

Abstract
Background
Nonadherence to antihypertensive medications is the leading cause of poor blood pressure control and thereby cardiovascular diseases and mortality worldwide.
Methods and Results
We investigated the global epidemiology, regional differences, and trend of antihypertensive medication nonadherence via a systematic review and meta‐analyses of data from 2010 to 2020. Multiple medical databases and clinicaltrials.gov were searched for articles. Observational studies reporting the proportion of patients with anti‐hypertensive medication nonadherence were included. The proportion of nonadherence, publication year, year of first recruitment, country, and health outcomes attributable to antihypertensive medication nonadherence were extracted. Two reviewers screened abstracts and full texts, classified countries according to levels of income and locations, and extracted data. The Joanna Briggs Institute prevalence critical appraisal tool was used to rate the included studies. Prevalence meta‐analyses were conducted using a fixed‐effects model, and trends in prevalence were analyzed using meta‐regression. The certainty of evidence concerning the effect of health consequences of nonadherence was rated according to Grading of Recommendations, Assessment, Development and Evaluations. A total of 161 studies were included. Subject to different detection methods, the global prevalence of anti‐hypertensive medication nonadherence was 27% to 40%. Nonadherence was more prevalent in low‐ to middle‐income countries than in high‐income countries, and in non‐Western countries than in Western countries. No significant trend in prevalence was detected between 2010 and 2020. Patients with antihypertensive medication nonadherence had suboptimal blood pressure control, complications from hypertension, all‐cause hospitalization, and all‐cause mortality.
Conclusions
While high prevalence of anti‐hypertensive medication nonadherence was detected worldwide, higher prevalence was detected in low‐ to middle‐income and non‐Western countries. Interventions are urgently required, especially in these regions. Current evidence is limited by high heterogeneity.
Registration
URL: www.crd.york.ac.uk/prospero/; Unique identifier: CRD42021259860.
Keywords: adherence, compliance, hypertension, meta‐analyses, prevalence
Subject Categories: Quality and Outcomes, Hypertension, Meta Analysis
Nonstandard Abbreviations and Acronyms
- MMAS
Morisky Medication Adherence Scale
- MPR
medication possession ratio
- WHO
World Health Organization
Clinical Perspective.
What Is New?
Anti‐hypertensive medication nonadherence was common globally (27%–40%), was more prevalent in low‐ to middle income and non‐Western countries, and did not improve between 2010 and 2020.
What Are the Clinical Implications?
Policymakers and clinicians should incorporate validated methods (eg, validated questionnaires, medication procession ratio, pill counting, electronic pills or pillbox, and biochemical detection by drug assays) into health care systems to routinely detect anti‐hypertensive medication nonadherence.
Once detected, clinicians could conceptualize the reasons for nonadherence, using the World Health Organization model, and manage them accordingly.
Medication adherence is defined as the “extent to which patients take their medication as prescribed.” 1 , 2 Although hypertension is one of the most common chronic conditions and a leading cause of death globally, 3 medication nonadherence among patients with hypertension is highly prevalent. Up to 50% of patients stop taking their prescribed antihypertensive medications within 1 year of initiation. 4 The high prevalence of antihypertensive medication nonadherence has contributed to poor blood pressure (BP) control worldwide. Accordingly, optimal control of BP is attained in less than one‐third and one‐tenth of patients with hypertension in high‐income and low‐ to middle‐income countries, respectively. 1 , 3 This poor control has consequently led to a high global burden of cardiovascular diseases, chronic kidney disease, dementia, and mortality.
The World Health Organization (WHO) has provided a conceptual framework to explain the multifactorial reasons underlying antihypertensive medication nonadherence, including socioeconomic factors (eg, age, sex, and educational status), patient‐related factors (eg, readiness to change and self‐efficacy), therapy‐related factors (eg, complexity of treatment and out‐of‐pocket costs), comorbidities (eg, comorbid cardiovascular diseases and mental illnesses), and health care system factors (eg, doctor‐patient relationships and doctors' burnout). 5 Clinically, antihypertensive medication nonadherence is detected by various methods, including validated self‐reported questionnaires, pill counting (by counting the pills left over since the last prescription), prescription refills (eg, medication possession ratio [MPR] and proportion of days covered by prescriptions by reviewing medication databases), electronic pill boxes (typically detect the opening of the pill box), blood/urine biomarkers or drug assays (detect the presence of drug metabolites in biological samples), and, recently, electronic medication monitors that directly detect gastric juice. 2
Despite the importance of antihypertensive medication nonadherence, a comprehensive meta‐analysis investigating its global epidemiology is yet to be conducted. Previous meta‐analyses included only certain countries or populations, for example, low‐ to middle‐income countries and only patients with resistant hypertension. 6 , 7 , 8 , 9 Furthermore, previous meta‐analyses only included self‐reported questionnaires or used both validated and nonvalidated methods to define medication nonadherence. 6 , 7 , 8 , 9 , 10 Moreover, the high heterogeneity of results from previous meta‐analyses has not been adequately investigated using subgroup analyses or meta‐regressions, despite the presence of multiple and complex factors associated with medication adherence. 6 , 7 , 10 Finally, although trends and regional prevalence of uncontrolled hypertension have been well studied, there is a lack of similar research on anti‐hypertensive medication nonadherence. 3
Therefore, the primary objective of this meta‐analysis was to estimate the global prevalence of antihypertensive medication nonadherence. Additionally, the prevalence was compared among different regions and countries. We hypothesized that antihypertensive medication nonadherence would be more prevalent in low‐ to middle‐income countries, attributable to lower availability and affordability of medication, and in non‐Western countries, attributable to different beliefs/cultures. 11 Trends in antihypertensive medication nonadherence from 2010 to 2020 were also examined. We hypothesized that because of the considerable research efforts and development of interventions for antihypertensive medication nonadherence over time, its prevalence would have decreased in the previous decade. 12 , 13 Additionally, the health consequences of antihypertensive medication nonadherence (eg, poor BP control) were investigated. The results of this study can inform patients, physicians, researchers, and policymakers regarding managing antihypertensive medication nonadherence.
METHODS
This meta‐analysis was registered in the International Prospective Register of Systematic Reviews (CRD42021259860) and reported according to the Meta‐Analyses of Observational Studies in Epidemiology standard of reporting and Preferred Reporting Items for Systematic Reviews and Meta‐Analyses guidelines. 14 Two of the authors (E.K.P.L. and P.P.) had full access to all the data and take full responsibility for its integrity and analysis. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study Eligibility
Observational studies were included if they (1) included patients with hypertension; (2) reported prevalence of antihypertensive medication nonadherence; (3) included ≥100 participants; (4) measured antihypertensive medication adherence using at least 1 of the following methods: validated questionnaire (eg, 4‐item or 8‐item Morisky Medication Adherence Scale [MMAS]), pill counting, prescription refills, electronic pill boxes, biochemical assays, or electronic medication monitoring 1 , 2 ; (5) used the validated or conventional cutoff of these methods (eg, scores of MMAS‐8 <6); and (6) were published in Chinese or English. The eligibility criteria were determined before the assessment of study eligibility (Table S1). 2 , 15 Studies were excluded if they included patients who (1) were aged <18 years, (2) had no hypertension, (3) received no antihypertensive medications, and (4) were pregnant. 7 Furthermore, studies that included only patients with resistant hypertension were excluded because these patients may have a higher prevalence of nonadherence and represent a different spectrum of nonadherence behaviors. Interventional trials, qualitative studies, animal studies, commentaries, and reviews were also excluded.
Information Sources
Chinese and English databases, such as the Cumulated Index to Nursing and Allied Health Literature Complete, Cochrane Library, Embase, Ovid Medline, PubMed, Scopus, Web of Science, and China Academic Journals Full‐text Database were searched for articles published up to December 2020.
Search Strategy
Keywords such as medication adherence, compliance, hypertension, antihypertensive medications, and medication adherence scale, were used as search terms (Table S2). The search was limited to studies of adults. In addition to English, studies published in Chinese were also included. Additionally, reference lists of relevant published systematic reviews were searched. 6 , 7 , 10 Clinicaltrials.gov was searched for unpublished trials, and the authors were contacted whenever possible.
Selection Process
All studies from the search were entered into the Covidence program (Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia; available at www.covidence.org). Two reviewers (from among E.K.P.L., P.P., Y.B., M.T.Z., and A.C.H.N.) independently assessed the eligibility of studies by screening the title/abstracts followed by the full texts in Covidence.
Data Collection Process
Data were dual extracted by reviewers (2 from among E.K.P.L., P.P., Y.B., M.T.Z., and A.C.H.N.) independently into Covidence. Discrepancies were compared and resolved by 2 reviewers (E.K.P.L. and P.P.).
Data Items
Extracted data included (1) details of the studies (eg, sample size, country, settings [ie, specialist center/hospital settings versus other settings], study design, inclusion/exclusion criteria). Countries were classified independently by 2 reviewers (from among E.K.P.L., P.P., M.T.Z., and A.C.H.N.) as Western or non‐Western (Western countries included Australia, New Zealand, Canada, all member countries of the European Union, the European microstates, the United Kingdom, and the United States) and high‐ or low‐ to middle‐income (as defined by the World Bank); (2) details of anti‐hypertensive medication nonadherence (methods used, cutoff, prevalence); (3) details for trend analyses (year of first recruitment and publication year); (4) socioeconomic and demographic variables of the participants that may affect adherence as defined by the WHO (age/sex, proportion with tertiary education or above, presence of cardiovascular diseases/renal diseases/diabetes/hyperlipidemia, number of years since hypertension diagnosis, the use of single‐pill combination and once‐daily medications, number of antihypertension classes, and proportion of current smokers); and (5) health consequences of nonadherence (systolic BP and diastolic BP differences between adherent and nonadherent participants and odds ratios [ORs] of suboptimal BP).
For cohort or case–control studies, health consequences, including ORs of suboptimal BP control, cardiovascular diseases, renal diseases, hospitalization, and death were also extracted. For cohort studies that reported adherence at multiple time points, the baseline value was used for analysis of comparability with cross‐sectional studies.
When only abstracts were found, the authors of the papers were contacted for published reports or articles. Abstracts were included only if they provided adequate information (ie, clear inclusion criteria, definition of anti‐hypertensive medication nonadherence, number of participants, and proportion of participants with antihypertensive medication nonadherence). For duplicated studies and cohort studies using potentially overlapping databases with overlapping dates, the latest study with the most extractable data was selected by 2 reviewers (E.K.P.L and P.P.).
Furthermore, the study by Saleem and colleagues was excluded post hoc because it reported a 100% nonadherence rate at a predetermined cutoff and could not be analyzed in Stata. 16
Study Risk‐of‐Bias Assessment
The Joanna Briggs Institute prevalence critical appraisal tool, a validated instrument, was used to rate the included studies. 17 Included studies were rated as having a low risk of bias only when no concern was raised regarding all questions in the instrument. All other included studies were rated as having unknown risk or high risk of bias. Quality assessments were conducted by 2 independent reviewers (from among E.K.P.L., P.P., Y.B., M.T.Z., and A.C.H.N.), and all discrepancies were resolved through discussion with E.K.P.L. and P.P. The certainty of evidence concerning the effect of health consequences of nonadherence was rated according to Grading of Recommendations, Assessment, Development and Evaluations.
Data Analysis
All meta‐analyses were conducted using Stata software (Stata Statistical Software: Release 15, StataCorp LLC, College Station, TX).
Global prevalence was estimated through the “metaprop” function, using a fixed‐effects model, which is the recommended and valid method to estimate prevalence from given populations. 18 Subgroup analyses were conducted on the basis of (1) the methods used to define nonadherence (eg, questionnaires, biochemical assays), (2) the countries where the studies were performed (Western versus non‐Western), and (3) the income level of these countries (high‐ versus low‐ to middle‐income). The nonadherence trend was analyzed using publication year and year of first recruitment. Heterogeneity, differences, and trends were further investigated by meta‐regression analyses using the “metareg” function. Heterogeneity across studies was assessed using I 2 statistics and P values. Furthermore, the effect of nonadherence on BP level and OR was investigated by comparing between adherent and nonadherent patients using the “metan” function and a random‐effects model because of a difference in population characteristics in the included studies. P values were 2‐tailed, considering those <0.05 to be statistically significant. Examples of the Stata commands can be found in Data S1.
