported are relative effects because patient risk behavior is multicategorical
95% CI [0.0005, 0.0720] without rounding and therefore statistically significant
95% CI [0.0007, 0.1157] without rounding and therefore statistically significant
Contrasts effects represent the difference in absolute magnitude of two specific indirect effects (mediational pathways). Only contrast effects involving significant specific indirect effects are shown. The patient risk multicategorical variable was recoded into dichotomous variables to generate contrast effects
p < 0.05
Fig. 4.
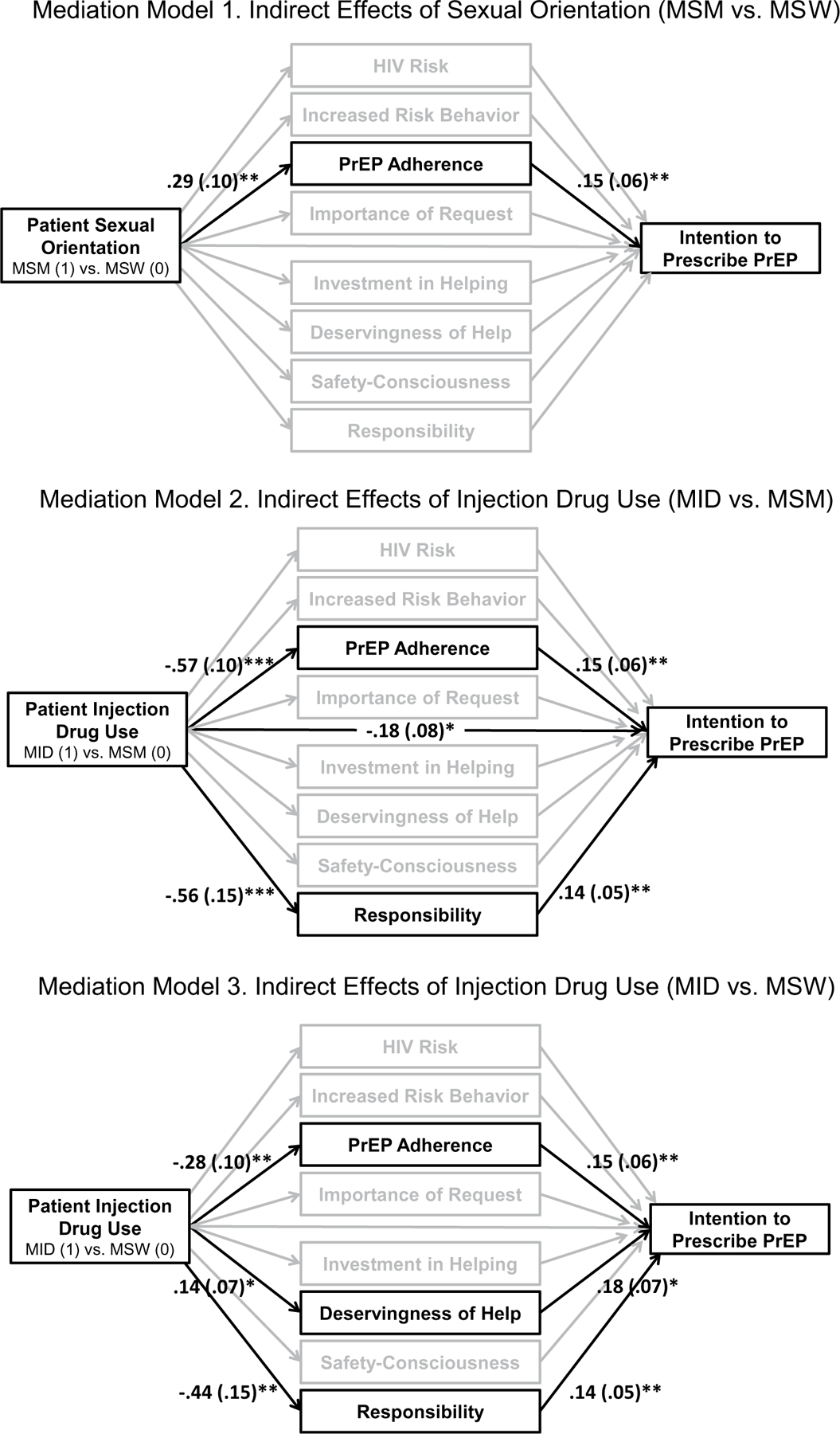
Indirect effects of patient characteristics on prescribing intention. Coefficients and standard errors are shown for significant indirect and direct effects. Model 1 shows that the MSM was judged as more likely to be adherent to PrEP than the MSW, which was associated with greater intention to prescribe PrEP. Model 2 shows that the MID was judged as less likely to be adherent to PrEP and less responsible than the MSM, which were associated with lower intention to prescribe PrEP. Model 3 shows that the MID was judged as less likely to be adherent to PrEP and less responsible than the MSW, which were associated with lower intention to prescribe PrEP. Additionally, the MID was judged as more deserving of help than the MSW, which was associated with greater intention to prescribe PrEP. *p < 0.05
Indirect effects of patient injection drug use on PrEP prescribing intention were found with respect to three mediators: anticipated PrEP adherence, deservingness of help, and perceived patient responsibility. Compared with the MSM patient, the MID patient was judged as being less adherent and less responsible, which in turn were associated with lower intention to prescribe PrEP. Contrast effects indicated that there were no significant differences in the absolute magnitude of these two specific indirect effects, suggesting that the two mediational pathways (via adherence and responsibility) did not differ in strength. Compared with the MSW patient, the MID patient was again judged to be less adherent and less responsible, which in turn were associated with lower intention to prescribe PrEP. However, the MID patient was also judged as more deserving of help than the MSW patient, which was associated with greater intention to prescribe PrEP. Contrast effects indicated that there were no significant differences in the absolute magnitude of the three specific indirect effects, suggesting that the three mediational pathways (via adherence, deservingness of help, and responsibility) did not differ in strength.
Moderated mediation was performed to determine whether any of the indirect effects of the experimentally manipulated patient characteristics on intention to prescribe PrEP varied systematically according to another variable, adjusting for background characteristics. The analytic models that were tested are summarized in Online Appendix 2 (see supplementary materials). The first analysis examining whether the indirect effects of patient risk behavior varied according to patient race yielded no significant interaction effects, suggesting that indirect effects of the patient’s risk behavior on prescribing intention were not impacted by whether the patient was Black or White.
Moderating Effects of Provider Prejudice
Subsequent moderated mediation analyses examined whether the indirect effects of patient characteristics on PrEP prescribing intentions varied according to the corresponding forms of provider prejudice as depicted in Fig. 1: Model C. Provider prejudice did not moderate any indirect effects with one exception: Sexual prejudice moderated a single indirect effect of sexual orientation (MSM vs. MSW) on prescribing intention (Index of Moderated Mediation = − 0.06, SE = 0.03, 95% CI [− 0.13, – 0.00], p < 0.050]). Specifically, the indirect effect of sexual orientation (MSM vs. MSW) on prescribing intention through adherence, whereby the MSM patient was judged as being more likely to adhere to PrEP, which was associated with greater prescribing intention, was only significant for providers with relatively low levels (e.g., 16th percentile: b = 0.08, SE = 0.04, CI [0.01, 0.16], p < 0.050) and moderate levels (e.g., 50th percentile: b = 0.05, SE = 0.03, CI [0.01, 0.11], p < 0.050) of sexual prejudice. The indirect effect was not significant for providers with relatively high levels (e.g., 84th percentile: b = 0.01, SE = 0.02, CI [− 0.03, 0.06], p ≥ 0.050) of sexual prejudice. Examining the interaction from an alternative perspective, sexual prejudice was indirectly associated with intention to prescribe via adherence, such that providers expressing higher (vs. lower) levels of sexual prejudice judged the patient as less likely to adhere to PrEP, which was associated with lower prescribing intention, when the patient was an MSM (b = − 0.06, SE = 0.03, CI [− 0.12, 0.00], p < 0.050]. However, this same indirect association between sexual prejudice and intention to prescribe via adherence was not significant when the patient was an MSW (b = 0.00, SE = 0.02, CI − 0.03, 0.04], p ≥ 0.050). Neither explicit racial prejudice nor implicit racial prejudice moderated any indirect effects of patient race on prescribing intention. Likewise, prejudice against PWID did not moderate any of the indirect effects of injection drug use on prescribing intention. Results of supplemental moderation analyses are presented in Online Appendix 3 (see supplementary materials).
Replication of Analyses with Larger Analytic Sample
The pattern of results was similar when analyses were repeated with the larger analytic sample (n = 370), including those participants who failed the attention/manipulation check. As was the case with the restricted sample, the adjusted MANCOVA revealed a significant effect of risk behavior but not race or risk × race effects. Post-hoc comparisons revealed the same pairwise differences among the MSM, MSW, and MID conditions as in the restricted sample. The marginally greater intention to prescribe PrEP to the MSM vs. the MID patient found in the restricted sample was significant in this larger sample (p = 0.004). Whereas no significant indirect effects of race on prescribing intention had been apparent in the adjusted parallel mediator analysis with the restricted sample, two of the eight indirect effects examined were significant in this larger sample: The Black patient’s request for PrEP was judged as more important than the White patient’s and the Black patient was judged as more responsible than the White patient, judgments that were in turn associated with higher intention to prescribe PrEP for the Black patient. There was no significant difference in the magnitude of these two indirect effects. The same indirect effect of sexual orientation on prescribing intention via anticipated patient adherence that was found with the restricted sample in the adjusted parallel mediator analysis was found in the larger sample, as were the indirect effects of injection drug use (MID vs. MSM and MID vs. MSW) on prescribing intention via adherence and perceived patient responsibility. There was no significant difference in the magnitude of the two significant indirect effects of injection drug use. The indirect effect of drug use (MID vs MSW) on intention to prescribe via deservingness of help observed in the restricted sample was not significant in the larger sample. Finally, none of the moderated mediation effects—including the single effect observed in the restricted sample—were significant. In summary, analyses repeated with the unrestricted sample upheld our primary findings, revealing biases in clinical judgment with adverse implications for PWID in particular and minimal variation according to provider prejudice.
Discussion
In this experimental survey study, two of three characteristics of a hypothetical male patient seeking PrEP influenced US providers’ PrEP-related clinical judgments: sexual orientation and injection drug use. The third patient characteristic, race, had no significant effect on any of the clinical judgments assessed. The observed effects of patient sexual orientation and injection drug use were not significantly affected by patient race (i.e., no intersectional biases were detected) and largely did not vary according to provider prejudice.
Findings in Context
Patient Sexual Orientation and Provider Sexual Prejudice
With respect to the hypothetical patient’s sexual orientation, the present work extends past studies [11–13] by experimentally manipulating patient sexual orientation (MSM vs. MSW) and examining the interaction of patient sexual orientation and provider explicit sexual prejudice relative to clinical judgments. Our hypotheses that (a) the MSM patient would be judged as more likely to increase risk behavior and as less safety-conscious and responsible than the MSW patient, (b) these judgments would function as mechanisms via which MSM sexual orientation was indirectly associated with lower intention to prescribe PrEP, and (c) provider explicit sexual prejudice would moderate these specific indirect pathways were not supported. However, differences in clinical judgments did emerge: The MSM patient was judged as being at greater risk for HIV and more likely to adhere to PrEP than the MSW patient. The perception of MSM being at greater risk for HIV aligns with the epidemiological distribution of HIV in the US [71]. It is also consistent with the greater per-act likelihood of HIV transmission for penileanal insertive sex (the type of sex specified in the medical record of the MSM patient) vs. penile-vaginal sex (the type of sex specified in the medical record of the MSW patient), which was communicated to providers prior to presentation of the fictitious medical record [58, 59]. The assumption that the MSM patient would be more adherent than the MSW patient converges with perceptions expressed by the US general public about gay men being more likely than people in general to adhere to PrEP [72] and judgments made by medical students about gay men being more likely to adhere to PrEP than heterosexual women (albeit not other groups) [13]. Although this assumption is stereotypical, it nonetheless appeared to help rather than hinder PrEP access for the MSM patient when endorsed by providers in this study. That is, among providers with relatively low and moderate levels of sexual prejudice, the favorable judgment about adherence served as a mechanism through which the MSM patient’s sexual orientation was associated with increased provider intention to prescribe PrEP.
At the same time, corroborating previous work with medical students [12], provider sexual prejudice was negatively associated with anticipated adherence when the patient was an MSM. Additionally, there was a significant negative indirect effect of provider sexual prejudice on prescribing intention via adherence for the MSM patient: Providers expressing higher (vs. lower) levels of sexual prejudice judged the MSM patient as less likely to adhere to PrEP, which was associated with lower prescribing intention.
Patient Injection Drug Use and Provider Prejudice Against PWID
With respect to the hypothetical patient’s use of injection drugs, consistent with our hypotheses, the MID patient was judged as being less likely to adhere to PrEP, less safety-conscious, and less responsible than either of the other two patients (MSM or MSW). He was also judged to be at greater HIV risk. As hypothesized, less favorable judgments about adherence and responsibility functioned as mechanisms through which the patient’s drug use decreased providers’ intention to prescribe PrEP for him. However, relative to the MSW patient only, an offsetting effect was observed through a third mechanism—deservingness of help. Specifically, the patient who injected drugs was considered more deserving of help than the MSW patient, which was associated with increased intention to prescribe PrEP for him. The indirect effects identified did not vary based on provider prejudice against PWID as hypothesized.
Providers’ judgment of the MID patient as less safety-conscious and responsible than the other patients coincides with the negative views of patients who use drugs commonly expressed in past research. Across 16 studies evaluating health professions students’ regard for different types of patients, including anticipatory feelings about treating them and perceptions about worthiness of care, patients who use drugs were consistently held in low regard—the lowest of all types of patients in 80% of studies [44]. Such low regard has been echoed among practicing providers, many of whom have expressed low empathy for patients who use drugs; a lack of motivation to work with them; and perceptions of such patients being aggressive, manipulative, rude, irresponsible, and uncooperative [45, 56, 57]. Past research has suggested that providers’ negative judgments have been driven in part by the culpability they ascribe to patients for their own drug use, perceiving such behavior and consequent development of a disorder as a function of controllable choices [56].
Our finding that providers anticipated the MID patient would be less likely to adhere to PrEP than other patients is consistent with their perception of him as being less safety-conscious and less responsible. Anticipated PrEP adherence was highly correlated with both judgments in our sample. Expectations about inferior adherence are congruent with the anticipated PrEP adherence challenges that providers have expressed in other research [28]. In actuality, although some people who use drugs have reported inconsistencies in their PrEP adherence [73], others have demonstrated adequate levels of adherence [41, 42], on par with non-users [41], or overcome initial adherence challenges when provided with added support [43, 74]. Thus, adherence concerns should not preclude PrEP prescription.