Sensitivity analyses were conducted to include only studies with a low risk of bias and larger studies (n>500 and n>3000 [when an adequate number of studies were available]). Within the subgroup of studies that used questionnaires, sensitivity analyses were conducted by (1) replacing studies in which the MMAS‐8 cutoff was <6 with studies that used cutoffs of ≤6; (2) including only studies that used MMAS‐4; and (3) including only studies that used MMAS‐8 because MMAS‐4 and MMAS‐8 were the most commonly used questionnaires. For cohort studies that reported adherence data after 1 year, the prevalence of nonadherence at the last follow‐up was used for the sensitivity analysis. For health consequences attributable to anti‐hypertensive medication nonadherence, sensitivity analysis was conducted using results from cohort studies only.
Publication bias was assessed by visual examination of a funnel plot, plotting the log of prevalence against the standard error of prevalence, and Egger's test.
RESULTS
Characteristics of Included Studies and Population
Of the 7004 studies identified, a total of 161 studies from 68 countries were included, with a sample size ranging from 100 to 23 833 000 (Figure 1). Over half of the included studies were conducted in low‐ to middle‐income countries (n=88). Only a few studies used biochemical assays (n=5), pill counting (n=4), and electronic pill boxes (n=3) to detect nonadherence. Therefore, meaningful corresponding subgroup and meta‐regression analyses in these subgroups was not possible. Furthermore, studies in low‐ to middle‐income and non‐Western countries predominantly used questionnaires to measure adherence during the study period, with no studies using biochemical assays or electronic pill boxes. Moreover, the sample size of studies conducted in low‐ to middle‐income countries was small, and only 1 had a sample size of >3000. Among the studies that used questionnaires, the MMAS‐8 (n=73) and MMAS‐4 (n=45) questionnaires were most commonly used (Table S5). Only 23 studies were rated as having a low risk of bias (Tables S6 through S8). Our study population consisted of 27 785 595 patients with hypertension, with a mean age of 57 (42.9% men). Other demographic data and the list of included studies are presented in Tables S3 and S4.
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flowchart.
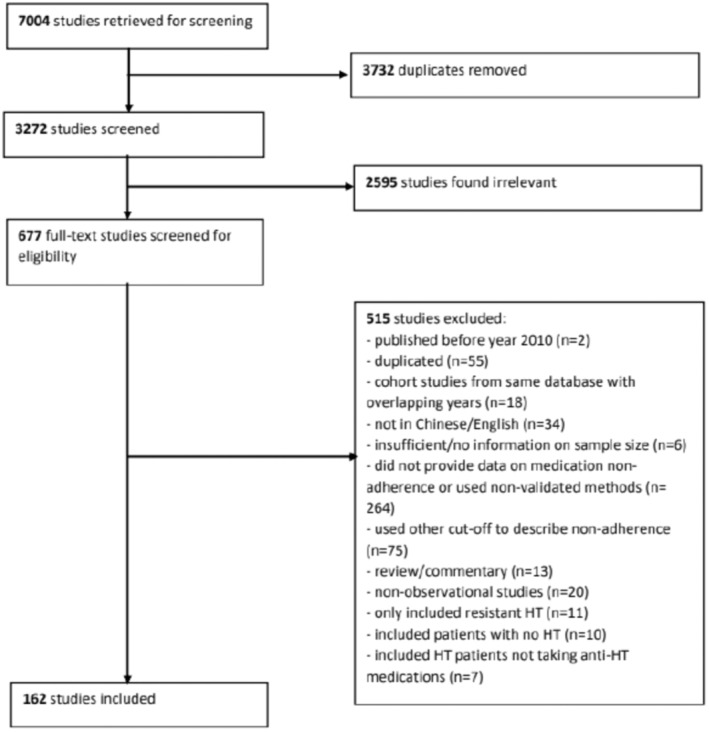
HT indicates hypertension.
Global Prevalence, Regional Differences, and Trends in Antihypertensive Medication Nonadherence
The prevalence varied with methods used to define nonadherence: 40% by questionnaires (95% CI, 40%–40%), 28% by prescription refill (95% CI, 28%–28%), 28% by pill counting (95% CI, 26%–29%), 28% by electronic pill boxes (95% CI, 25%–31%), and 27% by biochemical assays (95% CI, 26%–29%) (Figure 2, Table S9).
Figure 2. Prevalence of nonadherence presented with 95% CIs (subgroup: nonadherence definitions, West vs non‐West, income levels).
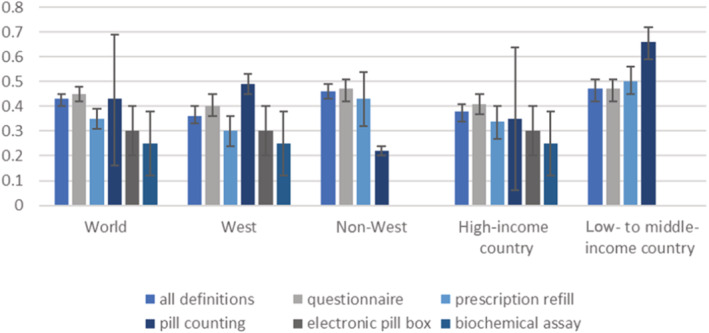
Nonadherence was more prevalent in low‐ to middle‐income countries than in high‐income countries, when defined by questionnaires (43% versus 38%; P=0.145), prescription refill (50% versus 28%; P=0.37), and pill counting (66% versus 25%; P=0.382). Similarly, nonadherence was more prevalent in non‐Western countries than in Western countries, when defined by questionnaires (43% versus 38%; P=0.108), and prescription refill (49% versus 26%; P=0.086; Figure 2, Table S9). Although nonadherence was less prevalent in non‐Western countries than in Western countries when pill counting was used, this included only 4 unclear to high risk‐of‐bias studies (22% versus 49%; P=0.974; Figure S1). Depending on the method used to define nonadherence, the prevalence of nonadherence ranged from 20% to 49% among continents (Tables S9 through S13, Figure S1).
No significant trend in antihypertensive medication nonadherence was detected over the past decade in all meta‐regression analyses, including subgroup analyses, using publication year or year of first recruitment (Figure 3, Tables S14 and S15).
Figure 3. Trend of medication nonadherence according to nonadherence prevalence and included studies' publication year.
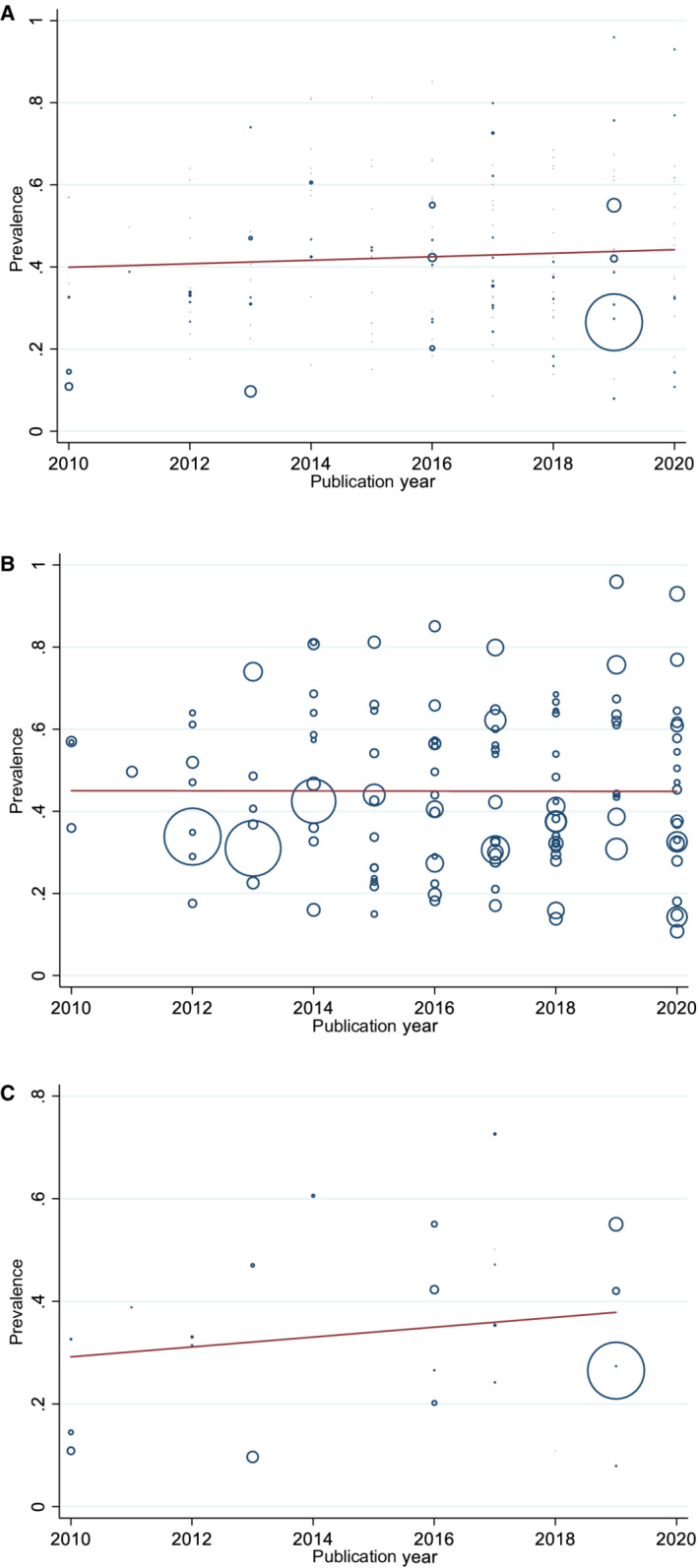
A, By any definition: regression coefficient: 0.004, P=0.434; (B) by questionnaires: regression coefficient: −0.0002, P=0.977; (C) by prescription refills: meta‐regression coefficient: 0.010, P=0.416. DBP indicates diastolic blood pressure; HT, hypertension; and SBP, systolic blood pressure.
When using meta‐regression to explore heterogeneity, in the subgroup analysis of studies using the prescription refill method of adherence, nonadherence was less common in older patients (P=0.001), patients receiving free medical service or insurance (P=0.044), and patients receiving more classes of antihypertensive medications (P=0.014; Table S16). Other factors, such as the presence of cardiovascular diseases and medication frequency, were not significantly associated with the prevalence of nonadherence (Table S16). These meta‐regression analyses did not explain the heterogeneity, and all residual I 2 remained >95%.
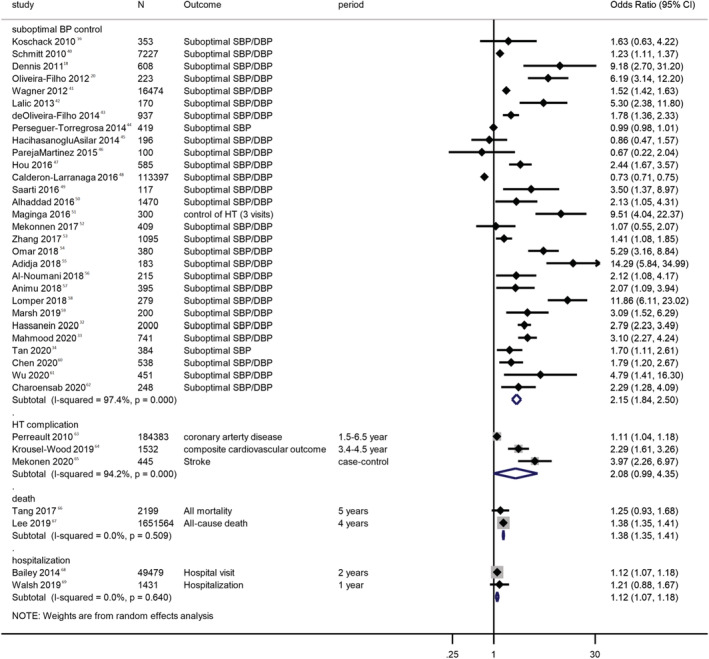
Consequences of Antihypertensive Medication Nonadherence
Compared with adherent patients, patients with antihypertensive medication nonadherence had higher systolic BP (mean difference, 3.76 mm Hg [95% CI, 2.23–5.28 mm Hg]; I 2, 87.1%; P<0.001), and diastolic BP (mean difference, 3.11 mm Hg [95% CI, 2.24–3.99 mm Hg]; I 2, 76%; P<0.001; Figure 4). 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 Furthermore, patients with antihypertensive medication nonadherence had increased odds of having suboptimal BP control (OR, 2.15 [95% CI, 1.84–2.5]; I 2, 97.4%; P<0.001), complications from hypertension (OR, 2.08 [95% CI, 0.99–4.35]; I 2, 94.2%; P<0.001), all‐cause hospitalization (OR, 1.38 [95% CI, 1.35–1.41]; I 2, 0; P=0.64), and all‐cause mortality (OR, 1.38 [95% CI, 1.35–1.41]; I 2, 0; P=0.509; Figure 5). 19 , 21 , 33 , 34 , 35 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 , 52 , 53 , 54 , 55 , 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 , 66 , 67 , 68 , 69 , 70 Sensitivity and subgroup analyses revealed similar results but did not resolve high heterogeneity (Figures S2 and S3, Tables S17 and S18). According to Grading of Recommendations, Assessment, Development and Evaluations, the certainty of evidence was low for all health outcomes, owing to inclusion of observational studies only.