The biases related to anticipated adherence, perceived safety-consciousness, and perceived responsibility were particularly striking in the context of the medical scenario presented. The patient who injected drugs was perceived as less likely to adhere to PrEP, less safety-conscious, and less responsible than the patients who engaged in condomless sex (MSM and MSW) even though all three patients reported behavior that posed a risk for HIV and all three were proactively seeking preventive healthcare. Arguably, the act of requesting PrEP from a provider conveys motivation to take PrEP, conscientiousness about one’s safety, and responsibility for one’s health, yet the patient who engaged in injection drug use and abstained from sex was judged more harshly for his behavior than the patients who engaged in condomless sex and abstained from injection drug use. Differential judgment could partially reflect recognition of the greater per-act transmission risk associated with sharing needles with a person with HIV during injection drug use compared with condomless sex with a person with HIV [58, 59], discrepancies communicated to providers and reflected in their ratings of the patients’ HIV risk. However, the comparable ratings of safety-consciousness and responsibility between patients who engaged in anal vs. vaginal sex despite discernable differences in per-act transmission risk for these behaviors (also reflected in providers’ ratings) suggest harsher judgment ascribed to the act of injecting drugs itself.
Because only about 26% of US PWID are aware of PrEP [8] and therefore capable of initiating conversations about PrEP with a provider, most are dependent on their providers to broach the topic of PrEP. As a result, providers’ judgments about the adherence, safety-consciousness, and responsibility of most PWID presenting for care could be even less favorable than the judgments expressed in this study because the patients would not be displaying the same proactive, healthcare-seeking behavior. As suggested by the linkages to PrEP prescribing intention that emerged in the study, these unfavorable judgments could discourage providers from initiating conversations about PrEP altogether, compounding existing disparities in access driven by disparities in awareness [8].
The finding of a positive indirect effect of deservingness of help in the mediation model comparing the MID patient with the MSW patient, which suggested that the MID patient was judged as more deserving of help protecting himself from HIV and that this contributed to greater prescribing intention, was unexpected. Although this finding may seem out of step with other judgments of the MID patient and with past research documenting providers’ negative attitudes about substance-using patients [56], it may instead reflect nuance and evolution in providers’ thinking about PWID. For example, a provider may believe a patient’s drug use will contribute to adherence challenges and compromise the patient’s ability to carry out responsibilities because the provider is aware of the potential biological effects of drug use on executive functioning [75], reasoning that would not necessarily detract from the provider’s empathy for the patient or desire to help. The finding related to deservingness may also signal growing recognition that substance use disorders are a biologically-based form of chronic illness rather than a character flaw. Providers may be particularly inclined to perceive the patient as deserving of help to the extent that they attribute injection drug use to opioid prescription practices or other circumstances outside of the patient’s control. By contrast, providers are likely to view condomless sex as a controllable behavior rather than a symptom of disease and may consequently regard an MSW patient as less deserving or in need of help.
Patient Race and Provider Racial Prejudice
Compared with results related to other forms of bias, particularly bias related to injection drug use, results of the current study are more encouraging with respect to racial bias. There were no significant effects of patient race on the outcomes assessed in our analytic sample, and no moderating effects of provider explicit or implicit racial prejudice emerged. Whereas early experimental survey research with medical school students suggested the potential for racial bias to adversely affect assumptions about patient behavior and consequent intention to prescribe PrEP [11], a subsequent study with medical students [12] and the present study with practicing providers did not substantiate these earlier findings. In reconciling inconsistent evidence, it may be valuable to consider the increasing attention to racial prejudice that has emerged in the field of medicine [76, 77] and US society more broadly over time. Heightened awareness about racial bias could lead providers to exercise greater vigilance to guard against racial bias in their judgment of Black patients.
Clinical and Public Health Implications
Insights for Future Interventions
A critical issue illuminated by the current study is the potential for provider biases related to patient injection drug use to adversely affect their clinical judgment. Findings suggest that biases in judgments about a PWID not only occur but can influence PrEP prescribing decisions. Our finding that reported explicit prejudice against PWID was low in our sample and did not moderate the indirect effects of patient drug use on prescribing intention suggests that even providers who do not consciously harbor prejudice against PWID may nonetheless doubt the capacity of PWID to effectively manage a PrEP regimen. Such biases are especially disconcerting given the multiple benefits that PrEP offers to PWID. Injection-related HIV risk commonly co-occurs with sexual HIV risk, and PrEP uniquely protects against both forms of risk [78]. Additionally, PrEP promotes engagement in healthcare more generally, which may be especially advantageous given the prospective health risks and complications that can coincide with drug use [79].
In order for PWID to attain the benefits of PrEP, PWID must be informed about PrEP and have access to it. Both within and beyond the healthcare system, health education campaigns are needed to increase PWID’s awareness not only that PrEP exists, but also that PrEP is an effective prevention option for them [8, 36]. Newly engaging providers already working with PWID to become PrEP prescribers and integrating PrEP education, prescription, and follow-up care into health settings where PWID are already accessing care could facilitate PrEP awareness and use among PWID [42, 80]. For example, psychiatrists treating substance use disorders may be particularly well suited to adopting PrEP services into their practice because they have established ongoing relationships with their patients, and some may have previous experience incorporating biomedical harm-reduction services (e.g., syringe exchange) into care [81]. Additionally, for those PWID who are not engaged in health services and may experience unique barriers to accessing continuous care in traditional clinical settings, PrEP uptake and persistence can be facilitated via community outreach, navigation, and support services [82].
It is imperative that providers’ biases about PWID do not exacerbate existing barriers to PrEP access and persistence that PWID encounter. Early research suggests malleability in providers’ explicit attitudes toward PWID. Training, exposure, and institutional support (e.g., opportunities for consultation) have been tied to more favorable attitudes among providers [83–87]. For example, providers who engaged in a 40-min eLearning module that encompassed stories about the lived experiences of PWID and interactive discussion expressed less negative attitudes toward PWID, fewer concerns about PWID patients engaging in stereotypical behavior (e.g., violence, deceit), and lower support for discriminatory treatment of PWID enacted by other providers when evaluated immediately following the module [87]. Provider-targeted PrEP trainings and PrEP implementation programs could incorporate these or other interventions to address bias against PWID, which could yield gains that extend to provision of other health services for PWID.
Importantly, further research is needed to optimize interventions aimed at addressing bias against PWID and other forms of bias, including evaluation of their longer-term effects on provider attitudes and patient outcomes. Evidence that interventions can have a lasting impact on social biases—particularly implicit biases—is limited [67, 88–90], leading some experts to recommend that interventions target mitigation of the harm caused by biases rather than the biases themselves [67]. One strategy that has been suggested to mitigate such harm is discretion elimination, which refers to using a decision-making procedure that removes the opportunity for awareness about an individual’s characteristics, such as their use of injection drugs or race, to impact decisions made about that person [67, 88]. In the context of PrEP service delivery, this could involve a standardized approach whereby all adolescent and adult patients are educated about PrEP and all are given access to PrEP unless they have a medical contraindication (e.g., an HIV diagnosis, severe kidney disease). A number of early-adopting PrEP prescribers have previously advocated a standardized approach to care as a strategy for minimizing the impact of provider bias on clinical decisions, in some cases due to past experiences in which inaccurate assumptions about patients skewed their judgment [28]. Integrating PrEP into healthcare as a standard prevention option could help to increase awareness about PrEP among patients and their social networks and reduce the likelihood of patients feeling stigmatized, either because providers initiated a conversation about PrEP with them (implying the provider assumed them to be “high risk”) or because the provider did not initiate a conversation about PrEP with them (implying the provider intentionally withheld this resource due to disapproval of their behavior; [19,36,91]).
Caveat When Extrapolating Findings to Clinical Practice
The extent to which providers’ judgments about the hypothetical patient presented in the fictitious medical record represent their judgments if confronted with an analogous case in clinical practice is unknown. The experimental design that we used was advantageous in allowing us to systematically manipulate key characteristics while controlling others, thereby isolating biases related to sex-related vs. drug-related risks. We opted to create a fictitious medical record for use as our experimental stimulus rather than using a clinical vignette as has been done in past studies because we believed it would more closely emulate clinical practice. However, caution must be exercised when extrapolating findings to clinical practice or using them to infer training needs or lack thereof. This caveat applies to all of our findings—including both the presence of biases related to injection drug use and absence of nearly all racial, sexual, and intersectional biases.
In this section, we consider the relevance of the caveat to the absence of biases in particular and aspects of the study design that may have contributed to the absence of biases given the seeming misalignment of these findings with the original vignette-based medical student study [11] along with many firsthand accounts of interpersonal racial, sexual, and intersectional biases reported in clinical encounters. For example, MSM have reported encountering judgmental reactions from providers upon inquiring about PrEP, including disapproval of their presumed motivations for seeking PrEP and homonegativity in response to disclosure of their sexual orientation [54, 55, 92]. Black MSM in particular have described unique forms of stigmatization by providers (e.g., fetishization) and vulnerability to mistreatment due to their intersecting racial and sexual identities, which have discouraged them from seeking PrEP [52, 53].
It is possible that biases would have emerged in our study among providers harboring higher levels of prejudice. Overall, providers in our sample reported minimal explicit prejudice, and they exhibited similar albeit slightly weaker implicit racial prejudice than other provider samples on average [93]. Biases may also have emerged if other outcomes had been assessed. Collectively, research to date has yielded stronger evidence for associations between provider implicit prejudice and patient-provider communication than for associations between provider implicit prejudice and treatment recommendations [94].
Additionally, previous studies have suggested that biases are more likely to manifest in clinical decision-making when providers are experiencing conditions that involve time pressure and/or enhance their cognitive load (e.g., multitasking) [95, 96]. The context in which providers made clinical judgments in the present study—an online survey free of the time limitations and distractions commonly encountered in clinical practice—was one in which physicians may have had adequate cognitive resources to limit the impact of racial and sexual prejudice on clinical judgments. Furthermore, they may have been more motivated to do so to the extent that they regarded racial and sexual prejudice to be less acceptable than prejudice against PWID [97].
The characterization of the patient and medical scenario also deserves consideration when making inferences based on study findings. In all study conditions, the patient had informed the provider of behavioral risk, was aware of PrEP, and was proactively seeking a prescription. In clinical settings where PrEP counseling and provision are not part of standard care, disparities in patients’ awareness and comfort initiating conversations about PrEP or disclosing behavioral risk could translate to disparities that were indiscernible in the current study. For example, men who disclose to their providers that they have sex with men are more likely to be offered PrEP and less likely to have requests for PrEP denied [22]. Due to historical mistreatment, inequitable disruptions in care continuity, and other circumstances caused by social injustice, Black MSM may be less likely to disclose their sexuality than White MSM [52, 53, 98, 99].
Furthermore, past research has suggested that ambiguity surrounding the proper course of care may differentially affect providers’ judgment of Black and White patients and treatment decision-making [100]. Such ambiguity was lacking in the current study: We deliberately portrayed all patients’ risk for HIV as very high so that their potential to benefit from PrEP was unquestionable. All three patients were exchanging bodily fluids on an ongoing basis with a partner with HIV whose HIV viral load was not suppressed. Additionally, the patient was described as healthy and medically uncomplicated, with no history of other illnesses, past hospitalizations, medications, or medical contraindications on record. In reality, many patients present with a more ambiguous level of HIV risk than the patient in our study—because they are not engaging in behavior that poses such high risk or because they do not feel comfortable disclosing it—but could nonetheless benefit from PrEP. Additionally, patients present with medical comorbidities or social circumstances that may challenge providers’ confidence in their PrEP candidacy and openness to prescribing for them. These complicating factors may be more prevalent among communities whose stigmatized social statuses confer enhanced vulnerability to health problems, socioeconomic disadvantage, housing instability, and discrimination [101].
Limitations and Future Directions
In addition to the caveat described above, the following study limitations merit consideration and offer insights for future research. First, our sample of providers is unlikely to be representative of US HIV and primary care providers broadly in terms of sociodemographic and clinical characteristics, and generalizability is correspondingly limited. Most providers (77.0%) reported practicing in urban settings, many (40.0%) practiced in the Northeastern US, and the vast majority had clinical experience caring for MSM patients (98.9%) and patients who inject drugs (96.8%). Additionally, participants were highly aware of and experienced with PrEP prescription: All but one participant had some level of familiarity with PrEP, and 78.9% had prescribed it, percentages that are considerably higher than those typically reported by providers, particularly at the time that data were collected (2016–2017; [17]). This is likely because many (56.2%) of our participants were recruited through the email distribution list for an HIV-focused professional organization composed of medical professional involved in HIV prevention and care (American Academy of HIV Medicine). Findings may not generalize to providers with less familiarity with HIV and PrEP. Furthermore, participants cannot be assumed to represent the sources from which they were recruited, as they composed a minority of providers invited (e.g., 6.9% of American Academy of HIV Medicine members emailed and 2.5% of Society of General Internal Medicine members emailed). Unfortunately, suboptimal response rates have been a widely shared limitation of online survey studies investigating medical providers’ attitudes about PrEP to date [102].
As noted earlier, the generalizability of our findings is also limited to the extent that providers in our analytic sample had lower prejudice than the larger population of providers [92]. Furthermore, we found that participants who were initially excluded from the analytic sample when restricting it to participants who passed the attention/manipulation check had, on average, higher levels of explicit prejudice. The overall pattern of study findings was largely the same when we repeated the analyses including participants who failed the attention/manipulation check. However, given that there may be systematic differences in attention to patient characteristics by level of prejudice, we recommend future experimental studies in this area report findings from both the restricted and unrestricted analyses as we have done here.
Second, only about half of participants who completed all of the self-report measured proceeded to complete the race IAT that followed. This may be due to survey fatigue or time limitations that prompted premature discontinuation of the study at an obvious transition point, or a lack of desire to engage in the stimulus–response task. However, we suspect the more likely explanation is that the software that we employed to administer the IAT (Inquisit by Millisecond; https://www.millisecond.com/) required participants to download a plugin. Participants may have been understandably wary of installing outside software on their device or unable to do so because of workplace restrictions. In future research involving IAT administration, we recommend using IATgen or other software that does not require participant download ([103]; https://iatgen.wordpress.com/).
Third, the generalizability of the conclusions that we derived from providers’ differential judgments about a specific patient to other patients with divergent characteristics is uncertain. Providers may have judged patients of other ages, sexes, employment statuses, insurance statuses, health statuses, or levels of health agency differently. Our patient was described as a 31-year-old male who was employed, insured, healthy, and proactively seeking PrEP. Whereas intention to prescribe PrEP for the patient was high across conditions, it may have been less so in a female patient condition, for example, given documented discrepancies in PrEP discussion with female vs. male patients at risk for HIV [104].
Likewise, our findings may not generalize to MSM, MSW, and MID patients whose social/behavioral histories deviate from those described in the fictitious medical record presented. For example, whereas no significant difference was detected in providers’ intention to prescribe PrEP for the MSM vs. MSW patients, both of whom were reportedly engaging in insertive sex, providers may be more inclined to prescribe for an MSM who engages in receptive anal sex given the substantially greater per-act HIV transmission risk that receptive anal sex carries compared with insertive sex [58, 59], which could result in a significant discrepancy in prescribing intention relative to an MSW patient.
Fourth, our fictitious medical record captured the patient’s sex as male or female but did not specify the patient’s gender identity or sexual orientation. Although we describe the patient as a “man” throughout, doing so assumes he identifies as a man. Given that transgender and gender nonbinary people are disproportionately affected by HIV, particularly those who are Black or Latino/x/a [105–107], understanding biases related to gender and their intersection with biases based on race, sexual orientation, and other characteristics is an important avenue for future research. We recommend that studies employing an experimental design similar to the one used in the present study specify patient sex, gender, and sexual orientation in separate fields of the fictitious medical record and consider distinguishing between sexual behavior, sexual identity, and other dimensions of sexual orientation.