Figure 4. Blood pressure difference attributable to medication nonadherence.
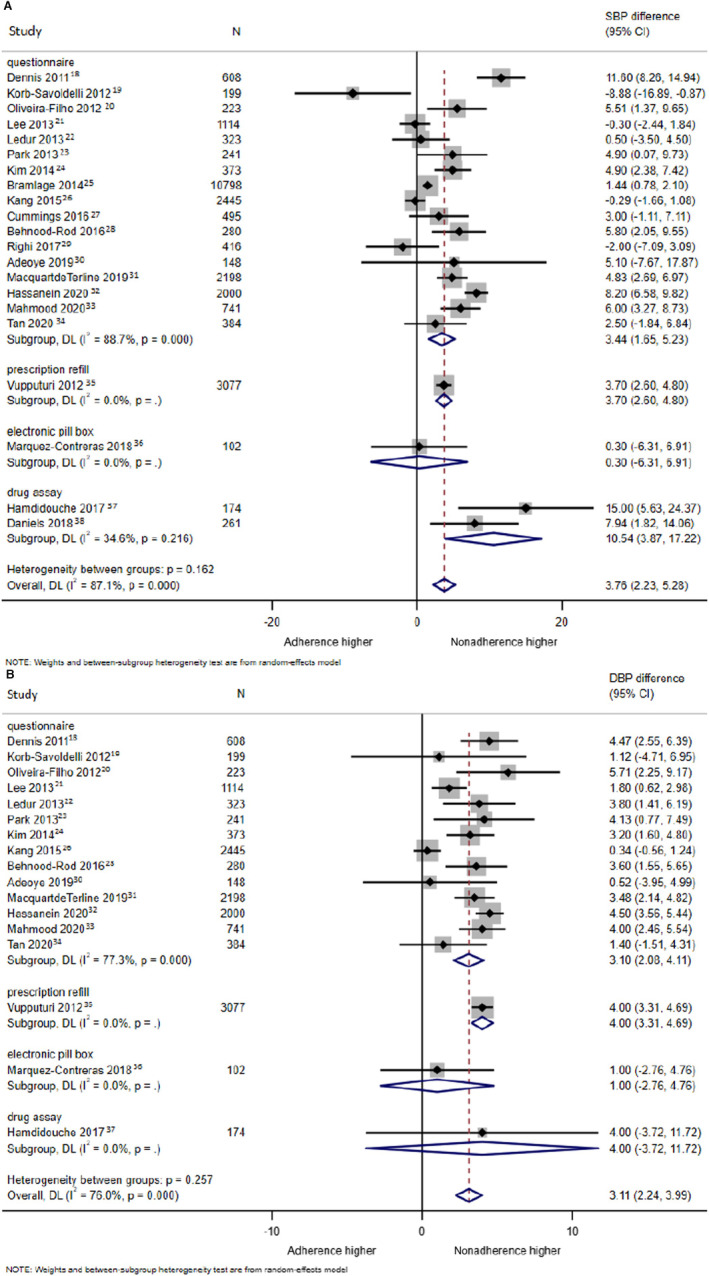
A, Systolic blood pressure difference attributable to medication nonadherence; (B) diastolic blood pressure difference attributable to medication nonadherence.
Figure 5. Health consequence attributable to medication nonadherence.
DBP indicates diastolic blood pressure; DL, xxx; and SBP, systolic blood pressure.
Sensitivity Analyses
Sensitivity analyses generally showed a decrease in nonadherence prevalence when only larger studies were included. This result is congruent with our findings on regional differences because larger studies were predominantly from high‐income countries. Moreover, almost all sensitivity analyses consistently found lower nonadherence prevalence in Western and high‐income countries. For instance, this was observed when only low‐risk‐of‐bias and questionnaire studies (prevalence, 38% [95% CI, 37%–39%]; Figure S3), and only studies using MMAS‐4 (prevalence, 41% [95% CI, 41%–42%]; Figure S3) were included. The differences in systolic BP/diastolic BP and health outcomes between adherent and nonadherent participants remained similar in the sensitivity analyses. Moreover, no significant trend in prevalence of nonadherence was detected in various sensitivity analyses (Tables S17 and S18, Figure S3). However, no sensitivity analysis adequately explained the results' high heterogeneity (Tables S17 and S18, Figure S3).
Publication Bias
The funnel plots and Egger's test did not show a significant small study bias (Egger's test, P=0.332; Figure S4).
DISCUSSION
Main Findings and Comparison With Previous Literature
Subject to different detection methods, the global prevalence of antihypertensive medication nonadherence ranged from 27% to 40%. Furthermore, antihypertensive medication nonadherence was more prevalent in low‐ to middle‐income countries and non‐Western countries. For instance, using our results from prescription refill and the latest WHO data, this translates to ≈426 million people from low‐ to middle‐income countries, and 119 million people from high‐income countries. 71 Our results are similar to those of another meta‐analysis that reported a global prevalence of 45%, but that meta‐analysis included only studies that used MMAS. 10 Our results are also similar to those of previous large observational studies revealing that antihypertensive medication nonadherence led to poor BP control, higher health care resource use, cardiovascular complications, and death. 72 , 73 However, this is the first study to suggest that, in addition to the known factors of underdiagnosis and undertreatment, nonadherence plays an important role in the differential poor hypertension control in low‐ to middle‐income countries. 3 The exact reasons underlying these regional differences cannot be determined from our data, but they could be attributed to differences in cultures, beliefs, the use of alternative medicine, health care systems, and drug affordability and availability. 32 To date, there has been a lack of primary studies that directly investigate regional differences (eg, Western versus non‐Western or high‐income versus low‐ to middle‐income countries) in antihypertensive medication nonadherence.
Although a decreasing trend in nonadherence has been described in a few US studies, this trend has not been observed globally. 74 , 75 This suggests that, although evidence‐based interventions, such as reduction in daily number of pills and single‐pill combinations, can reduce medication nonadherence, they were not adequately implemented in clinical practice. 13 , 76 , 77 A Cochrane review also suggested that significant improvements in adherence and clinical outcomes were uncommon in well‐conducted randomized controlled trials, and these called for advances and more interventional studies in the field. 78
Our results also suggested that the prevalence of nonadherence was generally lower when more objective detection methods were used (ie, electronic pill boxes and biochemical assays). However, these studies were conducted only in Western and high‐income countries. This difference could, therefore, be attributable to the regional differences described. These differences could also result from the Hawthorne effect, that is, an improved nonadherence rate when patients know that they are being monitored. 79 In the current study, nonadherence was detected by these objective methods in only 8 studies, and no study used electronic medications.
Clinical and Research Implications
Our results are consistent with international guidelines that state that antihypertensive medication nonadherence is highly prevalent and clinicians treating hypertension should screen for nonadherence during every clinician visit. 80 However, clinicians' predictions of drug nonadherence are known to be no better than “a coin toss.” Therefore, policymakers and clinicians should incorporate validated methods into health care systems to routinely detect anti‐hypertensive medication nonadherence. 81 However, all existing methods, including the use of questionnaires, calculation of MPR, or telemonitoring by electronic pill boxes, would require extra time and resources, which could be difficult to implement. Newer methods, including the use of dried blood samples and oral fluid assays, are being developed and investigated to provide reliable and quick methods for clinicians to routinely detect nonadherence. 82 , 83 Once detected, clinicians could conceptualize the reasons for nonadherence, using the WHO model, and manage them accordingly. 5
Our results also call for implementation research to examine how the latest evidence can be translated into clinical practice and trials to investigate interventions that can effectively improve medication adherence and clinical outcomes. 78 While most existing research investigated single interventions, clinical practice guidelines suggest that complex interventions combining several interventions to target the factors listed by the WHO are most likely needed. 80 However, real‐life data concerning such complex interventions are scarce. Furthermore, there is still no reference standard for the detection of medication nonadherence. Even biochemical assays, which are one of the most objective measures, suffer from the white‐coat adherence effect, in which patients have improved adherence only before doctor visits. 84 A feasible, affordable, and reliable reference standard to define nonadherence would facilitate research and its clinical detection. Additionally, existing validated antihypertensive medication nonadherence detection methods could not provide a comprehensive assessment of patients' adherence behaviors, which include the processes of “initiation,” “implementation,” and “discontinuation.” 85 For instance, although 90% MPR signified good medication adherence using a conventional cutoff, the missing 10% can represent both occasional drug holidays or complete discontinuation. Moreover, the reasons for the higher nonadherence prevalence in low‐ to middle‐income and non‐Western countries could be explored and examined further. Finally, large population‐based studies on antihypertensive medication nonadherence from low‐ to middle‐income countries are lacking.
Strengths and Limitations
This study has many strengths. This is the first meta‐analysis that describes not only global prevalence but also regional differences and trends in antihypertensive medication nonadherence in the previous decade. This study represented the best available evidence in view of the lack of similar primary research across continents with different income levels. Our meta‐analysis also involved a comprehensive search, including Chinese databases, with the largest number of studies among similar meta‐analyses. Meta‐regressions were conducted to investigate the relationship between prevalence of nonadherence and patients' determining factors (eg, presence of cardiovascular diseases), and treatment factors (eg, once‐daily or combined‐pill treatments, number of medications; Table S16). There was no significant publication bias, and the sensitivity analyses showed congruent results.
However, all results were highly heterogeneous because studies included different populations, used different definitions of nonadherence, and included diverse factors that this study could not encompass (eg, characteristics of health care and insurance systems, quality of doctor‐patient relationships, and level of doctors' burnout). Furthermore, questionnaires had different sensitivities and specificities to detect medication nonadherence and measured different aspects of nonadherence (beliefs, barriers, and actual use of medications), which could partially explain the statistical heterogeneity. 86 To minimize heterogeneity, we included only studies that used validated or conventional definitions and cutoffs for antihypertensive medication nonadherence. Relevant subgroups, meta‐regression, and sensitivity analyses were also used to investigate heterogeneity; however, these did not adequately explain the heterogeneity. Although the use of only population‐based samples may further reduce heterogeneity (a methodology commonly used in other meta‐analyses that investigated hypertension epidemiology), this was not possible because large studies from low‐ to middle‐income countries were not available. For instance, only 1 study from a low‐ to middle‐income country had a sample size >3000. 3 Moreover, our sensitivity analyses, which included only large studies, did not resolve heterogeneity (Tables S17 and S18, Figure S3).
Second, methods including prescription refills, pill counting, electronic pill boxes, and biochemical assays were rarely used in studies from non‐Western or low‐ to middle‐income countries. These precluded comparative analyses or statistical significance in several subgroups. Therefore, prevalence estimates from these countries were derived primarily using questionnaire methods, which are prone to self‐reporting bias and have poor agreement with objective methods. 87 Furthermore, many questionnaires, such as MMAS‐8, cannot provide the exact timing and number of doses missed. However, since questionnaires tended to underestimate nonadherence as compared with objective methods (eg, biochemical assays), this strengthens our conclusion that nonadherence was more prevalent in non‐Western or low‐ to middle‐income countries. 2 Third, we included only studies published in English or Chinese. Nevertheless, of the 677 full‐text studies screened, only 34 were excluded because of language issues. Fourth, interventional trials were excluded because patients who volunteered and consented to these trials (especially trials to improve drug adherence) could be systematically different from other patients with hypertension. Strict inclusion and exclusion criteria of randomized controlled trials often results in the selection of patients with similar characteristics, which may bias our results. Nevertheless, including baseline data from these intervention trials could further enhance our comprehensiveness and sample size. Fifth, high heterogeneity of the results could hinder the detection of trends of antihypertensive medication nonadherence in the meta‐regression analysis.