Fifth, we used pre-established measures to assess prejudice that were not matched on content. Thus, associations can be examined, but scores cannot be directly compared to infer the strength of one form of prejudice over another. Additionally, our measures of explicit sexual prejudice and implicit racial prejudice were male-specific. That is, sexual prejudice scale items were worded to be about “gay men,” and the race IAT included only male faces. Our measures of explicit racial prejudice and explicit prejudice against PWID were gender non-specific: Scale items were worded to be about “Blacks” or “injection drug users,” respectively. Thus, two of four measures of prejudice could have captured intersectional forms of prejudice involving gender, whereas the other two did not.
Sixth, although the conceptual models that we tested were guided by van Ryn and colleagues’ social-cognitive theory of biases in clinical decision-making [25, 26], they did not include all proposed pathways and components of the theoretical model and thus represent a simplified version. A more nuanced application of the model to future work in this area could illuminate additional mechanisms and moderators.
Finally, we performed and reported multiple analyses (e.g., MANCOVA, mediation) that imply causal associations among variables despite our data being cross-sectional. Our use of an experimental design is a strength of the study because the design enables causal claims about the effects of patient race and risk (i.e., the experimentally manipulated variables) on subsequent clinical judgments made about the patient [68]. However, causal inferences made about other variables rest on logic, theory, and earlier empirical evidence and must therefore be interpreted with caution. For example, considering the causal pathways between mediating clinical judgments and PrEP prescribing intention in our multiple mediator models, theory supports providers’ beliefs about a patient influencing treatment decision-making [25, 26], previous empirical work has suggested a causal linkage between several of the mediating judgments and prescribing intention [37, 108, 109], and we attempted to statistically control for potential confounding variables; nonetheless, it is possible that another variable unaccounted for in our models caused both the mediating judgments and prescribing intention rather than the mediating judgments themselves causing prescribing intention [68].
Conclusion
The present study demonstrated the potential for provider biases, particularly biases against PWID, to affect clinical judgment in the context of PrEP service delivery. The past two decades have brought heightened attention to healthcare disparities and the need to address provider biases related to race [77, 110] and sexual orientation [111, 112] and have coincided with waning explicit and implicit prejudice against racial and sexual minorities among members of the US general public [113]. However, some providers may be less attuned to their biases based on drug use or the need to address such biases. Accordingly, it would be beneficial for provider-targeted PrEP training programs and protocols to sensitize providers to their own vulnerability to racial, sexual, injection drug use, and other biases that could cloud their judgment when providing PrEP care; to encourage a standardized approach to PrEP service delivery to mitigate the harm of such biases; and to explicitly underscore the value of PrEP for all people at risk for HIV, including PWID.
Supplementary Material
Acknowledgements
The authors are grateful to the providers who generously dedicated their time and effort to study participation. We are also grateful to the American Academy of HIV Medicine, the Society of General Internal Medicine, and the other professional organizations that assisted with recruitment.
Funding
This study was funded by the National Institute of Mental Health (Grant No. NIMH; K01-MH103080; PI: S.K. Calabrese). Resources and support were contributed by the Yale University Center for Interdisciplinary Research on AIDS (Grant No. P30-MH062294), the District of Columbia Center for AIDS Research (Grant No. P30-AI117970), and the Harvard University Center for AIDS Research (Grant No. P30-AI060354), all funded by the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIMH or the NIH.
Footnotes
Supplementary Information The online version contains supplementary material available at https://doi.org/10.1007/s10461-021-03495-3.
Code Availability Syntax for statistical analyses are available from the lead author (SKC) upon request.
Declarations
Conflict of interest SKC, KHM, and DSK have received compensation for their efforts in developing and/or delivering medical education related to PrEP. SKC received partial financial support from Gilead Sciences to attend a research conference. KHM has conducted research with unrestricted project support from Gilead Sciences, Merck, and ViiV Healthcare. DSK has been a consultant to Fenway Health for research studies funded by Gilead Sciences and has a pending grant with unrestricted project support from Merck. The authors have no other relevant financial or non-fianical interests to disclose.
Ethical Approval All study procedures were approved by the Yale University Human Subjects Committee (IRB #HSC-1308012487) and the George Washington University Office of Human Research (IRB #061636) prior to implementation. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to Participate Online informed consent to participate was obtained from all study participants.
Consent for Publication Participants were informed of the authors’ intention to publish the results from the study as part of the online consent process.
Although “MSW” and “MID” are not conventional abbreviations, we use them here (instead of the more commonly used “heterosexual man” or “PWID,” respectively) to more accurately represent the experimental conditions.
There is wide variation in how the term “sexual orientation” has been conceptualized and measured in research [50, 51]. In this study, we operationalized sexual orientation behaviorally according to the respective sex—male or female—of a patient’s current sexual partner. However, we acknowledge that partner sex at any given time may not represent the full spectrum of a patient’s sexual behavior and does not reflect psychological dimensions of a patient’s sexual orientation (e.g., identity, attraction).
Data Availability
Data are available from the lead author (SKC) upon request.
References
- 1.Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med 2010; 363(27):2587–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med 2012; 367(5):399–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med 2012; 367(5):423–34. [DOI] [PubMed] [Google Scholar]
- 4.Choopanya K, Martin M, Suntharasamai P, Sangkum U, Mock PA, Leethochawalit M, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2013; 381(9883):2083–90. [DOI] [PubMed] [Google Scholar]
- 5.US Public Health Service. Preexposure prophylaxis for the prevention of HIV infection in the United States - 2017 update 2018.
- 6.US Preventive Services Task Force. Preexposure prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement. JAMA 2019; 321(22):2203–13. [DOI] [PubMed] [Google Scholar]
- 7.Saag MS, Gandhi RT, Hoy JF, Landovitz RJ, Thompson MA, Sax PE, et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2020 recommendations of the International Antiviral Society-USA Panel. JAMA 2020; 324(16):1651–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jones JT, Smith DK, Wiener J, August EM, Finlayson T, Wejnert C. Assessment of PrEP awareness, PrEP discussion with a provider, and PrEP use by transmission risk group with an emphasis on the Southern United States. AIDS Behav 2021; 25(9):2985–91. [DOI] [PubMed] [Google Scholar]
- 9.Kanny D, Jeffries WLT, Chapin-Bardales J, Denning P, Cha S, Finlayson T, et al. Racial/ethnic disparities in HIV preexposure prophylaxis among men who have sex with men - 23 urban areas, 2017. MMWR Morb Mortal Wkly Rep 2019; 68(37):801–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Harris NS, Johnson AS, Huang YA, Kern D, Fulton P, Smith DK, et al. Vital signs: status of human immunodeficiency virus testing, viral suppression, and HIV preexposure prophylaxis - United States, 2013–2018. MMWR Morb Mortal Wkly Rep 2019; 68(48):1117–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Calabrese SK, Earnshaw VA, Underhill K, Hansen NB, Dovidio JF. The impact of patient race on clinical decisions related to prescribing HIV pre-exposure prophylaxis (PrEP): assumptions about sexual risk compensation and implications for access. AIDS Behav 2014; 18(2):226–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Calabrese SK, Earnshaw VA, Krakower DS, Underhill K, Vincent W, Magnus M, et al. A closer look at racism and heterosexism in medical students’ clinical decision-making related to HIV pre-exposure prophylaxis (PrEP): implications for PrEP education. AIDS Behav 2018; 22(4):1122–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bunting SR, Feinstein BA, Hazra A, Garber SS. Effects of patient sexual orientation and gender identity on medical students’ decision-making regarding pre-exposure prophylaxis (PrEP) for HIV prevention: a vignette-based study. Sex Transm Dis 2021. 10.1097/OLQ.0000000000001488. [DOI] [PMC free article] [PubMed]
- 14.Leichliter JS, Cuffe KM, Kelley KR, Gift TL. Availability of STD and HIV clinical services: ending the HIV Epidemic (EHE) vs. non-EHE jurisdictions, 2018. Sex Transm Dis 2021. 10.1097/OLQ.0000000000001482. [DOI] [PMC free article] [PubMed]
- 15.Smith DK, Maier E, Betts J, Gray S, Kolodziejski B, Hoover KW. What community-based HIV prevention organizations say about their role in biomedical HIV prevention. AIDS Educ Prev 2016; 28(5):426–39. [DOI] [PubMed] [Google Scholar]
- 16.Tookes H, Yao K, Chueng T, Butts S, Karsner R, Duque M, et al. Pre-exposure prophylaxis access in federally qualified health centers across 11 United States metropolitan statistical areas. Int J STD AIDS 2019; 30(10):978–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhang C, McMahon J, Fiscella K, Przybyla S, Braksmajer A, LeBlanc N, et al. HIV pre-exposure prophylaxis implementation cascade among health care professionals in the United States: implications from a systematic review and meta-analysis. AIDS Patient Care STDS 2019; 33(12):507–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dovidio JF, Fiske ST. Under the radar: how unexamined biases in decision-making processes in clinical interactions can contribute to health care disparities. Am J Public Health 2012; 102(5):945–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Calabrese SK, Krakower DS, Mayer KH. Integrating HIV pre-exposure prophylaxis (PrEP) into routine preventive healthcare to avoid exacerbating disparities. Am J Public Health 2017; 107(12):1883–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dovidio JF, Gaertner SL. Intergroup bias. In: Fiske ST, Gilbert DT, Lindzey G, editors. Handbook of social psychology Hoboken: Wiley; 2010. p. 1084–121. [Google Scholar]
- 21.Brooks RA, Landrian A, Nieto O, Fehrenbacher A. Experiences of anticipated and enacted pre-exposure prophylaxis (PrEP) stigma among Latino MSM in Los Angeles. AIDS Behav 2019; 23(7):1964–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Furukawa NW, Maksut JL, Zlotorzynska M, Sanchez TH, Smith DK, Baral SD. Sexuality disclosure in U.S. gay, bisexual, and other men who have sex with men: impact on healthcare-related stigmas and HIV pre-exposure prophylaxis denial. Am J Prev Med 2020; 59(2):79–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Calabrese SK, Magnus M, Mayer KH, Krakower DS, Eldahan AI, Gaston Hawkins LA, et al. “Support your client at the space that they’re in”: pre-exposure prophylaxis (PrEP) prescribers’ perspectives on PrEP-related risk compensation. AIDS Patient Care STDS 2017; 31(4):196–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Doblecki-Lewis S, Jones D. Community federally qualified health centers as homes for HIV preexposure prophylaxis: perspectives from South Florida. J Int Assoc Provid AIDS Care 2016; 15(6):522–8. [DOI] [PubMed] [Google Scholar]
- 25.van Ryn M, Fu SS. Paved with good intentions: do public health and human service providers contribute to racial/ethnic disparities in health? Am J Public Health 2003; 93(2):248–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.van Ryn M, Burgess DJ, Dovidio JF, Phelan SM, Saha S, Malat J, et al. The impact of racism on clinician cognition, behavior, and clinical decision making. Du Bois Rev 2011; 8(1):199–218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pleuhs B, Quinn KG, Walsh JL, Petroll AE, John SA. Health care provider barriers to HIV pre-exposure prophylaxis in the United States: a systematic review. AIDS Patient Care STDS 2020; 34(3):111–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Calabrese SK, Tekeste M, Mayer KH, Magnus M, Krakower DS, Kershaw TS, et al. Considering stigma in the provision of HIV pre-exposure prophylaxis: reflections from current prescribers. AIDS Patient Care STDS 2019; 33(2):79–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Degenhardt L, Peacock A, Colledge S, Leung J, Grebely J, Vickerman P, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Glob Health 2017; 5(12):e1192–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cicero TJ, Ellis MS, Surratt HL, Kurtz SP. The changing face of heroin use in the United States: a retrospective analysis of the past 50 years. JAMA Psychiat 2014; 71(7):821–6. [DOI] [PubMed] [Google Scholar]
- 31.Peters PJ, Pontones P, Hoover KW, Patel MR, Galang RR, Shields J, et al. HIV infection linked to injection use of oxymorphone in Indiana, 2014–2015. N Engl J Med 2016; 375(3):229–39. [DOI] [PubMed] [Google Scholar]
- 32.Kuo I, Olsen H, Patrick R, Phillips G 2nd, Magnus M, Opoku J, et al. Willingness to use HIV pre-exposure prophylaxis among community-recruited, older people who inject drugs in Washington, DC. Drug Alcohol Depend 2016; 164:8–13. [DOI] [PubMed] [Google Scholar]
- 33.Schneider KE, White RH, O’Rourke A, Kilkenny ME, Perdue M, Sherman SG, et al. Awareness of and interest in oral pre-exposure prophylaxis (PrEP) for HIV prevention and interest in hypothetical forms of PrEP among people who inject drugs in rural West Virginia. AIDS Care 2021; 33(6):721–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sherman SG, Schneider KE, Park JN, Allen ST, Hunt D, Chaulk CP, et al. PrEP awareness, eligibility, and interest among people who inject drugs in Baltimore, Maryland. Drug Alcohol Depend 2019; 195:148–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Shrestha R, Karki P, Altice FL, Huedo-Medina TB, Meyer JP, Madden L, et al. Correlates of willingness to initiate pre-exposure prophylaxis and anticipation of practicing safer drug- and sex-related behaviors among high-risk drug users on methadone treatment. Drug Alcohol Depend 2017; 173:107–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carter G, Meyerson B, Rivers P, Crosby R, Lawrence C, Cope SD, et al. Living at the confluence of stigmas: PrEP awareness and feasibility among people who inject drugs in two predominantly rural states. AIDS Behav 2021; 8:1–12. [DOI] [PubMed] [Google Scholar]