Sixth, although we used the most validated and conventional cutoffs for questionnaires and MPR, these cutoffs can still be questioned. For example, at a cutoff of 6, MMAS‐8 has only a sensitivity and specificity to detect nonadherence of ≈0.43 and 0.74, respectively. 15 Similarly, the MPR cutoff of 0.82, instead of 0.80, may be more appropriate to detect antihypertensive medication nonadherence. 88 However, alternate cutoffs (eg, MPR <0.82), were not used by the current studies and therefore could not be used in the current meta‐analyses. We have presented questionnaire data using MMAS‐8 <6 and ≤6 (sensitivity analysis in Tables S17 and S18 and Figure S3). Finally, although the results of the health consequences of antihypertensive medication nonadherence were rated low according to Grading of Recommendations, Assessment, Development and Evaluations because of the inclusion of only observational studies, this matter is difficult and unethical to investigate using clinical trials.
CONCLUSIONS
Globally, ≈27% to 40% of patients with hypertension are nonadherent to their medications. A higher prevalence of antihypertensive medication nonadherence was detected in low‐ to middle‐income and non‐Western countries. Interventions are urgently required to detect antihypertensive medication nonadherence and improve medication adherence, especially in countries where antihypertensive medication adherence is suboptimal.
Sources of Funding
None.
Disclosures
None.
Supporting information
Data S1
Tables S1–S18
Figures S1–S4
References 16, 65, 75, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152, 153, 154, 155, 156, 157, 158, 159, 160, 161, 162, 163, 164, 165, 166, 167, 168, 169, 170, 171, 172, 173, 174, 175, 176, 177, 178, 179, 180, 181, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199, 200, 201, 202, 203
Supplemental Material is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.122.026582
For Sources of Funding and Disclosures, see page 12.
References
- 1. Hamdidouche I, Jullien V, Boutouyrie P, Billaud E, Azizi M, Laurent S. Drug adherence in hypertension: from methodological issues to cardiovascular outcomes. J Hypertens. 2017;35:1133–1144. doi: 10.1097/HJH.0000000000001299 [DOI] [PubMed] [Google Scholar]
- 2. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124:1124–1140. doi: 10.1161/CIRCRESAHA.118.313220 [DOI] [PubMed] [Google Scholar]
- 3. Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, Chen J, He J. Global disparities of hypertension prevalence and control. Circulation. 2016;134:441–450. doi: 10.1161/CIRCULATIONAHA.115.018912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Vrijens B, Vincze G, Kristanto P, Urquhart J, Burnier M. Adherence to prescribed antihypertensive drug treatments: longitudinal study of electronically compiled dosing histories. BMJ. 2008;336:1114–1117. doi: 10.1136/bmj.39553.670231.25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86:304–314. doi: 10.4065/mcp.2010.0575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Nielsen JØ, Shrestha AD, Neupane D, Kallestrup P. Non‐adherence to anti‐hypertensive medication in low‐ and middle‐income countries: a systematic review and meta‐analysis of 92443 subjects. J Hum Hypertens. 2016;31:14–21. doi: 10.1038/jhh.2016.31 [DOI] [PubMed] [Google Scholar]
- 7. Durand H, Hayes P, Morrissey EC, Newell J, Casey M, Murphy AW, Molloy GJ. Medication adherence among patients with apparent treatment‐resistant hypertension. J Hypertens. 2017;35:2346–2357. doi: 10.1097/HJH.0000000000001502 [DOI] [PubMed] [Google Scholar]
- 8. Bochkareva EV, Butina EK, Kim IV, Kontsevaya AV, Drapkina OM, Leon D, Mckee M. Adherence to antihypertensive medication in Russia: a scoping review of studies on levels, determinants and intervention strategies published between 2000 and 2017. Arch Public Health. 2019;77:43. doi: 10.1186/s13690-019-0366-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tola Gemeda A, Regassa LD, Weldesenbet AB, Merga BT, Legesse N, Tusa BS. Adherence to antihypertensive medications and associated factors among hypertensive patients in Ethiopia: systematic review and meta‐analysis. SAGE Open Med. 2020;8:2050312120982459. doi: 10.1177/2050312120982459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Abegaz TM, Shehab A, Gebreyohannes EA, Bhagavathula AS, Elnour AA. Nonadherence to antihypertensive drugs: a systematic review and meta‐analysis. Medicine. 2017;96:e5641. doi: 10.1097/MD.0000000000005641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lim MK, Sadarangani P, Chan HL, Heng JY. Complementary and alternative medicine use in multiracial Singapore. Complement Ther Med. 2005;13:16–24. doi: 10.1016/j.ctim.2004.11.002 [DOI] [PubMed] [Google Scholar]
- 12. Ruppar TM, Dunbar‐Jacob JM, Mehr DR, Lewis L, Conn VS. Medication adherence interventions among hypertensive black adults: a systematic review and meta‐analysis. J Hypertens. 2017;35:1145–1154. doi: 10.1097/HJH.0000000000001260 [DOI] [PubMed] [Google Scholar]
- 13. Thakkar J, Kurup R, Laba T‐L, Santo K, Thiagalingam A, Rodgers A, Woodward M, Redfern J, Chow CK. Mobile telephone text messaging for medication adherence in chronic disease: a meta‐analysis. JAMA Intern Med. 2016;176:340. doi: 10.1001/jamainternmed.2015.7667 [DOI] [PubMed] [Google Scholar]
- 14. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB. Meta‐analysis of observational studies in epidemiology: a proposal for reporting. JAMA. 2000;283:2008–2012. doi: 10.1001/jama.283.15.2008 [DOI] [PubMed] [Google Scholar]
- 15. Moon SJ, Lee W‐Y, Hwang JS, Hong YP, Morisky DE. Accuracy of a screening tool for medication adherence: a systematic review and meta‐analysis of the Morisky Medication Adherence Scale‐8. PLoS One. 2017;12:e0187139. doi: 10.1371/journal.pone.0187139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Saleem F, Hassali MA, Shafie AA, Awad GA, Atif M, Aljadhey H, Farooqui M. Does treatment adherence correlates with health related quality of life? Findings from a cross sectional study. BMC Public Health. 2012;12:1–7. doi: 10.1186/1471-2458-12-318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Migliavaca CB, Stein C, Colpani V, Munn Z, Falavigna M. Quality assessment of prevalence studies: a systematic review. J Clin Epidemiol. 2020;127:59–68. doi: 10.1016/j.jclinepi.2020.06.039 [DOI] [PubMed] [Google Scholar]
- 18. Hoeffding W. On the distribution of the number of successes in independent trials. Ann Math Stat. 1956;27:713–721. doi: 10.1214/aoms/1177728178 [DOI] [Google Scholar]
- 19. Dennis T, Meera NK, Binny K, Sekhar MS, Kishore G, Sasidharan S. Medication adherence and associated barriers in hypertension management in India. CVD Prev Control. 2011;6:9–13. [Google Scholar]
- 20. Korb‐Savoldelli V, Gillaizeau F, Pouchot J, Lenain E, Postel‐Vinay N, Plouin PF, Durieux P, Sabatier B. Validation of a French version of the 8‐item Morisky Medication Adherence Scale in hypertensive adults. J Clin Hypertens. 2012;14:429–434. doi: 10.1111/j.1751-7176.2012.00634.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Oliveira‐Filho AD, Barreto‐Filho JA, Neves SJ, Lyra Junior DP. Association between the 8‐item Morisky Medication Adherence Scale (MMAS‐8) and blood pressure control. Arq Bras Cardiol. 2012;99:649–658. doi: 10.1590/S0066-782X2012005000053 [DOI] [PubMed] [Google Scholar]
- 22. Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky Medication Adherence Scale. PLoS One. 2013;8:e62775. doi: 10.1371/journal.pone.0062775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ledur PD, Leiria LF, Severo MD, Silveira DT, Massierer D, Becker AD, Aguiar FM, Gus M, Schaan BD. Perception of uncontrolled blood pressure and non‐adherence to anti‐hypertensive agents in diabetic hypertensive patients. J Am Soc Hypertens. 2013;7:477–483. doi: 10.1016/j.jash.2013.07.006 [DOI] [PubMed] [Google Scholar]
- 24. Park YH, Kim H, Jang SN, Koh CK. Predictors of adherence to medication in older Korean patients with hypertension. Eur J Cardiovasc Nurs. 2013;12:17–24. doi: 10.1016/j.ejcnurse.2011.05.006 [DOI] [PubMed] [Google Scholar]
- 25. Kim JH, Lee WY, Hong YP, Ryu WS, Lee KJ, Lee WS, Morisky DE. Psychometric properties of a short self‐reported measure of medication adherence among patients with hypertension treated in a busy clinical setting in Korea. J Epidemiol. 2014;24:132–140. doi: 10.2188/jea.JE20130064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Bramlage P, Ketelhut R, Fronk EM, Wolf WP, Smolnik R, Zemmrich C, Schmieder RE. Clinical impact of patient adherence to a fixed‐dose combination of olmesartan, amlodipine and hydrochlorothiazide. Clin Drug Investig. 2014;34:403–411. doi: 10.1007/s40261-014-0188-z [DOI] [PubMed] [Google Scholar]
- 27. Kang CD, Tsang PP, Li WT, Wang HH, Liu KQ, Griffiths SM, Wong MC. Determinants of medication adherence and blood pressure control among hypertensive patients in Hong Kong: a cross‐sectional study. Int J Cardiol. 2015;182:250–257. doi: 10.1016/j.ijcard.2014.12.064 [DOI] [PubMed] [Google Scholar]
- 28. Cummings DM, Wu JR, Cene C, Halladay J, Donahue KE, Hinderliter A, Miller C, Garcia B, Penn D, Tillman J, et al. Perceived social standing, medication nonadherence, and systolic blood pressure in the rural south. J Rural Health. 2016;32:156–163. doi: 10.1111/jrh.12138 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Behnood‐Rod A, Rabbanifar O, Pourzargar P, Rai A, Saadat Z, Saadat H, Moharamzad Y, Morisky DE. Adherence to antihypertensive medications in Iranian patients. Int J Hypertens. 2016;2016:1508752. doi: 10.1155/2016/1508752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Righi CG, Martinez D, Gonçalves SC, Gus M, Moreira LB, Fuchs SC, Fuchs FD. Influence of high risk of obstructive sleep apnea on adherence to antihypertensive treatment in outpatients. J Clin Hypertens. 2017;19:534–539. doi: 10.1111/jch.12992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Adeoye AM, Adebiyi AO, Adebayo OM, Owolabi MO. Medication adherence and 24‐h blood pressure in apparently uncontrolled hypertensive Nigerian patients. Niger Postgrad Med J. 2019;26:18–24. doi: 10.4103/npmj.npmj_147_18 [DOI] [PubMed] [Google Scholar]
- 32. Macquart de Terline D, Kane A, Kramoh KE, Ali Toure I, Mipinda JB, Diop IB, Nhavoto C, Balde DM, Ferreira B, Dèdonougbo Houenassi M, et al. Factors associated with poor adherence to medication among hypertensive patients in twelve low and middle income Sub‐Saharan countries. PLoS One. 2019;14:e0219266. doi: 10.1371/journal.pone.0219266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Hassanein M. Adherence to antihypertensive fixed‐dose combination among Egyptian patients presenting with essential hypertension. Egypt Heart J. 2020;72:1–9. doi: 10.1186/s43044-020-00044-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Mahmood S, Jalal Z, Hadi MA, Orooj H, Shah KU. Non‐adherence to prescribed antihypertensives in primary, secondary and tertiary healthcare settings in Islamabad, Pakistan: a cross‐sectional study. Patient Prefer Adherence. 2020;14:73–85. doi: 10.2147/PPA.S235517 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Tan CS, Hassali MA, Neoh CF, Ming LC. Beliefs about medicine and medication adherence among hypertensive patients in the community setting. Drugs Ther Perspect. 2020;36:358–367. doi: 10.1007/s40267-020-00744-8 [DOI] [Google Scholar]