- 37.Adams LM, Balderson BH. HIV providers’ likelihood to prescribe pre-exposure prophylaxis (PrEP) for HIV prevention differs by patient type: a short report. AIDS Care 2016; 28(9):1154–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Edelman EJ, Moore BA, Calabrese SK, Berkenblit GV, Cunningham C, Patel V, et al. Primary care physicians’ willingness to prescribe HIV pre-exposure prophylaxis for people who inject drugs. AIDS Behav 2017; 21(4):1025–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Smith DK, Mendoza MC, Stryker JE, Rose CE. PrEP awareness and attitudes in a national survey of primary care clinicians in the United States, 2009–2015. PLoS ONE 2016; 11(6):e0156592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Adams LM, Balderson BH, Brown K, Bush SE, Packett BJ 2nd. Who starts the conversation and who receives preexposure prophylaxis (PrEP)? A brief online survey of medical providers’ PrEP practices. Health Educ Behav 2018; 45(5):723–9. [DOI] [PubMed] [Google Scholar]
- 41.Hoenigl M, Jain S, Moore D, Collins D, Sun X, Anderson PL, et al. Substance use and adherence to HIV preexposure prophylaxis for men who have sex with men. Emerg Infect Dis 2018; 24(12):2292–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Shrestha R, Copenhaver M. Exploring the use of pre-exposure prophylaxis (PrEP) for HIV prevention among high-risk people who use drugs in treatment. Front Public Health 2018; 6:195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shrestha R, Altice F, Karki P, Copenhaver M. Developing an integrated, brief biobehavioral HIV prevention intervention for high-risk drug users in treatment: the process and outcome of formative research. Front Immunol 2017; 8:561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ducray K, Pilch M. Health student regard for substance-using patients as measured by the Medical Condition Regard Scale: a systematic review. Ir J Psychol Med 2017; 34(3):183–96. [DOI] [PubMed] [Google Scholar]
- 45.van Boekel LC, Brouwers EPM, van Weeghel J, Garretsen HFL. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013; 131(1):23–35. [DOI] [PubMed] [Google Scholar]
- 46.Biancarelli DL, Biello KB, Childs E, Drainoni M, Salhaney P, Edeza A, et al. Strategies used by people who inject drugs to avoid stigma in healthcare settings. Drug Alcohol Depend 2019; 198:80–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Fong C, Mateu-Gelabert P, Ciervo C, Eckhardt B, Aponte-Melendez Y, Kapadia S, et al. Medical provider stigma experienced by people who use drugs (MPS-PWUD): Development and validation of a scale among people who currently inject drugs in New York City. Drug Alcohol Depend 2021; 221:108589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.McMahan VM, Violette LR, Andrasik MP, Martin A, Garske L, Stekler JD. “I make sure my doctor doesn’t know that I use meth”: Perceived barriers to pre-exposure prophylaxis (PrEP) uptake among community peer educators in Seattle (WA, USA). Sexual Health 2020; 17(1):29–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Muncan B, Walters SM, Ezell J, Ompad DC. “They look at us like junkies”: Influences of drug use stigma on the healthcare engagement of people who inject drugs in New York City. Harm Reduct J 2020; 17(1):53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Sell RL. Defining and measuring sexual orientation: a review. Arch Sex Behav 1997; 26(6):643–58. [DOI] [PubMed] [Google Scholar]
- 51.Wolff M, Wells B, Ventura-DiPersia C, Renson A, Grov C. Measuring sexual orientation: a review and critique of U.S. data collection efforts and implications for health policy. J Sex Res 2017; 54(4–5):507–31. [DOI] [PubMed] [Google Scholar]
- 52.Quinn K, Bowleg L, Dickson-Gomez J. “The fear of being Black plus the fear of being gay”: the effects of intersectional stigma on PrEP use among young Black gay, bisexual, and other men who have sex with men. Soc Sci Med 2019; 232:86–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Quinn K, Dickson-Gomez J, Zarwell M, Pearson B, Lewis M. “A gay man and a doctor are just like, a recipe for destruction”: how racism and homonegativity in healthcare settings influence PrEP uptake among young Black MSM. AIDS Behav 2019; 23(7):1951–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Brooks RA, Nieto O, Landrian A, Fehrenbacher A, Cabral A. Experiences of pre-exposure prophylaxis (PrEP)-related stigma among Black MSM PrEP users in Los Angeles. J Urban Health 2020; 97(5):679–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Owens C, Hubach RD, Williams D, Lester J, Reece M, Dodge B. Exploring the pre-exposure prophylaxis (PrEP) health care experiences among men who have sex with men (MSM) who live in rural areas of the Midwest. AIDS Educ Prev 2020; 32(1):51–66. [DOI] [PubMed] [Google Scholar]
- 56.Brener L, Von Hippel W, Kippax S, Preacher KJ. The role of physician and nurse attitudes in the health care of injecting drug users. Subst Use Misuse 2010; 45(7–8):1007–18. [DOI] [PubMed] [Google Scholar]
- 57.Strauser DR, Ciftci A, O’Sullivan D. Using attribution theory to examine community rehabilitation provider stigma. Int J Rehabil Res 2009; 32(1):41–7. [DOI] [PubMed] [Google Scholar]
- 58.Patel P, Borkowf CB, Brooks JT, Lasry A, Lansky A, Mermin J. Estimating per-act HIV transmission risk: a systematic review. AIDS 2014; 28(10):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.US Centers for Disease Control and Prevention. HIV risk and prevention estimates: HIV risk behaviors; 2016. https://www.cdc.gov/hiv/risk/estimates/riskbehaviors.html.
- 60.Bertrand M, Mullainathan S. Are Emily and Greg more employable than Lakisha and Jamal? A field experiment on labor market discrimination. Am Econ Rev 2004; 94(4):991–1013. [Google Scholar]
- 61.Ewens M, Tomlin B, Wang LC. Statistical discrimination or prejudice? A large sample field experiment. Rev Econ Stat 2014; 96(1):119–34. [Google Scholar]
- 62.McConahay JB. Modern racism, ambivalence, and the Modern Racism Scale. Prejudice, discrimination, and racism San Diego: Academic Press; 1986. p. 91–125. [Google Scholar]
- 63.Morrison MA, Morrison TG. Development and validation of a scale measuring modern prejudice toward gay men and lesbian women. J Homosex 2002; 43(2):15–37. [DOI] [PubMed] [Google Scholar]
- 64.Palamar JJ, Kiang MV, Halkitis PN. Development and psychometric evaluation of scales that assess stigma associated with illicit drug users. Subst Use Misuse 2011; 46(12):1457–67. [DOI] [PubMed] [Google Scholar]
- 65.Greenwald AG, McGhee DE, Schwartz JL. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol 1998; 74(6):1464–80. [DOI] [PubMed] [Google Scholar]
- 66.Greenwald AG, Nosek BA, Banaji MR. Understanding and using the implicit association test: I. An improved scoring algorithm. J Pers Soc Psychol 2003; 85(2):197. [DOI] [PubMed] [Google Scholar]
- 67.Greenwald AG, Dasgupta N, Dovidio JF, Kang J, Moss-Racusin C, Teachman BA. Implicit bias remedies: what is known and what is not known [Unpublished manuscript] 2021. [Google Scholar]
- 68.Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach 2nd ed. New York: The Guilford Press; 2018. [Google Scholar]
- 69.Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr 2009; 76(4):408–20. [Google Scholar]
- 70.Hayes AF. Partial, conditional, and moderated moderated mediation: quantification, inference, and interpretation. Commun Monogr 2018; 85(1):4–40. [Google Scholar]
- 71.US Centers for Disease Control and Prevention. HIV surveillance report: diagnoses of HIV infection in the United States and dependent areas, 2019 2021.