- 36. Vupputuri S, Muntner P, Winkelmayer WC, Smith DH, Nichols GA. Low medication adherence is related to poor hypertension control among patients with chronic kidney disease. Circulation. 2012;125. doi: 10.1161/circ.125.suppl_10.AP097 [DOI] [Google Scholar]
- 37. Marquez‐Contreras E, de Lopez G‐RL, Martell‐Claros N, Gil‐Guillen VF, Marquez‐Rivero S, Perez‐Lopez E, Garrido‐Lopez MA, Farauste C, Lopez‐Pineda A, Casado‐Martinez JJ, et al. Validation of the electronic prescription as a method for measuring treatment adherence in hypertension. Patient Educ Couns. 2018;101:1654–1660. doi: 10.1016/j.pec.2018.04.009 [DOI] [PubMed] [Google Scholar]
- 38. Hamdidouche I, Jullien V, Boutouyrie P, Billaud E, Azizi M, Laurent S. Routine urinary detection of antihypertensive drugs for systematic evaluation of adherence to treatment in hypertensive patients. J Hypertens. 2017;35:1891–1898. doi: 10.1097/HJH.0000000000001402 [DOI] [PubMed] [Google Scholar]
- 39. Daniels JS, Morrison RD, Milne SB, McNaughton CD, Sutherland JJ. Adherence assessment via comprehensive identification and quantitation of circulating medications with significant correlation to lower blood pressure observed in hypertensive patients. Hypertension. 2018;72:AP367. [Google Scholar]
- 40. Koschack J, Marx G, Schnakenberg J, Kochen MM, Himmel W. Comparison of two self‐rating instruments for medication adherence assessment in hypertension revealed insufficient psychometric properties. J Clin Epidemiol. 2010;63:299–306. doi: 10.1016/j.jclinepi.2009.06.011 [DOI] [PubMed] [Google Scholar]
- 41. Schmitt KE, Edie CF, Laflam P, Simbartl LA, Thakar CV. Adherence to antihypertensive agents and blood pressure control in chronic kidney disease. Am J Nephrol. 2010;32:541–548. doi: 10.1159/000321688 [DOI] [PubMed] [Google Scholar]
- 42. Wagner S, Lau H, Frech‐Tamas F, Gupta S. Impact of medication adherence on work productivity in hypertension. Am J Pharm Benefits. 2012;4:e88–e96. [Google Scholar]
- 43. Lalic J, Radovanovic RV, Mitic B, Nikolic V, Spasic A, Koracevic G. Medication adherence in outpatients with arterial hypertension. Acta Fac Med Naissensis. 2013;30:209–218. doi: 10.2478/afmnai-2013-0013 [DOI] [Google Scholar]
- 44. de Oliveira‐Filho AD, Morisky DE, Neves SJF, Costa FA, de Lyra DPJ. The 8‐item Morisky Medication Adherence Scale: validation of a Brazilian‐Portuguese version in hypertensive adults. Res Social Adm Pharm. 2014;10:554–561. doi: 10.1016/j.sapharm.2013.10.006 [DOI] [PubMed] [Google Scholar]
- 45. Perseguer‐Torregrosa Z, Orozco‐Beltrán D, Gil‐Guillen VF, Pita‐Fernandez S, Carratalá‐Munuera C, Pallares‐Carratalá V, Lopez‐Pineda A. Magnitude of pharmacological nonadherence in hypertensive patients taking antihypertensive medication from a community pharmacy in Spain. J Manag Care Spec Pharm. 2014;20:1217–1225. doi: 10.18553/jmcp.2014.20.12.1217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Hacihasanoglu Asilar R, Gozum S, Capik C, Morisky DE. Reliability and validity of the Turkish form of the eight‐item Morisky Medication Adherence Scale in hypertensive patients. Anadolu Kardiyol Derg. 2014;14:692–700. doi: 10.5152/akd.2014.4982 [DOI] [PubMed] [Google Scholar]
- 47. Pareja Martinez E, Esquivel Prados E, Franco Trigo L, Garcia‐Corpas JP. Adherence to antihypertensive therapy in community pharmacy: evaluating the psychometric properties of the Morisky Medication Adherence Scale (MMAS‐8) translated into Spanish. Pilot study. Lat Am J Pharm. 2015;34:86–93. [Google Scholar]
- 48. Hou Y, Zhang D, Gu J, Xue F, Sun Y, Wu Q, Zhao X, Wang X. The association between self‐perceptions of aging and antihypertensive medication adherence in older Chinese adults. Aging Clin Exp Res. 2016;28:1113–1120. doi: 10.1007/s40520-015-0516-z [DOI] [PubMed] [Google Scholar]
- 49. Calderon‐Larranaga A, Diaz E, Poblador‐Plou B, Gimeno‐Feliu LA, Abad‐Diez JM, Prados‐Torres A. Non‐adherence to antihypertensive medication: the role of mental and physical comorbidity. Int J Cardiol. 2016;207:310–316. doi: 10.1016/j.ijcard.2016.01.069 [DOI] [PubMed] [Google Scholar]
- 50. Saarti S, Hajj A, Karam L, Jabbour H, Sarkis A, El Osta N, Rabbaa KL. Association between adherence, treatment satisfaction and illness perception in hypertensive patients. J Hum Hypertens. 2016;30:341–345. doi: 10.1038/jhh.2015.86 [DOI] [PubMed] [Google Scholar]
- 51. Alhaddad IA, Hamoui O, Hammoudeh A, Mallat S. Treatment adherence and quality of life in patients on antihypertensive medications in a Middle Eastern population: adherence. Vasc Health Risk Manag. 2016;12:407–413. doi: 10.2147/VHRM.S105921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Maginga J, Guerrero M, Koh E, Holm Hansen C, Shedafa R, Kalokola F, Smart LR, Peck RN. Hypertension control and its correlates among adults attending a hypertension clinic in Tanzania. J Clin Hypertens. 2016;18:207–216. doi: 10.1111/jch.12646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Mekonnen HS, Gebrie MH, Eyasu KH, Gelagay AA. Drug adherence for antihypertensive medications and its determinants among adult hypertensive patients attending in chronic clinics of referral hospitals in Northwest Ethiopia. BMC Pharmacol Toxicol. 2017;18:27. doi: 10.1186/s40360-017-0134-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Zhang H, Sun J, Zhang H, Zhu Y, Mao X, Ai F, Tang S, Li R. Correlation between compliance in patients with anti‐hypertensive therapy and blood pressure control. Pak J Pharm Sci. 2017;30:1455–1460. [PubMed] [Google Scholar]
- 55. Omar SM, Elnour O, Adam GK, Osman OE, Adam I. Assessment of blood pressure control in adult hypertensive patients in eastern Sudan. BMC Cardiovasc Disord. 2018;18:26. doi: 10.1186/s12872-018-0769-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Adidja NM, Agbor VN, Aminde JA, Ngwasiri CA, Ngu KB, Aminde LN. Non‐adherence to antihypertensive pharmacotherapy in Buea, Cameroon: a cross‐sectional community‐based study. BMC Cardiovasc Disord. 2018;18:150. doi: 10.1186/s12872-018-0888-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Al‐Noumani H, Wu J‐R, Barksdale D, Knafl G, AlKhasawneh E, Sherwood G. Health beliefs and medication adherence in Omanis with hypertension. J Cardiovasc Nurs. 2018;33:518–526. doi: 10.1097/JCN.0000000000000511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Animu Y, Assefa AT, Lemma DG. Blood pressure control status and associated factors among adult hypertensive patients on outpatient follow‐up at University of Gondar Referral Hospital, Northwest Ethiopia: a retrospective follow‐up study. Integr Blood Press Control. 2018;11:37–46. doi: 10.2147/IBPC.S150628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Lomper K, Chabowski M, Chudiak A, Białoszewski A, Dudek K, Jankowska‐Polańska B. Psychometric evaluation of the Polish version of the adherence to Refills and Medications Scale (ARMS) in adults with hypertension. Patient Prefer Adherence. 2018;12:2661–2670. doi: 10.2147/PPA.S185305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Marsh JJ, Silver J, Johnson T, Mohundro B, Peacock E, Krousel‐Wood M. Low self‐report antihypertensive medication adherence (using Krousel‐Wood medication adherence scale) is associated with uncontrolled blood pressure (Bp), using established (>= 140/90 Mmhg) and 2017 definitions (>= 130/80 Mmhg). J Invest Med. 2019;67:540. [Google Scholar]
- 61. Chen PF, Chang EH, Unni EJ, Hung M. Development of the Chinese version of medication adherence reasons scale (ChMAR‐scale). Int J Environ Res Public Health. 2020;17:5578. doi: 10.3390/ijerph17155578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Hu XJ, Zhang X, Chen XP. The disparities of hypertension control rate and risk factors among hypertensive residing in high‐altitude and plain in Sichuan Province. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020;51:376–382. doi: 10.12182/20200560505 [DOI] [PubMed] [Google Scholar]
- 63. Charoensab N, Pinyopornpanish K, Thangsuk P, Jiraporncharoen W, Angkurawaranon C. Lowered blood pressure targets identify new, uncontrolled hypertensive cases: patient characteristics and implications for services in Thailand. BMC Health Serv Res. 2020;20:869. doi: 10.1186/s12913-020-05719-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Perreault S, Dragomir A, Roy L, White M, Blais L, Lalonde L, Bérard A. Adherence level of antihypertensive agents in coronary artery disease. Br J Clin Pharmacol. 2010;69:74–84. doi: 10.1111/j.1365-2125.2009.03547.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Krousel‐Wood M, Peacock E, Joyce C, Li S, Frohlich E, Re R, Mills K, Chen J, Stefanescu A, Whelton P, et al. A hybrid 4‐item Krousel‐Wood medication adherence scale predicts cardiovascular events in older hypertensive adults. J Hypertens. 2019;37:851–859. doi: 10.1097/HJH.0000000000001955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Mekonen HH, Birhanu MM, Mossie TB, Gebreslassie HT. Factors associated with stroke among adult patients with hypertension in Ayder comprehensive specialized hospital, Tigray, Ethiopia, 2018: a case‐control study. PLoS One. 2020;15:e0228650. doi: 10.1371/journal.pone.0228650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Tang KL, Quan H, Rabi DM. Measuring medication adherence in patients with incident hypertension: a retrospective cohort study. BMC Health Serv Res. 2017;17:135. doi: 10.1186/s12913-017-2073-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Lee H, Park JH, Floyd JS, Park S, Kim HC. Combined effect of income and medication adherence on mortality in newly treated hypertension: nationwide study of 16 million person‐years. J Am Heart Assoc. 2019;8:e013148. doi: 10.1161/JAHA.119.013148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Bailey JE, Hajjar M, Shoib B, Tang J, Ray MM, Wan JY. Risk factors associated with antihypertensive medication nonadherence in a statewide Medicaid population. Am J Med Sci. 2014;348:410–415. doi: 10.1097/MAJ.0b013e31825ce50f [DOI] [PubMed] [Google Scholar]
- 70. Walsh CA, Cahir C, Bennett KE. Association between adherence to antihypertensive medications and health outcomes in middle and older aged community dwelling adults; results from the Irish Longitudinal Study on Ageing. Eur J Clin Pharmacol. 2019;75:1283–1292. doi: 10.1007/s00228-019-02699-w [DOI] [PubMed] [Google Scholar]
- 71. Hypertension. Available at: https://www.who.int/news‐room/fact‐sheets/detail/hypertension. Accessed May 31, 2021.
- 72. Corrao G, Parodi A, Nicotra F, Zambon A, Merlino L, Cesana G, Mancia G. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011;29:610–618. doi: 10.1097/HJH.0b013e328342ca97 [DOI] [PubMed] [Google Scholar]
- 73. Corrao G, Rea F, Monzio Compagnoni M, Merlino L, Mancia G. Protective effects of antihypertensive treatment in patients aged 85 years or older. J Hypertens. 2017;35:1432–1441. doi: 10.1097/HJH.0000000000001323 [DOI] [PubMed] [Google Scholar]
- 74. Tajeu GS, Kent ST, Kronish IM, Huang L, Krousel‐Wood M, Bress AP, Shimbo D, Muntner P. Trends in antihypertensive medication discontinuation and low adherence among Medicare beneficiaries initiating treatment from 2007 to 2012. Hypertension. 2016;68:565–575. doi: 10.1161/HYPERTENSIONAHA.116.07720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Tajeu GS, Kent ST, Huang L, Bress AP, Cuffee Y, Halpern MT, Kronish IM, Krousel‐Wood M, Mefford MT, Shimbo D, et al. Antihypertensive medication nonpersistence and low adherence for adults <65 years initiating treatment in 2007–2014. Hypertension. 2019;74:35–46. doi: 10.1161/HYPERTENSIONAHA.118.12495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Parati G, Kjeldsen S, Coca A, Cushman WC, Wang J. Adherence to single‐pill versus free‐equivalent combination therapy in hypertension: a systematic review and meta‐analysis. Hypertension. 2021;77:692–705. doi: 10.1161/HYPERTENSIONAHA.120.15781 [DOI] [PubMed] [Google Scholar]
- 77. Schroeder K, Fahey T, Ebrahim S. Interventions for improving adherence to treatment in patients with high blood pressure in ambulatory settings. Cochrane Database Syst Rev. 2004;2004:CD004804. doi: 10.1002/14651858.CD004804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Nieuwlaat R, Wilczynski N, Navarro T, Hobson N, Jeffery R, Keepanasseril A, Agoritsas T, Mistry N, Iorio A, Jack S, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;2014:CD000011. doi: 10.1002/14651858.CD000011.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Gupta P, Patel P, Štrauch B, Lai FY, Akbarov A, Gulsin GS, Beech A, Marešová V, Topham PS, Stanley A, et al. Biochemical screening for nonadherence is associated with blood pressure reduction and improvement in adherence. Hypertension. 2017;70:1042–1048. doi: 10.1161/HYPERTENSIONAHA.117.09631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, Ramirez A, Schlaich M, Stergiou GS, Tomaszewski M, et al. 2020 International Society of Hypertension global hypertension practice guidelines. Hypertension. 2020;75:1334–1357. doi: 10.1161/HYPERTENSIONAHA.120.15026 [DOI] [PubMed] [Google Scholar]
- 81. Meddings J, Kerr EA, Heisler M, Hofer TP. Physician assessments of medication adherence and decisions to intensify medications for patients with uncontrolled blood pressure: still no better than a coin toss. BMC Health Serv Res. 2012;12:270. doi: 10.1186/1472-6963-12-270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Peeters LE, Feyz L, Hameli E, Zwart T, Bahmany S, Daemen J, van Gelder T, Versmissen J, Koch BC. Clinical validation of a dried blood spot assay for 8 antihypertensive drugs and 4 active metabolites. Ther Drug Monit. 2020;42:460–467. doi: 10.1097/FTD.0000000000000703 [DOI] [PubMed] [Google Scholar]
- 83. Lauder L, Ewen S, Kunz M, Richter LH, Jacobs CM, Kindermann I, Böhm M, Meyer MR, Mahfoud F. Adherence to antihypertensive drugs assessed by hyphenated high‐resolution mass spectrometry analysis of oral fluids. J Am Heart Assoc. 2020;9:e014180. doi: 10.1161/JAHA.119.014180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Zueger T, Gloor M, Lehmann V, Melmer A, Kraus M, Feuerriegel S, Laimer M, Stettler C. White coat adherence effect on glucose control in adult individuals with diabetes. Diabetes Res Clin Pract. 2020;168:108392. doi: 10.1016/j.diabres.2020.108392 [DOI] [PubMed] [Google Scholar]
- 85. Vrijens B, De Geest S, Hughes DA, Przemyslaw K, Demonceau J, Ruppar T, Dobbels F, Fargher E, Morrison V, Lewek P, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73:691–705. doi: 10.1111/j.1365-2125.2012.04167.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Nguyen TMU, La CA, Cottrell N. What are validated self‐report adherence scales really measuring?: a systematic review. Br J Clin Pharmacol. 2014;77:427–445. doi: 10.1111/bcp.12194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Bergland OU, Halvorsen LV, Søraas CL, Hjørnholm U, Kjær VN, Rognstad S, Brobak KM, Aune A, Olsen E, Fauchald YM, et al. Detection of nonadherence to antihypertensive treatment by measurements of serum drug concentrations. Hypertension. 2021;78:617–628. doi: 10.1161/HYPERTENSIONAHA.121.17514 [DOI] [PubMed] [Google Scholar]
- 88. Karve S, Cleves MA, Helm M, Hudson TJ, West DS, Martin BC. Good and poor adherence: optimal cut‐point for adherence measures using administrative claims data. Curr Med Res Opin. 2009;25:2303–2310. doi: 10.1185/03007990903126833 [DOI] [PubMed] [Google Scholar]
- 89. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self‐reported measure of medication adherence. Med Care. 1986;24:67–74. doi: 10.1097/00005650-198601000-00007 [DOI] [PubMed] [Google Scholar]
- 90. Lee CS, Tan JH, Sankari U, Koh YL, Tan NC. Assessing oral medication adherence among patients with type 2 diabetes mellitus treated with polytherapy in a developed Asian community: a cross‐sectional study. BMJ Open. 2017;7:e016317. doi: 10.1136/bmjopen-2017-016317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the Adherence to Refills and Medications Scale (ARMS) among low‐literacy patients with chronic disease. Value Health. 2009;12:118–123. doi: 10.1111/j.1524-4733.2008.00400.x [DOI] [PubMed] [Google Scholar]
- 92. Lefort M, Neufcourt L, Pannier B, Vaisse B, Bayat S, Grimaud O, Girerd X. Sex differences in adherence to antihypertensive treatment in patients aged above 55: the French League Against Hypertension Survey (FLAHS). J Clin Hypertens. 2018;20:1496–1503. doi: 10.1111/jch.13387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Hogan TP, Awad AG, Eastwood R. A self‐report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity. Psychol Med. 1983;13:177–183. doi: 10.1017/s0033291700050182 [DOI] [PubMed] [Google Scholar]
- 94. Warren‐Findlow J, Seymour RB. Prevalence rates of hypertension self‐care activities among African Americans. J Natl Med Assoc. 2011;103:503–512. doi: 10.1016/s0027-9684(15)30365-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Unni EJ, Farris KB. Development of a new scale to measure self‐reported medication nonadherence. Res Social Adm Pharm. 2015;11:e133–e143. doi: 10.1016/j.sapharm.2009.06.005 [DOI] [PubMed] [Google Scholar]
- 96. de Santa Helena ET, Nemes MIB, Eluf‐Neto J. Development and validation of a multidimensional questionnaire assessing non‐adherence to medicines. Rev Saude Publica. 2008;42:764–767. doi: 10.1590/S0034-89102008000400025 [DOI] [PubMed] [Google Scholar]
- 97. Espeche W, Salazar MR, Sabio R, Diaz A, Leiva Sisnieguez C, Olano D, Balbin E, Renna N, Grosse P, Flores RA, et al. Adherence to antihypertensive drug treatment in Argentina: a multicenter study. J Clin Hypertens. 2020;22:656–662. doi: 10.1111/jch.13830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Lötsch F, Auer‐Hackenberg L, Groger M, Rehman K, Morrison V, Holmes E, Parveen S, Plumpton C, Clyne W, De Geest S, et al. Adherence of patients to long‐term medication: a cross‐sectional study of antihypertensive regimens in Austria. Wien Klin Wochenschr. 2015;127:379–384. doi: 10.1007/s00508-015-0782-y [DOI] [PubMed] [Google Scholar]
- 99. Morrison VL, Holmes EA, Parveen S, Plumpton CO, Clyne W, De Geest S, Dobbels F, Vrijens B, Kardas P, Hughes DA. Predictors of self‐reported adherence to antihypertensive medicines: a multinational, cross‐sectional survey. Value Health. 2015;18:206–216. doi: 10.1016/j.jval.2014.12.013 [DOI] [PubMed] [Google Scholar]
- 100. Amin ZA, Kabir MI, Karami JH, Nahar N. Doctor‐patient communication to improve adherence to anti‐hypertensive treatment. Bangladesh Med Res Counc Bull. 2018;44:145–151. doi: 10.3329/bmrcb.v44i3.39938 [DOI] [Google Scholar]
- 101. Jafar TH, Gandhi M, Jehan I, Naheed A, de Silva HA, Shahab H, Alam D, Luke N, Wee Lim C, COBRA‐BPS Study Group . Determinants of uncontrolled hypertension in rural communities in South Asia—Bangladesh, Pakistan, and Sri Lanka. Am J Hypertens. 2018;31:1205–1214. doi: 10.1093/ajh/hpy071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. da Barreto MS, Cremonese IZ, Janeiro V, Matsuda LM, Marcon SS. Prevalence of non‐adherence to antihypertensive pharmacotherapy and associated factors. Rev Bras Enferm. 2015;68:54–60. doi: 10.1590/0034-7167.2015680109p [DOI] [PubMed] [Google Scholar]
- 103. Demoner MS, de Paula Ramos ER, Pereira ER. Factors associated with adherence to antihypertensive treatment in a primary care unit. Acta Paulista De Enfermagem. 2012;25:27–34. doi: 10.1590/S0103-21002012000800005 [DOI] [Google Scholar]
- 104. Aielo A, Santos R, Giatti S, Silva W, Parise B, Souza S, Cunha L, Lotufo P, Bensenor I, Drager LF. Obstructive sleep apnea, short sleep duration and drug adherence in patients with hypertension: the ELSA‐Brasil study. Sleep Sci. 2019;12:80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Ben AJ, Neumann CR, Mengue SS. The Brief Medication Questionnaire and Morisky‐Green test to evaluate medication adherence. Rev Saude Publica. 2012;46:279–289. doi: 10.1590/s0034-89102012005000013 [DOI] [PubMed] [Google Scholar]
- 106. Ungari AQ, Fabbro AL. Adherence to drug treatment in hypertensive patients on the Family Health Program. Braz J Pharm Sci. 2010;46:811–818. doi: 10.1590/S1984-82502010000400024 [DOI] [Google Scholar]
- 107. Tizato Feriato K, Lima de Gusmão J, Silva A, dos Santos CA, Sallazar Ferrera Pereiram R, Amendola F. Antihypertensive treatment adherence in workers of a general hospital. Rev Bras Enferm. 2018;71:1875–1882. doi: 10.1590/0034-7167-2016-0469 [DOI] [PubMed] [Google Scholar]
- 108. Akoko BM, Fon PN, Ngu RC, Ngu KB. Knowledge of hypertension and compliance with therapy among hypertensive patients in the Bamenda Health District of Cameroon: a cross‐sectional study. Cardiol Ther. 2017;6:53–67. doi: 10.1007/s40119-016-0079-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Natarajan N, Putnam W, Van Aarsen K, Beverley Lawson K, Burge F. Adherence to antihypertensive medications among family practice patients with diabetes mellitus and hypertension. Can Fam Physician. 2013;59:e93–e100. [PMC free article] [PubMed] [Google Scholar]
- 110. Gentil L, Vasiliadis HM, Preville M, Berbiche D. Impact of mental disorders on the association between adherence to antihypertensive agents and all‐cause healthcare costs. J Clin Hypertens (Greenwich). 2017;19:75–81. doi: 10.1111/jch.12869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Li Y. Analysis on the medication compliance of antihypertensive therapy and nursing strategy in hypertension patients. Chin J Prev Control Chronic Dis. 2017;12:893–897. [Google Scholar]
- 112. Zhao Y. Prevalence and risk factors for poor medication adherence among chinese hypertensive patients. Chin Pharm J. 2015; 24:559–562. [Google Scholar]
- 113. Shen Z, Shi S, Ding S, Zhong Z. Mediating effect of self‐efficacy on the relationship between medication literacy and medication adherence among patients with hypertension. Front Pharmacol. 2020;11:569092. doi: 10.3389/fphar.2020.569092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Shi S, Shen Z, Duan Y, Ding S, Zhong Z. Association between medication literacy and medication adherence among patients with hypertension. Front Pharmacol. 2019;10:822. doi: 10.3389/fphar.2019.00822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Tam L. Medication treatment analysis of 287 eldery hypertensive patients. Clin Med Res Pract. 2017;8:47–48. [Google Scholar]