- 72.Calabrese SK, Underhill K, Earnshaw VA, Hansen NB, Kershaw TS, Magnus M, et al. Framing HIV pre-exposure prophylaxis (PrEP) for the general public: how inclusive messaging may prevent prejudice from diminishing public support. AIDS Behav 2016; 20(7):1499–513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Felsher M, Ziegler E, Amico KR, Carrico A, Coleman J, Roth AM. “PrEP just isn’t my priority”: adherence challenges among women who inject drugs participating in a pre-exposure prophylaxis (PrEP) demonstration project in Philadelphia, PA, USA. Soc Sci Med 2021; 275:113809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Mistler CB, Copenhaver MM, Shrestha R. The pre-exposure prophylaxis (PrEP) care cascade in people who inject drugs: a systematic review. AIDS Behav 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Volkow ND, Koob GF, McLellan AT. Neurobiologic advances from the brain disease model of addiction. N Engl J Med 2016; 374(4):363–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Ben J, Cormack D, Harris R, Paradies Y. Racism and health service utilisation: a systematic review and meta-analysis. PLoS ONE 2017; 12(12):e0189900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Hardeman RR, Medina EM, Kozhimannil KB. Structural racism and supporting Black lives—the role of health professionals. N Engl J Med 2016; 375(22):2113–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Edeza A, Bazzi A, Salhaney P, Biancarelli D, Childs E, Mimiaga MJ, et al. HIV pre-exposure prophylaxis for people who inject drugs: the context of co-occurring injection- and sexual-related HIV risk in the US Northeast. Subst Use Misuse 2020; 55(4):525–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Visconti AJ, Sell J, Greenblatt AD. Primary care for persons who inject drugs. Am Fam Phys 2019; 99(2):109–16. [PubMed] [Google Scholar]
- 80.Roth AM, Tran NK, Felsher M, Gadegbeku AB, Piecara B, Fox R, et al. Integrating HIV preexposure prophylaxis with community-based syringe services for women who inject drugs: results from the Project SHE demonstration study. J Acquir Immune Defic Syndr 2021; 86(3):e61–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Bunting SR, Hazra A, Sheth NK. Psychiatrists as prescribers of HIV pre-exposure prophylaxis: an untapped resource for HIV prevention among patients living with mental illness. J Gay Lesbian Ment Health 2020. 10.1080/19359705.2020.1855007. [DOI] [Google Scholar]
- 82.Biello KB, Bazzi AR, Vahey S, Harris M, Shaw L, Brody J. Delivering preexposure prophylaxis to people who use drugs and experience homelessness, Boston, MA, 2018–2020. Am J Public Health 2021; 111(6):1045–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Ding L, Landon BE, Wilson IB, Wong MD, Shapiro MF, Cleary PD. Predictors and consequences of negative physician attitudes toward HIV-infected injection drug users. Arch Intern Med 2005; 165(6):618–23. [DOI] [PubMed] [Google Scholar]
- 84.Howard V, Holmshaw J. Inpatient staff perceptions in providing care to individuals with co-occurring mental health problems and illicit substance use. J Psychiatr Ment Health Nurs 2010; 17(10):862–72. [DOI] [PubMed] [Google Scholar]
- 85.Ford R, Bammer G, Becker N. Improving nurses’ therapeutic attitude to patients who use illicit drugs: workplace drug and alcohol education is not enough. Int J Nurs Pract 2009; 15(2):112–8. [DOI] [PubMed] [Google Scholar]
- 86.Ford R, Bammer G, Becker N. The determinants of nurses’ therapeutic attitude to patients who use illicit drugs and implications for workforce development. J Clin Nurs 2008; 17(18):2452–62. [DOI] [PubMed] [Google Scholar]
- 87.Brener L, Cama E, Hull P, Treloar C. Evaluation of an online injecting drug use stigma intervention targeted at health providers in New South Wales, Australia. Health Psychol Open 2017; 4(1):20551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Greenwald AG, Lai CK. Implicit social cognition. Annu Rev Psychol 2020; 71:419–45. [DOI] [PubMed] [Google Scholar]
- 89.Paluck EL, Porat R, Clark CS, Green DP. Prejudice reduction: progress and challenges. Annu Rev Psychol 2021; 72:533–60. [DOI] [PubMed] [Google Scholar]
- 90.Lai CK, Skinner AL, Cooley E, Murrar S, Brauer M, Devos T, et al. Reducing implicit racial preferences: II Intervention effectiveness across time. J Exp Psychol Gen 2016; 145(8):1001–16. [DOI] [PubMed] [Google Scholar]
- 91.Golub SA. PrEP stigma: implicit and explicit drivers of disparity. Curr HIV/AIDS Rep 2018; 15(2):190–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Thomann M, Grosso A, Zapata R, Chiasson MA. “WTF is PrEP?”: attitudes towards pre-exposure prophylaxis among men who have sex with men and transgender women in New York City. Cult Health Sex 2018; 20(7):772–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Sabin J, Nosek BA, Greenwald A, Rivara FP. Physicians’ implicit and explicit attitudes about race by MD race, ethnicity, and gender. J Health Care Poor Underserved 2009; 20(3):896–913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Hagiwara N, Dovidio JF, Stone J, Penner LA. Applied racial/ ethnic healthcare disparities research using implicit measures. Soc Cogn 2020; 38(Supplement):s68–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Burgess DJ, Phelan S, Workman M, Hagel E, Nelson DB, Fu SS, et al. The effect of cognitive load and patient race on physicians’ decisions to prescribe opioids for chronic low back pain: a randomized trial. Pain Med 2014; 15(6):965–74. [DOI] [PubMed] [Google Scholar]
- 96.Stepanikova I Racial-ethnic biases, time pressure, and medical decisions. J Health Soc Behav 2012; 53(3):329–43. [DOI] [PubMed] [Google Scholar]
- 97.Crandall CS, Eshleman A, O’Brien L. Social norms and the expression and suppression of prejudice: the struggle for internalization. J Pers Soc Psychol 2002; 82(3):359–78. [PubMed] [Google Scholar]
- 98.Philbin MM, Parker CM, Parker RG, Wilson PA, Garcia J, Hirsch JS. Gendered social institutions and preventive healthcare seeking for Black men who have sex with men: the promise of biomedical HIV prevention. Arch Sex Behav 2018; 47(7):2091–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Petroll AE, Mosack KE. Physician awareness of sexual orientation and preventive health recommendations to men who have sex with men. Sex Transm Dis 2011; 38(1):63–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Hirsh AT, Hollingshead NA, Ashburn-Nardo L, Kroenke K. The interaction of patient race, provider bias, and clinical ambiguity on pain management decisions. J Pain 2015; 16(6):558–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health 2013; 103(5):813–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Silverman TB, Schrimshaw EW, Franks J, Hirsch-Moverman Y, Ortega H, El-Sadr WM, et al. Response rates of medical providers to Internet surveys regarding their adoption of preexposure prophylaxis for HIV: methodological implications. J Int Assoc Provid AIDS Care 2018; 17:1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Carpenter TP, Pogacar R, Pullig C, Kouril M, Aguilar S, LaBouff J, et al. Survey-software implicit association tests: a methodological and empirical analysis. Behav Res Methods 2019; 51(5):2194–208. [DOI] [PubMed] [Google Scholar]
- 104.Yumori C, Zucker J, Theodore D, Chang M, Carnevale C, Slowikowski J, et al. Women are less likely to be tested for HIV or offered preexposure prophylaxis at the time of sexually transmitted infection diagnosis. Sex Transm Dis 2021; 48(1):32–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Becasen JS, Denard CL, Mullins MM, Higa DH, Sipe TA. Estimating the prevalence of HIV and sexual behaviors among the US transgender population: a systematic review and meta-analysis, 2006–2017. Am J Public Health 2019; 109(1):e1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Poteat T, Scheim A, Xavier J, Reisner S, Baral S. Global epidemiology of HIV infection and related syndemics affecting transgender people. J Acquir Immune Defic Syndr 2016; 72:S210–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Clark H, Babu AS, Wiewel EW, Opoku J, Crepaz N. Diagnosed HIV infection in transgender adults and adolescents: results from the National HIV Surveillance System, 2009–2014. AIDS Behav 2017; 21(9):2774–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Krakower D, Ware N, Mitty JA, Maloney K, Mayer KH. HIV providers’ perceived barriers and facilitators to implementing pre-exposure prophylaxis in care settings: a qualitative study. AIDS Behav 2014; 18(9):1712–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Villeneuve F, Cabot J-M, Eymard-Duvernay S, Visier L, Tribout V, Perollaz C, et al. Evaluating family physicians’ willingness to prescribe PrEP. Med Mal Infect 2020; 50(7):606–10. [DOI] [PubMed] [Google Scholar]
- 110.Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care Washington: The National Academies Press; 2003. [PubMed] [Google Scholar]
- 111.Institute of Medicine. The health of lesbian, gay, bisexual, and transgender people: building a foundation for better understanding Washington: Institute of Medicine; 2011. [PubMed] [Google Scholar]
- 112.Morris M, Cooper RL, Ramesh A, Tabatabai M, Arcury TA, Shinn M, et al. Training to reduce LGBTQ-related bias among medical, nursing, and dental students and providers: a systematic review. BMC Med Educ 2019; 19(1):325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Charlesworth TES, Banaji MR. Patterns of implicit and explicit attitudes: I. Long-term change and stability from 2007 to 2016. Psychol Sci 2019; 30(2):174–92. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available from the lead author (SKC) upon request.