- 116. Yue Z, Bin W, Weilin Q, Aifang Y. Effect of medication adherence on blood pressure control and risk factors for antihypertensive medication adherence. J Eval Clin Pract. 2015;21:166–172. doi: 10.1111/jep.12268 [DOI] [PubMed] [Google Scholar]
- 117. Ding W, Song H, Shi J. Observation and analysis of 956 cases of essential hypertension in primary hospitals. Chin Foreign Med Res. 2017;5:145–147. [Google Scholar]
- 118. Pan J, Lei T, Hu B, Li Q. Post‐discharge evaluation of medication adherence and knowledge of hypertension among hypertensive stroke patients in northwestern China. Patient Prefer Adherence. 2017;11:1915–1922. doi: 10.2147/PPA.S147605 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119. Song W, Song D, Chen L, Pan Z. Influence of personality characteristics on medication compliance in hypertensive patients. J Public Health Prev Med. 2016;4:110–112. [Google Scholar]
- 120. Ha C. Analysis of the relationship between drug use and compliance of hypertensive patients in units. J Mod Med Health. 2012;3:396–397. [Google Scholar]
- 121. Wang X, Li P. Compliance and influencing factors of drug therapy in hypertensive patients in community. Chin Community Doctors. 2018;25:176–177. [Google Scholar]
- 122. Yang S, He C, Zhang X, Sun K, Wu S, Sun X, Li Y. Determinants of antihypertensive adherence among patients in Beijing: application of the health belief model. Patient Educ Couns. 2016;99:1894–1900. doi: 10.1016/j.pec.2016.06.014 [DOI] [PubMed] [Google Scholar]
- 123. Lui Y, Mao L, Liu HL. The study on the compliance of patients with antihypertensive therapy and on compliance relation to complication of hypertension. Guide China Med. 2010;20:179–182. [Google Scholar]
- 124. Chen P. Discussion about drug use and medication complicance in hypertensive patients. Heilongjiang Med J. 2015;6:1283–1285. [Google Scholar]
- 125. Gao J, Ding Y, Fu H. Evaluation of five common antihypertensive drugs in community hypertensive patients. Chin J Integr Med Cardio/Cerebrovasc Dis. 2017;15:2592–2594. [Google Scholar]
- 126. Li Z, Zhao Y‐P, Hu X‐Y. The association between multimorbidity and medication non‐adherence in elderly with hypertension in Western China. Hu Li Za Zhi. 2016;63:65–75. doi: 10.6224/JN.63.5.65 [DOI] [PubMed] [Google Scholar]
- 127. Long Y, Shen Q, Long Q, Liang YD, Tao XF, Xl Z. Current status of medication compliance of Kakka hypertension patients: a 642‐case study. J Nurs (China). 2020;27:40–43. [Google Scholar]
- 128. Xu H. Analysis of the use situation of antihypertensive drugs and medication adherence with hypertension. China Contin Med Educ. 2015;33:167–169. [Google Scholar]
- 129. Chen S. Analysis of clinical medication use and research on medication adherence in primary care hypertensive patients. Strait Pharm. 2018;7:261–262. [Google Scholar]
- 130. Li X, Peng M, Li Y, Kang Z, Hao Y, Sun H, Gao L, Jiao M, Wu Q, Quan H. Chinese herbal therapy and Western drug use, belief and adherence for hypertension management in the rural areas of Heilongjiang province, China. PLoS One. 2015;10:e0123508. doi: 10.1371/journal.pone.0123508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. Lulebo AM, Mutombo PB, Mapatano MA, Mafuta EM, Kayembe PK, Ntumba LT, Mayindu AN, Coppieters Y. Predictors of non‐adherence to antihypertensive medication in Kinshasa, Democratic Republic of Congo: a cross‐sectional study. BMC Res Notes. 2015;8:526. doi: 10.1186/s13104-015-1519-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Berhane Y, Worku A. Adherence to antihypertensive treatment and associated factors in Central Ethiopia. Int J Hypertens. 2020;2020:9540810. doi: 10.1155/2020/9540810 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Asgedom SW, Atey TM, Desse TA. Antihypertensive medication adherence and associated factors among adult hypertensive patients at Jimma University Specialized Hospital, southwest Ethiopia. BMC Res Notes. 2018;11:27. doi: 10.1186/s13104-018-3139-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Berhe DF, Taxis K, Haaijer‐Ruskamp FM, Mulugeta A, Mengistu YT, Burgerhof JGM, Mol PGM. Impact of adverse drug events and streatment satisfaction on patient adherence with antihypertensive medication—a study in ambulatory patients. Br J Clin Pharmacol. 2017;83:2107–2117. doi: 10.1111/bcp.13312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Bezie K, Mamo M. Antihypertensive medication non‐adherence and predictors among adult patients on follow‐up, Ethiopia: prospective cross‐sectional study. Eur J Clin Pharmacol. 2020;22:70–79. [Google Scholar]
- 136. Breitscheidel L, Ehlken B, Kostev K, Oberdiek MSA, Sandberg A, Schmieder RE. Real‐life treatment patterns, compliance, persistence, and medication costs in patients with hypertension in Germany. J Med Econ. 2012;15:155–165. doi: 10.3111/13696998.2011.635229 [DOI] [PubMed] [Google Scholar]
- 137. Schulz M, Krueger K, Schuessel K, Friedland K, Laufs U, Mueller WE, Ude M. Medication adherence and persistence according to different antihypertensive drug classes: a retrospective cohort study of 255,500 patients. Int J Cardiol. 2016;220:668–676. doi: 10.1016/j.ijcard.2016.06.263 [DOI] [PubMed] [Google Scholar]
- 138. Kretchy IA, Owusu‐Daaku F, Danquah S. Patterns and determinants of the use of complementary and alternative medicine: a cross‐sectional study of hypertensive patients in Ghana. BMC Complement Altern Med. 2014;14:44. doi: 10.1186/1472-6882-14-44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Sarkodie E, Afriyie DK, Hutton‐Nyameaye A, Amponsah SK. Adherence to drug therapy among hypertensive patients attending two district hospitals in Ghana. Afr Health Sci. 2020;20:1355–1367. doi: 10.4314/ahs.v20i3.42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Stavropoulou C. Perceived information needs and non‐adherence: evidence from Greek patients with hypertension. Health Expect. 2012;15:187–196. doi: 10.1111/j.1369-7625.2011.00679.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Wong MCS, Jiang JY, Griffiths SM. Factors associated with antihypertensive drug compliance in 83,884 Chinese patients: a cohort study. J Epidemiol Community Health. 2010;64:895–901. doi: 10.1136/jech.2009.091603 [DOI] [PubMed] [Google Scholar]
- 142. Lo SHS, Chau JPC, Woo J, Thompson DR, Choi KC. Adherence to antihypertensive medication in older adults with hypertension. J Cardiovasc Nurs. 2016;31:296–303. doi: 10.1097/JCN.0000000000000251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Li YT, Wang HH, Liu KQ, Lee GK, Chan WM, Griffiths SM, Chen RL. Medication adherence and blood pressure control among hypertensive patients with coexisting long‐term conditions in primary care settings: a cross‐sectional analysis. Medicine. 2016;95:e3572. doi: 10.1097/MD.0000000000003572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Sarika ML, Swain I, Mohanta P, Rout D, Quadari M. Relation between knowledge on hypertension management and medication adherence among patients with hypertension in selected hospital in Khurdha. Eur J Mol Clin Med. 2020;7:1140–1148. [Google Scholar]
- 145. Meena JK, Rustagi N. Compliance and complications of hypertension treatment among lifestyle clinic patients, Jodhpur, India. J Hypertens. 2018;36:e102. [Google Scholar]
- 146. Balasubramanian A, Nair SS, Rakesh PS, Leelamoni K. Adherence to treatment among hypertensives of rural Kerala, India. J Family Med Prim Care. 2018;7:64–69. doi: 10.4103/jfmpc.jfmpc_423_16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. Sheilini M, Hande H, Prabhu M, Pai MS, Devi ES, Kamath A, George A. Antihypertensive prescription pattern, self‐reported reasons for non adherence to antihypertensives and lifestyle practices among the elderly. J Clin Diagn Res. 2018;12:OC01–4. doi: 10.7860/JCDR/2018/29729.11025 [DOI] [Google Scholar]
- 148. Athiyah U, Machfud AR, Aldila F, Yunita L, Ananda MR, Rizka NE. Measurement of patient adherence to the use of Ntihypertensive drugs by Mmas‐8 nnd pill count in 5 primary health Centres of Surabaya. FABAD J Pharm Sci. 2013;38:91. [Google Scholar]
- 149. Sulistiyowatiningsih EN, Herawati MU. A multicenter study treatment adherence of hypertension focused on primary healthcare in Indonesia. Asian J Pharm Clin Res. 2017;10:24–27. doi: 10.22159/ajpcr.2017v10s3.21356 [DOI] [Google Scholar]
- 150. Heizomi H, Iraji Z, Vaezi R, Bhalla D, Morisky DE, Nadrian H. Gender differences in the associations between health literacy and medication adherence in hypertension: a population‐based survey in Heris County, Iran. Vasc Health Risk Manag. 2020;16:157–166. doi: 10.2147/VHRM.S245052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Mamaghani EA, Hasanpoor E, Maghsoodi E, Soleimani F. Barriers to medication adherence among hypertensive patients in deprived rural areas. Ethiop J Health Sci. 2020;30:85–94. doi: 10.4314/ejhs.v30i1.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152. Dillon P, Smith SM, Gallagher P, Cousins G. The association between pharmacy refill‐adherence metrics and healthcare utilisation: a prospective cohort study of older hypertensive adults. Int J Pharm Pract. 2019;27:459–467. doi: 10.1111/ijpp.12539 [DOI] [PubMed] [Google Scholar]
- 153. Saito I, Kushiro T, Matsushita Y, Sato Y, Sagawa K, Tanaka Y, Tanigawa M, Okutani Y. Medication‐taking behavior in hypertensive patients with a single‐tablet, fixed‐dose combination in Japan. Clin Exp Hypertens. 2016;38:131–136. doi: 10.3109/10641963.2015.1047949 [DOI] [PubMed] [Google Scholar]
- 154. Otenyo S, Maranga A. Factors affecting adherence to antihypertensive medication regimen among hemodialysis patients attending a private Hospital in Mombasa, Kenya. Int J Pharma Sci Res. 2018;9:755–760. [Google Scholar]
- 155. Gavrilova A, Bandere D, Rutkovska I, Šmits D, Mauriņa B, Poplavska E, Urtāne I. Knowledge about disease, medication therapy, and related medication adherence levels among patients with hypertension. Medicina. 2019;55:715. doi: 10.3390/medicina55110715 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156. Yassine M, Al‐Hajje A, Awada S, Rachidi S, Zein S, Bawab W, Zeid MB, El Hajj M, Salameh P. Evaluation of medication adherence in Lebanese hypertensive patients. J Epidemiol Glob Health. 2016;6:157–167. doi: 10.1016/j.jegh.2015.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157. Bou Serhal R, Salameh P, Wakim N, Issa C, Kassem B, Abou Jaoude L, Saleh N. A new Lebanese medication adherence scale: validation in Lebanese hypertensive adults. Int J Hypertens. 2018;2018:3934296. doi: 10.1155/2018/3934296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158. Farah R, Zeidan RK, Chahine MN, Asmar R, Chahine R, Salameh P, Pathak A, Hosseini H. Predictors of uncontrolled blood pressure in treated hypertensive individuals: first population‐based study in Lebanon. J Clin Hypertens. 2016;18:871–877. doi: 10.1111/jch.12775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159. Shakya R, Shrestha S, Gautam R, Rai L, Maharjan S, Satyal GK, Bhuvan KC, Rai MK. Perceived illness and treatment adherence to hypertension among patients attending a tertiary hospital in Kathmandu, Nepal. Patient Prefer Adherence. 2020;14:2287–2300. doi: 10.2147/PPA.S270786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160. Van Kleef ME, Van Maarseveen EM, Visseren FL, Blankestijn PJ, Bots ML, Spiering W. Prevalence and characteristics of medication non‐adherence assessed by quantitative liquid chromatography‐tandem mass spectrometry in patients with hypertension. Eur Heart J. 2019;40:746. doi: 10.1093/eurheartj/ehz748.0068 [DOI] [Google Scholar]
- 161. Warren J, Warren D, Yang HY, Mabotuwana T, Kennelly J, Kenealy T, Harrison J. Prescribing history to identify candidates for chronic condition medication adherence promotion. Stud Health Technol Inform. 2011;169:634–638. [PubMed] [Google Scholar]
- 162. Akintunde AA, Akintunde TS. Antihypertensive medications adherence among Nigerian hypertensive subjects in a specialist clinic compared to a general outpatient clinic. Ann Med Health Sci Res. 2015;5:173–178. doi: 10.4103/2141-9248.157492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163. Ekanem US, Dan EI, Etukudo GG, Ndon II, Etebom EE, Nkobo KB. An assessment of antihypertensive medication adherence among hypertensive patients attending the outpatient clinics in the University of Uyo Teaching Hospital, Uyo. Niger Med J. 2020;61:120–125. doi: 10.4103/nmj.NMJ_95_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164. Okwuonu CG, Ojimadu NE, Okaka EI, Akemokwe FM. Patient‐related barriers to hypertension control in a Nigerian population. Int J Gen Med. 2014;7:345–353. doi: 10.2147/IJGM.S63587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165. Saqlain M, Riaz A, Malik MN, Khan S, Ahmed A, Kamran S, Ali H. Medication adherence and its association with health literacy and performance in activities of daily livings among elderly hypertensive patients in Islamabad, Pakistan. Medicina. 2019;55:163. doi: 10.3390/medicina55050163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166. Zyoud SH, Al‐Jabi SW, Sweileh WM, Morisky DE. Relationship of treatment satisfaction to medication adherence: findings from a cross‐sectional survey among hypertensive patients in Palestine. Health Qual Life Outcomes. 2013;11:191. doi: 10.1186/1477-7525-11-191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167. Fernandez‐Arias M, Acuna‐Villaorduna A, Miranda JJ, Diez‐Canseco F, Malaga G. Adherence to pharmacotherapy and medication‐related beliefs in patients with hypertension in Lima, Peru. PLoS One. 2014;9:e112875. doi: 10.1371/journal.pone.0112875 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168. Jankowska‐Polanska B, Chudiak A, Uchmanowicz I, Dudek K, Mazur G. Selected factors affecting adherence in the pharmacological treatment of arterial hypertension. Patient Prefer Adherence. 2017;11:363–371. doi: 10.2147/PPA.S127407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169. Pluta A, Sulikowska B, Manitius J, Posieczek Z, Marzec A, Morisky DE. Acceptance of illness and compliance with therapeutic recommendations in patients with hypertension. Int J Environ Res Public Health. 2020;17:6789. doi: 10.3390/ijerph17186789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170. Wilinski J, Dabrowski M. Medication adherence in hypertensive patients of different cardiovascular risk treated in primary health care. Przegl Lek. 2013;70:377–380. [PubMed] [Google Scholar]
- 171. Jankowska‐Polanska B, Dudek K, Szymanska‐Chabowska A, Uchmanowicz I. The influence of frailty syndrome on medication adherence among elderly patients with hypertension. Clin Interv Aging. 2016;11:1781–1790. doi: 10.2147/CIA.S113994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172. Cabral AC, Moura‐Ramos M, Castel‐Branco M, Fernandez‐Llimos F, Figueiredo IV. Cross‐cultural adaptation and validation of a European Portuguese version of the 8‐item Morisky Medication Adherence Scale. Rev Port Cardiol (Engl Ed). 2018;37:297–303. doi: 10.1016/j.repc.2017.09.017 [DOI] [PubMed] [Google Scholar]
- 173. Efanov A. Predictors of antihypertensive medical treatment adherence decline. J Hypertens. 2018;36:e326. doi: 10.1097/01.hjh.0000549333.08779.21 [DOI] [Google Scholar]
- 174. Fatani FN, AlSobaei RM, Alobodi NS, Alshehri ZH, Alrajih HA, Fallatah AA. Poor compliance to anti‐hypertensive drugs among patients in Saudi Arabia. Indo Am J Pharm Sci. 2019;6:3752–3758. [Google Scholar]
- 175. Khayyat SM, Khayyat SM, Hyat Alhazmi RS, Mohamed MM, Abdul HM. Predictors of medication adherence and blood pressure control among Saudi hypertensive patients attending primary care clinics: a cross‐sectional study. PLoS One. 2017;12:e0171255. doi: 10.1371/journal.pone.0171255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176. Kang GCY, Koh EYL, Tan NC. Prevalence and factors associated with adherence to anti‐hypertensives among adults with hypertension in a developed Asian community: a cross‐sectional study. Proc Singapore Healthc. 2020;29:167–175. [Google Scholar]
- 177. Janezic A, Locatelli I, Dolenc M, Kos M. Patient adherence to antihypertensives in Slovenia. Int J Clin Pharm. 2014;36:850. [Google Scholar]
- 178. Olowe OA, Ross AJ. Knowledge, adherence and control among patients with hypertension attending a peri‐urban primary health care clinic, KwaZulu‐Natal. Afr J Prim Health Care Fam Med. 2017;9:e1–e7. doi: 10.4102/phcfm.v9i1.1456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179. Choi HY, Oh IJ, Lee JA, Lim J, Kim YS, Jeon TH, Cheong YS, Kim DH, Kim MC, Lee SY. Factors affecting adherence to antihypertensive medication. Korean J Fam Med. 2018;39:325–332. doi: 10.4082/kjfm.17.0041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180. Kim HJ, Yoon SJ, Oh IH, Lim JH, Kim YA. Medication adherence and the occurrence of complications in patients with newly diagnosed hypertension. Korean Circ J. 2016;46:384–393. doi: 10.4070/kcj.2016.46.3.384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181. Choi KH, Yu YM, Ah YM, Chang MJ, Lee JY. Persistence with antihypertensives in uncomplicated treatment‐naive very elderly patients: a nationwide population‐based study. BMC Cardiovasc Disord. 2017;17:232. doi: 10.1186/s12872-017-0665-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182. Márquez‐Contreras E, de la Figuera‐Von Wichmann M, Franch‐Nadal J, Llisterri‐Caro JL, Gil‐Guillén V, Martín‐de Pablos JL, Casado‐Martínez JJ, Martell‐Claros N. Do patients with high vascular risk take antihypertensive medication correctly? Cumple‐MEMS Study. Rev Esp Cardiol (Engl Ed). 2012;65:544–550. doi: 10.1016/j.recesp.2012.01.018 [DOI] [PubMed] [Google Scholar]
- 183. Lee CY, Huang CC, Shih HC, Huang KH. Factors influencing antihypertensive medication compliance in Taiwan: a nationwide population‐based study. Eur J Prev Cardiol. 2013;20:930–937. doi: 10.1177/2047487312451252 [DOI] [PubMed] [Google Scholar]
- 184. Ho CP, Yeh JI, Wen SH, Lee TJF. Associations among medication regimen complexity, medical specialty, and medication possession ratio in newly diagnosed hypertensive patients: a population‐based study. Medicine. 2017;96:e8497. doi: 10.1097/MD.0000000000008497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185. Cinar FI, Mumcu Ş, Kiliç B, Polat Ü, Bal ÖB. Assessment of medication adherence and related factors in hypertensive patients: the role of beliefs about medicines. Clin Nurs Res. 2021;30:985–993. doi: 10.1177/1054773820981381 [DOI] [PubMed] [Google Scholar]
- 186. Baran AK, Demirci H, Budak E, Candar A, Akpinar Y. What do people with hypertension use to reduce blood pressure in addition to conventional medication—is this related to adherence? Eur J Integr Med. 2017;13:49–53. [Google Scholar]
- 187. Okello S, Nasasira B, Muiru ANW, Muyingo A. Validity and reliability of a self‐reported measure of antihypertensive medication adherence in Uganda. PLoS One. 2016;11:e0158499. doi: 10.1371/journal.pone.0158499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188. Khan MU, Shah S, Hameed T. Barriers to and determinants of medication adherence among hypertensive patients attended National Health Service Hospital, Sunderland. J Pharm Bioallied Sci. 2014;6:104–108. doi: 10.4103/0975-7406.129175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189. Gupta P, Patel P, Štrauch B, Lai FY, Akbarov A, Marešová V, White CMJ, Petrák O, Gulsin GS, Patel V, et al. Risk factors for nonadherence to antihypertensive treatment. Hypertension. 2017;69:1113–1120. doi: 10.1161/HYPERTENSIONAHA.116.08729 [DOI] [PubMed] [Google Scholar]
- 190. Sandy R, Connor U. Variation in medication adherence across patient behavioral segments: a multi‐country study in hypertension. Patient Prefer Adherence. 2015;9:1539–1548. doi: 10.2147/PPA.S91284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191. Siddiqui M, Judd EK, Dudenbostel T, Zhang B, Gupta P, Tomaszewski M, Patel P, Oparil S, Calhoun DA. Masked uncontrolled hypertension is not attributable to medication nonadherence. Hypertension. 2019;74:652–659. doi: 10.1161/HYPERTENSIONAHA.119.13258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192. Chang TE, Ritchey MD, Park S, Chang A, Odom EC, Durthaler J, Jackson SL, Loustalot F. National rates of nonadherence to antihypertensive medications among insured adults with hypertension, 2015. Hypertension. 2019;74:1324–1332. doi: 10.1161/HYPERTENSIONAHA.119.13616 [DOI] [PubMed] [Google Scholar]
- 193. Sim JJ, Bhandari SK, Shi J, Liu IL, Calhoun DA, McGlynn EA, Kalantar‐Zadeh K, Jacobsen SJ. Characteristics of resistant hypertension in a large, ethnically diverse hypertension population of an integrated health system. Mayo Clin Proc. 2013;88:1099–1107. doi: 10.1016/j.mayocp.2013.06.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194. Cummings DM, Letter AJ, Howard G, Howard VJ, Safford MM, Prince V, Muntner P. Medication adherence and stroke/TIA risk in treated hypertensives: results from the REGARDS study. J Am Soc Hypertens. 2013;7:363–369. doi: 10.1016/j.jash.2013.05.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195. Bautista LE, Vera‐Cala LM, Colombo C, Smith P. Symptoms of depression and anxiety and adherence to antihypertensive medication. Am J Hypertens. 2012;25:505–511. doi: 10.1038/ajh.2011.256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196. Lor M, Koleck TA, Bakken S, Yoon S, Dunn Navarra AM. Association between health literacy and medication adherence among Hispanics with hypertension. J Racial Ethn Health Disparities. 2019;6:517–524. doi: 10.1007/s40615-018-00550-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197. Al‐Ruthia YS, Hong SH, Graff C, Kocak M, Solomon D, Nolly R. Examining the relationship between antihypertensive medication satisfaction and adherence in older patients. Res Social Adm Pharm. 2017;13:602–613. doi: 10.1016/j.sapharm.2016.06.013 [DOI] [PubMed] [Google Scholar]
- 198. Silver J, Marsh JJ, Johnson T, Mohundro B, Peacock E, Krousel‐Wood M. Trust in healthcare providers is associated with antihypertensive medication adherence among older black hypertensive adults. J Invest Med. 2019;67:540–541. [Google Scholar]
- 199. Breaux‐Shropshire TL, Brown KC, Pryor ER, Maples EH. Prevalence of blood pressure self‐monitoring, medication adherence, self‐efficacy, stage of change, and blood pressure control among municipal workers with hypertension. Workplace Health Saf. 2012;60:265–271. doi: 10.1177/216507991206000606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200. Gallagher BD, Muntner P, Moise N, Lin JJ, Kronish IM. Are two commonly used self‐report questionnaires useful for identifying antihypertensive medication nonadherence? J Hypertens. 2015;33:1108–1113. doi: 10.1097/HJH.0000000000000503 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201. Rajpura J, Nayak R. Medication adherence in a sample of elderly suffering from hypertension: evaluating the influence of illness perceptions, treatment beliefs, and illness burden. J Manag Care Pharm. 2014;20:58–65. doi: 10.18553/jmcp.2014.20.1.58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 202. Fortuna RJ, Nagel AK, Rocco TA, Legette‐Sobers S, Quigley DD. Patient experience with care and its association with adherence to hypertension medications. Am J Hypertens. 2018;31:340–345. doi: 10.1093/ajh/hpx200 [DOI] [PubMed] [Google Scholar]
- 203. Nguyen TP, Schuiling‐Veninga CC, Nguyen TB, Vu TH, Wright EP, Postma MJ. Adherence to hypertension medication: quantitative and qualitative investigations in a rural Northern Vietnamese community. PLoS One. 2017;12:e0171203. doi: 10.1371/journal.pone.0171203 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1
Tables S1–S18
Figures S1–S4
References 16, 65, 75, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152, 153, 154, 155, 156, 157, 158, 159, 160, 161, 162, 163, 164, 165, 166, 167, 168, 169, 170, 171, 172, 173, 174, 175, 176, 177, 178, 179, 180, 181, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199, 200, 201, 202, 203